In presenting to the profession the fifth and concluding volume of the “SYSTEM OF PRACTICAL MEDICINE BY AMERICAN AUTHORS,” the Editor may be permitted to refer briefly to labors which for years have called forth his strenuous endeavors. The original prospectus of the work was issued in 1881. The first volume was published in January, 1885; the second, in May, 1885; the third, in September, 1885; and the fourth, in February, 1886. In view of the delays inevitable in large and complicated literary enterprises, such unusual punctuality reflects credit alike on the zeal of the contributors and the energy and resources of the publishers. The duties of the Editor have been lightened and rendered agreeable by the unvarying courtesy and cordial co-operation of all connected with him in the undertaking; and he has been amply rewarded by the realization of his hopes in the favorable reception accorded to the successive volumes by the profession on both sides of the Atlantic. The plan of the work has been strictly adhered to, and the articles promised have been furnished without exception, although in a very few cases circumstances required a change in the authorship. Special mention is due to Dr. Louis Starr and to Dr. Judson Daland for the very valuable assistance they have rendered.
The only alloy to the pleasure which the Editor has had in the progress of the work has been the removal by death of so many of his distinguished collaborators: such men as Flint, Van Buren, Armor, Bemiss, and Elsberg will long be mourned by the profession.
The number of articles is 185, written by 99 authors, covering, with indexes, about 5600 pages, and throughout its whole extent the original purpose has been kept constantly in view, that the practical character of the work should adapt it specially to the needs of the general practitioner. In conclusion, the Editor feels that it is a subject of congratulation that through the combination of so many leading members of the profession it has been rendered possible to present in this work, for the first time, the entire subject of practical medicine treated in a manner truly representative of the American School.
PHILADELPHIA, JUNE, 1886.
GENERAL SEMEIOLOGY OF DISEASES OF THE NERVOUS SYSTEM; DATA OF DIAGNOSIS. By E. C. SEGUIN, M.D.
THE LOCALIZATION OF LESIONS IN THE NERVOUS SYSTEM. By E. C. SEGUIN, M.D.
MENTAL DISEASES. By CHARLES F. FOLSOM, M.D.
HYSTERIA. By CHARLES K. MILLS, A.M., M.D.
HYSTERO-EPILEPSY. By CHARLES K. MILLS, A.M., M.D.
CATALEPSY. By CHARLES K. MILLS, A.M., M.D.
ECSTASY. By CHARLES K. MILLS, A.M., M.D.
NEURASTHENIA. By H. C. WOOD, M.D., LL.D.
SLEEP, AND ITS DISORDERS. By HENRY M. LYMAN, A.M., M.D.
ACUTE AFFECTIONS PRODUCED BY EXPOSURE TO HEAT. By H. C. WOOD, M.D., LL.D.
HEADACHE. By WHARTON SINKLER, M.D.
VERTIGO. By S. WEIR MITCHELL, M.D.
TREMOR. By WHARTON SINKLER, M.D.
PARALYSIS AGITANS. By WHARTON SINKLER, M.D.
CHOREA. By WHARTON SINKLER, M.D.
ATHETOSIS. By WHARTON SINKLER, M.D.
LOCAL CONVULSIVE DISORDERS. By ALLAN MCLANE HAMILTON, M.D.
EPILEPSY. By ALLAN MCLANE HAMILTON, M.D.
THE NEURAL DISORDERS OF WRITERS AND ARTISANS. By MORRIS J. LEWIS, M.D.
TETANUS. By P. S. CONNER, M.D.
DISORDERS OF SPEECH. By EDWARD P. DAVIS, A.M., M.D.
ALCOHOLISM. By JAMES C. WILSON, A.M., M.D.
THE OPIUM HABIT AND KINDRED AFFECTIONS. By JAMES C. WILSON, A.M., M.D.
CHRONIC LEAD-POISONING. By JAMES C. WILSON, A.M., M.D.
[p. 6]PROGRESSIVE UNILATERAL FACIAL ATROPHY. By CHARLES K. MILLS, A.M., M.D.
DISEASES OF THE MEMBRANES OF THE BRAIN AND SPINAL CORD. By FRANCIS MINOT, M.D.
TUBERCULAR MENINGITIS. By FRANCIS MINOT, M.D.
CHRONIC HYDROCEPHALUS. By FRANCIS MINOT, M.D.
CONGESTION, INFLAMMATION, AND HEMORRHAGE OF THE MEMBRANES OF THE SPINAL CORD. By FRANCIS MINOT, M.D.
SPINA BIFIDA. By JOHN ASHHURST, JR., M.D.
ANÆMIA AND HYPERÆMIA OF THE BRAIN AND SPINAL CORD. By E. C. SPITZKA, M.D.
THE CHRONIC INFLAMMATORY AND DEGENERATIVE AFFECTIONS OF THE SPINAL CORD. By E. C. SPITZKA, M.D.
CONCUSSION OF THE BRAIN AND SPINAL CORD. By WILLIAM HUNT, M.D.
INTRACRANIAL HEMORRHAGE AND OCCLUSION OF THE CEREBRAL VESSELS, APOPLEXY, SOFTENING OF THE BRAIN, CEREBRAL PARALYSIS. By ROBERT T. EDES, M.D.
ATROPHY AND HYPERTROPHY OF THE BRAIN. By H. D. SCHMIDT, M.D.
SYPHILITIC AFFECTIONS OF THE NERVE-CENTRES. By H. C. WOOD, M.D., LL.D.
TUMORS OF THE BRAIN AND ITS ENVELOPES. By CHARLES K. MILLS, A.M., M.D., and JAMES HENDRIE LLOYD, A.M., M.D.
TUMORS OF THE SPINAL CORD AND ITS ENVELOPES. By CHARLES K. MILLS, A.M., M.D., and JAMES HENDRIE LLOYD, A.M., M.D.
INFANTILE SPINAL PARALYSIS. By MARY PUTNAM JACOBI, M.D.
DISEASE OF ONE LATERAL HALF OF THE SPINAL CORD. By H. D. SCHMIDT, M.D.
PROGRESSIVE LABIO-GLOSSO-LARYNGEAL PARALYSIS. By H. D. SCHMIDT, M.D.
DISEASES OF THE PERIPHERAL NERVES. By FRANCIS T. MILES, M.D.
NEURALGIA. By JAMES J. PUTNAM, M.D.
VASO-MOTOR AND TROPHIC NEUROSES. By M. ALLEN STARR, M.D., PH.D.
ASHHURST, JOHN, JR., M.D.,
Professor of Clinical Surgery in the University of Pennsylvania.
CONNER, P. S., M.D.,
Professor of Anatomy and Clinical Surgery in the Medical College of Ohio; Professor of Surgery, Dartmouth Medical College; Surgeon to Cincinnati and Good Samaritan Hospitals, Cincinnati.
DAVIS, EDWARD P., A.M., M.D.,
Lecturer on Physiology, Rush Medical College, Chicago, and lately Medical Superintendent of the Presbyterian Hospital, Chicago.
EDES, ROBERT T., M.D.,
Jackson Professor of Clinical Medicine in Harvard University, Boston, Mass.
FOLSOM, CHARLES F., M.D.,
Visiting Physician for Nervous and Renal Diseases, Boston City Hospital; formerly Assistant Professor of Mental Diseases in Harvard University, Boston.
HAMILTON, ALLAN MCLANE, M.D.,
Consulting Physician to the New York City Male and Female Insane Asylums; Hudson River State Asylum for the Insane; Consulting Neurologist to Hospital for Ruptured and Crippled; Attending Physician to Hospital for Nervous Diseases; Member of the New York Neurological Society.
HUNT, WILLIAM, M.D.,
Surgeon to the Pennsylvania Hospital, and to the Philadelphia Orthopædic Hospital and Infirmary for Nervous Diseases.
JACOBI, MARY PUTNAM, M.D.,
Professor of Therapeutics at the Women's Medical College, New York.
LEWIS, MORRIS J., M.D.,
Physician to the Episcopal Hospital and to the Children's Hospital; Assistant Physician to the Orthopædic Hospital and Infirmary for Nervous Diseases, Philada.
LLOYD, JAMES HENDRIE, A.M., M.D.,
Instructor in Electro-Therapeutics in the University of Pennsylvania.
LYMAN, HENRY M., A.M., M.D.,
Professor of Physiology and of Diseases of the Nervous System in Rush Medical College, Chicago; Professor of Theory and Practice of Medicine in the Woman's Hospital Medical College, Chicago; one of the Attending Physicians to the Presbyterian Hospital, Chicago, Ill.[p. 8]
MILES, FRANCIS T., M.D.,
Professor of Physiology and Clinical Professor of Diseases of the Nervous System, University of Maryland, Baltimore.
MILLS, CHARLES K., A.M., M.D.,
Professor of Diseases of the Mind and Nervous System in the Philadelphia Polyclinic and College for Graduates in Medicine; Lecturer on Mental Diseases in the University of Pennsylvania; Neurologist to the Philadelphia Hospital.
MINOT, FRANCIS, M.D.,
Hersey Professor of the Theory and Practice of Physic in Harvard University; Physician to Massachusetts General Hospital.
MITCHELL, S. WEIR, M.D.,
Member of the National Academy of Sciences; President of the College of Physicians of Philadelphia.
PUTNAM, JAMES J., A.B. (Harv.), M.D. (Harv.),
Physician to Out-patients at the Massachusetts General Hospital; Clinical Instructor at Harvard Medical College.
SCHMIDT, H. D., M.D.,
Pathologist to the Charity Hospital of New Orleans.
SEGUIN, EDWARD C., M.D.,
Clinical Professor of Diseases of the Mind and Nervous System in the College of Physicians and Surgeons, New York City.
SINKLER, WHARTON, M.D.,
Physician to the Philadelphia Orthopædic Hospital, and Infirmary for Nervous Diseases.
SPITZKA, E. C., M.D.,
Consulting Neurologist to the North-eastern Dispensary, and Physician to the Department for Nervous Diseases of the German Poliklinik.
STARR, M. ALLEN, M.D., PH.D.,
Professor of Diseases of the Mind and Nervous System, New York Polyclinic; Attending Physician to Department of Nervous Diseases, Demilt Dispensary.
WILSON, JAMES C., A.M., M.D.,
Physician to the Philadelphia Hospital, and to the Hospital of the Jefferson College; President of the Pathological Society of Philadelphia.
WOOD, HORATIO C., M.D., LL.D.,
Clinical Professor of Diseases of the Nervous System and Professor of Materia Medica and Therapeutics in the University of Pennsylvania; Neurologist to the Philadelphia Hospital; Member of the National Academy of Sciences.
| FIGURE | |
| 1. | DIAGRAM SHOWING THE ARC FOR REFLEX ACTION |
| 2. | DIAGRAM AND TABLE SHOWING THE APPROXIMATE RELATION TO THE SPINAL NERVES OF THE VARIOUS SENSORY AND REFLEX FUNCTIONS OF THE SPINAL CORD |
| 3. | CONTRACTION OF NORMAL ABDUCTOR INDICIS WITH STRONG CURRENT (AMIDON) |
| 4. | CONTRACTION OF PARALYED MUSCLE ON THIRTY-FIRST DAY OF BELL'S PALSY OF THE FACE (AMIDON) |
| 5. | DIAGRAM OF A TRANSVERSE SECTION OF THE SPINAL CORD THROUGH THE CERVICAL ENLARGEMENT |
| 6. | DIAGRAM OF A TRANSVERSE SECTION OF THE SPINAL CORD THROUGH THE LUMBAR ENLARGEMENT |
| 7. | HORIZONTAL SECTION THROUGH THE CENTRE OF THE RIGHT CEREBRAL HEMISPHERE |
| 8. | DIAGRAM OF VISUAL PATHS, DESIGNED TO ILLUSTRATE SPECIALLY LEFT LATERAL HEMIANOPSIA FROM ANY LESION |
| 9. | LONGITUDINAL (SAGITTAL) SECTION THROUGH THE BRAIN, TO SHOW THE DISTRIBUTION OF THE FASCICULI OF THE INTERNAL CAPSULE |
| 10. | DIAGRAM OF THE LATERAL ASPECT OF THE CEREBRAL HEMISPHERE |
| 11. | DIAGRAM OF THE MESAL ASPECT OF THE CEREBRAL HEMISPHERE |
| 12. | TOPOGRAPHICAL LINES APPLIED TO THE EXTERNAL CONTOUR OF THE HEAD |
| 13. | TOPOGRAPHICAL LINES APPLIED TO HENLE'S FIGURE OF THE SKULL |
| 14. | THE SAME TOPOGRAPHICAL LINES APPLIED TO THE LEFT CEREBRAL HEMISPHERE IN HENLE'S SKULL |
| 15. | SPECIMENS OF HANDWRITING IN TWO CASES OF GENERAL PARALYSIS OF THE INSANE |
| 16. | FEET OF A PATIENT WITH ACUTE MYELITIS |
| 17. | FEET OF A PATIENT WITH HYSTERICAL PARAPLEGIA |
| 18. | POSITION ASSUMED BY A HYSTERO-EPILEPTIC |
| 19. | POSITION OF CRUCIFIXION ASSUMED BY A HYSTERO-EPILEPTIC (SAME CASE AS FIG. 18) |
| 20. | POSITION ASSUMED BY A HYSTERO-EPILEPTIC (SAME CASE AS FIG. 18) |
| 21. | EXTREME OPISTHOTONOS IN A HYSTERO-EPILEPTIC (SAME CASE AS FIG. 18) |
| 22. | PRINCIPAL HYSTEROGENIC ZONES, ANTERIOR SURFACE OF THE BODY (AFTER RICHER) |
| 23. | PRINCIPAL HYSTEROGENIC ZONES, POSTERIOR SURFACE OF THE BODY (AFTER RICHER) |
| 24. | POSITION ASSUMED BY A HYSTERO-EPILEPTIC |
| 25. | OPISTHOTONOS OF TETANUS |
| 26. | CASE OF ATHETOSIS |
| 27. | LOWER FACE OF RIGHT HEMISPHERE |
| 28. | MOVEMENTS OF WRIST IN TELEGRAPHING) |
| 29. | METHOD OF WRITING ADOPTED BY A PATIENT WHO HAS MARKED SPASM OF FLEXORS OF FINGERS AND THUMB |
| 30. | TEMPERATURE CHART OF A CASE OF TUBERCULAR MENINGITIS IN A BOY EIGHT YEARS OLD |
| 31. | TRANS-SECTION OF UPPER LUMBAR CORD OF A PATIENT MODERATELY ADVANCED IN TABES DORSALIS |
| 32. | CHANGES IN THE CORD IN A CASE OF DIFFUSE SPINAL SCLEROSIS |
| 33. | CHANGES IN THE CELLS OF THE ANTERIOR HORN IN DIFFUSE SPINAL SCLEROSIS (SAME CASE AS FIG. 32) |
| 34. | SECONDARY DEGENERATION OF INTEROLIVARY LAYER |
| 35. | SECONDARY DEGENERATION OF INTEROLIVARY LAYER, CAUDAL OR DESCENDING PORTION |
| 36. | DECUSSATING DEGENERATION OF INTEROLIVARY LAYER |
| 37. | TEMPERATURE CHART OF A CASE OF CEREBRAL HEMORRHAGE |
| 38. | TEMPERATURE CHART OF A RAPID CASE OF CEREBRAL HEMORRHAGE |
| 39. | CHART SHOWING THE EXCESS OF TEMPERATURE IN A CASE OF MENINGEAL HEMORRHAGE |
| 40. | CHART SHOWING RISE OF TEMPERATURE BEFORE APOPLECTIC SYMPTOMS IN A CASE OF TUMOR OF RIGHT TEMPORAL LOBE |
| 41. | CHART SHOWING THE DIFFERENCE OF TEMPERATURE BETWEEN THE TWO SIDES IN A CASE OF HEMIPLEGIA |
| 42. | CHART SHOWING THE SAME AS FIG. 41 IN ANOTHER CASE OF HEMIPLEGIA |
| 43. | FLAT GLIOMA-CELL WITH ITS FIBRILLAR CONNECTIONS (OSLER) |
| 44. | HOMOGENEOUS TRANSLUCENT FIBRE-CELL (OSLER) |
| 45. | DIAGRAM OF SPINAL COLUMN, CORD, AND NERVE-EXITS (AFTER GOWERS) |
| 46. | SARCOMA PRESSING CERVICAL CORD (E. LONG FOX) |
| 47. | SARCOMA OF LOWER CERVICAL CORD |
| 48. | THE SAME AS FIG. 47 |
| 49. | THE SAME AS FIG. 47 |
| 50. | THE SAME AS FIG. 47 |
| 51. | FIBROMA OF LOWER DORSAL CORD |
| 52. | TUMOR OF CAUDA EQUINA |
| 53. | PSAMMOMA OF DORSAL CORD, JUST ABOVE LUMBAR ENLARGEMENT |
| 54. | THE SAME AS FIG. 53 |
| 55. | DIAGRAM SHOWING THE MENTAL RELATIONS OF MOTOR AND TROPHIC CELLS WITH CEREBRAL AND SPINAL NERVE-FIBRES (AFTER ERB) |
| 56. | VASO-MOTOR NERVES AND GANGLIA ACCOMPANYING THE ARTERIOLES IN A FROG (GIMBERT) |
| 57. | DIAGRAM TO REPRESENT THE MODE OF ACTION OF COUNTER-IRRITANTS APPLIED TO THE CHEST (LAUDER-BRUNTON) |
| 58. | DIAGRAM OF THE ARRANGEMENT AND CONNECTION OF THE MOTOR AND TROPHIC CENTRES AND FIBRES IN THE SPINAL CORD AND MOTOR NERVE (AFTER ERB) |
ABNORMAL EMOTIONAL STATES.—Emotional manifestations, spontaneous or provoked from without, are, in the civilized adult, held in check directly or indirectly by the will, or by so-called strength of character. Extreme variations are allowed as being within the normal, from the stupidity of the peasant and the impassability of the hero to the sensitiveness and almost unrestrained reactions of the child or of the artist. Each individual must be judged by his own and his racial and family standards in this respect. It is more particularly when the dulness or over-active state observed is in contrast with the subject's habitual demeanor that the condition is called pathological.
Emotional dulness, or the complete absence of any emotional manifestation, may depend upon (1) diminished sensibility to external influences; (2) sluggishness of cerebral action, more especially in the range of sensori-ideal processes, or to general want of intelligence; (3) absorption of the subject's cerebral powers in some special object, real or delusive. The first form is illustrated in various grades of idiocy and backwardness; the second, in fatigue, prostration, and in conditions of dementia; the third is well exemplified in cases of insanity where the patient is devoted to one delusion or dominated by hallucinations (melancholia attonita), in which case the subject may be told the most painful news, insulted most grievously, or threatened fearfully without manifesting grief, anger, or fear. In some instances absolutely no emotional life can be detected.
Emotional exaltation may be due to (1) increased sensibility to external influences; (2) to deficient self-control. The first condition is illustrated in neurasthenic and hysterical subjects and in forms of mania: slight or almost imperceptible provocations call forth reaction, a noise causes fear, a look anger or tears, etc.; the second mechanism is apparent in diseases (dementia paralytica) where the cerebral hemispheres are extensively diseased and the cerebral power lessened (more especially is this the case where the right hemisphere is injured), and in cases of simple debility or asthenia, as when we see a previously mentally strong man shed tears or start most easily in convalescence from acute disease.
It may also be stated, in general terms, that the emotions are manifested in inverse ratio to the subject's mental or volitional power. [p. 20] Psychologically, the emotions are intimately related, on the one hand, with sensory functions, and on the other with more purely mental functions. Anatomically, it is probable that emotions are generated in basal ganglia of the brain (thalami optici and ganglion pontis), in close association with the sensory areas of the cortex cerebri, while the volitional, inhibitory power is derived from regions of the cortex situated frontad. Clinically, we meet with abnormal emotional states in a great many diseases of the nervous system, more especially in hysteria, neurasthenia, and insanity.
DEPRESSION in the psychic sphere manifests itself by the presence of psychic pain (psychalgia), by slowness of emotive reaction and of intellection, and by the predominance of fear, grief, and other negative emotional states. This complex mental state is usually accompanied by corresponding physical symptoms—general debility, reduced muscular strength, slowness of visceral functions, and retarded metamorphosis. The features are relaxed and passive; the posture sluggish, indifferent, or cataleptoid; the animal appetites are reduced. It is seldom that the entire economy does not sympathize with the psychic state. In exceptional cases some emotions are abnormally active, as in hypochondriasis; or there may be abnormally active muscular movements, as in melancholia agitata. Usually, depression is a part (a fundamental part, however) of a more complex symptom group, as in hypochondriasis, melancholia, hysteria, the prodromal stage of mania or paralytic dementia, etc.; but sometimes it constitutes a so-called disease—melancholia sine delirio. Although depressed subjects often appear indifferent to their surroundings, and react slowly or not at all, it must not be supposed that their emotions are not subjectively active. They are often abnormally so, and psychic hyperæsthesia coexists with psychalgia. No anatomical seat can be assigned to the processes which constitute this state and the following; their psychic mechanism is unknown.
EXALTATION, or abnormally great mental activity (including emotions), so-called psyclampsia, manifests itself by a pleased or happy subjective state, by increased reaction to external stimuli, by unusually abundant and rapid ideation, and by a corresponding increase of somatic activity, as shown by apparent (?) excess of muscular power, of circulation, of visceral activity, and of the appetites. The entire being, in certain cases, becomes endowed with additional capacity and power. In the mental sphere this over-activity easily passes into incoherence and verbal delirium, while in the physical sphere it may translate itself into violence. Clinically, exaltation may show itself as an independent morbid state, known as mania sine delirio. It more commonly appears, with other symptoms, in the shape of ordinary mania, of delirium tremens, of dementia paralytica, etc. Exaltation often follows morbid depression, and these two states sometimes alternate for years (circular insanity). Exaltation, even when accompanied by violent muscular action, must not always be considered an evidence of increased nervous power. On the contrary, it is often a result of irritable weakness, and as such indicates a tonic and restorative medication.
ILLUSIONS.—By illusion is meant the result of malinterpretation of an external impression by disordered sensorial or cerebral apparatuses. All of the special senses and the common sensory nerves may be the [p. 21] media of illusions, but they more commonly manifest themselves in the visual and auditory spheres. A few examples will best illustrate the exact meaning of the term. An insane person mistakes a casual visitor for his brother or father: he fancies that a piece of furniture is a flowering shrub or a threatening animal; another patient will declare that the food in his mouth tastes of a particular poison; still another, having pains in the night, solemnly avers that he has been beaten or cut, etc. A real impression is made upon the centres for vision, taste, and common sensation, but it is wrongly interpreted or appreciated. The exact mechanism of illusions escapes our present means of analysis: the peripheral apparatus or the perceptive centre may be disordered; probably, in most cases, the latter. This is borne out by the fact that in many insane the illusions are in harmony with the delusions present in the mind, and then they are nearly akin to hallucinations. The word illusion is sometimes employed as synonymous of delusion, but this is an abuse of terms to be avoided. Healthy persons are subject to illusions, but the error is quickly corrected by more careful observation by the same sense, or by the use of others. The state of intoxication by cannabis indica (hasheesh) presents numberless illusions of all the senses, together with hallucinations.
HALLUCINATIONS.—By this term is designated the result of the projection into the external world, through nerves of common or special sensations, of formed sensations which arise in a disordered sense-apparatus or nerve-centre; or, in more popular language, it may be said to mean the perception of non-existent objects or impressions, creations of the imagination. Examples: Disease (sclerosis) of the posterior columns of the spinal cord irritates the roots of the sensory nerves, the result being pain at the periphery in the parts connected with the affected segment of the cord. So objective and real do these peripheral pains seem that if the patient's mind be weakened he may assert that they are due to his being beaten, stabbed, or bitten by some one or by an animal. After amputation, the absent member is long perceived by the subject, often with startling distinctness, and even after the sensation has passed away it may be brought back by faradizing the nerve-trunks above the stump. The patient may hear voices, music, or simple sounds when in reality there is silence, or he may be surrounded by imaginary images or plagued by hallucinatory smells and tastes. Hallucinations may also arise in the distribution of optic nerves.
Besides common hallucinations with their seeming reality and objectivity, we admit others which are less vivid, which do not startle or frighten the subject, and which are simply the outward projections of the patient's own thoughts (delusions). The subject of persecution by imaginary enemies may see around him the faces of his pursuers with appropriate expressions, or hears their insulting or threatening remarks, as outward plastic reproductions of his thoughts; but the patient himself recognizes the want of actual objectivity and clearness in these images. These we call, after Baillarger, psychic hallucinations or pseudo-hallucinations. Similar phenomena are observed in some sane persons under excitement and betwixt sleep and waking.
The mechanism of hallucinations is partly understood, and may be stated as follows: In some few cases a real disorder or defect in the [p. 22] peripheral sense-organ may give rise to false projections; for example, a tinnitus may become transformed into a distinct voice, a scotoma may be the starting-point of false pictures of a man or animal. The simpler hallucinations of pain, cutaneous, muscular, and visceral sensations may originate in irritation of the nerve-trunks (as where the nerves of an arm-stump are faradized and the patient feels his hand with fingers in motion). But the general or common genesis of hallucinations is in disordered states of nerve-centres, those for common sensations and the special centres or cortical areas in the brain. Thus, a morbid irritation of the cortical visual area or sphere will give rise to abundant hallucinations of sight; irritation of the auditory sphere to hallucinations of hearing, as sounds and voices, etc. It must be borne in mind that, however pathological hallucinations may be, they arise from the operation of a fundamental physiological law. In health we constantly refer our sensations or transfer them into the external world, thus creating for ourselves the non-Ego. All terminal sensory nerve-endings receive only elementary impressions or impulses from external agencies, and these are perceived and conceived as images, formed sounds, etc. in the appropriate cortical centres; then by the law of reference of sensations these elaborated, idealized conceptions or pictures are thrown outward again and contemplated as objective. In this physiological mechanism lies the kernel of truth which is included in idealism.
Hallucinations may occur without derangement of mind or impairment of judgment. Many instances are on record of transient or permanent hallucinations of various senses in perfectly healthy persons who were fully aware of the unreal character of what they saw or heard. Being of sound mind, they were able to make the necessary correction by reasoning or by the use of other senses. In very many forms of insanity hallucinations are prominent, though they also occur in quasi-sane conditions, as in hypochondriasis, hasheesh, belladonna, and opium intoxication, the stage between sleeping and waking, etc. As long as the subject is able to correct the false projections by reason or by the use of other senses he is considered sane.
Hallucinations are sometimes the cause of acts by the insane, some of them violent and even murderous actions. Hallucinations of sight and hearing are especially prone to lead to assaults, murders, etc. The occurrence for any length of time of acoustic hallucinations in insanity is accounted of bad prognosis.
DELUSIONS are synonymous, in a popular way, with false beliefs. Thus, we often speak of eccentric opinions, of fanatical or extravagant creeds, as delusions. In a certain sense probably all mankind cherish innumerable delusions. In a strictly medical and medico-legal sense, however, the term is applied only to false beliefs in respect to clearly-established, indisputable facts. Thus, a man who believes in Spiritualism or even in metempsychosis, or in the divinity of a certain personage, is not medically deluded; whereas, one who believes that a bare court is a flowering garden or that he himself is divine is deluded. The essential element in the conception of delusion is belief or conviction on the patient's part; and that is why delusions mean that the psychic functions are deeply and seriously impaired. Delusions may be conveniently divided into ideal and sensorial.
[p. 23](a) Ideal delusions are false ideas or concepts arising more or less spontaneously, or by morbid association in the subject's mind. For example: he believes that he is a god, that he has millions of money, that his soul is lost, that he has a thousand children, etc. Many of the delirious ideas experienced by insane patients are delusions, and so to a certain extent (subject to temporary corrections by reasoning and demonstration) are the notions of hypochondriacs about their health.
(b) Sensorial delusions are such as are founded upon illusions and hallucinations. The moment a subject is convinced of the reality of an illusion or hallucination, believes in its actuality, he is said to have a delusion. The change from illusion and hallucination to the state of sensorial delusion indicates a deeper psychic alteration—a failure of critical capacity or judgment. Examples: A man imagines the stump of a tree in front of him to be a human being, but by reasoning, by closer visual inspection, or by palpation he concludes that it is a tree, after all; this is a simple illusion. If he persists, in spite of argument and demonstration, in his assertion that the stump is a human being, he is said to have a delusion or to be deluded. If a person sees wholly imaginary flowers or hears imaginary voices, as long as he is capable of recognizing the falsity or want of actuality of these images or sounds he has a simple hallucination; if he ceases to make the necessary correction, and believes the flowers and voices to really exist, he has sensorial delusions. It should be borne in mind that sane persons may have hallucinations, and that some insane have no sensorial delusions; also, that some insane are capable of correcting, for a time at least or when closely questioned, their illusions and hallucinations. Apart from these exceptional conditions, delusions, sensorial and ideal, are most important symptoms of insanity. We also meet temporary delusions in toxic conditions (from Indian hemp, alcohol, etc.) and in the delirium of acute general disease, of low febrile states, starvation, etc. Delusions are sometimes named in groups, according to the prevailing type of mental action; then, we have exalted delusions, in which the false notions and beliefs are rose-colored or extremely exaggerated (as in paralytic dementia, etc.). Again, we speak of delusions of persecutions, where the patient fancies himself pursued, maltreated, insulted, or where he insanely follows up and persecutes others. Such classification is useful for purposes of clinical and psychical study.
Imperative conceptions or controlling morbid ideas and desires are ideal delusions presenting certain peculiarities; one of which is that of growth by accretion and assimilation by a sort of false logic and grotesque analogical reasoning, until from a mere fancy or notion the growth invades and governs the entire subjective life of the subject.
VIOLENCE is a complex symptom always deserving of study and psychological analysis. It may present itself as an increase of a naturally bad disposition or as a wholly new exhibition of irritability and temper. Beyond these limits it may assume the shape of abusive and foul language (not before employed by the subject), or of physical acts of a destructive or dangerous character. Viewing the condition from a psychological standpoint, we should endeavor to distinguish between merely impulsive or animal violence due to over-activity of the emotional state or to a loss of self-control (cortical inhibition), and quasi-deliberate acts due either to special delusions or to delirium. Abnormal irritability, or increase in an [p. 24] originally bad temper, is met with in hysteria, neurasthenia, and partial dementia. Masturbators and epileptics frequently exhibit this condition. In a state less pathological, from mere fatigue or overwork, irritability may temporarily show itself as a result of reduced cortical energy; and in such cases rest, a cup of tea or coffee, alcohol, or even ordinary food, restores good-nature and equanimity as by magic. In little children bad temper is a frequent precursor of illness, more especially of cerebral disease. Greater degrees of violence in speech and acts are met with in hysteria, neurasthenia, and in many forms of insanity, in the guise of exaggerations of animal propensities, to make a noise, break objects, injure persons in an aimless general way. Voluntary or quasi-voluntary acts of violence are those which are done under the influence of hallucinations, delusions, or of delirious ideas, usually by insane patients. The delirium of acute or inflammatory disease or of the typhous state is rarely active, although pericarditis sometimes gives rise to very violent delirium, and the mild delirium with picking and gesticulating of pneumonia, typhoid fever, etc. may sometimes simulate mania. In general terms, the words and acts of patients represent the ideas passing through their minds in a rapid confused way, much as in dreams. Violence done under the influence of clearly-defined hallucinations and delusions is most dangerous, because it is executed with apparent deliberation and volition. Thus, a man laboring under hallucinations of hearing, fancying himself insulted, may turn in the street and strike or shoot some one near him, the supposed author of the insult. An epileptic falls in a partial attack or has epileptic vertigo; as a part of the seizure there is a dream-like scene of assault, actual or threatened, upon him, and on rising from the ground, or after the momentary vertigo the patient, acting in accordance with the demands of the dream-like scene, makes an onslaught upon those near him or smashes furniture, etc. Seeing such acts, without knowing their genesis, one is liable to consider them normally deliberate and malicious. On recovering consciousness (which may not be for several hours or days) the epileptic patient appears utterly oblivious of his actions, and is much astonished to learn what he has done. In many cases of insanity violent acts are done through a similar psychic mechanism—i.e. through the domination of delusions. Delusions often give rise to what may be termed negative violence—resistance to personal care, treatment, giving of food, etc. This is exemplified in acute melancholia, with overpowering fears of all kinds and terrorizing hallucinations of sight and hearing. The patients crowd in corners or sit curled up, and resist with all their might whatever is done for them, even striking and biting the attendants.
Therapeutically, the question of physical restraint or non-restraint in the management of violence might be discussed here, but the question is one which can be much better considered in connection with the general treatment of insanity, and the reader is consequently referred for information to the article on that subject.
DELIRIUM is a term which has been so variously applied that a brief definition of it is wellnigh impossible. Illogical or unreasoning and incoherent thoughts expressed in words and acts may suffice to give a general idea of the condition. Extreme applications of the term are, for example, to say that in a case of extreme dementia the rambling, disconnected talk is delirium, or that in certain forms of monomania the [p. 25] expression of the patient's peculiar delusion is delirium. It seems to us that there should be a certain degree of activity in the production of morbid ideas, with confusion in their expression, to justify the use of the term delirium. Again, in some instances the delirious talking and acting are only the reflex of abundant hallucinations of various senses which beset the patient. In some other respects the term delirium is applied in several distinct ways: first, in a substantive form as a designation for the incoherent words and acts of a patient. Usually, it is then put in the plural form of deliria. Thus we have the more or less highly organized, fixed or changeable deliria of monomania, chronic mania, melancholia, paretic dementia, etc., and the confused and evanescent deliria of acute general diseases, intoxications, and many forms of insanity. In short, we may speak of a sick person's deliria as we would of a normal person's thoughts; or in still more elementary analysis deliria are abnormal or insane thoughts and corresponding action. Second, delirium is used adjectively as designating certain diseases—e.g. delirium tremens, delirium a potu, acute delirium, delirium of acute diseases, etc. The seat of the psychic processes which go to make delirium is undoubtedly the cerebral cortex. This view is supported partly by the clinical consideration that delirium bears a certain relation to the psychic development of the subject. Thus, we see in children and in the higher animals rudimentary or fragmentary deliria; in advanced age the delirium is feeble and wellnigh absent; while in ordinary adults with well-developed cerebration deliria are abundant and varied. From pathological anatomy we learn that deliria become simplified and subside in proportion as the cerebral cortex becomes more and more damaged by effusions, by pressure effects, or by degenerative changes. As to the relation between special histological pathological changes, our knowledge is small and to a certain extent paradoxical. Thus, it is universally admitted that delirium may be due either to hyperæmia or to anæmia of the brain. The delirium of alcoholic or cannabis intoxication may be fairly assumed to be of sthenic or hyperæmic origin, either by the nervous elements themselves being in an exalted state of irritability, or because an increase in the circulation of arterial blood in the brain leads to greater activity of the cellular elements. Again, delirium appears in conditions of general or cerebral anæmia, as in starvation, after prolonged fever, after the withdrawal of customary stimuli, etc. These views are confirmed by the fact that some deliria cease upon the administration of sedatives and narcotics, while others are relieved and cured by rest, stimulants, and food. On the other hand, a large class of deliria, as exhibited in the insane, escape pathological analysis; for example, the delirious conceptions of monomania occurring in apparent somatic health and without well-marked symptoms of cerebral disease. We are much in the dark as to what the processes may be by which delusional notions grow in the subjective life and manifest themselves outwardly as deliria. It is probable that in such cases there is no material lesion (appreciable to our present means of research), but a morbid dynamic condition, false reactions, abnormal centripetal and centrifugal associations in the psychic mechanism, with or without inherited bias. The diagnosis of delirium as a symptom is usually easy, but it is a task of no small difficulty to determine its pathological associations in a given case, and to draw from this study correct therapeutic indications. [p. 26] A careful review of the antecedent circumstances, of the patient's actual somatic condition, more especially as regards hæmic states and vaso-motor action, is indispensable.
LOSS OF CONSCIOUSNESS, COMA.—Suspension of all sensibility, general and special, with loss of all strictly cerebral (cortical) reflexes, is met with in many pathological states. Its physiology or mode of production is unknown, but there are good reasons for believing that the lesion, vascular or organic, affects chiefly the cortical substance of the hemispheres. Its clearest manifestation, clinically, is after depressed fracture of the skull or after concussion of the brain, without or with abundant meningeal hemorrhage. In the last case unconsciousness or coma appears as an exaggeration of drowsiness or stupor; after a fall the patient may be able to walk into the hospital, but soon becomes drowsy, then stupid, and lastly completely insensible. In the first case, that of depressed fracture of the skull, the raising of the depressed bone is often followed immediately by return of consciousness; the patient seems to wake as from a deep sleep. In medical practice there are many analogous conditions of abnormal pressure causing coma, as in meningitis, cerebral abscess, hemorrhage, embolism of cerebral vessels, etc. Long-continued or fatal coma may be caused by general morbid states, as uræmia, acetonæmia, surgical hemorrhage, intoxication by narcotics, alcohol, ether, etc., and by asphyxia. Momentary loss of consciousness is induced in the various forms of epilepsy, lasting from a fraction of a second (so short as not to interrupt walking) to one or two minutes, followed by the more prolonged coma of the asphyxial stage. Temporary unconsciousness is also caused by physical or moral shock, but in many such cases the heart is primarily at fault, and the condition is termed syncope. Although in practice it is most important to distinguish syncope from more strictly cerebral coma, yet it must be admitted (and such admission is important for therapeutics) that in both categories of cases anæmia of the brain (cerebral cortex) is the essential factor or immediate cause of suspension of consciousness. This view of the pathology of coma is borne out by the fact that the condition may be produced at will, experimentally or therapeutically, by compression of both carotid arteries. It may be well to mention here the pseudo-coma of hysteria. In these cases consciousness is really present, as shown by responses to violent cutaneous irritations (faradic brush), by quivering of the closed eyelids and resistance to attempts to open them, by vascular or muscular movements evoked by remarks of a flattering or abusive nature made in the patient's hearing, and by cessation of the condition after complete closure of the nose and mouth for forty-five seconds or one minute (asphyxia). In the typically unconscious state, as in cases of fracture of the skull or of intracranial pressure by exudations, clots, tumors, etc., there are several objective symptoms to be noted. The pupils are usually dilated and immovable (exceptions chiefly in narcotic poisoning); the pulse is reduced in frequency and retarded; it is sometimes full and bounding, or in other cases feeble and irregular. The breathing is often slow and irregular; the patient fills out his cheeks and puffs (smokes the pipe); sometimes the Cheyne-Stokes type of respiration is observed. In hysterical or hypnotic impairment of consciousness these important symptoms are absent: the patient seems simply asleep. Although coma is, strictly speaking, a [p. 27] symptom, it so often appears as the leading one of a group that it deserves study almost as a disease. Indeed, there are few more difficult problems for the physician than the case of a comatose subject without a good history of the preceding condition, causes, etc. It is impossible here to consider all the possibilities of this problem in diagnosis;1 we can only state the chief and most probable pathological conditions which may cause coma.
1 An able attempt at the differential diagnosis of comatose cases, by J. Hughlings-Jackson, will be found in Reynolds's System of Medicine, Am. ed., 1879, vol. i. p. 920.
(1) The patient may be epileptic. The following signs of a past convulsive attack should be sought for: a bitten tongue, fleabite-like ecchymoses on the face, neck, and chest, saliva about the face and neck, evidences of micturition or of seminal emission in the clothing, etc. There is usually a small rise of temperature after a single fit, and consciousness soon returns without assistance, or a second seizure appears.
(2) The patient may be suffering from surgical cerebral compression or concussion. Signs of injury about the head or other parts of the body, oozing of blood or sero-sanguinolent fluid from the ears and nose, will sometimes clear up the diagnosis. Especially suggestive of meningeal hemorrhage is a gradually increasing stupor without distinct hemiplegia.
(3) The coma may be uræmic. In some cases anasarca and slow pulse point at once to this pathological condition. In all comatose cases without history the urine should be drawn with a catheter for testing, and signs of various forms of Bright's disease may be detected. The ophthalmoscope (easily used in comatose subjects) may yield most valuable indications by revealing retinitis albuminurica or neuro-retinitis.
(4) The patient may be under the effects of a clot in the brain or of acute softening of a considerable part of the organ. Hemiplegia with conjugate deviation of the eyes and head is usually present, the head and eyes turning away from the paralyzed side, the patient looking, as it were, toward the lesion. A latent hemiplegic state may sometimes be determined by one-sided redness of the buttock, and by a slight difference of temperature between the two hands (paralyzed side warmer). The general temperature of the body (measured preferably in the vagina or rectum) exhibits a marked rise. After cerebral hemorrhage there is, according to Charcot and Bourneville, a fall below the normal during the first hour, followed by a steady rise to 106° or 108° F. at death in severe cases. After embolism or thrombosis, causing softening, the rise of temperature is less in extent and not as regularly progressive.
(5) The subject may be simply drunk or poisoned by alcohol. In such a case the patient may usually be roused momentarily by loud speaking, shaking, or by painful impression; the breath is alcoholic; the cerebral temperature subnormal or normal. The urine must be tested for alcohol.2 It must not be forgotten that on the one hand intoxicated persons are most prone to falls causing fracture of the skull or concussion, and on the other hand that the early stage of coma from meningeal hemorrhage resembles narcosis.
2 Anstie's Test.—A test solution is made by dissolving one part of bichromate of potassium in three hundred parts by weight of strong sulphuric acid. The urine is to be added drop by drop to the solution. If a bright emerald-green color suddenly results from this manipulation, it signifies that there is a toxic amount of alcohol in the urine.
(6) The coma of congestive or malignant malarial fever is to be [p. 28] distinguished mainly by the absence of physical or paralytic symptoms, coinciding with a high rectal temperature. The spleen is often enlarged. Some would add that Bacillus malariæ and pigment might be found in the splenic blood, withdrawn by a long, fine needle.
(7) Toxic narcosis, from opiates, morphia, chloral, etc., are often difficult of diagnosis, except that from opiates and morphia, in which extremely slow respiration and contracted pupils, with lowered temperature, point at once to the cause.
In studying cases of coma all the above-enumerated symptoms should be considered as of great negative or positive value: often the diagnosis is only made by exclusion. The Cheyne-Stokes respiration, pupillary variations, differences in pulse-rate and volume, are present in such varied conditions, irrespective of the nature of the lesion, as to render them of minor value in differential diagnosis.
DOUBLE CONSIOUSNESS is a rare condition, in which the subject appears to have separate forms or phases of consciousness, one normal, the other morbid. This occurs in hypnotic and somnambulic states, probably also in certain cases of insanity and epilepsy. The current of normal consciousness is suddenly broken; the patient enters into the second or abnormal state, in which he acts, writes, speaks, moves about with seeming consciousness; but after a variable time a return to normal consciousness reveals a break in the continuity of the memory: the patient has no recollection whatever of what he did or said in the morbid period. In the hypnotic state subjects may show increased power of perception, and are strangely susceptible to suggestions or guidance by the experimenter. In a second attack the patient often refers back to the first, and does things in continuation or repetition of what he previously did, apparently taking up the same line of thought and action. The morbid states, long or short, are joined together by memory, but are wholly unknown in the normally conscious states. In other words, the patient leads two (or three, according to a few observations) separate lives, each one forming a chain of interrupted conscious states. In epilepsy we observe remarkable breaks in normal consciousness: the patient goes through certain acts or walks a distance or commits a crime in a dream-like state, and suddenly, after the lapse of a few minutes, hours, or days, becomes normally conscious and has no recollection of what he did with such apparent system and purpose during the seizure. It might, perhaps, be as well to classify these phenomena under the head of amnesia. A case is on record where a man travelled, seeming normal to fellow-travellers, from Paris to India, and who was immensely astonished on coming to himself (return to common consciousness) in Calcutta. Many murders have been committed with apparent design and with skill by epileptics, who upon awaking from their dream-like state were inexpressibly horrified to hear of their misdeeds.
AMNESIA, or loss of memory, may vary in degree from the occasional failure to remember which is allowed as normal, to the absolute extinction of all mental impressions or pictures. This word and the expression memory are here used in a restricted sense, reference being had only to purely intellectual and sensorial acts related to intellection. If we take the general or biological sense of the term memory as meaning the retention of all kinds of residua from centripetal impressions and of motor [p. 29] centrifugal impulses, including common sensory and visual impressions, special sense impressions, all unconsciously received impressions, emotional, intellectual, and motor residua, we should consider amnesia in a correspondingly general way. This, however proper for a physiological study, would be far too complex and premature for an introduction to practical medicine. Recognizing memory, therefore, as a universal organic attribute—a capacity to retain impressions—we will treat of it only in the commonly-accepted sense referred to supra.
Failure of memory may be real or apparent. In the latter sense amnesia is induced by diversion of the attention into a channel different from that in which the line of inquiry is conducted. A normal example of this is seen in the state known as preoccupation, where a person intent upon a certain thought or action forgets who is about him, where he is, and if asked questions fails to answer or answers incorrectly. In pathological states, as in acute curable insanity, apparent loss of memory is often caused by the domination of an emotion or of delusions. In both cases, if the subject can be roused or brought to himself, he remembers all that we inquire about and is amused at his previous false answers or silence. Real amnesia consists in the actual blotting out of recollections or residua in a partial or general manner, for a time or permanently. These differences serve as the basis of a complicated subdivision of amnesia which it is not necessary to fully reproduce here.
Temporary partial amnesia is a variety which is frequently observed in normal persons, even the most gifted. A word or fact escapes us, seems wholly lost for a few minutes, hours, or days; the more we strive to recall it, the less we succeed; yet later, when not sought for, the fact or word appears in our consciousness as if spontaneously, but more probably by some effect of the law of association. Such partial and momentary forgetfulness may assume proportions which render it pathological. What is known as transitory aphasia may be classed in this group. In a few minutes or hours a person without apoplectic, epileptic, or paralytic phenomena loses all power to express his thoughts by speaking or writing; there is verbal amnesia and agraphia. The subject is conscious of his condition and of the wholly futile or incorrect attempts he makes to communicate with others.
Temporary complete amnesia is almost equivalent to loss of consciousness, yet not strictly so. For example, after a sharp blow upon the head a person may perform complicated acts, reply to questions, and apparently act normally, yet after a variable time he will declare that he remembers absolutely nothing of the injury and what he did or said for hours or days afterward. The same phenomenon is observed in the course of psychoses, neuroses (epilepsy), in some acute diseases, and in certain states of intoxication.
Permanent partial amnesia occurs in states of dementia, such as senile dementia, paralytic dementia, and in certain cases of aphasia. Great gaps exist in the patient's memory; some things are well recalled, others wholly and for ever effaced. The psychological law governing the failure of memory in these cases is that the earliest and strongest impressions survive, while recent and less forcible (i.e. less interesting) ones are lost. Substantives or names are especially liable to obliteration, as are also many of the delicate residua which lie at the basis of the subject's ethical conceptions and acts.
[p. 30]Permanent complete amnesia is observed at the end of degenerative cerebral diseases, as organic dementia, whether of the form termed secondary or that designated as paralytic. Sometimes after acute general diseases the memory may be a perfect blank for a considerable length of time, and education has to be repeated. Memory may be so completely absent that cases are known in which the patient gave a fresh greeting to the asylum physician every two or three minutes indefinitely, as if each were a first meeting. Momentary perception and automatic (reflex) response are there, but no impression is made; there is no residuum left in the cortical centres. In these cases amnesia is accompanied by degeneration of the visual, auditory, etc. cortical areas or centres.
An interesting form of amnesia, not generally recognized as such, is the loss of acquired skill in muscular movements, such as are necessary for writing, for using tools, and for doing various delicate professional movements. Here the motor residua acquired by laborious education or training are gradually lost without actual paralysis or ataxia. This variety is exquisitely illustrated by certain cases of dementia paralytica where long before marked intellectual symptoms occur there is loss of skill in mechanical arts and in handwriting.
In testing a subject's memory due attention should be paid to the law of the survival of older and more interesting residua, as well as to the power of the law of association. Such questions should be asked as pertain to recent events in the patient's experience, and about matters which are not closely related logically. A patient who might tell us nearly all about his early personal experiences, his business and family relations, incidents of his childhood, etc., would fail to remember what he had for breakfast, what he did the day before, etc.
The physiological cause of real amnesia is impairment in the vitality (nutrition) of ganglion-cells in the various cerebral sensory areas or centres, and of the motor area as well (motor residua). In cases of transitory amnesia we suppose this to be due to the action of toxic agents, to anæmia, and impaired molecular or chemical nutrition, as after acute diseases, in extreme debility, in psychoses, etc. In cases of terminal permanent dementia, autopsies afford us evidence of degeneration and disappearance of ganglion-cells: we find granular and fatty pigmentation, atrophy, calcarous degeneration of these bodies, thickening and shrinkage of the neuroglia, and degenerative changes in blood-vessels. Doubtless degeneration or destruction of association fasciculi of nerve-fibres in the cortex cerebri or in the white substance plays a considerable part in the production of permanent amnesia, but we are as yet unable to give a clear demonstration of this. Theoretically, we may admit an organic loss of memory with the following conditions of the brain: (1) diseased perceptive (sensory) centres or motor area with normal association fasciculi; (2) normal perceptive centres and motor area with degenerate or broken association fasciculi, connecting these parts with one another and with the more strictly ideational or expressive (centrifugal) areas and parts of the brain and spinal cord.
Amnesia—or, more properly speaking, dulness of perception and feebleness of retention of residua—occurs as a strictly congenital condition from imperfect cerebral development, or a little later in life from infantile diseases, constituting one of the aspects of idiocy.
[p. 31]WORD-DEAFNESS is a special morbid psycho-sensory state in which the sounds of language lose their significance for the patient. The sense of hearing is preserved for common sounds, and even music in certain cases; words are heard, but not understood. A patient of mine having this symptom used to say, “If I go to a lecture or hear a sermon, I hear the speaker, but what he says is all Greek to me.” On the other hand, this gentleman could go to a concert and understand the musical notes. This condition occurs as a part of the symptom-group aphasia, or it may show itself independently in the course of limited cerebral cortical degenerations. The lesion causing word-deafness is usually found in the left hemisphere, in the first and second temporal gyri, or it may be in the inferior parietal lobule and gyrus supra-marginalis, penetrating deeply enough to injure fasciculi going into the temporal lobe. It would appear, from the evidence now before us, that the centre for psychic hearing is in the caudo-dorsal part of the temporal lobe.
WORD-BLINDNESS, or alexia, is another special morbid psycho-sensory state, in which the visible signs of language lose their significance for the patient. Usually there is no impairment of sight; the patient can see the letters and words as objects, but he cannot read them at all, or must do so letter by letter. Even numerals and pictures of objects in some cases become unintelligible. In testing for this condition a possible confusion with verbal amnesia must not be forgotten. In such a case the patient knows the word or object, but cannot name it; usually he can, however, inform us by signs or indirect expressions that he takes proper cognizance of the object. Alexia is present in a certain proportion of cases of aphasia, and it may be complicated with lateral hemianopia. The exact seat of the lesion producing alexia is at present unknown. Theoretically, however, we must place it in the course of paths from the cortical visual area (cuneus and adjacent gyri) to the general speech-centre. Psychic blindness for objects in general (soul-blindness of the Germans) is now quite conclusively proved to be due to degeneration of both occipital lobes, more especially their mesal gyri, where the visual centres are. This psycho-sensory state, with the accompanying cortical changes, has been demonstrated in cases of dementia paralytica.
APHASIA, or loss of the faculty of language, is so important a symptom as to deserve elaborate consideration in a separate article of this volume; and to it the reader is referred. Suffice it here to state that aphasia may be classified into three forms: (1) Sensory aphasia, in which there is primary disorder of the psycho-sensory (perceptive or centripetal) part of the complex central mechanism for speech; (2) Motor aphasia (including ataxic aphasia), in which the primary lesion affects the motor (expressive or centrifugal) parts of the mechanism; (3) Amnesic aphasia, in which loss of memory (effacement of residua) of words and signs is the prime condition.
HYPERÆSTHESIA is a condition of exalted excitability in the various parts of the sensory apparatus: terminal nervous organs, nerve-trunks, central gray matter. We may admit such a state as existing [p. 32] independently of consciousness, as where a lesion cuts off communication between the perceptive cerebral centres and the periphery, but in practice we consider only conscious hyperæsthesia. In this state the subject may be able to perceive (feel) slighter impacts than would affect a normal individual, or he receives an exaggerated, usually unpleasant, impression from ordinary excitations. It may also be said that hyperæsthesia exists as a purely subjective state, psycho-sensory hyperæsthesia, without external mechanical excitations.
(a) Hyperæsthesia of common tactile sensibility in the skin and mucous membranes is frequent. The least touch is felt with unpleasant acuteness and causes unusual reactions of a reflex order; frequently, but not necessarily always, a sensation of pain is produced at the same time. It has been claimed that in certain cases the points of the æsthesiometer could be perceived (distinguished as two points) at smaller distances than the average normal, but I have never been able to demonstrate this to my satisfaction. The simplest form of tactile hyperæsthesia is met with in persons of a highly nervous organization, in those under the influence of strong emotions, in the hypnotic state, and while intoxicated. The common pathological conditions in which increased sensibility is found are meningitis (cerebral and spinal), hydrophobia, tetanus, neuritis, dermatitis, hysteria, and spinal irritation; also in connection with inflammations and traumatisms.
(b) Hyperalgesia, often coinciding with (a), is that condition in which pain is produced by excitations so slight that they would not affect a healthy nervous apparatus: it is commonly designated as tenderness. Acute and dull, superficial and deep tenderness should be sought for and distinguished, as having different values in diagnosis. A type of deep tenderness is that found upon pressing steadily upon a diseased nerve-trunk. Acute superficial hyperalgesia is best studied in cases of trigeminal neuralgia and spinal irritation. Occasionally, universal hyperalgesia is met with, usually in hysterical women.
(c) Hyperæsthesia to thermal impressions is ordinarily shown with reference to cold. In cases of neuralgia or neuritis cold is felt excessively and painfully; in some cases of posterior spinal sclerosis there is the greatest dread of draughts of cold air, and patients protect their legs in an extraordinary manner.
(d) Hyperæsthesia of the muscular sense.3 The special sensations or notions of muscular states and activities which we possess may be considerably exalted, as shown by greater delicacy and rapidity of movements, and by the abnormally acute way in which perceptions of form and dimensions are obtained by the subject without assistance from other senses. Examples of this condition are met with in hysteria and hypnotism.
3 This term is employed as clinically sufficient. It is impossible in this article to enter into a consideration of the various theories held with reference to the function in question, whether it be psycho-motor, psycho-sensory, or a true muscular sensibility. It certainly differs much from the various forms of common sensibility, and has special paths.
(e) Visceral hyperæsthesia is chiefly shown by abnormal consciousness of the presence and action of an organ. Visceral pain usually accompanies this, and is the more prominent symptom.
(f) Increased reflex actions (emotional, motor, vaso-motor, and [p. 33] secretory) rarely fail to accompany hyperæsthesia in its various forms. In the hypnotic exaltation of muscular sense remarkable psychic effects may be induced, partly in a reflex way, but perhaps chiefly through the law of association.
PARÆSTHESIÆ are sensations which arise centrally in nerve-fibres or nervous centres, and are projected outward and referred to the periphery or surface by consciousness, in obedience to the general law of outward projection of sensations in the Ego. They may be produced by external agencies or arise centrally without demonstrable cause. Their number and variety are very great, varying somewhat with the descriptive powers and self-consciousness of the patient, the chief being pain, formication, numbness, coldness and heat, constriction and distension, malposition, imaginary movements, etc. etc.
(a) Pain, the most distinct and frequent of paræsthesiæ, is by most authors classed as a hyperæsthesia, yet a careful analysis will show the difference. Pain and hyperæsthesia often coexist and are inseparable, yet in a large proportion of cases of nervous diseases the former sensation occurs independently, sometimes in regions where absolute anæsthesia exists (anæsthesia dolorosa), and even apparently in lost parts (neuralgia after amputations). We are consequently justified in considering most pains as paræsthesiæ. Pain assumes many forms, some real and typical, others as various as the lively imagination of nervous patients can make them. Thus we have sharp, cutting, darting pains in neuralgia, posterior spinal sclerosis, etc.; aching, throbbing, pounding pains in cephalalgia, inflammatory and traumatic conditions; boring, crushing, distending, constricting, burning pains, etc. etc. In some cases the sensation is only semi-painful, and more akin to paræsthesia (neuritis, parenchymatous lesions).
(b) Numbness, prickling, and formication usually coincide. They may easily be produced experimentally by pressure upon a nerve-trunk or by the exhibition of aconitia, so that any one may study these sensations for himself. By taking one-fiftieth of a grain of Duquesnel's crystallized aconitia the experimenter will soon find himself the possessor of intense subjective sensations of prickling, numbness, vibrations, and cold, lasting several hours. He will be able to satisfy himself that though the finger-tips feel numb, as if there was a coating or layer of something interposed between the skin and objects, he can distinguish tactile perceptions very well. In the more serious experiment of compression of a nerve-trunk a most interesting succession of phenomena will be observed: the first effects of pressure are various paræsthesiæ in the parts supplied by the nerve; then these sensations (prickling, numbness, swelling, vibration, heat, and cold) cease; paralysis and anæsthesia occur. If the compression be now interrupted, after a few moments the paræsthesiæ reappear, more intensely, as a rule, and as they gradually fade a normal state of sensibility is re-established. By making such experiments it is easy to convince one's self that anæsthesia and numbness are different conditions: indeed, during the stage of recovery from nerve-pressure distinct hyperæsthesia may be demonstrated. These results throw much light on the origin and diagnostic value of paræsthesiæ as expressions of irritation, central or neural, of nervous elements. At the same time, in practice, we occasionally meet with slight dulness of tactile sensibility in numb [p. 34] parts. Another point to be remembered is that while patients usually complain loudly of paræsthesiæ, they are sometimes wholly unaware of anæsthesia (hysterical analgesia, for example); therefore sensibility should be tested even if the patient does not mention sensory disturbances.
Numbness, formication, etc. occur in a vast number of nervous affections—in cerebral and spinal organic lesions, in neuritis, in toxic conditions, and in neuroses. The distribution of paræsthesiæ is a valuable index to the seat of the lesion.
(c) Cutaneous itching and prickling may occur independently of any other skin lesion, constituting true or nervous prurigo. This may be universal and last for years.
(d) Paræsthesiæ of pressure are felt either as expansive or constrictive. The part appears swollen to consciousness, or it seems to be tightly compressed. Both these sensations are often felt about the head in a variety of pathological states, and an absurd and dangerous fashion has arisen of looking upon a sense of fulness in the head as indicative of hyperæmia. The sense of constriction may show itself around one toe, a leg, the trunk, around the neck, etc.; it may be narrow, like a cord, or broad and extensive, like a stocking or corset. Sometimes it is localized, and likened to the grasp of a hand or a spot-pressure. Not infrequently, especially in cases of paraplegia, the sensation of pressure is combined with subjective cold, the legs feeling as if tightly encased in ice.
(e) Subjective sensations of heat and cold are often of the strongest kind, and are very distressing. A part whose real objective temperature is normal may appear to the patient's consciousness as icy cold or burning hot, even to the degree of apparent contact of fire (causalgia of Mitchell). We observe such sensations in posterior spinal sclerosis, myelitis, neuritis, injuries to nerves. In some functional cases complaint is made of patches of hot or cold skin, not relieved by cold or heat.
(f) Odd sensations, such as rolling or longitudinal motion of something under the skin, general or local throbbing, coition movements, are described, especially in functional or hysteroid cases.
(g) Sensations of hunger, thirst, dyspnœa, defecation, micturition, the sexual feeling, may all appear in an abnormal or unprovoked manner, and are to be classed as visceral paræsthesiæ. An important paræsthesia of this variety is met with in cases of hypochondriasis and melancholia; it is a sense of indescribable distress, with constriction, usually at the epigastrium and about the heart—the precordialangst of the Germans, or, as we would term it, præcordial anguish.
(h) Paræsthesiæ of the muscular sense occur. The subject has a feeling as if a part were lying in an unnatural position, or as if it were being pulled or twisted in various ways, and he is sometimes obliged to assure himself by the use of sight and by tactile examination that the sensation is illusory.
(i) Hallucinatory paræsthesiæ are those which are so well defined and strong as to need the aid of other senses and reasoning to convince the patient of their unreality. A peculiar example of this is what occurs after amputation of a limb: for days or weeks the lost member is felt with the utmost distinctness; the absent fingers or toes may be moved in imagination and their position described.
(j) Delusional paræsthesiæ are such in which the patient (usually [p. 35] insane), no longer correcting his sensations by the use of other senses and by reasoning, firmly believes in their reality—i.e. externality. For example: in such patients visceral sensations give rise to the belief that there is a foreign body or an animal inside the patient, or that parts are misplaced or wrenched and beaten. Pains are thought to be due to blows received or to the bites of animals or projectiles thrown upon the patient. With perversions of muscular sense an insane patient may believe that he is flying or floating in the air.
In hypochondriasis many of the symptoms complained of are nothing but paræsthesiæ exaggerated by a morbid state of the mind, and sometimes created (projected) by expectant attention. The hallucinations of the insane are in great measure phenomena of this group, the projections, though special and common, never being so strong and definite as to acquire apparent objectivity.
The auræ of epilepsy are paræsthesiæ. For example: a sensation in the epigastrium preceding a fit indicates an irritation at the origin of the vagus nerve and its projection as a subjective sensation at the distribution of the nerve. An auditory or visual aura similarly represents a discharge or projection from the acoustic and visual cortical areas respectively.
In most cases of malingering, and in some cases of so-called railway spine, the symptoms so loudly complained of belong to the two classes of hyperæsthesiæ and paræsthesiæ; they are undemonstrable and non-measurable; only the patient himself can vouch for their reality. A diagnosis in such cases, without objective symptoms indicating well-known lesions, should be very reserved.
ANÆSTHESIA, or loss of sensibility, may exist in every degree, from one so slight as to be hardly demonstrable by delicate tests to the most absolute loss of all feeling. It manifests itself in various modes corresponding to the normal physiological varieties of sensibility; in most cases the loss of feeling involves all of these, but in others they are separately affected, and we observe the following types, pure or combined:
(a) Tactile Anæsthesia. The capacity to perceive superficial and gentle impressions upon the skin and mucous membrane, and the ability to locate and separate such impressions, may be lost, while other modes of sensibility remain normal.
(b) Analgesia is that condition in which painful impressions are not perceived, though common, caloric, or muscular sensibility may be normal or nearly so. Pricking, cutting, and bruising are unperceived. This, the most common variety, is usually met with in hysterical cases; it occurs at a certain stage of general artificial anæsthesia, in chronic alcoholism, extreme emotional states, and in hypnotism. Though a very striking symptom, it is not one of as serious meaning as loss of tactile or thermic sensibility. Often the patient is unaware of analgesia until tests reveal its existence.
(c) The sensibility of the skin to caloric is usually the last to disappear in the progress of an organic lesion, so that in certain cases (injury to nerves or spinal cord, myelitis, etc.) testing by ice or by a burning object is a sort of last resort. Before deciding in a given case that there is a complete break in the sensory tract, this test should be used as well as the application of the most intense induced electric current delivered upon the dry skin by a wire end.
[p. 36]In some cases of partial anæsthesia (e.g. in posterior spinal sclerosis) cold may be felt as heat and vice versâ, or pinching may be felt as burning, and be quite persistent.
(d) The so-called muscular sense may be greatly impaired or lost without ordinary anæsthesia. In such a case the subject is no longer directly and spontaneously aware of the exact position of his limbs, of passive motions done to them, and he executes voluntary movements with uncertainty. He is also unable to judge correctly of differences of weight in objects successively placed in his hand or hung from his foot. He needs the aid of sight to guide the affected limb and to judge of its position, etc. The awkwardness and uncertainty in voluntary movements by impairment of muscular sense must not be confounded, as is sometimes done, with ataxia, in which the attempted volitional movement is jerky and oscillatory, owing to the inharmonious action of antagonistic muscular groups.
(e) When a strong induced electrical current is passed through a muscle by means of wet electrodes applied to the skin, so as to cause a strong contraction, a special quasi-painful feeling, akin to that of cramp, is experienced in the contracting muscle, and is clearly distinguishable from the cutaneous sensation. This, the electro-muscular sensibility, may be lost independently of other modes of feeling and without loss of contractile power.
(f) Some observers claim that a special mode of sensibility exists in the skin by which varying degrees of pressure are estimated, independently of traction upon tendons and muscles (muscular sense), and that this may be separately impaired or lost.
(g) Visceral anæsthesia shows itself in the ordinary way by loss of that feeble degree of common sensibility which the internal organs possess, and also by impairment of their special functions, giving rise to anorexia, hydroadipsia, retention of feces and urine, loss of sexual feeling (without progenital anæsthesia). Of course, these symptoms may be due to other conditions, and each case must be carefully studied. In the insane, visceral anæsthesia gives rise to delusions of emptiness, destruction of organs, and even, if coinciding with general cutaneous anæsthesia, to the notion that the body is dead or absent.
A singular phenomenon often witnessed is retardation in the transmission of an impression (usually a painful one). Thus, in testing the sensibility of the skin of the legs in tabetic patients, it is observed that instead of the normal, almost instantaneous, appreciation of the impression made by a needle-point, there is a lapse of two, five, ten, or even sixty seconds between the pricking and the signal of sensation by the patient. It should always be determined in such cases whether the retardation is peripheral and actual, or central and due to psychic conditions (dementia, absorption in a delusional state). Thus, in a case of profound melancholia we may observe extreme slowness and dulness of sensory impressions or complete anæsthesia; but the symptoms would have a very different significance, diagnostic and prognostic, from the same noted in a mentally clear patient.
An important result of impairment of sensibility is a reduction or loss of reflex movements originating from the area or organ which is anæsthetic. This is shown in anæsthesia of the distribution of the trigeminus [p. 37] when the reflex protecting movements of the eyelids no longer take place, in atrophy of the optic nerve when the pupillary reflex actions are lost. In posterior spinal sclerosis we see several illustrations of this law: progressive degeneration of nerve-fibres in the posterior root-zones of the spinal cord, causing loss of patellar reflex, of vesical, rectal, and sexual reflexes, and in most cases of cilio-spinal reflexes and of muscular tonus. In these and analogous conditions one arc of the reflex mechanism is deranged, centripetal conduction is interfered with, and the reflex motor discharge can no longer be evoked.
That a similar pathological condition occurs in the cerebral mechanism, and may serve to explain many psychic symptoms, is very probable.
On the other hand, a destructive lesion may be so placed in the spinal cord or brain as to allow centripetal impressions to reach healthy spinal gray matter in the normal way, but preventing their passage frontad (upward) to be recognized by consciousness. In such a case we observe normal, or more commonly exaggerated, reflex action in parts which are insensible in the ordinary sense of the term. Indeed, in many cases the disconnected caudal portion of the spinal cord is in a state of vastly exaggerated reflex activity, as shown by the tetanoid and convulsive involuntary and reflex movements which take place in completely paralyzed and anæsthetic limbs (paraplegia from transverse myelitis). In general terms, it may be stated that when anæsthesia is due to lesions of peripheral nervous endings, of nerve-trunks, and of the posterior root system of the spinal cord, reflexes are diminished or lost.
It is often stated that anæsthesia causes ataxia of movement. This, from the results of experiments on animals and from clinical study, we believe to be a gross error. In animals and in man loss of sensibility gives rise to awkwardness or uncertainty in movement (increased if the eyes be closed) which is properly to be classed as a special variety of inco-ordination; but it is not from ataxia, in which irregular, jerky, oscillating motions occur when a volitional act is attempted, these movements resulting from want of harmony in the action of antagonistic muscles which in the normal educated state automatically act together to produce the desired result. Besides, we occasionally observe cases of typical spinal ataxia in which no impairment of sensibility can be observed.
THE TOPOGRAPHICAL DISTRIBUTION of alterations of sensibility requires careful determination in practice, as from it we obtain most valuable aid in diagnosis. The following are the principal types observed:
(a) Alterations of sensibility in one lateral (vertical) half of the body and head. We thus have hemihyperæsthesia, hemiparæsthesia, or hemianæsthesia, and the special senses on one side are frequently involved. This clearly hemi-distribution indicates that the lesion or functional disorder is in the cerebral hemisphere of the opposite side, more especially in the caudal segment of the internal capsule or in its areas of cortical distribution (occipital, temporal, and parietal lobes). The distribution of hemianæsthesia, etc. from organic disease in these parts is identical with that observed in some functional (hysterical) cases; we can make the diagnosis only by the help of other data.
If the sensory disorder does not affect the head, but is limited to one [p. 38] lateral half of the body, it is, if due to organic disease, quite certainly of spinal origin.
(b) Two homonymous extremities or the two lateral halves of the body may exhibit opposite states of sensibility—anæsthesia on one side and hyperæsthesia on the other. This rare condition is witnessed in hysteria and in some forms of injury to the spine (lesion of one lateral half of the cord at a certain level). In the latter case paralysis is usually present on the hyperæsthetic side: the symptoms constituting, with some others, Brown-Séquard's spinal hemiplegia or hemiparaplegia.
(c) Alterations of sensibility in one caudal (horizontal) half of the body are said to have a paraplegic distribution, and are usually due to lesions of the spinal cord. The upper level of the symptom may be at any point between the neck and the toes; and the frontal (upper) level indicates, due regard being had to the origin and oblique distribution of the spinal nerves, the highest limit of disease in the nervous centres. Very often, in organic disease especially, this is also indicated by the presence of a cincture feeling (paræsthesia) at the frontal (upper) limit of the anæsthesia, etc.
(d) Disorders of sensibility may be limited to one extremity. This very rarely depends upon cerebral disease, and in such a case the anæsthesia, etc. is evenly distributed throughout the member, being most intense at its extremity, and being without sharp, distinct limits near the trunk. When due to diseases of the spinal cord, the cerebral (upper) limit of the symptom is usually clearly defined in accordance with the distribution of sensory nerves from the other (healthy) parts of the cord: a constriction band often marks the limit. Sometimes the peripheral anæsthesia, etc. is more or less in the territory of certain nerve-trunks. When we find the distribution of the sensory symptoms to coincide exactly in the areas supplied by the large nerves of the limb, without cincture feeling, it is certain that the lesions affect one or more of these nerve-trunks or the plexus above. In not a few cases the symptoms are due to hysterical or dyscrasic conditions, and the seat of the lesions (dynamic or molecular lesion) is uncertain. In judging of the distribution of anæsthesia, etc. in a limb due regard must be paid to variations in nerve-branching and to collateral nerve-supply.
(e) Alterations of sensibility occurring in well-defined areas of the hand, trunk, or extremities, corresponding to the known distribution of nerves, almost always indicates disease of the nerve itself, much more rarely disease in the spinal cord at the origin of the nerve. The reflexes are then diminished or lost. In judging such cases Van der Kolk's law of the distribution of the motor and sensory filaments of nerve-trunks should be remembered: it is, that of the two sets of fibres in a mixed nerve, the sensory fibres are distributed to parts which are moved by muscles which receive the motor fibres of the same nerve. Thus, in nerve lesions the chief sensory symptoms are always peripheral or distal from the chief motor symptoms.
(f) Disorders of sensibility sometimes appear in patches or irregular areas whose nervous connections are indefinite. Such patches of anæsthesia, hyperæsthesia, or paræsthesia sometimes indicate foci of disease in the spinal cord (and brain?); as, for example, the pains, etc. of posterior spinal sclerosis. These patches may also occur in consequence of [p. 39] interference with local circulation of peripheral parts; and we meet with them in such conditions as hysteria, neurasthenia, alcoholism, etc.
(g) Universal hyperæsthesia, paræsthesia, and anæsthesia may be observed. The last condition, in the insane, is very apt to give rise to delusions of non-identity and death of the body.
THE SENSORY DISTURBANCES OF THE SPECIAL SENSES are well worth separate consideration.
(a) Optic Apparatus.—Hyperæsthesia of the retina shows itself directly in photophobia, and indirectly (reflexly) by lachrymation and involuntary closure of the eyelids. Paræsthesiæ of the optic nerve and retina show themselves as flashes or projections of white or colored light in the visual field. These may be irregularly or generally distributed in the field, or appear as hemiopic (vide infra), or sector-like forms. Phenomena of this order may be experimentally produced by pressure on the eyeball or by the application of electricity over or near the eye. Photopsiæ of most varied sorts, as flashes, colored scotomata, or quasi forms may immediately precede epileptic seizures or attacks of migraine, constituting an optic aura. In some cases this assumes a definite picture form, when it partakes of the character of an hallucination. Anæsthesia of the optic nerve and retina varies infinitely in degree, from slight blurring or veiling of vision (amblyopia) to complete blindness (amaurosis). Another result is sluggishness or complete immobility of the iris under the action of light. As regards distribution, optic anæsthesia may affect the visual fields uniformly and generally, or it may assume definite geometric forms, or may appear in irregular patches (scotomata).
The definite geometric defects are classed under the general head of hemianopsia, by which term is meant that one horizontal or vertical half of the visual field is obscured. (1) Horizontal hemianopsia is not bounded by a very sharp or straight boundary-line, and is almost always due to intraocular disease (retinal lesions, embolism of one large branch of the retinal artery, injuries, etc.). (2) Vertical hemianopsia is usually marked by a sharply-defined vertical limit in the visual field, passing through the point of fixation, or a little to one side of it more usually, leaving central vision very acute. (α) Temporal hemianopsia, in which the temporal halves of the visual fields are dark, represents anæsthesia of the nasal halves of the retinæ, and is usually caused by a lesion of the chiasm of the optic nerve, so placed at its frontal or caudal edge as to injure the fasciculi cruciati. This variety is usually bilateral, but a lesion might be so situated as to affect only one fasciculus cruciatis. (β) Nasal hemianopsia, in which the inner (nasal) halves of the visual fields are dark, represents anæsthesia of the temporal halves of the retinæ, and is caused by a lesion injuring one fasciculus lateralis or both fasciculi. In the former case the nasal hemianopsia would be unilateral; in the second case, bilateral or symmetrical, (γ) Lateral or homonymous hemianopsia is that condition in which physiologically similar halves of the visual field are darkened; for example, the temporal half-field of the left eye and the nasal half-field of the right. This represents anæsthesia of the nasal half of the left retina and of the temporal half of the right. The patient can only see, with one or both eyes, the right half of any object held directly in front of him. In such cases the lesion is always caudad of the chiasm, and may consist in interruption of the right optic tract, [p. 40] of disease of the primary optic centres (corpus geniculatum laterale and lobus opticus) on the right side, of the caudo-lateral part of the right thalamus, of the caudal extension of the internal capsule or optic fasciculus within the right occipital lobe, of the right superior parietal lobule or gyrus angularis penetrating deep enough to interrupt the optic fasciculus; or, finally, the lesion may injure the visual centre itself—viz. the cortex of the right cuneus and fifth temporal gyrus (of Ecker). Hemianopsia of any type may be incomplete or only sector-like—i.e. involving only a quadrant or less of one visual field or of both fields. (Vide article on Localization).
Perception of color may be reduced, confused, or abolished in the retina, either a diffused general way, throughout the field of vision, or following the laws of hemiopic distribution. In cases of hysteria, achromatopsia is not rarely met with, affecting the eye corresponding to the side on which the skin is analgesic or where paralysis exists. Hysterical achromatopsia may be transferred from one eye to another by the application of metals, by hypnotic manipulations, etc.
Hemianopsic phenomena may be functional and transient, as witnessed just before attacks of migraine or sick headache.
Attempts recently made, from purely theoretical considerations, to locate centres in the occipital cortex for perception of light, form, and color separately, are wholly unjustified or at least premature.
Loss of reflex pupillary movements is a symptom of much importance. It occurs chiefly under these conditions: (1) with paralysis of the iris due to lesion of the third cerebral nerve; (2) with amaurosis or anæsthesia of the retina; (3) with posterior spinal sclerosis. The last condition is distinguished from the others by the fact that while the reflex iritic movements are lost, the quasi-voluntary movement of accommodation efforts is preserved. This condition is known as the Argyll-Robertson pupil.
Diplopia, or double vision, is due to paresis or paralysis of one or more of the ocular muscles, and as such is to be classed under motor symptoms.
Megalopsia (apparent enlargement of objects) and micropsia (apparent reduction in size of objects) are sometimes due to disorder of the accommodation apparatus within the eye, and to local diseases causing displacement of the rods and cones of the retina; but they are often, no doubt, fanciful (in neurasthenia and hysteria). The same remarks apply to monocular diplopia.
(b) Acoustic Apparatus.—We know less of the sensory disturbances in the organs of hearing. Hyperæsia shows itself by undue (painful) sensitiveness to sounds, and by the ability to perceive sounds which are inaudible to normal persons. In meningitis, hydrophobia, the hypnotic state, etc. this condition is observed. Paræsthesiæ are very common, appearing as subjective noises or musical tones (tinnitus aurium) of the most varied kinds (roaring, hissing, blowing, tinkling, whistling, crashing, bell-sounds, etc.), which seem to the subject to be in his ear or in his head. In the present state of our knowledge it is impossible to positively distinguish tinnitus due to local non-nervous ear disease from that which is strictly neural or cerebral in origin. Certainly, intense tinnitus may coincide with complete anæsthesia of the acoustic nerve and a [p. 41] normal state of the middle ear. Theoretically, we may admit tinnitus (corresponding to photopsia in the optic apparatus) as due to an irritative lesion of various parts of the acoustic terminal nervous organ, the acoustic nerve, or the acoustic centre. An acoustic aura (subjective blowing, hissing, etc.) may immediately precede an epileptic attack. Subjective noises may be produced by excitation of the acoustic nerve and terminal organs by the galvanic currents; these galvanic acoustic reactions are regular in the normal condition, and are fully stated in works on electro-therapeutics. Anæsthesia of the acoustic system by peripheral, neural, or central (?) destructive lesions is frequent, and is distinguished from other forms of deafness chiefly by the fact that a sound transmitted through the bones of the cranium (as by a vibrating tuning-fork held against the upper teeth or above the ear) is not heard on one or both sides. Although in a few rare cases the attempt has been made to define nervous deafness for certain sets of notes or as limitations at either end of the musical scale, yet we are not prepared to recognize in neurological practice a condition of partial acoustic anæsthesia corresponding to hemianopsia or achromatopsia. We believe that this progress will be made, however, thus enabling us to locate disturbances in parts of the organ of Corti and in the cortical centre for hearing.
(c) Olfactory Apparatus.—Hyperæsthesia of this sense is at present considered more a personal peculiarity than as a symptom of disease. Paræsthesiæ show themselves as subjective odors of various sorts, and when transient may be an olfactory aura preceding epileptic attacks. In conditions of organic disease subjective odors may coincide with complete loss of smell. Anæsthesia of the olfactory nervous apparatus may be due to (1) strictly local disease in the nose, catarrh, etc.; (2) to anæsthesia of the trigeminus nerve and consequent local lesions; (3) to a truly nervous lesion affecting the olfactory nerves, the olfactory bulbs, the olfactory tracts, or, lastly, the cortical centre for smell (at present unknown in man). The two last morbid conditions are usually unilateral, and coexist with subjective odors.
(d) Gustatory Apparatus.—In this sense hyperæsthesia is clinically unknown, though as a result of education extreme delicacy of taste, a relative hyperæsthesia, may be produced. Paræsthesiæ are rare. In two cases in which we have observed the symptom (one of neurasthenia, the other of hypochondriacal melancholia) it consisted in a constant and most distressing sweet taste. The application of the galvanic current at the base of the brain, under the jaw, on the cheeks, and within the mouth produces subjective tastes of an acid or metallic nature. Anæsthesia of the gustatory nerve occurs after section of the lingual branch of the trigeminus—an operation sometimes done for lingual neuralgia, in which case the frontal two-thirds of the tongue on one side loses its property of perceiving taste. As the result of central disease next to nothing is known of this symptom. It is probable that sweet and acid tastes are perceived in the mouth and forward part of the tongue; bitter tastes on its caudal (posterior) third and in the throat (glosso-pharyngeal nerve). In the insane, paræsthesiæ and anæsthesia give rise to a great variety of delusions about the state of the parts, the nature of their food, poison in the food, etc.
As a part of typical complete hemianæsthesia the special senses are [p. 42] involved. When of hysterical origin the whole retina of one eye is generally devoid of sensibility, or it does not perceive colors. When the hemianæsthesia is due to a lesion of the caudal part of the internal capsule (organic anæsthesia), we should expect to find lateral hemianopsia, with dark half-fields on the same side as the cutaneous anæsthesia. We would not be understood as claiming that this point of distinction is as yet positively determined, but would advance it suggestively, subject to the result of observations on new cases.
PARALYSIS, or AKINESIS, is a condition in which loss of voluntary or involuntary muscular movement occurs through defective innervation. Such a strict definition is desirable, as excluding cases in which motion is abolished by local or general morbid states not essentially nervous, as in acute articular rheumatism, ruptures of muscles or tendons, fractures, extreme asthenia, etc.
Paresis is a term often employed to designate a paralysis partial in degree; it does not mean an essential muscular paralysis.
Paralysis varies infinitely in extent and distribution, yet certain types are recognized as having diagnostic value, and their exact determination is of great importance in practice.
(a) Hemiplegia, or paralysis of many muscular groups in one lateral half of the body.
(α) Common Hemiplegia.—In this, the most frequent form, we find loss of voluntary motion in many muscles of one side of the face and body. This condition may or may not be preceded by apoplectic or epileptic symptoms: it may occur gradually or suddenly. Although it is customary to say that in hemiplegia a patient is paralyzed on one side, this is not strictly correct, as careful observation shows that (1) in the face only the lower facial muscles are distinctly affected; the tongue itself is rarely paralyzed, but its projecting muscular apparatus is, so that when protruded it deviates as a whole toward the paralyzed side; the eye-muscles and masticatory muscles are unaffected; (2) in the extremities the loss of power is greatest in the hand and foot, less so in the arm and thigh, very slight in the muscular groups of the shoulders and hips; (3) the muscles of the neck and trunk, the respiratory muscles, and in general the muscles of the vegetative life are practically unaffected. These facts may be summarized by the statement that in common hemiplegia the greatest paralysis is shown in those muscular groups whose action is most independent on either side of the body; or, in other words, in those whose functions are most highly differentiated and whose innervation is most cortical (from the motor centres in the cerebral cortex). Those muscular groups, on the other hand, whose action is usually or necessarily simultaneously bilateral or associated across the median line—or, in other words, whose innervation is largely spinal or subcortical—are least paralyzed; while the purely automatic or reflex muscular apparatuses, those having a strictly spinal or sympathetic innervation, are not at all affected.
Common hemiplegia is rarely accompanied by hemianæsthesia.
[p. 43]It must not be forgotten that double hemiplegia may occur, in which case the symptoms are simply duplicated.
As regards the seat of the lesion in common hemiplegia, it may here be said, in general terms, that it is in the cerebral hemisphere opposite to the paralysis (with excessively rare exceptions which are susceptible of explanation), in its motor cortex, in the subjacent associated white fasciculi, or in the knee and caudal part of the internal capsule; the lesion may directly injure those parts or act upon them by compression.
(β) Crossed Hemiplegia (hémiplégia alterne).—In this form there is paralysis of many muscular groups on one side of the body, while the facial nerve or some other cranial nerve (or several cranial nerves together) show loss of innervation on the other side of the median line. Theoretically, therefore, there may be as many varieties of crossed hemiplegia as there are cranial nerves, but, practically, we meet only with a few forms, of which the following are the most common: (1) motor oculi (N. iii.) on one side, and body and face on the other; (2) facial nerve (N. vii.) on one side, and body on the other; (3) trigeminus nerve (N. v.) on one side (anæsthesia of face, paralysis of masticatory muscles), and body on the other; (4) abducens (N. vi.), facial (N. vii.), and acoustic (N. viii.) together on one side, and the body on the other. (5) With symptoms of No. i. we may have lateral hemianopia, dark half-fields on the same side as paralyzed extremities.
In crossed hemiplegias anæsthesia is more common; there is a strong tendency to bilateral extension of the paralysis, and neuro-retinitis is seldom absent before the close of life.
As regards the location of the lesion in crossed hemiplegias, it may be stated, in a general way, that it is in the base of the brain on one side of the median line, so placed as to directly injure one or more cranial nerves at their origin, and to compress or destroy the cerebral motor tract (pyramidal tract) above its decussation-point, and in some cases also the sensory tract in the crura, pons, and oblongata.4
4 For a statement of the exact seat of the lesion causing various forms of crossed hemiplegia, vide article on the LOCALIZATIONS OF LESIONS IN THE NERVOUS SYSTEM.
(b) Spinal Hemiplegia.—In this type the face and head are normal, excepting in some cases the iris; the extremities and trunk are more or less paralyzed on one side, the loss of power being more evenly distributed (i.e. less distal) than in hemiplegia of cerebral origin. Often there is also anæsthesia, and this is always on the other side of the median line, involving more or less of the whole side. The coincidence of these symptoms below the head indicates positively that the lesion is in the spinal cord, involving one of its lateral halves. Where there is no anæsthesia, care must be taken not to confound the condition with that in which a cerebral lesion causes paralysis of one arm and leg (combined brachial and crural monoplegia).
(c) Paraplegia.—The loss of voluntary power involves one transverse half of the body, usually the caudal. When only the lower extremities are affected, the condition is designated simply a paraplegia; when all the parts below the head are paralyzed, the term cervical paraplegia is employed. Frequently, the bladder and rectum are paralyzed, and in some cases the thoracic muscles also, leaving inspiration to be performed by the diaphragm alone. Often there is coextensive anæsthesia.
[p. 44]Hemiparaplegia is a rare variety in which one lower extremity is paralyzed while the other is anæsthetic.
The location of the lesion in paraplegias is in the spinal cord at various levels and in various portions of the gray and white columns. Theoretically, we may now again admit the old proposition that a paraplegia may be of cerebral origin: in such a case the loss of power should follow the laws of distal prevalence (vide (α)); there should be no anæsthesia or vesical paralysis, and the lesion ought to be one involving the paracentral lobules of both hemispheres (meso-vertex at fissure of Rolando).
(d) Monoplegia, or paralysis of one extremity or of one side of the face, is not rarely observed. It may be caused by central lesions in the brain or spinal cord, or by an affection of the nerve-trunks of the part. Cerebral monoplegias are of great importance in diagnosis, and may be distinguished from others by—(1) loss of power is greatest in the distal part of the affected member; (2) the precedence or coincidence of spasm (usually clonic or epileptiform) in the limb; (3) the absence of marked anæsthesia; (4) the preservation of muscular nutrition.
(e) Localized Paralysis.—The extreme types of this form of paralysis are paralysis of one external rectus and of one superior oblique. These muscles are each supplied by one whole nerve, and may therefore exhibit isolated paralysis. In the rest of the body, however, localized paralysis shows itself in groups of muscles as innervated by nerve-trunks or by certain so-called centres in the spinal cord. As examples of the former variety may be cited common facial paralysis (Bell's palsy) and paralysis of the extensor muscles of the hand by injury to the musculo-spinal (radial) nerve, of the foot and leg from lesions of the sciatic nerve. As examples of the second variety we have the irregular paralysis of anterior poliomyelitis (infantile spinal paralysis). In localized paralyses due to lesion of the nerve-trunks anæsthesia is usually present, whereas it is not common in the second variety. The determination of the seat of lesion in neural localized paralysis is much facilitated by bearing in mind Van der Kolk's law of the distribution of the motor and sensory fibres of a nerve-trunk.
Pseudo-paralysis—i.e. conditions in which voluntary motion is lost without defect in innervation, as from muscular disease, injuries, inflammations, etc.—is usually localized or irregularly distributed.
(f) The various internal organs, the viscera, supplied with striped or unstriped muscular fibres, may be paralyzed.
(g) The muscular coat of the vascular system beyond the heart may be paralyzed in extensive or limited areas—the so-called vaso-motor paralysis. This may assume hemiplegic or monoplegic or localized forms.
SPASM, or HYPERKINESIS, consists in abnormal and often violent involuntary muscular contractions, with or without loss of consciousness.
1. A purely mechanical classification of spasms into tonic and clonic forms is generally admitted as serviceable for clinical description, though we have as yet no positive knowledge of their relations to pathological conditions.
(a) Tonic or tetanic spasm is one in which the muscular contraction is continuous or constant for a measurable length of time. Thus, in some cases of petit mal there is a momentary stiffness or rigidity of the entire [p. 45] voluntary muscular apparatus (respiratory muscles included): the patient sits or stands with staring eyes as if petrified. In tetanus and local tetanoid seizures the muscles of large regions or of a part of a limb may remain contracted for many minutes; in the disease called tetany this condition may endure days and weeks—in hysteria and in some paralyses dependent upon organic disease for years or permanently. Prolonged tonic spasms occurring in chronic diseases are designated as contractures, and the affected parts are said to be tetanoid or spastic. A tonic spasm of long duration may show itself in involuntary muscles, as in the arteries, causing vaso-motor spasm and ischæmia; in the ciliary muscle, causing spasm of accommodation; in the urethra, œsophagus, etc.
A tonic muscular contraction accompanied by intramuscular pain is termed cramp.
Under this general head may also be classed the emotional or dramatic expressive spasms of hysteria and hystero-epilepsy—a condition in which the emotions or ideas occurring in the patient's mind are involuntarily translated externally into attitudes or gestures: e.g. anger, fear, disgust, amorous and religious feelings, etc.
(b) Clonic spasms are those which consist in rapidly intermittent muscular contractions, local or general. These may be rhythmical in time or form, as in paralysis agitans, or wholly irregular, as in chorea. Jerking is a quasi-popular designation of clonic spasms.
Tremor, or trembling, observed in persons during repose in any attitude, consists in small, wholly involuntary muscular contractions of sufficient extent to communicate to the parts a visible to-and-fro movement which is very often rhythmical. In order to distinguish this from any form of inco-ordination it is necessary that the observed movement should occur independently of all volitional effort. Thus in the senile state, in chronic alcoholism, in paralysis agitans, and in dementia paralytica we observe trembling of the facial and lingual muscles, of the extremities, and even of the whole body in some cases. These are usually conditions of permanent or chronic tremor, but the symptom is sometimes observed as a transient phenomenon, as after violent muscular effort, after excesses of various sorts, under the influence of emotions, etc. Occasionally, persons are met with who have trembled from childhood or early years without actual disease of the nervous system. It is clinically useful to divide tremor into varieties, as rhythmical and irregular, fine and coarse, constant and occasional. These terms define themselves sufficiently, so that no further statement is necessary, but we would repeat that it is of much advantage in diagnosis to determine accurately the characteristics of tremor.
2. A much more useful classification of spasms, and to a certain extent a physiological one, is into types according to their distribution in the body, following exactly the classification of paralyses. There are few topics of more utility for the physician to study, in our opinion, than that of monoplegias and monospasms, of hemiplegias and hemispasms in their genesis, mutual relations, and diagnostic significance.
(a) Hemispasm of cerebral origin, tonic or clonic (or both forms associated), may affect the face and limbs on one side of the body, with or without paralysis. As in hemiplegia, the morbid phenomena are greatest in the most distal muscular groups or in those whose innervation is most [p. 46] cortical. Very often hemispasm precedes, immediately or remotely, hemiplegia in the same parts. In other cases the relation is inverse, as when, after a severe hemiplegia, we find the paralyzed muscles in a state of nearly constant tonic contraction (secondary contracture), or when hemi-epilepsy follows a cerebral lesion. In the former case the spasm, clonic or tonic, is designated as pre-paralytic; in the second case, as post-paralytic. These terms are useful, because they are associated with laws of diagnosis and prognosis.
(b) Conjugate deviation of the eyeballs and head is an important symptom of gross cerebral lesions, and may be considered here, although it is probably due to paralysis. Still, the deviation itself always strikes the observer as a spasmodic effect. The symptom consists in a steady turning of the eyes, face, and head toward one or the other side, and may be best described by likening it to the normal act of looking at an object which is on one side or a little back of us. In one form—that due to an irritative lesion of the motor cortex of one hemisphere—the conjugate deviation forms a part of the hemiplegic epileptiform convulsions (mixed tonic and clonic) which are produced: the deviation is away from the lesion. In a second form, where severe hemiplegia is produced by an acute lesion of the motor area and the subjacent fasciculi of one hemisphere, whether the patient be comatose or semi-conscious, the deviation, of paralytic origin, is away from the paralyzed side of the body and toward the injured hemisphere: the patient is said to be looking at his lesion. In a third form, when the lesion is in one side of the base of the brain (more particularly of the pons), the deviation, again paralytic, is away from the lesion, as a rule. In some cases conjugate deviation exists only as a tendency to look to either side. It is always a valuable symptom in severe cerebral affections, more especially the apoplectic state.
(c) Paraplegic spasm is also shown in tonic and clonic forms. Partial tonic spasm of this distribution, with paresis of the legs, causes the gait or attitude known as tetanoid or spastic. The four extremities may be in this state of mixed paresis and contraction, as observed in some very young children whose cerebral motor area is probably undeveloped or ill-developed, or which has been damaged shortly after birth by meningeal hemorrhage.
(d) Monospasm, spasm affecting one side of the face or one extremity, may be of cerebral, spinal, or neural origin. Very often monospasm of clonic form serves to indicate with wonderful precision beginning disease (irritation stage) in limited parts of the cerebrum (in cortical centres and in the connected fasciculi for the face and limbs). Cerebral monospasms are sometimes combined so as to almost constitute hemispasm—i.e. brachio-facial or brachio-crural monospasm. Monospasm may precede or succeed monoplegia.
(e) Universal spasms, tonic, clonic, or mixed, occur in numerous diseased states—in hysteria, epilepsy, chorea, tetanus, toxic conditions, etc. A universal tonic spasm may last long enough (tetanus, epilepsy) to kill by apnœa.
(f) Localized spasms, not monoplegic, are observed. For example, the orbicularis palpebrarum may be the seat of clonic spasm, or the masseters of tonic spasm for long periods of time; the œsophagus or urethra may be temporarily closed by constriction; chorea may affect a small muscular [p. 47] group. A rhythmic spasm limited to a single muscle is termed myoclonus; the use of this term should not lead one to forget the nervous origin of the spasm. A localized tonic arterial spasm may be so severe and prolonged as to produce great ischæmia, even gangrene of the affected part.
(g) Fibrillary contractions, non-rhythmic contractions of fasciculi in muscles, spontaneous or provoked by direct mechanical excitation, may be considered as hyperkinesis. Subjectively, fibrillary contractions are felt as a quivering or as if a worm moved under the skin; objectively, they appear not unlike the rising and falling of a cord under the cutaneous covering. They unquestionably occur frequently in muscles which are undergoing degenerative or atrophic changes (progressive muscular atrophy), but they are also met with in cases of lead paralysis, neurasthenia, etc.
INCO-ORDINATION, or DYSKINESIS, is the condition in which volitional movements are not performed with normal precision and steadiness. Several varieties are recognized.
(a) Ataxic tremor is distinguished from common or spasmodic tremor by the fact that it is developed during the performance of a volitional act in parts which are quiet when not used. Thus, tremor appears in speaking, putting out the fingers, using the hands, etc. in the muscles actively employed, and occasionally also in others at the same time. This form of tremor is well seen in dementia paralytica, where in certain cases the patient's muscles are still until we induce him to make voluntary movements or provoke expression movements. In cases of disseminated sclerosis the same phenomenon is a characteristic symptom, a coarse tremulous ataxia or oscillatory trembling appearing whenever volitional acts are attempted. In looking, there appears nystagmus, a rhythmic ataxic tremor of some of the ocular muscles; in speaking, an irregular, jerky, slow, or syllabic speech is heard; and when the hand is carried to a given object or pointed the extremity exhibits oscillatory trembling. Common and ataxic tremors may coincide, as in some cases of dementia paralytica and in alcoholism.
(b) Ataxia is a symptom of the utmost importance, and its strict definition should be maintained. It is that form of inco-ordination in which there is want of harmony in the action of the various muscular groups employed in the voluntary performance of a given act. The simplest movement of an extremity (and more complicated ones a fortiori) is made up of simultaneous contractions of flexor and extensor muscles, often also of adductors and abductors in due proportion, so as to produce a steady position and movement of the parts. This is not accomplished by the will acting directly on the different muscles themselves, but through the medium of a co-ordinating mechanism which is strictly spinal (including the intracranial expansion of the cord as far frontad as the third ventricle), and which is educated or trained from the first days of life. We will the action and set the co-ordinating mechanism going, so that the movement is in a certain sense indirectly accomplished. Yet volition does interfere directly to a certain extent by estimating through the muscular sense, and by exerting the proper amount of force required, and by guiding the movement in a general way. The most striking peculiarity about ataxic movements is the defect in the harmonious action of the various [p. 48] (antagonistic) muscles employed, resulting in jerky, oscillatory, but non-rhythmic movements, constantly made worse by greater tension of the will. In simple tremor volition may for a few moments stop the movements (as best shown in paralysis agitans), while in ataxia the more the patient tries to achieve the act, the greater becomes the disorder. The anatomical fault is mostly in the spinal co-ordinating mechanism; the long-established motor and sensori-motor associations are interrupted or confused, and in some cases besides the muscular sense is impaired.5 The idea that ataxia results from faulty centripetal impressions due to various degrees of anæsthesia is certainly erroneous and misleading. In the first place, there are cases recorded in which typical ataxia of the extremities occurred without the slightest impairment of sensibility; and, secondly, neither in animals (section of posterior roots of spinal nerves) nor in man does ataxia appear as a result of anæsthesia. In this condition there is inco-ordination, to be sure, but not ataxia in the strict meaning of the term. Ataxia is nearly always a symptom of organic disease of the spinal cord, more especially posterior spinal sclerosis and diphtheritic myelitis. It may also occur from disease of the oblongata, pons, and crura cerebri. In certain cases of lesion in caudo-lateral part of the thalamus involving the caudal part of the internal capsule (irritation or partial destruction), we observe various forms of irregular movements which have been designated by Weir Mitchell as post-paralytic chorea. We long ago became satisfied that this term included quite a number of forms of inco-ordination, some cases showing choreiform and trembling movements, others ataxic tremor, true ataxia, and athetoid movements (also the true athetosis of Hammond?). It seems probable that diseases of the cerebellum, by exerting pressure on or by irritating subjacent parts, may sometimes cause pure ataxia of the extremities on the side opposite the lesion. That a strictly localized cortical lesion can give rise to ataxia we are not now prepared to admit.
5 Ataxia is greatly aggravated by closing the eyes.
(c) Uncertainty in voluntary movements is sufficiently defined by the term employed and by the absence of ataxia. This is well illustrated in those rare cases in which the muscular sense is impaired or lost: in such a case volitional movements, such as placing the fore finger on an object or fastening a button, are fairly well done with the aid of sight, but without it the hand and fingers grope almost or quite hopelessly about the object. It is important to note that persistent trying to do the act does not aggravate the disorder, but that, on the other hand, success is often achieved after feeling about. In certain cases of blindness irregular movements of the eyeball are observed, due to semi-voluntary efforts to look or to direct the eyeballs in the direction of a person or object. In states of cutaneous anæsthesia when the eyes are closed the same disorder appears in muscular movements. Claude Bernard many years ago showed that section of the posterior roots of spinal nerves in an animal was followed, not by ataxia, but by vague inco-ordination and staggering. In human cases we find that where the sensibility of one hand is lost or greatly impaired, without paralysis, there is extreme awkwardness and uncertainty in delicate muscular movements, but no ataxia. The staggering exhibited by patients having plantar anæsthesia is largely of this type: they stand fairly well while their eyes are open, but oscillate or [p. 49] fall when they are closed. This variety of inco-ordination may result from toxic conditions (alcohol), peripheral, neural, or central nervous disease. A few cases are on record which would seem to show that there is a centre for muscular sense in the cortex of the brain, in a part intermediate between the caudal sensory area and the central motor one—viz. in the inferior parietal lobule, supramarginal gyrus (and angular gyrus?). It has also been shown (by Spitzka and others) that there is a conduction tract for muscular sense, dorsad of the pyramidal tract in the pons and oblongata (in the stratum intermedium and interolivary tract), lesions of which produce inco-ordination (ataxia?) without marked paralysis or anæsthesia.
(d) Titubation, or staggering, is the inability to stand erect or walk straight because of impaired equilibrium. There is neither tremor nor ataxia present, and paralysis and anæsthesia are not necessary factors. It is distinguished from vertigo and dizziness by absence of subjective sensations of movement. Staggering may show itself in a general way or in the shape of latero-, retro-, or propulsion (disease of the internal ear, paralysis agitans). A well-defined variety of staggering is the wrongly-termed cerebellar ataxia. In this the patient, having disease of the cerebellum involving its vermis superior, stands with feet widely separated to increase his base of support; the body is bent somewhat forward, and the arms and hands are used as balancing-rods to maintain a sort of equipoise. In walking, this attitude is exaggerated, and if the feet be bare it will be seen that the toes are unconsciously clutching the floor for support; there is no outward jerk of the leg or stamp of the heel as in the ataxic gait, and closing the eyes does not aggravate the attitude or walk. Besides, if the extremities be separately tested, it is found that with closed eyes the patient can perfectly well place his fore-finger on his nose or one heel on the opposite patella (lying down). The proper term for the disorder is cerebellar titubation. Yet it must be remembered that titubation also occurs from disease of the oblongata and pons, from lesions of the base of the brain in general, and from alcoholic, etc. intoxication. In many cases titubation occurs in connection with vertigo or dizziness.
(e) Inco-ordination more or less of the ataxic form often affects the muscles of articulation, phonation, and deglutition, giving to the symptoms dysarthria, dysphonia, and dysphagia. Dysarthria and dysphagia are probably often caused by lesions of the insula and subjacent white substance, as well as by those affecting the oblongata. There are two recent autopsies which would indicate that there may be a cerebral cortical centre for phonation laryngeal movements: in the ventral extremity of the right third frontal gyrus—a part homologous to the speech centre on the left side of the brain. In some cases, however, dysphonia and aphonia indicate a lesion of the laryngeal nerves or of the oblongata (nucleus of NN. x. and xi.).
(f) Doubtless the internal muscular organs and the blood-vessels are frequently the seat of inco-ordinate or quasi-ataxic movements, but our present knowledge of these conditions amounts to very little.
It may be permissible to consider vertigo under the general head of inco-ordination, because it usually finds a motor expression, either actual or subjective. Subjective vertigo consists in a sense of whirling or horizontal movement which is clearly referred to the brain by the patient. The [p. 50] sensation is variously expressed: in some the head seems to whirl around; in others external objects seem to whirl about the patient horizontally or vertically; in others still there is a sensation of falling in a given direction or of dropping into a hole. Dizziness is a minor degree of subjective motion conjoined with more or less confusion and other paræsthesiæ in the head. Static vertigo is that form in which there is actual loss of equilibrium, or falling. It is observed more especially in diseases of the internal auditory apparatus, and it may be produced artificially by galvanization of the brain. If the electrodes are placed exactly on the median line, and the current passed fronto-caudad through the brain, no loss of equilibrium or vertigo is produced. If, however, the current is passed transversely through the brain, there is produced at the moment of the closure and opening of the circuit a distinct tendency to fall or an actual fall to one side: in closing the current the fall is always away from the negative pole or cathode. The greatest amount of disturbance is produced when the electrodes are placed on the mastoid processes or near them. Whether the disturbance of equilibrium is caused by a change in electrotonus in the hemispheres, or by a change in the vascular supply of the hemispheres (in one anæmia, in the other relative hyperæmia), is uncertain. A third explanation is equally plausible—viz. that the vertigo is caused by unequal excitation of the internal acoustic organs and the two halves of the cerebellum. This view would be supported by the fact that in animals and man a lesion of the acoustic nerve and of the processus ad pontem on one side produces strong rotary movements about the long axis of the body.
ABNORMAL REFLEX MOVEMENTS.—Some reference has already been made to absence or exaggeration of reflexes in the preceding paragraphs, but the importance of these symptoms demands that they should be separately considered.
A reflex action, in its simplest conception, is a movement (muscular, vascular, or psycho-motor) or a secretion which is the result of the transformation of a centripetal impression into a centrifugal impulse. The apparatus required for the accomplishment of the reflex action consists essentially of a sensitive surface of skin or mucous membrane, of tendinous or other deep structure, to receive the impression; a sensory afferent nerve to convey it; a nervous centre of the simplest structure (one or two ganglion cells) to receive and transform it; a motor or efferent nerve to transmit the resulting impulse to a common muscle, to the vascular wall of a vessel or viscus, or to a gland. These various terminal organs execute their normal functions in response to the centrifugal impulse, and thus give external or tangible evidence that the reflex action or reflex is completed. This mechanism, the reflex arc, is illustrated by the diagram (Fig. 1), which will also serve for the explanation of many of the morbid reflex states.
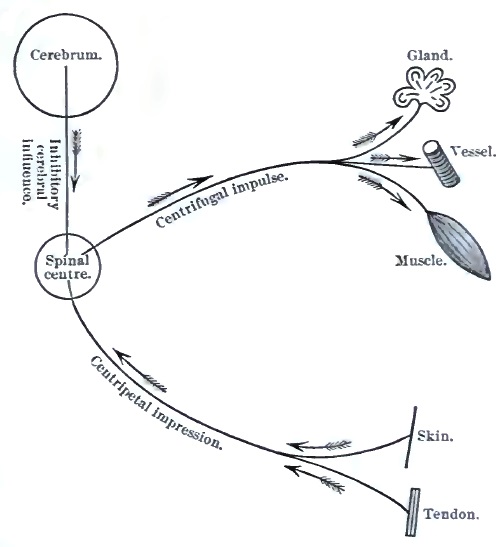
In the healthy animal body many important functions are performed under the law of reflex action; for example, many organic or secretory functions, the movements of hollow viscera, vascular movements, muscular tonus, defensive and expressive muscular movements. In the process of education many acts which at first must be learned by oft-repeated efforts, such as walking, playing upon musical instruments, etc., later become habitual and automatic, and are then largely executed by reflex [p. 51] action unconsciously, co-ordinated by the spinal (?) apparatus. Much of our intellectual activity is governed by the same law operating between the psycho-sensory and the psycho-motor apparatus.
Reflex actions are only to a moderate extent under the control of volition—indeed, most of them are subconscious—but a strong restraining action is unconsciously exerted by the cerebrum (vide Fig. 1) upon the spinal reflex centres. This is the so-called inhibitory cerebral influence. The existence of such an influence is shown by experiments upon animals, and by human cases in which, the cerebral activity being reduced or abolished, we observe a great increase in the frequency and extent of reflex movements, particularly in the common muscular apparatus.
Clinically, we distinguish cutaneous or superficial, tendinous or deep reflexes, according to the seat of the original excitation or testing-point. Cerebral or psychic reflexes are, however, also to be borne in mind. These reflexes may be abolished or increased.
(a) Diminution and abolition of reflex action are frequent symptoms of disease of the nervous system. The fault or break may be anywhere in the reflex arc, so that each case must be analyzed by itself. Let us consider the phenomena as exhibited by two widely distant and different apparatuses.
First, in the eye. In case of atrophy of the optic nerve the pupillary reflex is lost, the reflex action failing because the receptive surface and efferent nerve are injured. In certain cases of spinal disease (posterior spinal sclerosis) the same pupillary immobility is observed (the [p. 52] Argyll-Robertson pupil); and in this case the lesion either affects indirect efferent spinal fibres destined for the iris, or it is situated in the centre for the reflex action—viz. the gray matter of the lobus opticus. There may be loss of pupillary reflex due to injury of the direct efferent fibres of the arc (paralysis of the motor oculi, N. iii.). Lastly, the iris itself may be so diseased as to be incapable of contracting, though it receive the reflex impulse properly; the lesion is then in the terminal organ of the arc.
Second, the patellar tendon reflex. In a healthy individual, sitting at ease with one leg thrown over the other (knee over knee), upon tapping the ligamentum patellæ of the overhanging or free leg a contraction of the quadriceps muscle occurs, causing a visible forward movement of the leg and foot. This is the well-known patellar reflex or knee-jerk. The arc in this case consists of the ligamentum patellæ with its included sensory fibres as receptive organs, sensory (afferent) fibres of the crural nerve, a segment of the lumbar gray matter of the cord as centre, motor (efferent) fibres of the crural nerve, supplying the quadriceps extensor femoris, which is the terminal organ. Theoretically (vide Fig. 1), we can conceive of numerous abnormal conditions of parts of this arc which would lead to abolition of the patellar reflex, but in practice the following are the principal lesions to be thought of: Disease (sclerosis) of the posterior root-zones of the lumbar enlargement of the cord, as exhibited in the pre-ataxic stage of tabes; disease of the posterior roots themselves through meningitis or meningo-myelitis, as in diphtheritic ataxia; lesion of the nervous centre, as is frequently observed in cases of infantile poliomyelitis; a lesion of the crural nerve, involving its efferent or afferent fibres, or both sets of fibres, would produce the same result, as would also, lastly, a severe myositis or cancerous infiltration of the quadriceps muscle.
It is therefore evident that there is, or can be, nothing pathognomonic in the loss of a given reflex: it simply indicates a break in the reflex arc, the seat and nature of which remain to be determined in each case. The topographical study of reflexes in disease is of very great importance, more especially as a help to the correct location and extent of neural and spinal diseases. To assist this study, and for use more especially in connection with the ensuing sections on localization, Gowers's excellent diagram and table are reproduced in Fig. 2.
[p. 53]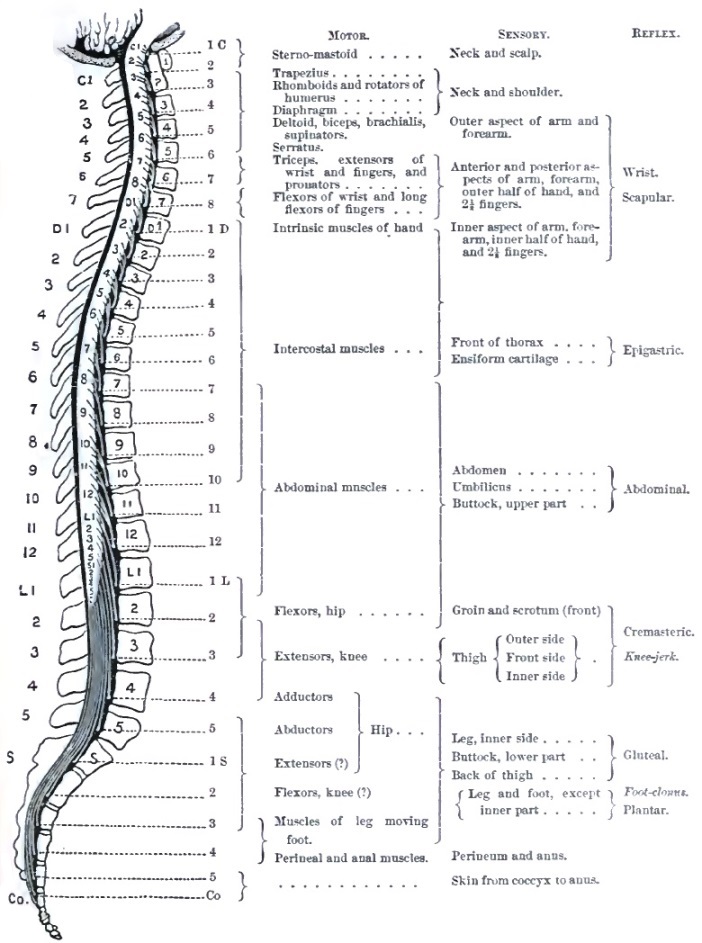
(b) Exaggeration of reflex actions. This is due, theoretically, to any condition which increases the excitability of the reflex arc, but practically and usually the cause of the increase is more or less complete removal of the inhibitory supraspinal or cerebral influence. The reflex arc itself remains structurally sound, but its function is abnormally active. Thus, we meet with the most exquisite exhibition of exaggerated reflexes in the paralyzed part after a transverse lesion of the dorsal part of the cord. The lesion cuts off all communication between the lumbar enlargement and the brain; no sensations pass to consciousness, and no volitional influence can be exerted upon the legs; yet the legs are abnormally active, the least touch on or pricking of the skin, tapping a tendon, handling a joint, the pressure of feces in the rectum, etc., produce more or less violent spasmodic movements of mixed clonic and tonic forms (spinal epilepsy). Increased knee-jerk, foot-clonus, and epileptoid trepidation are also present. Other proofs that removal of the inhibitory cerebral influences is the chief cause of increase of spinal reflexes are given by the [p. 54] history of various cerebral diseases. Thus, in hemiplegia with secondary contracture the cutaneous and tendinous reflexes on the paralyzed side are much exaggerated; in dementia paralytica, as a rule, the patellar reflex is increased on both sides; and in cerebral neurasthenia all reflexes are often extremely great.
A variety of increased tendon reflex is known as clonus—a series of rhythmic clonic muscular contractions set up by stretching the body and tendon of a muscle. This is best studied at the ankle. By holding the patient's leg nearly extended upon our left hand, and rather suddenly forcing back the foot (dorsal flexion) by pressing under the ball of the foot with our right hand, a series of oscillations or to-and-fro movements of the ankle-joint are produced for a few moments (ankle- or foot-clonus). Sometimes the same rhythmic clonic contractions may be produced in the quadriceps by quickly pulling down the patella with the leg semi-extended.
In some instances, together with great increase of tendon reflex, we observe a transfer of the centrifugal impulse to other nerves of the same extremity, or across the spinal cord to nerves and muscles of the homologous limb.
Another interesting manifestation of morbid reflex movements is the defensive tonic spasm of muscles about a diseased joint (of the hip-muscles in coxitis, of vertebral muscles in Potts' disease). This constitutes a valuable symptom for the differential diagnosis between articular and neural diseases in certain cases.
Clinically, increase of reflex action is not as valuable an indication as its absence, many healthy persons having high reflexes. Still, when studied comparatively as to topography (comparing the two sides of the body) and as to variations at different times in a given case, the symptom is of considerable assistance.
Our present knowledge of this great group of symptoms of nervous disease is in a somewhat chaotic state; and although we possess a large accumulation of facts of this category, their classification is incomplete and their explanation is for the most part theoretical and unsatisfactory. The following subdivisions may be made to include all the phenomena, and is sufficient for clinical purposes:
1. DEGENERATIVE ATROPHY, as distinguished from the simple atrophy of insufficient nutrition, of disuse of the parts, and of retarded growth, includes all those trophic symptoms in which, under the influence of nervous disease, the solid tissues exhibit histological and chemical alterations as well as reduction of volume. The principal factor of this group is—
(a) Muscular atrophy due to lesions of some part of the nervous apparatus (thus excluding directly traumatic or inflammatory atrophy), as seen in the course of progressive muscular atrophy, of various forms of poliomyelitis, of lead paralysis, of neuritis, and injuries of nerves. These muscular atrophies are characterized by reduction in the size of the affected muscles, by altered electrical reactions, and by histological [p. 55] changes. Reduction in size may affect one muscle or a muscular group shortly after paralysis (as in poliomyelitis, lead paralysis, affections of nerve-trunks), or without evident paralysis it may involve only small fasciculi of a muscle at a time (as in progressive muscular atrophy); so that we speak of diffused and fascicular atrophy, of secondary (post-paralytic) and primary atrophy. In some cases the wasting proceeds to such a degree that apparently no muscular tissue remains, and the skin seems to rest directly on the bones; in others the reduction in bulk is moderate, and is compensated by increase in the intra- and extra-muscular fat (thus in stout children the atrophy of severe poliomyelitis may be quite masked to the eye); in still another category the increase in connective tissue with fatty accumulation overbalances the muscular wasting, and we have the pseudo-hypertrophic condition. Alterations in electro-muscular contractility are most important signs of impaired muscular innervation and nutrition. They present numerous and somewhat complicated variations of value for diagnosis and prognosis, but which cannot here be noticed at length. The general principle underlying these variations is this: that a muscle deprived of its normal innervation (centrifugal or motor) soon loses its capacity to respond to the induced (faradic) current, and reacts in an abnormal way to the galvanic current. This constitutes the reaction of degeneration of Erb.6 The chief abnormality in the galvanic reaction of a paralyzed and diffusely atrophied muscle is its slow or wave-like contraction, which on a graphic, or even to the observer's eye, presents a striking contrast to the sharp, jerking, complete contraction of a healthy muscle. Besides, the reactions to the two poles become equal, or even reversed, so that we may obtain in testing by the polar method such formulas as CaCC = AnCC, or CaCC < AnCC. With reference to the failure of atrophied muscles to respond to the induced or faradic current, this qualification must be added: If the poles are applied on the moistened skin, as usual in testing or treating cases, no reaction occurs even with most intense currents; but if a needle be made one pole of the battery and inserted into the affected muscle, slight and limited contractions may be obtained with a moderate current for many months. Of this we have repeatedly satisfied ourselves in cases of poliomyelitis, lead paralysis, and traumatic peripheral paralysis. In the later stages of diffused paralytic atrophy, after an uncertain number of years, no reaction can be obtained with either electrical current. In fascicular non-paralytic muscular atrophy (as in progressive muscular atrophy) the loss of faradic contractility is only demonstrable in the affected fasciculi, good contractions being obtained in adjacent healthy fasciculi of the same muscle. The amount or extent of contraction varies pari passu with the progress of the atrophy. The galvanic reactions of this form of muscular atrophy are not yet well established. Muscles and muscular groups in a condition of impaired nutrition exhibit at an early period an interesting condition—viz. that they no longer contract by reflex excitation. Thus in a case of infantile poliomyelitis with paralysis of the muscles of the leg, these muscles no longer contract when the sole of the foot is tickled, and if the thigh-muscles are affected even so slightly as to appear of normal size and consistence, the patellar reflex is found wanting. In these and in traumatic cases the [p. 56] reflex act is prevented by lesion of the centrifugal motor nervous apparatus, and perhaps also by the associated muscular trophic alterations.
6 Conveniently expressed by the symbol De R.
Histological changes in atrophied muscles vary somewhat in character in different diseases, and vary much in degree at different periods of the atrophy. An early appearance is the presence of proteinaceous and of fatty granules or molecules in the sarcous substance. Later, the muscular fibres become reduced in size, lose their striation, and show inequalities; the interstitial connective tissue becomes active and increases in amount, at the same time that fat is deposited. The fatty change in some cases, in others the granular or proteinaceous transformation, ultimately completely destroys the muscular substance, so that in the place of a muscle we find abnormal connective and fatty tissues, blood-vessels, fatty and proteinaceous débris, the whole presenting a pale yellowish-white aspect. It is in this final stage of degenerative atrophy that all electrical reactions are lost. In the pseudo-hypertrophic state the interfibrillary and interfascicular connective-tissue growth is much more active, and the wasting muscular fibres are buried in masses of wavy and fatty connective tissue. In this condition also electrical reactions may be wholly absent.
(b) Atrophy due to defective innervation sometimes affects the skin and bones. In the former, after nerve-injuries more especially, we observe loss of thickness, glossiness, and perverted circulation and secretion; the hairs may fall out or grow abnormally; the nails are slow of growth, thick, rugose, incurvated, and brittle. In other cases, as in cerebral and spinal paralyses, the skin of the paralyzed part is abnormally dry, rough, and furfuraceous, and it loses its elasticity. In some varieties of so-called skin diseases the patches of altered nutrition (eczema, bullæ, herpes, psoriasis, leucoderma, scleroderma, etc.) are often, probably, dependent upon nervous lesions.
In the very rare disease known as progressive facial atrophy the skin, subcutaneous areolar tissue, and the bones undergo extreme atrophy. The initial lesion is usually a patch of scleroderma with or without neuralgic phenomena; the skin is thin, darker and smoother than normal; it soon adheres to the subjacent bone (maxilla or zygoma), which itself steadily diminishes in size. Almost the entire half of the face (including the palate and tongue) may ultimately show the atrophic changes. We are not yet prepared to state the causal nerve-lesion in this disease.
The bones are abnormally fragile (fragilitas ossium) in some nervous diseases, more especially in dementia paralytica and posterior spinal sclerosis; but whether this condition is due directly to the nervous disease or is the expression of more general malnutrition is now undecided.
The complex lesions of joints observed in the course of posterior spinal sclerosis, the spinal arthropathies of Charcot, probably belong to this category. The affected joint (knee, shoulder, or ankle) rather suddenly swells, and the swelling usually invades the rest of the member or extends to the next distal joint; it is a hard, semi-elastic swelling unlike common œdema. After its gradual subsidence it is found that changes have taken place in the articulation itself, and later distinct evidences of destructive disease, such as erosion of cartilages, relaxation of ligaments, swelling, are observed. In many cases extra-articular lesions appear in the shape of osteophitic formations from the adjacent bones. The hydrarthrosis may persist or disappear. So complete may be the destruction of [p. 57] the joint that—for example, in a case of arthropathy of the knee—the leg may be twisted about in all directions, and even over-extended so as to lie upon the anterior surface of the thigh. Examination of the joint post-mortem reveals non-suppurative destruction of all its component parts, cartilages, ligaments, and epiphyses; the eroded, deformed ends of the bones rub against one another in a false joint-cavity formed of the skin, connective tissue, tendons, and remains of ligaments. The absence of pain and tenderness in the course of arthropathies is a striking feature—so much so that when, in an adult patient, it is observed that manipulation or puncture of a diseased joint is painless, special inquiry should be made for symptoms of posterior spinal sclerosis.7
7 We have known one case in which the diagnosis of tabes dorsalis was made (and verified after death) in this way, after the surgeon in charge of the patient had mentioned the fact that puncturing a swollen diseased knee-joint was painless.
(c) Under the head of degenerative atrophies should be included the secondary changes which affect certain nerve-tracts within the nervous system itself. It is impossible in this introduction to treat fully of this interesting category of trophic changes; the following summary must suffice: (1) When the cerebral motor cortex or any part of the associated pyramidal (or motor) tract is destructively injured, there occurs, in from three to six weeks, a degeneration of the whole tract caudad of (below) the brain. The myeline becomes granular and disappears, the cylinder-axes are broken up and vanish, the connective tissue (neuroglia) increases in amount; the atrophied and degenerated area appears in a transection rather translucent in contrast to the pearly white of the normal medullary tissue, and when the preparation is stained with carmine the patch takes up an abnormal amount of pigment. This is the so-called descending degeneration, or centrifugal atrophy of the central nervous system. (2) After total transverse lesions of the spinal cord, besides the above-described centrifugal degeneration caudad of the lesion, we observe frontad of (above) it similar changes in the posterior median columns, and in the direct cerebellar tracts—centripetal degeneration. At present we have no knowledge of centripetal (ascending) degenerations in the cerebrum and in nerve-trunks; and if the results of von Gudden's experimental method be cited against this statement, it must be replied that its effects are best seen in newly-born animals, and that its pathology is yet unknown. (3) Lesions of the anterior gray matter (ventral cornua) of the spinal cord, and of mixed nerve-trunks produce only centrifugal or descending degeneration. All the nerve-fibres deriving their innervation from the injured area in the cord, or in case of nerves all fibres below the injury, perish—i.e. their myeline breaks up and undergoes granular and fatty degeneration, their cylinder-axes are segmented and disappear, while at the same time the connective tissue of the nerve becomes abnormally active and increases. Furthermore, in cases of this category there are, inevitably, degenerative and atrophic changes in the attached muscles, and peculiar electro-muscular reactions (vide supra). All these central and peripheral nervous degenerations, due to a local lesion, are conveniently grouped under the name of Wallerian degeneration.
2. ERUPTIONS AND ULCERATIONS.—(a) The cutaneous eruption about whose nervous origin there is the least doubt is that known as herpes or [p. 58] zona. This manifests itself, with or without paræsthesiæ (pain, itching, formication, etc.), as vesicles upon deeply-inflamed spots of skin distributed in the territory of one or more sensory nerves, and almost always unilaterally. The destructive process in the derma is so profound as to leave scars which are indelible as a rule. In general terms it might be stated that herpes may occur in the range of any sensory nerve distributed to the skin or mucous membranes. The neuralgia attending its development may be severe, and in some cases lasts for years after the healing of the eruption. The pathology of this affection appears to be inflammation of the ganglion of the posterior root of one or more spinal nerves (including the trigeminus and glosso-pharyngeal) or of their trunks. Herpes may appear in the course of spontaneous and traumatic neuritis; and in the last-named conditions a variety of eruptions have been observed in the area supplied by affected nerves, such as eczema, bullæ, etc.
(b) That ulceration may result directly from a nervous lesion is shown by the history of herpes, where a destructive process takes place in the derma under such conditions as to exclude the action of external agencies. But the same cannot be said of the ordinary ulcerations and gangrenous lesions observed in a number of nervous diseases, as the bed-sores of myelitis or of spinal injuries, the ulceration of the cornea in trigeminal anæsthesia, the digital ulcers and gangrene of lepra, asphyxia of the extremities, and nerve-injuries. As regards all these, the proper explanation is, it seems to us, that the anæsthesia existing as a predisposing cause (leading to imperfect protection of the part), the ulceration itself, is directly, actively caused by external agencies. Let me briefly cite a few instructive experimental and pathological facts bearing on this question.
It is well known that in animals and man lesions of the trigeminus nerve sufficient to produce anæsthesia (of its first branch more especially) are frequently, if not invariably, followed by ulceration and perforation of the cornea and phthisis bulbi. These were long held to be true dystropic changes, but about thirty and twenty years ago Snellen and von Gudden demonstrated independently and by different methods that these ocular lesions could be entirely prevented by absolute closure (perfect protection) of the eyelids prior to the experiment on the trigeminus. Not long afterward Brown-Séquard showed that the sloughing ulcers which occur about the foot of an animal whose sciatic nerve has been cut may be entirely prevented by care, cleanliness, and soft bedding. The conclusion to be drawn from these observations is that in almost all cases the ulcerations and sloughing observed in man during the course of a nervous disease sufficient to produce anæsthesia, such as traumatic neuritis, lepra anæsthetica, traumatic or simple myelitis transversa, disease of the trigeminal nerve, etc., are in reality produced by external agencies, injuries to the cuticle, action of filth, and, we think, the entrance of bacteria, which are well known to possess extraordinary powers of penetration into tissues whose protecting epithelial layer is removed. Clinical observation corroborates this view, for, with strict antiseptic treatment and under sealed dressings (collodion to ulcerated finger-tips), these ulcerations heal rapidly and completely, while the anæsthesia remains unchanged and the nervous lesions may even progress. At the same [p. 59] time, while we believe the above to be the pathology of so-called trophic ulcers, we would admit the possibility of spontaneous neuritic ulceration and gangrene, as shown more especially in herpes.
3. ALTERED SECRETIONS.—Under the influence of disordered innervation secretions may be altered in quantity and in quality. Symptoms of this class may be caused by neural or by central lesions, and the mechanism of their action may be direct or reflex.
(a) After section or lesion by disease of the cervical sympathetic nerve we observe increased activity of the entire skin in the affected area of the head and face: there is more perspiration, lachrymation, and more cerumen is found in the ear. In cases of lesions of a certain part of the oblongata we find one result to be polyuria. In many cases of nerve-injuries the sweat-glands and hair-follicles of the parts supplied by the affected nerve appear to be sometimes abnormally active, or in other cases inactive. In some rare cases of insanity profuse salivation and extraordinary growth of hair are striking symptoms. Lastly, in some functional nervous affections the various secretions and excretions may be altered to extraordinary extremes (e.g. the polyuria and anuria of hysteria).
(b) Qualitative modifications of secretions also occur, as exhibited in the many variations in the composition of the urine in various neuritic conditions, the watery urine of hysteria, the phosphatic urine of neurasthenia. Injuries of a part of the floor of the oblongata (and very probably other lesions of the nervous system) give rise to the appearance of sugar, and sometimes of albumen, in the urine. Under the influence of disease or of an emotion the breast-milk may become toxic to the nursing child, causing diarrhœa, convulsions, etc. In some forms of nervous dyspepsia large quantities of acid or of alkaline fluid may be rapidly poured out into the stomach as a result of disturbed glandular and vaso-motor action. In a few cases of neurosis malodorous or perfumed perspiration has been observed.
In a general way it may be stated that, inasmuch as the normal function of glands is largely, if not exclusively, under direct and reflex nervous control, their secretions may be quickly altered in quantity or quality by rapid nervous disease or by functional disorders. It is probable that much of our future progress in the semeiology of nervous diseases will be in this direction by the aid of improved medical chemistry.
4. ASSIMILATION, METAMORPHOSIS OF FOOD, TISSUE-LIFE, and BLOOD-MAKING are probably under nervous control to a certain extent, but our knowledge is not now in a state to speak positively and definitely of alterations in these processes as symptoms of nervous disease.
Having in the preceding pages surveyed the field of neurological semeiology in an analytical way, it remains to briefly indicate how far and in what manner these data can be best utilized for logical diagnosis in the present state of science. If we may be allowed an illustration, we [p. 60] would say that the foregoing sections contain a nearly complete vocabulary of the language of nervous diseases, and that the following pages express an attempt at formulating its grammar.
In the first place, it is important to classify the symptoms observed according to their probable immediate cause in the nervous organs, whether they are due to irritation or to the destruction of parts. The extreme value of such a distinction in practice was first emphatically brought forward by Brown-Séquard in his famous Lectures on the Physiology and Pathology of the Central Nervous System (Philada., 1860); and to the observance of this law of genesis of symptoms we believe that a large part of the subsequent extraordinary progress of neurological science is due.
The symptoms produced by irritation of nervous organs are usually hyperkineses or paræsthesiæ in their various forms. The symptoms, spasm, pain, or numbness, are usually, though by no means always, intermittent. That paralysis and anæsthesia may occur from irritation, by an inhibitory process, is not to be denied, yet we must maintain the extreme rarity of such a mechanism. The phenomena of inhibition are so prominent in the normal nervous system that a physician who looks at nervous diseases from the standpoint of the physiologist may well be excused for seeing morbid inhibitory processes where others do not.
The symptoms due to destructive lesions—i.e. those indicating destruction of parts of the nervous system—are paralysis, hyperkinesis, and anæsthesia, of absolutely or relatively constant presence. Thus, for example, the paralysis of common hemiplegia due to destruction of the motor part of the internal capsule is constant and permanent, while the accompanying tonic spasm (late contracture), which is considered an even more positive sign of serious destructive injury to the cerebral motor tract, is permanent, but intermittent—i.e. it is absent in profound sleep, and reappears as soon as the patient awakes.
The association of symptoms of irritation and those of destruction is frequent but variable. In many cases, as in cerebral tremor and posterior spinal sclerosis, spasm and paræsthesiæ precede paralysis, anæsthesia, and ataxia. In other cases (in many at a certain period) they coexist. In a small group of cases the irritative symptoms follow those indicating destruction, sometimes occurring years afterward, as in post-hemiplegic epilepsy and neuralgia due to cicatrices. We would repeat that very often, more especially in organic nervous affections, much light is thrown on the diagnosis by careful noting of the topographic distribution and chronological order of appearance of the symptoms.
In the second place, it is necessary to group the symptoms of disease of the nervous system in two great classes—viz. those representing demonstrable lesions, macro- or microscopic, and those dependent upon perverted functions or molecular malnutrition of the nervous organs or elements. The first group is designated as organic diseases; the second as functional affections. Mental diseases, so called, can also be classified, according to their symptoms, in either of these groups.
The symptoms of the first group, that of organic nervous diseases, are characterized by definiteness of distribution, by permanency, by relative invariability, and by the predominance of objective signs. Another important characteristic of organic diseases is their progressive or fatal [p. 61] tendency, either with reference to life in general or to that of parts or organs. A third peculiarity of these diseases is that they do not occupy the patient's attention as strongly or as constantly as neuroses: in other words, the Ego is less involved.
The symptoms of the second group, that of functional nervous affections (neuroses and psychoses), are characterized by generality and indefiniteness of distribution, by relative variability, by easy removal or spontaneous disappearance, and by the preponderance of subjective symptoms. The affection may endure for many years or for a lifetime without fatal result and without special aggravation. The Ego is very strongly and deeply affected, fear, depression, and constant dwelling upon the symptoms being prominent features.
These are general statements intended to serve as guides for the preliminary study of a case. It must be remembered that they are all liable to exceptions, and that each patient must be separately considered. It should be borne in mind that what to-day appears as a functional affection, chiefly indicated by subjective symptoms, may in a few months present distinct signs of organic changes in the nervous system. Also, it must be added that in the present state of knowledge we sometimes are not sure as to the presence or absence of organic changes even after careful study of a case; as, for example, in some epilepsies and neuralgias.
Furthermore, allowance must be made for the following sources of error:
Anatomical variability; as, for example, in the distribution of peripheral nerves and in the amount of decussation of fibres of the pyramids;
The coincidence of diseases and multiplicity of lesions;
The toxic effects of drugs taken by the patient previous to our examination; as, for example, bromism.
This should invariably consist, in the observer's mind at least, of three separate diagnoses, each formed by the application of widely different sources of knowledge, and each requiring a different logical process. One diagnosis forms the indispensable preliminary to the others, and the last one, when correct, demonstrates that the neurologist is a physician as well as a specialist. A further utility of this procedure by the method of the threefold diagnosis is, in our opinion, that it constitutes the sure inductive reasoning to be employed in the search after the pathology of new diseases, and must prove of help in the future growth of neurological medicine.
These diagnoses are—
The diagnosis of the symptoms or symptom-group;
The diagnosis of the location of the lesion;
The diagnosis of the nature of the lesion or of the functional disorder.
1. The diagnosis of the symptom or symptom-group is to be made by—(a) careful inquiry into the manner of appearance, development, and chronological order of the symptoms as related by the patient or by his friends, and more especially by (b) an exact, and in some directions [p. 62] minute, determination of the symptoms, obvious or latent, present in the patient. This valuable method of exact observation is sometimes, no doubt, carried to a ridiculous extreme, entailing much loss of time without corresponding results; but in medical practice, as in all forms of professional work, there enters a sort of genius, partly innate, but largely developed by cultivation, which enables the observer to seize at once, apparently by intuition or in the course of a few minutes of study, the really valuable and suggestive phenomena; and it is in this line, the line of important and correlated facts, that observation cannot be too minute and exact. In following this method technical terms must be correctly used and definitions rigidly adhered to, as superficial and loose records nearly always mislead. Sometimes in the course of the examination a symptom is discovered or a hint is thrown out by the patient which suggests new lines of inquiry, and occasionally necessitates an entire rearrangement of the data obtained. Consequently, it is important that the observer should approach a case tabula rasa, and should, as far as possible, prevent his being biassed by anticipations of, and immature guesses at, the third or final diagnosis.
Besides exactness of observation, it is necessary that the physician should have a thorough knowledge of nervous nosology in order to complete the first diagnosis: he must be acquainted by book-study and by personal observation with the numerous types of symptom-groups which fill up our present classification of diseases, so that he can at once say, approximately at least, in what category the case before him belongs.
2. The second diagnosis, that of the location of the lesions, is to be arrived at by the application of the observer's knowledge of the anatomy and physiology of the nervous system; and therefore it is here that special training is of the greatest advantage. The anatomy and physiology of use in this connection are not the bare sciences as taught in ordinary text-books, but a higher sort of knowledge, corrected and extended by the teachings of pathology and pathological anatomy. The physician must be well versed in the recent revelations of experimentation and of autopsies bearing upon the architecture and functions of the central nervous system, and should be able to apply this knowledge deductively to the case in hand. In this manner the now abundant material grouped under the term Localization of Cerebral and Spinal Diseases (vide the next article) can be made of the greatest utility in every-day practice. The solution of the problem of localization of the lesion is much simplified if it be first accurately determined whether the lesion is peripheral, spinal, or cerebral.
3. The final diagnosis is with respect to the nature of the lesion. While the second diagnosis may be said to possess the greater scientific interest, this one must be admitted to possess paramount practical importance, as from it we derive the indications for rational treatment and the data of prognosis. The third diagnosis is to be made by the application of the observer's knowledge of general pathology and etiology; hence it is in this field that the best-trained physician succeeds—where the experienced practitioner may sometimes eclipse the brilliant specialist. The truth of this is maintained by those who hold, as we do, that it is unwise to embark in specialism without having had good hospital advantages and extensive general practice.
[p. 63]In order to arrive at the diagnosis of the nature of the lesion we must consider the family history, trace out predispositions, study the various causes of disease to which the patient has been exposed, and by a thorough examination of the various functions and the objective condition of the patient ascertain what pathological processes are active in him. Often the clue to the diagnosis is found in signs afforded by non-nervous organs, as nervous syphilis by nodes and cutaneous cicatrices, cerebral hemorrhage by renal disease and increased arterial tension, cerebral tuberculosis by pulmonary lesions, etc.
A purely empirical form of knowledge of some utility in proving the pathological diagnosis is that of the relative frequency of certain lesions in the two sexes, at different ages, in various professions, etc.—a statistical knowledge which is to be applied deductively to the case under study.
Considerable uncertainty sometimes remains even after the most careful analysis of a case, and often, after stating the first and second diagnoses quite positively, scientific caution and due regard for truth compel us to state the third diagnosis in alternative propositions or as a diagnosis of probability, to be finally settled by the appearance of new symptoms, or in some rare cases only by a post-mortem examination.
In some diseases of this class—as, for example, epilepsy—it is desirable to make the triple diagnosis as stated supra, but usually the two problems to be solved are—What is the symptom-group? and what is the pathology of the affection? The question of localization is less important and less easy of solution, as the symptoms are more usually generalized, often vague, and sometimes purely subjective.
1. The first diagnosis is to be made in the same manner as already stated, but besides, in many cases, a close psychological analysis is required to ascertain the emotional and mental state of the patient. Not only is this indispensable in cases of insanity, but it is often of great utility in other conditions, as hysteria, hypochondriasis, and simulation. In the course of this study we are frequently brought face to face with a most difficult problem—viz. the correct estimation of the degree of pain experienced by a patient. Is it a quasi-objective, correctly-portrayed sensation? is it magnified by abnormal sensitiveness or by true exaggeration? or is it simulated for a purpose? These questions demand the greatest freedom from prejudice and most delicate tact for their solution, and occasionally the most experienced physician is deceived. More especially are caution and scientific doubt to be exercised when this symptom (pain) stands alone or nearly so, as in some medico-legal cases and in certain hypochondriacal states where self-delusion seems to constitute the only real disease.
2. The diagnosis of the pathological nature of the functional disturbance (functional lesion) is to be made only by an exhaustive study of the patient's personal and family history and of his general condition. The following are the principal lines of inquiry to be followed:
[p. 64](a) As to hereditary predisposition: direct or indirect inheritance of neurotic tendencies, of psychic peculiarities, and as to the presence of the various psychic and physical signs grouped under the term psychic degeneration.
(b) As to personal habits: overwork, masturbation, the abuse of tobacco, alcohol, or coitus, injudicious diet, abnormal postures, injurious avocations, etc.
(c) As to dyscrasic and hæmic conditions: uræmia, lithæmia, anæmia, malarial and syphilitic infection, etc.
(d) As to the condition of important organs: of the eye in connection with headaches and vertigo; of the ear in relation to vertigo and epileptiform attacks; of the heart (and arterial tension) in various head-symptoms; of the sexual organs in hysteria, hypochondriasis, epilepsy, etc.
A serious stumbling-block in this last line of inquiry is the ever-recurring question as to the causal relation between the symptoms observed. Is the asthenopia the cause of the headache, or does the neurasthenia, giving rise to the headache, cause the asthenopia? Does the extremely slow action of the heart in a given case produce the epileptoid attacks, or are both due to a lesion of the medulla? Does ovarian hyperæsthesia and neuralgia (with or without organic changes) cause the hystero-epilepsy, or is the ovaria one of the numerous peripherally projected sensory symptoms of the hysteric state? Does the lithæmia, oxaluria, azoturia, or phosphaturia found in a patient give rise to the nervous symptoms complained of, or are they (the morbid excretions) the result of defective innervation? The candid neurologist, looking at his cases from the standpoint of the general physician rather than from the loophole of narrow specialism, must admit that these questions vex him daily, and that they are often not to be resolved in the present state of knowledge except by a recurrence to the therapeutic test.
For this extremely difficult diagnosis of the pathology of functional nervous affections we would obtain much immediate assistance if observers had the courage to publish their cases in continuous series, instead of giving us successful cases, which often only serve to mislead. For example, how greatly would the question of the relation between ovarian symptoms and epilepsy (also hystero-epilepsy) be advanced if we had the final results of all cases of removal of the ovaries for these diseases at a period not less than one year after the operation! And so with the attempts made to cure headaches by the correction of errors of refraction and weakness of the interni. The profession has a right to demand a frank and full report of the experience of those who practice and teach in these directions.
There are two ways in which this important subject may be treated. Of these, the more interesting and logical would be to systematically expose the results of anatomical researches and of physiological experiments which tend to demonstrate the organic independence and the functions of various parts of the nervous system, and to give a classified series of results of autopsies bearing on localization. This would be all the more satisfactory because the questions involved, although of much importance in practice, are in reality physiological. The localization of functions being known, the physician could from the symptoms (i.e. perverted or abolished functions) present make a deductive diagnosis of great exactness. A treatise on medicine, however, cannot allow the space necessary for such a treatment of the topic which is best suited for monographic writing. The other method of exposition, the one we will follow, is that of summary statement of the association of the symptoms with definite lesions, with occasional anatomical and physiological explanations. This will, after all, be a series of diagnostic propositions stated as concisely and classified as practically as possible. With this end in view we divide the subject into five parts:
The localization of lesions in the peripheral nervous system (including the cauda equina);
The localization of lesions in the spinal cord;
The localization of lesions in the medulla oblongata;
The localization of lesions in the encephalon.
Cranio-cerebral topography.
In general terms, it may be said that lesions of peripheral (cerebro-spinal) nerves give rise to various sensory symptoms in the area of cutaneous distribution of the affected nerves, and to a flaccid atrophic paralysis in muscles supplied by the same nerves. These muscles almost always exhibit the De R. in varying degrees, and other trophic and vaso-motor symptoms are common. Many of these symptoms also occur in cerebral and spinal diseases, so that, after all, the diagnosis of peripheral localization depends largely on a correct knowledge of the course and [p. 66] distribution of nerves; of the relative distribution of the sensory and motor filaments of nerve-trunks; and of the frequent anomalies which occur. The subject of collateral innervation at the periphery must also receive attention, as involving a source of error.
Of extreme importance is the law of the relative distribution of motor and sensory filaments derived from one nerve-trunk. This, Van der Kolk's law,1 has hardly received the attention it deserves from practical neurologists. Briefly stated, it is that of the two sorts of fibres in a mixed nerve the sensory filaments go to those parts which are moved by muscles innervated by the motor filaments of the same nerve. The reader can verify for himself the exactness of this law by making sketches of an extremity and tracing the motor and sensory distribution of its various nerves. There are partial and apparent exceptions to the formula, but this objection applies to almost all our medical laws. In the cranial system of nerves it is necessary to consider the trigeminus as the sensory companion of the six anterior motor nerves; the pneumogastric as the associate of the spinal accessory (in part).
1 Van der Kolk, On the Minute Structure and Functions of the Spinal Cord, etc., p. 7, New Sydenham Soc. transl., London, 1859; Hilton, On Rest and Pain, p. 101, Am. ed., N. Y., 1879.
(a) Irritative lesions of nerves, as tumors, punctured wounds, perineuritis, moderate pressure, etc., are indicated by pain, numbness, and other paræsthesiæ in their cutaneous distribution, and of spasm or cramp with paresis only, in the associated muscles. Pain is the most prominent symptom by far, and many cases of so-called neuralgia belong to this category. As a rule, there is no anæsthesia, and the electrical reactions of nerves and muscles remain normal, or at least they do not present De R. In some cases vaso-motor spasm (coldness, white or bluish appearance of parts) shows itself in the most peripheral distribution of the nerve. The cutaneous and tendinous reflexes are variable, but usually preserved.
(b) Destructive lesions of nerves, by section, severe pressure, true neuritis, etc., are characterized by anæsthesia with or without paræsthesiæ, by motor and vaso-motor paralysis, and by loss of superficial and deep reflexes. Later, there occurs degenerative atrophy of the paralyzed muscles with fully-developed De R., and dystrophic changes in the skin, etc. supplied by the sensory filaments of the injured nerve. In these anæsthetic parts ulceration is easily caused by traumatism and want of cleanliness.
The abnormal electrical reactions of the paralyzed muscles are of much importance for the diagnosis of the amount of injury done to the nerve and for the purpose of prognosis. They may be summarized as follows, assuming a case of complete section of a nerve-trunk:
α. The Faradic Reactions diminish rapidly in degree in both nerve and muscles from the third or fourth day, and in the nerve they are, as a rule, completely lost at the end of from ten to fifteen days. In the muscles complete loss of faradic reaction is noted only somewhat later, and is absolute. A return of musculo-faradic contractility is a most positive sign of recovery of the nerve.
β. The Galvanic Reactions.—In the nerve, distal of the lesion, the result is similar to that stated above—viz. after a few days (from five to fifteen) all reaction disappears. The anatomical cause of the complete [p. 67] loss of the faradic and galvanic reactions in the nerve is its disintegration by the Wallerian degeneration. In the attached muscles the phenomena are widely different, and present interesting and complicated variations. In the first place, during a variable number of days there is increased excitability—i.e. the paralyzed muscles, deprived of innervation, contract to a much weaker current then do the homologous normal muscles. This is best shown in cases of peripheral facial paralysis (Bell's palsy) in the second and third weeks, by placing the electrodes in the median line, one upon the cervical vertebræ, the other (a small testing interrupting electrode) on the chin; on closing a very weak current of from four to eight elements it will be seen that the muscles on the paralyzed side of the face (the lower muscles) contract distinctly, while those on the normal side remain quiet. In the course of time, many weeks usually, the excitability diminishes, and falls below the normal, and in some cases ultimately disappears. These are known as the quantitative changes in musculo-galvanic reactions. During the long period preceding recovery, or without it, various qualitative changes are also observed in the reaction. The normal general formula of CaCC > AnCC (with rapid, jerking and full contractions of the muscle) becomes CaCC = AnCC or CaCC < AnCC. Often, too, distinct opening contractions occur, usually AnOC. The muscular contractions also tend to the tonic type or tetanus, expressed as CaDT or AnDT, etc.
The form of the contractions obtained is much altered. Throughout a practically endless period in some cases, or until regeneration of the nerve takes place in others, it is observed that musculo-galvanic contractions are delayed, are slower, less jerking, or assume an undulating wave-like character, easily passing into tetanus. This change from the rapid, jerky, and full normal muscular contraction to one which is slow and wave-like we consider to be the most positive and reliable evidence of neuro-muscular degeneration and of the cutting off of the spinal-cord influence. Fig. 4 shows the characters of a human degenerative myogram contrasted with a normal one, Fig. 3.

2 “The Myography of Nerve-degeneration in Animals and Man,” Archives of Medicine, viii., No. 1, 1882.
In the period of recovery or regeneration of the nerve the musculo-galvanic reactions slowly reacquire their normal characters; the normal suddenness and completeness of the contractions gradually appear, and faradic excitation causes slight responses. Lastly, the nerve also begins to exhibit excitability under galvanism and faradism. These various abnormal electrical reactions, also frequently observed in diseases of the spinal cord, constitute the so-called reaction of degeneration, or De R. The subject is one of much practical importance, and for details the reader is referred to the treatises on electro-therapeutics of Erb and De Watteville.
Just as we depend upon the De R. to prove interruption of motor nerve-fibres (or, in other cases, destruction of ganglion cells in the anterior horns of the cord), so do we rely upon the demonstration of complete anæsthesia to prove interruption of sensory fibres. In seeking for the area of anæsthesia several points must be borne in mind: (1) The normal [p. 68] distribution of the principal nerve-trunks as taught by ordinary anatomical works; (2) the remarkable anomalies of distribution which sometimes occur; (3) that many nerves near their endings exchange filaments in very variable numbers; loops for collateral innervation, which will supply some sensibility to parts which, judging by ordinary anatomical rules, should be made anæsthetic by section of a given nerve-trunk; (4) another consideration is the degree of anæsthesia. Before pronouncing upon the complete and fatal division of a nerve-trunk (by injury or by disease), absolute anæsthesia should be demonstrated in its area of principal and isolated distribution. Ordinary tests are not, as a rule, sufficient for this purpose. The best means in our experience consists in the use of a very strong induction (faradic) current, as follows: The skin of the suspected region to be thoroughly dried and rubbed with chalk or powdered starch; one pole, consisting of an ordinary wet electrode, to be applied just above the part to be tested, and the other pole, consisting of a single wire, with which different parts of the anæsthetic area are to be touched. By this means partially insensible regions, not responding to pricking and burning, may be made to yield reaction, and the area of absolute anæsthesia be thereby much reduced. Malingering may also be readily exposed by this test, which presents another advantage—viz. of not causing local injury or scars as burning will.
It follows from the preceding statements that in cases of limited atrophic paralysis with De R. the diagnosis between a central lesion (destruction of ganglion cells of the anterior horns of the cord) and a strictly peripheral (or neural) lesion is to be chiefly based upon two considerations: (1) The distribution of the paralysis, which in the first case affects muscles which are physiologically grouped or associated, while in the second case the simple law of anatomical associations or grouping is observed; (2) by the state of sensibility, which is normal in disease of the anterior horns of the cord, and is frequently impaired or abolished in nerve lesions.
Lesions affecting the cauda equina cause all the above-mentioned symptoms of peripheral lesions in a limited (partial) paraplegic distribution. If the lesion or injury be in the sacro-coccygeal region, the symptoms will, as a rule, be found confined to parts below the knee, occasionally also involving the muscles on the posterior aspect of the thigh (flexors of the leg). Below the knees we find an atrophic paralysis with De R., anæsthesia of the foot and part of the leg, loss of plantar and achillis reflexes, and the sphincter ani will be paralyzed. The patellar reflex is [p. 69] preserved or exaggerated. In case the lesion be in the lumbar region, below the first lumbar vertebræ, the symptoms will be found to extend as high as the groin, involving also the buttocks and sphincter ani; state of the bladder variable. All reflexes will be lost in the paralyzed extremities, except in some cases the cremasteric reflex.
Strange as it may appear, physicians do not always remember that there is practically no lumbar spinal cord (vide Fig. 2.), and that injuries, etc. of the lumbar vertebræ and dura tend to affect nerves, and not a nervous centre.
Diseases of the spinal cord are distinguished by the following general characters, positive and negative:
Positive Characters.—Tendency to primary bilateral or paraplegic distribution of all the symptoms. In the majority of cases preservation of electro-muscular excitability, and in one well-defined group of cases De R. more or less typically developed in the paralyzed parts. Frequent vesical and rectal paralysis, either of the retaining or of the ejecting apparatus. Pains and other paræsthesiæ in the extremities, the pains often possessing the electric or fulgurating character. Anæsthesia of paraplegic distribution. Sensations of constriction or cincture about a limb or about the body at various levels. Occurrence of ataxia without paralysis. Progressive muscular atrophy without actual paralysis. Easy production of eschars (bed-sores).
Negative Characters.—Absence of typical hemiplegic or monoplegic distribution of symptoms. Rarity of head symptoms, as headache, vertigo, mental disturbance; of lesions of the optic nerve. Absence of epileptiform convulsions. Absence of such grouping of motor and sensory symptoms as would exactly correspond to the area of distribution of one or more large nerve-trunks.
The above symptomatic indications are, of course, of the most general meaning only, and are liable to exceptions and subject to varying conditions.
The DIAGNOSIS of the exact localization of lesions in the spinal cord, considered from the clinical standpoint, is perhaps best arrived at by following an anatomical and physiological order of subdivision of the problem into three questions, as follows:
FIRST QUESTION.—BEING GIVEN SYMPTOMS INDICATING DISEASE LIMITED TO ONE OR MORE SYSTEMS OF THE SPINAL CORD, TO DECIDE WHICH ARE AFFECTED.
Physiology and the results of embryological and pathological researches justify us in making a general division of the spinal cord, for purposes of diagnosis, into two great systems, whose limits are fairly well known—viz. the æsthesodic or sensory system, and the kinesodic or motor system. The following outline diagram (Fig. 5) of section through the spinal cord exhibits the ascertained limits of the two systems.
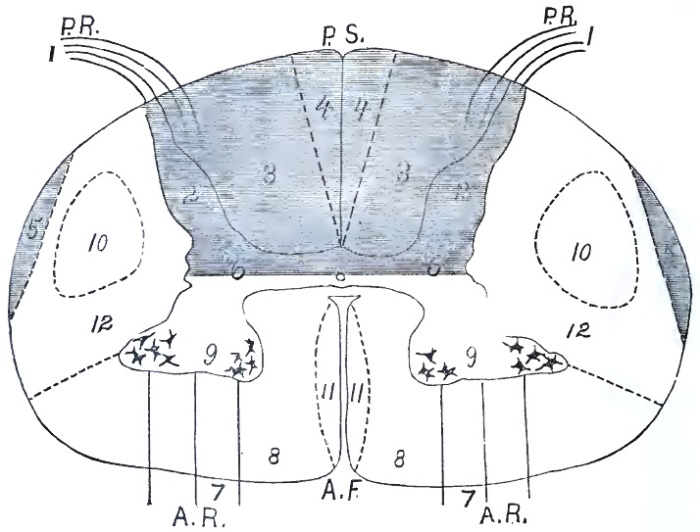
A. Lesions of the Æsthesodic System.—Limits of the Æsthesodic System.—By this term we mean that combinations of ganglion-cells and nerve-fibres whose functions are locally sensory, and of those fibres which transmit impressions centripetally (frontad) to the encephalon. The [p. 70] following are the recognized parts of this system, as outlined on the diagram: (1) the posterior (dorsal) nerve-roots and attached ganglia; (2) the posterior gray horn and central gray substance to an unknown distance ventrad; (3) the fasciculi cuneati (columns of Burdach), whose lateral parts are more particularly designated as posterior root-zones; (4) the fasciculi graciles (columns of Goll) or posterior median columns; (5) the fasciculi ad cerebellum; (6) the vesicular columns of Clarke (most developed in the dorsal part of the cord). All of these parts have sensory functions, or at least transmit impressions centripetally, and they undergo secondary (Wallerian) degeneration toward the encephalon—i.e. frontad of a transverse lesion of the cord.3
3 There are some results of physiological experiments and a few isolated pathological facts which would seem to point to the existence of other sensory (centripetal) fasciculi in the lateral columns, but it would be wholly premature to make use of these facts in a practical consideration of the subject.
At the present time there is only one lesion of the æsthesodic system which can be diagnosticated during the patient's life from positive symptoms.
(a) Lesions of the fasciculi cuneati (posterior root-zones, 3). The symptoms of lesion (usually sclerosis) in this region are wholly sensory [p. 71] and ataxic. At an early stage acute pains, fulgurating pains, occur in the extremities; later paræsthesiæ, anæsthesia, and ataxia. The fulgurating pains caused by the slowly-progressive lesion of the posterior root-zones are very peculiar, and almost pathognomonic (vide preceding article for their description). In some cases paræsthesiæ precede the pains, which inversion of the usual order must be due to a difference in the starting-point of the sclerosis within the large fasciculi cuneati. Tendinous reflexes (especially the patellar) are lost at an early period in the disease, and by noting the disappearances of the different reflexes we can trace with some accuracy the longitudinal extension of the sclerosis (vide Fig. 2). In many cases the pupillary reflex is also abolished, constituting the Argyll-Robertson pupil.
As negative characters of lesions of the posterior root-zones (and of the rest of the æsthesodic system) we note absence of paralysis, contracture, atrophy, and De R.
In the present state of our knowledge of spinal physiology and pathology we think that a lesion in this location should be recognized by the physician early and positively—in some cases years before ataxia and other grosser symptoms make the diagnosis of locomotor ataxia obvious even to a layman's eye.
(b) Lesions of the fasciculi graciles (column of Goll, 4) cannot, we believe, be recognized directly by positive symptoms. There are a few cases on record of primary (?) sclerosis of these columns, in which during life vague sensory symptoms had been noted, but we cannot build upon such data. Indirectly, however, we can in many cases diagnosticate degeneration of these fasciculi, reasoning from the data of pathological anatomy. Thus, for example, in advanced cases of sclerosis of the fasciculi cuneati (posterior spinal sclerosis) we know that in the dorsal and cervical regions of the cord the columns of Goll are in a state of secondary degeneration. After complete transverse division of the cord by injury, extreme pressure, or focus of myelitis, etc. the same (centripetal) degeneration exists above the lesion.
The same remarks apply fairly to our clinical knowledge of the remaining parts of the æsthesodic system, columns of Clarke (6), and fasciculi ad cerebellum (5). We know absolutely nothing of lesions of the posterior horns (2) in their clinical and diagnostic relations.
B. Lesions of the Kinesodic System.—Limits of the Kinesodic System.—In general this includes the antero-lateral parts of the cord. In a trans-section of the cord (vide Figs. 5 and 6) the following columns and fasciculi are recognized, their location and limits being made known to us by embryology, descriptive and pathological anatomy: (7) The anterior (ventral) nerve-roots emerging from (8) the true anterior columns or anterior root-zones; (9) the ventral (anterior) gray horns with their groups of ganglion cells; (10) the crossed pyramidal fasciculus, which is the caudal continuation of the cerebral motor tract of the opposite hemisphere; (11) the direct pyramidal column (column of Türck), which is the caudal continuation of the cerebral motor part of the hemisphere on the same side; (12) the antero-lateral column. Fasciculi 10 and 11 bear an inverse relation to each other—i.e. 11 is larger in proportion as 10 is smaller.
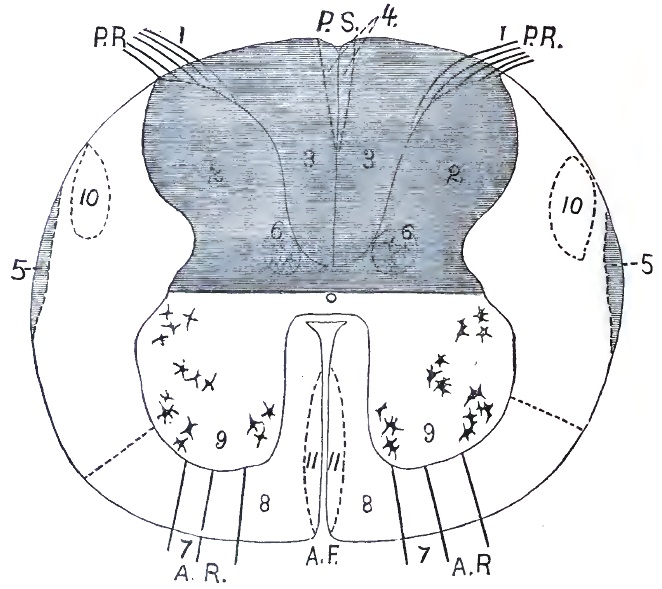
In a general way it may be stated that lesions of the kinesodic system are characterized positively by the isolated existence or predominance of [p. 72] motor symptoms, by impairment of muscular nutrition, and by De R.; also by contractures. The reflexes are almost never normal, being either exaggerated or lost. Negative symptoms are—absence of sensory symptoms, of ataxia, and of vesical or rectal symptoms.
(a) Lesions of the anterior gray horns (9) are revealed by most definite and characteristic symptoms. There occurs a flaccid paralysis involving more or less extensive groups of muscles in the extremities, rarely truncal muscles, and never those of organic life. In a few weeks the paralyzed muscles undergo atrophy, sometimes to an extreme degree, and various degrees of De R. are present. Cutaneous and tendinous reflexes are abolished. The bladder and rectum are normal. Sensory symptoms absent, and if present consist only of mild paræsthesiæ, which are probably due to postural pressure upon nerve-trunks or to disturbance of the peripheral circulation. There is no tendency to the formation of bed-sores, but circulation and calorification are reduced in the paralyzed members. It should be remembered that paralysis due to systematic lesion of the anterior gray horns is never typically paraplegic, with horizontal limit-line of sensory symptoms, a cincture feeling, and vesical paralysis.
[p. 73]The above symptom-grouping is characteristic of lesion of the anterior horns en masse; in other words, of poliomyelitis. In that form of systematic disease of the anterior horns which consists primarily and chiefly of a degeneration or molecular death of the ganglion cells there is no true paralysis; the atrophy of muscles is infinitely slower, and it proceeds in various muscles fasciculus by fasciculus, the wasting being usually preceded by fibrillary contractions, and being almost always symmetrically located on the two sides of the body (affecting analogous or homologous parts). The electrical reactions are abnormal, in that musculo-faradic reaction is lost in exact proportion to the wasting; so that in a large muscle one part may contract normally, while the adjacent fasciculi do not. It is as yet uncertain whether De R. occur in this disease (progressive muscular atrophy). Calorification and circulation are much less impaired than in poliomyelitis; the negative symptoms are much the same.
It is sometimes difficult to distinguish poliomyelitis from generalized neuritis. The diagnosis is to be made by the presence in the latter disease of marked sensory symptoms—neuro-muscular pains, numbness, slight anæsthesia—and by a grouping of symptoms coinciding with the distribution of nerve-trunks and branches. No assistance can be derived from electrical tests, as both diseases yield more or less typical De R.
(b) Lesions of the spinal pyramidal tract (of fasciculi 10 and 11) are followed by motor symptoms only—viz. paralysis and contracture—or, in other words, by a spastic paralysis. Sensibility is unaffected; the bladder, rectum, and truncal muscles are not distinctly paralyzed; the reflexes are much increased, and ankle-clonus is often present. The electrical reactions of the paralyzed muscles are normal, qualitatively at least. The diagnosis of localization may be pushed still farther by the following considerations:
(1) When the condition of spastic paralysis is unilateral, of hemiplegic distribution, and follows an attack of cerebral disease of some sort, we may feel sure that both the crossed and the direct fasciculi of the pyramidal (10 and 11) belonging to one cerebral motor tract are degenerated throughout the length of the spinal cord, the crossed fasciculus on the paralyzed side and the direct on the healthy side (same side as injured hemisphere). It would thus appear that lesion of the direct pyramidal fasciculus (11) produces no symptoms,4 except, of course, in those rare cases in which it is larger than its associated crossed fasciculus.
4 Unless it be the increase of reflexes which is so often observed on the non-paralyzed side in hemiplegics.
(2) The above symptoms may be bilateral, as observed in children as a congenital or early-acquired condition. In such cases the four fasciculi of the motor tract are degenerated or undeveloped, in correspondence with a symmetrical bilateral lesion of the motor area of the cerebrum—imperfect development or early destruction.
(3) When the legs alone are the seat of spastic paralysis, with increased reflexes, spastic or tetanoid gait, without sensory symptoms, the diagnosis of a primary sclerosis of both lateral columns (inclusive of 10) of the spinal cord is justified.
(c) Lesions of antero-lateral columns of the cord (8 and 12), primary and independent of lesions of the anterior horns or of the crossed [p. 74] pyramidal fasciculus, cannot now be diagnosticated during life. These large masses of fibres include fasciculi whose functions are probably motor; others (especially in 12) whose functions, according to recent experiments, may be sensory; and still others which are associating or commissural.
(d) Various combinations of the above lesions occur, and may be recognized positively during life: (1) Combined sclerosis of the posterior columns and of the crossed pyramidal fasciculi (3 and 10), indicated by ataxia with paralysis, absence of patellar reflex, tendency to contracture, pains, and anæsthesia less marked than in typical posterior spinal sclerosis. This symptom-group is usually found in children; it is pre-eminently a family disease, and is known as Friedreich's disease. Similar cases also occur in adults as a strictly personal disease. (2) Secondary degeneration of the pyramidal tract (10 and 11), with more or less localized atrophy of cells in the anterior horns (9) coexists in two forms: First, in a few cases of cerebral hemiplegia with contracture, and pathological atrophy of various muscles on the paralyzed side; second, as a distinctly spinal bilateral affection, characterized by a spastic or tetanoid state of the lower extremities, and a mixture of atrophic paralysis (vide (a)), with contracture in the arms and hands. This latter form is the amyotrophic lateral sclerosis of Charcot.
SECOND QUESTION.—BEING GIVEN SYMPTOMS INDICATING A TOTAL TRANSVERSE LESION OF THE SPINAL CORD, ONE INVOLVING ITS VARIOUS SYSTEMS AT A CERTAIN LEVEL, TO DETERMINE THE ELEVATION OR FRONTO-CAUDAL SITUATION OF THE LESION.
This question is usually easy of solution by the following method: Since a transverse lesion of the spinal cord gives rise to both motor and sensory symptoms of horizontal, paraplegic distribution caudad of the lesion, the first thing to do is to determine accurately the upper level of the symptom, either the line of anæsthesia or the limit of paralysis. The former is always much more definite than the latter, and usually serves as the guide to diagnosis, indicating accurately the uppermost part of the lesion. In the thorax the levels of sensory and motor symptoms nearly coincide, but in the extremities the operation of Van der Kolk's law of distribution of motor and sensory fibres of nerve-trunks must be borne in mind, although it does not apply as strictly in this case as in nerve lesions strictly speaking. Gowers's diagram will prove very serviceable in making a diagnosis of transverse lesions, and will also prove of use in the study of vertebral injury and disease, as it indicates with sufficient accuracy the relation between vertebræ (spinous processes) and segments of the spinal cord. (Vide Fig. 2.)
The following are the principal transverse localizations of disease which are usually recognized during life by the above procedure:
(a) Lesions of the cauda equina (by tumors, caries, or fracture of the bones, etc.) produce paralysis, anæsthesia, atrophy of muscles, with De R., in the range of distribution of the sciatic nerves mainly. The sphincter ani is paralyzed and relaxed, while the bladder remains normal as a rule. In all essential respects this paraplegiform, but not paraplegic, affection resembles that following injury to mixed nerve-trunks. It is in reality an intra-spinal peripheral paralysis. The more exact location of the lesion, in the absence of external physical signs (fracture, etc.), may be [p. 75] approximately determined by a study of the distribution of the symptoms and their relation to nerve-supply.
(b) Lesions of the lower end of the lumbar enlargement, or conus medullaris, behind the first lumbar vertebra, will give rise to the same symptoms as (a). The expression, lumbar part of the spinal cord, should be more carefully used than it is at present in the discussion of spinal injuries and spinal-cord diseases, disease of the lumbar enlargement being common enough, but disease of the lumbar part of the cord very rare. In the discussion of railway cases, more especially, it is often forgotten that the spinal cord practically ends behind the first lumbar vertebra.
(c) Lesions of the middle and upper parts (segments) of the lumbar enlargement are evidenced by true paraplegia, without paralysis of the abdominal muscles. In some cases the quadriceps group, supplied by the crural nerve, is not paralyzed. The constriction and the limit of anæsthesia are about the knees, at mid-thigh, or near the groin in different cases. The paralyzed muscles, as a rule, retain their irritability and show normal electrical reactions; the cutaneous and tendinous reflexes are preserved or increased. The sphincter is usually paralyzed, while the bladder is relatively unaffected.
(d) Transverse lesion of the dorsal spinal cord produces the classical type of paraplegia—i.e. paralysis and anæsthesia of all parts caudad of the lesion. The limit of anæsthesia and the constriction band are nearly horizontal, and their exact level varies with the height of the lesion, from the hypogastric region to above the nipples. Below the level of anæsthesia, which indicates by the number of the dorsal nerve the upper limit of the cord lesion, there are complete paralysis, retention of urine, constipation with relaxed sphincter ani, greatly exaggerated reflexes in the lower extremities, even to spinal epilepsy; the muscles preserve their volume fairly well, and their electrical reactions are normal—sensibility in all its modes is abolished; bed-sores are easily provoked. Retention of urine is an early symptom in lesion of the middle dorsal region of the cord—sometimes, in our experience, preceding symptoms in the legs.
(e) A transverse lesion of the cord at the level of the last cervical and first dorsal nerves—i.e. in the lower part of the cervical enlargement—gives rise to typical paraplegia with a sensory limit-line at or just below the clavicle, but also with some very peculiar symptoms superadded. These characteristic symptoms are in the upper extremities, and consist of paralysis and anæsthesia in the range of distribution of the ulnar nerves. In the arms the anæsthesia will be found along the lower ulnar aspect of the forearm, the ulnar part of the hands, the whole of the little fingers, and one half of the annuli. There will be paralysis (and in some cases atrophy with De R.) affecting the flexor carpi ulnaris, the hypothenar eminence, the interossei, and the ulnar half of the thenar group of muscles, producing in most cases a special deformity of the hand known as claw-hand or main-en-griffe. Another important symptom of a transverse lesion in this location is complete paralysis of all the intercostal and abdominal muscles, rendering respiration diaphragmatic and making coughing and expectoration impossible. The breathing is abdominal in type, and asphyxia is constantly impending.
(f) A transverse lesion of the upper part of the cervical enlargement, below the origin of the fourth cervical nerve, gives rise to symptoms [p. 76] designated as cervical or total paraplegia. The lower extremities and trunk are as in (d) and (e), but besides both arms are completely paralyzed and anæsthetic. The limit of anæsthesia usually extends along the clavicles to the acromion processes, or a little below, near the deltoid insertions. All reflexes caudad of this line are vastly increased, either with tonic or clonic contractions. In some cases of pressure upon the cervical cord by tumors, caries of vertebræ, etc. the tetanoid or spastic state of the extremities (the lower more especially) may precede paralysis for a long time; as the compression increases paralysis becomes more and more marked, while the reflexes remain high. This constitutes the clinical group we described in 1873 as tetanoid pseudo-paraplegia.
(g) Transverse lesions of the spinal cord from the decussation of the pyramids to the fourth cervical nerve are very rare, and usually of traumatic origin. They produce complete paralysis of the entire body, and also of the diaphragm (third and fourth cervical nerves), thus causing death by apnœa in a very short time.
(h) In ascending paralysis (Landry) the above symptom-groups, excepting (a), (b), are met with at successive stages of the disease, often by almost daily accession, until finally respiration ceases.
(i) The height of a transverse localized lesion (e.g. a stab-wound) of one lateral half of the spinal cord is to be determined by the various groupings of symptoms stated in the preceding paragraphs, the chief guide being the limit-line between the sensitive and anæsthetic portions of the body, measured vertically. The symptoms are, however, distributed in a very remarkable manner on either side of the median line. The paralysis will be found on the same side as the lesion, often accompanied by hyperæsthesia, vaso-motor paralysis, and loss of muscular sense, while the anæsthesia is on the other side of the body. When such a lesion occurs below the first dorsal nerve, the symptom-group is designated as hemiparaplegia; when the lesion is higher up, so as to paralyze the arms, the affection is termed spinal hemiplegia (Brown-Séquard).
Above the decussation of the pyramids total transverse lesions are practically unknown, so that the second question need not be followed farther.
By means of the data above given we are also enabled to determine the length—i.e. fronto-caudal extension—of the systematic lesions of the cord.
The symptoms of transverse lesions of the spinal cord are not exclusively caudad of the lesion, and some very striking ones are observable in the head. In lesions of the upper part of the dorsal cord and of the cervical enlargement (e, f, g) we observe vaso-motor and pupillary symptoms, due to injury of the spinal origin of the cervical sympathetic nerve; the pupils are contracted; the cheeks and ears congested and unnaturally warm; the cutaneous secretions are increased. In other words, the symptoms about the head, frontad of the lesion, are the same as those we produce experimentally in animals by section of the cervical sympathetic or of the lower cervical cord. In hemi-lesion of the cord, in man as in animals, these symptoms are unilateral, on the same side as the injury.
Another point to be remembered in the study of transverse lesions of the spinal cord is that the lesion may involve enough of the anterior [p. 77] gray horns to give rise to atrophic paralysis with De R. in some few muscles deriving their motor innervation from the focus of disease. This is not rarely seen in cervical paraplegia.
THIRD QUESTION.—BEING GIVEN VERY LIMITED MOTOR OR SENSORY SYMPTOMS OF SPINAL ORIGIN, TO DETERMINE THE EXACT LOCATION OF THE FOCAL LESIONS CAUSING THEM.
(a) In the range of sensory disturbances this question rarely presents itself for solution. Localized anæsthesia and pain of spinal origin (except the fulgurating pains of tabes) are rare, and we do not know the relation of cutaneous areas with the spinal segments as well as we know the motor innervations. It should be stated here, however, that the location of a fixed pain and of a zone of anæsthesia is often of great value in determining what spinal nerve is affected, just outside of the cord itself, by such directly-acting lesions as vertebral caries, spinal pachymeningitis, tumors upon the spinal cord, etc. Among the various symptoms of Pott's disease of the spine, fixed pains in one side of the trunk, in one thigh, or in the upper occipital region, etc. is a sign against which the physician should always be on his guard, as it is a very early and valuable indication of the existence of an affection which requires special treatment as soon as a diagnosis can be made.
(b) Localized motor symptoms of spinal origin calling for a diagnosis of the focal lesions causing them are frequent, and are mostly met with in two affections—viz. progressive muscular atrophy and poliomyelitis. The problem is now capable in many cases of an approximately exact solution by the deductive application of our knowledge of the intimate connection between certain muscles and muscular groups and limited portions or segments of the spinal cord (anterior gray horns more especially). This knowledge has been accumulated and organized from ordinary anatomy, physiological experiments, and more especially from carefully-made autopsies with microscopic examination of the cord. We cannot present this subject better than by reproducing a tabular statement of these results prepared by M. Allen Starr.5 Future autopsies may correct this table, and in making use of it the occurrence of anomalous nerve-distribution should be remembered:
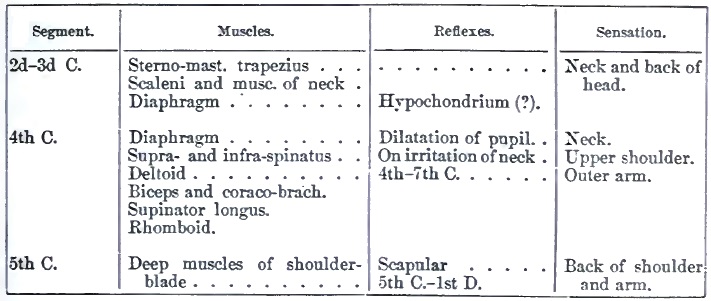
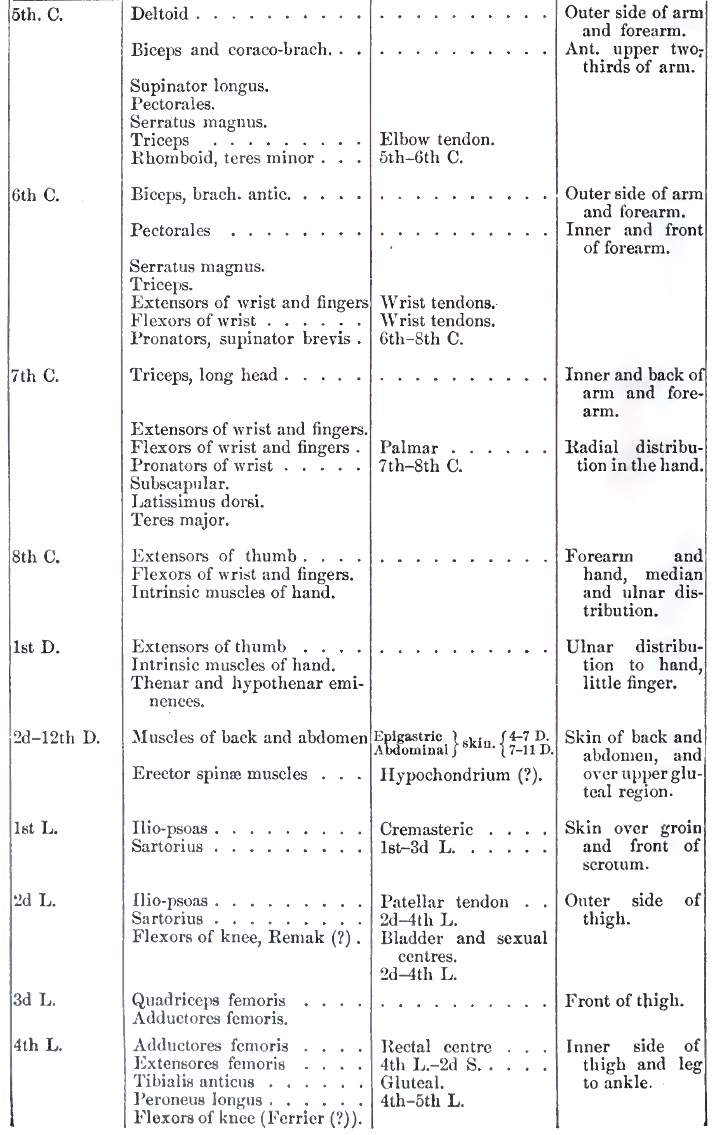
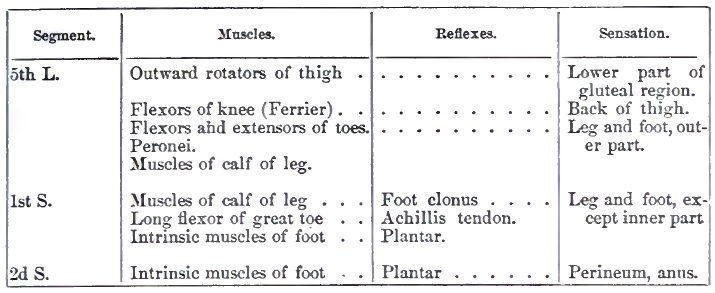
5 “The Localization of Functions of the Spinal Cord,” American Journal Neurology and Psychiatry, iii., 1884.
The above table should be studied in connection with Gowers's diagram of the vertebral column and spinal cord (Fig. 2, p. 53), for the thorough study of cases of neural and spinal localization. Additional details of much value with respect to the peripheral nerve distribution are accessible in the works of Ranney6 and Ross7.
6 The Applied Anatomy of the Nervous System, N. Y., 1881, p. 355 et seq.
7 Handbook of Diseases of the Nervous System, Am. ed., Philada., 1885, p. 356 et seq.
In general terms, lesions of the oblongata are characterized by the early appearance and prominence of motor symptoms in the mouth, throat, and larynx, and by bilaterality of the symptoms. Remote symptoms consist of disturbances in the cardiac action and in the functions of some intra-abdominal organs. There may also be more or less paralysis of all the extremities. These lesions may conveniently be classified, like those of the cord, into systematic and focal.
A. SYSTEMATIC LESIONS OF THE OBLONGATA.—1. Systematic lesions of the æsthesodic system of the oblongata are, for purposes of practical diagnosis, unknown at the present time.
2. Systematic lesions of the kinesodic system of the oblongata, on the other hand, are often positively recognizable during the patient's life.
(a) The most strictly systematic and most frequent of these lesions is that of secondary (Wallerian) degeneration of the pyramids, the prolongation of the cerebral motor tract. This morbid change gives rise to no distinct bulbar symptoms, and it can only be diagnosticated inferentially or inclusively by determining the existence of secondary degeneration of the entire pyramidal tract, from the occurrence of hemiplegia followed by contracture and increased reflexes. If the phenomena present be those of double spastic hemiplegia, there is surely degeneration of both pyramids.
(b) A systematic lesion affects the nuclei (origins) of the facial, hypoglossal, pneumogastric, spinal accessory, and the motor root of the trigeminus nerves, giving rise to a classical symptom-group. The symptoms thus produced are exclusively (?) motor and trophic, consisting of progressively increasing paresis, with atrophy of the muscles about the lips [p. 80] and cheeks, the intrinsic lingual muscles, the laryngeal and pharyngeal muscles. Later, the masseters, temporals, and pterygoids are sometimes involved; and, finally, extremely rapid action of the heart with pneumonic symptoms indicates the gravest extension of the morbid process. An early symptom in such cases is abnormal salivation. These affections, generally designated as varieties of bulbar paralysis, subacute or chronic, are usually readily recognized intra vitam, and recent discoveries in morbid anatomy have enabled us to correctly diagnosticate the seat of the lesion in its various extensions. The laryngeal paralysis represents disintegration (atrophy) of ganglion-cells in the bulbar origin of the spinal accessory nerve; lingual atrophic paralysis indicates the same lesion in the nuclei of the hypoglossal nerves; the labio-buccal symptoms are produced by lesion of the facial nerve nucleus (inferior facial nucleus of older writers); the paralysis of the muscles of mastication is due to extension of cell-degeneration to the motor nucleus of the trigeminus in the pons; and the final cardio-pulmonary symptoms indicate an extension of the lesion into the sensory (?) origin of the pneumogastric nerves.
It is evident that this systematic lesion of the oblongata is the equivalent or analogue of the various acute and chronic lesions of the anterior horns of the spinal cord, described supra, and in practice we sometimes find these bulbar and spinal lesions associated: progressive muscular atrophy of the extremities and amyotrophic lateral sclerosis being complicated with bulbar paralysis.
B. FOCAL LESIONS OF THE MEDULLA OBLONGATA, as at present known, occur mostly in the kinesodic system, but may also involve several fasciculi and nuclei at one time. The symptoms of such lesions are grouped in two principal types:
(a) Single symptoms, such as atrophy or atrophic paralysis of some one muscle or muscular group innervated by the hypoglossal, facial, or spinal accessory nerves. For example, unilateral atrophy of the tongue, when not due to neural injury, is quite surely the representative of destruction of one hypoglossal nucleus. It is possible that some cases of peripheral facial paralysis, so-called, or Bell's palsy, and cases of paralysis of the sterno-mastoid and trapezius, are not due to neural lesion, but to primary disease of the nuclei of the facial and spinal accessory nerves, either as poliomyelitis or as progressive cell-degeneration and atrophy.
A similar reserve must be used in speaking of the localization of small lesions in the oblongata, causing diabetes mellitus, polyuria, albuminuria, and salivation. From experiments upon animals and a few post-mortem examinations in human cases we know that such lesions may occur and cause the symptoms, but their recognition during the patient's life is at the present time next to impossible.
(b) The symptoms may be complex and belong to the general class of crossed paralysis, the mouth, face, tongue, and larynx being paralyzed (often with anæsthesia of the face) on one side, while the extremities are paralyzed on the other side. Such a symptom-group would indicate a large lesion (tumor) in one lateral half of the oblongata, more especially in its ventral aspect. These localizations will be studied more in detail farther on, under the general head of Crossed Paralysis due to Lesions of the Base of the Brain.
[p. 81]Under this head, to prevent repetition and to facilitate condensation, we will consider the various localizations which can now be diagnosticated in the cerebrum, basis cerebri, and cerebellum.
It would be of the greatest advantage to preface these statements by a full summary of the anatomical and physiological data on which the localizations rest, but space is wanting for such an exposition, and the reader who is not already familiar with these branches of medical science will have to seek information in other accessible works.8
8 Ferrier, The Functions of the Brain, Am. ed., N. Y., 1876; Charcot, Lectures on Localization in Disease of the Brain, Am. ed., N. Y., 1878; Seguin, E. C., “Lectures on the Localization of Spinal and Cerebral Diseases,” N. Y. Medical Record, 1878; Ranney, Applied Anatomy of the Nervous System, N. Y., 1881; Meynert, Psychiatry: A Clinical Treatise on Diseases of the Fore-brain, Part I., Am. ed., 1885.
In a general way, encephalic lesions are distinguished by the following:
Positive Characters.—Tendency to strictly hemiplegic or bilaterally hemiplegic grouping of symptoms; frequency of contracture or of a spastic state of the paretic muscles; increase of reflexes in the affected extremities; spasmodic manifestations in remote muscular groups, but not in areas of nerve-distribution (forms of Jacksonian epilepsy); the presence of paralytic and anæsthetic symptoms in the range of distribution of cranial nerves; frequency of neuro-retinitis or atrophy of the optic nerves; occurrence of lateral hemianopsia; production of symptom-groups known as varieties of crossed paralysis; frequency of head symptoms, as headache, vertigo, apoplectic and epileptic seizures; mental symptoms of various sorts, dementia, coma, etc.
Negative Characters.—Absence of truly paraplegiform distribution of symptoms, even when they are bilateral; of cincture feelings; of pain or other paræsthesiæ and anæsthesia in the distribution of nerve-trunks; of muscular atrophy and De R. in paralyzed parts. Rarely do we observe visceral paralysis and bed-sores.
Pathological localizations in the encephalon may conveniently be grouped under two heads—viz. systematic and focal lesions.
A. SYSTEMATIC LESIONS OF THE ENCEPHALON.—The recent advances of embryology, anatomy, physiology, and pathological anatomy have conclusively established the existence, and fairly well defined the limits, of a sensory (æsthesodic) and of a motor (kinesodic) tract in the brain; and certain lesions of these tracts produce such precise symptom-groups that their diagnosis during the patient's life is often possible, and that, too, with great exactness.
1. SYSTEMATIC LESIONS OF THE ÆSTHESODIC SYSTEM OF THE ENCEPHALON.—The limits of this system are as follows: Within the oblongata and pons it occupies a somewhat uncertain (from a clinical standpoint) location, its fasciculi and ganglia lying in a general way dorso-laterad of the motor or kinesodic system. In the crus cerebri the fibres of the sensory tract are more closely packed together, and constitute a dense fasciculus of white substance in the lateral part of the crus in its subcerebral extremity, estimated by Flechsig at about one-fifth of the entire crus, and thence it enters into the composition of what is known as the internal capsule. This narrow but all-important mass of [p. 82] white fibres, as revealed by a horizontal section of the hemisphere (vide Fig. 7), lies between the nucleus caudatus and the nucleus lentiformis, and between the latter and the thalamus, thus assuming a V or elbow shape. Of this, the caudal third of that part of the capsule behind the bend or angle contains all the sensory paths for the opposite half of the body, reinforced by paths for the special senses; it is the carrefour sensitif of French writers. From this region sensory fasciculi radiate to various parts of the cerebral cortex—in the parietal, temporal, and occipital gyri—in which physiological experiments and human cases of disease have shown sensory areas or centres. Of the fasciculi from special sense-organs which reinforce the internal capsule, the only one which is well defined and easily traceable is the fasciculus opticus (fasciculus of Gratiolet), derived in part directly from the optic tract of the same side and from the primary optic centres (lobus opticus, corpus geniculatum laterale, and pulvinar), proceeds, along with fibres of the internal capsule, dorso-laterad of the posterior cornu of the lateral ventricle, to the mesal aspect of the occipital lobe. A fasciculus from the olfactory apparatus doubtless also joins the internal capsule, but its course is unknown.
The following localization diagnoses are now possible in the æsthesodic system as above defined:
(a) A lesion of the internal capsule, just above the crus cerebri, involving its bend or knee and caudal segment, with or without injury to the nucleus lentiformis and thalamus, will give rise to the following symptoms: Complete typical hemiplegia and total hemianæsthesia on the opposite side of the body; the anæsthesia involves the special senses as well as the body. Vision is, however, unaffected, unless the lesion extend far enough back to involve the pulvinar and fasciculus opticus, when lateral hemianopsia occurs (dark half-fields on the side opposite the lesion). When this lesion is in the left hemisphere, sensory aphasia also occurs.
(b) A lesion involving the caudal part of the thalamus and of the internal capsule. With such a lesion the motor symptoms consist in transient paralysis, with usually persistent post-paralytic chorea or ataxia. The sensory symptoms are more marked, and resemble those produced by lesion (a). It may be determined with some degree of accuracy whether the lesion be in the thalamus border, or in the internal capsule near to the nucleus lentiformis by the absence in the latter case of lateral hemianopsia.
The topography of such lesions is illustrated by Fig. 7.
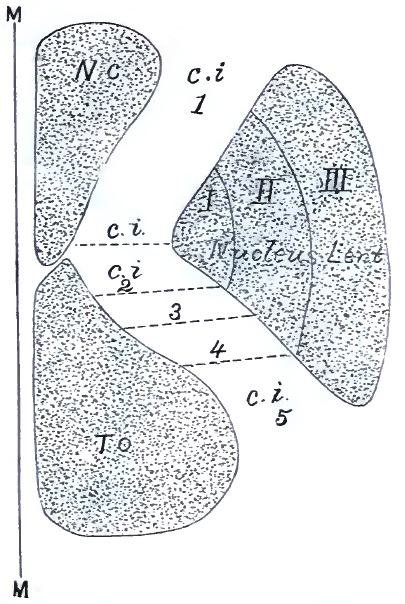
(c) Lesions of cortical areas connected with fasciculi of the sensory part of the internal capsule (c. i. 5).
(α) Lesion of the cortical area or centre for smell cannot at present be diagnosticated. From the results of experiments upon higher mammals we would expect such a centre to be in the cortex of the mesal gyri of the temporal lobe.
(β) Lesions of the cortical centre for taste are equally unknown; it is probably situated in the meso-basal aspect of the temporal lobe.
(γ) Lesions of the acoustic centre are somewhat better known, at least as far as the function of hearing language-sounds (psychic hearing) is concerned. A number of recently-published cases9 have quite positively [p. 83] shown that the existence of word-deafness indicates a destructive lesion of the dorsal gyri (more particularly the first and second) of the temporal lobe (the left always?). The lesion may also be in the inferior parietal lobule and gyrus supramarginalis, penetrating deeply enough to injure the acoustic fasciculus on its way from the internal capsule to the centre.
9 R. W. Amidon, “On the Pathological Anatomy of Sensory Aphasia,” New York Medical Journal, xl. 113, 181.
(δ) The centre for visual impressions is now the best known of any of the sensory cortical areas. The experimental studies and pathological results of the last few years have indicated that the occipital lobe was probably the seat of higher, organized vision (for form and color). More recent autopsies and re-examination10 of the subject point to the cuneus and adjacent gray matter as the visual centre. The anatomical arrangement is, however, peculiar and complex, in that each cortical visual area receives impressions from one lateral half of both retinæ, through the fasciculus opticus.
10 E. C. Seguin, “A Contribution to the Pathology of Hemianopsia of Central Origin (Cortex-hemianopsia),” Journal of Nervous and Mental Diseases, 1886, No. 1.
Destructive lesion of one visual centre is therefore indicated during [p. 84] life by the symptom lateral hemianopsia alone (the dark half-fields on the side opposite the lesion).
The accompanying diagram illustrates the course of the visual paths from the eyes to the cortical centres, and the mechanism of production of various forms of hemianopsia:
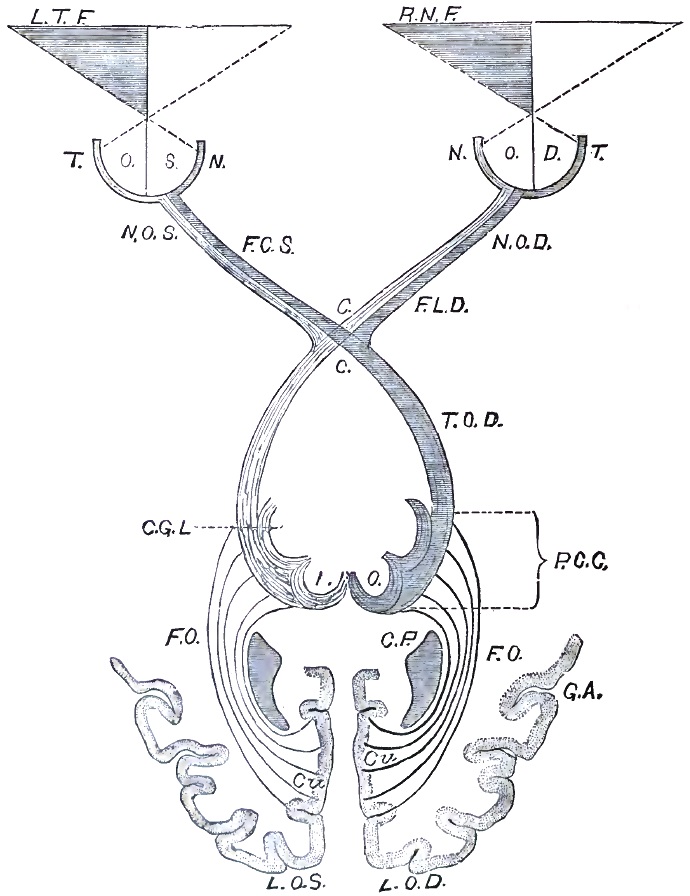
The following diagnostic propositions are applicable to cases presenting the symptom lateral hemianopsia:
“1. Lateral hemianopsia always indicates an intracranial lesion on the opposite side from the dark half-fields.
“2. Lateral hemianopsia, with pupillary immobility, optic neuritis, or atrophy, especially if joined with symptoms of basal disease, is due to lesion of the tractus opticus or of the primary optic centres on one side.
“3. Lateral hemianopsia, or sector-like defects of the same geometric order, with hemianæsthesia and choreiform or ataxic movements of one-half of the body without marked hemiplegia, is probably due to lesion of the caudo-lateral part of the thalamus or of the caudal division of the internal capsule (vide Fig. 7).
“4. Lateral hemianopsia, with complete hemiplegia (spastic after a few weeks) and hemianæsthesia, is probably caused by an extensive lesion of the internal capsule in its central and caudal part.
“5. Lateral hemianopsia, with typical hemiplegia (spastic after a few weeks), with aphasia if the right side be paralyzed, and with little or no anæsthesia, is quite certainly due to an extensive superficial lesion in the area supplied by the middle cerebral artery; we should expect to find softening of the speech-centre, of the motor zone and of the gyri lying at the extremity of the fissure of Sylvius—viz. the gyrus supramarginalis, inferior parietal lobule, and gyrus angularis. Embolism or thrombosis of the middle cerebral artery would be the most likely pathological cause of the softening.
“6. Lateral hemianopsia, with moderate loss of power in one-half of the body if associated with impairment of muscular sense, but without ordinary anæsthesia, would probably be due to a lesion of the inferior parietal lobule and gyrus angularis, with their subjacent white substance, penetrating deeply enough to sever or compress the optic fasciculus in its way caudad to the visual centre.
“7. Lateral hemianopsia, without motor or common sensory symptoms; this symptom alone, is due, we believe from the convincing evidence afforded by Cases 28, 29, 41, and 45, to lesions of the cuneus only, or of it and of the gray matter immediately surrounding it on the mesal surface of the occipital lobe in the hemisphere opposite the dark half-fields. Most surgical cases of lateral hemianopsia come at once or after convalescence within this rule, or No. 6.”11
11 Seguin, op. cit.
The cortical visual area, as above defined, is supplied by one large vessel—viz. the occipital artery, a branch of the posterior cerebral. Embolism or thrombosis of the former vessel is to be thought of as the probable cause of a suddenly-developed lateral hemianopsia without paralysis or anæsthesia.
(ε) The cortical centre for sensory impressions of muscular sense, so called, is probably located in the inferior parietal lobule. The diagnosis of a lesion so placed, in a case presenting along with other sensory or with motor symptoms marked impairments of muscular sense in the arm and leg of one side, is justified by a few recent cases.12 Spitzka [p. 86] believes that he has clinically and pathologically demonstrated a basal path (fasciculus) for this mode of sensibility in the pons and oblongata, dorsad of the pyramidal tracts.13
12 Westphal, Charité Annalen, vii. p. 446, 1882; Stenger, Archiv f. Psychiatrie u. Nervenkrankheiten, xiii. p. 240, Case viii.; Wernicke u. Hahn, Virchow's Archiv, lxxxvii. p. 325; Ball and Seguin, Archives of Medicine, New York, v. p. 136.
13 Spitzka, “A Contribution to the Morbid Anatomy and Symptomatology of Pons Lesions,” American Journal of Neurology and Psychiatry, ii. p. 617 (1883).
(ζ) Lesions of the cortical area for common cutaneous sensibility cannot be positively recognized at the present time. By exclusion of the better-known centres, and from experimental data, we may approximately locate it in the gray matter lying ventrad of (below) the inferior parietal lobule, extending to the base, and possibly the mesal aspect, of the temporal lobe, and possibly also on the lateral aspect of the occipital lobe.
2. LESIONS OF THE KINESODIC SYSTEM OF THE ENCEPHALON.—The kinesodic system is far better understood, anatomically and physiologically, than the æsthesodic. Its limits, beginning from the junction of the cord and oblongata, are as follows: The pyramids, containing the fibres of the direct and crossed pyramidal fasciculi of the cord (Fig. 5, Nos. 10 and 11), form the meso-basal aspect of the oblongata, appearing on either side of the median line as two large distinct bundles of white substance which enter the pons under its projecting transverse fibres. Within the pons each pyramid is divided into quite a number of fasciculi more or less separated by fibres of other systems. Again collected, these bundles constitute a considerable part of the crus cerebri—its basal middle two-fifths. (The outer or latero-dorsal one-fifth part of the crus belongs to the æsthesodic system, the middle (intermediate) two-fifths are the pyramidal fibres, and the remaining two-fifths, meso-basal part, contain some fibres from the direct cerebral motor tract destined for the hypoglossal and facial nuclei, and also large bundles probably derived from the nucleus caudatus and frontal lobes). As the crus enters the cerebrum and becomes what we know as the internal capsule, the pyramidal fibres occupy the bend or elbow of the capsule and part of its caudal segment (vide Fig. 7).
From this level the fibres of the internal capsule again diverge, as fasciculi whose physiological independence has been well determined, going dorsad and frontad to certain gyri of the cerebral cortex where their fibres join ganglion-cells. Three large fasciculi and corresponding cortical areas are recognized as constituting the pyramidal tract, strictly speaking: (1) A fasciculus which extends frontad to the base of the second frontal gyrus where it coalesces with the precentral, the centre and fasciculus for movements of the facial muscles of the opposite side; (2) a fasciculus which extends to the precentral and postcentral gyri, more especially in their middle part, constituting the centre and fasciculus for movements of the arm and hand; (3) another fasciculus which goes dorso-mesad, almost vertically in the brain, to join the ends of the pre- and postcentral gyri at the top of the hemisphere, and their continuation upon its mesal aspect known as the paracentral lobule, centre and fasciculus for movements of the opposite foot and leg. Besides these three great cortical areas and their connected fasciculi of nerve-fibres, which go to make up the pyramidal tract, we recognize (4) a cortical centre for speech movement of the tongue and lips in the base of the left third frontal gyrus over the fissure of Sylvius (Broca's speech-centre), with a connected white fasciculus which passes into the elbow of the internal [p. 87] capsule, and can be traced (by means of secondary degeneration) into the inner part of the base of the crus and into the pons, but not to the pyramid. Another probable centre (5), for coarse lingual movements and for the various movements of deglutition, is in the folds of the insula, its fasciculus not joining the pyramid.
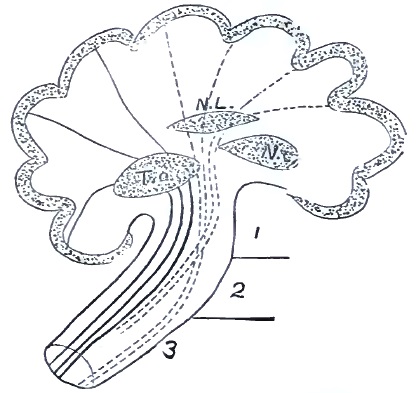
The location of two other motor centres—one for the movement of the eyeballs in or near the gyrus angularis, and one for vocal laryngeal movements in the base of the right third frontal gyrus (homologous to the speech-centre in the left hemisphere), is problematical, or at least not well enough established to be recognized in a practical treatise.
Recent experimental researches have shown that to electrical excitation at least the fasciculi for the tongue, face, arm, and leg yield the same distinct reaction (isolated muscular contractions) as do their respective centres or cortical areas; perhaps they are more excitable.
When these cortical areas are destroyed by disease, or when their connected fasciculi are severed, secondary degeneration takes place and extends to the end of the respective bundles, even to the lower extremity of the spinal cord.
Before leaving the subject of the composition of the kinesodic system it is desirable to add a few words concerning the decussation of the pyramids or distribution of the pyramidal tract in the spinal cord. As is well known, this is double, a small part of the pyramidal bundle remaining on the same side of the median line, the so-called direct pyramidal fasciculus or column of Türck (Fig. 5, No. 11) forming the mesal edge of the anterior column of the cord. The larger part of the pyramid crosses the median line at the decussation, and enters the opposite lateral half of the cord, in which it is found as the crossed pyramidal fasciculus (Fig. 5, No. 10) in the posterior part of the lateral column, rapidly diminishing in size in the dorso-lumbar part of the cord. The [p. 88] important point to bear in mind for the study of monoplegias and of hemiplegia is that the amount of decussation is far from uniform. This variability was first demonstrated by Flechsig.14 He found in a series of sixty fœtuses such variations in the relation of the crossed and direct fasciculi as 100:0 (complete decussation), 92:8, 84:16, 70:30, 52:48 (nearly semi-decussation, producing equal fasciculi), 35:65, 10:90 (almost non-decussation).
14 Die Leitungsbahnen im Gehirn und Rückenmark des Menschen, Leipzig, 1876.
It should also be added that quite certainly the cerebellum, nucleus caudatus, nucleus lentiformis, and nucleus pontis form parts of the complete kinesodic system, but we are as yet ignorant of their exact connections and functions.
With respect to the anterior part of the frontal lobe, forward of the oblique line A B across Figs. 10 and 11, the study of human cases of destructive injury and disease would indicate that it is not associated either with the kinesodic or with the æsthesodic systems.
The SYMPTOMS of lesions of the kinesodic system, particularly of the pyramidal tract, are exclusively motor, consisting of spasm and paralysis. Contracture of the paralyzed parts follows the paralysis after a few weeks if the lesion be a destructive one.
Clinically, the following DIAGNOSES of localization of lesions in this system are now possible:
(a) Lesion of the speech-centre (4) and of its associated white fasciculus is indicated by intermittent or constant aphasia of the motor form, with or without paralysis of the face and limbs (on right side usually).
(b) Lesion of the facial centre (1) and of its associated fasciculus is characterized by the occurrence of spasm or paralysis, or of both in rapid succession, in the facial muscles; their electrical reactions remaining normal.
(c) Lesion of the brachial centre (2) and of its associated fasciculus is made known by spasm or paralysis, or by both in succession, in the hand and arm. In many cases (tumor especially) the first symptom is clonic convulsive movements of two or more fingers, extending to other parts of the arm. Such brachial monospasm or monoplegia is usually accompanied or followed by incomplete hemiplegia.
(d) Lesion of the crural centre (3) in the paracentral lobule and of its associated fasciculus of white substance is indicated by priority and predominance of convulsive and paralytic phenomena in the foot and leg: a crural monospasm or monoplegia exists with or without incomplete hemiplegia.
The positive diagnosis of these separate localizations is most feasible in cases of tumors or of cranial injury where the initial lesion is limited in extent and where the morbid process is for a time localized. As a rule, localized spasm (Jacksonian epilepsy) without loss of consciousness is the first symptom, followed after a time by localized paralysis (always in the same muscular groups); and later still the symptom-group becomes obscured by the supervention of other symptoms indicating extension of disease to other parts of the kinesodic system, or even to the æsthesodic system.
(e) Lesion of the insula and adjacent white substance laterad of the nucleus lenticularis (5) may be suspected from the rapid or sudden development of symptoms imitating those of acute bulbar paralysis, but [p. 89] without bilateral paresis of the body and anæsthesia. Aphasia is very apt to coexist with the bulbar symptoms if the lesions involve the left insula, whose frontal folds are continuous with the speech-centre.
Common hemiplegia with contracture, but without anæsthesia, represents a gross lesion of the kinesodic system, involving several cortical centres or the motor part of the internal capsule:
(1) A widely-spread lesion of the cortex of the brain, softening of the motor zone (centres 1, 2, 3, 4) from embolism or thrombosis of the middle cerebral artery.
(2) Hemorrhage from vessels of the nucleus caudatus and nucleus lentiformis compressing or destroying the motor segment of the internal capsule at various levels. More rarely there is a form of softening or gliomatous growth involving the same parts. Any of these lesions may be so localized as to destroy only one fasciculus of the capsule, giving rise to monoplegia.
The limits of the so-called sensory and motor centres or cortical areas, and the possible localization of lesions in them, will be better understood by the help of the accompanying diagrams (Figs. 10 and 11, p. 90) of the lateral and mesal aspects of the hemisphere.
B. FOCAL LESIONS OF THE ENCEPHALON.—1. FOCAL LESIONS OF THE CEREBRUM, OF ITS CORTEX AND SUBJACENT WHITE SUBSTANCE, AND BASAL GANGLIA.—(a) Focal lesions of the frontal lobe produce no specific symptoms, and cannot be directly diagnosticated unless they extend as far caudad as the base of the second and third frontal gyri. The forward mass of the frontal lobe, including the orbital lobule (vide Fig. 10), appears to be inexcitable and insensitive. Even psychic symptoms do not necessarily appear after the loss of considerable amount of cerebral substance from this region. The diagnosis of tumors, abscesses, etc. in this part of the brain must be made by taking into consideration the seat of pain, the presence of cicatrices or other etiological indications, the general signs of the cerebral irritation and compression, but, after all, usually by exclusion. In some cases unilateral anosmia is produced.
(b) Focal lesions of the caudal part of the frontal lobes, of the insula, the pre- and postcentral gyri, and other parts of the motor zone are usually easy of diagnosis. The symptoms of such lesions have already been detailed when speaking of lesions of the kinesodic system.
(c) Focal lesions of the parietal, temporal, and occipital lobes of the brain have the characteristic semeiology of lesions of the æsthesodic system, considered supra.
(d) Lesions of the so-called basal ganglia, the nucleus caudatus, nucleus lentiformis, and thalamus, usually give rise to motor and sensory symptoms indirectly by pressure upon or destruction of the segments of the internal capsule which lie between these bodies (vide Figs. 7 and 9). Lesions of the nuclei caudatus and lentiformis are thus more prone to produce purely motor symptoms, while sensori-motor and ataxic symptoms result from lesion of the thalamus.
The symptoms indicating lesions strictly limited (in extent and in effect) to these ganglionic bodies are at present practically unknown.
(e) Lesions (tumors, etc.) of the lobi optici (tubercula quadrigemina) are productive of early neuro-retinitis and blindness, of convulsions, and of diffused bilateral incomplete paralysis of the body, without symptoms [p. 90] of disease at the base of the brain (vide infra). The diagnosis intra vitam remains of great uncertainty, inasmuch as other lesions in the median line, involving parts adjacent to the lobi optici, may give rise to the same symptom-group.
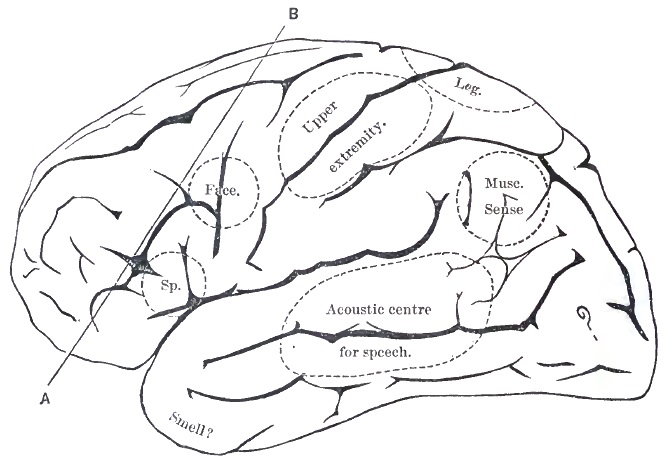
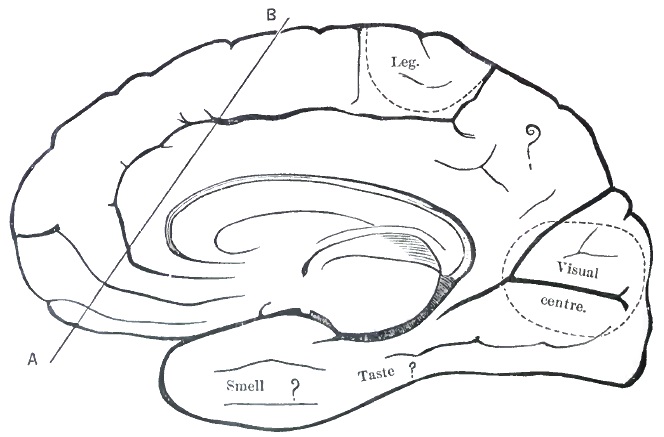
2. FOCAL LESIONS OF THE CEREBELLUM.—(a) Lesions strictly limited to one lateral lobe or hemisphere of this organ do not give rise to any characteristic symptoms—in some cases, indeed, to no symptoms at all. When the lesion tends basad, irritating and compressing the subjacent pons and oblongata on one side, incomplete paralysis appears in the limbs opposite the lesion, the face usually remaining normal. Occipital [p. 91] headache, attacks of vomiting, opisthotonos, or intense subjective stiffness of the back of the neck, with neuro-retinitis, would strengthen the diagnosis. If the lesion extend laterad, so as to involve the processus ad pontem (lateral peduncle), a tendency to rotate while lying or to deviate in walking toward the side of the lesion may be added.
(b) Lesions of the middle lobe, or vermis superior in particular, may be positively recognized during life. Besides the above-mentioned general symptoms of cerebellar and bulbar irritation and compression—viz. occipital headache, cervical stiffness, attacks of vomiting, neuro-retinitis, and atrophy of the optic nerve—there is a very characteristic, almost pathognomonic, symptom. This is cerebellar titubation, miscalled cerebellar ataxia. The patient, whose equilibrium may be perfect while lying or sitting, upon rising and attempting to walk does so somewhat like an intoxicated person: the head and body are bent forward; the arms and hands held out and moved as balancing weights; the feet are widely separated, the toes clutching the floor or carpet; the body oscillating somewhat over its base of support. There are not the wide excursions of the entire body, the zigzagging, of alcoholic intoxication, nor is there any of the stamping or jerky step of locomotor ataxia. If the patient be tested lying or sitting, it is found that neither in the hands nor in the legs is there a trace of ataxia: muscular strength and sensibility are long preserved, and the patellar reflex is exaggerated.
3. FOCAL LESIONS OF THE BASE OF THE BRAIN, either within the nervous substance or springing from the dura, and acting by irritation and pressure upon various parts of the basal aspect of the encephalic mass.
(a) Diffused bilateral lesions of this class situated frontad of the crura give rise to more or less distinct symptoms, and a diagnosis is sometimes possible. (1) Lesions in the vicinity of the sella turcica and optic chiasm produce symptoms in the optic apparatus very early, and these remain prominent throughout the illness. These symptoms are, irregular (at least not lateral) hemianopsia, neuro-retinitis followed by atrophy of the optic nerve, temporary or permanent paralysis of one or several ocular nerves. If these exist without symptoms of lesion of other parts of the brain (reasoning by the process of exclusion), we may strongly suspect the seat of the lesion to be in the region named. Other symptoms are paroxysmal headache and occasional vomiting, epileptiform convulsions (never Jacksonian in distribution), partial hemiplegia, or general muscular weakness. By such data we were recently led to the correct localization of a tumor. (2) If the lesion be farther frontad—i.e. strictly in the orbital areas of the basis cerebri—anosmia, uni- or bilateral, usually with hallucinations of smell, will be an early symptom, along with neuro-retinitis and obscure motor and sensory symptoms (headache and convulsions more especially).
(b) Lesions situated caudad of the infundibulum. (1) Bilateral lesions give rise to symptoms which are the symmetrical duplication on either side of the face and body of those to be next described as characteristic of—
(2) Unilateral focal lesions of the base of the encephalon from the crura caudad to the pyramidal decussation.
In a general way, the symptoms of these lesions are designated as varieties of crossed paralysis.
Clinically, a crossed paralysis is one in which one or several cranial [p. 92] nerves show symptoms of irritation or destruction on one side of the median line, while body symptoms are present on the opposite side.
Physiologically and anatomically, a crossed paralysis is one in which the lesion is so placed as to affect a cranial nerve (or more than one) at a point caudad (below) of the decussation of the fibres which connect its nucleus with the cerebral cortex, or at its nucleus of origin, or so as to injure the nerve-trunk itself; while at the same time the lesion affects the main fasciculus of the pyramidal tract frontad (above) of its decussation, in the crus, pons, or oblongata.
In many cases of crossed paralysis, besides common motor and sensory symptoms, there is apt to be neuro-retinitis with its consequences.
The chief forms or types of crossed paralysis are:
(α) Lesions involving the meso-ventral aspect of one crus cerebri. The direct symptoms of such a lesion are in the range of distribution of the motor oculi (N. iii.), such as ptosis, mydriasis, external strabismus, and heteronymous diplopia; the crossed symptoms are more or less complete paralysis of the lower part of the face and of the extremities on the opposite side (hemiplegia). This relatively frequent form of crossed paralysis we designate as the eye-and-body type.
(β) The lesion occupies the latero-ventral part of the crus. This rare localization would give rise to direct paralysis of the fourth nerve, indicated by homonymous diplopia in the lower inner field of vision; to lateral hemianopsia with dark half-fields opposite the lesion, from injury to the tractus opticus (vide Fig. 8); and to a mixed motor and sensory disturbance in the opposite side of the face and body, without anæsthesia of the olfactory and auditory apparatus. A very large lesion involving almost the entire crus would probably also cause direct paralysis of N. iii.
(γ) Lesion of the basal part of the pons frontad of an imaginary transverse line passing through the apparent origin of the trigemini (NN. v.). Symptoms: A common hemiplegia of the lower face and extremities on the opposite side with neuro-retinitis and other general signs of basal disease. The abducens nerve (N. vi.) would in some cases be involved in its course frontad over the pons, giving rise to internal strabismus and homonymous diplopia on the same side as the lesion.
(δ) A focal lesion in the caudo-ventral part of the pons—i.e. caudad of an imaginary transverse line passing through the trigeminus roots—gives rise to highly characteristic symptoms. These are: Direct paralysis of the face, not (?) affecting all the muscles, but without De R., and common hemiplegia of the limbs on the opposite side.
If the lesion be strictly basal—i.e. one springing from the membranes or bone, the trunks of the sixth and seventh (facial) nerves are directly injured, and the resulting facial paralysis is of the peripheral form, affecting all the muscles and yielding De R. The body symptoms on the side opposite the lesion are less marked.
In the first category of cases, those in which the lesion is in the substance of the pons, the motor fasciculus from the cortex cerebri to the nucleus of N. vii. is injured caudad of (below) its theoretical decussation-point on the middle part of the pons, while the pyramidal tract is involved frontad of (above) its decussation.
This symptom-group is known as face-and-body type, or as crossed hemiplegia, strictly speaking.
[p. 93](ε) A lesion so placed laterally in or on the pons as to affect the origin of one trigeminus (N. v.) will cause, besides motor symptoms in the face and body (types γ or δ), special direct symptoms—viz. anæsthesia in the distribution of the fifth nerve and paralysis of the masticatory muscles opposite to the body symptoms. This is the trigeminus and body type.
Lesions may be so placed ventrad or laterad upon or in the oblongata as to give rise to other types of crossed paralysis: these are easily assumed in a theoretical manner, but in practice such cases are extremely rare, present a complicated semeiology, and are usually not correctly diagnosticated during the patient's life.
The study of cerebral localizations from a diagnostic and practical point of view would be incomplete without a brief reference to the relations existing between the various gyri of the cerebrum and the external surface of the head, in order to render more accurate the estimation of the actual location of cerebral injuries and diseases.
The surgical anatomy of the head with reference to its contents has been developed with remarkable completeness during the past fifteen years, chiefly by the researches of Broca, Bischoff, Heftler, Turner, and Féré. Acting upon these data, a number of surgeons have successfully trephined the skull for the result of injuries, for abscess, and even for tumors.
The location of many convolutions and fissures of the cerebrum can be accurately mapped out upon the surface of the skull, or even upon the head of the living subject, from the projections of certain lines and measurements from points thus obtained, as well as from some natural landmarks. For the projection of these lines the head is placed in a particular position, as can easily be done when we operate upon a bare skull, but which can also be approximated when we deal with a living subject either sitting or lying in bed. The skull or the shaven head should be so placed and held that a line passing from the alveolar process of the superior maxilla and through the lowest part (condyles) of the occipital bone shall be truly horizontal. The greatest care should be used to determine this line—the alveolo-condyloid plane of Broca—for upon it all other projections and measurements are based. This position of the head and the alveolo-condyloid plane (line 1-1) are represented in Fig. 12.
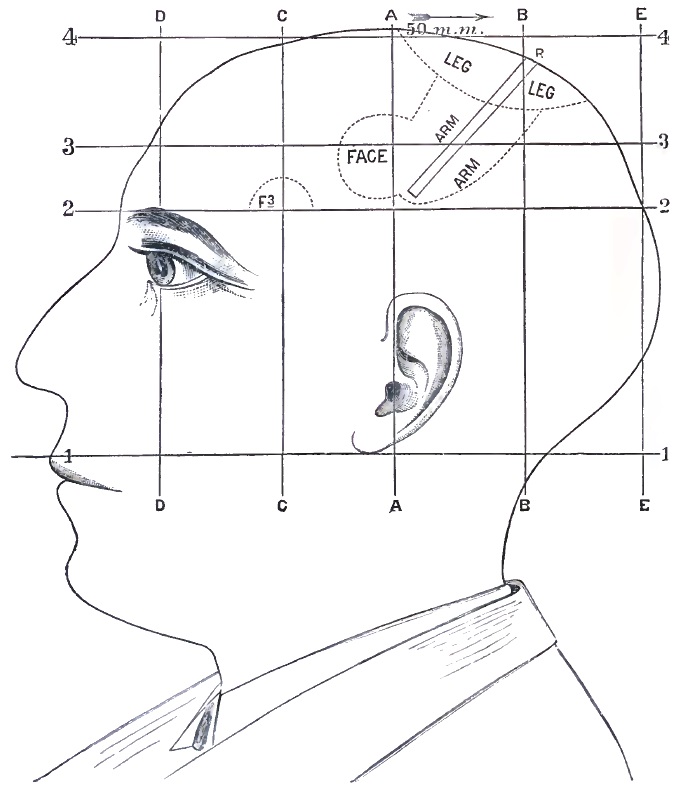
From this line (1-1) a vertical line, or one exactly perpendicular to the first, is drawn through the external auditory meatus. At the top of head this line—the auriculo-bregmatic line (A A)—indicates the bregma or true vertex, which important landmark is to be marked with carmine or aniline upon the scalp. Upon the top of the head an imaginary horizontal line (4-4), parallel with the alveolo-condyloid plane, is projected, and upon it we measure backward a distance of 50 mm. (2 inches), and then draw a second vertical line (B B). At the point where this line reaches the convexity of the head is the Rolandic point (R), under which, [p. 94] in average heads, lie the upper or posterior extremity of the fissure of Rolando, the upper ends of the pre- and postcentral gyri, and within the longitudinal fissure the paracentral lobe, which together constitute the cortical centre for the leg of the opposite side. The Rolandic point, thus determined, should be distinctly marked upon the shaven scalp.
A third horizontal line is next to be drawn from the external angular process of the frontal bone backward, parallel with Broca's plane. This line (2-2), which may be termed the fronto-lambdoid because its posterior extremity usually passes at or near the upper angle of the lambdoidal suture, serves for the determination of several important parts. In the first place, the line (2-2) passes at about 5 mm. above the upper border of the squamous suture, or through it, and under this line, mostly [p. 95] parallel to it, are the anterior two-thirds of the fissure of Sylvius. Secondly, at about 5 mm. above and behind the intersection of lines (A A) and (2-2) is the inferior extremity of the fissure of Rolando, bounded by the pre- and postcentral gyri. In the third place, upon this line (2-2), at a distance of 18 or 25 mm. behind the external angular process, is the folded part of the base of the third frontal gyrus or Broca's speech-centre (F 3).
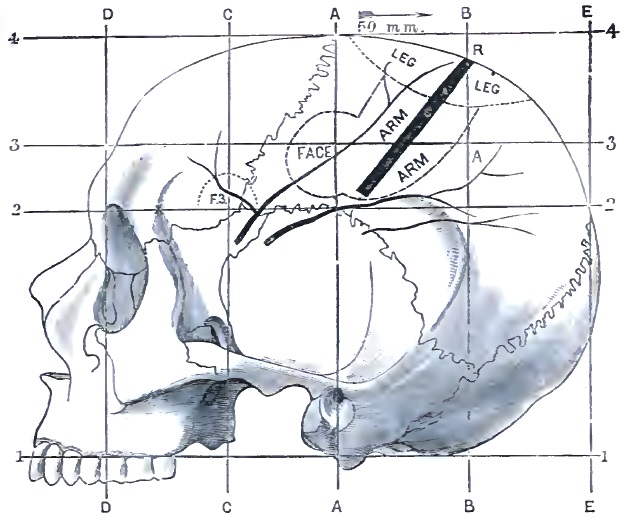
Having exactly determined and marked the situation of the Rolandic point and of the inferior termination of the fissure of Rolando above the ear, these two points are to be connected by a line, which is represented on the diagram by a black bar. This, the Rolandic line, is the guide for nearly all operations for the relief of spasm or paralysis of traumatic origin, or of such as may be caused by tumors, abscesses, etc. It is surrounded by the so-called motor centres for the face, arm, and leg (?) as demonstrated by experiments upon animals and by now numerous autopsies in human cases of injury and disease.
Other relations of interest are the apex of the temporal lobe, a little beneath the line (2-2) and at about 10 to 15 mm. posterior to the external angular process of the frontal bone; the situation of the occipito-parietal fissure, almost immediately under the posterior end of the line (2-2) at its junction with the lines (E E), which indicate the posterior extremity of the cerebrum; the anterior end of the brain being marked off by the line (D D).
[p. 96]Furthermore, for certain purposes the limits of the basal or central ganglia may be estimated as follows: Their superior limit is indicated by a horizontal line (3-3) drawn at 45 mm. below the vertex, their anterior limit corresponding to the head of the nucleus caudatus by the vertical line (C C), and their posterior limit, the hinder end of the thalamus, by the vertical line (B B).
Upon the median line at the top of the head an allowance of full 15 mm. should be made for the width of the superior longitudinal sinus separating the hemisphere.
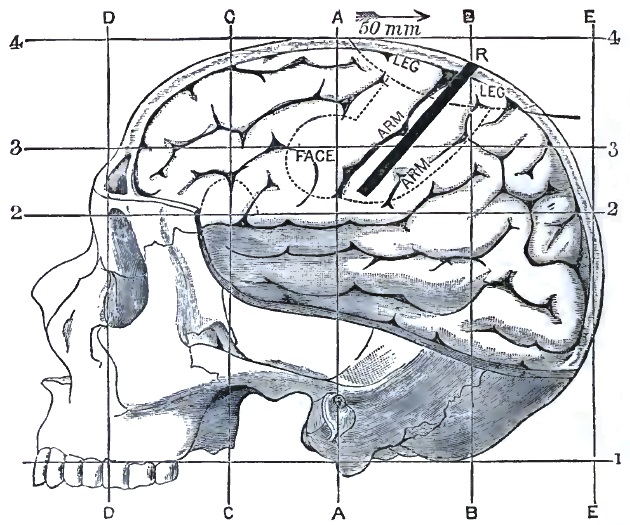
The location of the middle meningeal artery, which so often furnishes the blood that compresses the brain after various injuries to the head, is surgically of great importance. The course of its two principal branches is approximately indicated upon Fig. 13 by the branching lines drawn on the anterior inferior angle of the parietal and the upper part of the squamous portion of the temporal bone. In the living subject the main trunk of the artery would be found under the horizontal line (2-2) a little posterior to the speech-centre, about 30 mm. behind the external angular process, and in front of the beginning of the fissure of Sylvius.
Upon the shaven head of a patient seated in a chair or lying in bed the principal landmarks and relations above defined can be mapped out with sufficient approximation to accuracy by the use of a ruler to mark [p. 97] the alveolo-condyloid plane, and a cardboard cut so as to stand astride the head in the auriculo-bregmatic vertical. A light wooden apparatus can easily be made to indicate these two lines, while the remaining measurements can be made with a steel tape-measure, and the points marked with carmine ink or an aniline pencil.
The value of cranio-cerebral topography is obvious for ordinary surgical purposes, but it may in the future prove of great utility in the treatment of cerebral diseases (tumors, abscesses, etc.) by surgical means. A bold and nearly successful attempt at removing a tumor of the brain has already been made,15 and doubtless there are surgeons who will not hesitate to follow the path thus opened up when physicians give them a diagnosis of localized tumor or abscess in parts of the cortex cerebri to serve as a basis.
15 Bennett and Godlee, The Lancet, 1884, ii. 1090; 1885, i. p. 891.
The indications for trephining or raising bone after cranial injuries, for the relief of symptoms of cerebral irritation, compression, or disorganization, may be provisionally stated as follows:
(a) When aphasia supervenes immediately or within a few days or weeks after an injury of the anterior portion of the head on the left side. It is extremely probable that in the first case a clot or bony spiculum will be found compressing the speech-centre; in the second case, that an abscess has formed in or near it (Broca's case).
(b) When simple hemiplegia or hemiplegia with hemispasm follows an injury, however slight, in the temporo-parietal region. If the paralysis or spasm be limited to one side of the face or to one extremity, the indication to operate is even stronger. Even if in such cases the injury be not immediately over the motor area, the surgeon is justified in exploring that region.
(c) In conditions of stupor and coma after cranial injuries, sometimes without external wound, in which meningeal hemorrhage is the cause of impending death, the discovery of slight hemiplegia should justify trephining planned according to the topographic rules above laid down (Weir's case, 1882). In some cases latent hemiplegia may be discovered by the presence of an erythematous flush on one buttock and of a slightly increased peripheral temperature (taken between fingers or toes).
(d) In the very rare cases in which paralytic phenomena are found on the same side as the evident cranial injury, it would be proper to trephine on the opposite side of the skull in search of fracture or hemorrhage, the result of contre-coup.
(e) In chronic epilepsy after traumatism of the head the indication for trephining is present, but it is seldom a specific indication connected with the subject of localization. Lesions of any part of the skull and dura may be a cause of epileptic attacks, irrespective of motor centres.
(f) In cases of tumor in the motor centres, if there be not symptoms of tumors in other parts of the brain (multiple tumors) or of penetration of the tumor to the central parts of the brain, we believe trephining not only justified, but demanded in the present state of science.
Some of the contraindications to trephining may be thus stated:
(a) Whenever in apparently favorable cases there are signs of injury to the base of the brain, such as paralysis of cranial nerves, [p. 98] neuro-retinitis, and Cheyne-Stokes respiration (although the last symptom may occur from simple compression).
(b) When hemispasm or hemiplegia is accompanied by hemianæsthesia, thus making it probable that the lesion is deeper and farther back.
It should be added, in conclusion, that these indications and contraindications are formulated from the standpoint of the neurologist.
DEFINITIONS OF INSANITY.—The term insanity conveys quite different meanings to the community, to lawyers, and to physicians. From the three points of view its definition has been constantly widening for the past century. A great part of the alleged recent increase in insanity is due to the fact that its definition is applied to more people. Our insane asylums are more quiet and orderly, not only because of the more humane treatment of the inmates, but largely also because quieter and less insane people are now sent there than formerly. Doubtless the mistake is sometimes made of going so far, in zeal for science and philanthropy, as to make the definition of insanity too broad; and in a refined civilization the nice adjustment of complicated social relations, or even a fastidious taste, requires people to be sent to insane asylums who in simpler states of society would be cared for at home.1
1 The physician in general practice is referred to Clouston's Clinical Lectures on Mental Diseases, and to Part 1 of Spitzka's Manual of Insanity. For those who wish to study insanity thoroughly the literature is rich and its bibliography is readily available. Of many parts of the subject only an outline, of course, can be given within the limits of the present paper.
The popular idea of insanity is of wild, incoherent, or crazy conduct. If maniacal, the timid or frightened young girl who would not hurt a fly, and the tottering, harmless old man if confused and partly demented, are hurried off to the asylum with the use and show of force suitable for a desperate criminal, while the victim of overwhelming delusions, because he seems clear, logical, and collected, is vigorously defended against the physician's imputation of insanity until he commits an offence against the laws, when he is fortunate if he is not treated as a criminal. It is often impossible for judges, juries, counsel, and even medical experts, to wholly divest themselves of the popular notions of insanity in cases appealing strongly to the passion or prejudice of the day. Cases involving the question of responsibility for crime are decided against science and the evidence because of certain preconceived notions upon insanity which no amount of skilled opinion can controvert. Jurors, and less often judges, make up their minds what a sane man would do under given conditions, and of what an insane man is capable, judging from the facts within their own experience; and in forming their decisions it is the act itself, and not the man, diseased or otherwise, in connection with the act, that chiefly governs them. Often they are right, not seldom wrong. Strange, apparently purposeless, illogical, inconsistent action is frequently attributed to the author of it being insane on that subject, whereas he may be [p. 100] simply acting from strong impulse or emotion, and may be by no means insane. On the other hand, because a man knows right from wrong in the abstract, and can ordinarily behave well, the very characteristic workings of his insane mind are often seized upon as unquestionable proof of sanity, even when they admit of no other explanation to the skilled physician than that of insanity. There is no doubt of the fact that the whipping commonly used in the treatment of the insane by the monks several centuries ago put an end to much insane conduct; and in insane asylums now, in spite of the best efforts of the medical staff to the contrary, a brutal, bullying patient is sometimes struck by another patient or an attendant in return for some unusually exasperating and cruel conduct, with the result of making him behave well in the future. It is with reference to this class of cases that the crowd oftenest errs in its definition of insanity. Society claims a voice in the enforcement of the laws for its own protection, assuming to know who could control themselves from crime and who not, and naturally wishes the standard of responsibility to be kept high. Of course its sympathies and prejudices largely govern its voice in the matter.
With precisely the same degree of insanity and the same power to control their actions two murderers may be sentenced, one to death for an act where the motive and method were those of the criminal, and the other to an insane asylum for killing a person under circumstances which are not explainable by sane reasons. The Pocasset Adventist who sacrificed his loved child, as he thought, by the Lord's command, would probably have been hanged if he had committed a crime similar to John Brown's, Wilkes Booth's, Orsini's, or Guiteau's. Sometimes the accused gets the benefit of the doubt, and sometimes society, according to the view of the merits of the case taken by the judge in his charge or by the jury in their verdict.
To the lawyer insanity means only a condition of mind with reference to certain conduct. An insane man is simply non compos mentis. Insanity is irresponsibility. The whole question to the lawyer is with regard to a certain act or series of acts. The lawyer's definition is narrower than that of the physician. In wills and contracts the course is usually clearer than when there is a question of serious crime, and even an insane person in an asylum may be a party to a valid contract or make a will that will hold in law. It is not necessary that a will or contract be such as would be made by a just man or a reasonable man, but simply that it fairly represent the wishes and character of the man making it, uninfluenced by any insane delusion or prejudice caused by mental impairment; that the will or contract in itself bear evidence of a correct appreciation of the circumstances and conditions of the case; and that the mind be able to act independently enough, with a reasonable knowledge of the duties of the individual and the just rights of others. An unsound mind, as defined by the physician, would cover a large portion of the convicts in our workhouses and prisons to-day if they could be critically examined, but the lawyers and courts would not find many of them insane. A man is not insane in law unless his act is traceable to, or its nature has been determined by, mental disease affecting his free agency; in other words, unless insanity caused his act either wholly or in great part.
[p. 101]In the partly irresponsible condition of mind often produced by grave hysteria, so-called nervous prostration, and the general mental and moral demoralization often seen in seduced and abandoned women, or after exhausting illness, or following apparent recovery from cerebral hemorrhages or embolism, blows upon the head, sunstroke, chronic alcoholism, syphilis, etc., there may be loss of self-control and a distinct moral perversion or decided change of character without very evident mental impairment; and the courts recognize a diminished capacity, as the result of disease, to appreciate and follow what is right and just and to avoid what is wrong or unjust, and yet not complete irresponsibility. In this connection the fact should be borne in mind that a very little mental disease can make bad people criminals, and may not take others beyond the bounds of propriety. A criminal may become insane and be still pretty much the same kind of a criminal as before. Morality, too, is relative, and many criminals, like children, know almost nothing of abstract truth, justice, or virtue, because they have never been taught them; and there are many cases where the perverse or criminal actions of people may be about equally explainable on the theory of insanity or wickedness. The criminal, a creature of his surroundings and associations, may often not be discriminated from the man with mental disease. Indeed, it is not difficult to take the philanthropic position that all criminals are insane because they are not in sympathy with the moral conceptions of their time, or, to use the fashionable expression of the day, because they are not in harmony with their environment. Such a view of crime, however, leads to only one of two conclusions—either that insanity is no sufficient defence for wilful violation of the laws, or that all criminals should be treated as persons of unsound mind.
The free agency of the individual is affected or modified in many different ways by the different diseases of the mind, and the question of responsibility will often be found to be one of the most perplexing problems with which the physician has to deal. If well-marked forms of insanity alone were to be investigated, the matter would be comparatively a simple one; but such is far from always being the case. The insane man often commits certain crimes precisely as an ordinary sane criminal would do the same thing. Often the evidence is contradictory, the testimony as to previous life and character conflicting, and the disease of so obscure a stage or type that it is almost impossible to form a clear opinion. The determination of a man's degree of free agency is no simple affair which can be decided in all cases by a few or a few dozen interviews. Not seldom the mystery remains unsolved after the autopsy. Man's free will is not the property of any substance which can be demonstrated by chemistry, physiology, or microscopical research, but it is the result of the combined action of a whole group of functional activities the very relations of which to each other are as unknown as their method of action. No stethoscope or ophthalmoscope can reveal its morbid action, which can only be inferred indirectly from the operations of the mind.
The cases in which the physician is called upon to define insanity as the term is used by the lawyers are (1) to secure limitation or control of an individual's actions, usually by a guardianship; (2) to control him absolutely in an asylum; (3) to estimate his culpability or criminality, or [p. 102] his capacity to make a will or contract or to transact business. It is quite important, therefore, that the medical man should understand that there may be, as regards some particular person, a wide difference between medical insanity or mental disease and legal insanity or irresponsibility. He does most wisely when he confines his testimony to an explanation of the changes caused by disease in the particular case, and to the effect of such changes upon the mind, leaving to the judge's charge and the jury's verdict the questions of guilt and responsibility.
Insanity may be of congenital origin or slowly developed from early childhood, but usually it indicates a change caused by disease, so that the person alleged to be insane must, as a rule, be compared with himself at some previous time, and not with some ideal standard of mental health which does not exist. Indeed, if we could measure nicely no two of us could be fairly held to precisely the same degree of accountability. The knowledge of right and wrong is not a fair criterion, as many insane men possess that knowledge well enough in the abstract. The ability to distinguish right from wrong in the particular act is possessed by some insane persons whose will and power of self-control have become so limited by disease that they cannot avoid what they know to be crime. Delusion overpowering the mind is sufficient evidence of irresponsibility, but all delusions are by no means so powerful that they cannot be resisted, and many must be classed as simply false beliefs or mistaken views which could be, and should be, controlled. In case, therefore, of alleged delusions not manifestly insane further evidence of insanity is required, and the way in which a man believes or does anything may be more of an indication as to the soundness or unsoundness of his mind than what he believes or does. A crime committed under the influence of maniacal delirium, acute delirious mania, epileptic furor, uncontrollable impulse, alcoholic insanity, or hysterical mental disease will usually explain itself, while a demented insane person is so characteristic an object that his crime cannot well be mistaken for that of a responsible agent.
The different conditions of mind grouped under the general terms moral insanity, affective insanity, and impulsive insanity are still the bugbear of jurists, and there is a wide difference of opinion as to the degree of accountability for actions performed under the influence of moral perversion with only slight intellectual impairment; but the degree to which the individual deviates from the path of the law may depend more upon his training and surroundings than upon his disease—points which must always be considered in establishing a definition of insanity in obscure cases. Of two persons whose circumstances in life, in connection with a certain amount of disease, have produced as nearly as possible identical morbid mental states, it now and then happens that the necessary surroundings of the one steady and support him, while the associations and conditions of life throw the other still more off his balance. The one is able to sustain the ordinary relations with the world, the other not.
The intelligent study of mental disease by medical men has resulted in its being detected at so early a stage and in such a mild form that its proper treatment might almost be called, when successful, the prevention of insanity. Cerebro-mental disease, though it be only in its incipient form, implies to the physician the necessity for medical treatment; but it [p. 103] is another question whether the disease is sufficient in amount to impair the power of self-control and will so as to determine irresponsibility. It is not the doctor's province to punish for crime, but to treat for disease, and he often forgets that fact. The various medical definitions of insanity in textbooks and on the witness-stand do not clearly enough state how far the medical and how far the forensic meaning of the word is implied. What seem to be wide differences of opinion regarding responsibility for crime, as given in the courts, are often due to different ways of stating the question, and nothing more.
Boileau said that all men are insane, the only difference between them being the varying degrees of skill with which they are able to conceal the crack; and Montesquieu, that insane asylums are built in order that the outside world may believe itself sane. In 1832, Haslam, one of the first experts in mental disease in England at that time, testified in court that he had never seen a sane man in his whole life, adding, “I presume the Deity is of sound mind, and He alone.”
It is impossible to give a satisfactory definition of insanity, to draw any hard and fast line on one side of which we should put all the sane, and on the other all the insane. It is not possible to divide insanity from sanity by a single criterion, such as the existence of delusions, inasmuch as many sane people have very curious delusions; for instance, Sir William Blackstone's belief in witchcraft, as stated in his Commentaries on the Laws of England; Martin Luther's assertion that he saw the devil and threw an inkstand at him at a time when a belief in a personal devil was required by the canons of the Church of England; Napoleon's faith in his star; the common belief of the French generals that Joan of Arc's hallucinations were divine messages. Insane delusions have been defined as false beliefs, impossible from the nature of things or the circumstances of the case, according to general belief. One can only judge of each case and each person by the conditions attending them. A belief consistent with one person's whole life and character might indicate such a change in another as to be a mark of insanity.
Hallucinations—"psycho-sensorial disturbances characterized by sensations perceived when the exercise of the sense has not been determined by any external excitation”—are characteristic of many conditions of disturbed health besides insanity; and the same is true of illusions—erroneous interpretations of sensations actually perceived. In both cases the existence of insanity is determined by the fact whether or not the erroneous impressions are corrected by the judgment. An important point is to consider most carefully every unnatural, strange, or unexplained action, whether deliberate or from impulse, particularly in the large class of eccentric, ill-balanced, or weak-minded persons on the border-line between sanity and insanity. There are people who at one time seem to belong to the sane and at another to the insane class. Baillarger states that the essential element of insanity is loss of free will. Ball of Paris describes an insane man as one who, in consequence of a profound disturbance of the intellectual faculties, has lost more or less completely his free will (liberté morale), and has ceased thereby to be responsible to society for his actions.
Bucknill describes insanity, in his Sugden prize essay, as “a condition of the mind in which a false action of conception or judgment, a [p. 104] defective power of the will, or an uncontrollable violence of the emotions and instincts has been separately or conjointly produced by disease.” Maudsley's definition is, “Insanity is, in fact, disorder of brain producing disorder of mind; or, to define its nature in greater detail, it is a disorder of the supreme nerve-centres of the brain—the special organs of mind—producing derangement of thought, feeling, and action, together or separately, of such degree or kind as to incapacitate the individual for the relations of life.... Mind may be defined physiologically as a general term denoting the sum-total of those functions of the brain which are known as thought, feeling, and will. By disorder of the mind is meant disorder of those functions.”
Bucknill considers insanity a disease of the brain affecting the integrity of the mind. Maudsley calls it a disorder of the mind of such a degree as to incapacitate one for the ordinary relations of life, implying that there may be certain deviations from the condition of sound mind which do not constitute insanity. Tuke's definition is that “insanity consists in morbid conditions of the brain, the result of defective formation or altered nutrition of its substance, induced by local or general morbid processes, and characterized especially by non-development, obliteration, impairment, or perversion of one or more of its psychical functions.” Instead of itself being a disease, insanity, properly speaking, is a symptom of diseases which under varying manifestations probably affect different functions of the brain—at least they affect the brain in different ways.
As Krafft-Ebing says, “It is a logical, self-evident proposition that the organ whose function under normal conditions is to bring about all mental processes must be the seat of changes when these functions are disturbed;” and Schüle adds, “The study of disturbances of the mind involves the changes of the normal mental functions produced by disease.... Mental diseases are brain diseases, but they are more than that.” The normal action of the mind is a strange combination of reason and impulse, varying greatly in different persons, and in the same person at different times and under varying influences. The relations of the one to the other, and their influence on action, often change, under varying conditions and circumstances, in sane persons, but still more in the insane.
Lord Bramwell once said that insanity is strong but not conclusive evidence of innocence; and Lord Blackburn has stated that the jury must decide in each individual case whether the disease of the mind or the criminal will was the cause of the crime. The position of Sir James Stephen in his History of the Criminal Law in England best states the most recent views of irresponsibility—namely, that “no act is a crime if the person who does it is, at the time when it is done, prevented either by defective mental power or by any disease affecting his mind from controlling his own conduct, unless the loss of the power of control has been produced by his own default.” He says that a man laboring under such a defect of reason that he does not know that he is doing what is wrong may be defined as one deprived, by disease affecting the mind, of the power of passing a rational judgment on the moral character of the act which he meant to do. There are persons too insane to make a valid will by virtue of a single delusion, whose right to vote, under the law prohibiting the insane from voting, would not be questioned. Another [p. 105] might not be held responsible for crime, and still make a contract involving the rights of others besides himself that would hold in law.
Bucknill's recent medico-legal definition of insanity is, incapacitating weakness or derangement of mind produced by disease; meaning, in criminal cases, inability of abstaining from the criminal act, which would be expressed by Lord Bramwell's test, Could he help it? Bucknill suggests as an amendment to the law of England that no act is a crime if the person who does it is at the time incapable of not doing it by reason of idiocy or of disease affecting the mind.
Any definition of insanity would be incomplete without the statement of Hughlings Jackson's view, that disease only produces negative mental symptoms answering to dissolution, and that all elaborate positive mental symptoms (illusions, hallucinations, delusions, and extravagant conduct) are the outcome of activity of nervous elements untouched by any pathological process; that they arise during activity on the lower level of evolution remaining; that the insane man's illusions, etc. are not caused by disease, but that they are the outcome of activity of what is left of him (of what disease has spared), of all there then is of him. His illusions, etc. are his mind.
THE CLASSIFICATION OF MENTAL DISEASES.—There is no universally accepted classification of mental diseases, and the same terms even are used by different writers to convey entirely different meanings. The classification according to the causes of insanity was suggested by Morel of Paris, and fully elaborated by Skae of Edinburgh, as follows: (1) Moral idiocy; (2) intellectual idiocy; (3) moral imbecility; (4) intellectual imbecility; (5) epileptic insanity; (6) insanity of masturbation; (7) insanity of pubescence; (8) hysterical mania; (9) amenorrhœal mania; (10) post-connubial mania; (11) puerperal mania; (12) mania of pregnancy; (13) mania of lactation; (14) climacteric mania; (15) ovario- and uteromania; (16) senile mania; (17) phthisical mania; (18) metastatic mania; (19) traumatic mania; (20) syphilitic mania; (21) delirium tremens; (22) dipsomania; (23) mania of alcoholism; (24) post-febrile mania; (25) mania of oxaluria and phosphaturia; (26) general paralysis; (27) epidemic mania; (28) idiopathic sthenic mania; (29) idiopathic asthenic mania.
In a large proportion of cases the causes of insanity are so many and so complex that it is not within human power to say which of a number has been the most important, or the assigned and classified cause may be only an accidental complication or the most striking, but by no means most potent, cause.
The classification, according to the functions interfered with, is that adopted by Maudsley and by Bucknill. According to Bucknill, we have
(1) Insanity of the intellect or ideas: Idiocy, imbecility, dementia, delusional insanity, monomania, mania.
(2) Insanity of the feelings and the moral sentiments: Moral imbecility, moral insanity, melancholia, religious insanity, hypochondriacal insanity, nostalgic hypochondriacal insanity, exaltation regarding religion, pride, vanity, ambition.
(3) Insanity of the propensities, instincts, or desires: Mania, homicidal mania, suicidal mania, erotomania, dipsomania.
Maudsley's classification, according to the faculties thought to be affected, [p. 106] is also inconsistent: I. Affective insanity: (1) Simple mania; (2) simple melancholia; (3) moral insanity. II. Ideational insanity: (1) General (acute and chronic mania and melancholia); (2) partial (monomania and melancholia); (3) dementia (primary and secondary); (4) general paralysis; (5) idiocy and imbecility.
The classification according to symptoms is most generally adopted, being used, more or less modified, in Germany, generally in France, and more commonly than any other in this country and in England. It has been suggested by different writers in a dozen different forms, differing only in details. Griesinger's is as follows:
(1) States of mental depression: Hypochondriasis; simple melancholia; melancholia with stupor; melancholia with destructive tendencies; melancholia with persistent excitement of the will or impulse (moral insanity).
(2) States of mental exaltation: Mania; monomania.
(3) States of mental weakness: Chronic mania; dementia; idiocy; cretinism.
As important complications of insanity he places general paralysis of the insane and epilepsy, and various disorders of sensation and movement, such as convulsive gait, general cramps, choreic movements, hyperæsthesia of the skin, etc.
A classification according to the morbid condition of the brain has thus far proved unsuccessful. Up to the present time this remains largely a field of speculation, and even with the immense progress of the past dozen years it is a subject upon which there is now little definite to be said. Voisin's system is purely visionary—namely: I. Idiopathic insanity, due to vascular spasm. II. Insanity dependent on brain lesions: Congestive insanity; insanity from anæmia; atheromatous insanity; insanity from brain tumors. III. Insanity from alterations of the blood: Diathetic insanities; syphilitic insanity.
In basing his nomenclature on the clinical history of the various forms of insanity, Clouston makes his classification as follows:
(1) States of mental depression (melancholia, psychalgia): (a) Simple melancholia; (b) hypochondriacal melancholia; (c) delusional melancholia; (d) excited melancholia; (e) suicidal and homicidal melancholia.
(2) States of mental exaltation (mania, psychlampsia): (a) Simple mania (folie raisonnante); (b) acute mania; (c) delusional mania; (d) chronic mania.
(3) States of regularly alternating depression and exaltation (folie circulaire, psychorhythm, folie à double forme, circular insanity, periodic mania, recurrent mania).
(4) States of fixed and limited delusion (monomania, monopsychosis): (a) Monomania of pride and grandeur; (b) monomania of unseen agency; (c) monomania of suspicion.
(5) States of mental enfeeblement (dementia, amentia, psychoparesis, congenital imbecility, idiocy): (a) Secondary (ordinary) dementia (following acute or subacute disease, ending in chronicity); (b) primary enfeeblement (imbecility, idiocy, cretinism), the result of deficient brain development or of brain disease in very early life; (c) senile dementia; (d) organic dementia (the result of organic brain disease).
(6) States of mental stupor (stupor, psychocoma): (a) Melancholic [p. 107] stupor (melancholia attonita); (b) anergic stupor (primary dementia, dementia attonita); (c) secondary stupor (transitory, after acute mania).
(7) States of defective inhibition (psychokinesia, hyperkinesia, impulsive insanity, volitional insanity, uncontrollable impulse, insanity without delusion): (a) Homicidal impulse; (b) suicidal impulse; (c) epileptiform impulse; (d) animal impulse; (e) dipsomania; (f) pyromania; (g) kleptomania; (h) moral insanity.
(8) The insane diathesis (psychoneurosis, neurosis insana, neurosis spasmodica).
Some of the German mental pathologists have endeavored to combine in their classification the clinical history with the little that is known of its morbid anatomy. Meynert has gone so far in this direction as to have constructed an ideal mental pathology belonging to the sphere of brilliant speculation rather than exact science. Schüle has well summarized our knowledge on these points, as follows:
I. States of mental defect or degeneration. (1) States of mental defect: (a) Microcephalism; (b) idiocy. (2) States of mental degeneracy, chiefly as the result or further development of (a) Hereditary insanity, impulsive insanity, moral insanity; (b) insanity from the severe neuroses, epileptic insanity, hysterical insanity, hypochondriacal insanity; (c) periodic and circular insanity.
II. Insanity in persons of full mental and physical development:
(A) The cerebral neuroses causing mental disease, affecting primarily the mind alone (psychoneuroses): (1) The acute or subacute typical cerebral neuroses in healthy neurotic persons and with a vaso-motor origin: (a) Primary form, melancholia, melancholia agitata, simple mania; (b) secondary form, chronic mania and monomania, dementia. (2) The chronic cerebral neuroses giving rise to mental disease founded on degeneration and of neurotic origin primarily (delusional insanity): (a) Primary monomania of persecution, with a condition of pure mental depression or with exaggerated and exalted ideas; (b) delusional insanity, strictly speaking, psycho-convulsive form (maladie du doute), psycho-cataleptic form (delusional insanity attended with anomalies of sensation).
(B) The organic mental diseases affecting the psychic functions (cerebro-psychoses), differing from (A) chiefly in being deeper-seated: (1) With motor symptoms of excitement (acute mania): (a) Mania furiosa (including mania transitoria); (b) mania gravis; (c) acute delirious mania. (2) With motor neuroses and symptoms resembling catalepsy, tetanus, and anergic stupor, or the various forms of Spannungsneurosen: (a) Melancholia attonita; (b) delusional stupor; (c) primary dementia (stupor), acute and chronic. (3) With progressive paralysis, the typical form of paralytic dementia.
(C) The distinct lesions of the brain, giving rise secondarily to psychical disturbances. The modified paralyses or cerebral diseases in which dementia and paralysis are both observed clinically: (a) Meningo-periencephalitis, chronic and subacute; (b) pachymeningitis and hæmatoma; (c) diffuse encephalitis with sclerosis, without mental excitement and with mental excitement; (d) diffuse encephalitis with local softening, apoplexy, capillary aneurisms in groups or singly, multiple sclerosis; (e) diffuse encephalitis arising from foreign growths in the brain; (f) chronic [p. 108] periencephalitis, with previous tabes dorsalis; tabic paralysis: (g) primary atrophy of the brain, with accompanying spinal tabes, tabic dementia; (h) syphilitic encephalitis, with disturbances of the mind.
Krafft-Ebing's classification is as follows:
A. Mental Diseases of the Normal Brain.—I. Psychoneuroses: 1. Primary, curable diseases: a, Melancholia—_α, Simple melancholia; β, melancholia with stupor; b, Mania—α, Maniacal exaltation; β, acute mania; c, Stupidity (primary dementia) or curable dementia; d, confusional insanity (Wahnsinn). 2. Secondary, incurable diseases: a, Chronic delusional insanity; b, terminal dementia—α, with agitation; β, with apathy.
II. Conditions of Mental Degeneration.—a, Constitutional affective insanity (folie raisonnante); b, moral insanity; c, primary monomania—α, With delusions of persecution; β, with delusions of ambition; d, with imperative conceptions; e, insanity from constitutional neuroses—α, epileptic; β, hysterical; γ, hypochondriacal; f, periodic insanity (folie circulaire).
III. Diseases of the Brain with Mental Disturbances Predominating.—a, Paralytic dementia; b, cerebral syphilis; c, chronic alcoholism; d, senile dementia; e, acute delirium.
B. Conditions of Arrested Mental Development.—Idiocy and cretinism.
Krafft-Ebing agrees with Schüle in dividing mental diseases into two classes—those of a degenerative nature arising from the development of an hereditary or congenital neurotic tendency, or from injury, sexual or alcoholic excess, etc., and those which occur from what may be called accidental causes in otherwise healthy persons, in whom mental disease would not be anticipated, and from which the late Isaac Ray said that, with sufficient exciting cause, no one has any privilege of exemption. The essential distinction between them was pointed out by Moreau and Morel, and is best stated by Krafft-Ebing:
Degenerative insanity is a constitutional disease arising from slight exciting causes, even physiological conditions (puberty, menstruation, the puerperal state, climacterium), but for the most part from pathological conditions, chiefly hereditary predisposition, injury to the head, acute disease, etc., occurring during development of the sensitive brain, forming often the last in a series of neuropathic disorders, such as spinal irritation, hysteria, hypochondria, epilepsy. The tendency to recovery is slight, and generally there is only temporary return to the primary condition. Relapses and progressive development of graver forms of disease are common. There is progressive hereditary mental degeneration or a strong tendency to appear in descendants in progressively severer form. All forms of the psychoneuroses occur, but of severe type and irregular course, with sudden and rapid changes in the character of the disease, which does not follow any particular course and cannot be definitely classified, rarely ending in dementia, and often lasting in some form through life. The tendency to periodicity is strong. Delusions are chiefly physio-pathological as direct creations of the diseased brain, entirely without apparent cause, to the astonishment of the person and independent of his frame of mind at the time. They appear and disappear, to be replaced by morbid impulses or mental weakness. Delusions are strange, mysterious, monstrous, without possible explanation from the [p. 109] nature of the disease. There is, for the most part, an inseparable transition from pathological predisposition to actual disease, with a strange mixture of lucidity and diseased mental perversion. Acts are often from impulse. There are sudden outbursts or short attacks; as, for instance, in periodic, hysterical, and epileptic insanity.
In psychoneuroses developed in persons of previously normal brain-function heredity is only a latent predisposing cause. The tendency is to recovery; relapses are infrequent. They are not so readily transmitted to later generations. The disease follows the course of some well-defined type. There is not a tendency to periodicity. Delusions arise chiefly from psychological sources as the result of diseased mental conditions. They are usually not early symptoms, and in general they correspond with the prevailing state of the mind. Delusions correspond with the mental state. The change from health to disease is well defined.
These are the main features of the two classes of mental disease, but the line between them is not a hard and fast one, and it is not seldom impossible to place a particular diseased person definitely in the one or the other.
The objection to all of the classifications of insanity now in use, that they have not an accurate scientific basis, and that a diagnosis must often be delayed or changed as symptoms develop, applies, although in a less degree, to other diseases than of the mind.
HISTORY.—The history of insanity is probably as old as the human race, although its rarity among savage nations at the present day, and its greatest prevalence where there are the widest extremes of wealth and poverty, indicate that it is essentially a disease of the high civilizations. It is found even in the lower animals. It is described in the early writers on medicine from Hippocrates and Plato down. The ancient Egyptians had temples dedicated to Saturn, where they cared for the insane with music and dancing. The Greeks and Romans treated the sick, and probably some of the insane, in rooms adjoining their temples. The monks of Jerusalem built an asylum for the insane of their number in the sixth century. There were several asylums in existence among the Moors in the seventh century, and it is thought that at the time of their invasion of Spain they introduced them into Western Europe. The monks, who were the chief depositaries of medical knowledge in the Middle Ages, treated the insane, as they did to a less extent each other, by flagellations, until St. Vincent de Paul and the Knights of Malta proclaimed insanity a disease and treated it as such. It would be idle to estimate how many were put to the rack, burned, and otherwise maltreated as possessed of the devil or as witches—how many were called prophets or saints.
As late as the last quarter of the last century the insane, when not starving or neglected, were for the most part confined in jails and poorhouses or kept in chains. In Scotland a farmer reputed to be as large as Hercules was said to cure them by severity. In England the practice of exhibiting the inmates of Bethlehem Hospital (Bedlam) to the populace for a small fee was given up only in 1770. In Paris a few of the insane were treated in general hospitals, and the asylums were considered as receptacles for chronic cases, where the attendants, often convicts serving out their time, were allowed to whip them. Van Helmont recommended the sudden immersing of the insane into cold water and keeping them [p. 110] there for several moments—a remedy brought even to this country. Rush says, as late as 1812, that by the proper application of mild and terrifying modes of punishment (the strait waistcoat, the tranquillizer chair, privation of customary pleasant food, pouring water under the coat-sleeve so that it may descend into the armpits and down the trunk of the body, the shower-bath continued for fifteen or twenty minutes, and a resort to the fear of death) chains will seldom, and the whip never, be required to govern mad people. The intelligent ideas of the Egyptians, Greeks, and Romans regarding insanity were degraded first by the Jewish, and then by the Goth and Vandal, influences in Europe, until, after sixteen centuries of perverse teaching, the stimulus given to all medical work by John Hunter and Bichat, and to humanity by John Howard, prepared the way in France for the philosopher-physician Pinel and his pupil the clinical observer Esquirol. In Italy, Chiarruggi; in Germany, Langemann; in England, Tuke; in America, Rush,—began the reform. Up to that time the metaphysicians had nearly usurped the study of insanity. Hospitals for the treatment of curable mental disease were built in Germany besides the asylums for the chronic insane, but still sudden plunges in water, rapid whirling around, and all sorts of shocks and surprises formed a part of the treatment, while Heinroth, Pinel's leading pupil in Germany, thought that all insanity began in vice, that its source was a conscious neglect of God's will, that its best treatment consisted in a pious life, and the only means of prevention to be in the Christian religion. From that time to this, especially since the metaphysical theory of insanity was abandoned, and more particularly during the last quarter of this century, during which the theory of physical disease as the basis of insanity has prevailed, there has been a great and rapid advance in our knowledge of the pathology and treatment of the diseases of the mind, so as to place them beyond the pale of mystery, but on the same footing with other diseases, to be treated on the general principles of common sense and medical science.
PREVALENCE.—It would be idle to attempt to say what proportion of the population was insane at any time or in any country of the world until the most recent years. In Massachusetts in 1820 there were under custody in the one insane asylum in the State 50 patients, or 9.55 in each 100,000 of the population. This number had increased to 11.34 to every 100,000 people in 1830, 61.99 in 1840, 84.97 in 1850, 97.90 in 1855, 122.17 in 1860, 121.24 in 1865, 134.83 in 1870, 138.50 in 1875, and 177.67 in 1880, in six State, one county, one city, one corporate, and six private asylums. The number of the insane in asylums had increased sixty times, and the rate proportionately to the population had augmented more than eighteen times.
In the United States, even after due allowance for the fact that the enumeration of the insane was quite complete for the first time in 1880, the following table shows a recent large increase in their numbers. Of the 91,997 insane reported in 1880, there were 40,942 in lunatic hospitals, 9302 in almshouses without special departments for the insane, and 417 in jails. There are no statistics of the insanity prevalent among the 265,565 Indians living in tribal relations by the enumeration of 1883.
[p. 111]| Year. | Total. | Native. | Foreign. | White. | Colored. |
| 1860 | 31,443,321 | 27,304,624 | 4,138,697 | 26,922,537 | 4,441,830 |
| 1870 | 38,558,371 | 32,991,142 | 5,567,229 | 33,589,377 | 4,880,0092 |
| 1880 | 50,155,783 | 43,475,840 | 6,679,943 | 43,402,970 | 6,580,7933 |
| Insane. | |||||
| 1860 | 24,042 | 17,399 | 5,784 | 23,276 | 766 |
| 1870 | 37,432 | 26,205 | 11,227 | 35,610 | 1,774 |
| 1880 | 91,997 | 65,651 | 26,346 | 85,840 | 5,998 |
| Idiotic. | |||||
| 1860 | 18,930 | 17,685 | 1,125 | 16,952 | 1,978 |
| 1870 | 24,527 | 22,882 | 1,645 | 21,324 | 3,188 |
| 1880 | 76,895 | 72,888 | 4,007 | 67,316 | 9,4904 |
2 Unknown, 55.
3 Unknown, 148.
4 Unknown, 1.
| Total. | Native. | Foreign. | White. | Negro and Mixed. |
Native White. |
Foreign White. |
|
| Insane. | 91,997 | 65,651 | 26,346 | 85,840 | 5,998 | 59,600 | 26,240 |
| Idiotic. | 76,895 | 72,888 | 4,007 | 67,316 | 9,490 | 63,314 | 4,002 |
| Of unsound mind. | 168,892 | 138,539 | 30,353 | 153,156 | 15,488 | 122,914 | 30,242 |
| Population to 1 insane. | 545 | 662 | 253 | 505 | 1,097 | 618 | 250 |
| Population to 1 idiotic. | 652 | 596 | 1,666 | 644 | 693 | 581 | 1,642 |
| Population to 1 of unsound mind. | 297 | 314 | 220 | 283 | 425 | 299 | 217 |
5 Total population, 50,155,783; native, 43,475,840; foreign, 6,679,943; white, 43,402,970 (unknown, 148); negro and mixed, 6,580,793; native white, 36,828,640; foreign white, 6,574,330; civilized Indians, 66,407; Chinese, 105,465. Among the Indians there were 53 insane, 84 idiotic, 137, or 1 in 485, distributed over 30 States and Territories; among the Chinese, 105 insane, 5 idiotic, 110, or 1 in 959.
In England and Wales in 1860, with a population of 19,902,713, there were known to the lunacy commissioners 38,058 persons of unsound mind, including the insane, idiots, and imbeciles, or 523 persons to 1 of unsound mind. In 1870 this number had increased to 1 in 411. It seems by the census of 1871, however, that there were 39,567 insane and 29,452 idiots and imbeciles, in all 69,019 of unsound mind, or 1 in 330 of the population. In 1880, with a population of 25,708,666, there were known to the lunacy commissioners 71,191 persons of unsound mind, or 1 to 362 of the population. The census returns of 1881 are not available. The most recent statistics in Ireland indicate 1 person of unsound mind to each 260 of the population by the census, and in Scotland 1 in 362, according to the returns (not complete) to the lunacy commission.
In the following list, after the original States, of which Vermont, Maine, and West Virginia were parts later separated, the others are given in the order of their having been admitted as States to the Union, and finally the eight Territories. The States maintaining slavery up to the time of the civil war are printed in italics. The large proportion of insane persons in the District of Columbia is due to the fact that the [p. 112] government hospital contains so many officers and privates who really belong to the several States; and in California the insane hospitals have been used to a considerable extent by the adjoining States and Territories.
By the United States census of 1880 there was 1 person of unsound mind (insane and idiotic) in the United States to each 297 of the population; in the District of Columbia, 1 in 169; Connecticut, 1 in 245; Delaware, 313; Georgia, 373; Maryland, 294; Massachusetts, 249; New Hampshire, 197; New Jersey, 326; New York, 251; North Carolina, 270; Pennsylvania, 289; Rhode Island, 301; South Carolina, 368; Virginia, 290; Vermont, 182; Kentucky, 261; Tennessee, 259; Ohio, 232; Louisiana, 457, Indiana, 239; Mississippi, 415; Illinois, 330; Alabama, 337; Maine, 226; Missouri, 324; Arkansas, 371; Michigan, 328; Florida, 433; Texas, 414; Iowa, 334; Wisconsin, 305; California, 286; Minnesota, 416; Oregon, 312; Kansas, 478; West Virginia, 263; Nevada, 1270; Nebraska, 561; Colorado, 1104; Arizona, 1263; Dakota, 839; Idaho, 836; Montana, 529; New Mexico, 434; Utah, 481; Washington, 412; Wyoming, 3464.
The proportion of the enumerated insane in asylums was—District of Columbia, 90.6 per cent.; Connecticut, 39; Georgia, 36.8; Maryland, 49.1; Massachusetts, 60.1; New Hampshire, 27.1; New Jersey, 67.8; New York, 57.2; North Carolina, 13.2; Pennsylvania, 36.1; Rhode Island, 57.3; South Carolina, 38.2; Virginia, 45.5; Vermont, 44.7; Kentucky, 50.7; Tennessee, 16; Ohio, 48; Louisiana, 44.9; Indiana, 26; Mississippi, 33.7; Illinois, 42.7; Alabama, 24.5; Maine, 26.1; Missouri, 40.7; Michigan, 41.5; Florida, 30; Texas, 22.3; Iowa, 37.8; Wisconsin, 48.6; California, 80.3; Minnesota, 61.8; Oregon, 65.5; Kansas, 31.9; West Virginia, 40.1; Nebraska, 38; Colorado, 34.3. In Arkansas and in Nevada there was no insane asylum in 1880, and in Delaware the insane were sent to a Pennsylvania asylum or to the almshouse. In the Territories the provisions for the insane are very incomplete.
The statistics just given indicate an enormous increase in the numbers of the insane who become a public charge, and the figures gathered from all countries prove conclusively that more insane people are known to be in existence proportionately to the population from decade to decade. The question naturally arises, Is insanity increasing as fast as appears at first sight to be the case, or is the increase apparent rather than real?
In the first place, the definition of insanity has so widened of later years as to include vastly greater numbers of the population than hitherto. The nice adjustment of social relations in a high order of civilization and greater medical skill make insanity easier of detection. Large numbers of persons now confined would have been considered far from being fit subjects for insane asylums a half century ago. Again, it is hardly a generation ago that we began taking proper care of the insane. Some States have hardly commenced yet, and even in the oldest parts of our country many of unsound mind are kept neglected and squalid in town almshouses or county jails. Wherever humanity has demanded improved accommodations for the insane they have accumulated enormously, from the simple fact that they are protected like children, and kept from dying of neglect, suicide, and exhaustion. In other words, science and humanity have prolonged their lives of illness, in some cases to as much as tenfold their natural length if they had been left to themselves, even where nothing can be done but to prolong their misery. The [p. 113] more intelligent views now held of insanity as a physical disease rather than a family disgrace have led people to be less backward in reporting their insane relatives as such, while the increasing number of insane asylums and the growing confidence in them have brought many of the insane to notice who formerly would have been concealed in attics and cellars and never mentioned.
Whether or not more persons become insane each year in proportion to the population we have no methods of determining statistically. The mortality returns in Massachusetts for the last five census years show that the deaths from insanity, paralysis, apoplexy, softening of the brain, and unspecified diseases of the brain, including cephalitis, were 12.06 per 10,000 inhabitants in 1860, 14.39 in 1865, 14.95 in 1870, 16.42 in 1875, and 17 in 1880; which would probably indicate an increase, even after allowing for a considerable source of error due to inaccurate diagnoses, imperfect registration, and the influx of a large foreign population. It is claimed that the table on page 111 indicates a direct importation of insane persons from Europe. It is certainly a curious fact that the proportion of idiots and of the insane differs so little in the native population, and that among foreigners the idiots, who could not easily be sent here without being detected and sent back, are less than one-sixth of the number of their insane. But it is also true that the amount of insanity among strangers in a foreign land would naturally be greater than among those who are at home.
The prevalence of insanity as compared with other diseases at the present time may be fairly estimated from the statistics of Massachusetts for twenty years, where there were 604,677 deaths reported, including 2145 from suicide, 1995 from insanity, 1838 from delirium tremens and intemperance. The reported deaths from pulmonary consumption are fifty times as many as from insanity; from diarrhœal diseases, thirty times; from pneumonia, twenty times; from diphtheria, including croup, fifteen times; from scarlet fever, heart disease, and typhoid fever, each eleven times; from accidents, ten times; from cancer, five times; from childbirth and measles, each more than twice as many. The average death-rates reported from insanity per 100,000 inhabitants were 6.24 from 1861-70, and 7.12 from 1871-80, whereas the increase in the number of admissions to Massachusetts insane asylums in the twenty years was from 846 to 1610. The total number of insane people living in the State is less than the number of consumptives dying each year, and far less than the number of syphilitics.
CAUSATION.—It is clear that only a small proportion of the human race is liable to become insane, and one can only wonder that so few brains are overthrown by the multiplicity of causes in modern life which tend to disturb those “invisible thoroughfares of the mind which are the first lurking-places of anguish, mania, and crime.” When we come to investigate the causes of mental disease, we find that they are of two kinds—remote or predisposing and immediate or exciting. They are also moral or mental and physical.
Among the predisposing causes heredity includes nearly or quite 75 per cent. of all cases, and is easily first; in considering which not only the immediate parents are to be taken into account, but also the collateral branches, grandparents, uncles, aunts, sisters, brothers, and cousins, for [p. 114] hereditary insanity often skips one generation, and even appears, sometimes, first in the child, then later in the parent. An insane parent may have several children, of whom some may be exposed to the exciting causes of insanity and become insane, transmitting their disease, intensified or not, to their children, while others may avoid the exciting causes of mental disease, escape insanity, but yet transmit to their children a temperament predisposing them to disorder of the mind, which becomes the starting-point for actual mental disease as soon as the exciting causes are sufficient to develop the taint. If the exciting causes do not appear, however, in that generation, and wise marriages are made, the stock returns to the normal healthy standard and the disease disappears from the family. The same form of disease, too, is frequently not transmitted from parent to child or grandchild, but the neuroses, the psychoneuroses, and the cerebro-psychoses, the degenerative forms and the developed forms, are interchangeable. In the ancestry of insanity we find not only actual cerebro-mental disease, but epilepsy, brain disease due to syphilis, habitual drunkenness, any of the severe neuroses, apoplexy, pulmonary consumption, a closely-allied disease, and suicide. Very often the patient's friends think that there is no hereditary predisposition to mental disease, when the physician trained to study such cases would discover so strong a taint that he would not expect all of several children to escape insanity or some of its allied diseases even in a case where there had not been actual insanity in the family for several generations. For instance, where one parent is habitually using alcoholic liquors to such a degree as never to be drunk, and yet rarely quite himself, with the other a sufferer from one of the severe neuroses or cerebral diseases, a single child from such a marriage might stand a fair chance of inheriting and retaining mental health, but if several children should be born the chances that all would escape mental disorder are few. Again, if one parent were the victim of that intense intellectual strain and moral perversion so often seen in the eager pursuit of position and wealth, and the other, straining to keep up in the race, died early of pulmonary consumption, if there had been in the family cases of convulsions, chorea, apoplexy, or suicide, and if some member were hysterical or, without sufficient external cause, unreasonable, anxious, irritable, full of baseless fears, there might have been no insanity in the family, and yet a tendency to insanity might be transmitted to a considerable proportion of the offspring. On the other hand, the existence of a number of cases of insanity in a family may be due to external or accidental causes, and not indicate any general taint.
It is true that there are families in which insanity occurs where the allied neuroses do not often appear, and that various diseases of the nervous system may be frequent in a stock in which insanity is rare or absent. A person who has recovered from an acute attack of cerebro-mental disorder, if previously healthy and without hereditary predisposition to such diseases, may marry and not transmit to offspring either insanity or any of its allied diseases, while it is not uncommon for an individual seemingly the least liable to mental disease of a whole family to become insane, leaving several brothers and sisters with ill-balanced minds to get through life without breaking down, the morbid energy in the latter case expending itself in irregularities of conduct and of mental operations as fast as it is created, instead of being stored up for [p. 115] occasional outbreaks. The degree to which insanity may be expected to follow any given antecedents can only be estimated very approximately, as the laws of heredity are very little known, and as there is a tendency in nature, so strong that it is constantly asserting itself, to return to the healthy type if it has a chance. But, in general, it may be said that the more individuals of both branches in whom insanity and its allied diseases are found, just so far may a larger proportion of the children be expected to suffer. The character of the particular disease or tendency to disease which is likely to develop from any given antecedents is still a very obscure matter. But the case is often clear enough to justify the remark that if childhood has any rights it has the right to be born healthy.
It must be admitted that geniuses and men of extraordinary talent appear in families tainted with insanity, and, indeed, that comparatively few families have had distinguished men among them for several generations without also showing a considerable number of insane members. Schopenhauer, “mad Jack Byron's son,” and Johnson—who said that his inheritance made him mad all his life—are conspicuous examples of this well-known fact; and it is also observed that children and grandchildren of men distinguished for their great intellectual powers are subjects of degenerative mental disorders, or at least are of less than ordinary mental capacity and moral force. The sound and the unsound, too, may exist together in the same mind, each acting in certain ways independently of the other, and cerebro-mental disease not seldom, occurs in persons of the highest intellectual attainments. Dean Swift, with his delusion that parts of his body were made of glass; Bishop Butler, tormented all his life by his morbid fancies; Chatterton, committing suicide in an attic; Rousseau, Tasso, Pascal, Comte, Beethoven, Charles Lamb, John Bunyan, the author of Rab and His Friends, Schumann, Shelley, Cowper, Swedenborg, and the epileptics Julius Cæsar, Mohammed, and Napoleon,—are only a few of the many illustrations of this law. In the descending scale from insanity we find also crime, drunkenness, and all sorts of moral perversions, which may be its antecedents also. Even a man's self-indulgences may be intensified as mental or moral degeneration in his children. The degenerative processes may go on where there is intellectual stagnation in small communities, with the vices of civilization, as well as in the crowd, producing a large class of persons for whom doctors have only compassion, considering them as invalids although treated as responsible by law and society.
It is difficult to estimate the influence of intermarriage as predisposing to insanity. The history of the early Ptolemies, of numerous savage or uncivilized races, and of many selected cases in the enlightened world may be quoted to show that it is often attended with no evil results; and there are other causes of degeneration in the royal families and aristocracies of Europe and in the cases of individuals where intermarriage of relations has resulted in deterioration of stock. It is, at all events, certain that marriages may be made so as to intensify morbid tendencies or so as to eliminate them—to produce a race of clear heads with sober judgment, or a race part of whom shall be great sufferers from neuralgia or mental pain; another part ill-balanced or explorers in fields of thought and action never tried by calmer intellects, perhaps with now and then at [p. 116] long intervals a genius; a third part morbid and brilliant or stupid and imbecile; and still a fourth part near enough to the normal standard of mental health.
Undoubtedly, a great portion of the mental and nervous disorder commonly attributed to heredity is largely caused or aggravated by imitation and by vicious training of children. Schopenhauer says that the normal man is two-thirds will and one-third intellect—in other words, two-thirds made by education and one-third by inheritance. The intellect is often trained so as to enfeeble the will as well as to hinder the development of the physical man. Self-culture may so degenerate into self-indulgence as to destroy individuality and force; and mental health, as a rule, depends upon bodily health and the exercise of self-control.
In the uncivilized and half-civilized races of the world insanity is rare; in the early civilizations the insane perished from neglect, were hanged and burned, starved and died in famine and pestilence, and fell among the foremost in war. Some of the tribes of North American Indians shoot the insane, considering them possessed of evil spirits, while their white neighbors keep them in chains and squalor. Civilization brings better food, clothing, and shelter, and less danger from war, famine, and pestilence than savage or mediæval times. In the struggle for existence, however, physical strength no longer wholly wins the day, but also those faculties that involve great mental and bodily strain in mines, factories, crowded tenements, counting-rooms, offices; in the eager, excited over-study for prizes or rank in overheated, badly-ventilated schools, and, indeed, in every walk of life. People with marked neuroses, who would have gone to the wall a couple of centuries ago from want of physical strength, now support themselves by indoor light work, marry, and reproduce their kind. Minute division of labor involves monotonous toil and increases the impairment of the body's resistance to mental and nervous strain, and abuse of the nerve-stimulants tea, coffee, tobacco, or, worst of all, alcohol and narcotics, add to the evil. Degeneration due to the reproduction of poor stock is intensified by intermarriage. Luxury, idleness, excesses, syphilis, debility, drunkenness, poverty, disease, and overwork produce vitiated constitutions in which varying types of insanity appear in various nations and climates, but, so far as is known at present, not in very different degree under similar conditions. One of the great problems of the day is whether the many conditions incompatible with health in our crowded populations can be overcome so as to prevent the degeneration going on thereby.
In early life chiefly the degenerative or the hereditary type of insanity occurs, or some modification of it. The prevalent forms coming next are insanity of puberty and adolescence and the curious morbid psychological developments of lying, stealing, running away from home, all sorts of perversity of action and thought—impulse overpowering reason; often resulting in cure if wisely treated, but not seldom ending in various forms of so-called moral insanity, suicide, epilepsy, hysteria, primary insanity, prostitution, and offences against the laws. It is largely a matter of accident rather than a result of any established principle whether such boys and girls are sent to reformatories and prisons or to insane asylums. In the progressively advancing years of life organic [p. 117] mental disease and the psychoneuroses are more common, the favorable or unfavorable type of which depends largely upon the degree of degenerative tendency in each case.
The exhaustion and the disturbed cerebral circulation arising from acute and chronic diseases, profound anæmia, or prolonged mental strain, associated with emotional disturbance from any cause, are among the antecedents of insanity. By our asylum reports ill-health is second only to intemperance as an exciting cause of insanity, and ill-health comes probably more largely from poverty than from any other direct cause. Diseases and accidents to the mother during gestation and injuries to the infant's head during parturition may reasonably be supposed to so affect the fœtal brain as to predispose to insanity in later life.
Of 18,422 admissions tabulated from reports of Massachusetts asylums, the prevalence of insanity by ages was approximately as follows:
| Age. | Number of Admissions. |
Population by Census of 1875. |
Admissions per 100,000 of Population. |
| 15 and under | 366 | 312,1036 | 117 |
| 15 to 20 | 1,380 | 165,936 | 832 |
| 20 to 30 | 5,269 | 310,861 | 1695 |
| 30 to 40 | 4,632 | 240,966 | 1922 |
| 40 to 50 | 3,372 | 182,823 | 1789 |
| 50 to 60 | 1,797 | 126,430 | 1421 |
| 60 to 70 | 976 | 79,186 | 1106 |
| 70 to 80 | 382 | 38,283 | 997 |
| Over 80 | 58 | 11,167 | 519 |
| Age not reported | 190 | 10,302 | |
| Total | 18,422 | 1,478,0576 | 1246 |
| Total of all ages | —— | 1,651,912 | 1115 |
6 Excluding those under five years of age.
Of the 36,762 persons of unsound mind known to the English lunacy commission in 1859, there were 31,782 paupers, or 86.45 per cent., as compared with 4980, or 13.55 per cent., supported by themselves or their relatives. At the close of 1880, of 73,113 insane, 65,372, or 89.41 per cent., were paupers, and 7741, or 10.59 per cent., were private patients or self-supporting. The increase in the number of the latter from 1859 to 1883 was from 2.53 to 2.96 per 10,000 of the population, or 17 per cent., and of the pauper insane from 16.14 to 25.72, or 59 per cent., while general pauperism had rapidly diminished from 43.7 to 29.5 per 1000 inhabitants.
Similarly, of 9541 admissions to the State hospitals for the insane in Massachusetts from 1871 to 1880 inclusive, there were 4166 State patients, 4050 supported by cities and towns, and 1325 private patients; in other words, 86 per cent. were supported by public charity. Of 7963 admissions in the same time in which the nationality was stated, 4532 were natives and 3431 foreigners, respectively 57 and 43 per cent., whereas by the census of 1875 the natives were 74.64 per cent. of the population, showing more than twice as great a percentage among foreigners (chiefly laborers) as among natives. It is quite clear, therefore, that insanity is more prevalent, or at least increasing more rapidly, [p. 118] among the lower parts of the social scale than higher up; but it is impossible to say how many people have dropped from higher planes of life to lower.
Although women are probably more predisposed to insanity than men, and men more exposed to its objective causes than women, it is not certain that more insanity occurs in either sex. It is somewhat more prevalent in single and widowed and divorced people than in those married. The period of greatest prevalence is earlier in women than in men.
Insanity prevails not only at a time of life when the strain on mind and body is great, as is shown by the preceding table, but also in those places where the effort is most intense. That fact is well shown in the distribution of insanity over the State in the large and small towns, being greatest where the concentration of population brings with it extremes of poverty and wealth, as indicated by the following table, showing the number of admissions accredited to cities and towns in the McLean, South Boston, and State hospitals for the insane per 100,000 inhabitants from 1871 to 1880, the difference being exaggerated by the proximity of the hospitals and greater ease of commitment in the larger towns:
| Number of Towns. |
Population. | Inhabitants by Census of 1875. |
Insane Patients. |
Insane Patients per 100,000 Inhabitants. |
| 341 | The State | 1,651,912 | 5689 | 344 |
| 1 | Boston | 341,919 | 1987 | 581 |
| 12 | 20,000 to 50,000 | 405,655 | 1486 | 367 |
| 42 | 5000 to 20,000 | 367,957 | 1193 | 324 |
| 286 | 5000 and under | 536,381 | 1023 | 190 |
Of 9381 men and 9041 women admitted to our asylums, 7435 were married, 8193 single, and 1620 widowed or divorced. Of the 9381 males, 2215 were laborers, 1357 farmers, 313 clerks, 62 clergymen, 59 physicians, 43 lawyers, 201 students, of whom 114 were in school. Of 4673 females, 52 were school-girls.
The exciting or immediate causes of insanity are usually so complex that many of the statistics on that point conform to the preconceived views of the various compilers of them, as it is very easy to pick out a few from the many; but out of a large number of persons exposed to the alleged causes of insanity, one can never feel certain how many, nor indeed what, individuals will become insane.
It is not always easy to say how and when the furrows left in the brain by the mental and so-called moral causes of insanity have deepened into actual mental disease. Prolonged emotional and mental strain or severe mental shock often are directly associated with the immediate appearance of insanity. In armies, among people separated from their homes, in prisons, insanity oftener occurs than among the same people at home. Severe grief, disappointment, great and sudden joy or success, chagrin, fear, religious or political excitement, wars, pestilences, domestic or business troubles, poverty, and misfortune are among the commonly-reported moral causes of insanity, as are certain occupations involving steady and monotonous toil, especially if involving mental worry or necessitating unhappy relations.
[p. 119]Of the physical exciting causes of insanity, intemperance in the use of alcohol is easily first: luxury and excess in eating, drinking, and sexual indulgence, especially if associated with overwork or physical inactivity and mental anxiety, are also dangerous. It is difficult to estimate the influence of syphilis except when giving rise to coarse disease of the brain. Masturbation acts as an exciting cause, chiefly by creating a morbid psychical state and by exalting the sensibility of the nervous system, but probably not often, even with the young. Injuries to the brain and nervous system are usually slow in their operation, unlike the severe mental shock which is at once followed by insanity. Pain also, if intense, like great loss of blood, acts slowly by wearing out the powers of resistance, or rapidly by producing delirium.
A relation between pulmonary consumption and mental disease is frequently observed—partly, perhaps, due to general anæmia, in part to circulation of diseased blood in the brain, and partly from tubercular deposits. Other diseases act directly upon the brain and nervous system, as leptomeningitis, pachymeningitis, sclerosis, capillary aneurisms, embolisms, cerebral hemorrhage, tumors, disease of arteries, syphilis, caries, exostosis, abscess, internal otitis, sunstroke; still others by disturbances in the cerebral circulation, as diseases of the heart and kidneys; others by vitiating the blood circulating in the brain, as in the acute stage of febrile disorders; others in some general unknown way, as chorea, hysteria, epilepsy, gout, rheumatism, malaria, pneumonia; and still others during the period of convalescence or of general exhaustion, which is often associated with infectious diseases or chronic disease attended with general anæmia. The more violent and curable psychoses occur at the height of acute diseases, those of longer duration and of less favorable result during convalescence. Among other recognized causes are prolonged and obstinate dyspepsia, the psychological changes, if morbidly developed or attended with accident, at puberty, during pregnancy, at childbirth, during the puerperal state or lactation, and at the climacterium, and rarely various affections of the abdominal and pelvic organs.
Chronic alcoholism produces disease of the small blood-vessels of the brain and the consequences of that condition, causing insanity in a considerable proportion of cases, and almost always some mental impairment. Insanity occurs under conditions of cerebral hyperæmia and of cerebral anæmia, although their relation as cause and effect is very obscure. The habitual use of hasheesh gives rise to a disagreeable form of dementia, and so does opium, but more rarely. The effects of poisoning from iodoform, lead, mercury, bromide of potassium, hydrate of chloral, belladonna, tobacco, when reported as producing insanity, are usually transitory.
Cases have been reported of two persons being exposed to the same causes and having similar attacks of insanity (folie à deux), and also of folie induite or folie communiquée, where several persons have adopted the delusions of a person of influence among them, one of the most remarkable instances of which was the case of the seventeen grammar-school-taught Adventists of Pocasset, who accepted the insane belief of their leader, Freeman, that, like Abraham, he had been commanded by the Lord to kill his child, that she was to rise on the third day after he [p. 120] had killed her, and that he was to become a great evangelist. So-called epidemic insanity, choreomania, and demonopathy belong in this class.
From untrained, ill-balanced men and women, whose lives are ill regulated, the ranks of the insane are largely filled. Insanity is often the ultimate wreck of a life ill guided, directed chiefly by caprice and passion and weakened by indulgence. In that case it is, like much habitual drunkenness, as much a fault as a disease. The individual will not behave with decency and propriety for so long a time that, finally, especially after the age when the brain begins to fail, he cannot.
SYMPTOMATOLOGY AND COURSE.—The distinguishing symptoms of insanity are mental. In some forms of insanity they are mental only; in others these symptoms are associated with others, such as also occur in diseases not necessarily affecting the mind. The earliest mental symptoms are change of character, increased irritability, less feeling of accountability, a lower moral tone, moral perversion, diminished stability, loss of interest, lessened power of concentration and self-control, impulsive acts, anxiety or the opposite condition of mind, perverted or exaggerated force of the emotions, restlessness, apprehension, sleeplessness, impaired will, slight depression or barely noticeable exhilaration: things and persons seem changed in some vague, unexplained way. There is an alteration in the way in which the person is affected by his surroundings.
The next symptoms are more purely intellectual. Delusions are often at first based upon some fact, and are merged into insane delusions only as the mind, in becoming weakened, loses power of comparison and judgment. Often they arise out of the disordered condition of mind. Hallucinations of any of the special senses, illusions, perverted ideas, mental confusion, mental hyperæsthesia or anæsthesia, delirium, stupor, exaltation, depression, impairment or loss of memory, quickened or dulled conception and perception, increased or diminished intellectual activity and acumen, distorted association of ideas, imperative conceptions, all sorts of anomalies of consciousness and free will, uncontrollable and uncontrolled insane impulses, are common. The intellectual and moral symptoms appear nearly or quite together in very acute disease, and they together increase in intensity, and finally entirely control the individual. Many of the insane recognize the fact of their insanity. Some of them understand the nature of their disease quite well, discuss their cases intelligently, and frequently ask why they, automaton-like, are impelled by a force which they cannot resist to constantly do things which their intelligence and better nature condemn. Not a few are confined in places of safety by their own preference.
The physical symptoms of insanity are perverted sensations of almost every conceivable kind, resulting in depraved instincts and acts, psycho-motor excitability, convulsive action, choreic movements, uncontrollable muscular agitation (springing, shouting, swearing, dancing, running, destructive tendencies, etc.), elevation or depression of pulse, respiration, or temperature, loss of appetite, digestive disturbances, pain, fever, tetanic and cataleptic rigidity, paralysis, tremor, ataxia, epileptic seizures, convulsions, muscular contractions, increased or decreased secretions and excretions, disturbances of general nutrition.
The course of the various mental diseases is to a great extent chronic, some forms being incurable from the beginning, others curable to such [p. 121] an extent that of recent cases from one-half to nine-tenths recover, of whom a considerable proportion remain well to their death. The duration of the mental diseases is from a few days to a lifetime, sometimes not even shortening life. The termination is oftenest in incurable chronicity or dementia, less often in permanent recovery without recurrence, and still less often in death from the first attack. Unfortunately, the essentially incurable and the curable forms of mental disease are classed together in statistics of insanity. While many types are absolutely fatal or certain to end in hopeless chronicity or dementia, others tend to recovery. In some forms relapses and recurrent attacks are to be expected: in others they seldom occur. In many cases there is no more probability of transmission to children than in Bright's disease, and no more likelihood of subsequent attacks than in typhoid fever.
MORBID ANATOMY AND PATHOLOGY.—It is thought by the best observers that insanity depends upon a functional brain disturbance, or at least upon a disordered condition which it is beyond our present power to discover, and that the normal working of the mind depends upon a brain healthy to such an extent that its millions of functional activities, in their endless relations to each other, preserve a state of equilibrium; or, in other words, that the higher centres maintain their power of control over the lower. It is doubtless true that this relation depends in general upon a healthy brain, but it is not yet known to what extent. Disease of the brain or its membranes, apparently slight, often seems to cause insanity, and often there is marked disease without insanity. We certainly cannot place all the pathological conditions found in the brain of a person dying insane in direct causal relation to his insanity. The anæmia observed by Meynert in melancholia and the hyperæmia of maniacal excitement, even if proved to be universal in those conditions, may be only symptoms of the underlying disease or caused by it. It is certain that there are indications of as great anæmia or hyperæmia in other states without insanity.
Insanity in its initial stage does not, as a rule, involve a recognizable deviation from the normal structure of the brain, and the patient may die before such pathological changes are so manifest that we can detect them. But if the disease has been of long standing, in the majority of cases the brain shows evident marks of disease, and there may be found no striking indication to the naked eye of deviation from a healthy condition, when a microscopic examination reveals signs of advanced cerebral disease. The limited knowledge of the cerebral structure and function which pathologists possess, and the consequent difficulty in detecting changes from the healthy state, indicate that the failure to find them is attributable in not a few instances to the fault of the investigator rather than to the nature of the disease. Certain it is that the better acquainted we have become with the anatomy of the brain and with its functions and sensible qualities, and the more thorough and painstaking we have been in our examinations, the rarer it has become to find a case of insanity where no organic changes are observed after death, although it is true that we do not understand all the relations between these changes and the symptoms observed during life.
A large abscess of the brain, a hemorrhage, a tumor, or a wound of the cortex or other portion of the brain, various degrees of inflammation, [p. 122] meningitis, are sometimes followed by insanity and sometimes not; and we do not yet understand the reason for the difference. Indeed, nearly every pathological condition of the brain known in insanity—in kind, if not in extent and degree—may be found in diseased or injured brains where there has been no mental disease in consequence. There is only one disease, general paralysis of the insane, in which the morbid appearances discoverable after death with our present knowledge bear a definite relation to the most constant manifestations during life. And yet, with pathological changes so similar that we are not able to detect their essential difference, the mental symptoms of the first stage of general paralysis may be most various. Rosenbach has found in the brains of starved dogs and guinea-pigs as extensive changes as in well-marked primary dementia, in which the pathological conditions are more extensive than in any other form of acute insanity.7 That is to say, when we have discovered and described all the morbid appearances in the brain of an insane person we have taken only the first step in accounting for his insanity.
7 Centralblatt für Nevr. Psych. und ger. Med., 1884, p. 33.
The localization of many of the cerebral functions, the discovery of a psychomotor tract, and the constant accessions to our knowledge of the physiology of the brain are throwing much light on the subject. But all efforts to localize the intellectual and moral functions of the brain, except generally to agree with the teachings of a century ago and to place them for the most part in the anterior and antero-lateral portions of the cortex, have thus far failed of success, the most careful observers still thinking that local lesions when apparently causing insanity do so by injuring the action of the brain as a whole, and not of any particular part.
In some cases of insanity, with never anything like acute disease, where death occurs from the weakness of old age or some intercurrent malady, the brain does not present any recognizable difference from those of sane people whose brains have worn out with their bodies. In those forms of mental disease where changes are found, the most important and constant are in the cortex of the brain, especially in the fore, upper, and middle parts of the periphery, involving usually also the membranes. In beginning acute mania the condition of the blood affecting the brain or the pathological changes are probably as nearly identical with those in the acute stage of pneumonia, certain forms of typhoid fever, cerebro-spinal meningitis, and other diseases as the symptoms of the mania are now and then difficult to differentiate from those of the other diseases just mentioned. In rheumatism, syphilis, malarial poisoning, and Bright's disease with mania we find no distinctive pathological conditions to account for the maniacal symptoms.
If asked whether there is a fixed lesion of the brain or any of its parts corresponding to given psychological changes, we should be obliged to say no, except in the case of incurable dementia. If asked whether there are important morbid changes corresponding with all cases of insanity, we can only say yes, sooner or later, in the majority of cases, and that there are certain destructive lesions, chiefly inflammatory, atrophic, and degenerative, which invariably mean marked deterioration of the mind. As regards diseases of other organs than the brain, the insane, like the sane, die of all of them, and in especially large numbers of pulmonary consumption.
[p. 123]Insanity may, both in its acute and chronic form, be the result or symptom of simple anomalous excitation or nutrition of the brain or of inhibition of some of its portions, without any change in its gross appearance which can be detected by our present methods of research. In the majority of cases there are found diseased conditions which become more manifest the longer the duration of the disease, appearing for the most part in the blood-vessels, pia mater, and cortex of the brain, but also in the medullary portion, many of which are recognized only in their late stages. In the functional mental diseases there is no characteristic lesion of the brain as yet recognizable, even in the latest stages, more than is to be found in the brains of persons dying from other causes. When apparently local injuries or diseases cause insanity, they probably do so through a general disturbance of the brain or through diffuse disease resulting therefrom and for the most part affecting both hemispheres. The molecular, chemical, anatomical, physiological, pathological, or physical changes in the brain which give rise to insanity, and their relation to the grosser pathological conditions of the brain, are still not clearly made out.
In terminal dementia, especially in the last stage of paralytic dementia, nearly every tissue and organ of the body may be found to have undergone pathological changes, of which by far the greater portion is secondary to disease of the brain; and it is impossible to say how much of the brain lesions in these and other conditions of mental unsoundness is secondary to the disease or an accidental complication.
DIAGNOSIS.—In the diagnosis of insanity the physician assumes a responsibility for which he is liable under the common law. It is important, therefore, to avoid mistakes as far as possible. In the majority of cases the patient's unsoundness of mind is evident before he is brought to the doctor, but in not a few the symptoms are obscure, and they are often rendered more difficult of correct understanding and appreciation by the deception or reticence of the patient and by the prejudices of his friends.
First, before seeing the patient it is well to get from his family, friends, and physician a full knowledge of his natural state, all the facts known to them relating to strange behavior, delusions, etc., as they give most useful hints with regard to the method of examination. Apparent familiarity with an insane person's delusions will often secure their immediate acknowledgment. In a case of any obscurity or where there is doubt that other causes than insanity may have produced the unusual behavior, and particularly if any legal steps are to be taken regarding guardianship, restriction of liberty, commitment to an asylum, validity of wills and contracts, capacity to manage property, marriage, etc., it is imperative that both sides of the question be fully heard before any positive opinion is given. After the patient's confidence has been gained in general conversation, during which his appearance, manner, and mental condition as to intelligence, coherence, memory, judgment, perception, and capacity may be noted and compared with his normal standard, he should be examined carefully for any external evidence of lack of development or of injuries to the head. As in all other diseases, the condition of every organ of the body should be noted; a complete diagnosis should be made. The expression of the face often indicates such excessive excitement, gloom, stupor, suspicion, or fear as must be due to insanity alone.
[p. 124]Throughout the examination the questions and manner of the physician should be such as to avoid suggesting unpleasant ideas or associations to the patient. The matter of suicide should never be first mentioned by the questioner, and not seldom he does best who listens most and lets his patient disclose his morbid ideas and impulses, as he will frequently be led to do, if at all, by the manifestation of interest and sympathy, and of knowledge of the symptoms of the disease in hand, on the part of the physician. He often gets enough for his purpose without getting the whole story, upon which it sometimes does harm, or at least is not best, that the patient should dwell. In the diagnosis of mental disease, however, as well as in estimating responsibility, the fact must be borne in mind that a controlling delusion may be concealed for months or even years, and that the symptoms and mental condition of insane people vary so much at different times that it may be quite possible to get distinct evidence of unsoundness of mind at one time and not at another. The power of self-control is also liable to the same variation or alternation.
If the patient has no reason for simulation, it is commonly best to tell him the object of the examination. The family history should be learned from others, as questioning the patient on these points is apt to put him in a train of thought unfavorable to a hopeful view of his own case. After full personal questions concerning himself and his environment, one can usually tell whether there are unreasonable suspicions, violent impulses, perverted feelings with regard to his family, delusions, hallucinations, or illusions. A delusion's existence must often be accepted, however, from the behavior of the patient and from the statements of those about him. Hallucinations of hearing must sometimes be inferred from the attitude of listening to imagined voices; and prolonged observation under circumstances such that the patient does not know that he is watched will often settle the question of his insanity when other means have failed. A careful examination should, of course, be always made for the physical and rational signs of disease. In the differential diagnosis care must be used not to mistake for insanity the acute diseases typhoid fever, meningitis, smallpox before the period of eruption, pneumonia, cerebro-spinal meningitis, narcotism or delirium from drugs, and alcoholism—errors which have been made, and which can be avoided by deferring one's opinion for a sufficient time.
The detection of simulation is more difficult, especially as the insane sometimes feign insanity for a purpose, or, on the other hand, accuse themselves of wrong acts which they never committed. In general, it may be said that sane persons pretending to be insane very much overdo their part, do not make their symptoms conform to any recognized type of disease, and have a strong motive for their deception, as well as for the act for which they wish to be considered irresponsible. Their insanity first appears after the deed; they are exhausted by their efforts to seem mad, and appear quite sane if watched when they think that they are unobserved. A crime performed without accomplices, with no plan or a silly one for escape, and with no sane motive, is usually itself evidence of insanity. On the other hand, people partly demented by chronic insanity often commit crimes with all the method and motive of the criminal. In not a few cases, especially when the fact or not of impaired intellect cannot be decided by comparison with a previous condition, the question of [p. 125] insanity, or at least of responsibility, will be beyond human wisdom. A correct diagnosis can, of course, not be made without a familiarity with the various forms of mental disease; and insanity is now so well understood that a sufficient examination of an insane person should develop the clinical history of some known type of disease in nearly every case.
Little has been said of the physical evidences of insanity, because there is little to say. Conditions of mental torpor, depression, and excitement are associated with the physical manifestations which we would naturally expect in those mental states. Coarse brain disease with insanity or without may have identical physical signs; paralytic dementia is the only disease in which corporeal indications really assist in forming a diagnosis.
A family predisposition to mental disease does not materially affect the question of fact whether a given individual is insane or not, except that in a doubtful case it adds to the probability of insanity, and is thus far a factor of importance as corroborating other evidences of an unsound mind.
PROGNOSIS.—The prognosis in insanity depends first upon the type of disease, mania, melancholia, and some forms attended with confusion and stupor being the most curable; the forms attended with systematized delusions or with periodicity which is not dependent upon menstruation, folie circulaire, and moral insanity rarely so, and the organic brain diseases, congenital insanity, and confirmed primary delusional insanity (monomania) hopeless. The acute forms are far more curable than those of a subacute type: 60 per cent. of the cures in insanity occur in the first half year of treatment, 25 per cent. in the second half, and 2.5 per cent. in the second year, roughly speaking. In chronic cases a reported cure is most commonly only a remission, and after several years of existence insanity is generally incurable, although rare cases of cure in mania have been reported after even from six to fourteen years of treatment, and in melancholia after twelve years. So long as there is no permanent dementia and there are distinct intervals of mental clearness, no matter how short or how far apart, there is hope of final recovery in the curable mental diseases.
People of sound families, with insanity of an acute type arising from physical causes, often make such speedy and complete recovery as to justify their subsequent marrying if they wish, while those of unstable nervous organization recover more slowly and oftener relapse. Insanity from so-called moral causes, too, is of more unfavorable outlook than if from the physical causes, if we exclude organic brain disease. A person with good physical education, excellent mental training, and self-control is more likely to get well than one with a vicious bringing up. The ages of maturity and middle years are most favorable to complete recovery. In women there are more first cures and more relapses, according to Krafft-Ebing. In general, the mortality of the insane in asylums is about four times that of the sane of all ages, or approximately six times that of the sane at the ages when insanity prevails.
Prolonged stupor, profound incoherence, loss of memory, and moral debasement are unfavorable symptoms, unless quite acute, of short duration, or occurring after the rapid subsidence of acute symptoms. Hallucinations of hearing, and to a less extent of sight, impulses to violence, and especially systematized delusions, are grave indications. Paralysis, [p. 126] epilepsy, and convulsions usually mean chronicity or death. Extensive disease of the heart, kidneys, or lungs, confirmed dyspepsia, especially of alcoholic origin, and a previous history of syphilis, seriously affect the prospects of recovery. If there is actual cause for self-accusation, if the knowledge of wrong-doing is added to the morbid mental state, the period of convalescence is apt to be much retarded, or even recovery is prevented, by the difficulty of establishing a healthy reaction. Even an irresponsible act is often magnified into so depressing an influence as to prevent restoration to health, as in the case of those who have injured or killed members of their family.
Of 9689 persons admitted into the Worcester Insane Asylum8 during fifty years ending September, 1881, of whom 1083 had been in other asylums, 35.49 per cent. were discharged well, 26.61 per cent. improved, 17.71 per cent. not improved, 0.5 per cent. not insane, and 14.85 per cent. died. Of those discharged, 25.41 per cent. were readmitted, and of 798 discharged recovered, with regard to whom inquiries were made, 156 were reported well at the time of replying, 197 as having died sane, 30 committed suicide, 162 relapsed and died, 94 relapsed and were alive, 30 were in hospitals or almshouses insane, and of 129 no information was got. Out of 798, there were 316, or 39.6 per cent., known to have become insane again or to have committed suicide. Of 1966 second admissions, 668 recovered; of 607 third, 263; of 261 fourth, 119; of 132 fifth, 70; of 70 sixth, 42; of 48 seventh, 30; of 37 eighth, 21; of 30 ninth, 19; of 26 tenth, 15; of 23 eleventh, 11; of 18 twelfth, 11; of 15 thirteenth, 10; of 12 fourteenth, 8; of 8 fifteenth, 5; of 4 sixteenth and seventeenth, 3; of 4 eighteenth, 2; of 2 nineteenth, 1, who was admitted and discharged well twenty-three times.
8 Forty-ninth Annual Report, including tables by John G. Park, Medical Superintendent.
Thurnam's statistics, that one-half of the recent cases of insanity treated in asylums recover, and that of the recovered only two-fifths remain so, receive constant confirmation. There is a considerable proportion of the inmates of asylums whose brain-condition is so unstable that they come in and go out frequently. Their brains are unstable, too, in the little affairs of life, and many of the nominally cured remain comfortable only by being shielded from sources of physical wear and mental worry. It is impossible to get statistics of the curability of mental diseases properly treated outside of asylums, but the results would probably be more favorable than those just quoted, partly from the greater chances of cure in the mild cases and in those acute cases which can be kept at home, or at least do not require hospital treatment.
It is difficult to form an opinion as to the probability of subsequent attacks in those who have recovered from any of the curable forms of mental disease. The same constitution, of course, remains as that which predisposed the individual to the first attack, and no one can look far enough into the future to predict the influences which will be brought to bear upon any given person for a considerable period of time. If they are favorable for preserving mental health, the chances of escaping mental disorder in the future are very much greater than if the occupation which must be pursued and the life which must be led predispose to bodily exhaustion, anxiety, and brain-worry. If the disease first appeared under slight exciting causes, it will not often be possible to [p. 127] avoid similar conditions again, and some forms of insanity are characterized by relapses and recurrent attacks.
Of the persons reported recovered from mental disease, a large proportion fail to recover in the sense of being fully themselves again. There is left some change of character, no matter how slight, some moral perversion, irritability, instability, impaired will, lessened power of self-control, diminished mental capacity—some lowering of the intellectual or moral standard, some deterioration of some kind.
TREATMENT.—Not long after Leuret recommended and practised severe discipline in the treatment of the insane a case was reported at the Medical Congress in Naples (1845) where douches, setons, blisters, bleedings, internal medication, shocks, terror, harsh discipline—nothing succeeded in restoring to sanity a woman become insane three months after her confinement. There probably are places where similar methods are practised at the present day, and yet it is not unreasonable to suppose that the very treatment used is sufficient to render incurable patients who might otherwise get well. The modern management of mental disease by rest, diet, baths, fresh air, occupation, diversion, change of scene, no more medicine than is absolutely necessary, and the least restraint possible—in a word, improving the patient's general condition, meeting the indications of his disease, diverting his mind from its morbid thoughts, or putting the brain in a splint, so to speak, as each case demands—gives much better results, the value of which is much diminished by the enormous increase in the size of our asylums and the great aggregation in them of diseased persons in all stages of insanity.
In twenty American asylums, the statistics of which have been analyzed by Pliny Earle in his paper on the Curability of Insanity, the average diminution of reported recoveries for about twenty-five years has been from 46.08 to 34.26 per cent. annually of cases admitted, and in the Massachusetts State asylums from 25.95 to 22.25 per cent. of 3371 persons admitted from October, 1879, to October, 1882. The prospect of treatment of insanity does not, from these figures, look very hopeful, and it must be conceded that there is in the proportionate number of reported recoveries a decrease which it is important should be explained. It is undoubtedly true that a larger number of the chronic and quiet incurable insane are sent to the asylums now than formerly, thereby diminishing the curable proportion. The character of the asylums, too, has changed from being small, easily-managed institutions to overgrown affairs, crowded with so many incurables that the duties of the superintendents have become largely administrative, and the medical treatment of the sick has been driven to a subordinate position. Medical officers, too, are more cautious in using the word cured after experience has shown them how many reported cures are only remissions.
In treating insanity, even more than any other disease, the fact must be borne in mind that one is treating a diseased person; and indeed it is often necessary to treat a whole family of persons predisposed to insanity in giving directions for one actually insane. There probably has been no time during the last quarter of a century when there was more uncertainty in the minds of the medical profession regarding the best treatment for patients suffering from curable mental diseases than at present. Twenty-five years ago the almost universally-accepted practice was to send [p. 128] them to an insane asylum with as little delay as possible, without much regard to the character and duration of their disease. Twenty years ago, in the medical school the professor of obstetrics advised sending all well-marked cases of puerperal insanity early to the hospitals for the insane, and only a few years later Godding, then superintendent of the asylum at Taunton, advised that patients with puerperal insanity be kept at home until every available resource but the asylum had been tried without success.9 Meynert lectures to his classes in Vienna that in every case there is a disadvantage in sending curable insane persons to asylums, although it is often a necessity to do so. Maudsley thinks that a large proportion of the curable insane can be treated to best advantage either at home or in small private asylums or houses; while Bucknill says that by home treatment more cases would be cured than with our present methods. The late Isaac Ray summed up his vast experience in the treatment of the insane by saying that it cannot be shown that the introduction of insane asylums has added anything to the curability of insanity, much as they are to be praised from the humanitarian point of view. According to the statistics of Pliny Earle—to which the only objection we can make is that they are so exhaustive and conclusive that we cannot controvert them—the permanent curability of mental diseases in asylums for the insane is not only small, but decreasing.
9 Boston Medical and Surgical Journal, vol. xci. p. 317.
Part of the results obtained by Earle may be due to the fact that curable cases are more treated at home now than formerly, that the degenerative types of insanity are more common, and that in our cleaning up and civilizing processes we are not only driving out filth diseases, but letting in disorders due to greater efforts and more intense struggles for the kind of existence which modern life demands. But it is also true that in enlarging our asylums, as we have been compelled to do, we have lost something in personal care of patients, and that we have increased the depressing influences of large masses of sick people to such an extent as to involve serious disadvantages in their treatment. It is a matter of common observation that some insane people do well at home, others away from home, and others in asylums—that some do badly in asylums, and quickly get well if discharged, and that others, after continually going down at home, immediately improve upon being sent to an asylum. There seems, however, to be no fixed rule in individuals, and certainly there is very far from unanimity of opinion among alienists generally as to the conditions for home treatment or removal from home or sequestration in asylums, except, of course, that few men of experience would take the responsibility of keeping out of asylums persons with alcoholic insanity or with delusions of persecution, or cases of violence and delirium, or any insane patients under conditions involving danger to the community or to individuals, although it is often a matter of extreme difficulty to decide when restraint becomes necessary or justifiable.
I have selected from a large number a few cases where I have acted contrary to the usually accepted views as to indications for removal from home, and with such success that I am led more and more each year to rather widen than narrow the lines within which home treatment seems to me desirable.
Case I.—Mr. ——, age 20, of sound constitution and without [p. 129] marked hereditary tendency to disease, although several members of his family are people of very little force. The patient had masturbated in college, as many boys do, and was compelled to give up his studies upon his father's failure in business. An attack of slowly-advancing melancholia developed, for which he was sent to the farm of a relative in the South without improvement, so that he returned home at the end of a year in pronounced acute melancholia. He secreted himself in a marsh not far from home, where he was by accident found bleeding freely from the radial artery, which he had cut to kill himself. He had the usual delusions of the disease. He thought the world was all wrong, that he had committed great crimes—the unpardonable sin—and that there was nothing but destruction before him and his family. He was desperately suicidal. The circumstances giving rise to his disease and the associations of his delusions were entirely connected with his home and members of his family. His people could not afford to hire a nurse, but his three brothers and one cousin were only partly employed, and they agreed to take care of him. The treatment was tonic and supporting, with plenty of sleep, food and outdoor exercise, with careful attention to daily details of life, arranging it as to amusements, occupation, etc. etc. from day to day to suit his condition, and with absolute watchfulness day and night to prevent suicide. He remained in the home where his disease arose, and he was taken care of by the people most actively associated with his delusions. He made a rapid and perfect recovery, and is now very successful in his work as a professional man.
Case II.—Miss ——, age 35, a sound, healthy woman, without any known hereditary predisposition to disease. Without any assignable cause, except a moderate amount of overwork and steady home-life without sufficient recreation, she became very ill with acute melancholia, much mental confusion, very varied delusions that the world was all wrong, her friends distorted and changed, and herself so great a sinner that she could not escape everlasting damnation. Her most constant and distressing delusion was that people were constantly lying in wait to kill her and her mother and her sisters. When I saw her she was taking large quantities of hydrate of chloral and bromide of potassium, which were at once stopped. With plenty of food, fresh air, exercise, rest, malt, and cod-liver oil she slept well. She was first put under the care of a professional nurse, who was not liked by the family, and I then decided to let the mother and sisters assume full charge. She was watched with unremitting care day and night, and yet managed to make three attempts at suicide, which of course were not successful. She made a rapid and most perfect recovery, and is still perfectly well.
Case III.—A letter-carrier about 25 years old, without known hereditary tendency to disease, under-fed, over-tired, and worried, broke down with pronounced mania of the simple type, without marked delirium or delusions. He was much exhilarated, often excited, rarely noisy, and, as he had no delusions, he was not dangerous. He was somewhat troublesome, and I feared that his disease might become more active, and so I recommended his removal to an asylum, to which his friends fortunately refused to consent. He became progressively worse, but still not maniacal or delirious. He had no specific insane delusions, but he had a generally exalted notion about all the events of life and his own affairs. His [p. 130] surroundings were not conducive to quiet, as he lived in the noisy part of the city, and his associations were those under the influence of which his disease appeared. But he made a most excellent recovery, and resumed his work with only a year's interruption.
Case IV.—A healthy young woman, without hereditary predisposition to insanity, confined with her first child. Her delivery was not attended with any especial difficulty, and she made rapid progress toward health and strength until the beginning of the third week, when a slight change of character was noticed which soon developed into active mania. She was delirious, profane, obscene, filthy in her habits, and filled with delusions regarding herself, her family, and her surroundings. She had a great aversion to her infant, and often did not know the several members of her household. Hers was as violent a case of puerperal mania as I have ever seen in an insane asylum. She was naturally not very strong, however, and people could always be near enough at hand to prevent her doing any harm to herself or others. Her infant was kept out of her sight most of the time for five months, and all of the time for many weeks. The usual treatment was adopted, an excellent recovery was made in six months, at the end of a year strength was restored, and the patient remains quite well now.
Case V. was quite similar to the last, except that the disease was melancholia, and that the patient had tried to kill herself and her infant before I saw her. She made a complete recovery. Both cases were taken care of in their own homes, and for the most part by members of their own families.
I have reported these cases with as little detail as possible to illustrate the point which I have insisted upon for several years, that many cases at least of mental disease are to be treated precisely like typhoid fever or rheumatism or a broken leg, so far as removal from home is concerned, and that home-associations are no more harmful in properly-selected cases than in pneumonia or phthisis. I do not mean, however, that the patient should not be under the most careful treatment. On the contrary, the little details of medical care are fully as important as in early Pott's disease or beginning inflammation of the hip-joint. But it is often difficult to decide what cases should be best treated at home, what by slow travel or removal to other places than home, and what in asylums.
The objections to asylum treatment, when it is not absolutely necessary, are very great. On the other hand, the advantages that asylums possess for supervision and control are so obvious that they must continue by far the best means of treating the vast majority of cases of incurable insanity, and a large proportion of those in which a cure may be reasonably expected. The exigencies of many cases demand them. If, however, it can be shown that the aggregation of invalids in them is unfavorable to the best chances of recovery, and if, as I think is the case, many of the restraints and restrictions now common in them are unnecessary—for many of the patients, to say the least—the deduction is clear that a change must be made in asylum construction and management to correspond to these views. A common depressing influence in the treatment of mental disease is the fact that the patient remembers some member of the family who has had to go to an insane asylum, and fears the same fate for himself, or after one commitment and recovery fears that he may [p. 131] have a relapse and be obliged to enter an asylum again. I am quite sure that a considerable number of the recovered patients of insane asylums who commit suicide do so from this dread; which is not altogether unnatural, as the tendency there is downward, so that the patient, as he in the progress of his disease more and more loses self-control and power of decent behavior, is progressively dropped into lower wards, with more disorderly or demented patients, at a time when all the surrounding influences should be, on the contrary, of a tendency to lift up. On the other hand, many who recognize their infirmity wish to be taken away from old friends and associations, and prefer the seclusion of an asylum, which is their best home.
The more acute the disease, the more likely it is to be of not long duration, and, as a rule, the easier it is to treat it without removal from home, except in cases of great violence. The question whether home-influences are benefiting or injuring an individual patient must often be settled by experiment. It is a great comfort to many of the insane to see their friends, no matter how seldom, at times when they feel that they need their support and influence; and this is impossible unless the friends are near at hand. There are cases in which familiar scenes and faces and voices reassure the patient when delirium subsides, and during a short interval of comparative mental clearness their sedative influence is great as compared with the confusion and worry of trying to understand the new surroundings of a hospital ward or the sight of strange people and the sound of unknown voices. The mere fact of delusions being connected with the home-surroundings and members of the family is not so important as the character of the delusions; and the influence of the relatives is often most salutary, even when the patient has most distressing thoughts concerning them or even when he is too insane to be always sure of their identity. If the insanity arises in a violent emotional shock, and home sights and surroundings recall and arouse the mental pain, as is the rule in such cases, recovery usually depends upon removal from home. The matter of suicide where there are means of proper watching does not influence me in my decision, as I think that the dangers of self-destruction are fully as great in asylums as outside with sufficient care, whereas the stimulus to the patient to kill himself from both insane and sane motives is greater the more he is surrounded with depressing influences. On the other hand, it not seldom happens that the diversity of sights in the hospital, the routine, the varied events of the day, the amusements, the walks, the drives, even the discomforts and annoyances, serve to distract the patient's mind from his delusions better than the same result can be accomplished under the pleasant influences at home, while a natural feeling of self-respect prevents those who have power of self-control from giving way to their impulses before strangers, especially when they know that such conduct will take them to a lower ward with less agreeable associates.
There is no doubt, however, that home-treatment of the insane in the majority of cases is synonymous with neglect of all those minute attentions to details that make the difference between recovery and chronic mental disease. Home-associations often act upon the insane mind like frequent passive motion to a diseased or fractured hip; the relatives of the insane patient oftener than not share with him a common inheritance [p. 132] of an unstable mental organization, and will not be judicious in their treatment of him, or they cannot be subjected to the risk of becoming insane themselves in taking care of an insane brother or parent; and it is seldom that a private house away from home can be converted into a hospital, as it must be for the treatment of an insane person. One of the greatest difficulties in the home-treatment of the insane is during the many months of slow convalescence, when it is difficult to prevent a too early resumption of cares or work or methods of life prejudicial to complete restoration to health; so that in that stage of the disease, if in no other, removal from the familiar and usual surroundings of the patient will usually be quite necessary. The small private hospitals, with all their many and obvious advantages, always have been, and inevitably must be, chiefly devoted to wealthy patients who wish for a home where they can have medical supervision, rather than curative institutions for any large number of persons; and there is not enough going on in them to sufficiently occupy the attention of certain curable patients who must be removed from home, although they are well adapted to those who need quiet and seclusion chiefly. The larger hospitals, with their large staff of skilled officers and nurses, and with all their appliances for recreation or rest, amusements or occupation, discipline or gentle support, must be our chief means for treating the insane. They are indispensable for a large number of the insane who are of such unstable mental equilibrium that a little over-exertion or a trifling deviation from a carefully regulated routine throws them off their balance; and they must be used, temporarily at least, for many of the incurable or partially curable insane who need a place and an opportunity to learn self-control and self-management. Enormous advances have been made in the construction and management of hospitals for the insane, more especially in the last fifteen years. We see it everywhere. But the greatest need, of opportunities to combine advantages of the asylum treatment with the benefits of home-comforts, to place sick people where the influences surrounding them will be healthy, and where there are not so many harmful as well as useless restrictions upon liberty, and so many morbid associations, is as yet entirely unfilled in this country. The question of the best, or even of an improved, organization for our insane asylums is too wide a subject to be discussed here. That our present system tends to make the medical staff narrow if they are appointed to their duties without previous broad training and experience or for political reasons, is a self-evident proposition; and yet there are manifest objections to just such a visiting staff as is customary in general hospitals.
As Maudsley says, squalor in an attic with liberty is better than being locked up in a palace with luxury. Many of the insane share that feeling with their sane brothers. To not a few it makes the difference between recovering their mental health and lapsing into incurable dementia. Many would voluntarily consent to remain in places less distasteful to them. If we could separate them into classes, as Mr. Mould10 has done in England by buying or hiring ordinary dwellings one or two miles even from his asylum, we could have separate houses with open doors or shut, as the case demands, for those who require them, and reserve the [p. 133] associated halls and large buildings for a different class. Mr. Mould has not applied his own system to those cases which need it the most, the curable insane, except to a very moderate degree.
10 Presidential Address at the Annual Meeting of the British Medico-Psychological Society, October, 1880.
It is not often that the physician is called, or his advice heeded if given, in the early stages of mental disease, and the first symptoms are by no means easy to differentiate from the less harmful results of mental strain. If there be, however, sufficient loss of equilibrium to suggest the question of beginning insanity, it is of course better to take the safer way and recommend removal of all sources of irritation, and to advise rest, sleep, simple food, attention to the general laws of health, outdoor life, and change of scene for a sufficient length of time to restore the mental poise, avoiding narcotics and sedatives as far as possible, and keeping the patient with a safe adviser or within easy reach of one. In many cases, especially of young persons, this may involve a radical change in their choice of a profession and whole plans of life. If the question of marriage comes up in these cases before the physician as to preventing further developments of threatened disorder, it can only be said that what may be well for the individual is not always best for society. A few years' delay will usually give time for the question to settle itself.
When insanity has actually appeared the same rules should govern its management as in other diseases. If, like smallpox and diphtheria, it is a great source of danger to others, the patient should be put in a safe place; if, like typhoid fever arising from bad drainage, its cure depends upon the removal of a given cause, the patient must leave the infected locality or have the cause displaced; if, like rheumatism in a damp cellar, it can be treated successfully only under different conditions, the patient must be removed; and if poverty or other conditions prevent the best possible treatment, the next best practicable plan must be followed.
The first question which comes up in the care of the insane is with regard to removal from home and commitment to an asylum; and here a great many points must be taken into consideration. It is not always that a home can be accommodated to the use of an insane member of the family. There are not many in which there can be proper quiet and seclusion without depriving the patient of that abundance of fresh air and outdoor exercise which is so often required in treatment. Frequently those nearest to him irritate him to the last degree, or he has some aversion or delusion in regard to them rendering their presence injurious. If the delusions and impulses of a patient are not such as to endanger the lives of the household, his violence and excitement and uneasiness or melancholia may make life simply intolerable to his relatives, or his exactions may be exhausting to their strength and his constant presence a means of making still others insane. His noise may disturb a whole neighborhood. His vagaries may require control, his indecencies concealment, his enfeeblement help more than can be sufficiently given outside of a hospital, his general condition more judicious care than his friends can command, and his example may have a pernicious effect upon children growing up with an insane diathesis. In many people a long time insane much of their vicious conduct is due to habit or to tendencies which they cannot or will not control without the steady, kind discipline which cannot be got at home.
A man with delusions by virtue of which he thinks that some one is [p. 134] plotting to ruin or kill him is apt to commit murder; a mother who believes that the world is going to ruin and her children to torture may be expected to put herself and them out of misery; a demented woman chops off her infant's head because its cries disturb her; and the maniac's delirium or epileptic's fury drives him into any horrible act. Such people need to be watched always by some person or persons fully able to prevent their doing harm, which in many cases can only be done, with any reasonable degree of liberty to the patient, in a hospital for the insane. If the danger is obviated by removal of certain persons—children, for instance—or if watching by nurses serves the purpose, and there are no Other objections to such a course, there are cases in which the chances of cure are more if the patient remains at home whenever the disease pursues an acute course. Most of the insane, however, have passed the curable stage; the majority need the moral support and freedom from responsibility or the regular life and regimen of a hospital; and a large proportion of the cases following a subacute or chronic course must be removed from home. The expense attendant upon the safe treatment of mental disease in a private house is entirely beyond the means of most families, just as they cannot send their consumptives to Colorado or France, and so the hospital becomes a necessity. Except in dangerous cases, however, the hospital should never be hastily decided upon. A little delay does not diminish the patient's chances of recovery, and may show that the attack is only transient, whereas removal to a strange place might aggravate the disease and increase its duration. It is particularly important not to choose an unfavorable time to commit an insane person to an asylum, and thereby add to discouraging conditions already existing an additional source of despair at a time when every influence should be as elevating and cheering as possible. In most cases, especially if there is a suicidal or homicidal tendency, it is best, when removal to an asylum has been decided to be necessary, not to argue the question with the patient, but to explain why it must be done, and then do it without delay.
The law provides the methods of commitment to asylums. They are so different in the different States that they cannot be discussed here.11 The one rule holds good everywhere, however—that it is far better to use force than deception in sending the insane from home to asylums, and that the cases are very few in treating the insane in or out of asylums where deception is either justifiable or wise. A second safe rule is that a person of unsound mind is always a source, immediate or remote, of more or less danger.
11 An abstract of the various laws may be found in the appendix to the American edition of Clouston's Clinical Lectures on Mental Diseases.
Commitment to an asylum means so much that safeguards against improper action should provide careful examination of the case by competent physicians, as little restraint as is required by safety, good medical treatment in the hospital, thorough supervision by experienced persons on the part of the state, safe-keeping of the dangerous patients, and easy removal of those who have recovered or who may be sent out to their own advantage. In too many States confinement in an asylum means that two physicians, or even one, who may know little or much of insanity, think it best, and removal depends upon the word of one man, [p. 135] the superintendent. Once in the asylum, the best practice of the present day should be followed—namely, to allow free communication and visits from friends until it is shown that they do harm, to multiply cheerful and natural influences to the last degree, to furnish rest, exercise, occupation, or recreation as each case requires, and to remove all that is morbid and disagreeable so far as that can be done. A permanent removal from the hospital should be insisted upon as soon as it is safe to complete the convalescence at home or elsewhere, and an abundance of fresh air, indoors and out, should be supplied as the best curative agent from first to last. Arguing, moralizing, cheering up, rigid restraint, disciplining, sedative drugs simply for quieting patients, and still more bleeding and blistering, are for the most part things of the past. Mechanical restraint is all but abolished in the best hospitals, and is used only so far as it is considered the best medical treatment. A prison-like appearance of the wards has been found to be not only quite unnecessary, but harmful.
In many cases of insanity I make the question of removal to a large hospital one of circumstances and of money. If separation from the influences under which the disease occurs is necessary, and that cannot be secured at home, I usually select, as the case demands and opportunity is afforded, a private house with good nurses, a small private hospital, or an insane asylum where the general influences are the healthiest, where the medical treatment is in accordance with the best modern principles, and where the construction of the hospital is most nearly adapted to the requirements of the present day. Accessibility to visits of friends and the family physician where they help in the cure, and remoteness from them when they do harm, are also points to be considered. In many cases where the illness is of long duration a change of scene and association will prove of great service, even from one hospital to another. The permanent settling down into the routine of hospitalism is especially to be avoided. Of course there are cases, or rather conditions, in which a change would be detrimental to the last degree.
The associations, surroundings, and influences brought to bear upon the patient—what has been called the moral treatment—are of the first importance in the treatment of mental disease, and diet and hygiene come next. Medicines are of use in properly selected cases. The appetite must often be stimulated, the digestion regulated, and various painful symptoms must be relieved, so far as possible, without a resort to internal sedatives and narcotics. Rest and sleep are essential to recovery, but every effort should be made to obtain them by judicious regulation of outdoor exercise and of quiet as each case requires, abundant non-stimulating food frequently given, fresh air, tonics, baths, and removal of sources of irritation. Stimulants will sometimes be needed to prevent excessive exhaustion. Seclusion in a room darkened or not is useful in some conditions of excitement, and not seldom distressing symptoms are relieved by the simple presence of another person or by the absence of certain individuals.
Drugs of sufficient strength and in such quantity as to produce quiet or sleep should be used only when absolutely necessary, and then for as short a time as possible. Their prolonged use is open to many manifest objections in all persons, and particularly in those suffering from mental disorders, inasmuch as with them large doses, if any, are commonly given, [p. 136] and it is very difficult often, in the impaired state of mind of the patient, to get indications of symptoms which contraindicate the use of a particular drug or to learn when it is producing harmful effects. Tonics are often indicated, but should be used with discrimination, as some of them, especially those affecting the cerebral circulation, frequently produce disagreeable results.
After apparent recovery there should be a long period of after-treatment, which in most cases will be best met in rest or travel.
In the various forms of mental disease, through concentration of the mind on various delusions and by excess or deficiency in mental activity, the ordinary symptoms of physical disturbance or disease, independent of the insanity, are so much modified as to be often overlooked. It goes without saying that intercurrent diseases and distressing symptoms should be treated on the principles generally applicable to those conditions, so far as that can be done without aggravating the insanity. The usual treatment of pneumonia, for instance, may in an insane person provoke such determined opposition or so excite or aggravate delusions that, so far as the disease of the lungs is concerned, it may be better to let it take its chance, with good general care, including food, warmth, etc.
The conditions of cerebral hyperæmia require cold applications to the head, the wet pack, prolonged warm baths, a non-stimulating diet, and quiet. If the condition is acute and of short duration, rest in bed is useful, provided it can be secured without force. For prolonged mental excitement from cerebral hyperæmia it will be usually better to equalize the circulation by that motor activity which is characteristic of the disease, and to allow free exercise in the open air, keeping within the limits of exhaustion. My experience has not justified the use of bleeding, except, possibly, in acute delirium (mania peracuta). It is difficult to limit the action of blisters, and they often irritate the patient so much as to do more harm than good. Persistent refusal of food is usually due to delirium or delusions, and should be met with a resort to feeding with the stomach-tube before the point of exhaustion is reached if the tact of a skilled nurse fails of success. Mechanical restraint increases the cerebral hyperæmia, and there are few homes or general hospitals where it must not be used if there is excessive violence or delirium, making the insane asylum in those cases a necessity. Objectionable as it is, however, mechanical restraint is less harmful than the continued use of large doses of sedative drugs, as is so often the practice, in order to keep patients quiet enough to remain at home.
Ergot, hydrate of chloral, and opiates, which sometimes must be given by the rectum or stomach-tube, are sometimes advisable for a short time, but must be used with great caution. Milder sedatives, especially the bromides, serve a temporary use in the less violent cases; but less sleep will often serve if secured by quiet, abundant liquid food, and general measures, and in exhaustion by alcoholic stimulants.
Menorrhagia is very common in the maniacal states. It usually requires no special treatment, unless so great as to produce exhaustion. Amenorrhœa is commonly conservative, and then demands only general treatment; if it causes evident disturbance of the cerebral circulation, the ordinary methods, including electricity, massage, and local use of leeches, should be used.
[p. 137]Galvanism is sometimes useful, applied to the head, in cases of mental torpor and stupor. That and the faradic current, used with great care, act as powerful tonics to the general nervous and muscular system.
Insomnia is often the chief manifestation of the insane taint, in which case drugs are, for the most part, worse than useless. In all forms of sleeplessness it is better to try malt, cod-liver oil, beer, food, massage, baths, exercise, rest, etc. before resorting to narcotics and sedatives. Camphor, hyoscyamus, cannabis indica, the valerianates, bromides, codeia are much less objectionable than chloral, morphine, and opium.
Where masturbation is simply an evidence of loss of self-control, it is met best by constant watching, and gradually, as the mental state improves, arranging the daily life so as to develop the feeling of self-respect. Where it depends upon local paræsthesia, opium and camphor and cold bathing are indicated.
Constipation is a troublesome symptom, especially in the states of mental depression. When a full, laxative diet, cod-liver oil, and malt do not correct it, small doses of laxatives given frequently act better than the occasional use of purgatives.
There is a class of cases which are best treated by educating the patients as one would educate a child.
In the general care of the insane it is the duty of the state to see that they have all the rights of the citizen which are consistent with their proper and safe treatment, including the benefits of property and estate. There certainly should be in all countries, as in England, officers whose duty it is to see that this is done. For a large number of people with defective or diseased brains, who are now allowed to wander about committing crimes and serving repeated sentences in reformatories, houses of correction, and prisons, an enlightened public policy would find the best, and in the end the cheapest, treatment to consist in keeping them under supervision and control as unsound members of society.
The more particular treatment of the insane differs in the various mental diseases, varying as it necessarily must according to different conditions. Its prevention is not an easy problem. Many of the external causes of insanity seem inevitable in our complex civilization: it would be impossible to widely regulate marriages, even if we knew how; those people predisposed to insanity are usually too self-confident and self-willed to receive advice; and moderation in all things, healthful occupation, temperate habits, good digestion, and, above all, out-of-door life, seem as much like a sarcasm if suggested to many of the toilers as a waste of words if recommended to the idle and luxurious, while the parents who have transmitted to their children unstable or diseased brains generally impair what chances they have in life by vicious training.
Where syphilis, drunkenness, and other marked sources of mental degeneration do not obtain, simple food, plenty of sleep, avoidance of extremes of heat and cold, plain dressing, baths, good digestion, out-of-door life, fresh air, careful attention to slight disorders or injuries of the brain and nervous system, guidance against too much study and too much excitement or dissipation, development of character and moral force, intellectual and physical training, avoidance of too much emotional, sentimental, or even artistic culture, careful watchfulness during the period of adolescence, occupation without overwork, healthful recreation, a [p. 138] contented or philosophical mind, and suitable marriages, would produce the strong wills and healthy organisms needed to combat the tendencies of modern life. Such a course would undoubtedly make many a child with an hereditary predisposition to insanity become a healthy parent of children in whom the same treatment would soon eliminate the family taint. The character should be strengthened to learn to overcome difficulties rather than evade them. There are cases in which such a course can be adopted, and where the physician's advice may be of untold benefit to generations.
There are many crises in life when the mind totters and seems ready to fall, which the physician is more likely to recognize than any other person. Sometimes the odds are too heavy to fight against, but often there is a transient mental disturbance in such critical cases, or an incipient insanity, according as the indications are met with wisdom and patience or with neglect, indifference, and lack of judgment. The treatment called for is of the person rather than of the mental state, and in all forms of mental disease success in treatment depends very materially upon the personality of the physician, who must adapt himself also to the personality of the patient.
In about one-fourth of the cases of insanity there is no hereditary predisposition to the disease, and its prevention can be most hopefully looked for in attention to the general laws of health, the observance of which tends to secure immunity from all diseases. In the remaining cases—three times as many, in round numbers—the most hopeful course is in abstaining from marriage altogether or in the avoidance of unwise marriages; and it is an encouraging fact that many people in the community now take that conscientious view of the matter, although if they decide what to do without competent advice they are liable to err in the opposite direction of exaggerating their morbid tendencies, and so increasing their unhealthy predisposition. There are certain groups of physical and mental manifestations which the experienced physician recognizes as signs of tendencies which only await favorable conditions—a sufficient exciting cause—in the indulgence in drink or other excesses, in the exclusive search for wealth or fame, in the absence of healthy occupation, in mental wear and worry, in over-excitement, in the various conditions of ill-health, to develop into actual insanity. This physiognomy of temperament suggests to the observant physician a warning against excess of all kinds, and a recommendation for that course in life which promises the greatest likelihood of preserving a quiet mind and a healthy body and of securing a rational employment. Too much work is less dangerous to most people than too little.
12 Compare Moreau's La Psychologie morbide and Morel's Traité des Dégénérences physiques, intellectuelles, et morales de l'Éspèce humaine.
MICROCEPHALISM, CRETINISM, INTELLECTUAL IDIOCY, MORAL IDIOCY, INTELLECTUAL IMBECILITY, MORAL IMBECILITY (under which Westphal, Spitzka, and others place moral insanity) are really names for different degrees of similar defects, for the most part hereditary and [p. 139] congenital or resulting from disease or injury in infancy and early childhood, as distinguished from dementia, which is the result of later destructive mental or brain diseases. Idiots and the demented insane are sometimes so alike in their mental condition that, if young persons, they can be definitely distinguished one from the other only by a knowledge of the previous history of the case. Idiocy has its origin at or before birth or soon after, and terminal dementia seldom before puberty, commonly after maturity. In the United States census, where there is a doubt in the matter, the individual is classed as an idiot if the mental disorder occurred before the age of twelve in girls and fourteen in boys, and as insane (demented) if above that age.
The microcephalic brain may be as small as one-fifth the normal size, due chiefly to intra-uterine conditions for the most part unknown. Of course that means complete idiocy. The brains of other idiots differ in size and development. The mental condition in all is similar. Idiocy with the small or large or asymmetrical brain is classified, practically rather than scientifically, by Shuttleworth, as follows:
A. Congenital or Developmental13 Cases.—1, Microcephalic, with small heads: forehead and occiput defective; 2, hydrocephalic; 3, plagiocephalic, with distorted heads: features in an oblique plane; 4, scaphocephalic, with keel-like distortion of forehead; 5, scrofulous cases; 6, Mongol type; 7, cretinoid cases, with stunted bodies: irregularly expanded heads and enlarged thyroid glands; 8, syphilitic cases; 9, primary neurotic, with body well developed: signs of irregular nervous action; 10, sensorial idiocy, with two or more senses deficient (e.g. sight and hearing); 11, mixed cases.
13 Developmental conveniently includes those cases which, though of intra-uterine origin, become more pronounced as physical development proceeds.
B. Non-Congenital, Acquired, or Accidental.—1, Traumatic; 2, post-febrile; 3, hydrocephalic; 4, hypertrophic, with large square-built heads; 5, eclampsic; 6, epileptic; 7, paralytic; 8, idiocy by deprivation: loss of two or more senses in infancy (e.g. sight and hearing); 9, emotional idiocy, with no bodily deformity: shrinking, scared expression; 10, toxic idiocy, with no bodily deformity: malnutrition.14
14 “The Physical Features of Idiocy,” Liverpool Medico-Chirurgical Journal, July, 1883.
From the creature of deformed limbs and ape-like movements, incapable of articulate speech, even in monosyllables, or systematized ideas, leading a purely vegetative life, unclean, and with the instincts of a wild beast, up to moderate mental or moral imbecility, there are endless varieties of defects and monstrosities in mind, character, morals, and instincts, differing according to the profoundness of the disorder of the brain (hydrocephalus, atrophy, sclerosis, inflammation of the brain substance or membranes, injury from compression, blows, falls, convulsions, etc.), the extent of the defect in the brain development, the amount of the degenerative hereditary taint, or, in the case of cretinism, the importance of the endemic as well as the congenital influences.
In some of the higher planes of imbecility a considerable degree of intellectual brightness, or even talent, is often observed, and every variety of mental and moral perversion or simple reckless brutality. Training often does a great deal to bring many of these unfortunate creatures within the bounds of good behavior, but their care oftener falls within [p. 140] the province of the medical superintendent in an asylum or the teacher than to the physician in general practice. They are easily led astray by others, and commit all sorts of motiveless crimes or with a trivial or disproportionate motive, and with blind disregard of consequences or inability to comprehend them. In the gallery, at Washington, of photographs of counterfeiters and of passers of counterfeit money, the faces of the latter show conclusively that they belong to the intellectually weak-minded or imbecile class. Their own amusement, gratification, or impulse is so far the basis of their conduct that only a minority are harmless if not more or less constantly watched. Fortunately, a great portion—unfortunately, not all—of the idiots are sterile, but many of the mentally and morally weak-minded, with striking congenital defects which no training can fully remedy, propagate their species indefinitely for the benefit of our prisons and asylums.
Intellectual idiocy and marked intellectual imbecility are so common as to constitute 1 in 650 of our population. Less noticeable intellectual imbecility is quite frequent in the large class of troublesome and perverse children and youth of both sexes, commonly called weak-minded.
Moral imbecility, which cannot be corrected by education, is less common.
Moral idiocy is rare. It consists in such an absence of the moral sense that it cannot be aroused. It is sometimes associated with sufficient intellectual powers to make deliberate action and premeditation quite possible. Such persons are monstrosities, who, for the safety of the community, must be kept shut up for life like wild beasts.
The fact should be remembered, from a medico-legal point of view, that the defective in mind are quite liable to short attacks of simple mania and mental depression and to epilepsy, both of the obvious type and of the obscure or masked form, so that their degrees of responsibility, or rather of irresponsibility, vary from time to time. As a rule, a good physical organization and a general condition denoting healthy circulation and nutrition mark the better brains, and constitute important elements in forming a prognosis in regard to the possibility of educating imbecile and feeble-minded children up to the point of reasonably good behavior and ability to at least partly take care of themselves. The simpler their lives and the more purely routine or imitative their work, the less their defect is noticed. Many can wheel a barrow as well as any one.
THE INSANE TEMPERAMENT (Insane Diathesis, Neuro-psychopathische Constitution) is an exaggeration of the nervous temperament. It is closely allied to insanity and the neuroses, and at the critical periods of life is very apt to develop into one of them. It is congenital or due to early interference with the normal development of the brain by injury or disease. It shows itself in childhood and infancy by irregular or disturbed sleep, irritability, apprehension, strange ideas, great sensitiveness to external impressions, high temperature, delirium, or convulsions from slight causes, disagreeable dreams and visions, romancing, intense feeling, periodic headache, muscular twitchings, capricious appetite, and great intolerance of stimulants and narcotics. At puberty developmental anomalies are often observed in girls, and not seldom perverted sexual instincts in both sexes. During adolescence there are often excessive shyness or bravado, always introspection and self-consciousness, and sometimes abeyance or absence of the sexual instinct, which, however, [p. 141] is frequently of extraordinary intensity. The imitative and imaginative faculties may be quick. The affections and emotions are strong. Vehement dislikes are formed, and intense personal attachments result in extraordinary friendships, which not seldom swing suddenly around to bitter enmity or indifference. The natural home associations and feelings easily become disturbed or perverted. The passions are unduly a force in the character, which is commonly said to lack will-power. The individual's higher brain-centres are inhibited, and he dashes about like a ship without a rudder, fairly well if the winds are fair and the seas calm, but dependent upon the elements for the character and time of the final wreck. Invention, poetry, music, artistic taste, philanthropy, intensity, and originality are sometimes of a high order among these persons, but desultory, half-finished work and shiftlessness are much more common. With many of them concentrated, sustained effort is impossible, and attempts to keep them to it result disastrously. Their common sense, perception of the relations of life, executive or business faculty, and judgment are seldom well developed. The memory is now and then phenomenal. In later life there is a ready reaction to external circumstances, even to the weather, by which the individual is usually a little exhilarated or somewhat depressed. All sorts of vaso-motor disturbances are common and create distressing symptoms. Such people are said to be on the border-line between sanity and insanity. They are apt to be self-conscious, egoistic, suspicious, and morbidly conscientious; they easily become victims of insomnia, neurasthenic, hypochondriacal, neurotic, hysterical, or insane, and they offend against the proprieties of life or commit crimes with less cause or provocation than other persons. At the same time that many of them are among the most gifted and attractive people in their community, the majority are otherwise, and possess an uncommon capacity of making fools of themselves, being a nuisance to their friends and of little use to the world. Many of them get fairly well through life if their lives are tolerably easy or especially well regulated; if not, even they seldom escape further disturbance during the period of growing old. Their mortality-rate, especially from pulmonary consumption, is high. The prognosis is usually stated as unfavorable, largely, perhaps, because proper treatment is seldom pursued. If such children could be placed in the hands of judicious and experienced physicians from earliest years, much better results would undoubtedly be got and the downward tendency might be stopped. In the critical physiological periods of life, and under the influence of mental worry with physical strain, there is danger of breaking down. At the senile dissolution some of them lose much of their lifelong peculiarities, and as the mind fails in force and activity become more like other people. After the climacteric there may be also great improvement.
TREATMENT should consist in the general principles of mental hygiene, especially in training the mind to self-control and to avoid introspection—in a word, in maintaining health and in having healthy occupation. The earlier in life it begins, the better. It is well for such persons, unless of uncommon gifts in some direction, as many are, to obtain quiet, routine positions in life, and to avoid its wearing responsibilities as much as possible. The question of marriage is a difficult one for the physician if he is called upon for advice. Of course the risk often can be estimated only [p. 142] approximately, even after knowing both parties, who will heed medical counsel implicitly if it happens to coincide with their own notions. The further propagation of the neuro-psychopathic constitution in the world involves much entirely uncompensated misery, as well as genius, enthusiasm, and originality, the compensation for which is estimated by society in one way as regards Burns, Byron, De Quincey, Carlyle, Goldsmith, John Howard, and Frederick the Great's father, and in another when considering the inmates of jails and almshouses and the destroyers of home peace. Maudsley thinks that one such poet as Shelley justifies the risks of marriage in the insane diathesis, and Savage considers the neuro-psychopathic constitution a useful element in society; while Clouston holds that the world would be better off to lose the few ill-balanced geniuses, the hundreds of impracticable, unwise talented men and women, and the thousands of people who cannot get on, shiftless, given to drink, idle, improvident, and unpractical, to get rid of the insane diathesis, especially if we shall find a middle course and learn to apply the laws of heredity so as to save the best and eliminate the unsound. It is to this class probably that Pinel refers in saying that what he calls moral insanity is largely a matter of bad education. It is undoubtedly true that judicious training in very many cases would limit, if not prevent, the further development of the morbid element and strengthen the healthy side, so as to prevent actual insanity.
CONSTITUTIONAL AFFECTIVE MENTAL DISEASE is a further development of the congenital or hereditary predisposition to nervous or mental disease, with more or less of the marks of the neuro-psychopathic constitution. It is of two forms, the depressed and the mildly exhilarated, in neither case amounting to simple melancholia or mild mania. Sometimes the two forms are seen in a single member or in different members of one family where mental degeneration has begun. The frequent association of pulmonary consumption with these cases is possibly, in part, due to malnutrition in those persons living under the influence of more or less perpetual gloom, and to exposure and over-exertion in those who are constantly unnaturally excited, sleeping too little and driving their alert brains to the extent of exhaustion. Misanthropists, communists, iconoclasts of all kinds, enthusiasts and reformers, useful people and worse than useless, common nuisances, criminals, saints, and heroes, are found among them. Undoubtedly, in the case of criminals the tyranny of their organization deprives the intellect of much of the proper inhibitory power over the passions and evil tendencies, and yet with sufficient motive they can hold themselves considerably in check.
The PROGNOSIS is not favorable. At the critical periods of life, after severe diseases or injuries and with undue mental or physical strain, there is danger of further progress of the disease into more pronounced types; and this result is often the only way of satisfying the community that what they called meanness or wickedness was only disease. The progress of the disease is commonly very slow. It often seems like simple progressive development of character, except for the fact, generally overlooked, that it advances often in a different direction to what would be natural, and is independent of normal development. The subsidence of habitual severe headache not seldom marks a sharp advance in the severity of the mental symptoms.
[p. 143]The TREATMENT is hygienic. It must begin early in life, and be devoted especially to avoidance of mental overwork, to healthy occupation, to simple habits, and to a wise mental training.
MORAL INSANITY (Insanity of Action, Affective Insanity, l'Insanite morale, Moralisches Irresein, Folie raisonnante, Folie lucide, Manie sans délire of Pinel), the general moral mania of Ray, is distinguished by that writer from partial moral mania (instinctive mania, manie raisonnante of Pinel, la folie impulsive, impulsive insanity, emotional insanity, impulsives Irresein), which includes suicidal insanity, homicidal insanity, dipsomania, pyromania, kleptomania, erotomania, nymphomania, satyriasis (aidoiomania), animal impulse, perverted sexual instinct (conträre Sexualempfindung, la sensation sexuelle contraire), and topophobia, if that disease be classed among the insanities.
Moral insanity is seldom seen in the insane asylum until the disease has passed over into pronounced mental enfeeblement or delusional insanity. Purely moral insanity—“an uncontrollable violence of the emotions and instincts”—is probably as rare as purely intellectual insanity. Moral insanity is attended with some mental impairment, just as moral perversion is part of intellectual insanity. Indeed, I have heard patients complain as much of the degradation of character in their insanity as of any symptoms referable directly to the intellect. The term is not a fortunate one, but, like the expression moral treatment of the insane, it is in quite general use. It is recognized by all the authorities on mental disease, whatever may be their opinions as to the limitations of responsibility in it. It is especially to it that we can apply the words of the Autocrat of the Breakfast-Table, that the worst forms of insanity are those to which the asylum shuts its doors. It is marked by moral perversion, change of character and action, and so little intellectual impairment as to be easily overlooked by one not familiar with morbid mental phenomena.
Mild simple mania ending in recovery has been described as moral insanity even by Pinel and Pritchard, and is so miscalled rather generally at the present day. Moral deterioration is observed after fevers or physiological periods of life, following slight and moderate cerebral hemorrhages or injuries to the back and head, affecting the brain, mental strain, etc., which, in persons of the neuro-psychopathic constitution, now and then end in permanent change of character. A similar but curable mental state is the frequent beginning of more pronounced insanity, and often remains the sole evidence of unsoundness of mind even after the patient is thought well enough to be discharged from the asylum.
Although moral insanity is probably a common cause of young persons of both sexes being led into lives of licentiousness, wickedness, and crime, it is to be carefully differentiated from deliberate yielding to temptation and following lives of vice until a strong enough motive is offered for doing better or a punishment is made sufficient to be deterrent.
Moral insanity is essentially a very slowly progressive and incurable disease, starting in congenital or acquired mental deterioration, and with its symptoms. It usually ends, after long years of wretchedness to the individual and misery to his friends, in more general insanity, slowly advancing dementia, death by intercurrent disease or accident, or in suicide. It is a most distressing disease in the young, who are punished [p. 144] by parents and teachers in succession, sent about from one school to another, boarded with friends or with disciplinarians until all are wearied out in turn, and all too late conclude that the case is one for a doctor or perhaps an asylum. At the evolution of the sexual power and at its decadence, during menstruation, pregnancy, childbirth, lactation, especially after fevers, blows injuring the brain, and cerebral disease or disorders of any kind, are the periods of especial danger, as more general mental disease is then developed with seemingly trivial exciting causes. The friends observe that the sufferers do not seem entirely natural. They imagine and suspect a great deal, rather than possess real delusions. They often say that their heads are not quite right, and manifest an evidently diminished capacity for mental work, which tires them or makes them irritable. Modest girls become indelicate, the truthful lie, the delicate use profane and obscene language, the mild-mannered destroy furniture and clothing, the peaceful quarrel, the gentle storm and rave; and yet there is a standard of virtue and right, often a high one, on which they theorize, and up to which they often think that they live. They take strong dislikes to those with whom they are brought in contact, especially their nearest relatives. They often lose the capacity to do work, and now and then become spendthrifts or drunkards. As a rule, there are frequent periods of quiet, amounting to depression, but rarely reaching the condition of melancholia. Alternation or periodicity in the symptoms is the rule. After threatening and even endangering the lives of those nearest to them, insulting and indelicate conduct in public, perhaps frequent arrests, a dozen times outwitting those who wish to confine them in asylums, where they belong, their minds being alert enough to attribute their conduct to drink or some cause for which they receive slight punishment, and to argue their own cases so as to convince almost any jury of their sanity, the rule is that their doubts, imaginations, and suspicions deepen into active insane delusions, their mental impairment advances to noticeable dementia, their moral deterioration goes on to such a degree of depravity that every body wonders why they had not been seen to be insane long ago, and they are secluded in an asylum or elsewhere. A not uncommon but unfortunate end is when they kill themselves before anybody but a few specialists recognize their irresponsibility. Their recklessness and want of judgment are often the cause of fatal illnesses and accidents. Clouston reports the case of a lady who by a series of extraordinary misrepresentations and clever impostures raised large sums of money on no security whatever, and spent them as recklessly; imposed on jewellers, so that they trusted her with goods worth hundreds of pounds; furnished grand houses at the expense of trusting upholsterers; introduced herself by open impudence to one great nobleman after another, and then introduced her dupes, who, on the faith of these distinguished social connections, at once disgorged money. To one person she was a great literary character; to another of royal descent; to another she had immense expectations; to another she was a stern religionist. At last all this lying, cheating, scheming, and imposture developed into marked insanity and brain disease, of which she soon died; and it was seen that all these people had been the dupes of a lunatic whose very boldness, cunning, and mendacity had been the direct result of her insanity.
S. K. Towle has reported the case of a man whom he had under [p. 145] his care at the Soldiers' Home near Milwaukee, Wis., as follows: “He had been a lieutenant in a volunteer regiment, and I gave him rather more privileges on that account, but after a time I found that he was more nearly an example of total depravity than I had ever seen. There was no truth in him, and he was intelligent enough to make his lies often seem plausible to me as well as to others. By his writing and talking and conduct generally he kept the patients and their friends in a ferment, and gave me more trouble than the whole hospital besides. He had a small scar about the middle of his forehead, which he said was due to a slight flesh wound from a glancing ball in battle. While he was under my care an older brother came to see him, and he told me that up to the time his brother, my patient, who so tried my patience, entered the army he was almost a model young man, amiable and affectionate, the pet of the whole family and intimate friends; ‘But,’ said he, ‘ever since he came back he has been possessed of a devil if ever any one was.’ After a time, much to my delight, he asked for a transfer to the Soldiers' Home at Dayton, Ohio, which I got for him with commendable alacrity; and he went there. His conduct at Dayton was the same as with me, but after a few months he quite suddenly died, when an autopsy was made. In sawing open the skull, at the point of the small scar on his forehead the saw came directly upon the butt end of a conical bullet, two-thirds of which projected through the skull, piercing the membranes and into the brain. The internal table of the skull had been considerably splintered by the ball, the pieces not being entirely separated, and there was evidence of severe chronic inflammation all around, and quite a collection of pus in the brain where the ball projected into it. Here was the devil that had possessed the poor fellow—that not only took his life, but destroyed his character, lost him the love and esteem of his friends, and doomed him for half a dozen years to do things he would most have hated and despised when he was himself. Dunlap, the assistant surgeon at Dayton, told me that he found in this man's trunk letters from several—half a dozen, I think, at least—women in various places, from which it appeared that he was engaged to be married to each one of them. The letters were neatly tied up in packages, each one's separately, in several instances with photographs supposed to be of the writers, and the date of reception and reply was noted on many of the letters in a business-like way.”
As Westphal well says15 of such persons, “They often think correctly and logically, and show reflection and deliberation to a certain degree; but there is a certain something lacking, and there are some general conceptions, general processes of thought and judgment, of which they are incapable. Their mentality stops short on a certain plane, especially in matters of judgment where every even uneducated person easily succeeds. They sometimes act as if they had good judgment and common sense, of which they are really destitute, particularly in regard to the proprieties of life and their proper social relations and duties. Certain of the finer feelings are absolutely impossible of development in them. Through their various nets, perverted by their mental defect, the patients often seem perverse (bösartig), passionate (leidenschaftlich), although of true sustained passion they are incapable. What seems passion is a sudden idea or fitful impulse to which they yield at once. Moral insanity is a defect in the affective [p. 146] sphere, but also an intellectual defect of a peculiar kind, which is often concealed under the mask of a perverted moral sense, and which requires time and practice on the part of the physician for its detection.”
15 Berl. klin. Wochenchrift, 1878, No. 15.
Moral insanity is quite certain to pursue a downward course, although something can be done by training, general hygiene, simple diet, mental discipline, avoiding overwork, a judicious choice of the few occupations of which the moral insane are capable, and a constant steadying hand to help them try to keep their balance.
IMPULSIVE INSANITY is perhaps more properly called instinctive monomania, as the morbid impulse is usually shown in only one insane propensity at a time. Like moral insanity, its manifestations are commonly periodic, or at least alternating. Under the name of emotional insanity it furnishes sympathetic juries with an excuse for finding not guilty of murder women who kill their betrayers and husbands who shoot a wife's seducer. It is a not uncommon symptom in a considerable proportion of the persons suffering from the various forms of insanity. As a separate disease it is quite rare, and includes those persons whose insanity is manifested, as Marc says, by what they do rather than by what they say. The insane impulse does not come from any logical process. It is rarely provoked by or associated with a criminal motive, except in an analogous way to the production by excitement of an epileptic attack, to which, indeed, it offers some points of similarity. There would be reason to doubt the existence of the disease unless other indications of mental degeneration were present, especially where there is proof of a criminal motive or where the criminal act and the prisoner's statements are the sole evidence of unsoundness of mind. Unconsciousness, even temporary, and loss of memory, are not symptoms of instinctive monomania. On the contrary, the mind is quite clear, and resists successfully the insane impulse so long that the person affected with it has often gained confidence that he will never yield to it; and he soon learns the fact that, there being in circumstances external to himself no reason for the crime suggested to the mind with such force, temptations do not occur to the act. While the impulse lasts a great variety of distressing mental symptoms accompany it, so intense that the impulse often cannot be resisted, and then the terrible brain-tension is relieved. I doubt whether hallucinations of hearing are found in impulsive insanity, and incline to think that all the reported cases where crimes of impulse have been committed in obedience to a voice commanding the individual to do this or that act of violence are more properly classified under other forms of mental disease. One kind of instinctive monomania sometimes disappears to be replaced by another. In developing boys and girls there is not seldom a pathological mental state during which lying, stealing, running away from home, etc. are common for several months or a few years; but this is a curable condition, and does not by any means necessarily end in instinctive monomania.
Suicidal insanity is probably the most common form of instinctive monomania. The force, or even presence, of the suicidal impulse is largely dependent upon the general tone of the system. The suicidal idea is common; it occurs to the minds of a vast number of sane people at one time or another under adverse circumstances. Hysterical women talk a lot of nonsense on the subject. Self-destruction due to [p. 147] self-depreciation, weariness of life, and general gloom is not uncommon in the insane temperament. It is also a refuge to proud and sensitive people who have sacrificed their honor. But this is quite different from suicidal insanity, in which the impulse is often strongest at a time when there are the most reasons for living and the greatest happiness in life if the tormenting demon urging to self-murder could be excluded. Such people finally kill themselves, in spite of their best resolutions and efforts to the contrary, if the various faculties of the mind become more and more involved as the disease goes on and the power of self-control is progressively weakened. More general insanity of the degenerative type is sometimes developed from suicidal insanity.
Homicidal insanity is fortunately still rarer than the last-mentioned form, although motiveless homicidal ideas occur to husbands and wives and parents with reference to those dearest to them, under conditions of prolonged mental strain or exhaustion, during pregnancy and the puerperal state, and at the climacterium. In suspected crimes the evidence of homicidal insanity should be clear and should rest upon the general signs of the degenerative mental state. Homicidal impulses are common enough among the insane. Just as there are persons who do not dare to have sharp instruments in their rooms for fear of killing themselves, so there are others to whose minds axes, knives, and razors suggest imperative conceptions of plans for killing another. It is difficult in either case for the physician to satisfy himself at what point real insanity begins. Seclusion under the morbid influences of an asylum is very bad treatment for the individual, and symptoms which seem very serious often disappear by restoring the general health. In a recent case,16 where a youth of nineteen was acquitted of the murder of his mother on the ground of homicidal insanity, he knew that the act was wrong, realized that he had committed a crime, and was full of grief for it, as occurs in all such cases. It is the rule, too, that there is some condition of mental defect or degeneration out of which the homicidal insanity is developed.
16 Quarterly Journal of Mental Science, October, 1883, p. 387.
Dipsomania, a rare manifestation of impulsive insanity, differs entirely from the acquired alcohol habit, drunkenness, acute or chronic alcoholism, delirium tremens, or habitual intoxication, all of which conditions are also more readily developed in the neuro-psychopathic constitution than in persons with healthy brains, and may reach a point constituting insanity. Dipsomania is periodic, uncontrollable, and associated with other evidences of the insane diathesis. The prognosis is unfavorable. The treatment is to improve the general nervous tone and to seclude the patient during his attacks.
Pyromania and kleptomania are not rare as symptoms of insanity of the marked forms which are observed in asylums. As manifestations of impulsive insanity—that is, as constituting a form of insanity—they are associated with other evidences of mental defect or degeneration. Burning and stealing alone are not indications of insanity. As such, they are without sane motive, and directed to objects in burning or stealing which there is no gain to the person and usually no gratification except the sense of relief which comes from yielding to the impulse, and of distressing mental symptoms if the impulse is resisted.
Nymphomania in the female, satyriasis in the male, and the various [p. 148] perverse and degrading methods of gratification of the sexual instinct, may, when joined with other evidences of mental or nervous disorder, constitute one form of impulsive insanity. Erotomania, an ideal attachment without erotic feeling, is a more common mental disease, but the other evidences of insane conduct are quite striking. The same statement holds true of the many perverted instincts which, according to circumstances, are or are not manifestations of the defective brain-inhibition of disease. Animal impulse as a form of impulsive insanity I had been inclined to doubt until I recently saw two cases of as extreme mental suffering as I ever witnessed, in two refined ladies who had suffered also from some cerebral symptoms, occasional dizziness, and suicidal insanity, but who had no other symptoms of cerebral disorder than those which are grouped under the head of insane diathesis, and they not marked. It is not associated with any erotic feeling or with particular persons. There is more rapid wasting in flesh and strength and loss of sleep than in the other forms of impulsive insanity, and, in my experience, greater dread of yielding to the demon of unrest.
The perverted sexual instinct, with a feeling of repugnance to the opposite sex, has thus far been observed chiefly in persons who have been addicted to masturbation. It is marked by a passion for some individual of the same sex, by other evidences of the neuropathic condition, and commonly by a grotesque imitation of the habits or dress of the opposite sex.
The indications for treatment in impulsive insanity are cod-liver oil, the bromides, simple non-stimulating diet, open-air life, judiciously regulated exercise, mental occupation so far as is possible, and removal from suggestive surroundings and associations. The prognosis is not favorable as to the final result. If the symptoms disappear on restoration of the general health, other marked indications of cerebro-mental disorder are pretty certain to appear sooner or later.
HYSTERICAL INSANITY is one of the states of mental degeneration, much less common among men than among women, arising from the further development of a neurosis, hysteria, and probably to a great extent due to bad training. Hysterical symptoms, quite marked, are very common among young persons and in single women of all ages in simple mania. They are not uncommon in simple melancholia and in other forms of mental disease. They add somewhat to the gravity of the prognosis in these cases. They constitute a group of symptoms which I suppose to be understood by those authors who speak of hysterical insanity as a disease in which the cure-rate is high. But hysterical insanity, as quite distinct from other psychoses, is quite a different matter. It is characterized by extreme and rapid mobility of the mental symptoms—amnesia, exhilaration, melancholic depression, theatrical display, suspicion, distrust, prejudice, a curious combination of truth and more or less unconscious deception, with periods of mental clearness and sound judgment which are often of greater degree than is common in their families; sleeplessness, distressing and grotesque hallucinations of sight, distortion and perversion of facts rather than definite delusions, visions, hyperæsthesias, anæsthesias, paræsthesias, exceeding sensitiveness to light, touch, and sound, morbid attachments, fanciful beliefs, an unhealthy imagination, abortive or sensational suicidal manœuvres, occasional outbursts of violence, a curious combination of unspeakable [p. 149] wretchedness alternating with joy, generosity, and selfishness—of gifts and graces on the one hand and exactions on the other. The mental instability is like a vane veered by every zephyr. The most trifling causes start a mental whirlwind. There is no disease giving rise to more genuine suffering or appealing more strongly for the sympathy which, freely given, only does harm. One such person in the house wears out and outlives one after another every healthy member of the family who is unwisely allowed to devote herself with conscientious zeal to the invalid.
The PROGNOSIS is unfavorable. While the symptoms may be alleviated and a nominal cure may be effected, a relapse or the development of some other troublesome form of insanity or neurosis is the rule, to which the exceptions occur for the most part in women in whom there is also some serious curable uterine disease or a state of excessive physical prostration which can be relieved.
The TREATMENT of hysterical insanity demands tact and educating power which will tax to the utmost the ingenuity of the wisest physician. Sympathetic friends, and sympathy in general, are useful in moderation, but they oftener do great harm, because they are excessive; and the care which does good is that which, while being kind and firm, tends to develop strength and character. The will and the imagination are so extraordinarily powerful that their wise direction and government constitute the most important part of successful treatment. Diversion, occupation, and the development of self-control, with careful attention to the general laws of health, are quite important. The temptation to use drugs is, like the fascination of being pitied and petted, very great, as alcohol, chloral, or opium often acts like magic for the time being, and there is generally a craving for one or all of them. But they are utterly demoralizing in the end. The habitual use of stimulants and narcotics in such cases only increases the evil. The fact must be recognized that the hysterical insane are often least responsible where they seem most so, and that they must be treated with unending patience, kindness, gentle firmness, and a wise ignoring of most of the symptoms. Simple palliative sedatives which cannot do harm must sometimes be used, but the general rule, the less active treatment the better, is safest. In the few cases where benefit has been got from removal of the ovaries, healthy or diseased, the improvement, if it shall prove to be lasting, will probably be attributable to the great physiological shock from the operation rather than to any relation of the ovaries to the disease. Removal from home is usually advisable for a time at least—often it is necessary; and if residence in an asylum is not thought to be wise, properly-selected hydropathic establishments or private asylums are useful. Living in a judicious physician's home is desirable when a suitable one can be found. In an asylum a rational letting-alone treatment is found to be the most successful. If the patient remains at home, hired nurses should be in charge of the patient, or at least not members of the family. Safe seclusion will be found necessary for the few who will not otherwise be prevented from committing crimes and offences of startling ingenuity or conspicuous publicity.
EPILEPTIC INSANITY arises from a neurosis, epilepsy, which almost inevitably ends in mental deterioration of greater or less degree, from scarcely noticeable impairment to complete dementia. The insanity may [p. 150] be a continuous state; it may be subsequent to the epileptic attack, or precede it, or take the place of it. Epileptic dementia is more nearly allied to idiocy than dementia following other mental diseases, and it is associated with a degree of moral perversion and brutality which is quite uncommon in other dementia. The insanity following or preceding the epileptic attack is attended with stupor, delusions of persecution, confusion, transitory fury, or a condition quite analogous to somnambulism or cerebral automatism; and the same may be said of insanity replacing the epileptic attack, except that the most common condition in it is a violent maniacal fury, with unconsciousness, and subsequent nearly if not quite complete amnesia. The forms of mental impairment are progressive in the vast majority of cases. The other forms are more amenable to the usual treatment of epilepsy, and sometimes diminish in severity as the disease advances and the mind becomes weakened. In the fury which takes the place of the epileptic convulsion there is in nearly every case—I am inclined to think in all cases—an intellectual aura, a slight change of action, observable early enough to give warning of the approaching storm, which can always be mitigated, and often entirely prevented, by absolute rest in bed and the use of chloral and the bromides.
Although some few epileptics become well without treatment, and a small number permanently recover under treatment, the PROGNOSIS is even less favorable for the epileptic insane. The care of insane epileptics should embrace, in the first place, safety to the community by secluding those dangerous to it, and, second, the usual hygienic and medical treatment of epilepsy.
Epileptic vertigo, analogous to petit mal, is a transitory mania, often associated with passing delusions.
With regard to the responsibility of the epileptic insane—and, indeed, all epileptics—the facts should be borne in mind that their mental state is usually one of such instability that a slight irritation of any kind is apt to induce a full or modified convulsion, and that under provocation they commit partly volitional crimes, for which they are not fully responsible.
HYPOCHONDRIACAL INSANITY differs only in degree from hypochondriasis, described on a subsequent page. It is an incurable manifestation of one type of the mental degenerations. It is slowly progressive, and often ends in dementia. It differs from hypochondriacal melancholia in being an evolution of mental defect or degeneration, and in the fact that the mental depression, which is usually of a mild, periodic, or impulsive form, is secondary to the other symptoms, and not, as in hypochondriacal melancholia, the mental condition out of which the hypochondriacal symptoms are evolved.
The TREATMENT consists in attention to the general laws of health, occupation, and a fattening diet. It is seldom successfully managed without occasional recourse to an asylum at least, and oftenest a permanent residence in hospitals, occasionally changing, is quite necessary.
PERIODIC INSANITY, usually mania or melancholia, is marked by attacks recurring at more or less regular intervals, with a partial but not complete return to the previous mental health between them. It is one of the incurable degenerative mental diseases. The seeming recovery is only apparent, and the mental deterioration is progressive, although quite slow. The form of insanity is also not seldom a folie raisonnante (affective [p. 151] or moral insanity) with periods of all sorts of excesses, destructive tendencies, tramp-life, destructive acts, drunkenness, stealing, indecent exposure, etc. In the intervals, which may be short or long, and which sometimes correspond to certain seasons of the year, the mental condition is still a pathological one, with the usual signs of mental degeneration, thereby being differentiated from recurrent insanity, one of the curable psychoneuroses, in which there is a state of mental health between the successive attacks, but no sort of regularity or periodicity in the recurrences. The prognosis is unfavorable, except in so far as a quiet life in an asylum tends to prolong the intervals between the periodic outbreaks, as well as to prevent annoyance to the community during them.
CIRCULAR INSANITY (Alternating insanity, Folie circulaire, Folie à double forme, Folie à formes alternes, Die cyclische Psychose, Das circuläre Irresein) consists in a psycho-rhythm or succession, in uniform order in each particular case, of (1) mental exaltation in all degrees, from mild exhilaration or even gayness to acute mania, and (2) mental depression of all conditions, torpor, or anergic stupor. These two opposite mental conditions are separated in the vast majority of cases by a shorter or longer interval of the normal mental state, in which, however, there is soon observed some mental impairment, however slight, rarely amounting to pronounced dementia except in old age. Sometimes the three states shade off into each other, so that it is difficult to say just where one begins and the other ends; less often the transition is abrupt, sometimes during sleep. The interval between the two opposite conditions of mind may succeed either of the other mental stages, but the order once established is maintained. The duration of the vicious circle varies in succeeding attacks, sometimes becoming longer, sometimes shorter, in the progress of the disease. The relative duration of the three succeeding mental condition also varies, but the type of each remains identical, or at least changes very gradually. The state of mental exaltation often resembles moral insanity, with all sorts of immoral impulses and tendencies, and may then properly be called an insanity of action. The depression sometimes goes no farther than sluggishness of will. The tendency of the disease is to shorten life only slightly, if at all, except from the chance of suicide in the depressed state and from exhaustion when the excited stage is one of active mania. The shortest duration of the cycle in my experience has been twenty-four hours, and the longest reported extends over several years. It sometimes remains an affective insanity in its whole course, without delusions and with little more dementia than might happen from simply a corresponding advance in age without mental disease.
During the period of excitement some supervision or control will usually be desirable, and removal to some retreat or asylum will often be necessary. In the depressed stage the indications are to maintain the general health, to meet the chances of suicide, and if there are delusions to obviate the risks of danger to other persons. If the interval of comparative mental health is of considerable duration, the ordinary occupation of the patient can commonly be followed at that time for a number of years, rarely for life; but a better result may be looked for if the patient's circumstances are such that he can give up active and anxious work for some quiet occupation not involving great care.
PRIMARY INSANITY (primäre Verrücktheit, primordiale Verrücktheit, [p. 152] originäre Verrücktheit) is usually a further development of an hereditary predisposition to mental disease. The term primary monomania, although used as an equivalent for primäre Verrücktheit, seems to me too narrow for a disease in which the leading delusion may change so many times. Primary insanity is sometimes congenital, and may be developed also by injury or by disease involving the brain early in life or during the physiological changes at puberty, possibly by self-abuse, in persons of an unstable mental organization. It often develops so slowly with the character as to almost seem part of it, until it reaches such a degree of insane delusion of self-importance and expansive ideas as to be unmistakable insanity. There are also delusions of persecution, distrust, and suspicion, erotomania, and moral perversion, in spite of high claims to superior character, and indeed in spite of a high standard of life in some particulars. Perhaps the most striking symptom of primary insanity is the great variety of imperative conceptions (Zwangsvorstellungen) by virtue of which the individual is impelled, by a force often irresistible, to commit various offences against propriety and the laws, even to murder, as well as to perform countless acts of unwisdom or folly. There are usually physical indications of chronic or old cerebral disease, or of defect or degeneration in the incomplete or asymmetrical development of the brain, which, however, may be no more than are found in persons who might not be classed as of unsound mind. Attacks of simple mania (mental excitement) of short duration are quite common, and there is a progressive impairment of the higher faculties of the brain—those which come last in a high order of civilization—although there may be acuteness of memory, perspicacity, and shrewdness which seem altogether phenomenal as compared with the other mental qualities. There is no form of mental disease which is better expressed by the word craziness than primary insanity, no other in which the victim is more thoroughly in the grasp of his malady, and yet no other in which he is more likely to be held responsible for the crazy acts which he may perform, because his inherent mental state, out of which his generally deluded frame of mind is evolved, gives rise to delusive ideas of such a character that they are not universally recognized, even by physicians of experience in mental disease, as insane delusions, but are considered by some of them as the prevarications of a criminally-minded person. When these persons commit crimes, too, they often do so with methods and motives quite like those of the ordinary criminal.
The PROGNOSIS in primary insanity, after the disease is fully developed, is in the highest degree unfavorable. It remains to be seen how much can be done by moral training in childhood and youth to correct the evil tendency. The education of those who get into the courts and insane asylums, so far as my knowledge of such cases goes, has been bad to the last degree, so that, in my opinion, there has been a fair difference of opinion as to which of them the law should treat as criminals and which as insane persons.
TREATMENT for the most part requires absolute control of the individual, which there is usually no one in the family sound enough to maintain. If begun early, training away from home may accomplish much. Restraint in some institution is commonly called for, but the vast majority of the primary insane are allowed to take their chances in [p. 153] the world, and as many end in jails and prisons or on the scaffold as in asylums.
The states of mental defect and degeneration, except in the case of idiocy or marked imbecility, are not associated with such obvious physical evidences of deviation from a normal mental standard as to make them pathognomonic. While asymmetry and other cerebral defects are frequently observed in them, it must be acknowledged with Schüle that similar and as extensive gross intracranial anomalies are found in persons who could not be called of unsound mind, and that this statement holds true even of primary insanity, in which some writers have laid so much stress upon the value of any indication of imperfect or asymmetrical cerebral development. Any defect in the brain, however, is far more common among persons of unsound mind than among those of sound mind, and therefore in doubtful cases it is of a certain value as corroborative evidence of mental infirmity or impairment.
Spitzka places as signs of the insane constitution (1) atypical asymmetry of the cerebral hemispheres as regards bulk; (2) atypical asymmetry in the gyral development; (3) persistence of embryonic features in the gyral arrangement; (4) defective development of the great interhemispheric commissure; (5) irregular and defective development of the great ganglia and of the conducting tracts; (6) anomalies in the development of the minute elements of the brain; (7) abnormal arrangement of the cerebral vascular channels,—at the same time acknowledging that there are cases of insanity of inherited origin in which cerebral defects are not discernible. It is too early to estimate the value and importance of the finer or qualitative cerebral defects as giving rise to insanity. Benedikt finds them also in criminals.
With regard to responsibility before the law, the statutes of no country provide for any criterion by which accountability is defined in these cases; medical witnesses differ in opinion as to their criminality, and the courts are obliged to interpret the law to suit individual cases.
The states of mental defect and degeneration are not sharply defined. They run more or less into one another. The fact should also be kept in mind that isolated symptoms and groups of symptoms belonging to them are repeatedly found in curable conditions of physical and mental exhaustion in neurotic persons.
The degenerative mental states are thought to be increasing, to furnish material for the increase in the otherwise curable insanities, and to thus include much of that portion of the community which is most filling up our institutions with incurable cases. It is probably in the prevention of them, or at least in the proper training and disposition of children affected with them or predisposed to them, that the most can be done to stay the increase of insanity. Perhaps at some time unwise marriages of passion and sentiment will be less common than now, and the rights of children to a fair start in life more considered.
AFFECTIVE MENTAL DISEASE is a folie raisonnante, one of the reasoning insanities, sometimes called moral insanity, and very like the moral [p. 154] insanity already described, except in the absence of signs of mental degeneration and in the fact that it is a curable disorder. It is an insanity of action, marked by scarcely noticeable mental impairment. It often is the early stage of more serious mental disease, and not seldom its symptoms remain, as simply change of character, after the striking symptoms of extensive mental disorder have disappeared. It also exists and is cured without the appearance of more pronounced insanity. At the time of the climacteric it is a form of mental disorder not uncommon among women, who, however, usually fail to recognize it as such until they have recovered. Maudsley includes under this head simple melancholia, simple mania, and moral alienation, but it will be more convenient for the present purpose to use the term affective mental disease as indicating a curable moral alienation or change of character affecting the intellect chiefly so far as the judgment and sense of propriety only are concerned, and not dependent upon constitutional defect or developed degenerative mental state. There is usually slight exhilaration or depression, which alternates or varies from time to time.
The PROGNOSIS is favorable.
The TREATMENT is brain-nutrition, with those general measures already described.
HYPOCHONDRIASIS, as Flint17 well says, belongs in the list of disorders of the mind, although the mental alienation is not regarded as amounting to insanity. The mental state is one of morbid imagination and apprehension rather than of definite delusion, and it consists in a belief in the existence, present or to come, of maladies and diseased conditions for which there is no foundation in fact, in spite of sufficient proof of their unreality. There is usually, not always, mental depression. Its causes lie in conditions, usually obscure, which lower the tone of the general health, including hereditary weaknesses, or depress the vitality of the brain either by physical wear or mental worry, and the exhausting influence of functional disorders or of organic diseases which may not be discovered before the autopsy. Disappointment, bad habits, want of proper mental occupation are often at fault.
17 Practice of Medicine, p. 854.
The physical symptoms of hypochondriasis are commonly those associated with impaired digestion and nutrition—namely, anæmia, dyspepsia, neurasthenia, constipation, flatulence, headache or a feeling of discomfort after using the brain, less appetite, slight loss of flesh, disordered sleep.
The mental indications are more or less melancholy, indisposition to exertion, irritability, diminished power of self-control, and an inability to cease except temporarily from interpreting signs, proved to be trivial, as indicating grave maladies or as forewarnings of severe disease to come. Sometimes the fixed idea is limited to a single false conception, but oftener slight changes in physical symptoms or differing phases of morbid introspection produce a complete kaleidoscope of pictures of fancied misery. The whole catalogue of diseases, or a large part of it, may be exhausted, with the help of some of the many foolish treatises always ready for hypochondriacs or from reading medical books and talking with charlatans, who are consulted at rapid intervals, one after another, both by those who wander from office to office and those who take to their beds. The most common type of hypochondriasis arises, directly or indirectly, [p. 155] in some form of unhealthy or false ideas regarding the sexual function, and in the idea that some imagined or exaggerated abuse of it has produced or will produce most serious evils; but there is not an organ of the body which may not be the basis for the unwholesome thoughts. Not seldom there is simply the delusion of especial weakness or sensitiveness or delicacy.
Hypochondriasis may be only the early stage of more serious mental disease. It may be one manifestation of an hereditary neurosis or psychoneurosis, or it may arise from deterioration of the body's vitality by organic disease, especially of the abdominal or pelvic organs or through some incurable weakness or functional disorder. In either of these cases its cause and duration will be determined by the clinical history. As an uncomplicated psychoneurosis hypochondria lasts from a few months to a number of years, with very little change in its prominent symptoms, resulting in recovery for the most part, becoming chronic in a moderate proportion of cases, and rarely proving fatal except by some accidental complication, including suicide.
The PATHOLOGY AND MORBID ANATOMY of the disease are unknown.
The differential DIAGNOSIS consists in the exclusion of other diseases.
The PROGNOSIS is favorable in uncomplicated cases.
TREATMENT consists in measures to improve the general health, especially a full diet carefully selected, hydro-therapeutics, massage, gymnastics, horseback riding, walking, rowing, abundant and agreeable exercise in the open air, and the management of the patient's surroundings so as to lighten the mind and relieve from worry, perhaps by travel, sea-voyages, etc. Argument is commonly worse than useless, but there should be a decided impression given that the generally morbid state is due to ill-health. The risk of suicide is so small that restrictions of liberty directed to its prevention do more harm than good. It goes without saying that bad habits should be reformed, narcotics should be avoided, and a healthy occupation should be encouraged, or, if possible, insisted upon. The difficulties in treatment are fully as great with the highly-educated superstitious and credulous people whom we find in the literary and professional circles as in the ignorant and weak-minded.
MELANCHOLIA (Die Melancholie, Schwermuth, Tiefsinn, Trübsinn, Lypemanie, Mélaneolie, Aliénation partielle depressive, Monomanie triste, Phrenalgie, Psychalgia) is one of the functional mental diseases, in the sense that the pathological condition of the brain upon which it depends is not yet known, although it is thought to begin with disturbances in circulation and nutrition, which end, if not resulting in cure, in atrophic, degenerative, and inflammatory states, indicating, in the great majority of cases, extensive brain disease. As a rule, melancholia first appears in a slight change of character; the patient is said by his friends to be not quite like himself. After some days or months, as the case may be, the symptoms develop into settled gloom associated with mental pain—the state known as
Simple Melancholia (Mélancolie raisonnante), in which the events of life are correctly observed, but, incorrectly interpreted, are the source of constant apprehension, self-depreciation, depression, and despondency. There are no delusions, properly speaking, and yet there is a disposition to take the dark-side view even of circumstances which promise [p. 156] favorably, which amounts to a generally deluded state of mind. Commonly there is increased irritability, now and then a genuine moral insanity, and occasionally in neuropathic constitutions the state of mind already described under the head of Impulsive Insanity, of which the suicidal impulse is the least infrequent. Sometimes there are no physical indications of disease, but as a rule there are headache, increased sensibility to light and noise, sleeplessness, restlessness, impaired appetite and digestion, gastro-intestinal catarrh, marked loss of flesh, diminished or abolished sexual desire, and in women usually delayed menstruation or amenorrhœa. A few persons are able to keep up, in an irregular sort of way, their customary employment. In the majority of cases it is impossible to concentrate the mind upon work, mental occupation fatigues the brain, and the physical strength is too impaired for steady labor. Suicide is thought of probably in nearly every case, as it is by many sane people at some time in their lives, but it is very seldom committed unless there are such disgraceful or distressing acts performed or suffered by them as would tempt to suicide in sane people. There is no danger of deliberate homicidal acts in persons of good character. A criminally disposed person would more readily commit murder in simple melancholia than if free from that disease.
Simple melancholia may be the initial stage of almost all of the mental diseases, especially acute mania, paralytic dementia, and the severer forms of melancholia. It may be differentiated from the first stage of mania only by waiting until other symptoms appear or not, and the same is true with regard to distinguishing it from the forms of melancholia involving danger to life. In the latter case, however, there is much greater difficulty in diagnosis, inasmuch as insane delusions may be concealed, and there may be so slight a change in the patient's behavior when delusions appear in his mind that the closest observation is needed to guard against them. The simple melancholia marking the first stage of paralytic dementia is characterized by noticeable although often slight mental impairment—a distinctly diminished capacity for work, of which the individual himself is not seldom conscious, whereas in the disease simple melancholia the mind's usual power is exerted, provided its attention can be withdrawn from morbid introspection and concentrated upon any subject, as it commonly can be for a while.
Melancholia with delusions (acute melancholia) is commonly a further development of simple melancholia, but sometimes its course is so rapid that if there is a period of mental depression without delusion it is overlooked. The earliest and most common delusion is some form of causeless self-reproach with regard to some matter, whether trivial or important, or of groundless self-accusation, of impossible sins of omission or commission, but generally of some vague, undefinable fault, as having irretrievably offended God or committed the unpardonable sin, etc. Often this and an unfounded belief in self-unworthiness are the only delusions present, and in that case within narrowed limitations the mind acts soundly in other matters. The feeling of personal fault or sin often expands to a sense of the justice of punishment, and the consequent delusion that all sorts of terrible things are to happen—poverty, the poorhouse, or some great unknown dread, even involving family and friends; and from personal sin or fault it is only a step to the belief [p. 157] that the world is all wrong, and to the certainty that everything is going to worse than ruin. Illusions of sight and hearing may magnify common fires and locomotive whistles into general conflagrations of the world and shrieks of tormented persons. Hallucinations of the special senses may create visions of all sorts of imaginary horrors, sounds of voices saying every possible dreadful thing, odors most disagreeable, tastes most vile. Anæsthesia prompts the delusion of death, and hyperæsthesia of burning, freezing, scalding, etc. Some mysterious force within them, which they can neither explain nor understand, drives them to automatic acts of all kinds—to obscenity, profanity, verbigeration, intonation of sentences, wailing, screaming, destructiveness, etc. In cases of exceptional severity the mind seems deluded on almost every subject: the food is poisoned, the atmosphere is deadly, the world loses all its reality, friends their identity, things their substance. They are to be burned alive, starved, quartered, suffocated, smothered, drowned. Every conceivable and inconceivable thing is to happen. The delusions are nearly always of the illogical or unsystematized kind, although systematized delusions of persecution are met, for the most part, in incurable cases. Deliberate plans of suicide are formed in most cases, and are to be suspected in all. Homicidal attempts are apt to be made upon persons whom it is desired to save from impending calamities. Suicidal, and less often homicidal, impulses occur. Suicide and homicide from deliberation need, to be successful, (1) the opportunity, (2) lack of power of self-control, and (3) a strong determination. Sometimes there is the will without the opportunity, or the opportunity with self-control; and for this reason persons in danger of killing themselves or others often for months escape any acts of violence. Not seldom, too, they determine to kill themselves or family in a particular way, and neglect other chances so long that they are thought to be not meditating destruction of self or others. When the determination or impulse to suicide or homicide is persistent and desperate, no means are too horrible and no opportunities too hopeless to be attempted. There is no reason for a special name for these symptoms, but they have been called suicidal melancholia and homicidal melancholia. No more is there any justification of the term hypochondriacal melancholia for melancholia with hypochondriacal symptoms.
In melancholia with delusions there is sooner or later, in the majority of cases, refusal to eat, from lack of appetite, nausea, or disgust of food, from disagreeable hallucinations of taste or smell, from delusions that it is a sin to eat, that the stomach is full, that the mouth is sealed or the throat obstructed, that the food is not and cannot be paid for, that eating will do no good, etc., from a wish to commit suicide by starving, or in the states of stupor (attonitäts-zustände) from mental torpor or stupidity. Sometimes there is resistance to the calls to eat, urinate, or defecate by virtue of resistive melancholia—a condition to resist and oppose everything—or from delusions that it will destroy the soul, etc. to follow the natural inclinations. Refusal of food may be under certain conditions instinctive and conservative. It is the exception for the bodily functions to be well performed. Usually, there is obstinate constipation, with headache, coated tongue, greater variation in daily temperature than is usual in health, accelerated pulse, and rapid wasting in flesh. The various anomalous sensations observed in functional diseases of the nervous [p. 158] system are common. Masturbation is a not infrequent symptom of loss of self-control in both sexes.
Acute melancholia is sometimes confounded with delusional insanity with mental depression. In the former the delusions are evolved from the mental state; in the latter, the mental state from the delusions. In the former the delusions are for the most part unsystematized: the patient cannot state why he believes them to be true; in the latter there is correct reasoning from false premises: the delusions are logical or systematized and of a depressing character, so that a belief in them naturally gives rise to sadness.
Before the courts the fact should be kept in mind that persons with acute melancholia have diminished power of self-control by virtue of their disease, and so yield more readily to temptation than in health. They also may have imperative conceptions—ideas so strong that they cannot, or can with difficulty, resist carrying them out even when they know them to be wrong; and there may be sudden outbursts of almost maniacal excitement. They are often able to make wills and perform contracts, in form and in detail, as well as ever, when they are so filled with insane delusions as to be on the point of killing themselves and their families. There is impaired capacity, however, of recognizing the relations of persons and things to one another, a distinct moral perversion, and a diminished recognition of obligations and sense of responsibility. In other words, they are not always fully themselves on those points in which they seem to be so, and yet patients in asylums with acute melancholia have been known to give the best of advice to their business-partners.
Melancholia with stupor (melancholia attonita) appears like complete dementia or a mindless state, but there are now and then evidences of intelligence. The mind is filled with overwhelming and terrible delusions, which paralyze the will and place mental and physical activity for a while in abeyance. It arises commonly in the course of the less profound form of melancholia, after some great mental shock, and there is a condition of marked anæmia of the brain, probably symptomatic rather than pathognomonic, which if not soon relieved goes on rapidly to atrophy and degeneration. Except when there are attacks of frenzy, which may occur at any time, there is little danger of active violent acts except suicide, desperate refusal of food, and determined resistance to any care or treatment. There are the usual indications of physical exhaustion.
In melancholia agitata the mind is clear and active, the opposite of the condition last described, and the distressing delusions produce such a degree of motor excitement arising from the mental suffering that the disease closely simulates acute mania. The mind not only reacts as readily as in health to distressing ideas, but abandons itself more fully to their domination through diminished will-power and lack of self-control. Almost blind acts of desperation and fury are committed from which the utmost vigilance can hardly save them.
The three severe forms of melancholia just described are interchangeable in the same person during the course of his illness, so that the states of frenzy and stupor are more properly called symptoms than classes of disease.
Melancholia among children is more common than the books state it to be, although rarely met in the asylums. Magnan has reported a [p. 159] suicidal case in a child four years old, and it occurs up to the latest years of life.
The DURATION of simple melancholia is from a few weeks to a dozen years; of acute melancholia, from a month to two or three years, after which it is apt to end in chronicity; melancholia stupida (with stupor) is usually curable, if at all, in the first year, although relapses are frequent, and in melancholia agitata from a year to three years is the common limit of the possibility of a cure.
The PROGNOSIS in simple melancholia is favorable. Including cases treated out of asylums, probably 90 per cent. recover; in acute melancholia, uncomplicated with other diseases, not far from two-thirds recover; in melancholia attonita less than half get well; and in melancholia agitata nominal recovery occurs perhaps in a third of the cases, although I doubt whether complete restoration to health is seen often.
In chronic melancholia the process of mental deterioration is slow. As the mind becomes impaired the delusions lose their activity and the mind reacts less readily, so that a state of less suffering and greater calm is reached, and the patients are often useful workers in asylums for many years, or remain in their own homes a constant source of anxiety to those who understand their condition. Many of them commit suicide.
In treatment of melancholia the first indication is to protect society and the individual against acts of violence. Homicidal acts are not to be feared in simple melancholia, unless in persons of bad character and ugly temper, or in those few cases with the symptoms, in addition, of moral insanity or impulsive insanity. Suicide is so rare that precautions will not often be needed against it, provided the patient is so frank or so transparent that the appearance of distinct delusions may be detected and then guarded against. In cases of long standing, especially in persons beyond middle age, this is extremely difficult, and their treatment outside of asylums must always be attended with risk. In the other forms of melancholia the fact should be taken for granted that the patient is suicidal, and he may be also homicidal, so that he should be watched constantly and efficiently, and never left alone or with weak or helpless persons, no matter how free from suicidal determination or impulse he may have appeared. The puerperal mother, especially, is a source of the greatest danger to her child, even when she seems natural and fond. The degree and kind of watching varies, according to the severity of the case, from the constant presence or close proximity of some responsible person, who may sleep in the same room with the usual home-surroundings, to the most vigilant and wakeful personal care every moment day and night, and removal of every source of possible self-injury. In some few cases this can be well done only in an asylum or in a padded room. Some form of restraint, either personal or by confining or limiting the movements of the hands in rare cases of exceptional desperation, will be found necessary.
Placing the patient in an entirely healthy atmosphere is next in importance. In the very earliest stage quiet, recreation, change of scene, and association with a pleasant and judicious companion are often sufficient to effect a cure. If the disease is pronounced, rest and removal from sources of irritation are more important until convalescence, when travel may be tried. The question of removal from home and commitment to an asylum [p. 160] should be decided upon the grounds already stated in considering the general treatment of mental diseases. The degree in which the patient should have exercise, occupation, and recreation or be let alone will be determined for each individual case. The fact should be borne in mind that the disease is a debilitating one, and that it arises in conditions of mental or physical exhaustion. Massage and a modified rest-cure, without seclusion, are beneficial in some cases, especially of elderly people. Baths and the cold pack should be used with discrimination. Electricity, where it does not give rise or add to delusions, is a useful tonic, especially in passive cases. There are very few patients of such desperate frenzy as to require confinement of the hands, and that should only be done with an attendant close at hand. Whatever is done, nothing should be attempted which excites delusions unless it be absolutely necessary. Fresh air, and an abundance of it, are very important. Experience and careful study of the particular case will be needed to know how far to press the taking of food. But the necessary amount should be given by the stomach-tube if ordinary means fail, and it is better to use it early rather than tire the patient out with ineffectual attempts with spoons, etc. Whether the nasal or œsophageal tube be used—of which I prefer the latter—the greatest care should be taken not to inject food into the lungs, the throat being so devoid of sensitiveness sometimes that the tube may be passed into the trachea. Nutrient enemata may be relied upon for a week or two if the patient is in bed, but no longer.
Tonics are indicated—cod-liver oil with bark, the hypophosphites, dilute phosphoric acid, malt. Strychnia, iron, and quinine should be used with caution, as they often cause disagreeable headache with indisposition to sleep. Fattening food will be found useful in most cases. The few fat melancholies need nitrogenous food and graduated exercise. Constipation will be corrected in many cases by a full, laxative diet, cod-liver oil, malt, or it may be beer. Mineral water or Sprudel salts are usually indicated. A pill containing aloin, strychnia, belladonna, mastich, or even colocynth or podophyllin, may be needed in obstinate constipation.
Medicines to control restlessness and sleeplessness should be avoided if possible. Hydrate of chloral, opium, bromides, valerian, sometimes increase the difficulty, and the objections to their prolonged use are obvious, and yet they must sometimes be used for a time. The bromides, with cannabis indica, valerianate of zinc, camphor, and hyoscyamus, may serve an excellent purpose for a time. Opium and its preparations, where they agree, act like magic in producing mental calm and sleep. They may relieve constipation and increase the desire for food, but the danger of the opium habit is so great that their use should be decided upon only in extreme cases, and the effect should be watched from dose to dose, each one of which should be given under medical direction. Wilful masturbation, one of the signs of loss of self-control which occurs in the best of people, cannot be corrected by drugs or appliances, but only by constant watching and by placing the individual where his self-respect, as soon as it can be appealed to, will keep him from it. If it is uncontrollable and symptomatic, fresh air and exercise, and, if necessary, bromides or opiates in moderate doses, with a tonic (not iron), should be used.
[p. 161]MANIA (Manie, Exaltation générale), according to Morel, meant, in the original Greek, folie or madness, while Esquirol derives it from the Greek word meaning moon, making the words maniac and lunatic equivalent. The word mania is still used in this loose way, even by writers on mental disease, as a synonym of insanity. Its use is properly restricted to conditions of mental exhilaration or excitement with motor activity. The morbid anatomy of the disease is not yet made out, and the indications of hyperæmia observed in the acute stage after death are no greater than are found in diseases in which mania is not a symptom. In its final stages atrophic, degenerative, and inflammatory signs are abundant and well marked.
Simple mania18 (manie sans délire, manie raisonnante), an exaltation of the mental faculties similar to the exhilaration produced by too much wine, with an accelerated flow of ideas, impaired judgment, and motor activity, without definite delusions, delirium, or incoherence, has been called an insanity of action, affective insanity, folie raisonnante, and even moral insanity, from which it differs in being marked by constant mental elation and exaltation of the physical functions, and not necessarily by striking moral perversion. It is a mental erethism, an exaggerated gayety, an uncontrollable exhilaration, an unbounded joy, an excessive anxiety, a perpetual anger, unusually good spirits, increased intellectual and physical energy, with such striking loss of self-control, diminished powers of reflection, and so decided weakening of the judgment that all sorts of unwonted errors of commission or omission may be performed. Under its influence many fortunes have been lost, many reputations have been ruined, and the happiness of many families has been sacrificed before the existence of insanity was suspected, except possibly by a very few persons. Indeed, the wit is usually so sharpened, the flow of ideas often so clear and rapid, the capacity for brain- and body-work without fatigue is generally so increased, that not seldom the patient is remarked upon as being unusually well. The most troublesome symptoms arise from the tendency to squander property, to drink alcoholic liquors to excess, and, especially in women, to allow the exalted sexual desires to get control of the judgment and reason, thereby bringing about unfortunate marriages or scandalous relations with the opposite sex. In women there is commonly increased menstrual flow.
18 Also called by some writers moral insanity, folie morale, folie des actes, folie or manie instinctive.
The course of the disease is without material change, and the duration is from several weeks to a number of years. When it does not constitute the initial stage of other types of mental disease, especially severer forms of mania, circular insanity, general paralysis, or (in the neuropathic constitutions and at the critical ages) mental degeneration, the termination is in recovery in about 90 per cent. of the cases, although sometimes some moral impairment or deterioration in character remains for life. The recklessness incident to the disease leads to unusual risks, now and then to fatal accidents. Simple mania rarely becomes chronic.
TREATMENT involves the necessity of proper control to prevent scandals, disasters, and perhaps crimes. The matter of the degree of seclusion and control should be governed by the general considerations already mentioned in the general treatment of insanity, bearing in mind that [p. 162] repression of the motor energy, except to prevent exhaustion, does harm. The demand for food is enormous; its supply should be abundant and judiciously chosen with reference to easy digestion. Frequent prolonged warm baths and cool applications to the head are indicated, and the usual palliatives for headache, sleeplessness, constipation, etc. The surroundings should be such as to favor rest and undisturbed sleep, and to dispel sources of excitement, whether they arise in certain associations, localities, occupations, or persons.
Acute mania (Tobsucht) follows an incubative stage of simple melancholia, often of simple mania, and rarely bursts out without previous indications of disease. Delusions, unsystematized and illogical, are abundant; the ideas flow so rapidly that the mechanism of speech is not adequate to their expression; the motor excitement is intense. In the most severe forms there is mental confusion, delirium, incoherence of ideas, and furious muscular action, to the point often of acts of destructiveness and self-injury. The clothing is torn to shreds, and no act of violence is too wild not to be attempted without warning. The skin is hot, the tongue heavily coated, the pulse accelerated, the temperature elevated, more, probably, than would be accounted for by the physical activity—from one to two or three degrees—now and then, in conditions of exhaustion, a little below the normal. Just as there is liable to be maniacal frenzy in the course of severe melancholia, so in acute mania outbursts are seen of desperately suicidal melancholic frenzy. Unless great care is used to keep up the strength, and often in spite of it, exhaustion rapidly sets in, under the influence of which the symptoms are very much aggravated. The amenorrhœa in women in this condition is conservative.
The COURSE AND DURATION of acute mania vary within wide limits, with an average of not far from six months, with recoveries in about 60 per cent. of first cases uncomplicated by pneumonia, chronic disease, or a marked neuropathic state: 5 or 6 per cent. die, chiefly from pneumonia, phthisis, accidents, or exhaustion, seldom suicide. Incurable cases drop slowly into dementia or into chronic delusional insanity, the motor excitement subsiding. The delusional insanity may be simply a stage in the process toward dementia.
In the DIAGNOSIS of acute mania, unless great care is used, the physician sometimes finds that he has sent to the asylum a case of acute, especially infectious disease, in the early stage and with unusual manifestations of febrile delirium. The indications for avoiding this unfortunate mistake are care and time in making diagnoses.
In the TREATMENT of acute mania the matter of foremost importance is that the physician should be able to sufficiently control his patient to prevent harm, and that he should have him in such a place as to give him an abundance of fresh air, unhampered by annoying and irritating limitations of his free will, restrictions of his liberty, and repression of his motor excitement. The risks of injury to others must be reasonably provided against. It goes without saying that few homes meet these indications: very few people can command a house to be converted into a virtual hospital, with the care of trained physicians to direct every little detail of treatment, and proper nursing. The public asylum, therefore, or the private retreat must usually be depended upon. In the case [p. 163] of quiet young people, especially of young women whose illness may be of such a nature as to justify their marrying after recovery, and in the acute mania following childbirth, it is well worth the physician's while to make an effort to keep the patient in a private house when the conditions are such as to make such a course practicable. To the rest and quiet which may be had under such circumstances, with all the goings on of the house regulated to the patient's comfort and convenience, to prolonged hot baths, a full simple diet, given with the stomach-tube if necessary, as few medicines as can be got on with, the supervision of the nurses by some judicious member of the family, and the gentleness (combined, of course, with proper firmness) of home-influences, I attach very great importance in properly selected cases. But I attribute as much to the restful influence of keeping the patients among familiar scenes, and where some familiar face and voice can reassure them in their comparatively clear moments, instead of their being agitated and distressed to know how to account for the strange people and cell-like room of the insane ward to which they will awaken from their delirium in the hospital. It is something to avoid the excitement of commitment and removal to an asylum, with all that they involve, as well as the sight of demented patients, whose noise may make sleep impossible just when it is most needed. Acute mania seems to me to arise much less often than other mental diseases in definite associations which need to be escaped from for successful treatment.
The term subacute mania is used by some writers for the milder cases of acute mania, just as acute delirious mania is a term which is applied to those violent cases of acute mania in which furious and prolonged delirium marks the disease, and in which there is a high death-rate and low proportion of recoveries.
In chronic mania the motor excitement, mental instability, and, sooner or later, delusions, if not present at the beginning, as is usual, continue. The progress to dementia is commonly slow, and there are few cases which it is wise to treat away from an asylum or its dependencies on account of the possible danger to others from sudden exacerbations of the disease or through uncontrolled violent impulses.
Although there is no pathological condition distinctive of mania in its curable stage, conditions indicating hyperæmia are usually found, whether as a result of the disease or its underlying cause, and sometimes meningitis. In chronic mania there is in the terminal stages evidence of atrophic and degenerative changes which do not distinguish it from other forms of mental disease.
ACUTE DELIRIUM is the typhomania of Bell. Its prevailing mental state is of mania oftener than of melancholia. It resembles the worst cases of typhoid fever so closely, and it is so uncommon a form of disease, that the mistake has often been made of sending typhoid-fever patients to insane asylums. The mistake is unnecessary, as the clinical features of typhoid fever are so well marked that with sufficient care and delay they may be recognized if the physician does not commit the common error in mania of being too much afraid of his patient to examine him thoroughly. The tendency to exhaustion in acute delirium is rarely successfully combated, as the motor excitement is so intense and the delirium so furious that nourishment to meet the tremendous demands of the [p. 164] system can seldom be given, and death is the usual result. Recoveries are rare, but less uncommon in the melancholic than in the maniacal form.
Little need be said in the way of TREATMENT, except that in so speedily fatal a disease it is well to keep the patient at home, if he can be properly cared for there.
TRANSITORY INSANITY is used by Krafft-Ebing19 (Transitorisches Irresein) as indicating mental disease differing from other insanity only in the fact that it is of short duration—namely, from two to six days. If it is applied to sudden and transient outbursts of mania, with delirium, loss of power of self-control, and inability to clearly recollect the circumstances of the attack and what happened during its continuance, it is a rare disease, occurring for the most part in epileptics and in persons under the influence of alcohol or addicted to its habitual use. It is sometimes, under the latter-named condition, called alcoholic trance. It consists in an automatic state resembling the epileptic delirium, which may occur also in sleep and resemble somnambulism. The actions are guided by co-ordinated will without conscious intelligence, and may consist in crimes and brutalities and foolishness entirely inconsistent with the character in health. It seldom lasts more than a few hours. When caused by alcohol or as a symptom of epilepsy, it may occur without other marked inciting cause; otherwise it is commonly due to mental shock. Several cases happened during the mental excitement of the first battle in our civil war. The most striking case within my own experience was that of a man who under the strain of prolonged grief and the mental shock of a great fire destroying a large part of the town in which he lived, perhaps moderately affected by alcohol, suddenly grasped an axe and cut off with one blow the head of a beloved child. He was found in the street without knowing how he had got there or what he had done.
19 Irrenfreund, 1883, p. 113.
One attack is the rule, although several, probably of an epileptic nature, have been reported. It is an extremely difficult condition to diagnosticate with certainty, and is therefore often the refuge of criminals and a resource of criminal lawyers. The most likely honest mistake liable to be made regarding it is to confound it with an outburst of passion.
PRIMARY DEMENTIA (Acute dementia, Stuporous insanity, Anergic stupor) is a disease chiefly of youth and early maturity in persons of inherited weakness or under the influence of prolonged exhausting conditions, to which some mental shock usually adds the immediate cause. Although most of the cases are under the age of twenty-five, it occurs up to forty-five. Masturbation is so common a symptom in its course—and it may be one of the debilitating and enervating factors constituting a predisposing cause—that most of the primary dementia is classed in some asylums as insanity of masturbation. There may be an initial stage of a number of days, marked by moderate melancholia or by maniacal excitement, but there is usually mental torpor advancing rapidly to pronounced dementia. In rare cases there is marked chorea, and slight choreic movements are often observed. The course of primary dementia may be subacute and advance with extreme slowness.
There is no overwhelming delusion paralyzing the mind, so to speak, as in melancholia attonita (melancholia with stupor). In acute cases the brain quickly falls into a state of profound anæmia, precisely such as is [p. 165] found post-mortem in starved dogs, and loses its power to a greater or less extent of reacting to the stimulus of the senses. There is little or no sensation of hunger, the sensory nerves are nearly or quite paralyzed, the bladder and rectum become distended until urine and feces are voided unconsciously or at least uncontrolled, and voluntary movements almost cease, although the muscles are capable of acting if directed: if led or pushed, the patient walks; if placed in a chair or bed, remains there; and in the worst cases lies on the floor quite inattentive to all the decencies of life unless constantly looked after. There is always partial, and there may be complete, anæsthesia, to such an extent that even the involuntary muscles do not respond to the ordinary stimuli. There is rapid loss of flesh, very sluggish circulation, and feeble heart-action. After recovery the patient speaks of the stage of his greatest illness as a blank in his memory.
This description of pronounced cases of primary dementia of the most severe type needs modification as applied to milder cases, which may exist in all degrees, down to a state of mental impairment of very moderate extent.
The mental impairment may be progressive and quite incurable, but also so slight in the beginning, and may make such slow progress, as to entirely escape detection for several years, and then attract attention at first by the lowered plane of character and loss of self-control in little matters of daily life, rather than by the intellectual deterioration, which by that time has become quite marked. This subacute form of primary dementia in young people rarely finds its way into the insane asylum until the second, third, or fourth year of its course, and then its progress is slowly downward. It has none of the eccentric or grotesque features of hebephrenia, and little of its emotional disturbances.
Subacute primary dementia in the later years of maturity, just before or several years before the climacteric, is of grave import, as it indicates the development of an hereditary predisposition to insanity in a form which not only offers no reasonable hope of recovery, but also is quite certain to manifest a change of character which is even more difficult to treat and properly control than the intellectual failure. As it is most likely to arise under circumstances of wear and worry, its symptoms may be for a long time attributed to disappointment or bad temper. After the dementia becomes pronounced its downward course is seldom otherwise than very rapid.
SECONDARY DEMENTIA is a convenient name for the curable dementia which appears at the subsidence of acute symptoms occasionally in mania, and rarely in melancholia—that is, just about the beginning of the period of convalescence. It is also called secondary stupor.
In primary and secondary dementia, resulting in recovery, the progress of the disease is rarely otherwise than very rapid, and unless a cure takes place in a few months at the outside, secondary changes occur in the brain and the tendency is to terminal or incurable dementia. So many cases are treated outside of asylums that it is difficult to estimate the cure-rate, but it is probably not less than 60 or 70 per cent., although it is quite common in the apparent cures for the brain to remain on a lower intellectual or moral plane than if the disease had not occurred.
TREATMENT does not involve the necessity of removal from home in [p. 166] the acute cases, except when that is demanded for convenience of treatment. There is no melancholia to suggest the possibility of suicide, and no mental exhilaration or motor excitement to make restraint necessary. The most important indications are met by abundant, easily-assimilated food, which must usually, for a time at least, be given with a spoon or by the stomach-tube; fresh air, attention to the processes of digestion, relief of the gastro-intestinal catarrh by the usual remedies, stimulating baths, tonics, stimulants, and general galvanism. Proper care in emptying the bladder and rectum and entire cleanliness will suggest themselves.
In mild cases a tonic and stimulating regimen, including sea-bathing and gymnastics, will often be sufficient.
In the subacute cases young people are easily depressed by the asylum associations, but there is usually a time in the progress of the disease when home-discipline is too weak for them, and they must be sent away; older people have usually complications in their home-life such as to make a change desirable for the comfort of the household. Recoveries are extremely exceptional.
In all cases there is little to be gained in keeping up home-associations for so disturbing, distressing a disease after there is pronounced dementia.
Medicines, other than tonics, are of little use, except opiates to control various distressing nervous symptoms, including masturbation, but they should be used with great caution.
KATATONIA (Katatonie of Kahlbaum; Katatonische Verrücktheit of Schüle) presents, with more or less regularity of appearance, symptoms of (1) mild melancholia without the characteristic mental pain; (2) mental excitation, sometimes ecstatic, with cataleptiform conditions; (3) confusion and torpor or apathy. There is an underlying well-marked intellectual impairment, slowly advancing in incurable cases to pronounced dementia. Delusions, more of the unsystematized than of the systematized character, but resembling both, constitute a prominent part of the disease from the beginning. Verbigeration and a curious sort of pomposity are usually found in more or less pronounced degree. The delusions are mixed. They are exalted, hypochondriacal, melancholic, with all sorts of self-accusation, and may be full of suspicion, fears of poisoning, and ideas of persecution. Hallucinations of the special senses and illusions are not uncommon. If the term katatonia is not used, or at least if a special place in the nosology were not given this disease, it would be difficult to know whether to class these cases as primary dementia, melancholia with delusions, delusional insanity, or confusional insanity.
The verbigeration, when it exists, and the expression of delusions are often associated with a manner on the part of the patient suggesting disbelief in them, and sometimes the patient smiles or laughs at the astonishing character of his statements. There is a self-conscious element at times, suggesting mimicry or hysteria; a certain pathos is universal; opposition and contradiction, even to refusal to eat, leave the bed, dress, wash, are quite common; and nurse and physician are tired out with the monotony of the mental and physical state. Well-marked catalepsy is not common in my experience, although it occurs; and in all cases I have seen the mental state and physical atony suggesting that condition. Little attention has as yet been given to katatonia in asylums in this country. Judging from my own experience, it is not a common disease.
[p. 167]Its CAUSES apparently lie in prolonged mental exhaustion and inattention to bodily health. I have been led to suspect syphilis as at least a predisposing cause.
The COURSE AND DURATION of katatonia are tedious, and even if there is apparent recovery from the first attack, the tendency is to relapses and to slowly-advancing dementia and death from those causes of which dements in hospitals die, especially phthisis. I have never seen a complete and permanent recovery.
The MORBID ANATOMY of katatonia suggests a deep-seated neurosis, the precise nature of which we do not understand. In terminal stages there are atrophy and degeneration and all that goes with them.
The CLINICAL HISTORY of katatonia is so characteristic that it need be confused with the other diseases already mentioned as simulating features of it, and with the early stage of general paralysis, only through insufficient observation or too hasty diagnosis.
It is difficult to treat katatonia without the conveniences of a hospital.
PRIMARY CONFUSIONAL INSANITY is a term recently introduced for a form of mental disease of which the most marked features are moderate fever rapidly developed, confusion, incoherence, and mild delirium. The onset of the disease is rapid. In some of the cases which I have seen the diagnosis was made of typhoid fever, although the clinical marks of that disease were absent, the general appearance of the patient in the two diseases being quite similar.
There is no real melancholia or exaltation, no rapid flow of ideas, and no dementia. Hallucinations of the special senses are common; there is a consciousness of illness; the delusions are unsystematized, and the confusion of ideas frequently goes to the point of not being able to recognize persons and places. The usual signs of fever are present for a few days, but the temperature rarely exceeds 102° F., and soon drops to nearly or quite the normal.
The COURSE of the disease is quite rapid, and if recovery does not take place in several weeks or a few months, chronic insanity with delusions or dementia of various degrees may be expected.
The MORBID ANATOMY is not distinctive of this condition in the early stage, and we cannot yet differentiate it from simple fevers by the post-mortem. If ending in incurability, the atrophic and degenerative changes of chronic mental disease are found.
As regards removal from home, the considerations already referred to should be the guide. It is a good rule to keep the patient at home if a suitable one for the purpose, and to resort to the asylum in case of chronicity or troublesome complications.
PRIMARY DELUSIONAL INSANITY (Folie systematisée, Verrücktheit20) differs from secondary delusional insanity in the facts that the disease arises primarily, and not secondarily to other mental diseases; that there is little or no mental enfeeblement in the early stage; and that the delusions, although fixed and systematized, are limited. It has the advantage of allowing the avoidance of the misleading terms monomanie of the French and monomania of English and American writers, the narrower forms of which may be included under the term primary insanity (primäre [p. 168] Verrücktheit), including the further developments of the neuropathic constitution, especially those with the physical marks of degeneration described by Sander as originäre Verrücktheit, and those marked by imperative conceptions and such delusions of self-importance, suspicion, etc. as seem to some people evidence of insanity, while by others they are considered as simply false beliefs not indicating mental disease. Unlike primary insanity, which is one of the states of mental defect and degeneration, and incurable, primary delusional insanity may occur in persons of healthy mental organization, and may end in recovery,21 although it is one of the most distinctly hereditary forms of insanity, generally speaking.
20 Called also by some writers Wahnsinn, although they use the term for secondary delusional insanity also.
21 Some writers include both diseases under the term monomania, and make both incurable degenerative states, which is contrary to my experience. Clouston also has seen cures in what he calls monomania (primary delusional insanity) without the neuropathic taint.
There are several subdivisions of primary delusional insanity, according to the character of the delusions: (1) with delusions of unseen agency, suspicion, and persecution; (2) with delusions of personal exaltation; (3) with delusions transformed from sensations.
Delusions of unseen agency, suspicion, and persecution appear either acutely and expand very rapidly in a few weeks, or from a very insidious beginning so gradually that they may exist for months or years before they are detected. The general indications of illness consist in impaired sleep, slight loss of flesh, some reserve or shyness in relations with other people, and diminished ability to concentrate the mind in the usual occupations. The mental impairment at first is very slight, and shows itself (1) in the readiness with which the absurd delusions are believed and the fixedness of their hold on the mind, and (2) in the diminished general power of judgment and self-control in the little matters of daily life, at first so slight that it is not seen except in matters requiring some effort to maintain the customary equilibrium. Hallucinations, especially of hearing, appear. In the progress of the disease the mind loses power of self-control more and more, the delusions become more fixed, concealment is no longer possible, and the patient is so annoyed or angered that he repeatedly seeks relief from the courts (Querulantenwahnsinn) or commits some act of violence in self-defence. The common delusions are of marital infidelity, attempts at poisoning, mesmerism, electricity, influence through telegraphs, telephones, poisoned air, etc., signs of which are evolved directly from the consciousness or transformed from common sights and sounds, such as ringing of bells, striking of clocks, simple ordinary motions, etc. The delusions in time produce a state of mental depression.
In some cases the primary delusion is of personal exaltation, attended with persecution and mental depression. The individual thinks himself some great personage unjustly deprived of his rights.
Delusions of grandeur or of personal exaltation develop in the same way, usually subacutely from what might seem a foolish fancy rather than an insane belief. The Napoleons, kings, queens, greatest financiers, gods, etc. of the insane asylums are those who reason correctly if one concedes the truth of their false premises, until the progress of the disease produces such general brain-enfeeblement that their premises and their [p. 169] reasoning from them are both insane. The delusions lose their fixedness, and their force too, in the general lowering of the mind's strength, and complaints and boasts and acts of anger become fewer, and finally cease.
The COURSE of the disease is nearly always subacute in the beginning and chronic to the end in the two forms of primary delusional insanity—that is, with (1) delusions of persecution and mental depression, and (2) delusions of grandeur. A few cases with acute development result in recovery, most of which relapse. The course is for the most part to chronic delusional insanity attended with moderate dementia.
The MORBID ANATOMY is not known, except that atrophic and degenerative changes—not distinctive, however—are found in the terminal stages.
The patient is rarely willing to be treated as an ill person, for he is sure of the correctness of his delusions. If during the first attack he can be entirely removed from his daily associations by change of scene and travel, or, if that is not possible, by admission or commitment to an asylum, before the delusions become fixed and while it is still safe for him to be at large, there is reasonable chance of recovery. Second or third attacks very seldom end in recovery unless they arise from alcoholic excess, when entire abstinence for a sufficient length of time affords fair hope of a favorable result, except in cases of long-standing drunkenness.
TREATMENT, when the delusions have become fixed, involves, chiefly, safety to society or its comfort. The patients rarely commit suicide, driven to desperation by their delusions of persecution when they are particularly horrible. The more common tendency is to acts of violence toward others, so that seclusion in an asylum is usually the only safe course to pursue for delusions which one week may be directed against certain persons who can easily be gotten out of the way, the next week may be directed against others, and so on indefinitely. Delusions of grandeur may be only a nuisance or annoyance, but may at any time become sources of danger. The course is, for the most part, to slowly-advancing dementia. Asylum treatment offers no chances of recovery in cases not depending upon alcoholic excess, but becomes necessary for the protection of society.
Transformed delusions (sensorielle Verrücktheit) arise usually in some anomaly of sensation, which probably directs the delusions already forming in a mind in the early stage of disease rather than causes the disease. The causes lie in a deep-seated exhaustion of the nervous system, especially in the neuropathic constitution and profound hysteria. Various anomalous sensations give rise to a belief in delusions as to their being caused by individuals for a purpose, or to their being an indication of all sorts of impossible and most extraordinary changes in the part: the chest is of stone, the leg of brass, the head on fire, the hand ice, and so on indefinitely. Hallucinations and a cataleptiform state are common. The variety of delusions which may arise is almost endless, and they may have their origin in the unhealthy action of any organ in the body: one of the most troublesome forms, called ovarian insanity by Skae, causes single women of severely continent lives to imagine all sorts of impossible marital relations with men whose lives are equally beyond scandal and above suspicion.
Without proper care the COURSE of the disease is to slowly-advancing [p. 170] dementia; and this may be expected when there is organic disease of any important organ of the body.
Before the delusions are fixed, diversion, change of scene, travel under agreeable circumstances and judiciously regulated, may be of great benefit. In the later stage of firmly-fixed delusion asylum treatment offers more chances of success.
In all the forms of primary delusional insanity the whole history of the case is difficult to get at, and there may be, and usually is, so strong a tinge of possibility at least, if not of actual probability, in the delusions, in the early stage of the disease, that a correct diagnosis cannot be arrived at until the time and opportunity for a cure have passed.
DOUBTING INSANITY (Folie du doute, Maladie du doute, Grübelsucht) is classed by Régis22 as a form of melancholia (mélancolie délirante), on the ground that it has the three elements of melancholia—namely, fixed ideas (délire) of a sad nature, general mental depression, and tendency to suicide. The melancholia is secondary, however, rather than primary, and doubting insanity belongs more properly under the head of a psycho-convulsive mental disease closely allied to delusional insanity, like which it is more commonly a manifestation of psychoneurotic heredity, appearing for the most part among the cultivated classes. It consists in an uncontrollable doubt and indecision, unanswerable by any degree of rational explanation, regarding the occupations, duties, or events of the day, religion, a future life, the commonest acts, or the most abstruse problems of life. Doubting insanity essentially depends upon an anomalous action of the will, with imperative conceptions and impulses. It is classed by some writers as a monomania of the degenerative type. Schüle calls it Verrücktheit sensu strictiori, using the term Verrücktheit also for the three forms of primary delusional insanity just described.
22 Manuel pratique de Médecine mentale.
Délire du toucher, an insane dread of touching certain objects, and the morbid fear of defilement, called by Hammond mysophobia (similar names may be multiplied indefinitely), belong in the same category.
There are mild cases of all these forms of disease, which seem like simple weakness of character, others requiring for treatment the conveniences of the retreat for nervous and mental diseases, with a fair prospect of recovery, and still others tending to chronicity in which hallucinations, delusions, and dementia appear only as a further development into another form of insanity. They may, in mild degrees, be symptoms in the course of other mental diseases, especially melancholia, like many other manifestations of morbid mental energy, such as Doctor Johnson's inability to enter a room with his left foot first or to pass a lamp-post without striking it with his cane, etc.
PRIMARY MENTAL DETERIORATION or PRIMARY BRAIN ATROPHY is a term suggested for a curable impairment of the mind arising from brain-exhaustion in persons, usually men, between the ages of from fifty-five to sixty-five. I have found it in some cases associated with interstitial nephritis and with degenerative disease of the walls of the heart, and have suspected atheroma of the cerebral arteries or possibly endo-arteritis of specific or other origin. It occurs at a time when atrophy of the brain is naturally taking place. There are the usual indications of physical wear and such marked deterioration of the mental powers as to [p. 171] seriously interfere with the capacity to attend to customary business and every-day duties, and to closely simulate the early stage of paralytic dementia. There occur also, in a certain proportion of cases, epileptiform convulsions, slight attacks of dizziness, petit mal, and always disappearance of sexual power and desire. There may or may not be headache. The patient recognizes his condition, his mental depression does not far exceed the physiological limit, and there is no reasonable risk of suicide, except from reasons which would impel a sane man to it.
Under the influence of rest, if begun early, tonics, and a strict regard to the laws of health the symptoms commonly disappear if there is no organic disease. I have never seen the brain recover its tone to the extent of making it safe or even possible to resume the previous kind and amount of work. In a certain proportion of cases there is striking mental impairment, even dementia, and the primary atrophy of the brain sometimes makes rapid progress to unconsciousness and death.
It is not possible to say, by the degree of atrophy found post-mortem, whether there was or was not primary mental deterioration during life.
The TREATMENT consists in entire freedom from care, rest from work, travel, tonics, etc.
As mental disease is more than a brain disease, and is a disease of the intellect, each age from infancy up (and each individuality) impresses its peculiar mark upon it, and there are certain terms in common use to express insanity associated with certain physiological processes whose meaning should be explained.
INSANITY OF CHILDHOOD is for the most part only a further development of a congenital state of mental defect. I have seen, however, well-marked mania, melancholia, primary dementia, and primary delusional insanity before the age of puberty. Typical acute mania I have seen twice in children two years old, apparently arising in normal brains after severe injuries to the head. This is quite uncommon, and the number of cases thus far observed is too few to make me feel sure that my own experience of a favorable result as to recovery in uncomplicated cases will be generally confirmed. At best, after a cure there is a more or less decided arrest of brain development.
HEBEPHRENIA (insanity of pubescence and adolescence) occurs within the ages of fourteen and twenty-three or thereabouts. Like insanity in general among persons in early life, it most commonly indicates an hereditary predisposition to mental or nervous diseases or an early-developed brain defect or injury, possibly an exalted emotional state or an increased nervous sensitiveness produced by masturbation. It is a mild form of primary dementia, modified by the mental changes going on during adolescence. Indeed, it is simply an exaggeration and prolongation of the curious psychological development of that period, too well known to need description, which goes on in the most insidious way possible through months or years of what seems silliness, absurd fancies, foolish sentimentality, egotism, impaired common sense, and diminished judgment and self-control, to a slowly-advancing dementia, which even then is not always recognized as disease. The result is an arrest of brain development on various planes of intellect, and a preservation of the youth's tastes and sense and intelligence, as modified by the morbid propensities characterizing an unhealthy development of the change from boyhood or girlhood and [p. 172] youth to adult life, with the adult's strength—a curious combination of intellectual brightness, it may be, with lack of mind. For this characteristic condition Westphal uses the expressive term Permanenz der Flegeljahre (permanence of the usually transitory state, which then commonly results in permanent arrest of brain development on the plane of the mind at a definite age of adolescence); and yet there may be more than that—mental deterioration, which in years may lead to pronounced dementia. Cases of primary dementia occurring within the years of puberty and adolescence are often classed as hebephrenia and conversely, so that one term, primary dementia, is thought sufficient by many writers on insanity.
In the early stage there is sadness, hardly amounting to melancholia, and it usually constitutes an important symptom to the end, although, like all the other changes in the mental state, it is superficial to the extent of at times seeming almost insincere. Masturbation is common. Occasional outbursts of violence are also common, often with mental confusion, incoherence, or stupor, and in severe cases there occur, usually, attacks of temporary fury, with distressing or agonizing hallucinations of sight and hearing, and delirium, which may all last for a very short time or for a number of days. In young women and girls these outbursts may be coincident with menstruation or in the intervals. The countenance loses somewhat in expression in all cases, and becomes almost vacant or quite so in those in which the dementia becomes well marked. A mild form of the disease is quite common, and consists in an undue intensity or a prolongation of the curious psychological phenomena commonly observed during adolescence. It is marked by aimlessness, changeability, self-assertion, exaggerated self-consciousness, with, perhaps, propensity to lie or steal or run away from home, and ending without any apparent damage to the mind, except that the individual is less of a success in life than he would have been but for his illness.
The course is slow, and although in the majority of cases mental impairment is arrested before reaching what may be properly called complete dementia, in well-marked cases the duration of the disease is long and its results last for life. In many cases progress continues with extreme slowness to extinction of the mental faculties. Oftener the individual simply, in a certain sense, fails to reach that stage of intellectual maturity and strength which he otherwise would have attained. It is not always easy to draw the line between the psychological and the pathological changes that take place during the years of adolescence, and there are many mild cases of hebephrenia in which various kinds of failure in life are due to this disease rather than to the faults or vices to which the failure may be attributed.
In TREATMENT irritability, restlessness, absence of a power and sense of responsibility, and sleepless, excitable nights, are the most difficult symptoms to combat. The restlessness and irritability often lead to refusal to be reasonably controlled and to a tendency to wander away from home with theatrical displays, so as, in the case of girls particularly, to require restraint, especially if the excitability should be so great as to amount to outbursts of violence or should lead to sexual improprieties.
The fact should be borne in mind that there is a diseased brain which needs nutrition, rest, and discipline, which must be proportioned to suit each case. Outdoor, simple life, with sea-bathing, carefully-selected diet, [p. 173] without too much meat, exercise, mental training limited to the requirements of each patient, are the chief reliances. Iron, cod-liver oil, and arsenic are useful tonics. Stimulants, including tea and coffee, should be avoided. Quiet nights and necessary repose can be secured by bromides, exercise, and opiates used sparingly, which also control the impulse to masturbation. A sound education, a healthy experience of the rough and tumble of youthful life, and the careful avoidance of processes and habits of indulgence will often prevent the symptoms of disease from growing into traits of character and habits of life. On the other hand, in some cases there is a half-conscious struggle between the fine traits of character and the demoralizing influences of the disease, and a most pathetic effort to keep the better nature's supremacy over the lower impulses set free or developed by the destructive tendencies of a fearful malady.
MENSTRUAL INSANITY differs from other periodic insanity in not being necessarily a further development of an hereditary or acquired state of mental degeneration, and in being curable in a fair proportion of cases.
INSANITY OF GESTATION, PUERPERAL INSANITY, AND INSANITY OF LACTATION do not call for any further comment than the remark that they represent causes and conditions rather than types of disease.
CLIMACTERIC INSANITY in women and in men is usually a curable folie raisonnante—insanity of action or affective insanity, which may develop into secondary dementia or chronic insanity with delusions. It does not necessarily include all acute forms of insanity occurring at the climacterium, but only those slowly developing with the physiological changes going on.
The course is usually subacute, the duration a couple of years or more, and the termination in about half the cases is in recovery. Permanent change of character and further progress to incurable insanity are perhaps about equally common.
TREATMENT consists in a sedative and fattening diet, simple, healthful conditions of life. Removal to an asylum or some form of restraint is needed where the conduct is such as to demand seclusion and control.
SENILE INSANITY arises in suspicions and a generally deluded state of mind regarding those persons whom there is every reason to trust—namely, relations and near friends—and as extraordinary credulousness of designing persons whose interest and character would naturally suggest being on the guard against them. There is impaired judgment, as shown by the mismanagement of property and diminished capacity for business, usually some perversion of the sexual instinct. The suspicions and credulousness in time amount to insane delusions, and if life lasts the end is in marked dementia. But there may be no mental impairment evident to casual observers or to ordinary acquaintances for many years. The improper relations assumed with the opposite sex, the neglect or abuse of those nearest by ties of blood, the squandering of property on strangers, and the omission to provide properly for the members of the family, are wrongly attributed to a character become bad rather than to destructive brain disease, where they belong. Not seldom senile insanity is a moral insanity, and shows itself by an entire change of character not explainable by other circumstances than disease, and is then marked by [p. 174] indecent exposures, loss of the fine sense of the decencies and proprieties of life, destruction of the discriminating power between right and wrong acts.
The course of senile insanity is slow, unless there be also some fatal disease with it, and evident mental impairment may be so late that the disease may be overlooked for years.
The TREATMENT is abundant nutrition, including wine, removal from irritating conditions of life, protection of the individual against himself, and guarding the community against harm or indecencies. Small doses of morphia daily are often of great benefit, and there is no real danger of acquiring the opium habit if reasonable discretion is exercised in its use.
SENILE DEMENTIA is simply an excess of the natural mental weakness of old age out of proportion to the bodily state, an exaggerated childishness of senility to the extent of producing irresponsibility. It is in reality a subacute primary dementia modified by the peculiarities of old age. Memory fails first, and a condition of general weakness of mind follows rapidly afterward. Secretiveness, suspicions, delusions, and hallucinations of the special senses are almost always present.
It is not uncommon for the early symptoms to consist in an inhibition of the higher faculties of the mind, so that the lower impulses become prominent. The sense of right and wrong and the moral perceptions may become entirely weakened. Acts of indecency, dishonesty, injustice, depravity may follow impaired judgment, and yet so far precede strikingly perverted memory and general intelligence as to make the insanity, which is obvious to an experienced observer, entirely fail to impress itself upon the minds of the community.
The TREATMENT consists in caring for the comfort of the patient, which can usually be done at home or at least in a private family, unless there are persistent impulses requiring the control of an asylum. The preparations of opium are useful to control extreme restlessness, and may be given freely, avoiding narcotism. A bland diet of fattening food is best suited to the wants of the aged. A simplified life often serves every purpose, especially in the quiet of the country, although it is best not to remove them from familiar scenes unless as a matter of necessity.
Complicating insanities simply add to the usual symptoms of the special forms of mental disease many of the characteristics of the particular disease, rheumatism, gout, phthisis, organic diseases of the heart, etc. Choreic movements depend upon the same pathological changes as are found in the sane, and certain diseases are attended with such profound changes in the nutrition of the brain as to give rise to mental impairment, which amounts to almost extinction of the mind, such as myxœdema and chronic nephritis. Acute mania occurs in the last stage of Bright's disease, which may be difficult to differentiate from uræmia. Mania, melancholia, and delusional insanity occur in the course of acute febrile diseases or appear during the period of convalescence; in the latter case the prognosis is much more unfavorable than in the former. The close [p. 175] alliance between insanity and pulmonary consumption is a matter of frequent observation. The two diseases are interchangeable, and they often coexist. The relation between rheumatism and insanity is less close.
Maniacal symptoms have been reported from the use of various drugs, including iodoform, mercury, etc. Hasheesh dementia is not uncommon in the East. Acute delirium arises from hydrate of chloral and the preparations of opium analogous to acute alcoholic mania from excessive drinking, and chronic impairment from their prolonged use. Bromide of potassium rarely produces symptoms similar to those of mania; taken for a long time in even moderate doses, it tends to mental sluggishness, and in long-continued large quantities given uninterruptedly there is a danger of well-marked dementia.
All of these conditions may be prolonged beyond the usual action of the particular drug or give rise to symptoms in excess of those usually observed. The characteristic indications of the particular drug, sometimes marked by the combined use of several, will be found if they are carefully looked for.
The TREATMENT consists in breaking off the bad habit gradually or abruptly as each case may require, and in otherwise treating the persisting symptoms in accordance with the general principles already stated in considering the various mental diseases.
ALCOHOLIC INSANITY includes mental disorder from the use of alcohol in both the acute and chronic forms.
Acute alcoholic mania may come from a single excess in drinking, which in some individuals is always attended with maniacal symptoms. It may constitute the alcoholic trance described under the head of Transitory Insanity. From long drinking and exhaustion or by withdrawal of the accustomed stimulant we may have the familiar mania-a-potu or delirium tremens.
Under the prolonged use of alcohol primary delusional insanity, melancholia, mania, and dementia occur.
From long-continued drinking of alcohol, even to slight excess, for many years, it is rare not to find some mental impairment, if only an “uncontrollable violence of the instincts and emotions,” a sort of moral insanity.
The PROGNOSIS is more favorable than in most forms of insanity uncomplicated by the abuse of alcohol, especially in the case of primary delusional insanity, if the bad habits can be effectually corrected and if the alcoholic excesses have not been continued long enough to produce organic changes in the cerebral blood-vessels. In the latter case the dementia sometimes simulates that of general paralysis so closely as to be called pseudo-paralytic dementia from alcohol.
TREATMENT is rarely successful outside of some asylum.
SYPHILITIC INSANITY does not properly include those cases of mania, melancholia, and delusions of persecution of the ordinary type of which the exciting cause is found in the train of thought aroused and kept up by the consciousness of having contracted syphilis, but only such as [p. 176] depend upon the presence of the syphilitic poison in the system. There are no diagnostic marks to distinguish it from insanity not caused by syphilis, except in a certain proportion of cases of organic syphilitic disease of the brain.
The PROGNOSIS is rendered much less favorable from the fact of the syphilitic cachexia.
In addition to the usual means of TREATMENT for the several forms of insanity, the appropriate measures for syphilis should also be tried, except where there is evidence of diffuse organic disease.
GENERAL PARALYSIS OF THE INSANE is a disease marked by definite pathological changes in the central nervous system, chiefly in the cortex of the brain, but which may extend to any part of the cerebro-spinal tract or to the sympathetic ganglia and cranial and spinal nerves. Its constant symptoms are—(1) vaso-motor disturbance ending in vaso-motor paresis; (2) mental impairment, which makes progress, for the most part unevenly, to complete terminal dementia or extinction of mind; (3) impaired muscular control, which advances more or less uniformly to almost entire paresis or nearly total paralysis. Expansive delusions, the delirium of grandeur, megalomania (which may change suddenly to micromania), or simply a feeling of elation, happiness, self-satisfaction, or undue complacency, are found, but often not until or near the end. The other symptoms vary in individual cases within a wide range, so as to simulate almost every form of insanity; and it is quite possible that they include what a more exact pathology will hereafter recognize as several distinct diseases.
SYNONYMS.—General paralysis is also known as general paresis, progressive paralysis of the insane, paretic dementia, paralytic dementia, cirrhosis of the brain, paralysie-générale, folie paralytique, démence paralytique, periencephalite chronique diffuse, meningo-myélo-encephalite chronique interstitielle diffuse, encephalite généralisée, periencephalite chronique diffuse, encephalite interstitielle diffuse, encephalite avec proliferation sclereuse interstitielle, Allgemeine Paralyse, progressive Paralyse der Irren, chronische progressive parenchymatöse Encephalitis der Rindensubstanz, pericerebritis, periencephalo-meningitis diffusa chronica, periencephalo-myelitis chronica diffusa, encephalitis interstitialis corticalis, paralytische Blödsinn, primäre Encephalitis interstitialis mit Ausgang in Sclerose. Griesinger placed general paralysis among the complications of insanity. It is popularly known as softening of the brain (Gehirnerweichung).
HISTORY.—The combination of the two series of symptoms, paralysis and dementia, was recognized by Haslam, and at the beginning of this century by French writers, who also knew their fatal import. Esquirol describes a typical case of general paralysis of the insane under the head of monomania in his Maladies mentales. His pupils, especially Bayle and Calmeil, have studied and described general paralysis. At the time of his first visit to England, forty years ago, the late Luther Bell had never recognized a case, and there can be no doubt of the fact that it has [p. 177] rapidly increased, particularly in the last dozen or twenty years, with the rapid increase in the aggregation of the population.
ETIOLOGY.—So far as heredity is concerned, general paralysis has not such close relations with mental diseases as insanity in general. It is estimated to be hereditary, in the sense of being closely related to other forms of insanity, about one-half as often, and it is nearly allied to apoplexy and epilepsy. My own experience leads me to the conclusion that in those cases of general paralysis without a previous history of syphilis (and the same statement is true in less degree of persons who have had syphilis) the vast majority occur in families in which there have been cases of insanity, epilepsy, or apoplexy. It is rare among people living simple agricultural lives, but is intimately connected with the faults and vices of civilization—specialized overwork, involving strain in the office, study, factory, mine, etc., especially if to bodily exhaustion and brain wear and worry there be added hard living and hard drinking, sexual excesses, and syphilis. The Scotch Highlander rarely has the disease until he comes to Edinburgh or Glasgow. In Ireland general paralysis is so rare that of 9271 cases of insanity in 1882, only 6 were general paralytics, as compared with 1151 out of 13,581 in England the same year; during which, in Scotland, of 238 deaths from insanity, 10 were from general paralysis; but the Irishman has no special exemption from general paralysis in American cities or in large English towns and mines and factories, where he works hard, drinks hard, and lives hard generally. It is, so far as I am able to learn, unreported thus far among our negro population until they come to the great centres of population; it is said to have been unknown among the slaves. Among the English, Scotch, and Americans it prevails most among those people who are in, or who have dropped down to, the lower strata of society. Of 2212 private patients in England, 139, or about 6 per cent., were general paralytics, while 1012, or about 9 per cent., were found among 11,359 pauper patients. French and German writers report it as most common among the brain-workers. In women of the upper class it exceedingly seldom occurs. In some of our Western asylums not more than 1 or 2 per cent., or even less, of the patients are reported as general paralytics, coming chiefly from farms. In the asylum for the centre of the manufacturing districts of Massachusetts about 9 per cent. of the patients are general paralytics. From the iron- and coal-mines of England from 14 to 17 per cent. of the insane confined in asylums are general paralytics. It is more common in cold climates than in warm, other things being equal. From one-sixth to one-tenth of the cases, varying in different localities, are women.
General paralysis not only is most frequent in the stronger sex, but it selects the strong individuals in the prime of life, between the ages of thirty-five and fifty. It is extremely rare under the age of twenty, although Turnbull has reported an unique case at the age of twelve;23 it is not common under thirty or over sixty; I have seen two cases in men sixty-five years old. It is seldom seen in individuals who have been weak from childhood, unless as the probable result of syphilis.
23 Journal of Mental Science, October 1881.
The excesses of the habits of the city and of mining and manufacturing centres, hard work, high living, late hours, predispose to general [p. 178] paralysis in strong constitutions at the period of their greatest activity, especially if the physical strain, the violent struggle for existence, has begun early in life with insufficient food and excessive work, and if ordinary paralysis be not uncommon in the family. Alcoholic and sexual excesses are considered to be particularly common predisposing causes. Recent investigators find syphilis to be a part of the antecedent history of from one-half to three-fourths of the cases, but chiefly in those slowly advancing or subacute from the beginning. By some writers syphilis is considered to be in those cases only a diathesis, as is held by Fournier, or a debilitating antecedent, like chronic malarial poisoning. Others think that so large a proportion can be accounted for only by some specific relation between the two diseases. If the fact so often stated is true, that syphilis is rapidly increasing, perhaps part at least of the increase in general paralysis can be thus accounted for.
Mental shocks of various kinds, excessive emotional strain with mental exhaustion, and injuries to the brain, are the commonly reported exciting causes of general paralysis, but it is not certain that—in many cases, at least—they do more than hasten the pathological process and call attention to the symptoms. So far as my observation goes, the injury to the head, supposed to be the cause of general paralysis, often has appeared to probably come from an accident due to the impaired physical strength and to the vaso-motor disturbance in the brain incident to the early stage of the disease and while it was still unrecognized. Cases are observed in which no predisposing or exciting cause is found by the physician. I have seen it following diphtheria and other debilitating diseases, after long exposure to malaria, and apparently due simply to prolonged mental strain in persons otherwise living in moderation under circumstances exceptionally favorable to health.
SYMPTOMATOLOGY AND COURSE.—As a rule, to which the exceptions are few, the early symptoms of general paralysis are obscure. Their appearance and progress are so gradual and insidious that they are usually overlooked for a period varying from several weeks to a year or more, sometimes for four or five years, perhaps even longer. There is a slight change in character, which is frequently attributed to wilfulness or perverseness arising from some disagreeable circumstance; to want of a reasonable attention to the little affairs of daily life; to indifference, temper, carelessness, or recklessness; to a want of aptitude and receptivity having an ethical rather than medical significance; to an impaired moral sense. The patient may be observed to be simply more quiet and heavy; inclined to be depressed rather than distinctly melancholy; a little heedless; unusually indifferent, and indisposed to worry over things that formerly would have disturbed him; drowsy or dropping off to sleep at work or in the theatre; disturbing the household by his restlessness at night—in and out of bed, up and down stairs, for trivial and yet not seemingly insane reasons. He may become easily disturbed by trifles, and yet careless to more important matters. He begins to overlook, perhaps rather than forget, recent little things. His power of attention is diminished, his will weakened, his self-control impaired. He becomes less careful of the niceties and proprieties of life, less interested in his family and all that is nearest to him—self-absorbed, egotistic, indulging in inconsequent stories and remarks. Although the memory is not [p. 179] distinctly at fault, fresh impressions do not make their usual imprint on the mind. His moods are unnaturally changeable. A certain slovenliness in habits or carelessness in dress, an inattention to customary little courtesies and attentions, slight yet noticeable, are not uncommon early symptoms of general paralysis. There is soon observed, often noticeable to the patient, a lack of endurance, an early sense of fatigue from exertion, a sense of muscular prostration, physical discomfort, or general pains which may be attributed to malaria or rheumatism. Commonly, not always, there is disturbed sleep or restlessness. There may or may not be headache, slight or severe, transient or persistent. There may be a sense of pressure or an uncomfortable feeling about the head, especially the forehead, or it may be the seat of no pain or discomfort whatever. There may be a slight or severe local or general sensation of distress or uneasiness in the head after mental effort only. There is often pain, anæsthesia, hyperæsthesia, paræsthesia affecting any sensitive nerve, often none at all, or impaired muscular sense.
The average daily temperature is higher in general paralytics than in health. It is sometimes lower, and the range is greater than the normal. In the only extremely rapid case which I have seen (two months in all) it was 97° F., and thereabouts for a number of days, and then rapidly rose to 103° and 104°, where it remained until near death. After the congestive, epileptiform, and apoplectiform attacks it rises from two to seven degrees, and remains high for a considerable time, while in pure epilepsy it quickly falls. This difference, however, is not sufficient, as between epilepsy proper and epilepsy as an early symptom of general paralysis, to establish the differential diagnosis with certainty in all cases.
The vaso-motor disturbances in the brain are indicated by transient congestions or local anæmia, dizziness, faintness, temporary outbursts of anger, excitement, or confusion, and rapid changes in the mental and emotional state. Convulsive attacks are not common in the early stage of the disease, except in those cases due to syphilis, but may occur, and may so resemble hysteria, petit mal, epilepsy, and apoplexy as to be confidently diagnosticated for those diseases. The emotional state is of indifference, despondency, gloom, melancholia, elation, a feeling of self-satisfaction, or mania.
The symptoms thus far are not clear except on minute examination. The family and most intimate friends of the patient observe that he is changed, but cannot tell how, and are apt to say that he is not the same man that he was, that his troubles have been too much for him, that he does foolish things as never before, etc. Sometimes he estimates his symptoms correctly, sees the downward change himself, and is oppressed by it; oftener he is indifferent to it, or still oftener quite well satisfied with his condition and prospects, or even mildly elated. He may squander his fortune, ruin his reputation, become addicted to drink. His sexual appetite, not held back by his normal power of self-control or exaggerated with a general physical and intellectual erethism, may lead him into all sorts of improprieties and immoralities or to exhausting excesses, which are perhaps more common among the married than among the unmarried; and yet his disease is not recognized, because the later symptoms of general paralysis—namely, grand delusions, staggering gait, tremor, and marked dementia—have not yet appeared.
[p. 180]The pianist loses his skilled touch; the actor fails to learn a new part; the ready salesman no longer has his great facility of selling; the singer does not see that his notes have become false and harsh; the engraver's fine lines are no longer possible to him; the preacher reads the same hymn three times in his Sunday service; the man of promptness fails to keep his appointments; the speech seemingly clear to others becomes indistinct to a deaf wife; the eye trained to close, exact work loses its capacity of fine distinctions of form or color; the expert accountant can no longer add up his three columns of figures at a time; the doctor writes prescriptions showing unwonted carelessness or impaired judgment to the extent of injuring his practice; a banker loses his property by foolish ventures; the saving business-man buys quantities of useless articles; the moral man becomes licentious or the temperate a drunkard; the respected father of a family goes to the State prison for running off with a pretty servant-girl; the lawyer ruins his client's cause; the considerate husband shows unwonted harshness and violence to his wife; the industrious worker becomes a tramp or a vagabond; the amiable friend becomes irritable, disagreeable, perverse, hard to please, easily excited, cranky. These are some of the facts I have known to occur in the early stage of general paralysis without giving rise to the suspicion of cerebral disease, the conduct of the individual generally not suggesting insanity. In one case the cerebral vaso-motor disturbance caused marked intoxication from a small amount of wine, previously taken habitually without showing it, for several weeks before the most careful examination revealed other indications suggesting general paralysis. In the upper walks of life, wherever a nice intellectual adjustment or fine muscular co-ordination is required in the daily duties, symptoms to put the physician at least on his guard against general paralysis will rarely be overlooked in this early stage of the disease if they are sought for with sufficient care and appreciation of their import. In proportion as the employment is coarser, and not requiring much mental or muscular exactness, the symptoms are more difficult of correct apprehension, until we get to the day-laborers, in whose dull nervous organizations quick reactions do not occur, and in whose simple labor, requiring little thought and only muscular co-ordination of a low grade, a partially demented brain and muscles considerably impaired in strength serve their purpose so well that an early diagnosis is next to impossible. Routine work, to which he is long accustomed, is often done well by a general paralytic, provided it does not require exact mental or muscular co-ordination, when the disease has so far advanced that any new work except of the simplest kind could not be performed.
It is seldom that general paralysis, in its early stage, receives careful enough attention to be recognized or to create a suspicion of its existence until exhaustion, a long period of sleeplessness, perhaps a violent shock, a strong emotion, a fall or a blow, a congestive attack, an epileptiform seizure, an apoplectiform convulsion, or some unknown cause—probably a vaso-motor disturbance in the brain—hastens the progress of the disease, and the previously slight or obscure symptoms (at least some of them) are suddenly so aggravated as to make them of unmistakable signification. It is usual in such cases to date the appearance of general paralysis from this point, and to overlook its previous existence for the weeks, months, or it may be years, of its prodromal period. It is [p. 181] especially easy to overlook the period of invasion of general paralysis of the insane, as the symptoms may, and generally do, have that temporary, transient, and variable character which is common to diseases or stages of disease in which vaso-motor disturbances predominate; inasmuch, also, as the individual character has to be taken so much into account in estimating the import of particular symptoms, and as few or many of the leading indications of general paralysis may be present in a particular individual, while the physician might happen to make several examinations of his patient at times when the symptoms did not appear at all. For now and then all symptoms absolutely disappear in a time which may be short or long. In two cases of general paralysis in the period of invasion, where the moral perversion was said by the other members of the family to be a source of great trouble, I sent both patients to an insane asylum entirely upon the statements of their wives, without being able myself to see any evidence of insanity, but where the clinical history of general paralysis in its early stage was so accurately given that I was sure there could be no mistake; and a few days' continuous observation in the hospital showed the diagnosis to be correct.
The dementia, ataxia, and muscular impairment of the prodromal period of general paralysis of the insane may be masked by the prominence of almost any of the symptoms of nearly all the mental diseases; and many of the indications of the prodromal period are symptoms of disease only as they are departures from ordinary customs and habits, although in other persons they might be quite the reverse and natural to their daily life. Much that might be done by a general paralytic with great care in the early stages may quite resemble the careless work of the same person in health.
The following case is quite typical of the development of general paralysis of the insane:
Mr. ——, age 52, married, a clergyman: his mother died of apoplexy; two of his four brothers are insane. He had the usual illnesses of childhood in mild form, diphtheria of the worst type in 1869, and in recent years, according to his belief, malaria, as he had lived in a malarial region eleven years. As a young man he was of robust frame and vigorous health, brought up on a farm. He overworked, denied himself, and overtaxed, in getting his education, a brain not trained from early years to exacting labor. Eight years ago, for the first time, and at intervals since then, he has had attacks of mental confusion, dimness in sight, and indistinct articulation lasting from a few moments to several minutes. Three years ago, after great emotional strain, people began to notice that his preaching had lost in animation and force, and they complained that he had suddenly become more radical in his views. Great mental worries occurred soon after. There had been no alcoholic or other excess, except of mental overwork, and there could be no reasonable possibility of syphilis, unless we adopt Hebra's dogma, “Jeder Mensch kann syphilitisch sein”—that the means of innocently acquiring that disease are so widespread that no one can be said to be free from the danger of it. Nearly two years ago, in the dark, while feeling tired mentally and physically, but not ill or dizzy, in alighting from a coach he missed the step and came to the ground on his feet with great force. He walked to the house of a friend, and was found by one of the family on their entry floor [p. 182] groaning, but not unconscious. He could not stand or talk, vomited incessantly, and complained of a horrible pain in the back and top of his head. Two days later, and each succeeding Sunday, he preached, obstinately and unlike him refusing to listen to advice to keep quiet; but he remained in bed between Sundays for three weeks, when the striking symptoms disappeared; but he had never felt entirely well since then—never had the same animation. He was supplying various pulpits, and found, wherever he had preached before, that people complained that there was a general lack of vigor in his preaching. Two years ago he observed that his right leg had less life in it than was natural, and soon after that both legs seemed heavy—that it was less easy to run up and down stairs, which his wife also noticed several months later. He also has had for a year a strange feeling, a sort of numbness, in his legs. He thought that his handwriting and speech have continued as good as ever, but has observed that he has had to change to a stub pen, as he found difficulty in writing with the old sharper-pointed kind; that his voice had grown less clear; and that he has rapidly become farsighted. He has never had any dizziness, pain, ache, or uncomfortable feeling about his head, except during the attacks already referred to. There have been no thoracic or abdominal symptoms, no neuralgia or rheumatism. Appetite and digestion have been faultless. He has lost about ten pounds in flesh. He has slept soundly, but is often restless, getting in and out of bed. He says that he was depressed for lack of employment; that he is not irritable, but that his family would say that he is not as tractable as he was, not as patient, less easily satisfied; that his son and wife would say that he is not what he once was—that his memory is not as clear and vivid as it was. He is conscious that within the last two years he has had violent, uncontrollable passionate outbreaks from trivial causes. He preaches his old sermons, because he thinks they are too good to be lost, and because he takes pleasure in rewriting them, in doing which he remarks that the handwriting becomes progressively worse toward the end of each sermon. He says that he can write still better sermons, but does not like to make the effort. When he went into the pulpit a week ago he was told not to announce a second service, but everybody seemed to him so pleased with his preaching that a week later he gave word that there would be an evening service, to which, he laughingly said, only one person came. In standing with his eyes closed and feet together there was a little unsteadiness. On attempting to turn around or to stand on one foot with eyes closed there was some, not very great, ataxia. In these trials the unsteadiness and ataxia soon became very striking on prolonging the muscular effort a few moments. His hands had a powerful grasp, each marking 74 with the dynamometer, and on being stretched to their full extent, with fingers spread, immediately thereafter the fibrillary tremor could be seen only on close examination. There was no marked tremor of the muscles of the lips or face, except in movements which placed them at extreme tension. The tongue was quite tremulous on being protruded to its full length and held there. In walking in a rather dark entry the steps seemed to me shortened and the feet wider apart than in his natural gait, and he did not raise his feet as much, which he noticed also. In going up stairs he placed the whole foot, heel and all, on each step to keep his balance. He turned very deliberately, [p. 183] keeping the feet near together and not raised from the landing. On coming down he evidently steadied himself by a muscular effort extending to his head and shoulders. The knee-jerk was well marked and alike in both legs, but I could not say that it was exaggerated. There had been no change in the sexual function.
His general mental state seemed to me to be of a quite superficial kind of despondency at his prospects, and yet absence of a corresponding degree of anxiety for the future; of satisfaction with his ability and worth; of a feeling that his family are unduly anxious about him; and of a prevailing state of inappreciation of the whole situation, and of a general state of happiness which was abnormal—an opinion which his wife afterward corroborated. He was quite emotional, and easily and rapidly moved to smiles, and from them almost to tears.
In explaining his restlessness at night he stated that he was taking quinine for his malaria, and that it acted on the liver so as to increase the flow of urine, which he repeated several times, but laughingly said, “Of course; how foolish!” when I suggested that he meant the kidneys. In removing his clothes for a physical examination I found that he had two starched shirts on—the one in which he went from home, and that in which he preached, in order not to rumple the second one. When I asked why he could not take home a soiled shirt in his valise after having brought a clean one in it, the idea struck him that he, after all, had done something foolish.
The examination of chest, abdomen, and of the urine was negative. I could not find anywhere evidence of anæsthesia, hyperæsthesia, or paræsthesia, general or local. The reaction of the muscles to the faradic current seemed normal. By ophthalmoscope and otherwise the eyes showed only the emmetropia already referred to. Hearing was also normal, as well as the other special senses. In a close examination I could at first not discover anything about his speech more than an extreme deliberation in articulation, which might perhaps have been natural to some scholarly men, but which I afterward learned had been only of recent origin, and increasing. It was more pronounced after the patient became a little wearied, and then I found that he could not articulate a long word with several labials and linguals without manifest difficulty. I gave him a sheet of paper and asked him to write from top to bottom. He could not think of anything to write. When I told him to put down the text of his sermon of the previous day, he could not possibly remember it; no more could he call to mind a sentence or a sentiment from it. What he wrote is marked No. 1. His normal handwriting, No. 2, is of the date of 1881. Nos. 3 and 4 were copied from an old sermon a few weeks previous to his visit to me, and are taken respectively from the first page and the next to the last of the copy. The facts may be observed that the old handwriting is quite free, with an easy sweep of the pen. In the copy of the sermon the first page shows that the pen is held stiffly and tightly, and that the lines are not made with as steady a movement of the hand as in the old handwriting. The lower lines on the first page are a trifle worse than the upper, and pretty much like the second and third pages, from which there is progressive deterioration to the end. The page written in my office was very carefully done, and, under the circumstances, is marked by such muscular unsteadiness and evidence of mental [p. 184] impairment and enfeebled memory as to be almost, if not quite, of itself pathognomonic of general paralysis.
[p. 185]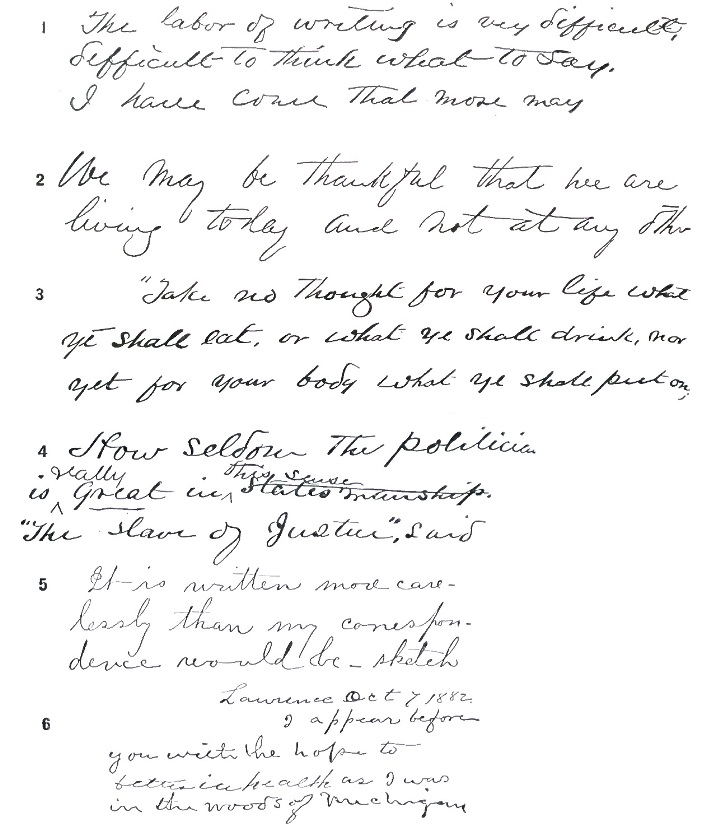
I purposely made no remark to the patient, and he made no inquiry, about diagnosis or treatment. He would have missed his train, although there was a clock in my office, had I not reminded him of the late hour, whereupon he made all his arrangements with care, good judgment, and accuracy, and reached his home safely. As he walked briskly down the even sidewalk I doubt whether any one, even a physician, would have remarked any unsteadiness or anything abnormal about his gait. If he had been followed a few blocks, until the idea of catching his train had ceased to stimulate him, and after he had reached the crowded thoroughfares of the city, especially as he stepped up and down curbstones or walked slowly to avoid teams at crossings, a close examination would undoubtedly have shown the defects in gait already pointed out.
Mr. ——'s wife had noticed that her husband did not raise his feet as of old in walking—that he walked as if they were heavy, but under the influence of coca wine or a decided mental stimulus he walked apparently as well as ever for a short distance. She had noticed a slight impairment in memory, an increased fractiousness, a diminished ability to appreciate things in their proper light, a changeability in his moods and mental state, a scarcely-observed but noticeable neglect or oversight of little customary duties, occasional passionate outbreaks from trifling causes, a disposition to laugh and cry easily; and that often he did and said unwonted foolish little things, like attributing increased flow of urine to his liver, wearing two starched shirts, announcing the Sunday evening service; but she had not considered any of the symptoms as evidence of disease, especially as he kept accounts, attended to his preaching, etc., and showed no manifest indications of a disturbed or impaired mind. She had remarked a decided change in the character of his handwriting, also an unusual deliberateness in speech, but no indistinctness or hesitation, although his voice had become less clear. He had had no delusions, illusions, hallucinations, or unreasonable ideas. It was for the weakness in his legs that she asked my advice.
I found that the mental and cerebral symptoms in this case had been overlooked, and that the weakness in the legs had been attributed to spinal concussion, for which a favorable prognosis had been given.
I examined the patient after he had been away from home nine days, preaching two Sundays, and making many new acquaintances in the mean while, besides having travelled nearly two hundred miles by rail, so that he was fatigued. After three weeks' complete rest I saw him at his house. The knee-jerk was increased as compared with the previous examination. Otherwise the symptoms had so ameliorated that some of them could be brought out only after a long and patient examination, and the rest had to be accepted as a matter of history of the case. I had his photograph taken, and by comparing it with another taken three years previously his family noticed what was quite obvious in that light, but what had thus far been overlooked—namely, that the facial muscles had lost very much in expression.
The specimen of handwriting marked 5 is of a gentleman in whom the paralytic speech is quite evident after a half hour's talk, but quite masked in the beginning of a conversation, when rested. It is written [p. 187] with care, after a long rest, and, as compared with his former writing when done with equal care, there is seen only a wider separation of the letters. Its general appearance, on casual inspection, is better than that of his ordinary writing before his illness, as that was hurried and careless. But the second or third page brings out the ataxia distinctly. It shows how well a general paralytic, under the influence of rest and quiet, may control certain groups of muscles—how completely the ataxia may be concealed under an ordinary examination; and yet the symptoms in his case may be clearly brought out by the method just described. The tongue was quite tremulous.
The writer of No. 6 was more advanced in general paralysis, but had been thought not to be ataxic, from the fact that he had been able to write a single word pretty well. His few lines are quite characteristic of a general paralytic. Although he was in my office in Boston, he dated his statement from his home, and wrote the word Lawrence not badly for a man not in the habit of writing much. Seeing me for the first time, he addressed me as Friend Folsom, and he signed his name by his old army title of nearly twenty years before—corporal.
The characteristic writing in advanced general paralysis, irregular, distorted, full of omissions of letters and words, and finally illegible, may be seen in the textbooks on insanity.
It very rarely happens that the onset and early progress of general paralysis are so sudden and rapid that there is no prodromal period or that it is very short.
The symptoms of well-marked general paralysis include four tolerably distinct types, as follows: (1) The demented and paralytic; (2) the hypochondriacal; (3) with melancholia; (4) with exaltation and mania. There are mixed cases in which some or all of these forms occur. The period of invasion or prodromal period, be it short or long, has, as a rule (not always), gone by when the disease has arrived at a point in its progress to be definitely placed in any or several of these four types.
The demented form of general paralysis is the most common, and is also that in which the greatest increase has been noticed during the last decade, whether from more accurate diagnosis or by reason of an actually greater proportion, probably to a certain extent due to both causes. It consists in a very slowly-advancing mental impairment, making progress side by side with muscular loss of control and power, which may continue several months or years before their importance is appreciated, the vaso-motor disturbances not being so marked as in more acute forms of the disease, and the changes in the mental state and bodily strength from week to week being so slight as to escape observation. Attacks of dizziness, petit mal, and epileptiform seizures are quite common in this type of general paralysis. In one of my cases a lawyer in the third year of the disease was retained as counsel in a will case involving over a million dollars, when he fell repeatedly in the streets, and when his occasional, indeed frequent, mental lapses were so apparent to his partners that they did not allow any of his business letters to leave the office without being first inspected by them. Mental excitement, maniacal symptoms, and delusions of grandeur rarely occur, except as transient attacks, until the final stages. The patient commonly realizes that something is the matter with him until he becomes quite demented, and can often describe his [p. 188] mental state and general symptoms quite intelligently, although rarely with a full appreciation of their extent and import. He easily persuades himself that it is not worth while to take steps for medical treatment, and keeps on with his work until some distinct failure in his mental or physical powers, usually a sense of malaise, muscular pains, a feeling of exhaustion, convinces him and his friends that a physician should be consulted. Perhaps he goes to some health-resort or water-cure, or tries rest and recreation in travel, still thinking his case not an important one, until he seeks medical advice to please his family or friends. He may say that he is only tired mentally and physically.
In the hypochondriacal form of general paralysis, vaso-motor disturbances, flushed or pale face, headache, defective circulation, and various abnormal sensations referred to the peripheral nerves and internal organs are associated with a hypochondriacal mental state, which is also marked by an evident mental impairment, manifested in an almost childish changeability of complaints. Grand delusions and great mental and motor excitement do not, as a rule, appear until the later stages, but the hypochondriacal form is less subacute than the demented.
In general paralysis with melancholia the sad delusions are apt to be associated with some form of expansive ideas or to be transformed into them at some stages of the disease, although the classical delusions of grandeur are a late symptom.
The maniacal form of general paralysis with the délire de grandeur is the disease as described by Calmeil. Mental exhilaration and delusions of personal importance are its conspicuous features. It may develop at any time in the course of the other three forms just mentioned; its prodromal period may be such as has been described, usually shorter, or the symptoms may be of excitement and maniacal from the beginning. It is the general paralysis of the books until within recent years.
It is doubtful whether these four forms of general paralysis depend upon any pathological basis which can now be determined, but their recognition is practically important for an early diagnosis, and they differ from each other very little in their later and final stages. They constitute what is known as the descending form of general paralysis, in the majority of cases of which descending degeneration of the lateral columns of the spinal cord or posterior spinal sclerosis, or both, appear, secondary to the brain disease.
In the ascending form of general paralysis there are posterior spinal sclerosis and the usual symptoms of that condition—which are described in another article of this work—from one year to a dozen or more years before there are indications of dementia.
In the first stage of general paralysis, although a distinct loss of power is an early symptom, it is not so striking in its manifestations as loss of control. The moral obliquity and the mental lapses seem entirely out of proportion to the general mental impairment. What seems moral perversion is often strictly so, but oftener it depends upon a want of attention or appreciation of the facts in the case, which can be aroused if there is opportunity for it. There is a clear inability to use the force that the mind has. The foolish credulity and readiness to be duped are often only a temporary condition. There is, at the same time, an inability to co-ordinate the muscles to a striking degree at a time when there is still [p. 189] only slight impairment of the muscular strength, or inversely, and the co-ordinating power may improve up to a certain point, while the muscular impairment goes on. This ataxia is first noticed in those muscles requiring the nicest adjustment for their usual work, the penman's and the pianist's fingers, the proofreader's eyes, the singer's throat. But it may be for a long time very slight or not easily detected.
Although this muscular ataxia may be observed, even if not constantly, in the prodromal period of general paralysis, it is usually well marked only when the symptoms have become well developed. There is also a fibrillary tremor of one group of muscles or of one set of fibres after another when these muscles are exerted, and increasing as they become wearied, as they soon do, from the exercise. The handwriting may show no conspicuous fault at the top of the page, and at the bottom be full of evidences of muscular tremor and unsteadiness, or a single word may be written without conspicuous fault, and a few lines serve to show ataxia of the muscles used in writing. In beginning to read there may be only the most trifling want of clearness of tone and steadiness of articulation, noticeable only to the most practised ear, which after a number of minutes becomes a distinct harshness of voice or evident stumbling over linguals and labials, or hesitation in speech, which may seem like the utterance of a person slightly under the influence of wine or with lips cold from frosty air. The hesitancy of speech is due partly to a slower flow of ideas than in health, an impaired power of attention to the subject in hand, a diminished creative power or expression of thoughts, but also to a distinct ataxia, an inability to promptly co-ordinate the muscles required to perform the act. The difficulty in reading is partly mental and in part due to inco-ordination of the muscles governing the eyes as well as those of articulation.
These muscular defects and mental inefficiencies, when slight, may be hardly detected after the patient has had a prolonged rest and is quiet and calm. After some emotional irritation, weariness, sleeplessness, vaso-motor disturbances, or congestive attacks they become very pronounced. After several weeks of absolute rest, with the patient still at rest, it may be impossible for a time to find any trace of mental defect or muscular deficiency until the patient has again been put to the strain following some effort. They are very much increased after epileptiform or apoplectiform attacks, which, however, are uncommon so early in the case.
In the progress of the disease, as the mental impairment increases, the reaction of the nervous system to external conditions becomes less active, the mind weakens, the loss of flesh may be, at least in part, regained, a great portion of the irritability and active symptoms disappears, and as the patient grows worse he may seem for a while to his friends to improve.
The leading symptoms of general paralysis of the insane are—(1) vaso-motor, (2) mental, (3) physical.
The vaso-motor symptoms consist in a progressive paresis or lessened power, which in the progress of the disease advances to complete arterial paralysis—at first a functional disorder of impaired innervation, and finally organic. They are marked early by rapid changes in the cerebral circulation, a diminished arterial tension, with occasional or frequent attacks of vertigo, dizziness, or faintness, confusion and incoherence that may amount to a transient dementia, localized and general elevation or [p. 190] depression of the bodily temperature; frequent attacks of congestion or at long intervals, with a flushed face or transient cerebral anæmia, may be marked by sharp emotional disturbances, fits of temper, irritability, maniacal excitement, loss of self-control, etc., or by epileptiform and apoplectiform seizures of various degrees of severity, with or without temporary or transient loss of muscular power, local or of the monoplegic, hemiplegic, or paraplegic nature, of a much less severe character than similar attacks later in the disease, due in part also to organic changes. The circumscribed loss of power of the vessels of the skin leads to various functional disturbances, and finally to paralysis, involving bed-sores, etc. Cyanosis, neuroparalytic hyperæmia of the lungs, bladder, and intestines, cold feet, œdema of the skin, local sweatings, etc. are final evidences of vaso-motor paralysis. Throughout the disease, at least nearly to the end, this vaso-motor paresis and paralysis causes marked variations in the mental state which are too rapid to be accounted for by organic changes.
After there is evidence of definite atrophic and degenerative disease in the brain, as indicated by great mental impairment and muscular paralysis, the mental and physical symptoms may be subject to great changes, without any apparent cause but vaso-motor disturbances, and alternating rapidly from extreme intellectual confusion and absence of mind to a clear, even if temporary, mental state. Less extreme changes in the condition of the mind are common.
The mental symptoms, after the disease is pronounced, consist in an intensification of those already mentioned as characterizing the prodromal period—in an increase in the loss of power of control over all mental operations and in the loss of mental power, the two symptoms making progress side by side. In the form of the disease attended with maniacal excitement the prodromal period is usually shorter than in the others, but may last several years. After the prodromal period has passed the mental impairment increases, so that the judgment, memory, power of attention and expression grow progressively worse; and this impairment constitutes the only characteristic mental state universally present in all stages of general paralysis of the insane—namely, progressive dementia. The accidental symptoms may be those belonging to any type of insanity except logical systematized delusions. They very rarely simulate the states of mental defect and degeneration.
If there are delusions of persecution, they are marked by a degree of confusion or incoherence not compatible with logical inference. The state of melancholia may change rapidly to mania, and the demented form may at an hour's notice become the excited. Where the symptoms of mental exaltation and depression alternate, resembling folie circulaire, the alternation is less regular than in alternating insanity properly speaking; hallucinations of sight and hearing and of all the special senses are quite common, although, as a rule, rather late symptoms, and then confused and often only partially intelligible. There are also all sorts of illusions and delusions.
The impairment of the sense of right and wrong becomes quite marked; the patient loses the sense of property and ownership. In no other disease could the reported case occur of a man, to outward appearance well, going up to a policeman and asking his assistance in rolling off a barrel [p. 191] of liquor which belonged to some one else, and which he meant to appropriate. For this reason what seem to be thefts are very common, and although by that time there is striking mental impairment, it may not be obvious to every-day people. Almost every other moral obliquity occurs, particularly a tendency to drunkenness and every possible violation of the proprieties and laws regarding property and the sexual function. It is all done, too, in such a foolish way that the insanity would be apparent to almost any intelligent person before whom the facts might be fully and clearly placed. There may be a curious consciousness in the patient of the fact that something is the matter with him, and a most extraordinary unconsciousness of what an inordinate fool he is acting. If he can be made to see what folly he is committing, perhaps a few moments later he is saying that he was n-ever b-better in his life. The emotions change most rapidly, and an adroit examiner will have his patient crying over some trifle one moment, and another moment laughing over something equally inconsequent. The prevailing mental state changes as rapidly as the emotions. Violent anger, outbursts of passion, penitence, amusement do not succeed each other more rapidly than indifference, melancholy, and exaltation.
The suicidal idea is common in general paralytics before they become very demented; the suicidal impulse is rarely strong enough to result in anything more than futile attempts at self-destruction. Suicide by deliberation is also rare, for even when it is meditated the weakened, indecisive mind usually fails to prepare adequate plans for its successful issue. Homicidal attempts are not to be expected as a rule, except in the delirium of the states of maniacal excitement or in an outburst of anger for a fancied wrong or deliberately for some trifling reason. Even from suicide and homicide a practised physician or attendant will easily turn the general paralytic who is not maniacal to some amusing or silly thought. He has become credulous, simple-minded, and easily moulded to an expert's wishes, so far as his general conduct is concerned, and yet at any moment he is capable of a furious mania or a violent storm of passion, which after cerebral congestive attacks may be long and severe. Sometimes these symptoms just described may be very pronounced at night and not especially troublesome during the daytime. I have had patients who were dangerous, violent, noisy, deluded at night, and entirely quiet by day, for several months.
The mental state is of progressive impairment. The ideas flow slowly, and there is slowness or hesitation in speech in giving utterance to them, even to the degree of amnesic aphasia. Word-blindness occurs, and word-deafness and the various disturbances of speech associated with the several forms of aphasia. After the dementia is very marked there is often a most extraordinary variation in it. The patient may be confused, incoherent, and to appearance hardly capable of sustained thought, but soon quite able to perform a business transaction. The friends say of such patients, “He is crazy to-day,” or “To-day he is sane;” and this quite independent of the marked increase in the dementia which occurs from organic changes, epileptiform and apoplectiform attacks, after which the advance in the mental impairment is rapid and great. Accompanying dizzy and congestive attacks there is a temporary dementia which may be over in an hour or two.
[p. 192]The patient may recall many long-past events fairly well when he cannot find his way to the dinner-table without blundering, when he does not know morning from afternoon, and after he is unable to dress and undress himself without constant remindings or even actual help. Such paralytics wander off and die of exposure, are picked up by the police as having lost their way or as not knowing where their home is, or fall into some fatal danger from which they have not mind enough to extricate themselves. When the mental impairment has reached this point the lack of mind shows itself in a lack of facial expression, which is so characteristic of the disease that with a practised eye it is recognized as far as the countenance can be distinctly seen; and from this point the progress is commonly quite rapid to absolute dementia, entire inability to form or express thoughts, too little intellect to even attend to the daily natural wants, and a descent to the lowest possible plane of vegetative life, and then death.
At some time or other in the history of general paralysis delusions of grandeur, a general feeling of personal expansiveness or extreme self-satisfaction, may be confidently looked for. In the melancholic and hypochondriacal forms of the disease, as has already been mentioned, they are late symptoms; in the demented type they occur only, for the most part, near the final stage of absolute dementia; and in the excited form they are usually found from the beginning or at least developing from a general feeling of bien-être. They may vary from what would pass as inordinate, silly conceit to a wildness of delirium which stops hardly short of infinity. The patient is the greatest financier, the handsomest man, the best runner, can out-box the champion pugilist, can write the finest sermons. Delusions of this degree, especially in women, are apt to refer to the reproductive faculty or to the qualities which please the opposite sex. One man can make a million dollars a day writing poetry; another is building cities of solid gold; another owns all the railroads in the country, is king over all the earth, god over God; another is running express-trains over his bridge across the Atlantic or has a doctor who comes to see him in a balloon. There is often a depth of vulgarity and obscenity about the delusions which is rarely seen in other diseases. When the grand delusions appear in the melancholic form, they are apt to be tinged with gloom, as of a queen whose diamonds are withheld from her, a lover who is kept from his princess bride, etc. In the hypochondriacal form it may be a crystal liver, a silver stomach, a brain of solid gold, etc.
Delusions of personal belittlement, called micromania, sometimes follow or alternate with the megalomania.
Maniacal excitement is a late symptom in the demented, hypochondriacal, and melancholic forms of general paralysis; and it rarely occurs in them except in the final months of the disease, unless as a direct sequence of congestive, epileptiform, or apoplectiform attacks, and then it lasts usually from a few hours to several days. These attacks may occur at any time without any warning whatever, and may be attended with fury or stupor also. As a matter of fact, they are very rare at an early stage except in the excited form of general paralysis, of which they are a pretty constant symptom until marked dementia has appeared, and they may continue to the end. The fury of these maniacal attacks is of the most furious and maddest kind, blind, the most utterly regardless of consequences [p. 193] of any kind of insane excitement, and without the intelligence even of the acute maniac.
The ability to recognize his own mental state is sometimes retained by the patient, at certain times at least, to a quite late stage in the disease, so that he learns to call his visions hallucinations and his strange fancies delusions. He may even agree that his illusions are all nonsense, that the disease is in his brain. The so-called lucid intervals are not uncommon until the final stage of absolute dementia, when attention, memory, judgment, conception, connection of ideas, imagination, desires, the exercise of the senses, general sensibility, after becoming more and more imperfect are at last completely suspended. The moral sense and finer feelings had gone long before.
Although the story of the mind's decay in general paralysis is a comparatively short one, from a few weeks to four or five years for the prodromal period, and then an average of two or three years for the rest, but varying from a few weeks to a rare extreme of twenty years, there may be at any stage of the disease, except at the very end, a more or less complete remission lasting from a few months to ten years. It is dangerous to say, therefore, that there is any degree of dementia which may not be temporarily at least, or in some part, recovered from. Most of the reported cures of general paralysis have been at last proved to be simply remissions, which may be partial or so complete as to leave no trace to the most practised observer. It is not uncommon to see a remission of six months or a year or two, in which the patient can lead a quiet life; it is seldom that he undertakes responsibilities without bringing the remission rapidly to an end. There are a few cases where active business has been resumed and followed successfully for several years. But there is apt even then to be some deterioration in character, which may amount to an actual moral insanity. An arrest in the downward progress, so that the symptoms remain for a considerable time without essential change, is not very uncommon, and may occur at any stage of the disease.
The physical symptoms of general paralysis consist in impaired control over the muscles, diminished power of co-ordinating them, followed at once by progressive muscular enfeeblement ending in complete paralysis.
The ataxia first shows itself in the finer muscles—of the eye, of the fingers, of articulation. There is a little hesitancy or rather deliberateness of speech, the voice loses its fine quality, the intonation may be slightly nasal. Instead of contracting smoothly and evenly as in health, the muscles show a hardly noticeable jerkiness; an irregular fibrillary tremor is seen when they are exerted to their utmost and held in a state of extreme tension for several moments. In attempts to steady the handwriting the patient forms his letters slowly, makes them larger than usual, or tries to hurry over the letters, making them smaller. The coarser muscles show ataxic symptoms much later. It is observed by the patient or his friends that he does not walk off with his usual rapid gait, and the effort to co-ordinate his muscles produces an early or unusual fatigue, which may be associated with general muscular pain. Extreme soreness and pain, following the course of some one or more of the main nerve-trunks, may be most persistent and obstinate to treatment, lasting for several years, limiting the motion of the limb, [p. 194] sometimes beginning a year or two before other symptoms are observed. Sooner or later, especially after a little weariness or excitement, there are observed at times, not constantly, indistinctness or an occasional trip in enunciating linguals and labials, a tremor in the handwriting, a slight unsteadiness in the gait. When the tongue is protruded as far as possible, when the hands and arms are stretched out, when the muscles of facial expression are exerted, in standing with feet together with closed eyes, a decided muscular tremor and unsteadiness are remarked. These muscular symptoms soon become constant, although they may be so slight as to be well marked only by some unusual test, such as prolonged use after excitement or fatigue, and the ataxia may diminish, the gait, speech, or handwriting may improve, while muscular power is growing progressively less.
In walking the feet are not raised as usual, the steps are shorter, the legs are kept wider apart; turning about is accomplished in a very deliberate way, such as to suggest an insecure feeling; movements like dancing are impossible. Going up and down stairs is difficult; the whole foot is rested carefully on each step, and the head and shoulders are held stiffly, so as to maintain the balance. The muscular movements are generally uneven and tremulous, and yet the strength may not be so very much impaired, although perhaps available only for short periods at a time. Even these symptoms may so improve by a few days' quiet, or even by a night's rest, as to quite throw the physician off his guard unless a thorough examination is made. The patient, too, on an even floor or sidewalk may walk so as not to attract attention, and yet in a new place, over a rough surface, or in the attempt to perform difficult or rapid movements, exhibit striking ataxia and feebleness of gait. In starting off with a definite purpose he may for a short distance walk quite well, as he may do under the influence of a glass of wine.
From this point the progress is usually rapid. The handwriting becomes more and more tremulous, unsteady, full of omissions of letters and words, disjointed, disconnected, and finally illegible; the articulation more thick, stammering, hesitating, indistinct, unintelligible; the gait staggering, shuffling, straddling, uncertain, unsteady, even to causing frequent falls. There may be still a considerable degree of strength for a single short effort, but the co-ordination is so imperfect as to make it avail little. The voice, for instance, may be loud and forcible, but the co-ordination sufficient for only a short explosive utterance of one syllable, and then quite an interval before the force can be concentrated for the next. Progressive muscular paresis becomes finally absolute paralysis.
Remissions in the physical symptoms follow the same general laws as in the mental symptoms, but are not so complete, and there may be an arrest in their progress also.
In all stages of the disease, especially the later, there may be almost any of the symptoms observed which occur in the various functional and organic diseases of the nervous system. The hyperæsthesia, local or general, may be most absolute, or the anæsthesia so complete that acts of self-mutilation ordinarily causing exquisite pain are performed without apparent suffering. Any motor ganglia, any nerve, any tissue, may degenerate, giving rise to various degrees of impairment up to total [p. 195] destruction of function—of the optic nerve, causing blindness; of the auditory, deafness; of the olfactory, glosso-pharyngeal, or any of the cranial or spinal nerves.
The pupils may be of normal size. They may be of normal or sluggish accommodation to light and distance, or there may be dilatation or contraction of either or both pupils and no response to light or accommodation. The pinhole pupil is not uncommon. There may be neuro-retinitis, atrophy of the disc, neuritis, nystagmus, diplopia, amblyopia, hemianopsia, color-blindness, ptosis, conjugate deviation of both eyes, or paralysis of any of the ocular muscles. The paralysis of one of the muscles of the eyeball may be one of the earliest and most persistent symptoms. The optic neuritis or atrophy may also occur early, but seldom appears in time to aid in a doubtful diagnosis.
Sugar has in a few cases been found in the urine; albumen is not uncommon.
The sexual function is commonly exaggerated in the early stages, then diminished, lost, and finally returns in the stage of absolute loss of self-respect and self-control, although it may be impaired from the beginning or not materially changed at first. There may be temporary or persistent incontinence or retention of urine.
At first there is a marked loss of flesh, then a gain. As the muscles lose in power they increase in size, with an interstitial degeneration. The deposit of fat is sometimes enormous. In the final stage there is emaciation.
The convulsive attacks usually are of the nature of cortical epilepsy, or at least commonly begin as such. They are associated with and followed by a considerable rise in temperature—from two to seven degrees F.—and are immediately succeeded by marked increase in the severity of the symptoms, both mental and physical, especially if the attacks follow each other in rapid succession or last for a number of days. They may be due to hemorrhage, embolism, or effusion, and be marked by any or all of the usual symptoms and sequences of those conditions, permanent or transient. General and aural vertigo are not uncommon.
The muscular tremor before the last stages varies in different muscles—excessive perhaps in the tongue, moderate in the fingers, and so on. It may also seem slight as compared with the other symptoms, or, on the other hand, be enormously exaggerated in certain groups of muscles out of all proportion to all other indications. At the end extreme and constant tremulousness accompanies every voluntary movement.
Spastic paralysis, muscular tension, contractures, rigidity of the most persistent character seem at times to be under the influence of the will, although of cortical origin and in a certain sense automatic, like convulsions.
The knee-jerk is changed in somewhat more than half the cases, a little oftener exaggerated than abolished; but sometimes the reflexes are enormously increased all over the body, so that a strong puff of air in the face even will set the arms and legs going like a jumping-jack. I have twice seen the patellar reflex abolished in one leg, and so marked in the other as to seem to me exaggerated.24 I have also known it to disappear [p. 196] absolutely in both legs two weeks after it had been found to be excessively exaggerated. It also varies under conditions of rest, fatigue, excitement, etc. Intense pain in the joints occurs, and I have found it where the knee-jerk was exaggerated, in one case giving rise in a physician to the delusion that his arms and elbows had been resected. This may disappear in time. Charcot's joint disease has been observed.
24 There was no evidence, and there had been no history, of a hemiplegic attack in either case.
In the final stages the bones are fragile and easily break; hemorrhages under the periosteum or perichondrium arise from trifling force or injury, giving rise to hæmatomata, the most common of which are on parts exposed to pressure, etc., as the ear. The patient is confined to his bed, fed like a small child, demented, hardly able to articulate the extravagant delusions which form such a grotesque contrast to his actual state, until the mind is as incapable of forming or receiving ideas as of expressing thoughts; and the body is simply a filthy, helpless mass of humanity, dying of exhaustion or decay, unless lung gangrene, bed-sores superficial and deep, necrobiosis, exhausting diarrhœa, pneumonia, pulmonary consumption, perhaps asphyxia from an epileptic fit or choking, have followed incontinence of urine and feces to the fatal end, or heart failure or apoplexy have closed the scene.
PATHOLOGY AND MORBID ANATOMY.25—General paralysis of the insane is, according to Mendel, following Rokitansky's idea, a connective-tissue disease, affecting the nerve-cells and tissues secondarily, while Tuczek and Wernicke think that the primary disease is of the nerve-elements (primäre Atrophie der Nervenelemente)—a diffuse interstitial cortical encephalitis on the one hand, or a diffuse parenchymatous cortical encephalitis on the other. There is also, in well-marked cases, atrophy of the white substance, due, according to general opinion of pathologists, to primary interstitial encephalitis ending in sclerosis.
25 For a detailed statement of the post-mortem appearances in general paralysis compare Spitzka's Insanity, pp. 218-243; Beiträge zur pathologischen Anatomie und zur Pathologie der Dementia Paralytica, von Dr. Franz Tuczek; Die Progressive Paralyse der Irren, von Dr. E. Mendel; Lehrbuch der Gehirnkrankheiten, von Dr. C. Wernicke, iii. pp. 536-541. Westphal's classical work is not referred to, as his latest views and others of interest are given in a report of a discussion by the German Association of Alienists in the Allgemeine Zeitschrift für Psychiatrie, iv. 1883, pp. 634-638 and 648-654. In the third number of the Neurol. Centralblatt, Mendel reports an autopsy of a patient diagnosticated to have melancholia, who died a violent death, where he thought that he found evidence of the early stage of general paralysis in moderate opacity of the pia mater, with nodules as large as a pin's head in both parietal regions, and in slight indications of diffuse interstitial inflammation of the cortex, the blood-vessels in the frontal convolutions being extensively filled with white blood-corpuscles.
In the majority of cases there is pachymeningitis, often extensive and excessive, with hemorrhages, but which may be no more than is quite commonly found in persons dying of phthisis or chronic nephritis. There is also, usually, leptomeningitis, with adhesions to the cortex, especially of the anterior and antero-lateral portions, so firm that the arachnoid cannot be removed without tearing off portions of the brain; but it is sometimes scarcely observed, and may be no more than is found in persons dying simply of old age. The pia may be in places thickened, opaque, and without adhesions. Ependymitis is usual.
In the terminal stage of general paralysis there is well-marked atrophy (with compensatory serous effusion), which is, as a rule, most marked in the cortex of the brain, but which is of varying degrees in its different [p. 197] portions. Rarely there is scarcely any atrophy of the cortex. The central portion of the brain may be of leathery consistence, but usually shows marked sclerosis, which also may affect its different portions and the different ganglia very differently. The changes resulting from inflammatory, degenerative, and atrophic processes are general and profound.
An opinion is beginning to obtain that general paralysis is primarily a disease of the small cerebral blood-vessels, functional or vaso-motor; and Meynert holds that the transition line between that stage, which he considers curable, and organic disease may be recognized clinically.
In general paralysis, as in other mental diseases, the nervous discharge is accompanied by a greater disturbance in the structure of the gray substance of the brain, a more extensive decompounding of it, and consequently by a more complete exhaustion of nervous force than in healthy mental processes. Longer periods of rest and improved nutrition are therefore necessary to restore healthy function. In general paralysis, as in all other mental diseases dependent upon destructive disease of the brain, there is not only decompounding, but decomposing and disintegrating, of the structure of the brain.
Posterior spinal sclerosis is frequently found. If alone or predominating over sclerosis of the lateral columns of the cord, the knee-jerk is abolished if the morbid process has gone far enough. If descending degeneration of the lateral columns is chiefly found, and is sufficiently advanced, the knee-jerk is increased. At least one of these forms of sclerosis exists in the vast majority of cases.
There is also a distinctly syphilitic disease of the smaller cerebral arteries, together with a diffuse parenchymatous and interstitial encephalitis of syphilitic origin. At present we have no means of differentiating it at the autopsy from general paralysis following a subacute or chronic course, except inferentially from the presence of other evidences of syphilis. It is not always possible, therefore, to distinguish between syphilis and a syphilitic diathesis as the chief factor in diffuse encephalitis.
DIAGNOSIS.—Although a well-marked case of general paralysis is unmistakable, the diagnosis in the early stages or in obscure cases may be extremely difficult. The varying degrees in which the various portions of the cortex, medullary portion, and different ganglia of the brain may be involved in the morbid process naturally give rise to a great variety in the symptoms, mental and physical, sensory and motor, emotional and intellectual, and in the relative preponderance of one or another in individual cases. The usual symptoms of any form of mental disease may for a time obscure the dementia which sooner or later must appear in general paralysis, and which, as has already been said, is the only mental symptom universally present in all cases. This mental impairment must also be associated with progressive muscular loss of power, although the relation of the two symptoms to each other, the degree to which a given amount of the one leads to a fair inference of a certain amount of the other, is liable to the greatest variation, the range of which can only be learned by observation and experience. There is a certain quality to the dementia, as already described, which is often sufficient of itself to establish the diagnosis with a practised physician.
[p. 198]The early mental symptoms may simulate those of cerebral neurasthenia, in which the patient thinks that there is decided mental impairment, although there is no progressive dementia. The tremor in neurasthenia is greater and more universal than in the stage of general paralysis with which it might be confounded, and the subjective symptoms are much more prominent.
Muscular malaise and pains throughout the body give rise to the diagnosis of malaria or rheumatism, in which there may be loss of power, but no ataxia or dementia.
The sclerosis may be predominating or pronounced in the basal ganglia and bulbar nuclei, giving occasion for a hasty diagnosis of labio-glosso-pharyngeal paralysis, until it is found that the clinical history of that disease is not followed. In the same way, any motor or sensory ganglia or nerve-roots may be so early implicated in the degenerative process as to mislead the physician into giving attention to only the local symptoms.
Once I have known the early convulsions of general paralysis in a very self-conscious woman mistaken for hysteria, the mental impairment and physical weakness having been overlooked on account of the prominence of the convulsive attacks and the hysterical symptoms, which may be a complication of any form of insanity in young and middle-aged people, particularly women.
It is not uncommon for the attacks to so thoroughly resemble epilepsy as to be mistaken for it, the dementia not being observed or being supposed to be the ordinary mental deterioration generally following epilepsy. In such cases the progressive dementia, ataxia, and muscular weakness may advance so slowly as to entirely escape observation for a long time, and give rise to the confident diagnosis of epilepsy for five or six years. Epilepsy, however, arising in a vigorous, middle-aged person without evident cause, should always suggest the suspicion of syphilis, cerebral tumor, or general paralysis, when careful scrutiny of all the symptoms will show where it belongs.
Embolisms, hemorrhages, cerebral effusions, more or less diffuse encephalitis from an injury to the head, sometimes give rise to the suspicion of general paralysis, until it is found that its characteristic progressive symptoms do not appear, but chiefly when the history of the case has not been definitely ascertained, or when the usual symptoms of those conditions are not well marked.
Chronic endarteritis, arterio-sclerosis, atheroma of the cerebral arteries may be so diffused as to simulate general paralysis, especially in drunkards and syphilitics, but the symptoms do not advance in the manner characteristic of that disease.
Multiple cerebro-spinal sclerosis of the descending form may be confounded with general paralysis while the symptoms are obscure and consist in change of character, when, indeed, organic disease can only be suspected to be present.
Lead has been known to attack the central nervous system in such a way as to produce an intellectual apathy and muscular weakness somewhat resembling the early stage of the demented form of general paralysis, but without its ataxic symptoms and its regular progress. The presence of lead in the urine, and the marked improvement from the use of [p. 199] iodide of potassium, tonics, and electricity, are sufficient to establish the diagnosis.
Chronic and persistent alcoholism is always attended with some mental impairment, which may so resemble the dementia of general paralysis, with marked moral perversion, mental exaltation, grand delusions, muscular tremor, ataxic symptoms, and impaired muscular power, as to make the diagnosis doubtful for several months, until removal of the cause (alcohol) in the course of time causes the symptoms to so abate as to make the real character of the disease evident.
I have once seen chronic interstitial nephritis without its usual prominent symptoms and with mild uræmic convulsions mistaken for general paralysis.
A tumor of the brain, if not attended with the common symptom of vomiting, may be the cause of convulsions and headache resembling those often seen in general paralysis. Optic neuritis or atrophy is usual in cerebral tumor, but rare in a stage of general paralysis so early that the diagnosis might be doubtful.
Hemorrhagic pachymeningitis also now and then simulates an obscure case of general paralysis in the early stage, but a few weeks at most settle any doubts in the matter.
Although diffuse cerebral syphilis is more apt to be associated with distinctly localized symptoms than the demented form of general paralysis, and although it is characterized by a mental apathy and physical torpor which follow a more regular course with more definite symptoms, resulting in a slow decay, yet there may be doubtful cases in which the differential diagnosis is impossible, and in which antisyphilitic treatment does not throw any light on the subject. Syphilitic new growths, endarteritis, and meningitis may so far improve from the use of mercury or the iodide of potassium as to end in an apparent cure, but in those cases the symptoms are not so marked as to make an exact diagnosis always possible. A distinct syphilitic cachexia is presumptive evidence of syphilitic encephalitis when there is doubt whether the syphilis is the cause or the diathesis.
Profound melancholia is not so often as varying gloom or moderate despondency a symptom of general paralysis. When it is such, there are developed in time the other marks of that disease, and it will only be necessary to hold the diagnosis in reserve for their appearance. The melancholia masks the dementia unless it is very carefully sought for, and the tremor may be as marked in melancholia as in the early stage of general paralysis, but more universal.
Acute mania is not uncommonly mistaken for general paralysis, when, as often happens, the delusions are as expansive and the tremor as great in the mania as in general paralysis; and it may be several months before the differential diagnosis can be made with certainty. In the presence of a high degree of maniacal excitement, with great emotional agitation and muscular tremor, it is difficult to establish the fact of the existence or not of dementia in doubtful cases until it is well developed. Acute mania has been known to constitute the prodromal period of general paralysis for a number of years.
Primary mental deterioration cannot be always differentiated from general paralysis of the demented type in its early stage. After the [p. 200] age of sixty the probabilities are in favor of primary mental deterioration in doubtful cases, but general paralysis occurs—seldom, to be sure—up to the age of sixty-five.
Early senile dementia may simulate general paralysis of the subacute form, but has not its clinical history. General paralysis of the quiet, insidious type and primary mental deterioration have been called premature senility. The three diseased conditions have certain points of similarity, and the pathological processes involved in them do not differ sufficiently to authorize the assumption that they are not closely related, if not simply variations, due to age and other causes, in one morbid process.
Finally, the mental impairment caused by the prolonged use of bromide of potassium and hydrate of chloral has been mistaken for general paralysis, until a critical examination unmistakably showed the presence of the well-known symptoms of those drugs.
In examining the patient it is especially important to avoid leading questions, as in general paralysis and in those conditions which simulate its early stage the mind is in a condition to readily fall into the train of thought suggested to it. The fact should be kept in mind, too, that the symptoms in early general paralysis are so variable as to be sometimes quite evident, and at other times not to be got at with certainty at all or only after long and patient examination; that they sometimes quite disappear under the influence of complete mental and bodily rest; and that in all stages, until near the end, such complete remissions may occur as to make the diagnosis, independent of the history of the case, difficult if not impossible.
A gentleman once committed an offence characteristic of general paralysis in marrying a pretty servant-girl while temporarily away from his home. His wife, daughters, and friends saw that the act was so contrary to his natural character that he was placed in an insane asylum and kept there several weeks under observation for an opinion as to his responsibility. He appeared so well in the absolute quiet and rest that he was declared sane, tried, and sentenced to the State prison, where he showed his marked mental impairment as soon as he was set to work. He could not concentrate his mind sufficiently for the simplest labor, and a couple of years later he was sent to the insane asylum to die, a complete mental and physical wreck, in the late stage of general paralysis.
PROGNOSIS.—The very few reported cures in so common a disease as general paralysis, and the circumstances under which they have been reported, lead to the suspicion that there was an error in diagnosis or that the mistake was made of supposing a remission to be a cure, as has often happened. The course of the disease is more rapid in men than women, and in young persons than in the older. From the galloping cases of a couple of months to those slowly advancing, with long remissions, over twenty years, the average, including the prodromal period, is probably not far from five (perhaps six) years. Collected from asylum statistics, it is given as from two to three years. When I am sure of the diagnosis, I generally say that the patient may die within twenty-four hours (of paralysis of the heart, from suffocation by an accident in an epileptic attack, from choking, from cerebral hemorrhage or effusion, or suddenly with cerebral symptoms of which the autopsy gives no [p. 201] satisfactory explanation), within a short time of intercurrent disease, especially diarrhœa or pneumonia, or that he may live several years, as he probably will, and possibly have a remission, during which he may lead for a while somewhat the same kind of life as other people.
Persons presenting symptoms which can in no way be positively distinguished from those at the beginning of the prodromal period of general paralysis recover, but not many come under the physician's care so early. We are not yet in a position to say whether they were suffering from a mild, transient illness or from what would otherwise have become serious organic disease.
TREATMENT.—Life may be prolonged in general paralysis, and usually is prolonged, by the use of such measures as contribute to the patient's comfort, and which in a general way have already been considered under the head of treatment of mental disease on a previous page.
In my experience, stimulating tonics, wine, and even coffee, increase the morbid cerebral energy of the early stage of the disease, but are sometimes of use later. Cod-liver oil and the hypophosphites do better, and many of the disagreeable symptoms of the period of loss of control over the involuntary muscles are relieved by strychnia. Ergot and the judicious use of the bromides abate the cerebral congestion. Gastro-intestinal disorders, when not controlled by attention to diet, require the usual treatment.
Iodide of potassium in the large or small dose, and mercury, I have never found to benefit those cases of general paralysis with a previous history of syphilis. On the contrary, they have proved debilitating and harmful.
When furious excitement is not relieved by prolonged warm baths, with cool applications to the head if possible, and quiet, chloral is of use, and sometimes opium and its preparations.
Frequently-repeated violent convulsions, the epileptic state, are usually at once mitigated by chloral given by the rectum; the inhalation of nitrite of amyl is reported also to have been of use.
There are few cases in which I find that morphine does not quiet restlessness, calm delusions, abate distressing hallucinations, and make the patient generally more comfortable; and I give it freely, seldom more than twice a day, often almost daily, for two or three years. In this way it can be used in quite moderate doses. Coca also relieves symptoms.
Rest and quiet are most important in all stages of the disease. This can be best accomplished in a quiet private house in the country, which can be made a virtual hospital, and next in a private asylum. But such care is beyond the reach of the vast majority of the insane, to whom the public asylum becomes a necessity. Wherever they are, an orderly life is best for them, with as little irritating interference with their ways or control of them as is possible.
If the results of treatment are in the highest degree unsatisfactory, and consist chiefly in meeting symptoms as they come up, without hope of permanent recovery, it is not impossible that when we can put the patient under treatment at the very beginning of his disease, as we can now do in pulmonary consumption, the prognosis in the former disease may change as much for the better as it has changed in the latter.
A general paralytic is at any time liable to congestive or maniacal [p. 202] attacks of short duration, and so is always, potentially, a dangerous person. In the prodromal period the risk is small; in all stages there will, in the majority of cases, be some warning; but in the developed disease the only safe way is to have some responsible person near at hand, both to prevent the patient from doing harm to others and to save him from injuring himself, whether by intent or through not knowing better than to wander off or fall into all sorts of accidents. In many conditions several should be readily available, or else the security of an asylum must be sought.
In the treatment of general paralysis by society the same rule should obtain as in all forms of insanity—that distinct mental disease is presumptive proof of irresponsibility, or at least of limited responsibility; that a diseased mind means lessened intellectual power throughout and diminished ability to choose the right and avoid the wrong; that there are changes in circulation or nutrition, or some unknown condition in the brain, especially in general paralysis, by virtue of which the mental state and power of self-control vary from time to time, and as a result of which a person seeming responsible one day may have been quite irresponsible some previous day.
INSANITY FROM GROSS LESIONS OF THE BRAIN (tumors, new growths of all kinds, exostoses, spicules or portions of depressed bone, embolisms, hemorrhages, wounds, injuries, cysticerci, etc.) is attended with the usual indications of those conditions which may determine diffuse disorders of the brain, giving rise to any of the symptoms of the various psycho-neuroses and cerebro-psychoses. The lowered mental and moral tone after cerebral hemorrhages is a matter of common observation, and after one an individual is rarely observed to be fully himself again.
The PROGNOSIS is very unfavorable. Although there are rare cases of improvement, the tendency is toward profound dementia.
CEREBRAL SYPHILITIC INSANITY comes either under the head of the insanity last described or belongs to the slowly-advancing dementia with final paralysis already referred to under the head of Diagnosis in General Paralysis, and called by some authorities on mental disease pseudo-paralytic dementia from syphilis.
Antisyphilitic treatment is of value in the first class of cases, and although most of the recoveries end in relapses and incurability, the prolonged use of iodide of potassium seems sometimes to effect a permanent cure. It is claimed that similar treatment is followed by the same result in the cases of dementia with paresis, but the weight of authority, and certainly my own experience, are against that statement.
CHRONIC ALCOHOLIC INSANITY depends upon the vascular and other changes due to abuse of alcohol so long continued that the pathological condition has become organic and incurable. It is commonly associated with delusions of suspicion or persecution. It may be a purely moral insanity, with gross beliefs rather than distinctly insane delusions, and it rarely fails to be at least that when the persistent excessive drinking is kept up until the age of beginning dissolution of the brain. It then gives rise to all sorts of embarrassing complications in regard to property, family relations, and wills. Chronic alcoholic insanity may take the form of mild dementia, by virtue of which the patient cannot control himself, but can be easily kept within bounds of reasonable conduct by various degrees of restraint, from the constant presence of a responsible [p. 203] person to the seclusion of an asylum. In well-marked cases this dementia is associated with muscular weakness, tremor, and exhilaration to such an extent as to simulate general paralysis. It is then called by some—especially French—writers pseudo-paralytic dementia from alcohol.
The condition is susceptible of improvement by removal of the cause, alcohol, and by a carefully-regulated life, hydropathic treatment, etc., but complete recoveries cannot be expected.
SECONDARY DELUSIONAL INSANITY is slowly developed from various mental diseases, incurable or uncured, where the progress to marked dementia is slow, by the persistence of delusions in those forms of insanity characterized by delusions. It is chronic and incurable. In melancholia and mania the mental depression and the exaltation and motor excitement disappear to a great extent, and there are left a slowly-advancing dementia, confusion, and expanding delusions, with apathy or with agitation, for which the asylum is the only safe place unless physical weakness makes the patient harmless. It is either a terminal state in which many forms of insanity end, or a stage through which they pass to terminal dementia. It depends upon incurable, and therefore organic, changes in the brain, like all incurable insanity, although those changes are not yet determined exactly. It might be a question whether chronic delusional insanity properly belongs under the head of Organic Mental Diseases, and a similar criticism may be made regarding terminal dementia. But in this paper no definite classification of insanity is attempted, because our knowledge of the subject is still so indefinite, although the several mental diseases are grouped in a certain order for convenience to the reader and the writer; and this order of course approximately follows natural lines.
TERMINAL DEMENTIA is the end to which most of the insanity not resulting in recovery finally comes. The features marking the disease in its early stages for the most part disappear, leaving all the functions of the mind impaired in all degrees up to total extinction—the whole character on a lower plane. It is the disease which to so great an extent crowds the wards of insane asylums and almshouses with the (1) agitated or (2) apathetic chronic insane, the worst of whom are mental and physical wrecks, squatting on floors, uttering an unintelligible jargon, noisy, filthy, without intelligence for the simplest natural wants. Their chief function, under the prevalent methods of construction and management of lunatic hospitals in most places, is to blight with a certain feeling of hopelessness many of the curable insane who are obliged to go for rest and quiet to institutions where the overwhelming majority of the inmates are manifestly and painfully incurable.
French writers include a great part of chronic delusional insanity (secondary confusional insanity, Wahnsinn, secundäre Verrücktheit) and terminal dementia (Blödsinn) under one head, démence; and with much reason, as it is not always possible to differentiate between the two.
The proper TREATMENT of the incurable, demented insane should provide not only that they be not at large, where they annoy the strong and the well, but also that they shall not disturb the insane who are acutely ill and in need of treatment suited to sick people, and whose chances of recovery at best are none too favorable. Experiments, now quite numerous, have shown that the lives and occupations of many of them may be [p. 204] made not entirely unlike those to which they were reared, and that nearly all may be suitably provided for without the expensive hospitals and appliances necessary for the proper treatment of acute mental disease.
A comparison of countries in which there is and is not a comprehensive system of State supervision of the insane by a competent board seems to me to reveal so unquestionably the fact that such a system alone provides the proper protection for the insane, and the needed variety and uniformly high standard of excellence in the provisions for their treatment, that I hope to see the medical profession using its vast influence upon public opinion to secure it.
If we meet in the wards of our insane asylums hopeless mental and physical wrecks, if we find there the extremity of human wretchedness, the supreme control of all that is evil or vile in our nature, the worst antitypes of all the virtues, so, on the other hand, nowhere else do we see such struggles for the mastery of the better impulses, such efforts against such odds to hold back the mind in an unequal fight. Nowhere else, too, are developed finer sympathy, more beautiful unselfishness, more generous charity, or more heroic resignation where no hope in life remains but for death.
The State has taken charge of these most unfortunate people, shutting up behind the same locked doors and barred windows people of all social grades, often mingling together in one presence the so-called criminal insane, insane criminals, idiots, imbeciles, epileptics, paralytics, the chronic insane, and the demented, with patients suffering from acute mental disease. Some of them are unconscious of their condition, many are better off than ever before, but others are painfully alive to their situation and surroundings, fully aware of the gravity of their illness, keenly sensitive to the distressing sights and associations, disturbed by the noises, and discouraged by the many chances of becoming like the worst incurables around them. The State cannot evade the responsibility of seeing that their confinement is made the least rigorous, wretched, and injurious possible.
DEFINITION.—Hysteria is a functional disease of the cerebro-spinal axis, characterized either by special mental symptoms or by motor, sensory, vaso-motor, or visceral disorders related in varying degree to abnormal psychical conditions.
This, like all other definitions of hysteria, is imperfect. No absolutely satisfactory definition can well be given. It is not abnormal ideation, although this is so often prominent; it is not emotional exaltation, although this may be a striking element; it is not perversion of reflexes and of sensation, although these may be present. Some would make it a disease of the womb, others an affection of the ovaries; some regard it as of spinal, others as of cerebral origin; some hold it to be a disease of the nerves, others claim that it is a true psychosis; but none of these views can be sustained.
Sir James Paget1 says of hysterical patients that they are as those who are color-blind. They say, “I cannot;” it looks like “I will not,” but it is “I cannot will.” Although, however, much of the nature of hysteria is made clear in this explanation, hysteria is not simply paralysis of the will. A true aboulomania or paralysis of the will occurs in non-hysterical patients, male and female, and of late years has been studied by alienists.
1 “Clinical Lecture on the Nervous Mimicry of Organic Diseases,” Lancet for October, November, and December, 1873.
In many definitions the presence of a spasmodic seizure or paroxysm is made the central and essential feature; but, although convulsions so frequently occur, typical hysterical cases pass through the whole course of the disorder without suffering from spasm of any kind.
In a general neurosis a definition, well considered, should serve the purpose of controlling and guiding, to a large extent at least, the discussion of the subject.
The definition given asserts that hysteria is a functional disease. In the present state of knowledge this is the only ground that can be taken. It is claimed that in a strict sense no disease can be regarded as functional; but it is practically necessary to use such terms as functional in reference to affections in which disordered action without recognizable permanent alteration of structure is present. Temporary anatomical changes must sometimes be present in hysteria; organic disease may be a complication in special cases; post-mortem appearances may [p. 206] occasionally be found as accidents or coincidences; it is possible that structural alterations may result from hysteria; but no pathologist has as yet shown the existence of a special morbid anatomy underlying as a permanent basis the hysterical condition.
The mental, motor, sensory, and other phenomena of hysteria cannot be explained except by regarding the cerebro-spinal nervous system as the starting-point or active agency in their production.
The term vaso-motor is used in a broad sense to include not only peripheral vascular disturbances, but also cardiac, respiratory, secretory, and excretory affections of varying type. Some of these disorders are also visceral, but under visceral affections are also included such hysterical phenomena as abdominal phantom tumors, hysterical tympanites, and the like.
That all hysterical phenomena are related in varying degree to abnormal psychical conditions may perhaps, at first sight, be regarded as open to dispute and grave doubt. It is questionable whether in every case of hysteria the relation of the symptoms to psychical states could be easily demonstrated. I certainly do not look upon every hysterical patient as a case of insanity in the technical sense, but hold that a psychical element is or has been present, even when the manifestations of the disorder are pre-eminently physical. James Hendrie Lloyd,2 in a valuable paper, has ably sustained this position, one which has been held by others, although seldom, if ever, so clearly defined as by this writer.
2 “Hysteria: A Study in Psychology,” Journal of Nervous and Mental Disease, vol. x., No. 4, October, 1883.
The alleged uterine origin of hysteria has been entirely disregarded in the definition. This has been done intentionally. It is high time for the medical profession to throw off the thraldom of this ancient view. The truth is, as asserted by Chambers,3 that hysteria “has no more to do with the organs of reproduction than with any other of the female body; and it is no truer to say that women are hysterical because they have wombs, than that men are gouty because they have beards.”
3 Brit. Med. Journ., December 21, 1861, 651.
SYNONYMS.—Hysterics, Vapors. Many Latin and other synonyms have been used for hysteria: most of these have reference to the supposed uterine origin of the disease, as, for instance, Uteri adscensus, Asthma uteri, Vapores uterini, Passio hysterica, Strangulatio uterina seu Vulvæ. Some French synonyms are Maladie imaginaire, Entranglement, and Maux ou attaques de nerfs. Other French synonyms besides these have been used; most of them are translations from the Latin, having reference also to the uterine hypothesis. In our language it is rare to have any other single word used as a synonym for hysteria. Sir James Paget4 introduced the term neuromimesis, or nervous mimicry, and suggested that it be substituted for hysteria, and neuromimetic for hysterical. Neuromimesis is, however, not a true synonym. Many cases of hysteria are cases of neuromimesis, but they are not all of this character. Among the desperate attempts which have been made to originate a new name for hysteria one perhaps worthy of passing notice is that of Metcalfe Johnson,5 who proposes to substitute the term ganglionism, as giving a clue to the pathology of hysteria. His main idea is that [p. 207] hysteria exhibits a train of symptoms which are almost always referable to the sympathetic or ganglionic nervous system. This is another of those half truths which have misled so many. The term hysteria, from the Greek ὑστερα, the uterus, although attacked and belabored, has come to stay; it is folly to attempt to banish it.
4 Op. cit.
5 Med. Times and Gaz., 1872, ii. 612.
METHOD OF DISCUSSING THE SUBJECT.—It is hard to decide upon the best method of discussing the subject of hysteria. One difficulty is that connected with the question whether certain affections should be considered as independent disorders or under some subdivisions of the general topic of hysteria. Certain great phases of hysteria are represented by hystero-epilepsy, catalepsy, ecstasy, etc.; but it will best serve practical ends to treat of these in separate articles. They have distinctive clinical features, and are capable of special definition and discussion.
HISTORY AND LITERATURE.—To give a complete history of hysteria it would be necessary to traverse the story of medicine from the time of Hippocrates to the present. A complete bibliography would require an immense volume. Volume vi. of the Index Catalogue of the Library of the Surgeon-General's Office, United States Army, which has appeared during the present year (1885), contains a bibliography of nearly seventeen double-column pages, most of it in the finest type. The references are to 318 books and 914 journals. The number of books and articles cited as having appeared in different languages is as follows: Latin, 99; Greek, 2; German, 180; British, 177; American, 159; French, 449; Italian, 75; Spanish, 45; Swedish, 12; miscellaneous, 34. Even this wonderful list probably only represents a tithe of the works written on this subject. Those desirous of studying it from a bibliographical point of view can do so by consulting this great work.
Many as are the names and voluminous as is the literature, certain names and certain works are pre-eminent—Sydenham, Laycock, and Skey in England; Tissot, Briquet, Charcot, and Landouzy in France; Stahl, Frank, Eulenburg, and Jolly in Germany; and in America, Weir Mitchell. The greatest work on hysteria is the treatise of Briquet.6
6 Traité clinique et thérapeutique de l'Hystérie, par le Dr. P. Briquet, 1859.
Mitchell7 has organized into a scientific system a valuable method of treating hysteria, and has given to the world a series of studies of some types of the affection best or only seen in the United States.
7 Fat and Blood: An Essay on the Treatment of Certain Forms of Neurasthenia and Hysteria, and Clinical Lecture on Diseases of the Nervous System, especially in Women.
Among other American monographs on hysteria and allied subjects worthy of note are the contributions of Shaffer on The Hysterical Element in Orthopædic Surgery;8 Seguin's essay on Hysterical Symptoms in Organic Nervous Affections;9 Beard's volume on Nervous Exhaustion;10 the chapters on Hysterical Insanity, etc. in Hammond's text-books;11 and the papers of G. L. Walton12 on Hystero-epilepsy. Spitzka, Mann, Hughes, and [p. 208] Kiernan have made important contributions to the psychical aspects of the subject in various American medical journals.
8 The Hysterical Element in Orthopædic Surgery, by Newlin M. Shaffer, M.D., New York, 1880.
9 Archives of Neurology and Electrology, for May, 1875, and Opera Minora, p. 180.
10 A Practical Treatise on Nervous Exhaustion (Neurasthenia), by George M. Beard, A.M., M.D., New York, 1880.
11 A Treatise on Diseases of the Nervous System, and A Treatise on Insanity in its Medical Relations.
12 Brain, vol. v. p. 458, Jan., 1883; Journal of Nervous and Mental Disease, vol. xi. p. 425, July, 1884.
During the last five years I have published a number of articles and lectures on the subject of hysteria and hystero-epilepsy, some of which have been freely used in the preparation of this and the succeeding sections.13 My first paper on hystero-epilepsy, in the American Journal of the Medical Sciences, was written to strongly direct the attention of the American profession to the subject as studied in France. It was in large part a translation from the works of Charcot, Richer, and Bourneville, with, however, notes of some observed cases.
13 “Hystero-epilepsy,” American Journal of the Medical Sciences, October, 1881.
“Epileptoid Varieties of Hystero-epilepsy,” Journal of Nervous and Mental Diseases, October, 1882.
“Illustrations of Local Hysteria,” Polyclinic, vol. i., Nos. 3 and 4, September 15, October 15, 1883.
“Clinical Lecture on the Treatment of Hysterical Paralysis by Rest, Massage, and Electricity,” Med. and Surg. Reporter, vol. 1. p. 168, February 9, 1884.
“Clinical Lecture on the Differential Diagnosis of Organic from Hysterical Hemianæsthesia, etc.,” ibid. vol. 1. p. 233, 265, February 23, March 1, 1884.
“Clinical Lecture on Spinal Traumatisms and Pseudo-Traumatisms,” Polyclinic, vol. i. No. 9, March 15, 1884.
“A Case of Nymphomania, with Hystero-epilepsy, etc.,” Medical Times, vol. xv. p. 534, April 18, 1885.
“Hystero-epilepsy in the Male, etc.,” Medical Times, vol. xv. p. 648, May 30, 1885.
“Some Forms of Myelitis, their Diagnosis from each Other and from Hysterical Paraplegia,” Medical News, vol. xlvii., Nos. 7 and 8, August 15 and 22, 1885.
“Clinical Lecture on Acute Mania and Hysterical Mania,” Medical Times, vol. xvi. p. 153, November 28, 1885.
PATHOLOGY.—Strictly speaking, hysteria cannot be regarded as having a morbid anatomy. In an often-quoted case of Charcot's,14 an old hystero-epileptic woman, affected for ten years with hysterical contracture of all the limbs, sclerosis of the lateral columns was found after death. On several occasions this woman experienced temporary remissions of the contracture, but after a last seizure it became permanent. This is one of the few reported cases showing organic lesion; and this was doubtless secondary or a complication. In a typical case of hystero-epilepsy at the Philadelphia Hospital, a report of which was made by Dr. J. Guiteras,15 the patient, a young woman, died subsequently while in my wards. Autopsy and microscopical examination revealed an irregularly diffused sclerosis, chiefly occupying the parieto-occipital region of both cerebral hemispheres. Undoubtedly, as suggested by Charcot, in some of the grave forms of hysteria either the brain or spinal cord is the seat of temporary modification, which in time may give place to permanent material changes. Old cases of chronic hysteria in all probability may develop a secondary degeneration of the cerebro-spinal nerve-tracts, or even degeneration of the nerve-centres themselves may possibly sometimes occur. Two cases now and for a long time under observation further indicate the truth of this position. One, which has been reported both by H. C. Wood16 and myself,17 is a case of hysterical rhythmical chorea in a young woman. Although the hysterical nature of her original trouble cannot be doubted, she now has contractures of all the extremities, which seem to have an organic basis. The other patient is a woman who has [p. 209] reached middle life; she has several times temporarily recovered from what was diagnosticated as hysterical paraplegia, in one instance the recovery lasting for months. Now, after more than four years, she has not recovered from her last relapse. Contractures, chiefly in the form of flexure, have developed, and she has every appearance of organic trouble, probably sclerosis or secondary degeneration of the lateral columns.
14 Leçons sur les Maladies du Système nerveux.
15 Philadelphia Medical Times, 1878-79, ix. 224-227.
16 Ibid., vol. xi. p. 321, Feb. 26, 1881.
17 Ibid., vol. xii. p. 97, Nov. 19, 1881.
Briquet18 reviews the various hypotheses which have been held as to the pathological anatomy of hysteria, giving a valuable summary of the autopsies upon supposed hysterical cases up to the time of the publication of his treatise in 1859. About the sixteenth century, Rislau, Diemerbroeck, and Th. Bonet sought to establish a relation between lesions of the genital organs met with in the bodies of hysterical women and the affection from which they suffered. About 1620, Ch. Lepois believed that he had established the existence of certain alterations of the brain in cases of hysteria. Hochstetter and Willis toward the beginning of the present century arrived at similar conclusions. That researches into the state of the genital organs have chiefly occupied those investigating hysteria is shown by the writings of Pujol, Broussais, Lovyer-Villermay, and, above all, by those of Piorry, Landouzy, Schutzenberger, and Duchesne-Duparc. Georget, Brachet, Girard, Gendrin, Bouillaud, Forget, and Lelut, about the fourth or fifth decades of the present century, made numerous autopsies on those dying when hysterical phenomena were in full activity, and concluded that the genital organs of these individuals revealed nothing in particular. This, in brief, is also the conclusion of Briquet. Jeanne d'Albret, the mother of Henry IV., who was all her life subject to hysterical headache, had her brain examined after death, but absolutely nothing was found. Vesalius made an autopsy with equally negative results on a woman who died from strangulation in an hysterical attack. Royer-Collard also found nothing in an old hysteric. Briquet believed—and I fully accord with this view—that in some of the cases of Ch. Lepois, Hochstetter, and Willis diseases such as chronic meningitis were present with the hysteria. He concludes that anatomy does not show anything positive as to the seat or nature of hysteria, except the suspicion of a certain degree of congestion in various parts of the brain.
18 Op. cit.
While, however, hysteria may not have a morbid anatomy, it, like every other disease, has, in a correct sense, a pathology.
The ancients saw only the uterus when regarding hysteria. Hippocrates described the hysterical paroxysm and its accompanying disorders under the name of strangulation of the uterus. The ancients generally supposed that the disease originated in the ascent of the uterus to the diaphragm and throat. They believed that this accommodating organ could wander at will throughout the body, doing all manner of mischief. Hippocrates asserted that it was the origin of six hundred evils and innumerable calamities.
According to Sydenham,19 the disorders which are termed “hysterical in women and hypochondriac in men arise from irregular motions of the animal spirits, whence they are hurried with violence and too copiously to a particular part, occasioning convulsions and pain when they exert [p. 210] their force upon parts of delicate sensation, and destroying the functions of the respective organs which they enter into, and of those also whence they came; both being highly injured by this unequal distribution, which quite perverts the economy of nature.” Speaking of the strangulation of the womb, or fits of the mother, he says: “In this case the spirits, being copiously collected in the lower belly and rushing with violence to the fauces, occasion convulsions in all the parts through which they pass, puffing up the belly like a ball.”
19 The Entire Works of Dr. Thomas Sydenham, newly made English from the Originals, etc., by John Swan, M.D., London, 1763, pp. 416, 417.
After a time, the idea that the uterus was the exclusive seat of hysteria was in large measure supplanted by the view that the sexual organs in general were concerned in the production of hysterical phenomena. Romberg defined hysteria as a “reflex neurosis caused by genital irritation.” Woodbury20 concludes as late as 1876 that only where the pathological source of hysterical symptoms resides in the uterus or ovaries, cases may, with some show of propriety, be termed hysterical; and where the uterus and organs associated with it in function are not in a morbid condition no symptoms can be correctly called hysterical.
20 Medical and Surgical Reporter, December 2, 1876.
Bridges,21 another American writer, in a paper on the pathology of hysteria, says that hysteria does not occur most frequently in women with diseased wombs, but in those whose sexual systems, by pampering and other processes, are abnormally developed and sensitive. He makes the same point with reference to the male sex. Sometimes, however, besides the emotional state in the male, there is actual disease of the sexual organs, caused by abuse or over-indulgence. Uterine disease and hysteria are sometimes like results of one cause, and not respectively cause and effect: women are hysterical oftener than men because the uterine function in woman's physiology plays a more important part in the production of emotional diseases than any organ of the male sex.
21 Chicago Medical Examiner, 1872, xiii. 193-199.
The truth would seem simply to be, that, as the uterus and ovaries are the most important female organs, they are therefore a frequent source of reflex irritation in hysterical patients.
Seguin22 adopts with some reservation Brown-Séquard's hypothesis that cerebral lesions produce the symptoms which point out their existence, not by destroying organs of the brain, but by setting up irritations which arrest (inhibit) the functions of other parts of the encephalon. He says that he finds no difficulty in believing that the same symptom may exist as well without as with a brain lesion. “In typical hysteria the functions of parts of the encephalon included in the right hemisphere, or in physiological relation with it, are inhibited by a peripheral irritation starting from a diseased or disordered sexual apparatus or other part; and in case of organic cerebral disease the same inhibitory action is produced. In both kinds of cases we may have loss of rational control over the emotions, loss of voluntary power over one-half of the body, and loss of sensibility in the same part.”
22 “On Hysterical Symptoms in Organic Nervous Affections,” Archives of Electrology and Neurology, for May, 1875.
Simply as a matter of passing interest, the attempt of Dupuy23 to frame a pathology of hysteria is worthy of attention. According to him, every [p. 211] local hysterical phenomenon is dependent upon an abnormal state of either lateral half of the upper part of the pons varolii. The centres of the pons, he holds, are perhaps merely passive in the process, only becoming organically implicated when various forms of permanent contractures and paralyses ensue.
23 Medical Record, New York, 1876, ii. 251.
The pathology of hysteria must be considered with reference to the explanation of the exact condition of the cerebro-spinal axis during the existence of certain special grave phenomena of hysteria, such as hemianæsthesia, hemiplegia, paraplegia, and contractures.
What is the probable state of the nerve-centres and tracts during these hysterical manifestations? If, for example, in a case of hysterical hemianæsthesia it is admitted that the brain of the other side of the body is somehow implicated, although temporarily, what is the probable condition of this half of the brain? Is the cerebral change vascular or is it dynamic? If vascular, is the state one of vaso-motor spasm or one of paresis, or are there alternating conditions of spasm and paresis? Are true congestions or anaæmias present? If the condition is dynamic, what is its nature? Is it molecular? and if molecular in what does it consist? Is it possible to say absolutely what the pathological condition is in a disorder in which autopsies are obtained only by accident, and even when obtained the probabilities are that with fleeting life depart the changes that are sought to be determined?
Two hypotheses, the vaso-motor and the dynamic, chiefly hold sway. The vaso-motor, attractive because of its apparent simplicity, has been well set forth by Walton,24 who contends that while it may not be competent to easily explain all hysterical symptoms, it will best explain some of the major manifestations of hysteria—for example, hemianæsthesia. Hemianæsthesia, he argues, may appear and disappear suddenly; it may be transferred from one side of the body to another in a few seconds; so blood-vessels can dilate as in a blush, or contract as in the pallor of fear, in an instant. In fainting the higher cerebral functions are suspended, presumably because of vaso-motor changes; therefore the sudden loss of function of one-half of the brain-centres, seen sometimes in hysterical hemiplegia and hemianæsthesia, may easily be imagined to be the result of an instantaneous and more or less complete contraction of cortical blood-vessels on that side. Neurotic patients have a peculiarly irritable vaso-motor nervous system. He records a case seen in consultation with H. W. Bradford. The patient had a right-sided hemianæsthesia, including the special senses, the sight in the left eye being almost wanting. The fundus of the right eye was normal; the left showed an extreme contractility of the retinal blood-vessels under ophthalmoscopic examination; these contracted to one-third their calibre, and the patient was unable to have the examination continued. The explanation offered is, that spasm of the blood-vessels on the surface of the left cerebral hemisphere had caused, by modification of the cortical cells, a right-sided hemianæsthesia, including the sight, and by reaching the meninges a left-sided spastic migraine, and by extending to the fundus of the left eye an intermittent retinal ischæmia.
24 Journal of Nervous and Mental Disease, vol. xi., July, 1884, p. 424 et seq.
The vaso-motor hypothesis is held by Rosenthal,25 who, however, wrongly [p. 212] gives the spinal cord the preponderating part in the production of the symptoms. According to this author, the anæsthesia and analgesia present in hysteria conform to the law as established by Voigt with regard to the distribution of the cutaneous nerves. The sensory nerves form at the periphery a sort of mosaic corresponding to an analogous arrangement in the spinal cord. “It is evident,” he says, “that the peripheral disorders in hysteria merely represent an exact reproduction of the central changes, and that the latter are situated, in great part, in the spinal cord.” He attributes a large part of the symptoms of hysteria to a congenital or acquired want of resistance of the vaso-motor nervous system. “Motor hysterical disorders are also due in the beginning to a simple functional hyperæmia, but in certain forms the chronic hyperæmia may lead to an inflammatory process which may terminate (as in Charcot's case) in secondary changes in the columns of the cord and nerve-roots.” When the brain is involved in hysteria, he holds that the most serious symptoms must be attributed to reflex spasms of the cerebral arteries and to the consequent cerebral anæmia.
25 “A Clinical Treatise on Diseases of the Nervous System,” by M. Rosenthal, Vienna, translated by L. Putzel, M.D., vol. ii. Wood's Library, New York, 1879.
The dynamic pathology of hysteria is probably believed in by most physicians, and yet it is difficult to explain. Thus, Briquet26 says that hysteria manifests itself by derangement of the nervous action, and what is called nervous influence is something like electricity. It is simply the result of undulations analogous to those which produce heat and light; in other words, it is a mode of movement. Wilks27 compares some of the conditions found in hysteria to a watch not going; it may be thought to be seriously damaged in its internal machinery, yet on looking into it there is found a perfect instrument that only needs winding up. As regards the brain being for a time functionless, the possibility of this is admitted by all, as in sleep or after concussion. He mentions the case of a young girl who had been assaulted, and had complete paralysis of motion and sensation. The shock had suspended for a time the operations of her brain, and organic life only remained. We have only to suppose that half of the brain is in this way affected to account for all the phenomena of hemianæsthesia.
26 Op. cit.
27 Lectures on Diseases of the Nervous System, delivered at Guy's Hospital, by Samuel Wilks, M.D., F. R. S., Philada., 1883.
According to the dynamic view, the central nervous system is at fault in some way which cannot be demonstrated to the eye or by any of our present instruments of research. The changes are supposed to be molecular or protoplasmic, rather than vaso-motor or vascular.
As innervation and circulation go hand in hand or closely follow each other, my own view is that both vaso-motor and molecular changes, temporary in character, probably occur in the central nervous system in grave hysterical cases.
Whatever the temporary conditions are, it is evident, on the one hand, that they are not states of simple anæmia or congestion, and, on the other hand, that they are not inflammations or atrophies. Patients with hysterical manifestations of the gravest kind as a rule are free for a time from their harassing and distressing symptoms. This could not be if these symptoms were due to lesions of an organic nature. Sudden recoveries also could not be accounted for if the changes were organic.
[p. 213]Lloyd28 contends that most hysterical symptoms, if not all, are due to abnormal states of consciousness. The development of this idea constitutes his argument for the recognition of the disease as a true psychosis. In the reflex action, not only of the lower spinal cord and ganglia of special sensation, but of the highest centres of the brain, he sees the explanation of many of the characteristics of hysteria. In other words, he finds that the sphere of the disease is more especially in the automatic action of the brain and cord.
28 Op. cit.
Dercum and Parker29 have published the results of a series of experiments on the artificial induction of convulsive seizures which bear upon this discussion of the pathology of hysteria. The experiments were performed by subjecting one or a group of muscles to a constant and precise effort, the attention being at the same time concentrated on some train of thought. The position most frequently adopted was the following: The subject being seated, the tips of the fingers of one or both hands were placed upon the surface of the table, so as to give merely a faint sense of contact—i.e. the fingers were not allowed to rest upon the table, but were held by a constant muscular effort barely in contact with it.
29 Journal of Nervous and Mental Disease, vol. xi., October, 1884, pp. 579-588.
Tremors commenced in the hands; these became magnified into rapid, irregular movements which passed from one limb or part to another until the subject was thrown into strong general convulsions. Opisthotonos, emprosthotonos, and the most bizarre contortions were produced in various degrees. No disturbances of sensation were at any time present. Disturbances of respiration and phonation were often present in a severe seizure, and the circulatory apparatus was profoundly affected. A flow of tears, and occasionally profuse perspiration, were sometimes induced. After severe seizures large quantities of pale urine were passed. The reflexes were distinctly exaggerated. No unconsciousness was ever observed, but a progressive abeyance or paresis of the will. Nitrite of amyl seemed to arrest the convulsive seizures at once.
In attempting to explain these phenomena Dercum and Parker refer to the induction of Spencer as to the universality of the rhythm of motion. Through the whole nervous system of every healthy animal a constant rhythmical interchange of motion takes place. What might be called nervous equilibration results. In man the will modifies and controls the action of the nervous system; it assists in maintaining nervous equilibrium when it is threatened. The will being withdrawn from the nervo-muscular apparatus, and this being subjected to strain, a disturbance takes place. This same explanation may be applied to some of the convulsive and other phenomena of hysteria.
Comparing and analyzing the various views, it may be concluded with reference to the pathology of hysteria as follows:
(1) The anatomical changes in hysteria are temporary.
(2) These changes may be at any level of the cerebro-spinal axis, but most commonly and most extensively cerebral.
(3) They are both dynamic and vascular: the dynamic are of some undemonstrable molecular character; the vascular are either spastic or paretic, most frequently the former.
(4) The psychical element enters in that, either, on the one hand, violent mental stimuli which originate in the cerebral hemispheres are [p. 214] transmitted to vaso-motor conductors,30 or, on the other hand, psychical passivity or torpor permits the undue activity of the lower nervous levels.
30 Rosenthal.
ETIOLOGY.—Heredity has much to do with the development of hysteria. It is not that it is so frequently transmitted directly after its own kind, but this disorder in one generation generally indicates the existence of some ancestral nervous, mental, or diathetic affection.
Briquet31 has shown that of hysterical women who have daughters, more than half transmit the disease to one or several of these, and, again, that rather more than half of the daughters of the latter also become hysterical. Amann, according to Jolly,32 has stated that in 208 cases of hysteria he proved with certainty an hereditary tendency 165 times—that is, in 76 per cent. This is too big to be true.
31 Op. cit.
32 Ziemssen's Cyclopædia of the Practice of Medicine, vol. xiv., American translation.
Briquet has also made some careful investigations into the subject of the health of infants born of hysterical mothers. The investigations were based upon a study of 240 hysterical women, with whom he compared 240 other patients affected with such diseases as fever, phthisis, cancer, diseases of the heart, liver, and kidneys, but without any hysterical symptoms. In brief, the result of his investigations was that children born of hysterical mothers die more frequently and at a younger age than those who are born of mothers not hysterical.
The relation of hysteria to certain morbid constitutional states has long been recognized, particularly its connection with the tubercular diathesis. This has been shown by numerous observers, especially among the French. The most valuable recent contribution is that of Grasset,33 who believes that a direct connection can be traced between the tubercular diathesis and hysteria. When the relations of hysteria to the scrofulous and tubercular diathesis are spoken of by him, it is not meant that hysterical subjects have tubercles in the lungs, but that these diatheses are found in various generations, and that among some subjects of the hereditary series the constitutional states manifest themselves as hysteria. It is not the evidences of hysteria with pulmonary and other tuberculous conditions that he is considering, but that hysteria may be, and often is, a manifestation of the tubercular diathesis. Two cases may present themselves: in one the neurosis is the only manifestation of the diathesis; in the other, it is continued in the same subject along with the other diathetic manifestations. In demonstration of his thesis he concludes with a series of most interesting cases, which he arranges into two groups. In the first, hysteria is the only manifestation of the tubercular diathesis; in the second, are simultaneous pulmonary and hysterical manifestations. In the first group he has arrayed eight personal observations and seventeen derived from various authors; in the second he has two personal and seventeen compiled observations.
33 “The Relation of Hysteria with the Scrofulous and the Tubercular Diathesis,” by J. Grasset, Brain, Jan., April, and July, 1884.
Personal experience and observation go far to confirm the views of Grasset, although I recognize fully the strength of the objection of Brachat and Dubois and others that, phthisis being such a common complaint, it might be demonstrated by statistics that it was related to [p. 215] almost any disease. Not only hysteria, but other neuroses or psychoses, have a close connection with the tubercular diathesis.
Among the insane and idiotic and among epileptics phthisis is of frequent occurrence. At the Pennsylvania Training School for Feeble-minded Children the frequency of phthisis among the inmates of the institution is one of the most striking clinical facts. The insane of our asylums die of pulmonary troubles oftener almost than of any other disease. The fact that hysteria is met with in the robust and vigorous does not invalidate the position taken, for the robust and vigorous who are not hysterical are not infrequently found in the descendants of the tuberculous.
Laycock34 believed that the gouty diathesis was particularly liable to give rise to the hysterical paroxysm or to irregular forms of hysteria. Gairdner, quoted by Handfield Jones,35 supports this view.
34 A Treatise on the Nervous Diseases of Women, by Thomas Laycock, M.D., London, 1840.
35 Studies on Functional Nervous Disorders.
Gout in England plays a greater part in the production of nervous and other disorders than in this country, but even here its instrumentality is too often overlooked. In Philadelphia are many families, some of them of English origin, in which gout has occurred, sometimes of the regular type, but oftener of anomalous forms. Among the most striking examples of hysteria that have fallen under my observation, some have been in these families. In a few of them remedies directed to the lithæmic or gouty conditions in connection with other measures have been efficient. More frequently they have failed, for while a relation may exist between the neurotic disorder and the diathesis, it is not the diathesis, but the neurotic disorder, which we are called upon to treat.
That a certain mental constitution predisposes to hysteria cannot be doubted. Ribot36 describes, chiefly from Huchard,37 the hysterical constitution. It is a state in which volition is nearly always lacking. The prominent trait is mobility. The hysterical pass with increditable rapidity from joy to sadness, from laughter to tears; they are changeable, freakish, or capricious; they have fits of sobbing or outbursts of laughter. Ch. Richét compares them to children, who oftentimes can be made to laugh heartily while their cheeks are still wet with tears. Sydenham says of them that inconstancy is their most common trait: their sensibilities are aroused by the most trivial cause, while profounder emotions scarcely touch them. They are in a condition of moral ataxy, lacking equilibrium between the higher and lower faculties.
36 Diseases of the Will.
37 Axenfeld et Huchard, Traité des Neuroses, 2d ed., 1883, pp. 958-971.
As to sex, it is almost unnecessary to say that hysteria occurs with greater frequency among females than males; and yet it is all important to emphasize the fact that it is not exclusively a disease of the former sex. Some statistics on this subject have been collected. In Briquet's often-quoted 1000 cases of hysteria, 50 only occurred in men. I believe, however, that the proportion of hysterical men to hysterical women is greater than this. Instead of a ratio of 1 to 20, as these statistics would indicate, 1 to 15 would probably be nearer the truth. Statistics upon this subject are deceptive.
The occurrence of hysteria in the male was little discussed before the publication of Briquet's great work, but since that time it has received [p. 216] great attention from the medical profession. Charcot38 in some recent lectures at Salpêtrière has called attention to this subject. From 1875 to 1885 he says that five doctoral theses have been written on hysteria in men. Batault has collected 218 and Klein 80 cases. The Index Catalogue contains 102 references to hysteria in the male.
38 Le Progrès médical, 1885.
Hysteria in men may take on almost any form that it shows in women. It may occur in the strong, although more likely to be seen among the weak and effeminate. Even strong, vigorous workmen are susceptible, at times, to hysteria. According to Charcot, the duration of the affection differs somewhat in the two sexes. In male patients it lasts a long time and the symptoms are troublesome; in females the contrary is usually although not always the case. The occurrence of hysteria in the male sex has probably been overlooked through the tendency to class symptoms which would be regarded as hysterical in women as hypochondriacal in men.
One of the most typical half-purposive hysterical attacks that has ever come under my observation was in a literary man of some prominence. Hysterical syncope, contracture, hysterical breathing, hysterical hydrophobia, coccygodynia, hemiparesis, hemianæsthesia, and blindness are some other forms of hysteria in the male of which there are clinical records the result of personal observation. A remarkable case of hysterical motor ataxy was seen in a boy who was for some time a patient at the Philadelphia Polyclinic. Wilks39 records several interesting cases of hysteria in boys. One simulated laryngismus stridulus, with paroxysmal suffocative attacks and barking. Another was a case of hysterical maniacal excitement; another was an example of malleation, or constant movement as in hammering; still others were instances of extreme hyperæsthesia, of anorexia, and of nervous dyspnœa. The same author also dwells on the hysterical perversion of the moral sense found in boys as in girls. He gives some instances clipped from English newspapers—attempts to poison, murder or attempts to murder, confessions false and true. Many instances could be added from our own sensational American sheets.
39 Op. cit.
No age is free from a liability to hysteria. Its occurrence, however, at certain periods of life with great frequency is well known. The following table has been arranged from tables given by Briquet and Jolly, and shows that it is of most frequent occurrence between the ages of fifteen and thirty:
| Age. | Landouzy. | Georget. | Beau. | Briquet. | Scanzoni. | Total. |
| 0-10 | 4 | 1 | — | 66 | — | 71 |
| 10-15 | 48 | 5 | 6 | 98 | 4 | 161 |
| 15-20 | 105 | 7 | 7 | 140 | 13 | 272 |
| 20-25 | 80 | 4 | 3 | 71 | 64 | 289 |
| 25-30 | 40 | 3 | — | 24 | ||
| 30-35 | 38 | — | — | 9 | 78 | 149 |
| 35-40 | 15 | — | — | 9 | ||
| 40-45 | 7 | 1 | — | 1 | 44 | 65 |
| 45-50 | 8 | — | 1 | 3 | ||
| 50-55 | 4 | — | — | 3 | 11 | 25 |
| 55-60 | 4 | — | 1 | 2 | ||
| 60-80 | 2 | — | — | — | 3 | 5 |
| 355 | 21 | 18 | 426 | 217 | 1037 |
Hysteria in the United States assumes almost every form, probably because we have here represented almost every race and nationality, either pure or mixed. While it cannot be clearly shown that certain races are much more prone to hysteria than others, the type of this disease is doubtless much influenced by racial and climatic conditions. Certain phases of the disease prevail in certain sections more than in others. Mitchell's40 experience is that the persistent hystero-epilepsies, and the multiple and severe contractures which Charcot and others describe, are rare in this country among all classes, and especially uncommon in the lowest classes, among which Charcot seems to have found his worst and most interesting cases. He says that while his own clinic furnishes numerous cases of neural maladies, and while he has examples of every type of the milder form of hysteria, it is extremely uncommon to encounter the more severe and lasting forms of this disease. When Mitchell's Lectures were first published I was inclined to regard hystero-epilepsy of the grave type as of rare occurrence, and so stated in answer to a communication from him. Recently, as the result of a longer experience, I have become persuaded that some irregular forms are met with somewhat frequently in various sections of our country. It remains true, however, that in the Middle and Northern sections of the United States the graver hysterias of the convulsive type are not nearly as frequently observed as in the southern countries of Europe.
40 Op. cit.
Dr. Guiteras, formerly physician to the Philadelphia Hospital, and Lecturer on Physical Diagnosis in the University of Pennsylvania, now in the United States marine hospital service, has for several years been on duty, most of the time, in Florida, the West Indies, and the Gulf of Mexico. In answer to an inquiry made by me, he writes: “Hysteria prevails with extraordinary frequency amongst the Cubans. It presents itself in the shape of excito-motory and mental phenomena, almost to the exclusion of all other manifestations. The motory anomalies comprise the whole range from mild hysterics to the gravest hystero-epilepsy. The latter is incomparably more frequent in Key West than in Philadelphia. The confirmed hystero-epileptics are few, but it is the rule for well-marked cases of hysteria to present occasionally, often only once in the course of the disease, hystero-epileptic seizures which may be of frightful intensity. By mental disorders I do not mean only the acute attacks of excitement and delirium which attend upon or take the place of convulsive attacks, but I mean also to include the chronic form of hysterical insanity, which is generally some variety of melancholia. These are the peculiarities of hysteria as seen by myself in the Latin race in the tropics. My experience teaches me that the Saxon race in the tropics shows the same peculiarities to a less extent.”
In the region referred to by Guiteras it will be remembered there is a mixed population composed largely of Spanish, French, and Portuguese. Climatic and other local influences may have something to do with the particular form which this disorder assumes in these tropical or semitropical districts, but race would seem to be the most important factor. In the section on Hystero-epilepsy I will speak of the irregular type of this disorder, which has fallen most frequently under my own observation.
Hysteria in the negro is of somewhat frequent occurrence, and is more [p. 218] likely to be of the demonstrative or convulsive than of a paralytic or negative form. Hysterical convulsions, particularly of the purposive kind, and hysterical mania, are often met with in the colored population of our large city hospitals and asylums.
The influence which climate exerts, like that of race, is rather on the type of hysteria than upon the disease itself. Hysteria is found in every climate, but in warm countries the disorder seems more likely to be mobile and dramatic than when found in the more temperate or colder zones.
Season and meteorological conditions have some influence on the production of hysterical attacks. It is well known that hysteria, chorea, and other allied nervous disorders are more likely to appear in the spring than at other seasons. This fact has been shown by various observers.
Hysteria may occur in any rank of life. It is not, as has been held by some, a disease of the luxurious classes. The American physician who has seen much of this disorder—and that means every physician of large practice—has met with hysterical cases in every walk of life. While this is true, however, hysteria of certain types is met with more frequently in certain social positions. Some of the remarks about race and climate apply also here. It is the type of the disorder, and its relative frequency among various classes, which are affected by social position. Young women of the richer classes, who have been coddled and pampered, whose wants and whose whims have been served without stint or opposition, often pass into hysterical conditions which do not have any special determining causative factor, or at least only such as are comparatively trivial. Occasionally, in them hystero-epilepsy, catalepsy, and the train of grave hysterical phenomena are observed. We are more likely, however, to have the minor and indefinite hysterical symptoms; or, if grave manifestations be present, they are most usually ataxia, paralysis, contractures, or aphonia, and not convulsive phenomena. Hysteria in our American cities is especially prevalent among certain classes of working-people, as among the operatives in manufacturing establishments. Dividing American society into the three classes of rich, middle, and poor, hysteria is most prevalent in the first and the last. It is, however, by no means absent in the middle class.
The absence of occupation on the one hand, and, on the other, the necessity of following work for which the individual is unfitted, particularly irritating lines of work, predispose to the occurrence of hysteria. It may be caused, therefore, either by no work, overwork, or irritating work. As to the special occupations, hysteria would seem to result most commonly in those positions where physical fatigue combines with undue mental irritation to harass and reduce the nervous system. In men it occurs often as the result of overwork conjoined with financial embarrassment. It is met with not infrequently among teachers, particularly those who are engaged in the straining and overstraining labor of preparing children for examinations. A good method of education is the best preventive; a bad method is one of the most fruitful causes of the affection. The injurious effect of American school or college life in the production of hysteria is undoubted, and should be thoroughly appreciated. Our educational processes act both as predisposing and exciting causes of this disorder. Both in our private and public educational institutions the [p. 219] conditions are frequently such as to lead to the production of hysteria or to confirm and intensify the hysterical temperament. In our large cities all physicians in considerable practice are called upon to treat hysterical girls and boys, the former more frequently, but the latter oftener than is commonly supposed. Hysteria in boys, indeed, does not always meet with recognition, from the fact that it is in boys. Cases of hysteria in girls under twelve years of age have come under my observation somewhat frequently. About or just succeeding examination-time these cases are largely multiplied. The hysteria under such circumstances may assume almost any phase; usually, however, we have not to deal in such patients with convulsive types of the disease.
Clarke41 has considered some of these questions in connection particularly with the physiological processes of menstruation, and its bearing upon the inability of girls to maintain equally with boys the stress of such competition.
41 Sex in Education, etc., by Edward H. Clarke, M.D., Boston, 1873.
The cramming processes which are resorted to in order to force children at fixed times from the lower to the higher grades of public schools, and more especially from grammar to normal or high schools, is a fruitful source of evil in this direction. It is not always so much hard study as it is the badly-arranged and too numerous subjects of study that make the strain. I have spoken of this in another connection as follows:42 “Our children are too largely in the hands of those educationalists to whom Clouston refers,43 who go on the theory that there is an unlimited capacity in every individual brain for education to any extent and in any direction. Children varying in age and original capacity, in previous preparation, and in home-surroundings are forced into the same moulds and grooves. The slow must keep pace with the fleet, the frail with the sturdy, the children of toil and deprivation with the sons and daughters of wealth and luxury. A child is always liable to suffer from mental overwork when the effort is made to force its education beyond its receptive powers. Education is not individualized enough. The mind of the child is often confused by a multitude of ill-assorted studies. Recreation is neglected and unhealthy emulation is too much cultivated. In many communities admissions to various grades of public schools are regulated entirely by the averages obtained at examinations, instead of on the general record of the pupils in connection with proper but not too severe examinations. In consequence often, after the campaign of overwork and confusion called an examination, we see children developing serious disturbances of health or even organic disease—paroxysmal fever, loss of appetite, headache or neckache, disturbed sleep, temporary albuminuria, chorea, hysteria, and hystero-epilepsy.”
42 “Toner Lecture on Mental Overwork and Premature Disease among Public and Professional Men.” delivered March 19, 1884, Washington, Smithsonian Inst., January, 1885.
43 Clinical Lectures on Mental Diseases.
The term students' hysteria has been applied to the neuromimetic disorders from which medical students frequently suffer during their attendance upon lectures. Some years since, when engaged in examining students upon the lectures upon the practice of medicine delivered by Professor DaCosta, I saw many illustrations of this affection, [p. 220] some of which were very amusing. In a paper on hysteria which received the prize at the Physical Society of Guy's Hospital, P. Horrocks44 writes that during the fortnight following the death of the late Napoleon, Sir James Paget was consulted for stone in the bladder by no less than four gentlemen who had nothing the matter with them. “How many students,” says Horrocks, “are there, of one year's standing or more, who have not imagined and really became convinced that they were suffering from some disease, generally a fatal disease?” In such cases we have a combination of true psychical influence with overwork and the unhygienic surroundings for which our medical colleges are notorious.
44 Med. and Surg. Reporter, vol. xxxvii., Nov. 24, 1877.
It has been my personal experience that comparatively few cases of hysteria occur among female medical students. Not long since a thesis was presented at graduation by a woman medical student45 on the curative effects of professional training in neurasthenic and hysterical women. In this she shows that there are certain relations of mind over body which enable it to modify bodily conditions and ward off disease when other remedies appear almost powerless. She illustrates the therapeutic power of mental impressions and occupations by two cases in which a judicious and careful course of study acted to cure severe nervous and uterine troubles. One of these women, who had suffered with neurasthenia and general debility, severe nervous headaches, and other symptoms, was able during her last year at college to attend fifteen lectures a week, besides clinics, prepare for examination on five subjects, and was seldom troubled with even headache. She afterward was employed in hospital work, and could walk five miles a day without discomfort. That women medical students know when and how to take care of themselves during the menstrual period, and that they can, if they see fit, cease work or lighten their labors at that time, would partly account for their escaping from nervous break-down.
45 “The Therapeutic Value of Mental Occupation,” by Hannah M. Thompson, M.D., Medical and Surgical Reporter, November, 1883.
That any form of irritation in a patient predisposed to hysteria may act as an exciting cause in this affection has led Laségue to apply the term peripheral hysteria to certain cases. One of his cases was a girl fourteen years old, who, having suffered for a few hours with her eyes because of some sand thrown into one of them by a playmate, awoke the next morning with a spasm of the eyelid on that side, which rendered it impossible for her to open that eye; and it remained closed during four months. He considered that the irritation produced by the sand was not the immediate cause of the spasm, but that its long duration was an hysterical phenomenon. The patient afterward became the subject of hysterical manifestations. In another complete hysterical aphonia came on after a slight bronchitis. Another, after an attack of indigestion, refused to touch either food or drink for twenty-four hours, and later was troubled with regurgitation from constriction of the pharynx or œsophagus which lasted for some weeks.
Anæmia and chlorosis are frequent exciting causes of hysteria in children, particularly in girls.
Disorders of menstruation play a prominent part as exciting causes of [p. 221] special hysterical manifestations. The period of the establishment of the menstrual function is one that is particularly fertile in the production of hysteria, much more so than acquired disorders of menstruation occurring later. Menorrhagia, dysmenorrhœa, and certain local utero-vaginal disorders may act upon those predisposed to hysteria as exciting causes. These conditions themselves are, on the other hand, sometimes caused by nervous, hysterical states in the individual.
With reference to the very common assertions that continence on the one hand, and sexual over-indulgence on the other, are the most prolific causes of hysteria, the true stand to take is that neither of these positions is philosophically correct; for, as Briquet has shown, nuns on the one hand and prostitutes on the other are frequent victims of this protean disorder.
As affirmed by Jolly, sexual over-irritation, particularly that induced by onanism, more frequently causes hysteria than sexual abstinence or deprivation.
The occurrence of hysteria and hysterical choreas among pregnant women has long been recognized. Scanzoni, quoted by Jolly,46 states that of 217 patients whom he had treated, 165, or 76 per cent. had been puerperal, and that of the latter not less than 65 per cent. had borne children more than three times. Cases of grave hysteria or hystero-epilepsy have been aggravated by pregnancy and have led to premature labor.
46 Op. cit.
Chrobak attacks the etiological problem of hysteria by referring its causation to movable kidneys! He observed 19 such patients in Vienna, 16 being in Oppolzer's clinic.47 Three times no subjective symptoms accompanied the anomaly; eight times the trouble could be referred either to the dislocation of the kidneys or to disease of the same; and eight times the evidence of hysteria was unmistakable. Among the latter eight cases neither vaginal, uterine, nor ovarian conditions were recognized. He concludes that there is a direct nervous connection between the kidneys and the genital organs, and between both and hysteria.
47 Medizinische-Chirurgische Rundschan, quoted by Boston Medical and Surgical Journal, 1870, lxxxiii. 430-432.
In brief, the truth is that frequent or severe local irritation in any part of the body in an individual of the hysterical diathesis may act as the exciting cause of an hysterical paroxysm or of special hysterical manifestations. Irritation or disease of the uterus or ovaries may result in hysteria, as may the bite of a dog, a tumor of the brain, a polypus in the nose, a phymosis, an irritated clitoris, a gastric ulcer, a stenosis of the larynx, a foreign body in the eye, a toe-nail ulcer, or a movable kidney.
Whatever tends to exhaust the nervous system will also cause hysteria, but only in those who have some inherited predisposition to the disorder. C. Handfield Jones48 mentions heatstroke and severe physical labor as such causes. One of the sequelæ of heatstroke enumerated by Sir R. Martin, and quoted by Jones, is a distressing hysterical state of the nervous system, with an absence of self-control in laughing and crying, the paroxysm being followed by great prostration of nervous power.
48 Op. cit.[p. 222]
The effect of imitation in the production of hysteria has been known in all ages. Most of the epidemics and endemics of nervous disorders which have from time to time prevailed in various parts of the world have either been hysterical in character or have had in them a large element of hysteria. While it is impossible in a practical work to devote much space to this branch of the subject, a discussion of hysteria in its etiological relations would be imperfect without some reference to these outbreaks. In ancient times, in the Middle Ages, and within comparatively recent periods extraordinary epidemics have occurred. No country within the range of medical observation has been entirely free from them. Communities civilized and semi-civilized, Christian and Mohammedan, Protestant and Catholic, have had a fair share of the visitations. Some of them constitute epochs in history, and, as Hecker,49 their greatest historian, has remarked, their study affords a deep insight into the work of the human mind in certain states of society. “They are,” he says, “a portion of history, and will never return in the way in which they are recorded; but they expose a vulnerable part of man—the instinct of imitation—and are therefore very nearly connected with human life in the aggregate.”
49 The Epidemics of the Middle Ages, from the German of J. F. C. Hecker, M.D., Professor at the Frederick William University at Berlin, etc., translated by B. G. Babington, M.D., F. R. S., etc.; 3d ed., London, 1859.
Some authors under hysteria, others under catalepsy, others under ecstasy, still others under chorea, have discussed these epidemics—a fact which serves to emphasize the truth that while these affections have points of difference, they have also an easily-traced bond of union. They are but variations of the same discordant tune. Briquet in an admirable manner sketches their history from the age of Pausanias and Plutarch to the time of Mesmer. Of American writers, James J. Levick50 of Philadelphia has furnished one of the most valuable contributions to this subject.
50 “An Historical Sketch of the Dance of St. Vitus, with Notices of some Kindred Disorders,” Med. and Surg. Reporter, vol. vii., Dec. 21 and 28, 1861, p. 276, and Jan. 4 and 11, 1862, p. 322.
In the year 1237 a hundred children or more were suddenly seized with the dancing mania at Erfurt; another outbreak occurred at Utrecht in 1278.
As early as the year 1374 large assemblages of men and women were seen at Aix-la-Chapelle affected with a “dancing mania.” They formed circles and danced for hours in wild delirium. Attacks of insensibility, of convulsions, and of ecstasy occurred. The disease spread from Germany to the Netherlands. In a few months it broke out in Cologne, and about the same time at Metz. “Peasants,” we are told, “left their ploughs, mechanics their workshops, housewives their domestic duties, to join the wild revelry, and this rich commercial city became the scene of the most ruinous disorder.”
The festival of St. John the Baptist was one celebrated in strange wild ways in these early days. Fanatical rites, often cruel and senseless, were performed on these occasions. Hecker supposes that the wild revels of St. John's Day in 1374 may have had something to do with the outbreak of the frightful dancing mania soon after this celebration. It at least brought to a crisis a malady which had been long impending.
[p. 223]The Flagellants afford another illustration of an early religio-nervous craze. Self-flagellation was indulged in for generations before the fourteenth century, but it then became epidemic. A brotherhood of Flagellants was formed; they marched in processions carrying scourges, with which they violently lashed and scourged themselves. As late as 1843, Flagellant processions, but without the whips and scourging, were continued in Lisbon on Good Friday.
Strasburg was visited by the dancing plague in 1418. Those afflicted were conducted to the chapel of St. Vitus, where priests attempted to relieve them by religious ceremonies. The name St. Vitus's dance, still so common as a synonym for chorea, has come down to us because of the alleged wonderful doings of this saint in behalf of those affected during some of the dancing epidemics. Both Hecker and Madden51 give interesting details of the personal history of St. Vitus, who was a Sicilian, born in the time of Diocletian, and even in childhood is said to have worked great miracles, and was delivered from many sufferings and torments. He died about the year 303. His body was moved to Apulia, afterward to St. Denys in France, and still later to the abbey of Corvey in Saxony. A legend was invented that St. Vitus, just before he bent his neck to the sword, prayed to God that he might protect from the dancing mania all those who should solemnize the day of his commemoration and fast upon its eve.
51 Phantasmata; or, Illusions and Fanaticisms, etc., by R. R. Madden, F. R. S., London, 1857.
Another strange disorder called tarantismus derived its name from the fact that it was supposed to be caused by the bite of the tarantula, a ground-spider common in Apulia, Italy. According to Hecker, the word tarantula is the same as terrantola, a name given by the Italians to a poisonous lizard of extraordinary endowments. The fear of the insect was so general that its bite was much oftener imagined than actually received. The disorder was probably in existence long before the fifteenth century, although the first account of it, that of Nicholas Perotti, refers to its occurrence in this century. Many symptoms followed the bite or supposed bite: the individuals became melancholy, stupefied, lost their senses, and, above all, were irresistibly impelled to dance until exhausted and almost lifeless. It was believed that the results of the bite could be cured, or at least much benefited, by dancing to a certain kind of music. Tarantism was at its height in the seventeenth century. To this day, in some parts of Italy, dances called tarantellas are performed with intricate figures to marked time.
Abyssinia was visited by a dancing mania called the tigretier, which, according to Hecker, resembled the original mania of the St. John dancers. It exhibited a similar ecstasy. Those affected with it were cured by dancing to the music of trumpeters, drummers, fifers, etc.
Levick says that the dancing mania of the fifteenth century is still kept in popular remembrance in some places by an annual festival, especially at Echtermarch, a small town in Luxembourg, where a jumping procession occurs annually on Whit Tuesday. In the year 1812, 12,678 dancers were in the procession.
The Anabaptists, a religious sect of the sixteenth century, exhibited many of the wild and grotesque phenomena of hysteria or hystero-epilepsy.
[p. 224]The French Calvinists or Camisards, who appeared near the close of the seventeenth century, were also the subjects of ecstasy and of peculiar fits of trembling. These trembleurs experienced convulsive shocks in the head, the shoulders, the legs, and the arms, and were sometimes thrown violently down.
About 1731 and later great crowds frequented the tomb of Deacon François de Paris, an advocate of the doctrines of Jansenius. It was reported that miracles were performed at his tomb: the sick were brought there, and often were seized with convulsions and pains, through which they were healed. The subjects of these attacks are sometimes spoken of as the Jansenist Convulsionnaires. The tomb was in the cemetery of St. Médard, and hence those who visited the place were also termed the Convulsionnaires of St. Médard. This disorder increased, multiplied, and disseminated, lasting with more or less intensity for fifty-nine years. Great immorality prevailed in the secret meetings of the believers.
Hecker gives some remarkable instances of the effect of sympathy or imitation exhibited on a smaller scale than in the epidemics of the Middle Ages. One is of a series of cases of fits in a Lancashire factory, the first one brought on by a girl putting a mouse into the bosom of another. In Charité Hospital in Berlin in 1801 a patient fell into strong convulsions, and immediately afterward six other patients were affected in the same way; by degrees eight more were attacked. At Redruth, England, a man cried out in a chapel, “What shall I do to be saved?” Others followed his example, and shortly after suffered most excruciating bodily pain. The occurrence soon became public; hundreds came, and many of them were affected in the same way. The affection spread from town to town. Four thousand people were said in a short time to be affected with this malady, which included convulsions.
Hecker in the edition of his work referred to has also a treatise on child pilgrimages.52 These pilgrimages, like the dancing mania, occurred in the Middle Ages. The greatest was the boy crusade in the year 1212. The passion to repossess the Holy Land then had its grip on Catholic Europe. The first impulse to the child pilgrimages was given by a shepherd-boy, who had revelations and ecstatic seizures, and held himself to be an ambassador of the Lord. Soon thirty thousand souls came to partake of his revelations; new child-prophets and miracle-workers arose; the children of rich and poor flocked together from all quarters; parents were unable to restrain them, and some even began to urge them. A host of boys, armed and unarmed, assembled at Vendôme, and started for Jerusalem with a boy-prophet at their head. They got to Marseilles, and embarked on seven large ships. Two ships were wrecked, and not a soul was saved. The other five ships reached Bougia and Alexandria, and the young crusaders were all sold as slaves to the Saracens. In Germany child-prophets arose, especially in the Rhine countries and far eastward. An army of them gathered together, crossed the Alps, and reached Genoa. They were soon scattered; many perished; many were retained as servants in foreign lands; some reached Rome. A second child's pilgrimage occurred twenty-five years later. It was confined to the city of Erfurt. One thousand children wandered, dancing [p. 225] and leaping, to Armstadt, and were brought back in carts. Another child's pilgrimage from Halle, in Suabia, to Mount St. Michel in Normandy, occurred in 1458.
52 Translated by Robert H. Cooke, M. R. C. S.
In the convent of Yvertet in the territory of Liège, in 1550, the inmates were seized with a leaping and jumping malady. The disorder began with a single individual, and was soon propagated.
Sometimes the convulsive disorders of early days, especially those occurring in convents, were associated with the strange delusion that the subjects of them were changed into lower animals. Various names have been given to disorders of this kind, such as lycanthropia or wolf madness, zoomania or animal madness, etc. Burton in the Anatomy of Melancholy gives an interesting summary of these disorders, which are also discussed by Levick.
In 1760 a religious sect known as the Jumpers prevailed in Great Britain. They were affected with religious frenzy, and jumped continuously for hours. Other jumping epidemics have appeared at different times, both in Great Britain and in this country.
The New England witchcraft episode is of historical interest in connection with this subject of epidemic hysteria. This excitement occurred during the latter part of the seventeenth century. Adults and children were its subjects. The Rev. Cotton Mather records many cases, some of which illustrate almost every phase of hysteria. Individuals who were seized with attacks, which would now be regarded as hysterical or hystero-epileptic, were supposed to have become possessed through the machinations of others. Those who were supposed to be possessed were tried, condemned, and executed in great numbers. Many accused themselves of converse with the devil. The epidemic spread with such rapidity, and so many were executed, that finally the good sense of the people came to the rescue.
The nervous epidemics, nearly all religious, which have occurred in this country have usually been during the pioneer periods, and have therefore appeared at different eras as one part of the country after another has been developed. Kentucky, Tennessee, Virginia, and neighboring States were visited time and again. Even to-day we occasionally hear of outbreaks of this kind in remote or primitive localities, whether it be in the far South-west or in the woods of Maine.
David W. Yandell53 has published a valuable paper on “Epidemic Convulsions,” the larger part of the materials of which were collected by his father for a medical history of Kentucky. From this it would appear the convulsions were first noticed in the revivals from 1735 to 1742. Many instances are related of fainting, falling, trance, numbness, outcries, and spasms. The epidemic of Kentucky spread widely, reappeared for years, and involved a district from Ohio to the mountains of Tennessee, and even to the old settlements in the Carolinas. Wonderful displays took place at the camp-meetings. At one of these, where twenty thousand people were present, sobs, shrieks, and shouts were heard; sudden spasms seized upon scores and dashed them to the ground. Preachers went around in ecstasy, singing, shouting, and shaking hands. Sometimes a little boy or girl would be seen passionately exhorting the multitude, reminding one of the part taken by [p. 226] the children in the epidemics of the Middle Ages. A sense of pins and needles was complained of by many; others felt a numbness and lost all control of their muscles. Some subjects were cataleptic; others were overcome with general convulsions.
53 Brain, vol. iv., Oct., 1881, p. 339 et seq.
The term jerks was properly applied to one of the forms of convulsion. Sometimes the jerking affected a single limb or part. The Rev. Richard McNemar has given a graphic description of this jerking exercise in a History of the Kentucky Revival. The head would fly backward and forward or from side to side; the subject was dashed to the ground, or would bounce from place to place like a football, or hop around with head, limbs, and trunk twitching and jolting in every direction. Curiously, few were hurt. Interesting descriptions of the jerks can be found in various American autobiographical and historical religious works. In such books as the Autobiography of Peter Cartwright, a Western Methodist, for instance, striking accounts of some of the phases of these epidemics are to be found. Lorenzo Dow in his Journal, published in Philadelphia in 1815, has also recorded them.
Hysterical laughter was a grotesque manifestation often witnessed. The holy laugh began to be a part of religious worship. Dancing, barking, and otherwise acting like dogs, were still other manifestations. It is remarkable that, according to Yandell, no instance is recorded in which permanent insanity resulted from these terrible excitements.
The absurd and extraordinary exhibitions witnessed among the Shakers belong to the same category, and have been well described by Hammond and others.
In a History of the Revival in Ireland in 1859, by the Rev. William Gibson, instances of excitement that fairly rivalled those which occurred in our Western States are given. Cases of ecstasy are described.
The religious sect known as the Salvation Army, which has in very recent years excited so much attention, curiosity, and comment both in America and England, has much in common with the Jumpers, the Jerkers, and the Convulsionnaires. The frenzied excitement at their meetings, with their tambourine-playing, dancing, shouting, and improvising are simply the same phases of religio-hysterical disorder, modified by differences in the age and environment.
In 1878, in the district of Tolmezo, Italy, an epidemic of hysteria which recalls the epidemics of the Middle Ages occurred. It has been described by M. Léon Colin.54 It was reported to the prefect of Undine that for three months some forty females living in the commune of Verzeguis had been attacked by religious mania. “From the report it appears that the first was in the person of a woman named Marguerite Vidusson, who had been the subject of simple hysteria for about eight years. In January, 1878, she began to suffer from convulsive attacks, accompanied by cries and lamentations. She was regarded as the subject of demoniacal possession, and on the first Sunday in May was publicly exorcised. Her affection, however, increased in severity; the attacks were more frequent and more intense, and were especially provoked by the sound of the church-bells and by the sight of priests. Seven months later three other hysterical girls became subject to convulsive and clamorous attacks. Here, again, an attempt was made to get rid of the [p. 227] supposed demon. A solemn mass was said in the presence of the sufferers, but was followed only by a fresh outbreak. At the time of the visit of the delegates eighteen were suffering, aged from sixteen to twenty-six years, except three, whose ages were respectively forty-five, fifty-five, and sixty-three years. Similar symptoms had also appeared in a young soldier on leave in the village.” During the attacks the patients talked of the demon which possessed them, stated the date on which they were seized by it, and the names of the persons who were possessed before them. Some boasted of being prophetesses and clairvoyants and of having the gift of tongues. In all, the sound of church-bells caused attacks, and religious ceremonies appeared not only to aggravate the disease in the sufferers, but also to cause its extension to those not previously attacked. M. Colin points out that the soil is particularly favorable for the development of an epidemic of this nature. The people of Verzeguis are backward in education and most superstitious. Functional nervous diseases are common among them. The inhabitants of the village are largely cut off from intercourse with the adjacent country in consequence of comparative inaccessibility and the frequent interruption of communications by storms and floods. Craniometric observations on twelve of the inhabitants seemed to show that the brachycephalic form of skull predominated, and that the development of the cranium was slightly below the average. The epidemic proved extremely obstinate.
54 Annales d'Hygiène, quoted in Lancet, Oct. 16, 1880.
In Norway and New Caledonia similar hysterical outbreaks have been observed in recent times.
An endemic of hysteria from imitation occurred in Philadelphia in 1880. Some of the cases fell under my own observation. A brief account of them is given by Mitchell in his Lectures. The outbreak occurred in a Church Home for Children, to which Dr. S. S. Stryker was physician. The Home contained ninety-five girls and six boys; all of them were well nourished and in good condition. The epidemic began by a girl having slight convulsive twitchings of the extremities, with a little numbness. Attacks returned daily; respiration became loud and crowing. She soon had all the phenomena of convulsive hysteria. Many of her comrades began to imitate her bark. Soon another girl of ten was attacked with harsh, gasping breathing, with crowing, speechlessness, clutching at her throat, and the whole series of phenomena exhibited by the first girl attacked. Nine or ten others were affected in like manner, and many of the remaining children had similar symptoms in a slight degree. At first convulsions occurred irregularly; after a while they appeared every evening; later, both morning and evening. The presence of visitors would excite them. Many interesting hysterical phases occurred among the children. One night some of them took to walking about on their hands and knees; others described visions. The girls often spoke of being surrounded by wild beasts, and one child would adopt the fiction which another related in her hearing. The cases were scattered about in different hospitals, and made good recoveries in from one to two months.
The Jumpers or Jumping Frenchmen of Maine and Northern New Hampshire were described by Beard in 1880.55 They presented nervous phenomena in some phases allied to hysteria. In June, 1880, Beard [p. 228] visited Moosehead Lake and experimented with some of them. Whatever order was given them was at once obeyed. One of the Jumpers, who was sitting in a chair with a knife in his hand, was told to throw it, and he threw it quickly so that it struck in a beam opposite; at the same time he repeated the order to throw it with a cry of alarm. They were tried with Latin and Greek quotations, and repeated or echoed the sound as it came to them. They could not help repeating any word or sound that came from the person that ordered them. Any sudden or unexpected noise, as the report of a gun, the slamming of a door, etc., would cause them to exhibit some phenomena. It was dangerous to startle them where they could injure themselves, or if they had an axe, knife, or other weapon in their hands. Since the time of Beard's observation accounts of their doings have now and then found their way into newspapers. One recent account tells of one of these peculiar people jumping from a raft into the Penobscot River on an order to jump.
55 Journal of Nervous and Mental Diseases, vol. vii., 1880, p. 487.
Hammond56 has described under the name Miryachit an affection which seems to be essentially the same disorder as that of which the Jumpers are the victims. He quotes from a report of a journey from the Pacific Ocean through Asia to Europe by Lieutenant B. H. Buckingham and Ensigns Geo. C. Foulk and Walter McLean of the United States Navy, an account of this disease. The party made their first observations on this affection while on the Ussuri River in Siberia. The captain of the general staff approached the steward of the boat suddenly, and without any apparent reason or remark clapped his hand before his face; instantly the steward clapped his hand in the same manner, put on an angry look, and passed on. When the captain slapped the paddle-box suddenly, the steward instantly gave it a similar thump. Some of the passengers imitated pigs grunting or called out absurd names, etc.; the poor steward would be compelled to echo them all. The United States naval officers were informed that the affection was not uncommon in Siberia, and that it was commonest about Yakutsk, where the winter cold is extreme. Both sexes were subject to it, but men much less than women. It was known to Russians by the name of Miryachit.
56 New York Med. Journ., Feb. 16, 1884.
In both these classes of cases a suggestion of some kind was required, and then the act took place independently of the will. “There is another analogous condition known by the Germans as Schlaftrunkenheit, and to English and American neurologists as somnolentia or sleep-drunkenness. In this state an individual on being suddenly awakened commits some incongruous act of violence, ofttimes a murder. Sometimes this appears to be a dream, but in others no such cause could be discovered.” Curious instances are mentioned by Hammond of this disorder.
The phenomena of automatism at command in hypnotized subjects have much similarity to the phenomena of these affections, and the same explanation to a certain extent will answer for both.
Paget57 has ably discussed the subject of neuromimesis in general, and Mitchell58 devotes two lectures to its consideration. As already stated when discussing the synonyms of hysteria, the mistake must not be made of supposing all cases of hysteria to be instances of neuromimesis; but, as Mitchell remarks, the hysterical state, however produced, is a fruitful [p. 229] source of mimicry of disease in its every form, from the mildest of pains up to the most complete and carefully-devised frauds. “Its sensitiveness and mobility, its timidity and emotionalness, its greed of attention, of sympathy, and of power in all shapes, supply both motive and help, so that while we must be careful not to see mimicry in every hysteric symptom, we must in people of this temperament be more than usually watchful for this form of trouble, and at least reasonably suspicious of every peculiar or unusual phenomenon.”
57 Op. cit.
58 Op. cit.
SYMPTOMATOLOGY.—At the outset of the discussion of the symptomatology of hysteria, hysterical cases should be divided into four classes—viz. (1) Cases in which the symptoms are involuntary; (2) cases in which the symptoms are artificially induced and become involuntary; (3) cases in which the symptoms are acted or simulated, but in which the patient, because of impaired mental power, is irresistibly impelled to their performance; (4) cases in which the symptoms are purely acts of deception which are under the control of the patient.
Keeping in mind these different classes, we will always be able to link to the phenomena of hysteria the psychical element which is present in all genuine cases of this disorder. To comprehend the existence of the psychical element in the first class, in which the manifestations are absolutely involuntary, may offer difficulties. In these cases, at a period more or less recent or remote, psychical stimuli may have acted to produce the hysterical phenomena, and, once produced, these have been repeated and intensified by habit, and continue independently both of volition and consciousness. The experiments of Dercum and Parker show how hysterical symptoms may be artificially induced and may get beyond the patient's control. The difference between induced and simulated manifestations must always be clearly borne in mind. To induce a set of phenomena a certain mechanism must be set in action, and this, through rational, explicable processes, leads to certain results. The psychical element enters here both positively and negatively—positively, in the determination to produce a certain train of events; negatively, in the condition of mental concentration or abstraction which is a part of the procedure. In the third class of cases acting or simulation is dependent upon the irresistible inclinations of the patient. This may seem to some an uncertain and even dangerous ground to take. I am convinced, however, after observing many hysterical cases, that acts clearly purposive, so far as the particular performance is concerned, are sometimes the result of a general unstable mental condition. Some at least of these patients are as irresistibly impelled to swallow blood and vomit, to scream and gesticulate, etc., as is the monomaniac to commit arson, to ravish, or to kill. In the fourth class, the cases of pure, unmitigated, uncontrollable deception, the psychical element is very evident, although some may question whether such cases should be ranged under the banner of hysteria, where it is both convenient and customary to place them.
The symptoms of hysteria may develop in any order or after any fashion. The graver hysterical phenomena, such as convulsions, paralysis, and anæsthesia, often seem to come on suddenly, but usually this suddenness of onset is apparent rather than real. Minor hysterical symptoms, such as general nervous irritability, pains, aches, and discomforts, and mental peculiarities, have usually been present for a long [p. 230] time. These minor evidences of the hysterical constitution are sometimes the only phenomena ever presented.
Todd59 has described an expression of countenance which he designates as the facies hysterica. The characteristics of this expression are a remarkable depth and prominent fulness, with more or less thickness, of the upper lip, and a peculiar drooping of the upper eyelids. It would be absurd to assert that all hysterical patients presented this cast of countenance, but an appearance which approaches closely to this description is presented in a fair percentage of cases. It has seemed to me that male hysterics were more likely to have this peculiar facies than hysterical females.
59 Reynolds's System of Medicine, vol. ii. p. 656.
The psychical peculiarities or mental disorders of hysteria form a large and important part of its phenomena. We have to deal not only with peculiar and diverse psychical manifestations, but to one form of mental disorder it is clinically convenient and correct to apply the designation hysterical insanity.
In the mildest cases of ordinary hysteria conditions of mental irritability and mobility are sometimes the only striking features. “Patients,” says Jolly,60 “are timid, easily overcome by any unexpected occurrence, sentimental, and sensitive. Every trifle annoys and upsets them; and there is this peculiarity—that a more recent stimulus may often effect a diversion in an exactly opposite direction.”
60 Op. cit.
As bearing upon the question of the mental state in hysteria, the confessions obtained by Mitchell from several patients are of great interest. One patient, who had learned to notice and dwell upon any little symptom, vomited daily and aroused much sympathy. She took little or no food. Spasms came on, and she confessed that every new symptom caused new anxiety, and that somehow she rather liked it all. She gradually lost all her symptoms except vomiting, and overcame this by desperate efforts. Another patient confessed to having played a game upon her doctor for a long time by pretending she took no food. She would get out of bed at night, but remain there all day; she filled up a vessel with water to make others believe she passed large quantities of urine, etc. Another patient, a girl of nineteen, who came on a litter from a Western State, after a time regained her feet. In her confession she stated that what she lacked was courage. She believed that she would have overcome her difficulties if any one had told her that nothing was the matter. “In looking back over the year with the light of the present,” she says, “I can only say that I believe that there was really nothing the matter with me; only it seemed to me as if there was, and because of these sensations I carried on a sort of starvation process physical and mental.”
The older and some of the more recent classifications of insanity recognize hysterical insanity as a distinct form of mental disease. Morel and Skae, however, in their etiological classifications, and Hammond, Spitzka, Mann, and Clouston in their recently-published works, give it a “local habitation and a name.” Krafft-Ebing not only recognizes hysterical insanity as a distinct form of mental disease, but, after the German fashion, subdivides it quite minutely, as follows: First, transitory forms: a. with fright; b. hystero-epileptic deliria; c. ecstatic visionary forms; [p. 231] d. moria-like conditions. Second, chronic forms: a. hystero-melancholia; b. hystero-mania; c. degenerative states with hysterical basis.
Spitzka61 speaks of chronic hysterical insanity as an intensification of the hysterical character, to which “a silly mendacity is frequently added, and develops pari passu with advancing deterioration.” At the State Hospital for the Insane at Norristown and at the department for the insane of the Philadelphia Hospital cases of chronic hysterical insanity have come under my observation. Hammond under hysterical mania includes several different and somewhat distinct mental disorders.
61 Insanity, its Classification, Diagnosis, and Treatment, by E. C. Spitzka, M.D., New York, 1883.
With regard to the occurrence of hysterical manifestations amongst patients suffering from some well-recognized non-hysterical forms of insanity, a tour through any large asylum will afford abundant evidence. Cases of tremor closely simulating cerebro-spinal sclerosis have been observed frequently among the insane. Paralysis, contracture, hysterical joints, hysterical neuralgias, convulsions, and cataleptoid phenomena are among other hysterical manifestations which have fallen under personal observation among the insane of various classes.
A remarkable case of hysterical motor paralysis was observed at the State Hospital for the Insane at Norristown. This patient was an intelligent single woman about thirty-five years of age, of good family, well educated; she had been a teacher and writer, and became insane through family and business troubles. When only eight years of age she was paralyzed for two years and a half, and had had at times during her life, before becoming insane, attacks of partial or complete unconsciousness. Prior to coming under observation she had been an inmate of an English private asylum. She was sick on shipboard coming to this country, and on her arrival was in a state of delirium and insomnia, with attacks of loss of sight. Four months later she developed mania with suicidal inclinations. Just before the development of this maniacal condition her lower limbs became comparatively helpless, and soon after she entirely lost their use. I found her in this condition, and examination showed no change in knee-jerk, electrical reactions, nutrition, nor genito-urinary conditions, which led me to diagnosticate the absence of any organic spinal trouble. The case was pronounced one of hysterical paralysis, and it was prophesied that she would eventually completely recover, probably suddenly. For one year her paralysis remained, her mental condition varying very greatly during this time—sometimes in a lethargic state; sometimes with variable delusions and delirium; occasionally violent and destructive, again peaceable and pleasant; sometimes requiring strong anodynes and hypnotics. Fourteen months after her paralytic condition began, one day she suddenly threw away her crutches and ran up and down the corridor of the hospital. From that time she walked without difficulty, although her mental condition did not entirely clear.
I wish to impress the fact that because hysterical manifestations occur in a case of insanity it should not necessarily be diagnosticated as one of hysterical insanity. Monomania, melancholia, mania, paretic dementia, epileptic insanity, and other forms of mental disorder may at times have an hysterical tinge or hysterical episodes.
[p. 232]The whole question of hysterical insanity is one of great difficulty. The psychical element is probably at the root of all cases of hysteria, but this does not justify us, as I have already stated, in declaring that all cases of hysteria are insane. In practical professional life we must make practical distinctions. In the matter before us distinctions are necessary to be made for legal as well as medical purposes. It might be right and proper to place a case of hysterical insanity in a hospital or asylum under restraint, but no one would dare to claim that every case of hysteria should be so treated.
Hysterical insanity may be conveniently subdivided into an acute and chronic form.
Acute hysterical insanity or hysterical mania is a disorder usually, in part at least, purposive, and characterized by great emotional excitement, which shows itself in violent speech and movement, and often also in deception, simulation, and dramatic behavior. The phenomena indicated by this definition may constitute the entire case, or, in addition, the patient may have, at intervals or in alternation, various other phases of grave hysteria, such as hystero-epileptic seizures or attacks of catalepsy, trance, or ecstasy.
In chronic hysterical insanity we have a persisting abnormal mental condition, which may show itself in many ways, but chiefly as follows: (1) A form in which occur frequent repetitions, over a series of years, of the phenomena of acute hysterical insanity, such as hysterical mania, hystero-epilepsy, catalepsy, etc.; (2) a form in which sensational deceptions—sometimes undoubtedly self-deceptions—are practised.
In a case of chronic hysterical insanity you may have both of these forms commingling in varying degree, as in the following case: G—— is a seamstress, twenty-one years of age. Although young in years, she is an old hospital rounder: she has at various times been in almost all the hospitals of the city. She has been treated for such alleged serious affections as fractured ribs, hemorrhages from the lungs, stomach, and vagina, gastric ulcer, epilepsy, apoplexy, paralysis, anæsthesia of various localities, amenorrhœa, dysmenorrhœa, and fever with marvellous variations of temperature. She has become the bane and terror of every one connected with her treatment and care-taking. She has developed violent attacks of mania, with contortions and convulsions, on the streets and in churches. Sums of money have been collected for her at times by those who have become interested in her as bystanders at the time of an attack or have heard of her case from others. She has made several pseudo-attempts at suicide. Recently an empty chloroform-liniment bottle tumbled from her bed at a propitious moment, she at the same time complaining of pain and symptoms of poisoning. She has refused to partake of food, and has been discovered obtaining it surreptitiously. Her large and prolonged experience with doctors and hospitals has so posted her with reference to the symptomatology of certain nervous affections that she is able at will to get up a fair counterfeit of a large variety of grave nervous disorders.
One of her recent attacks of hysteria was preceded by a series of hysterical phenomena, such as vomiting, hemorrhage, aphonia, ovaralgia, headache, and simulation of fever. She began by crying and moaning, which was kept up for many hours. She fell out of bed, apparently [p. 233] insensible. Replaced in bed, she passed into a state closely simulating true acute maniacal delirium. She shrieked, cried, shouted, and moaned, threw her arms and legs about violently, and contorted her entire body, snapping and striking at the nurses and physicians in attendance. At times she would call those about her by strange names, as if unconscious of the true nature of her surroundings. Attacks of this kind were kept up for a considerable period, and after an interval of rest were repeated again and again.
Many of the extraordinary facts which fill the columns of the sensational newspapers are the results of the vagaries of patients suffering from the second of the forms of chronic hysterical insanity. “When,” says Wilks,62 “you see a paragraph headed ‘Extraordinary Occurrence,’ and you read how every night loud rapping is heard in some part of the house, how the rooms are being constantly set on fire, or how all the sheets in the house are torn by rats, you may be quite sure that there is a young girl on the premises.” It is unnecessary to add that said girl is of the hysterical genus.
62 Op. cit.
A story comes from an inland town, for instance, of a respectable family consisting, besides the parents, of three daughters and six sons, one of whom died of pneumonia. Since his death the family had been startled by exciting and remarkable events in the house—a clatter of stones on the kitchen floor, the doors and windows being closed; shoes suddenly ascending to the ceiling and then falling to the floor, etc. Search revealed nothing to explain the affair. As throwing light upon this matter, a visitor, who confessed his inability to explain the occurrences, nevertheless referred to one of the daughters as looking like a medium.
Charcot and Bourneville give frequent instances of extraordinary self-deceptions or delusions among hysterical patients. The story of an English lady of rank, who reported that she was assaulted by ruffians who attacked her in her own grounds and attempted to stab her, the weapons being turned by her corsets, is probably an example of this tendency. Investigation made by the police force threw grave doubts upon the story.
Many of the manifestations classed as hysterical by medical writers are simply downright frauds. The nature of others is doubtful. The erratic secretion of urine, for example, has frequently engaged the attention of writers on nervous diseases, and has awakened much controversy. American hysterics are certainly fastidious about this matter, as I have not yet met, in a considerable experience, with a single example of paruria erratica. Charcot63 refers sarcastically to an American physician who in 1828 gravely reported the case of a woman passing half a gallon of urinous fluid through the ear in twenty-four hours, at the same time spirting out a similar fluid by the navel. He also alludes to the case of Josephine Roulier, who about 1810 attained great notoriety in France, but was discovered by Boyer to be a fraud. This patient vomited matter containing urea, and shortly after came a flow of urine from the navel, the ears, the eyes, the nipples, and finally an evacuation of fecal matters from the mouth.
63 Op. cit.
Hemorrhages from eyes, ears, nostrils, gums, stomach, bowels, etc. [p. 234] have often been observed among the hysterical; these cases sometimes being fraudulent and sometimes genuine. In the Philadelphia Hospital in 1883 was a patient suffering from grave hysteria, vomiting of blood being a prominent symptom. Although close watch was kept, several days elapsed before it was discovered that she used a hair-pin to abrade the mucous membrane of her nose, swallowed the blood, which passed into the throat, and then vomited it.
Sir Thomas Watson tells of a young woman who made a hospital surgeon believe that she had stone in the bladder; and Fagge, of a patient who had been supposed to have hydatid in the liver, and who produced a piece of the stomach of a rabbit or some other small animal, which piece she declared she had vomited. A few hours later she again sent for her medical man to remove from her vagina another fragment of the same substance.
A case is reported by Lopez64 of spiders discharged from the eye of an hysterical patient. He regarded the case as one of hysterical monomania. Fragments of a dismembered spider were undoubtedly from time to time removed from the eye of the patient. Lopez believed that at first the fragments may have got into the eye accidentally, but that afterward the patient, under the influence of a morbid condition, introduced them from day to day. The total number of spiders removed in fragments was between forty and fifty. Silvy65 relates a case in which a large number of pins and needles made their exit from a patient. Other needle cases are given, and also examples of insects and larvæ discharged from the human body. In one case worms crawled out of the nose, ears, and other natural openings; in another worms were found in active motion under the conjunctiva; in a third a beetle was discharged from the bladder, and several beetles were vomited by a boy.
64 American Journal of Medical Sciences, Philadelphia, 1843, N. S., 74-81.
65 Mémoires de la Société médicale, Anné 5, p. 181.
Jolly66 records in a foot-note a case published in 1858, by I. Ch. Leitz of Pesth, of a young girl from whose eyes fruit-pips sprang, from whose ears and navel feces escaped, and from whose anus and genitals fleshy shreds came away, while worms with black eyes were vomited. He further tells of a woman from whose genitals four-and-twenty living and dead frogs passed, some of these, indeed, with cords of attachment. The birth of the frogs was witnessed and believed in by several physicians!
66 Op. cit.
Hardaway67 reports a curious case with simulated eruptions. The woman appeared to be in fear of syphilis contracted by washing the clothes of a diseased infant. She had blebs irregularly distributed upon the fingers and arm of the left side; these, the doctor concluded, had been caused by the application of vitriol. He reports another case in which a woman had an eruption on her left arm, and the sores, instead of getting better under treatment, got worse. On one visit he found needle-scratches on the old sore. Nitric acid, according to Hardaway, is a favorite substance for the production of such eruptions. The best diagnostic test is that the blister is linear, while in pemphigus it is circular, unlike that which would be produced by a running fluid. Hysterical women have irritated their breasts with cantharides. Niemeyer68 mentions a woman at Krutsenberg's clinic who irritated her arm in such a way that amputation became [p. 235] necessary, and after that she irritated the stump until a second amputation had to be performed.
67 St. Louis Courier of Medicine, 1884, xi. 352.
68 Textbook of Practical Medicine.
Nymphomania is a form of mental disorder which sometimes occurs among the hysterical; or it would perhaps be more correct to say that nymphomania and grave hysterical affections are sometimes associated in the same case. It is a condition in which is present extreme abnormal excitement of the sexual passion—a genesic, organic feeling rather than an affection associated with the sentiment of love. Hammond treats of it under the head of acute mania, and considers cases of nymphomania as special varieties of this disease. Undoubtedly, this is the correct way of looking at the subject in many cases. In man the corresponding mental and nervous condition often leads to the commission of rape and murder. In woman the affection is most likely to show itself with certain collateral hysterical or hysteroidal conditions, as spasms, hystero-epilepsy, and catalepsy, or with screaming, crying, and other violent hysterical outbreaks. Sometimes there is a tendency to impulsive acts, but this does not usually go so far as to lead to actual violence.
Nymphomaniacs may be intelligent and educated, and if so they usually resist their abnormal passions better than the ignorant. A number of nymphomaniacs have been under treatment at the Philadelphia Hospital. One case was an epileptic and also hysterical girl. She had true epileptic seizures, and at other times had attacks of a hysteroidal character. She would make indecent proposals to almost any one, and would masturbate and expose herself openly. She also had occasional maniacal attacks. She died in the insane department of the hospital.
Nymphomania and what alienists call erotomania are sometimes not differentiated in practice and in books. They are, however, really different conditions. Erotomania and nymphomania may be associated in the same case, but it is more likely that erotomania will not be present in a case of nymphomania. Erotomania may exist as a special symptom or it may be one of the evidences of monomania. It is found in both men and women. Patients with this condition may have no sexual feeling whatever. The individual has some real or imaginary person to love. It is rather the emotion of love which is affected, not the sexual appetite. It is shown by watching or following the footsteps of the individual, by writing letters, and by seeking interviews. In the history of Guiteau an incident of this kind is mentioned by Beard.69 He followed a lady in New York whom he supposed to be the daughter of a millionaire—followed her, watched her house and carriage, and wrote letters to her. Out West he showed the same sort of attentions to another lady. He went to the house, but was kicked out. Many of the great singers have been followed in this way.
69 Journal of Nervous and Mental Disease, vol. ix., No. 1, January, 1882.
Some time ago I examined a man condemned to be hanged and within twenty-four hours of his death. He was an erotomaniac, whatever else he may have been. In the shadow of the gallows he told of a lady in the town who had visited him and was in love with him, and how all the women in the neighborhood were in love with him. He had various pictures of females cut from circus-posters in his cell. Erotomania is not generally found associated with hysteria.
Convulsions or general spasms are among the most prominent of [p. 236] hysterical manifestations. Under such names as hysterical fits, paroxysms, attacks, seizures, etc. they are described by all authors. Their presence has sometimes been regarded as necessary in order that the diagnosis of hysteria might be made; but this, as I have already indicated, is an erroneous view.
Under hysterical attacks various conditions besides general convulsions are discussed by writers on hysteria; for instance, syncope, epileptiform convulsions, catalepsy, ecstasy, somnambulism, coma, lethargy, and delirium. According to the plan adopted in the present volume, catalepsy, ecstasy, somnambulism, etc. will be considered in other articles, and therefore my remarks at this point will be limited to hysterical general convulsions.
These convulsions differ widely as to severity, duration, frequency, motor excitement, and states of volition and consciousness. Efforts have been made to classify them. Carter70 describes three forms as primary, secondary, and tertiary. In the primary form the attack is involuntary and the product of violent emotion; in the secondary it is reproduced by the association of ideas; and in the tertiary it is deliberately shammed by the patient. Lloyd71 divides them into voluntary and involuntary forms, and discusses the subject as follows: “The voluntary or purposive convulsions are such as emanate from the conscious mind itself. Here are the simulated or foolish fits into which women sometimes throw themselves for the purpose of exciting sympathy or making a scene. I am convinced that a large number of hysteric fits are of this class: these are the patients who are cured by the mention of a hot iron to the back or the exhibition of an emetic. The involuntary forms of convulsion are more important. They happen in more sensible persons, and some of them are probably akin to starts, gestures, and other forcible or violent expressions of passions or states of the mind. A person wrings the hands, beats the breast, stamps upon the floor in an agony of grief and apprehension, and if terror is added he trembles violently. It is no great stretch of the imagination to suppose that great fear, anger, or some kindred passion, acting upon the sensitive nervous organization of a delicate woman or child, should throw them into a convulsion. This, in fact, we know happens. Darwin72 believes that in certain excited states of the brain so much nerve-force is liberated that muscular action is almost inevitable. He instances the lashing of a cat's tail as she watches her prey and the vibrations of the serpent's tail when excited; also the case of an Australian native, who, being terrified, threw his arms wildly over his head for no apparent purpose. The excito-motor reflexes of the cord may possibly take on true convulsive activity if released from the control of the will, which, as already said, is apt to be weak or in abeyance to this disease. Increased temperature is stated by Rosenthal to be always present in the great fits of epilepsy and tetanus, but absent in those of hysteria.”
70 On the Pathology and Treatment of Hysteria, London, 1853.
71 Op. cit.
72 Expression of Emotion, etc.
This subdivision of hysterical convulsions into voluntary and involuntary, or purposive and non-purposive, is a good practical arrangement; but the four groups into which I have divided all hysterical symptoms—namely, the purely involuntary, the induced involuntary, the impelled, [p. 237] and the purely voluntary—include or cover these two classes, and allow of explanation of special cases of convulsion which cannot be regarded as either purely shammed or as entirely, and from the first, independent of the will.
Absolutely involuntary attacks with unconsciousness constitute what are commonly called hystero-epileptic seizures, and will be described under Hystero-epilepsy.
The voluntary, impelled, or induced hysterical fit may be ushered in in various ways—sometimes with and sometimes without warning, sometimes with wild laughter or with weeping and sobbing. The patient's body or some part of it is then usually thrown into violent commotion or convulsion; the head, trunk, and limbs are tossed in various directions. Frequently the arms are not in unison with each other or with the legs. Screaming, shouting, sobbing, and laughing may occur during the course of the convulsive movement; sometimes, however, the patient utters not a word, but has a gasping, noisy breathing. She may talk in a mumbling, incoherent manner even during the height of the attack. She is tragic in attitude or it may be pathetic. The face is contorted on the one hand, or it may be strangely placid on the other. Quivering, spasmodic movements of the eyelids are often seen; but the eyes are not fixed and turned upward with dilated pupils, as in epilepsy. The patient does not usually hurt herself in these purposive attacks. She may or may not appear to be unconscious. She does not bite her tongue, nor does she foam, as does the true epileptic, although she may spit and sputter in a way which looks somewhat like the foaming of epilepsy. She comes out of the fit often with evident signs of exhaustion and a tendency to sleep, but does not sink into the deep stupor of the post-paroxysmal epileptic state. The paroxysm may last a few or many minutes. Large quantities of colorless urine are usually passed when it is concluded.
Hysterical paralysis, so far as extent and distribution are concerned, may be of various forms, as (1) hysterical paralysis of the four extremities; (2) hysterical hemiplegia; (3) hysterical monoplegia; (4) hysterical alternating paralysis; (5) hysterical paraplegia; (6) hysterical paralysis of special organs or parts, as of the vocal cords, the œsophagus and pharynx, the diaphragm, the bowels, and the bladder. Russell Reynolds73 has described certain cases closely allied to, if not identical with, some forms of hysterical paralysis under the head of paralysis dependent upon idea. These patients have a fixed belief that they are paralyzed. The only point of separation of such cases from hysterical paralysis is the absence of other hysterical manifestations. Perhaps it would be better to regard the condition either simply as hysterical paralysis or as a true psychosis—an aboulomania or paralysis of the will. Such cases often last for many years.
73 Brit. Med. Journ., 1869, pp. 378, 483.
Among the 430 hysterical cases of Briquet, only 120 were attacked with paralysis. In 370 cases of Landouzy were 40 cases of paralysis.
Briquet reports 6 cases in which paralysis attacked the principal muscles of the body and of the four extremities; 46 cases of paralysis of the left side of the body, and 14 of the right; 5 of the upper limbs only; 7 of the left upper limb, and 2 of the right; 18 of the left lower limb, [p. 238] and 4 of the right; 2 of the feet and hands only; 6 of the face; 3 of the larynx; and 2 of the diaphragm. Landouzy gathered from several authors the following results: General paralysis in 3 cases; hemiplegia in 14; 8 cases of paralysis of the left side; in other cases the side affected not indicated; and 9 cases of paraplegia.
Hysterical paralyses, no matter what the type, may come on in various ways—suddenly, gradually, from moral causes or emotional excitement, or from purely physical causes, as over-fatigue. They may have almost any duration, from hours or days to months or years, or even to a lifetime. They are frequently accompanied by convulsive or emotional seizures. They may be of any degree of severity, from the merest suspicion of paresis to the most profound loss of power. Hysterically paralyzed muscles retain their electro-contractility. Limbs which have become atrophied from disuse may show a temporary lessening of response, but this is quantitative and soon disappears. In rare cases, owing probably to the condition of the skin, the response to electricity is not obtained until the current has been applied for several minutes to the muscles.
Hysterical hemiplegia and monoplegia may simulate almost any type of organic paralysis. The paralysis is usually in a case of hemiplegia, confined to the arm and leg, the face being slightly, if at all, implicated. Hysterical paralysis, limited to the muscles supplied by the facial nerve, is very rare. According to Rosenthal, it sometimes coexists with paralysis of the limbs of the same side, and is usually accompanied by anæsthesia of the skin and special senses. In a few rare cases, according to Mitchell, the neck is affected.
Several cases of hysterical double ptosis have come under my observation. The condition is usually one of paresis rather than paralysis. Cases of unilateral ptosis hysterical in character have also been reported. Alternating squints are sometimes hysterical, but they are usually of spasmodic rather than of paralytic origin.
Hysterical hemi-palsy is more frequent on the left than in the right side. In Mitchell's cases the proportion was four left to one right. The figures of Briquet have been given. It is usually, but not always, accompanied by diminished or abolished sensibility, both muscular and cutaneous. Electro-sensibility especially is markedly lessened in most cases.
When hemiplegia is of the alternating variety, the arm on one side and the leg on the other, or, what is rare in paralysis of organic causation, both upper extremities and one lower, or both lower and one upper, may be affected. Alternating hemiplegia of the organic type is usually a paralysis in which one side of the face and the leg and arm of the opposite side are involved.
Hysterical paraplegia is one of the most important forms of hysterical paralysis, and is sometimes the most difficult of diagnosis. It occurs usually, but not exclusively, in women. It comes on, particularly in young women, between puberty and the climacteric period, commonly between the twentieth and thirtieth years. Such a patient is found in bed almost helpless, possibly able to move from side to side, but even by the strongest efforts seemingly incapable of flexing or extending the leg or thigh or of performing any general movements of the foot. The feet are probably in the equino-varus position—extended and [p. 239] turned inward. Certain negative features are present. The muscles do not waste to any appreciable extent, as they would in organic paralysis. Testing the knee-jerk, it is found retained, possibly even exaggerated. The electrical current causes the muscles to contract almost as well as under normal conditions; if a difference is present, it is quantitative and not qualitative in character. Paralysis of the bowels and bladder is not usually found, although it is but fair to state that this appears not to be the conclusion arrived at by some other observers.
Paralysis or paresis of the vocal cords, with resulting aphonia, is a common hysterical affection. Hysterical aphonia is also due to other conditions—for instance, to an ataxia or want of co-ordinating power in the muscles concerned in phonation; or to spasm, real or imaginary, in the same parts. Hysterical paralysis of the vocal cords is almost invariably bilateral; viewed with the laryngoscope, the cords are seen not to come together well, if at all. One may be more active than the other; but a distinct one-sided paralysis of this region nine times out of ten indicates that the case is not hysterical.
The following case is of interest, not only because of the aphonia, but because also of the loss of the power of whispering. The patient, a young lady of hysterical tendencies, while walking with a friend stumbled over a loose brick and fell. She got upon her feet, but a moment or two after either fainted or had a cataleptoid attack. Several hours later she lost her voice and the power of whispering. She said that she tried to talk, but could not form the words. This condition had continued for ten months in spite of treatment by various physicians. She carried a pencil and a tablet, by means of which she communicated with her friends. She had also suffered with pains in the head, spinal hyperæsthesia; and occasional attacks of spasm. Laryngoscopic examinations showed bilateral paresis of the vocal muscles, without atrophy. The tongue and lips could be moved normally. She was assured that she could be cured. Faradic applications with a laryngeal electrode were made daily; tonics were given; and the patient was instructed at once to try to pronounce the letters of the alphabet. In less than a week she was able to whisper letters, and in a few days later words. In three weeks voice and speech were restored. Just as this patient was recovering another came to be treated for loss of voice. She was markedly aphonic, but could whisper without difficulty. She was told, to encourage her, that she need not be worried about her loss of voice, as another patient, who had lost not only her voice, but the ability to whisper, had recovered. The patient returned next day unable to whisper a syllable. She made, however, a speedy recovery. Under the name apsithyria, or inability to whisper, several cases of this kind have been reported by Cohen.
Hysterical paralyses of the pharynx and of the œsophagus have been reported, but are certainly of extreme rarity. Hysterical dysphagia is much more frequently due to spasm or a sensation of constriction.
Paralysis of the diaphragm in hysteria has been described by Duchenne and Briquet. I have had one case under observation. The abdomen is drawn inward instead of being pushed outward in the act of inspiration in organic paralysis of the diaphragm; this condition is simulated, but not completely or very closely, in the hysterical cases. In some of the [p. 240] cases of nervous breathing, which will be referred to hereafter, the symptoms are rather of a spastic than of a paretic affection of the diaphragm.
Paralysis or paretic states of the stomach and intestines are not uncommon among the hysterical, and produce tympanites, one of the oldest symptoms of hysteria. Jolly asserts that this “sometimes attains such a degree that the patients can be kept afloat in a bath by means of the balloon-like distension of their bellies”! The loss of power in the walls of the stomach and bowels is sometimes a primary and sometimes a secondary condition. The abdominal phantom tumors of hysterical women sometimes result from these paralytic conditions. These abdominal tumors are among the most curious of the phenomena of local hysteria. At one time two such cases were in the women's nervous wards of the Philadelphia Hospital. Both patients had been hysterical for years. In the first the tumor occupied the middle portion of the abdomen, the greater portion of its bulk more to the right of the median line. It was firm and nearly spherical, and the patient complained of pain when it was handled. She was etherized, and while under ether, and during the time that she was vomiting from the effects of the anæsthetic, the tumor disappeared, never to return. The other patient had a similar tumor for three days, which disappeared after the etherization of the first case.
Mitchell74 has recorded some interesting paretic and other hysterical disorders of the rectum and defecation. Great weakness, or even faintness, after each stool he has found not uncommon, and other more formidable disorders occur. A patient who had been told that her womb was retroverted and pressing upon her rectum, interfering with the descent and passage of the feces, was troubled with hypersensitiveness of the lower bowel. This condition Mitchell designated as the excitable rectum. Patients in whom it is present apparently have diarrhœa; certainly they have many movements daily. Single stools, however, are small, and may be quite natural or they may seem constipated. The smallest accumulation of fecal matter in the rectum excites to defecation. One case had small scybalous passages every half hour. The forms of hysterical paresis or paralysis or pseudo-paralysis of the rectum observed by Mitchell were due—(1) to a sensory paralysis of the rectum; (2) to a loss of power in the rectal muscular walls; (3) a want of co-ordination in the various muscles used in defecation; (4) to a combination of two or of all of these factors. In rare cases the extrusive muscles act, but the anal opening declines to respond.
74 Op. cit.
Hysterical locomotor ataxia, or hysterical motor ataxia, is an affection less common than hysterical palsy, but by no means rare. Various and diverse affections of motion are classed as hysterical ataxia by different authors. Mitchell speaks of two forms independent of those associated with vertigo. The first, that described by Briquet and Laségue, seems to depend upon a loss of sensation in both skin and muscles; the second often coexists with paralysis or paresis, and is an affection in which the patient has or may have full feeling, and is able to use the limbs more or less freely while lying down. As soon as she leaves the recumbent position the ataxia is very evident. She falls first to one side and then to the other. She “seems to be unable to judge of the extent to which balance is lost, and also to determine or evolve the amount of [p. 241] power needed to overcome the effect.” Mitchell believes that this disorder is common in grave hysteria, and is likely to be confounded with one of the forms of hysterical alternating spasm, in which first the flexors and then the extensors contract, the antagonistic muscles not acting in unison, and very disorderly and eccentric movements being the result. I have reported a case of hystero-epilepsy75 in which a spasmodic condition closely simulated hysterical ataxia. The patient had various grave hysterical symptoms, with epileptoid attacks. She became unable to walk, or could only walk a few steps with the greatest difficulty, although she could stand still quite well. On attempting to step either forward or backward, her head, hips, shoulders, and trunk would jerk spasmodically, and she would appear to give way at the knees. No true paralysis or ataxia seemed to be present, but locomotion was impossible, apparently because of irregular clonic spasms affecting various parts of her body.
75 Journal of Nervous and Mental Disease, vol. ix., No. 4, October, 1882.
Mary Putnam Jacobi76 has reported a case occurring in an Irish woman aged thirty-five years as one of hysterical locomotor ataxia. It is questionable whether this case was not rather one of posterior spinal sclerosis with associated hysterical symptoms. The existence of pain resembling fulgurating pains, and especially the absence of the patellar tendon reflex, would incline me to hesitate a long time before accepting the diagnosis of hysteria, particularly as it is known that organic locomotor ataxia often has a much-prolonged first stage, and that wonderful temporary improvements sometimes take place.
76 Arch. of Medicine, New York, 1883, ix. 88-93.
Ataxic symptoms of a mild form are of frequent occurrence in hysteria. They are shown by slight impairments of gait and difficulty in performing with ease and precision many simple acts, as in dressing, writing, eating, etc.
Hughes Bennett and Müller of Gratz call attention to the fact that young women may exhibit all the signs of primary spastic paralysis, simulating sclerosis, and yet recover.77 I have seen several of these cases of hysterical spasmodic paralysis, and have found the difficulties in diagnosis very great. These patients walk with a stiff spastic or pseudo-spastic gait, and as, whether hysterical or not, the knee-jerk is likely to be pronounced, their puzzling character can be appreciated.
77 Quoted by Althaus: On Sclerosis of the Spinal Cord, by Julius Althaus, M.D., M. R. C. P., etc., New York, 1885, p. 330.
In one class of cases, which cannot well be placed anywhere except under hysteria, a sense or feeling of spasm exists, although none of the objective evidences of spasmodic tabes can be detected. Comparing these to those which Russell Reynolds describes as paralysis dependent upon idea, they might be regarded as cases of spasm dependent upon idea.
One case of this kind which was diagnosticated as lateral sclerosis by several physicians recovered after a varying treatment continued for several years, the remedy which did him the most good being the actual cautery applied superficially along the spine. The patient described his condition as one of “spasmodic paralysis of all the muscles of the body.” If sitting down, he could not at once get up and walk or run, but would have to use a strong effort of his will, stretching his limbs several times [p. 242] before getting on his feet. Movements once started could be continued without much difficulty. When his hands were closed he would be unable, at times, to open them except by a very strong effort of the will. If one was opened and the other shut, he could manipulate the latter with the former. He sometimes complained of a sensation as of a steam-engine pumping in his back and shaking his whole body. He would sometimes be in a condition of stupor or pseudo-stupor, when he had a feeling as if he was under the influence of some poison. The spasms or jumpings in the back he thought sometimes caused emissions without erections. He compared the feeling in his back to that of having a nerve stretched like a piece of india-rubber. The excitement of mind would then cause the nerve to contract and throb. This description shows that the symptoms were purely subjective. Examination of the muscles of the legs and arms did not reveal, as in true spastic paralysis, conditions of rigidity. The limbs would sometimes be stiff when first handled, volition unconsciously acting to keep them in fixed positions; but they would soon relax. The knee-jerk, although well retained, was not markedly exaggerated, as in spastic paralysis, nor was ankle clonus present. The patient did not get progressively worse, but his condition vacillated, and eventually he recovered. A friend of the patient, living in the same neighborhood and going to the same church, was affected with true lateral sclerosis. It is worth considering how far in an individual of nervous or hysterical temperament observation of an organic case could have influenced the production of certain subjective symptoms, simulating spasmodic tabes.
Certain special forms of chorea are particularly liable to occur in the course of cases of hysteria. The most common type of the chorea of childhood, if not strictly speaking hysterical, is frequently associated with a hysteroid state, and is best treated by the same measures that would be calculated to build up and restore an hysterical patient. The following conclusions, arrived at by Wood78 after a clinical and physiological study of the subject of chorea, show that certain forms of chorea may be hysterical or imitated by hysteria:
1st. Choreic movements may be the result of organic brain disease.
2d. Choreic movements exactly simulating those of organic brain disease may occur without any appreciable disease of the nerve-centres.
3d. General choreic movements, as well as the bizarre forms of electric and rhythmical chorea, may occur without any organic disease of the nervous system.
78 “Chorea: a Study in Clinical Pathology,” by H. C. Wood, M.D., LL.D., Therapeutic Gazette, 3d Series, vol. i., No. 5, May 15, 1885.
To these propositions may be added a fourth—viz. Choreic movements may be the result of a peripheral irritation, or, in other words, may be reflex.
Hysterical rhythmical chorea is a form of chorea in which involuntary movements are systematized into a certain order, so as to produce in the parts of the body which are affected determinate movements which always repeat themselves with the same characters. The movements are strikingly analogous to the rhythmical movements, as those of salutation, which often occur in the second period of the hystero-epileptic attack. Rhythmical chorea should undoubtedly be arranged among the [p. 243] manifestations of grave hysteria. An account of an interesting case of this kind is given in a lecture by Wood, reported by me in the Philadelphia Medical Times for Feb. 26, 1881.
As Charcot has shown, rhythmic chorea is usually of hysterical origin, although it may exist without any of the phenomena which usually characterize hysteria. In these cases the movements imitated are according to a certain plan; thus, they may be certain expressive movements, as some particular form of dancing or the so-called saltatory chorea. They may be, again, certain professional or trained actions, such as movements of hammering, of rowing, or of weaving. Charcot speaks of a young Polish girl in whom movements of hammering of the left arm lasted from one to two hours, and occurred many times in a day for seven years. He has also given an account of another case, a patient with various grave hysterical manifestations, who would have a pain and beating sensation in the epigastrium, accompanied by a feeling of numbness. The right upper extremity would then begin to move; this would soon be followed by the left, and then by the lower extremities; then would follow a succession of varied action, complex in character, but in which rhythm and time and correct imitation of certain intentional and rational movements could readily be recognized. The attacks could be artificially induced in this patient by pulling the right arm or by striking on the patellar tendons with a hammer. During the whole of the attack the patient was conscious. In another patient rhythmical agitations of the arm, the movement of wielding a hammer, were produced in the first stage; then followed tonic spasms and twisting of the head and arms, suggesting a partial epilepsy; finally, rhythmical movements of the head to the right and left took place, the patient at the same time chanting or wailing.79
79 Charcot's lectures in Le Progrès médical for 1885.
In the following case an hysterical jumping chorea was probably associated with some real organic condition or was due to malarial infection. The patient was a middle-aged man. During the war he received a slight shell wound in the back part of the right thigh, and from that time suffered more or less with numbness and some weakness of the right leg. He was of an active nervous temperament. About three months before coming under observation he had without warning a peculiar attack which, in his own words, came on as if shocks of electricity were passed through his head, back, limbs, and other parts of the body. In this attack, which lasted for fully an hour, he jumped two or three feet in the air repeatedly; his arms, legs, and even his head and eyes, shook violently. He was entirely conscious throughout, but said nothing except to ask for relief. His wife, who was present, stated that at first he was pale, and afterward, during the attack, he became almost turgid under the eyes. Attacks appeared to come at intervals of seven and fourteen days for a time, so that his family physician surmised that there might be some malarial trouble, and prescribed for him accordingly. They soon, however, became irregular in character, and did not occur at periodical intervals. After the attacks he would lie down and go to sleep; he did not, however, pass into the condition of stupor that is observed after a grave epileptic seizure. His sleep seemed to be simply that of an exhausted nervous system.
[p. 244]Hysterical tremor is of various forms and of frequent occurrence: a single limb, both upper or both lower extremities, or the entire body may be affected. In a case of hystero-epilepsy, which will be reported in the next article, the patient had a marked tremor of the left arm, forearm, and hand, which was constant, but worse before her attacks; it remained for many months, and then disappeared entirely. Caraffi80 reports the case of an hysterical girl of eighteen, anæsthetic on the right side and subject to convulsive attacks, who fell on the right knee and developed an arthritis. At the Hôpital Beaujon service of Lefort and Blum she presented herself with the above symptoms, aphonia, and an uncontrollable tremor of the right lower extremity, and trophic disturbances of the same. Immobilization of the limb was tried without benefit, and Blum then stretched the sciatic, with complete relief of the tremor and of the troubles of sensibility and of nutrition.
80 L'Encéphale, June, 1882.
Hysterical contracture, like hysterical paralysis, may assume a variety of forms: it may be hemiplegic, monoplegic, paraplegic, alternating, or local, as of the ocular muscles, the facial or neck muscles; laryngeal, pharyngeal, or œsophageal; of the fingers or of the toes.
Richardson81 records the case of a young lady who saw in India a religious devotee with his leg flexed upon his body and fastened there. In a few hours she was found with her leg in a similar position, and this contracture remained until after she had been taken to London; then it disappeared as suddenly as it came. Conscious purpose could not have maintained the leg in such a position for an hour.
81 Diseases of Modern Life.
Some of the most remarkable cases of hysterical contracture are those chiefly studied by the French, which originate before or after convulsive seizures. Among the hystero-epileptics at Salpêtrière, Richer82 reports many varieties of contracture: one with hemianæsthesia and varying pain in the right side had permanent contracture with tremulousness of the lower extremities; another, with hemianæsthesia, pain, and frequent attacks of demoniacal delirium and paresis, had momentary contractures of the upper and lower extremities on the right side. In two other cases the contractures were of the hemiplegic form, while three others were paraplegic. In still other cases the contracture was monoplegic. Besides hemiplegic, monoplegic, and paraplegic contractures, I have seen illustrations of a number of local forms—among others, several remarkable cases of hysterical contractures of the wrist and hand and of the feet and toes, and one of hysterical torticollis. Hysterical contracture in any of its forms may occur as an isolated symptom or series of symptoms unconnected with the grave hysterical attack.
82 Op. cit.
Many forms of hysterical local spasms occur. Hysterical strabismus from spasm of the ocular muscles has been observed. Several cases have come under observation in which hysterical blepharospasm was present. In these cases, when the lids are forced open, the eyes disappeared in an extraordinary manner, usually being drawn downward and toward the internal canthus. Hysterical facial spasm occurs, and is usually clonic. One of the most remarkable hysterical local spasmodic affections which has come under personal observation was reported by me in a paper on chorea.83 In this case the right ear twitched and moved up and down. [p. 245] The movement of the ear was peculiar; it continued nearly all the time, even when the patient's attention was not directed toward the part. The act seemed to be partially under the control of the will, as by a strong effort the left ear could be moved very slowly in the same up-and-down direction. The nostrils and upper lip were affected with twitching, and slight choreic movements were present in the entire right side of the body. The patient's general condition improved under treatment, but when last seen the local affection persisted, although it was not so severe.
83 Philada. Med. Times, March 27, 1875.
Spasm of the pharynx, larynx, and œsophagus have been separated by several authors. In hysterical laughter spasmodic contraction of the laryngeal muscles occurs. Spasm of the glottis occurs in rare cases, according to Rosenthal, from the reflex effect of hyperæsthesia of the laryngeal mucous membrane, from irritation of the recurrent laryngeal nerve. Death from asphyxia has occurred in consequence of this form of spasm of the glottis.
Hysterical dysphagia, which is usually spasmodic, is sometimes a dangerous, and always an annoying, affection. An unmarried lady, forty years old, with a neurotic family history, a maternal uncle and aunt having been insane, at intervals since puberty had had various hysterical manifestations. After a severe winter, during which she had suffered more or less with rheumatism, she became depressed with reference to her spiritual condition: she had, in fact, a form of mild religious melancholia. After this had lasted for weeks she began to experience difficulty in swallowing. She would rise from the table suddenly, alarmed and gasping, and exclaiming that she could not swallow and was choking. She got so bad that she could not take anything but liquid food, and not nearly enough of this. She believed that her throat was gradually closing, and of course suspected cancer. She was assured that if any local obstruction existed it could be removed with one application of a probang. Cancer was also confidently excluded, and she was given iron, valerian, and quinine, and in a few days an instrument was passed down her throat. She as told that she would have no more difficulty. Tonics and full feeding were continued, and in less than a week she swallowed without any difficulty.
Of the so-called hysterical asthma or hysterical breathing I have seen several examples. A curious form of hysterical breathing, at least partly spasmodic, recently came to the Philadelphia Polyclinic—a young man twenty-one years of age, who confessed that he had been guilty of excessive masturbation for five or six years. He had been a moderate drinker and was the victim of an old hip disease. According to his story, this abuse had never appeared to have impaired his health until about one month before applying for treatment, when he began to have attacks of peculiar breathing. He would have a series of rapid, forced expirations which lasted for a period of from one to two or three minutes. He would then stop for a moment; then again the shallow breathing with forced expirations would ensue. He said that he breathed in this way because he thought he was going to die, and did so to keep alive. When he stopped he felt cold. He thought his belly did not go outward as it should in the act of breathing. During the time that the symptoms had been present he had had several frightful attacks of excitement, in one of which he ran breathing in the manner described to a [p. 246] drug-store from one to two blocks away, jumping, gesticulating, and calling for remedies. He had an anxious expression of the face, a look of excitement and worriment. His pulse was 110 and weak. Respirations during these attacks ranged from 38 to 50.
Coates,84 speaking of hysterical or nervous breathing, gives the details of five cases. Four of these had been supposed to be suffering from phthisis; the fifth was apparently a case of hypertrophy of the heart. The breathing was quick and shallow. The patients could not be induced to draw long breaths until the expedient was adopted of having them count twenty without taking breath. During this the lungs expanded perfectly, air entering freely into every part. Coughing, and even blood-spitting of a venous character, were present. They might perhaps be classed as cases of hysterical or simulated phthisis.
84 British Medical Journal, 1884, ii. 13.
Vaginismus, or spasm of the vagina, may with propriety be regarded as hysterical in some but not in all cases. Spasmodic contracture of the sphincters of the bladder and anus is also mentioned by Rosenthal. Goose-flesh, according to the same author, is a frequent phenomenon in the hysterical, and is due to spasmodic contraction of the muscular fibres contained within the skin.
The sensorial affections of hysteria can be classified according either to character or location. According to the character of the sensory disturbance a good practical arrangement is into cases of (1) Anæsthesia; (2) paræsthesia; (3) hyperæsthesia; (4) neuralgias and localized pains,—although one of these classes may sometimes be difficult to separate from another, or a doubt may arise as to whether or not a special symptom should be placed under one or another head. In hysterical anæsthesia sensation is decreased or abolished; in paræsthesia it is faulty or perverted; in hyperæsthesia it is increased over a more or less extensive surface; in neuralgia, pain is confined to certain nerve-trunks. The localized pains are neuralgic or mimetic, and are found in special localities, as in joints and in the breast.
Anæsthesia is one of the most frequent of hysterical phenomena, but is not, as stated by some authorities, present in all cases of genuine hysteria.
In 400 hysterical cases Briquet found 240 positive examples of anæsthesia. In this statement, however, he does not include cases of insensibility of the conjunctiva of the left eye or those cases in which anæsthesia lasted but a few hours after an attack. It is safe to say that anæsthesia of some sort is present in from 60 to 75 per cent. of all cases of well-marked hysteria. Analgesia, or insensibility to pain, is present frequently when loss or diminution of sensibility to touch, pressure, heat and cold, etc., is not observed.
Hysterical anæsthesia, may be of various forms, according to the parts of the body affected, as general anæsthesia; hemianæsthesia; anæsthesia of the lower half of the body; anæsthesia of one limb or one side of the face; anæsthesia of mucous membranes; anæsthesia of muscles, bones, and joints; anæsthesia of the viscera.
General anæsthesia is extremely rare. No example of it has ever fallen under my observation, but by Briquet and others a few cases have been reported.
[p. 247]Hemianæsthesia has in recent years received much attention from neurologists. In hystero-epilepsy it is the rule to find it present, but it is also observed in cases without spasms. In hemianæsthesia the loss of sensation exists in one lateral half of the body. Parts are insensible to various methods of stimulation—to impressions of touch, pain, temperature, and weight. Sometimes the mucous membranes of the side affected are involved. The sight, hearing, taste, and smell are commonly impaired if not lost.
Much attention has been paid to the study of hemianæsthesia by French physicians. Charcot85 has an admirable historical summary and clinical description of the condition, leaving little for others to add. Piorry, Macario, Gendrin, Szokalsky, and Briquet are referred to by him. Briquet found it present in 93 cases out of 400. It is of much more frequent occurrence on the left side. According to Briquet, 70 cases were affected on the left side to 20 on the right.
85 Op. cit.
Next to hemianæsthesia, anæsthesia of the lower half of the body is most common in hysterical cases. While hemianæsthesia often presents itself conjoined with hystero-epileptic symptoms, anæsthesia of the lower half of the body may be present as frequently without as with convulsive manifestations. Anæsthesia of one limb or of one side of the face is almost as rare as general anæsthesia, but does occur.
Anæsthesia of mucous membrane is an old observation. It may affect mucous membranes everywhere—of the nose, pharynx, larynx, vagina, urethra, the bladder, rectum, etc. Many of the peculiar and apparently inexplicable hysterical symptoms are due to the presence of this anæsthesia—such symptoms, for instance, as want of inclination to evacuate the bowels or the bladder, absence of sexual desire, absence of sensibility when applications are made to the throat, etc. Loss of sensibility in muscles, bones, joints, and viscera may be present, but is of course frequently overlooked from want of minute investigation. In hemianæsthesia the viscera of the anæsthetic side are sometimes hyperæsthetic. Thus the ovary, as has been especially shown by Charcot, may be very painful on pressure when the abdominal wall is perfectly insensible.
A striking characteristic of hysteroid sensory disorders of the anæsthetic variety is the suddenness with which they come and go. A complete transference of anæsthesia from one side of the body to another may occur in a few seconds, either without special interference or under the use of metals or electricity.
The term achromatopsia is due to Galezowski. Hysterical achromatopsia is a condition in which there is a failure to appreciate colors. In Daltonism, or true color-blindness, one color may be taken for another; in achromatopsia the notion of color may be completely lost. These colors are found by the patient to disappear in a regular order, and return in a reverse order as the patient recovers. Some remarkable cases of this kind have been reported as occurring among French hysterics. A few examples of the same affection have been reported in America. Sometimes the patient has lost perception of one or several colors. When only one color is lost, it is usually the violet; if two, the violet and green; then in regular succession follow the colors of the spectrum.
[p. 248]Hysterical blindness and achromatopsia have been well studied by Charcot and Richer and others of the French school. Special articles on hysterical or simulated affections of the eye have also been published by Schweigger,86 Harlan,87 and others.
86 “On Simulated Amaurosis,” by C. Schweigger, Prof. at the University of Berlin, New York Medical Journal, Feb., 1866.
87 “Simulated Amaurosis,” by George C. Harlan, M.D., American Journal of Medical Sciences, October, 1873; “Hysterical Affections of the Eye,” Transactions of the College of Physicians of Philadelphia, 3d Series, vol. ii., 1876.
In several cases of hystero-epilepsy under my care both amblyopia and achromatopsia were present. In one of these cases the patient was unable to read print of any size or to distinguish any colors, although she could tell that objects were being moved before the eyes. An ophthalmoscopic examination showed a normal fundus. Each eye was tested for near vision. It was found that she could read quite well with the right eye, and not at all with the left. While reading at about sixteen inches a convex glass of three inches focus was placed in front of the right eye, but she still continued to read fluently.
C. H. Thomas of Philadelphia has given me the particulars of a case of a woman about thirty-eight years old, both of whose eyes were, to all appearances, absolutely blind. The attack came on suddenly, the apparent cause seeming to be worry over a sick child. Ophthalmoscopic and other examinations of the eye showed nothing. She had no perception of light. She could look without winking at a blinding reflection of a whitewashed fence. In six weeks under a mere tentative treatment she got absolutely well. S. D. Risley of Philadelphia,88 in a discussion at the Philadelphia Neurological Society, held that the feeble innervation of the hysterical patient was liable to diminish the range of accommodation and power of convergence, rendering the comfortable use of the eye impossible; and also that the feeble or deranged circulation in the hysterical individual might set up a group of symptoms in the eye presenting many of the characteristics of serious disease; which, however, were not simulated, but were, in fact, a relative glaucoma. While there was no absolute increase of intraocular tension, the normal tension of the eyeball was sufficient to interrupt the entrance of the feeble blood-stream into the eyes, and thus was set up the same group of symptoms as were present in actual increase of tension—viz. inadequate blood-supply to the retina, contracted field of vision, impaired central perception, diminished range of accommodation, and inability to use the eyes, particularly at a near point.
88 The Polyclinic, vol. ii., No. 8, Feb. 15, 1885, p. 124.
Very few observations in cases of hysteria have been made with the ophthalmoscope, and probably little is to be learned in this way. In one of Charcot's patients, however, Galezowski saw an infiltration and capillary reddening of the disc with fusiform dilatations of the artery.
What might be termed hysterical dilatation of the pupil is sometimes observed. In the case reported by Harlan, to be hereafter detailed, the patient, a young girl who had a train of hysterical symptoms, began to complain of blindness or imperfect vision in the right eye, the pupil of which was found to be dilated. No proof could be obtained of the use of any mydriatic. The pupil remained dilated when exposed to a bright light. The dilatation came and went at intervals, and finally disappeared under [p. 249] the applications of a wooden magnet. W. Chester Roy has acquainted me with the facts of the case of a man who could at will alternately contract and dilate his pupils. This case would seem to lend color to the idea that the hysterical girl may have had voluntary control of the pupillary movements. In her case, however, only one pupil was involved. F. X. Dercum has given me the particulars of a case of rhythmical dilatation of the irides in a case of confirmed masturbation with hysterical symptoms.
Hysterical deafness has been observed and studied. Walton,89 at Charcot's suggestion, has published the results of the examination at La Salpêtrière of 13 patients affected with hemianæsthesia with reference to anæsthesia of hearing. He divides hemianæsthetic patients into three classes: (1) Those with complete anæsthesia of one side, the other side remaining normal; (2) those having incomplete anæsthesia on one side, the other remaining normal; (3) those with anæsthesia more or less complete on both sides. In the first class anæsthesia of hearing extended to the deep parts of the ear; the membrane of the drum could be touched without eliciting any acknowledgment of sensation and without the least reflex movement. He also showed that the anæsthesia extended to the middle ear by the fact that insufflation by Politzer's air-douche produced no sensation in the ear of the affected side. In this class neither the watch, voice, nor tuning-fork was heard. In the second class, with incomplete anæsthesia on one side, the lost sensibility corresponded, as a rule, with that of the body in general. A common form was analgesia with thermoanæsthesia and diminution of the tactile sensibility. In the third class completeness of the anæsthesia is rarely the same on both sides, a common form being complete hemianæsthesia on one side and analgesia on the other.
89 Brain, January, 1883.
A noticeable feature in all the cases under consideration was the uniformity with which the deafness for conveyance by the bone exceeded that for sounds conveyed by the ear. Walton says: “This is probably due to the fact that the vibrations conveyed to the ear by the air are better adapted for the irritation of the peripheral auditory apparatus than those conveyed by the bone. When, then, the receptive power of the auditory centres is lessened, as is probably the case in hysterical patients, the hearing for sounds conveyed by the bones disappears before that for sounds conveyed by the ear. This enfeeblement of the auditive centres in hysteria is quite analogous to that in old age, in which, as is well known, the perception for sounds conveyed by the bone disappears before that for sounds conveyed by the air, the former being sometimes completely lost before the age of sixty.” His principal conclusions are as follows: (1) The sensibility of the deep parts of the ear, including the tympanum and middle ear, disappears in hysterical hemianæsthesia with that of other parts of the body, and in the same degree. (2) The degree of deafness corresponds with that of the general anæsthesia, being complete when the latter is complete, and incomplete when the latter is incomplete. (3) When loss of hearing is incomplete, the deafness for sounds conveyed by the bone exceeds that for sounds conveyed by air. (4) When the transfer is made, the hearing, as well as the general sensibility of the deep parts of the ear, improves on one side (allowance being made for accidental [p. 250] lesions in the ear itself) in exactly the same degree in which it disappears on the other.
The following case has been kindly furnished to me by Charles S. Turnbull, the patient having in the first instance come to Philadelphia to consult his father, Laurence Turnbull: The patient was a young lady from New Jersey, eighteen years old. Her general health was good, although at times she had a pale and anxious look. She had never had any unusual sickness. Soon after the death of her mother, for whom she grieved very much, she began to grow deaf, and was for a time treated by her family physician. When she first came to Philadelphia she was absolutely deaf, but the most careful examination failed to discover a cause for the deafness in any affection of the external or middle ear. A current from ten cells of a galvanic battery was painful, but elicited no sound. She declared that she could not hear a musical box held close to the side of her head. In communicating with her, everything had to be written. A faradic current was used daily to her ears. Suddenly one morning, after a powerful current had been applied, her hearing returned, but before she came back for treatment the next day it had again left. The electrical treatment was continued: each day the hearing stayed longer and longer, and finally returned in full force and remained good.
By hysterical paræsthesia is meant that form of perverted sensation which is not distinctly depressed on the one hand or markedly increased on the other. Under this head would come such conditions as numbness, formications, prickling and tingling sensation, the sensation of a ball in the throat or globus hystericus, etc. These forms of perverted sensation are quite common among the hysterical.
Hyperæsthesia may present itself in almost any locality, its areas of distribution corresponding very well to those which have been given for anæsthesia. Hyperæsthesia of the special senses is of especially frequent occurrence. Great sensitiveness to sounds and to bright lights or to particular colors is commonly observed. What might be termed hysterical tinnitus aurium is met with occasionally.
Perversions of the senses of smell and taste are among the rarer phenomena in the sensory sphere in hysteria. These may be of three kinds: the senses may be completely obtunded; they may be hyperacute; or they may show peculiar perversions. To some individuals of the hysterical temperament certain smells are almost unendurable, and these may be odors which to others are particularly pleasant. In like manner, certain articles of food or drink may be the source of great discomfort or absolute suffering. It is one of the oldest of observations that hysterical and morbid cravings for disagreeable or disgusting substances sometimes exist.
In one group of hysterias the presence of pain is the predominating feature. Some of the situations in which hysterical pains are most frequently felt are the head, the pericardial or left inframammary region, over the stomach and spleen, the left iliac region, the region of the kidneys, the sacrum, the hip, the spine, the larynx and pharynx, one or both mammæ, or over the liver and the joints. Of these locations, omitting the consideration of headache, the most common seats of hysterical pain are the spine, the breasts and inframammary region, the left iliac or ovarian region, the sacrum or coccyx, and the joints.
[p. 251]Charles Fayette Taylor, in a brochure on sensation and pain,90 has given a philosophical explanation of such pain, drawing largely from Carpenter, Bain, Spencer, and others. The pith of the matter is that many of our sensations are centrally initiated, the memory of previous objective sensations. “Pain is different from ordinary sensations, in that it requires an abnormal condition for its production, and that it cannot be produced without that abnormal condition. Hence it is impossible to remember pain, because the apparatus does not exist for causing such a sensation as pain after the fact or when it is to be remembered. Memory is a repetition, in the nerve-centre, of energy which was first caused by the sensory impulse from without. But centrally initiated sensations may be mistaken, in consciousness, for pains depending wholly on a certain intensity of excitability in the cerebral mass.”
90 Sensation and Pain, by Charles Fayette Taylor, M.D.—a lecture delivered before the New York Academy of Sciences, March 21, 1881.
A large percentage of all cases of hysteria complain more or less of spinal irritation. Spinal periostitis, spinal caries, and perhaps some cases of spinal meningitis, are organic diseases which may give rise to tenderness on pressure along the spine; but the majority of cases of spinal irritation are found among neurasthenic or hysterical patients. So much has already been written about spinal irritation that much time need not be spent on the subject, were it not that even yet many practitioners are inclined to regard cases as organic spinal trouble because of the presence of great spinal tenderness, whereas this symptom is almost diagnostic of the absence of real spinal disease.
Painful diseases of the joints, especially in women, are not infrequently hysterical or neuromimetic. Many such cases have been reported. Taylor states, as the results of much carefully-guarded experience, that hundreds of lame people are walking about perfectly who do not know that they ought to limp, and that a much larger number are either limping and walking on crutches, or not walking at all, who have no affection whatever causing lameness.
Paget—and his experience accords with that of others—makes the hip and knee, among the joints, the most frequent seats of nervous mimicry as well as of real disease. According to him, mimicries in other joints are almost too rare for counting; and yet in my first case of this kind the pain was located in the shoulder. This case made a lasting impression. The patient was a young lady of nervous temperament, who came complaining of severe and continuous pain in the left shoulder. No history of injury was given. The pain was said to be rheumatic. Handling the arm and pressure round the joint caused extreme pain. No heat, no redness, no swelling were discoverable. The patient left me and went to a magnetic doctor, who entirely dispelled the disorder on her first visit by gently stroking the arm and shoulder. Another patient had been accidentally struck in the knee. No swelling, heat, or other signs of inflammation followed the accident, and did not afterward appear; but at intervals, for several years, she complained of severe pain in and around this joint. She would be for days, or it might be for weeks, without speaking of the pain; and then again she would complain almost incessantly, and would sometimes limp. These periods [p. 252] always corresponded with times of mental and physical depression, and the pain was evidently neuromimetic or hysterical.
The affection which has come down to us from ancient times under the name of clavus hystericus is an acute boring pain confined to a small point at the top of the head, and is sometimes described as resembling the pain which would be produced by driving a nail into the head; hence the term, from clavus, a nail. It may last for hours, days, or even weeks. Instead of clavus hystericus, hemicrania, occipital headache, or nape-aches may be present. On the whole, aches and pains of the head in hysterical cases are more likely to be localized to some point or area than to be general. Hysterical patients, however, not infrequently complain of constricting, contracting, or compressing sensations in the head.
In hysterical women the pulse is apt to be rapid, even sometimes twenty, thirty, to fifty pulsations to the minute above normal. The heart in these patients is irritable and prone to beat rapidly. One of Mitchell's cases is worthy of brief detail: A neurasthenic, hysterical woman, thirty-eight years old, when lying down had a heart-beat never less than 130 per minute. Exertion added twenty or thirty pulsations. Despite this irritability, however, the rhythm was good. Ovarian pressure and pressure along the spine would suddenly increase the heart-beats. Her temperature ranged from 95° in the morning to 100° or 101.5° F. in the evening, although she had no pulmonary or visceral trouble.
The high temperatures which have been observed in many cases of hysteria have been due to some form of shrewd fraud; but Briand91 maintains with Gubler, Rigel, Dieulafoy, and others that the term hysterical fever is correct, and he describes three forms of the fever: (1) The slow continued fever of Briquet, characterized sometimes by simple acceleration of the pulse, without elevation of temperature; sometimes by a temperature rise, either with or without phenomena or accompanied by headache, thirst, and other symptoms; (2) a shorter form, always the result of a more or less active disturbance of the nervous system by terror, fear, chagrin, and like causes; (3) a form with intermittent febrile phenomena. Examples of the different forms are given. Debove92 supports the view of the entity of the hysterical fever, citing cases—one a woman twenty-four years old who had, at intervals, marked fever, the temperature sometimes reaching 1021/5° to 104° F. Malaria and tuberculosis were excluded. Sulphate of quinia had no influence upon her attacks, but antipyrine reduced the temperature and her general condition improved. Debove has observed the temperature to rise from 1° to 2° F. by mere suggestion when the patient was in a somnambulistic state.
91 Gazette hébdomadaire, quoted in Med. News, Dec. 1, 1883.
92 Ibid., quoted in Med. News, April 4, 1885.
On the other hand, it has been claimed that a true hysterical fever never occurs or is extremely rare. Admitting this view, several explanations may be given of the rise of temperature observed. It may be due to intercurrent affections, as typhoid or intermittent fever, or some local inflammatory disorder. It may be secondary fever, the result of muscular effort or some similar cause. Lastly, and most probably, it may be due to ingenious fraud, as to friction of the bulb, pressure, or tapping [p. 253] with the finger, dipping the instrument into hot water, connivance with the nurse, etc. Du Castel93 has reported a trick of this kind. An hysterical girl, convalescent from an attack of sore throat, displayed remarkable alternations of temperature. One day the thermometer reached 163.4° F.! By carefully watching the patient it was found she had learned the trick of lightly tapping the end of the thermometer, which caused the mercury to ascend as far as she wished. In the case of chronic hysterical insanity of which the details have been given the temperature in the axilla on several occasions reached 102°, 103°, and even 105° F.
93 Revue de Thérapeutique méd.-chir., No. xi., 1884.
Extreme states of pallor or blushing, sometimes in the extremities and at others in the face, are mentioned by Mitchell as among the vaso-motor disturbances of hysteria. Rosenthal gives a most interesting observation with reference to vaso-motor conditions in hysteria: the patient, a girl twenty-three years old, had epileptiform attacks, which were preceded by a subjective sensation of cold and discoloration of the hands and tips of the fingers. The hands became very pale, the tips of the fingers and nails of a deep blue; the patient experienced a disagreeable sensation of cold in the hands, and their temperature sank more than 3°, while the pulse dropped from 72 to 65 or 66. After the attack the temperature rose 2° higher than the normal condition; the fingers and nails became very red, and were the seat of an abundant perspiration; the pulse increased to 84 or 88. Other interesting symptoms were present.
Mitchell94 has put on record three cases of hysteria in which was present unilateral increase in bulk at or near the menstrual period, and also at other seasons after emotional excitement. He does not give any opinion as to its nature, but believes that it is not a mere increase of areolar serum, and that it does not appear to resemble the vasal paralysis in which the leg throbs and exhibits a rise in temperature and tint. He is unable also to identify it with any form of lymph œdema which it resembles, for in this disorder there is more obvious œdema, and it is also quite permanent. Whatever the cause of the swelling, he believes that it is under the influence of the nervous system, and that it varies with the causes which produce analgesia or spasm. I have seen swelling of this kind in several cases, and have probably overlooked it in others. In one of my reported cases of hystero-epilepsy it was a very marked symptom, coming and going, increasing and diminishing, with other symptoms.
94 American Journal of the Medical Sciences, New Series, vol. lxxxviii., July, 1884, p. 94.
Buzzard calls attention to the fact that in many cases belonging to the class of hysteria the epidermis, which has arrived at extraordinary thickness, apparently from disuse of the limbs, offers great resistance to the passage of electric currents. Under these circumstances a more than usual amount of care in thoroughly soaking and rubbing the skin, as well as in selecting the motor points, is necessary to avoid fallacies. Absence of reflex from the sole of the foot, according to the same authority, is a very constant symptom in hysterical paraplegia.
Some wasting does not negative the idea of hysteria, but this wasting a not associated with changing the electrical reaction.
Disturbance of the secretion of the urine is among the most frequent of the minor hysterical troubles, and has often been noted by writers upon [p. 254] this subject since a very early date. Sydenham95 says that of the “symptoms accompanying this disease, the most peculiar and general one is the making great quantities of urine as clear as rock-water, which upon diligent inquiry I find to be the distinguishing sign of those disorders which we call hypochondriac in men and hysteric in women. And I have sometimes observed in men that soon after having made urine of an amber color, being suddenly seized with some disturbance of mind, they made a large quantity of clear water, with a continued violent stream, and remained indisposed till the urine came to its former color, when the fit went off.” This symptom shows itself as strikingly in the hysteria of the present day as in the age of Sydenham.
95 Op. cit.
A complete anuria or ischuria is one of the older observations in hysteria. Laycock, Charcot, and many others have written at length on this subject. Finch96 has published a curious case of complete anuria. The patient had various hysterical symptoms, including paroxysms with unconsciousness, contracture, also vomiting. Micturition and defecation were entirely suspended (?) from Dec. 24, 1877, to Feb. 22d of the following year. During a period of fifty-eight days paroxysms were frequent; but on using the catheter the bladder was always found empty. The probability of hysterical fraud is very great in this case. A few case of hysterical retention of the urine in men have been reported.
96 Nice médicale.
Increase of the uterine and vaginal secretions is mentioned by Jolly as sometimes attributable to nervous influences in cases of hysteria. He mentions the case of a woman suffering from hysterical symptoms at the change of life whose disposition was decidedly depressed; though at times lively, particularly erotic. In this case simultaneously with tympanites appeared a thin, clear fluor albus. Local treatment with quiet had no decided effect, but it disappeared with the tympanites when the patient was excited by the visit of a sister who overwhelmed her with reproaches.
Hysterical vomiting of food sometimes persists for weeks; strangely enough, the patients usually appear to suffer little in consequence. Chambers believes that the articles swallowed do not all get into the stomach. The phenomena of rejection in these cases are similar to those of an œsophageal stricture; some of the matter swallowed is really retained, and therefore the patient will not starve as soon as might be supposed.
Two cases of simulated pregnancy by hysterical women have come under my observation. Cases are reported also in which hysteria simulated closely the process of natural labor, as one for instance, by Hodges.97 A woman said to be in the fifth month of pregnancy engaged him to attend her at term. Four months afterward he was sent for, the patient having severe pains, supposing herself to be in labor. On examination, however, a tumor present turned out to be the bladder distended and prolapsed. Sparks98 reports the case of a young married woman who had the symptoms of the third stage of labor, the case being purely hysterical.
97 Lancet, 1859, ii. 619.
98 Chicago Med. Journ. and Examiner, 1880.
Walker99 reports a group of hysterical symptoms closely simulating the prodromes of puerperal eclampsia. The patient, a married woman only [p. 255] eighteen years old, when pregnant six months lifted a tub of water, rupturing the membranes. In the eighth month, after she had remained in bed three days, she began to complain of severe headache; soon she said she was blind; the pupils of the eye were neither dilated nor contracted, and responded sluggishly to light. Ophthalmoscopic examination gave negative results, but she did not flinch from the light of the mirror. Temperature, pulse, and respiration were about normal. The urine contained no albumen. She recovered her sight in twelve hours, and had no continuing trouble.
99 Arch. of Medicine, New York, 1883, x. 85-88.
Paget mentions cases of phantom tumor occurring in the calf, thigh, and breast. These phantoms shift from one place to another, or disappear when the muscles are relaxed by anæsthetics or otherwise. The nervous mimicry of aneurisms (of Paget) are what Laycock and others treat of as pulsations. They are most frequent in the carotid artery and abdominal aorta. Of imitations of cancer it need only be said that the average hysterical female suspects every lump in the breast and elsewhere to be a cancer.
Mitchell mentions certain peculiar symptoms quite common among hysterical women, but which also occur, but more rarely, among men. When falling asleep these patients have something like an aura rising from the feet and going up toward the head. One patient had an aura which passed upward from his feet, and when it had reached his head he felt what he described as an explosion. Another had a sensation as though something was about to happen, but no distinct ascending aura. If he roused himself in time, he could by turning over release himself from the sensation and break the chain of morbid events. At the close of the attack he had a noise in his head—something like the sound of a bell which had been struck once. Other patients when going to sleep have constant sounds, faint usually and rarely loud and without a feeling of terror. Most of the patients were women worn out or tired out and hysterical.
Sometimes hysterical women awake with numbness and tingling, which rapidly passes away or yields to a little surface friction. Some persons who have in a measure recovered from hemiplegia of organic origin are liable to awake out of sleep with a numbness and lessening of power on the side once palsied. Palpitation of the heart, vertigo, and a certain fear of a respiratory character are among the milder forms of trouble which Mitchell mentions as haunting the sleep of nervous or hysterical women.
Under hysteria some of the affections, more common among men than women, known as railway brain, railway spine, etc., may be classified. These disorders might be termed traumatic hysteria. The amount of money that has been paid out by corporations, beneficial societies or individuals because of suits or threatened suits for damages in cases of railway or other accidents is something almost incredible. At least two classes of cases, besides those of recognizable gross lesion, are to be found in the ranks of those claiming such damages. These are first the bogus cases or malingerers, and secondly cases of nervous mimicry. An hysterical individual who has been in a railway collision, or has been the victim of an accident for which somebody else may possibly be made responsible, may deliberately practise fraud, or he may [p. 256] consciously or unconsciously imitate or exaggerate real symptoms of serious import. Sometimes there may be in the same case a mingling of real and of simulated or of neuromimetic disorders. As long as a claim of damages in this class of cases exists, great care should be taken in making a diagnosis. The neuromimetic cases, however, do occur, particularly in the hysterical and neurasthenic, without any reference to litigation.
A lady fell off her chair backward. She was not rendered unconscious, but became nervous, and began to have considerable pain and soreness in the sacral region and about the right sacro-iliac juncture. She had no palsy, nor spasm, nor anæsthesia, nor paræsthesia, and had no difficulty in her bladder, but nevertheless was helpless in bed for many weeks, supposing herself unable to stand. She recovered promptly, under treatment with electricity, as soon as a favorable prognosis was given in a very positive manner.
A man fell on the ice and struck his back, but was able to go on with his usual occupation, although complaining of his limbs. Two months afterward, while recovering from typhoid fever, he fell from a chair, and was unable to raise himself, and found that he had lost control of his legs and arms. During the attack he was not unconscious. He was bed-ridden for two months, but did not lose control of his bladder and bowels. He was put on his feet by a little treatment and much encouragement.
A woman was badly pushed about while riding in a street-car by the car being thrown off the track. She miscarried in about six weeks, flooding a good deal after injury to the time of miscarriage. Later, spinal symptoms began. She had extensive pain and tenderness at the lower end of the spine. She sometimes fainted. Examination revealed general spinal tenderness, much more marked in the sacro-coccygeal region. She was pale, anæmic, and neurasthenic. She brought suit against the railway company for damages, which were very properly awarded, as the miscarriage, hemorrhage, and consequent anæmia were without doubt the result of an accident for which she was in no wise responsible. Some organic spinal-cord disease, however, was supposed to exist, the chief foundation for this view being the extreme spinal tenderness, which was hysterical.
Finally, some hysterical cases present a succession of local hysterical phenomena following each other more or less rapidly. One symptom seems to take possession of the patient for the time being, but when relieved or cured of this, suddenly a new manifestation occurs. A new figure appears upon the scene, or perhaps I might better say a new actor treads the boards. Even in these cases, however, it would be difficult to say that the phenomena are really simulated. They are rather induced, and get partly beyond the patient's will.
A remarkable case of this kind is well known at the Philadelphia Polyclinic and College for Graduates in Medicine. She is sometimes facetiously spoken of as the “Polyclinic Case,” because she has done duty at almost every clinical service connected with the institution. The case has been reported several times: the fullest report is that given by Harlan.100 The patient was taken sick in September with sore throat, and was confined to the house for about two weeks. She was attended by S. Solis [p. 257] Cohen. There was difficulty in swallowing, and some regurgitation of food. At the same time she had weakness of sight in the right eye. Later, huskiness of voice came on, and soon complete aphonia. Her voice recovered, and she then had what appeared to be pleuro-pneumonia. During the attack her arms became partially paralyzed. She complained of numbness down her legs and in her feet.
100 Transactions of the Amer. Ophthalmological Soc., 20th annual meeting, 1884, 649.
Before these symptoms had disappeared twitchings of the muscles of the face set in, most marked on the right side. The face improved, but in two days she had complete spasmodic torticollis of the left side. One pole of a magnet was placed in front of the ear, and the other along the face; and under this treatment in a week the spasm ceased entirely.
In a short time she complained of various troubles of vision and a fixed dilatation of the pupil. Homonymous diplopia appeared. Reading power of the right eye was soon lost. The pupil was slightly dilated, and reacted imperfectly to light. She had distressing blepharospasm on the right side and slight twitchings on the left. Two months later a central scotoma appeared, and eventually her right eye became entirely blind except to light. The pupil was widely dilated and fixed, and the spasm became more violent and extended to the face and neck. The sight was tested by Harlan by placing a weak convex lens in front of the blind eye, and one too strong to read through in front of the sound eye, when it was found that she read without any difficulty. The use of the magnet was continued by Cohen. Blepharospasm and dilatation of the pupil improved. She, however, had an attack of conjunctivitis in the left eye, and again got worse in all her eye symptoms. A perfect imitation of the magnet was made of wood with iron tips. Under this imitation magnet the pupil recovered its size and twitching of the face and eyelids ceased.
The next campaign was precipitated by a fall. She claimed that she had dislocated her elbow-joint; she was treated for dislocation by a physician, and discharged with an arm stiff at the elbow. A wooden magnet was applied to the arm, the spasm relaxed, and the dislocation disappeared.
This ends Harlan's report of the case, and I had thought that this patient's Iliad of woes was also ended; but I have just been informed by J. Solis Cohen and his brother that she has again come under their care. The latter was sent for, and found the patient seemingly choking to death. The right chest was fixed; there was marked dyspnœa; respiration 76 per minute; her expectoration was profuse; she had hyperresonance of the apex, and loud mucous râles were heard. At last accounts she was again recovering.
This patient's train of symptoms began with what appeared to be diphtheria. The fact that she had some real regurgitation would seem to be strong evidence that she had some form of throat paralysis following diphtheria. She was of neurotic temperament. From the age of seven until ten years she had had fits of some kind about every four weeks. Because of her sore throat and subsequent real or seeming paralytic condition she came to the Polyclinic, where she was an object of interest and considerable attention, having been talked about and lectured upon to the classes in attendance. Whether her first symptoms were or were not hysterical, those which succeeded were demonstrably of this character. [p. 258] Frequently some real disease is the starting-point of a train of hysterical disorders.
DURATION AND COURSE.—Hysteria is pre-eminently a chronic disease; in the majority of cases it lasts at least for years. Its symptoms may be prolonged in various ways. Sometimes one grave hysterical disorder, as hysterical paralysis, persists for years. In other cases one set of symptoms will be supplanted by others, and these by still others, and so on until the whole round of hysterical phenomena appears in succession.
Deceptive remissions in hysterical symptoms often mislead the unwary practitioner. Cures are sometimes claimed where simply a change in the character of the phenomena has taken place. Without doubt, some cases of hysteria are curable; equally, without doubt, many cases are not permanently cured. It is a disease in which it is unsafe to claim a conquest too soon. In uncomplicated cases of hysteria the disorder often abates slowly but surely as age advances. As a rule, the longevity of hysterical patients is not much affected by the disorder.
COMPLICATIONS.—We should not treat a nervous case occurring in a woman or a man as hysterical simply because it is obscure and mysterious. Unless, after the most careful examination, we are able by exclusion or by the presence of certain positive symptoms to arrive at the diagnosis of hysteria, it is far better to withhold an opinion or to continue probing for organic disease. I can recall five cases in which the diagnosis of hysteria was made, and in which death resulted in a short time. One of these was a case of uræmia with convulsions, two were cases of acute mania, another proved to be a brain abscess, and the fifth a brain tumor. Hughes Bennett101 has reported a case of cerebral tumor with symptoms simulating hysteria in which the diagnosis of the true nature of the disease was not made out during life. The patient was a young lady of sixteen at the time of her death. Her family history was decidedly neurotic. She was precocious both mentally and physically, was mischievous and destructive, sentimental and romantic; she had abnormal sexual passions. She had a sudden attack of total blindness, with equally sudden recovery of sight some ten days afterward. Sudden loss of sight occurred a second time, and deafness with restoration of hearing, loss of power in her lower limbs, and total blindness, deafness, and paraplegia. Severe constant headaches were absent, as were also ptosis, diplopia, facial or lingual paralysis, convulsions with unconsciousness, vomiting, wasting, and abnormal ophthalmoscopic appearances. She had attacks of laughing, crying, and throwing herself about. Her appearance and character were eminently suggestive of hysteria. The patient died, and on post-mortem examination a tumor about the size and shape of a hen's egg was found in the medullary substance of the middle lobe of the right hemisphere.
101 Brain, April, 1878.
The association of hysteria with real and very severe spinal traumatism partially misled me in the case of a middle-aged man who had been injured in a runaway accident, and who sustained a fracture of one of the upper dorsal vertebræ, probably of the spines or posterior arch. This was followed by paralysis, atrophy of the muscles, contractures, changed reactions, bladder symptoms, bed-sores, and anæsthesia. The upper extremities were also affected. Marked mental changes were present, [p. 259] the man being almost insanely hysterical. The diagnosis was fracture, followed by compression myelitis, with descending motor and ascending sensory degeneration. An unfavorable prognosis was given. He left the hospital and went to another, and finally went home, where he was treated with a faradic battery. He gradually improved, and is now on his feet, although not well. In this case there was organic disease and also much hysteria.
Seguin102 holds that (1) many hysterical symptoms may occur in diseases of the spinal cord and brain; (2) in diseases of the spinal cord these diseases appear merely as a matter of coincidence; (3) in cases of cerebral disease the hysterical symptoms have a deeper significance, being in relation to the hemisphere injured. He collects, as illustrative of the propositions that hysterical symptoms will present themselves in persons suffering from organic disease of the nervous system, the following cases of organic spinal disease: One case of left hemiplegia with paresis of the right limbs, which proved after death to be extensive central myelitis, with formation of cavities in the cord; two cases of posterior spinal sclerosis, two of disseminated sclerosis, and one of sclerosis of the lateral column. In some of these cases the organic disease was wholly overlooked. Sixteen cases of organic disease of the brain accompanied by marked hysterical manifestations are also given: 9 of left hemiplegia; 2 of right hemiplegia with aphasia; 1 of left alternating with right hemiplegia; 1 of hemichorea with paresis; 1 of double hemiplegia; and 2 of general paresis. It is remarkable and of interest, in connection with other unilateral phenomena of hysteria, that emotional symptoms were present in 14 cases of left hemiplegia and in only 2 of right.
102 Op. cit.
Among the important conclusions of this paper are the following: “1. In typical hysteria the emotional symptoms are the most prominent, and according to many authors the most characteristic. In all the cases of cerebral disease related there were undue emotional manifestations or emotional movements not duly controlled. 2. In typical hysteria many of the objective phenomena are almost always shown on the left side of the body, and we may consequently feel sure that in these cases the right hemisphere is disordered. In nearly all of the above sixteen cases the right hemisphere was the seat of organic disease, and the symptoms were on the left side of the body.”
The possibility of the occurrence of hysteria in the course of acute diseases, particularly fevers, is often overlooked. Its occurrence sometimes misleads the doctor with reference to prognosis. Such manifestations are particularly apt to occur in emotional children. A young girl suffering from a moderately severe attack of follicular tonsillitis, with high fever, suddenly awoke during the night and passed into an hysterical convulsion which greatly alarmed her parents. Her fingers, hands, and arms twitched and worked convulsively. She had fits of laughing and shouting, and was for a short time in a state of ecstasy or trance. Once before this she had had a similar but slighter seizure, during the course of an ephemeral fever.
Among other complications of hysteria which have been noted by different observers are apoplexy, disease of the spleen, mania-a-potu, heart [p. 260] disease, and spinal caries, and among affections alluded to by competent observers as simulated by hysteria are secondary syphilis, phthisis, tetanus, strychnia-poisoning, peritonitis, angina pectoris, and cardiac dyspnœa.
DIAGNOSIS.—Buzzard103 significantly remarks that you cannot cure a case of hysteria as long as you have any serious doubt about its nature; and, on the other hand, if you are able to be quite sure on this point, and are prepared to act with sufficient energy, there are few cases that will not yield to treatment. The importance of a correct diagnosis is a trite topic, but in no affection is it of more consequence than in hysteria, that disorder which, although itself curable, may, as has been abundantly shown, imitate the most incurable and fatal of diseases.
103 Clinical Lectures on Diseases of the Nervous System, by Thomas Buzzard, M.D., Philada., 1882.
A few remarks with reference to the methods of examining hysterical patients will be here in place. Success on the part of the physician will often depend upon his quickness of perception and ability to seize passing symptoms. It is often extremely difficult to determine whether hysterical patients are or are not shamming or how far they are shamming. The shrewdness and watchfulness which such patients sometimes exercise in resisting the physician's attempts to arrive at a diagnosis should be borne in mind. A consistent method of procedure, one which never betrays any lack of confidence, should be adopted. “Trifles light as air” will sometimes decide, a single expression or a trivial sign clinching the diagnosis. On the other hand, the most elaborate and painstaking investigation will be frequently required.
The physician should carefully guard against making a diagnosis according to preconceived views. On the whole, the general practitioner is more likely to err on the side of diagnosticating organic disease where it does not exist; the specialist in too quickly assigning hysteria where organic disease is present, or in failing to determine the association of hysteria and organic disease in the same case.
Special expedients may sometimes be resorted to in the course of an examination. Not a few hysterical symptoms require for their continuance that the patient's mind shall be centred on the manifestations. If, therefore, the attention can, without arousing suspicions, be directed to something else during the examination, the disappearance of the particular hysterical symptom may clear away all obscurity. In a case reported by Seguin,104 in which staggering was a prominent symptom, the patient was placed in the middle of the room and directed to look at the ceiling to see if he could make out certain fine marks; he stood perfectly well without any unsteadiness. In the case of a boy eleven years old whose chief symptoms were hysterical paralysis with contracture of the lower extremities, great hyperæsthesia of the feet, and a tremor involving both the upper and lower extremities, and sometimes the head, I directed him, as if to bring out some point, to hold one arm above his head and at the same time fix his attention on the foot of the opposite side. The tremor in the upper extremities, which had been most marked, entirely disappeared. This experiment was varied, the result being the same.
104 Op. cit.
The method adopted in the cases supposed to be phthisis, but which proved to be hysterical, which has already been alluded to under the [p. 261] head of hysterical or nervous breathing, is worthy of note. The patients, it will be recalled, could not be induced to draw a long breath until the plan was adopted of having them count twenty without stopping, when the lungs expanded and the diagnosis was clear.
It is important to know whether or not children are of this hysterical tendency or are likely, sooner or later in life, to develop some forms of this disorder. In children as well as in adults the hysterical diathesis will be indicated by that peculiar mobility of the nervous system, which has been referred to under Etiology. It is chiefly by psychical manifestations that the determination will be made. These are often of mild degree and of irregular appearance. Undue emotionality under slight exciting cause, a tendency to simulation and to exaggeration of real conditions, inconsistency in likes and dislikes, and great sensibility to passing impressions, are among these indications. Children of hysterical diathesis are sometimes, although by no means always, precocious mentally, but not a few cases of apparent precocity are rather examples of an effort to attract attention, which is always present in individuals of this temperament.
It is also important, as urged by Allbutt,105 to make a distinction between hysterical patients and neurotic subjects, often incorrectly classed as hysterical. Many cases of genuine malady and suffering are contemptuously thrown aside as hysteric. Allbutt regards some of these neurotic patients as almost the best people in this wicked world. Although, however, this author's righteous wrath against the too frequent diagnosis of hysteria, hysterical pain, hysterical spine, etc. is entirely justifiable, he errs a little on the other side.
105 On Visceral Neuroses, being the Gulstonian Lectures on Neuralgia of the Stomach and Allied Disorders, delivered at Royal College of Physicians, March, 1884, by T. Clifford Allbutt, M.A., M.D. Cantab., F. R. S., Philada., 1884.
Hysteria and neurasthenia are often confounded, and, while both conditions may exist in the same case, just as certainly one may be present without the other. The points of differential diagnosis as given by Beard106 are sufficient for practical purposes. They are the following: In neurasthenia convulsions or paroxysms are absent; in hysteria they are among the most common features. In neurasthenia globus hystericus and anæsthesia of the epiglottis are absent, ovarian tenderness is not common, and attacks of anæsthesia are not frequent and have little permanency; in hysteria globus hystericus, anæsthesia of the epiglottis, ovarian tenderness, and attacks of general or local anæsthesia are all marked phenomena. The symptoms of neurasthenia are moderate, quiet, subdued, passive; those of hysteria are acute, intense, violent, positive. Neurasthenia may occur in well-balanced intellectual organizations; hysteria is usually associated with great emotional activity and unbalanced mental organization. Neurasthenia is common in males, although more common in females; hysteria is rare in males. Neurasthenia is always associated with physical debility; hysteria in the mental or psychical form occurs in those who are in perfect physical health. Neurasthenia never recovers suddenly, but always gradually and under the combined influences of hygiene and objective treatment; hysteria may recover suddenly and under purely emotional treatment.
106 Op. cit.[p. 262]
An affection termed general nervousness has been described by Mitchell. It does not seem to be strictly a neurasthenia, nor does it always occur in hysterical individuals. These cases are sometimes “more or less neurasthenic people, easily tired in brain or body; but others are merely tremulous, nervous folks, easily agitated, over-sensitive, emotional, and timid.” It is sometimes an inheritance; sometimes it results from the misuse of alcohol, tobacco, tea or coffee. Usually, it is developed slowly; occasionally, however, it arises in a moment. Thus, Mitchell mentions the case of a healthy girl who fell suddenly into a state of general nervousness owing to the fall of a house-wall. General nervousness is to be distinguished from hysteria, into which it sometimes merges, only by the absence of the mental perversions and the special motor, sensory, vaso-motor, and visceral disorders peculiar to the latter.
The differential diagnosis of hysteria and hypochondria, or what is better termed hypochondriacal melancholia, is often, apparently at least, somewhat difficult. Formerly, it was somewhat the fashion to regard hysteria in the male as hypochondria; but this view has nothing to support it. Hypochondria and hysteria, as neurasthenia and hysteria, are sometimes united in the same subject; one sometimes begets the other, but they have certain points of distinction. Hypochondria more frequently passes into real organic disease than does hysteria; it is more frequently associated with organic disease than is hysteria. Hypochondria is in the majority of cases a true insanity, while hysteria can only be regarded as such in the special instances which have been discussed. In hypochondria the individual's thoughts are centred upon some supposed disease until a true delusional condition is developed; this does not often occur in hysteria. Hypochondria is seen with as great a frequency in the male as in the female, while hysteria prevails much more largely in the female sex. In typical hypochondria more readily than in hysteria the patient may be led from one set of symptoms to another, the particulars of which he will detail in obedience to questions that are put to him, these symptoms not unusually partaking of the absurd and impossible. In hypochondria are absent those distinctive symptoms which in nearly all cases of hysteria appear in greater or less number, such as convulsions, paralysis, contracture, aphonia, hysterical joints, and the like. In hypochondria is present the groundless fear of disease without these outward manifestations of disease. The symptoms of hypochondria, as a rule, but not invariably, are less likely to change or abate than those of hysteria.
It is often of moment to be able to distinguish between two such well-marked affections as common acute mania and hysterical mania. In acute mania the disorder usually comes on gradually; in hysterical mania the outbreak of excitement is generally sudden, although prodromic manifestations are sometimes present. This point of difference is not one to be absolutely depended upon. In acute mania incoherence and delusions or delusional states are genuine phenomena; in hysterical mania delusional conditions, often of an hallucinatory character, may be present, but they are likely to be of a peculiar character. Frequently, for instance, such patients see, or say that they see, rats, toads, spiders, and strange beasts. These delusions have the appearance of being affected in many cases; very often they are fantastical, and sometimes at least they are spurious or simulated. In hysterical mania such [p. 263] phenomena as obstinate mutism, aphonia, pseudo-coma, ecstasy, catalepsy, and trance often occur, but they are usually absent in the history of cases of acute mania. In acute mania under the influence of excitement or delusion the patients may take their own lives: they may starve or kill themselves violently; in hysterical mania suicide will be threatened or apparently attempted, but the attempts are not genuine as a rule; they are rather acts of deception. In acute mania the patients often become much reduced and emaciated; in hysterical mania in general, considering the amount of mental and motor excitement through which the individuals pass, their nutrition remains good. In acute mania sleeplessness is common, persistent, and depressing; in hysterical mania usually a fair amount of sleep will be obtained in twenty-four hours. In many cases of hysterical mania the patients have their worst attacks early in the morning after a good night's rest. Acute mania under judicious treatment and management may gradually recover; sometimes, however, it ends fatally: this is especially likely to occur if the physician supposes the case to be simply hysterical and acts accordingly. Hysterical mania seldom has a serious termination unless through accident or complication.
In order to make the diagnosis of purposive hysterical attacks watchfulness on the part of the physician will often suffice. Such patients can frequently be detected slyly watching the physician or others. Threats or the actual use of harsh measures will sometimes serve for diagnostic ends, although the greatest care should be exercised in using such methods in order that injustice be not done.
In uræmia, as in true epilepsy, the convulsion is marked and the condition of unconsciousness is usually profound. An examination of the urine for albumen, and the presence of symptoms, such as dropsical effusion, which point to disorder of the kidneys, will also assist.
Hysterical paralysis in the form of monoplegia or hemiplegia must sometimes be distinguished from such organic conditions as cerebral hemorrhage, embolism or thrombosis, tumor, abscess, or meningitis (cerebral syphilis).
When the question is between hysteria and paralysis from coarse brain disease, as hemorrhage, embolism, etc., the history is of great importance. The hysterical case usually has had previous special hysterical manifestations. The palsy may be the last of several attacks, the patient having entirely recovered from other attacks. In an organic case, if previously attacked, the patient has usually made an incomplete recovery; the history is of a succession of attacks, each of which leaves the patient worse. In cerebral syphilis it happens sometimes that coming and going paralyses occur; but the improvement in these cases is generally directly traceable to specific treatment. Partial recoveries take place in embolism, thrombosis, hemorrhage, etc. when the lesion has been of a limited character, but the improvement is scarcely ever sufficient to enable the patient to be classed as recovered. The exciting cause of hysterical and organic cases of paralysis is different. While in hysterical paralysis sudden fright, anxiety, anger, or great emotion is frequently the exciting cause, such psychical cause is most commonly not to be traced as the factor immediately concerned in the production of the organic paralysis. In the organic paralysis an apoplectic or apoplectiform attack of a peculiar kind has usually occurred. In cerebral hemorrhage or embolism the [p. 264] patient suddenly loses consciousness, and certain peculiar pulse, temperature, and respiration phenomena occur. The patient usually remains in a state of complete unconsciousness for a greater or less period. In hysteria the conditions are different. A state of pseudo-coma may sometimes be present, but the temperature, pulse, and respiration will not be affected as in the organic case.
Hysterical monoplegia or hemiplegia, as a rule, is not as complete as that of organic origin, and is nearly always accompanied by some loss of sensation. The face usually escapes entirely. In organic palsy the face is generally less severely and less permanently affected than the limbs, but paresis is commonly present in some degree. Hysterical palsies are more likely to occur upon the left than upon the right side. Embolism is well known to occur most frequently in the left middle cerebral artery, thus giving the palsies upon the right. In hemorrhage and thrombosis the tendency is perhaps almost equal for the two sides. Some of these and other points of distinction between organic and hysterical palsies have been given incidentally under Symptomatology.
In organic hemiplegia aphasia is more likely to occur than in hysterical cases; and acute bed-sores and wasting of the limbs, with contractures, are conditions frequently present as distressing sequelæ. Such is not the rule in hysterical cases, for while there may be wasting of the limbs from disuse and hysterical contractures, bed-sores are seldom present, and the wasting and contractures do not appear so insidiously, nor progressively advance to painful permanent conditions, as in the organic cases. Mitchell mentions the fact that in palsies from nerve wounds feeling is apt to come back first, motion last; while in the hysterical the gain in the power of motion may go on to full recovery, while the sense of feeling remains as it was at the beginning of treatment. This point of course would help only in cases where both sensory and motor loss are present.
The examination of an hysterically palsied limb, if conducted with care, may often bring out the suppressed power of the patient. Practising the duplicated, active Swedish movements on such a limb will sometimes coax resistance from the patient. As already stated, electro-contractility is retained in hysterical cases.
The disorders from which it may be necessary to diagnosticate hysterical paraplegia are spinal congestion, subacute generalized myelitis of the anterior horns (chronic atrophic spinal paralysis of Duchenne), diffused myelitis, acute ascending paralysis, spinal hemorrhage, spinal tumor, posterior spinal sclerosis or locomotor ataxy, lateral sclerosis or spasmodic tabes, multiple cerebro-spinal sclerosis, and spinal caries.
In spinal congestion the patients come with a history that after exposure they have lost the use of their lower limbs, and sometimes of the upper. Heaviness and pain in the back are complained of, and also more or less pain from lying on the back. Numbness in the legs and other disturbances of sensation are also present. The paralysis may be almost altogether complete. Such patients exhibit evidences of the involvement of the whole cord, but not a complete destructive involvement. A colored woman, age unknown, had been in her ordinary health until Nov. 24, 1884. At this time, while washing, she noticed swelling of the feet, which soon became painful, and finally associated with loss of power. She had also a girdling sensation about the abdomen and pain in the back. She was [p. 265] admitted to the hospital one week later, at which time there was retention of the urine and feces. She had some soreness and tenderness of the epigastrium. She complained of dyspnœa, which was apparently independent of any pulmonary trouble. It was necessary to use the catheter for one week, by which time control of the bladder had been regained. The bowels were regulated by purgatives. She was given large doses of ergot and bromide and iodide of potassium, and slowly improved, and after a time was able to get out of bed and walk with the aid of a chair. An examination at the time showed that the girdling pain had disappeared. There was distinct loss of sensation. Testing the farado-contractility, it was found that in the right leg the flexors only responded to the slowly-interrupted current, while in the left both flexors and extensors responded to the interrupted current. In both limbs with the galvanic current the flexors responded to twenty cells, while the extensors responded to fifty cells. She gradually improved, and was able to leave after having been in the hospital three months.
The diagnosis of subacute myelitis of the anterior horns from hysterical paraplegia is often of vital importance. “A young woman,” says Bennett,107 “suddenly or gradually becomes paralyzed in the lower extremities. This may in a few days, weeks, or months become complete or may remain partial. There is no loss of sensation, no muscular rigidity, no cerebral disturbances, nor any general affection of the bladder or rectum. The patient's general health may be robust or it may be delicate. She may be of emotional and hysterical temperament, or, on the contrary, of a calm and well-balanced disposition. At first there is no muscular wasting, but as the disease becomes chronic the limbs may or may not diminish in size. The entire extremity may be affected or only certain groups of muscles. Finally, the disease may partially or entirely recover, or remain almost unchanged for years.” This is a fair general picture of either disease.
107 Lancet, vol. ii. p. 842, November, 1882.
Two facts are often overlooked in this connection: first, that poliomyelitis is just as liable to occur in the hysterical as in the other class; and, secondly, that the symptoms of hysterical paraplegia and poliomyelitis may go hand in hand.
The history is different in the two affections. Frequent attacks of paralysis in connection with hysterical symptoms are very suggestive, although not always positive. In poliomyelitis the disease may come on with diarrhœa and fever; often it comes on with vomiting and pain. The patellar reflex is retained, often exaggerated, and rarely lost, in hysteria, while it is usually lost in poliomyelitis. Electro-muscular contractility is often normal in hysterical paralysis, although it is sometimes slightly diminished quantitatively to both faradism and galvanism: the various muscles of one limb respond about equally to electricity: there are no reactions of degeneration in hysterical paralysis as in poliomyelitis. In poliomyelitis reactions of degeneration are one of the most striking features. The cutaneous plantar reflex is impaired in hysterical paraplegia; bed-sores are usually absent, as are also acute trophic eschars and the nail-markings present both in generalized subacute myelitis and diffused myelitis. True muscular atrophy is also wanting in hysterical paraplegia, although the limbs may be lean and wasted from the original [p. 266] thinness of the patient or from disuse. The temperature of the limbs is usually good. There is no blueness nor redness of the limbs, nor are the bowels or bladder uncomfortably affected.
Buzzard108 gives two diagrams (Figs. 16 and 17), which I have reproduced. They are drawn from photographs. They show two pairs of feet, which have a certain superficial resemblance. In each the inner border is drawn up into the position of a not severe varus. They are the feet of two young women who were in the hospital at the same time. A (Fig. 16), really a case of acute myelitis, had been treated as a case of hysteria; and B (Fig. 17), really a case of hysteria, came in as a paralytic. In these cases the results of examination into the state of the electrical response and of the patellar-tendon reflex was sufficient to make a diagnosis clear. In the organic case the electrical reactions were abnormal and the patellar-tendon reflex was abolished. These conditions were not present in the hysterical case.
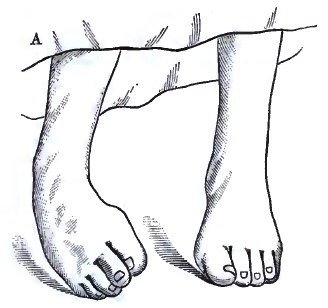
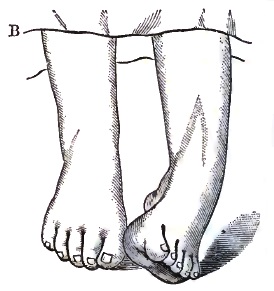
108 Clin. Lectures on Diseases of the Nervous System, London, 1882.
The diagnosis of hysterical paraplegia from diffused myelitis is governed practically by the same rules which serve in subacute myelitis of the anterior horns, with some additional points. In diffused myelitis, in addition to the motor, trophic, vaso-motor, electrical, and reflex disorders of myelitis of the anterior horns, affections of sensibility from involvement of the sensory regions of the cord will also be present. Anæsthesia and paræsthesia will be present.
Acute ascending paralysis, the so-called Landry's paralysis, particularly when it runs a variable course, might be mistaken sometimes for hysterical paralysis. In one instance I saw a fatal case of Landry's paralysis which had been supposed to be hysterical until a few hours before death. In Landry's paralysis, however, the swiftly ascending character of the disorder is usually so well marked as to lead easily to the diagnosis. In Landry's paralysis the loss of power begins first in the legs, but soon becomes more pronounced, and passes to the arms, and in the worst cases swallowing and respiration become affected.
Spinal hemorrhage and spinal tumors, giving rise to paralysis, may be mistaken for hysterical paralysis, partly because of the contractures. Reactions of degenerations are usually features of this form of organic paralysis. The contractures of hysterical paralysis can be promptly [p. 267] relieved by deep, strong pressure along supplying nerve-trunks; this cannot be accomplished in the organic cases. Severe localized pains in the limbs, sometimes radiating from the spinal column, are present in the organic cases. Pain may be complained of by the hysterical patient, but close examination will show that it is not of the same character, either as regards severity or duration.
Hysterical locomotor ataxy is usually readily distinguished from posterior spinal sclerosis, although the phenomena are apparently more marked and more peculiar than those exhibited as the result of organic changes. Hysterical ataxic patients often show an extraordinary inability to balance their movements, this want of co-ordinating power being observed even in the neck and trunk, as well as the limbs. In hysterical cases a certain amount of palsy, often of an irregular type, is more likely to be associated with the ataxia than in the structural cases. The knee-jerk, so commonly absent in true posterior spinal sclerosis that its absence has come to be regarded as almost a pathognomonic symptom of this affection, in hysterical motor ataxy is present and exaggerated. In hysterical locomotor ataxy other well-marked symptoms of general hysteria, such as hysterical convulsions, aphonia, etc., are present.
In the diagnosis of spastic spinal paralysis from hysterical paraplegia great difficulties will sometimes arise. A complete history of the case is of the utmost importance in coming to a conclusion. If the case be hysterical, usually some account of decided hysterical manifestation, such as aphonia, sudden loss and return of sight, hysterical seizures, etc., can be had. Althaus holds that a dynamometer which he has had constructed for measuring the force of the lower extremities will, at least in a certain number of cases, enable us to distinguish between the functional and spinal form of spastic paralysis. In the former, although the patient may be unable to walk, the dynamometer often exhibits a considerable degree of muscular power; while in the latter, more especially where the disease is somewhat advanced, the index of the instrument will only indicate 20° or 30° in place of 140° or 160°, and occasionally will make no excursion at all.
The diagnosis of multiple cerebro-spinal sclerosis from hysteria occasionally offers some difficulties. Jolly goes so far as to say that it can only with certainty be diagnosticated in some cases in its later stages and by the final issue—cases in which the paralytic phenomena frequently alter their position, in which paroxysmal exacerbations and as sudden ameliorations take place, and convulsive attacks and disturbances of consciousness of a like complicated nature as in hysteria are met with. Disorders of deglutition and articulation, also characteristic of multiple cerebro-spinal sclerosis, are now and again observed in the hysterical. Recently, through the kindness of J. Solis Cohen, I saw at the German Hospital in Philadelphia a patient about whom there was for a time some doubt as to whether the peculiar tremor from which he suffered was hysterical or sclerotic. At rest and unobserved, he was usually quiet, but as soon as attention was directed to him the tremor would begin, at first in the limbs, but soon also in the head and trunk. If while under observation he attempted any movement with his hands or feet, the tremor would become violent, and if the effort was persisted in it would become convulsive in character. The effort to take a glass of water threw him into [p. 268] such violent spasms as to cause the water to be splashed in all directions. The fact that this patient was a quiet, phlegmatic man of middle age, that his troubles had come on slowly and had progressively increased, that tremor of the head and trunk was present, that cramps or tonic spasms of the limbs came and went, indicated the existence of disseminated sclerosis. The knee-jerk was much exaggerated, taps upon the patellar tendon causing decided movement; when continued, the leg would be thrown into violent spasm.
Spondylitis, or caries of the vertebræ, is sometimes difficult to distinguish from hysterical paraplegia or hysterical paraplegia from it, or both may be present in the same case. Likewise, painful paraplegia from cancer or sarcoma of the vertebræ may offer some difficulties. A woman aged forty-four when two years old had a fall, which was followed by disease of the spine, and has resulted in the characteristic deformity of Pott's disease. She was apparently well, able to do ordinary work, until about five years before she came under observation, when her legs began to feel heavy and numb, and with this were some pain and slight loss of power. These symptoms increased, and in three months were followed by a total loss of power in the lower extremity. She was admitted to the hospital, and for about three years was unable to move the legs. She went round the wards in a wheeled chair. The diagnosis was made of spondylitis, curvature, and paralysis and sensory disorders depending on compression myelitis, and it was supposed she was beyond the reach of remedies. One day one of the resident physicians gave her a simple digestant or carminative, soon after which she got up and walked, and has been walking ever since. She attributes her cure entirely to this medicine.
What is the lesson to be learned from this case? It is, in the first place, not to consider a patient doomed until you have made a careful examination. There can be much incurvation of the spine without sufficient compression to cause complete paralysis. In this patient organic disease was associated with an hysterical or neuromimetic condition. This woman had disease of the vertebræ, the active symptoms of which had subsided. The vertebral column had assumed a certain shape, and the cord had adjusted itself to this new position, yet for a long time she was considered incurable from the fact that the conjunction of a real and a mimetic disorder was overlooked.
Another patient aged twenty-seven had whooping cough, which lasted six weeks, and was followed by severe pain in the back. For this she consulted various physicians, being treated for Pott's disease and spinal irritation. She, however, continued to grow worse, and every jar and twist gave severe pain. At this time she had lost much flesh, had pain in her back and elsewhere, and was subject to numerous and violent spasms. When first seen by the physician who consulted me she was complaining of pains in her legs, hips, and left shoulder, which she considered rheumatic, and with pain in the abdomen. Examination of the back with the patient on her side showed a slight prominence over the position of the first or second lumbar vertebra. The spot was painful on pressure, and had been so ever since the attack of whooping cough three years before. A tap on the sole of either foot made her complain of severe pain in the back. The same result followed pressure on the head. The [p. 269] patient was unable to stand or walk, but occasionally sat up for a short time, although suffering all the time. There was no muscular rigidity. The limbs and body were quite thin, but, so far as could be detected, she had no loss of motor or sensory power. At times, when the pains were worse, the arms would be flexed involuntarily, and she stated that once the spine was drawn back and a little sideways. The pain in the hips was augmented by pressure. During the application of a plaster bandage she had a sort of fit and fainted, and the application was suspended. She soon recovered consciousness, but refused to allow the completion of the dressing. I diagnosticated the affection as largely hysterical, and a few months later received word that the patient was on her feet and well.
Kemper109 relates the case of a lady who eventually died of sarcoma of the vertebræ, the specimens having been examined by J. H. C. Simes of Philadelphia and myself. She was supposed at first and for some time to be a case of hysteria with spinal irritation. In the case of a distinguished naval officer, who died of malignant vertebral disease after great suffering a short time since, this same mistake was made during the early stages of the disease: his case was pronounced to be one of neurasthenia, hysteria, etc. before its true nature was finally discovered. The absence of muscular rigidity in the back and extremities is the strongest point against vertebral disease in these cases.
109 Journal of Nervous and Mental Diseases, vol. xii., No. 1, January, 1885.
In hysterical hemianæsthesia, ovarian hyperæsthesia, hystero-epileptic seizures, ischuria, and other well-known hysterical symptoms have usually been observed. The anæsthesia in hysterical cases is most commonly on the left side of the body, but it may happen to be so located in an organic case, so that this point is only one of slight value.
Some older observers, as Briquet, who is quoted and criticised by Charcot, believed that hemianæsthesia from encephalic lesions differed from hysterical hemianæsthesia by the fact that in the former case the skin of the face did not participate in the insensibility, or that when it existed it never occupied the same side as the insensibility of the limbs. Recently-reported cases have disproved the accuracy of this supposed diagnostic mark. In his lectures, delivered ten years ago, Charcot observed that up to that period anæsthesia of general sensibility alone appeared to have been observed as a consecutive on an alteration of the cerebral hemispheres, so that obtunding of the special senses would remain as a distinctive characteristic of hysterical hemianæsthesia. He, however, expected that cases of cerebral organic origin would be reported of complete hemianæsthesia, with derangements of the special senses, such as is presented in hysteria. His anticipations have been fulfilled. In the nervous wards of the Philadelphia Hospital is now a typical case of organic hemianæsthesia in which the special senses are partially involved.
Paralysis and contractures, if present, are apt to be accompanied in cases of organic hemianæsthesia, after time has elapsed, by marked nutritive changes, by wasting of muscle, and even of skin and bone. This is not the case in hysteria.
The subsequent history of these two conditions is different. The hysterical patient will often recover and relapse, or under proper [p. 270] treatment may entirely recover; while all the treatment that can be given in a case of organic hemianæsthesia will produce no decided improvement, for there is a lesion in the brain which will remain for ever. Hemianopsia, so far as I know, has not been observed in hysterical hemianæsthesia.
In the monograph of Shaffer, with reference to both true and false knee-joint affections certain conclusions are drawn which I will give somewhat condensed:
Chronic synovitis produces very few if any subjective symptoms; hysterical imitation presents a long train of both subjective and objective symptoms and signs, the former in excess. Chronic ostitis may be diagnosticated if muscular spasm cannot be overcome by persistent effort; when the spasm does not vary night nor day; when it is not affected by the ordinary doses of opium or chloral; when reaction of the muscles to the faradic current is much reduced; when a local and uniform rise of temperature over the affected articulation is present; when purely involuntary neural symptoms, such as muscular spasm, pain, and a cry of distress, are present. Hysterical knee-joint is present, according to this author, when the muscular rigidity or contracture is variable, and can be overcome by mildly persistent efforts while the patient's mind is diverted, or which yields to natural sleep, or which wholly disappears under the usual doses of opium or chloral; when the faradic response is normal; when rise of temperature is absent or a reduced temperature is present over the joint; when variable and inconstant, emotional, and semi-voluntary manifestations are present.
To recognize the neuromimesis of hip disease Shaffer gives the following points: The limp is variable and suggests fatigue; it is much better after rest; it almost invariably follows the pain. Pain of a hyperæsthetic character is usually the first symptom, and it is found most generally in the immediate region of the joint. “In place of an apprehensive state in response to the tests applied will be found a series of symptoms which are erratic and inconstant. A condition of muscular rigidity often exists, but, unlike a true muscular spasm, it can in most cases be overcome in the manner before stated. A very perceptible degree of atrophy may exist—such, however, as would arise from inertia only. A normal electrical contractility exists in all the muscles of the thigh.”
In the neuromimesis of chronic spondylitis or hysterical spine the pain is generally superficial, and is almost always located over or near the spinous processes; it is sometimes transient, and frequently changes its location from time to time; a normal degree of mobility of the spinal column under properly directed manipulation is preserved; the nocturnal cry and apprehensive expression of Pott's disease are wanting.
With reference to the hysterical lateral curvature, Shaffer, quoting Paget, says “ether or chloroform will help. You can straighten the mimic contracture when the muscles cannot act; you cannot so straighten a real curvature.”
In the diagnosis of local hysterical affections one point emphasized by Skey is well worthy of consideration; and that is that local forms of hysteria are often not seen because they are not looked for. “If,” says he, “you will so focus your mental vision and endeavor to distinguish the minute texture of your cases, and look into and not at them, you will [p. 271] acknowledge the truth of the description, and you will adopt a sound principle of treatment that meets disease face to face with a direct instead of an oblique force.” According to Paget, the means for diagnosis in these cases to be sought—(1) in what may be regarded as the predisposition, the general condition of the nervous system, on which, as in a predisposing constitution, the nervous mimicry of disease is founded; (2) in the events by which, as by exciting causes, the mimicry may be evoked and localized; (3) in the local symptoms in each case.
Local symptoms as a means of diagnosis can sometimes be made use of in general hysteria. A case may present symptoms of either the gravest form of organic nervous disease or the gravest form of hysteria, and be for a time in doubt, when suddenly some special local manifestation appears which cannot be other than hysterical, and which clinches the diagnosis. In a case with profound anæsthesia, with paraplegia and marked contractures, with recurring spasms of frightful character, the sudden appearance of aphonia and apsithyria at once cleared all remaining doubt. Herbert Page mentions the case of a man who suffered from marked paraplegia and extreme emotional disturbance after a railway collision, who, nine months after the accident, had an attack of aphonia brought on suddenly by hearing of the death of a friend. He eventually recovered.
To detect hysterical or simulated blindness the methods described by Harlan are those adopted in my own practice. When the blindness is in both eyes, optical tests cannot be applied. Harlan suggests etherization.110 In a case of deception, conscious or unconscious, he says, “as the effect of the anæsthetic passed off the patient would probably recover the power of vision before his consciousness was sufficiently restored to enable him to resume the deception.” Hutchinson cured a case of deaf-dumbness by means of etherization. For simulated monocular blindness Graefe's prism-test may be used: “If a prism held before the eye in which sight is admitted causes double vision, or when its axis is held horizontally a corrective squint, vision with both eyes is rendered certain.” It should be borne in mind that the failure to produce double images is not positive proof of monocular blindness, for it is possible that the person may see with either eye separately, but not enjoy binocular vision, as in a case of squint, however slight. Instead of using a prism while the patient is reading with both eyes at an ordinary distance, say of fourteen or sixteen inches, on some pretext slip a glass of high focus in front of the eye said to be sound. If the reading is continued without change, of course the amaurosis is not real. Other tests have been recommended, but these can usually be made available.
110 Loc. cit.
The diagnosis of hysterical, simulated, or mimetic deafness is more difficult than that of blindness. When the deafness is bilateral, the difficulty is greater than when unilateral. The method by etherization just referred to might be tried. Politzer in his work on diseases of the ear111 makes the following suggestions: Whether the patient can be wakened out of sleep by a moderately loud call seems to be the surest experiment. But, as in total deafness motor reflexes may be elicited by the concussion of loud sounds, [p. 272] care must be taken not to go too near the person concerned and not to call too loudly. The practical objection to this procedure in civil practice would seem to be that we are not often about when our patients are asleep. In unilateral deafness L. Müller's method is to use two tubes, through which words are spoken in both ears at the same time. When unilateral deafness is really present the patient will only repeat what has been spoken in the healthy ear, while when there is simulation he becomes confused, and will repeat the words spoken into the seemingly deaf ear also. To avoid mistakes in using this method, a low voice must be employed.
111 A Textbook of the Diseases of the Ear and Adjacent Organs, by Adam Politzer, translated and edited by James Patterson Cassells, M.D., M. R. C. S. Eng., Philada., 1883.
Mistakes in diagnosis where hysteria is in question are frequently due to that association with it of serious organic disease of the nervous system of which I have already spoken at length under Complications. This is a fact which has not been overlooked by authors and teachers, but one on which sufficient stress has not yet been laid, and one which is not always kept in mind by the practitioner. Bramwell says: “Cases are every now and again met with in which serious organic disease (myelitis and poliomyelitis, anterior, acute, for example) is said to be hysterical. Mistakes of this description are often due to the fact that serious organic disease is frequently associated with the general symptoms and signs of hysteria; it is, in fact, essential to remember that all cases of paraplegia occurring in hysterical patients are not necessarily functional—i.e. hysterical; the presence of hysteria or a history of hysterical fits is only corroborative evidence, and the (positive) diagnosis of hysterical paraplegia should never be given unless the observer has, after the most careful examination, failed to detect the signs and symptoms of organic disease.”
PROGNOSIS.—Hysteria may terminate (1) in permanent recovery; (2) in temporary recovery, with a tendency to relapse or to the establishment of hysterical symptoms of a different character; (3) in some other affection, as insanity, phthisis, or possibly sclerosis; (4) in death, but the death in such cases is usually not the direct result of hysteria, but of some accident. Death from intercurrent disorders may take place in hysteria. It is altogether doubtful, however, whether the affection which has been described as acute fatal hysteria should be placed in the hysterical category. In the cases reported the symptom-picture would in almost every instance seem to indicate the probability of the hysteria having been simply a complication of other disorders, such as epilepsy, eclampsia, and acute mania.
As a rule, hysterical patients will not starve themselves. They may refuse to take food in the presence of others, or may say they will not eat at all; but they will in some cases at the same time get food on the sly or hire their nurses or attendants to procure it for them. In treating such cases a little watchfulness will soon enable the physician to determine what is best to be done. By discovering them in the act of taking food future deception can sometimes be prevented. Hysterical patients do sometimes, however, persistently refuse food. These cases may starve to death if let alone; and it is important that the physician should promptly resort to some form of forcible feeding before the nutrition of the patient has reached too low an ebb. I have seen at least two cases of hysteria or hysterical insanity in which patients were practically allowed to starve themselves to death, but an occurrence of [p. 273] this kind is very rare. Feeding by means of a stomach-tube, or, what is still better, by a nasal tube, as is now so frequently practised among the insane, should be employed. Nourishment should be administered systematically in any way possible until the patient is willing to take food in the ordinary way. In purposive cases some methods of forcible feeding may prove of decided advantage. Its unpleasantness will sometimes cause swallowing power to be regained.
Wunderlich112 has recorded the case of a servant-girl, aged nineteen, who, after a succession of epileptiform fits, fell into a collapse and died in two days. Other cases have been recorded by Meyer. Fagge also speaks of the more chronic forms of hysteria proving fatal by marasmus. He refers to two cases reported by Wilks, both of which were diagnosticated as hysterical, and both of which died. Sir William Gull describes a complaint which he terms anorexia nervosa vel hysterica. It is attended with extreme wasting; pulse, respiration, and temperature are low. The patients were usually between the ages of sixteen and twenty-three: some died; others recovered under full feeding and great care. In many of the reported fatal cases careful inquiry must be made as to this question of hysteria being simply a complication.
112 Quoted in The Principles and Practice of Medicine, by the late Charles Hilton Fagge, M.D., F. R. C. P., etc., vol. i. 1886, p. 736.
Are not hysterical attacks sometimes fatal? With reference to one of my cases this view was urged by the physician in attendance. Gowers113 on this point says: “As a rule to which exceptions are infinitely rare, hysterical attacks, however severe and alarming in aspect, are devoid of danger. The attacks of laryngeal spasm present the greatest apparent risk to life.” He refers to the paroxysms of dyspnœa presented by a hemiplegic girl as really alarming in appearance, even to those familiar with them. He refers also to a case of Raynaud's114 in which the laryngeal and pharyngeal spasm coexisted with trismus, and the patient died in a terrible paroxysm of dyspnœa. The patient presented various other hysterical manifestations, and a precisely similar attack had occurred previously and passed away, but she had in the interval become addicted to the hypodermic injection of morphia, and Raynaud suggested that it might have been the effect of this on the nerve-centres that caused the fatal termination. Such cases have been described in France as the hydrophobic form of hysteria.
113 Epilepsy and Other Chronic Convulsive Diseases, by W. R. Gowers, M.D., London. 1881.
114 L'Union médical, March 15, 1881.
Patients may die in hysterical as in epileptic attacks from causes not directly connected with the disease. One of these sources of danger mentioned by Gowers is the tendency to fall on the face sometimes met with in the post-epileptic state. He records an example of death from this cause. He also details a case of running hysteria or hystero-epilepsy, in which, after a series of fits lasting about four hours, the child died, possibly from some intercurrent accident.
TREATMENT.—Grasset,115 speaking of the treatment of hysteria, says that means of treating the paroxysm, of removing the anæsthesia, of combating single symptoms, are perhaps to be found in abundance, but the groundwork of the disease, the neurosis or morbid state, is not attacked. Here he indicates a new and fruitful path. In his own [p. 274] summing up, however, he can only say that the hysterical diathesis offers fundamental grounds for the exhibition of arsenic, silver, chloride of gold, and mineral waters!
115 Brain, January, 1884.
No doubt can exist that the prophylactic and hygienic treatment of hysteria is of paramount importance. To education—using the term education in a broad sense—before and above all, the most important place must be given. It is sometimes better to remove children from their home surroundings. Hysterical mothers develop hysterical children through association and imitation. I can scarcely, however, agree with Dujardin-Beaumetz that it is always a good plan to place a girl in a boarding-school far from the city. It depends on the school. A well-regulated institution may be a great blessing in this direction; one badly-managed may become a hotbed of hysteria.
Recently I made some investigations into the working of the public-school system of Philadelphia, particularly with reference to the question of overwork and sanitation.116 I had special opportunities during the investigations to study the influences of different methods of education, owing to the fact that the public-school system of Philadelphia is just now in a transition period. This system is in a state of hopeful confusion—hopeful, because I believe that out of its present condition will come eventually a great boon to Philadelphia. At one end of the system, in the primary and the secondary schools, a graded method of instruction has been introduced. The grammar and the high schools are working on an ungraded or differently graded method. I found still prevailing, particularly in certain of the grammar schools for girls, although not to the same extent as a few years since, methods of cramming and stuffing calculated above all to produce hysteria and allied disorders in those predisposed to them.
116 The results of these investigations were given in a lecture which was delivered in the Girls' Normal School of Philadelphia before the Teachers' Institute of Philadelphia, Dec. 11, 1885.
Education should be so arranged as to develop the brain by a natural process—not from within outward; not from the centre to the periphery; not from above downward; but as the nervous system itself develops in its evolution from a lower to a higher order of animals, from the simple to the more complex and more elaborate. Any system of education is wrong, and is calculated to weaken and worry an impressionable nervous system, which attempts to overturn or change this order of the progress of a true development of the brain. To develop the nervous system as it should be developed—slowly, naturally, and evenly—it must also be fed, rested, and properly exercised.
In those primary schools in which the graded method was best carried out this process of helping natural development was pursued, and the result was seen in contented faces, healthy bodies, and cheerful workers. In future the result will be found in less chorea, hysteria, and insanity.
To prevent the development of hysteria, parents and physicians should direct every effort. The family physician who discovers a child to be neurotic, and who from his knowledge of parents, ancestors, and collateral relatives knows that a predisposition to hysteria or some other neurosis is likely to be present, should exercise all the moral influence which he possesses to have a healthy, robust training provided. It is not within the [p. 275] scope of an article of this kind to describe in great detail in what such education should consist. Reynolds is correct when he says that “self-control should be developed, the bodily health should be most carefully regarded, and some motive or purpose should be supplied which may give force, persistence, unity, and success to the endeavors of the patient.” In children who have a tendency to the development of hysteria the inclinations should not always or altogether be regarded in choosing a method or pursuing a plan of education. It is not always to what such a child takes that its mind should be constantly directed; but, on the contrary, it is often well to educate it away from its inclination. “The worst thing that can be done is that which makes the patient know and feel that she is thought to be peculiar. Sometimes such treatment is gratifying to her, and she likes it—it is easy and it seems kind to give it—but it is radically wrong.”
In providing for the bodily health of hysterical children it should be seen that exercise should be taken regularly and in the open air, but over-fatigue should be avoided; that ample and pleasant recreation should be provided; that study should be systematic and disciplinary, but at the same time varied and interesting, and subservient to some useful purpose; that the various functions of secretion, excretion, menstruation should be regulated.
The importance of sufficient sleep to children who are predisposed to hysteria or any other form of nervous or mental disorder can scarcely be over-estimated. The following, according to J. Crichton Browne,117 is the average duration of sleep required at different ages: 4 years of age, 12 hours; 7 years of age, 11 hours; 9 years of age, 10½ hours; 14 years of age, 10 hours; 17 years of age, 9½ hours; 21 years of age, 9 hours; 28 years of age, 8 hours. To carefully provide that children shall obtain this amount of sleep will do much to strengthen the nervous system and subdue or eradicate hysterical tendencies. Gymnastics, horseback riding, walking, swimming, and similar exercises all have their advantages in preventing hysterical tendencies.
117 Education and the Nervous System, reprinted from The Book of Health by permission of Messrs. Cassell & Co., Limited.
Herz118 has some instructive and useful recommendations with reference to the treatment of hysteria in children. It is first and most important to rehabilitate the weakened organism, and especially the central nervous system, by various dietetic, hygienic, and medicinal measures. It is important next to tranquillize physical and mental excitement. This can sometimes be done by disregard of the affection, by neglect, or by removal or threatened removal of the child from its surroundings. Such treatment should of course be employed with great discretion. Anæmia and chlorosis, often present in the youthful victims of hysteria, should be thoroughly treated. Care should be taken to learn whether children of either sex practise masturbation, which, Jacobi and others insist, frequently plays an important part in the production of hysteria. Proper measures should be taken to prevent this practice. The genital organs should receive examination and treatment if this is deemed at all necessary. On the other hand, care should be taken not to direct the attention of children unnecessarily to those organs when they are entirely innocent [p. 276] of such habits. Painting the vagina twice daily with a 10 per cent. solution of hydrochlorate cocaine has been found useful in subduing the hyper-irritation of the sexual organs in girls accustomed to practise masturbation. Herz, with Henoch, prefers the hydrate of chloral to all other medicines, although he regards morphine as almost equally valuable, in the treatment of hysteria in children. Personally, I prefer the bromides to either morphia or chloral. Small doses of iron and arsenic continued systematically for a long period will be found useful. Politzer of Vienna regards the hydrobromate and bihydrobromate of iron as two valuable preparations in the hysteria of children, and exhibits them in doses of four to seven grains three to four times daily.
118 Wien. Med. Wochen., No. 46, Nov. 14, 1885.
Hysteria once developed, it is the moral treatment which often really cures. The basis of this method of cure is to rouse the will. It is essential to establish faith in the mind of the patient. She must be made to feel not only that she can be helped, but that she will be. Every legitimate means also should be taken to impress the patient with the idea that her case is fully understood. If malingering or partial malingering enters into the problem, the patient will then feel that she has been detected, and will conclude that she had better get out of her dilemma as gracefully as possible. Where simulation does not enter faith is an important nerve-stimulant and tonic; it unchains the will.
Many physicians have extraordinary ideas about hysteria, and because of these adopt remarkable and sometimes outrageous methods of treatment. They find a woman with hysterical symptoms, and forthwith conclude she is nothing but a fraud. They are much inclined to assert their opinions, not infrequently to the patient herself, and, if not directly to her, in her hearing to other patients or to friends, relatives, nurses, or physicians. They threaten, denounce, and punish—the latter especially in hospitals. In general practice their course is modified usually by the wholesome restraint which the financial and other extra-hospital relations of patient and physician enforce.
Although hysterical patients often do simulate and are guilty of fraud, it should never be forgotten that some hysterical manifestations may be for the time being beyond the control of patients. Even for some of the frauds which are practised the individuals are scarcely responsible, because of the weakness of their moral nature and their lack of will-power. Moral treatment in the form of reckless harshness becomes immoral treatment. The liability to mistake in diagnosis, and the frequent association of organic disease with hysterical symptoms, should make the physician careful and conservative. It is also of the highest importance often that the doctor should not show his hand. The fact that an occasional cure, which is usually temporary, is effected by denunciation, and even cruelty, is not a good argument against the stand taken here.
Harsh measures should only be adopted after due consideration and by a well-digested method. A good plan sometimes is, after carefully examining the patient, to place her on some simple, medicinal, and perhaps electrical treatment, taking care quietly to prophesy a speedy cure. If this does not work, in a few days other severe or more positive measures may be used, perhaps blistering or strong electrical currents. Later, but in rare cases only, after giving the patient a chance to arouse [p. 277] herself by letting her know what she may expect, painful electrical currents, the hot iron, the cold bath, or similar measures may be used. Such treatment, however, should never be used as a punishment.
The method of cure by neglect can sometimes be resorted to with advantage. The ever-practical Wilks mentions the case of a school-teacher with hemianalgesia, hemianæsthesia, and an array of other hysterical symptoms who had gone through all manner of treatment, and at the end of seven months was no better. The doctor simply left her alone. He ordered her no drugs, and regularly passed by her bed. In three weeks he found her sitting up. She talked a little and had some feeling in her right side. She was now encouraged, and made rapid progress to recovery. Neglect had aroused her dormant powers. It must be said that a treatment of this kind can be carried out with far more prospects of success in a general hospital than in a private institution or at the home of a patient. It is a method of treatment which may fail or succeed according to the tact and intelligence of the physician.
I cannot overlook here the consideration of the subject of the so-called faith cure and mind cure. One difference between the faith cure as claimed and practised by its advocates, and by those who uphold it from a scientific standpoint, is simply that the latter do not refer the results obtained to any supernatural or spiritual agency. I would not advise the establishment of prayer-meetings for the relief of hysteria, but would suggest that the power of faith be exercised to its fullest extent in a legitimate way.
A young lady is sick, and for two years is seen by all the leading doctors in London; a clergyman is asked in and prays over her, and she gets up and walks. The doctors all join in and say the case was one of hysteria—that there was nothing the matter with her. Then, says Wilks, “Why was the girl subjected to local treatment and doses of physic for years? Why did not the doctors do what the parson did?”
Tuke119 devotes a chapter to psychotherapeutics, which every physician who is called upon to treat hysteria should read. He attempts to reduce the therapeutic use of mental influence to a practical, working basis. I will formulate from Tuke and my own experience certain propositions as to the employment of psychological measures: (1) It is often important and always justifiable to inspire confidence and hope in hysterical patients by promising cures when it is possible to achieve cures. (2) A physician may sometimes properly avail himself of his influence over the emotions of the patient in the treatment of hysterical patients, but always with great caution and discretion. (3) Every effort should be made to excite hysterical patients to exert the will. (4) In some hysterical cases it is advisable to systematically direct the attention to a particular region of the body, arousing at the same time the expectation of a certain result. (5) Combined mental and physical procedures may sometimes be employed. (6) Hypnotism may be used in a very few cases.
119 Influence of the Mind upon the Body.
The importance of employing mental impression is thoroughly exemplified, if nothing else is accomplished, by a study of such a craze as the so-called mind cure. Not a few people of supposed sense and cultivation have pinned their faith to this latest Boston hobby. A glance at the published writings of the apostles of the mind cure will show at once to the [p. 278] critical mind that all in it of value is dependent upon the effects of mental impression upon certain peculiar natures, some of them being of a kind which afford us not a few of our cases of hysteria. W. F. Evans has published several works upon the subject. From one of these120 I have sought, but not altogether successfully, to obtain some ideas as to the basis of the mind-cure treatment. It is claimed that the object is to construct a theoretical and practical system of phrenopathy, or mental cure, on the basis of the idealistic philosophy of Berkeley, Fichte, Schelling, and Hegel. The fundamental doctrine of those who believe in the mental cure is, that to think and to exist are one and the same, and that every disease is a translation into a bodily expression of a fixed idea of mind. If by any therapeutic device the morbid idea can be removed, the cure of the malady is assured. When the patient is passive, and consequently impressible, he is made to fix his thoughts with expectant attention upon the effect to be produced. The physician thinks to the same effect, wills it, and believes and imagines that it is being done; the mental action to the patient, sympathizing with that of the physician, is precipitated upon the body, and becomes a silent, transforming, sanitive energy. It must be, says Evans, “a malady more than ordinarily obstinate that is neither relieved nor cured by it.”
120 The Divine Law of Cure.
Hysteria cannot be cured by drugs alone, and yet a practitioner of medicine would find it extremely difficult to manage some cases without using drugs. Drugs themselves, used properly, may have a moral or mental as well as a physical influence. Among those which have been most used from before the days of Sydenham to the present time, chiefly for their supposed or real antispasmodic virtues, are galbanum, asafœtida, valerian, castor and musk, opium, and hyoscyamus. The value of asafœtida, valerian, castor, and musk is chiefly of a temporary character. If these drugs are used at all, they should be used in full doses frequently repeated. Sumbul, a drug of the same class comparatively little used, is with me a favorite. It can be used in the form of tincture or fluid extract, from twenty minims to half a drachm of the latter or one to two drachms of the former. It certainly has in many cases a remarkably calmative effect.
Opium and its preparations, so strongly recommended by some, and especially the Germans, should not be used except in rare cases. Occasionally in a case with sleeplessness or great excitement it may be absolutely indispensable to resort to it in combination with some other hypnotic or sedative. The danger, however, in other cases of forming the opium habit should not be overlooked. According to Dujardin-Beaumetz, it is mainly useful in the asthenic forms of hysteria.
Of all drugs, the metallic tonics are to be preferred in the continuous treatment of hysteria. Iron, although not called for in a large percentage of cases, will sometimes prove of great service in the weak and anæmic hysterics. Chalybeates are first among the drugs mentioned by Sydenham. Steel was his favorite. The subcarbonate or reduced iron, or the tincture of the chloride, is to be preferred to the more fanciful and elegant preparations with which the drug-market is now flooded. Dialyzed iron and the mallate of iron, however, are known to be reliable preparations, and can be resorted to with advantage. They should be given in large doses. Zinc salts, particularly the oxide, phosphide, and [p. 279] valerianate; the nitrate or oxide of silver, the ammonio-sulphate of copper, ferri-ferrocyanide or Prussian blue,—all have a certain amount of real value in giving tone to the nervous system in hysterical cases.
To Niemeyer we owe the use of chloride of sodium and gold in the treatment of hysteria. He refers to the fact that Martini of Biberach regarded this article as an efficient remedy against the various diseases of the womb and ovaries. He believed that the improvement effected upon Martini's patient was probably due to the fact that this, like other metallic remedies, was an active nervine. He prescribed the chloride of gold and sodium in the form of a pill in the dose of one-eighth of a grain. Of these pills he at first ordered one to be taken an hour after dinner, and another an hour after supper. Later, he ordered two to be taken at these hours, and gradually the dose was increased up to eight pills daily. I frequently use this salt after the method of Niemeyer.
The treatment of hysteria which Mitchell has done so much to make popular, that by seclusion, rest, massage, and electricity, is of value in a large number of cases of grave hysteria; but the proper selection of cases for this treatment is all important. Playfair121 says correctly that if this method of treatment is indiscriminately employed, failure and disappointment are certain to result. The most satisfactory results are to be had in the thoroughly broken-down and bed-ridden cases. “The worse the case is,” he says, “the more easy and certain is the cure; and the only disappointments I have had have been in dubious, half-and-half cases.”
121 The Systematic Treatment of Nerve-Prostration and Hysteria, by W. S. Playfair, M.D., F. R. C. P., 1883.
Mitchell122 gives a succinct, practical description of the process of massage: “An hour,” he says, “is chosen midway between two meals, and, the patient lying in bed, the manipulator starts at the feet, and gently but firmly pinches up the skin, rolling it lightly between his fingers, and going carefully over the whole foot; then the toes are bent and moved about in every direction; and next, with the thumbs and fingers, the little muscles of the foot are kneaded and pinched more largely, and the interosseous groups worked at with the finger-tips between the bones. At last the whole tissues of the foot are seized with both hands and somewhat firmly rolled about. Next, the ankles are dealt with in the same fashion, all the crevices between the articulating bones being sought out and kneaded, while the joint is put in every possible position. The leg is next treated—first by surface pinching and then by deeper grasping of the areolar tissue, and last by industrious and deeper pinching of the large muscular masses, which for this purpose are put in a position of the utmost relaxation. The grasp of the muscles is momentary, and for the large muscles of the calf and thigh both hands act, the one contracting as the other loosens its grip. In treating the firm muscles in front of the leg the fingers are made to roll the muscles under the cushions of the finger-tips. At brief intervals the manipulator seizes the limb in both hands and lightly runs the grasp upward, so as to favor the flow of venous blood-currents, and then returns to the kneading of the muscles. The same process is carried on in every part of the body, and especial care is given to the muscles of the loins and spine, while usually the face [p. 280] is not touched. The belly is first treated by pinching the skin, then by deeply grasping and rolling the muscular walls in the hands, and at last the whole belly is kneaded with the heel of the hand in a succession of rapid, deep movements, passing around in the direction of the colon.”
122 “Fat and Blood,” etc.
Massage should often be combined with the Swedish movement cure. In the movement cure one object is to call out the suppressed will of the patient. This is very applicable to cases of hysteria. The cure of cases of this kind is often delayed by using massage alone, which is absolutely passive. These movements are sometimes spoken of as active and passive, or as single and duplicated. Active movements are those more or less under the control of the individual making or taking part in them, and they are performed under the advice or direction, and sometimes with the assistance, of another. They proceed from within; they are willed. Passive movements come from without; they are performed on the patient and independently of her will. She is subjected to pushings and pullings, to flexions and extensions, to swingings and rotations, which she can neither help nor hinder. The same movement may be active or passive according to circumstances. A person's biceps may be exercised through the will, against the will, or with reference to the will.
A single movement is one in which only a single individual is engaged; speaking medically, single movements are those executed by the patient under the direction of the physician or attendant; they are, of course, active. Duplicated active movements require more than one for their performance. In these the element of resistance plays an important part. The operator with carefully-considered exertion performs a movement which the patient is enjoined to resist, or the latter undertakes a certain motion or series of motions which the former, with measured force, resists. Still, tact and experience are here of great value, in order that both direct effort and resistance should be carefully regulated and properly modified to suit all the requirements of the case. By changing the position of the patient or the manner of operating on her from time to time any muscles or groups of muscles may be brought into play. It is wonderful with what ease even some of the smallest muscles can be exercised by an expert manipulator.
The duplicated active movements are those which should be most frequently performed or attempted in connection with massage in hysterical patients. The very substance of this treatment is to call out that which is wanting in hysteria—will-power. It is a coaxing, insinuating treatment, and one which will enable the operator to gain control of the patient in spite of herself. As the patient exerts her power the operator should yield and allow the part to be moved.
Much of the value of massage and Swedish movements, in hysteria as in other disorders, is self-evident. Acceleration of circulation, increase of temperature, direct and reflex stimulation of nervous and muscular action, the promotion of absorption by pressure,—these and other results are readily understood. “The mode in which these gymnastic proceedings exert an influence,” says Erb,123 “consists, no doubt, in occasioning frequently-repeated voluntary excitations of the nerves and muscles, so that the act of conduction to the muscles is gradually rendered [p. 281] more facile, and ultimately the nutrition of the nerves and muscles is augmented.”
123 Ziemssen's Cyclopædia.
The objects to be attained by the use of electricity are nearly the same as from massage and duplicated active movements: in the first place, to improve the circulation and the condition of the muscles; and in the second place, to make the patient use the muscles. The faradic battery should be employed in these cases, and the patient should be in a relaxed condition, preferably in bed. A method of electrical treatment introduced some years ago by Beard and Rockwell is known as general faradization. This is sometimes used in the office of the physician. In this method the patient is placed in a chair with his feet on a large plate covered with chamois-skin; the operator then takes hold of the patient's hand and the other electrode is passed over the muscles of the neck, back, trunk, and extremities.
When the patient is in bed, as in the regular rest treatment, this method has to be modified, and then the best treatment is by direct muscular faradization. Two sponge electrodes are employed. The sponges are moistened, so that the current may pass through the skin and reach the muscles. Both electrodes are taken in one hand, the handle of one, pointing backward, being between the first and second fingers, while the handle of the other is between the third and fourth fingers. In this way the distance between the points of application can be readily altered. The current is then applied to the muscles everywhere, beginning with those of the feet. Muscles should be relaxed before passing the current through them. The whole body can be gone over in this way in the course of half an hour.
The hydropathic treatment of hysteria is one that has much in it to be commended. Jolly approves the systematic external application of cold water; Chambers advocates the daily morning use of shower-baths, holding that the bracing up of the mind to the shock of a cold shower-bath is a capital exercise for the weak will-power of the hysterical individual, and some admirable results have been reported by Charcot in inveterate neurasthenics and hysterics. Hydrotherapeutic treatment, continued perseveringly for a long time, says Rosenthal, “diminishes the extreme impressionability of hysterical patients, strengthens them, and increases their power of resistance to irritating influences, stimulates the organic functions, combats the anæmia, calms the abnormal irritability of the peripheral nervous system, and by diminishing the morbid increase of reflex power relieves the violence of the spasmodic symptoms. Even chronic forms which are combined with severe paroxysms of convulsions are susceptible of recovery under this plan of treatment.”
The hydrotherapeutic treatment may be contrasted with the treatment by seclusion, rest, massage, and electricity. Undoubtedly, one class of hysterical patients is greatly benefited by the latter method systematically carried out; these have already been described. In other cases, however, this method of treatment is useless; in some of them it has a tendency to prolong or aggravate the hysterical disorder, while in the same cases a well-managed hydrotherapeutic treatment will answer admirably. This is applicable in hysterical patients who eat and drink well, who, as a rule, preserve a good appearance, but whose mind and muscles are equally flabby and out of tone, and need to be stirred up both physically and mentally.
[p. 282]Dujardin-Beaumetz recommends prolonged warm baths of from one to two hours' duration, and believes that the therapeutic virtues of these baths are augmented by infusions of valerian.
In order to obtain satisfactory results from hydrotherapy, as well as from massage, electricity, etc., it is best to remove patients from their family surroundings. Good sanitariums near our large American cities where hydrotherapy and other special methods of treatment can be carried out are sadly needed. Hydrotherapeutic treatment is much more efficacious when conducted at a well-regulated institution, for several reasons. Measures troublesome in themselves are here carried out as a matter of daily routine. Numerous patients permit of the employment of competent attendants. The change is often of great benefit. The close personal supervision which hysterical patients are likely to have in a hydrotherapeutic establishment is also to be taken into consideration. Better modes of living, proper forms of exercise, regulated diet, etc. also enter; but still, a fair share of the good which results can be attributed to the water treatment.
While, however, it is better to remove hysterical patients, for hydrotherapeutic as well as for other treatment, from their family surroundings, and to place them in some well-regulated establishment, it is not by any means impossible to carry out such treatment in private practice, particularly in a house supplied with a bath-room. Many of our hydrotherapeutic institutions are in the hands of charlatans or of individuals who are not practically well fitted for their work. Not infrequently, however, good results are obtained even under these circumstances. Much more can be done in this direction with modest buildings and appliances than is generally supposed. It is not necessary to have numerous apartments: three or four rooms in a well-appointed house, if the arrangements for carrying out the hydrotherapeutic treatment are of a proper kind, will suffice for a large amount of good work. In almost any house provided with bath-rooms with hot and cold water some useful hydrotherapy may be attempted. The spinal douche or pour can be used by placing the patient in a sitz- or ordinary hip-bath and pouring the water from a spout or hose held at a certain height, the distance being regulated according to the patient's condition. Again, the patient sitting in a tub, water can be poured upon her, beginning at first with a high temperature and gradually lowering it. The shower-bath may also be used. An extemporaneous shower-bath can be provided by an ordinary watering-pot. Whole, three-quarters, or half baths at different temperatures can be given. One method of carrying out the wet pack is very simple. A comforter is spread upon the bed; next to this is placed a woollen blanket, and over the blanket a wet linen sheet, upon which the patient rests, with the head on a low pillow. The wet sheet, blanket, and comforter are then wrapped closely about the patient, bottles of hot water being placed at the feet. The cold drip-sheet method is another easily used. It consists in placing about the patient, while sitting up or standing, a sheet wet with cold water, and then vigorously rubbing her through the sheet.
Baths to the head may be used in some cases; cool head-baths are most frequently applied. One method of using these baths is to have the patient lie in such a position that the head projects a little beyond the [p. 283] edge of the bed and over a basin or receptacle of some kind. Water of a suitable temperature is then poured gently or squeezed out of a sponge over the head. For some forms of insomnia or some of the disorders of sleep in hysteria this treatment is a valuable auxiliary to other measures.
For the hysterical spine cold compresses may be used along the spine. On the other hand, hot fomentations may be found of benefit in some cases. Where hydrotherapeutic measures are employed attention should be paid to the condition of the circulation, particularly in the extremities. If the feet or hands are cold, hot applications or frictions should be used.
For certain of the vaso-motor disorders of hysteria, such as cold or hot feet, flushings, etc., local hydrotherapeusis will be of service. In hysterical contractures local stimulation by the douche method or by the steam bath may be tried. For the excitable rectum cold enemata in small quantities, so as not to be expelled, will be found to be very efficacious. For spasmodic attacks, whether purposive or involuntary, the use of the wet pack or the plunge-bath will sometimes be found of good service. In neuralgias and other painful local disorders of hysteria, frictions, fomentations, Turkish or Russian baths, and the wet pack are often very beneficial.
When hysteria is complicated, as it very often is, with disorders of the liver and stomach, hydrotherapeutic measures will be of added efficacy. When it is associated with genito-urinary disorders, even though the latter are not regarded as the cause of the former, special beneficial effects, both local and general, can be obtained from hydrotherapeutic measures. Locally, sitz-baths, hip-baths, douche-baths, hot and cold injections, and foot-baths may act as revulsives, astringents, or local tonics, while at the same time they are measures which tend to strengthen the system as a whole.
Sea-bathing is often of the greatest value, although it is sometimes difficult to induce hysterical patients, who are willing enough to go to the seashore, to resort to surf-bathing. Few measures are better calculated to bring up the tone of the nervous system of an hysterical or neurasthenic patient than well-directed sea-bathing. Where sea-bathing cannot be employed sea-water may be used indoors. Sea-water establishments, where baths at various temperatures may be had, are now to be found at all the best seaside resorts. In a few cases the internal use of large quantities of either hot or cold water, or of the ferruginous mineral waters, may be associated with the external treatment.
The climatic treatment of hysteria has received little or no attention; undoubtedly, much could be said in this connection. In a great country like ours a climate suited to the requirements of almost every form of disease can be had. The climate of those regions, either of the seaboard or inland, particularly well suited to cases of lung trouble, will often be useless, and sometimes harmful, to neurotic patients. For a certain class of hysterical patients a sojourn at the seashore, if not too protracted, will prove of great value. On the whole, for most hysterical patients of the neurasthenic type the best plan is to go first to the seashore for a few weeks, and then resort to an inland hilly or mountainous country, but not at too great an elevation. I have known the climate of some of the high altitudes of Colorado to be of positive injury by depressing the nervous system. Resorts like Capon Springs in West Virginia, out of [p. 284] the reach of steam and worry, with prevailing south-west winds, are desirable places.
The treatment of hysteria by the method of metallotherapy is worthy of some consideration. It is a method by no means new. It was known and practised by the ancients with rings and amulets. Popularized at the beginning of the present century by certain travelling charlatans, it was later, for a time, wholly ignored. In recent years it has been received with considerable attention. One Burq for many years practised metallotherapy in Paris disregarded or scouted by the profession, but claiming many remarkable cures. Finally, Charcot was induced to give him an opportunity of demonstrating the truth or falsity of his claims at Salpêtrière.124 Cases of grave hysteria were submitted to the treatment, and in certain instances with striking results.
124 Lancet, Jan. 19, 1878.
After having determined by a series of experiments the particular metal to which the patient is sensitive, bits of metal may be applied to the surface of the body in various places; this constitutes external metallotherapy. Or the metal, in the form of powder (as reduced iron) or an oxide or some other salt, may be administered; this is internal metallotherapy. That certain definite effects may be produced by the application of metals to the surface of the body is unquestionable. Some of the results which have followed their employment are the removal of anæsthesia and analgesia, relief of hysterical paralysis, improvement in the circulation, removal of achromatopsia, relief of contracture.
Many investigations in Germany, England, France, and this country have demonstrated that the same or similar effects can be produced by the application of other non-metallic substances, such as discs of wood, minerals, mustard plasters, etc. Hammond, among others, has shown this. How the results are obtained is still a matter of dispute. On the one hand, it is claimed, principally by the French observers, that the cures are due to the metals themselves, either by virtue of some intrinsic power or through some electrical currents generated by their application. On the other hand, it is asserted, particularly by the English observers, that the phenomena are best explained on the doctrine of the influence of the mind on the body; in other words, by the principle of expectant attention. Some at least of the effects are to be explained on the latter hypothesis, but it is likely that the monotonous impressions made upon the peripheral sense-organs by different substances applied locally may act reflexly on the brain.
Seguin125 reports a case of convulsion and hemianæsthesia in an adult male cured by metallotherapy; the metal used was gold. Two ordinary twenty-dollar gold pieces were placed in the patient's hands, and afterward on his forearm, cheek, and tongue. Nothing else was suggested or done to him; sensibility returned, and the staggering and other symptoms disappeared. The patient left the hospital claiming to be perfectly well. The same author reports several other successful cases of metallotherapy, all of them reactions to gold. One was a girl sixteen years old with analgesia.
125 Arch. of Medicine, New York, 1882.
Not a few cases are now on record of the cure of hysterical contracture and other forms of local hysterical disorders by the application of a magnet. Charcot and Vigouroux cured one case of hysterical contracture [p. 285] of the left arm by repeated applications of the magnet to the right or healthy arm. Debove by prolonged application of magnets relieved hemianæsthesia and hemiplegias—not only the hysterical varieties, but also, it is said, when dependent upon such conditions as alcoholism, plumbism, and even cerebral lesions. Maggiorani of Rome studied the physiological action of the magnet and laid down the first rules for its therapeutic use. In the case of powerful magnets we have more room for believing that an actual, tangible force is at work in producing the results than in the case of simple metals.
The question has been sometimes asked whether hypnotism can be used with success in the treatment of hysteria. Richer reports a few cures of hysteria through this agency. Braid has put on record between sixty and seventy cases which he claims to have cured by the same means. This list undoubtedly includes some hysterical cases—of paralysis, anæsthesia, aphonia, blindness and deafness, spinal irritation, etc. Both on theoretical grounds and from experience, however, I believe that the practice of hypnotization may be productive of harm in some cases of hysteria, and should be resorted to only in rare cases of mental or motor excitement.
By some, special measures during the hysterical fit are regarded as unnecessary. Jolly, for instance, says that we must merely take care that the patients do not sustain injury in consequence of their convulsive movements, and that respiration is not impeded by their clothing. Rothrock126 reports several cases of hysterical paroxysms relieved by the application of either snow or ice to the neck. The applications were made by stroking up and down either side of the neck along the line of the sterno-cleido-mastoid muscles. He believed that the most probable explanation of the results obtained was the shock received from the cold substance, but that supplemental to this there may have been supplied through the pneumogastric nerve a besoin de respirer. This measure and the use of the cold spinal douche are both to be recommended.
126 Philada. Med. Times, 1872-73, iii. 67.
Emetics are sometimes valuable. Miles127 reports several cases of severe hysterical seizure in which tobacco was promptly efficient in controlling the affection. He used the vinum tabaci in doses of one drachm every half hour or hour until the system was relaxed and nausea induced, the effects usually being produced after taking three or four doses. Fifteen grains of sulphate of zinc may be used in adult cases. James Allen for a case of hysterical coma successfully used a hypodermic injection of one-tenth of a grain of apomorphia. Recently, at the Philadelphia Hospital this remedy has been successfully employed in two cases, one of hysterical coma and the other of hysterical mania. Inhalations of nitrite of amyl are often of surprising efficiency. This and other measures referred to under HYSTERO-EPILEPSY are also applicable in the treatment of any form of hysterical spasm.
127 Clinical Med. Reporter, 1871, iv. 25-27.
For hysterical convulsions occurring during pregnancy an enema of asafœtida, camphor, the yolk of an egg, and water, such as has been recommended by Braun of Vienna, will often be found promptly efficacious.
Fagge128 mentions a procedure which he had often seen adopted by Stocker—namely, pressure upon the arteries and other structures on each side of the neck.
128 British Medical Journal, March 27, 1880.[p. 286]
For hysterical paralysis faradism and galvanism hold the chief place. Metallic-brush electricity should be used in the treatment of anæsthesia.
Whenever, in local hysteria, particularly of the paralytic, ataxic, or spasmodic form, it is possible to coax or compel an organ or part to perform its usual function long unperformed or improperly performed, treatment should be largely directed to this end. Thus, as Mitchell has shown, in some cases of aphonia, especially in those in which loss of voice is due to the disassociation of the various organs needed in phonation, by teaching the patient to speak with a very full chest an involuntary success in driving air through the larynx may sometimes be secured. Once compel a patient by firm but gentle means to swallow, and œsophageal paralysis begins to vanish.
Mitchell makes some interesting remarks upon the treatment of the peculiar disorders of sleep, which he describes and to which I have referred. When the symptoms are directly traceable to tobacco, he believes that strychnia and alcohol are the most available remedies, but gives a warning against the too liberal use of the latter. A treatment which was suggested to him by a clever woman who suffered from these peculiar attacks consists in keeping in mind the need of breaking the attack by motion and by an effort of the will. As soon as the attack threatens the patient should resolutely turn over, sit up, or jump out of bed, and move about, or in some such way overcome the impending disorder. Drugs are of little direct use. Small doses of chloral or morphia used until the habit is broken may answer, but general improvement in health, proper exercise, good food, and natural sleep are much more efficient.
Fagge says that he has seen more benefit in hysterical contracture from straightening the affected joints under chloroform, and placing the limb upon a splint, than from any other plan of treatment. Hammond129 (at a meeting of the New York Neurological Society, Nov. 6, 1876) reports a case of supposed hysterical contracture in the form of wry neck, in which he divided one sterno-cleido-mastoid muscle; immediately the corresponding muscle of the other side became affected; he cut this; then contraction of other muscles took place, which he kept on cutting. The case was given up, and got well spontaneously about two years later. Huchard130 entirely relieved an hysterical contracture of the forearm by the application of an elastic bandage.
129 Philadelphia Medical Times, vol. vii., Nov. 25, 1876.
130 Revue de Thérapeutique, quoted in Med. Times, vol. xiii., June 16, 1883.
A lady with violent hysterical cough was chloroformed by Risel of Messeberg131 for fourteen days at every access of the cough, and another for eight days. In both the symptoms were conquered. Nitrite of amyl is useful in similar cases.
131 Allg. Med. Centralzeitung, Oct. 9, 1878.
Graily Hewitt132 reports a case of hysterical vomiting of ten months' duration, caused by displacement of the uterus, and cured by reposition of that organ. The same authority, in a paper read to the London Congress, advanced the opinion that the exciting cause of attacks of hysteria and hystero-epilepsy was a distortion of the uterus produced by a flexion of the organ upon itself, either forward or backward. He believed the attacks were the result of reflex irritation. He recited [p. 287] eighteen cases, all of which were relieved. Flechsig133 favors the gynæcological treatment of hysteria, including castration or oöphorectomy. He reports three cases with good results. His article favors the idea that any morbid condition of the genital organs present ought to be remedied before treating the hysterical symptoms. Zeuner,134 on the other hand, refers to a number of cases in which gynæcological treatment gave either entirely negative results or was productive of positive injury to hysterical patients. He quotes Perreti,135 physician to an asylum for the insane, who gives the details of a number of cases in which gynæcological examinations or treatment were directly productive of injury. He mentions a case of a female patient who had delusions and hallucinations of a sexual type in which the physician was the central figure. He reports cases in which proper constitutional treatment, without gynæcological interferences, led to a full recovery. Playfair, also quoted by Zeuner, states that he has often known the condition of hysterical patients to be aggravated by injudicious gynæcological interference. Oöphorectomy will be more fully discussed under HYSTERO-EPILEPSY.
132 Med. Press and Circ., June 2, 1880.
133 Neurol., 7 Abt., 1885, Nos. 19, 20.
134 Journ. American Med. Ass., Chicago, 1883, i. 523-525.
135 Berliner klinische Wochenschrift, No. 10.
DEFINITION.—Hystero-epilepsy is a form of grave hysteria characterized by involuntary seizures in which the phenomena of hysteria and epilepsy are commingled, and by the presence in unusual number and severity, between the paroxysms, of symptoms of profound and extensive nervous disturbance, such as paralysis, contracture, hemianæsthesia, hyperæsthesia, and peculiar psychical disorders.
SYNONYMS.—Hystero-epilepsy has long been known under various names, as Epileptiform hysteria, by Loyer-Villermay and Tissot; as Hysteria with mixed attacks, by Briquet; as Hysteria major or Grave hysteria, by Charcot. The term hystero-epilepsy has been used with various significations, and often without due consideration, and for these reasons some authorities advise that it should not be used at all. Gowers,1 for instance, refers to epileptic hysteria, hysterical epilepsy, and hystero-epilepsy as hybrid terms which tend rather to hinder than to advance the study of the nature of these convulsive attacks and their relations to other forms of hysteria. He holds that it is a clear advantage to discard them as far as possible, and suggests the use of the term hysteroid, as proposed by W. W. Roberts, or that of co-ordinate convulsions, as describing accurately the character of the attack. These suggested terms do not strike me as improvements upon those which he wishes the profession to avoid. The word hysteroid, while good enough in its way, is certainly objectionable on the ground of indefiniteness. Co-ordinate is proposed, because the convulsive movements are of a quasi-purposive appearance; that is, they are so grouped as to resemble phenomena which may be controlled by the will. This meaning of co-ordinate, however, as applied to the disorder in question, would not be easily grasped by the average physician. When it is impossible to name a disease from the standpoint of its pathological anatomy, the next best plan is to use a clinical term which in a plain common-sense manner gives a fair idea of the main phenomena of the affection. Hystero-epilepsy, if it means anything, means simply a disorder in which the phenomena of both hysteria and epilepsy are to some degree exhibited. Certainly, this is what is seen in the cases known as hystero-epileptic. In forming the compound the hysterical element is, very properly, expressed first, the disease being a hysteria with epileptic [p. 289] or epileptoid manifestations, rather than an epilepsy with hysterical or hysteroid manifestations. A study of the definition of hystero-epilepsy which has been given will show that it is intended to restrict the application of the term in the present article to cases with involuntary or non-purposive attacks, the voluntary or purposive having been considered in the last article.
1 Epilepsy and other Chronic Convulsive Diseases: their Causes, Symptoms, and Treatment, by W. R. Gowers, M.D., F. R. C. P., etc., London, 1881.
HISTORY.—The greatest impulse to the study of hystero-epilepsy in recent years has been given by the brilliant labors of Charcot and his pupils and assistants in his famous service at La Salpêtrière. In his lectures on diseases of the nervous system2 (edited by Bourneville), and in various publications in Le Progrès médical and other journals, Charcot has reinvestigated hysteria major with great thoroughness, and has thrown new light upon many points before in obscurity. He deserves immense credit also for the work which he has stimulated others to do. Bourneville, well known as the editor of some of Charcot's most valuable works, has published, alone or with others, several valuable monographs upon hysteria and epilepsy.3 The most valuable work on hystero-epilepsy, however, because the most elaborate and comprehensive, is the treatise of Richer.4 Richer was for a time interne in the Salpêtrière Hospital, and with Regnard pursued his investigations under the superintendence and direction of Charcot. His book is a volume of more than seven hundred pages, containing a vast amount of information and profusely illustrated, in large part by original sketches by the author. Charcot himself has written for it a commendatory preface.
2 Leçons sur les Maladies du Système nerveux. A portion of these lectures have been translated by G. Sigerson, M.D., and published by the New Sydenham Society of London, and reprinted in 1878 and 1879 in Medical News.
3 Bourneville, Recherches clinique et therapeutique sur l'Épilepsie et l'Hystérie, 1876; Bourneville et Voulet, De la Contracture hystérique-permanente, 1872; Bourneville et Regnard, Iconographie photographique de la Salpêtrière. I have made special use of the second volume of the last of these works.
4 Études cliniques sur l'Hystero-épilepsie, ou Grande Hystérie, par le Dr. Paul Richer, Paris, 1881.
No article on hystero-epilepsy can be written without frequent use of this work of Richer, and also of the numerous contributions of Charcot. To them we are indebted for new ways of looking at this disease, as well as for an almost inexhaustible array of facts and illustrations of the diverse phases of this disorder.
While the curious, grotesque, or outrageous manifestations now known as hystero-epileptic have been discussed with more or less minuteness by authors from the time of Sydenham to the present, usually, and more especially in all countries but France, these manifestations have been studied as isolated phenomena. Charcot and Richer, however, present a comprehensive view of hysteria as a disease of a certain typical form, but often manifesting itself in an imperfect or irregular manner. This regular type is characterized particularly by a frequently- or infrequently-recurring grave attack, which is divided into distinct periods, and these periods into phases.
This regular type of grave hysteria once understood, a place of advantage is gained from which to study the disease in its imperfect, irregular, and abortive forms. Whatever its pathology may be, such striking symptoms as loss of consciousness with spasm, hallucinations, and [p. 290] illusions show at least temporary disturbance of the integrity of the cerebrum.
Hystero-epilepsy of imperfectly developed or irregular type is a not uncommon affection in this country, but the disease in its regular type is comparatively rare.
VARIETIES.—Hysteria and epilepsy, so far as seizures are concerned, may show themselves in two ways in the same patient; but I believe that it is best that the term hystero-epilepsy should be restricted in its application, as Charcot, Bourneville, and Richer have advised, to the disorder in which hysterical and epileptic symptoms are commingled in the same attack—what is spoken of by the French as hystero-epilepsy with combined crises. The other method of combination is in the affection known as hystero-epilepsy with separate crises, in which the same patient is the victim of two distinct diseases, hysteria and epilepsy, the symptoms of which appear independently of each other.
The fact that hysteria is at times associated with true epilepsy is often overlooked. A patient who is known to have had pure hysterical seizures of the grave type has also a genuine paroxysm of epilepsy, and thus the medical attendant is deceived. I will dismiss the consideration of hystero-epilepsy with separate crises with a few paragraphs at this place, devoting the rest of the article to the disorder with combined crises.
The coexistence of hysteria and epilepsy, with distinct manifestations of the two neuroses, has been most thoroughly considered by D'Olier.5 Beau in 1836, and Esquirol in 1838, first showed this coexistence. Landouzy in 1846 first made use of the name hystero-epilepsy with separate crises.
5 Memoir which obtained the Esquirol prize in 1881, by M. D'Olier, interne of the hospitals of Paris, on “Hystero-Epilepsy with Distinct Crises, considered in the Two Sexes, and particularly in Man,” translated and abstracted by E. M. Nelson, M.D., in the Alienist and Neurologist, April, 1882.
In France the distinct existence of hysteria and epilepsy in the same individual is not, according to D'Olier, a very exceptional fact. Beau has reported it 20 times in 276 cases. The different modes of coexistence have been summed up by Charcot as follows: “1, Hysteria supervening in a subject already epileptic; 2, epilepsy supervening in a subject previously hysterical; 3, convulsive hysteria coexisting with epileptic vertigo; 4, epilepsy developing upon non-convulsive hysteria (contracture, anæsthesia).”
The following case, now in the Philadelphia Hospital, illustrates the first of these modes of combination: S——, aged thirty-nine, female, a Swede, came to this country in 1869. She said that her mother had fits of some kind. The patient had her first fit when she was four years old. Her menses did not come on until she was nineteen. With the appearance of her periods she had fainting-spells off and on for two years, and in these spells she would fall to the ground. After two years she improved somewhat, but still would have an occasional seizure like petit mal. Four years ago she had a severe fit, in which she bit her tongue. This was a paroxysm of true epilepsy. It was witnessed by the chief nurse in the hospital, a competent observer. Since then she has had attacks of some kind every month or oftener. She rarely had a true epileptic seizure. Often, however, she had hysterical and [p. 291] hystero-epileptic attacks. These paroxysms have been witnessed by myself and by the resident physician and nurse. Rarely they were epileptic, frequently they were hysterical. Mental excitement will often induce an hysterical spasm.
PATHOLOGY.—Holding that hystero-epilepsy is a form of grave hysteria, the remarks which have been made in the last article on the probable nature of severe convulsive attacks will be applicable here. In hystero-epilepsy with the typical grave attack we have the highest expression of that disturbance of cerebro-spinal equilibrium which constitutes the pathology of hysteria.
ETIOLOGY.—It will also be unnecessary to go at length into the discussion of the predisposing and exciting causes of hystero-epilepsy. In general, its predisposing causes are those of hysteria of any form. Certain causes or conditions, however, predispose to certain types or forms of hysteria. The Latin races are more inclined to the hystero-epileptic form of hysteria than are the natives of more temperate or colder climates. Bearing upon this point, I have already quoted the letter of Guiteras with reference to hysteria and hystero-epilepsy in Cuba and semi-tropical America. Forms of religion which cultivate to an extreme degree the emotional or the sentimental side of human nature tend to produce hystero-epilepsy.
With reference to sex it may be said that hystero-epilepsy prevails to a greater extent among females than males, even proportionately to a larger degree than some of the other marked phases of hysteria. It does, however, occur in men and boys, although rarely. Richer records, from the practice of Charcot, a case in a lad of twelve years. Several cases have fallen under my own care.
Ten years since I saw a case of hystero-epilepsy, which in some respects closely simulated tetanus, in a youth nineteen years old. He was well until seventeen years of age, when he slightly wrenched his back. Shortly afterward he felt some pain between the shoulders. From that time, at irregular intervals, generally of a few days only, he was subject to attacks of dull pain, which seemed to run up the spine to the head. About two months after this injury he first had a spasmodic attack. A spasm would come on while he was quietly sitting or working. The body assumed the backward-arched position. As his father described the case, there was always space enough under his back for a baby to crawl through. Generally, he would have more than one seizure on a given occasion. He would sometimes have as many as six or seven in one hour. On coming to, he would stare and mutter and work his mouth and lips, at the same time pointing around with his hands and fingers in a wild way. Sometimes he would sleep for several hours afterward if not disturbed, but his sleep was not of a stertorous character. He said that he could feel the attacks coming on; his body felt as if it was stretching, his head going back. He thought he was not conscious during the whole of the attacks, but between the spasms he could take medicine when directed. When first examined he had decided tenderness on pressure over the second, third, and fourth dorsal vertebræ. Pressure in this region would sometimes bring on a convulsive paroxysm. When first seen he had been for three months having seizures every two or three weeks. He was under observation for several months, during which time he was treated with faradization to the spine, the hot spinal douche, tonics, and bromides, and made a complete recovery.
[p. 292]W. Page McIntosh6 has reported several cases of hystero-epilepsy in the male, one of which is doubly interesting because it was in a negro. This patient was twenty-one years old, stout, and previously in good health. He complained of intense pain in the stomach, and soon passed into a violent convulsion. To show the importance of diagnosis in these cases, it is interesting to note that the doctor first thought of strychnia-poisoning, then of acute indigestion, next of tetanus. Soon, however, he decided that he had a case of hysteria. The patient had other convulsions on the day following the first attack. The seizures were evidently hystero-epileptic or hysterical. He was not unconscious, and believed that on a recent previous evening he had been conjured by an old negress. The spell was to work in three days, which it did. The doctor counter-spelled him with a hypodermatic syringe, after which he promptly recovered. McIntosh reports another case in a man forty years old and the father of six children, who was laboring under strong mental excitement because of the sufferings of a dangerously ill child. His whole form was convulsed, and his body underwent a variety of peculiar contortions. He had had similar attacks before, and had subsequent recurrences.
6 Med. News, vol. xlviii., No. 1, Jan. 2, 1886, pp. 5-8.
The following case was observed in the Philadelphia Hospital: W. F. ——, aged twenty-eight years, married, has one child. His seizures began seven years ago, when he had an attack while playing a game of pool. At this time he had, according to his account, a sudden feeling of giddiness or vertigo in which he fell over and had a spasm, during which he thinks he was unconscious. After the seizure he suffered from headache, but had no disposition to sleep.
From that time until the present he has been subject to these spells, though the paroxysms are very irregular in frequency. Sometimes he will have several attacks in a day; again, he will be free from them for days, and perhaps for two or three weeks, but never for more than a month at a time. They have come on him while walking in the street, and on several occasions he has been taken to different hospitals. He was admitted to the Philadelphia Hospital four times. On his first admission he only remained over night; on his second and third he remained for two or three weeks. On the last admission he remained four weeks, and had spasms every day and night after admission. He had, by actual count, from five to six hundred after he went in; and in one evening, from seven P.M. to midnight, he had no less than thirty-eight. These seizures, which were witnessed by myself and two resident physicians, differed but little from each other, although at times some were more violent than others. They began with a forced inspiration; then the patient straightened himself out and breathed in a stertorous or pseudo-stertorous manner. The pulse in that stage became slow, and at times was as low as 48 per minute. The temperature was normal or subnormal. The arched position was sometimes taken, but the opisthotonos was not marked. The paroxysm ceased by an apparent forced expiration, and the breathing then became normal; the patient remained in a somewhat dazed condition, which was only momentary. During the attack the patient said that he was unconscious of his surroundings. In the interval between the attacks he suffered from headache and from pain [p. 293] over the region of the stomach. He also had tenderness on pressure over the lumbar vertebræ. He never bit his tongue.
Age has some influence in the development of hystero-epilepsy. It is of most common occurrence at the period of pubescence; it is rare in old age, but occurs with comparative frequency in middle life; or, rather, it should be said that middle-aged hystero-epileptics are not uncommonly met with, individuals who have for many years been subject to the attacks. In young children, girls or boys, it is certainly rare.
With reference to the exciting causes of hystero-epilepsy, it will only be necessary to say that of those which have already been enumerated in the general discussion of the etiology of hysteria, a few, such as domestic troubles, abnormal sexual excitement, and painful menstruation, are likely to induce the paroxysm, but fright, excitement, anxiety, sudden joy, and other psychical disturbances are the most frequent of the exciting causes of the seizures. A threat or a blow has been known to precipitate an attack. The use or abuse of alcohol is sometimes an exciting cause. Reflex irritation, such as that from intestinal worms, and digestive disorders sometimes produces hystero-epileptic attacks in children.
SYMPTOMATOLOGY.—In considering the symptoms of hystero-epilepsy the subject must be approached from several points of view. In the first place, the disorder can be divided (1) into the regular or typical grave attack; and (2) into the irregular attacks. These irregular seizures can be greatly subdivided, but their discussion will be confined to those types which have been most observed in this country, although I do not think that any variety of hystero-epilepsy is distinctively American; and this is what might be supposed from the largeness of our country and the different nationalities of which it is composed.
I have seen but few cases of hystero-epilepsy of the regular type. One of these was first described at some length in the American Journal of Medical Sciences for October, 1881. I will here give the case, with illustrations, somewhat condensed from the accounts as first published.7
7 For the opportunity of studying and treating this case I was under obligations to Charles S. Turnbull and J. Solis Cohen, the patient having been for several months under their care at the German Hospital of Philadelphia. Carefully prepared notes of the case were furnished to me by H. S. Bissey and H. W. Norton, resident physicians at the hospital. I was also under great obligations to my friend J. M. Taylor for a series of sketches of the positions assumed by the patient at different stages of the attack.
R——, æt. 21, single, was first admitted to the German Hospital Nov. 13, 1879. Between her ninth and twelfth years she had had several attacks of chorea. During childhood she was often troubled with nightmare and unpleasant dreams; she often felt while asleep as if she were held down by hands. She was frequently beaten about the head and body. Her menses did not appear until she was nearly eighteen. Before and at her first menstrual epoch she suffered severe pain and cramp. During the first year of her menstruation, while at Atlantic City, the flow appeared in the morning, and she went in bathing the same afternoon. She stayed in the water two hours, was thoroughly chilled, and the discharge stopped. Ever since that time she had only menstruated one day at each period, and the flow had been scanty and attended with pain. When about eighteen she kept company with a man for five months, and after having put much confidence in him learned that he had a wife and two children. This episode caused her much worriment. She positively [p. 294] denied seduction. She became much depressed. September 2, 1879, she was seized in a street-car with a fainting fit. On coming to, she found her left arm was affected with an unremitting tremor. Seven weeks later she was admitted to the German Hospital. She had severe spasmodic attacks, and the diagnosis of hysteria was made. She remained in the hospital about four weeks. On leaving she again went into service. She was readmitted June 9, 1880, in an unconscious or semi-conscious condition. She had been on a picnic, and while swinging was taken with an attack of spasm and unconsciousness. During two hours after admission she had a series of convulsions. After this she had similar attacks two or three times a week, or even oftener.
I first saw her about the middle of January, 1881. She had an hysterical face, but was possessed of considerable intelligence, and when questioned talked freely about herself. The most prominent physical symptom that could be discovered was a large tremor, affecting the left arm, forearm, and hand. This was constant, and had been present since her admission to the hospital. The left half of her body was incompletely anæsthetic, the anæsthesia being especially marked in the left forearm. Ovarian hyperæsthesia could not at this time be made out. She was, however, hyperæsthetic over the occipital portion of the scalp and the cervico-dorsal region of the spine. Pressure or manipulation of these regions would in a few moments bring on an attack of spasm. The attacks, however, usually occurred without any apparent exciting cause.
For a period of from six to twelve hours before an attack she usually felt dull, melancholy, and strange in the head. Frequently she had noises like escaping steam in her ears, but more in the right ear than in the left. She complained of cardiac palpitations. She usually had pain in the small of her back. Her limbs felt weak and tired. Just as the attack was coming on her eyes became heavy and misty, her head felt as if it was sinking backward, and if not supported she would fall in the same direction.
On several occasions I had the opportunity of watching every phase of the attack or series of attacks, the spasms continuing sometimes from one to four or five hours. The order of events was not always the same, and yet a general similarity could usually be seen in the successive stages of the phenomena. I will try to give an outline of the different stages and phases as observed on an occasion when the seizures were severe.
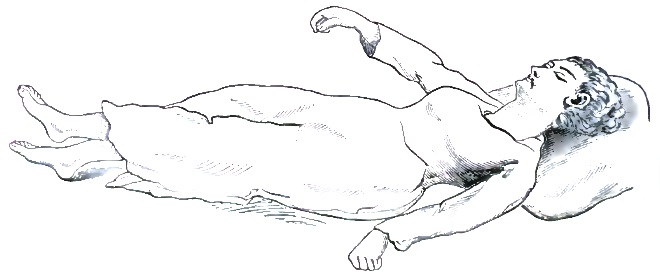
After lying down, the first noticeable manifestation was a twitching of [p. 295] the eyelids and of the muscles of the forehead and mouth. Her head was next moved from side to side, and she looked around vaguely. Respiration became irregular. In a few moments a convulsive tremor passed down her body and limbs. Her arms were now carried outward slightly from the body, the hands being partly clenched. The lower extremities were straightened, the left foot and leg being carried over the right (Fig. 18). Her limbs were rigid. Her mouth was closed, the teeth being ground together. Consciousness was lost, and respiration seemed to stop.
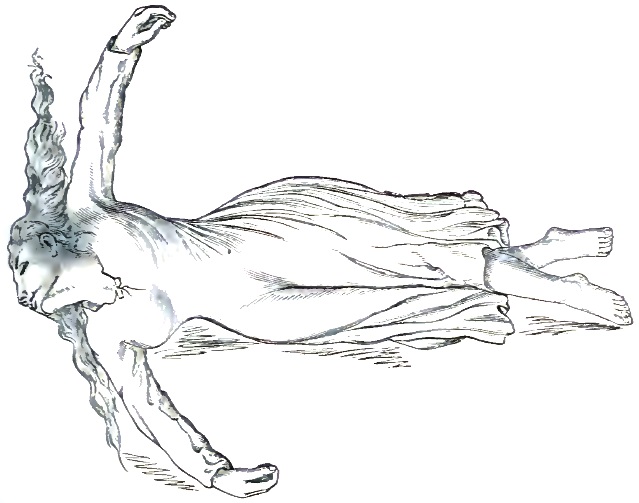
A series of strong convulsive movements next ensued. Her entire body was tossed up and down and twisted violently from side to side. Sometimes she assumed a position of opisthotonos. Her whole body was then again lifted and hurled about by the violence of the movements. A [p. 296] few seconds later she became quiet but rigid, in the position shown in Fig. 19, corresponding to the position of crucifixion of the French writers.
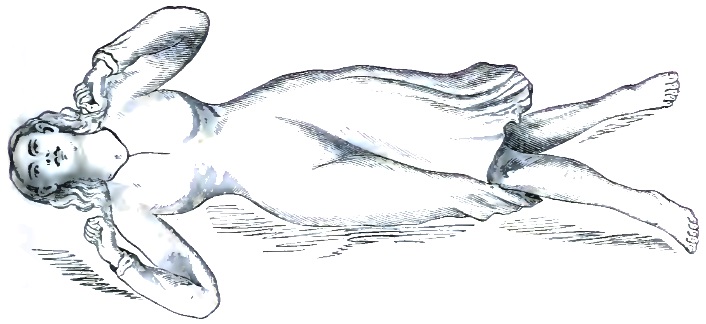
Soon she assumed the position represented by Fig. 20, and the convulsions were renewed with violence, the patient's limbs and body being frequently tossed about and the latter sometimes curved upward. After these movements had continued a brief period the patient became calm and partially relaxed; but the respite was not long. A series of still more remarkable movements began, chiefly hurling and lifting of the body. Eventually, and apparently as a climax to a succession of efforts directed to this end, she sprang into the position of extreme opisthotonos represented in Fig. 21. This sketch, by Taylor, is a very faithful view of her exact position. She remained thus arched upward for a minute, or even more. A series of springing and vibratory movements followed, the body frequently arching.
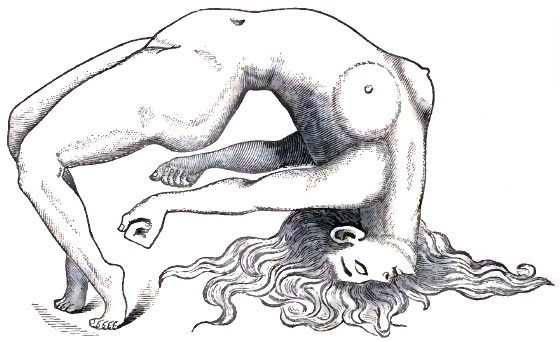
As the spasms left she sat up on her bed, and at first looked around with a bewildered expression. She turned her head a little to one side and seemed to gaze fixedly at some object. Her expression was slightly smiling. When spoken to she looked straight at the one addressing her, but without appearing to know what was said, and the next moment the former position and attitude were resumed. After a few minutes she lay down muttering incoherently, and in about a quarter of an hour fell asleep.
I have simply described one attack. Sometimes she would have several in succession, or the spasmodic manifestations would be repeated several times in a regular or an irregular manner. Strong pressure in the ovarian regions usually would not cut short the spasms. They could be stopped, however, by etherization or by active faradization of the limbs or trunk. She did not always conduct herself in the same manner in the period which succeeded the spasms. Sometimes, after getting into the sitting posture, instead of smiling, she would look enraged and speak a few words. The following expressions were noted on one occasion: “You know it! Yes, you do! Yes! yes!” Often she was heard to mutter for hours after the attack. Her lips would sometimes be seen to be moving without any words being heard. Sooner or later she would fall into sound sleep which would last several hours.
[p. 297]During the spasms she seemed to be entirely unconscious of her surroundings. To a looker-on her movements seemed sometimes to have the appearance of design, but I soon convinced myself that such was not the case. She was insensitive to painful or other impressions. Her expression was blank and unchanging. She said that the only thing that she remembered about the attacks was that she heard a strange, confused sound; this was most probably just as she was returning to consciousness.
Numerous remedies were tried without any apparent effect. These included sodium and potassium bromides, iron, zinc salts, physostigma, cimicifuga, camphor, ether, etc. A uterine examination was made, but nothing especially calling for local treatment was found. She was placed upon equal parts of tincture of valerian and tincture of iron in half-teaspoonful doses three times daily. Capsules of apiol were also ordered to be taken three times daily just before and during her menstrual period. Her menses became more profuse and continued longer. The attacks began to diminish in frequency, and became less severe. In March, not having had a seizure for several weeks, she left the hospital and again went into service. Six months elapsed and she had no attack. She reports occasionally at my office. She says that she feels entirely well. The tremor of the left upper extremity entirely disappeared. She continued to take valerian and iron for four months, but stopped the apiol after the second or third menstrual period.
With this case before us the phenomena of the disease can be more readily grasped. I will necessarily make free use of the labors of Richer in my description of symptoms.
Hystero-epileptic attacks usually, although not always, have distinct prodromes. These have been more thoroughly studied and reported by Richer than by any other author. They are classed by him under the four heads of psychical affections, including hallucinations, affections of the organic functions, motor affections, and affections of sensibility. The patient's condition is changing; she is listless, irritable, melancholy, despairing, slovenly. Sometimes she is noisy, sometimes mute. At times she is full of wild excitement. Hallucinations of sight sometimes come on at this period—most commonly visions of cats, rats, spiders, etc. These visions of animals, as first pointed out by Charcot, in passing before the patients run from the left to the right or from the right to the left, according as the hemianæsthesia is situated on the left or on the right. Hallucinations of hearing, as of music, threats, demands, whistling, trumpeting, etc., also occur, chiefly on the hemianæsthetic side. These hallucinations are worse at night. Sometimes at night the patients are the victims of imaginary amours. Want of appetite, perverted taste, nausea and vomiting, flatulence, tympanites, ptyalism, unusual flow of urine, feelings of oppression, hiccough, laughing, barking, loss of voice, palpitation of the heart, and flushings are among some of the many disorders of the organic functions which are sometimes present during the prodromal period. Loss of muscular power or a species of ataxia, peculiar limited spasmodic movements, contracture, first of one limb and then of another, may be observed. Charcot, Bourneville, Regnard, and Richer, all give admirable illustrations of different forms of contracture. In one case the right arm and wrist are flexed, [p. 298] and the hand held at the level of the shoulder with fingers extended. Anæsthesia—total, unilateral, or local, tactile, of pain, temperature, etc.—may also occur. Sometimes achromatopsia or color-blindness shows itself; sometimes deafness in one ear is present. Tenderness over the ovarian region is often an immediate precursor. To Charcot we owe the most careful study of these symptoms.
Among the most interesting prodromic affections of sensibility are the hysterogenic or hystero-epileptogenic zones. These have been well studied and described by Richer, from whose work Figs. 22 and 23 have been taken. Brown-Séquard has shown that animals rendered epileptic by lesions of the spinal cord, medulla oblongata, or nerves are sometimes attacked with convulsions spontaneously, but it is also possible to provoke these attacks by exciting a certain region of the skin which he designates as the epileptogenic zone. This zone, situated on the same side of the body as the nervous lesion, has its seat about the angle of the lower jaw, and extends toward the eye and the lateral region of the neck. The skin of this region is a little less sensitive than that of the opposite side, but touching it most lightly provokes epileptic convulsions. The simple act of breathing or blowing on it brings about the same result.
Something analogous to this epileptogenic zone has been noticed among hystero-epileptics, and has been pointed out by several writers. Richer gives the particulars of a number of cases. In one patient the hyperæsthetic zone was between the two shoulder-blades. Simply touching this region was sufficient to provoke an attack, and this was more easily done if near the time of a spontaneous seizure. After the grave attacks the excitability would seem to be exhausted, and pressure in the zone indicated would not cause any convulsive phenomena. A second case presented a similar condition. If touched over the dorsal spine between the shoulders, she felt a violent pain in the belly, then a sense of suffocation, which brought on at once loss of consciousness. In a third patient the hysterogenic zone was different. It was double. It was necessary to touch two symmetrical points situated to the outside and a little below the breasts in order to bring on the hystero-epileptic convulsions. Touching one of these points did not produce any result. Other cases are given in detail, but a glance at the two figures (22 and 23) will show some of the principal hysterogenic zones both for the anterior and posterior surfaces of the body. A zone of ovarian hyperæsthesia was common to all the patients. It did not differ essentially from the other hysterogenic zones. If the ovarian hyperæsthesia existed along with other hysterogenic points, the excitation of the ovarian region was always the most efficacious. The hysterogenic zones always occupy the same place in the same case. They are found on the trunk exclusively; they are more frequently in front than behind; in front they occupy lateral positions, and are often double and symmetrical; behind they are more often single and median; they exist more frequently to the left than to the right, and the unilateral zones have always been met with on the left side.
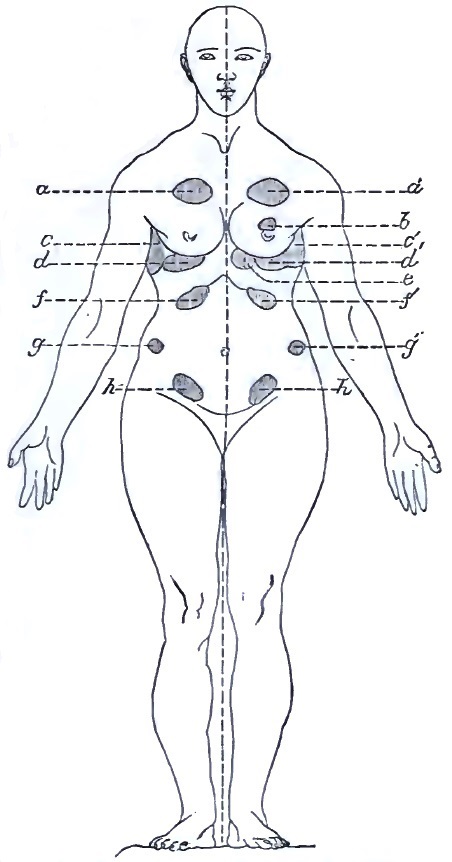
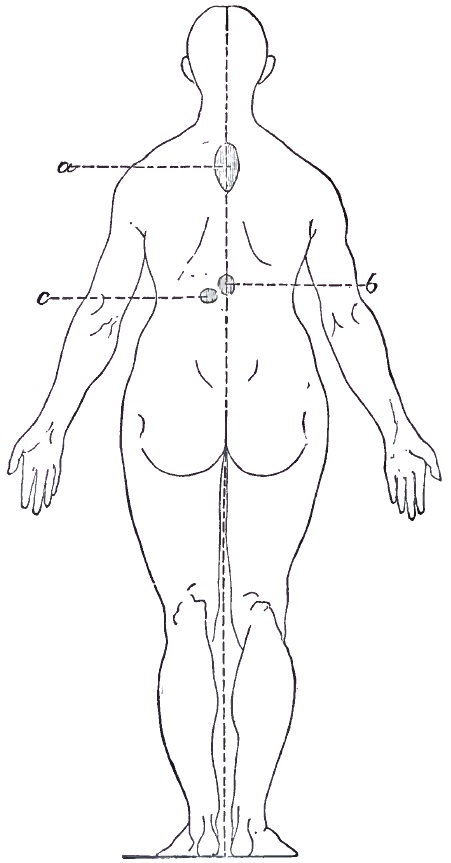
The hysterogenic zones bear no constant relation to the hemianæsthesia. It is true that the ovarian pain is most often seated on the hemianæsthetic side, but sometimes it is present on the opposite side. They [p. 299] are not at all times equally excitable. They are more so when the convulsive attack is imminent.
Ovarian pressure gives rise to the spasmodic attacks: the same pressure arrests them. What is true of ovarian compression is equally true of all the hysterogenic zones. A light touch brings on the convulsions, which have scarcely commenced when they can be stopped by a new excitation of the same point.
As already stated, the attack of hystero-epilepsy, having fully begun, is divided by Richer into distinct periods. Although these are seldom seen in perfection, it is necessary to have some clear idea of their [p. 300] phenomena in order to view the affection comprehensively. They were seen well developed in the case given. These periods are—(1) The epileptoid period; (2) the period of contortions and of great movements; (3) the period of emotional attitudes; (4) the period of delirium.
In the first or epileptoid period of the hystero-epileptoid attack, which receives its name from its resemblance to true epilepsy, various phases always reproduce themselves in the same order. Loss of consciousness and arrest of respiration, muscular tetanization in various positions, followed by clonic spasms, and, finally, muscular resolution, are the successive phenomena of this period, which usually lasts several minutes. Loss of consciousness is complete during this period. Muscular [p. 301] tetanization shows itself in movements large and small, sometimes of the whole body. The trunk may become as stiff as a bar of iron; the face is sometimes cyanosed, puffed; froth even appears, which it is well to remember, as this is considered by some as absolutely diagnostic of epilepsy. Many positions may be assumed. The important significant features of the tonic phase of period are muscular tetanization with loss of consciousness and respiratory spasm. In the clonic phase movements at first rapid and short, later larger and more general, ensue, and are accompanied by whistling inspiration, jerking expiration, hiccoughs, noisy deglutition. The phase of muscular resolution comes on, in which the patient completely relaxes; sometimes a true stertor occurs. The epileptoid period usually lasts altogether several minutes, the first two phases usually occupying about one minute.
In the period of contortions and great movements wonderful attitudes and contortions are observed in one phase, and in another great movements. One of the attitudes particularly fashionable with hystero-epileptics is the arched position, in which the body is curved backward in the form of an arch so as to rest only on the head and feet. Sometimes the patient may rest on the belly or side, the remainder of the body preserving its curved position; the body may indeed assume almost any strange and seemingly impossible attitude. The so-called great movements are executed by the entire body or by a part of the body only; they are of great variety; sometimes they are movements of salutation; sometimes the semiflexed legs are projected upward, etc. Often the phase of great movements is marked at its beginning by a piercing cry; loss of consciousness is not the rule.
The period of emotional attitudes or statuesque positions is the most dramatic stage of a highly dramatic disease. Hallucinations ravish and transport the patient: sometimes they are gay, sometimes they are sad. The dramatic positions assumed are in consonance with the patient's hallucinations. The patient reproaches, opposes, supplicates, is angry, is furious; she assumes positions of supplication on her knees, becomes menacing, and even strikes. In the great works of Bourneville, of Regnard, and of Richer many cases are related at great length and with vivid details. Camera and pencil are frequently called in to assist the pen in presenting scenes which read as if drawn from an exciting drama or novel. Among the expressions and attitudes which they have succeeded in photographing are those illustrating emotions of menace, appeal, amorous supplication, erotism, ecstasy, mockery, beatitude.
After the period of the emotional attitude consciousness returns, but only in part, and for a time the patient remains a prey to a delirium whose character varies. This delirium may be concerned with subjects the most varied; it may be gay, sad, furious, religious, or obscene. It is mingled with hallucinations; voices are heard; sometimes are seen personages who are known; sometimes the scenes are purely imaginary. During this fourth period the patients will sometimes make the most astounding statements and accusations. They will wrongfully charge theft, abuse, etc. upon others; they believe in the reality of their hallucinations, and, what is more important, they will sometimes persist in this belief after the attack is over. The third and fourth periods are sometimes confounded. When the four periods described succeed each other in [p. 302] order, they constitute a regular and complete attack of hystero-epilepsy.
By comparing the notes upon the case detailed with the description given of the typical hystero-epileptic attack, it will be seen that the different periods, and even the phases, can be made out with but little difficulty. After a few moments of convulsive movements and irregular breathing the patient was attacked with muscular tetanization, arrested respiration, and loss of consciousness. Tonic convulsions followed, and then immobilization in certain positions. Next came the clonic spasms and resolution. In the period of contortions the arched position is one more extreme than any represented by the illustrations of the French authors, although it is closely approximated by some of their illustrations. After this position of opisthotonos had been taken a succession of springing and lifting movements occurred, probably corresponding to the phase of great movements. The period of emotional attitudes was very clearly represented by the position assumed, the expression of countenance, and sometimes by the words uttered. Even the period of delirium was imperfectly represented by the mutterings of the patient, which were sometimes long continued after the attack.
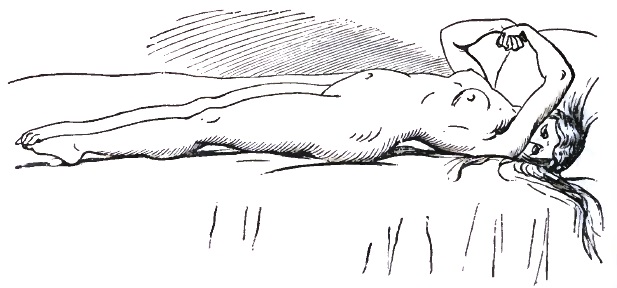
A beautiful illustration of one of the positions assumed by a hystero-epileptic is shown in Fig. 24 from Allan McLane Hamilton's treatise on Nervous Diseases. The patient, æt. eighteen, represented in the figure had suffered from hystero-epileptic attacks since the beginning of the menstrual period. Usually, she had severe but distinct epileptic seizures, and afterward an hystero-epileptic paroxysm. The muscles of her back were rigidly contracted in opisthotonos. Her arms were drawn over her chest, and her forearms slightly flexed and crossing each other. Her thumbs were bent in and covered by her other fingers, which were rigidly flexed. Her toes were also flexed, and her right foot presented the appearance called by Charcot le pied bot hystérique, or hysterical club-foot.
As has already been stated, hystero-epilepsy of irregular, imperfect, or abortive type is most commonly observed in this country, or at least in the Middle States, of which my own knowledge and experience are greatest. As has been demonstrated by Richer and Charcot, the irregular type may be of any form, from a paroxysm with a scarcely detectible convulsive seizure and scarcely recognizable loss of consciousness up to [p. 303] frightful attacks which from their terrible nature have been termed demoniacal, and in which occur the wildest phenomena of movement, frightful contortions and contractions, with grimaces and cries of fury and rage. Sometimes the movements show a violence beyond description. These frightful seizures are of extreme rarity in America. Sometimes attacks of ecstasy or attacks of delirium are the predominating or almost the only feature. The epileptoid attack, so far as my experience has gone, is the most prevalent variety of hystero-epilepsy. Epileptoid attacks are simply the result of the predominance and modification of the first or epileptoid period of the typical grave attack. Richer has described several varieties.
I have seen a number of cases of the epileptoid variety or other irregular forms. These cases have presented a few or many of the symptoms of grave hysteria, such as anæsthesia, analgesia, hyperæsthesia, blindness, aphonia, paralysis, contracture, etc., and have also had attacks of tonic and clonic spasm, with complete or partial loss of consciousness. The phenomena of the periods of contortions and great movements, of emotional attitudes, and of delirium have been, however, altogether or almost entirely absent. These epileptoid attacks have varied somewhat in different cases.
The following are the notes of three cases observed by me:8
8 Published in Journal of Nervous and Mental Disease, vol. ix., No. 4, October, 1882.
M——, æt. twenty-seven, a widow, admitted to the Philadelphia Hospital February 4, 1882, was married thirteen years before, when only fourteen years of age, and remained in comparatively good health for four years after her marriage, during which time she had three children, all of whom died in early infancy. Four years after her marriage, while carriage-riding, she for the first time had a spasm. According to her story, the seizure was very severe; she lost consciousness, and passed from one spell into another for an hour or more. She had a second attack within two weeks, and since has had others at intervals of from one week to three or four months. Four years ago she passed into a condition of unconsciousness or lethargy in which she remained for three days. On coming out of this state she found that the left half of her body was paralyzed and that she was speechless. In two weeks she recovered her speech and the paralysis disappeared. On June 15, 1881, she gave birth to a male child. On the night of the 16th she became delirious, and on the 17th she again lost her speech and had a paralytic seizure, the paralysis now affecting both legs. She recovered her speech in a few days, but the paralysis remained. Her babe lived, and with her was admitted to the hospital. He had had seven attacks of spasm at intervals of about a month. The patient's mother was for a time insane, and had been an inmate of an insane asylum for some months since her first epileptiform attack.
She was carefully examined on the day of her admission. She was bright, shrewd, and observant. She gave an account of her case in detail, and said she was a puzzle to the doctors. Both legs were entirely helpless; the feet were contractured in abduction and extension, assuming the position of talipes equino-varus; the legs and thighs were strongly extended, the latter being drawn together firmly. The left upper extremity was distinctly weaker than the right, but all movements were retained. She [p. 304] had no grasping power in the left hand. She was completely anæsthetic and analgesic below the knees, and incompletely so over the entire left half of the body. Pain was elicited on pressure over the left ovary and over the lower dorsal and lumbo-sacral region of the spine. Both knee-jerks were exaggerated.
I lectured on this patient at my clinic at the hospital, stating that I believed the case to be one of hystero-epilepsy, and only needed to see an attack of spasm to confirm the diagnosis. Up to this time she had not had a seizure since admission. She had, however, been complaining for several days of peculiar sensations in the head and of severe headache. She had also been more irritable than usual, and said that she felt as if something was going to happen to her. The same afternoon, Dr. Rohrer, the resident physician in charge of the patient, was sent for, and found her in a semi-conscious state. She did not seem to know what was going on around her, but was not in a stupor. Her pulse was 114 to 120; respirations were 20 to 22, regular. The corneæ responded on being touched. Some twitching movements of the eyeballs and eyelids were noticed; the thumb and forefinger of the left hand also moved, as if rubbing something between them.
In a few moments an epileptoid paroxysm ensued. She became unconscious and rigid. The lower extremities were strongly extended in the equino-varus position already described. The arms were extended at her sides, the wrist being partly flexed and rotated outward, the hands clenched. Her face, at first pale, became deeply congested. Her trunk became rigid in a position of partial opisthotonos. Brief clonic spasms followed, then resolution, the whole seizure not lasting more than from two to three minutes. She lay for a minute or two unmindful of anything or anybody, and then sat up and looked around wildly. She dropped back again and began to mumble, as if she wished to speak, but could not. Paper and pencil were given to her, and she wrote that she was conscious, but could not speak. Her temperature, taken at this time, was 99.8° F.
Attacks similar to the one just described occurred at irregular intervals for two days. On their cessation she was speechless, and the permanent symptoms already detailed—the anæsthesia, paralysis, etc.—were deepened. During the attacks but little treatment was employed; hypodermic injections of morphia and potassium bromide by the mouth were, however, administered. After the attack the valerianate of iron by the mouth, faradization of the tongue, and galvanization of the legs below the knees with weak currents, were ordered. Her speech returned in a week. For about a month she showed no other signs of improvement; then she began to mend slowly, gradually using her limbs more and more. On May 11, 1882, she was discharged, and walked out of the hospital with her child in her arms, apparently perfectly well. During the last month of her stay no treatment was used but mild galvanization every other day.
Mrs. A——, æt. forty-five, was seen by me in consultation. For some months at her menstrual period she had been out of sorts. At times she had had hallucinations of sight. For several weeks she had been troubled more or less with a feeling of numbness and heaviness in the left arm and leg, particularly in the latter, and also with diffused pain in the head and [p. 305] a sensation of aching and dragging in the back of the neck. For three weeks, off and on, she had had diarrhœa, which had weakened her considerably. She awoke one morning feeling badly and yawning every few minutes. She passed into a condition of unconsciousness with attacks of spasm. I did not see her on this the first day of her severe illness, but obtained from the physician in attendance some particulars as to the character of her seizures. Evidently the condition was similar to that presented by the last case, that described by Richer as the epileptoid status, in which tonic and clonic spasm and resolution are repeated again and again. Attack after attack occurred for nine or ten hours, sometimes one immediately following another, sometimes an interval of several minutes or of half an hour or more intervening. Respiration was partially arrested. Tonic spasm predominated; the limbs became rigid in various positions; sometimes the neck and trunk were strongly bent backward, producing partial opisthotonos. While the body and limbs remained tetanized they were thrown into various positions (clonic phase of an epileptoid attack). Although she answered questions addressed to her by her physician between the spells, she did not recognize him until evening, after the spasms had ceased, and then was not aware that he had been in attendance during the day, although he had been with her almost constantly. Leeching and dry cupping to the back of the neck were employed, and potassium bromide and tincture of valerianate of ammonia were given.
Early on the morning of the next day she had another attack of unconsciousness and spasm, in which I had the opportunity of seeing her. The spasm amounted only to a slight general muscular tetanization. The whole attack lasted probably from half a minute to a minute. The following day, at about the same hour, another paroxysm occurred, having a distinct but brief tonic, followed by a clonic, phase, in which both the head and body were moved. The next day, also at nearly the same hour, she had an attack of unconsciousness or perverted consciousness without spasm. She had a similar seizure at 4 P.M. For two days succeeding she had no attacks; then came a spell of unconsciousness. After this she had one or two slight attacks, at intervals of a few days, for about two weeks.
Between the attacks the condition of the patient was carefully investigated. On lifting her head suddenly she had strange sensations of sinking, and sometimes would partially lose consciousness. She complained greatly of pain in the head and along the spine. Her mental condition, so far as ability to talk, reason, etc. was concerned, was good, but any exertion in this direction easily fatigued her and rendered her restless. She had at times hallucinations of animals, which she thought she saw passing before her from left to right. The left upper and lower extremities showed marked loss of power. The paralysis of the left leg was quite positive, and a slight tendency to contracture at the knee was exhibited. She was for two weeks entirely unable to stand. The knee-jerks were well marked. Left unilateral sweating was several times observed.
A zone of tenderness was discovered in the occipital region and nape of the neck, and she had also left ovarian hyperæsthesia. Left hemianæsthesia was present, head, trunk, and limbs being affected. She complained of dimness of vision in the left eye, and examination by the [p. 306] attending physician and myself showed both amblyopia and achromatopsia, she was unable to read print of any size or to distinguish any colors with the left eye, although she could tell that objects were being moved before the eye. A distinguished ophthalmologist was called in consultation. An ophthalmoscopic examination showed a normal fundus. Each eye was tested for near vision. It was found that she could read quite well with the right eye, and not at all with the left. While reading at about sixteen inches a convex glass of three inches focus was placed in front of the right eye, but she still continued to read fluently. A few minutes later, however, on retesting, she could not read or distinguish colors with the left eye. Sometimes toward evening her feet would become slightly œdematous. Examination of the urine showed neither albumen nor sugar. The heart-sounds were normal.
Owing to the apparent periodicity of the attacks quinine in large doses was administered, and seemed to act beneficially. In addition, valerianate of zinc and iron, strychnia, and other nerve-tonics were used in her subsequent treatment. Applications of faradic electricity, both with the metallic brush and the moist sponges, were made every other day. She was persistently and strongly encouraged as to the certainty of her recovery. Her paralysis, anæsthesia, etc. gradually disappeared, and in little more than two months she was able to leave home and go to the country. She has since remained well, but is more easily fatigued than formerly, and does not feel as strong in the left side of her body as she did when in perfect health. At her menstrual period she becomes very nervous.
M——, æt. twenty-three, a well-educated young lady,9 in the autumn of 1880 had nursed her mother faithfully through a serious illness. She became anæmic and nervous. Choreic twitchings and occasional slight spasms were the first symptoms that alarmed her family. The spasms came on apparently from any over-exertion. Gradually they became a little more severe in character. Under rest-treatment, with gentle massage, tonics, and steady feeding, in six weeks she greatly improved. A few weeks later, however, she again relapsed, and became worse than she had ever been. The spasms returned with greater force and frequency. She became unable to walk, or could only walk a few steps with the greatest difficulty, although she could stand still quite well. On attempting to step either forward or backward her head, shoulders, hips, and trunk would jerk spasmodically and she would appear to give way at the knees. No true paralysis or ataxia seemed to be present, but locomotion was impossible, apparently because of irregular clonic spasms affecting various parts of her body. Eventually she became extremely hypersæsthetic in various regions (hysterogenic zones), along the spine, beneath the breasts, in the ovarian area, etc. The slightest pressure or any applications of heat or cold, electricity, etc. would generally bring on an attack of spasm.
9 This patient was for a long time under the professional care of George McClellan of Philadelphia, who has kindly furnished me with some notes. I shall simply give an outline sketch of the case, describing particularly her epileptoid attack. For several weeks, during the absence of McClellan from the city, she was attended by M. O'Hara, and with him I saw her frequently in consultation.
While trying to apply galvanism on one occasion she suddenly complained of nausea, and her expression changed, becoming somewhat fixed. [p. 307] Her face became flushed, her limbs and body rigid. The head and body were thrown backward to a moderate extent. Next, the shoulders were drawn upward, the head appearing to be sunk between them; the arms were found to be rigidly extended at her sides, the wrists partly flexed, and the fingers clenched; the legs also were spasmodically extended, the thighs drawn together, and the feet in the equino-varus or hysterical club-foot position. Phenomena like those described above as visceral spasm now were observed. The chest, and even the abdomen, were lifted up and down rapidly, and the respiration became quick, irregular, and apparently very difficult. Consciousness seemed to be impaired, but not absolutely lost. The symptoms just described took about one minute for their exhibition. Muscular relaxation now occurred, and an interval of calm, lasting about two minutes, followed, during which the patient spoke, answering one or two questions addressed to her. After the brief period of repose, however, another phase of the attack came on. In this the heaving movements of the body and what appeared to be intense respiratory spasms were the chief features. This portion of the attack endured scarcely a minute; the patient came to quickly, and was able to converse. In general, her attacks were of a similar character.
The drugs used included bromides, iodides, strychnia, chloride of sodium and gold, zinc salts, iron, etc. etc.; her condition vacillating, sometimes better, sometimes worse. She was finally placed in bed by McClellan, and an extension apparatus was employed, under which treatment, in a little more than one year from the time she was first attacked with spasm, she recovered.
The permanent or intervallary symptoms of hystero-epilepsy are in the main the phenomena which have been described when speaking of the prodromes of this affection. They are, indeed, the whole train of symptoms—the mental or psychical disorders, the motor, sensory, reflex, vaso-motor, and isolated phenomena—which have been described under special heads when considering the general symptomatology of hysteria. The full-fledged case of hystero-epilepsy is hysteria with a full array of special permanent hysterical manifestations, and the great paroxysm superadded. Certain phenomena are, however, more prominent and of much more frequent occurrence. Among these are paralysis or paresis, either of the unilateral or paraplegic variety; hemianæsthesia, including anæsthesia of all the senses; and contractures, particularly in the lower extremities.
DURATION AND COURSE.—The duration and course of hystero-epilepsy are very uncertain; most cases last many years. In a few instances the hystero-epileptic attacks are all from which the patient suffers; even in the cases of long duration the general health does not appear to become greatly impaired.
DIAGNOSIS.—To arrive at a correct diagnosis between hystero-epilepsy and epilepsy is sometimes very difficult. The fact that the patient is a male does not decide for epilepsy. In making this diagnosis close attention should be given to—1, The history and the causes of the disease; 2, the physical and mental condition of the patient; 3, above all, the phenomena of the spasmodic attacks.
In hystero-epilepsy a careful study of the history of the case will often [p. 308] elicit a moral cause. The patients rarely injure themselves seriously by falling, whereas in true epilepsy they often suffer from severe injuries. The mental and physical health of a person suffering from hystero-epilepsy differs widely from that of the true epileptic. In hystero-epilepsy the number of attacks has little or no apparent influence on the patient's mental or physical condition. Little or no deterioration of the mind occurs. The memory is not much impaired. Hystero-epileptics are usually well nourished and frequently of good physique. This is not the case in true epilepsy; the number of attacks has a decided effect on the patient's mental condition. The demented appearance of the old epileptic is well known, whereas in the hystero-epileptic nothing in physiognomy or carriage indicates that the patient has been suffering from any disease. It cannot be said that all epileptics have no mental power, but some deterioration of the mind usually occurs, and becomes well marked as the case progresses.
The paroxysms in epilepsy are very well marked, especially if it is epilepsy of the grave form. They are often ushered in with a scream. The patient suddenly falls, and at times is severely injured. The convulsion is generally violent, rapidly alternating from clonic to tonic spasm, without special phases or periods. Complete and profound loss of consciousness, with great distortion of face and eyes, is present. The tongue is frequently bitten. After the attack the patient passes into a deep stupor. In hystero-epilepsy usually the seizure does not begin with a scream or sudden fall, the convulsion has periods and phases, and the tongue is not bitten.
It is said that in hystero-epilepsy there is no loss of consciousness, but this is not strictly true. This point is the most difficult one for physicians to clear up in arriving at a diagnosis, as in many textbooks complete loss of consciousness is laid down as the strongest evidence of epilepsy. Loss of consciousness does occur in hystero-epilepsy, particularly in certain varieties. Richer says that the loss of consciousness is complete during the entire epileptoid period in a case of the regular type. To decide as to consciousness or unconsciousness is not as easy as might be supposed. Varying degrees of consciousness may be present. At times in hystero-epileptic attacks the patient may respond to some external influences and not to others. Consciousness is perverted or obtunded often, and it is hard to decide whether the patient is positively and entirely unconscious of her surroundings. In epilepsy the loss of consciousness is profound and easily determined. In regard to the distortion of the face and eyes, this sign is usually absent in hystero-epilepsy, as in the German Hospital case, in which the patient had a series of violent seizures lasting two hours, with marked opisthotonos, yet the facial expression remained calm and serene throughout.
In hystero-epilepsy the attacks are rarely single; usually they are repeated, constituting the hystero-epileptic status. They are more frequently repeated than in epilepsy, although it is of course well known that there is an epileptic status terrible in character. In a series of hystero-epileptic attacks usually the seizures come on in rapid succession, the interval being brief. These series are apt to last for hours or days. The attacks that compose a series in hystero-epilepsy vary in duration and in violence. At first they are of violent character; toward the end [p. 309] the seizures may gain in extent, but they are likely to lose in intensity.
Charcot and Bourneville make a strong diagnostic point between hystero-epilepsy and true epilepsy of the fact that in epilepsy there is a peculiar rise of temperature during the convulsion, even to 104° F., whereas in hystero-epilepsy the temperature is nearly or quite normal.
Arrest of attacks by ovarian compression in females, and by nerve compression, nitrite of amyl, and the application of electric currents, can be brought about in hystero-epilepsy, and not in epilepsy. A study of the effect of bromides may assist in arriving at a diagnosis. The action of bromides, drugs which are often used in both affections, favors the opinion that the two diseases are distinct. Bromides, according to Charcot and Richer, so effective in epilepsy, are without effect in hystero-epilepsy. Dujardin-Beaumetz, however, on the other hand, declares that “who says hysteria says bromides,” and also that at the present time there is not an hysterical patient but has taken bromides, the bromide of potassium being most frequently used. The truth is, that bromides may be useful for temporary purposes, for certain phases and symptoms of the disease, but produce no radical permanent improvement in the disease hystero-epilepsy.
D. Webster Prentiss,10 in reporting a case, gives some good points of distinction between real and hysterical tetanus, which is practically hystero-epilepsy. In his case, which was hysterical, the attack was ushered in by noise in the ears, deafness, and blindness, whereas in true tetanus and strychnia-poisoning the senses are preternaturally acute. There was unconsciousness during the paroxysm, which does not occur except just before death in the other affections. The eyes were closed during the spasms; they stare wildly open in the other diseases. The patient had long, uninterrupted sleep at night; in true tetanus no such relief comes until convalescence.
10 American Journal of the Medical Sciences, 1879.
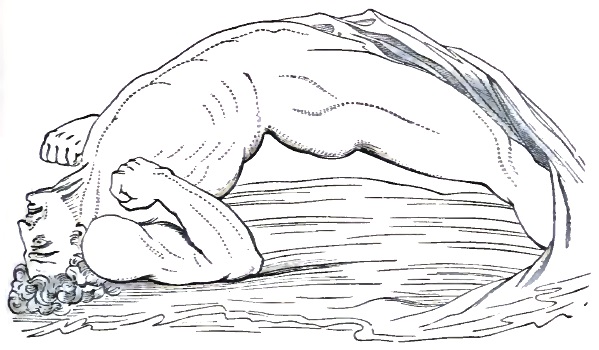
The figure is a representation of the opisthotonos of tetanus.11 It is the sketch of a soldier, struck with opisthotonos after having been [p. 310] wounded in the head; and in connection with it I will briefly call attention to the points of differential diagnosis as given by Richer, and which have been confirmed by my own observations. In the opisthotonos of tetanus the contraction of the face and the peculiar grin are distinguishing points, and are well represented in Bell's sketch. In the hysterical arched position, while the jaws may be strongly forced together, the features are most often without expression. The contracture of the face and the distortion of the features will be met with more often in the other varieties of contortion. The curvature of the trunk differs but little in the two cases, but the abdominal depression observed in the sketch of Bell is far removed from the tympanitic appearance present in the majority of hystero-epileptics. In the tetanic cases the patient rests only on the heels, while in the hysterical cases the knees are slightly flexed, and the patients are usually supported on the bed by the soles of the feet.
11 From Sir Charles Bell's Anatomy and Physiology of Expression as connected with the Fine Arts.
Hystero-epileptics are often suspected of simulation. Richer refers to many facts which seem to throw out conclusively the idea of simulation. Among these are the results obtained by æsthesiogenic agents, the experiments in hypnotism, where many of the results produced could not be simulated. Some English authors—and among them notably the physiologist Carpenter—have endeavored to find the explanation of the results obtained by the æsthesiogenic agents in a special action of the moral on the physical nature which they designate expectant attention. While the reality of the action of expectant attention in certain cases will not be denied, it cannot be invoked to explain satisfactorily all the phenomena. The patients are not aware of the results sought; which, indeed, in some cases, are contrary to the expectations of the observer himself.
PROGNOSIS.—A few cases of hystero-epilepsy get well, either with or without treatment, in a short time. Some cases, which in addition to the grave attack have had in the intervals the other striking symptoms of major hysteria, such as hemianæsthesia and contractures, get well only after many months or years; some never recover, although, as a rule, they do not die from anything directly connected with the disease, but from some accident or more commonly from some intercurrent disorder. Cases supposed to be cured often relapse. The patient may be apparently well for months, or even years, when under some exciting cause the old disorder is again aroused. On the whole, the prognosis is more serious the longer the case has endured. Family history and environment have much to do with determining the prognosis.
TREATMENT.—In considering the treatment of hystero-epilepsy I will, in the main, confine my attention to a discussion of the methods of managing and treating the convulsive seizures. With reference to the numerous special phenomena of this disease, the directions given and the suggestions made in the general article on Hysteria will be equally applicable in this connection.
Ruault12 has recently recommended compression of a superficial nerve-trunk in order to terminate an attack of hysteria or hystero-epilepsy. The face being always accessible, he prefers making pressure on the infraorbital nerves as they emerge from their foramina, but he has also [p. 311] compressed the ulnar nerve behind the inner condyle of the humerus. In a brief note to the Philadelphia Neurological Society, made Feb. 23, 1884, I called attention to the value of strong nerve-pressure for the relief of hysterical contracture, and can confirm from several successes Ruault's recommendation for the employment of the same measure to avert convulsive attacks.
12 La France médicale, vol. lxxxvi., p. 885.
Thiery13 of the Saint Pierre Hospital, Brussels, arrests paroxysms by what he calls torsion of the abdominal walls. He grasps in his hands the walls of the abdomen and imparts to them a certain kind of torsion, which he gradually increases. This treatment is practically the same as the deep ovarian pressure of Charcot. This compression of the ovary on the side of the seat of the lesion ordinarily will arrest immediately the convulsions. The patient is extended horizontally, and the physician plunges the closed fist into the iliac fossa, often using great force to overcome the muscular resistance. Poiner has invented an apparatus called a compressor of the ovaries, which can sometimes be used with advantage.
13 Medical and Surgical Reporter, Oct. 7, 1876.
Nitrate of amyl is undoubtedly of value in averting grave hysterical attacks—convulsions, trance, ecstasy, pseudo-coma, mania, etc. It is frequently used with marked success. Its action was studied on a vast scale at La Salpêtrière. The convulsions usually stop almost immediately after one, two, or three inhalations. It is to be preferred to inhalations of chloroform or ether.
Nitro-glycerin can be used in the treatment of the hystero-epileptoid convulsions. Notes of a very interesting case of hystero-epilepsy in which this remedy was successfully employed have been furnished me by David D. Stewart of Philadelphia. The case was one of hystero-epilepsy with combined crises. Amyl nitrate on several occasions broke the convulsive attack, but the patient did not completely regain consciousness. Stewart was called in during an attack, and found that the patient had been unconscious for an hour and a quarter. He gave her hypodermically three minims of a 1 per cent. solution of nitro-glycerin, and another injection after an interval of about eight minutes. She became conscious within one minute after the second injection. After this she had two seizures, both of which occurred on the same day, and yielded with remarkable promptness to a few minims of nitro-glycerin given by the mouth. She was put on three minims three times a day of this drug, the dose being gradually increased. Sufficient time has not elapsed to report as to the effect of the drug given during the intervals.
Strong faradic currents, applied with metallic electrodes to the soles of the feet or to the spine, are occasionally efficacious. The galvanic current to the head has been extensively employed in the service of Charcot to arrest hysterical and hystero-epileptic attacks of the grave variety. One electrode is applied to the forehead, the other to any convenient place upon the body, as the leg, the ovarian region, or the spine. The current is applied continuously for several minutes, or voltaic alternations are made. This method has been used with success in a few instances, but should never be resorted to by a physician uncertain of his diagnosis or one practically unfamiliar with the powers and properties of the electrical current.
[p. 312]The question of oöphorectomy for the relief of hystero-epilepsy is one of increasing importance in these days of major surgery. At the meeting of the American Neurological Association (June, 1884) G. L. Walton read a paper14 in which he concludes that hysteria is sometimes set up by ovarian irritation, and can be relieved by removing the offending organ. He cited a single case. Carsten15 concludes that it is criminal neglect not to perform Battey's operation in cases which fail to be benefited by other treatment. In the discussion which followed the reading of this paper the subject was well traversed by Spitzka of New York, Putnam of Boston, Putnam-Jacobi of New York, and others. Spitzka referred to one case of Israel's of Breslau, in which a patient was cured of hystero-epilepsy by a sham operation—a superficial incision in the parietes of the abdomen. Under the title of castration in hysteria the Lancet16 tells of an hysterical patient who had suffered for years from obstinate vomiting and severe ovarian pain. She became extremely weak, and finally consented to spaying as the only hope. The operation—performed under chloroform with antiseptic precautions—was a mockery, the skin only being incised; she was, however, perfectly cured of her hysterical symptoms.
14 “A Contribution to the Study of Hysteria as Bearing on the Question of Oöphorectomy.”
15 Quoted by Walton from American Journal of Obstetrics, March, 1883.
16 Vol. ii. p. 588.
In two clinical lectures published in the Philadelphia Medical Times17 I have given the histories of two cases of hystero-epilepsy in which oöphorectomy was resorted to for hystero-epilepsy. In the first of these cases, in which clitoridectomy was also performed, nymphomania, which was a distressing symptom, was benefited, but even this was not completely cured. The following is the patient's own statement: “Since the removal of the ovaries I have been able to control the desire when awake, but at times in my sleep I can feel something like an orgasm taking place. My experience leads me to say that my cure (?) is not due to the absence of the ovaries; there is no diminution of the sexual feeling. There would be as much excitement of the parts if the clitoris were still there. If my will gave way, I would be as bad as ever.” Her general mental and nervous condition is much the same as before the operations. She is still dominated by morbid ideas, still unable to take up any vocation which demands persistence, and still the frequent subject of hystero-epileptic seizures.
17 April 18 and May 30, 1885.
The second of these cases was a young girl about seventeen years old who had never menstruated. She had had epileptic or hystero-epileptic seizures for several years. An operation was performed in which the ovaries and Fallopian tubes were removed. Twelve days after the operation, from which she made a good recovery, she had four convulsive seizures. She had several attacks subsequently, and then for a considerable period was exempt. She had, however, acute inflammatory rheumatism, with endocarditis and valvular trouble. About seven months after the operation she had several severe convulsions with loss of consciousness, and died about a year after the operation, having had many severe seizures during the last few weeks of her life.
There is no warrant either in experience or in a study of the subject for spaying hysterical girls who have never menstruated. In a case [p. 313] diagnosticated as hysterical rhythmical chorea removal of the ovaries was advised by a distinguished specialist. The girl's trouble came on at about the age of thirteen years. She had never menstruated properly, although on one occasion, after several weeks of electric treatment, she had a slight show for a few days. It was proposed to remove the ovaries in this case on some general principle of given hysterical trouble; the ovaries must go. In this case, as in the last, it would have been far better to have put in a good pair of ovaries, or to have developed these rudimentary organs into health and activity.
With reference to oöphorectomy for hystero-epilepsy or any form of grave hysteria it may be concluded—1, It is only rarely justifiable; 2, it is not justifiable in the case of girls who have not menstruated; 3, when disease of the ovaries can be clearly made out by local objective signs, it is sometimes justifiable; 4, it is justifiable in some cases with violent nymphomania; 5, the operation is frequently performed without due consideration, and the statistics of the operation are peculiarly unreliable.
When we come to consider the treatment of the disease hystero-epilepsy, the practical importance of the distinction between this affection and true epilepsy becomes apparent. Cures of hystero-epilepsy are not rare. The original cases here reported have all apparently recovered. Grave hysteria is sometimes cured spontaneously, either by gradual disappearance with the progress of age, or suddenly because of some violent impression or under the influence of unknown causes. One of the worst cases in the service of Charcot has shown a gradual diminution of the hystero-epileptic manifestations with the advance of age. In another case under the influence of strong moral impressions the disease disappeared at a stroke. The affection, however, should not be abandoned to nature, as treatment is often of value.
The hydrotherapeutic method of treatment has been found of the greatest service. Hydrotherapy must be methodically employed by experienced hands. A number of cases cited by Richer were cured at hydrotherapeutic institutions. Limited success has followed the use of metallo-therapy. Besides metallic plates, the same results may be obtained with other physical agents, to which have been given the name of æsthesiogenic agents. Among these are feeble electric currents, vibrations of a tuning-fork, static electricity, etc.
Static electricity has a position of undoubted importance in the treatment of hystero-epilepsy in some of its phases. Those who have walked in the wards and visited the laboratories of Salpêtrière will recall the enormous insulated stools to which are brought troops of hystero-epileptic patients, who, to save time, are given a vigorous simultaneous charge of electricity. Even this wholesale plan of treatment is sometimes markedly efficacious. Vigoroux recommends static electricity as an æsthesiogenic agent, and regards it as the most valuable of all agents of this character.
Those drugs should be resorted to which have a tonic influence on the nervous system. Potassium bromide, as has already been indicated, is not efficacious. More is to be hoped from tonics and antispasmodics, such as valerian, iron, salts of silver, zinc, copper, sodium, and gold chlorides, etc. Good hygienic influences, moral, mental, and physical, are of the utmost importance.
DEFINITION.—Catalepsy is a functional nervous disease characterized by conditions of perverted consciousness, diminished sensibility, and especially by muscular rigidity or immobility, which is independent of the will, and in consequence of which the whole body, the limbs, or the parts affected remain in any position or attitude in which they may be placed.
Catalepsy sometimes, but not frequently, occurs as an independent disease; that is, the cataleptic seizure is the only abnormal phenomena exhibited by the patient. It is sometimes present, although also rarely, in organic disease of the nervous system. It has been noted, for instance, as occurring in the course of cases of cerebral hemorrhage, softening of the brain, abscess, tumor, and tubercular meningitis. One case is referred to by C. Handfield Jones in which it seemed to be due to intracranial epithelioma. As commonly seen, it is a complication, or perhaps, more properly speaking, a form of hysteria—hystero-catalepsy.
SYNONYMS.—Some of the many synonyms which have been used for catalepsy are Catochus, Morbus attonitus, Stupor vigilans, Synochus, Eclipsis, and Hysteria cataleptica. Trance and ecstasy are discussed sometimes as synonymous with catalepsy, but they will be considered as separate affections, as they have certain distinctive features. Catalepsy, trance, ecstasy, hystero-epilepsy, and other severe nervous disturbances may, however, all appear in the same patient at different times or at different stages of the same seizure.
With reference to the term catochus (κατοχη, from κατεχω, I take possession of), which has been used as synonymous with catalepsy, Laycock1 points out what he considers to be the proper use of this word, differentiating two cataleptic conditions, which he designates as the tetanic and the paralytic states. Catochus is the tetanic form, in which the trunk and limbs are rigidly extended and consciousness is abolished. Catalepsy proper is Laycock's paralytic form, although the term paralytic, as here applied, is by no means happy. It is the form characterized by the peculiar and striking symptom known as waxen flexibility (flexibilitas cerea)—a condition in which the limbs or parts are passive and are capable of being moulded like wax or lead pipe. Rosenthal would not consider any case as one of genuine catalepsy if this waxen flexibility was absent. I do not think that this rigorous criterion should always be imposed, [p. 315] although it might perhaps be better to apply the term cataleptoid to all cases which do not present true wax-like flexibility. The distinction sometimes made between catalepsia vera, or true catalepsy, and catalepsia spuria, or false catalepsy, is practically that indicated between Laycock's two forms. According to Charcot and Richer,2 the flexibilitas cerea is not present in the cataleptic state of hypnotism.
1 A Treatise on the Nervous Diseases of Women, by Thomas Laycock, M.D., London, 1840.
2 Journal of Mental and Nervous Diseases, Jan., 1883.
HISTORY.—The word catalepsy was used by Greek writers in its etymological signification of a seizure or surprise. Hippocrates described catalepsy; Galen, Aëtius, Rondeletius, and Fernelius have all related cases; Aëtius has left an accurate description of both catochus and catalepsy. In 1683, Laurence Bellini published a quarto volume on various subjects, one of which was catalepsy. From time to time interesting cases of catalepsy have been reported by medical writers. One of the best is that recorded by John Jebb in 1782, and quoted by Chambers in Reynolds's System of Medicine. The researches in hypnotism during the present century, and particularly those of Heidenhain and of Charcot and Richer, have thrown new light on many cataleptic phenomena.
ETIOLOGY.—In catalepsy, as in hysteria, insanity, and many neuroses, inheritance frequently plays a predisposing part. Eulenburg places it in the large group of diseased conditions designated by Griesinger constitutional neuropathies. The cataleptic of one generation may be the descendant of the insane, the epileptic, the syphilitic, or the alcoholized of a former. Catalepsy is particularly likely to occur in families which have a history of insanity or drunkenness. Of the cases detailed or alluded to in this paper, more than a majority had a clear neurotic history. Catalepsy, like hysteria, occurs with some frequency among the tuberculous.
Age plays some part in the development of catalepsy. It is of most frequent occurrence between the ages of fifteen and thirty, but has been observed at all ages. It is of unusual occurrence in very early childhood, but A. Jacoby,3 Clinical Professor of the Diseases of Children in the College of Physicians and Surgeons in New York, reports a case of well-marked catalepsy in a child three years old. This patient, a girl, was admitted to the Mt. Sinai Hospital, New York, in September, 1879. She had whooping cough and some symptoms of typhoid fever. After she had been in the hospital three weeks choreic twitchings of the eyes and eyelids, with divergent strabismus, were observed. Examining her, it was found that she was cataleptic; her arms and legs would remain in any position in which they were placed; she would drop the uplifted arms slowly when commanded; sensibility to contact, pain, and temperature were entirely lost, and the skin and patellar reflexes were diminished. Her appetite was ravenous, and urine was passed in large quantities. Other phenomena and details of cataleptic symptoms, which continued for about a month, are recorded by Jacoby. The child recovered, but remained weak and anæmic for a long time.
3 American Journal of Medical Science, N. S. lxxxix., 1885, p. 450.
Monti4 records eleven cases of catalepsy met with in children, male and female in about equal numbers, of from five to fifteen years, the average age being nine years. Eulenburg speaks of catalepsy at five [p. 316] years of age, and quotes Schwartz, who noticed in a boy seven years old, in consequence of rough treatment, first a choreic condition, which later passed into catalepsy. Lloyd's case, to be detailed later, also studied by myself at the University Hospital, was in a boy eight years old. B. L. Hovey5 of Rochester, New York, reports an interesting case of catalepsy in a boy eight years old.
4 Gerhardt's Handb. d. Kinderk., vol. v., L. P., 186 et seq., quoted by Jacobi.
5 The Hospital Gazette, 1879, vi. p. 19.
C. E. de Schweinitz of Philadelphia, Ophthalmic Surgeon to the Children's Hospital and Prosector of Anatomy at the University of Pennsylvania, has kindly put into my hands the unpublished notes of a highly interesting case of catalepsy or automatism at command, or of both, in a child two and a half years old. I will give this case in full, chiefly in the language of De Schweinitz, because it is, so far as I know, the youngest case on record. Some of the tests which were applied in this case are among the most useful which can be resorted to in determining how far the phenomena presented are genuine or induced, simulated, or imitated:
The patient was a girl aged two and a half years, who had recently recovered from an attack of diphtheritic conjunctivitis. During the period of her convalescence the attending nurse called attention to the unusual position assumed by the child while sleeping—viz. a lateral decubitus, the head raised a short distance from the pillow, and the forearm slightly elevated and stretched out from the body, the muscles at the same time exhibiting marked tremulousness. A series of trials readily demonstrated that the child when awake could be placed in any position compatible with her muscular power, and that she could thus remain until released. She was placed, for instance, in the sitting posture, the arm brought at right angles to the body, the forearm at right angles to the arm, and the hand at right angles to the forearm, both legs raised from the bed, and the head bent backward. This position, a most uncomfortable and difficult one to preserve, would be maintained until the little subject dropped from sheer exhaustion. Flexion and extension of each separate finger were easily produced, and the fingers remained until replaced in the positions in which they had been fixed. At the beginning the child's mind was sluggish, although she asked for food and made known her various wants. How far she appreciated surrounding objects could not be accurately ascertained, inasmuch as the previous disease of her eyes had left her with a central corneal macula on each side, rendering her almost sightless in one eye and with but indifferent object-perception in the other. Voluntary motion was preserved, and she sat up, turned, and moved whenever she pleased, but most often when at rest at this stage maintained somewhat of the position before described which during sleep first attracted attention to this condition.
In conjunction with Morris Lewis an examination of the cutaneous sensibility and reflexes was made, which showed diminished sensibility in the legs and thighs, but not higher up, where the pricks of the instrument were quickly appreciated. Her knee-jerk was apparently absent on the right side and present on the left; but this test, always most unsatisfactory in children, yielded no certain evidence and constantly gave contradictory results. Scratching the skin of the soles of the feet, legs, thighs, and abdomen with a pointed instrument was [p. 317] followed by marked reflex movements. Electro-muscular contractility was everywhere preserved. The child at this time was feeble and anæmic, but her appetite was good—not depraved nor voracious; the tongue was clean, the bowels regular. The urine was of a light amber color, specific gravity 1020, free from albumen and sugar.
As the nutrition of the child improved, it was found that the curious positions could be produced by word of command as well as by manipulation. In short, within six weeks after the first manifestations of this disorder, as a usual thing the little patient ate, slept, and played as a normal child should do, but could at any time be thrown into this cataleptoid state. Her one dominant idea apparently was to maintain the position in which she had been placed. She was often turned into some constrained posture, and all attendants absented themselves from the room and left her to her own devices; but no attempt on her part was made to in any way change her attitude. If at dinner-time a bowl of broth was placed before the patient, she would begin to eat with great relish, but if the spoon was taken away and her hands raised over her head, they would so remain, the child making no effort to return to her meal, although the bowl stood before her and all watchers again retired from the room. This experiment was suggested by H. C. Wood, who examined the child with me. To show how completely her consciousness was occupied with one idea of maintaining any position in which she had been placed, the following additional experiments may be quoted: If she was put into a sitting position, as in the act of supplication, with her hands folded and arms extended, and then given a sudden push sufficient to overthrow her equilibrium, the arms would be quickly and intuitively thrown out to protect her from the impending fall, but, the fall accomplished, they would as quickly be returned to their former position. If a heated silver spoon was gradually brought in contact with her extended hand, an expression of pain would pass the child's face, perhaps a cry escape her, and the injured member be rapidly withdrawn, but again almost immediately returned to its original place. It seemed as if the idea of fixity in a certain position which occupied the child's mind was suddenly disturbed by another outside impression, but, being dominant, it quickly drove away the intruder and the former state was restored. At this time the phenomena noted were somewhat in accord with those induced by the mesmeric process, inasmuch as the consciousness seemed largely given up to the one impression operating at that time—i.e. the maintenance of certain fixed positions. Unlike this condition, however, the readiness to receive new impressions, and the complete abeyance of those senses not operating was wanting, for, as seen above, the new impression only for a moment disturbed the child's one idea, to which she quickly returned; nor was there any true absence of sensibility, as was evidenced by the result from touching her with a heated spoon.
As time wore on, a new phase of this condition became evident. The induced manifestations seemed to act the part of some amusement to the child, and the complete absence of volition which had been an early characteristic phenomenon was not now so marked a feature. Thus, if, after the experimenter had for a time moulded and twisted the child into various shapes, he would suddenly leave the room, the little subject [p. 318] would cry lustily, as a child does when suddenly deprived of its playthings, although, curiously enough, no matter how hard she cried, she would not release herself from the last position in which she had been left. Often during any series of observations that were being made it was noted that a faintly-amused look played about her lips, which speedily gave way to a fit of crying when the performance stopped. The hand which, when formerly placed in any position, remained a perfectly motionless and passive object, was now seen slightly to change its place, move the fingers, or the like—an observation first made by A. K. Meigs while examining the patient. The house-physician, Nathan P. Grimm, took great care and interest in observing the case.
De Schweinitz, in reporting the case, briefly discusses the probable cause of the phenomena exhibited. He discards the views that either fear of the experimenter, such as is shown by a trained animal, or the partial blindness of the child, was responsible for the manifestations. He believes that a direct relation existed between the phenomena and the state of the child's nutrition. The more run down her system was, the more nearly did the nervous phenomena resemble those of true catalepsy. Evidently, her symptoms were partly cataleptic and partly phenomena of automatism at command, similar to those which have been observed in hypnotic experiments, and which will be alluded to later.
Catalepsy is of more frequency in the female than in the male sex, but the statistics are not sufficient to give any exact ratio.
The periods of puberty and early menstruation and of pregnancy furnish the most favorable opportunities for the development of cataleptoid seizures in predisposed individuals. In 3 of 10 cases observed by Landouzy catalepsy appeared to be developed in consequence of the sudden suppression of menstruation; in a fourth it occurred in a young girl after a dysmenorrhœa with chronic phlegmasia of the genitals. Masturbation is sometimes mentioned as a cause, particularly in boys.
Reflex irritation undoubtedly often acts as an exciting cause of catalepsy. Preputial irritation, relieved in part by circumcision, was present in the case of Lloyd, and has been noted by others. Handfield Jones mentions a case, recorded by Austen in his work on General Paralysis, in which the cataleptic seizure was, to all appearances, due to fecal accumulations. The attack disappeared promptly after an enema had thoroughly operated.
Briquet believed that catalepsy, when it did not follow upon organic disease, was ordinarily the result of moral causes, such as vivid and strong emotions—fear, chagrin, indigestion, anger, or profound and prolonged meditation. He refers to the able and curious thesis of Favrot,6 who states that in twenty cases in which the causes of the malady were indicated it had been always the result of a moral affection. A magistrate insulted at his tribunal, seized with indignation, is suddenly taken with catalepsy, etc. According to Puel, its causes are always depressing moral affections, as chagrin, hatred, jealousy, and terror at bad treatment. Unrequited love is set down as a cause, but what has not unrequited love produced? Jones mentions a case which occurred in a man sixty years old on the sudden death of his wife.
6 “De la Catalepsie”—Mémoire couronné par l'Académie de Médecine, Mémoires de l'Académie de Médecine, Paris, 1856, t. xx. p. 409, A. 526.[p. 319]
Cullen believed that catalepsy was always a simulated disease; he preferred, therefore, to place it as a species of apoplexy. Temporary catalepsy may, according to Rosenthal, be produced in hysterical patients by covering their eyes with their hands or a cloth. Malaria has been charged with the production of catalepsy, and apparently properly. Traumatism is another of its well-authenticated causes. Blows upon the head have been particularly recorded as having an etiological relation to this disorder.
Partial catalepsy has been observed after typhoid fever with severe cerebral symptoms, and also associated with meningitis and intermittent fever. Mancini7 relates a case of cerebral rheumatism complicated or causing catalepsy. A blacksmith, aged thirty-three, had nearly recovered from a rheumatic attack when he became melancholic, complaining also of severe headache. When admitted to the hospital he was found to be imperfectly nourished. He lay on his back, his face without expression, speechless, motionless, pupils insensible to the light, smell impaired, sensation of heat and pain and reflexes absent, galvanic and faradic contractility increased, the rectum and bladder paralyzed. He presented the phenomena of waxen flexibility, the trunk and limbs remaining in whatever position was given them. Considering the previous attack of articular rheumatism and the sudden appearance of nervous disorder during the convalescence of this disease, Mancini believed that the case was probably one of cerebral rheumatism. The man recovered under diaphoretics and counter-irritation.
7 Lo Sperimentale, March, 1878.
Among the important causes of catalepsy bad nutrition may undoubtedly be placed. In the case of De Schweinitz the cataleptoid phenomena rapidly improved, and eventually disappeared as the child's general health was restored by tonics and good diet. Hovey's case was insufficiently clad and badly fed. One of Laségue's cases, quoted by Handfield Jones, died of gradual marasmus, another of pulmonary phthisis. Attacks of catalepsy have sometimes resulted from a combination of excitement, fatigue, and want of food. They occur also in diseases or conditions like phthisis, anæmia, and chlorosis, affections which practically gives us the same cause—namely, bad nutrition. In these cases the nervous system, like other parts of the body, takes part in the general exhaustion.
Rosenthal refers to the production of symptoms of temporary catalepsy by the administration of narcotics and the inhalation of ether and chloroform. In a somewhat ancient American medical periodical8 Charles D. Meigs of Philadelphia gives an interesting account of a case of catalepsy produced by opium in a man twenty-seven years of age. The man had taken laudanum. His arms when in a stuporous condition remained in any posture in which they happened to be left; his head was lifted off the pillow, and so remained. “If he were made of wax,” says Meigs, “he could not more steadily preserve any given attitude.” The patient recovered under purging, emetics, and bleeding. Darwin, quoted by Meigs, mentions a case of catalepsy which occurred after the patient had taken mercury. He recovered in a few weeks.
8 The North American Medical and Surgical Journal, vol. i. p. 74, 1826.
That imitation is an exciting cause of catalepsy has been shown by the [p. 320] often-told story of epidemic hysteria, but more especially by accounts given of certain peculiar endemics of catalepsy. Handfield Jones9 gives an account of an endemic which prevailed at Billinghausen near Wurzburg: “The population consists of peasants who are well off, but who intermarry very much, and are small and deformed. The affected individuals constitute half of the number, males as well as females. They are called there the stiff ones (starren). A chill is commonly said to be the exciting cause of the attacks. The patients are suddenly seized by a peculiar sensation in their limbs, upon which all their muscles become tense, their countenances deadly pale; they retain the posture which they first assume; their fingers are bent and quiver slightly, and the eyeballs in the same way, the visual axis converging; their intellects and senses are normal, but their speech consists only of broken sounds. The attack ceases in from one to five minutes, and the body becomes warm.”
9 Op. cit., quoted from Schmidt's Jahrbuch.
SYMPTOMATOLOGY.—The cataleptic seizure, when it is not the result of some hypnotizing procedure, usually takes place in the following manner: The patient usually, after some patent exciting cause, suddenly ceases whatever she may chance to be doing, becoming rigid and immobile in the last position which she had been in before the attack ensued. “She remains,” says Rosenthal, “as if petrified by the head of Medusa.” The features are composed, the eyes usually directed forward. She is pale; breathing, pulsation, and temperature are usually somewhat reduced. At first the limbs may be found to offer some resistance; soon, however, and sometimes from the beginning, they can be moulded like wax into any possible position, where they will remain until again changed by external agency.
Attacks of catalepsy, as a rule, come on suddenly, without special warning; sometimes, however, special phenomena, which may be compared to epileptic aura, may precede the attack. Thus, Rosenthal speaks of two cases that were ushered in, and also bowed out, by hiccough. The attacks may terminate as suddenly as they begin, but sometimes the patients come out of the state gradually. They are quite likely to appear dazed and stupid when emerging.
Perverted consciousness is another marked symptom of catalepsy. According to some authors, the loss of consciousness is absolute, and upon this symptom they base their diagnosis from two or three other somewhat similar conditions. As I have already indicated in discussing the general subject of Hysteria, this question of consciousness or unconsciousness is not one to be decided in haste. In catalepsy, as in hystero-epilepsy, the conditions as to consciousness may differ. What might be termed volitional consciousness is in true catalepsy certainly in abeyance. Flint10 divides catalepsy, according to the condition as to consciousness, into three kinds—namely, complete, incomplete, and complicated. He, however, regards trance and day-mare as instances of incomplete catalepsy, in which the intellectual faculties are not entirely suspended and the senses are not materially affected, the patient being unable to move or speak, but conscious of all that is going on around him. He believes that such cases resemble more closely the cataleptic condition than they do that of ecstasy. In genuine catalepsy with waxen flexibility, analgesia, etc. there may be [p. 321] greater or less depths of unconsciousness, but some degree of unconsciousness or of obtunded consciousness is necessary to the existence of true catalepsy.
10 Buffalo Medical Journal, xiii., 1857-58, p. 141.
Catalepsy presents well-marked disturbances of sensation, although these, like the conditions as to consciousness, differ somewhat in different cases. Anæsthesia in its different forms, and especially analgesia, are always present in some degree. Experiments without number have been tried on cataleptic patients, showing their insensibility to painful impressions: they have been pinched, pricked, pounded, burned with heated irons, and rubbed down with blocks of ice. Skoda reports a case in which general sensibility was abolished, but a lighted paper rotated rapidly before the eyes gave rise to tremors of the limbs, and strong odors induced slight movement, redness of the cheeks, lachrymation, acceleration of the pulse, and elevation of the temperature.
Hyperæsthesia, although rare, has been noted in a few isolated cases of catalepsy. Puel records a case in which, during the cataleptic paroxysm, the slightest touch or noise caused the patient to grind the teeth and cry out. In some cases sensibility to certain special impressions, as to a strong current of electricity, has been retained, while all others were abolished. In a case of hystero-catalepsy at the Philadelphia Hospital, when all other measures had failed an attack was aborted and evidence of pain produced by the application of a strong faradic current with metallic electrodes.
A marked change in the state of reflex irritability is another of the striking symptoms of true catalepsy. Varying conditions as to reflex irritability have been observed by different authors. So far as I am aware, few special observations have been made upon the tendon reflexes in catalepsy. In the case of De Schweinitz the knee-jerk was apparently absent on one side and present on the other, although the cataleptic symptoms were not unilateral.
The symptom known as flexibilitas cerea, or wax-like flexibility, to which I have referred under Synonyms, is, as has been stated, by some considered pathognomonic of this affection. While I do not hold to this view, I regard the symptom as the most important phenomenon of the disease. It is a symptom which from its very nature can be, up to a certain point, readily shammed, and when considering Diagnosis some methods of determining its genuineness will be given.
Careful observation as to the pulse, respiration, and temperature are lacking in the reported cases of catalepsy. According to Eulenburg,11 “the respiration is generally of normal frequency, sometimes rather slow, more frequently of diminished or irregular intensity, so that lighter and deeper inspirations alternate. The pulse may also be slower, with slight excursion and diminished tension of the arteries. The temperature generally remains normal, but in certain cases is decidedly lowered.” The lowering of temperature, and particularly the presence of extreme coldness of the surface, with exceedingly weak pulse and respiration, have doubtless always been present in the cases—a few, at least, authentic—in which catalepsy has been supposed to be death.
11 Op. cit.
The investigations into the subject of hypnotism made in recent years have given to the profession a series of interesting phenomena which should be considered, at least briefly, under the symptomatology of catalepsy. In a general review of the subject of hypnotism12 by me many of the facts observed and theories advanced by Braid, Heidenhain, Charcot, Richer, and others were examined. I will here recall those observations of Heidenhain13 and of Charcot and Richer14 which relate to the production of a cataleptic or cataleptoid state, and to the phenomena which take place in this state.
12 Am. Journ. Med. Science, Jan., 1882.
13 Animal Magnetism: Physiological Observations, by Rudolph Heidenhain, Prof. Physiology in the University of Breslau, London, 1880.
14 Etudes cliniques sur l'Hystero-epilepsie, ou Grande Hystérie.
The method of Heidenhain was similar to that employed by Braid. The latter, however, did not make use of passes. In the first place, the individual was made to gaze fixedly at a shining faceted glass button for some six or eight minutes, the visual axes being made to converge as much as possible. Heidenhain, like Braid, found the most advantageous direction of the visual axes to be that of upward convergence. According to Carpenter, in the fixation this upward convergence is very important; it suffices of itself in blind people or in the night to produce hypnosis. After the fixation of gaze had been continued for some six or eight minutes, the operator stroked over the face, without immediately touching the surface, from the forehead to the chest, after each pass bringing the hands, which were warm, around in an arc to the forehead again. He either allowed the eyelids to be closed or gently closed them. After ten or twelve passes he asked the person to open his eyes. When this occurred without hesitation or with only slight difficulty, he again made the person stare at the glass for some six minutes, and then repeated the passes, which often brought about the hypnotic state when the simple fixation did not succeed.
The symptoms of the hypnotic state were in the main those which have just been described as the symptoms of catalepsy—namely, diminution of consciousness, insensibility, increased reflex irritability, and fixity of the body or limbs in any position given.
In the slighter forms of hypnotism the subjects were able to remember what had occurred during their apparent sleep. In more fully-developed forms they had no remembrance of what had taken place, but by giving hints and leading questions of their various actions they were able to call them to mind. In the most complete forms of hypnotism no remembrance whatever was retained. It can nevertheless be proved that even during the most completely developed hypnosis sensory perceptions take place, but they are no longer converted into conscious ideas, and consequently are not retained by the memory; and this is undoubtedly because the hypnotized individuals have lost the power of directing their attention to their sensations.
A symptom of the hypnotic state in its most complete development was highly marked insensibility to pain. A pin could be run right into the hand, and only an indistinct feeling of contact was brought about. [p. 323] Immediately on awaking the full sense of pain was again present. The fact that the tactile sense and the sense of pain are distinct was corroborated.
Increased reflex irritability and tonic spasm of the voluntary muscles accompanied the hypnotic condition. Stroking the flexible right arm of a subject, it at once became stiff, since all the muscles were thrown into a state of reflex spasm. Reflex muscular contraction spread over the body when certain definite cutaneous surfaces were irritated. With slight increase of reflex irritability those muscles alone contracted which lay immediately under the area of the skin which had been stroked. Stroking the ball of the thumb caused adduction of the thumb. Stimulating the skin over the sterno-mastoid caused the head to assume the stiff-neck position. When the irritability was somewhat more increased, by a continuous irritation of a definite spot of skin neighboring and even distant groups of muscles could be set into activity. Heidenhain stroked continuously the ball of the left thumb of his brother, when the following muscle-groups were successively affected with spasm: left thumb, left hand, left forearm, left upper arm and shoulder, right shoulder and arm, right forearm, right hand, left leg, left thigh, right thigh, right leg, muscles of mastication, muscles of the neck.
From a study of such phenomena Heidenhain was inclined to consider that the hypnotic state was nothing more than artificially produced catalepsy.
The possibility of fixing any part of the body in any given position constituted an essential factor in the exhibition of Hansen. He made one of his subjects, for instance, sit before him in a chair, and adapted the hands to the seat so that his fingers grasped the edges. After hypnotizing him he stroked along his arms, and his fingers took convulsive hold of the edges of the seat. Placing himself in front of the subject, he bent forward; the subject did the same. He then walked noisily backward, and thereupon the subject followed him through the hall, carrying his chair with him like a snail its shell.
One of the observations of Richer was on the influence of light on catalepsy and hysterical lethargy. The patient was placed before a bright focus of light, as a Drummond or electric light, on which she was requested to fix her sight. In a short time, usually a few seconds or several minutes, sometimes instantaneously, she passed into the cataleptic state. She was as one fascinated—immobile, the wide-open eye fixed on the light, the conjunctiva injected and humid. Anæsthesia was complete. If the patient was hemianæsthetic, she became totally anæsthetic. She did not present contractures. Her limbs preserved the suppleness of the normal state or nearly this—sometimes being the seat of a certain stiffness; but they acquired the singular property of preserving the attitude which one gave them. One interesting peculiarity was the influence of gesture on physiognomy. The features reflected the expression of the gesture. A tragic attitude imprinted a severe air on the physiognomy; the brows contracted. If one brought the two hands to the mouth, as in the act of sending a kiss, a smile immediately appeared on the lips. It was an example of what Braid calls the phenomena of suggestion—of Heidenhain's imitation. The state of catalepsy endured as long as the agent which produced it—that is, as long as the light continued to impress the retina.
[p. 324]The characteristics of the two abnormal states—catalepsy and lethargy—into which hystero-epileptics may be thrown were summarized by Richer as follows: (1) Cataleptic state: The eyes wide open; total and absolute anæsthesia; aptitude of the limbs and different parts of the body to preserve the situation in which they are placed; little or no muscular rigidity; impossibility of causing muscular contraction by mechanical excitation. (2) Lethargic state: The eyes wide open or half closed; persistent trembling of the upper eyelids; convulsion of the eyeballs; total and absolute anæsthesia; muscular hyperexcitability; the limbs, in a condition of resolution, do not preserve the situation given to them, except the provoked contracture impressed upon them.
In the experiments at Salpêtrière the hystero-epileptics were sometimes plunged into the states of catalepsy and lethargy under the influence of sonorous vibrations instead of frights.
During the state of provoked hysterical catalepsy it was found that sight and hearing could be affected by various procedures. The eyes were fixed, and seemed not to see anything. If, however, an object was slightly oscillated in the axis of the visual rays at a little distance from the eyes, soon the gaze of the patient followed these movements. The eyes, and sometimes even the head, seemed to turn at the will of the operator. Hallucinations were produced. When the look was directed upward the expression became laughing; when downward, sombre. The cataleptic state might now cease completely. The patient walked, followed the object on which her gaze was fixed, and took attitudes in relation with the hallucination suggested. Music also caused her to assume positions related with the various sentiments suggested to her by the music. Sudden withdrawal of the object from before the eyes or of the sound from the range of hearing caused a return of the catalepsy. The cataleptic patient in whom the eye was in such a state as to perceive the movements of an experimenter placed in front of her reproduced these movements exactly. At the Philadelphia Hospital I have repeated most of the experiments of Heidenhain and of Charcot and Richer.
Hemi-catalepsy or unilateral catalepsy is sometimes observed, and has been studied both in hypnotic investigations and as a special nervous affection. Charcot and Richer found that hemi-catalepsy or lethargy may be produced on a patient, and that they may both exist simultaneously in the same subject. When, for instance, a patient was plunged into the cataleptic state under the influence of a bright light, shutting with the hand one of the eyes, the patient at once became lethargic on the same side only; the other side remained cataleptic. Heidenhain and Gruetzner studied some remarkable phenomena, which they have recorded under the name of unilateral hypnosis, in which some surprising sensory disturbances occur. They also found, among other things, a striking disturbance in the process of accommodation and in the perception of colors in the eye of the cataleptic side. In a case of hystero-epilepsy upon which I performed numerous hypnotic experiments which have been reported15 [p. 325] the patient nearly always presented unilateral cataleptic phenomena. These were present on the left side, the patient being subject to convulsions which were more marked on the right side, this being also much wasted.
15 Philadelphia Med. Times, Nov. 19, 1881.
I witnessed some curious unilateral cataleptoid phenomena in the case of a medical friend, who has made a note of his experience.16 He says: “In the course of some experiments on table-tipping, which were conducted mainly to satisfy the curiosity of persons who had never seen anything of the kind, I became the subject of a very peculiar and marked hypnotic influence. The ordinary tricks of tipping, answering questions, guessing numbers, etc. had been performed with the table, during the greater part of which I had been one of the circle, when my right hand began to contract so as to form an arch, and was then lifted from the table. These movements were not volitional; I was unable to control them. While my hand was in this position one of the persons sitting at the table suddenly put his hand on my forehead, and I sank back in the chair, passing into a conscious but apparently powerless state, but only for a few moments. Later in the evening the hypnotic influence in the right hand was still more distinctly manifested. If allowed to remain a short time on the table, the fingers began to vibrate vertically and horizontally, the motion finally extending to the forearm and becoming so violent as to throw the hand about in a rapid and forcible manner. While thus affected I found it utterly impossible to sign my name. I would be able to form the first letter or so, and then most extraordinary gyrations would be made. In one instance I wrote very slowly, using all the muscular control at my command, and succeeded in writing the full name, but in a form wholly different from my ordinary signature.”
16 Polyclinic, Sept. 15, 1883.
My attention was called to these phenomena, and the experiments were repeated the next week in my presence, with like results. In addition, I succeeded in forcibly placing the affected arm in various positions—bent at right angles, the hand resting on the top of the head, etc.—from which positions he was unable to move it. He seemed to have lost the connection between volition and the motor impulse. The experiments were continued for several hours at each sitting, but owing to the depressed mental state which was produced for a short time, apparently by them, they have not been repeated.
Occasionally, cases of unilateral catalepsy associated with rotatory phenomena are met with, especially in hysterical children. In 1882, I studied in the nervous dispensary of the hospital of the University of Pennsylvania an interesting case with rotatory and unilateral cataleptoid symptoms. This case has been reported by James Hendrie Lloyd.17 The patient was a boy eight years old. His paternal grandfather hanged himself. On the mother's side there was a history of tuberculosis. Two years before coming to the hospital he had had four attacks of spasms. For two weeks he had been having from twelve to twenty similar spasms daily; some of these were observed in the dispensary. “The boy's head was suddenly drawn upward and to the right to its extreme limits by the action chiefly of the sterno-cleido-mastoid muscle. The eyes turned also to the extreme right, with slight convulsive (clonic) action, and became [p. 326] fixed in that position, with very wide dilatation of the pupils. In a second or two he began to rotate his whole body to the right, and turned completely around, perhaps ten or twelve times. On some occasions he had fallen down, his mother said, toward the end of the spell. If taken hold of and steadied—which required but little force by the physician—the rotation could be stopped, though the head and eyes remained drawn, and the boy's arms could be placed in any desired position. If now he was once more let loose, his body again rotated, while his arms were held in true cataleptoid rigidity. The whole duration of the attack was from one half to one minute. The boy was intelligent, and said he knew what was taking place about him while he was in the fit, though he gave no satisfactory evidence of such knowledge at the time. There was no history of headache or any disease. His ears were subsequently examined and found normal. He had taken worm medicine in abundance from the family physician without results. There were no psychical traits of importance to suggest foolish or wilful simulation. The only accident had been a fall from a wagon years previously. As the patient had an adherent prepuce, Wood advised circumcision, and took pains to explain the operation to the mother. This evidently made a great impression on the child's mind, which is worthy of notice in considering the case. The potassium bromide was continued. At the third visit, which had been appointed for the operation of circumcision, the mother reported the patient much better. The boy had been having great fear of the proposed operation, and now said that he thought he could control the spells. A psychical element was thus distinctly indicated, and its likeness to chorea major to some extent increased. It was thought best, however, instead of circumcision, to break up adhesions and retract the foreskin, which was done by J. William White. At the fourth visit, after ten days, a still greater improvement was noted.”
17 Philada. Med. Times, vol. xii., June 17, 1882.
Lloyd in reporting this case discusses the physiology of the condition, and refers to other cases in medical literature. According to Brown-Séquard, the great cause of rotation phenomena is a convulsive contraction in some of the muscles on one side of the body. Carpenter believes they are due to weakness of the sensori-motor apparatus of one side. Laycock holds that the cerebellum is involved. Lloyd likens the case to chorea major. He refers to cases reported by Radcliffe18 and J. Andrew Crawford.19
18 Reynolds's System of Medicine, art. “Chorea.”
19 Cycl. of Pract. Medicine, art. “Chorea.”
At the Pennsylvania Training School for Feeble-minded Children at Elwyn is a little patient familiarly spoken of as the Dervish. I have examined this boy several times, and have frequently watched his performances. I. N. Kerlin, superintendent of the institution, has kindly furnished me with some notes of this case. The antecedents of the patient are unknown. He is about fifteen years of age, is of small stature and weight, a demi-microcephalic, epileptic, and mute idiot. His epilepsy, however, supervened only in 1884, and the seizures continue now at the rate of three or four a month. At all times he is subject to certain automatic tricks with his hands, putting and twisting them into various positions. Periodically almost during every day he gives exhibitions of the habit which has led him to be called the [p. 327] Dervish. He commences by tattooing his chin with his left hand; next he delicately and rapidly touches the fingers of his left hand to the wrist of the right, makes two or three salaams, and then impulsively gyrates the body from left to right. The right heel is pivotal, and the force is maintained by touches of the left toe or heel upon the floor. He will usually take from three to seven turns at a time, with a salaam or two between every series. Fifteen minutes or more will be thus consumed before he darts away toward a window, where he remains a few moments in a dazed state, from which he rouses to recommence his hand tricks. Perhaps he will select a broad belt of light in which to display his hand for visual enjoyment. He has a cataract of the right lens, and possibly partial amaurosis of the left eye. A supplemental performance sometimes indulged in is to stand at one fixed point and throw his head and shoulders from side to side, describing with the former two-thirds of a circle, the occiput being flexed backward as far as the neck will permit. These movements, rapidly made, reach three and four hundred under favorable conditions.
Kerlin regards the displays made by this boy to be the pure automatic phenomena of idiocy which have been developed to an artistic finish, and out of which the patient gets enjoyment. This enjoyment probably exists in some anæsthetic or stuporous condition of certain nerve-centres, something like the sensation of common dizziness. He does not look upon the case, therefore, as one of genuine catalepsy, but I have recorded it here in connection with the case just given because it illustrates a phase of automatism and rotation movements closely allied to cataleptoid conditions.
Catalepsy and cataleptoid or cataleptic phenomena are of comparatively frequent occurrence among the insane. Niemeyer says20 that they are especially common among persons suffering from melancholia. Kahlbaum21 has described a form of insanity which he names katatonia, from the Greek κατατονος, stretching down. This disease is “characterized by alternate periods, supervening with more or less regularity, of acute mania, melancholia, and epileptoid and cataleptoid states, with delusions of an exalted character and a tendency to dramatism.”22
20 Textbook of Practical Medicine, Felix von Niemeyer, American trans., 1876, vol. ii. p. 387.
21 Klinische Abhandlungen über psychische Krankheiten, 1 Heft, “Die Katatonie,” Berlin, 1874.
22 A Treatise on Insanity in its Medical Relations, by William A. Hammond, M.D., New York, 1883, p. 576.
Kiernan23 has written a valuable memoir on this affection. He has collected fifty cases, a few of which he gives in detail. Hammond and Spitzka discuss the disorder, giving new cases, in their treatises on insanity.
23 American Journal of Insanity, July, 1877, and Alienist and Neurologist, October, 1882.
Katatonia may begin in various ways, but it usually pursues a certain cycle. First appears stuporous melancholia, accompanied or followed by cataleptoid manifestations; then a period of mania with illusions, hallucinations, and delusions. Melancholia reappears in some form, with [p. 328] cataleptoid, waxy condition of the muscles, and a disposition to talk in a pompous or dramatic manner; convulsions or choreic movements may be present.24 Sometimes some phase of the cycle is absent.
24 Hammond.
In some cases in which the peculiar cycle and special phenomena which characterize katatonia are not present marked cataleptic or cataleptoid states may be observed among the insane, either as episodes or as long-continuing conditions.
As cases illustrating cataleptoid phenomena among the insane have not yet been published in large number, and are not well understood, I will record here, under the Symptomatology of Catalepsy, some illustrative cases which have either fallen under my own observation or have been supplied to me directly by medical friends.
M. A. Avery, assistant physician to the insane department of the Philadelphia Hospital, has kindly furnished notes of the following interesting case:
T——, aged twenty, single, dressmaker. The patient was somewhat below medium height, slender and emaciated, of nervous temperament, expression melancholy. The attack of insanity for which she was admitted was her first. It began four months before admission. No satisfactory history of the attack could be obtained; she was said to have been depressed in spirits and to have delusions of poisoning. She had attempted suicide by throwing herself from the window.
Upon admission, Sept. 20, 1883, she was quiet and gentle in her manner, but much depressed; she answered questions rationally. No delusions were detected. Sept. 21st she sat quiet and motionless. Her eyes were fixed, with marked double, inward squint. She was apparently insensible to external impressions. This condition lasted about three hours, when she suddenly sprang up, rushed through the ward, and made vigorous efforts to escape. On the 22d she lay in bed in a perfectly passive state, with eyes open and fixed, but the squint had disappeared. There was a constant slight tremor of the lids. The conjunctiva was apparently insensible to touch. She seemed to be unconscious of what was going on around her. Her arms remained raised in any position in which they were placed. About three o'clock in the afternoon this condition passed away, and from that time until she went to bed at eight o'clock she was bright and cheerful and talked in a rational and intelligent manner. For five days she was quiet and melancholy, with one spell of a few hours in which she was in a passive and cataleptic state, as on the 22d.
On the 28th she stood erect with arms extended, whirling rapidly. She continued this for about half an hour, and then, after a short rest, began again. She paid no attention to what was said to her, and seemed unconscious of what took place around her. The next day she remained in a stupid condition most of the time, but occasionally sprang up and danced violently or spun round rapidly with arms extended for a few moments at a time. On the 30th her cataleptic condition was uninterrupted. She lay motionless, with pulse slow and feeble, extremities cold; her limbs were easily placed in any desired position, and remained so for about twenty minutes; then they returned slowly to a more natural and comfortable position. She continued for several days in this condition, then aroused and ate heartily. She seemed brighter and more cheerful, [p. 329] and talked rationally. She said that she knew all that was said and done when she seemed unconscious, and that she wanted to speak, but could not. For several weeks cataleptic symptoms prevailed, with occasional lucid intervals of a few hours. She eventually settled into a childish, demented condition.
In the insane department of the Philadelphia Hospital was a middle-aged man who remained for several years in a stuporous and cataleptoid state. On several occasions he was before the class in the clinic-room. He could not be made to speak, but remained perfectly silent in any condition in which he was placed. His head and trunk could be bowed forward, sideway, or backward; one foot could be elevated while he stood; his arms could be placed in grotesque positions. In whatever attitude he was placed he would remain for a long time. The only history that could be obtained of this man was that he had for several months been in a state of melancholia, after which he was maniacal for three or four months. He escaped from the hospital, and was brought back in the stuporous and cataleptoid condition in which he continued. He had been a masturbator.
A Dane, while on a voyage from Copenhagen, fell and broke his leg, for which he was treated in a hospital. He recovered and became a nurse in the institution. He fell in love with a female nurse, and was to be married, but the lady suddenly fell dead. He became melancholic, and three weeks afterward tried to hang himself. He also had hystero-epileptic seizures, and was for a long time in a condition of extreme stupor with cataleptoid phenomena, from which he passed into a rather excited condition. He had no special delusions, but there was a tendency to dramatism.
Another case came into the nervous wards of the Philadelphia Hospital. No history could be obtained from the patient. Whether or not he had previously suffered from melancholia could not be learned. He would retain for a long time any position in which he was placed. He also had hystero-cataleptic spells, and a peculiarity of enunciation with a tendency to pose. When asked, “How are you to-day?” he would reply, “I pre-sume-that-I-am-a-bout-the-same—that-it-is-likely-that-some-thing-has-dis-ap-peared-in-the-mind.” When asked, “How long have you been sick?” he would begin in the same way: “I-pre-sume-that-I-will-have-to-say-that-at-a-time-re-mote-ly-dis-tant;” and then he would branch off into something else.
Wilks25 speaks of a man whom he saw in the asylum at Morningside who could be moulded into any position. While in bed on his back his arms and legs could be arranged in any position, and there they would remain. He also speaks of a case seen by Savage in Bethlem—a young man who kept his arms stretched out for two hours, and stood on one leg for a very long time or until he fell.
25 Lectures on Diseases of the Nervous System, delivered at Guy's Hospital.
William Barton Hopkins of Philadelphia has given me brief details of a case observed by him at the Pennsylvania Hospital, which would seem to have been either one of katatonia or one of cataleptoid attacks occurring in an inebriate. The patient was an habitual moderate drinker. For three weeks before he was admitted to the hospital he had been drinking heavily. His family history showed a tendency to insanity. He showed [p. 330] great mental anxiety; his face was pale and had a very troubled aspect. He had no hallucinations. Two days after admission a sudden outbreak of mania occurred, in which he showed destructive and dangerous tendencies, and mechanical restraint had to be employed. Under treatment he became quiet, and was removed by his friends, having been altogether five days in the hospital. On the day of his departure, while awaiting some of his friends in the main hall, he suddenly ran up stairs, and was quickly followed by a nurse, who found him raising a window with the apparent intention of jumping out. His face at this time had lost its troubled look, and had rather a pleased but vacant appearance. While in this condition his limbs were placed in various positions, and there remained. On another occasion, while lying on the bed, his limbs and trunk were placed in various grotesque positions, and there remained. The condition of waxen flexibility was well marked; many tests were made.
To Wharton Sinkler I am indebted for the unpublished notes of the case of a woman twenty-seven years of age, who had no family history of insanity, but whose father was a highly nervous man. She had always had good health, and was of good physique. Seven years ago she had an attack of melancholia lasting four or five months; since then she had no trouble until six months since. At this time she began to be low-spirited. Then delusions came on—that she was unworthy to live; that it was wicked for her to eat, because no one else had food; that those about her were in ill-health. She refused to eat, and would not talk, and slept badly. When first seen by Sinkler she was stout and with apparently good nutrition, but was said to have lost flesh. Her face was expressionless, and she was unwilling to converse, but said she was quite well, and that her stepmother was ill and needed treatment. She was undecided in all her movements, and would stand in one spot until led to a chair, where she would remain if seated.
The patient was placed under the care of two nurses, and for a week improved daily—ate food, conversed, read aloud, and sewed. At the end of this time she was left with one nurse, but became obstinate about eating, and had an altercation with the nurse, in which she became violent. After this she gradually got into a cataleptoid state. At first she would stand for a long time in one place, and if seated in a chair would remain in any position in which she was placed. She began to have attacks in which she would lie on the floor motionless for hours. A sharp faradic current was applied to the forearms on one occasion, and she soon became relaxed. In the attacks the eyes were closed or rolled upward and fixed on the ceiling. The muscles were rigid. The arms and legs could be placed in any attitude, and would there remain. There was no analgesia: she had decided objection to pin-pricks. For two or three days she was readily aroused from the cataleptic state by electricity, but it lost its effect, and etherization was resorted to. The first time a few whiffs of ether relaxed the rigid limbs. The next day the rigidity continued until complete etherization was effected. In fact, when the breathing was loudly stertorous and the conjunctiva insensible to touch, the rigidity was complete, and it was not until a large amount of ether had been inhaled that the limbs relaxed. While under the effects of the ether a vaginal examination was made, and the uterus found normal in position and size. No evidences [p. 331] of self-abuse were found, nor had there been any reason for suspecting this. She continued in the condition described for many days. She was filthy in her habits, and would not use the commode, although she was made to sit on it for hours. She would have a stool on the floor or in bed immediately after rising from the commode. She seemed imbecile, and scarcely spoke, or, if she did, would say she was dead or was a baby. She would eat nothing voluntarily: food was put into her mouth, and she would swallow it, but made no effort to close the lips herself. She was fed in this way for four or five weeks. If taken up to be dressed, she would make the procedure as difficult as possible, and when dressed would not let her clothing remain buttoned, so that her clothes had to be sewed on her.
After about ten weeks a slight improvement showed itself, first in her taking food voluntarily, then in speaking. By degrees she became reasonable, and in about four months from the time she was first seen was perfectly well. The medication used was very slight, but she was thoroughly fed, took bromide of sodium and ergot for a time, and occasionally a dose of paraldehyde to produce sleep. She had two efficient nurses, who carefully carried out all directions, and who never yielded a point, but tried to be always as kind as firm. This case is instructive, not only because of its phenomena, but also because of the method of feeding and managing the patient and the result of treatment.
At a meeting of the Philadelphia Neurological Society held February 22, 1886, I exhibited, at the request of Dr. C. P. Henry, of the Insane Department of the Philadelphia Hospital, a case presenting cataleptoid symptoms, the phenomena of automatism at command, and of imitation automatism.
This patient had been recently admitted to the hospital, and no previous history had been obtained. He was a middle-aged man, not unintelligent-looking, and in fair physical condition. His condition and his symptoms had remained practically the same during the short time that had elapsed since admission. He remained constantly speechless, almost continually in one position; would not open his eyes, or at least not widely; would not take food unless forced; and his countenance presented a placid but not stupid or melancholy appearance. He had on several occasions assumed dramatic positions, posing and gesticulating. It had been discovered by Henry that the patient's limbs would remain where they were placed, and that he would obey orders automatically. The case had been regarded as probably one of katatonia, but in the absence of previous history it was not known whether or not he had passed through the cycle of mania, melancholia, etc. which constitutes this fully-developed disease. He had had since admission attacks of some severity, probably, from description, hystero-epileptic in character.
In exhibiting the patient I first placed his arms and legs and body and head in various positions, where they remained until he was commanded to place them in other positions. His mouth was opened, one eye was opened and the other was shut, and he so remained until ordered to close his mouth and eyes. In most of these experiments the acts performed were accompanied by remarks that the patient would do thus and so as he was directed.
Various experiments to show automatism at command were performed. [p. 332] I remarked, for instance, that the gentleman was a good violin-player, when he immediately proceeded to imitate a violin-player. In a similar way he took a lead-pencil which was handed to him and performed upon it as if it were a flute. He danced when it was asserted that he was an excellent dancer; placed his arms in a sparring position and struck out and countered on telling him that he was a prize-fighter; went through many of the movements of drilling as a soldier, such as attention, facing, marking time, and marching. He was told that he was a preacher and must preach, and immediately began to gesticulate very energetically, as if delivering an earnest exhortation. He posed and performed histrionically when told that he was an actor. He was given a glass of water and told that it was good wine, but refused to drink it, motioning it away from him. He was then told that it was very good tea, when he tasted it, evincing signs of pleasure. During all these performances he could not be induced to speak; his eyes remained closed, or at least the eyelids drooped so that they were almost entirely closed. He showed a few phenomena of imitation, as keeping time and marching to the sound of the feet of the operator.
In the nervous wards of the Philadelphia Hospital there is now an interesting case of melancholia with catalepsy and the phenomena of automatism at command—a man aged twenty-five, white, single, who for thirteen years had worked in a type-foundry. Three years before coming to the hospital he had an attack of acute lead-poisoning with wrist-drop. Two years later he had an attack of mental excitement with other evidences of insanity. He had hallucinations of sight and hearing, and thought that he heard voices accusing his sister of immorality. He at times accused this sister of trying to poison him. He believed that his fellow-workmen were trying to have him discharged. This condition lasted for six weeks, when he became gloomy and stuporous, and would make no effort to do anything for himself. His friends had to feed him. When first admitted to the nervous wards he sat in the same position all day long, with his head almost touching his knees, his arms fully extended by his sides. He would not help himself in any way. His eyes were always open, and he never winked. He never slept any during the day, but was perfectly oblivious to all surroundings. He did not speak or move out of any position in which he was placed. He could be placed in all sorts of uncomfortable positions, and would remain in them. After treatment with strong electrical currents and forced exercise he brightened considerably, and would walk, after being started, without urging. When treatment was discontinued, he relapsed into his former state. Frequent experiments have been performed with this man. Placing his limbs in any position, they will remain if a command is given to retain them. He marches, makes movements as if boxing, etc. at command.
The phenomena shown by both of these patients are those which have for many years been known and described under various names. I well remember when a boy attending a series of exhibitions given by two travelling apostles of animal magnetism, in which many similar phenomena were shown by individuals, selected apparently at haphazard from a promiscuous audience, these persons having first undergone a process of magnetizing or mesmerizing. In experiments of Heidenhain of [p. 333] Breslau upon hypnotized individuals many similar phenomena were investigated, and described and discussed by this physiologist under the names of automatism at command and imitation automatism. The hypnotized subjects, for instance, were made to drink ink, supposing it to be wine, to eat potatoes for pears, to thrust the hand into burning lights, etc. They also imitated movements possible for them to see or to gain knowledge of by means of hearing or in any other way. They behaved like imitating automatons, who repeated movements linked with unconscious impressions of sight or hearing or with other sensory impressions. It was noted in the experiments of Heidenhain that the subjects improved with repetition. The manifestations of my patients, although not simulated, improved somewhat by practice. Charcot, Richer, and their confrères have made similar observations on hysterical and hypnotized patients, which they discuss under the name of suggestion. Hammond26 suggested the term suggignoskism, from a Greek word which means to agree with another person's mind, as a proper descriptive designation for these phenomena. In referring to persons said to be in one of the states of hypnosis, he says that he does not believe that the terms hypnotism and hypnosis are correct, as, according to his view, the hypnotic state is not a condition of artificial somnambulism; the subject, he believes, is in a condition where the mind is capable of being affected by another person through words or other means of suggesting anything. In the clinical lecture during which these opinions were expressed he is reported to have performed on four hypnotized young men experiments similar to those which were exhibited by my insane patients. His subjects, however, were not insane. A bottle was transformed by suggestion into a young lady; sulphur was transmuted into cologne; one of the subjects was bent into all sorts of shapes by a magnet; another was first turned into Col. Ingersoll and then into an orthodox clergyman, etc. In reading such reports, and in witnessing public exhibitions of the kind here alluded to, one often cannot help believing that collusion and simulation enter. Without doubt, this is sometimes the case, particularly in public exhibitions for a price; but what has been observed in the mentally afflicted, what has been shown again and again by honest and capable investigators of hypnotism, prove, however, not only the possibility, but the certainty, of the genuineness of these phenomena in some cases.
26 Med. and Surg. Reporter, vol. xlv., Dec. 10, 1881.
Catalepsy and this automatism at command are sometimes confused, or they may both be present in the same case; indeed, they are probably merely gradations of the same condition, although it is well to be able to differentiate them for the purposes of more careful and accurate investigation. In automatism at command the individual does what he is directed as long as he remains in this peculiar mental condition. In experimenting upon him, his arms or legs, his trunk or head, may be put in various positions, and if commanded to retain them in these positions he will do so, or he will, at command, put them in various positions, there to stay until a new order is given. Imitation automatism occurs also in such cases; patients will imitate what they see or hear. These cases differ only from those of genuine catalepsy in that they do not seem to present true waxen flexibility. The phenomena presented are those [p. 334] which result from control over an easily-moulded will, rather than phenomena due to the fact that the will is entirely in abeyance.
PATHOLOGY—Attempts to explain the nature of catalepsy leave one in a very uncertain and irritable frame of mind. Thus, we are told very lucidly that most authors are inclined to the opinion that the cataleptic rigidity is only an increase of the normal tonus of the voluntary muscles occurring occasionally in the attacks. What appears to be present in all genuine cases of catalepsy is some absence or abeyance of volition or some concentration and circumscription of cerebral activity. The study of the phenomena of catalepsy during hypnosis throws some light upon the nature of catalepsy. Heidenhain's theory of hypnotism is that in the state of hypnosis, whether with or without cataleptic manifestations, we have inhibition of the activity of the ganglion-cells of the cerebral cortex. Herein is the explanation of many cataleptic phenomena even in complicated cases. In hysteria and in catalepsy the patient, dominated by an idea or depressed in the volitional sphere by emotional or exhausting causes, no longer uses to their full value the inhibitory centres. When organic disease complicates catalepsy, it probably acts to inhibit volition by sending out irritative impulses from the seat of lesion.
DURATION.—Usually, attacks of catalepsy recur over a number of years; but even when this is the case the seizures are not as frequent, as a rule, as those of hystero-epileptic paroxysms. Uncomplicated cases of catalepsy, or those cases which occur in the course of hystero-epilepsy, usually preserve good general health.
Of the duration of attacks of catalepsy it need only be said that they may last from a few seconds or minutes to hours, days, weeks, or even months. The liability to the recurrence of cataleptic attacks may last for years, and then disappear.
DIAGNOSIS.—In the first place, the functional nervous disorder described as catalepsy must be separated from catalepsy which occurs as a symptom in certain organic diseases. It is also necessary to be able to determine that a patient is or is not a true katatonic.
It must not be forgotten that genuine catalepsy is very rare. Mitchell at a recent meeting of the Philadelphia Neurological Society said that in his lifetime he had seen but two cases of genuine catalepsy—one for but a few moments before the condition passed off. The other was most extraordinary. Many years ago he saw a young lady from the West, and was told not to mention a particular subject in her presence or very serious results would ensue. He did mention this subject, rather with the desire to see what the result would be. She at once said, “You will see that I am about to die.” The breath began to fail, and grow less and less. The heart beat less rapidly, and finally he could not distinguish the radial pulse, but he could at all times detect the cardiac pulsation with the ear. There was at last no visible breathing, although a little was shown by the mirror. She passed into a condition of true catalepsy, and to his great alarm remained in this state a number of days, something short of a week. Throughout the whole of this time she could not take food by the mouth. Things put in the mouth remained there until she suddenly choked and threw them out. She apparently swallowed very little. She had to be nourished by rectal alimentation. She was so remarkably cataleptic that if the pelvis were raised, so that [p. 335] the head and heels remained in contact with the bed, she would retain this position of opisthotonos for some time. He saw her remain supported on the hands and toes, with feet separated some distance, with the face downward, for upward of half an hour. She remained as rigid as though made of metal. On one occasion while she was lying on her back he raised the arm and disposed of the fingers in various ways. As long as he watched the fingers they remained in the position in which they had been placed. At the close of half an hour the hand began to descend by an excessively slow movement, and finally it suddenly gave way and fell. Not long after this she began to come out of the condition, and quite rapidly passed into hysterical convulsions, out of which she came apparently well. He was not inclined to repeat the experiment.
Catalepsy is to be diagnosticated from epilepsy. It is not likely that a grave epileptic seizure of the ordinary type will be mistaken by an observer of even slight experience for a cataleptic attack. It is some of the aberrant or unusual types of epilepsy that are most closely allied to or simulate catalepsy. Cataleptic or cataleptoid conditions undoubtedly occur regularly or irregularly in the course of a case of epilepsy, but I do believe that it is true, as some observers contend, that between catalepsy and some types of true epilepsy no real distinction can be made. Hazard,27 in commenting on a case reported by Streets,28 holds that no difference can be made between the attacks detailed and those forms of epilepsy described as petit mal.
27 St. Louis Clin. Rec., iii. 1876, p. 125.
28 “Case of Natural Catalepsy,” by Thomas H. Streets. M.D., Passed Assistant Surgeon U. S. N., in the American Journal of Medical Sciences for July, 1876.
The case was that of a sailor aged forty-two years, of previous good health. The attacks to be described followed a boiler explosion, by which he was projected with great force into the water, but from which he received no contusion nor other appreciable injury. There was no history of any nervous trouble in his family. It was the patient's duty to heave the lead. The officer noticed that he was neglecting his business, and spoke to him in consequence, but he paid no attention to what was said to him. “He was in the attitude he had assumed in the act of heaving the lead, the left foot planted in advance, the body leaning slightly forward, the right arm extended, and the line held in the left hand. The fingers were partially flexed, and the sounding-line was paying out through them in this half-closed condition. The eyes were not set and staring, as is the case in epilepsy, but they were moving about in a kind of wandering gaze, as in one lost in thought with the mind away off. The whole duration of the trance was about five minutes.”
Dickson29 reports a very striking case, and in commenting on it holds to the same views. The patient had apparently suffered from some forms of mania with delusions. She was found at times sitting or standing with her body and limbs as rigid as if in rigor mortis, and her face blanched. These spells were preceded by maniacal excitement and followed by violence. On being questioned about the attacks, she said that chloroform had been given her. Numerous experiments were performed [p. 336] with her. Her arms and hands were placed in various positions, in all of which they remained; but it was necessary to hold them for a few moments in order to allow the muscles to become set. She was anæsthetic. After recovering she said that she remembered being on the bed, but did not know how she came there; also, that she had been pricked with a pin, and that her fit had been spoken of as cataleptic. Her mind became more and more affected after each attack, and she finally became more or less imbecile. From the facts observed with reference to this case, Dickson thinks that we may fairly conclude that the mental disturbance in either epilepsy or catalepsy is identical, and results from the same cause—viz. the anæmia and consequent malnutrition of the cerebral lobes; while its termination, dementia, is likely to be the same in either case; also, that catalepsy, instead of being a special and distinct form of nervous disorder, is to be considered as a specific form of epilepsy, and to be regarded as epilepsy, in the same manner as le petit mal is considered epilepsy, and a result of the same proximate cause; the difference in the muscular manifestation bearing comparison with any other specific form of epilepsy, and occurring in consequence of one or other particular cerebral centre becoming more or less affected.
29 “On the Nature of the Condition known as Catalepsy.” by J. Thompson Dickson, M.A., M.B. (Cantab., etc.), British Med. Journ., vol. ii., Dec. 25, 1869.
I do not believe that this ground is well taken. The conditions present in petit mal are sometimes somewhat similar to, but not identical with, those of genuine catalepsy. In the first place, the loss of consciousness, although more complete and more absolute—or rather, strictly speaking, more profound—than in genuine catalepsy, is of much briefer duration. The vertigo or vertiginous phenomena which always accompany genuine petit mal are rarely if ever present in catalepsy. To say that the mental disturbance in catalepsy and in epilepsy is identical is to admit an imperfect acquaintanceship with both disorders. The mental state during the attack of either disorder it is only possible to study by general inspection or by certain test-experiments.
Tetanus is not likely, of course, to be mistaken for catalepsy, but there is a possibility of such an occurrence. The differential diagnosis already given between hystero-epilepsy and tetanus will, however, furnish sufficient points of separation between catalepsy and tetanus.
Catalepsy has been supposed to be apoplexy, or apoplexy catalepsy. The former mistake is, of course, more likely to be made than the latter. A careful study of a few points should, however, be sufficient for the purposes of clear differentiation. The points of distinction given when discussing the diagnosis of hysterical and organic palsies of cerebral origin will here apply. In true apoplexy certain peculiar changes in pulse, respiration, and temperature can always be expected, and these differ from those noted in catalepsy. The stertorous breathing, the one-sided helplessness, the usually flushed face, the conjugate deviation of the eyes and head, the loss of control over bowels and bladder, are among the phenomena which can be looked for in most cases of apoplexy, and are not present in catalepsy.
It is hardly probable that a cataleptic will often be supposed to be drunk, or a man intoxicated to be a cataleptic; but cases are on record in which doubts have arisen as to whether an individual was dead drunk or in a cataleptic stupor. The labored breathing, the fumes of alcohol, the absence of waxen flexibility, the possibility of being half aroused by [p. 337] strong stimuli, will serve to make the diagnosis from catalepsy. The stupor, the anæsthesia, the partial loss of consciousness, the want of resistance shown by the individual deeply intoxicated, are the reasons why occasionally this mistake may be made.
Catalepsy is simulated not infrequently by hysterical patients. Charcot and Richer30 give certain tests to which they put their cataleptic subjects with the view of determining as to the reality or simulation of the cataleptic state. They say that it is not exactly true that if in a cataleptic subject the arm is extended horizontally it will maintain its position during a time sufficiently long to preclude all supposition of simulation. “At the end of from ten to fifteen minutes the member begins to descend, and at the end of from twenty to twenty-five minutes at the most it resumes the vertical position.” These also are the limits of endurance to which a vigorous man endeavoring to preserve the same position will attain. They have therefore resorted to certain experimental tests. The extremity of the extended limb is attached to a tambour which registers the smallest oscillations of the member, while at the same time a pneumograph applied to the chest gives the curve of respiratory movements. In the case of the cataleptic the lever traces a straight and perfectly regular line. In the case of the simulator the tracings at first resemble those of the cataleptic, but in a few minutes the straight line changes into a line sharply broken, characterized by instants of large oscillations arranged in series. The pneumograph in the case of the cataleptic shows that the respirations are frequent and superficial, the end of the tracings resembling the beginning. In the case of the simulator, in the beginning the respiration is regular and normal, but later there may be observed irregularity in the rhythm and amplitude of the respiratory movements—deep and rapid depressions, indicative of the disturbance of respiration that accompanies the phenomena of effort. “In short, the cataleptic gives no evidence of fatigue; the muscles yield, but without effort, and without the concurrence of the volition. The simulator, on the contrary, committed to this double test, finds himself captured from two sides at the same moment.”
30 Journal of Nervous and Mental Diseases, vol. x., No. 1, January, 1883.
Chambers31 says that no malingerer could successfully feign the peculiar wax-like yielding resistance of a cataleptic muscle. He speaks of using an expedient like that of Mark's. Observing that really cataleptic limbs finally, though slowly, yield to the force of gravity and fall by their own weight, he attached a heavy body to the extended hand of a suspected impostor, who by an effort of will bore it up without moving. The intention of the experiment was explained, and she confessed her fraud. This rough test, although apparently different, is in reality similar to that of Charcot and Richer. In both proof of willed effort is shown.
31 Reynolds's System of Medicine, vol. ii., No. 108.
It must not be forgotten that in catalepsy, as has been already noted in hysteria, real and simulated phenomena may commingle in the same case; also, that upon a slight foundation of genuine conditions a large superstructure of simulated or half-simulated phenomena may be reared.
PROGNOSIS.—The prognosis of catalepsy is on the whole favorable. It must be admitted, however, that owing to the presence of neurotic or neuropathic constitution a tendency to relapse is present. [p. 338] Hystero-catalepsy tends to recover with about the same frequency as any of the other forms of grave hysteria. Those cases which can be traced to some special reflex or infectious cause, as worms, adherent prepuce, fecal accumulations, scars, malaria, etc., give relatively a more favorable prognosis. Cases complicated with phthisis, marasmus, cancer, insanity, etc. are of course relatively unfavorable.
TREATMENT.—The treatment of the cataleptic seizure is not always satisfactory, a remedy that will succeed in one case failing in another. Niemeyer says that in case of a cataleptic fit he should not hesitate to resort to affusion of cold water or to apply a strong electrical current, and, unless the respiration and pulse should seem too feeble, to give an emetic. The cold douche to the head or spine will sometimes be efficacious. In conditions of great rigidity and coldness of surface Handfield Jones recommends a warm bath, or, still better, wet packing. Chambers quotes the account of a French patient who without success was thrown naked into cold water to surprise him, after having been puked, purged, blistered, leeched, and bled. This treatment is not to be recommended unless in cases of certain simulation, and even here it is of doubtful propriety and utility. If electricity is used, it should be by one who thoroughly understands the agent. A galvanic current of from fifteen to thirty cells has been applied to the head with instantaneous success in hystero-epileptic and hystero-cataleptic seizures. A strong, rapidly-interrupted faradic current, or a galvanic current to the spine and extremities, sometimes succeeds and sometimes fails. Rosenthal reports that Calvi succeeded in relieving cataleptic stiffness in one case by an injection of tartar emetic into the brachial vein—a procedure, however, not to be recommended for general use. Inhalations of a few drops of nitrate of amyl is a remedy that should not be passed by without a trial; it is of great efficacy in the hysteroidal varieties. Inhalation of ammonia may also be tried. A hypodermic injection of three minims of a 1 per cent. solution of nitroglycerin, as recommended for severe hystero-epileptic seizures, would doubtless be equally efficient in catalepsy.
Music has been used to control hysterical, hystero-epileptic, and cataleptic seizures. The French cases reported have all been of the convulsive types without loss of consciousness and those varieties in which the special sensibility sometimes persists, as in hystero-catalepsy, lethargy, and somnambulism. Music has been used as medicine from the times of Pythagoras to the present, although it can hardly be claimed to have attained a position of much prominence as a therapeutic agent.
In one case a vigorous application of fomentations of turpentine to the abdomen was promptly efficacious in bringing a female patient out of a cataleptic seizure.
Meigs, whose case of catalepsy produced by opium has been reported under Etiology, suggests that purgative medicines, used freely in the treatment of his case, might be advantageously resorted to in any case of catalepsy.
Powerful tonics, such as quinine, iron, salts of zinc and silver, should be used in connection with nutrients, such as cod-liver oil, peptonized beef preparations, milk, and cream, to build up cataleptic cases in the intervals between the attacks.
DEFINITION.—Ecstasy is a derangement of the nervous system characterized by an exalted visionary state, absence of volition, insensibility to surroundings, a radiant expression, and immobility in statuesque positions. The term ecstasy is derived from two Greek words, ἐκ and στάσις, which means to be out of one's senses or to be beside one's self. Commonly, ecstasy and catalepsy, or ecstasy and hystero-epilepsy, or all three of these disorders, alternate, coexist, or occur at intervals in the same individual. Occasionally, however, the ecstatic seizure is the only disorder which attracts attention. Usually, in ecstasy the concentration of mind and the visionary appearance have reference to religious or spiritual objects.
SYNONYMS.—Trance is sometimes used as synonymous with ecstasy. While, however, ecstasy is a trance-like condition, conditions of trance occur which are not forms of ecstasy. Other synonyms are Carus-extasis, Catochus, Catalepsia spuria.
HISTORY AND LITERATURE.—Accounts of cases of ecstasy abound in both ancient and modern medical and religious literature. The epidemics of the Middle Ages, the days of the New England witchcraft, the revivals in England and America, have afforded many striking illustrations. Not a few special cases of ecstasy have become historical. Elizabeth of Hungary and Joan of Arc were both cataleptics and ecstatics. Saint Gertrude, Saint Bridget, Saint Theresa, Saint Catharine, and many other saintly individuals of minor importance have owed their canonization and their fame to the facility with which they could pass into states of ecstasy, catalepsy, or hystero-epilepsy.
Gibbon1 has well described the occurrence of ecstasy in the monks of the Oriental Church in the following passage: “The fakirs of India and the monks of the Oriental Church were alike persuaded that in total abstraction of the faculties of the mind and body the purer spirit may ascend to the enjoyment and vision of the Deity. The opinions and practices of the monasteries of Mount Athos will be best represented in the words of an abbot who flourished in the eleventh century. ‘When thou art alone in thy cell,’ says the ascetic teacher, ‘shut thy door and seat thyself in a corner; raise thy mind above all things vain and transitory; recline thy beard and thy chin on thy breast; turn thine eyes and thy thoughts toward the middle of thy belly, the region of the navel; [p. 340] and search the place of the heart, the seat of the soul. At first all will be dark and comfortless; but if you persevere day and night you will feel an ineffable joy; and no sooner has the soul discovered the place of the heart than it is involved in a mystic and ethereal light.’ This light, the production of a distempered fancy, the creature of an empty stomach and an empty brain, was adored by the Quietists as the pure and perfect essence of God himself; and as long as the folly was confined to Mount Athos the simple solitaries were not inquisitive how the divine essence could be a material substance, or how an immaterial substance could be perceived by the eyes of the body. But in the reign of the younger Andronicus the monasteries were visited by Barlaam, a Calabrian monk, who was equally skilled in philosophy and theology, who possessed the languages of the Greeks and Latins, and whose versatile genius could maintain their opposite creeds according to the interest of the moment. The indiscretion of an ascetic revealed to the curious traveller the secrets of mental prayer, and Barlaam embraced the opportunity of ridiculing the Quietists, who placed the soul in the navel—of accusing the monks of Mount Athos of heresy and blasphemy.”
1 Decline and Fall of the Roman Empire, by Edward Gibbon, Esq., in 8 vols., vol. viii. p. 64, London, 1838.
Some of Swedenborg's supernatural visions were, so far as can be judged, simply accounts of attacks of ecstasy; and of like character were the visions of John Engelbrecht as related by Arnold.2
2 Observations, etc., London, 1806.
In a very curious American book3 published in 1815 a history is given of the wonderful performances of a woman named Rachel Baker, who was undoubtedly in the habit of passing into conditions of religious ecstasy, during which were present many of the phenomena which occur in ecstatics, Catholic or Protestant, religious or otherwise. When seventeen years old she witnessed the baptism of a young lady, which impressed her strongly and caused her to become much dejected and affected about her religious state. She began to have evening reveries or night talks which soon attracted attention. She united with the Presbyterian Church. These reveries after a while expanded into evening exercises which began with prayer, after which she exhorted and made a closing prayer. She removed from Marcellus to Scipio, New York, in 1813, and shortly afterward, in the same year, she went to New York City for medical advice. While there she gave many opportunities to witness her powers when in what her editors quaintly call her somnial paroxysms. Her discourses were good illustrations of what is sometimes termed trance-preaching.
3 Devotional Somnium; or, A Collection of Prayers and Exhortations Uttered by Miss Rachel Baker, by Several Medical Gentlemen, New York, 1815.
One of the most interesting parts of this curious book is a dissertation by Samuel L. Mitchill, M.D., on the function of somnium. He says there are three states of animal existence—wakefulness, sleep, and vision or dream. The definition of somnium, which he quotes from Cicero, is a very fair one to be applied to some of the conditions which we now speak of under such heads as lethargy, trance, ecstasy, etc. “By somnium,” he says, “may be understood the performance of certain mental and bodily actions, which are usually voluntary, without the direction or government of the will or without the recollection afterward that such volition existed.” He divides somnium into symptomatic and [p. 341] idiopathic. The symptomatic somnium occurs from indigestion, the nightmare, from affusions of water into the chest, from a feverish state of the body, from debility with fasting, from fresh and vivid occurrences, etc. The idiopathic somnium is divided into somnium from abstraction, somnium with partial or universal lunacy, with walking, with talking, with invention, with mistaken impressions of sight and of hearing, with singing, with ability to pray and preach or to address the Supreme Being and human auditors in an instructive and eloquent manner, without any recollection of having been so employed, and with utter incompetency to perform such exercises of devotion and instruction when awake. To the last of these affections he refers the case of Rachel Baker, whose devotional somnium he describes.
A number of other curious cases are recorded in this book: that of Job Cooper, a weaver who flourished in Pennsylvania about the year 1774; that of the Rev. Dr. Tennent, who came near having a funeral in one of his states of trance, who has related his own views, apprehensions, and observations while in a state of suspended animation. He saw hosts of happy beings; he heard songs and hallelujahs; he felt joy unutterable and full of glory: he was, in short, in a state of ecstatic trance. Goldsmith's history of Cyrillo Padovando, a noted sleep-walker, who was a very moral man while awake, but when sleep-walking a first-class thief, robber, and plunderer of the dead, is also given.
One of the most remarkable instances of ecstasy is that of the girl Bernadette Soubirons, whose wonderful visions led to the establishment of the now famous shrine of Our Lady of Lourdes in the south of France. It is related of this young girl by her historian Lasserre4 that when about to cross the Gave, a mountain-stream of the Pyrenees, she suddenly saw in a niche of a rock a female figure of incomparable splendor, which she described as a real woman with an aureola about her head and her whole body of surprising brightness. The child afterward described in detail the vision she had seen. Later, on a number of occasions at the same spot, she saw the same vision, described as appearing transfigured. The child believed that she saw the Immaculate Virgin. The Virgin told her that she wished a church to be built on the spot. The place has since become a shrine for Catholics of all nations.
4 Our Lady of Lourdes, by Henri Lasserre, translated from the French, 7th ed., New York, 1875.
Meredith Clymer5 has written an elaborate communication on ecstasy. Ambrose Paré, quoted by Clymer, defines ecstasy as a reverie with rapture of the mind, as if the soul was parted from the body. Briquet describes it as a state of cerebral exaltation carried to such a degree that the attention, concentrated on a single object, produces the temporary abolishment of the other senses and of voluntary movements.
5 “Notes on Ecstasy and other Dramatic Disorders of the Nervous System,” Journal of Psychological Medicine, vol. iv., No. 4, October 1870.
ETIOLOGY.—Under the predisposing causes of ecstasy may be comprised almost all of those described under hysteria. The predisposition to the development of ecstasy will be governed in great measure by peculiarities of religious education and of domestic and social environment.
Extreme religious feeling is undoubtedly among the most frequent of [p. 342] the exciting causes of ecstasy. The accidents and incidents of love have also had a place. Sexual excitement is sometimes associated with the production of ecstasy. “In pre-Christian times,” says Chambers, “when, in default of revelation, men worshipped their incarnate passions, we have from the pen of Sappho a description of a purely erotic ecstasy which can never be produced again.” Fear or fright has been known to throw a predisposed individual into an attack of ecstasy. Severe threats have occasionally had the same influence.
SYMPTOMATOLOGY.—In considering the symptomatology of ecstasy it will only be necessary to call attention to the ecstatic attack. The accompanying phenomena are those of hysteria, hystero-epilepsy, etc., already fully described. I cannot do better than quote from Lasserre the account of one of the ecstatic seizures of Bernadette Soubirons. Although given in turgid language and from the religious point of view, the description is a good one of the objective phenomena of ecstasy:
“A few moments afterward you might have seen her brow light up and become radiant. The blood, however, did not mantle her visage; on the contrary, she grew slightly pale, as if Nature somewhat succumbed in the presence of the apparition which manifested itself to her. All her features assumed a lofty and still more lofty expression, and entered, as it were, a superior region, a country of glory, significant of sentiments and things which are not found below. Her mouth, half open, was gasping with admiration and seemed to aspire to heaven. Her eyes, fixed and blissful, contemplated an invisible beauty, which no one else perceived, but whose presence was felt by all, seen by all, so to say, by reverberation on the countenance of the child. This poor little peasant-girl, so ordinary in her habitual state, seemed to have ceased to belong to this earth.
“It was the Angel of Innocence, leaving the world for a moment behind and falling in adoration at the moment the eternal gates are opened and the first view of paradise flashes on the sight.
“All those who have seen Bernadette in this state of ecstasy speak of the sight as of something entirely unparalleled on earth. The impression made upon them is as strong now, after the lapse of ten years, as on the first day.
“What is also remarkable, although her attention was entirely absorbed by the contemplation of the Virgin full of grace, she was, to a certain degree, conscious of what was passing around her.
“At a certain moment her taper went out; she stretched out her hand that the person nearest to her might relight it.
“Some one having wished to touch the wild rose with a stick, she eagerly made him a sign to desist, and an expression of fear passed over her countenance. ‘I was afraid,’ she said afterward with simplicity, ‘that he might have touched the Lady and done her harm.’”
Side by side with this description by the devout Lasserre of the appearance presented by Bernadette when in a state of ecstasy, I will quote the often-recorded account which Saint Theresa has given in her Memoirs of her subjective condition while in a similar state:
“There is a sort of sleep of the faculties of the soul, understanding, memory, and will, during which one is, as it were, unconscious of their working. A sort of voluptuousness is experienced, akin to what might [p. 343] be felt by a dying person happy to expire on the bosom of God. The mind takes no heed of what is doing; it knows not whether one is speaking or is silent or weeping; it is a sweet delusion, a celestial frenzy, in which one is taught true wisdom in a way which fills us with inconceivable joy. We feel as about to faint or as just fallen into a swoon; we can hardly breathe; and bodily strength is so feeble that it requires a great effort to raise even the hands. The eyes are shut, or if they remain open they see nothing; we could not read if we would, for, though we know that they are letters, we can neither tell them apart nor put them together, for the mind does not act. If any one in this state is spoken to, he does not hear; he tries in vain to speak, but he is unable to form or utter a single word. Though all external forces abandon you, those of the soul increase, so as to enable you the better to possess the glory you are enjoying.”
Occasionally striking illustrations of ecstasy are to be found among hysterical and hystero-epileptic patients in whom religious faith has no place. In these cases usually other special phases of grave hysteria are present. In some of the descriptions given by Charcot and Richer of hystero-epileptics in the stage of emotional attitudes or statuesque positions the patients are, for a time at least, in an ecstatic condition in which the hallucinations may be connected with sentiments of religion, love, fear, or other emotions. One shows an attitude of menace or an expression of fear; in another the expression is of beatitude or saintly happiness: to this expression perhaps succeeds one of intense joy; to this, one of passion and lubricity. Throughout all the changing phases of attitude and expression the patient has the other concomitants of the true ecstatic state, such as want of volition and insensibility.
DIAGNOSIS.—A cataleptic may also be an ecstatic or the reverse; but not a few cases are on record in the history of which, on the one hand, an individual has been subject over a long period to cataleptic seizures without the recurrence of ecstasy, or, on the other hand, to fits of ecstasy without a single attack of true catalepsy. Cataleptic attacks usually occur with more suddenness than ecstasy; the cataleptic may suddenly become rigid and statuesque—the ecstatic gradually, although it may be somewhat rapidly, passes step by step into a visionary state. In catalepsy and ecstasy the expression of the patient differs. One of the striking features of ecstasy is not simply the absorbed and abstracted, but also the radiant, expression of countenance. In catalepsy the expression is more likely to be vacant or at least negative. In ecstasy waxen flexibility is not present. The muscles can act in obedience to the will, and the trunk and limbs do not maintain the positions in which they are placed for any unusual time. In genuine catalepsy the consciousness is so suspended or altered that the period of the seizure afterward remains a blank in the memory of the patient. In ecstasy, however, the visions and fancies present during the fit can afterward be recalled, and are frequently recounted by the individual.
DURATION, COURSE, PROGNOSIS.—Nothing need be said as to duration, course, prognosis, etc. of ecstasy. The remarks made in considering hysteria, hystero-epilepsy, etc. fully cover these matters.
TREATMENT.—With reference to the treatment of ecstasy little need be said. It must, in part at least, be directed to rousing and changing [p. 344] the dormant or dreamy condition of the individual. As it is the mind or the volitional nature which is chiefly affected, the use of agents which either directly or reflexly exert a powerful impression on the cerebral centres is indicated. Thus, in all ages harsh measures have received more or less applause in the treatment of ecstasy. The cold douche or shower-bath, the plunge-bath, the hot iron, painful electric currents, scourging, and beating have all had their advocates. Flint6 gives details of a case in which burning with a heated hammer was employed for three weeks, the patient eventually recovering, either because of, or in spite of, the treatment. Chambers believes in the forcible repression of ecstatic and emotional exhibitions. “In Unst, the most northerly of the Shetland Islands,” he says, “an epidemic of convulsive fits occurring in sermon-time began to prevail in several parish churches. At one of these, Northmaven, the disease was cut short by a rough fellow of a Turk who carried out a troublesome patient and tossed her into a wet ditch. Nobody else caught it. From what scandalous scenes Europe might have been saved had the first dancer on St. John's Eve been tossed into a wet ditch!”
6 Loc. cit.
Trance may be defined as a derangement of the nervous system characterized by general muscular immobility, complete mental inertia, and insensibility to surroundings. The condition of a patient in a state of trance has been frequently, and not inaptly, compared to that of a hibernating animal. Trance may last for minutes, hours, days, weeks, or even months. Astonishing stories, some true, others—and these the greater number—false, frequently find their way into newspapers. A recent story is that of a hystero-cataleptic young woman of Nebraska who is reported to have been for seventy days in a state of trance, during which she was to all appearance lifeless with the exception of respiration and pulsation. She said that she was unconscious during the whole time of her protracted trance, but, although she exerted her utmost power to evince her consciousness, she could not move a muscle. Such cases like the Welsh fasting girl either live or seem to live for a long time on little or no food; doubtless food is often taken secretly.
In an interesting case which, so far as I know, has never been put upon record in any medical publication, attacks of catalepsy or of trance, or of both, occurred three times at long intervals during the life of this individual. The first time was while held in the arms of his mother preparatory to receiving the baptismal rite: the clergyman and others observed that the infant changed appearance and suddenly became rigid. It was feared that he was dying; the ceremonies were stopped, but in response to efforts after a time he came back to a normal state. When about sixteen years of age, while at school, he was accidentally wounded; it was necessary to probe for the ball, and while this was being done he again passed into a trance-like condition. Many years later, while in good health, a prosperous and well-known citizen, he suddenly again fell into an unconscious condition, and was believed to be dead. So marked were the appearances of death [p. 345] that after numerous efforts to resuscitate him preparations were made for his funeral. The knowledge of his previous attacks, however, induced his friends and relatives to defer his interment and continue their efforts. He finally revived just as they were about to give up in despair.
Aëtius, according to Laycock,7 mentions hysteric death as being very common in his day, and asserts that real death may supervene without any of the ordinary symptoms. The eyes preserve their brightness and the color of the skin remains vivid. Good cites the case of a woman whose funeral was postponed to ascertain the cause of her death, and whom the first touch of the scalpel brought to her senses. Authors and travellers have described wonderful cases of trance which have been observed in Persia and in India. A Persian youth is recorded to have possessed the power to restrain his breath for two days; and fakirs in India are said sometimes to have allowed themselves to be buried alive for weeks. Doubtless, a little Caucasian light let in upon some of these stories might dissolve them, as the esoteric Buddhism of Madame Blavatzsky has been dissipated into thin air by a hard-headed English investigator. According to Diogenes,8 Empedocles, a celebrated disciple of Pythagoras, obtained great fame by curing a female supposed to be dead, but whom he discovered to be suffering from hysteria. He termed the affection under which she labored apnoë, and maintained that a female might live in an apparently lifeless state for thirty days.
7 Op. cit.
8 Quoted by Laycock.
Landouzy has reported an interesting instance of lethargy produced by the application of a magnet to a patient suffering from hysteria major. The attacks of hysterical sleep are often preceded by convulsive phenomena, and, according to Briquet, are often ushered in by epileptoid signs, such as whistling inspiration, movements of deglutition, frothing, and transient rigidity of the limbs. Richer reports a remarkable case of Plendlers of Vienna, in which a young girl, after a series of violent hysterical attacks, fell apparently dead. Preparations were made to bury her, when she was found to be living, having been in a state of lethargy. Among cases observed in Salpêtrière the duration of lethargy has been from two to eight days. Sometimes, in cases of grave hysteria, attacks of lethargy complicated with general or partial contractures and epileptoid phenomena have been observed. The presence of neuro-muscular hyperexcitability is of diagnostic value in determining the nature of such cases; if present, we have probably to deal with phenomena of hysterical lethargy. This symptom may, of course, pass unperceived. A woman came under observation a short time since, being then far gone in pregnancy. About a month before delivery she had a very marked hysterical outbreak, in which she so simulated apoplexy as to make it almost impossible to decide what was the matter with her. She had apparently lost sensation, her breathing was stertorous, her pulse labored, and she had divergent strabismus. In the course of half an hour the symptoms passed off.
In trance, as in ecstasy, the patient may remain motionless and apparently unconscious of all surroundings; but in the former the visionary state, the radiant expression, and the statuesque positions are not necessarily present. In trance, as stated by Wilks, the patients may lie [p. 346] like an animal hibernating for days together, without eating or drinking, and apparently insensible to all objects around them. In ecstasy the mind, under certain limitations, is active; it is concentrated upon some object of interest, admiration, or adoration. Conditions of trance, as a rule, last longer than those of ecstasy.
Beard's9 theory of trance is that it is “a functional disease of the nervous system in which the cerebral activity is concentrated in some limited region of the brain, with suspension of the activity of the rest of the brain, and consequent loss of volition. Like other functional nervous diseases, it may be induced either physically or psychically—that is, by all the influences that act on the nervous system or on the mind; more frequently the latter, sometimes both combined.”
9 Quoted by Crothers in Quarterly Journal of Inebriety, January, 1880.
T. D. Crothers10 has contributed some papers upon the subject of the trance state in inebriety. He gives the clinical history of some cases of inebriety which presented the phenomena of cerebral automatism or trance. He concludes that loss of memory and consciousness may come on in inebriety and the patient give little or no evidence of his actual condition. His conclusions are, that when the trance state is established beyond doubt the individual is irresponsible for his acts during this period. The study of the trance state in affections of such definite origin and positive pathology as inebriety helps to throw light upon its occurrence and explanation in cases of hysteria.
10 “Cerebral Trance; or, Loss of Consciousness and Memory in Inebriety,” Quarterly Journal of Inebriety, January, 1880; and The Trance State in Inebriety: its Medico-Legal Relations; with an Introduction on the Nature and Character of the Trance State, by George M. Beard, M.D., a paper read before the New York Medico-Legal Society, November 2, 1881, Hartford, Conn., 1882.
Dana11 reports about fifty cases of prolonged morbid somnolence. Nearly all those reported previous to 1878 are cases of what has been termed trance-like sleep or lethargy. In 1878, Gelineau called attention to a disease which he termed narcolepsy. Dana has seen five cases, and reports two others from notes furnished by Putzel of New York. Some of the cases collected are both interesting and remarkable. Dana calls attention to the distinction made by Briquet between prolonged hysteria and lethargy. In lethargy the condition of unconsciousness is generally more profound, the reflexes are abolished, and the patient cannot be aroused. A patient may even have periods of sleep within the lethargy.
11 “Morbid Drowsiness and Somnolence,” Journ. of Nervous and Mental Disease, vol. xi., No. 2, April 18, 1884.
Dana excludes from his cases of prolonged somnolence those cases of drowsiness due to ordinary causes, as old age, diseased blood-vessels, cerebral malnutrition, or inflammation; various toxæmiæ, as malaria, uræmia, colæmia, and syphilis; dyspepsia, diabetes, obesity, insolation, cerebral anæmia and hyperæmia, cerebral tumors and cranial injuries, exhausting diseases, and the sleeping sickness of Africa.
He found that the prolonged somnolence shows itself in very different ways. Sometimes the patient suffers from simply a great prolongation of natural sleep; sometimes from a constant, persistent drowsiness, which he is often obliged to yield to; sometimes from frequent brief attacks of somnolence, not being drowsy in the intermission; sometimes from single or repeated prolonged lethargic attacks; finally, sometimes from [p. 347] periodical attacks of profound somnolence or lethargy which last for days, weeks, or months.
He says that most cases of functional morbid somnolence are closely related to the epileptic or hysterical diathesis; but a class of cases is met with in which no history or evidence of epilepsy or hysteria can be adduced, and though they may be called epileptoid or hysteroid, these designations are simply makeshifts; the patients seem to be the victims of a special morbid hypnosis. Possibly they have a cerebral hyperæmia or anæmia.
Under the name of morbid somnolence a case has been reported by P. J. Cremen.12 The patient was a man fifty-five years old, who was admitted to the hospital under the care of Cremen. He said he had recently returned from America, where he had taken a drink which had affected his head. He went to bed, and the next morning was found in a deep sleep, from which he could not be aroused. He presented the appearance of a person in a sound sleep or under the influence of anæsthetics. All ordinary measures were unavailing to awaken him from his trance-like condition. He was completely analgesic over the entire surface of the body. He would not eat or drink when simply directed, but when the drinking-cup was placed in his hand he drank, and when bread or meat was given he ate. Subsequently he was seen eating while in the somnolent state with the eyes closed; but after a time he would stop, and had to be urged to commence again. Evidently, tactile sensibility was not lost. The muscular sense appeared to be diminished. The superficial reflexes were abolished, the knee-jerks exaggerated; ankle clonus was absent. Smell and taste were obtunded. Hearing was retained. The state of muscular rigidity during the somnolence was remarkable. He was placed between two chairs, the tip of the shoulder resting upon one chair, the heel of the left foot on the other, and the right leg bent at a right angle to the trunk. A weight of forty pounds was then supported on the rigid chest without causing the slightest yielding or movement from the position described until muscular relaxation took place. He often remained in this state for four or five days at a time or longer. He could be aroused by a strong magneto-electric current. In the intervals between the attacks he was sometimes bright and cheerful, at others gloomy and depressed. When requested to walk, he would do so in a perfectly straight line, from which he would not deviate for obstacles. When told to walk around a table, however, or other obstacle, he would do so. He would try to do anything that he was told, even to standing on his head. The somnolent or hypnotic state could be induced at will by closing the eyelids and pressing the eyeballs for about two minutes. Of the genuineness of the phenomena Cremen had no doubt; he believed that the somnolence partook, in some degree, of the nature of that which has been designated narcolepsy. This case in many respects is similar to cases of catalepsy and automatism at command. A very similar case has been reported in the article on Catalepsy.
12 Brit. Med. Journ., Dec. 12, 1885.
Self-concentration in those of robust minds differs rather in degree than in essence from ecstasy or trance and allied conditions in the weak and hysterical. “Archimedes,” says Clymer, “engrossed with a problem in [p. 348] geometry, feels no hunger and is deaf to the tumult of the soldiers in a captured town; Socrates, occupied with his own thoughts, stands twenty-four hours immovable in one spot exposed to the burning rays of the sun.” Goethe, Blake, and others are on record as having the power to call up images at will. Francis Galton13 in a recent work advocates the cultivation of this power of the reproduction at will of mental imagery. Clarke14 records many wonderful instances of pseudopia. In what does the ecstatic differ from these except in that the mental status of the individual is different, and that the object of mental concentration is of a special character, consonant with the person's ideas, training, and surroundings?
13 Inquiries into Human Faculty and its Development, Francis Galton, F. R. S., New York, 1883.
14 Vision, a Study of False Sight, by Edward H. Clarke, M.D., Boston, 1878.
In brown study or reverie, according to Laycock, the eye is fixed by a muscular action analogous to that of the cataleptic; and not the eye only, for a limb or the whole body will remain in the same position for many minutes, the senses themselves being in deep abstraction from surrounding objects.
Stigmatization (from the Greek στιγμα, a small puncture) is a symptom or appearance which usually presents itself in the form of bloody or blood-like markings on the palms of the hands, the backs of the feet, and the left side, the positions in which Christ was lacerated by the nails and the spear at the crucifixion. In some cases the stigmata are found in scattered points on various parts of the body, sometimes upon the forehead at the position of the lacerations produced by the crown of thorns. In various ages it has been claimed by Catholics that cases of genuine stigmatization have occurred. It is not, however, a matter of Catholic faith, the claim being simply that it is a genuine experience which has some supernatural significance. Hammond15 has an interesting chapter on the subject of stigmatization, of which I have made use, and Clymer's16 article, already referred to, gives the details of several of the most interesting historical cases. Space will not permit more than a glance at this subject. A case of stigmatization is not necessarily one of hysteria, but the phenomena of simulated, and possibly of genuine, stigmatization usually occur among the hysterical.
15 On Certain Conditions of Nervous Derangement, New York, 1881.
16 Op. cit.
According to Garres, the first to exhibit stigmatization was Saint Francis of Assisium, who was born in 1186 and died in 1236. In 1224 he was marked, and in memory of the event the 17th of September was set apart as the Feast of the Holy Stigmata by Pope Benedict XI. The story of this occurrence is of a highly emotional and sensational character. Christine de Stumbele, born in 1242, a few miles from Cologne, is another of the famous hystero-cataleptics and ecstatics who were the victims of numerous stigmata. These were irregular as to position and to times of appearance. On one occasion, for instance, she had wounds on each foot from which the blood flowed freely; a little later, on the same [p. 349] occasion, she was wounded on the knee, and to the wondering priest who was ministering to her at this time she showed hot nails of hideous shapes. She was not only a case of ecstasy and stigmatization, but a filthy creature withal, who covered herself and others with excrement, which they had the foolishness to believe came from the hand of the devil. Veronica Giuliani, another ecstatic, who conversed with Christ and the Virgin Mary, received the stigmata during one of her prayers, and was canonized in 1839. Imbert-Gourbeyre gives a list of 145 persons who have received stigmata, besides 8 now living known to him. He details one American case, that of a young French Canadian.
Two of the most extraordinary recent cases are those of Palma d'Oria and Louise Lateau. These have become stock cases in books and dissertations on the subject under consideration, and therefore the briefest accounts of them will be all that is required. Palma in 1871 was sixty-six years old, humpbacked, thin, small, and with light expressive eyes. It is important to note that she had seen Louisa Lateau in ecstasy. Wonderful accounts are given of her performances—eating the Host in the presence of the priest; having visions of the devil with a little horn on his forehead; on another occasion Jesus Christ himself bringing to her the communion; seeing the Host flying through the air before entering her mouth. After the communion, usually when others were not present, the stigmatization occurred. Bleedings from the forehead or near it, and hemorrhagic spots on various parts of the body of various shapes, as of hearts and of the cross, appeared. Examination of the skin subsequently showed it to be intact, except that she had a hole in the cranium, which Hammond suggests was of syphilitic origin. Plates are given in the work of the credulous Imbert-Gourbeyre representing these figures.
In most respects the most celebrated of all cases of stigmatization is that of Louise Lateau—celebrated because of the investigations which have been made of her case; because of the amount of literature, theological, scientific, and medical, which has been devoted to her; because of the conflict of opinions even among medical observers in regard to the true explanation of the phenomena she exhibited. Louise Lateau was a Belgian peasant-girl, born January 30, 1850. Her parents were poor. She suffered the hardships of her class, and was as badly nourished and educated as a poor Belgian peasant-girl is likely to be. During the cholera epidemic of 1866 she nursed kindly and patiently many of the victims. In 1867 she became weak, pale, and neuralgic, and sometimes spat blood. On Friday, April 24, 1868, she for the first time noticed blood immediately below the left breast; the following Friday it appeared at the same place, and also on the back of the left foot; later, it oozed from the left side and both feet, from the palms and backs of the hands, and from the forehead. Some weeks after this she began to exhibit the phenomena of ecstasy; and subsequently for months and years, regularly on every Friday, she had a recurrence of the stigmata and ecstasy, with accompanying phenomena, sometimes varying a little in detail. Some of the accounts given by Lefevre and others of her seizures are beautiful descriptions of attacks of ecstasy. She stated that during her attacks she had a distinct vision of the whole scene of the crucifixion.
Numerous experiments, some of them cruel in character, were [p. 350] performed to test the genuineness of her conditions of unconsciousness and insensibility. Sight, hearing, and touch were tested. The mucous membrane of the nose was tickled; strong hartshorn was applied to the nostrils; she was pricked and stabbed with needles, pins, and even penknives; painful currents of electricity were used. To none of these did she respond. During her attacks her pulse was thready, ranging from 120° to 130° and upward; respiration sometimes could be scarcely detected, and sometimes fell as low as 10; body-heat was also much diminished. She recollected everything which passed during the attack. Different from Palma d'Oria, the examination of her skin revealed certain appearances. Between Saturday and Thursday oval spots and patches of rosy hue were to be seen on the backs and palms of the hands and on the backs and soles of the feet. They were very much in appearance as if the epidermis were thinned or scraped. The marks on the forehead were not permanent; the chest was only examined during the ecstasy. Before the bleedings blebs began to rise at the position of the spots. The bleeding commonly began in the night between Thursday and Friday. From the forehead of the girl blood sometimes oozed from minute points, which looked as if they had been made by microscopic leeches.
As regards the phenomena presented by Louise Lateau, various hypotheses have been advanced; the chief, however, are the three following: (1) The theological view—namely, that the stigmata were genuine miraculous performances, the blood flowing by supernatural command. (2) The view that the stigmata were genuine pathological phenomena, vaso-motor in character—that the bleedings were in some way similar to attacks of purpura hemorrhagica or to hæmidrosis or bloody sweat. (3) The view that the stigmata were produced by deceit—that in all probability, in order to excite the sympathy and astonishment which are so dear to the hysterical mind, the girl in some way caused the bleedings. The carefully detailed accounts of the phenomena seem to lend the strongest support to the last view.
A good test was employed for the detection of simulated stigmatization in the following case,17 which came under the care of Mr. Henry Lee at St. George's Hospital, London. An unmarried seamstress aged sixteen had on the outside of her right leg above the ankle a discolored patch, from which she said that every month for two years there had been a discharge of about a tablespoonful of blood. The patch was covered with minute red spots resembling flea-bites. Fresh red spots and effusion of blood were seen at succeeding visits. Lee ordered a sheet of lead to be applied over the bleeding surface, to be secured by a starched bandage. On the next visit, when the dressings were removed, a few spots and a little blood were found, but the sheet of lead was pierced with holes large enough to admit a needle. When asked how this had happened the girl was silent, and was discharged as a convicted impostor. In Lefevre's experiment with Louise Lateau he placed a leather glove upon one hand, tying and sealing it at the wrists; but it is easily to be seen why this test was not as thorough as that with the lead.
17 British Medical Journal, vol. i., 1871, p. 479.
Another case of ecstasy with stigmatization is cited by Bourneville and Hammond from Magnus Huss of Stockholm—a servant-girl twenty-three years old who was subject to convulsions, and also to [p. 351] hemorrhages, which usually came on as the result of great emotional disturbance. In her case examination showed no cicatrices. The hemorrhages occurred from the scalp, the eyes, the face around the eyes, the left ear, and the stomach. Her menstruation went on regularly during the attacks: sometimes she had ecchymoses and apparent bruises on the left half of the body, the limbs of which were semi-paralyzed for short periods. The attacks occurred with convulsions and unconsciousness, which usually lasted about half an hour, and from which she awakened as if from a long sleep.
Certain peculiar phenomena have been described under the head of femmes autographiques, or the autographic women, and are worthy of note. Dujardin-Beaumetz18 in a case of well-marked hysteria with loss of general sensibility reports that he was able to write or trace with a needle or pointed instrument on the skin. Within a space thus traced the skin was elevated in a white patch or plate. After some five minutes the line would show itself more and more in relief, until it attained from one and a half to two millimeters in thickness. It would remain from three to six, and sometimes twelve, hours. He varied the experiments in many ways, executing upon the skin designs, tables, and names of from ten to fifteen letters. He detected in the centre of some of the spaces traced a marked elevation of temperature, sometimes appreciable to the hand. This woman was known by the name of femme diche, or the autographic woman.
18 Bull. et Mém. Société médicale de Hôpital de Paris, 1880, 12, xvi. 197-202.
Dujardin-Beaumetz held that the phenomena were vaso-motor. The red lines traced readily admit of this explanation. The white space in relief, however, was not so easily explained. He had observed among hysterical women, under the influence of pressure, irritation, or the application of magnets, the appearance of patches of urticaria. One of the common tricks of the Spiritualists is to have the name of a spirit that has been called up appear upon the bared arm of the medium. Among friends and private patients, and among the hysterical patients in the wards of the Philadelphia Hospital, I have successfully performed experiments similar to those reported by Dujardin-Beaumetz. Such phenomena are by no means confined to cases of hysteria. One of my most striking successes in an attempt at skin-writing was in the case of a male physician of a peculiarly clear and pale complexion. Certain peculiar conditions of the skin will allow this to be done with facility. The similarity of this class of phenomena to that of the stigmata will at once appear evident. Such phenomena occur among the hysterical with a tendency to vaso-motor deficiency of control.
The wonderful saints who starved themselves or lived on sacramental bread are almost a multitude. Saint Joseph, Saint Catherine of Sienna, [p. 352] Saint Rose of Lima, Saint Collete, Saint Peter of Alcantara are of the number. In modern and even in recent times not a few of these cases have become widely known. Margaret Weiss, about whom a book was written in 1542, is said to have done without food and drink for three years. She suffered from pains and contractures. She passed neither urine nor feces; at least, such are the accounts which have come down to us.
Sarah Jacob, the Welsh fasting girl, has shared with Louise Lateau popular and medical notoriety. When about ten years old she suffered from various hysterical and hystero-epileptic symptoms. The quantity of food she took gradually dwindled; on October 10, 1867, it was said that she ceased to take any food whatever, and so continued till the day of her death, more than two years later. She had many visitors, pilgrims from far and near, who often left money or gifts. The vicar of her neighborhood came to believe in her, and an investigation was suggested. At one investigation, not very rigidly conducted, nothing was discovered. After a time she was visited by Fowler of London, who decided that the case was one of hysteria with simulation, probably associated with the power or habit of long fasting. Trained nurses were sent from Guy's Hospital to conduct the second watching. Under the watching the girl died, starved to death. The father was afterward condemned to imprisonment and hard labor for twelve months, the mother for six months. In Brooklyn a few years since one Molly Fancher, a similar case, attracted much attention, and was written about and commented upon by the press.
INTRODUCTION.—The term neurasthenia, signifying nervous weakness, and not rarely paraphrased by nervous exhaustion, indicates by its very derivation that it denotes not a distinct disease, but a condition of the body. The relations of the nervous system to the functions of organic and animal life are so intimate that almost all forms of exhaustion might well be discussed under the present heading. A further difficulty in attempting to decide the exact limitations of this article is to be found in the fact that hysteria, insanity, chorea, and various other nervous diseases are very closely connected with nervous exhaustion. Indeed, many of the cases which are considered by authorities as instances of neurasthenia would be more appropriately classed with one or other of the especial diseases. Thus, the nervous fears discussed in such detail by George M. Beard in his work upon neurasthenia plainly belong with the monomaniacal insanities, and, although they usually are associated with nervous depression, may coexist with great physical and mental power.
Further, very many chronic diseases produce neurasthenia. It has not been many years since general debility was a common inscription upon records of diagnosis. In very many cases the general debility afflicted the diagnostic powers or zeal of the physician rather than the body of the patient, and it is to be feared that neurasthenia not rarely at present replaces it. Malarial poisoning, chronic Bright's disease, chronic diarrhœa, lithæmia, and various other affections may be readily overlooked, and patient and physician satisfied with the diagnosis of neurasthenia; indeed, in my own experience in a very considerable proportion of the cases which had been diagnosed as nervous exhaustion the patient was really suffering from definite disease.
The folly of attempting to make neurasthenia a distinct affection is strongly brought out whenever it is attempted to give sharp diagnostic differences between it and other diseases. As examples may be noted the flat contradictions which exist in the different diagnostic tables given in the elaborate work of the late George M. Beard.
It is necessary, therefore, in the outset, to recognize that neurasthenia is a bodily condition which is very frequently associated with various chronic disorders, or not rarely coexists with perverted functional activity of the nervous centres, which perverted nerve-functions may, however, exist independently of any perceptible neurasthenia, and are not simply the outcomes of the neurasthenia. Under these circumstances an apology [p. 354] for devoting an article in this work to the consideration of neurasthenia may seem necessary to readers. The justification of the present discussion is to be found in the facts that neurasthenia often exists without the presence of definite disease, and that still more frequently it is a bodily condition which dominates in its therapeutic importance the manifestations of perverted functions, so that the patient is to be treated for it rather than for the disease with which it is associated.
ETIOLOGY.—There are various chronic diseases which may lead directly to nervous exhaustion. Neurasthenia may, moreover, be the result of disease which is long past; neglected diarrhœas, bleeding piles, and other affections with exhausting discharges, when they have been cured, may leave behind them conditions whose source and nature it is most important to recognize.
Overwork, excessive mental emotion, need only to be alluded to as capable of producing a pure neurasthenia. As Samuel Jackson was accustomed to say, in his lectures at the University of Pennsylvania thirty years ago, “Whenever the expenditure of nerve-force is greater than the daily income, physical bankruptcy sooner or later results.” It is to be remembered that the nerve-capital of persons differs almost as widely as does their moneyed capital. There are numerous families many of whose members are neurasthenics from birth—i.e. who are born with less power of creating nervous energy than is necessary to meet the requirements of the ordinary duties of life. There is every grade of natural endowment between the most feeble person, scarcely able to produce more nervous energy than is necessary for breathing, eating, and drinking, and the organism that is capable of enduring incessant toil. The development of neurasthenia is therefore not so much the result of a strain which is absolutely great as of a strain which is excessive in its relations to the organism which has to bear it.
SYMPTOMS.—The onset of neurasthenia is always gradual, although at times the condition appears to develop with great suddenness. Under these circumstances, however, the explosion has been preceded by a long train of more or less overlooked phenomena: thus, in a case that just now occurs to me a gentleman had long suffered from the premonitory symptoms of neurasthenia, to which he had paid but little attention until he was one day seized with violent vertigo, accompanied by such prostration of strength that he had to be taken home from the street in a carriage. The symptoms vary very much according to the portion of the nervous system which is especially affected, and also to some extent according to the etiology of the attack. Nervous exhaustion may in the beginning affect the whole of the nervous system, or it may be at first purely local and coexist with general nervous strength. Many cases of spermatorrhœa are instances of the local form of neurasthenia, the sexual centres being primarily affected; but as in these cases, sooner or later, the whole of the nervous system becomes implicated, so in other forms of the disorder the exhaustion, at first local, finally, if neglected, implicates the whole organism. There are not rarely cases of brain exhaustion in which the symptoms are at first purely local. Almost always the cause of a local neurasthenia is excessive use of the part; thus, cerebral asthenia is usually the result of mental overwork, sexual asthenia of sexual excesses, etc. When to the intellectual fatigue is added the depressing effects [p. 355] of excessive anxiety or allied emotions, the symptoms usually from the first are more general. The exhaustion may affect chiefly a single function of the brain. As an instance may be cited the case of a postal clerk now under my care, who has been accustomed to distribute five to eight thousand letters every day from a general mass into three hundred pigeon-holes representing as many post-office districts scattered over a large territory. As soon as the address is read there must be an instantaneous automatic recognition of the district to which the letter goes. It is at this place where, in the case now under consideration, the symptoms manifest themselves. Reading the address fails to produce immediate recognition of the locality to which the letter is to be assigned. Asked in what district such a post-office is, the clerk answers instantly, but seeing the address himself he hesitates, and sometimes balks so that he can distribute only about one-third as many letters as when in health. As in most cases of local nerve exhaustion, in this patient some evidences of general implication exist, there being decided disturbance of the sexual organs.
Another form of local neurasthenia which is frequently associated with brain exhaustion is that of writer's cramp. I have repeatedly seen it come on as the herald of a general breakdown; but under such circumstances the symptoms have usually not been those of typical writer's cramp: there have usually been not so much marked spasms as loss of power and distress in the arm on attempting to write.
In pure brain exhaustion loss of the disposition to work is usually the first symptom, the sufferer finding that it constantly requires a more and more painful effort of the will to perform the allotted task. The basis of this difficulty is largely loss of the power of fixing the attention, and this by and by is accompanied with weakness of the memory. Disturbances of sleep are frequent. Various abnormal sensations in the head are complained of. In most cases there is not absolute headache, but a feeling of weight or fulness or an indescribable distress, usually aggravated by mental effort.
It is true that in some cases of very dangerous brain-tire cerebration is performed with extraordinary vigor and ease; the power of work is for the time markedly increased, and even the quality of the product may be raised; the patient may even glory in a wild intellectual exaltation, a sense of mental power, with an almost uncontrollable brain activity. It is probable, however, that these cases are not instances of pure neurasthenia, but that there is an active congestion of the cortical gray matter. It is certain that they are very prone to end in serious organic brain trouble. In some cases of cerebral asthenia there are disturbances of the special senses, tinnitus aurium, flashes of light, and even the seeing of visions. Under these circumstances it is again probable that active congestion of the affected centres exists.
Severe cerebral neurasthenia may be associated with good spirits, but usually there is marked depression, and this perversion of function may finally go on to decided melancholy. The will-power, as all other functional activities of the brain, is prone to be weakened; morbid fears may finally develop themselves; and at last that which was at the beginning a simple brain exhaustion may end in hypochondriasis or insanity. In my own experience such ending is very rare unless there have been from the [p. 356] beginning marked symptoms of hypochondriasis or melancholy; in other words, unless there be the inborn tendency to distinct mental disorders, cerebral neurasthenia rarely produces them, but in a person who inherits such tendency the brain exhaustion may become an exciting cause of insanity.
The symptoms of brain-tire may be very largely existing in the individual who still has muscular strength and is capable of enduring much physical labor; but in most cases, sooner or later, the more general symptoms of neurasthenia manifest themselves.
Amongst the earliest of these symptoms may be disorder of the special senses. For reasons which are not very evident it is the eye which is generally affected. Although existing deafness is often greatly intensified by the coming on of nervous exhaustion, I cannot remember ever to have seen severe deafness entirely neurasthenic. The nature of the optical trouble is to be recognized by the fact that vision is at first good, but fails when the eye is steadily used for a few minutes, although the organ is physically perfect. This weakness of the eye may long be the most troublesome manifestation of the disorder.
In some instances, before any loss of muscular strength is marked, vaso-motor weakness is prominent. Excessive blushing on the slightest provocation, great flushing of the face after the use of alcohol or other stomachic irritant, waves of heat passing over the body, occasional pallors provoked by exertion or apparently causeless, and cold extremities, are some of the phenomena which mark the lack of power in the centres that control the blood-vessels. Closely allied to these disturbances are those of secretion. In my own experience the most marked of these is a tendency to night-sweats, but in some cases the hands, and more rarely the palms of the feet, are perpetually bathed in perspiration, which may be greatly increased by any emotional disturbance. In some patients there is a very great tendency to serous diarrhœa, which in its turn of course increases the nervous exhaustion.
In many neurasthenics the heart as well as the vaso-motor system sympathizes in the weakness, so that palpitation and shortness of breath not rarely follow even slight exertion: a more characteristic symptom is, however, a peculiar dropping of the heart's beat, which is to the patient at first very alarming, but which is entirely independent of any lesion of the heart itself. The true nature of this cardiac intermission is to be recognized by the existence of other symptoms of neurasthenia, and by the fact that it is not constant, and that it is very prone to follow eating or gastric irritation of any kind. Not rarely it is relieved at once by the belching up of wind. When tobacco has been very freely used the cardiac symptoms of neurasthenia usually come on very early, and may be very severe. Under these circumstances it is really a mixture of neurasthenia and tobacco-poisoning with which we have to deal.
The muscular strength may finally fail almost altogether. It is almost characteristic that the patient should be capable of much exertion under excitement, and should suffer from the results of such exercise not immediately, but after one or two days.
In many cases of neurasthenia atonic dyspepsia exists, but it is always a question for careful consideration how far a nervous condition is due to the dyspepsia and how far the dyspepsia is caused by the nervous condition.
[p. 357]Disturbances of sensation are common in neurasthenia, these disturbances taking the form in many instances of itchings or formication or other similar minor ills. Neuralgia is often severe and its attacks frequent, but I am convinced that something more than simple nervous exhaustion is responsible for its production. I believe that there is a neuralgic diathesis or temperament which is often associated with neurasthenia, but may exist without it, and which probably has, at least on many occasions, relations to a gouty ancestry. When such temperament exists the neuralgic attacks are greatly aggravated by the coming on of neurasthenia. Hyperæsthesia and anæsthesia mark the line where simple neurasthenia passes into hysteria. The same also is true of the peculiar tenderness over the spinal processes of the vertebræ, which is especially frequent in women, and is the chief symptom of the so-called spinal irritation or spinal anæmia—an affection which I believe to be a form of neurasthenia allied to hysteria.
In neurasthenia disturbances of the sexual organs are very common; in women great pain on menstruation, ovarian irritation, the so-called irritable uterus of Hodge, are closely connected with a general nerve weakness. In not a small proportion of the cases of uterine disorders which are often locally treated I believe the local disease is largely the expression of the general condition. It is well known that masturbation and sexual excess in the male may produce an exhaustion of the nerve-centres especially implicated and also a general nervous exhaustion. This is the common history of spermatorrhœa. It is no less true that a general neurasthenia may produce a local weakness of the sexual centres, with symptoms at least resembling those of spermatorrhœa—namely, great irritability of the sexual organs, with a practical impotence due to immediate seminal discharge whenever coition is attempted. I have certainly seen this condition result from excessive intellectual labor when there has been no sexual excess, and at a time when the muscular strength was still good. Such cases may, perhaps, be distinguished by the fact that unprovoked emissions are not nearly so apt to occur as in true spermatorrhœa.
TREATMENT.—The natural cure for neurasthenia is rest, and my own experience coincides with the logical inferences to be drawn from an etiological consideration of the subject—namely, that medicines are only of limited value, and unless very judiciously administered may readily do harm. Disturbing symptoms should be met and tonics may be used, especially strychnine and arsenic, but all drugs hold a secondary position in the relief of a pure neurasthenia. In using remedies the practitioner must be guided by general principles, and I shall not engage in any detailed consideration of the subject, but employ the space at my disposal with a discussion of rest.
When nervous exhaustion has been produced by over-use of any one organ or system of organs, absolute rest of such organ is a primary necessity. Thus, when there has been sexual excess absolute avoidance of use of the sexual organs must be enjoined, and in married Americans it is often essential to insist upon man and wife occupying distinct apartments1 or even to separate them by a journey.
1 Because in this country man and wife habitually occupy one bed. Sexual continence under these circumstances can only be obtained at the cost of a suppressed sexual excitement worse than moderate indulgence.[p. 358]
Again, in cases of brain-tire it is the brain which should be rested. To rest an overwearied, excited brain is often not an easy task. In attempting it the effort should be to obtain the following results: 1st. The removal of all cares, anxieties, and all brain-work, especially those of such character as have been connected with the breakdown. 2d. The maintenance of the interest of the patient, so that the past shall for the time being be forgotten, and the present not overweighted with irksomeness. 3d. Invigoration of the physical health of the whole body, and especially of the nervous system. In order to obtain the first of these measures of relief, isolation of some sort is essential; for the second mental occupation is usually required; for the third fresh air, exercise, or some substitute is to be superadded to abundant food and rest.
The proper method of meeting these indications varies greatly, not only with the varying physical conditions and idiosyncrasies of patients, but also with their diverse domestic and pecuniary relations. To give detailed directions for every case is impossible, and I shall therefore limit myself first to simple cases of brain-tire in which the muscular strength is preserved; second, to cases of profound general neurasthenia.
In brain-tire travel is usually recommended, and travel affords, when properly directed, separation from old cares and thoughts, a maintenance of interest by a succession of novel sights and experiences, and the physical stimulation of fresh air and exercise. In bad cases general travel is too stimulating, and ocean-voyaging is much better. Upon the ocean is to be found nothing provocative of thought, only complete isolation, fresh air, enjoyment if the patient be fond of the sea, and a sufficient exercise, especially if the sufferer in any large measure works in the management of a sailing vessel. Hence prolonged yachting affords in many cases our best method of relief. The isolation of the North Woods or any other large primeval wilderness may be complete, the air most fresh, and the exercise to be had also boundless, but at the same time controllable; the man may, according to his will, lie in his tent and be fed by his guide or be unceasingly active. If the life be agreeable to the sufferer, and sufficient care against undue exposure be exercised, the camp-cure is most efficient. European travel may serve almost equally well, provided hard journeying, sight-seeing, and even cities are avoided. The quiet of Switzerland or the Tyrol may bring restoration when the bustle of London and Paris might complete the ruin.
To those who cannot travel extensively the seashore, mountains, or lowlands of the United States are open, and the best way of meeting the indications in any individual case must be determined by a joint consultation between doctor and patient.
There are cases of neurasthenia in which the slightest exercise does harm, and in which even the unconscious effort of company and conversation is an injury. Between the extremely exhausted and the slightly brain-tired is every grade of case, and much tact is often required in properly regulating the treatment of the individual case.
It is only the most severe forms of neurasthenia which require the use of the so-called rest-cure. For such, however, it is a very valuable method of treatment. It finds its most brilliant application undoubtedly in neurasthenic women, but, more or less modified according to circumstances, it has a wide scope in the treatment of both sexes. When the bodily condition is [p. 359] developed by prolonged lactation, nursing, grief, overwork, acute disease, or other temporary or removable cause, the rest-cure may give permanent relief; and even when the cause of the neurasthenia is largely inherited feebleness of constitution, it is a valuable though a more temporary remedy. This method of treatment has long been used in this city, and was especially dwelt upon in its general scope by Samuel Jackson, but in its modern form it has become a very valuable method of treatment, essentially different in its details from what it was formerly, and far more potent in its influence. To S. Weir Mitchell is due a great debt of gratitude, for by him has this improvement been made.
The principles of the rest-cure are absolute rest, forced feeding, and passive exercise. Absolute rest is often prescribed by the physician without being sufficiently definite and insisted upon. When it is desired to apply it most strictly, it should be clearly explained that the patient is not to be allowed to get out of bed even to pass urine or feces, not to feed himself or herself, or perform any act of the toilet whatsoever. The rest also must be for the mind as well as for the body, and it is essential that the patient be isolated. Separation from friends should especially be insisted upon in the case of women. It may be possible to separate a man in his own house completely from his daily cares, but a woman in her own house is in the midst of her daily business, and is like a man placed in the corner of his factory. In obstinately severe cases of neurasthenia complete and absolute isolation is a sine quâ non, and especially when there is a decidedly hysterical element is it necessary to separate the patient entirely from her friends. Under these circumstances there must be a well-trained nurse who is personally agreeable to the patient. The confinement would be very irksome to any except the most exhausted patient were it not for the daily visit of those engaged in the treatment; to further provide against ennui the nurse should be a good reader, so that under the definite instructions of the physician she can occupy a certain portion of the time in reading to the patient.
In order to maintain the functions of the skin the patient should be well sponged in bed every morning after breakfast. A strong solution of salt, or, better, sea-brine, is to be preferred to simple water, and frequently it may be followed by the use of alcohol. In very feeble cases the alcohol may be employed alone. I have seen very good effects from momentarily rubbing each portion of the skin with ice just after the bathing.
The question of feeding is one of great importance, and requires the utmost care and attention from the physician. The end to be attained is to feed the patient as much as can be digested, but not to overdo and derange the digestion. Food should be given at intervals of two or three hours, and must be both light and nutritious. It should, at least at first, largely consist of milk, except in those rare cases in which that fluid does really disagree, and not merely is thought to do so. The milk should be skimmed or given in the form of koumiss. Beef and other concentrated meat-essences are valuable as stimulants, and may be used, especially as the basis of soups. Various farinaceous articles of food may be added to them, or if an egg be broken into the concentrated bouillon or beef-essence just as it ceases boiling a nutritious, and to many persons palatable, dish is obtained. When constipation exists, oatmeal [p. 360] porridge, Graham bread, fresh or dried fruits may be allowed if readily digested by the patient. In order to give an idea of the general plan of the dietary, the following schedule of the daily life is given. Such a schedule should always be put into the hands of the nurse, who should be required to follow it strictly. It must be altered from day to day, so as not to weary the patient with monotony. It is especially important to remember that the diet must be carefully studied for each patient, and be adapted to the individual requirements of the case. Success will in a great measure depend upon the practical skill and tact of the physician in this adaptation:
| 8 | A.M. | Rolls or toast; cocoa or weak coffee, or roasted wheat coffee; beefsteak tenderloin or mutton chop. |
| 9 | A.M. | Bathing. |
| 11 | A.M. | Oatmeal porridge, with milk, or else a pint of koumiss. |
| 12 | M. | Massage. |
| 2 | P.M. | Dinner: Bouillon with or without egg; beefsteak; rice; roast white potatoes; dessert of bread pudding, blanc mange, or similar farinaceous article of diet. |
| 4 | P.M. | Electricity. |
| 5 | P.M. | Milk toast. |
| 9 | P.M. | Half pint of skimmed milk or koumiss. |
In many cases the patient at first can take very little food, and it is very frequently best to begin the treatment with an entirely liquid diet, giving milk every two hours, or using Liebig's raw-meat soup, with milk or plain farinaceous food, and only after a time gradually accustoming the patient to solid food. Not rarely a prolonged treatment by the so-called milk diet is of avail. The rest-cure is indeed largely based upon a careful regulation of the food; but a full discussion of the various dietaries to be used would require a treatise upon dietetics.
Passive exercise is to be obtained by the use of electricity and massage, the object being to get the effects of exercise upon the nutrition and circulation without the expenditure of the patient's nerve-force. By the use of electricity muscular contractions are secured which simulate those which are voluntary and more or less thoroughly replace them. By the general application of the current to the whole body we probably affect the tone of all of the minute blood-vessels, and certainly in this or some other way stimulate the general nutrition, and, as has been shown by S. Weir Mitchell, for the time being elevate the bodily temperature.
The faradic current is alone used. It is applied in two ways: first, to the individual muscles; second, to the whole body. The séances should be daily, the operator beginning at the hand or foot, and systematically faradizing each muscle of the extremities and trunk.
The slowly-interrupted current is generally preferable, but advantage is sometimes gained by varying the rapidity of the interruptions. The general rule is to select that current which produces most muscular contraction with the least pain. The poles should be applied successively to the motor points of the muscles, so as to contract each firmly and thoroughly. This process should occupy from thirty to forty minutes. The electrodes are then to be replaced by large sponges well dampened with salt water: one of these should be put at the nape of the neck and the other against the soles of the feet, and a rapidly-interrupted current, as [p. 361] strong as the patient can bear, should be sent through the body for twenty minutes or half an hour. It is not necessary for the operator to remain during this time. In some cases the electrical programme may be varied so as to get a local stimulant action from the general current; thus, when digestion is enfeebled and the bowels costive for a portion of the time one of the sponges may be placed upon the epigastric region. In women when there is great abdominal and pelvic relaxation one pole may be placed high up in the vagina. I have seen old-standing prolapses cured in this way. Some electro-therapeutists claim great advantage from galvanization of the cervic sympathetic ganglia, but I do not myself believe that they ever succeeded in reaching these ganglia with the current.
Massage, like electricity, affects greatly the peripheral circulation, empties the juice-channels, and gives tone to the muscular system. It must be clearly distinguished from rubbing of the skin. It consists in manipulations of such of the muscles as are not too deep to be reached, and of the cellular tissue: in order to lessen as much as may be the skin friction by these manipulations, it is often well to anoint the surface with cocoanut or other bland oil. As sold in the drug-stores, cocoanut oil is very often rancid, and at any time it is well substituted by the cheaper cottonseed oil. In practising massage it is essential to remember that the natural course of the venous blood and the juices of the cellular tissue is toward the centre of the body; therefore, all general movements should be practised in this direction.
The manipulations are percussion, rolling, kneading, and spiral. They consist of movements made with the pulpy ends of the fingers and thumbs, and spiral movements with the whole hand so folded as to adapt its palm to the limb. In percussion the strokes should be from the wrist, and should be quick and short. It is probably not possible, even by long strong strokes, to affect deep muscles. In the rolling manipulation the effort is to roll the individual muscles beneath the pulps of the fingers. This manipulation may be varied by pinching the muscles, not the skin, and kneading. In each case it is intermittent pressure upon the muscles which is aimed at. The circular movements are to be in opposite directions with both hands simultaneously, the limb being grasped by one hand a little above the other, and a spiral sweep made up the limb, the ball of the thumb and the palm of the hand resting upon the patient, and the pulpy parts of the thumb and the fingers grasping the limb. It is especially such motions as these which affect the circulation of the flesh-juices.
The length of time the patient is to be kept in bed and treated in the manner described varies of course with the individual case, but usually less than four weeks is not sufficient, and rarely are more than six weeks required. In getting up, the patient should begin by sitting up one or two hours a day, increasing daily, but not too rapidly, the time of being out of bed and the amount of exertion made. The electrical treatment should be gradually intermitted: in many cases massage twice a week seems to be of service even after the patient is about. In the going back to ordinary daily life great care is to be exercised to proportion the amount of exertion to the newly-obtained strength, so as not to lose what has been gained. In cases of natural or of long-standing acquired [p. 362] severe neurasthenia the mode of life must be arranged to correspond with the small daily product of nervous energy.
In dismissing this subject I desire to caution against a routine employment of this so-called rest-cure, which might readily degenerate into a species of quackery; and, again, to call attention to the widespread value of the principles which underlie it, and the importance of the physician applying those principles with endless modifications of detail.
The regularly-recurring incidence of natural sleep forms one of the most important subjects of physiological investigation. Occurring ordinarily at stated intervals connected with the diurnal revolution of the earth, it may for a time be postponed by an effort of the will, but an imperious necessity for repose finally overcomes all opposition, and the most untoward circumstances cannot then prevent the access of unconsciousness. Thus produced, the relation of cause and effect between weariness and sleep becomes very apparent. The refreshing influence of such repose points clearly to the restorative character of the physical processes that continue despite the suspension of consciousness; it also renders evident the final cause of that periodical interruption of activity which the brain experiences in common with every other living structure.
Careful observation of the manner in which sleep invades the body indicates that its evolution is not associated with a simultaneous suspension of every mode of nervous function. The sense of sight is the first to yield. The eyelids close and the muscles that support the head give way. The body seeks a recumbent position; quiet and seclusion are instinctively sought. The purely intellectual faculties are not yet depressed, and the reflex energies of the spinal cord are exalted. Soon, however, the other senses fail; hearing persists the longest of all. Released from the control of external impressions, the internal senses preserve their functions after a strangely-disordered fashion, dependent upon the progressive suspension of activity in the various cerebral organs. First the power of volition ceases; then the logical association of ideas comes to an end. Presently the reasoning faculties disappear, and judgment is suspended. We thus become no longer capable of surprise or astonishment at the vagaries of memory and imagination, the only mental faculties that remain in action. To their unrestrained function we owe the presentation in consciousness of the disorderly picture which we call a dream. During the early stages of this somnolent state we often remark the fact of dreaming, and an effort at attention may produce a partial awakening; but usually the subsidence of cerebral function is progressive and rapid. The fire of imagination fades; the field of consciousness becomes less and less vividly illuminated; the entire nervous apparatus yields to the advancing tide; and, finally, the dominion of sleep is fully confirmed.
[p. 364]During the act of awaking the order of sequences is reversed. From the end of the first hour of repose the depth of sleep, at first rapidly, then more gradually, diminishes.1 Dreams disturb its quiet, mental activity increases, the power of volition revives; once more the individual is awake.
1 Kohlschütter, Messungen der Festigkeit des Schlafes, Dissert., Leipzig, 1862, and Zeitschr. f. Rat. Med., 1863.
Sleep, then, is that condition of physiological repose in which the molecular movements of the brain are no longer fully and clearly projected upon the field of consciousness. This condition is normal, and must, consequently, be differentiated from all pathological states which produce its counterfeit by the more or less complete abolition of consciousness. This distinction becomes the more necessary because the presence of the common factor, unconsciousness, in the result has frequently led to the mistake of supposing a community of antecedents in the changes by which the passage from sensibility and consciousness to insensibility and unconsciousness is effected. It needs no argument to show that the insensibility of artificial anæsthesia is a very different thing from the unconscious condition which obtains during natural sleep. Between the stupor of intoxication and the healthful restoration of cerebral energy which accompanies genuine sleep there can be no rational comparison. It is therefore in the phenomena of syncope that the likeness of sleep has usually been sought. The well-known fact that a copious hemorrhage can speedily develop a condition of muscular relaxation, insensibility, and unconsciousness has led certain observers to the belief that natural sleep is, after all, only a species of physiological syncope. The antecedent conditions of syncope are so different from the prodromata of sleep that it is difficult to see how either state can be properly likened to the other. The bloodless condition of the brain which occasions syncope is always the result of pathological or accidental causes, and is not identical with the comparatively insignificant reduction of blood-pressure which may be observed in the brain of the healthful sleeper. It is, moreover, worthy of note that sleep is the normal condition of the unborn child, despite the fact that the growing brain receives a richer supply of oxygenated blood than the trunk and the lower limbs—a state of the circulation quite unlike that of syncope.
Fully impressed by the force of such considerations, certain physiologists2 have reasoned from the analogies suggested by the results of muscular fatigue, and have imagined an hypothesis accounting for the occurrence of sleep by a supposed loading of the cerebral tissues with the acid products of their own disassimilation during wakeful activity. The acid reaction of the brain and of the nerves after exertion suggested the probability that an excessive presence of lactic acid and its sodic compounds might be the real cause of cerebral torpor and sleep. Could the hypothesis be proved, ordinary sleep would take its place in the anæsthetic category and sodic lactate should be the very best of hypnotic agents. Unfortunately for this doctrine, the administration of the lactates has yielded only the most contradictory and unsatisfactory results. It, [p. 365] moreover, furnishes no explanation of intra-uterine sleep nor of the invincible stupefaction produced by cold.
2 Obersteiner, “Zur Theorie des Schlafes,” Zeitschr. f. Psych., xxix.; Preyer, “Ueber die Ursachen des Schlafes,” Vortrag. Stuttgart, bei Enke, 1877; and Centralbl. f. d. Med. Wiss., 1875, S. 577.
Far more comprehensive is the hypothesis of Pflüger.3 According to this view, the cortical tissues of the brain are recruited by the assimilation of nutrient substances derived from the blood. By this process oxygen is stored up in chemical combination, forming explosive compounds whose precise composition is not fully understood. Under the influence of the various nervous stimulations that reach the brain these unstable compounds break up into simple forms. The motion thus liberated by these explosions is, in some way at present utterly unintelligible to us, projected into the field of consciousness where the mind dwells, and we are thus brought into conscious relation with the external world. That the capacity for thus signalling across the gulf which separates matter from mind is the result of a certain perfection and complexity of material structure is rendered probable by the utter failure of the infracortical organs of man to impress the conscious intelligence by any amount of independent activity. It is also indicated by the unconscious sleep of the rudimentary fœtal brain and by the brevity of the intervals of wakefulness which mark the life of the new-born babe. That this capacity is dependent upon the mobility of the atoms of the brain is shown by the speedy cessation of intelligence which follows great reduction of temperature, as in hibernation or during exposure to severe frost. That its exercise is largely dependent upon the activity of the senses is proved by the effects of interference with their function. A recent observation, recorded by Strümpell,4 is very significant in this connection: A young man had lost all power of sensation excepting through the right eye and the left ear. A bandage over the eye and a plug in the ear arrested all communication between his brain and the external world. Thus imprisoned within himself, he gave utterance to an expression of surprise, and sought in vain, by clapping his hands, to arouse the sense of hearing. At the end of two or three minutes these efforts ceased; respiration and pulsation were deepened and retarded, and removal of the bandage exhibited the patient with his eyes closed in genuine sleep.
3 “Theorie des Schlafes,” Arch. f. d. Ges. Physiol., x. 468.
4 “Beobachtungen ueber ausgebreitete Anästhesien und deren Folgen,” Deutsch. Arch. f. klin. Med., xxii.
The dependence of the waking state upon the presence and functional activity of a sufficient quantity of a peculiarly unstable form of protoplasm in the brain is an hypothesis which presents no great difficulty of comprehension. But how may we explain the passage from the vivacity of that waking state into the inactivity of sleep? I have elsewhere5 discussed the manner in which artificial sleep is produced by impregnation of the brain with anæsthetic substances, and the same general line of argument may be extended to cover the action of every stupefying agent with which the blood may become overcharged. Could the hypothesis of Obersteiner and Preyer be accepted, it would be an easy matter to explain the advent of sleep when it gradually supervenes; but we cannot thus explain the rapid and intentional passage from wide-awakefulness into the profoundest sleep, such as becomes a matter of habitual experience with sailors and with others who have formed the habit of going at once [p. 366] to sleep at regularly-recurring periods of time. Certain writers have endeavored to account for this fact by imagining a special mechanism at the base of the brain (choroid plexuses of the fourth ventricle, etc.), by means of which the current of blood through the brain may be voluntarily diminished, with a consequent arrest of conscious activity. But, still adhering to the hypothesis of Pflüger, we shall find a clearer explanation of the facts by considering the phenomena connected with the succession of impressions upon the organs of sense. It has been ascertained6 that such impressions must persist for a certain measurable length of time in order to excite conscious perception. A sound must be prolonged for at least 0.14″, a ray of light must agitate the retina for 0.188″–0.2″, ordinary contact with the surface of the body must continue during 0.13″–0.18″, in order to produce any knowledge of sound and light and common sensation. For the simplest act of perception 0.02″–0.04″ are necessary. It is therefore perfectly reasonable to suppose that when the explosive material of the brain has been sufficiently reduced in quantity and quality by prolonged cerebral effort, the impression of sense may no longer suffice to excite in the cortical substance vibrations of sufficient length, or following each other in sufficiently rapid succession, to sustain the conscious state. The cortex of the brain may then be likened to the surface of a body of water into which bubbles of soluble gas are introduced from below. When the bubbles are large and succeed each other rapidly, the surface is maintained in a state of continual effervescence. But if the size of the bubbles be diminished or if the solvent capacity of the liquid be increased, its surface will become almost, if not quite, perfectly tranquil. In some such way, without any great amount of error, may we picture forth the molecular changes that determine the advent of sleep.
5 Artificial Anæsthesia and Anæsthetics, pp. 15-17.
6 Carpenter's Physiology, 8th ed., p. 852.
Returning now to the subject of the rapid induction of sleep, we find that it usually occurs among people who lead an active life in the open air, like children and laborers, and are perhaps compelled to endure frequent interruptions of their rest. The sailor who is trained to sleep and to work in rapidly-successive periods of time—four hours on deck and four hours below—has virtually become transformed by this habit into a denizen of a planet where the days and the nights are each but four hours long. His functions become accommodated to this condition; his nervous organs store up in sleep a supply of protoplasm sufficient only for an active period of four or five hours, so that when his watch on deck is ended he is in a state as well qualified for sleep as that of a laborer on shore at the end of a day of twelve or fifteen hours. Moreover, the majority of those who manifest the ability thus to fall asleep are individuals whose waking life is almost entirely sustained by their external perceptions. So soon, therefore, as such excitants are shut out by closing the eyes and by securing shelter against the sounds and impressions of the air, comparatively little remains for the production of ordinary consciousness, and sleep readily supervenes, especially if the excitable matter of the brain has been already depleted by active exertion.
It is well known that a predisposition to sleep may be very quickly induced by extraordinary expenditures of force; witness the effect of the venereal act and the consequences of an epileptic fit. That analogous [p. 367] predispositions may indeed be very rapidly developed by modifications of cerebral circulation is shown by the sudden reduction of cerebral excitability during the act of fainting. But this does not prove that cerebral anæmia should be elevated to the rank of the principal cause of natural sleep. In all such cases the nervous process is the primary factor and the direct cause of change in the circulation.7 The character of these changes has been admirably illustrated by the observations of Mosso.8 By the aid of the plethysmograph this experimenter was enabled to compare the state of the circulation in the human brain, laid bare by erosion of the cranial bones, with the movement of the blood in other portions of the body. The occurrence of sleep caused a diminution in the number of respirations and a fall of six or eight beats in the pulse. The volume of the brain and its temperature were at the same time slightly reduced through the diversion of a portion of the blood-current to other regions of the body. If during sleep a ray of light was allowed to fall upon the eyelids, or if any organ of sense was moderately excited without waking the patient, his respiration was at once accelerated, the heart began to beat more frequently, and the blood flowed more copiously into the brain. Similar incidents accompanied the act of dreaming. The renewal of complete consciousness was followed by an immediate increase in the activity of the intracranial circulation.
7 W. T. Belfield, “Ueber depressorische Reflexe erzeugt durch Schleimhautreizung,” Du-Bois Reymond's Archiv, 1882, p. 298.
8 Ueber den Kreislauf des Blutes im menschlichen Gehirn, Leipzig, 1881.
In all these variations it is worthy of note that the nervous impression was the primary event. The changes of blood-pressure and circulation were invariably secondary to the excitement of nerve-tissue. Sleep, therefore, is the cause, rather than the consequence, of the so-called cerebral anæmia which obtains in the substance of the brain during repose. This condition of anæmia is nothing more than the relatively lower state of circulation which may be discovered in every organ of the body during periods of inactivity. Every impression upon the sensory structures of the brain occasions a corresponding liberation of motion in those structures. The movement thus initiated arouses the vaso-dilator nerves of the cerebral vessels and excites the vaso-constrictor nerves of all other portions of the vascular apparatus. Hence the superior vascularity of the brain so long as the organs of sense are fresh and receptive; hence the diminishing vascularity of the brain as its tissues become exhausted and unexcitable; hence the unequal and variable vascularity of different departments of the brain as sleep becomes more or less profound. These modifications of the brain and of its circulation are well illustrated by the effects of a moderate degree of cold applied to the cutaneous nerves of the body, as not infrequently happens when the night air grows cool toward morning. Such moderate refrigeration of the skin excites its sensitive nerves, which transmit their irritation to the brain. The excitement of this organ causes dilatation of its vessels, with increased irritability of the cortex, vigorous projection into the field of consciousness, and the consequent occurrence of dreams denoting imperfect slumber or even complete awakening. The remedy consists in the application of gentle heat to the surface of the body. By this means the transmission of peripheral irritation is checked; the brain becomes tranquil; sleep [p. 368] supervenes. A similar wakefulness is in like manner produced by unusual heat. The remedy here consists in the employment of measures calculated to reduce the temperature of the skin to the normal degree. Sometimes wakefulness is maintained by some less general irritant. The feet alone may be cold, either because of previous refrigeration or because of local hyperæmia occurring elsewhere in an anæmic subject. There, again, equalization of the circulation—that is, the removal of cerebro-spinal irritation—may be all-sufficient to procure sleep. Noteworthy also is the tranquillizing effect of foot-baths or of the wet sheet in many cases of cerebral excitement and wakefulness. In like manner, that form of sleeplessness which often follows intense mental activity may generally be obviated by a light supper just before going to bed. Activity of the stomach is thus substituted for activity of the brain, and the consequent diversion of blood is sufficient to reduce the production of excitable matter in the brain to a point that permits the occurrence of sleep. A morbid exaggeration of this process is sometimes witnessed in the soperose condition that accompanies digestion in patients whose blood has been reduced by hemorrhage or by disease. In such cases the nutrition of the brain proceeds at so slow and imperfect a rate that any considerable diversion of blood toward other organs produces a syncopal slumber which resembles normal sleep only by the fact of unconsciousness. If, however, food be taken in excessive quantity or of irritable quality, the consequent indigestion will produce nervous excitement, reaching perhaps to the brain, and preventing sleep.
The most interesting question regarding sleep concerns the condition of the mind during repose. We know that while the body is awake the mind is always active: does this activity entirely cease during the period of sleep? The phenomena of certain varieties of trance indicate that the mere semblance of death is not incompatible with great mental activity. In like manner, the phenomena of dreams serve to prove that various intellectual processes, such as memory, imagination, attention, emotion, and even volition, may still be exercised while every external avenue of special sense is closed by sleep. The result of the exercise of mental activity under such conditions constitutes a dream. The fact that observers who have made trial in their own persons have always found themselves engaged with the details of a dream when suddenly awakened from deep sleep has been supposed to afford valuable proof of the proposition that the mind is never wholly inactive during the deepest sleep. To say nothing of the significance of certain somnambulic states (double consciousness), in which intelligence evidently exists for a long period of time without leaving any subsequent trace in memory, the mere fact that we remember very few of the events that occupy the mind in dreams cannot be urged against the doctrine of continuous mental action, for we remember very few of the images and ideas that have stirred the depths of consciousness during the waking state. Our recollection of dreams is exceedingly variable. Sometimes we retain in memory all the events of a long and complicated vision, but usually, though entranced by the vivid [p. 369] beauty of the spectacle that unrolls its splendor before the eye of the mind in sleep, and though the intensity of its seeming action may be sufficient to awaken the dreamer, who recalls each incident as he reviews the picture during the first waking moments, the impression soon fades, and the coming day finds him incapable of reproducing a single scene from the nocturnal drama.
The space allotted to this article will not admit a full discussion of the physiology of dreams. A brief reference to the definition of sleep must suffice to indicate what is signified by the process. Sleep does not wholly arrest the functions of the brain. A certain amount of projection into the field of consciousness seems to continue even during the most perfect repose, and the ideas thus aroused form the material of our dreams. Our waking hours are occupied with the ideas and with the associated trains of thought that are presented in consciousness through the action of our several senses. As a consequence of the harmonious function of these senses, correcting and supplementing each other, a continuous process of logical thought is maintained. But along with the procession of ideas which are distinctly conceived by the mind, the field of consciousness is also invaded by a cloud of half-formed perceptions that are too imperfect and too fleeting to occupy the attention. As in the act of sight, though the periphery of the visual field is clouded with a whole world of objects dimly perceived without arresting particular attention, the centre of that field alone presents a clear image before the brain, so the eye of the mind perceives clearly only a few of the impressions which enter the sphere of consciousness. These neglected perceptions, however, are none the less the result of abiding impressions graven in the substance of the brain, from which, through the action of memory, they may at any favorable opportunity re-enter consciousness. It is well known that a suspension of the functions of any portion of the nervous apparatus tends to increase the energy of the remaining organs; consequently, it becomes highly probable that with the arrest of external perception in sleep the activity of certain portions of the brain must be considerably exalted, so that the impressions which they have previously registered may now more clearly reach the seat of consciousness. The probability of this hypothesis is greatly strengthened by numerous facts that lie open to observation. During the first moments that succeed the closing of the eyes mental activity and the power of attention are not diminished, but are rather increased. As the controlling influence of the cerebrum is withdrawn the reflex energy of the spinal cord becomes temporarily exalted. Witness the paroxysms of cough that sometimes harass a sleeping child who has scarcely coughed at all during his waking hours. Witness the voiding of urine in the bed by nervous children during the early hours of sleep. Witness the phenomena of night-terrors, which always occur at the time of night when sleep should be most tranquil.
It appears, therefore, that the harmonious activity of all parts of the nervous system is indispensable to the highest exercise of the conscious mind. Healthy intellectual life is the perfectly-balanced outcome of the complex polygon of forces which has its seat within the brain. But the suppression of certain lines of this polygon does not suppress life, nor does it necessarily destroy consciousness. It only occasions a redistribution of force and a proportionate narrowing of the stream of related [p. 370] ideas. Since the suppression just mentioned is not an absolute quantity, but a variable factor, the polygon of forces in the brain and the corresponding succession of ideas in consciousness must necessarily be in a state of continual change. Accordingly, our dreams are as variable as the clouds that drift upon the currents of the air. As on a hot day in summer, when the steady equatorial draught has ceased to guide the wind, we may observe all manner of local tides in the masses of vapor which arise from the earth, so in sleep, when the guiding influence of the senses is withdrawn from the brain, the ideas that still arise are chiefly dependent upon its automatic and reflex action for their origin and association. Undisturbed by impulses from the external world, the brain seems then more sensitive to impressions that originate within the body. An overloaded stomach, an enfeebled heart, a turgid sexual apparatus, or an irritable nervous ganglion may become the source of irregular and uncompensated movements which may invade the cerebral cortex, and may there set in motion a whole battery of mechanisms whose influence upon consciousness would be quite unnoticed were the external senses in full operation.
The preceding argument will render it easy to comprehend the phenomena of night-terrors. These are commonly observed in young children of a highly nervous temperament before the conclusion of their second dentition. The subjects of the disorder are generally of neurotic descent. Insanity, hysteria, neurasthenia, epilepsy, chorea, and nervous dyspepsia are often discovered among their near relatives. Not infrequently they have been or will become themselves choreic.
The attack is often preceded by symptoms of indigestion, but it may result simply from the commotion of a brain wearied by the excitement and effort of the previous day. The little patient starts up out of an apparently sound sleep crying with alarm, calling for his mother, and staring wildly with every possible expression of terror. Sometimes he springs from his couch and runs headlong into a corner or seeks to hide under the bed, as if escaping from some frightful object. The eyes are open, tears flow, perspiration covers the skin, there is the greatest excitement, and the little one, convulsively clinging to its parent, will not be quieted. Only after fifteen or twenty minutes, as tranquillity gradually returns, does the child seem to recover the power of recognizing his friends. Presently, however, he lies down and falls quickly asleep, waking in the morning without the slightest recollection of the unpleasant event.
Such paroxysms occur during the early part of the night, one or two hours after the child has been put to bed, just at the time when, according to the previously-quoted experiments of Kohlschütter, sleep is passing from its maximum intensity to a lesser degree of depth. This, then, is the time when the controlling power of the sensory apparatus over other portions of the nervous system has already reached its minimum. The spinal centres and those intracranial ganglia which do not share in the full measure of this repose are therefore in a condition of relative [p. 371] exaltation. Disturbances of internal organs consequently produce inordinate excitement of these waking portions of the nervous apparatus. The morbid quality of this excitement is attested both by the history of the patient and by the fact that it does not arouse the whole brain. The distribution of motion in the cerebrum is impeded, so that certain portions of the organ remain asleep while other regions are thrown into a state of tumultuous uproar. Disconnection of these different organs of the nervous system, by withdrawing particular portions from the inhibitory influence of the remaining parts, gives opportunity for violent explosions of nervous force analogous to the convulsions of a headless fowl or to the course of an epileptic paroxysm. Now, in sleep, in somnambulism, in hypnotism, in delirium, in certain stages of intoxication with alcohol or with narcotics, such ungearing of the different nervous ganglia is more or less completely effected. In narcotic and anæsthetic sleep besides the disassociation of ganglia there is paresis of the nervous molecules; hence the phenomena soon merge into insensibility and coma. But in natural sleep, in somnambulism, or in hypnotism there is no toxic paresis; hence the dissociated portions of the brain and nervous system, if aroused, are in a physiological condition to dispense great stores of force. Hence the vividness of certain dreams and the astonishing vigor of particular nervous functions in somnambulism and hypnotism.
The phenomena of night-terrors constitute merely a special form of somnambulism, a condition of which the mechanism, so far as the present state of cerebral physiology will permit, has been already suggested. The affection should not be ranked by itself as a particular variety of disease, but should rather be considered a violent perturbation in the cerebral organs of a neurotic subject during the period of sleep. In ordinary dreaming the muscular apparatus usually remains passive, even though the dream be a nightmare or an incubus of the most terrifying character. But when the desires and the emotions are powerfully addressed by the dream, a certain amount of muscular movement may ensue, as when a dog barks in his sleep, or when a child laughs upon his nurse's lap, or when a weary soldier marches on though overpowered by sleep. One night, when parched with thirst during a voyage at sea,9 I saw in sleep a sparkling fountain, by the side of which appeared a young girl holding out a cup of cold water. Awakened by the excitement, I found myself sitting up in bed with my right arm extended in the direction of the tantalizing vision: my dream had merged itself in action. In like manner, the victim of night-terrors not only moves his body, but gives vocal expression of his feeling of apprehension and alarm. In like manner, projecting his dream into action, a sleep-walker may arise from his bed; he climbs out of the window and descends to the ground, executing all manner of complicated and dangerous movements; he walks long distances, and finally returns to his couch without waking. In the morning no recollection of the event of the night survives. Again, the movement [p. 372] may be less locomotive in its character. The intellectual faculties chiefly may be aroused, and then only such movements are executed as may be necessary to give expression to the mental process.
9 A proclivity to dreaming has often been remarked among the consequences of partial starvation.
Such, then, are the principal characteristics of somnambulism, a state in which dreams are supplemented by more or less complete and appropriate action, ordinarily without subsequent recollection of either dream or action.
The somnambulistic dream generally occurs during or soon after the period of deepest sleep, when the influences of the external world are largely suppressed. Released from the control of its sensory portion, the remainder of the brain awakes and becomes aroused to a condition of functional exaltation. No longer distracted by the recollection of the special senses, the attention is concentrated upon the hallucinations which constitute the dream. In the simpler forms of noctambulism only the automatic locomotive apparatus is awakened, and the sleeper moves in accordance with the impressions derived from habit aided by exaltation of the muscular sense. But in some of the more complicated cases a certain amount of special sensibility seems to exist. The patient is capable of exercising just that amount of sensation which is necessary to accomplish his purpose, though blind and deaf and insensible to every other impression. The more complete the waking of the organs of sense, the closer the resemblance to the condition of ecstasy in which cerebral exaltation is the prominent feature. Accordingly, it sometimes happens that the somnambulist can recall the events of his paroxysm.10 In such cases the power of recollection is due to the same conditions that control the recollection of our ordinary dreams. We remember very imperfectly, if at all, the dreams that occur during sound sleep, but the visions with which sleep sometimes commences (hypnagogic hallucinations) and those that occupy the period of morning slumber are very easily reviewed in memory, because they are associated with impressions directly derived from the partially-waking organs of sense. Such dreams are therefore chiefly recalled through their association with the train of our waking thoughts. But the dreams of somnambulism and the dreams of night-terrors, and all other visions during profound sleep, are as completely as possible cut off from all connection with the mental activities which arise directly from the action of the senses. By reason of such isolation the ordinary association of ideas affords no help to the memory, and the dream remains in the limbo of oblivion.
10 A. Bertrand, Traité du Somnambulisme, p. 80.
Alfred Maury expresses the opinion11 that the principal cause of forgetfulness of the events of somnambulism consists in the exhaustion of the cerebral elements through the intensity of the excitement to which they are subjected during the paroxysm. Doubtless this in certain cases may contribute to the loss of memory, but it should be remembered that the excitement may be relative rather than absolute. Certain elements wake while others are asleep, and the waking cells may be aroused to a degree far in excess of what is usual during the sleep of the brain without attaining to the level of their diurnal activity. The mind, undisturbed by external impressions, gives its attention to the activity of these waking organs, and a dream with all its consequences, somnambulic or otherwise, is the result. In other words, the plane of consciousness, so to speak, is lowered [p. 373] during sleep to the level of these molecular vibrations. But when the whole brain is again awakened after sleep the residual vibrations of those elements which yielded the physical basis of the dream, and which, had they occurred during the waking state, might have persisted with energy sufficient to furnish a groundwork for recollection of the ideas which they had originally suggested, are no longer sufficiently energetic to be felt in consciousness. Recollection of mental states thus generated must necessarily be impossible so long as the mind is dependent upon the brain as its register of events. Sometimes, however, the somnambulist, who while awake had forgotten all the incidents of his somnambulic experience, can remember in a subsequent paroxysm all that occurred during the preceding attack. Facts of this kind have been observed in the waking life of certain hysterical persons,12 but the apparent interruptions of their personality attach to the waking state, while in ordinary somnambulism it is only in sleep that the alternations of memory and forgetfulness occur. A similar recollection of previous visions is sometimes experienced in dreams, showing the close relation that subsists between the dreams of sleep and of somnambulism. The bond of association between these events thus isolated in time must be sought in a renewal of like conditions of the brain during the successive periods of somnambulic exaltation. We must suppose that the molecules which were in a state of functional excitement during the first paroxysm are again aroused in like manner after a period of waking quiescence. If, during sleep, their movements, though of an exalted character, have only just sufficed to arouse consciousness in the form of a dream, it would not be probable that during the phase of comparative inactivity which supervenes when the whole brain is awake their residual motion could disturb the sphere of consciousness. Hence the time occupied by their somnambulic vigor must remain a blank in memory during the waking state. But when the original state of exaltation has been reproduced by a second period of disorder, if the same molecular movements be in any way renewed, the conditions of memory are fulfilled; consciousness is once more aroused as before, and the patient remembers the dream or the events of the previous attack.
11 Le Sommeil et les Rêves, p. 226.
12 Annales Medico-psychologiques, 5e Série, t. xvi. p. 5, 1876.
The phenomena which have now been passed in review are of apparently spontaneous origin during the ordinary period of sleep. But from the remotest antiquity it has been known that certain persons may be thrown into an artificial sleep which closely resembles the condition of the somnambulist. During the persistence of this state certain portions of the nervous system become utterly insensible to external impressions, while other portions acquire an exalted degree of sensibility. The subject of the experiment can then by special methods be placed in such relations with other waking individuals that his surviving sensations, mental processes, and physical actions shall be no longer regulated by his own volition, but by the will of another. Such susceptibility is not common to all persons. About 20 per cent. of the ordinary population is, by some observers, considered capable of experiencing this condition. [p. 374] Heidenhain,13 experimenting upon a class of medical students, found only one in twelve who was thus susceptible. Charcot, whose field of observation covers the inmates of the Salpêtrière Hospital, finds the best exemplars of the hypnotic state among the hystero-epileptic females in that asylum. To these experimenters we are largely indebted for the most extended scientific observation of the phenomena of hypnotism, giving precision and publicity to the knowledge of facts which, though equally well known within a narrow circle of investigation14 during the earlier decades of the present century, have been compelled to await the development of cerebral physiology before their full significance could become apparent to the mass of the medical profession.
13 Animal Magnetism: Physiological Observations, by Rudolph Heidenhain.
14 Braid, Neuro-hypnology considered in Relation with Animal Magnetism, London, 1843.
The antecedent condition most favorable to the production of the hypnotic state is a highly unstable constitution of the nervous system. For this reason the larger number of qualified subjects is furnished by the female sex, especially by those who possess the hysterical temperament. Frequent repetition of hypnotic exercises renders the subject still more susceptible. Heidenhain was at first inclined to believe that such experiences were not prejudicial to the health of the subject, but the observation of Harting in the University of Utrecht, and of Milne-Edwards in Paris,15 have demonstrated danger to the health of animals subjected to similar experiments. It is easy to discover, in the various clinical narratives published by Charcot and his pupils,16 evidence that hysterical patients often manifest considerable exhaustion after hypnotic exhibitions; consequently, it cannot be admitted that the practice is devoid of risk to the health of the individual.
15 Lancet, July 29, 1882, p. 164.
16 Paul Richer, L'hystéro-Epilepsie, Paris, 1881; Le Progrès médical, 1881-82.
Numerous methods of inducing the hypnotic state have been employed by different experimenters. The greater number consist in modifications of the sensory impulses derived from the periphery of the body. Gentle pressure upon the closed eyelids; convergence of the axes of the eyeballs upon some object nearer than the proper focal distance of the eyes; fatigue of the retina by gazing upon any brilliant or luminous object; monotonous excitation or sudden surprise of the auditory nerve; various impressions through gentle friction or pressure upon different regions of the body,—all these are capable of inducing hypnotic sleep. An appeal to the imagination, or even the mere attempt to abnegate the possibility of vigorous thought by confining the attention to the most trivial of things, sometimes suffices to produce the desired phenomenon. Thus, Heidenhain put one of his students to sleep at a distance by merely informing him beforehand that at a certain hour he would hypnotize him in his absence. The state of ecstatic meditation into which the monks of Mount Athos plunged themselves by the practice of omphaloscopy affords an illustration of the hypnotic effects of concentrated attention.
The duration of hypnotic sleep is exceedingly variable, but if left to himself the patient usually wakes spontaneously, without recollection of anything that has happened. If it be desirable to awaken him before the natural termination of the paroxysm, consciousness can be restored by almost any sudden and energetic appeal to the senses, such as an [p. 375] electric shock, a sudden illumination of the eye with vivid light, or a sharp puff of air upon the face.
According to Charcot,17 three principal types may be remarked among the hysterical subjects upon whom he experimented: (1) the cataleptic, (2) the lethargic, and (3) the somnambulic. Of these, the first may be developed primarily by any abrupt and powerful impression upon an organ of sense, as a bright light or a loud noise (gong). Fixing the eyes upon some object may produce the same result. Dumontpallier, for example, has reported the case of a young woman18 who accidentally hypnotized herself by gazing at her own image in the mirror before which she was dressing her hair. The cataleptic state may also be secondarily induced by merely opening the eyes of a patient in whom a condition of hypnotic lethargy has been previously developed. If only one eye is thus opened, the corresponding side of the body alone becomes cataleptic. Closing the eyes causes the disappearance of this symptom, with complete restoration of the purely lethargic state. During the cataleptic condition the several tendinous reflexes disappear, neuro-muscular hyperexcitability ceases; the skin becomes insensible, but the special senses, particularly those of sight and hearing, maintain a partial activity. In this state the senses may become avenues of suggestion for the production of muscular movements, but if left to themselves the limbs remain motionless.
17 Le Progrès médical, Feb. 18, 1882, p. 124.
18 Ibid., March 25, 1882, p. 223.
The lethargic state may be induced by simply closing the eyes of the patient or by causing him to fix his gaze upon some definite object. The paroxysm begins with a deep inspiration causing a peculiar laryngeal sound, followed by the appearance of a little foam on the lips. The eyelids are either wholly or partially closed, and are in a state of continual tremulous motion. The eyeballs are generally turned upward and inward. The muscles are completely relaxed. The tendinous reflexes are exaggerated; pressure over a muscle or upon a nerve arouses a peculiar contraction of synergic muscles and of groups of muscles which are supplied by the excited nerve-trunk. The facial muscles, however, do not thus become contractured: they merely contract during the application of the stimulus. If the lethargic patient be rendered cataleptic by opening the eyes, these contractions persist even after awaking, and they can only be dispelled by renewing the lethargic state before resorting to pressure upon the antagonistic muscles—a process by which the contractures peculiar to this species of lethargy may always be annulled. By the approach of a magnet to a contractured limb the phenomenon may be completely transferred to the corresponding muscles upon the opposite side of the body. If upon a limb of a lethargic patient who has been rendered cataleptic by opening the eyes an Esmarch's band be applied, pressure over the bloodless muscles excites no contracture until the band is removed. A contracture is then developed, and it may even be transferred to the opposite limb by the approach of a magnet. To this phenomenon has been applied the term latent contracture.
The extraordinary muscular excitability manifested by these hysterical hypnotics is further illustrated by an observation recorded by Dumontpallier.19 If one end of a caoutchouc tube one centimeter in diameter and [p. 376] five or six meters in length be applied over a muscle in the leg, and if the other end be in like manner connected with a watch, every movement of the second hand will be followed by a slight contraction in the muscle. The same result follows connection with the wire of a telephone, and if a microphone be introduced into the circuit the incidence of a ray of artificial light upon the instrument, or even its glancing reflection from the eye, will arouse a responsive muscular contraction. Charcot has sometimes observed muscular contractions upon the opposite side of the body when a mild galvanic current was applied to the parietal surface of the head. During the manifestation of muscular hyperexcitability there is complete analgesia, but the senses of sight and hearing seem to preserve some degree of activity. The patient, however, does not manifest any susceptibility to influence by suggestion.
19 Ibid., Jan. 14, 1882, p. 25.
The somnambulic state may be directly induced by fixed attention with the eyes, by feeble and monotonous excitation of the senses, and by various other methods of an analogous character. This forms the most common variety of the hypnotic condition. It may very easily supervene during either the lethargic or the cataleptic state as a consequence of pressure or gentle friction upon the top of the head. Thus, Heidenhain caused muscular paralysis by rubbing the scalp. Unilateral friction of the same surface produced paralysis of the opposite side of the body without notable affection of consciousness. The eye and the eyelids behave as in the lethargic state. The patient seems asleep, but there is less muscular relaxation than in hypnotic lethargy. There is no exaggeration of the tendinous reflexes, and muscular hyperexcitability is absent. But by lightly touching or breathing upon the surface of a limb its muscles may be thrown into a condition of rigidity which differs from the contracture of the lethargic state in the fact that it does not yield to excitation of the antagonistic muscles, though yielding readily to a sudden repetition of the same form of excitement by which it was originally produced. From the immobility of the cataleptic state it also differs by a greater degree of resistance to passive motion. Though analgesia may be perfectly developed in this state, there is generally an exalted condition of certain forms of cutaneous sensibility and of the muscular sense. Strange perversions of other special senses are sometimes remarked. Cohn20 discovered that a patient who was naturally color-blind “when unilaterally hypnotized was able to distinguish colors which were otherwise undistinguishable.” Conversely, when the cataleptic state is induced the eye becomes incapable of discerning colors. Spasm of accommodation is also present, and is one of the earliest demonstrable symptoms of the hypnotic condition.
20 Brain, vol. iii. p. 394.
These remarkable exaggerations and perversions of special sensibility have been the cause of much scepticism on the one hand regarding the verity of the phenomena of hypnotism, and of much credulity on the other, extending even to a belief in the existence of supernatural and miraculous gifts. But when the fact is once comprehended that in this capacity for uncommon feats of vision, hearing, touch, etc. we observe merely the exaggeration of a process which occurs in every act of attention, the miraculous semblance of the phenomena disappears. Attention implies an increase of activity in certain portions of the brain, with [p. 377] diminution of the function in the remainder of the organ. In the wild excitement of a cavalry charge the soldier feels not the sabre cut which will fill his consciousness with pain so soon as his attention is released from the fetters imposed by the more engrossing events of the combat. So in the somnambulic sleep those parts of the brain which remain awake perform their functions with a vigor that is enhanced by a concentration of cerebral energy in certain restricted portions of an organ that, by reason of its naturally excessive instability, had been previously fitted for the liberation of an inordinate amount of molecular motion. Hence the slightest suggestion of sense may suffice for the most extraordinary perception. Such persons see through their eyelids and hear at a surprising distance. The memory of past events, the recollection of long-forgotten words and thoughts, supplies in this state an abundance of materials out of which an exalted imagination may construct the most astonishing scenes. By this method of combination are produced those remarkable oratorical utterances which by the ignorant have been so widely attributed to the supervision of guiding spirits from another world. In this condition the essential characteristics of the mind of the so-called medium become the real guides of his mental processes. Hence the infinite variety and contrariety of the utterances of such declaimers.
Among other consequences of this exalted susceptibility of the waking portions of the brain may be noticed the effect of suggestions by others upon the mind of the somnambulist. Numerous examples scattered through the literature of the subject21 illustrate the manner in which the course of our ordinary dreams may be thus directed. The hypnotic dream is far more easily modified.22 The simplest manifestations of such influence are exhibited in movements in obedience to the command of the hypnotizer. Next in rank are those more complicated actions that are effected by excitement of the imitative faculties of the subject. Every suggested movement that can be in any way perceived by the patient will be at once reproduced. Various emotions and passions may thus be aroused by simply placing the sleeper in the appropriately suggestive attitudes. Under the influence of a pregnant idea intruded upon the mind of the patient the subsequent association of ideas will suffice for the evolution of a complicated series of hallucinations, as in the case of a young woman, who on being directed to put out her tongue immediately began to feel sensations of uneasiness in her stomach, followed by nausea and attempts at vomiting, accompanied by the impression of being on shipboard. In the lowest grades of the hypnotic state consciousness may remain, and the subsequent recollection of the events of the paroxysm may be quite persistent. In such cases illusions that were produced by suggestions from other minds generally survive in memory and become the causes of serious delusion. Witness the manner in which susceptible individuals, partially hypnotized in a so-called spiritual circle, believe in the reality of the illusions which have occupied their senses during a séance.
21 Carpenter's Physiology, 8th ed., p. 765; Le Sommeil et les Rêves, par L.-F. Alfred Maury, 4th ed., p. 153 et seq.
22 Loc. cit., p. 357.
A higher degree of insensibility to ordinary impressions is necessary to the production of the phenomena of passive obedience and of automatic [p. 378] imitation. It is probable that the degree of sensory hyperæsthesia which enables certain hypnotic patients to read the thoughts of others belongs rather to the first than to the last of these classes. This capacity is usually associated with preservation of consciousness and memory, and is, essentially, a mere exaggeration of that power which all possess in greater or less degree. Numerous well-authenticated examples of a surprising manifestation of this faculty have been recorded, so that the possibility of its existence no longer admits of doubt.23 In all cases it has been remarked that the hypnotic mediums can only respond correctly to questions for which the true answer is present in the mind of the questioner. For all other interrogations the replies are delivered purely under the influence of random suggestion. In certain of these cases the pathway of communication lies through actual physical contact, as in ordinary mind-reading, where the insensible molecular oscillations of the muscular elements of one individual serve to guide the movements of another. But more frequently the transmission of ideas is effected through the eyes. With these organs the table-rapper or the planchette-writer reads the unspoken words of the questioner in a manner very like, yet vastly more deliberate than, that by which deaf-mutes now learn to interpret the movements of the lips of persons with whom they converse. This fact is well illustrated by the experience of Maury24 in an interview with a celebrated table-rapper, who without the slightest hesitation made known to him the age, name, and date of death of a brother whom he had lost. She also gave the same information regarding his father, and related the names of other persons upon whom he had fixed his attention. But if he turned away his face or concealed his eyes, so that the woman could no longer watch their expression, her responses ceased to be of any value.
23 Luther V. Bell, Two Dissertations on what are termed the Spiritual Phenomena, read at the meetings of the Association of Medical Superintendents of American Insane Hospitals at Washington and Boston in 1854 and 1855.
24 Le Sommeil et les Rêves, 4th ed., p. 361.
In these partial developments of the hypnotic state it is worthy of note that the phenomena of sleep are so few and so comparatively insignificant that they are usually overlooked. Hence the veil of mystery which has so often obscured the interpretation of such cases. Careful observation, however, will always detect some characteristic departure from the normal standard—some loss of balance between the different parts of the nervous system—by means of which the true relations of each example may be determined.
TREATMENT.—A large proportion of the phenomena of somnambulism and hypnotism depend rather upon an originally irritable organization than upon a specially diseased condition of the nervous system. Their treatment, therefore, frequently resolves itself into the management of hysteria or of cerebrasthenia. But if the manifestations of somnambulism develop for the first time in a person advanced in years, who has previously enjoyed good health and a sound mind, it should be regarded as an omen of grave import, signifying the imminence of organic cerebral disease. Though the meaning of such incidents is less sinister in early life, they reveal an ill-balanced state of the nervous system and an imperfect process of nutrition in the growing body. Such children are the [p. 379] frequent victims of night-terrors, the form of disorder most commonly evolved by their somnambulistic proclivities. The treatment of night-terrors should therefore be chiefly directed to the invigoration of the general health of the patient. Indigestion and malnutrition are among the most prominent antecedents, and they should constitute the principal objects of therapeutical attention. Constipation is usually present. This may be relieved by the use of compound rhubarb powder or any other gently stimulating laxative. Digestion should be aided with pepsin as soon as the catarrhal condition of the alimentary canal, so uniformly present, has been measurably improved. Cod-liver oil or its substitutes should be administered for a long period of time. If the nocturnal paroxysms be frequently renewed, it may be well to employ the bromides, either with or without chloral hydrate; but as a general rule it is better to rely upon hygienic and restorative treatment, rather than upon any form of merely hypnotic medication.
The departures from the course of natural sleep which have been thus considered are not so much the direct consequence of acute disease as the result of structural deviation from the normal type of the nervous system. We must now briefly review the strictly pathological modifications to which sleep is liable.
Among those who indulge freely in the pleasures of the table a form of insomnia is not uncommon. Originating at first in mere overloading of the stomach, and consisting in a direct irritation of the brain through the medium of the intervening nervous apparatus, sleeplessness finally becomes a symptom of more serious mischief. The tissues become charged with nitrogenous waste, and a lithæmic25 or gouty condition is established. Such patients are wakeful, or if they sleep their slumbers are imperfect and unrefreshing.26 Grinding of the teeth,27 noticed by Graves during the sleep of the gouty, is a symptom indicative of a highly irritable condition of important ganglia at the base of the brain. These symptoms are sometimes associated with turgidity of the superficial vessels of the head, indicating imperfect function of the circulatory organs, with a tendency to accumulation of the blood in the venous channels of the body. The sleep of such partially-asphyxiated patients is fitful, irregular, and akin to stupor. Occurring in the subjects of periodical gout, these disturbances of sleep become increasingly serious as the paroxysm is approached, until loss of sleep and the unrefreshing character of such [p. 380] slumber as may be obtained become important factors among the causes of failing health.
25 DaCosta, “Nervous Symptoms of Lithæmia,” Am. Journ. Med. Sci., Oct., 1881.
26 Dyce Duckworth, “Insomnia in Persons of Gouty Disposition,” Brain, July, 1881.
27 Trousseau, Clinical Medicine, Am. ed., vol. iv. p. 362.
For all such patients a proper recognition of the cause of their disorder is essential. This must be corrected by measures appropriate to the treatment of the gouty diathesis. Since the condition of the cerebral tissues is a state of irritation caused by the presence of excrementitious substances, such hypnotic remedies must be selected as will not interfere with the defecation of those tissues. Bromide of potassium, valerian, scutellaria, hyoscyamus, hops, and cannabis indica are useful, together with all that class of drugs which quiet the brain without hindering the process of excretion. Chloral hydrate often produces an excellent result, but care should be taken to prevent its habitual use.
Closely related with the sleeplessness of lithæmia are the disturbances of repose which attend the evolution of the various specific fevers. In many cases the condition varies all the way from stupor to delirium. Excessive somnolence, such as often ushers in the fever, is an indication for evacuant treatment. Cerebral excitement calls for remedies like the bromides and chloral hydrate, which do not interfere with elimination. If pain, like headache or backache, be a symptom demanding attention, the addition of morphia in small doses forms a valuable reinforcement for the hypnotic mixture; but, as a general rule, opiates should be used with a sparing hand. The various resources of hydrotherapy are often invaluable when wakefulness results from the cutaneous irritability of the eruptive fevers. During the later stages of a protracted illness the occurrence of insomnia should direct attention to the nutrition of the patient. Wakefulness is then the symptom of an irritable weakness of the brain, demanding remedies which delay the process of disassimilation. The failing power of the heart requires attention, and diffusible nutriment must be given to convey the elements needful for restoration of the exhausted brain. These indications are most perfectly answered by the associated administration of opiates with alcohol, milk, and beef-juice in small and frequent doses.
Cerebral exhaustion is a not uncommon cause of wakefulness in cases uncomplicated with fever. It is usually the result of chronic conditions of ill-health and depression, such as are often encountered as the result of various cachexias or of dyspepsia, with or without the abuse of alcohol, tea, coffee, or tobacco. Overwork, debilitating discharges, pregnancy, parturition, mental anxiety, depressing emotions, chronic heart disease, and incipient insanity are fruitful causes of the exhaustion which produces this most distressing form of insomnia. In such cases the cessation of healthy nutrition leads to a condition of excessive instability in the cerebral tissues. The oxygen which they receive from the blood is not stored with any degree of permanence, but tends to pass directly into [p. 381]stable combinations with the oxidizable elements of the brain. Consciousness is thus continually aroused. The state of such a patient presents a very close analogy to the condition of the victim of diabetes whose liver refuses to retain its glycogen. The inordinate discharge of sugar into the blood not only exhausts the tissues of the liver, but also excites other organs—notably the kidneys—to excessive and unwholesome activity. In somewhat similar fashion, the failure of the brain to assimilate and to retain oxygen leads to an abnormal intramolecular oxidation, which excites an excessive and unwholesome activity on the part of the Ego in another region—namely, in the field of consciousness. Such wakefulness might justly be termed a psychical diabetes.
This variety of insomnia has frequently been ascribed to cerebral anæmia occurring as a part of a general spanæmia. But this universal impoverishment of the blood, though a sufficient cause of the morbid instability, the irritable weakness, of the cortical tissues, does not necessarily imply a comparatively bloodless condition of the brain. Unequal circulation and local hyperæmia in different organs of the body are no unusual consequences of the anæmic state. Slight disturbances suffice to arouse the brain of such a patient. The vaso-motor apparatus shares in the general irritability, permitting blood to inundate the cortical substance almost without provocation. The unstable protoplasm is only imperfectly renovated, usually at the expense of the other tissues of the body. The weary patient, busying himself with an unwilling review of the events of the day, tosses long upon his couch before he can secure the approach of “tired Nature's sweet restorer, balmy sleep.” When at length he yields, his slumbers are brief, and the latter part of the night is but a repetition of the earlier vigil.
Such patients need a very radical course of general treatment. A complete change of habits should be effected. A long vacation in the country, or, best of all, a protracted voyage in a sailing vessel, is desirable. Hot foot-baths, with cold affusion upon the head, and warm sponge-baths, or even the full bath in tepid water, at bedtime, are of great service as means of tranquillizing the nervous system. The indications for medicinal treatment, besides attention to the predisposing cachexia, are twofold—to calm and to nourish the enfeebled nervous substance. Opiates calm, but do not nourish—they hinder the process of nutrition; hence the sufferer wakes unrefreshed by the sleep which they procure, and is soon in a condition worse than ever. The same objection lies against the continuous use of the bromides. But alcohol and its hypnotic derivatives (chloral, paraldehyde, etc.) not only calm the excitable brain, but they also furnish to the tissues a certain amount of diffusible nutriment which suffices to steady the brain until a change of occupation, with rest and wholesome food, can produce a complete restoration of its normal stability. To this effect of alcohol must be ascribed its value as an hypnotic in the wakefulness of old people who cannot sleep without a preliminary nightcap. A moderate draught of hot toddy in such cases serves to arouse the feeble heart and to equalize the circulation by the production of a moderate degree of general vascular dilatation. The sugar and water afford an easily assimilated food, while the alcohol benumbs the cortical protoplasm to a degree which favors the cessation of conscious perception. If administered in excessive doses, it is not sleep but anæsthetic intoxication [p. 382] which follows. If this condition be unduly repeated, the phenomena of chronic alcoholism supervene, with all the horrible forms of insomnia that accompany cerebral starvation and delirium tremens. Non-alcoholic nerve-stimulants and tonics, with careful administration of easily-digested food, are then more than ever needed to overcome the neurasthenic wakefulness.
Still another form of sleeplessness is often experienced as a result of actual inflammation in some portion of the body, either involving the intracranial contents directly or reacting upon the brain through the medium of its circulation. In such cases many of the symptoms of acute inflammation are present. The head aches, the temples throb, the face and eyes are suffused with blood, the temperature is considerably increased. The senses become exalted, ideas pursue a tumultuous course, there may be actual delirium. These disturbances are due to an active hyperæmia of the brain. The substance of the cortex becomes hyperexcitable, and the ordinary incitements of sense produce an exaggerated effect in consciousness. The patient does not sleep, and he feels no need of sleep, because the nutrition of the brain is sustained at the expense of the remainder of the wasting body. The most speedy and effectual relief in such cases is obtained through a diminution of the current of blood in the brain. Moderate compression of the carotid arteries has been proposed as theoretically useful. Sedatives, like aconite, conium, digitalis, veratrum viride, ipecacuanha, and tartar emetic are useful, either alone if pain be absent or combined with opiates if the patient is suffering. Dover's powder or tartar emetic and morphia in small doses was formerly in general use. If there be a disposition to nausea the substitution of aconite for antimony is of great value. A combination of morphia, bromide of potassium, and chloral hydrate often gives excellent results. Paraldehyde may be preferable to chloral by reason of its more thoroughly sedative effect. Derivative measures—mercurial cathartics, cupping, leeching, or even general bleeding—may become necessary in certain cases. After the acute stage is passed blisters behind the ears should be employed. In the sleeplessness of acute mania Newington28 has used mustard baths with great satisfaction.
28 Brain, vol. i. p. 126.
Turning now to the other extreme, we find a class of cases in which the disorder consists not in wakefulness, but in an excess of sleep. Excluding those exceptional cases in which healthy individuals, as a consequence of inordinate physical exertion, have slept for many hours beyond their ordinary limit, every extraordinary manifestation of sleep-like unconsciousness must partake of the nature of coma. Between natural sleep and this condition may be placed the distinction that the one is always the effect of natural physiological processes, while the other is always the result of injury, of disease, or of some form of intoxication. Comatose [p. 383] unconsciousness may be the result of cerebral compression caused by traumatic impact or by the presence of inflammatory exudations. Intracranial tumors, embolisms, thrombi, degeneration of tissue, diseases of the arteries of the brain—in short, every morbid change of which the liquids and the solids within the cranium are capable—may become the causes of coma. So also the blood and lymph, contaminated with the products of internal disintegration, may benumb the brain with comatose sleep. Again, the tissues of the brain may be overwhelmed with poisons introduced from without the body, and thus a condition of coma may result. Few diseases, therefore, exist without the possibility of coma as one of their consequences—a coma which, however, must not be confounded with the genuine sleep which sometimes occupies the larger part of certain stages of convalescence from acute illness. During such convalescence there is a reversion to the infantile type of nutrition, with all its need of prolonged and frequent periods of repose. Like normal sleep, the comatose condition admits of considerable variation of intensity. The patient may sometimes be partially roused, as from the coma of alcoholic intoxication, and he may finally recover complete consciousness, but very often the reverse is the fact. The coma deepens into paralysis, and death terminates the scene without the slightest manifestation of sensibility or intelligence.
A singular disorder, characterized by daily paroxysms of somnolence, tending to become more and more continuous and profound until merged in fatal coma, is encountered among the negro inhabitants of the Atlantic coast of tropical Africa. Similar cases have been occasionally reported in other regions of the world, but it is among the Africans that they have been principally observed. For our knowledge of this disease we are chiefly indebted to the writings of Clark,29 an English surgeon residing at Sierra Leone, and of Guérin,30 a surgeon in the French navy, who enjoyed unusual opportunities for its study among the laborers recently brought from Africa to the island of Martinique. According to these observers, the onset of the malady is gradual, commencing with a slight frontal headache. Very soon a disposition to sleep after meals is remarked. This becomes increasingly urgent, and the paroxysms of sleep are prolonged, until at length the patient becomes continually soperose. The wakeful intervals are marked by a sluggish state of the intellectual faculties. The pulse is not accelerated, but remains full and soft. The veins of the sclerotic become turgid and the eyeball seems unusually prominent. The temperature does not increase, but rather tends to diminish its figure. The skin becomes dry and moderately cool. The tongue continues moist, and is covered with a white fur. The contents of the bowels and of the bladder are regularly voided, and the appetite persists with considerable vigor. Finally, the patient becomes completely comatose and dies quietly. Sometimes, however, the evolution of the disease is less tranquil. Epileptiform convulsions, followed by [p. 384] progressively deepening paroxysms of coma, interrupt its course, until a continuous muscular tremor marks the closing period. At the same time the pulse grows weaker and more frequent, until its movements cease in death. Recovery is almost unknown, though the duration of the disease often varies from three months to a year or longer. Examination of the body after death has thus far yielded very negative results: the sinuses and larger vessels of the brain are engorged with blood, but no evidence of inflammation is anywhere apparent. The other organs present no pathological alterations whatever. These observations seem to indicate that the disease originates in some form of general blood-poisoning rather than in any local inflammation or degeneration, and Clark has called attention to an enlargement of the cervical glands as a feature of the malady. According to G. H. Bachelder,31 the native physicians cure the disease by extirpation of the affected glands. He has also observed an initial lesion in the nasal mucous membrane. If this be confirmed, the malady will take its place among the forms of coma produced by septic poisoning.
29 Transactions of the London Epidemiological Society, vol. i. p. 116.
30 De la Maladies du Sommeil, 1869.
31 The Medical Record, July 1, 1882, p. 23.
A pathological variety of sleep, in which the repose of the body is even more complete than in coma. The victim of coma often presents a countenance suffused with blood; the pulse beats vigorously, and respiration may become stertorous. But in lethargy the abolition of bodily movements is almost total. In the milder forms of this disorder the patient may be partially roused, so as to attempt an answer when addressed, appearing like a person in very profound sleep; but in the majority of cases he remains insensible, unconscious, and utterly irresponsive to ordinary forms of irritation. Respiration and circulation are reduced to a minimum, even becoming for a time imperceptible. Uncomplicated with hysteria, the disorder is rapidly fatal, but according to Rosenthal32 hysterical lethargy is never mortal.
32 Real Encyc. der ges. Heilkunde, vol. viii. p. 276.
Many examples of this disorder have been furnished by the records of apparent death.33 I am well acquainted with a lady who in early childhood was laid out for burial at the supposed termination of some infantile disease. Her mother alone insisted that the child was still alive. After some time spent in weeping and expostulation, she applied a blister to the thorax of the babe, who at length began to exhibit signs of consequent irritation, followed by a complete recovery. Still more instructive is the case related by Rosenthal34 of a young woman twenty-four years of age who in consequence of violent emotional excitement became unconscious and presented no sign of life, though tested with a mirror before the mouth and by dropping melted sealing-wax upon the skin. On raising her eyelids the pupils gave no response to light; the limbs remained perfectly placid and the radial arteries were motionless. Careful auscultation, however, detected a very feeble and intermittent sound in the cardiac region. The thorax exhibited no movement, but the lateral surfaces of [p. 385] the abdomen presented a slow and almost imperceptible oscillation. Gentle faradization of the muscles and nerves of the face and hand aroused definite muscular contractions. By these observations Rosenthal became satisfied that, although the patient had remained for thirty-two hours in this condition, she was only apparently dead. In fact, after continuing forty-four hours in a state of suspended animation she awoke spontaneously, made a rapid recovery, and enjoyed as tolerable health as an excitable nervous temperament would permit.
33 See article “Mort apparente,” Dic. Encyc. Sci. méd., 2d Series, vol. ix. p. 598.
34 Loc. cit., p. 272.
Certain authors make a distinction between lethargy and apparent death. But, leaving out of view the cases of so-called lucid lethargy, a variety of the trance state, the difference is rather one of degree than of kind. The movements of respiration and of circulation, though greatly diminished, are readily observed in ordinary forms of lethargy, while in apparent death the pulse can no longer be discovered, and only the faintest sound can be distinguished in the region of the heart. It therefore becomes imperative to have within reach a crucial test of the persistence of general vitality. Such a test, according to Rosenthal, exists in the faradic current. Within two or three hours after genuine death the muscles cease to be excitable by the induced current, but in a case of apparent death this form of electro-muscular contractility never disappears. Every other test that has been proposed has failed under certain circumstances. This alone gives uniformly positive indications.
In certain cases of apparent death the patient presents the external phenomena of suspended animation, but the power of conscious perception does not cease. The senses of sight and hearing remain, and are perhaps intensified by inhibition of the power of projecting cerebral volitions into space. The sufferer hears and sees; perception, memory, reasoning, judgment, emotion, volition, all persist. The possibility of centrifugal projection from the sphere of consciousness into the realm of space seems to be the only thing that is wanting.
The victims of this form of apparent death are usually women, or men who are characterized by a feminine nervous organization. Great mental excitement, fatigue, semi-starvation, and exhausting diseases are the principal proximate causes of the event. The following case, which was observed by my friend P. S. Hayes of Chicago, illustrates all these facts: A female physician, about thirty years of age and consumptively inclined, after a long and wearisome hospital service was attacked with typhoid fever. After a period of great prostration the hour of death seemed to have arrived. In the presence of her physician and surrounded by her relatives she ceased to breathe and the pulse stopped. Bottles of hot water were applied to the limbs, and other methods of restoration were employed, but a number of hours elapsed before these efforts yielded any result. At last she began to breathe once more; life was resumed and [p. 386] a gradual recovery followed. During all this time of apparent death consciousness had been preserved. She seemed to be looking down from above her bed, by the side of which she could see the physician holding her wrist, and she felt grief at witnessing the sorrow of her friends. Ordinary sensation was suspended, for she did not feel the scalding heat of the bottles that were applied to her limbs. Borne upon the wings of a liberated imagination, she thought she beheld the celestial city, but might not enter within its gates. In this exaltation the reasoning faculties also shared, so that certain philosophical problems which had long baffled her intellect were now perfectly comprehensible, and the memory of their interpretation persisted after recovery.
Many similar narratives have been duly authenticated, but the limits of the present article will not permit a discussion which properly belongs to an investigation of the phenomena of trance. The important fact for present consideration is the persistence of conscious life despite the appearance of death. In this preservation of consciousness, notwithstanding temporary suspension of certain forms of sensibility, together with loss of the power of voluntary motion, may be discovered a relationship between the events of lucid lethargy and various somnambulic modifications of sleep which have been previously passed in review.
There are two distinct diseases—or, more correctly, conditions—of the human body which are produced by exposure to heat, and which have a certain similarity in their symptoms, but are very different in their immediate pathology and require directly opposite methods of treatment. Although their individuality was pointed out as long ago as 1851 by the late D. F. Condie of this city,1 yet they have been frequently confounded by writers upon the subject, and the terms heat-exhaustion and sunstroke have not rarely been used as strictly synonymous. In the present article it is proposed to consider them as separate affections under the respective names of heat-exhaustion and thermic fever.
1 Amer. Journ. Med. Sci., Jan., 1852.
Any one who has been long exposed to a high temperature under circumstances requiring physical exertion must have noticed the feeling of general weakness and relaxation which results. Thus far reaches our every-day experience, but cases in which acute symptoms are severe enough to cause alarm occur, although somewhat infrequently. The attack may come on slowly, but may be as abrupt as that of true sunstroke, and the severest cases may happen in those who have been in robust health as well as in the weak and feeble. The mind is usually clear, the pulse rapid and feeble, the surface cool, the voice very weak, muscular strength greatly lessened, and the feeling of exhaustion extreme. If this condition be intensified, syncope may be developed with its usual symptoms. In all this there is nothing peculiar and little that is necessary to notice here; but there is a form of heat-exhaustion in which the heart does not seem to suffer principally, but in which there is collapse with palsy of the vaso-motor system, great fall of the bodily temperature, and marked general nervous symptoms. At the International Exhibition of 1876 a very powerful man, whilst working in an intensely hot, confined space, fell down without giving warning, and was brought into the hospital. He was in a state of restless, delirious unconsciousness, incessantly muttering to himself, and when shaken and shouted at responding only by a momentary grunt. The pulse was rapid, fluttering and feeble. The [p. 388] surface was covered with a very heavy sweat and exceedingly cold. The muscular relaxation was extreme. The facies was that of collapse, and the temperature, as taken in the mouth, 95.25° F.
The PATHOLOGY of heat-exhaustion is best discussed in conjunction with that of thermic fever, and will therefore be for the present postponed.
The TREATMENT of heat-exhaustion is a very obvious one. The indications are to stimulate the circulation and warm the body by external heat with an energy proportionate to the severity of the attack. In mild cases the exhibition of a whiskey punch or similar beverage may suffice, but in severer attacks alcohol acts too slowly and is not capable of filling all the indications. It may re-excite the flagging heart, but it is probably not a vaso-motor stimulant, and if given too freely may even increase the vaso-motor depression. Digitalis is an excellent stimulant of the heart, and probably also of the vessels. It acts, however, comparatively slowly even when hypodermically injected, but in severe cases it should always be employed. The tincture is the most eligible preparation, and when injected under the skin in doses of fifteen drops causes no local irritation. Ammonia would be a very valuable remedy did not its use offer so many difficulties of administration: injected into the cellular tissue, it causes great pain and usually sloughing, and its intravenous use is by no means always easy. As a vaso-motor stimulant atropia is an excellent remedy, and, as it has also a very powerful influence in arresting the secretion from the skin and in raising the animal temperature, it should produce very good results in the peculiar form of collapse under consideration.
When the bodily temperature is below normal the most important measure of treatment is the use of the hot bath: the water should be from 100° to 120° F.—i.e. as hot as can be borne—and the whole body should be immersed in it until the mouth temperature becomes normal.
SYNONYMS.—Coup de soleil, Sunstroke, Heat apoplexy, Heat asphyxia, Heat fever, Sun fever, Thermohæmia, Erethismus tropicus, Insolation.
The immediate cause of thermic fever is always exposure to excessive heat in some form. As the body can cool itself much more readily in a dry than in a moist atmosphere, it is able to resist the influence of a dry, overheated air much better than when there is also moisture. It is for this reason that sunstroke is so much more infrequent upon the high table-lands of Abyssinia or in the dry belt of our Texan prairies than in the lowlands of India or upon our own seacoast. For the same reason it is especially prone to attack indoor workers in confined, moist factories, and especially in laundries and sugar-refineries. At one time it was thought that exposure to the direct rays of the sun was the chief cause of the disease, but there is now abundant clinical testimony to the fact that such exposure is in no sense necessary. Without occupying space in giving detailed references, it suffices, as an illustration of the fact that the most complete darkness is no protection, to allude to the epidemic upon the French man-of-war Duquesne, as recorded by M. Boudin, in which a [p. 389] hundred cases of sunstroke occurred in a short time, most of them at night when the men were lying in their bunks. Bonniman2 says: “By far the greater number of cases that yearly occur in India are of men who have not been exposed to the sun. It is not unusual for men to go to bed in apparent health, and to be seized during the night; and patients in hospitals who have been confined to bed for days previously are frequently the subjects of attack.”
2 Edinburgh Med. Journ., vol. xiv. p. 1029, 1864.
Although the immediate cause of the attack is excessive heat, there are certain conditions which act as predisposing causes by lessening the power of the system to resist the heat, or, in accordance with the theory of sunstroke which I believe established, by so weakening the inhibitory heat-centre that it is readily exhausted. The chief of these predisposing causes are race, excessive bodily fatigue, and intemperance. It is true that males are much more frequently affected than females; thus, in an epidemic occurring in St. Louis, Missouri, in 1878, there were 115 deaths in males and 39 in females. This is due, however, not to one sex being predisposed to the attacks, but to the habitually greater exposure of males than of females to heat. The much greater frequency of sunstroke in the laboring than in the upper classes has similar explanation.
Those races which are least accustomed to a tropical climate are most apt to be attacked; thus, both in this country and in India, Europeans suffer far more than do the natives. No race is, however, absolutely exempt. Even the negro and the Hindoo inhabitant of tropical India are occasionally prostrated.
The general experience in the United States shows that habitual excess of alcohol very strongly predisposes to attack, but some of those who have had widest experience in India are inclined to deny this. It has been especially noted in India that persistent bodily fatigue greatly weakens the resisting power of the European. As an instance of this may be cited the case of the Forty-third regiment of the line during the Sepoy rebellion, as recorded by its surgeon, Barclay. It had made a most extraordinary march of over eleven hundred miles, chiefly through the lowlands of India, and at the hottest season of the year. This march was continuous, with the exception of a few brief halts. No cases of sunstroke occurred until nine hundred and sixty-nine miles had been traversed and the men had become thoroughly exhausted and even markedly emaciated. Shortly after this the regiment rested some eight days, and then started again, arriving soon in a narrow ravine in the Bisramgunge Ghat, with precipitous walls nearly a mile in height. During the day the thermometer in the tents ranged from 115° to 127°, and on one occasion was noted 105° at midnight. The number of cases of insolation now became very great, and, although most of them recovered, 2 officers and 11 men were lost in the four days during which the regiment remained encamped. The air became cooler as the command emerged from the hills, yet 7 more fatal cases occurred in three days.
SYMPTOMS.—Under the name of ardent continued fever, or febris continuis communis, has been described in India an affection which may be considered as representing a mild form of thermic fever. In C. Morehead's clinical work On the Diseases of India the following account of the symptoms is given: “The attack is generally sudden, often without [p. 390] much chilliness. The face becomes flushed; there are giddiness and much headache, intolerance of light and sound. The heat of skin is great; the pulse frequent, full, and firm. There is pain of limbs and of loins. The respiration is anxious. There is a sense of oppression at the epigastrium, with nausea and frequent vomiting of bilious matters. The bowels are sometimes confined; at others vitiated discharges take place. The tongue is white, often with florid edges. The urine is scanty and high-colored. If the excitement continues unabated, the headache increases, and is often accompanied with delirium. If symptoms such as these persist for from forty-eight to sixty hours, then the febrile phenomena may subside, the skin may become cold, and there will be risk of death from exhaustion and sudden collapse. In most cases the cerebral disturbance is greater in degree, and in these death may take place at an earlier period in the way of coma.”
Until very recently the existence within the United States of this class of cases has not been recognized. But in a very able article in the Therapeutic Gazette of March 16, 1885, John Guiteras shows that the so-called typhoid fever of Key West is the disease described by Morehead.
In the Philadelphia Medical Times, vol. v. p. 664, C. Comegys calls attention to the cases of entero-colitis which are so abundant in the young children of our cities during the hot months. The immediate enormous rise of the mortality-rate among children which always accompanies a marked rise of temperature during July or August indicates very strongly that excessive heat is the chief factor in the production of the disorder. The symptoms may be summed up as high fever, dry tongue and mouth, rapid pulse and respiration, intense thirst, vomiting, purging of greenish, watery, fecal or serous matters with undigested particles of food, and more or less pronounced evidences of cerebral disturbance, such as insomnia, headache, contracted pupils, delirium, and finally coma. In some cases the bodily temperature rises before death to a point comparable with that it reaches in sunstroke of the adult. As pointed out first by Comegys, these cases are almost uniformly relieved by cold water used either, as Comegys himself employs it, in the form of cold affusions practised until the temperature of the child becomes normal, or, as, according to my own experience, is preferable, simple cold baths administered every two to three hours, with just sufficient vigor to produce the desired effect.
Thermic fever in the adult and in this latitude is usually first seen by the physician after the stage of insensibility has been reached. In many cases this condition comes on with great suddenness, but in other instances there are distinct prodromata, such as inaptitude and disinclination to exertion, vertigo, headache, confusion of ideas, great oppression or distress at the præcordia or epigastrium, and disturbances of the special senses. Swift has noticed a peculiar chromatopsia, the sufferer seeing everything of a uniform color, in most cases blue or purple, but in others red, green, or even white, and W. H. Kesteven3 has reported a case in which a man, after exposure to an excessively hot sun, was seized with severe headache, saw everything red or green, and had for some days a distinctly impaired color-sense.
3 Trans. Clin. Soc. of London, 1882, xv. 101.
At one period I saw a large number of advanced cases of sunstroke in [p. 391] the hospital, and the symptoms were quite constant. Total insensibility was always present, with, in rare instances, delirium of the talkative form, and still more rarely the capability of being roused by shaking or shouting. The breathing was always affected, sometimes rapid, sometimes deep and labored, often stertorous, and not rarely accompanied by the rattle of mucus in the trachea. The face was usually suffused, sometimes, with the whole surface, deeply cyanosed. The conjunctiva was often injected, the pupils various, sometimes dilated, sometimes nearly normal, sometimes contracted. The skin was always intensely hot, and generally, but not always, dry; when not dry it was bathed in a profuse perspiration. The intense burning heat of the skin, both as felt by the hand and measured by the thermometer, was one of the most marked features of the cases. The degree of heat reached during life was, in my cases, mostly 108°–109° F., but it sometimes reaches 112° F. The pulse was always exceedingly rapid, and early in the disease often not wanting in force and volume; later it became irregular, intermittent, and thready. The motor nervous system was profoundly affected: subsultus tendinum was a very common symptom; great restlessness was also very often present, and sometimes partial spasms or even violent general convulsions. The latter were at times epileptiform, occurring spontaneously, or they were tetanoid and excited by the slightest irritation. Sometimes the motor system suffered paralysis, the patient moving neither hand nor foot.
This extreme motor relaxation, which in my observation is rare, seems to have been very common in the epidemic described by Barclay,4 as he states that in a large proportion of the cases, from the commencement of the attack until its termination in death, the patient never moved a limb or even an eyelid. Petechiæ and ecchymoses, the evidences of broken-down blood, were present in some of my cases, and there was in one or two instances a fetid hemorrhagic exudation from the nostrils during life. A symptom which has almost escaped the attention of authors was a peculiar odor, which was most marked in patients who had involuntary passages, but was very distinct from any fecal odor. The stools emitted it very strongly, but so did the skin and breath. It was so distinctive as to render possible the recognition of a case by the sense of smell alone. The discharges from the bowels were liquid and very often involuntary. None of my cases passed urine whilst under observation.
4 Madras Quarterly Journal, 1860, 364.
It is plain that the symptoms of coup de soleil, as usually seen, may be summed up as those of intense fever, accompanied by profound nervous disturbance (as manifested by insensibility with or without delirium, and by motor symptoms, such as convulsions or paralysis), by arrest of glandular action, and by changes in the blood. In this ordinary form of sunstroke death takes place by asphyxia or by a slow consentaneous failure of both respiration and cardiac action. It very rarely occurs in less than half an hour after the first decided symptoms, and usually is postponed for a much longer period.
There is a form of coup de soleil in which death results almost at once, and probably always by cardiac arrest, and to which the name of the cardiac variety may well be given. It is very rarely, if ever, met with in civil life, and among soldiers is especially seen during battle or at other [p. 392] times when great exertion is being made. These cases will be more fully discussed in a later portion of this article.
POST-MORTEM CHANGES.—Owing to the excessive heat of the body, putrefactive changes occur very rapidly after death from sunstroke, and various described lesions, especially of the heart, have been undoubtedly the result of post-mortem changes. Later observers have confirmed my original observation, that if the body be opened directly after death the left ventricle will be found firmly contracted, though the right heart and the pulmonary arteries, with their branches, are gorged with dark fluid blood. In my cases the lungs did not present at all the appearance of congestion of their minute capillaries, but when they were cut the blood poured from them abundantly, seemingly from their larger vessels. Not only do the lungs suffer from venous congestion, but the whole body also. The blood appears to leave, as it were, the arterial system and collect in the venous trunks. The arterial coats are often stained red, apparently by the broken-down red corpuscles of the blood.
There can be no doubt that the blood suffers in sunstroke very similarly to what it does in low fevers. Its coagulability is impaired, but not always destroyed; and it is possible that in the very rapid cases it may not be decidedly affected. After death it appears as a dark, often thin, sometimes grumous fluid, whose reaction is very feebly alkaline, or, as I have seen it, even decidedly acid. Levick5 appears to assert that the blood-discs, as seen by him under the microscope, were shrivelled and crenated, and showed very slight tendency to adhere in rouleaux. In several of my cases the blood was carefully examined by the microscope, but nothing abnormal was found. The extravasations of blood which have been found by K. Köster in various parts of the nervous system are probably of the nature of petechiæ, the results of the altered blood-crasis, and not due to any especial affection of the nerve-centres.
5 Pennsylvania Hospital Reports, 1868, 373.
THEORY OF THE DISEASE.—The theories which have been brought forward as explanatory of the phenomena of sunstroke are so various that it would be impossible in the limits of this paper to discuss them. It does seem, however, proper to give a very brief historical sketch of the development of our present knowledge of the subject. In 1854, H. S. Swift6 said that the disease is “now generally admitted to be merely exhaustion produced by fatigue,” although he recognized the existence of an “apoplexy produced by insolation.” The cases which Swift so well describes as those of heat-exhaustion were true instances of thermic fever. The physicians of the Pennsylvania Hospital, especially Gerhard, early called attention to the resemblance of sunstroke to a fever, but it was not until January, 1859, that their views found expression in print in the paper published by James J. Levick in the American Journal of Medicine. This observer tabulated the post-mortem appearances of typhus fever and of sunstroke in contrast, calling attention also to the similarity of symptoms during life. In 1863, H. C. Wood7 claimed distinctly that sunstroke is a fever due to the development of a poison in the blood, and gave to the disease the name of thermic fever. To R. Cresson Stiles is due the credit of having first proven8 the possibility of producing in animals a sunstroke with symptoms and [p. 393] pathological changes similar to those which occur in man. He also came to the conclusion that the symptoms are the results of the direct action of heat, especially upon the muscular system. He says: “The dilatation of the capillaries is explicable by the direct effect of the heated blood upon the muscular fibres of the arteries and the arterioles. The cerebral symptoms and the full and forcible pulse may also be due to this dilatation.” George B. Wood, in the sixth edition of his Practice of Medicine (Philadelphia, 1866), wrote an elaborate article upon the disease, giving it the name of heat fever, and affirming that it “is, I believe, strictly an idiopathic fever.” He further asserts: “In heat fever all the organs, the brain, heart, lungs, stomach, kidneys, etc., are excessively stimulated by the great heat, and all exhibit disorder and at length depression of their functions.” The article of George B. Wood was not based upon experimental researches, but upon a very philosophic rendering of the clinical phenomena, and was a carrying out of the ideas which had permeated the medical teaching of the Pennsylvania Hospital.
6 New York Med. Journ., vol. xiii. p. 53.
7 Amer. Journ. Med. Sci., October.
8 Boston Med. and Surg. Journ., June, 1864, p. 349.
About 1869, Eulenberg and Vohl9 advanced the theory that death from sunstroke is the result of the sudden liberation of gases in the blood; and Weikard affirmed that the death is due to the increase of the coagulability of the blood and consequent formation of clots in the vessels, being in this supported by Richardson of London.10 Contrasting with these in its being really an important contribution is the article of Vallin:11 its chief merit is the conception of the idea of the local heating of isolated parts of the body, and the devising of a plan for carrying the idea into effect. The experiments of Vallin did not themselves prove very much, and led him to the erroneous conclusion, first, that the death in sunstroke is the result either of a coagulation of the left ventricle or else of a disturbance of the innervation of the heart by an action of the heat upon the nerve-centres in the base of the brain; second, that these two forms of death correspond to sthenic and asthenic varieties of insolation—varieties which, I believe, have no proper existence.
9 Virchow's Archiv, t. lxii.
10 St. Bartholomew's Reports, vol. vii.
11 Archives générales de Médecine, Fèvrier, 1870.
The first experiments of Claude Bernard upon the action of external heat were given in a lecture upon muscular respiration on May 3, 1864, published in his Leçons sur les Propriétés des Tissus vivants (Paris, 1866). They were merely incidental to another research, and simply showed that when a warm-blooded animal was exposed to heat it died, the death being, according to the observations of Bernard, the result of cadaveric rigidity suddenly attacking the heart. The more elaborate researches of Claude Bernard upon the effect of exposure of animals to external heat, so far as I have knowledge, were not published in detail until after the nature of sunstroke was determined, although the lectures were delivered in the years 1871 and 1872; they may be found reported in full in his Leçons sur la Chaleur animale, sur les Effets de la Chaleur, et sur la Fièvre (Paris, 1876).
It is proper also to state here that some of the physicians of India had previous to this time more or less imperfectly recognized the relation of sunstroke to fever, but, I believe, none of them distinctly postulated the theory.
The above historical sketch shows that by many authors the relation [p. 394] of sunstroke to fever had been more or less dimly perceived, and that George B. Wood had very clearly stated the true nature of the affection, in that it was simply the result of the direct action of heat. Such statement, however, not resting upon proof, had not been accepted: it was also wanting in detail, and where such details were attempted the surmises were not always correct. Under these circumstances my researches, made in 1870 and 1871, and first published in 1872, led to the complete understanding of the affection.
The space allotted to me in the present volume will not allow of any detailed account of my experiments, but I shall quote from my summing up of the results obtained by them. It was shown that sunstroke may be produced in animals as readily as in man either by natural or artificial heat; that the symptoms are similar to those seen in man; that death takes place ordinarily by asphyxia; that after death the characteristic lesions are alteration of the blood and rigidity of the heart, with immediate or quickly-appearing post-mortem rigidity of the general muscular system; that this rigidity of the heart comes on in most cases after, not before, death, and is a result, not cause, of death; that post-mortem rigidity is dependent upon coagulation of myosin, and that the rigidity of the heart is of similar origin, coagulation of the muscle-plasma occurring almost instantaneously at 115° F., a degree almost attained in sunstroke; that when a muscle has been in great activity immediately before death, myosin coagulates at a much lower temperature, and that the cases of sudden cardiac death occurring in battle among the East Indian English troops were no doubt due to the coagulation of the heart's myosin; that heating the brain of a mammal produces sudden insensibility, with or without convulsions, at a temperature of 108° F., and death when a temperature of 113° is reached; that this effect of the local application of heat is not due to induced congestion, but is the result of the direct action of the heat upon the cerebrum, and that consequently the nerve-centres are as perniciously affected by high temperature as the muscles are; that the nerve-trunks bear a temperature of 125° F. without their conducting power being immediately affected; that whilst the general symptoms induced by heating the brain of a rabbit are very different from those of sunstroke, the nervous symptoms are exactly similar; that the life of the blood is not destroyed by any temperature reached in sunstroke, the amœboid movements of the white blood-cells and the absorption power of the red disks not being injured; that the amount of oxygen of the blood is greatly lessened, as the result of gradual asphyxia combined with abnormal consumption of oxygen; that there is no reason for believing that capillary thrombi are common in sunstroke; that there is no specific poison developed in the blood; that the deterioration of the vital fluid is due to the rapid tissue-changes induced by the fever and the more or less complete arrest of excretion; that such deterioration is secondary to the nervous symptoms, not primary; that if the heat be withdrawn before it has produced permanent injury to the nervous system, blood, or other tissues, the convulsions and unconsciousness are immediately relieved and the animal recovers.
As a postulate from these facts and deductions, I think it follows that the nature of sunstroke is that of a fever; or, in other words, that coup de soleil is a fever, not dependent upon blood-poisoning, but upon heat.
[p. 395]It is of course possible that the external heat causes the fever, simply by preventing the body from throwing off the caloric which it is constantly forming. The extreme suddenness of the onset, however, indicates that in at least many cases there is a sudden outburst, as it were, in the production of heat in the body. This indication becomes more important when it is remembered that in cerebral rheumatism, so called, there is often an equally sudden attack of symptoms plainly the result of a sudden production of animal heat.
In an elaborate research12 I showed the truth of Setschenow's theory, that there is in the pons a centre whose function it is to inhibit the production of animal heat, and that in the medulla a centre (probably the vaso-motor centre) which regulates the dissipation of the bodily heat; and that fever is due to disturbance of these centres, so that more heat is produced than normal, and proportionately less heat thrown off. Let it be supposed that a man is placed in such an atmosphere that he is unable to get rid of the heat which his body is forming. The temperature of his body will slowly rise, and he may suffer from a gradual thermic fever. If early or late in this condition the inhibitory heat-centre becomes exhausted by the effort which it has been making to control the formation of heat, or becomes paralyzed by the direct action of the excessive temperature already reached, then suddenly all tissues will begin to form heat with the utmost rapidity, the bodily temperature will rise with a bound, and the man drop over with some one of the forms of coup de soleil.
12 Fever, Smithsonian Institute, 188-.
Under this view of the case the widespread popular belief, that protecting the back of the head and upper neck from the direct rays of the sun is useful against sunstroke, gains in significance, because it is possible that local heating of the parts spoken of may occur and aid in the production of inhibitory paralysis.
If this theory of thermic fever be correct, heat-exhaustion with lowered temperature probably represents a sudden vaso-motor palsy—i.e. a condition in which the exhausting effects of the heat paralyzes not the inhibitory heat-centre, but the vaso-motor centres in the medulla, since my experiments have shown that vaso-motor palsy increases enormously the loss of animal heat and diminishes its production.
In most cases of sunstroke death comes on gradually by arrest of respiration, such arrest being without doubt due to direct paralysis of the respiratory centres by the excess of heat. Allusion has already been made to the cases of sudden death by cardiac arrest, which have especially been seen in India, almost always during a march or during a battle. “As an example of it may be cited the account given by a witness to Parkes, and incorporated in his work on hygiene,13 of an occurrence during the first Chinese war. The Ninety-eighth regiment was marching on a very hot day, and the surgeon who was with the rear-guard stated to Parkes that the men fell suddenly on their faces as though struck with lightning, and on his running up and turning them over many of them were already dead. Maclean, who was present at this occurrence, confirms the account given by Parkes, but states that it was at the attack on Chiang-Kiang-Foo. The men were thickly clothed, with tight accoutrements and tight, rigid stocks, and were charging up a very steep hill. A great [p. 396] number of them were stricken down, and fifteen died instantly, falling on their faces and giving merely a few convulsive gasps.”
13 Pract. Hygiene, 2d ed., p. 360.
It has been shown that excessive exercise so alters the condition of the myosin of muscle as to cause it to coagulate much more readily than normal. During battle the amount of muscular effort that is made is enormous, and hence it is that men are so often found stiffened in the attitude in which they were struck by the bullet, instantaneous death being followed by equally instantaneous post-mortem rigidity. The description that has been given by Parkes and Maclean of the circumstances in which the sudden deaths just described occurred shows that the heart-muscles must have been strained to their utmost limit. The men were making violent exercise going up hill, so that the heart must have been in exceedingly active exertion, increased by the impediment to the circulation afforded by the tight accoutrements, and under these circumstances the victims probably died instantly because the heart-muscle suddenly set itself from life into the stiffness of death.
The DIAGNOSIS of thermic fever is usually made with great readiness. In distinguishing between it and heat-exhaustion the temperature of the body is the guide. In apoplexy with high temperature it is possible that a little embarrassment might be experienced, but in apoplexy the high temperature follows the nervous symptoms after a distinct interval, but in thermic fever it precedes the unconsciousness. An apoplexy may develop during a sunstroke, but such occurrence is rare. T. S——, now under my care, has had frequently repeated attacks of local convulsions affecting two fingers of the right hand, and one general epileptic attack whilst under observation. He dates his illness to a sunstroke on July 7, 1885, and O. D. Robinson of Georgetown, Delaware, writes me that the attack was undoubtedly true thermic fever, and that the movements of the fingers came on whilst the patient was recovering consciousness. It is probable, therefore, that there was a rupture of a small vessel in the brain-cortex during the sunstroke. The appearance of local convulsions or of localized paralysis during a sunstroke would be good ground for believing that either a clot or a thrombus had formed.
PROPHYLAXIS AND TREATMENT.—The prophylaxis of sunstroke is so evident in its nature that it may be dismissed in a few words. When exposure to heat is imperative the bodily health should be maintained by avoidance of alcoholic, sexual, or other excesses, and, as far as possible, of great bodily or mental fatigue; the diet should be almost purely farinaceous, and the glandular apparatus of the bowels, kidneys, and skin kept in an active state by the use of fruit, water in abundance, and mild salines if necessary. Many persons have a very strong prejudice against the drinking of cold water during exposure to heat; and it is conceivable that large draughts of intensely cold ice-water may do harm by suddenly chilling the stomach; but when the water is taken in small quantities at short intervals, by its action in reducing the general temperature, but especially by its rendering free perspiration more easy, it must exert a most favorable influence. The addition of claret or some other local stimulant to the water is often of great service when there is a tendency to gastric or intestinal depression.
In the mild cases of continued thermic fever the basis of the treatment should be the use of the cold bath. The plan adopted by Guiteras at Key [p. 397] West was to wrap the patient in a dry sheet, lift him into a tub of water, having the temperature between 80° and 85°, and then rapidly cool this water by means of ice. The time of the immersion lasted from fifty to fifty-five minutes, it being regulated by the thermometer in the mouth of the patient. The patient was then lifted out upon a blanket, the skin partially dried, and the body covered. Guiteras found great advantage by giving a moderate dose of whiskey and thirty minims of the tincture of digitalis twenty minutes before the bath. He states that it is very important to avoid currents of air blowing upon the patient and to have the bath given in a small warm room. The result of the bath was invariably a lowering of the temperature, a reduction of the rate of pulse and respiration, and a refreshing sleep. After the second bath the course of the temperature seemed permanently influenced for the better. It was never necessary to give more than two baths in the twenty-four hours, but in some cases they had to be used for many days.
In the severe acute form of thermic fever it is essential that the bodily temperature be reduced at once, and no time should be lost waiting for a physician. As soon as the patient falls he should be carried into the shade with the least possible delay, his clothing removed, and cold affusions over the chest and body be practised. This must not be done timidly or grudgingly, but most freely. In many cases the best resort will be the neighboring pump. In the large cities of the United States during the hot weather hospital ambulances should be furnished with a medical attendant and with ice and antipyrin, so that when a sunstroke patient is reached he may be immediately stripped underneath the cover of the ambulance and remedial measures applied during his passage to the hospital. I believe many lives are now sacrificed by the loss of critical moments in the interval between the finding of the patient and his reaching the hospital ward.
If circumstances favor, instead of the cold affusions, rubbing with ice may be practised. The patient should be stripped and the whole body freely rubbed with large masses of ice. When practicable, a still better plan is to place the patient in the cold bath (50° F.) The employment of enemata of ice-water, as originally suggested by Parkes, may sometimes be opportune.
In using these various measures it must always be borne in mind that the indication is the reduction of temperature: if the means employed do not accomplish this, they do no good.
Relaxation of the pupil is said to be “the first symptom that shows the good of the cold affusion;”14 but as, in my experience, the pupil frequently has not been contracted, reliance cannot be placed upon this, and the thermometer in the mouth or the rectum affords the only proper guide as to the effect of the treatment.
14 Aitken, Practice of Medicine, vol. ii. p. 394.
It must be borne in mind, however, that the cold douche, cold bathing, etc. are powerful remedies, and are capable, if used too long, of doing harm. In my experiments upon animals I have seen the temperature, when reduced by the cold bath after sunstroke, continue to fall, after the animal had been taken out of the water, until it was many degrees below normal.
In the cases which have come under my own observation after the use [p. 398] of the cold bath but little treatment has been required. If, however, the period of insensibility has lasted too long, there may be no return to consciousness, even though the bodily temperature be reduced to the norm. Under such circumstances the case is almost hopeless, and I know of no treatment other than that of meeting the symptoms as they arise, excepting that a large blister should, in my opinion, be applied to the whole of the shaved surface of the scalp.
After the temperature has been reduced, and even after consciousness has returned, there is sometimes a great tendency to a fresh rise of temperature, and consequent relapse. This tendency may be met by wrappings in wet sheets, and, if necessary, by a recourse to the more powerful measures for reduction of temperature which have been already cited. It can be to some extent controlled by the use of quinine, ten grains of which may be given hypodermically. During the heated term of the summer of 1885 antipyrin has been used both in New York15 and in Philadelphia16 with asserted most excellent results; and the testimony is so strong that I think it should always be employed as an aid to, not as a substitute for, the direct extraction of the bodily heat. It should be given hypodermically, as soon as the patient is found, in doses of from fifteen to thirty grains.
15 B. F. Westbrook, New York Med. Journal, July 25, 1883.
16 Orville Horwitz, Trans. College of Physicians of Philada., Oct., 1885.
In cases complicated with repeated severe convulsions, hypodermic injections of one-quarter of a grain of morphia have been very frequently given in the Pennsylvania Hospital, with excellent results. In such patients the use of anæsthetics to facilitate the giving of cold baths would be very proper, but so long as the temperature is high nothing should be allowed to substitute the external cold.
Severe headache and other evidences of cerebral inflammation, manifesting themselves directly after the recovery of consciousness, should be met by local or even general bleeding, blistering, the use of arterial sedatives, mercurials, etc.; or, in other words, by the treatment of cerebral inflammation from other causes adapted to the exigencies of the individual case.
Formerly, venesection was largely practised in sunstroke, with occasional excellent effects, but with, on the whole, very bad results. As free bleeding lowers temperature markedly, it can be readily understood that in some cases it might bring about a return of consciousness and yet be a very improper remedy. If in any instance sthenic apoplectic symptoms persist after the lowering of the bodily temperature by the bath, venesection should be carefully considered. There are cases of sunstroke in which the high temperature irritates the brain or its membranes into an acute congestion or inflammation. These complications are especially prone to occur when the high temperature has been allowed to continue for a long time. A case of this character, in which the autopsy revealed proof of the presence of an acute meningitis, may be found on p. 121 of my book on Thermic Fever. When, then, the patient has a tendency to excessive headache and continuous fever, bleeding may become an essential remedy, not for the cure of thermic fever, but of the cerebral inflammation which has been produced by that fever. The case of S. Weir Mitchell is in point. In his early manhood he had a sunstroke, and when [p. 399] consciousness began to return “the first sensation was that of an intense, agonizing headache, and the next was the perception of his father—J. K. Mitchell—and Mütter discussing the possibility of his recovery. As soon as he could speak, he said, ‘Bleed me.’ His father, coming to the bed, shook his head, but the son repeated, ‘Bleed me.’ He persisted in simply repeating this until they thought him delirious; but at last he mustered strength to say, ‘I am not delirious, but have a frightful headache: if you don't bleed me I will die.’ By this time his pulse had become full and bounding, and finally he sat up and was bled. Ten or fifteen ounces were taken without avail; but as more blood flowed the headache vanished, to be succeeded by a feeling of most delightful languor and rest from pain. Between twenty-five and thirty ounces were taken, and afterward recovery was a very simple matter.”
That Mitchell by the bleeding was saved from meningitis appears almost certain, but it is most probable that if he had been primarily immersed in a cold bath no bleeding would have been required.
SEQUELÆ.—Almost all persons who have had a coup de soleil suffer from after-effects. In the mildest form these are inability to bear exposure to heat without cerebral distress or pain, with more or less marked failure of general vigor, dyspeptic symptoms, and other indications of disturbed innervation. In other cases the symptoms are more decided. Pain in the head is usually prominent: it may be almost constant for months, but is always subject to exacerbations. It sometimes seems to fill the whole cranium, but not rarely is fixed to one spot; and I have seen it associated with pain in the upper cervical spine and decided stiffness of the muscles of the neck. With it may be vertigo, decided failure of memory and of the power of fixing the attention, with excessive irritability. When the symptoms approach this point in severity, there is usually marked lowering of the general health, loss of strength, possibly some emaciation, and the peculiar invalid look produced by chronic disease.
Epileptic convulsions occasionally follow a sunstroke, but, at least in my experience, are always associated with more constant evidences of cerebral disease.
A pathognomonic symptom in the sequelæ of sunstroke is the effect of heat. The glare and heat of summer are the most trying, but usually artificial heat is not well borne. It is very common for headache and severe general distress to be produced by going into a warm room even in the winter months. Where cerebral symptoms are affirmed to be the result of a sunstroke, if there be no excessive susceptibility to heat the alleged sunstroke has almost certainly been an attack of some other nature; and on several occasions I have been enabled to determine that a supposed epileptic attack or a fall followed by unconsciousness from violence was really a sunstroke by noting the extreme susceptibility to heat. The symptom I believe to be a diagnostic one.
The lesion in these cases is usually chronic meningitis, though it is possible that in some instances the gray matter rather than the membrane of the brain may be affected, and in severe cases the gray matter is of course more or less compromised. In one case occurring in the care of S. Weir Mitchell, and in one in my own practice in which death occurred from extraneous causes, severe chronic meningitis was found at the autopsy.
[p. 400]The TREATMENT of these cases is that of chronic meningitis, with the added precautions against exposure to heat. In any severe case change of habitation to a cool climate during the hot period of the year is essential: twenty-four hours' exposure may undo all the good achieved by months of careful treatment.
It is hardly proper here to enter into a detailed discussion of the remedial measures to be employed in this as in the other forms of non-specific chronic meningitis. Local bleedings, the use of counter-irritation, especially by the actual cautery, the internal administration of mercurials and of iodide of potassium in small continued doses, with abstinence from brain-work and the regulation of the habits of life, constitute an array of measures which will no doubt be fully discussed by the author of the article upon Chronic Meningitis.
Provided the patient can be entirely controlled, the PROGNOSIS in these cases is not so bad as at first it appears to be. As an instance of a remarkable recovery I condense from my notebook the case of T. W. H——, aged 49, who came under my care with a history that two years previously he had been seized during a hot day in the summer with a very violent headache, which continued for five weeks, confining him to bed, and was associated, as he said, with fever, but no other symptoms. This attack had been diagnosed by several physicians variously, but as I found that he was excessively affected by any exposure to the sun, was always worse in summer, and that in winter his symptoms were extremely exaggerated even by such heat in a room as is agreeable to many persons, I concluded that the original attack had really been one of thermic fever. He had lost about forty pounds in weight; his memory had become so bad for recent events that he could not call to mind things which had transpired one or two hours previously. Sight had failed much, and there was double vision. He suffered from almost incessant dull headache and excessive general wretchedness; the optic discs were slightly swollen, and one of the margins obscured. There was no albuminuria, and the dyspeptic symptoms were so bad that the man had been treated for months for dyspepsia. Nine months of treatment sufficed to restore this patient almost to his original health. The treatment consisted essentially in the alternate administration of minute doses of calomel and of iodide of potassium—in the meeting of various minor symptoms as they arose, but chiefly in the persistent, merciless use of counter-irritation at the nape of the neck. The actual cautery was applied every one or two weeks, and antimonial ointment freely used on the burnt surface.
SYNONYMS.—Cephalalgia, Cephalœa.
It is not possible to give in a few pages a complete treatise on headache, and it is therefore intended merely to describe the most common types of this malady.
Many forms of headache are symptomatic of some organic cerebral disease, like tumor of the brain or syphilitic diseases of the skull. Headache also constantly accompanies fevers of all kinds. A great number of cases are met with in which no cause for the headache can be discovered, and in which the pain is the only symptom. In these there must be some disordered state of the sensory nerves within the cranium, but just what the nature of the abnormal condition is it is impossible to decide.
The character of the pain in headaches is various. In some cases there is a violent general pain over the entire head. In others the pain is localized in one particular spot, feeling as if a nail were being driven into the skull. This is called clavus, and is often met with in hysterical patients.
Patients sometimes describe the head as feeling as if it were splitting open, or, again, as if it were being compressed. The pain may involve one side of the head alone, hemicrania, or it may be only in the back of the head. The top of the head is a frequent seat of pain, especially in women who have uterine disorders. In short, the pain may be in any or every portion of the head, or it may move about from place to place.
In almost all varieties of headache the pain is aggravated by noises or strong light. Any movements of the patient increase it, and coughing, sneezing, or straining—as, for instance, at stool—adds to the suffering. Tapping on the head usually does not increase the pain, and in some instances alleviates it.
Accompanying the headache is a variety of other symptoms: some of them are nervous, while others are not. There are often disturbances of vision, such as bright spots or zigzags before the eyes; and there may be ringing in the ears; palpitation or slowing of the heart. Nausea occurs in most varieties of headache, and a feeling of general prostration or nervous excitability is often experienced both during and after an attack.
The duration of an attack of headache varies from a few minutes to [p. 402] days or even months: one occasionally sees a patient who says she has not known what it is to have been without pain in the head for years.
The character of the pain may be either a dull aching or it may be excessively intense, so as to cause temporary aberration of mind. As to the structures within the cranium in which the pain is located, it is a mooted question. Some writers believe the dura mater may be the seat of pain in headaches, while other observers have declared this membrane to be insensitive. Probably the intracranial branches of the fifth pair of nerves are the principal site of pain.
We will now consider particularly the different varieties of headache most commonly met with.
ANÆMIC HEADACHE.—The pain is of a dull kind, often diffused over the head, but frequently in the vertex or temples. It occurs in weak, thin-blooded persons, and is relieved by the recumbent position. If the patient is sitting or walking, the pain becomes worse, and there is a sense of faintness or dizziness. Women are the most common sufferers from this form of cephalalgia, and uterine diseases or disorders of menstruation are connected with it. It is associated with palpitations of the heart, difficulty of breathing, a tendency to faint, and general weakness. Anything which exhausts the nervous system, like over-study or anxiety, loss of rest and sleep, is likely to bring on an attack.
CONGESTIVE (HYPERÆMIC) HEADACHE.—In this variety of headache, which is common, the pain seems to affect the whole head and is of a dull, throbbing character. The recumbent position aggravates it, as does coughing or straining. During the paroxysm the face is flushed, the eyes suffused, and the arteries throb violently. Sleep relieves the pain of a hyperæmic headache for a time, but as soon as the patient begins to move about, or even to exercise the mind, the pain returns. Erb1 speaks of a violent pain in the brow and temple, with a sense of pressure and fulness in the head, and heat and redness in the face and ears. This form may come in regular paroxysms. He has seen one case of this kind in which there was violent pain accompanied by fainting, and intense redness of the brow and vertex was observed.
1 Cyclopædia of the Practice of Medicine (Ziemssen), vol. xiv. p. 140.
THE HEADACHE OF HYSTERIA is usually seen in females, although it may occur in males. It is sometimes general throughout the head, but is often located in one spot (clavus), and is very intense. The seat of clavus hystericus is at the top of the head to one side of the sagittal suture. The pain is described as boring, gnawing, and burning. The headache is more severe at the menstrual period, and is increased by worry or trivial excitement. Nervous and hysterical subjects complain of headache which never ceases.
TOXIC HEADACHES are the result of the introduction into the system of various kinds of poisons. The headache following alcoholic excesses is a well-known instance of this kind. The pain, which is deep-seated and often intense, is supposed to be in the sensory nerves of the dura mater. Other forms of chronic poisoning give rise to headache. Lead, when retained in the system, produces headache, and so do many of the narcotic drugs. In some persons the administration of iron always causes pain in the head. The headache following a dose of opium is familiar to all. The excessive use of tobacco is often followed by dull headache next [p. 403] day. The intense pain in the head caused by uræmic poisoning is a well-marked symptom of this condition. Seguin has lately well described the headache of uræmia.2
2 Archives of Medicine, vol. iv. p. 102.
RHEUMATIC HEADACHE is often violent, and the pain seems to be located in the head-muscles. It occurs in rheumatic subjects. It is brought on by exposure to cold, and is increased by damp changes in the weather. In acute rheumatism there are sometimes met with attacks of intense headache. Headache also is associated with the gouty cachexia, and is accompanied usually by depression of spirits and sometimes vertigo.
PYREXIAL HEADACHES.—In all of the acute fevers headache is a prominent initial symptom, and usually continues throughout the course of the disease. The pain is generally dull and deep-seated, and is probably congestive in character. The headache of typhoid fever is constant, and often precedes the fever by many days. Following an attack of typhoid fever, it is not infrequent to find headache persisting for months or even for years.
SYPHILITIC HEADACHE is one of the most violent forms of headache. The pain is diffused or limited to one part of the head, and is associated with tenderness of the scalp. It becomes most severe at night, but never entirely intermits. The nocturnal exacerbations, although very common, do not always occur. The pain is so violent and so constant that the patient is unable to do any work or to occupy himself in any way. There is great mental depression, and the patient becomes gloomy and morose. The pain may be dull and heavy or acute and lancinating; sometimes it is like a succession of heavy blows on the skull. During a severe paroxysm of pain the scalp becomes so sensitive that the lightest touch cannot be borne. The sufferer is unable to sleep, and presents a worn, haggard appearance. Often he has hallucinations at night. Syphilitic headache is often a forerunner of some form of organic cerebral disease. One of the characteristic features of syphilitic headache is its constancy. It never ceases entirely, although at times there are paroxysms in which the pain is so intense as to cause great agony. During the little sleep the patient is able to get he is moaning or tossing about his bed. Minute doses of mercury, repeated at short intervals, have been found to afford great relief in headaches of this kind.
ORGANIC HEADACHE may be described as the headache which accompanies organic disease of the brain or its membranes. Violent pain, seated in one spot and constant in character, is one of the most unvarying symptoms of tumors within the cranium. Brain tumors may exist without headache, but rarely. The pain may be situated in any part of the head: sometimes it is occipital and sometimes frontal, and occasionally it extends over the entire head. It does not always correspond to the seat of the disease. The pain is constant and lasting, and, like syphilitic headache, is liable to exacerbations of excessive violence. These often occur at night. Localized tenderness of the scalp is often present, and percussing the skull over the seat of the disease will increase the pain.
Disease of the membranes of the brain, such as meningitis or new growths in the dura mater, will give rise to persistent headache. So will [p. 404] caries or any syphilitic affections of the skull. Catarrhal inflammation of the frontal sinuses causes dull frontal pain. In inflammatory diseases of the ear there is often headache. In these latter conditions the cephalalgia is probably reflex.
NEURASTHENIC HEADACHE is more or less allied to the hysterical headache. It is met with in persons who are run down in their nervous system by mental worry or overwork—in other words, in persons who are suffering from neurasthenia. Such patients describe the pain as being constant and deep-seated—seldom acute, but dull and throbbing. It is accompanied by a sense of weight and pressure on the vertex, and sometimes by a feeling of constriction. Mental effort increases the pain, and the patient usually prefers solitude and quiet on account of the relief he obtains. The headache of neurasthenia often persists after other symptoms of the affection have disappeared.
SYMPATHETIC HEADACHE is generally connected with disorders of the digestive and sexual organs. The headache of ovarian disease is well known to gynæcologists, and most of us have experienced the pain in the head associated with gastric disturbances. The headache from eye-strain may be considered in this connection, and deserves careful consideration. Many persons have suffered from headaches for years from this cause without its being suspected. Weir Mitchell brought prominently to notice the frequency with which headaches may be caused by defects of vision.3 The fact had been long known to oculists that disorders of the refractive apparatus of the eye would give rise to cerebral discomfort and pain, but it had not before occurred to physicians to look to defects of the eye to explain headaches whose cause was obscure. The points made by Mitchell were—1, that many headaches are caused indirectly by defects of refraction or accommodation; 2, that in these instances the brain symptom is often the only prominent symptom of the eye trouble, so that there may be no ocular pain, but the strain of the eye-muscles is expressed solely in frontal or occipital headache; 3, that long-continued eye troubles may be the unsuspected cause of insomnia, vertigo, and nausea; 4, that in many cases the eye trouble becomes suddenly injurious, owing to break-down in the general health or to increased sensitiveness of the brain from mental or moral causes.
3 Med. and Surg. Reporter, Aug. 1, 1874, and Amer. Journ. of the Med. Sci., April, 1876.
Occasionally the form of headache produced by eye-strain is a migraine, but most commonly there is a steady frontal or occipital pain, which comes on after undue use of the eyes, which are defective as to refraction or accommodation. Accompanying the pain are sometimes nausea and occasionally vertigo. It is not only over-use of astigmatic eyes in reading or other near work which causes the cerebral disorders, but the use of the eyes in the ordinary walks of life may produce pain in a sensitive brain should there be any imperfection in refraction or accommodation.
HEADACHE FROM SUNSTROKE.—A person who has had an attack of sunstroke often suffers from headache for years. The attacks are most likely to occur from exposure to the sun and in summer months, but they are brought on in some individuals even in winter should they be in the sun. Sometimes heat-exhaustion or exposure to the influence of the sun in hot weather, even should there be no actual sunstroke, is [p. 405] followed for a long time by violent headaches. Persons who have suffered in this way have to be extremely careful about exposing themselves to the sun or they will have severe and prostrating pains in the head. The cephalalgia in these cases is probably from congestion of the cerebral meninges or some disturbance of the submeningeal gray matter of the brain. The pain is usually frontal or on the top of the head. Sometimes it is confined to one side of the head. Mitchell4 has seen two cases in which this form of headache was relieved by ligature of the temporal arteries.
4 Med. and Surg. Reporter, July 25, 1874.
HEADACHE OF CHILDHOOD.—Children often suffer from headaches unconnected with meningitis or other organic brain trouble. Over-use of the brain in study is a frequent source of headache, in children especially, if associated with worry or anxiety. If a child complains of headache after study, it is always important to examine the eyes for defects of vision; but while this is often found to be the cause of the headache, in many cases there will be discovered no errors of refraction sufficient to account for the pain; and here the only relief will be to take the child from school and give him plenty of exercise and fresh air.
Another cause of headaches in children is hypertrophied tonsils, which prevent the free return of blood from the brain. Children also suffer from headaches from over-eating or improper food, or from over-exercise in the sun. Migraine, as will be seen later, is a disease which often begins in early childhood, and a child may suffer from frequent attacks of headache of this nature for a long time before they are understood.
Children who are precocious in any way are apt to be sufferers from neuralgias and headaches; but sexual precocity especially predisposes to headaches of the type of migraine. Anstie5 goes so far as to say that the existence of a severe neuralgic affection in a young child, if it be not due to tubercle or to other organic brain disease, is, primâ facie, ground for suspecting precocious sexual irritation.
5 Neuralgia and Diseases that Resemble it, p. 31.
Hillier6 observes that anæmic children from seven to ten years of age frequently suffer from neuralgic headache, and that girls between eight and twelve have violent headaches accompanied by nausea and vomiting (migraine).
6 Diseases of Children, p. 194.
HEADACHE FROM DYSPEPSIA.—Persons who have indigestion have more or less headache, either in paroxysms or as a constant pain. The pain is either frontal or occipital, and may affect the whole head; but it is not confined to one side of the head, as in migraine. The pain is usually dull, and is accompanied by nausea from the beginning of the attack. The tongue is coated, and has red edges, and there are general evidences of gastric disturbance, together with a history of some indiscretion in diet. Sleeping does not always relieve the headache.
DIAGNOSIS.—The diagnosis of the different forms of headache may be made by considering the symptoms. All of the means at our command should be used to carefully distinguish the variety of headache we have to deal with. The head should be palpated for tender or swollen and soft spots, such as are found often in syphilitic headaches. Sometimes percussion of the head will give us some indications as to the kind of [p. 406] headache which exists. The eyes should be examined ophthalmoscopically for changes in the fundus oculi, and the vision should be tested for errors of refraction should there be any reason to connect the pain with the use of the eyes. Inquiry into the habits, occupation, and family history of the patient will aid in arriving at a correct diagnosis.
TREATMENT.—Having reached a correct diagnosis, the treatment will naturally be directed to the special form of headache with which we have to deal. The indications vary more or less with the different varieties, but in all the same object is in view; that is, the relief of pain in the paroxysms, and the breaking up of the diseased condition which leads to the attacks. The means to be used for the former will be considered in the treatment of Migraine, and are more or less applicable to the treatment of all forms of headache.
In children, if no ocular cause is present, it will often be necessary to take them from school and study, and make them take plenty of exercise in the fresh air.
In all varieties of cephalalgia change of climate and travel exert a most beneficial influence. The seashore does not always benefit sufferers from headache, and sometimes the sea air seems to increase the pain.
SYNONYMS.—Hemicrania, Sick headache.
This form of headache is of great importance, from the frequency with which it is met in practice. It occurs in paroxysms at longer or shorter intervals, but the attacks come at periods of tolerable regularity, and, generally speaking, the intervals are entirely free from pain. From the name hemicrania it may be inferred that the pain is confined to one side of the head. This is often the case, but is not invariably the rule.
Migraine has been known for many years, and the term hemicrania is used by the old writers. Until recently, however, there has been some confusion regarding it. Hemicrania often meant trigeminal neuralgia, and nervous sick headache was generally believed to have its origin in the stomach or to be the result of biliousness. Of late years the disease has come to be better understood, and the valuable works of Liveing, Anstie, and others have given a full literature of the subject.
Various conditions predispose to migraine, and of these the foremost are period of life and hereditary influence. Sex also bears a part in the etiology. The majority of patients who are victims of migraine are females. Eulenburg7 states that the proportion is about 5 to 1 in favor of females. My own experience would lead me to believe that in this country the preponderance of migraine in females is not so great. Men are not so likely to consult a physician about headaches, unless they become very frequent and severe; especially is this true of the laboring classes, from whom Eulenburg's statistics were mainly taken. It is true that women are especially prone to neuroses of various kinds through menstrual disorders and at the time of the climacteric, but these do not always take the form of migraine.
7 Ziemssen's Cyclopædia, vol. xiv. p. 5.
Age has a decided influence on the production of migraine. Sometimes [p. 407] the attacks begin in very young children. Eulenburg mentions cases at four or five years. It is during the period of bodily development that the first outbreaks of migraine occur, but more particularly do they set in in both sexes at puberty, a time when sexual development is active and making a strong impression on the whole nervous system. Should migraine become established at this time, it will probably continue to harass the individual until he is forty-five or fifty years of age. After the development of puberty migraine is not likely to originate; indeed, Tissot8 declares that a person who is not attacked by migraine before his twenty-fifth year will escape from it for the rest of his life. It certainly is the case that in later life this affection is much more rare than earlier, as many of the old cases get well and new ones scarcely ever develop. It is a common thing to hear a patient who has reached the age of fifty extolling some new system or remedy as a cure for his headaches, from which he has suffered all his life, when in reality the attacks have ceased or become infrequent on account of the natural course of the disease.
8 Quoted by Eulenburg, op. cit.
Hereditation markedly affects the production of migraine. Eulenburg states that it follows the female line, and is inherited from the mother only; but this is surely a mistake, as we often see males whose fathers suffered from migraine. Persons whose ancestors were of a neurotic type, who suffered from neuralgias, paralysis, hysteria, insanity, etc., are particularly liable to migraine. Epilepsy is also likely to be in the family of an individual who has migraine. There has been observed by many writers the association of migraine and epilepsy in the same person. Epileptics who are predisposed to the disease by inheritance are likely to have attacks of it preceding the outbreak of epilepsy. In families of constitutional nervous tendencies it is common to see certain members who have hemicrania, while others have epilepsy or are insane.
Other predisposing causes in migraine are not so marked as those already mentioned. Station in life exerts but little influence in the causation of the disease. It is met with as often in the laboring classes as in the wealthy. Those who use the brain to any extent in study or business are likely to suffer more often from migraine than those who lead an outdoor life with much physical exercise. Habitual loss of sleep and anxiety also predispose to it.
As to the conditions connected with the immediate production of an attack of migraine, we are in ignorance. It has been thought to depend upon disorders in the circulation of the blood, but then the question arises, Whence these disturbances of circulation? Probably those circulatory disorders which are marked in every case are effect rather than cause of the attack. Indigestion and biliousness must be admitted to favor outbreaks of migraine.
SYMPTOMS.—Migraine occurs at intervals of one or two weeks or longer; often the attacks are not more frequent than every month or even two or three months. I have seen a number of patients who have attacks of migraine on Sunday with regularity, and escape during the interval. Some of these cases ascribed the attacks to sleeping later on this day than on others, but it is more likely that the attacks were the result of the culminating effect of a week's hard work. Between the attacks the patient is usually quite well as far as headache is concerned, [p. 408] but he may have slight neuralgia in branches of the trigeminal. The attacks are more or less alike. They are often preceded by prodromal symptoms for a day or two. The patient may feel languid or tired for a day before the attack. Sometimes there is unusual hunger the night before a paroxysm, or there may be violent gastralgia before each attack. The patient often wakes in the morning after sound sleep with a pain in the head. Should the attack come on in the day, it may be preceded by chilliness, yawning, or sneezing and a sense of general malaise. Ocular symptoms are frequent as a forerunner of an attack. First muscæ volitantes are seen, then balls of fire or bright zigzags appear before the eyes, making it impossible for the patient to read. These symptoms last for a few minutes or a half hour, and then cease, to be immediately followed by pain. Hemianopsia is a precursory symptom of rather frequent occurrence. Ross mentions a case in which the hemianopsia usually lasted about a half hour, and was followed by severe hemicrania. The ocular symptoms are often very alarming to patients.
The pain, as a general rule, is at first in the ophthalmic division of the fifth nerve and its branches. It may begin in the branches of the occipital nerve or in the parietal region. It comes on gradually, is dull and boring at first, but becomes more intense and spreads to one lateral half of the head, more especially the front part. As it increases in intensity the pain seems to involve the entire head. Either side of the head may be affected. Eulenburg thinks that the left side is attacked twice as often as the right. An individual may have the pain on opposite sides of the head alternately in different attacks. The pain is described by patients as dull and boring or intense, and the head feeling as if it would burst. Patients often make pressure on the head to obtain relief. At times the pain seems to be of a violent, throbbing kind, keeping time, as it were, with the pulsation of the arteries. Lying down usually relieves the pain, but if it is violent the recumbent position seems to favor the afflux of blood to the head, and thereby increases the pain. The eye of the affected side becomes bloodshot, and the tears stream from it. The eyelid droops, and the sight is dim and clouded or may fail entirely. The least light is unbearable. During the attack the subject is chilly and intensely depressed, and the feet are very cold. The pulse is at first slow, small, and compressible.
Painful points (Valleix's points) are not present, but there is usually tenderness over the supraorbital notch during an attack of migraine, and after the paroxysm there is a general soreness of the scalp and forehead. Sometimes there remains a tenderness of the parts surrounding the affected nerve. This is not in the nerve itself, but in the adjacent tissues. Anstie9 says that in his own case, after repeated attacks of migraine, the bone had become sensibly thickened in the neighborhood of the supraorbital notch. There is sometimes hyperæsthesia of the skin in the affected regions of the forehead and scalp during an attack. As well as hyperæsthesia, there may be an abnormal acuteness of the sense of touch. Deep pressure over the superior and middle ganglia of the sympathetic causes pain, according to Eulenburg. This observer also states that the spinal processes of the lower cervical and upper dorsal vertebræ are painful on pressure.
9 Op. cit., p. 182.[p. 409]
During the attack of migraine there is complete loss of appetite, and any food that may be taken remains undigested in the stomach for hours. As the pain intensifies there comes on a sense of nausea, there is a profuse flow of saliva, and large quantities of limpid urine are passed. Finally, when the pain seems to have reached its maximum, vomiting occurs. Immediately afterward the pain is greatly increased, but this is the result of the increased amount of blood in the cranial cavity from straining. Soon after, the patient is easier, and falls into a sleep, from which he awakes free from headache. The crisis is not always accompanied by vomiting. In some instances there is no nausea, but at the acme of the pain there are two or three profuse diarrhœic stools, after which the pain is relieved. I have lately seen such a case in a young man of twenty-three years of age. Sometimes there is only a profuse sweat or large flow of urine.
During the attack there are disorders of the circulation. The pulse may be intermittent or irregular, and the extremities are usually cold. Disorders of cutaneous sensibility are also often present. A condition of numbness confined to one lateral half of the body is sometimes experienced during the early part of the paroxysm. This numbness is noticed even in one half of the tongue.
The German writers have divided migraine into two types, and the arrangement may be followed in some instances. The first is called hemicrania spastica or sympathico-tonica. In this form there is supposed to be vascular spasm and a diminished supply of blood in the brain. The symptoms are as follows: When the attack has reached its height the face is pale and sunken; the eye is hollow and the pupil dilated; the arteries are tense and feel like a cord. The external ear and the tip of the nose are cold. Eulenburg10 states that by actual measurement he has found the temperature in the external auditory meatus fall 0.4° to 0.6° C. The pain is increased by stooping, straining, or anything which adds to the blood-supply in the head. At the end of the attack the face becomes flushed and there is a sense of heat. The conjunctiva becomes reddened, the eye is suffused, and the pupil, which had been dilated, contracts. The sense of warmth becomes general, the pulse is quickened, and the heart palpitates. The crisis is reached with vomiting and a copious flow of urine or perhaps a diarrhœic stool. There is sometimes an abundant flow of saliva. One observer has reported that he has estimated a flow of two pounds of saliva during an attack.
10 Op. cit.
The other variety is termed hemicrania angio-paralytica or neuro-paralytica. Here we find the opposite condition of things from that met with in hemicrania spastica. There is marked increase in the amount of blood in the brain. When the attack is at its height the face on the affected side is flushed deeply, hot, and turgid. The conjunctiva is injected, the lachrymal secretion increased, and the pupil contracted. Sometimes there is slight ptosis. The ear on the affected side is hot and red. The temperature of the meatus may rise 0.2° to 0.4° C. The temporal artery is swollen, and throbs with increased force. The carotid beats visibly. There is free perspiration, which is sometimes unilateral. Compression of the carotid on the painful side relieves the pain, while pressing on the opposite carotid makes it worse. The heart beats [p. 410] slowly, the pulse being sometimes as low as 48 to 56. At the end of the attack the face becomes paler and the other symptoms subside.
There are many cases in which the vascular conditions present no peculiarities during the attack, and which cannot be classed with either of the varieties just described.
In all forms, if the patient can be quiet, he usually falls asleep after the crisis has been reached, and awakes free from pain, but feeling haggard and prostrated.
The paroxysm lasts for several hours, generally the greater part of the day. It may last for several days, with variations of severity. The attacks are at longer or shorter intervals of time, and in women they often appear at the menstrual period. The attack may be brought on by over-mental or bodily exertion, imprudence in eating or drinking, and exposure to cold draughts of air. It will often begin as a supraorbital neuralgia from exposure to cold, and go on through all the phenomena of a regular migraine.
Seizures are often brought on by fatigue, and there are some persons who invariably have a violent attack of migraine after a journey. Nursing women are liable to more frequent paroxysms, and I have recently seen a lady who within a few days after delivery after both of her confinements suffered from typical attacks of migraine, although during gestation she had escaped them.
DIAGNOSIS.—Migraine can readily be distinguished from the other forms of headache by the comparative regularity of the attacks and its numerous other characteristics. It differs from neuralgia in the pain being less acute and shooting. The pain of migraine is more dull and throbbing, and extends more generally over the head. The ocular phenomena are more or less constant in migraine and do not occur in neuralgia.
PROGNOSIS.—Migraine is never fatal, and usually becomes less severe and less frequent as middle life is reached. Some patients continue to suffer from it during their entire life, and often when the typical migraine has ceased it is replaced with paroxysms of neuralgia. Therapeutic and hygienic means are of decided influence in the course of the disorder, and many patients experience great relief or temporary immunity from attacks as a result of treatment. Cases of long standing and those of an hereditary type are most unfavorable as to relief from treatment or by spontaneous cure.
PATHOLOGY AND MORBID ANATOMY.—Migraine not being a fatal disease, we know nothing of the changes which exist in the brain; we can only surmise what are the conditions which exist in the brain during and before an attack.
It is evident that there is a strong relationship between migraine and neuralgia of the trigeminal nerve, and if we study the symptoms of the two conditions, and consider the causes which produce attacks of each, we cannot but arrive at the conclusion that migraine is a variety of a neuralgia of the ophthalmic division of the fifth. The late Anstie has most clearly and forcibly given his reasons for believing this to be the case, and we cannot but uphold his view.
Migraine is constantly met with in early life as the type of a neuralgia which in later years loses the special features of a sick headache and becomes [p. 411] a pure neuralgia. The same forms of trophic lesions may occur in migraine and in trigeminal neuralgia. Anstie instances his own case, in which in early life he had distinct attacks of migraine, with corneal ulceration, orbital periostitis, and obstruction of the nasal duct, while later in life his attacks were only neuralgic, without any stomach complications.
Migraine, as already remarked, attacks early life especially at the time of sexual development, and the same is true of epilepsy. There is also the same hereditary predisposition to the former as to the latter. Patients who have migraine belong often to families other members of which suffer from epilepsy, chorea, and an uncontrollable tendency to alcoholic excesses. Indeed, occasionally migraine and epilepsy are interchangeable in the same individual. Many cases of epilepsy have suffered at some time of their lives from severe headaches.
Hughlings-Jackson describes the attacks of migraine as arising from a discharging lesion of the cortex of the brain in the sensory area, or in that part of it which corresponds to the region of pain in the head. Genuine epilepsy he holds to be due to a discharging lesion from the motor area of the cortex. During an attack of migraine the discharging lesion does not remain confined in the sensory portion of the cortex, but extends into the medulla oblongata and the cilio-spinal region of the cord, causing irritation or paralysis of some of these centres, and causing the vaso-motor and oculo-pupillary symptoms which are conspicuous during an attack.
In the form of migraine known as hemicrania sympathico-tonica there is tonic spasm of the vessels of one side of the head. This explains the pallid face, the lowered temperature, and the sunken eyes. After the cause of the contraction is removed, then the vessels relax and the amount of blood-supply greatly increases. Hence the redness of the conjunctiva, lachrymation, and redness of the ear at the close of an attack. The vomiting is explained by Eulenburg as being due to variations in the intracranial blood-pressure. This causes fitful contractions of the vascular muscles, alternating with partial relaxation. These conditions must arise in the sympathetic nerve of the corresponding side.
The dilation of the pupil during an attack depends upon irritation of the cervical sympathetic ganglia. Other symptoms, such as the largely increased flow of saliva and the flow of tears or drying of the Schneiderian mucous membrane, indicate a morbid condition of the cervical sympathetic. The sensitiveness to pressure in the region of the upper cervical ganglia and over the spinous processes of the lower cervical and upper dorsal vertebræ, corresponding to the cilio-spinal region of the cord, confirms the idea of a morbid state of the cervical sympathetic.
In hemicrania angio-paralytica there is supposed to be a relaxed condition of the vessels of one side of the head. Here, instead of an irritation of the sympathetic, there is a paralytic condition, and we have the same results as are seen in animals when the cervical sympathetic is divided. There seem to be good grounds for holding this view when we consider the flushed face, contracted pupil, retraction of the eyeball, and occasional ptosis which accompany this form of headache. Possibly there may be a brief stage of spasm of the vessels preceding the relaxation which occurs in hemicrania angio-paralytica.
[p. 412]The slowing of the pulse during an attack of migraine is due probably to cerebral hyperæmia from relaxation of the vessels, or to the secondary anæmia and irritation of the medulla oblongata. This irritation of the medulla is also able to explain the other symptoms of vaso-motor disturbance which occur during an attack of migraine; for instance, the small and contracted radial artery, the extreme coldness of the hands and feet, and the suppression of perspiration over the whole body except perhaps on the affected side of the head. Following the stage of irritation of the medulla with contraction of the vessels comes one of exhaustion with relaxation of the vessels. This latter state may account for the profuse flow of saliva and the copious secretion of sweat and urine, as well as the increased secretion of bile and the condition of broncho-tracheal catarrh during the attack.
We now come to the question of the origin and seat of the pain in migraine. This question has involved a great deal of thought, and has been answered in various ways by different writers. E. du Bois-Raymond thought that the pain was due to tonic spasm of the muscular coats of the vessels, and that thereby the nerves in the sheaths of the vessels were pinched, as it were, and so caused pain. Moellendorff was of the opinion that the pain was due to dilatation of the vessels, and not to contraction; and this theory might explain the pain in the angio-paralytic form. There are many cases in which neither of these views is sufficient, for we have no reason to believe that a condition of either anæmia or hyperæmia is present.
Romberg believed that the pain was situated in the brain itself, and Eulenburg holds that the pain must be caused by alterations in the blood-supply, without regard to their origin, in the vessels of one side of the head. He thinks that the vessels may contract and dilate with suddenness, just as is often seen in some neuralgias, and thus intensely excite the nerves of sensation which accompany the vessels. The increase of pain upon stooping, straining, or coughing, and the influence upon it by compression of the carotids, seem to give force to this view. But are we not here confusing cause with effect? Are not these variations in the calibre of the vessels due to the irritation of the sensory and vaso-motor nerves, which are in a state of pain? No doubt increase in the blood-supply augments the pain, just as it does in an inflamed part when more blood goes to the part. Let a finger with felon hang down, or let a gouty foot rest upon the floor, what an intensity of pain follows!
Anstie very ably advocated the theory of migraine being a variety of trigeminal neuralgia in the ophthalmic division; and we incline strongly to his view. An attack of migraine often begins with pain distinctly located in the supraorbital nerve as the result of exposure to cold. Frequently it begins in the infraorbital nerve or in the branches of the inferior maxillary division of the fifth. The pain then spreads over one side of the head, both outside and inside, and goes through the recognized symptoms of migraine. In my own case I have often had an attack begin with sharp pain in the supraorbital notch in a spot which could be covered by the tip of the finger. The nerve has seemed swollen, and has been highly sensitive to pressure. Then have come pain extending over the entire side of the head, without its limits being distinctly definable, and the accompanying phenomena of lachrymation, excessive salivation, [p. 413] and copious flow of urine, winding up with vomiting or ineffectual nausea and retching.
Anstie brings forward as arguments to support his view the facts that the attacks of migraine often interchange with neuralgic seizures, and that a person who has been migraineuse in early life may in later years lose his hemicranial attacks, and have violent neuralgia in the ophthalmic division of the fifth nerve.
The true seat of the lesion, if we may so call it, upon which the exaggeration of pain-sense depends, is probably in the nerve-centre; that is, in that part of the trigeminal nucleus back to which the fibres go which are distributed to the painful areas. The pain is no doubt chiefly intracranial, and in those portions of the cerebral mass and meninges to which branches of the trigeminal are distributed. All of the divisions of the trigeminus send branches to the dura mater. Many nerves are found in the pia mater as plexuses around the vessels, some of which penetrate into the centre of the brain. Most of these nerves come from branches of the trigeminus.
TREATMENT.—The treatment of migraine must be directed to the palliation of the attacks and to their prevention. So little is known of the direct cause of the disease that it is difficult to lay out any distinct course to be followed. Many cases, however, which seem to depend upon a run-down state of the patient are vastly improved by a course of tonics and building up. I have often seen anæmic and feeble women whose attacks were frequent become exempt for a long period by simply taking iron, quinine, and strychnia, and taking an increased amount of nourishment. The rest-treatment of Weir Mitchell is particularly applicable to these cases. In persons whose digestion is bad, and who suffer from constipation, much can be done by relieving these conditions. Some cases which are due to uterine disturbances are benefited by treatment directed to the womb. There are many cases, however, in which no cause is apparent. The patient is well nourished, his eyes are good, he undergoes no strain mentally, morally, or physically, and yet the attacks of migraine come with tolerable regularity. In these persons change of climate sometimes works marvellously beneficial results. I saw last year a young lady who suffered from terrific headaches which sometimes lasted for days. No plan of treatment or regimen seemed to exert the slightest influence upon the attacks, and yet on going to the far West for the summer she remained without an attack during the whole time she was there. In some individuals all forms of treatment may be tried in vain. Anti-periodics have been tested, but with doubtful benefit. Cannabis indica is probably the most potent remedy which is at our command. Its effects are most decided, and many cases of severe hemicrania have been cured by this means alone. It must be given for a long time, and in some instances it is necessary to give gradually-increasing doses up to the physiological effects. The drug must be of good quality, otherwise we need expect no good from it. Indian hemp is well known to be variable in strength, and the best form in which to use it is a fluid extract made by some reliable chemist. Arsenic, phosphorus, and strychnia do not seem to do as much good as in other neuralgias, except so far as they build up the general health.
Ergot has been used with success as a curative means, and it probably [p. 414] acts by contracting the vessels of the medulla oblongata. A combination of ergotin and extract of cannabis indica may be given together; and if persisted in for a long time will often be of benefit in lessening the frequency of the attacks. The prolonged use of one of the bromides is sometimes found curative.
Anstie has found the careful use of galvanism to the head and sympathetic of positive advantage in keeping off attacks, and Eulenburg has had the same experience.
In the treatment of the attack the patient should be freed from all sources of external irritation. He should lie down in a darkened room, and all noises should be excluded. If the attack is of the hyperæmic variety, the patient's head should not be low, as this must favor increase of blood to the head. In this form the patient is often more comfortable sitting up or walking about. Occasionally an impending attack can be warded off by the administration of caffeine, guarana, or cannabis indica. Purgatives are of but little value in this form of headache. The local application of menthol or of the oleate of aconitia to the brow of the affected side will sometimes prevent an attack. If a person can lie down quietly when he feels an attack coming on, one or two doses of fifteen grains each of the bromide of lithium will enable him to sleep, and wake free from pain. I have found the lithium bromide far more valuable in migraine than any other of the bromides. An effervescing preparation known as bromo-caffeine is often efficacious in aborting a paroxysm or in palliating it when it has got under way.
Quinine, in my experience, seems to be of little use in preventing or cutting short a paroxysm of migraine, although Ross11 has found that a dose of ten or fifteen grains may arrest it. Ergot has been found useful, and, as it acts by contracting the arterioles, should be given only in the angio-paralytic form. The fluid extract of ergot may be administered, but ergotin in pill form is more acceptable to the stomach.
11 Diseases of the Nervous System, vol. ii. p. 558.
Inhalations of nitrate of amyl have been used with advantage. Berger, who was the first to employ this remedy, found that a single inhalation of a few drops relieved the pain at once, and it did not return that day. It is indicated only in the sympathico-tonica type. If it is used, two or three drops of the nitrate in a glass pearl may be crushed in the handkerchief and inhaled. Nitro-glycerin may also be given in this variety of migraine.
Once the attack has begun fully, we can only attempt to mitigate the pain. Firm pressure on the head generally gives relief, and encircling the head firmly with a rubber bandage is often of great comfort. Compression of the carotids gives temporary but decided ease to the pain. Strong counter-irritation in the shape of a mustard plaster to the nape of the neck or a stimulating application, like Granville's lotion, to the vertex, will afford relief. I have found in some cases that placing a hot-water bag, as hot as could be borne, against the back of the head alleviates the pain. In other instances cold affords more relief, and an ice-bag resting upon the forehead is the most efficacious way of applying cold. Hot bottles to the feet are an accessory not to be overlooked.
In the way of medicine we may give the bromide of lithium every hour. The bromide of nickel has been recommended by DaCosta as [p. 415] having peculiar advantages. Cannabis indica may be given in doses of a quarter of a grain of the extract every two hours until relief is obtained. Anstie believes strongly in chloral, and says that a single dose of twenty or thirty grains will often induce a sleep from which the patient wakes free from pain. The same writer advises the administration of muriate of ammonium, but it is too nauseous a dose to be given when the stomach is as much disturbed as it usually is in an attack of migraine.
Croton chloral is preferred by some to the chloral hydrate. Ross, for example, gives it in doses of five grains every four hours until relief is obtained.
Galvanism through the head is often of relief, especially at the beginning of an attack; but this means is not often available, for it is not easy to have the suitable apparatus for the constant current at a patient's home when it is needed. Should galvanism be used, one pole should be placed on each mastoid process, and a weak current passed through the head for two or three minutes. The sympathetic may be galvanized by placing one pole over the upper cervical ganglion, just behind and below the angle of the jaw, while the other pole is held in the hand or placed upon the sole of the foot. In hemicrania spastica the positive pole is put over the ganglion, and in the angio-paralytic type the negative pole is placed in this location.
Should all of the above means fail, we may resort to morphia hypodermically. Jewell12 favors the administration of morphia and atropia, either by the mouth or hypodermically, from the beginning of an attack until the pain is eased; but I believe that morphia, except as a last resort, is very undesirable in migraine. Although a small dose hypodermically will usually promptly bring relief, there are the unpleasant after-effects of opium felt, and the patient feels more prostrated and with more disordered digestion than had no morphia been used. Besides, the morphia habit is liable to be formed, especially in women, when the drug has once begun to be taken.
12 Journal of Nervous and Mental Diseases, 1881.
It is for this reason that I prefer to use the bromides, and if a patient is seen at the beginning of a paroxysm, given a fifteen-grain dose of bromide of lithium, his feet put in hot mustard-water, and he then goes to bed, he will almost always cut his attack short, and on waking from sleep will feel refreshed and able to take food.
I am strongly convinced of the importance of arresting or shortening the paroxysms of migraine, especially in the young, at the beginning of the disease. By this means the habit of long attacks is prevented, and their prostrating after-effects are avoided. Should we succeed in checking the first few attacks, we may by tonics and regimen improve and fortify the constitution so as to eradicate or modify the neuralgic tendency.
DEFINITION.—The clinical meaning of vertigo has gone, as is common, far beyond what the term implies. We may define vertigo to be a sense of defective equilibrium, with or without actual disturbance of position, and accompanied by varying amounts of subjective feelings of motion of external objects, of the body itself, or of the contents of the cranium.
SYMPTOMATOLOGY.—Vertigo consists of attacks which are single or repeat themselves during a continuous condition lasting for hours or days, and which I have elsewhere described as the status vertiginosus.1
1 Med. and Surg. Rep., June, 1877.
The mildest form of vertigo is that in which the patient has a sensation of the contents of the head as being in motion. If more severe, there is disturbed equilibrium, an effort is needed to stand erect, or there is, as in most vertigo, a fear of falling. The brain seems to be moving round or upward. This type is found in insanity, in hysteria, and in the vertigo of mental effort observed in extreme cerebral exhaustion.
In a second clinical species of vertigo the patient appears to himself to be in motion, while outside objects maintain for him their places. This may or may not be accompanied with sensory disturbance or an approach to mental confusion. It is really a delirium of movement. The patient feels as if he were rolling or falling or reeling or dropping through space. Meanwhile, however grave the hallucination, he walks and stands without the least sign of defect in balancing power. These cases are very rare, but are sometimes seen as temporary results of hysteria.
Perhaps it is doubtful whether we should really class this symptom-group as vertigo.
The more common or typical expression of vertigo is marked in its fulness by a false sense of the movement of external objects and of the relations in space of the individual to such objects. The pavement rolls or seems to be coming up in front of him; the houses stand at angles; walls, pictures, chairs, and tables reel around him, are still a moment, and again move; or the bed seems to be aslant or to rock to and fro. In extreme instances objects are seen as if inverted, and whenever the vertigo is marked the victim reels or falls, or seeks by rest supine or by closing his eyes to lessen the terrors of the attack. In severe examples no such help avails, and for hours or days the patient may lie clutching at the bed for support or in deadly fear of a new onset of vertigo, [p. 417] which in some cases is brought on by the least movement of the head, by taking food, by efforts to think, or by mechanical vibrations.
In most cases there is some mental confusion, or even brief loss of consciousness at the close of the attack, and nearly always more or less nausea or vomiting occurs—symptoms which have frequently misled observers as to the cause of the vertigo, but which have in most cases only the significance gastric disturbance has in migraine. As in that disorder, but more rarely, the emesis may be associated with or replaced by looseness of the bowels, and is very apt to be followed by a flow of pale clear urine.
Fits of vertigo are often as distinct clinically as epileptic attacks. The patient has for a few moments, in an acute form, all of the phenomena of vertigo, and may then recover promptly, or it may chance that he has a vertiginous status and a series of fits, or remains for long periods in a state of chronic disorder of head, with now and then an acute onset.
Physicians do not often witness these fits: I have been so fortunate as to see several. I take this description of one from my notes: A young clergyman, after excessive overwork among the poor, came to consult me for vertigo. As I talked to him an attack came on. I asked him to keep as composed as possible and to tell me what he felt. He said: “It has just begun. The objects in the room are moving from right to left; I can seem to hold them still for a moment, then they go on and move faster. If I shut my eyes it is relief, but only for a time. I feel myself as if I were now going round with them. The chair rocks, and my brain seems moving too.” At the same time he became very pale, and slipped from his seat. His pulse was quick and feeble and rapid, and as he lay on the floor unconscious a profuse sweat broke out on his face. In a moment he was again himself, but did not recover so as to walk for a half hour. He then complained of headache, but was able to walk home. This is a fair example of a fit of vertigo, due, as it proved, to at least two of the causes of vertigo, which I shall presently discuss.
A few persons insist that something like a distinct aura precedes the attacks. In other cases the brain symptoms develop gradually, from a faint sense of dizziness up to a tumultuous feeling of confusion with sensory illusions. In a few rare cases there is, as in that above mentioned, an abrupt onset. Something seems to snap in the head, and the vertigo follows; or, most rare of all, we have a sensory discharge felt as light or sound, and followed by the ordinary symptoms.2
2 See the author in lectures on Nerv. Diseases, Disorders of Sleep, p. 63, 2d ed.
DIAGNOSIS.—Vertigo is of course, as a rule, only a complex symptom of one or more numerous conditions. Acute isolated fits of vertigo are sometimes puzzling, because epilepsy may be preceded by brief vertigo and exist without notable spasms. Time may bring to us a frankly expressive epilepsy to explain former and less distinct fits. But usually it is the attacks of vertigo which are the causes of doubt. A man has sudden giddiness, and falls unconscious for a moment. These attacks persist. How shall we know them as vertigo? how be secure that they be not some form of the lesser epilepsy? As a rule, if they be vertigo there will be nausea or emesis, while the intervals between attacks will offer the usual signs of confusion of head, fear of losing balance, and all the numerous evidences of disturbed and easily excitable states of the [p. 418] sensorium—conditions rare in the interepileptic periods. The effect of bromides may aid the diagnosis, for, although often of use in vertigo, they have not such power to inhibit the fits as they possess in epilepsy. Persons long liable to any form of vertigo can readily cause attacks, or at least vertiginous feelings, by closing the eyes while standing, by the least rotation, or by putting a prism on one eye, so that among these tests we may frequently find the material for a diagnosis, which will of course, in many instances, be made easy enough by the presence of causes obviously competent to occasion the one or the other disease.
PROGNOSIS.—In true vertigo, if we exclude the organic causes, and especially intracranial neoplasms, there is very little to be feared. Deaths have been seen in Menière's disease, but are most rare. Even in grave examples of labyrinthine vertigo there is a probability that the worst which can occur will be deafness, and that vertigo will gradually cease as the delicate neural tissues become so degenerated as to cease to respond to irritations.
The DURATION of other forms of vertigo it is less easy to predict. Ocular vertigoes get well soon after the eye trouble is corrected, and the like is true of most vertigoes due to peripheral causes. So also the giddiness which is sometimes seen as a very early symptom in locomotor ataxia is transient, and will be apt, like the ocular and bladder troubles which mark the onset, to come and go, and at last to disappear entirely. It is to be remarked that vertigo at the beginning of posterior sclerosis is common, and is not due to ocular motor conditions.
Sometimes in vertigo, as in epilepsy, the removal of a long-existing cause may not bring about at once a cessation of the abnormal symptoms its activity awakened, so that it is well, as to the prognosis of duration, to be somewhat guarded in our statements. Nor is this need lessened by the fact that vertigo may be an almost lifelong infliction, without doing any very serious damage to the working powers of the person so disordered.
ETIOLOGY.—It is generally taken for granted that vertigo has always for its nearest cause some disorder of cerebral circulation; but while either active congestion or anæmia of brain may be present with vertigo, and while extreme states of the one or the other are certainly competent to produce its milder forms, it does not seem at all sure that they are essential to its being. Indeed, there is much reason to believe that vertigo is due in all cases to a disturbance of central nerve-ganglia, and that the attendant basal condition is but one incident in the attack.
In vertigo there are the essential phenomena, as disturbed balance, with a false sense of movement within or without, or of one's self. Then there are the lesser and unessential phenomena, which vary in kind and degree, and these are the moral and mental symptoms—terror, confusion of mind, and sensory illusions; and, last, the nausea and sickness met with here as in migraine, and the flow of clear, thin urine.
All of these symptoms should be accounted for in speaking of the intracranial organs, disorder of which causes vertigo. Ferrier has especially made it clear that equilibration involves afferent impressions, co-ordinative centres, and efferent excitations preservative of balance.
Guiding impressions, which direct the muscles through centres below the cerebrum, so as to aid in preserving our balance, reach these centres [p. 419] from the skin and the muscles, so that great loss of tactility or of the compound impressions called muscular sensations results in disturbance of equilibrium, but not in true vertigo, which is clinically this and something more.
A second set of impressions, of use in preserving equilibrial status, come through the eye, or rather habitually through the eyes, because the consensual impressions arising out of double vision and the co-ordinate movements of the two fields of sight have, as is well known, much to do in this matter. It is hardly needful to dwell on this point. Certain parts of the ear have, however, the largest share in maintaining our balance, and it seems likely that the semicircular canals—the part most concerned—although lying within the petrous part of the temporal and receiving nerves from the stem which constitutes the nerve of hearing, may have slight relations or none to the sense of audition.3 When the horizontal canals are cut, the head moves from side to side and the animal turns on his long axis. When the posterior or lower vertical canals suffer, the head sways back and forward, and the tendency is to fall or turn over backward. When the upper erect canals are cut, the head moves back and forward, and the tendency is to turn or fall forward.
3 I have seen a single case of vertigo, with slight deafness on both sides, in which the sense of the position of sounds was absolutely lost.
In pigeons, injury on one side may get well, but when the canals are cut on both sides there is permanent loss of balance. In some way, then, these little organs appear to be needful to the preservation of equilibrium; and of late some interesting attempts have been made to explain the mechanism of this function. It probably depends on the varying pressure relations of the endo-lymph to the nerve-ends which lie in the membranous canals.
Wm. James of Harvard has shown that total loss of hearing is usually accompanied by lessened susceptibility to vertiginous impressions, so that the stone-deaf are not apt to be seasick or giddy from rotation, owing to their having lost the organ which responds to such impressions. It would seem also that the entirely deaf have peculiar difficulty in certain circumstances, as when diving under water, in recognizing their relations to space.
There is a general tendency to regard the cerebellum as the centre in which all the many impressions concerned in the preservation of equilibrium are generally received and made use of for that purpose. There may be several such centres, and the matter is not as yet clear. Whatever be the regulative ganglion, it seems clear that it must be in close relation to the pneumogastric centres, to account by direct connection or nerve-overflow for the gastric symptoms. But, besides this, vertigo has clinical relation to moral and mental states not easy to explain, and in extreme cases gets the brain into such a state of excitability that mental exertion, emotion, strong light, or loud sounds share with the least disorder of stomach capacity to cause an attack.
Vertigo may be due to many forms of blood-poisoning, as at the onset of fevers, inflammations, the exanthemata—notably in epidemic influenzas. It may arise in malarial poisoning, sometimes as the single symptom, as well as in diabetes, albuminuria, lithæmic conditions, and in all the disorders which induce anæmic states. Common enough as sign of brain [p. 420] tumor, and especially of growths in or near the cerebellum, as a result of degenerated vessels, it is also not very rare in the beginning of some spinal maladies, especially in posterior sclerosis, and is not always to be then looked upon as of ocular origin.
Alcohol, hemp, opium, belladonna, gelsemium, anæsthetics, and tobacco are all, with many others, drugs capable of causing vertigo.
In hot countries heat is a common, and sometimes an unsuspected, cause of very permanent vertigo.
Lastly, excess in venery, or, in rare cases, every sexual act, profound moral and emotional perturbations, and in some states of the system mental exertion, may occasion it, while in hysteria we may have almost any variety of vertigo well represented. Outside of the brain grave organic diseases of the heart are apt to produce vertigo, especially where the walls of the heart are fatty or feeble from any cause. Suppression of habitual discharges, as of hemorrhoids or menstrual flow, is certainly competent, but I have more doubt as to the accepted capacity of rapidly cured cutaneous disease.
The following are some of the more immediate causes of vertigo: They are disorders of the stomach or of the portal circulation; laryngeal irritation; irritation of the urethra, as passing a bougie, especially when the patient is standing up; affections of nerve-trunks; nerve wounds; sudden freezing of a nerve (Waller and the author); catarrhal congestion of the nasal sinuses; inflammation and congestion of inner ear, many irritations of the outer and middle ear; prolonged use of optically defective eyes; insufficiency of external muscles of the eye.
It will be needful to treat of some of these causes of vertigo in turn.
Gastric Vertigo.—Trousseau certainly misled the profession as to the frequency of this form, but he did little more than represent popular medical views, and we may now feel sure that a good many so-called gastric vertigoes are due to lithæmia or to troubles of ear or eye. There are, I think, three ways in which the gastro-duodenal organs are related to the production of vertigo. Acute gastric vertigo arises in some persons inevitably whenever they eat certain articles, and the limitations are odd enough. Thus, I know a gentleman who cannot eat a mouthful of ice-cream without terrible vertigo, but otherwise his digestion is perfect. I know another in whom oysters are productive of vertigo within ten minutes; and a curious list might be added, including, to my knowledge, milk, eggs, oysters, crabs, etc. In these cases digestion is arrested and intense vertigo ensues, and by and by there is emesis and gradual relief.
In other cases, owing to over-feeding or any of the numerous causes of acute dyspepsia, an individual has a sudden attack of acid stomach, and as this gets to its worst he has alarming vertigo. In these cases the room whirls around or the pavement rocks; the balancing power is disturbed or lost; the sense of movement in the brain itself is sometimes felt; there are slight buzzing or humming sounds in one or both ears; there may be double vision, which comes and goes, while the power to think is lessened and the terror created is quite unendurable. At last come the sweat of nausea, emesis, and relief, with a gradual fading away of all the symptoms.
As a rule, such an attack need cause no uneasiness as to a fatal result, but, unless the case be handled with skill, it is apt to repeat itself with [p. 421] or without repetitions of the originating cause, until what I have called the status vertiginosus is created, and we have more or less steadily present a slight sense of defective balance, of confusion of mind, of blurred vision, and, more rarely, of slight noises in the ears. After two or three grave attacks, attacks are added for which the patient sees no cause. He lives in a state of constant terror, and the status vertiginosus attains its highest development, and may last for unlimited periods, while the brain becomes endowed with new morbid susceptibilities. To read, to write, to face sudden sunlight, to see moving bodies or passing crowds, cause vertigo. Loud sounds disturb the balance; even music will affect it. Emotions or any decided mental efforts are equally competent to bring on attacks, while fatigue or sudden changes of posture have to be alike avoided.
I have sketched an extreme case, but whatever causes grave vertigo is able to bring on the set of symptoms here described, which are, after all, more apt to be due to aural than gastric states.
Vertigo as a result of chronic dyspepsia in any of its forms is rare, and as a rule is less severe than that which grows out of acute gastric dyspepsia. The sensory symptoms are trifling, and the confusion of head and the lack of balance less notable, while the vertigo, which is more or less constant, seems to be most often met with two to four hours after meal-time, so that it is usually doubtful as to how much is due to reflected impressions from the digestive tracts, and how much to the direct influence of imperfect material in the circulation.
In a third form the gastro-intestinal tract is but indirectly concerned. In a person who is anæmic, or who is nervous and perhaps hysterical without being anæmic, but in whom it is impossible to detect in the stomach or bowels, in the feces or urine, any sign of defective digestion or of malassimilation, we find that during the act of digestion there is at some time, and in a few cases constantly, some transient but not grave vertigo.
This is due simply to the influence exerted on an over-sensitive head of a normal functional activity, which may act directly as any peripheral cause would act, or may be due, in the anæmic, with this to the withdrawing of blood from other parts of the body which occurs in digestion. It is an illustration of what is too often overlooked, the capacity of a healthy functional act to disturb morbidly a sensitive brain.
Aural Vertigo.—Vertigo may be due to a variety of irritative causes acting on the outer, middle, or inner ear. We shall consider them separately.
Vertigo from Causes acting on the External Ear.—In animals I have found that the injection of iced water or a rhigolene jet into the meatus is at once the cause of convulsive movements in the rabbit, and that repetitions of this cause at last a permanently vertiginous state, so that when a rabbit or guinea-pig thus disordered was shut up in darkness for some hours, sudden sunlight caused it to be for a few moments vertiginous. It is remarkable that while in birds many parts of the skin are competent under irritations (Weir Mitchell, Ott, Brown-Séquard) to give rise to vertiginous phenomena, in mammals only the skin of the external auditory meatus appears to be thus responsive. The author was himself the best illustration of this fact. Some years ago, when by [p. 422] mishap water at about 52° F. was thrown into his left ear, he fell instantly on his left side, with slight disturbance of vision, the room seeming to rock in the direction of the fall—that is, to the left. He arose with some difficulty, his head swimming, and with a distinct sense of lack of power in the whole left side, and with, for a half hour at least, an alarming tendency to stagger to the left.
Thus, injections of cool water in some cases (or in others of water at any temperature), and in certain persons very hot water, will cause vertigo. Foreign bodies—hardened wax, aspergillus, ulcers—or any inflammation may occasion it, while it is curious that usually the painful abscesses of the ear do not, especially in children, who are, as a rule, less liable to vertigo than are adults.
The tendency of aurists is, I believe, to explain the phenomena by either direct influence propagated as sound-waves through the auditory apparatus to the labyrinth, or by admitting inhibitory impressions affecting the vaso-motor loops and causing increased pressure in the semicircular canals. I am disposed to think that the effect may be a more direct one, and to regard the centres as directly influenced through the fifth nerve, including vaso-motor phenomena of course—a question to be, however, easily solved in the laboratory.
In this form of vertigo tinnitus is slight or transient, coming and going, or if permanent but faintly felt.
Middle-ear vertigo may arise from any inflammation of the part or from closure of the Eustachian canal. There are then direct mechanical influences affecting the labyrinth, as well as sensory irritations, not causing auditory phenomena; whilst also the inner ear is apt soon to suffer from direct propagation of inflammatory processes. There is then paroxysmal vertigo, variable hearing,4 and early tinnitus.
4 Burnett, Sect. Otol., Int. Med. Cong. Proc., 1876.
Inner-ear vertigo seems to be due to irritations, auditory, mechanical, or inflammatory—whatever disturbs seriously the nerves of the semicircular canals, since, if we may trust recent research,5 the cochlea is not a source of vertiginous impressions. This form of vertigo was first described with pathological proof by Menière in 1860, and is probably in its variety of degrees the most common of all the origins of dizziness.
5 Gellé.
The acute attack is nearly always preceded by more or less deafness, and in many cases by middle-ear catarrh,6 with or without tinnitus. More rarely all the symptoms arise abruptly. There are sudden tinnitus, deafness, nausea, vertigo. The loss of hearing remains, and is variable, or, finally, the hearing is lost altogether. The tinnitus is permanent or varies in amount, but as the deafness grows complete the vertigo disappears, and although cases of death have been described, labyrinthine vertigo is, as a rule, prone to get well in time.
6 Burnett.
Single attacks are rare. It is apt to repeat itself, and finally to cause all the distressing cerebral symptoms which characterize the worst gastric vertigo, and at last to be capable of easy reproduction by light, heat, over-exertion, and use of the mind or eyes, by emotion, or by gastric disorder.
Even after the vertigo has ceased to exist the fear of loss of balance remains, while perhaps for years the sense of confusion during mental effort continues, and gives to the sufferer a feeling of what a patient [p. 423] described to me as mental vertigo—some feeling of confusion, lack of power to concentrate attention, loss of hold on trains of thought, with now and then a sensation as if the contents of the cranium moved up or down or swayed to and fro.
The attack in the gravest forms is often abrupt, and, according to Charcot, is always preceded by a sudden loud noise in the affected ear. I have, however, notes of many cases in which this was not present. The patient reels, staggers, or falls, usually forward or to one side, loss of consciousness being very rare. The sensory hallucinations are remarkable. If at rest or after his fall he seems to himself to sway, and tends to pitch or roll over; the bed rocks, the room and its contents reel. The patient's terror is intense; he clutches the bed; seeks relief in fixing his eyes on an object, which in slight attacks is competent to relieve, or else he closes them. The least motion starts the vertigo afresh. In some cases turning the head or looking up will bring it back, or the patient may remain for days or weeks in this condition, with continuous dizziness and frequent recurrences of severe vertigo, while there is more or less constant nausea and sometimes vomiting.
There should be no trouble in distinguishing the cases in which deafness exists, but the nausea is apt to direct attention to the stomach. Tinnitus is common in vertigo, however arising; and when, as I am sure does chance, there is for years now and then a slight and transient deafness with vertigo, or a permanent deafness in one ear, and therefore not noticed, the inner ear is apt to be overlooked as a source of trouble.
Vertigo from growths on the auditory nerve before it enters the inner ear is rare in my experience. It is described as slow in its progress, the deafness and tinnitus being at first slight, but increasing steadily, while there is tendency to fall toward the side affected.7 In the cases of disease attacking the seventh nerve within the cranium there is usually so much involvement of other and important nerve-tissues as makes the disorder of audition and equilibration comparatively unimportant.
7 Burnett.
Vertigo from coarse organic lesion of brain, such as a tumor, is common, and is, indeed, rarely absent in such cases. The cases in which it is lacking or least remarkable are, I think, to be found in the anterior and middle cerebral lobes, while it is almost sure to exist at some time when the tumor is in or near the cerebellum.
Growths or other causes of irritation in the crura of the cerebrum or cerebellum, or on the pons, are sure to give rise to disturbed equipoise or to methodical involuntary actions; but these are not always, though often, accompanied with delusive impressions as to exterior objects, or with the other symptoms found in typical vertigo. I recall one remarkable case where a blow on the left side of the occiput resulted in a tendency to roll to the left which finally triumphed over volitional control, so that the patient would at times roll over on the floor until arrested by a wall. After the rotation had lasted for a minute there was, when it ceased, a false sense of movement of objects to the left, but at the outset there were no sensory illusions, and at no time any mental disorder. The patient recovered, and is now in good health; but it is interesting to learn that while, during the time of these attacks, he had normal hearing, he has gradually lost hearing in the left ear and acquired permanent [p. 424] tinnitus. I have reached the conclusion that there is a group of functional vertigoes, and that in some of them the trouble lies in the semicircular canals; that is to say, the lesion is slight or transient, but in rare cases recurs until a more distinct and permanent result justifies the original diagnosis.
OCULAR CAUSES OF VERTIGO.—For the most part, the eyes as a source of vertiginous impressions are neglected in the textbooks; but as the cause of certain of the slighter vertigoes, and as a fertile agent in emphasizing or recalling vertigoes due to the stomach or inner ear, they are well worthy of careful study, nor is it ever wise to neglect these organs in cases either of headache or of vertigo.
A number of eye conditions cause giddiness or increase it or reproduce it. Thus, sudden loss of accommodation in one eye or in both may occasion it, and perhaps the enlarged pupil may have its share, since even in healthy people, and surely in all habitually vertiginous patients, sudden exposure to brilliant light gives rise to sense of instability.
Abrupt change in intraocular pressure is another cause, as in acute glaucoma or in sudden partial collapse of the eye from discharge of the aqueous humor.
Permanent vertigo of quite severe character may arise from astigmatic defects, and from almost any form of disorder affecting steadily the power of the eye to accommodate itself to distances; but simple myopia of moderate grades, excessive one-sided myopia, or presbyopia is unlikely to do so. Oculo-motor troubles, paralytic or spastic, are very effective causes of vertigo, which is sometimes quite promptly producible by the wearing of a prism on one eye or by the use of glasses which over-correct, or if exact are for some reason badly borne. This latter is apt to be the case, I think, in accurate corrections of long-standing hypermetropic astigmatisms. There is one point on which, in this connection, I have again and again insisted: Optically defective eyes may exist through life without notable brain disturbance, unless, from over-use with worry, work under pressure, the strain of prolonged or of brief and intense emotion, or any cause of ill-health, the centres become sensitive, as they are then apt to do. When this occurs defective eyes, and in fact many other sources of irritation, grow at once into competence for mischief, and occasion vertigo or headache or other cerebral disorders.
Then it is that even slight defects of the eye may cause vertigo, which if usually slight and transient, coming and going as the eyes are used or rested, is sometimes severe and incapacitating. I have over and over seen vertigo with or without occipital pain or distress in persons whose eyes were supposed to be sufficiently corrected with glasses, but who found instant relief when a more exact correction was made; and this is, I think, a matter which has not yet generally received from oculists the attention it demands.
When vertigo, essential, gastric, or aural, is present, the use of the normal eye becomes a common source of trouble. Bright lights, things in irregular motion, reading or writing, and especially rapid changes in accommodation, as watching the retreat or approach of a moving object, are prone to cause or increase the dizziness.
Vertigo in old age, if not due to the stomach or defective states of the portal system, kidneys, or heart, is either caused by atheromatous vessels [p. 425] or multiple minute aneurismal dilatations of vessels, or in full-blooded people by some excess of blood or some quality of blood which is readily changed by an alteration in the diet, of which I shall presently speak. Whatever be its source, it is in the old a matter of reasonable anxiety.
Laryngeal Vertigo.—Under this name J. R. Gasquet,8 and later M. Charcot, have described a form of vertiginous attack in which irritation of the larynx and a spasmodic cough invariably precede the onset. I have never seen such cases, nor do they seem to me entitled to be called vertigo. The symptoms are these: After bronchitis, gout, or rheumatism there occurs an irritation of the larynx or trachea, or of both, which at times is expressed in the form of a tickling cough, simple or in spasms. With these arises a slight sense of vertigo, or else in the grave attacks the patient falls insensible, without convulsion or with no more than one may see at times in fainting. The face is flushed, even deeply, and the attacks last but a few moments. The term vertigo seems to have in such a group of symptoms but little application, nor do these attacks ever bring upon the sufferer the status vertiginosus.
8 Practitioner, Aug., 1878.
Vertigo in Anæmia and in Neurasthenia and Hysteria.—A passing vertigo readily caused by abrupt changes of posture, felt even in health, at times is far more profoundly experienced in grave anæmic states, while in neurasthenic conditions, with deficiency of globules or defect of hæmaglobin, it is still more common. In well-pronounced neurasthenic states, where there is no measurable lack of red corpuscles, but where hæmaglobin is apt to be deficient, it is a frequent symptom, and is then either an immediate result of functional central disorder or of gastric or optical troubles. While the dizziness of neurasthenia is never profound, certainly never repeats the agony of Menière's vertigo, it is apt to be but a too constant symptom, and to be, like the other disqualifying cerebral symptoms of neurasthenia, almost the last to get well. Usually there is little, often no, tinnitus, no deafness, no nausea, slight but a pretty constant sense of unsteadiness, and rarely or but for a few moments any false subjective visual illusions. This, at least, is the type, but, on the other hand, in extreme cases and within these limits the brain is liable to be confused, and the sense of need for difficult controlling volitions called out by almost any use of the eyes in near vision, owing usually to oculo-muscular paresis. Even looking at a mirror or at persons passing by, or the least distinct mental effort, may reproduce it. There is, too, in most of these cases an extreme sense of mental confusion, and more often a false sense of movement within the head than without, while in no other patients is the sexual act so apt to increase all of the symptoms in question.
Hysteria, as might be expected, offers now and then examples of vertigo. It does not exclude the presence of true aural, optic, or gastric dizziness, which is then apt to become the starting-point of a long train of hysterical disorders. On the other hand, we meet with hysterical vertigoes which, in a sense, may be said to simulate any of the more usual types. I have certainly seen hysterical girls with deafness, tinnitus, and a great development of equilibrial disturbance, in whom the disease passed away without leaving a trace behind it, so that in these cases some caution is needed as to prognosis. They become far more difficult to deal [p. 426] with when they are found in old women or women in advanced middle life, since it is then hard to know what share senile changes may have in the production of the symptoms.
Vertigo from mechanical causes, such as sea-sickness, railway sickness, swinging, etc., it is hardly worth while to deal with here at length. The research of Prof. James has made it probable that disturbances of the labyrinth are responsible for the vertigo of sea-sickness. Certainly, deaf-mutes seem to have lost the power to be made vertiginous from rotation, and do not suffer at sea.
It is, however, worth recording here that I have more than once seen enduring vertiginous status, with occasional grave fits of vertigo, arise out of very prolonged sea-sickness. In the last example of this sequence seen by me there was, after a year or more, some deafness.
The elevators in use in our hotels sometimes cause, in those who live in them all day and control their movements, a cumulative vertigo, and I have known such persons to be forced on this account to seek other occupation.
Essential Vertigo.9—There can, I think, be no doubt that the centres may evolve the symptom vertigo from causes which are transient, and the nature of which sometimes evades our most careful search. We reach the diagnosis of a state of essential or true central vertigo by exclusion, but, once developed, this vertigo does not greatly differ from vertigo of peripheral cause. It is sometimes associated with states of pallor, at others with flushing, while the disturbance of balance and the false perceptions as to the place of outside objects may vary from the least to the most profound disturbance. In some of these examples the nausea or emesis does not appear at all, and the patient, escaping acute attacks altogether, may with occasional aggravation continue to be merely and almost constantly vertiginous.
9 Ramskill and others.
The TREATMENT of acute attacks of vertigo, however caused, consists, of course, in rest in bed and in the use of large doses of bromides or hydrobromic acid, and if the trouble be grave in that of hypodermatic injection of morphia, and where there is plainly pallor of face in inhalations of amyl nitrite or in the exhibition internally of nitro-glycerin and alcoholic stimulants. Sometimes to lie on the floor in total darkness is helpful when the disorder continues and is severe. I have known patients liable to be attacked suddenly to carry a little flask of brandy, and to find that very often an ounce of brandy, taken at the first sign of trouble, would enable them, by also lying down, to break the attack; and ether is yet more efficient. After the severer sense of vertigo has gone they find that stimulus is comforting, and for a time at least gives strength. I have used amyl nitrite but twice. In each case it is said to have broken the attack, but I have had no larger experience with it.
Gastric vertigo demands, in the acute attacks, a treatment directed to the cause. Antacids may be valuable, or in arrested digestion emetics, but in all cases these should be followed for some weeks by moderate doses of bromides, while gouty or lithæmic states should be treated by the usual means.
Vertigoes from portal disturbances are best treated by aperients, and a like lessening of animal food, which, in the vertigo of old age or middle [p. 427] life arising from excess of blood, will also be found available. The change of cerebral states of passive congestion, which can be brought about by a pure vegetable or milk-and-vegetable diet is sometimes quite remarkable; and I know of few things in therapeutics which are more satisfactory.
The treatment of anæmic or neurasthenic vertigo involves nothing peculiar. So long as the want of blood lasts, or some one of the several groups of symptoms loosely classed as neurasthenia exists, so long will the associated vertigo endure.
Aural vertigoes are easy or difficult to treat, as they arise from external or middle and internal ear troubles. Irritations in the external ear are of course to be removed, and catarrh of the middle ear to be treated by attention to its conditions, whether of blocking of the Eustachian canals with depression of the membrana tympani or of accumulations in the middle ear, with the opposite state of fulness. Aural vertigo, as has been pointed out, may arise from disorders of any part of the ear, so that it is needful to look for wax, ulcers, foreign bodies, etc. in the external meatus; for catarrhal states, closure of the tubes of Eustachius, states of fulness or of vacuum in the middle ear; and for inflammatory conditions, direct or transmitted, in the inner ear. Very often vertigoes from irritations of the outer or middle ear may be relieved with more or less ease, but labyrinthine vertigo, however acquired, is always troublesome, often lasting, and if grave gets well only when deafness has become great.
In this form of vertigo, and while acute, morphia is very serviceable, and is to be used with full doses of bromides. When, as happens, both cease to be of value, Charcot's plan of the heroic use of quinia salts I have seen do good; but it is advisable to use with it hydrobromic acid in full doses. It has been constantly my practice to employ over the mastoid or on the neck frequent but not deep cauterization. It is well in these cases to warn some near relative that while remote relief from the vertigo is probable, it will be bought at the cost of increasing deafness, and that we can rarely do more than help the patient to endure his state until time and the slow processes of pathological change have come to our aid.
Optic vertigo, if essentially that, is rarely discovered without the help of some one trained to study the defects of vision. Its relief demands, of course, as a rule, glasses, or in extra-optical muscle-troubles these or a compensatory operation. When, however, the vertigo has been grave, it is needful to manage corrections of the eyes with care and judgment, and sometimes experimentally. The sensorium, having become over-excitable, does not always bear accurate correction of the eyes, or this increases the vertigo. Then the glasses are cast aside and the case progresses. In others—and this is purely a matter of individual experimentation—nothing will answer except the most careful and absolute corrections: anything less does no good.
These remarks apply with equal force in chronic vertigoes, essential, gastric, or other. Defective eyes, unfelt in health, soon begin to trouble a head sensitized by chronic dizziness, and optical defects which are sometimes but trifling become then competent to increase the growing intracranial disorders, or to assist lithæmia or a troublesome stomach to create and sustain vertigo.
[p. 428]The Status Vertiginosus.—I have tried to make clear elsewhere and in this article that in several forms of vertigo the disorder ceases to owe its onsets to extracentral irritations, and becomes essential, precisely as happens in some epilepsies, and that we then are apt to have, with more or less distinct attacks or with no attacks, long continuance of a group of symptoms which constitute the status vertiginosus. Its treatment is important, because of its alarming and disqualifying effects. The attacks are often the least part of it, while the lack of power to read and write, to go into crowded streets, to face light, or to exercise, or stand emotions or the slightest mental strain, surround its management with embarrassments, and are well fitted to end in melancholia or hypochondriasis.
In these cases, after the eye has been corrected, the diet should be regulated with care. In extreme cases it may become desirable to limit it to milk, fruit, and vegetables where no obvious peculiarities forbid such a regimen; and I have found it useful to insist also on some food being used between meals.
I like, also, that these patients rest an hour supine after each meal, and spend much time out of doors, disregarding their tendency to lie down. Exercise ought to be taken systematically, and if the vertigo still forbids it, massage is a good substitute. At first near use of the eyes is to be avoided, and when the patient resumes their use he should do this also by system, adding a minute each day until attainment of the limit of easy use enjoins a pause at that amount of reading for a time.
Now, as in vertigo, especially labyrinthine, the eyes become doubly valuable as guiding helps to correct equilibration, I have long found it useful to train these patients to stand and walk with them closed. At first this is as difficult, or may be as difficult, as in locomotor ataxia, but the practice is sure to add steadiness to the postures. Somewhat later I ask my patient deliberately to make such movements of the head and such efforts of mind or memory as are apt to cause vertigo or confusion of head, and to conquer or inhibit these consequences by a prearranged effort of will; and these means also I have found useful. Meanwhile, nothing usually in these cases forbids the use of tonics or of moderate doses of bromides. As I have said, change of air is very serviceable. It is indeed rare that cases do not yield to some such combination of means, but very often it will happen that the fears of the patient are his most grievous foes, and are to be dealt with after every real symptom has vanished.
Tremor is a prominent symptom of many diseases of the nervous system, and is met with as an effect of certain poisons which have been taken into the system; so it should not be considered as a disease in itself. It may, however, occur without being associated with any other abnormal condition which can be discovered. It is then called tremor simplex or tremor essentialis. The tremor of old age (tremor senilis) comes under this head.
Tremor is sometimes hereditary, and may exist from early life. I have a patient in whom there is a trembling of the hands which has lasted since childhood. This lady's mother and grandmother both had the same form of tremor, and one of her own daughters also has it. In this case the trembling is most marked when voluntary movements are attempted, but it does not materially interfere with writing, sewing, or any other act she wishes to accomplish. There is slight tremor when the hands are at rest.
Tremor simplex is seen in hysteria. In this disease it affects the hands and the facial muscles as well. It is not uncommon in these cases to find the tongue tremble excessively when protruded.
Tremor from chronic poisoning is usually from the absorption of lead, mercury, or some of the narcotic drugs or alcohol. Lead tremor is to be looked for among persons who are exposed to the action of lead, such as painters, printers, or manufacturers of white lead.1 Such persons generally have had some other symptom of lead-poisoning, such as colic or paralysis. The tremor, however, may be the only symptom of saturnine poisoning. Mercurial tremor is not so often seen. It occurs in looking-glass makers or those who work in quicksilver, and may also be a result of the medicinal administration of mercury. The tremor from the excessive use of alcohol or opium is familiar to all. Tobacco, if used immoderately, also causes trembling in the hands. Tea or coffee may have the same effect. There are other drugs which, when taken for a length of time, are liable to cause tremor. Quinine is one of these.
1 Lead in hair dyes or in cosmetic powders often gives rise to plumbism by its absorption by the skin.
Exhausting diseases, like the fevers, or any conditions which enfeeble the system, cause tremor which occurs in voluntary effect. I saw a lady some years ago who was greatly weakened by a malignant growth. She was extremely anxious to sign her name to a legal paper, but, although the hand was perfectly quiet when at rest, when she attempted to write [p. 430] the first letter such intense tremor came on that it was impossible for her to make any mark which was legible.
Tremor follows violent bodily exertion or mental excitement. The action of cold or the chill of intermittent fever is accompanied with an extreme degree of trembling, which we all know. Tremor is also a result of neuritis, but in this case it is associated with other symptoms.
SYMPTOMS.—Tremor is met with as a fine or a coarse trembling. We may also find a fibrillar tremor, such as exists in progressive muscular atrophy. Tremor is divided by some (Van Swieten, Charcot, and others) into two classes: the first is where the tremor occurs while the part is at rest; the second is where it comes on during volitional muscular movements. The former has been termed by Van Swieten tremor coactus, because he believed that it arose from an irritation which affected the nervous centres in an intermittent way. The latter he conceived to depend upon a defect of stimulus, the result of an insufficient amount of nervous fluid, which causes contraction of the muscles under the influence of the will. This he called tremor a debilitate.2
2 Charcot, Lectures on Diseases of the Nervous System.
In paralysis agitans we have an example of tremor coactus, and in disseminated sclerosis, where the tremor occurs only as muscular effect, it belongs to the variety of tremor a debilitate. Those divisions, however, are of but little importance.
When tremor first begins it is slight in degree and extent, and occurs generally only on voluntary effort. Later there may be a constant trembling even when the part is at rest. Beginning usually in the hands, it may extend to the head and legs. It is seen in the tongue and facial muscles after the disease has lasted for some time.
In some cases the trembling can be controlled to some extent by a strong effort of will. The tremor from alcohol or opium is most marked when the individual has been without the use of the stimulant for a short time, and the trembling may be temporarily checked by renewing the dose of alcohol or opium as the case may be.
The muscular trembling from plumbism and mercurial poisoning is more violent than the other forms of simple tremor, and often resembles the tremor of paralysis agitans. In toxic tremors there are often secondary paretic symptoms and indications of other disturbances of the brain and nervous system.
In simple tremor there is no loss of muscular power, and the electrical reactions of the affected muscles are not abnormal. The duration of simple tremor is almost always great. Usually it persists throughout life, becoming more general and more intense as the subject of it grows older. The tremor of hysteria is shorter in duration. Occasionally there are seen cases of simple tremor, which are apparently the result of some trivial cause in a nervous person, which last but a short time.
I have seen a case of tremor of the head in a woman of about forty years, in which the trembling ceased entirely after it had lasted several weeks. Hammond3 describes what he calls convulsive tremor. Under this name he includes cases of non-rhythmical tremor or clonic convulsions, which are unaccompanied by loss of consciousness, but are paroxysmal in character. Pritchard in 1822 presented an account of this affection and [p. 431] related two cases; Hammond mentions six cases. The affection is characterized by paroxysms of violent and rapid convulsive movements, which are more or less general and occur many times a day. The seizures last from a few minutes to several hours.
3 Diseases of the Nervous System, p. 696.
The PROGNOSIS in convulsive tremor seems to be favorable.
Tremor may be regarded as a form of clonic spasm. It consists of slight intermittent contractions of individual muscles or groups of muscles. Fibrillar tremor, such as is seen in progressive muscular atrophy, depends on contractions and relaxations of the muscular fibrillæ, and can be seen under the skin, but does not cause any movements of the limb.
There are no pathological data for explaining what portions of the nervous system are the seat of disease in simple tremor. In experiments upon the lower animals it has been found that trembling occurs in muscles which have been separated from the nerve-centres by division of the nerve. So too in man: when there has been a wound or section of a nerve accidentally, there is likely to be tremor in the muscles which it supplies.
The tremor does not begin at once on section of the nerve, but comes on after a few days. As the peripheral end of the nerve undergoes degeneration the tremor increases. It may last months or even years.
In some of the conditions where tremor occurs the influence of the will is weakened or is entirely absent. This is seen in hysterical trembling and in the tremor of old age as well as in those cases where there is general enfeeblement of the body, as in the fevers.
Trembling is connected with disease of the pyramidal tracts, because in this way the influence of the cerebral centres is withheld from the muscles. When a muscle is in a condition of tonic spasm, it is the result of the running together of very rapidly-repeated muscular contractions. It is like the contraction in a muscle from an interrupted electrical current. If the interruptions are slow, the muscular contractions are seen at intervals like a tremor; but if the interruptions are rapid from frequent vibrations of the hammer of the instrument, then the contractions in the muscle are fused together, as it were, and the muscle is in a state of tonic spasm.
It is held by some writers that tremor is caused by the want of balance between the cerebrum and cerebellum. When, for example, the control of the cerebrum is enfeebled the action of the cerebellum is so great as to bring about tremor by its uncontrolled power.
If we accept the first view, we must consider the tremor as a preliminary stage of paralysis; for the lesion, which at first is slight and causes only an interruption of the conduction of impulses from the brain to the muscles, as it becomes more extensive totally prevents conduction, and paralysis ensues.
Hughlings-Jackson's view, that general convulsions are the result of discharges from the cortex of the brain, and that the tonic contractions of tetanus are caused by discharges from the cortex of the cerebellum, may be applied to the pathology of tremor as well. When, for instance, in a disease like disseminated sclerosis a voluntary effort instead of causing a steady muscular contraction results in irregular spasmodic contractions and relaxations of the muscle, we may imagine that a series of discharges were taking place from the cortex of the cerebellum as long as the voluntary efforts were persisted in. On the other hand, in paralysis agitans [p. 432] it is more probable that a lack of conducting power in the pyramidal tracts prevents the influence of the centres being continuously exerted upon the muscles through their motor nerves.
It is probable that in simple tremor the lesion is situated in the spinal cord; for in this disease we seldom see any evidences of cerebral disturbance. There are no paralytic or psychical symptoms, and no vertigo. In toxic tremors the disease is no doubt located in the brain, for accompanying the trembling resulting from alcohol, opium, mercury, and other drugs are mental changes and more or less muscular enfeeblement.
TREATMENT.—Should the tremor depend upon some cause which can be discovered, of course the obvious course is to attempt to remove the source of trouble. The effort is of greater or less success in different conditions. The tremor from mercurial poisoning sometimes yields to treatment which is directed to the elimination of the mercury. The free administration of the iodide of potassium is the best means to be used, and is often successful. The same means are available in lead tremor. Of course the patient must be removed during treatment from the risk of further absorption of the poisonous substances.
In simple tremor many remedies have been recommended, but the results of treatment are not encouraging. Baths of various kinds and galvanism have been used, and many drugs are advised. Hyoscyamus and its alkaloid, hyoscyamine, have enjoyed a high reputation, and good results have been reported from their use. I have seen relief, but not cure, from their administration. Arsenic is a more reliable remedy and it may be used hypodermically. Eulenburg4 has used this method with good results. I have given arsenic per orem with beneficial effects in cases of simple tremor. In a case to which I have referred above the tremor was relieved while the patient was taking Fowler's solution, and on changing to hyoscyamus the trembling got worse. On returning to the arsenic the symptoms improved, and finally the tremor ceased after the remedy had been taken for some weeks. Hysterical tremor requires that the hysteria should be relieved. Franklinic electricity sometimes controls the tremor in these cases.
4 Ziemssen's Cyclopædia, vol. xiv. p. 392.
SYNONYMS.—Parkinson's disease; Shaking palsy; Trembling palsy; Senile chorea; Chorea festinans. The first name is due to the fact that the disease was first fully described by Parkinson in a book published in England in 1817.
Paralysis agitans is a neurosis, chronic in its forms and characterized by a tremor which gradually increases in extent and severity. The tremor is not increased by voluntary muscular movements. A peculiar manner of walking, known as festination, comes on later in the disease, and there are also alterations in the attitude of the head and trunk.
It is a disease which belongs to middle age, being rarely seen before forty years, although cases are quoted by Charcot as early as twelve and sixteen years. Constant and prolonged exposure to dampness and cold seems to bring on the disease, and it is sometimes caused by sudden emotion, like fear or distress. The following case is an instance of the latter:
Case I.—Mr. A. M——, æt. fifty-two years, consulted me Oct. 1, 1883. He is a bookbinder by occupation. His habits have been good. He had a chancre in 1861, but had no secondary troubles. He was in the army from 1861 until 1866. In 1866 he went into business for himself, and, although his business was large, he had no great anxiety or worry. His general health has been good, and he has had no illness except an attack of malarial fever about six years ago. In May, 1883, he was standing by an elevator door on the fourth floor of his place of business, and, seeing that the elevator was caught by something, released it. It immediately fell with a crash to the second floor, and as there were two or three persons on it, Mr. M—— thought they must have been killed or severely injured. He was greatly excited and alarmed, and soon after he had assured himself that none of the occupants of the elevator had been hurt, discovered a trembling of the right hand. The tremor has continued ever since, and has extended to the arm and leg.
On examination there is seen a coarse tremor of the right arm and leg while the limbs are at rest. A voluntary muscular movement stops the tremor, and it also ceases during sleep. When he makes an effort with the right hand, as, for instance, in squeezing the dynamometer, the tremor ceases in the arm, but becomes greatly exaggerated in the right leg. While occupied in doing anything he does not notice the tremor, and it stops when he is lying down.
The dynamometer shows, right hand 150°, left hand 120°. After two years have elapsed the disease has gradually progressed in severity.
[p. 434]SYMPTOMS.—The course of the disease has been divided into three stages—the period of invasion, the stationary period, and the terminal period.1
1 Lectures on Diseases of the Nervous System, by J. M. Charcot.
Period of Invasion.—There are several modes of invasion, but the most frequent by far is slow in its onset. The disease comes on gradually, first showing itself as a slight tremor in the hand or fingers while the part is at rest. It is not constant, and ceases as soon as the patient's attention is called to it. There is sometimes preceding the tremor rheumatic or muscular pain in the affected arm. The tremor may first occur in the foot. Should the disease begin in the hand—and this is most common—the movements are peculiar. They may consist of a fine rhythmical tremor, or the fingers move in a methodical way over each other. Charcot speaks of the thumb and forefinger being rubbed together as if the patient were spinning wool. While this movement of the thumb and finger is going on the wrist is being flexed by jerks. During the early stages of the disease the tremor is observed only at intervals. It comes on intermittently when the patient is not thinking of it and while the limb is at rest, and ceases as soon as any voluntary muscular effort is attempted. The act of grasping the hand or taking up an object is enough to check it for the time. In a patient now under my care I have often noticed during the early stages a well-marked tremor of the right hand while it was lying in her lap, but it would at once cease when I called attention to it. As soon as the mind of the patient was diverted to some other subject the tremor would begin again.
As the disease progresses voluntary effort no longer controls the tremor, or if it does at all it is only for a few seconds, when it begins again. As the tremor increases in violence it extends to other parts of the body. At first it may have been confined to the hand; now it extends to the arm, a little later to the foot and leg on the same side. Then the other arm will be affected, and finally all of the limbs will succumb to the tremor.
Charcot speaks of decussated invasion—that is, the disease begins in the right upper extremity, for example, and next passes to the left lower extremity. This is a rare form; it is much more frequent to see the hemiplegic type, which may persist for some time, or the paraplegic type, when both legs are affected.
There is a progressive form of invasion when the tremor is not the first symptom. The patient has neuralgic or rheumatic pains in the limbs, which are afterward affected with tremor. Sometimes there is some mechanical injury of the limb, which subsequently is the seat of pain and tremor. The general health of the patient is at the same time more or less impaired. There is a sense of general weakness and lassitude; the temper is irritable, and there may be some vertigo. The features and countenance are characteristic even at the earliest periods of the disease. There is an absolute absence of expression, and the features are fixed. The face looks like a mask, and although the patient may smile or laugh, immediately after the features return to the original blank expression. Amidon showed two cases of paralysis agitans to the American Neurological Society in 1883, in which there was no tremor whatever, but all the other features of the disease were present.
[p. 435]After a great mental or moral shock the trembling begins suddenly, abrupt invasion, as in Case I., or the case described by Charcot, where the wife of a gendarme, seeing her husband's horse return riderless to the barracks, received a shock of great severity, which was followed on the same day by tremor. The tremor is at first confined to one limb. It may even disappear for a time, but gradually and slowly extends to the other limbs, and takes the same progressive course.
Period of Stationary Intensity.—After the disease has become fully developed the tremor is incessant. The intensity is not the same all the time. It may be augmented by cold, over-excitement, or voluntary effort, and is lessened by repose and sleep. The trembling ceases during anæsthesia.
During this time all the characteristic movements are at their height. The moving of the thumb and finger, already referred to, is present, and seems like a partly co-ordinated movement. Charcot describes these movements as being in some cases like the rolling of a pencil or a paper ball between the thumb and finger, and in others the movements, he says, are more complicated, and are like what occur in crumbling a piece of bread.
The handwriting is almost illegible, and every letter shows the excessive trembling of the hand, most marked in the up strokes of the pen. All this time the head and neck are unaffected. There is no nodding or shaking of the head to be observed on the closest inspection. This is an important fact to bear in mind, for it is a distinguishing feature between the disease under consideration and disseminated sclerosis. There is no nystagmus, and the muscles of the jaw are unaffected by tremor. The tongue, however, while lying on the floor of the mouth undergoes tremor, and this is increased when the organ is protruded.
The speech is slow and jerky, and the patient usually speaks in a low tone of voice. He eats his food without difficulty, but in advanced cases the saliva sometimes escapes from the mouth during deglutition. A characteristic symptom of the disease is a rigidity of the muscles of the extremities, trunk, and of the neck. When the muscular stiffness first begins the patient complains of cramps followed by a sense of rigidity. The flexor muscles are first affected. This stiffness causes peculiarities in the patient's attitudes. The head and neck are usually bent forward, and seem fixed in that position. The body is inclined slightly forward in standing. The elbows are held somewhat away from the chest, the forearms are flexed on the arms, and the hands are flexed on the forearms. The thumb and forefinger are extended and brought together as if holding a pencil. The other fingers are also flexed. The attitude of the hand and the prominence of the knuckles make it closely resemble the hand of rheumatoid arthritis. In paralysis agitans, however, there are no bony deposits in the joints, and no cracking is heard on bending the knuckles.
In the lower extremities there is often intense rigidity. Contractions occur, and the legs are strongly flexed. The feet often are extended in the position of equinus. It is this rigidity which causes the difficulty in walking (Charcot).
The gait of the patient now becomes very striking. He gets up from his seat slowly and with difficulty; hesitates a moment before starting to [p. 436] walk; then, once having made a few steps, goes at a rapid pace. The tendency is to fall forward; in order to preserve his equilibrium the patient hurries forward as if to catch up with his centre of gravity. This gait has been called paralysis festinans—festination or propulsion.
Although propulsion is the usual form the gait assumes, sometimes there is a tendency to fall or run backward. This tendency is not always apparent even when it exists. Charcot has a method of showing its existence which is very successful: when a patient is standing he pulls her slightly backward by the skirt, and this is sufficient to start a movement of retropulsion.
Propulsion and retropulsion are not necessarily always present. Many cases progress to the end without these symptoms.
As the disease advances the muscles become more rigid and the patient is confined to bed. He is, however, restless from a sense of prostration and fatigue. He is unable to turn himself, and often calls to his attendant to change his position. The sufferers from this disease, although not having actual pain, complain of disagreeable sensations. There is a constant sense of excessive heat whether the temperature of the room be high or low. In winter they cannot bear much bed-clothes at night, and prefer to wear very light clothing. Associated with this sensation of heat is often profuse perspiration (Charcot). Notwithstanding all these troublesome sensations the sensibility of the skin is not changed. Heat and cold are readily felt, and there is no anæsthesia or analgesia.
Terminal Period.—The duration of paralysis agitans is generally great. The disease may extend over many years—even as long as thirty years in some cases. As the tremors and rigidity increase in intensity the patient becomes obliged to sit all day in a chair or is confined to bed. Occasionally the tremor becomes less while the rigidity increases. The nutrition suffers, and the muscles especially become greatly wasted. Up to a certain point the intellect remains unaffected, but late in the disease the mind fails. General prostration of the whole system sets in, bed-sores occur, the urine and feces are passed unconsciously, and the patient dies of exhaustion. It is not often that the end comes in this way. It is much more frequent that some intercurrent disease, like pneumonia, ends the life of the patient. The disease is undoubtedly a most painful and trying one to both patient and physician. It lasts for years, and there is no prospect of relief. Charcot says that he has seen the terminal period last for three or four years. The following case is a fair example of the disease:
Case II.—Margaret Hays, aged fifty-four, single, applied for treatment at the Infirmary for Nervous Diseases, Oct. 9, 1882. She is housekeeper for her brother, who keeps a restaurant. She has had to be up late at night, and has had very much washing to do for many years. The kitchen in which she is most of the time is damp, and opens into a yard into which she has often to go. About two years ago she thought that she hurt herself in lifting something, and soon after this, on putting her hands from hot into cold water, suddenly felt a numbness in both forearms. One year ago she noticed tremor in both hands and both legs. The tremor interfered with her work, and has increased. She also felt as if there were loss of power.
Present Condition.—The face is expressionless and looks as if it were [p. 437] a mask. She articulates without using her lips to any extent, and speaks in a low tone, scanning the syllables. The head is held stiffly, and the attitude of the whole body is peculiar.
The tremor is fine, and is constant while the hands are at rest. On voluntary effort the tremor ceases. On examination with the dynamometer, right hand 95°, left hand 80°. She feels weak generally, and says she cannot use her hands even to button her clothes or to dress or undress without aid. She performs all movements slowly and with great deliberation. The patellar reflex is not excessive.
Sensation.—She has lost the sense of numbness she used to have, but says she cannot feel a needle between the fingers when she attempts to sew. There is loss of sensation in the finger-ends; the compass points are not felt at less than three lines.
Her walk is slow and deliberate like all her movements, and there is no festination. Her eyes were examined, and there was no decided change in the fundus and vision was about normal. Pupillary reflexes good.
This patient was under observation for several months, and steadily grew worse. One peculiar feature was observed, however: it was that at one time the tremor almost ceased, although all of the other symptoms were worse.
ETIOLOGY.—As already mentioned, the causes which have been observed are fright or sudden grief and prolonged exposure to cold and dampness. A number of cases of the former are mentioned by Charcot, and a case which I have related above is a good illustration of paralysis agitans produced by fright. When caused in this way the disease does not present any peculiar features in its progress or termination. I have seen many cases in which the disease had been preceded by more or less exposure to dampness. One of my patients had worked in a basement room which was damp; another (Case II.) was a great deal of the time in a kitchen which opened on a wet yard, and she was constantly going in and out of doors, getting her feet wet frequently. Sometimes irritation of a peripheral nerve seems to have been the origin of the trouble. Charcot quotes several cases of this kind.
Sex does not appear to exert any special influence in the production of the disease. Some writers assert that it is more common in males than in females, but Charcot in his large experience at La Salpêtrière has not found this to be the case.
MORBID ANATOMY.—A number of autopsies have been made in cases of paralysis agitans without any constant lesion of the nervous system having been discovered. Charcot refers to three cases in which he made careful post-mortem examinations in which the results were negative. Parkinson and Oppolzer each report one case in which was found induration of the pons, medulla, and cervical portion of the cord. More recently, however, Charcot and Joffroy have examined cases in which microscopic examination revealed blocking up of the central canal of the cord by increase of the epithelium of the ependyma and pigmentations of the ganglion-cells.
Leyden has reported a case in which the disease was confined to the right arm, and on post-mortem examination a tumor of the left optic thalamus was found.2
2 Quoted by Hamilton, Diseases of the Nervous System, p. 500.[p. 438]
Dowse and Kesteven found degeneration of the nerve-cells of the anterior pyramids, changes in the olivary body, nucleus of the ninth nerve, laminæ and corpus dentatum of the cerebellum and of the anterior cornua of the spinal cord. Also cortical sclerosis of the right lateral column of the cord and miliary changes in the white matter of the corpus striatum and hemispheres.3
3 Ross, Diseases of the Nervous System, vol. ii. p. 797.
In this disease, as in chorea, there must be two classes of cases—those in which there is no lesion to be discovered after death, and others in which there are changes throughout the brain and spinal cord more or less widespread. The cases in which the disease comes on suddenly from some moral shock probably belong to the former class; while in cases which have come on gradually during senility one would expect to find organic changes in the nervous system. Ross4 suggests that the cause of the tremor is probably a diminution in the conductivity of the fibres of the pyramidal tract, which prevents impulses from the cortex reaching the muscles in sufficiently close proximity to produce a continuous contraction. This, however, does not explain the cause of the tremor in the cases where it began suddenly from fright.
4 Op. cit., p. 798.
DIAGNOSIS.—The only diseases with which paralysis agitans may be confounded are disseminated sclerosis, senile tremor, and chorea in the aged. From senile tremor it may be distinguished from the fact that it begins before old age—that the tremor is more excessive and the gait and facial expression are distinctive. Chorea in old persons resembles paralysis agitans, but is not progressive, the tremor is not lessened as a rule by voluntary effort, and the peculiar gait and expression of the face are wanting.
There are many points of difference between paralysis agitans and disseminated sclerosis, as can be seen below:
| PARALYSIS AGITANS. | DISSEMINATED SCLEROSIS. |
| Tremor ceases on voluntary effort, or is not increased by it. | Tremor induced by muscular effort, and ceases during repose. |
| Tremor regular and fine. | Coarse tremor, becoming more so during voluntary effort. |
| Face expressionless; tremor of face rare. | Facial muscles affected; nystagmus frequent. |
| No tremor of head. | Tremor of head generally present. |
| Belongs to advanced age. | Usually comes on before middle age. |
| Propulsion (festination) and retrogression. | Staggering walk. |
TREATMENT.—The results of treatment are not encouraging. Cases have been reported in which cures were effected, but it is doubtful if they were true instances of paralysis agitans. Hyoscyamus and conium have been given with temporary relief to the tremor. Trousseau recommends strychnia, but Charcot declares that it aggravated the cases in which he gave it. Hammond advises the use of galvanism, at the same time giving strychnia or phosphorus. I have seen one case in which decided relief was obtained from arsenic hypodermically, and another in which the patient was benefited for a long time while taking small doses of strychnia combined with iron and quinine, and at the same time static electricity was applied.
Chorea, or St. Vitus's dance, has been known for years, and the literature of the subject, especially among the older writers, is as extensive as that of any other disease.
It has been recognized by a variety of names, some of the most common being derived from some saint who enjoyed a popular reputation of power to cure the disease. For example, it has been called St. John's dance, St. Guy's dance, St. Modestus's dance, and St. Anthony's dance. Besides these names it has been termed ballismus, paralysis vacillans, epilepsia saltatoria, and orchestromania.
It will be observed that almost all of the names which have been applied to the disease relate to a dancing movement. This arises from the fact that the first notice of the affection dates back to the fourteenth century, when a kind of religious mania appeared in Southern Europe in the form of an epidemic. It was characterized by excessive dancing and gesticulatory movements, and affected large numbers of people at a time. In 1375 an epidemic which arose was spoken of as St. John's dance, and in 1418, in another outbreak of the disorder which occurred at Strasburg, by the order of the authorities those suffering were conducted in troops to the chapel of St. Vitus in Zabern, and there masses were said and other religious ceremonies performed for its cure.
We are informed that St. Vitus removed from Sicily when a boy, at the time of Diocletian's persecution of the Christians in the year 303, and suffered martyrdom in Florence in company with Crescentia and his tutor, Modestus.1
1 “Hecker's Epidemics of the Middle Ages,” Sydenham Society's Transactions, contains full details of these outbreaks.
Von Ziemssen states that as a pandemic disease the dancing mania died out in the fifteenth century, but that traces have remained on the Rhine up to the present time.2
2 Cyclopædia of the Practice of Medicine, vol. xiv. p. 416.
In our own country there have been many epidemics of the same disorder on a small scale, and we may regard the Shakers as representing a type of the dancing mania. Weir Mitchell reports3 an outbreak which occurred quite recently In a children's asylum in Philadelphia. Prompt measures and separation of those affected from the well children checked the disorder, which at one time threatened to spread through the entire institution.
3 Lectures on Nervous Diseases, p. 69.[p. 440]
These epidemics were quite different from what we now call chorea, and the individuals suffering were clearly affected by a psychical disorder of an hysterical form. In time, however, the name has come to be applied to a systematic disease characterized by irregular spasmodic movements of the limbs and other parts of the body.
The disease has been divided by some writers into chorea magna and chorea minor. The former, however, as described, is only an aggravated variety of hysteria, and need not be considered in connection with this subject.
Although the name chorea does not correctly describe the disease under consideration, it has been used for so many years that it is more convenient to retain it.
DEFINITION.—Chorea, as we now understand it, is a spasmodic neurosis, characterized by constant involuntary and irregular jerkings and twitchings of muscles or groups of muscles, which, in the majority of cases, cease during sleep, and are accompanied by more or less psychical disturbance in most instances.
ETIOLOGY.—Hereditary influence in the production of chorea is more or less marked. In some cases the connection seems to be remote, but in many instances it will be found that one of the parents has suffered from some form of nervous disease or has inherited a nervous diathesis.
George Huntington of Pomeroy, Ohio,4 has recorded some remarkable instances of hereditary chorea. The affection, as he describes it, differs in many features from chorea as ordinarily met with, but it is apparently the same disease. It is found in the eastern end of Long Island, and has been studied in several generations by Huntington, his father, and grandfather. This part of Long Island is remarkably free from the usual type of chorea, none of these physicians having ever met with an example of it. The hereditary chorea is confined to a few families. It occurs more frequently in males than in females, and never attacks the patient until after middle life. It comes on gradually and takes years to develop, but when once established it yields to no form of treatment. In most cases there is a marked tendency to insanity and suicide in the later stages of the disease.
4 Medical and Surgical Reporter, April 13, 1872.
Some additional cases of hereditary chorea have been lately recorded by Peretti in No. 52 of the Berliner klin. Wochenschrift, 1885, and others by Clarence King in the New York Medical Journal, vol. i., 1885. The history of all these cases is strikingly like those of Huntington, and establishes without question a distinct form of chorea.
Mrs. N., one of Peretti's cases, had a mental affection with choreic movements, and there was a history of a similar condition in her parents and grandparents. Two of Mrs. N.'s four children, Mrs. A. and Anton N., had chorea in adult life; some of these became insane. Mrs. A. had five children; three of these became choreic; one had tremors and one became insane. Anton N. had ten children; of these six had chorea. In all of Peretti's cases the disease came on after the age of forty years, and persisted. In several members of the family insanity was associated with the chorea.
In the families where it occurs the nervous temperament predominates. It sometimes will be found that neither of the parents of the patient has [p. 441] had chorea or any other nervous disease, but that an uncle or an aunt has had St. Vitus's dance in childhood.
Chorea may occur at any period of life, from infancy to extreme old age. I have reported two cases in patients over eighty years of age5—one at eighty-two and the other at eighty-six—who had characteristic attacks of St. Vitus's dance. Robert Saundby has collected twelve cases of chorea in the aged. The two cases just referred to are included in the number. He considers the affection very rare in old persons.6 The following case is an example of congenital chorea, and I believe this to be very unusual. The movements of all infants are choreic, so that it is difficult to say when the chorea begins; still, it seems fair to infer that when a child has never had any but choreic movements it is a case of congenital chorea:
Case. I.—Jennie W——, aged nineteen years. Family history is good as regards nervous diseases. Her mother was frightened by seeing a case of chorea some time before the child was born. The movements were observed at birth, and have continued always. The patient was brought to my clinic at the Infirmary for Nervous Diseases, and her condition noted as follows: The movements are general and continuous; the arms and legs are in constant motion, and the mouth is perpetually grimacing; there is tremor of the tongue when it is protruded; volitional efforts increase the movements; during sleep they cease entirely; tendon reflexes are normal; there is no paralysis; heart-sounds are normal and the general health is good; menstruation is regular, and the choreic movements were not influenced in any way at the time of its first appearance.
5 Journal of Nervous and Mental Diseases, July, 1881.
6 Lancet, Nov. 24, 1884.
Chorea occurs most frequently during the period of approaching puberty. Sée in an examination of 531 cases found 453 between the ages of six and fifteen years.
I have examined the notes of 282 cases of chorea, most of which are in the case-books of the Infirmary for Nervous Diseases; the rest are from my own note-books. Of the 282 cases, 217 were between six and fifteen years. They were distributed as follows:
| Under 1 year | 2 | At 7 years | 23 | At 16 years | 6 |
| At 2 years | 6 | At 8 years | 24 | At 17 years | 10 |
| At 3 years | 4 | At 9 years | 31 | At 18 years | 5 |
| At 4 years | 7 | At 10 years | 23 | At 19 years | 5 |
| At 5 years | 9 | At 11 years | 18 | At 20 years | 1 |
| At 6 years | 24 | At 12 years | 25 | At 21 years | 3 |
| At 22, 25, 27, 28, 35, 38, 82, and 86 years, each 1 case. | |||||
Sex exerts considerable influence on the disease. Sée states that three-fourths of all the cases observed in the Children's Hospital in Paris occurred in girls. Of 328 cases which I have examined in reference to this point, 232 were females and 96 males.
Social condition has little or no effect on the production of chorea, but it is more common in cities than in the country. Indeed, everything which increases the excitability of the nervous system during development adds to the tendency to the disease.
West and Hamilton point to over-study as a cause, and I have frequently verified their observations. The annual examinations at our public schools give a number of cases of chorea.
[p. 442]A. McLane Hamilton7 has recently investigated the frequency of St. Vitus's dance among school-children in New York, and found that 20 per cent. of the children in the schools were affected with some variety of the disorder.
7 American Psychological Journal, Feb., 1876.
Rheumatism is certainly a predisposing cause, in my experience, but I have not found it associated with chorea as frequently as some authors have. In 279 cases which I examined with regard to this question, there was a clear history of rheumatism in but 37. Cardiac complications were much more frequent. In 82 cases there was a cardiac murmur heard. In some of these the murmur was no doubt anæmic, but in the majority there had probably been a rheumatic endocarditis. Many cases in which there is said by the friends of the patient to have been a previous attack of acute rheumatism, on investigation are found not to have had articular rheumatism, but merely some muscular or joint pains which were not inflammatory. Quite recently Joffroy and Saric have expressed the opinion that the pains in the joints during an attack of chorea are to be regarded as choreal arthropathies of nervous origin.
English and French writers have observed the relation between rheumatism and chorea in a large proportion of cases. Hughes and Burton Brown8 found that in 104 cases which they examined as to rheumatism and affections of the heart, there were but 15 in which some rheumatic condition had not preceded the attack or a cardiac murmur did not exist.
8 Guy's Hospital Reports, 1856.
Sée and Roget consider the causal relation between the two diseases so close as to make their connection almost a pathological law.
On the other hand, Steiner made quite opposite observations in Prague. He saw among 252 cases of chorea only four which originated during the course of acute articular rheumatism.9 This statement does not prove the absence of a relation between chorea and rheumatism, for Steiner does not say what proportion of cases occurred after an attack of rheumatism which had taken place some time previous. Hammond10 believes “that the influence of rheumatism upon chorea is not greater than that of a depressing agent to the organism.”
9 Ziemssen's Cyclopædia, loc. cit., p. 427.
10 Dis. of the Nervous System, p. 715.
Octavius Sturges, physician to the Hospital for Sick Children, Ormond St., London, says that in two years 219 cases of chorea have been treated at that institution: 20 per cent. of them were connected with rheumatism, but he does not believe in the rheumatic origin of the disease, because 15 per cent. of all children have rheumatism.11
11 Lancet, Sept. 20, 1884.
The following cases illustrate the direct sequence of chorea upon acute rheumatism:
Case II.—Kate S——, æt. 17 years, came under my care in May, 1877, with an attack of acute rheumatism which lasted for two weeks. She regained strength slowly, and about June 11th, not more than two weeks after the subsidence of the rheumatic symptoms, choreic movements were noticed in the right arm. The movements were constant, and were worse when she was conscious of being observed. She often dropped things. The right leg jerked often and gave away under her in walking. Under the use of liq. arsenici bromidi the patient was entirely well in one month. A sister had had chorea.
[p. 443]Case III.—Rudolph C——, æt. 5 years, was placed under my care May 12, 1883. He has had scarlatina, and in Dec., 1882, he had an attack of inflammatory rheumatism, accompanied with slight choreic movements, from which he recovered in a short time. Three or four weeks before coming under my charge he had a return of rheumatism from getting his feet wet, and at the same time choreic trouble began again. He rapidly became worse, and in a short time was utterly helpless. On examination he is found unable to sit up or make any voluntary movements. He is unable to move the legs on account of the intense pain in the knees and ankles from the rheumatism. These joints are swollen and red. The right arm is in constant and violent motion, swinging about or thrashing up and down. The left arm lies motionless, and, although painless, he seems unable to move it. The fingers are clenched, and they are continually and rhythmically being pressed against the palm. He cries if an attempt is made to open the fingers. The facial muscles are contorted all the time, and there is a peculiar vermicular movement of the upper lip. He cannot speak a word nor can he protrude the tongue. He sleeps but little, and during sleep the movements are occasionally seen. He is very fretful and irritable, but is perfectly intelligent. The appetite is poor. Bowels regular; urine phosphatic and contains no albumen. There is a loud but not harsh cardiac murmur heard at the apex, replacing the first sound of the heart. Temperature, May 12, evening, 100°; May 13, morning, 1002/5°. Pulse, 140. He was ordered sodii salicylat., gr. v. q. q. h., and inunctions of cod-liver oil.
On May 18 the rheumatism was so much better that the salicylate was stopped and Fowler's solution of arsenic was given instead. The chorea had also become better. The arsenic was continued in increasing doses, and the case convalesced steadily. On June 26 he was able to return to his home in Maryland entirely well.
He remained well until July, 1884, when he had a slight attack of chorea, which was preceded for about a week by rheumatism. The cardiac murmur, which was almost absent after recovery from the first attack, was now heard again, but faintly.
Scarlatina is sometimes the forerunner of an attack of chorea. Other diseases, whooping cough or measles, may also be the immediate cause of an attack of chorea, but it is generally in cases where there is a predisposition to the disease.
The connection between pregnancy and chorea is of great interest. Barnes12 has collected 58 cases, and Bodo-Wenzel13 has added 8 more, making 66 in all. Of 51 of these patients, 31 were primiparæ, and in the majority of cases the ages were between twenty and twenty-three years. Four cases which came under my own personal observation were all young primiparæ, and were between the second and fourth months of gestation when the disorder began. The affection usually appears in the first half of pregnancy. It may cease before the eighth month or may continue to the end of gestation. Sometimes it persists after delivery. It does not necessarily occur in patients who have had the disease in childhood, but from the above cases it would seem that an attack in one pregnancy would tend to its recurrence in another. Of the 66 cases, 14 [p. 444] had had chorea in previous pregnancies. Sometimes the chorea appears only at the time of labor.
12 Obstet. Transactions, vol. x. p. 147.
13 Ziemssen's Cyclopædia, loc. cit., p. 428.
The immediate cause of chorea in pregnancy, when a cause can be found, is most often fright or rheumatism. In two of my own cases the patients were unmarried. Of the 66 cases of Barnes and Wenzel, fright is named as a cause in 7, and in 7 more rheumatism and endocarditis are stated to have preceded the attack.
Climate has been supposed to have a marked influence upon chorea. It was thought to be less frequent in warm than in cold regions; but Hirsch denies this, and Weir Mitchell14 states that it does not appear to exist to any less extent in the southern than in the northern portion of this country.
14 Loc. cit.
Season, according to Mitchell,15 largely affects the production of chorea. He has gone to great pains to collect statistics on the subject. He shows that the majority of attacks in his cases occurred in spring. This agrees with Wicke,16 who found that among 35 relapses, 13 were in spring, 12 in winter, 9 in autumn, and 1 in winter. On the contrary, Hammond17 found 54 attacks in the six months from October to March, and but 28 in the remainder of the year. Gerhard18 in a study of 80 cases found that of 68 attacks, 39 occurred in spring, 10 in summer, 7 in autumn, and 12 in winter. In Mitchell's cases a study was made of 170 attacks. In the spring and summer months there were 115 attacks against 55 in the winter and autumn months. This observer does not find that rain or dampness has any notable effect in causing the disease, but that the influence of storms is probably great.
15 Loc. cit., p. 128.
16 Ziemssen, loc. cit., p. 443.
17 American Journ. Med. Sciences, July, 1876.
18 Loc. cit., p. 715.
Mitchell has written upon the relation between race and chorea. He states that in answer to a circular bearing on this question, sent out by the Smithsonian Institution, he has received a large number of letters from physicians in our Southern States and the West Indies. The general testimony was that chorea is rare among negroes.
Among the exciting causes of chorea are fright or mental apprehension of some kind. Of my 279 cases, 44 were ascribed to fright.
Malaria has been pointed out as influencing the production and course of chorea. Kinnecut has reported some cases in which the movements were aggravated with a certain periodicity.
Chorea may also be brought on by reflex irritation from nerve-injury. In a case which I saw in the practice of John H. Packard several years ago there was an injury to one of the digital nerves of the thumb from a splinter, which was the apparent cause of an attack of chorea; a portion of the nerve was excised, and the chorea ceased in a short time.
I have lately seen a case in which an attack of chorea came on apparently in consequence of a severe mash of the finger. The finger had been crushed by the runner of a sled, and the choreic movements began before the wound was healed.
Hamilton19 has found chorea associated with eczema. He saw a case in which eczema of the calves of the legs and of the scalp developed at the same time with an attack of chorea. Both got well about the same time.
19 Nervous Diseases, p. 490.[p. 445]
SYMPTOMS.—An attack of chorea is usually preceded by more or less failure of the general health and evidences of some mental disturbance. It is quite common to be told by the parents of a child suffering from chorea that the little patient had seemed unwell for some time previous to the attack; that the appetite had failed, and that the child had looked pale; that he had been irritable or excitable, and at school the teacher had complained of restlessness or inattention in the pupil. In a little girl who was brought to me recently with her second attack of chorea her mother stated that for several days before the outbreak the child had been in excessive spirits, and that she had been singing loudly and in a peculiar manner. The same symptoms had preceded the first attack. Sometimes nothing is observed until it is found by the parents or teacher that there are abnormal twitchings and movements of the limbs.
At first there is a general restlessness and fidgetiness. The child may be punished at school for not keeping still or for dropping things. Soon irregular movements of groups of muscles are seen. The shoulder is shrugged or the fingers move spasmodically. At first the patient is aware of the movements and tries to control them, but before long the twitching and jerking are constant, and extend to most of the voluntary muscles of the body. He is then unable to control them for any length of time.
The sudden jerk of a limb followed by an odd grimace, the quick protrusion of the tongue, and the rolling of the eyes or snapping of the lids give a characteristic picture which can hardly be mistaken.
The extent of the movements varies in different cases. In some they are slight and affect only certain muscles. Often the disorder is confined to one lateral half of the body. In other cases the movements involve all the limbs and the trunk, and are so violent and constant that the patient does not seem to have a moment's rest. The trunk may be suddenly drawn backward, then the arms are extended or thrown up, and the legs flexed and tossed about with great quickness. Sometimes the patient is thrown off the bed or from the chair on which he may be to the floor.
The speech is often affected. The patient speaks in a thick or jerky manner, as if the tongue were too large for the mouth, and saliva usually flows in great quantities. Sometimes in bad cases there are involuntary utterances made at frequent intervals.
The features undergo contortions continually, and when at rest relapse into a condition of vacancy which makes the patient look almost idiotic. The expression of a child with chorea is so peculiar that the disease may almost be diagnosticated by this.
During sleep the movements usually cease, but generally the patient is restless while asleep, and in some instances the irregular movements continue even at this time.
The mental condition commonly shows some change. The child is irritable and peevish, cries and laughs readily, or is sullen and morose. Sometimes he is violent to those about him, but this is rare. Intellectually the patient suffers somewhat. He is not able to study as before, and the memory may be impaired. Sometimes there is a mild form of dementia.
[p. 446]During the course of the disease there may be exacerbations, and sometimes after convalescence has seemed established there are relapses.
Recovery is gradual, and as the abnormal movements cease the mental condition improves, and the patient regains his health without any traces of the disease remaining.
We will now consider some of the symptoms separately. First, as to disturbances of motion. As before remarked, the disorderly movements occur soon after the general restlessness is seen. They most commonly begin in one upper extremity. The hand is thrown into various positions, the fingers are flexed and extended or separated, and all of the movements occur with great rapidity. In a day or two the whole arm is affected, and then the leg of the same side is involved in the jerkings and twitchings. In many cases the facial muscles are contorted, the mouth is pursed up or opened wide, and then quickly twisted into some other shape. If the patient is told to put out his tongue, it is protruded after a moment's hesitation, and then suddenly retracted, the jaws coming together with a snap. A smacking sound is made with the lips quite often, and words are uttered involuntarily. The movements may remain confined to one side of the body, constituting what is called hemichorea. This is quite common, and the right side is rather more frequently involved than the left. There is so great difference of opinion among authors on this point that it is probable that one side is affected about as often as the other. Of 252 cases which I have examined, 69 were right and 43 left hemichoreas. Gerhard20 found in 80 cases of chorea that 32 were unilateral; of these 20 were right and 12 were left. Sée, however, found that in 97 of 154 cases the movements were either confined to the left side or were more marked on that side. He states that in his experience the proportion between left and right hemichorea is as 37 to 27. Pye-Smith in 33 cases of unilateral chorea found 15 on the right and 18 on the left side. Many cases which begin as hemichorea soon become general.
20 American Journal of Med. Sci.
The disease reaches its greatest severity in about two weeks, and if the case is a bad one we find by this time all of the voluntary muscles are in constant movement. At this time the French name for chorea, folie musculaire, is most appropriate. Patients are often unable to walk or to sit up, and sometimes they may be thrown from the bed by violent spasmodic movements of the trunk. Strange as it seems, patients rarely complain of fatigue, notwithstanding the violent muscular exercise. This is probably because each set of movements is of short duration and is constantly changing its seat.
As a rule, the movements cease completely during sleep or under an anæsthetic. Sometimes occasional twitchings of muscles are seen in sleep, and in rare instances we are told by the parents of a child with chorea that the movements are as active in sleep as in the waking hours.
The movements of chorea occur either while the limbs are at rest or under the influence of voluntary effort. This fact has been pointed out by Mitchell and by Gowers. In some cases the movements are most marked when the patient is at rest. If a directed effort is made to use the member for a time, the choreic movements are suspended. For example, a patient may be able to carry a glass of water to the mouth without [p. 447] spilling a drop, while a moment before the hand may have been performing a continual dance. I have often observed that while the limb to which the whole attention has been directed in performing some movement has been steadied, the other limbs become violently agitated.
In another class of cases the movements are comparatively slight when the part is at rest, but when a motion is attempted the disorder of the muscles is so much increased that it is almost impossible for the act to be completed. The patient is told to pick up some small object: he throws the hand out toward it, and it is jerked away before he can grasp it. He again puts the hand forward, reaches the object, and the fingers open and shut and sprawl over the article before it is taken up. Sometimes it cannot be grasped at all. This has been called choreic ataxia, but it is only one type of the cases commonly seen.
This brings us to the influence of the will on the movements in chorea. There are some cases, as mentioned above, in which the movements may be controlled by the will for a brief period, but they will sooner or later return. In other cases it is quite impossible for the patient to check the movements at all, and one frequently sees in a case of hemichorea the sound hand used to grasp the other, so as to control the movements. We have referred to this because of Niemeyer's opinion that corporeal punishment would shorten an attack of chorea.
Chorea is sometimes confined to a single muscle or group of muscles. When limited in this way it is generally in the head, face, or perhaps in the shoulder. These cases of localized chorea have been spoken of by Mitchell as habit chorea.21 They are often very obstinate in resisting treatment, and sometimes last during life.
21 Lectures on Nervous Diseases, p. 146.
PARALYSIS.—Not infrequently in chorea there is paralysis to a greater or less extent. It is generally one-sided, and most often involves the upper extremity. The limb affected is the one in which the movements were most violent. The arm may hang entirely powerless or it may be only enfeebled, and feeling to the patient like a dead weight. The paralysis always recovers with the chorea or soon after.
POST-PARALYTIC CHOREA.—Under this term Mitchell and Charcot have described a variety of chorea which is seen in patients after an attack of hemiplegia. The movements are chiefly on voluntary effort, and are those of inco-ordination. They come on from one to several months after an attack of unilateral paralysis, and are sometimes seen in cases in which almost complete recovery has taken place. Mitchell has reported22 a case which was under my care for several years, and which he saw in consultation with me. This patient had two attacks of left hemiplegia, the last being fatal. After the first attack there was great gain of power to use the arm and leg, but the movements were performed awkwardly and with an irregular jerking movement. A post-mortem examination revealed a spot of softening the size of a filbert in the left corpus striatum, which was apparently recent, and a point of red degeneration in the right crus cerebri. The vessels at the base of the brain were extensively atheromatous.
22 American Journal of the Med. Sci.
Of the electrical condition of the muscles in chorea but little is known. Rosenthal23 found increase of faradic contractility in three cases of hemichorea, and the galvanic test showed a high degree of excitability, [p. 448] demonstrated by the fact that weak currents gave contractions at cathodic closure, or even tetanic contractions, and also contractions were produced at cathodic opening.
23 Ziemssen's Cyclopædia, loc. cit., p. 434.
The affection of speech which is so common in chorea is due to disordered action of the laryngeal muscles, or it may be from choreic action of the abdominal muscles. Sometimes it is chiefly from the awkwardness of the tongue. The usual form of trouble is that the patient speaks in a staccato manner and the syllables seem as if they were driven out. When the chorea is in the laryngeal muscles, the tone and pitch of the voice are altered.
Chorea of the heart is sometimes spoken of, but it has never been satisfactorily demonstrated that there is any real disorder of cardiac rhythm in chorea. It is not unusual in chorea to meet with over-action or palpitation of the heart, but these conditions do not necessarily depend on the disease.
Valvular murmurs are often met with from the beginning of an attack. In some instances they are the result of an endocarditis, but frequently they are functional or anæmic. They are usually heard at the apex. Sometimes there is a reduplication of the first sound, giving the idea of a want of synchronism in action of the two sides of the heart; but this is probably not the result of chorea of the heart. I recall one patient, a child of seven or eight years, in whom the reduplication of the first sound was very distinct during an attack of St. Vitus's dance. She was brought to me at the beginning of a second attack a year later, and the reduplication of the cardiac sounds was heard again, so it is likely that it had continued during the interval, and was probably a congenital condition.
The pupils are commonly dilated in chorea and respond sluggishly to light.
REFLEXES.—I have examined the condition of the patellar reflex in 50 cases. In 26 of these it was present in normal degree, in 15 it was diminished, and in 9 it could not be excited. In one patient it was absent during the height of the choreic movements, but could be readily produced after the patient had recovered. The condition of the reflexes has also been examined by Joffroy and Saric,24 and they found that of 16 cases of chorea the reflexes were abolished or diminished in 12.
24 L'Union médicale, Sept. 22, 1885.
SENSIBILITY.—Authors state that disorders of sensation are met with in chorea, such as localized anæsthesia or a general hyperæsthesia: I have never met with any such instances. Patients often complain of pain in the joints or in the limbs, and this may be unaccompanied with swelling or tenderness on pressure. Tenderness on pressure over the vertebræ is rare in my experience, although others speak of its being of frequent occurrence. Mental disorders are generally present, but only to a slight extent. There is almost always irritability of temper and peevishness. The most sweet-tempered children become cross and perverse, laugh immoderately at trifling things, or cry as readily if they are annoyed. There is generally failure of memory and incapacity for study or thought. In most cases, however, this exists to so slight an extent as not to be noticed except on very close observation. Sometimes there is marked mental disorder amounting almost to imbecility, and occasionally the mental weakness remains for some time after the motor disorders have recovered.
[p. 449]The condition of the pulse is generally unchanged, but sometimes it is abnormally frequent. The temperature, according to Von Ziemssen, is unchanged.
The nutrition generally suffers. The patient rapidly loses flesh, and becomes anæmic; the skin grows dry, and the hair gets harsh. The digestion is apt to be disordered. The tongue is large, pallid, and coated thickly, and there is sometimes nausea or vomiting. The appetite is not good. The bowels are often constipated. The urine has been examined by several observers. Bence Jones found an excess of urea at the height of the disease. Albumen is not present except accidentally, but there is usually an excess of phosphates. In several cases in which we have examined the urine at the Infirmary for Nervous Diseases we found that the specific gravity was high while the chorea was at its height, but fell to normal as the patient recovered.
Chorea is spoken of as acute and chronic, but all cases are more or less chronic. Those cases which last eight or ten weeks may be considered acute, while those running on for months or years are properly called chronic.
DURATION.—Considerable difference of opinion exists as to the duration of chorea. Some writers speak of three or four weeks as an average attack. Gray and Tuckwell, in a series of cases treated by the expectant plan,25 found an average duration of ten weeks. Occasionally a patient is seen with an attack of chorea which lasts only a few days. The parents of a little patient whom I saw a few days ago assured me that her second attack lasted only a week. They are educated and intelligent persons whose statement can be relied upon.
25 Lancet, Nov. 28, 1876.
The course is not always regular. In some cases the disease gradually reaches a crisis, remains stationary for a few days, and then by degrees declines; in others there are exacerbations. The patient will seem to be almost well, and then become very much worse for a time. Relapses are not infrequent, and are generally caused by fright or excitement.
The recurrence of attacks of chorea is well known. A child who has had the disease one year may have it a second or third year. It is most likely to recur in the spring. Some cases have as many as five attacks, but as puberty approaches the attacks are lighter, and finally cease. Of 282 cases to which I have referred, 198 were first attacks, 47 had had chorea twice; 23 were in their third attack, 8 in the fourth, and 3 in the fifth attack.
TERMINATION.—The disease in most instances terminates in complete cure, but sometimes there is nervousness or want of co-ordination remaining for a time. Rarely the inco-ordination or a certain quickness in movement becomes permanent.
Death is a rare termination of chorea except in pregnancy. If it does occur, it is usually from some complication. In pregnancy the mortality is great. Of 64 cases collected by Wenzel, 18 died. In Philadelphia, in seventy-four years from 1807 to 1881, there have been but 64 deaths from chorea; of these, 38 were under twenty years, and 26 over that age.
Hutchinson reports a fatal case in a boy of twelve years.26 After complaining of headache and rheumatic pains for several days, choreic [p. 450] movements began. They soon became general and very violent. At the end of two weeks he was admitted to the Pennsylvania Hospital. At this time the patient was so extremely convulsed that it was impossible to keep him in bed without tying him. The movements continued but little abated, and the child died in two days.
26 Philadelphia Med. Times, vol. vi. p. 535.
Another case of unusual interest is reported by Hunt.27 The patient, a man of twenty-nine years, had suffered from chorea of the face and arms for years. In consequence of a fall on the pavement he fractured the left humerus. The movements were immediately exaggerated, and in spite of a carefully adjusted splint it was impossible to keep the arm at rest. The fragments were in a state of constant movement, and the points of bone threatened to penetrate the skin. The skin was so much excoriated that it was determined to dispense with the splint and attempt to keep the limb at rest by the administration of morphia hypodermically in half-grain doses three times daily. This failed to keep the arm quiet, and the seat of fracture became greatly inflamed. No form of appliance or medication succeeded in keeping the arm at rest, and the patient finally sank and died from exhaustion on the tenth day after admission to the hospital. The post-mortem examination revealed no gross lesion of the brain or cord. No microscopic examination was made of the brain.
27 Pennsylvania Hospital Reports, vol. ii.
MORBID ANATOMY AND PATHOLOGY.—In a disease so seldom fatal as chorea it is not surprising that there have been but few post-mortem examinations made. In the earlier autopsies, before the microscope was extensively used, but little of value was recorded. Sée, who collected 84 cases in which post-mortem examinations were made, reported that in 16 no changes were found in the nervous system. In 32 there were lesions in the brain and nervous centres, usually softening and tuberculosis, and in the remainder inflammatory changes in the serous membranes. In 29 there were evidences of heart disease. Sée considered that but few cases of death in chorea were caused by inflammatory diseases of the heart, but that the majority should be referred to nervous excitement and anæmia.
Ogle28 in a report of 96 cases of chorea mentions 16 which were fatal. Post-mortem examinations were made in all of these. Cardiac lesions were found in 13. In 10 of these deposits were found upon the valves, and in 3 there was some change in the pericardium. He speaks of having noted congestion of the nervous centres six times, and softening of the cord once.
28 Brit. and For. Med.-Chir. Review, Jan., 1868.
In all of 11 autopsies reported by Pye-Smith29 there were cardiac lesions found. In every case old or recent deposits were observed upon the valves. In two instances the heart was hypertrophied, and in one there was pericarditis. Changes in the nervous system were less often found by this writer. In 1 case there was hyperæmia of the cord, and in 3 cerebral hyperæmia.
29 Guy's Hospital Reports, 1874.
Dickinson found in 22 fatal cases of chorea 17 in which the heart was diseased. “In every instance making up the large tale of cardiac disease there were recent vegetations on the mitral valve, and often also elsewhere.”
In the fatal case of Hutchinson referred to above the heart was found diseased, the aortic valves were incompetent, the leaflets being swollen [p. 451] and softened, and the aorta was atheromatous above the sinus of Valsalva.
Of late years a number of careful autopsies have been made in cases of chorea. The brain and spinal cord have been closely examined, and in almost every instance some lesion has been found in both of these organs.
Steiner reported in 1868 the results of post-mortem examinations in 3 fatal cases of chorea. In 1 case he found cerebro-spinal anæmia, serous effusion into the spinal canal, and proliferation of the connective tissue in the upper part of the cord; and in another hyperæmia of the brain and cord.
Elischer,30 who reports a fatal case in a parturient woman who had an attack of chorea in her eighth year, two in her sixteenth year, and another in a previous pregnancy, found at the autopsy hyperæmia and œdema of the brain and gray substance of the cord. Microscopically, the brain showed fatty, amyloid, and pigmentary changes in the nerve-elements and vessels of the large central ganglia, small secondary extravasations of blood in the connective tissue, and numerous emboli in the smallest vessels, especially in the cortex. In the spinal cord there was seen abundant proliferation of nuclei in the adventitia of the vessels. In the central canal serum was found, and the surrounding connective tissue was harder than usual.
30 Cyclopædia of the Practice of Medicine, Von Ziemssen, vol. xiv. p. 450.
Dickinson has contributed an excellent paper on the pathology of chorea.31 He relates the particulars of the autopsies in 7 fatal cases in which he personally made microscopical examination of the brain and spinal cord. He also adds the results of post-mortem examinations in 17 other cases at St. George's Hospital and at the Hospital for Sick Children. In all of the 7 cases in which microscopic examinations of the brain and cord were made there were found hyperæmia of both of these structures, in many instances hemorrhages into the substance of the nervous tissues, dilatation of the smaller vessels, and in chronic cases sclerotic changes in the course of the vessels. “The first visible change,” he remarks, “would seem to be the injection or distension of the arteries, succeeded by extrusion of their contents, to the irritation and injury of the surrounding tissue.” The changes seemed to affect both brain and cord in all cases. The parts of the brain most constantly affected lay between the base and the floor of the lateral ventricles in the track of the middle cerebral arteries, the substantia perforata, the corpora striata, and the beginning of the Sylvian fissures. “Of the cord no region was exempt, but perhaps the cervical and dorsal regions were usually more affected than the lumbar. With regard to the vertical or physiological divisions of the cord, these all, whether white or gray, shared in the vascular destruction; this condition, however, was usually most marked in the vessels belonging to or in connection with the lateral part of the gray matter about the root of each posterior horn. And it is to be observed that this was also the chosen situation of the more definite and special changes, whether hemorrhagic (as in two instances), sclerose, or exudatory. Speaking generally, the chosen seats of the choreic changes are the parts of the brain which lie between the beginning of the middle [p. 452] cerebral arteries and the corpora striata—the parta perforata; and in the cord the central portion of each lateral mass of gray matter comprising the root of each posterior horn.”
31 Medico-Chirurgical Transactions, vol. xli. p. 1, 1876.
The embolic theory of chorea has been held by several investigators, among them Hughlings-Jackson. It is undoubtedly an attractive and reasonable view, especially when we consider the large proportion of cases in which there is valvular disease of the heart. Dickinson, however, does not consider this hypothesis tenable. In none of the cases in which he made post-mortem examinations did he find evidences of embolism. “In none of the instances described were decolorized fibrin, detached clots, or signs of impaction detected, and the erraticism of embolic accident was wanting: the constancy indeed with which the changes repeated themselves in certain positions, and the equality with which they affected both sides of the body, are conclusive objections to this hypothesis. The corpora striata, for example, were affected with almost absolute symmetry, notwithstanding that these bodies receive their blood respectively from the right and left carotids and different parts of the aortic arch.”
Rheumatism is associated with or precedes chorea in a large proportion of cases, and this was pointed out by Kirkes in 1850 and again in 1863. This connection between rheumatism and chorea, and the frequent occurrence of endocarditis in chorea, has led some authors to believe that the endocarditis is always rheumatic, and that the chorea is the result of the endocarditis. Dickinson, however, points out that in cases in which there is a distinct history of the chorea beginning suddenly from fright there are often well-marked cardiac murmurs heard. He believes that in all cases of chorea in which there are cardiac murmurs they are due to endocarditis, and suggests that in these cases from fright the endocarditis is due to irregularity of cardiac action. This, of course, is mere hypothesis, and we must bear in mind that in all cases of chorea there is anæmia, and that the murmur may be purely functional.
H. C. Wood, in a communication read before the College of Physicians of Philadelphia,32 gives his views of the pathology of chorea, based upon the results of post-mortem examinations made in a number of dogs who had the disease. He believes the history of chorea to be this: “Owing to emotional disturbance, sometimes stopping of various vessels of the brain, or sometimes the presence of organic disease, there is an altered condition of the ganglionic cells throughout the nerve-centres. If the cause is removed and the altered condition of the nerve-cells goes only so far, it remains what we call a functional disease. If it goes so far that the cells show alteration, we have an organic disease of the nervous system.”
32 Philada. Med. News, May 30, 1885.
In two dogs which were choreic the movements continued after section of the cord. This shows that in dogs, at any rate, the movements originate in the cord. In four instances of canine chorea in which Wool made autopsies there were found in the cords of three mild grades of infiltration of leucocytes in the gray matter. In the fourth, in which the dog had died of the disease, the ganglion-cells were degenerated, and in some places had disappeared. He concludes, therefore, that choreic movements may depend upon a diseased condition of the motor cells of the cord.
[p. 453]Although there are several recorded cases of human chorea in which lesions of the spinal ganglionic cells have been found, we cannot believe that this can be a constant lesion in chorea. The disease is too transient in many cases, and presents too many variations and anomalies, for the cord to be always the seat of the diseased condition.
In an interesting paper read by Angel Money before the London Medical and Chirurgical Society in 1885 he detailed some experiments in which, by injecting a fluid containing arrowroot, starch-granules, or carmine into the carotids of animals, he produced movements closely resembling chorea; and this was found to be associated always with embolism of the capillaries of the cord. In the discussion which followed Broadbent and Sturges expressed their disbelief in the embolic origin of chorea in man. Hughlings-Jackson said that he held the view of the cerebral origin of chorea, one of his reasons being the frequency with which the face-muscles are affected in this disease.
The probabilities are that in chorea there is a disordered condition of the brain and cord more or less general. The lesions are no doubt slight in mild cases of short duration, but in severe cases of long standing there occur well-marked changes in portions of both brain and cord. We cannot do better than to sum up the pathology of chorea in the words of Dickinson: “A widely-distributed hyperæmia of the nervous centres, not due to any mechanical mischance, but produced by causes mainly of two kinds—one a morbid, probably a humoral, influence which may affect the nervous centres as it affects other organs and tissues; the other, irritation in some mode, usually mental, but sometimes what is called reflex, which especially belongs to and disturbs the nervous system, and affects persons differently according to the inherent mobility of their nature.”
DIAGNOSIS.—The only diseases for which chorea may be mistaken are paralysis agitans and disseminated sclerosis. The former occurs only in adult life, and the tremor is of a regular rhythmical character. In the latter the tremor occurs only on voluntary effort, and is also more regular than the movements of chorea. There are forms of congenital sclerosis seen in children which closely resemble chorea. Here the duration of the disease and the association of contractures with it distinguish it from chorea.
Hysterical subjects have a form of chorea which can only be differentiated from the true disorder by noting the general hysterical character of the case and the result of treatment, which strongly influences the will-power of the patient.
PROGNOSIS.—In the great majority of cases this is favorable. If the disease occurs in childhood and is without complications, recovery generally takes place spontaneously after a few weeks. Should the movements be violent and continuous, so as to interfere with sleep and the taking of food, or should there be any complication, such as acute rheumatism or cardiac disorder, then the prospect of recovery is not so good.
The prognosis as to relapses should be given with caution. If in a child, it is possible that there will be a return of the disease after a longer or shorter interval. It is not likely to recur until after several months, usually at about the same season the following year. As the child grows older the intervals become longer, and it may safely be [p. 454] asserted that after puberty is passed and bodily development completed there will be no more returns of the affection.
The cure is usually complete. It must be remembered, however, that for some time after an apparently complete cure there may be slight inco-ordination of movements, particularly in the arms and the face. These are shown in the unnecessary haste in making uncertain motions or in slight grimaces, or if excited an awkwardness in the use of the fingers.
Death is a rare termination in uncomplicated cases, especially in children. The fatal cases are generally when acute rheumatism has been associated with the chorea or when there has been a fracture or an injury as a complication.
In Sée's statistics there is a mortality of 5.7 per cent. in 158 cases in the Children's Hospital. In adults, and more particularly in pregnant women, death is more common. Wenzel's cases referred to above gave a mortality of 27.3 per cent.
The cause of death in chorea may be from the intensity of the disease, and in this case the symptoms are generally violent from the outset, increase to an extreme extent, and then collapse and coma come on. The movements may cease when the collapse occurs, but they may continue to the last, growing gradually less until death.
TREATMENT.—A vast number of remedies have been popular in this disease from all ages. The medicine which is most generally depended upon at the present day is arsenic. It is advised by most writers, and in my own experience is decidedly the most reliable remedy for chorea which we know. The best way to administer it is in the form of Fowler's solution, and it should be given in large doses. I have given the bromide of arsenic, but did not find it superior to Fowler's solution. The amount of arsenic which can be safely borne by children with chorea is surprising to those who have not had experience in its administration. The medicine should be given in gradually increasing doses until the toxic effects are well marked or until the patient is convalescing. In a child of six years three drops may be given to begin with, three times a day. One drop additional should be added to the dose each day, and the child soon acquires a remarkable tolerance of the drug. As much as twelve or fifteen drops at a dose is borne by a child of eight years. If vomiting or much œdema of the face occurs, the medicine should be stopped for a day or two, and then the original dose should be taken, to be again increased as before.
Seguin recommends that the patient should begin again with the dose at which tolerance ceased. For instance, if vomiting occurred after a dose of nine drops, he stops the medicine for a day, and begins again with eight drops. I have found that sometimes this causes vomiting again, and I think it preferable to resume the medicine with a small dose.
It is often seen that a patient becomes worse during the first few days that the arsenic is taken, but improvement generally begins after a week of the arsenical treatment, and is well marked after two weeks.
In obstinate cases it is of marked advantage to give the arsenic hypodermically. Cases which do not yield to the drug when given by the mouth often improve at once when it is given hypodermically. Chronic cases which have resisted all forms of medication sometimes are cured by [p. 455] hypodermic injections of arsenic. For giving arsenic in this way it is best to use Fowler's solution, made without the compound spirit of lavender. It is less likely to cause abscess to form at the point of puncture.
Other remedies enjoy a reputation in the treatment of chorea. Sulphate of zinc is relied upon by many, and it is the means which Ross recommends. It should be given in increasing doses like arsenic, and very large doses may often be taken without disturbing the stomach. Trousseau, Hammond, and Hamilton favor strychnia, but I have had no experience in its use.
Cimicifuga and conium are both often beneficial in their effects. I have seen the former do good when arsenic had failed. Conium to be efficacious must be given in large doses. Eserine and hyoscyamine have both been successfully employed, the former by Bouchut, and the latter by Oulmont and Laurent. Recently, DaCosta33 has reported, in a clinical lecture at the Pennsylvania Hospital, a case of very severe chorea successfully treated with hyoscyamine. The patient was a boy of eleven years, and the disorder had followed an attack of acute rheumatism. He was given 1/100 gr. of hyoscyamine three times a day.
33 Philada. Med. Times, Jan. 23, 1886.
Ziegler34 has recorded several cases which recovered under the use of nitrite of amyl. The bromides and chloral are useful adjuncts to treatment in case of sleeplessness or mental irritability. Cases of cure by the use of chloral alone have been reported. Bouchut gave a girl of fourteen and a half years, with chorea and dementia, 45 grains of chloral a day for twenty-seven days. She slept most of the time, but improvement was seen on the fifth day, and cure was completed on the twenty-eighth day of the use of the chloral. Electricity has been efficient in the hands of many writers. I have found galvanization of the spine to produce a quieting effect in some cases.
34 Ibid., vol. vi. p. 486.
Iron is always of use in chorea; it may be given during the course of the disease, and is generally necessary in convalescence. Cod-liver oil or malt extract should be given in feeble persons.
It is scarcely necessary to mention the other remedies which have been recommended. DaCosta has used the bromide of iron. H. C. Wood has used a preparation of skunk cabbage, and there are a great number of other remedies which have been found of value.
Next to the internal means come external applications. Baths and frictions are useful in their effect on the general health. The ether spray to the spine or the application of an ice-bag for ten minutes once or twice daily is sometimes found to assist the other means. Cold douches have been advised by some, but they may do harm. The care of the general health of the patient is of first importance, and his surroundings should be as quiet as possible.
It is of the greatest value in bad cases to place the patient in bed and keep him there until the symptoms improve. John Van Bibber of Baltimore has treated a number of cases of chorea successfully by keeping them secluded in a darkened room. Such an extreme degree of isolation is not often necessary, and it might make a child more nervous.
In children the patient should always be taken from school and kept from exciting play. Plenty of fresh air and wholesome food should be [p. 456] insisted upon. Change of air to the mountains or to the seashore often effects a cure in a short time.
Some cases do not appear to be benefited by any treatment. These are the hereditary form of chorea and some of the localized choreas. The latter are often helped or cured by the hypodermic use of arsenic even in long-standing cases.
This disease was first described by Hammond in his work on Diseases of the Nervous System in 1871, and cases have since been reported by many observers, among them Clifford Allbutt, Claye Shaw, Eulenburg, Oulmont, and Gowers. The disease is named by Hammond from the word ἀθετος, without fixed position.1 The principal features are an inability to retain the fingers and toes in any position in which they may be placed, and the continual movements which persist in the parts—a condition called by Gowers mobile spasm.
1 Diseases of the Nervous System, p. 722.
Athetosis is often connected with impaired mental powers; many of Shaw's cases were in imbecile children.
The movements of athetosis are not confined to the hand in all cases, but they are sometimes met with in the foot, and even in the muscles of the face and back.
The following is Hammond's original case:2 “J. P. R——, aged thirty-three, a native of Holland, consulted Hammond Sept. 13, 1869. His occupation was bookbinding, and he had the reputation, previous to his present illness, of being a first-class workman. He was of intemperate habits. In 1860 he had an epileptic paroxysm, and since that time, to the date of his first visit to me, had a fit about once in six weeks. In 1865 he had an attack of delirium tremens, and for six weeks thereafter was unconscious, being more or less delirious during the whole period. Soon after recovering his intelligence he noticed a slight sensation of numbness in the whole of the right upper extremity and in the toes of the same side. At the same time severe pain appeared in these parts, and complex involuntary movements ensued in the fingers and toes of the same side.
“At first the movements of the fingers were to some extent under the control of his will, especially when this was strongly exerted and assisted by his eyesight, and he could, by placing his hand behind him, restrain them to a still greater degree. He soon, however, found that his labor was very much impeded, and he had gradually been reduced from time to time to work requiring less care than the finishing, at which he had been very expert.
“The right forearm, from the continual action of the muscles, was much larger than the other, and the muscles were hard and developed like those of a gymnast. When told to close his hand he held it out at arm's length, clasped the wrist with the other hand, and then, exerting all his power, [p. 458] succeeded, after at least half a minute, in flexing the fingers, but instantaneously they opened again and resumed their movements.
“In this patient there was impairment of intellect, his memory was enfeebled, and his ideas were dull. There was no paralysis of any part of the body, but there was slight tremor of both upper extremities. The involuntary movements were of the right arm, and continued during sleep. Sensation was normal. The spasm of the muscles causes severe pain in the arm, and keeps him from sleeping at night.” Hammond used various remedies without relief, and had the patient under his charge for many years. Finally, he showed the patient to the American Neurological Society at the annual meeting in 1883, with almost complete relief to the movements as a result of nerve-stretching.
2 Ibid.
Athetosis is found in two forms—the hemiplegic and the bilateral varieties. In the former there has usually been an attack of hemiplegia more or less marked, or there has been an epileptic fit or unconsciousness from alcohol, as in Case I. There is often hemianæsthesia or some disorder of sensation. In the bilateral type the movements exist in all of the limbs, and are unaccompanied by weakness or disorder of sensation. The degree of movement varies in different cases. In some it is very slight, and can be controlled by extreme effort on the part of the patient. In other cases the movements are violent and uncontrollable. The muscles of the affected limbs become hypertrophied from the constant exercise.
The following case of athetosis has come under my care:
Case II.—W. A——, aged thirteen years, male. He had good health until 1877, when at the age of six years he had diphtheria. The attack was not severe, and he was up most of the time. About ten days after apparent convalescence he was suddenly seized with left hemiplegia. The paralysis was complete, involving the left arm and leg, the left side of the face, and the muscles of deglutition. There was also aphonia. In two weeks he began to talk, but indistinctly. In a month he could move the arm, but the movements were inco-ordinate. At about the same time he began to walk, but dragged the leg. The arm never regained power of voluntary motion, but instead there came on a spasmodic condition of the muscles which fixed the arm in various positions, and at the same time there were kept up constant but irregular movements of the hand and fingers. No spasmodic action of the leg-muscles occurred until a year later. He has never walked well since the attack of hemiplegia. The positions which the arm has assumed have varied at different times, but it usually retains one attitude for several months at a time. Sometimes the arm has been held in extension; at another time it has been flexed; indeed, the positions have been numerous. His general health improved and the speech became perfect.
Condition on examination Aug. 14, 1884: General health good, well grown for age. The nutrition of the affected side is good, but the left side of the face is markedly smaller than the right, although there is no paralysis. The position of the arm attracts immediate attention. The arm, hand, and fingers are in extreme extension, as shown in the cut, which is made from a photograph. The arm-muscles are tense and rigid. The fingers are continually in motion, sometimes flexed, sometimes extremely extended; then in a few moments they will be widely separated or distorted in some other way. The favorite [p. 459] position, however, seems to be with the fingers extended until bent backward, separated from each other, and the thumb adducted slightly. The patient is unable to bring the arm down by a voluntary effort, but when asked to put it by his side he pulls it down with the right hand, and keeps it down by sitting upon the hand. The muscles of the arm are hypertrophied, especially those of the upper arm and shoulder. The circumference of the left arm around the biceps is almost an inch greater than that of the right. The leg is stiff and the foot is usually inverted. Here also the position changes at different times. When he walks the stiffness increases and the foot is dragged. The speech is clear and distinct, and the intellect perfect. He goes to school, and is fully equal to or more advanced than boys of his age. There is no evidence of cardiac disease.

The patient's condition in Oct., 1885, had changed somewhat. The arm is in a different attitude. It is still extended, but is held down by the side or away from the body. At times the forearm is strongly supinated. There are still constant but slowly-changing movements of the fingers. One plan which the patient has of keeping the arm flexed is to put the forearm behind the back with the right hand, and it becomes locked there by the action of the extensors. By a strong effort of will he can slowly and with great difficulty open and shut the fingers, and can flex the forearm. The leg is in the same condition as before.
The resemblance between athetosis and post-paralytic chorea is very close. Most of the cases of the former disorder which have been reported have been of the hemiplegic type. In Case I. the disease came on after an attack of delirium tremens, which was followed by six weeks of unconsciousness. The first symptom the patient was capable of noticing was numbness of the right arm and leg. The involuntary movements came on later. This would look as if there had been some lesion involving the left hemisphere of the brain. It is stated that no paralysis existed when the case was examined by Hammond, but there may have been a slight hemiplegia which had passed away. In another case reported by the same author the peculiar movements were preceded by hemiplegia and aphasia.
Oulmont has written a complete essay on athetosis, and has collected therein all the literature of the subject.3 He sustains the view of the close connection between athetosis and post-paralytic chorea, but he [p. 460] considers that, although nearly allied, a difference does exist between the two affections. He believes this is most marked in the bilateral form of athetosis, for here the disorder is usually not preceded by paralysis, and it is not accompanied by disturbances of sensation.
3 Étude clinique sur l'Athétose, Paris, 1878.
Gowers4 has also collected a number of cases, some of which came under his own observation, and has written a valuable treatise on the subject.
4 Medico-Chirurgical Transactions, 2d Series, vol. xli.
PATHOLOGY.—The symptoms point to a brain lesion, probably in the gray matter, and a perverted condition of the nerve-cells which leads to over-action, either spontaneously or under the influence of a motor impulse. In most of the cases reported by Claye Shaw there was imbecility. Charcot found in three post-mortem examinations lesions in each instance in the posterior portion of the optic thalamus, the most posterior part of the caudate nucleus, and the most posterior part of the corona radiata. Gowers has made an autopsy in one case in which there was post-hemiplegic inco-ordination affecting the arm only, without the spasmodic fixation of the limb. In the brain was found but one lesion, and that was a cicatricial induration of the optic thalamus, extending across its centre beneath its upper surface, and approaching at its outer part, but not involving, the ascending white fibres of the crus. No secondary degeneration was found in the cord.
PROGNOSIS.—This is almost always unfavorable. In some cases the inco-ordination decreases and the spasm becomes less violent, but it seldom disappears altogether. One of Gowers's cases was benefited by treatment, and two of those related by Hammond were relieved.
TREATMENT.—Many remedies have been given without marked benefit. In Gowers's case there is no doubt that the decided improvement which took place was due to galvanism. The treatment lasted three months, and a descending galvanic current was used. The positive pole was put upon the nucha, and the negative on the over-acting muscles and on the hand and foot. One of Hammond's cases, as related above, was apparently cured by stretching the median nerve. A prolonged course of galvanism and some alterative, like mercury or chloride of gold and sodium, would seem to offer the best prospect of benefit.
SYNONYMS.—Rigidité musculaire avec impuissance de la volonté; Rigidité et hypertrophie musculaire; Myotomé congenitale.
In the year 1876, Thomsen,1 the medical officer of Kappeln, described a curious form of nervous disease which affected several members of his own family, himself included. It consisted of a tendency to cramp and limited spasm when a voluntary act was attempted, and a seeming and sudden loss of power. This condition disappeared after the performance of the act and its repetition. An attempt at walking would be attended by spastic rigidity of the flexor muscles of the lower extremities, by flexion of the thighs and legs at an angle of 120°, so that the patient often fell forward upon his knees. An attempt to arise from the chair was attended by the same difficulty, the person becoming utterly helpless. The arms and legs were most frequently affected, the trunk-muscles being usually exempt. In some cases the muscles supplied by cranial nerves were the seat of spasm, so that the patient could not close his mouth nor shut his eyes. Westphal, Erb, Peters, Schönfeld, Engel, and others have reported about eight cases in all, and in addition to the symptoms above referred to it was found that mental excitement and cold chiefly precipitated the seizure. The sphincters were never affected, and the general nervous functions were not impaired. The patients talked stiffly, and this was probably due to a spasmodic affection of the lips, tongue, and other articulating organs. The tendinous reflexes were normal, but irritation of the soles produced a peculiar cramp of the leg-flexors and bending of the knees. There is a species of muscular increase which resembles pseudo-hypertrophic paralysis.
1 Berliner klin. Woch., Mar. 12, 1883.
The malady seems to be of an hereditary nature, if we are to judge by Thomsen's cases. It begins early in life, and does not materially shorten the same. I have seen one case, a young child, which presented the main symptoms of, and was first mistaken for, pseudo-hypertrophic paralysis.
Westphal regards the affection as an “anomaly of muscular tonus;” others have shed no light upon its pathology.
I believe the condition to be an occasional feature of certain organic disorders, notably posterior spinal sclerosis, and there is a variety of paralysis agitans where there is no tremor which presents all the symptoms. The very rare nature of the malady and its peculiar [p. 462] expression render diagnosis easy. It possibly may be mistaken for pseudo-hypertrophic paralysis in young subjects, but in this latter disease we find electrical change in the muscles, and an absence of the tendon reflex. An examination of the enlarged muscles will not reveal fatty increase.
There is a form of spasm of the muscles supplied by the facial nerves which differs from ordinary tic douloureux by the fact that there is no pain in the former. The trouble may be one of a very limited nature, consisting of the involvement of a few fibres, or of limited groups of muscles, or of all the muscles of the side of the face. I never have seen a case of double spasm, though such undoubtedly exist.
The nature of the paroxysm is cumulative, and, as a rule, the attack increases until it reaches an acme of intensity, then quite suddenly ceases. It often begins by a slight drawing of the corner of the mouth, the levator anguli oris and other muscles in the neighborhood being the seat of chronic spasms. This limited spasmodic action is followed by further facial contractions. The orbicularis palpebrarum is often the sole seat of the convulsive movement, and this is common in excessive smokers.
As a rule, the trouble is peripheral and due to some reflex cause, such as cold, injury, bad teeth, which produces reflected irritation through the branches of the fifth nerve, or in rare cases it may be central or due to some bony or other pressure upon the nerve in its passage through the skull. In a recent case the trouble was of evident central origin, and I obtained a history of lightning pains in the lower extremities, some inco-ordination of muscles in both upper and lower extremities, and some paresis of the facial muscles. In this case the spasms involved all the muscles of the right side of the face, and recurred every few minutes. They had first appeared five or six years before I saw the patient, and had gained in frequency from two or three daily until within the past four months they occurred, as I have said, every few minutes. The other symptoms were of insignificant character compared to the spasms.
Of the large number of cases I have seen, many impressed me as being the result of a simple bad habit, yet moral or other measures did not avail much.
It is important to diagnose certain unusual forms of facial spasm from the petit mal of epilepsy, and careful observation will detect a transitory loss of consciousness in the latter. It is equally important to find a cause if any exists, and a careful examination of the state of the teeth, the integrity of vision, and the possible existence of aural disease should be made in all cases. In some cases over-use of the eyes, which may be defective in their power of accommodation, may precipitate blepharospasm. In other cases the act of masticating hard substances or taking very hot or cold fluids into the mouth may give rise to the spasm.
Hyoscyamine in repeated doses of from 1/200 to 1/25 grain of Merck's crystals does more in the way of relieving the spasms than any other drug of which I know. If this does no good, gelsemium cautiously used is often of great service. Local galvanic applications with currents of great intensity will form a valuable adjuvant. So far, I have never tried [p. 463] nerve-section or stretching in these cases, but recommend them as a dernier ressort.
SYNONYMS.—Wry neck, Rheumatismus colli, Obstipite, Cephaloxia.
Wry neck or torticollis consists essentially of a spasm of the sterno-cleido-mastoideus, though other muscles are nearly always involved: the result is a peculiar and striking distortion which is quite familiar. It consists in the drawing downward and backward of the head on the affected side, while the chin is pointed forward and upward to the other. The disease is presented in several forms. It may be a temporary disorder as the result of a rheumatic condition, disappearing rapidly, or occurs as an hysterical affection, or it may be a chronic and intractable nervous disease. We must also consider it from the standpoint of the form of distorted motility. In some cases there is simple tonic contraction, which may eventually result in tense contracture, shrinking, and tendinous hardness; and in others the attention of the physician is attracted by a species of tremor and agitation. Unlike the tremor of sclerosis, this is uninfluenced by the attempts of control upon the part of the patient, but is aggravated by fatigue and excitement. It rarely happens that both muscles are affected so that the head is drawn backward. Most of the cases are single, chronic, and progressive, and, though very slow in the onward march, are usually beyond the reach of remedies. The patient becomes greatly annoyed by his infirmity, and seeks every measure to overcome his unfortunate deformity. He commonly tries to hold his head or chin, pressing the latter downward, or, holding his cane against his head upon the dependent side, strives to keep it up. As a result, there is a sagging or drooping of the affected side of the body, so that one shoulder is lower than the other.
The disease, as a rule, begins in adult life, yet there are many young cases.2 Wilks calls attention to the fact that in these latter there is apt to be some facial asymmetry on the contracted side. One side of the head is smaller than the other, and one eye seems to be lower.
2 Diseases of the Nervous System, p. 454.
Most of the cases I have seen have been men, though I have met with many hysterical examples in young girls. The double torticollis (Newnham's salaam convulsion) usually affects children, and it is the rule to find associated strabismus and intellectual disturbance. In the adult cases there has usually been a history of hereditary neurotic influence and overwork.
Electrically, we find a susceptibility to both currents, and the reaction of degeneration may be detected in the affected muscles in old cases. The opposing muscles are usually the seat of diminished electrical excitability.
Torticollis may be due to peripheral or deep causes. Cold, reflex irritation, forced and uncomfortable positions, are to be mentioned among the former, and intracranial or vertebral disease as examples of the latter. The pathological explanation lies in a disorder of the motor fibres of the spinal accessory nerve. Any affection of the external branch will result in the condition above described.
[p. 464]In young cases the PROGNOSIS is good as a rule, though this is by no means invariably so, for sometimes the special symptoms are but forerunners of others of a more grave character. Hysterical torticollis is often instantly, or at least very readily, cured by electro-therapeutics and cauterization. A well-established adult case is almost hopeless and resists all ordinary treatment.
Many forms of TREATMENT have been recommended from time to time, and such drugs as the bromides, chloroform, conium, and hyoscyamine are suggested. The latter I believe to be the most serviceable remedy. Electricity has done good in either form, and vigorous faradization with the electric brush is earnestly recommended in hysterical, rheumatic, or functional cases. Some years ago I devised a method which in a number of cases has been of great service. I allude to the combined and simultaneous use of the galvanic and induced currents. A double electrode is applied to the back of the neck. This contains the anodal pole of the galvanic current and the cathodal of the faradic. The two other poles are placed—one, the galvanic cathode, over the origin of the affected muscle, the induced anodal pole over the weakened muscle which is not in spasm. I suppose in old cases the most valuable treatment is that of a surgical nature. I have twice seen the spinal accessory exsected with the result of a complete cure; and I think this is the only sure measure. H. B. Sands of this city has performed the operation quite successfully in other instances. Care should be taken not to operate in cases presenting other symptoms which suggest the remotest suspicion of organic cerebral disease, and the existence of unilaterally increased tendinous reflexes or tremor should be carefully looked for as contraindications.
Braces and apparatus are often worse than useless, increasing not only the patient's discomfort, but aggravating the malady.
(Εχλαμψις and λαμβω, “I shine,” brilliancy, flashes of light from the eyes.—Dunglison.)
DEFINITION.—A term used to express certain irregular convulsive attacks, as a rule due to eccentric irritation, uræmic poisoning, or like causes, and chiefly used in connection with the convulsions of infants.
This term has gradually been dropped in scientific medical literature, and many authors think it useless, believing the condition to be usually epileptoid. Nothnagel,3 who is more liberal than many other clinicians, says: “What is there now remaining of what was formerly eclampsia? Are we altogether justified in still retaining the name? We believe so, and are of the opinion that the title eclampsia should be reserved as the name of an independent affection, which, it is true, can at present be defined only by its clinical symptoms. We propose that the designation eclampsia should be made use of for those cases of epileptiform spasms which, independent of positive organic diseases, present themselves as an independent acute malady, and in which, so far as our present knowledge allows us to judge, the same processes arise generally in the way of reflex [p. 465] excitements, and the same mechanism in the establishment of the paroxysms comes into play, as in the epileptic seizure itself.”
3 Cyclopædia of the Practice of Med., Von Ziemssen, Am. ed., vol. xiv. pp. 301, 302.
If any distinction at all be made, it should be one founded upon the fact that epilepsy itself is usually an organic disease, or, more precisely, a disease which when established is dependent upon some disorganization, while eclampsia is used to express those seizures of a purely functional nature.
By far the greater number of eclamptic seizures are found among young children. There is no uniformity in their expression or return. Any eccentric irritation is apt to precipitate one or more attacks, and those forms of irritation dependent upon sensory disturbances of the mucous membrane are commonly present. The convulsions of teething belong to this class, as well as those in which gastric disorder plays a part; and in the first instance the cutting of the large teeth, and in the latter the presence of indigestion with diarrhœa, are quite commonly associated with the convulsion.
The high degree of irritability of the nervous system of children renders them peculiarly susceptible to causes which in after years would effect little or no disturbance; and this is especially true before the fifth year. West and Reynolds are of the opinion that convulsions occur in children as delirium in adults; in other words, they are the most common expression of neurotic instability.
Infantile convulsions are usually general, and neuro-spasms are not common, except when they are dependent upon neoplasm, ventricular dilatation, or local meningitis. It evidently takes very limited peripheral excitement to precipitate a general convulsion in the child, and a familiar example is the disturbance which may involve the peripheral branches of the fifth nerve in difficult dentition.
Eclamptic seizures occur at any time, and may be very slight: a trifling twitching may be all, or, on the other hand, the attack may consist of violent opisthotonos. There is great difficulty, of course, in getting anything from a young child as to its feelings before an attack, and I hardly think we are authorized in saying that there is any aura or ascertainable precursor. The history of a previous nervous state is, however, usually ascertainable, which is expressed by crying fits, peevishness, and great restlessness. Sometimes there is a disposition to sleep which almost amounts to stupor. The behavior of a child is often likened to that which marks the commencement of acute tubercular meningitis—night-terrors, grinding of the teeth, and flushing of the face. The first convulsions may be only partial, but in a short time their character becomes general, and they become exceedingly violent, and are sometimes fatal. The clinical features of an eclamptic seizure may in every respect resemble one of epilepsy, making allowance for the age of our patient.
The stage of pallor is perhaps more extended in the child.
Handfield Jones speaks of a form of eclampsia of hyperæmic causation in association with certain exanthemata. In children convalescing from scarlatina he observed the development of attacks which were relieved by carotid pressure and bleeding in subjects who presented anasarca and other indications of renal disease.
We are familiar enough with the convulsions of puerperal women, which, as a rule, though not always, are presented by subjects whose [p. 466] urine is albuminous. It can sometimes distinctly be traced to what must be regarded as uterine excitement. Just as chorea is often a feature of the pregnant state, so may convulsive seizures arise. The peculiarities of the epilepsy of pregnancy will, however, be elsewhere considered.
I shall purposely refrain from the consideration of those forms of symptomatic infantile convulsions which mark the occurrence of cerebral accidents or grave disease.
SYNONYMS.—Epilepsia; l'Épilepsie (Fr.); Fallsücht (Ger.); Epilessia (Ital.); Epilepsin fallendsot (Scand.); Falling sickness; Fainting sickness.
DEFINITION.—According to the most recent authorities, an epileptic attack is nothing more nor less than a discharge of nervous energy from an overexcited, or what may be called a dynamo-pregnant nerve-centre, or collection of centres, and the predominance of motor or sensory phenomena determines the extent and order of the parts involved. As a rule, an epileptic paroxysm is but a symptomatic expression of a complex derangement, and it is best to formulate our nomenclature with the idea, in the first place, of location; in the second, with reference to the prominence of motor or sensory expressions; and, finally, with regard to etiology.
HISTORY.—There is probably no nervous disease which has been more extensively written upon (even in ancient times) than that under consideration. We find references to it as early as the tenth century, when it figured in the text of Avicennes. Hippocrates called it ιερόν νοσεμα, or sacred malady, and πάθοϛ παιδήιον, or malady of children, believing that the attacks had their origin always in early infancy and never later. Plato and Aretæus advanced the theory that the disease sprang from a thirst for gold, and equally absurd and unreasonable explanations are found in the writings of the fathers of medicine. The older French writers were diligent investigators, but with them prevailed the tendency to explain the origin of the disease by mysticism, and among many it was supposed to bear some connection with the coming of St. John. The popular humoral theory of the malady originated by Mercurialis was afterward opposed by Averrhoes and Fernel, but even to this day it has devoted adherents. Bouchet and Causauvieilh maintained that the disease was inflammatory—a view that was vigorously combated by Bouillaud and Delasiauve. The theory of Broussais—which was and is the basis of the conclusions of modern investigators—is that it is dependent upon cerebral irritation. It is hardly necessary to refer to the many untenable and curious attempts that have been made to explain the pathology of the malady: suffice it to say that many of them were as extravagant as that of Vepfer, who considered the pineal gland to be the locus morbi of the affection—a conclusion in which Descartes coincided. Marshall Hall was the first writer to advance the theory of reflex irritation, [p. 468] believing that gastro-enteric or uterine irritation acted upon the brain. In later years Schroeder Van der Kolk, Reynolds, and others have written quite fully upon the part played by the medulla, while recently numerous French and German writers—among them Bourneville, Meynert, Sommers, and Tagges—have attached much importance to the discovery of a sclerosis of parts lying at the floor of the lateral ventricles.
Perhaps our knowledge of epilepsy has received its greatest impetus from the elaborate and exact researches of Hughlings-Jackson; and his observations, taken in connection with the recent work of the numerous students of localization, open up a new field of research, and, as matters stand, the future study of epilepsy must be fruitful in the extreme.
DIVISION.—It has been the custom to divide the epilepsies into epilepsia gravior and epilepsia mitior, the haut mal and petit mal of the French. These terms are in one way misleading, and only define differences in degree. The terms general and limited would much more properly express the forms of attack, and I shall use them as far as possible in the present article. A general epilepsy is one that corresponds with haut mal, in which there is an extensive convulsion, absolute loss of consciousness, and perversion of a widespread character. Limited epilepsy includes those forms in which there is a convulsion confined to a small group of muscles, and in which loss of consciousness plays an unimportant part. Under this latter head belongs the form known as petit mal and those monospasms which depend upon a cortical irritative lesion. There are other divisions which partake of the nature of one or the other, and are unilateral and dependent upon the destructive discharge of a motor centre. Under this head may be placed the epilepsie partielle of the French or the hemi-epilepsy or Jacksonian epilepsy of the English. There are also irregular or aborted attacks—the so-called masked epilepsy—and lastly the sensory varieties.
ETIOLOGY.—It cannot be denied that heredity plays the most important part in the genesis of epilepsy. Nearly one-half of my own cases when carefully investigated were clearly traceable to some inherited predisposition. Insanity, epilepsy, and phthisis in ancestral history stamp their constitutional imprint upon the unfortunate descendant, and the history of ten cases from my notebook (see Table) will show the extent of saturation that may exist in paternal or maternal branches and the evolution of the disease in male and female subjects. The statistics of other writers, though not showing quite so large a proportion of cases with hereditary history as my own, are quite significant. Gowers found that in “1218 cases, 429, or 35 per cent., presented evidence of neurotic inheritance.” Echeverria estimated the proportion of hereditary cases at 28 per cent., while Reynolds fixes it at 31 per cent. Of 980 cases, the notes of which I have examined, many of whom have been under my personal care, 435 presented a family history of insanity, phthisis, epilepsy, cerebral apoplexy, tumor, or some lesser neurosis. So far as the history of hereditary influence is known, it appears that females are more apt to present this form of epilepsy than males, and, according to Gowers's as well as my own investigations, the transmission comes from the mother's side more frequently than the other. So far as my own inquiries have gone, I find insanity more often among the progenitors of the epileptic than any other nervous disease, and in many cases phthisis. I am inclined, therefore, to give greater weight to this relationship than Nothnagel and others. Anstie, Bastian, Savage, and other careful clinicians have pointed out not only the close connection between phthisis and epilepsy, but between the former disease and migraine; and no one who has seen much of epilepsy can fail to be impressed with the frequent association of migraine with the more serious convulsive affection of which it is quite often the precursor. Perhaps the fact that phthisis was found so often—in 230 of my 980 cases—may be due to the fact that many of the patients were of the lower classes and among the Irish, who in this country are so frequently phthisical.
[p. 469]| Sex. | Paternal Ancestry. | Maternal Ancestry. | Brothers. | Sisters. | Remarks. | ||||||||
| Father. | Grand- father. |
Uncles. | Grand- mother. |
Aunts. | Mother. | Grand- mother. |
Uncles. | Grand- father. |
Aunts. | ||||
| F. | Died insane. | Suicide; probably insane. | Eccentric. | . . . | . . . | Died of cerebral hemorrhage. | Eccentric; died of cerebral hemorrhage. | Drunkard. | . . . | . . . | One a dipsomaniac; one in good health. | One epileptic. | A history of criminal proclivities. |
| M. | Alive. | Cerebral hemorrhages. | Insane. | . . . | . . . | Phthisis. | . . . | One died of phthisis. | . . . | Phthisis. | One brother has infantile paralysis. | Two sisters died of organic disease of the brain, one of cerebro-spinal sclerosis. | Peculiar cranium. |
| F. | Alive in third stage of post-sp. sclerosis. | Phthisis. | . . . | . . . | Phthisis. | Alive. | Not known. | . . . | Cerebral embolism. | . . . | One brother has infantile paralysis. | . . . | |
| M. | Died of phthisis. | Not known. | Phthisis. | . . . | Epileptic. | Migraine. | Phthisis. | . . . | . . . | . . . | No brothers. | No sisters. | |
| M. | Congestive headaches. | Cerebral hemorrhage. | Insane. | . . . | Migraine. | Phthisis. | . . . | . . . | . . . | One died of phthsis; one hemiplegic. | No brothers. | No sisters. | Peculiar cranium. |
| M. | Alive. | Insane. | . . . | . . . | Insane. | Phthisis. | . . . | Phthisis. | . . . | . . . | Eight brothers and sisters. | One died of epilepsy, and cerebral tumor was found; one paralyzed. | |
| M. | A confirmed drunkard. | Died of embolism and softening at 76. | . . . | . . . | Insane. | Phthisis. | Died in childbirth. | . . . | . . . | Phthisis. | . . . | . . . | Criminal proclivities. |
| M. | Phthisis. | Eccentric. | One phthisis; one cerebral tumor. | . . . | . . . | Migraine. | . . . | . . . | . . . | . . . | One brother died of secondary tubercular meningitis, the other in an asylum. | . . . | Child of this parent was choreic. |
| M. | A dipsomaniac and eccentric person. | A genius. | One died insane. | Cerebral hemorrhage. | None. | Peculiar and eccentric. | Migraine. | Peculiar character. | Insane and committed suicide. | . . . | Several brothers unaffected. | No sisters. | Criminal proclivities. |
| M. | Most eccentric; a somnambulist. | . . . | . . . | . . . | Migraine. | Epileptic. | . . . | . . . | . . . | Migraine. | No brothers. | No sisters. | |
In [p. 470] many idiopathic cases we find vices of cranial conformation, bodily asymmetry, and a history of early congenital syphilis. Laségue lays great stress upon cranial malformation, and goes so far as to say that all epilepsies not dependent upon some osseous trouble, either developmental or traumatic, are not epilepsies at all. Such epilepsy, which owes its origin to cranial asymmetry, rarely develops after the eighteenth year. The head is most often dolichocephalic or brachycephalic, and there is facial asymmetry. Laségue concludes that all the convulsions are identical; that it is not hereditary; that the attacks are always matutinal. It seems to me that Laségue's conclusions in regard to the non-existence of epilepsies from other causes are rather too arbitrary in view of the large amount of evidence to the contrary. In others, a very few, we find an apparent history of heredity explained by forceps-pressure during delivery.
So far as age and sex are concerned, and their predisposing influence, we find that by far the greatest number of cases begin before the twentieth year. This is the experience of Gowers, of Hammond, and of many others. Of my own 980 collected cases in which the beginning of the disease was known, there were—
| Females. | Males. | Total. | |
| Under 10 | 103 | 95 | 198 |
| Between 10 and 20 | 171 | 97 | 268 |
| Between 20 and 30 | 145 | 92 | 237 |
| Between 30 and 50 | 81 | 136 | 217 |
| Over 50 | 11 | 49 | 60 |
| 511 | 469 | 980 |
Of 1288 cases collected by nine French authorities, in 486, or over one-third, the disease began between the tenth and twentieth years. In Gowers's 1450 cases we find the following showing:
| Cases. | |
| Under 10 | 422 |
| From 10 to 19 | 665 |
| From 20 to 29 | 224 |
| From 30 to 39 | 87 |
| From 40 to 49 | 31 |
| From 50 to 59 | 16 |
| From 60 to 69 | 4 |
| From 70 to 79 | 1 |
In 29 per cent. of these cases the disease therefore began before the tenth year.
As to sex, it appears that females are much more subject to the disease than males, but this is not true at any age. Epileptics under ten are more apt to be girls, but the proportion is nearly equal: between ten and twenty the proportion of females is undeniably greater. In adult cases we find that pure epilepsy (excluding hysteria) is much more often a disease of males than females.
[p. 471]In the hereditary form the disease in the great proportion of cases begins before the twentieth year; and, so far as my experience goes, this kind of the disease makes its appearance at a very early age. The part played by particular predisposing influences appears to be well defined. The children of syphilitic parents develop the disease at a more advanced age than when alcoholism is found to exist. In adult males, when the disease develops late in life, it is almost always possible to find syphilitic or coarse brain diseases, while among women the history of antecedent migraine or menstrual derangement is nearly always present, and the convulsions in a very large number of instances have a hysteroid character.
The exciting CAUSES of the disease are quite numerous. Traumatism is a frequent and important etiological factor, and the head-injuries may be recent or remote. It is quite common to find old fractures, with depressions which have existed for years without any seeming bad effects, suddenly lighting up convulsions under the influence of some new excitement. Under such circumstances the depressed bone is quite apt to give rise to symptoms suggestive of meningeal irritation and inflammation, so that the diagnosis is comparatively easy. Several observers have called attention to epilepsy which has been undoubtedly due to cicatrices not only of the scalp, but elsewhere, and these may or not be found in association with osseous lesions. The literature of the subject is replete with curious cases which go to show that epilepsy may occur from a few days to many years—even twenty—after the initial head-injury. Unsuspected cortical pressure, the inner table being alone depressed, is common; in fact, the cases in which the most serious mischief is done seem to be those where the only external evidence of violence is the contused scalp. As a consequence of such injury we may have exostoses developed.
The influence of syphilis in the production of epilepsy is one of very great importance. Not only has specific epilepsy characteristics of its own, but its origin may be distinctly traced to syphilitic infection. Cases dependent upon gross cerebral disease, such as meningitis or gumma, are excluded from consideration, but it is conceded by all syphilographers that an epilepsy may mark the second stage of the disorder, and its pathological dependence is probably a simple vascular disturbance which cannot be determined after death. So-called specific epilepsy may be congenital.
Orwin1 mentions as a cause the influence of prolonged lactation. In several cases I have seen a metrorrhagia, or a loss of blood from hemorrhoids has been followed by a readily curable epilepsy.
1 Prov. Med. and Surg. Journal, London, 1862, v. 48.
As eccentric irritating causes may be mentioned intestinal worms, but I am convinced that it is too often the fashion to ascribe convulsions in children to intestinal parasites: in very young children, however, there are frequent examples of the disease in which the attacks are precipitated by worms. The fits are usually very severe, and are not regular in their appearance, occurring at night-time more often than during the day, and, though they usually disappear when the bowels are cleared of their unpleasant occupants, may recur when once initiated, even though anthelmintics of the most powerful kind are employed. Gall-stones are mentioned by Ross as an eccentric cause of the disease, but I have never witnessed a case of this nature.
[p. 472]Sudden terror, fright of all kinds, morbid example, and other psychic causes are detailed, and undoubtedly all have more or less influence. Hysteroid attacks are notably precipitated by these mental causes, and all forms of the disease are greatly modified by abnormal exercise of the mind.
A number of writers, among them Baly2 and Booth,3 have called attention to cases of the disease dependent upon carious teeth. I have seen but one such case, where a wisdom tooth produced so much violent inflammatory action that middle-ear disease followed, and with it subsequent extension to the brain took place.
2 London Med. Gazette, 1851, xlviii. 534-540.
3 Am. Journ. of the Med. Sciences, 1870, N. S. lix. 278.
In rare cases the administration of anæsthetics is followed by epilepsy, and Gowers alludes to a case in which convulsions were due to the inhalation of nitrous oxide gas.
Concussion of the brain as the result of railroad injury or falls may give rise to a progressive epilepsy which is usually of serious character.
Reflex causes play a prominent part in many instances, though I am inclined to think that their importance has been greatly exaggerated. This is especially true of so-called uterine epilepsy. It cannot be doubted that difficult menstruation, ovarian neuralgia, etc. are found in connection with epilepsy, but whether as a cause or effect it is not always possible to say. The fact that in some women we find accès at periods identical with menstruation would point to a very close relationship. Carstens4 reports a case due undoubtedly to stenosis of the cervix; Cohen,5 an example in which there was a uterine fibroid; and others have spoken of erosion of the cervix, etc. as possible explanation of the seizure.
4 Detroit Lancet (8), 1880, N. S. iii. 153.
5 Wochenschrift f. d. ges. Heilkunde, Berlin, 1839, vii. 648, 673.
The toxic forms of epilepsy hardly need discussion in this article. Metallic poisoning, which gives rise to a veritable plumbic encephalopathy, is rather the cause of a symptomatic than generic epilepsy. Curious cases of epilepsies which have followed the use of oil of tansy (Mitchell6), ergot, absinthe (Magnan7), and various drugs show that occasionally their mode of origin may explain the convulsive seizure. Alcoholic epilepsy I do not regard as being the rare affection some authors consider it. In cases of prolonged saturation, where perhaps there are no other symptoms of chronic alcoholism, I have found it perhaps associated with the trance state (cataleptoid) or appearing in the psychic form.
6 Cincinnati Lancet and Clinic, 1881, N. S. vi. 479.
7 Recherches sur les Centres nerveux, Paris, 1876.
In old persons I have found gout to have an undoubted influence in producing the disease, there being a spasm of the cerebral vessels which usually betokens a condition of uric-acid saturation. In these cases the painful symptoms were not decided. Such epilepsies have quite often preceded serious evidence of arterial degeneration.
Malarial epilepsy is rare: Jacobi8 reports a case and Payne9 another. A young man was brought to me last year who had lived for many years in a part of Pennsylvania which was exceedingly malarious. His attacks, which were more or less periodic, were violent, and his convulsions were [p. 473] general and attended by very great preliminary rise of temperature and intense congestion of the face and head. The patient was unusually somnolent, and between the paroxysms frequently suffered from facial neuralgia. The influences of change of habitation and quinine determined the correctness of my diagnosis.
8 Hospital Gazette, New York, 1879, v. 41-43.
9 Indian Ann. Med. Sci., Calcutta, 1860-61, vii. 597 et seq.
Day10 and Kerr11 have both ascribed epilepsies seen by them to hepatic congestion.
10 Clin. Histories, etc., London, 1866, 143-145.
11 Med. Times and Gazette, London, 1871, i. 568.
The important etiological relation of the exanthemata to epilepsy has been the subject of much attention. The books are full of cases which owe their origin not only to scarlet fever and measles, but to whooping cough, diphtheria, and the various zymotic fevers. In 35 cases tabulated by Gowers12 (p. 28) no less than 19 were due to scarlet fever, while the first fit followed measles in 9 cases. So far as my individual experience goes, I have in 23 cases found epilepsy to be the result of scarlet fever, and this form of the disease was often associated with other manifestations of coarse brain trouble. Cerebro-spinal meningitis was the undoubted cause of epilepsy in 6 cases I examined. It is probable that just as smallpox acts upon the nervous centres, so does scarlet fever, and I agree with Gowers that the convulsions that may begin during or just after the fever are not always due to uræmia. Bright's disease may give rise to an epilepsy, but this can hardly be regarded as a distinct affection.
12 Op. cit.
There are many cases, especially in adults, which grow out of a prolonged depletion of the brain—a continued cerebral anæmia. Among these cases are some which depend upon pressure upon the great vessels of the neck, and some due to debilitating disease of a general character. Schulz13 has seen a case which followed compression of the jugular vein, and enlarged cervical glands have in other cases acted as mechanical agents. Hammond alludes to the influence of prolonged general anæmia in the production of epilepsy.
13 Cor. Bl. Deutsches Gesellsch. f. Psych., Neuwied, 1855, ii. 35.
While I do not place much reliance on the claims that have been made regarding the frequent dependence of the disease upon preputial irritation, or that it may arise from phymosis or urethral stricture, it cannot be denied that some cases have originated in difficulties of the kind, and especially the former. Simmons14 reports a case of attachment of the prepuce to the glans in which a cure followed separation. Disease of the testicles in certain cases plays a part in its genesis, and Liégey15 details an epilepsy clearly due to testicular pressure. Some years ago I saw a case in which the pressure of an improperly applied truss, I am now convinced, had much to do with the development of the convulsions. The alleged sexual causes are many, and some of them are very doubtful. A fanciful continental writer, Montmeja,16 believes that sodomy explained the appearance of the disease in one of his patients.
14 Am. Journ. Med. Sci., 1880, N. S. lxxix. 444.
15 Gaz. méd. du Strasbourg, 1856, xvi. 105-107.
16 Rev. Photo. des Hôpitaux de Paris, 1873, v. 229-232.
The existence of vesical calculi as an exciting cause cannot be disregarded, and, while rare, the observations of Duncan,17 Muscroft,18 and one [p. 474] or two others have shown that the removal of a stone was followed by a cure of the epilepsy.
17 Ed. Med. Journal, 1868-69, xiv. 140.
18 Arch. Sci. and Pract. Med. and Surg., 1873, 1360.
Masturbation is a popular etiological factor. I really do not believe, even in face of the numerous alleged cases that have been recorded, that the habit of self-abuse often results in genuine epilepsy. So far as my experience goes, onanism is practised by epileptics as well as by healthy boys, and when indulged in to excess is due to the congenital moral deficiency which is so common, especially in hereditary cases. In rare examples the frequently-repeated act may give rise to a form of the disease of the nature of petit mal.
Gastric disorders have attracted much attention, especially from Paget, who speaks of a gastric epilepsy and reports cases. While I do not believe in the sole etiological influence of digestive derangement, I have too often witnessed examples in which disorders of this kind markedly influenced the precipitation of attacks and the duration of the disorder.
Occasional cases of peripheral origin have been from time to time presented, and go to support in some measure the pathological views of Brown-Séquard. Among observers who have brought forward cases besides those referred to on a previous page are Lande,19 who reported a case of epilepsy dependent upon injury of the right median nerve, and Short,20 in whose case a neuroma explained the cause of the convulsions. Billroth,21 Garnier,22 Brown-Séquard,23 and Raymond24 have brought forward cases where injury of the sciatic nerve was the origin of the trouble, and in more than one instance a cure was effected by excision. It seems strange that a bone dislocation should have anything to do with the genesis of epilepsy, yet in one case reported a severe dislocation at the shoulder-joint explained the appearance of the attacks, and reduction was speedily followed by cure.
19 Mém. et Bull. Soc. de Méd. et Chir. de Bordeaux, 1878, i. 56-65.
20 Med. Essays and Observation Soc., Edin., 1737, iv. 416.
21 Archiv f. klin. Chir., Berlin, 1872, xiii. 379-395.
22 Union médicale de Paris, 1872, 3d S., xiii. 656-658.
23 New York Medical Record, 1872, vii. 472.
24 Rev. méd. de Limoges, 1869-72, iii. 102-105.
I have seen several cases where disease of the internal ear or injury of the temporal bone gave rise to the most obstinate and violent epilepsies. Westmoreland25 and others report such cases, but more often the epilepsy is only symptomatic of pachymeningitis or abscess. Some years ago I presented26 a case of genuine epilepsy in which the seizure was produced at will by irritating the meatus auditorius. By simply blowing into the ear the same effect would be produced. Since then Blake and others have related examples. Quite lately a writer in Brain has collected other cases of this species of auditory epilepsy. A year or so since I examined a patient in whom not only hemi-epilepsy, but other unilateral symptoms, followed erosion of a large part of the mastoid and petrous portion of the temporal bone as the result of a bullet wound.
25 Atlanta Med. and Surg. Journal, 1876-77, xiv. 717-719.
26 New York Medical Record, 1878, xiii. 107-109.
The influence of climate and varying barometric pressure has been considered by Delasiauve. His conclusion was that the attacks were much more common during the season of the year when the prevailing winds were from the north-west, north, or south-west.
[p. 475]PRODROMATA.—There are various minor disturbances of sensation and motion which may not amount to the dignity of an epileptic attack. These may be so fugacious as to escape the attention of the persons in whose company the patient may happen to be, or he himself may be unaware of any disordered state of feeling. They may precede a severe paroxysm, when they are known as warnings or auræ. The term aura was originally applied to the familiar premonitory sensation which is so often likened by the subject to the blowing of wind over the skin, from whence it receives its name, but it has come to be applied to all primary indications of a fit. Such auræ may be sensory or motor—in the preponderance of cases the former, for motor precursors are quite rare, and when they occur are most likely to be but one stage, though a slight one, of the convulsion itself. There is no general rule about the occurrence of an aura, but, so far as my experience goes, there is great constancy in the character of the warning in each particular case. The sensory disturbance may vary from a vague feeling of confusion to a well-marked sensation. In many instances the patient speaks of an indescribable mental disturbance, which may precede the attack and last anywhere from a few minutes to several hours. This confusional state or psychical aura is most protean in its expression. It may simply be a heavy feeling, a feeling of tension, a sleepy feeling; a restlessness which is manifested by the patient changing his position frequently or wandering forth into the streets; an irritability of temper which often lasts twenty-four hours or more, and during the display of which he rebukes those who may be solicitous about him, or wantonly destroys articles of furniture, or vents his spleen upon inoffensive persons. I have had epileptic children under my charge who were wont to bite their little brothers and sisters or their nurses. A feeling of terror sometimes precedes the attack, and very often there is a sense of impending danger which has no basis whatever, and with it is associated a depth of depression which is very painful. In other cases the patient manifests a strange exhilaration, which may precede the occurrence of the attack for a period of from one or two hours to two or three days; and this is made manifest by great loquacity and a lively play of spirits. It is not rare to find errors in the speech as indications of an approaching attack. A minor degree of aphasia, slowness of speech, or anarthria betrays occasionally the preparatory state which is the precursor of a severe convulsion. By far the most common warnings, however, consist of disorders of the special senses, and generally these are visual. From an inspection of my notes I find that the patients saw colored lights, rings of fire, bright objects, dark spots, luminous clouds, a flood of light, sparks, stars, bright balls, lights which approached them, lights which receded, fireworks, and all became dark. While many were unable to define the color perceived, I found among those who were positive that red was the color most frequently seen, while blue came next; and this is a conclusion which I believe is accepted by Jackson and others who have analyzed their cases.
Hemiopia and diplopia in rare cases precede the major attacks, and are sometimes associated with distal pain and anæsthesia and with supraorbital pain as well.27 Among these ocular warnings we find constriction of the visual field to be often present, especially in cases where there is a [p. 476] history of migraine. Vague disorders of hearing, which may even amount to the dignity of hallucination, are complained of by some persons. There may be simply roaring in the ears or a sound of bells, and in one instance my patient declared that he heard whisperings at the time of the seizure. Some patients smell smoke or other foul odors, and in exceptional instances the odor of some particular flower or of some aromatic substance, such as camphor, turpentine, or tar, is perceived by the epileptic; and these are probably psychical.28 Sometimes there is a feeling of great suffocation, constriction of the chest or of the throat, palpitation, or vertigo.
27 See Sensory Epilepsy.
28 For curious examples of this kind consult Sir Charles Bell's Nervous System of the Human Body.
There are disorders of cutaneous sensation of great diversity of character, but those auræ which are of the most constant occurrence are the epigastric, which consist of a vague sensation starting below the sternum and ascending, its arrival at the throat being coincident with the commencement of the fit, and the patient very often likens its culmination to the violent grasp of a strong hand. So, too, we find crawling sensations starting in the extremities and running up to the trunk. These have been compared to the contact of insects in motion or to the blowing of wind over the surface. There may be tingling in one or two fingers or the whole hand, and such sensations may be unilateral or bilateral. It is quite common for the sensory warning to begin in the hand and foot of one side and to run up to the knee and elbow. Sometimes the tongue becomes hyperæsthetic, and I have frequently found that the gums became exquisitely tender just before the attack. According to Gowers, 17 per cent. of his cases began with unilateral peripheral auræ, but I think this is too small a proportion, for, so far as I have observed, at least 30 per cent. of all my cases in which any auræ at all could be ascertained presented the history of a one-sided warning, beginning most often in the right hand. Gowers says that in three-fourths of his cases in which the attack began in the hand consciousness was lost before the seizure extended beyond the arm, while in the others it extended much farther before the actual fit was precipitated. In Gowers's cases he rarely found that unilateral auræ were associated with other warnings; and his experience, which is like my own, goes to prove that unilateral sensory auræ and one-sided initial motor expressions go together, and very often indicate gross organic disease. In some cases there may be for several days a decided unilateral or general muscular weakness or recurring chronic spasms which may be frequently repeated. In aborted or irregular attacks there are also peculiar motor symptoms, to which reference will be made later on.
In two or three patients I have found that the attack was immediately preceded by a profuse discharge of saliva, and in one case the patient had frequently bleeding from the nose. Several authors have called attention to certain local vaso-motor disturbances which are expressed by limited patches of cutaneous hyperæmia or anæmia, so that the fingers—or, in fact, the whole hand—may either be swollen and of a dusky-red color, or, contrariwise, there may be blanching and an apparent diminution in size.
Sometimes the patient immediately before the attack makes more or less automatic movements, pressing his hands to his head, clasping his breast, [p. 477] or clutching at some imaginary object, and after this he loses consciousness and falls to the ground. In some irregular cases the patient runs aimlessly for some distance or describes a circle, and after a variable time, which rarely exceeds a minute or two, the actual fit begins. Here are two examples:
Case I.—Boy aged fifteen, has been subject to somnambulism; attacks began two years ago. He frequently when sitting at table rises suddenly, and runs either around the room or out into the street if possible. In thirty seconds or so he falls to the ground in a convulsion. Always falls backward in opisthotonos.
Case II.—Man aged thirty-four. Attacks always begin by stage of violent temper. While unconscious he runs about office, striking all who try to restrain him; finally falls to the floor. Convulsions, when they occur, are always severe. Sometimes running attack is the sole feature.
This disposition to run is no less remarkable than another queer prodroma I have seen in several patients, who began to take off their clothing when first seized, no matter where they were or under what circumstances. This is not, as has been suggested, the remains of a half-formed idea that they must seek their beds because of their impending trouble, but it is a much less complex mental act, and the several patients I have seen were fully unconscious when they did this, and were in places where there was no bed within reach. Equally curious mental precursors of the attack have come to my notice, and these I will detail subsequently.
SYMPTOMATOLOGY.—The Light Attack.—The epileptic attack may, as I have said, be scarcely perceptible to those about the patient, or may consist simply of a momentary loss of consciousness and very feeble convulsive movements. Reynolds has described two forms: (1) That without evident spasm; (2) that with evident spasm. Such seizures are always fugacious, and consist merely in some transient loss of consciousness and very little or no convulsive movement. The tonic spasms prevail, if any, and the disorder of motility may often consist simply in the arrest of some act in the performance of which the patient is engaged. While playing the piano the patient's hands may for a moment remain suspended over the keys he is about to strike; if eating, the hand which holds the fork may be arrested between the plate and his mouth. The attack consists sometimes in the rolling upward of the eyeballs, or when crossing the room the patient may stop, remaining quiet for an instant. Temporary unconsciousness, shown by cessation of conversation, by change of color, and absence of intelligent expression, accompanies the other trouble. In a well-marked attack of petit mal the patient may move his lips convulsively, and remain otherwise quiet, but bereft of consciousness, for one or two minutes.
The patient sometimes loses himself and loses the thread of the conversation, repeating what he has just said or showing his want of appreciation of what his companion has said. To this light grade belongs the case reported by Jackson of the individual who blew his nose upon a piece of paper and gave the conductor £2 10s. instead of twopence halfpenny.
The Major Attack.—An attack of epilepsy of the familiar severe form may or not follow an aura. The first intimation to the bystander may be a noise made by the patient, which is either a loud, startling, wild cry, or a gurgling groan due to compression of the thorax and the [p. 478] forcible escape of wind through the vocal cords. There are three stages of the attack: (1) The stage of tonic convulsion; (2) the stage of clonic convulsion; (3) the reactionary stage.
The first stage of the attack is symptomatized by tonic spasms, which may be local or general, usually the latter. It is very often unrecognized, for its duration may be so short that it is lost in the stage of clonic spasms, which is much more protracted. There is usually unilateral seizure, the muscles of the face being primarily involved, then those of the hand and upper extremity, and then those of the lower extremity; and finally there is a general involvement, so that the patient may be in a position of opisthotonos. In some cases there is strong tonic contraction to one side, or pleurosthotonos. The notes of a case which illustrates the beginning and development of convulsion with reference to the parts involved, which I observed carefully, are the following:
Bindewald: Epileptic attack observed at hospital for paralyzed and epileptic, Sunday, Mar. 12, 1882:
1. Long, shrill cry which attracted my attention. It probably lasted five seconds. At same time patient threw up arms and became unconscious, and fell to floor. Nurses ran to him and placed him upon bed.
2. Tonic convulsions began by fine twitchings at right corner of mouth. These became gross, and were separated by succeeding long intervals. Eyes directed to left side, face pale.
3. In twenty seconds twitching began in right hand and arm, which were rigidly flexed (five seconds); then leg and foot of right side became agitated, the face meanwhile changing in color successively from red-gray to purple; lips purple, ears livid and purple, edges white; eyes still turned to the left, pupils dilated, eyes widely open; breathing stertorous and irregular.
4. General convulsions of right side.
5. Head suddenly twisted to left side; position of eyes the same. Chin drawn down, movements moderated; still livid. A fit of coughing and expectoration of much frothy mucus. Left side, with exception of head, not implicated. Whole attack lasted about one minute and thirty-five seconds. Deep sleep afterward, lasting forty-five minutes.
This attack was one of many in a confirmed epileptic, and is a fair example of those commonly met with, though not as general as we sometimes find. In most cases the attack appears to be very much longer than it usually is, and the phenomena noted above, which seemed to occupy a considerable space of time, really lasted but little more than a minute and a half. Axenfeld and Beau fix the average period of the attack as follows: “Duration of the complete attack, which Beau divides into four phases: first stage, tetanic stage, five to thirty seconds; second stage, clonic convulsions, from one to two minutes; third stage, stage of stupor, three to eight minutes; fourth stage, return of sensibility and intelligence. It is not complete until the end of from ten to thirty minutes.”
To be more explicit, the manifestation of an ordinary epileptic attack of the more severe kind is very much like this: Usually without any warning to those about the patient he utters a shrill, peculiar cry of a character never to be forgotten if once heard, and then, perhaps throwing up his hands, he falls to the ground rigid and contorted. His body may [p. 479] be arched laterally or antero-posteriorly, his legs are thrown out, his forearms flexed, and his fists doubled, the thumbs being beneath the other fingers. His face may be for a moment flushed, but the color recedes, and it assumes a dusky-bluish tint, the lips being ashy-gray. The eyes are usually open, and the balls are rolled up and the pupils widely dilated. The breathing may for a moment be suspended, but it soon quickens, and becomes labored and noisy, and the pulse grows hard and full. The tonic contractions are succeeded in a very short time by more or less violent clonic contractions, which increase in violence and rapidity; the jaws work and the lips are covered with foam, which is blown in and out by the rapid inspirations and expirations. It may be tinged with blood in the severe attack if the tongue is bitten, which is by no means an uncommon accident. The teeth are sometimes firmly set and the jaws locked. The head is usually drawn to one side in the first stage, but afterward may be rolled from side to side. The movements are now more or less general, and occasionally the agitation is so great that the patient throws himself from the bed on which he may be lying. The face grows more pale, or rather more livid, and toward the end of this stage there may be a puffiness and congestion such as are seen in partially asphyxiated individuals, for this alteration in color is due to dyspnœa and consequent imperfect oxidation. The patient may defecate or pass his urine unconsciously, and sometimes we find seminal emission. The movements, after a period varying from ten seconds to a minute or two, become less violent, and he may talk in a silly manner, as a person does who is recovering from profound ether unconsciousness; or deeply sigh, and he is restless. The pulse is now much weaker and more rapid, and may be irregular. The color returns to the face, the patient closes his eyes, and the body is covered with profuse perspiration. The fingers are unlocked and every evidence of spasmodic movement disappears. He falls asleep, and remains so for several hours, awaking with a confused feeling, headache, and no remembrance of the attack, and is only reminded that something has happened by his wounded tongue or lips, the bruises he has received, or by the information of friends. He looks jaded and tired, and is indisposed to exert himself for several days if the attack has been at all severe. The transition from the attack to the normal state is not always the same. Some patients do not sleep at all, but after being dazed go about their occupation. This is even true occasionally of the severe form of disease.
The usual termination of the attack is, however, by sleep preceded by a period of confusion. The patient, after coming out of the clonic stage, mutters incoherently. He is apt to pass large quantities of wind from his bowels, or vomits. This is attended by a subsidence of the spasmodic movements, and perhaps by oscillation of the eyeballs. The pulse loses its rapid, hard character, and the reaction brings with it diminished frequency of respiration and the evidence of exhaustion.
Special Symptoms.—The eyes are, as a rule, open, and, there being spasmodic movement of the ocular muscles, we find that the balls are either rolled up or directed away from the side in which the spasms begin. This is especially true in those epilepsies due to cortical disease, and the same law of conjugate deviation laid down by Bourneville may be remembered.
[p. 480]The pupils are dilated pretty much throughout the fit, though they may vary, and a transient contraction may occur at the commencement of the first stage. During the clonic stage, especially toward the end, they not infrequently undergo a species of oscillation. The interparoxysmal state is revealed by a very great mobility of the pupil, which has been observed by Gray and others. Gray is disposed to consider it a diagnostic indication of value, but so far I have found it only in two-thirds of my cases. Dilatation of the pupil I believe to be a very constant feature of epilepsy.
The ophthalmoscope reveals in certain cases an abnormal increase in the circulation at the fundus, in others a very decided emptiness of the retinal vessels. Jackson is disposed to consider that certain visual auræ depend upon spasm of the arterioles in this location. Loring, whose opportunities for research have been very great, is not disposed to attach much importance to the ophthalmoscopic appearances, at least during the periods between the fits.
The pulse of the epileptic between the paroxysms is small and irritable. Voisin has found the following changes: “Two or three seconds before the attack it becomes rapid, sharp, and the sphygmographic curves are higher, rounded, and nearer together. When the attack begins we see five or six little undulations in the course of the ascending line, and the curves are higher and more accentuated. Several minutes after the attack there is dicrotism, and the line of descent is very sharp, the angle with the ascending being quite acute. This form of pulse lasts an hour or half hour after the attack. There is in some cases great irregularity, with paroxysms of cardiac pain resembling angina pectoris. There is occasionally epistaxis or more marked hemorrhages.” Parrot speaks of hemorrhages from the eyes and ears, and occasionally the cerebral congestion is so great as to result in cerebral hemorrhage in old subjects.
The temperature is usually lowered before the attack, but the surface temperature is increased during or after the second stage.
Cutaneous sensibility is often very much disturbed. Spots of hyperæsthesia and anæsthesia are sometimes left after the attack. The scalp is not infrequently exceedingly tender. The sensory troubles have been alluded to as prodromata of the ordinary motor attack. Some attacks of the sensory variety in which psychical excitement plays a part are characterized by unilateral and persistent formications.
A consequence of some epileptic paroxysms is the appearance of petechiæ, chiefly upon the face, neck, and upper extremities. The skin of old epileptics is harsh, cold, and rough, and the face is apt to be studded with spots of acne even when the patient is not taking the bromides. The hair is stiff and dry, and the ears and tip of the nose are apt to be the seats of a passive and old hyperæmia.
The urine of epileptics is apt to contain evidence of muscular waste, and an increase in the amount of earthy phosphates as well. Zapolsky found, however, that immediately after the attack there was diminution in the quantity of the phosphates. The occurrence of glycosuria has been noted by numerous clinicians. De Renzi29 has published an interesting article. I have seen no less than six well-marked cases within two years in which constant glycosuria was a feature of the disease, but in two of [p. 481] the patients well-marked symptoms of disease of the pons were present. After the paroxysm it is by no means uncommon to find the urine loaded with albumen. Otto, Mabille, Saundby, Bazin, and other writers speak of a transitory albuminuria. Kleudgen,30 however, does not attach much importance to this feature, believing that the albumen is often due to semen.
29 Gior. internaz. d. Sc. Med., Napoli, 1880, ii. 357-359.
30 Archiv für Psychiatrie, etc., 1880, xi. 478-506.
The tendinous reflexes are frequently abolished during the attack, but not always so, and in several cases in which I was enabled to make a test during the convulsion I found that the patellar reflex was very active, and in one case elsewhere reported it was transferred. The skin reflexes are ordinarily exaggerated.
Tongue-biting is, I think, a more common feature of the nocturnal than the other attacks. It is rare in infantile epilepsy, and is always a bad feature. The wound is sometimes very serious, and cases are mentioned where the tongue has been severed. An occasional sequel of the attack is a urinary difficulty and vesical tenderness. It is sometimes connected with great urethral irritability and spasmodic stricture, which prevents the introduction of a sound or catheter. Romberg speaks of the supervention of asthma and dysphagia.
THE IMMEDIATE AND REMOTE EFFECTS OF THE EPILEPTIC PAROXYSM.—As a result of violence we often find wounds and bruises, quite rarely fractures, but more often dislocations. Cases have been communicated to me where as a result simply of the great muscular force the humerus has been dislocated at its superior articulation. Muscular pain of great severity, and sometimes of great persistency, follows unusually severe fits, and rupture of muscular substance is not uncommon. An epiolecranon bruise in one of my cases produced a severe neuritis which was very intractable. In old cases, according to Axenfeld, there may be great muscular hypertrophy, the sterno-mastoidii attaining the size of the biceps, and in other cases there is fatty degeneration. He also calls attention to defects that may be due to frequent exercise of violence upon bones through repeated exaggerated muscular contraction. Paralysis of nerves which supply convulsed members is mentioned.
The psychical effects are various. For several days following the attack there may be simply confusion of ideas, irresolution, or drowsiness, which subsides in a short time. In not a few cases I have regarded the attack as beneficial in the sense of an explosion of relief when perverted mental states had preceded it. In such persons the discharging lesion was followed by a very conspicuous restoration of the mental equilibrium.
Occasionally the attacks are terminated by great violence or screaming or the commission of purposeless acts.
Post-epileptic aphasia has been described by Winslow, Moreau, and others, and among my own cases of the sensory variety of this disorder I have met with speech disturbance. The aphasia is of short duration, and consists either in a total incapacity for verbal expression or a transposition. It is not rare for it to be associated with the commission of a number of quasi-automatic actions.
Unilateral epilepsies are quite apt to leave behind them a species of paresis which may last even for several days. The loss of power is confined to the convulsed members, and may be accompanied by tingling. [p. 482] In the greater number of instances, however, there is some central organic change, and the epilepsy is purely symptomatic.
Deafness, amaurosis, and other pareses of the organs of special sense are rare sequelæ of the epileptic state.
The remote effects of the grave disease are not so decided as when the patient has been the subject of petit mal. Slight repeated losses of consciousness are apt to be followed by mental decay. The ultimate result is mental enfeeblement, a progressive and very great loss of memory, which advances to such an extent that a veritable dementia ensues. With this there is usually a very decided perversion of the emotions and affections, so that a good-natured, amiable child may in a few years become everything that is bad and trying, and the acts of mischief are almost inconceivable. Theft, incendiarism, and various moral perversions are common in some chronic epileptics. The dementia, it is true, is tardy in its establishment, but it comes eventually if the individual lives long enough.
In some individuals there is a very early tendency to the development of mania; there is a certain periodicity about the explosions, and when established the excitement either precedes the attack by a few days or occurs shortly afterward. The violence is characteristically acute, and such insanity very often makes itself known in homicidal acts rather than in those of a suicidal character. Hypochondriasis is quite likely to follow continued epilepsy.
It is the rule for epilepsy to undergo decided modifications in the beginning of its course. The first attack may be simply eclamptic, without any peculiarities or definite character, and with recurrence there is a tendency to regularity and constancy in expression. Infantile convulsions, that may occur at any time after inconsiderable exciting causes, may eventually be confined to the early morning or night. So-called fainting attacks may precede petit mal, and headache may be the precursor of ill-defined seizures. So, too, the relation of grave and light attacks may vary. In the beginning there may be nothing but attacks of petit mal, while later these may be supplemented by severe fits, and even disappear entirely. So far as my own cases go, I find that nearly two-thirds of the entire number happen at night or in the early morning, while the others may occur in the day or at any other time, or by day and night. Besides the terms nocturnal and diurnal, we may use the word matutinal in relation to the time of attack. So far as the number of attacks is concerned, we find great irregularity. It is not always possible to count them, or even to recognize them, for the examples are numerous where nocturnal attacks have been undetected for years, and have finally been followed by fits during the daytime. I have cases who have seizures but once or twice a year, and others who have ten to forty or fifty daily. In some cases there may be eight or ten attacks of petit mal daily, and but two or three grave attacks during the week.
The statistics of Delasiauve and Leuret go to show that of 296 cases of epilepsy, the cases of general epilepsy were most common—that is to say, the attacks which occur both by day and night.
| Attacks occurring occasionally by day | 26 |
| Attacks occurring habitually by day | 30 |
| Attacks occurring only at night | 9 |
| Attacks occurring habitually at night | 8 |
| [p. 483] Attacks occurring equally by day or night | 87 |
| Attacks occurring in larger proportion by day | 70 |
| Attacks occurring in larger proportion by night | 44 |
Delasiauve, Herpin, and others make delicate distinctions between the attacks, and the former grades the seizures beginning at accesses, and successively advancing to vertiges, accès intermédiares, and attaques or accès compléts.31 In fact, these are but varying degrees of violence of the discharge, after all. We thus have light discharges and severe discharges at different times, or, as the habit is established, only the light or only the severe, the manifestation depending probably upon the number of discharging cells and the importance of the exciting cause.
31 Traité de l'Épilepsie, etc., Paris, 1845, p. 55 et seq.
When the attacks occur in alarming frequency, as they sometimes do, the condition is known as the status epilepticus. Leuret had a patient who had eighty in two hours, and Delasiauve reports the case of a young man fifteen years old who had twenty-five hundred in one month. They may be so numerous as to be apparently continuous. The patient remains in a state of coma (the status epilepticus), with very high temperature. If he be not restored, he sinks into a deeper coma, and all the signs of collapse manifest themselves. Bed-sores form, œdema of the lungs ensues, and the patient dies. Happily, this condition of affairs is rare.
Delasiauve calls attention to the fact that the first two or three attacks that usher in this state do not usually attract much attention, but the succeeding ones are so violent as to immediately suggest violent consequences. In one of my cases the attacks, when they had once become numerous, were readily excited by the least jarring, noise, or handling, just as we find in strychnine-poisoning or tetanus.
Irregular Forms.—There are occasional cases of psychical or masked epilepsy, the study of which is intensely interesting. Such forms are characterized by perverted consciousness and a low degree of volitional direction which may vary from automatism to the undoubted exercise of complex functions of the mind, though badly co-ordinated. Mesnet's soldier, when subject to a paroxysm and apparently unconscious, would perform a number of suggested acts in a rhythmical manner and with no subsequent knowledge of the previous event: when started off by the word of command to march, he would blindly go on, marking time when he met with an obstruction until stopped, or when a paper and tobacco were placed in his hands he would proceed to roll an unlimited number of cigarettes.
Two cases of a more complex exercise of certain intellectual powers, while others were dormant, came under my observation some time ago. One of them was a young man of twenty-three, who had had irregular epileptic seizures for some years. He went to bed one evening as usual, arose, and breakfasted with his family without creating any suspicion that he was at all unwell. He then went down to his place of business, and after his arrival was sent to a distant part of the city for some tool. On his return down town he stopped at a tobacconist's and became involved in a quarrel with one of the persons in the shop. A policeman was called, who, more intelligent than many of his class, immediately detected something queer about the man, arrested him, and afterward took him to Bellevue Hospital. There he remained three days, and suddenly [p. 484] returned to consciousness and a knowledge of his surroundings, but was entirely ignorant of his unfortunate experience. It is unnecessary to say his habits were perfectly good and he was not drunk at the time of the quarrel or arrest. His last recollection was that of going to bed the night before the day of his arrest.
Another case of unusual interest which came under my care, illustrating a phase of sensory epilepsy, is worthy of reproduction:
C. O——, aged twenty-two, is a reporter attached to one of the New York afternoon papers, who received a severe injury of the head when but three years old. He fell from the second story of an unfinished building to the cellar, striking the upper and back part of his head upon a beam. He was rendered unconscious, and remained so for a day or more. He recovered from the immediate bad effect, but has suffered from severe general headaches, which recur every week or so, with an increase in the amount of urine excreted. About six months ago he began to have epileptic convulsions of a violent character almost every day, and sometimes more often. These were precipitated by excitement, and he had a great many when worried about his wife at the time of her delivery. Upon one occasion he fell down stairs and injured himself quite severely. The attacks were, as a rule, preceded by an epigastric aura of long duration, and occasionally by a visual aura, and, according to the testimony of his associates, he became strange and queer. When in such a dazed condition he would restlessly wander about his office, and suddenly, without any cry, become convulsed. After the attack he slept soundly. The bromides of sodium and ammonium and digitalis did little or no good, but the bromide of nickel appeared to have some influence. During the past month he has had only two or three attacks, but these have been of a quite irregular character. He told me that there were times when he felt like doing himself an injury, and that he had impulses to kill some one else. His companions said he was irritable, pugnacious, and easily thwarted, and his brother-in-law stated that upon several occasions he had queer turns, when he would raise his hand to strike some member of the family—that he subsequently knew nothing of his conduct, and when it was detailed to him he appeared greatly astonished.
Mr. O—— came to my office in company with a friend at ten o'clock in the morning of December 27, 1883. He had had one of his attacks at the newspaper office, of rather more severe character than usual, at eight o'clock, with a psychical aura, during the existence of which he was very morose and sullen. Upon recovery he was speechless, though he could communicate by signs. Upon his arrival at my office his manner was composed and he appeared somewhat dazed. His pupils were dilated, but contracted readily to light. I asked him one or more questions regarding his inability to speak, which he perfectly understood, and when I gave him a pencil and a piece of paper he replied without difficulty in writing. When told to make a great effort to speak he did so, and I thought I detected the word ‘To day,’ but he could not repeat it, though he tried and expressed great annoyance. He was unable to utter any sound except a sort of groan, which could not in any way be taken as an element of speech. I examined his larynx, but found nothing which could explain his impaired phonation, and I sent him to Dr. Asch, who found absolutely no abnormal appearances to account for the speech [p. 485] difficulty. The patient could not phonate, and though he made attempts to enunciate the vowel-sounds, and the vocal cords were approximated, he made no orderly sound. Asch found a slight laryngitis of no importance.
The patient went home, and remained speechless all day, and was seen by my associate, G. de Forrest Smith, in the evening. What occurred during and after that gentleman's visit is contained in his notes: “I was called to see patient about 8.15 P.M. He was lying upon the bed, but had not slept; recognized me and motioned that he could not speak, and I found that he could only say one or two words, and this with the greatest effort, and so all my questions were put so that he could answer them by nodding or shaking his head. He knew that he had had an attack in the morning, that he had seen Hamilton and Asch, and recalled various incidents of the day, answering intelligently my questions in regard to them. He indicated by motions that his inability to speak was due to a lump in his throat. When asked if he had any trouble to think of the word he wanted, he shook his head, but shortly afterward hesitated in an answer, and when asked if this was due to his inability to think of the word, said ‘Yes.’ Was asked if he had any loss of power in either side, and he motioned to his right arm and leg, and said that he felt a numbness and pricking on that side. On his grasping my hands with his, the right was perceptibly weaker.
“At one time he seemed confused as to which was his right or left side, and put up both hands, and after looking at first one and then the other in a puzzled manner, at last decided correctly, then smiled apparently at his confusion.
“All this time he had been half lying on the bed. He now intimated that he was tired, put his head down on the pillow and began to belch up wind, and as he appeared about to vomit I called for a basin; but this was only the beginning of an attack; the muscles of the neck and right side assumed a state of tonic spasm, the extensors predominating, so that the head was turned a little to the left and forcibly thrust back into the pillow, and the right arm and leg were firmly extended. He remained in this position about one minute; then, taking two or three full inspirations, put his hand to his throat and said plainly, ‘Something has fallen from there.’ On being asked ‘What?’ he replied, ‘A bone has fallen from my throat.’ I told him it was well that the bone had fallen, as now he could speak. ‘Why,’ said he, ‘I have had no difficulty in talking.’ On being asked why he had seen Asch, he said ‘Who is Dr. Asch? I never saw any such person.’ Further questioning showed that all the occurrences of the day (except those which had taken place immediately before the first attack) were an absolute blank, and he thought it still morning. He asked the time, and I told him half-past eight o'clock in the evening. At this he seemed much surprised and said, ‘Why, I went to work this morning; how did I come here?’ I then explained to him that he had been ill. After further conversation he said he felt sleepy, and, after resting a few minutes, he arose, put on his slippers, and came out into the room. He walked with difficulty, because of the loss of power in the right side, which he said felt numb and sore, as if it had been pounded, also a sensation of pins and needles. After the attack his mind was perfectly clear, and he could talk as well as ever, and all that had happened before the attack in the morning he could remember [p. 486] perfectly well, but the interval between the two was a complete blank. His inability to speak seemed due, not to lack of knowledge of what he wanted to say, but rather to want of power to form the words, although there was no paralysis of the vocal muscles. When he did manage to say a word, it was invariably the correct one, but it was always done with the greatest effort. The day after the attacks he remained at home; the next day he went to work, but his head felt heavy and confused. Two days after he complained of a pressure on the left side and back part of the head; otherwise he was all right. At this visit he said that after I had left him on the night of the attacks he intently thought, striving to recall the incidents of the day, and after a time concluded he could remember being at Thirty-third street, but did not know how he got there. He thought he could recall going to see Asch, but would not know him if he should see him. I then asked him how questions were answered by him on that day; he answered he did not know, as he had not thought of that; then, after a few moments' reflection, said he must have written the answers. He was then shown some of the answers he had written, which he recognized, and by an effort of memory could recall some of the incidents of writing them. He was still unable to remember anything that occurred after his arrival home previous to the last convulsion.”
January 27, 1885: This patient subsequently suffered from several attacks in which the psychical element predominated. His head presented a remarkable deformity, there being a prominence posteriorly which might be compared to a caput succedaneum, only it was entirely osseous. The upper margin was separated from the anterior parts by a deep sulcus.
Under such circumstances we find very often that acts of great violence are committed by such epileptics for which they are entirely irresponsible. Two or three cases of the kind occur to me now. One of them was a boy who always bit every one and everything—his family, the domestic animals, and inanimate objects; another, a most dignified and lady-like woman, who violently struck different members of her family; and within the past week a woman was brought to me who hurled a kerosene lamp at a perfect stranger with whom she was quietly talking before the seizure was precipitated. Numerous instances are related where individuals while in the masked epileptic state have wandered for long distances and committed a variety of purposeless acts, and undoubtedly many of the mysterious disappearances are of this order.
SENSORY EPILEPSY.—Some years ago Hammond referred to certain peculiar epileptic attacks in which sensory manifestations were very pronounced. To this condition he gave the name thalamic epilepsy, believing the condition to be one of the optic thalamus. Among the large number of unclassified and irregular cases reported by various authors there are many so much resembling each other that I think they should be relegated to a special place.32 The notable examples of Sommers, Bergmann, Tagges, Guislain, and others belong to this category.
32 I shortly afterward, believing the term a misnomer, invented that in use: “On Cortical Sensory Discharging Lesions or Sensory Epilepsy,” New York Med. Journal and Obstetrical Review, June, 1882; also see “A Contribution to the Study of Several Unusual Forms of Sensory Epilepsy which are probably Dependent upon Lesions of the Occipital Cortex,” New York Med. Record, April 4, 1885.[p. 487]
The features of this form of epilepsy are (1) the expression of some hallucination (prodromal stage), or hemiopia; (2) supraorbital neuralgia; (3) aphasia, formication; (4) slight loss of consciousness, and little if any motor disturbance.
I may present two illustrative cases:
A few months ago I was consulted by a medical gentleman in regard to a patient who had for years presented a curious train of nervous symptoms, which afterward assumed a form leading me to think she might have sensory epilepsy. She would, in the presence of the gentleman who consulted me, who was a personal friend of the patient and a medical man, stop short in the midst of an animated conversation, look fixedly ahead, appearing momentarily lost, remaining abstracted for a short period, possibly a minute, and on recovering herself go on, finishing the sentence she had commenced before the seizure. At this time she constantly had hallucinations of a visual character, when she saw animals, birds, figures of men and women, who approached her, as well as a variety of other objects. A common hallucination, which had been repeated quite frequently, consisted in visions in which green leaves and white rabbits and other objects familiar to her in childhood figured extensively. Upon one occasion, while sitting in the drawing-room, opposite a door which communicated with the hall, she suddenly called her companion's attention to the hand of a man which she saw clasping the baluster rail. The hand was seemingly disconnected from the arm. She was somewhat agitated, and it was nearly half a minute before the vision was dismissed. Sometimes she would call attention to the hallucinations before the attack, but more often she became transfixed, apparently lost, and then recovering she described her visions minutely. She has apparently been able to foresee the attacks and ward them off by a strong voluntary effort. So far as can be learned, there is no hysterical element in the case, but her seizures are more frequent at the time of menstruation. In a private note it is stated that “the family history of the patient is very good, and she has always seemed remarkably healthy and robust, and has shown more than usual intellectual ability. She has appeared to persons generally to be of a contented, happy disposition.... At night, when she closed her eyes, she suffered from these hallucinations, especially after a day of fatigue. Her pupils are usually dilated, but her color undergoes no change during the seizure.”
The second case is one of a more complex type:
J. B——, a bright boy aged sixteen, was sent to me by F. H. Bosworth in April, 1883. He comes of nervous stock, his mother being subject to epilepsy, and his father is an eccentric man who manifests his mental peculiarities chiefly in a morbid restlessness and irascibility. There is a brother who is healthy. The attention of the parents was first called to the boy's condition by his recital of a sudden attack which occurred during the summer of 1882. While rowing upon a river he suddenly and completely lost the visual use of the right eye, so that in looking at a number of ducks swimming near his boat he failed to perceive those upon one side of the flock. This condition lasted for twenty minutes, and after a brief and severe pain over the right eye he became unconscious, the unconsciousness being preceded by a tingling and numbness of the hand, forearm, arm, and left side of the tongue. He has [p. 488] subsequently had eight or ten of these attacks, of which the following is an example: Usually without any bad feelings, physical or mental, he, while engaged in any duty or at any time, suffers a sudden unilateral blindness. This is never gradual, and not like the form of amblyopia in which the visual field is gradually reduced. There is some hemichromatopsia. It would seem as if the retinal anæsthesia was unequal, for while usually the loss is complete and universal, it sometimes happens that there is only a limited loss. Upon one occasion, while reading, he suddenly lost the printed matter of the right lower half of the page below a diagonal line extending from the right upper corner to the left lower corner. There is never diplopia. This deprivation lasts anywhere from ten to twenty minutes; meanwhile, a distal anæsthesia, coming very gradually, involves at first the fingers of the opposite hand, and successively extends to the forearm, arm, and other parts, as I have already mentioned. There seems to be analgesia as well as anæsthesia, for a pin may be run into the muscles without producing pain, and upon one occasion the gum was freely pricked without any discomfort to the patient. It invariably happened that the cutaneous sensory trouble occurred upon the side opposite to the hemianopsia and neuralgia, and in the greater number of instances the left side was that affected. The third stage of the attack consists in migrainous headache of a very severe kind, and which sometimes lasts for an hour or more. There is a subjective feeling as if the eye was pushed forward. This disappears with nausea and relaxation. More often he loses consciousness when the anæsthesia reaches its limit, which seems to be the extension of the anæsthesia to the gums. Occasionally there are slight convulsive movements upon the anæsthetic side. While the attacks involve the left side of the body as a rule, it happens that when there is primary left hemianopsia and right-sided anæsthesia the boy becomes very much confused in speech, and sometimes is paraphasic, the trouble being but transitory. He is sometimes unable to speak at all, though perfectly conscious and in possession of his faculties. No pupillary disturbance has been noticed at any time. Upon two occasions there was a swelling of gums and tongue, which was not only subjective, but perceived by the mother. Occasionally he sees prismatic colors and rays before the blindness, but this has been only once or twice. During his early life he had attacks of slight numbness of the hands and feet which were not thought much of, and he had headache as well. He has been a somnambulist.
MORBID ANATOMY AND PATHOLOGY.—The literature of the experimental physiology of epilepsy is enriched by the observations of a variety of careful students, among them Sir Astley Cooper, Kussmaul and Tenner, Brown-Séquard, Nothnagel, Schroeder Van der Kolk, Pitres, Hughlings-Jackson, and the followers of the localization school, as well as many others more or less distinguished.
The experiments of many of the early writers were directed for the purpose of ascertaining the relations of circulatory variations to convulsive seizures, and the most notable were those of Burrows and Kussmaul and Tenner. These latter produced compression of the carotid arteries, and instituted cerebral anæmia by free and exhausting hemorrhages. As a consequence, the emptying of the cerebral vessels was followed by a loss of consciousness and by epileptiform convulsions, and it was [p. 489] necessary to produce the same result to compress all the great afferent vessels of the brain. The experience of surgeons generally is, that ligation of the common carotid upon one side of the neck is sometimes very apt to produce an alarming anæmia, with occasional convulsions, and sometimes fatal consequences.
The experiments of Hall, Landois, Hermann, and others, as well as those of the writers just mentioned, show that carotid compression results in capilliary anæmia and venous hyperæmia, and that with cessation of this pressure there is a sudden congestion of all vessels. The susceptibility of the brain is greatest at its posterior part and between the optic thalami and the cord. When the bulb was subjected to sudden changes in its nutrition—such, for instance, as followed the experiments of Hermann, who ligated simultaneously the superior and inferior venæ cavæ of a rabbit—there were not only convulsions, but various cardiac and other disturbances which were undoubtedly due to central impairment of function. Kussmaul and Tenner conducted their experiments with watch-glasses luted into the cranium—a procedure which, however, at best, is unreliable.
Brown-Séquard some years ago in part established an important pathological truth, the theory of epileptic zones, and demonstrated in certain animals that bruising and injury of the great nerve-trunks, especially the great sciatic, would give rise to epilepsy, and that irritation of certain tracts would precipitate the paroxysms. He further announced that the progeny of animals in whom epilepsy had been thus induced very frequently inherited the epilepsy of the parent. By some it was held that such epilepsies were purely peripheral, and Brown-Séquard even believed in spinal epilepsy. His spinal epilepsic theory has, for the most part, been explained by the anatomical researches of Hitzig and the doctrine of interrupted spinal inhibition. In fact, many of the spinal epilepsies are examples of exaggerated reflexes.
The epileptiginous zone theory, which, while it induced many to believe that the disease might have its origin outside of the brain, gave rise to the false assumption that attacks with distal auræ were primarily non-cerebral, has been discarded, and most observers have arrived at the conclusion that even in these cases the first explosion is due to some cerebral cell-discharge.
Hughlings-Jackson's grand work has revolutionized the views held prior to his first published writings, about twelve years ago. He believes that any part of the gray matter may, through over-excitability, give rise to convulsive attacks.
The production of convulsions by cortical irritation is now an old story.
The experiment of Pitres and Frank33 bears upon the sensorial function of the cortex in showing that, when the cortex is irritated, epileptiform convulsions follow, but if the exposed surface be subjected to the ether spray the same irritation will only produce definite movements, but no convulsions.
33 Gazette des Hôpitaux, No. 38, 1883.
The investigations of Van der Kolk especially, and his followers, certainly give the medulla an important place as the locus morbi of the malady; and it must be assumed, bearing in mind the existence of the vaso-motor centres of Dieters and the presentation of symptoms indicative [p. 490] of disturbance at the floor of the fourth ventricle, that the most important pathological changes must be looked for in this part of the brain.
Jackson's cortical explanation is, however, fully in consonance with the medullary theory. If we study the different stages of the attack, we shall find that there is probably a suspension of cortical inhibition—that a derangement of the cortical cells or discharge may cause a resulting disturbance in the bulb. On the other hand, a reflex irritation through the pneumogastric or from some distal part brings about the same disturbance of equilibrium. There is anæmia due to irritation of the vaso-motor centre, an inhibition of the great ganglion-cells, and a disturbance of function of the important cranial nerves. The primary anæmia and unconsciousness are accounted for by this primary irritation of sympathetic filaments and vascular constriction; the secondary hyperæmia is explained by the experiments of Kussmaul, which demonstrated the succeeding congestion; or by irritation of the spinal accessory and contraction of the muscles of the neck and compression of the large veins. The pupillary, ocular, respiratory, and other symptoms indicate the disturbance of the nerve-nuclei in the bulb. The respiratory difficulty and the interrupted decarbonization of the blood undoubtedly account for the secondary unconsciousness.
Van der Kolk34 in localizing the lesion in the medulla found capillary dilatations in the neighborhood of the hypoglossal nuclei in tongue-biters. In epileptic patients who were in the habit of biting their tongues during the fit the vessels were wider than in those who did not bite the tongue, on an average in the course of the hypoglossus by 0.096; in the corpus olivare, which certainly here plays an important part, by 0.098 mm.; and in the raphé by 0.055. In those who did not bite the tongue, on the contrary, the vessels in the path of the vagus were 0.111 wider than in those in the first, Table A.35
34 “On the Minute Structure and Functions of the Spinal Cord,” by J. L. C. Schroeder Van der Kolk, New Syd. Soc. Trans.
| Different Epileptics. | Hypoglossus. | Corpus olivare. | Raphé. | Vagus. |
| Table A—tongue biters | 0.306 | 0.315 | 0.315 | 0.237 |
| Table B—non biters | 0.210 | 0.217 | 0.217 | 0.348 |
| Difference | +0.096 A. | +0.098 A. | +0.055 A. | +0.111 B. |
Nothnagel36 is of the opinion that the anæmia of the brain is not the cause of the convulsions, but that the “excitation of the vaso-motor centre and that of the centre for the muscles are co-ordinate—that both go on side by side, and are independent of each other.”
36 Ziemssen's Encyclopædia, vol. xiv. p. 268.
He by this theory explains the occurrence of those forms of petit mal in which there is loss of consciousness without convulsions, and, on the other hand, twitchings before the coma.
The best argument in favor of this hypothesis is in Jacksonian epilepsy, when monospasms exist oftentimes with a succeeding extension.
In those cases which are the outgrowth of migraine the pathological condition is probably an exaggerated tendency to angio-spasm, the original impaired vascular tonus in the beginning giving rise simply to pain and lesser troubles, while after repeated changes of calibre not only [p. 491] nutritive alterations ensue, but hyperexcitability of the bulbar convulsion centres as well.
The labors of those who have endeavored to connect epilepsy with cerebral-tissue alterations have been attended by nothing very definite or positive, so far as pathological explanation is concerned. The post-mortem appearances have varied widely, and the only conclusion to be reached is that which shows that almost any morbid gross alteration of the cerebral mass may be symptomatized by convulsions, but such a production of paroxysmal trouble is much more likely to be the case, and in a more definite manner, when the cortical motor-centres are subject to destructive disease or irritative pressure. This is even not always the case, for numerous cases of injury of the paracentral lobe have been recorded with no showing of resulting convulsions. The long list of autopsies which I will not here consider show that an epilepsy may owe its origin to the pressure of a spicula of bone, or to the pressure exercised by depressed fragments of the same—to tumors or adventitious products, meningitis, cortical encephalitis, vascular degeneration, ventricular œdema, contusio-cerebri, and many other morbid processes which result in rapid or tardy degeneration. Of course, in such cases the genesis of the disease depends not so much upon the nature of the lesion as the location. The fruitful collections of cases of Ogle and Jackson are full of examples of limited growth or disease involving the cerebral cortex, while numerous cases collated by other writers show disease of the bulb or various peripheral parts which have been closely connected with the growth and behavior of the affection.
Several able pathologists have independently and repeatedly found that sclerotic degeneration of the hippocampal folds often existed. Delasiauve and Lébert first observed this lesion, but many modern authorities—among them Meynert, Nothnagel, and Charcot—who have also found this appearance, regard the change as of purely secondary, and consequently unimportant, character.
Tamburini37 reports a case of hemiplegic epilepsy with induration of the left optic thalamus and the left cornu ammonis, in which aphasia existed. Pfleger38 and Henkes have also found the sole lesion to be induration of the cornu ammonis. Of Pfleger's39 43 autopsies, atrophy and sclerosis of the cornu ammonis were found twenty-five times, and it was noted that the extent of the morbid change bore relation to the violence and frequency of the seizures.
37 Sallanzani, Modena, 1879, viii. 550-557.
38 Allg. Zeitschrift f. Psychiatrie, etc., Berlin, 1879, xxxvi. 359-365.
39 Ibid., lxxvi., and Arch. de Neurologie, No. 2, 1880, p. 299.
In many examples, especially where the disease has been found to be unilateral and associated with more or less hemiatrophy, the autopsy disclosed a corresponding hemiatrophy of the brain. Many such cases are reported. I have frequently found epilepsy in association with cerebral hypertrophy, and as a symptom of cerebral tuberculosis it has long been recognized, and numerous cases are reported in which for a long time the paroxysms were the only manifestations of the condition. In one of these cases, reported by Luys,40 the bulb was found involved by tuberculous matter.
40 Archives gén. de Méd., 1869, ii. 641 et seq.[p. 492]
Convulsions have very frequently been noted in association with imperfect cerebral development, and Echeverria laid great stress upon the hyperplastic increase in volume of certain parts of the brain.
Marie Bra41 has thus summed up her conclusions relating to the morbid anatomy of epilepsy:
“1. The mean weight of the brains of epileptics is less than the physiological mean.
“2. The cerebellum is greater than the physiological mean.
“3. There frequently exists an asymmetry between the lobes (not peculiar to epilepsy). The increase of weight is sometimes found on the right and sometimes on the left side. Equality is the exception.
“4. In no form of mental disease (excepting perhaps general paresis, which is accompanied also by epileptiform crises) have we met with so marked and constant a variation between the weights of the hemispheres as exists in epilepsy.”
41 Referred to by Axenfeld.
Drasche, Green, Greenhow, Löbel, and others have detailed cases in which tuberculous deposits were undoubtedly the causes of the disease.
Kussmaul and Tenner, Hoffman, and others have held that a stenosis of the superior part of the vertebral canal may explain, through pressure upon the cord, the genesis of the attack, and Kroon found asymmetry of the medulla oblongata.
The microscopical changes that have been found in brains where no gross lesion was apparent are by no means distinctive. I have myself examined the brains of many epileptics with discouraging results. The varying granular cell-degeneration, capillary dilatation, and exudative changes are common enough. In several cases of cortical epilepsy I found more or less advanced degeneration of the great cells in limited regions.
By far the most important and exact changes are those observed in the cases of sensory epilepsy. I have elsewhere collected some continental cases. In brief, areas of occipital softening or degeneration have been discovered in those cases with hallucination, sensory expressions, and hemiopia. In one case attended by hallucination of smell the autopsy disclosed the following:
M. M——, was a stout Irish woman about forty years of age. She had suffered from a light form of epilepsy dating from the tenth year, and resulting, as she stated, from a fall, when she struck her head and was unconscious thereafter for some hours. No scar was visible, however. No satisfactory history could be obtained regarding her early life and the first paroxysms. In the beginning these were rather frequent, and she had as many as four or five a month. They afterward diminished in number and severity, and for many years she had but three or four in the course of the year. They were not very severe, and she was enabled to pursue her work as a housemaid, but did not keep her places for any great length of time. She rarely bit her tongue, but usually frothed at the mouth and became livid and convulsed for a short time. There was no history of one-sided spasms. As I have stated, I could gain no accurate account of the previous attacks, except that she nearly always had an aura of a peculiar character, which was a prominent feature of the seizure and very pronounced. She suddenly perceived a disagreeable odor, sometimes of smoke, sometimes of a fetid character, and [p. 493] quite uncomplicated by other sensory warnings; and afterward became unconscious, and remained so for two or three minutes. She was invariably able to describe her sensations when she recovered, which she always did when I asked her, comparing her warning to the smell of burning rags, to the smell from a match, and, as she expressed it, it sometimes rose up in her head and choked her. She was under my observation for one or two years, but eventually developed phthisis, and died, her attacks occurring from time to time until her death.
Besides well-marked tuberculous lesions in the lungs, there was little of interest so far as the visceral examination was concerned. The brain was removed and its peculiarities were carefully observed. A great quantity of fluid was found, especially at the dependent portions of the membranes and in the ventricles, while the dura was thickened and pearly in spots. There was a condition that might be likened to a low grade of hemorrhagic pachymeningitis, and at the base of the brain old plastic changes were found, there being adhesions, especially in the region of the middle lobes, but more particularly on the right side and near the median line. The brain as a whole was small, and weighed forty-one ounces and a fraction. The sulci were deep and gaping, and the convolutions were distinct. There was no atrophy of the fore-brain convolutions, and no other pathological appearance was presented except that found in the meninges, but at the lower part of the temporo-sphenoidal lobe of the right side an appearance was found of an exceedingly interesting nature. At this point a decided shrinkage of tissue was discovered, with depression and adhesion of the pia, the induration involving the uncinate gyrus and parts of the adjacent convolutions, as represented in the drawing. No induration or softening of the great motor tracts was observed, and the optic thalamus and parts adjacent were uninvolved, as was the cord. An attempted microscopic examination, undertaken some months subsequently, was unsatisfactory, because of the bad condition of the brain, the preserving fluid having been improperly made. The olfactory nerves were not involved. The third frontal convolution was examined, but no disease was found there. Consequently, it is to be inferred that no lesion of the external root of the olfactory nerve existed.
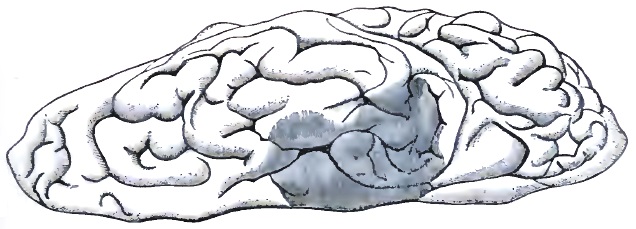
DIAGNOSIS.—Having spoken of epilepsy as in most instances a symptomatic disorder, it would be proper to confine this section to the differentiation of the simpler and more classical form of the idiopathic disorder from certain purely eclamptic attacks or those due to cerebral tumor or [p. 494] coarse degeneration. The epileptic attack itself is to be considered from its time of happening, its duration, the element of unconsciousness, its associations, and the antecedent history of the individual. It may be confounded with the similar phenomenon dependent upon cardiac weakness, uræmic poisoning, toxic or alcoholic saturation, etc.
Of course, when we find recurring seizures with a certain amount of what Carter-Gray calls quasi-periodicity, preferring perhaps the night, the early morning, or only the daytime, we are almost sure of epilepsy. This supposition is strengthened by the association with attacks of petit mal. The duration of an attack, which may be from a few seconds to several minutes, is also a guide, for in certain toxic and other paroxysms the rule is for a succession of attacks to occur.
The question of consciousness is one that has drawn forth a great deal of discussion, especially with reference to medico-legal cases. I think the majority of clinicians are agreed that loss of consciousness is an absolute belonging of epilepsy, yet there are cases in which the lapse is scarcely perceptible. It is a dangerous precedent to establish, for the convulsive symptoms in such cases are taken from the epileptoid category. It is quite true that there are many hemi-epilepsies in which the intellectual condition is one that may easily be mistaken. I have seen numerous cases in which an apparent conservation of consciousness remained throughout a slight monospasm, but I do not feel at all sure of this; and in cases of aborted or masked epilepsy there is a dual mental state which would readily deceive the lay observer. The case of Mrs. S—— is an example of this kind. After the obvious subsidence of the dramatic and conspicuous feature of the fit she remained for hours and days in a state of undoubted transposition, performing acts which required something more than a high degree of automatism—going to the table, talking about certain subjects which were suggested, with apparent ease, but not connecting them intelligently with her surroundings, as she would before and after the epileptoid state. After a time she apparently resumed her normal state, but was entirely unconscious of the happenings of her previous hours or days, not even recollecting her simplest actions. Julian Hawthorne's hero in Archibald Malmaison, though not drawn by a physician's pen, suggests the state of which I speak, and it has the merit of being based upon one of the elder Forbes Winslow's interesting cases.
When we find paroxysmal attacks occurring in individuals with atypical heads, thick swollen lips, scarred tongues, and irregular teeth, we may strongly suspect the patient to be epileptic. To these we may add the appearance of the eyes, the fishy, lack-lustre expression which betokens old epilepsy. The hands are clammy and the skin mud-colored; the hair is dry and coarse; and the body often has a death-like odor.
In children, certain mental peculiarities are to be inquired into. Unnatural brightness or dulness—what may be called the clumsy organization—is often present, and the muscular use is often imperfect. We find that there is often but little nicety in walking, in using the hands, in speaking, or after learning to write there is an incapacity, with ever so much teaching, to develop a character or style. Such children can never become ambidextrous. These little points may seem trifling, but to the physician who carefully studies his cases they may prove of great help. The history of the nights may often lead to the discovery perhaps of a [p. 495] long-existing nocturnal epilepsy. Incontinence of urine, blood upon the pillow, nightmares, morning headache, and petechiæ betoken unsuspected night attacks; and Le Grand du Saulk mentions the case of a young Englishman who committed a purposeless crime and was discovered to be epileptic, the diagnosis being confirmed by an antecedent history of nocturnal seizures, and subsequent watching resulted in the discovery of many night attacks.
As to special conditions with which the epilepsy may be confounded, I may refer to cardiac weakness. It not rarely happens that simple fainting attacks are confounded with those of an epileptic nature. Such is the case more often in heat-prostration, when some rigidity attends the loss of consciousness. The duration of such a state, the condition of the pulse and color, however, will easily clear up any doubts upon the part of the observer. The existence of a cause should also be considered, and the fact that usually the epileptic paroxysm is sudden, while a feeling of depression and feebleness precedes the fainting attack, should be remembered. I may present in tabular form the points of difference:
| EPILEPSY. | SYNCOPE. |
| Loss of consciousness sudden. | Loss of consciousness follows feeling of faintness. |
| Period of complete unconsciousness usually short. | Unconscious throughout, no convulsions. |
| The existence of auræ of a well-defined type. | The existence of preliminary vague prostration, nausea, and irregular heart action. |
| Often involuntary discharge from bowels and bladder. | Quite rare or never. |
| Patient usually falls into heavy sleep or is indifferent after convulsion. | After slight weakness patient is anxious and worried, and quickly seeks relief. |
The difficulty of diagnosis, however, is only in cases of petit mal.
There are light forms of auditory vertigo that may resemble vertiginous epilepsy. In the former there is never loss of consciousness, and the patient refers to the rotary character of the vertigo. A history of antecedent attacks, tinnitus, aural disease, and a certain constancy which is not a feature of petit mal, may be mentioned.
There are cases, however, which are puzzling, and come under the head of auditory epilepsy rather than auditory vertigo; and in these there is a multiplicity of expressions, the auditory symptoms predominating.
Of uræmic convulsions it is hardly necessary to speak. There is a previous history of renal disease which the microscope and less delicate tests will reveal, and clinically there is antecedent headache, some stupidity, and not unrarely thickness of speech and somnolence. There are some cases, however, which are obscure. I have known patients with chronic renal disease—such as waxy kidney, for instance—to develop a species of epilepsy, the paroxysms recurring from time to time and behaving very much as the idiopathic disease would; and their occurrence would mark some imprudence in diet or exposure, and their disappearance an improvement in the patient's general condition. The attacks were not classical, inasmuch as there seemed to be but one stage of violent clonic convulsion, preceded by intellectual dulness, and followed by a semi-comatose condition which was far mere profound than the somnolent [p. 496] stage of epilepsy. The movements were not accompanied by a great degree of opisthotonos or pleurosthotonos.
Alcoholic and absinthic epilepsies are usually preceded and followed by symptoms indicative of profound saturation.
The consideration of hysterical epilepsy may be found elsewhere, but it may do to briefly refer to some cases which do not present the phenomenon first described by Charcot and Bourneville. The ordinary hysterical attack is never attended by loss of consciousness, by any of the pupillary changes so constant in epilepsy, by the mobility of the pupil between the attacks which is present in a large number of true epileptic individuals. There are never the succeeding changes of color, and the seizures are commonly produced or attended by some emotional disturbance, or are associated with ovarian disturbance.
Epilepsy is occasionally simulated by malingerers, and sometimes the skill of the subject is so great as to even deceive the practised eye. Prisoners, soldiers, and litigants may counterfeit an epilepsy, and go through with great personal suffering to accomplish their purpose. “Clegg, the dummy-chucker,” whose remarkable case has figured in the medical journals, upon one occasion threw himself from an iron platform to the stone floor of the jail, nearly twenty feet below, to convince a suspicious physician of his honesty. The simulator rarely bears close watching. The dilatation and contraction of the pupil cannot be simulated, nor can the corneal or pupillary insensibility. The fraud cannot voluntarily change his color, as is the case in true epilepsy, and as a rule the thumbs of the impostor are never flexed, as they should be. Suggestions for a purpose are readily heard, and sometimes adopted, by the apparently unconscious man. Gottardi42 lays great stress upon the use of the ophthalmoscope as a means of detecting simulated epilepsy. He calls attention to the frequency of retinal changes with facial asymmetry and other evidences that suggest cerebral disease or non-development. Gottardi has found that the pulse in true epilepsy is always lower after an attack, but it soon reaches its normal standard.
42 Abstract in Journal of N. and M. Dis., Oct., 1881, p. 843.
The differentiation of idiopathic epilepsy from that due to syphilis is possible when we consider the element of pain. Besides the tibial pains of syphilis, the epilepsy thus produced is often preceded by intense frontal headache, while that of ordinary epilepsy follows the attack. The syphilitic epilepsy is not attended by so great or continued a loss of consciousness as the non-specific form, and the movements are apt to be most violent on one side or the other. The association of the attacks with various bodily signs, such as nodes, old scars, alopecia, erosions, etc., and in connection with possible cranial nerve-paralyses, will throw light upon its true character. The paralyses referred to seem most frequently to involve the motor ocularis, abducens, and patheticus. Syphilitic epilepsy, too, is quite irregular in its time of manifestation, and is not unrarely followed by aphasia; but the interparoxysmal mental state is one of extreme dulness, memory being blunted and there being a peculiar hebetude.
PROGNOSIS.—Within the past quarter of a century the ideas of the medical profession regarding the curability of epilepsy have certainly undergone a change. The statistics of Bennett and others show that since the introduction of the bromic salts the proportion of cures has [p. 497] been decidedly increased. Nevertheless, the disease is a most discouraging and troublesome one to manage, and especially is this the case when it assumes the form of petit mal. The rapid recurrence of light attacks is, as has already been said, very apt to lead not only to mental enfeeblement, but is very often followed by very severe paroxysms.
Epilepsy of a more or less constant form, in which the seizures resemble each other, is far more incurable than that of variable type; for example, we find that unilateral seizures are much more apt to be associated with established cortical disease than when they are general and simply explosive manifestations. It has been held that a tendency to permanency is marked by a diminution in the extent of the interval. This is by no means true. I have had cases under observation for ten or twelve years in which attacks separated by intervals of six months or one year marked the course of the disease, in which frequent initial attacks were present. These cases I regard as very bad so far as prognosis is concerned. I much prefer a history of irregular and comparatively disorderly attacks. In female subjects the menstrual influence is not always a bad factor. When we are enabled to remove some production of an exciting cause in connection with the catamenia the prognosis is more hopeful; but an opinion must be expressed with great caution, especially in those cases beginning at an early age and not after the establishment of the menses. Traumatic cases are not always bad, but those in which the element of heredity plays a part most certainly are, Herpin and Gowers to the contrary; and though these cases for a time do well under treatment, its good effects are not constant. Individuals with misshapen heads, whose deformity suggests premature sutural ossification, are not susceptible to the influence of treatment, and all other osseous changes, such as exostosis, plaques in the dura, and bony growths, whose existence can only be guessed at or inferred from suggestive appearances elsewhere, give rise to a variety of epilepsy which is beyond the reach of drugs. With symptomatic epilepsies the case is sometimes different, for while the seizures which arise from the irritation of a cerebral tumor are almost as hopeless as the form I have just mentioned, we know from experience that the epilepsy of syphilis and other allied diseases, and those of toxic origin, with the exception sometimes of those occasionally due to alcohol or lead, are curable. The meningeal thickening of alcoholic origin or the encephalopathy of lead may be the pathological bases of very intractable paroxysms.
So far as age is concerned, it may be stated that many eclamptic seizures of young children which are due to well-recognized irritable causes are promptly cured if there be no hydrops ventriculi or preossification of the coronal sutures, and if the epileptic habit is not established. The epilepsies of six or eight years' standing are not encouraging from a therapeutic point of view, and those of advanced life developing in aged persons are equally unfavorable.
The treatment of epilepsy due to heat-stroke is by no means satisfactory, and, though the attacks are often separated by long periods, they are apt to recur in spite of drugs.
Gowers has prepared several valuable tables which show the influence of age upon recovery. He says: “The following table shows that age has a distinct influence on prognosis. The percentage of the unimproved [p. 498] cases to the whole is 30 (43:143::30:100). The percentage of the cases commencing at each age arrested and unimproved is stated, and between brackets is indicated the excess of the arrested or unimproved cases at each period of life over the proportion for the whole 30 and 70 per cent. respectively:
| ———Cases.——— | ———Percentage.——— | |||||
| Unimproved. | Arrested. | Unimproved. | Arrested. | |||
| Under 10 | 14 | 29 | 32.5 | (+2.5) | 67.5 | |
| From 10-19 | 23 | 45 | 34 | (+4) | 66 | |
| 20 and over | 6 | 26 | 19 | 81 | (+11) | |
| 43 | 100 | 30 | 70 | |||
Thus, the proportion of the cases commencing under twenty in which arrest was obtained is considerably less than the proportion of cases commencing over twenty, the difference amounting to about 13 per cent. The period of the first twenty years of life at which the disease commences has little influence, but the prognosis is little better in the cases which commence under ten than in those which commence between ten and twenty: arrest is more frequently obtained. The cases which commence in women at the second climacteric period are also obstinate, although not sufficiently numerous to be separately given.”
He also finds, from an analysis of the same cases, the fact noted by others, that the prognosis is favorable in inverse proportion to the duration of the disease.
Attacks which chiefly occur in the daytime are much more amenable to treatment than the nocturnal seizures, and especially is this the case in the tongue-biting form. Sudden blows upon the head or falls have been known in isolated cases to effect an amelioration in the patient's disease, but these examples are rare.
The existence of an aura is much better than if none existed.
Death from the attack itself is rare, yet in the large pauper institution with which I was connected for many years I have known of several cases. More often the death results from asphyxia resulting from a bolus of food which chokes the patient or from a fall in some dangerous place—into the fire or elsewhere. Accidental death from drowning is more common than any other form.
The status epileptica into which patients sometimes pass who have had many convulsions is occasionally a fatal termination of the malady, and is always a serious feature.
The influence of different epochs in life is worthy of consideration: of menstruation, of marriage, of pregnancy, and of the menopause there is much to be said. I have sufficiently spoken of the establishment of the menstrual flow, and I would only add another word of caution against giving a too favorable prognosis except in those cases of very recent origin. Marriage appears to have very little to do with changing the attacks, unless they be of an hysteroid character. I have never known epilepsy to influence the course of a pregnancy in any unfavorable way, and I think this has been the observation of others. Gowers refers to cases in which the attacks ceased during the time the mother was carrying the child.
The occasional bad influence of the pregnant state has been illustrated [p. 499] by a case reported by Terrillon.43 This example was a woman who had been the victim of epilepsy of hereditary origin since her seventh year. At the commencement of menstruation her attacks became periodic, and recurred every two months, and she had several two or three days before the flow. Two pregnancies followed several years afterward. During the periods they were increased in number and severity, and occurred several times daily. She had more attacks at this period than in all the time after delivery.
43 Annales de Gynécologie, June, 1881, p. 401.
I have found that the relief of uterine flexion or the establishment of menstruation has exercised a decidedly modifying influence for the better in several cases.
Sometimes the disease is interrupted by the menopause, but very often in my experience it has changed in type and been followed by mental degeneration.
The prognosis of the epileptoid mental state is serious in the extreme, and even when in early life the attacks are aborted or changed to perversion of the intellect or emotions existing as a complication, the hope of cure dwindles almost to nothing.
The spontaneous cure of epilepsy is rare. Its course, however, is more often interrupted by some intercurrent disease. Of 33 cases observed by Delasiauve in which there was some complicating disease, such as erysipelas, pneumonia, pleurisy, acute articular rheumatism, burns and contusions, scarlatina, erythema, or the condition of pregnancy, it was found that in 25 cases there was a decided improvement (une heureuse influence), and in 8 only was there no modification of the attacks. Axenfeld is disposed to believe that acute and febrile disorders more decidedly influence the course of epilepsy than those of a chronic nature. The influence of either may be small or may diminish the number of attacks without curing the disease.
TREATMENT.—The treatment of epilepsy depends so much upon the form of the disease that no arbitrary rule can be laid down upon general principles, and we must bear in mind the necessity for removing the exciting causes if possible, the preservation of the balance of cerebral blood-pressure and cell-equilibrium, and the nutrition of the cerebral mass. It may be our purpose to remove various toxæmic or cachectic states as well. As a minor division of treatment we must consider the abortion of the attack when auræ are detected. It has been the custom, I think among too many, to manage the disease in an empirical manner, depending upon some routine course of treatment, such as the indiscriminate use of the bromides, for example. I am convinced that the intractable character of the disease has come to be greatly exaggerated through failures attendant upon the wholesale use of the bromic salts, without regard to the indication in each particular case. It behooves us first to select a reliable bromide, and then to give it with relation to the time of the fit, its severity, and the condition of the individual. The importance of this has impressed me very often. An equally divided daily dose will not do a patient who has matutinal attacks the same good as will a large dose at night, and in certain anæmic individuals the bromides very often increase the attack. Then, too, the cases in which seizures of petit mal predominate are not benefited to the extent that those are in which [p. 500] the repetition of severe attacks is the feature. The bromide should always be well diluted and given when the stomach is empty or nearly so. The bromide of sodium is, to my mind, the most serviceable salt, and when given alone or combined with the bromide of ammonium is better than the potassic salt or the various others. It should be carefully kept in solution or in waxed-paper powders in a tight preserve-jar. As to its method of administration, I much prefer the use of a solution which shall combine other adjuvants which I will presently mention, and separate powders as well, which may be used to reinforce the dose. The latter are to be employed by the patient in the event of an unlooked-for series of attacks, and are to be used to the point of producing mild bromism at the time. In certain cases it is all-important to take into consideration the condition of the heart. In some cases where there is manifest and continued cerebral congestion, with full vessels and hard pulse, I have found that the combination with chloral or aconite was desirable. In other cases where the heart's action was irregular and weak my experience with digitalis and nitro-glycerin or with strychnine was most happy. In those cases that passed large quantities of clear urine of low specific gravity the action of nitro-glycerin and digitalis has been most prompt, and the same has been true of epilepsies of migrainous origin.
There have been various methods of using the bromide suggested which are more or less practical. The writers of a few years ago suggested the prompt production of bromism—a state in which the patient should be kept for a long time. This I strongly disapprove of, not only because the mental and physical depression is a very disagreeable and sometimes permanent condition, but because I have found that the attacks are often increased after a time, though at first they may have been suppressed. Others believe in giving the bromides at intervals, with periods when no medicine at all is administered.
For my own part, I am in favor of the establishment of a mild bromism which does not extend beyond a slight anæsthesia of the fauces or the appearance of slight acne. If I find it necessary to increase the dose, I give cod-liver oil, iron, and bark or some of the many preparations of the hypophosphites for a time; and they do not diminish the specific effects of the drug to any great extent. In the event of a series of attacks I direct the patient to take an extra dose at such time as will anticipate the seizure.
This treatment should be kept up for at least two or three years after the attacks have disappeared, and it may be even necessary to continue a bromide course in a small way for an unlimited period.
If there be an hysterical element, or if ovarian excitement is supposed to have anything to do with the attacks, the combination of cannabis indica is strongly recommended. This suggestion holds good in the cases where migraine is associated with the epilepsy, or the latter is an outgrowth of the former.
Next to the bromides of potassium and sodium I have been very successful with the nickel bromide. I find that it is retained with little trouble, producing no gastric derangement if taken after eating. A syrup prepared by most of the good pharmacists is preferable to any other method of administering the salt. Quite recently Leaman44 has reported [p. 501] two cases of severe epilepsy which were greatly benefited. His conclusion is that it does most good in the form of the disease when the attacks are separated by long intervals.
44 Med. News, Apr. 18, 1885.
The bromate of potassium, which has been used by Weir Mitchell45 and Hinsdale, may be worthy of a trial. It should never be given, however, in larger doses than five or ten grains thrice daily. These investigators found that thirty grains slowed the heart very considerably, and forty grains produced watery discharges from the bowels and drowsiness. In their hands, notwithstanding these disagreeable effects, it controlled the seizures. The hydrobromate of conia is a comparatively new remedy which has been recommended. My own experience does not support that of Wolfenden.46 Severe cases were treated by him with benefit. The dose he recommends is half a grain, and not more than four and a half grains are to be given in twenty-four hours. Headache and dizziness attended its use.
45 Med. News, Dec. 27, 1884, p. 718.
46 Practitioner, June, 1884.
Erlenmeyer47 is an advocate of the mixed treatment, and his best results have been obtained by combining the bromides of potassium, sodium, and ammonium in the proportion of 1:1:½. He thinks much greater permanency of effect follows such a combination. A curious result witnessed by this author is the fact that the acne produced by one salt given alone is apt to disappear when the combination is administered.
47 Centralblatt für Nervenheilkunde, Psychiatrie, etc., No. 18, 1884.
A solution of hydrobromic acid, prepared after Fothergill and Wade's formula, is recommended by H. C. Wood of Philadelphia,48 who presented the record of its use in twelve cases of obstinate epilepsy. It seems that in his hands large doses acted much better than when the bromides were given alone. He recommends ounce iij per diem. My own experience, which I detailed some years ago, was to the effect that it possessed no virtues whatever in ordinary doses. The solution is so difficult to take, and so disagreeable in every way, that many patients prefer almost any other treatment. It cannot be doubted that some cases of epilepsy are benefited by a change of treatment, no matter what, and possibly Wood's cases belong to this class.
48 Med. News, Feb. 23, 1884.
Belladonna and ergot are remedies that have had many advocates, Trousseau being the most pronounced champion of the former. Their use in the lighter attacks is attended sometimes by the most happy results, but they cannot be said to have any permanent effect. The first is advantageous because of its power to diminish reflex excitement, and in those undeveloped infantile convulsions which are often grouped under the head of eclampsia its virtues are decided. Belladonna or its alkaloid may be given in combination with the bromides. Ergot or ergotin, in spite of its undeservedly bad reputation, may be given in large doses, one to two drachms of the tincture thrice daily, or five grains of the aqueous extract in the course of the day. Of chloral there is not much to be said. At one time it was thought to possess great virtues, especially in combination with the bromides, but subsequent experience has taught me that its use has many drawbacks, and only in exceptional cases is it to be recommended—viz. in those in which there is a disposition to excitement—either as a substitute for the attack or as a sequel.
[p. 502]The use of the iodide of potassium in combination with the bromides is of great service in symptomatic epilepsies or those of syphilitic origin. The iodide should be pushed, so that the patient may take three or four drachms daily, and its injurious gastric action and unpleasant taste may be done away with by administering it in large quantities of milk or some mild alkaline water, such as Vichy. Among the other remedies used and advocated by various writers are hyoscyamine, the salts of zinc, chloral, the ammonio-sulphate of copper, picrotoxin, strychnine, curare,—all of which have little or no effect in permanently changing the course of the disease. Cerebral galvanism, if properly employed, is certainly worthy of a trial as an adjuvant.
As abortants we may resort to diffusible stimulants—ammonia, alcohol, or some carminative. If the aura be perceived, a drachm of the aromatic spirits of ammonia or a glass of sherry will often prevent subsequent developments, and the inhalation of ten or fifteen drops of nitrite of amyl will avert the attack. Nitrite of amyl may be conveniently used in the form of pearls, which may be first crushed in the handkerchief. The nitrite of soda, which has been recommended as a substitute, is an unstable and dangerous drug, and is not to be recommended.
I called attention some years ago to the virtues of nitro-glycerin as an abortant in epilepsy. It may be given in alcoholic solution or tablets from 1/50–1/25 of a grain at a dose, to be perhaps repeated. Great care should be taken to procure a reliable preparation.
When a sensory aura proceeds from a particular locality in preference, the application of some local form of irritant is strongly recommended. A blister or light touch of the button of the actual cautery will do, and if the point of origin be one of the extremities a circular blister or cautery-line, after the method recommended by Buzzard, will be serviceable in the treatment of the case.
Buzzard has observed the fact, in several of his patients who complained of a sensory aura in the biceps, that when an encircling blister was applied just above this spot the attacks were aborted. In more than one of his cases of partial epilepsy the extraordinary result of a transfer of the convulsion to the other extremity is noted. He found that the circle should be complete, for a blister which half encircled the arm did no good. I have used the same treatment in cases of writer's cramp with marked benefit.
Brown-Séquard has pointed out the good effects of forcible and painful extension of one finger or toe if the aura is of sufficient duration to enable the individual to resort to this procedure.
The condition known as the status epilepticus is best treated by amyl nitrite, which can be administered frequently. Repeated doses of nitro-glycerin, so that its full effects are produced, do more good than chloroform or any of the well-known anæsthetics.
Of setons I have very little to say. At best, they are a barbarous and painful mode of treatment, and, although cures have been effected, I have never been much encouraged by their so-called influence.
Certain intractable cases are helped by surgical procedure, and trephining has sometimes resulted in a cure. I know of one brilliant result obtained by Leo of this city in an old epileptic, in which the use of the instrument over the occipital region resulted in a complete removal of [p. 503] the disease. It is especially recommended in cases in which the form of the attacks bears some relation to the probable disturbance of the cortical motor-centres; and even in such cases there must be constancy in the method of expression of the convulsion. So often do we find meningeal thickening of an extensive district that it is manifest that trephining would do little or no good. The statistics of the operation are unsatisfactory, for in the large mass of testimony there is great want of exactness as to the pathological suggestions of the attack, and a great deal about the method of procedure and recovery from the operation itself, and very little about the phenomena of the disease.
The diet of the epileptic should be of the most simple kind. Merson,49 whose carefully-prepared paper is full of valuable statistics, is strongly in favor of vegetable diet, and his results are encouraging. I am convinced that many children never would have become hysterical or epileptic but for injudicious indulgence in animal food. Whenever possible, I confine my patient to a diet of fish, poultry, and fresh vegetables, with fruit. As an exciting cause the overloading of the stomach has so often precipitated attacks as to lead Paget and others to invent the term gastric epilepsy for this form of the disease. The greatest care must be paid not only to diet, but to the general habits of the patient—over-exercise, especially after eating, the avoidance of hot places and high altitudes. A residence by the seashore is preferable to mountainous places; and excitement, over-study, and all agencies favoring cerebral congestion are to be avoided.
49 West Riding Reports, vol. v. p. 1.
DEFINITION.—These neural disorders consist of a certain train of nervous symptoms, such as spasm, paralysis, pain, tremor, vaso-motor disturbances, etc., either alone or in more or less complicated combinations, which follow certain muscular acts and are occasionally accompanied by a marked condition of general nervousness; they occur in many of the occupations of every-day life that require for their performance a constant muscular strain combined with more or less delicate movements of co-ordination continued for long periods at a time.
SYNONYMS.—Among the terms used to designate the various forms of the affections produced in the manner just stated may be mentioned the following:
Special Terms.—Writers' cramp, Scriveners' palsy, Steel-pen palsy, Chorea scriptorum, Paralysis notariorum, Graphospasmus, Mogigraphia, Crampe des écrivains, Nevrose des écrivains, Schreibekrampf, Le mal télégraphique, Crampe télégraphique, Klavierkrampf, Pianists' cramp, Tailors' cramp, Loss of grip, etc.
General Terms.—Professional dyscinesiæ, Professional impotence, Anapeiratic paralysis, Nevrose co-ordinatrice des professions, Functional spasm, Fatigue diseases, Professional hyperkineses, etc.
None of these terms are satisfactory, and, in fact, it is difficult to fine one that will include the various symptoms arising from the habitual use of a muscle or group of muscles, in the same way for long periods at a time, in the different occupations known to give rise to these neuroses, without including diseases belonging to entirely different classes.
It is with some hesitation that I suggest the term copodyscinesia (κόπος, toil, weariness, fatigue; and δυσκινησια—δυς, faulty, difficult, hard, and κινησις, motion, movement) as signifying difficult or faulty motion due to constant repetition of the same act.
HISTORY.—Some of these neuroses have been recognized for years; this is particularly true of writers' cramp, the earliest notice of which I have been able to discover is in a small work by Ramazini,1 printed in 1746.
1 Bern. Ramazini, Treatise on the Diseases of Tradesmen, etc., translated by Dr. James, London, 1746.
Most of the articles upon this subject have been written during the last fifteen or twenty years.
[p. 505]ETIOLOGY.—Many of our every-day actions, which we perform almost automatically, are the result of months and even years of practice; this is well exemplified in the act of writing. At first each letter is made by a separate and deliberate act of volition, and considerable thought has to be expended upon its formation; but little by little the preponderance of the volitional element decreases, until at last we write with but little consciousness of each separate movement, and the act becomes almost an automatic one, the sentence being conceived and the hand committing it to paper with but little thought of the intermediate muscular acts. In a somewhat analogous manner do we learn to walk, each movement being laborious and requiring much thought for its execution: in addition to this, we must regulate the amount of the movement and keep in abeyance all associated muscular action.
This last is spoken of by Hasse2 as an important factor in the etiology of these affections. When, however, any one of the various muscles whose integrity is necessary for the automatic performance of any act becomes affected, let the lesion be in the muscle itself or anywhere in the nerve-substance between it and its centre, or in that centre itself in such a way as to hinder its free response to the nervous stimulus, then the will has to be especially directed to the act in order to counteract the effect of the disability, and some other muscle or group of muscles must be substituted in the place of the one incapacitated. That which was previously performed easily and without fatigue now becomes difficult and exhausting.
2 Handbuch der speciellen Pathologie u. Therapie, “Krankheiten des Nervensystems,” 1te A., Bd. iv., 1869.
It will be in place here to consider in detail the action of the muscles concerned in performing one or two of the acts most prolific of the affections under consideration.
The first of these that will be examined is the act of writing.
Generally speaking, the methods of writing may be divided into two: 1st, where the fingers do all the stroke movements, the arm remaining quiescent except for the lateral movement; 2d, where the pen is held steadily by the fingers and the letters formed by the movement of the whole arm. In the latter the muscles of the hand and forearm are used almost entirely for pen-prehension and poising, although there is generally a slight finger movement for the long strokes; the forearm is allowed to rest upon the bellies of the flexor muscles as a sort of movable fulcrum, the pectorales, teres major, and latissimus dorsi, together with the biceps and triceps, being mainly employed in forming the letters.
This last method of writing is the one mostly taught in the public schools at the present day; and as a large number of muscles are brought into play, and as there is a more even division of the work, it is claimed that fatigue is not so soon complained of as in the first or older method.
The act of writing is primarily divisible, according to Poore,3 into three acts: 1st, the act of prehension; 2d, the act of moving the pen; 3d, the poising of the forearm and hand. The muscles concerned in the act of prehension are—the first two dorsal interossei, the opponens, abductor, and flexor brevis pollicis, and, to some extent, the flexor longus pollicis and the extensors of the thumb. The adductor should also be included in this enumeration.
3 G. V. Poore, Electricity in Medicine and Surgery, London, 1876.[p. 506]
The muscles employed in the movement of the pen differ somewhat according to the method of writing. In the finger movement Poore enumerates the following muscles as the ones used, viz.: flexor longus pollicis, extensor secundi internodii pollicis, flexor profundis digitorum, extensor communis digitorum, and also, to a lesser degree, the interossei.
In the second method of writing these muscles are comparatively quiet, except in making the letters which extend far above or below the line, while the muscles previously mentioned when describing this method are the ones called into play. The poising of the arm and hand is mainly accomplished by the supinator longus, supinator brevis, and possibly by the extensors of the thumb.
From a study of what has been written it will be seen that there are two classes of muscular actions concerned: 1st, the steady contraction of the muscles that poise the hand and hold the pen; and 2d, the intermittent contractions of the muscles concerned in moving the pen: both of these classes are equally important in the etiology of writers' cramp.
Chronic fatigue of the muscles is undoubtedly, in some cases, a precursor, if not a cause, of copodyscinesia, and, according to Poore,4 is occasionally the expression of hyperæmia or mild inflammation of a motor nerve. Acute local fatigue has symptoms which are well known to us all after having taken violent exercise, cramp and pain being the two most prominent ones.
4 “Writers' Cramp and Impaired Writing-Power,” Medico-Chirurgical Transactions, vol. lxi.
Any student who has dissected much has experienced the intense feeling of fatigue in the muscles required to hold the dissecting forceps, particularly when the spring is a little too strong. Much the same thing is noticed when one who has not been accustomed to write much is for some cause compelled to do so; he will probably notice that in a few hours he is exerting a greater amount of muscular force in pen-prehension than usual, and may even find that he is producing a disagreeable feeling in the distal phalanges by the pressure he is using; he will also probably be aware of a burning sensation between the shoulder-blades.
These symptoms are in all probability dependent upon, or are at least coincident with, a hyperæmia of the nerves and spinal cord, and, if persisted in for a long time without proper intervals of rest must sooner or later interfere with the healthy condition of the spinal cord, as well as of the nerves and muscles of the hand and arm.
Poore, while considering the symptoms of fatigue as in large part peripheral in origin, readily admits that they must generally be accompanied by central changes.
The manner of writing and of holding the pen is of considerable influence in the causation of this trouble. Practically, the fluent writer is more apt to contract this affection than he who writes badly, for the latter seldom obtains a position where steady copying is to be done; theoretically the reverse is true if the amount of work in the two cases is the same.
When the pen-holder is allowed to drop below the head of the first metacarpal bone the movements of the fingers are restricted; the middle and fore finger upon one side of the holder and the thumb on the other act upon the principle of the toggle-joint, so well known in mechanics, and, [p. 507] as the pen-holder is drawn backward to make a stroke, bind the distal phalanges tightly against the holder: this in a short time causes fatigue and awkwardness in writing; but if the holder is made to cross the proximal extremity of the first phalanx of the fore finger the toggle-joint movement is destroyed.
These remarks apply of necessity more strongly to the finger movements than to the conjoined finger-and-arm movement.
Writing with a pencil is not as liable to bring on fatigue and nervous trouble as pen-writing, this being mainly owing to the fact that with the former no particular angle is required to be maintained between the point and the paper; there is therefore less effort at poising, as the pencil may be rotated at pleasure, while with the pen one angle has to be maintained. The same remarks should apply to the fluid pencils (stylographic and Mackinnon pens) now so universally used; in fact, they have been considered by Putnam5 as much easier to write with than the pencil, as less weight need be applied upon the tip in order to write.
5 J. J. Putnam, M.D., “A New Adjuvant in the Treatment of Writers' Palsy,” Boston Med. and Surg. Journ., vol. ci. p. 320, 1879.
The idea that these troubles of writers were due to using steel pens, as once thought, is manifestly without foundation, as the affection was recognized before the time of the introduction of steel pens, which was from 1800 to 1820.
Fine sharp pens are, however, more productive of evil than composition pens or those with a broad soft nib, as they do not move as easily over the paper, and therefore introduce a difficulty, although a slight one, in the act of writing. The theory that the chemical action between the ink and the metallic pens, and the friction of the pen on the paper, generate sufficient electricity to affect the fingers through the medium of the metallic portion of the pen-holder is too preposterous to mention, except to show what curious reasons are given in attempting to explain obscure and difficult subjects.
The next occupation which very frequently gives rise to these affections is telegraphy.
The invention of the Morse telegraph in 1844, and its general introduction, both here and abroad, a few years later, has proved a most fertile source of copodyscinesia, although but little has been written on this form of neurosis, Onimus,6 Robinson,7 and Fulton8 being among the few to describe it, although several later writers mention its existence.
6 “Le Mal télégraphique ou Crampe télégraphique,” Compte Rend. Soc. de Biol., 1878, 6, S. V. 92-96; also “Crampe des Employés au Télégraph,” Gaz. méd. de Paris, 1875, p. 175.
7 Edmund Robinson, M.D., “Cases of Telegraphists' Cramp” (4 cases), British Med. Journ., Nov. 4, 1882.
8 Thomas Weymss Fulton, “Telegraphists' Cramp,” Edinburgh Clin. and Path. Journ., Feb. 2, 1884.
Telegraph operators, particularly those employed in large cities, whose time is nearly all taken up with their work, are more exposed to the causes of copodyscinesia than those following other trades. They are not only exposed to the danger of contracting the affection by using the telegraph-key in transmitting messages, but when not so employed are receiving messages by sound and writing them down, frequently at the rate of thirty to forty, or even more, words per minute. Thirty words a minute is good telegraphy: this would require, on the average, nearly 600 [p. 508] separate contractions. This would be 36,000 contractions per hour, while to write the same sentences would require about 10,000 less.
The operators employed by the Associated Press, although comparatively few in number, two hundred probably including all in the United States, write for hours at a time, using a stylus and manifold writing-books, making as many as twelve copies at one writing; this obliges them to grasp the stylus very firmly and to press with considerable force, making the act of writing much more difficult.
In addition to the work mentioned above, those who have large numbers of messages to transmit become so expert that to save time they make a record concerning the last message sent with the left hand, while they are telegraphing the next one with the right hand. A complicated act of co-ordination is thus being performed with each hand, the difficulty of which may be appreciated by any one if he but try to perform it.
An editorial in the London Lancet9 states that “telegraphers' cramp will, we have little doubt, take its stand among the last-mentioned curiosities” (milkers' cramp, hammer palsy, etc.), and "that the telegraph clerk usually enjoys repeated intervals of complete rest, and runs consequently hardly any risk.”
9 1875, vol. i. p. 585.
Hammond10 likewise states that telegraphers' cramp is rare in the United States, but a slight investigation proves these two statements to be, unfortunately, very far from the truth. According to recent statistics,11 the Western Union Telegraph Company employs nearly twenty thousand operators, who transmit annually over thirty-five million messages, and as investigation seems to prove that a very large number, if not the majority, sooner or later show some symptoms of copodyscinesia, it becomes evident that this neurosis is far from rare, although hitherto almost entirely overlooked by the medical profession.
10 Wm. A. Hammond, M.D., Dis. Nervous System, 6th ed., New York, p. 789.
11 J. B. Abernethy, Commercial and Railway Telegraphy, Cleveland, Ohio, 1883, 2d ed.
Operators are very loath to confess that they are suffering from loss of grip, as they have termed it, for then they are considered as less efficient than formerly, and may be asked to resign in favor of one not affected, or be lowered in their salary—a point of great moment, as telegraphy is their means of support. This accounts for the apparent small number of the cases.
In telegraphing, the knob of the key, a circular disc of hard rubber more than one inch in diameter, and placed about one and a half inches above the level of the table, is grasped, as a rule, between the thumb and middle finger, with the tip of the index finger resting on top, the position being quite analogous to the method of pen-prehension, the strain, although much less, falling on the same muscles, but as all lateral movements of the key are impossible, the muscles employed in poising are not brought into play as in writing. The arm is either allowed to rest upon the table, upon the flexor mass of muscles of the forearm near the elbow as a kind of movable fulcrum, or is held with the forearm parallel to the table and a short distance above it.
The movements of telegraphing are made by the alternate action of the triceps, which depresses the wrist by extending the forearm, assisted by the flexor carpi radialis, flexor carpi ulnaris, flexor sublimis, and flexor [p. 509] profundus digitorum on the one hand, and the biceps and supinator longus, which elevate the wrist by flexing the forearm, assisted by the extensor carpi radialis longior, extensor carpi radialis brevior, extensor carpi ulnaris, and extensor communis digitorum on the other.
The movement of the key-knob, being about the one-twenty-fifth of an inch, is so slight that it may be entirely ignored, so that with the fingers upon the key and the forearm resting upon the table near the elbow the motion must be a downward and upward one of the wrist; when, however, the arm is held above the table and parallel to it, the motion is more extended, the shoulder-muscles being used to support the arm.
The wrist is held in a supple manner, and not rigidly, the momentum of the downward movement being used to close the circuit; this, as before stated, is made mainly by the triceps, and is checked by the flexors and supinator longus.
The extensors of the wrist and fingers have a double duty to perform, for, besides assisting in recovering from the downward stroke, they have to support the hand during the whole act of telegraphing, in order to prevent the weight from resting on the key, which would prevent quickness in making and breaking the circuit.
On long circuits, particularly in wet weather, when much electricity escapes from the line, the movements have to be made with much more decision than usual in order to make the signals intelligible at the distant station.
The accompanying diagram shows well the movement of the wrist as above described, the hand and wrist moving into the position of the dotted lines when the downward stroke is made.
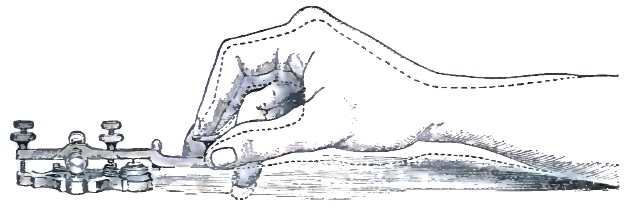
Our hand is essentially a prehensile organ, and as such causes us to educate the flexors the most; the extensors, being mainly used to relax the grasp of the fingers, are weaker, and the constant strain spoken of above, being thrown upon them, explains the fact that in telegraph operating these are the muscles most frequently attacked by cramp. (See Symptomatology.)
The following figures are of interest as proving the great superiority, in point of strength, of the flexor over the extensor muscles of the wrist and fingers. The measurements were made by the dynamometer of V. Burq, great care being taken to apply the instrument upon corresponding points of the palmar and dorsal surfaces of the hand. The grasp of the average man, which includes all the flexor muscles of the fingers and thumb, equals 125 pounds, while the power of the flexors of the wrist, exclusive of the fingers, equals 40 pounds. In marked contradistinction [p. 510] to this the extensors of the wrist register 35 pounds, and the extensors of the fingers only 7. The total power of all the flexors is therefore 165 pounds, and that of the extensors 42 pounds, nearly four times less (3.92). In women the ratio is the same, although the number of pounds registered is about half.
From the foregoing enumeration of the muscles used in writing and telegraphing it may be seen that the brunt of the work does not fall on the same muscles in the two acts, so that operators are seen utterly unable to telegraph more than a few words intelligibly who can still write a fluent hand. The two forms of neuroses often coincide in the same subject, as all telegraphers are of necessity scriveners; in fact, the majority suffer from both forms, and as a rule the most difficulty is experienced in telegraphing, and not in writing, although the reverse is frequently seen. But rarely does one see an operator who, unaffected as far as telegraphing is concerned, has difficulty in writing on account of this curious neurosis.
Of the muscles enumerated in the foregoing discussion, six are supplied, either wholly or in part, by the ulnar nerve—namely, the first two interossei, adductor pollicis, flexor brevis pollicis (inner half), flexor carpi ulnaris, and flexor profundus digitorum (inner part); and seven by the median nerve wholly or in part—namely, the opponens and abductor pollicis, flexor brevis pollicis (outer half), flexor longus pollicis, flexor profundus digitorum (outer part), flexor carpi radialis, and flexor sublimis digitorum.
The remaining important muscles are supplied by the musculo-spiral and its branches, except the biceps, which is supplied by the musculo-cutaneous.
The ulnar nerve supplies fifteen of the muscles of the hand; many of these are not prominently brought forward in writing, but are more or less used in keeping the hand in the required position.
Poore, after a careful study of 32 cases of undoubted writers' cramp, found the muscles affected in the following proportions:
| Interossei | (supplied by the ulnar nerve) | 18 times. |
| Extensors of the thumb | (supplied by the musculo-spiral) | 10 times. |
| Flexor brevis pollicis | (supplied by the median and ulnar) | 7 times. |
| Abductor pollicis | (supplied by the median) | 7 times. |
| Flexor longus pollicis | (supplied by the median) | 4 times. |
| Adductor pollicis | (supplied by the ulnar) | 3 times. |
| Opponens pollicis | (supplied by the median) | 2 times. |
| All the muscles of the forearm, more or less, | 2 times. | |
—showing that the muscles supplied by the ulnar nerve were affected more often than those supplied by the others.
The musculo-spiral and its branches supply the extensors of the thumb, fingers, and wrist, besides the two supinators; and by referring to the muscles most called into action in the act of telegraphing it will be seen that the majority are supplied by this nerve and by the median, which supplies the majority of the flexors. This statement explains to a great extent the fact that telegraph operators may be unable to telegraph and yet be able to write, as the muscles most important in the two acts have not the same nerve-supply.
The integrity of these nerves is therefore of the first importance in all [p. 511] cases requiring the use of the fingers and forearm, and many cases of copodyscinesia undoubtedly have a subacute inflammation of these nerves, or at least a congestion of the same, as their foundation, the neuritis or congestion being overlooked, owing to its mild type.
S. Weir Mitchell12 states that subacute neuritis is often incapable of distinct clinical discrimination when of a mild type and when there is an absence of traumatic cause. Mills13 states that “a lesion of the sensitive fibres profoundly affecting this power of conducting impressions may not cause pain, and that pain is not a necessary symptom of inflammation of a mixed nerve: this is an important fact, as I think too much stress is often laid on pain as a symptom of neuritis, leading to error in diagnosis and treatment.”
12 Injuries of Nerves, and their Consequences, by S. Weir Mitchell, M.D., Philada., 1872.
13 F. T. Mills, M.D., “On Two Cases of Neuritis of the Ulnar Nerve,” Maryland Med. Journ., vol. viii. p. 193, 1881.
Other Forms of Copodyscinesia.—In violin-playing the bow is held steadily between the fingers and thumb for long periods at a time, and the left arm is forcibly held in supination in order to bring the fingers upon the strings—actions well calculated to cause trouble if persisted in, not taking into account the rapid movements of the fingers which are necessitated in playing and the movements of the arm in bowing. The violinist is therefore liable to suffer in both arms, but in a different manner in each, as different muscles are used in bowing and in fingering.
The other musical instruments necessitating great education in the movements of the fingers and wrist are also liable to cause these neuroses, but this is not true of those wind instruments which require education of the movements of the lips and tongue. Piano-playing is a frequent cause of these troubles, which have been known to appear quite suddenly during the practising of some difficult piece.
In fact, all occupations which require a muscle or a group of muscles to be kept in a constant more or less firm contraction, together with fine movements of co-ordination in themselves and in the neighboring muscles, may be expected to furnish cases of this class of disease; the muscles affected necessarily varying with the work done, mere routine work being more liable to cause trouble than that which is new and original, as in the latter case time has to be taken to elaborate it, thus giving temporary rest to the muscles.
Besides the forms already mentioned these neuroses have been known to effect compositors, engravers; seamstresses, tailors, from using the needle or scissors; cobblers; bricklayers, from using the trowel; artificial-flower makers; weavers; milkers; painters; dentists; ballet-dancers, from standing on their toes; blacksmiths and those using the hammer; carpenters, from using the saw and screw-driver; electrical-instrument makers, from winding coils; turners; watchmakers; fencing-masters; cigar-makers; makers of photographers' gelatin plates; knitters and those using the crochet-needle; billiard-players; counters of money; dressers of hides; pedestrians; and a few others.
Writers, telegraph operators, and musicians are those which by far are the most frequently affected, the others being almost curiosities. Among the latter may be mentioned the case, recently coming under my notice, of pain in the right forefinger and arm, with cramp in the former, upon [p. 512] any prolonged attempt to read with this finger the raised letters of the alphabet of the blind. The patient was a blind woman depending for her living upon crocheting, which occupation was also seriously interfered with by this trouble.
After inquiring, in factories, etc., I find that the disease is by no means a recognized one among the workmen. Among telegraphers, however, it is so well known that they have called it the loss of grip, while in France it is known among them as le mal télégraphique.
Gardner,14 after a careful investigation, finds no proof that physical disease originates in, or is even aggravated by, the use of the sewing-machine, and he has “never even heard of a case of cramp.” He comes to this conclusion after having visited many large factories where sewing-machines are used and worked by foot-power; his remarks apply to those machines where the feet are worked together, and not alternately, which last has been known, according to Down,15 to cause serious troubles, of an entirely different kind, however, from the one under consideration, and with which this subject has nothing in common.
14 A. K. Gardner, M.D., “Hygiene of the Sewing-Machine,” Am. Med. Times, Dec 15-29, 1860.
15 “Hygiene of the Sewing-Machine,” London Lancet, 1866, vol. ii. p. 447.
PREDISPOSING CAUSES.—Tobacco and Alcohol.—Both of these articles exert a powerful effect upon the nervous system, tobacco particularly being a factor in the causation of many cases of neurasthenia. The first effect of tobacco and alcohol in small doses on the brain and spinal cord is, according to Boehm and Von Boeck,16 that of an excitant; subsequently it acts as a depressant. Eulenburg17 mentions tremor as of very frequent occurrence, and states that he has frequently noticed it in young cigar-makers who smoke to excess.
16 Ziemssen's Cyclopædia, Amer. ed., vol. xvii.
17 Ibid., vol. xiv.
Cigarettes are more injurious than other forms of tobacco used in smoking, as the smoke is nearly always inhaled, a greater effect being thus produced by a given amount of the drug. Besides this, cigarettes contain a large amount of other substances deleterious in their effects. Trembling of the fingers and hand is frequently seen in those smoking cigarettes freely.
The majority of the cases of copodyscinesia that are in the habit of using either of these articles acknowledge that their use increases their disability; in very exceptional cases the moderate use of tobacco appears to soothe and quiet, and thus relieve some of the symptoms.
Age.—Copodyscinesia is a disease of early adult life; it is rare in old age. In 39 out of 43 cases of telegraphers' cramp coming under my notice the age of the patient at the outset of the disorder could be accurately determined. The average was 23.94 years. The average age of all cases of the various forms of copodyscinesia seen by me up to the present time (1886) is 25.96 years.
Sex.—The influence of sex as a predisposing cause of these affections has not been studied with sufficient care, although a few authors allude to it.
Onimus18 states that women are more frequently affected than men with telegraphers' cramp. Erb19 states that writers' spasm is met with more [p. 513] frequently in men, much more rarely in women, and that pianoforte-players' spasm occurs more frequently in women, and particularly in neuropathic persons who belong to nervous families. Hasse20 and Romberg21 consider that writers' cramp especially occurs in men, women being affected very rarely. Of the 75 cases of impaired writing-power reported by Poore,22 only 17 were women, while of the 31 cases of undoubted writers' cramp included in the 75, all were men.
18 Loc. cit.
19 “Writers' Cramp and Allied Affections,” Ziemssen's Cycl., Amer. ed., vol. xi.
20 Loc. cit.
21 Nervous Diseases, vol. i. p. 320.
22 Loc. cit.
It may be seen that the male sex has been employed far more frequently than the female in most of the occupations previously mentioned, so that a larger percentage of men would naturally be affected; but now that women are being employed more generally a larger number of the female sex may be expected to suffer in this way.
Whether sex, per se, has much influence as a predisposing cause is difficult to say, as statistics are wanting, but it is probable that with the same amount of work given to each sex a large proportion would be found among women.
Women are being employed to a considerable extent in telegraphy, and although I have been able to collect but 4 cases of this form of copodyscinesia affecting women out of a total of 43, I have reason to believe it is quite common among them, my mode of collecting statistics (soliciting replies to printed questions) being much more likely to give a larger percentage of answers from men.
Hereditary Influence and Nervous Temperament.—Both of these factors seem to play an important rôle as predisposing causes to these affections. Cases are on record where several members of the same family were the subjects of writers' cramp. The statement made by Erb (vide supra), that neuropathic persons and those who belong to nervous families are more subject to these affections than others, seems to me to be true, at least to a great extent, for a careful inquiry into the history of cases coming under my knowledge has quite often elicited the statement that migraine, functional spasm, epilepsy, hay fever, neuralgia, writers' cramp, telegraphers' cramp, or general neurasthenia has existed either in the immediate family or in the patients themselves. Hasse23 is also of the same opinion.
23 Loc. cit.
Whittaker24 states that many of the cases coming under his notice, if not the majority, occurred in individuals of irritable nervous temperament, subject themselves to, or the descendants of parents afflicted with, migraine, chorea, epilepsy, paralysis, or some form or other of neurosis, but that a certain contingent of the minority of cases occurred independently of any neurosis or any abuse of alcohol or sexual excess.
24 Cincinnati Lancet and Clinic, N. S., vol. iv. p. 496, 1880.
Fritz,25 after studying 25 cases of writers' cramp, found 7 who either stuttered, squinted, or had choreoid movements or œsophageal spasm at the same time; but it is probable that a few of these cases at least were due to some central lesion (post-paralytic chorea?).
25 “Ueber Reflexionsfingerkrampf,” Oesterr. Jahrb., März u. April, 1844, quoted by Hasse, loc. cit.
Beard26 holds an opinion directly the reverse of the vast majority of the authorities upon this subject, and states that this disease occurs mostly in [p. 514] those who are of strong—frequently of very strong—constitution, and that it is quite rare in the nervous and delicate; and when it does occur in those who are nervous it is easier relieved and cured than when it occurs in the strong.
26 G. M. Beard, M.D., loc. cit.
That in the majority of the cases there is an emotional factor is evident to every one who has seen a considerable number, the knowledge that some one is looking on and will notice the disability being almost sure to aggravate the symptoms. This is frequently noticed among telegraph operators, and is well exemplified in the following answer made by a female operator: “If I am working with a disagreeable or fault-finding operator, who I know will make unpleasant remarks about my sending, and break me (break the circuit) on certain difficult letters, it is almost impossible to make those letters correctly with either hand.” Again she says, “If I come to the difficult letters without thinking about them, I can make them much easier than if I look ahead in the message and see them; for instance, some time after I had ceased using my right hand on account of the cramp, an outside occurrence made me very angry; just then a message was placed on my desk, and with my mind fully occupied with my grievance I sent the message with my right hand very easily and quickly.”
Wasting Diseases.—These favor the production of these affections in those predisposed to them by occupation or otherwise, by the constant drain upon the system. Numbness of the fingers and stiffness are occasional symptoms of renal disease, and would naturally aggravate any difficulty of writing and so-forth that the patient might have. Mitchell27 reports two cases of writers' cramp dependent upon or coincident with albuminuria, which were treated in vain until the condition of the kidneys was discovered: under appropriate treatment for this condition one recovered entirely from the cramp and the other improved greatly.
27 S. Weir Mitchell, M.D., “Nervous Accidents in Albuminuria,” Philada. Med. Times, Aug. 1, 1874, p. 691.
Traumatism, etc.—Injuries, etc. occasionally act as predisposing causes; thus cases are on record where the starting-point seemed to have been an ingrowing thumb-nail, and others where it was the pressure of large sleeve-buttons upon the ulnar nerve; and tight sleeves seem to have been the starting-point of inflammatory troubles ending in writers' cramp. An inflammation of the periosteum of the external condyle (node) and a painful ulcer upon the forearm are reported by Runge28 as giving rise to symptoms closely allied to this affection. Seeligmüller29 mentions a case where the symptoms came on after an insignificant grazing bullet-wound of the knuckle of one of the fingers.
28 “Zür Genese u. Behandlung des Schreibekrampfes,” Berl. klin. Wochensch., x. 21, 1873.
29 Adolph Seeligmüller, “Lehrbuch der Krankheiten der Peripheren Nerven, etc.,” Wreden's Sammlung, Kurzer Med. Lehrb., Band v. p. 29.
SYMPTOMATOLOGY.—Owing to the fact that various causes give rise to these affections, and that the different groups of muscles implicated differ with the varying occupations of those suffering, no one stereotyped set of symptoms can be described as applicable to each case, and no one symptom can be looked upon as diagnostic.
The symptoms most frequently seen may be classified under five heads—viz.: I. Cramp or spasm; II. Paresis or paralysis; III. Tremor; IV. [p. 515] Pain or some modification of normal sensation; V. Vaso-motor and trophic disturbances.
These may, and generally do, exist in various combinations, and they may be accompanied by other symptoms of nervousness; they are not of necessity confined to the hand or arm, but may become more or less general. At first they are usually only seen after long continuance of the occupation which produced them, but later any attempt to perform this act will cause their appearance, although it may not be noticed in any other of the daily avocations.
In some of the rarer cases the neurosis makes its appearance suddenly after a prolonged siege of work. It has been generally stated that writers' cramp, for instance, only manifests itself on attempting to write, but this is due to the fact that there is no other occupation which exactly needs the same co-ordination of the muscles, for others can be substituted in the place of those affected. This is particularly seen in the early history of the cases, but when it has become pronounced in character any analogous movement, such as holding a spoon or fork or paint-brush, will be sufficient to produce it. Difficulty in buttoning the clothes with the fore finger and thumb is frequently noticed.
I. Cramp or Spasm (Spastic Form).—The first form of this disease to be considered is that in which cramp or spasm is present. This is one of the most frequent symptoms, and when present usually attracts the most attention. In most of the articles written upon these affections great importance has been given to this symptom, which, however, may be absent during the whole history of the case, but when it does appear it usually indicates an advanced stage. The term writers' cramp is an evidence of the widespread opinion of the importance of this symptom.
The cases that present themselves to the physician have usually been affected for some time, and where cramp is present an earlier examination would probably have resulted in the discovery of premonitory signs before the appearance of the spasm or cramp; and in fact it may be stated that this symptom is always preceded, or at least accompanied, by one or two more. The muscular contraction may be so slight as to amount to a mere occasional awkwardness, in writers' cramp an abnormal grasp of the pen-holder being all that is noticed; or it may be so severe as to cause a tonic contraction of the muscles affected, which may continue for some time after the exciting cause has been removed, as in the cases reported by Poore30 and S. Weir Mitchell.31
30 Electricity in Medicine and Surgery, London, 1876, p. 209.
31 “Functional Spasm,” Amer. Journ. Med. Sciences, Oct., 1876, pp. 322, 323.
As might be supposed, these spasms affect most usually the upper extremities, although they may affect the lower, as is occasionally seen in workers on the lathe and in pedestrians. Other muscles than those necessary to perform the act that has become difficult may also be seized with spasm coinstantaneous with the spasm of the affected part; thus the left arm may be the seat of associated movements while the right is being used: these are, however, most frequently seen in the affected arm when the other is being used to relieve it; they may also be noticed in the legs, although much more rarely.
Gallard32 reports a case of a street-pavior who had associated spasm of [p. 516] both sterno-cleido-mastoid muscles, which came on only when using the instrument to settle the stones. Dally33 reports a case of a woman who had spasm of the left sterno-cleido-mastoid muscle at the time the right hand was seized with cramp in writing. More rarely all the muscles on one side of the body may be affected. Reynolds34 reports such a case.
32 “Crampe des Écrivains,” Progrès médical, v., 1877, p. 505.
33 “Traitement des Spasms professionnels,” Journ. de Thérapeutique, No. 3, 10 Fèvrier, 1882.
34 System of Medicine, “Writers' Cramp,” vol. ii. p. 287.
In the spastic form of the disease an early investigation usually shows a rigidity or spasm of one or more of the fingers, coming on when an attempt is made to perform the act which originated the trouble, and occasionally only on performing that act; but this statement, so strongly insisted upon by some authors as a diagnostic symptom, does not universally obtain.
The contraction may affect either the extensors or the flexors; in the former case—in writing, for instance—the pen can with difficulty be kept upon the paper, and the stroke movement is interfered with; if the spasm is of the flexors, which is of the most common occurrence, it usually affects the fore finger and thumb; the pen is then forced downward, and upon attempting to make the upward movement catches in the paper; besides, there may be with this a flexion and adduction of the thumb, which causes the pen-holder or pencil to be twisted from the grasp, occasionally with sufficient force to throw it to some distance. The other fingers may be similarly affected. The supinator longus is quite a common seat of spasm, the pen being thereby drawn from the paper by a partial supination of the forearm.
Sometimes the character of the spasm cannot be described, the hand seeming to run away with the pen.
The patient who feels these spasms or contractions coming on soon changes the manner of holding the pen-holder, so as to relieve the affected muscles and to use those which are but slightly or not at all affected. Many grotesque manners of writing may thus be encountered. One sometimes employed by those seriously affected is to grasp the holder in the closed hand, holding it nearly at a right angle to the forearm, all movements being made with the whole arm, thus relieving the finger-muscles. The diagram on p. 457 shows the method of writing adopted by a patient who has a marked spasm of the flexors of the fingers and thumb, preventing his writing in the ordinary manner; he is also the subject of telegraphers' cramp.
These means, however, give but temporary relief, as, sooner or later, if writing is persisted in, the muscles of the arm and shoulder become implicated.
In telegraphers the extensors of the wrist are frequently affected, so that the operator is unable on account of the spasm to depress the key of the instrument with sufficient force to close the circuit, the signals being made, so to speak, in the air, or else a dot (.) is made in place of a dash (—). The extensor spasm seems to be the most frequent form of the cramp among telegraphers, many of them saying that they are unable to keep their fingers upon the key-knob. It will generally be found that the characters that are the most difficult to make are those which are composed entirely of dots, such as h (....), p (.....), 6 (......), or those [p. 517] ending with dots, such as b (—...), d (—..), 8 (—....). Some of the spaced characters are also difficult to make, such as z (... .), & (. ...), y (.. ..).
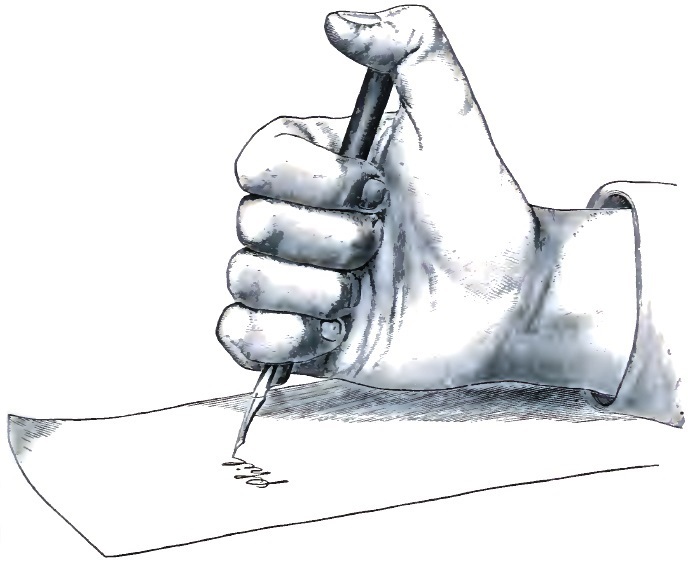
Occasionally one finger will become rigidly extended during telegraphing, and any attempt to prevent this will bring on great discomfort and greater disability. When, more rarely, it is the flexors which are affected, the key is depressed with undue force at the wrong time, and a dash is made where a dot was intended, or an extra dot or so introduced, or the proper spacing of the characters prevented, thus rendering the message unintelligible.
The telegraph operators who experience the most difficulty in transmitting usually have a cramp of the extensors, and those having the most difficulty in receiving (writing) usually have a cramp of the flexors, although the reverse is occasionally seen.
In some cases of the spastic form of copodyscinesia the contraction almost becomes tetany; thus there may be a contraction of the flexors of the wrist, which comes on whenever any attempt is made to use the hand, although the fingers may be entirely unaffected, or there may be a more or less constant contraction, greatly exaggerated on any attempt at motion.
Lock-spasm, as described by Mitchell,35 is a rare form of this affection: in this the fingers or hand become locked, so to speak, in a strong contraction, even stronger than the patient could ordinarily produce by an effort of will; this lasts for a considerable time, and after its disappearance the customary work may be resumed. Duchenne36 likewise reports some curious cases of functional spasm analogous to the foregoing.
35 Loc. cit.
36 Duchenne (de Boulogne), “Note sur le Spasm functionnel, etc.,” Bull. de Thérap., 1860, pp. 146-150.[p. 518]
II. Paresis or Paralysis (Paretic Form).—More or less weakness of some of the muscles of the hand or arm is frequently seen in cases of copodyscinesia; this is, however, less common than the spastic form, and, like the latter, is preceded or accompanied by other symptoms. This form occasionally follows the spastic, or it is seen in those cases where the cause of the trouble has been a preceding neuritis, or it may be due to professional muscular atrophy as described by Onimus,37 where, contrary to the ordinary rule, excessive use of a muscle or set of muscles produces, instead of hypertrophy, a condition of considerable atrophy, usually of the larger muscles first, which is preceded for some time by pain and cramp in the affected parts, with fibrillary twitchings; this is amendable rather rapidly under appropriate treatment, and thus differs from progressive muscular atrophy, with which it is apt to be confounded.
37 E. Onimus, “On Professional Muscular Atrophy,” Lond. Lancet, Jan. 22, 1876.
Some of the cases of this group may be confounded with those of the former, as there may be an apparent cramp or spasm of the unopposed healthy muscles. Zuradelli38 considers this condition to be the one ordinarily found in this disease.
38 Crisanto Zuradelli, Gaz. Med. Ital. Lomb., Nos. 36-42, 1857; also Ann. Universali, 1864.
A paretic condition of one muscle may coincide with a spastic condition of another not its opponent, the paralyzed muscle being the one first affected.
When a patient with paresis or paralysis as the most prominent symptom attempts to write, an intense feeling of fatigue usually appears, and the writing becomes difficult or impossible—not from a too ready response and spasm, but from an inability of the muscles to obey the will; the pen-holder is held in a feeble manner, and sometimes falls from the grasp. There may be a sense of utter weakness and powerlessness, the arm feeling as if glued to the table.
Duchenne39 calls attention to this form of trouble, which he styles paralysie functionelle, and states that it is much less common than functional spasm.
39 Loc. cit.
New methods of holding the pen are as constant in this form as in the spastic, as it is as necessary in one as in the other to avoid as much as possible the use of the affected muscles. A carpet-weaver, seen by myself, was obliged to tie the knots in the warp on the distal extremity of the second phalanx of the thumb, as the extensor secundi internodii pollicis was partially paralyzed, so that he was unable to keep the distal phalanx extended. This condition came on when he was a compositor, and compelled him to change his trade. A condition of spasm had preceded the paralysis.
The first dorsal interosseus muscle is frequently the seat of paresis; this is readily discovered by measuring the power which the patient has of lateral movement of the index finger and comparing it with that of the sound hand.
III. Tremor (Tremulous Form).—Trembling or unsteadiness of the fingers is occasionally seen, usually most marked in the fore finger when the hand is at rest with the fingers slightly separated. In some cases this may be sufficient to cause unsteadiness in work, prolonged work and over-fatigue being most apt to produce it; as previously mentioned, this is one of the premonitory symptoms of professional muscular atrophy. [p. 519] An oscillatory trembling, due to implication of the supinators and pronator, is described by Cazenave,40 which interfered greatly with the act of writing. Tremor is of itself rarely complained of by those affected with copodyscinesia, unless it becomes sufficiently marked to cause interference with work.
40 “Observations de Tremblements oscillatoires de la Main Droite,” Gaz. méd. de Paris, 1872, pp. 212-215.
A peculiar form of nystagmus occasionally seen in miners may be considered as belonging to this category. According to Nieden of Bochum41 it is caused by eye-strain in the defective illumination of the mines, and consists not of a spasm, but of a defective innervation, like the tremor of old persons. C. B. Taylor42 of Nottingham and Simeon Snell43 also speak of this as a fatigue disease.
41 “The Pathogenesis and Etiology of Nystagmus of Miners,” Am. Journ. Med. Sci., Oct., 1881.
42 Quoted by Poore, loc. cit.
43 “Miners' Nystagmus,” Brit. Med. Journ., vol. ii., 1884, p. 121.
IV. Pain, or Some Modification of Normal Sensation.—Every case of copodyscinesia, without exception, has at one period or another of the disease some modification of normal sensation in the hand or arm. Usually the very first symptom that attracts the patient's attention is a sense of fatigue or tire in the hand or arm, which at first appears only after a considerable amount of work; if rest is taken now, the part regains its normal condition, but if the work is continued the sensation increases, and the amount of labor necessary to cause the disability gradually grows less and less until any attempt suffices to produce it. A painful sensation or a sense of heat may be experienced in the shoulders or in the cervical or upper dorsal spine at the time the foregoing symptoms are felt.
These symptoms are due to chronic fatigue in many instances, this being an important factor in the causation of these troubles. An expression frequently used by those affected is that the hand or arm becomes lame; this sense of tire may be slight or may be of an intense aching character, almost unendurable.
Should spasm supervene, then there will be a sense of tension and pain in the rigid bellies of the muscles. When a subacute neuritis is present, as frequently occurs, all the symptoms common to that condition appear—viz. pain over the various nerve-trunks and at the points of emergence of their branches, either spontaneous or only solicited on pressure; areas of hyperæsthesia or anæsthesia; a sense of itching or tingling or pricking in the arm or hand; or a sense of numbness, causing the part to fall asleep.
As previously mentioned under Etiology, pain may be absent in some cases of subacute neuritis. Occasionally, the distal phalanx of the fore finger or thumb becomes exquisitely sensitive to pressure, and there may be a burning or stinging pain under the nail, severe enough to make the patient think local suppuration is about to take place.
Sensory disturbances in the region of the hand supplied by the radial nerve are quite common, less so in the region supplied by the median, and least of all in the ulnar distribution. This last having never been seen by Poore, although, as pointed out by him, the muscles supplied by the nerve are those most frequently implicated in this disease when it affects scriveners, his explanation is that the deep motor branches are [p. 520] widely separated from the sensory branches of the nerve, while this is not true of the radial.
One case of impaired sensation affecting the ulnar distribution, and consisting of slight numbness of the palmar surfaces of the ring and little fingers, has come under my observation. The patient was a young woman affected with pianists' cramp, having as its foundation a subacute neuritis of the musculo-spiral and ulnar nerves; the trouble had lasted five years.
A curious form of pain, as of a bar thrust diagonally through the hand, has been complained of; again, the arm, hand, or fingers may be the seat of a subjective sensation of weight, so that one arm will feel very much heavier than its fellow, or the hand may feel as heavy as lead. A soreness and sense of tightness, as of a band around the wrist, a throbbing and pulsation, or a tense feeling as if the skin would burst when the hand was closed, have been noticed occasionally.
V. Vaso-motor and Trophic Disturbances.—Among the rarer symptoms seen are vaso-motor and nutritional changes; these never occur alone, but are accompanied by cramp and fatigue or by some evidence of nerve-lesion.
When a patient with this symptom attempts to perform the task which produces the disability, in addition to the fatigue, spasm, or pain the veins on the back of the hand and fingers will be seen to slowly enlarge; this may gradually increase until it extends over the whole arm, the parts becoming more or less turgid with blood, the temperature at the same time being somewhat increased. A marked sensation of throbbing accompanies these symptoms.
Other parts more distant may become affected, the face becoming flushed, palpitation of the heart and profuse perspiration, either local or more or less general, ensuing, followed by exhaustion.
When there is a marked hyperæsthesia of the distal phalanges of the fingers, there may be a glossy appearance of the skin, or the parts may appear inflamed and as if about to suppurate, or there may be chilblains. A rare symptom is change in the character of the nails, which become brittle and crack off like shell, either spontaneously or when an attempt is made to cut them.
GENERAL SYMPTOMS.—Besides the various symptoms above enumerated, there may be others more general in character, such as intense headache and great general nervousness, the emotional character being generally well marked, as is shown by the disability being greatly increased when the patient knows some one is watching and criticising. There may be also vertigo and sleeplessness. When there is an associated spasm of the analogous muscles of the other arm and hand, although there is no apparent trouble in the arm which is being used, it shows that the hitherto almost automatic act is losing some of its automatism: this, although rare, is an important premonitory symptom.
A rare symptom, which, as far as my knowledge allows me to say, is confined to telegraph operators, is an inability to mentally grasp the proper number of dots and dashes composing certain Morse characters: this usually coincides with the difficulty experienced in making those characters after they have been thought of, and also makes it difficult for them to recognize them by sound even when properly made by another [p. 521] person. The characters composed entirely of dots seem to cause the most trouble in this way.
Electrical Reactions.—In those cases where spasm of one or more muscles is a more or less marked symptom electrical examination shows, both to the faradic and galvanic current, a quantitative increase in the reaction, both in the nerves and muscles; with the galvanic current the cathodal closing contraction is more marked than the anodal closing contraction, as in health (KaSZ > AnSZ); only this formula is most marked in the affected arm. When paresis is present there will be a quantitative decrease in the reaction, the formula still being KaSZ > AnSZ. In the same arm some muscles may show a quantitative increase and others a quantitative decrease. Where there is a neuritis present the electrical examination will show a quantitative increase, but where the disease has advanced to degeneration of the nerve the reaction of degeneration will be found, and the formula will be AnSZ > KaSZ; there is, therefore, a qualitative change, but this must be looked upon as rather uncommon in this class of diseases.
Poore44 is of the opinion that increased irritability shows an early, and decreased irritability a late, stage of the same condition. According to his tables, but very few of his 75 cases of impaired writing-power showed this quantitative increase, while every case showing the least evidence of cramp that has come under my observation has shown it in one or more muscles; in a few cases the antagonistic muscles showed a decrease. Increased sensitiveness to both currents is sometimes noticed.
44 “Writers' Cramp and Impaired Writing-power,” by C. V. Poore, M.D., Medico-Chirurgical Trans., vol. lxi, 1878.
COURSE.—The course of the disability is slow and, unless appropriate treatment is instituted, progressive, although at times there are periods during which the symptoms ameliorate without assignable cause, thus giving rise to false hopes. The usual history is that group after group of muscles becomes implicated as these are in turn used to relieve those first affected, the left arm, should this be used, becoming disabled in the same manner as the right, and the unfortunate sufferer is then compelled to give up his calling or else to lessen very materially the amount of his labor.
DURATION.—As might be inferred from what has been written, those who have suffered for years with this affection may expect it to continue for the remainder of their days; but the later investigations upon this subject give rise to much hope that in future the duration of this troublesome complaint will be materially shortened when the disease is recognized early and treatment instituted at the very first symptom.
DIFFERENTIAL DIAGNOSIS.—Although many of the cases of copodyscinesia are diagnosed with comparative ease, there are others which require much study, as there are several disorders which are apt to mislead by the similarity of symptoms.
Any affection of the finger-joints or of the muscles of the hand or arm, or any disease of the nerves or of the spinal cord, from which these nerves arise, or of the corresponding part of the brain, will necessarily interfere more or less with the finer movements of the hand, and yet all these, manifestly, cannot be considered cases of this affection.
Where the symptoms are undoubtedly caused by over-use of a part, by the constant repetition of the same muscular act, although the lesions [p. 522] may vary considerably in the different cases, they may be classed with propriety under the above head; but there is a second class which cannot be so considered, in which there has been a central lesion which has arisen entirely independently of the occupation which has become difficult to perform, and which disability is only one of the many symptoms that have arisen on account of the aforesaid lesion: these are the cases that it is important to differentiate from cases of true copodyscinesia.
When a patient is suffering from a difficulty in performing a fine act of co-ordination where previously there had been no trouble, much information as to the cause may be gained by examining critically the method in which that act is attempted to be carried out; thus, if the patient has a difficulty in writing, his method of holding the pen and his style of writing may throw some light upon the diagnosis; if he holds his pen too firmly or if the down strokes are too heavy, or the writing gradually grows smaller and smaller toward the end of the line, there is a spasm of the flexor muscles; if, on the contrary, the down strokes are imperfectly made or the thumb rises upon the holder, or one finger shows a tendency to straighten itself, the extensors are at fault. Each muscle should then be examined. By asking the patient to make the different movements possible with the fingers and hand of the affected side, and comparing them with those of the sound side, a feebleness of one or more muscles may be detected. The offending muscle may also be detected by electrical examination—by its reacting more or less strongly than its fellow on the other side to the faradic current or showing a quantitative change to the galvanic current.
By stripping the patient to the waist, or at least the arms, and making a careful examination, atrophy or local lesions may be detected that will aid in clearing up the diagnosis.
In telegraphers the mode of manipulating the key should be noted if possible, and the faults made in the different Morse characters studied; this will show as much in this form of the trouble as the mode of writing does in scriveners' palsy.
The condition described by Mitchell45 as post-paralytic chorea may easily be mistaken for these affections, especially where the cerebral lesion was coincident with much manual work (as writing or telegraphing), and was so slight in extent that the paralysis was transient and overlooked, the choreoid movements appearing later, and affecting, as they may do, only the hand. Of this condition Mitchell states “that it may exist in all degrees, with partial loss of power and with full normal strength—that it may consist in mere awkwardness, or exist to the degree of causing involuntary choreoid movements of the parts.”
45 “Post-paralytic Chorea,” by S. Weir Mitchell, Am. Journ. Med. Sci., Oct., 1874.
The diagnosis can, in most cases, be satisfactorily arrived at by careful consideration of the history of the case, the mode of onset, the presence of some other signs of cerebral lesion, and the examination of the heart and of the urine.
Some cases of paresis of the arm or hand from lesions of slight extent affecting the arm-centres in the brain (minute emboli, disease of the finer vessels, etc.) might possibly be mistaken for the paretic form of copodyscinesia. Two cases46 will illustrate this point:
[p. 523]Case I.—Mr. G.——, æt. 58, dentist. A great writer, although writing was always a difficult task and soon fatigued him. One day, after excessive writing the day previous, he awoke with a loss of power to write from an inability to properly co-ordinate his muscles; his hand was not unsteady, motion was apparently unimpaired, and his power good, but after laboring for ten or fifteen minutes he would drop the pen. He was treated for writers' paralysis, and gradually improved. One year later he was seized with aphasia and entire loss of power in the right arm and leg. His further history is that of right hemiplegia, and not interesting in this connection.
Case II.—Mr. W——, civil engineer, æt. 54. Until July, 1881, he considered himself a healthy man, although very excitable; he was then engaged in calculating and writing almost steadily for one week, which exhausted him exceedingly; following this, he was engaged in an abstruse calculation lasting another week, and at the end of this period he awoke to find himself powerless to extend or flex his wrist, and, to use his expression, his thumb would gravitate into his palm. The movements of the shoulder and arm were comparatively unimpaired, and with the exception of occasional dimness of vision of the right eye there was no other symptom noticed. In one week he considered himself well again. In July, one year later, after again passing through a period of exceedingly hard work, he awoke to find that he had lost sensation on the right side and had some difficulty in articulating (muscular). Although thus warned, he worked steadily for twelve hours the next day, in consequence of which he completely broke down. After this he would occasionally write down a wrong word or put down a wrong figure in calculating, etc. One month later he had a transient attack of loss of power in right leg and other signs of partial right hemiplegia, which was in all probability due to an embolus, as there was a marked aortic systolic murmur.
46 From S. Weir Mitchell's notebooks.
The point brought forward by Axenfield47 that the paralysis in brain lesions manifests itself equally in all movements of the fingers, while in writers' cramp, etc. there is integrity of all movements except those necessary for the special act, cannot be accepted as diagnostic.
47 Des Névroses, par le Docteur Axenfield, Paris, 1864, p. 389.
Progressive muscular atrophy, as previously mentioned, bears a close resemblance to professional muscular atrophy (Onimus), which may be considered one of the forms of copodyscinesia. The resemblance, together with the few points of difference, may be best seen in the form of a table, thus:
| PROGRESSIVE MUSCULAR ATROPHY. | PROFESSIONAL MUSCULAR ATROPHY. |
| 1. Heredity in 24.63 per cent. (Roberts). | 1. Heredity not marked. |
| 2. Affects adult males principally. | 2. Affects adult males principally. |
| 3. Frequently follows exhausting muscular activity. | 3. Always follows exhausting muscular activity. |
| 4. Atrophy a cardinal symptom. | 4. Atrophy a cardinal symptom. |
| 5. When it affects the upper extremities, the interossei and the thenar and hypothenar eminences are the first affected. (Eulenburg says in his experience the first dorsal interosseus is always first attacked, and the others later.) | 5. The muscles first affected are generally the largest ones, particularly those in the neighborhood of the shoulder-joint. The muscles of the hand may be affected first. |
| 6. Fibrillary twitchings frequent. | 6. Fibrillary twitchings frequent. |
| [p. 524] 7. Premonitory pains rare. | 7. Pains and cramps at the onset in the affected parts a distinctive sign. |
| 8. Diminution of electrical reactions to both faradism and galvanism. Reaction of degeneration occasionally a late symptom. | 8. (?). |
| 9. Prognosis generally unfavorable: as regards perfect restoration of muscles, almost hopeless. | 9. Rapid amendment under rest and the use of constant and continuous electric currents. |
The ordinary course of symptoms in this disease is not always followed out, and occasionally the resemblance of the initiatory symptoms to one of the forms of copodyscinesia is great; the following is a case in point:
W. F. G——, æt. 34, clerk, at one time an excessive smoker and a steady writer. In the autumn of 1883 he noticed a numbness on the ulnar side of the tip of the right index finger and on the radial side of the middle third of the right middle finger, at about the points touched by the pen-holder, which he held between these two fingers; this was soon accompanied by a hyperæsthesia to light touches, and the two together seriously interfered with pen-prehension; he then changed the pen to the left hand, and soon noticed a numbness on corresponding points on the left fingers. Any sudden extension of the right arm would cause a thrill to shoot down into the fingers. Weakness of the right opponens pollicis was present at the same time. These symptoms caused the first physician consulted to make a diagnosis of writers' palsy, but the later manifestations of the disease, six weeks subsequently, soon showed its true character: these were marked atrophy of the external portion of the thenar eminence (opponens pollicis) and weakness and partial atrophy, and finally total loss of power, of the anterior group of muscles of right leg (tibialis anticus, extensor proprius pollicis, and extensor longus digitorum); numbness and hyperæsthesia, as in the hand, appeared over instep. Fibrillary twitchings were absent. The affected muscles did not respond to the faradic current, while to the galvanic current there was a quantitative lessening, the reaction still being normal in kind—viz. KaSZ > AnSZ.
Paralysis agitans and multiple sclerosis both interfere with writing on account of the tremor of the muscles; the latter disease markedly so, as voluntary effort increases the trembling.
According to Sigerson,48 the flexors are the least affected in the former disease, and the extensors most so, especially the interossei, which are the earliest involved; the down strokes of the writing will therefore be made with comparative firmness, while the up strokes will show the tremor.49
48 Lectures on the Diseases of the Nervous System, by J. M. Charcot, trans. Philada., 1879, foot-note by Sigerson, p. 113.
49 Ibid., p. 112.
The writing in multiple sclerosis is much more wavy and irregular, although the same tendency to firmness in the down strokes may still be seen.50
50 Ibid., foot-note by Bourneville, pp. 153, 154.
Both these diseases, when well pronounced, should occasion no trouble in diagnosis, but there are cases where the symptoms are not typical, and where the sclerotic change is slight in amount and principally limited to the arm-centres in the cord, or at least to the anterior columns, the symptoms being confined to the finer movements of co-ordination of the hand and arm, and necessarily interfering with such occupations as writing [p. 525] much more than with those which only necessitate coarser movements. The following cases illustrate this point:
Case I.—J. S——, æt. 67, male. Two relatives had paralysis agitans (?). Previous health good; present trouble began nine years ago. Tremor first noticed in writing, and only then, but later any voluntary effort of right arm was accompanied by a fine tremor, which became particularly noticeable when the arm was semiflexed. This is now equal in both arms. When patient writes slowly and with great attention to each movement, he can write fairly for a short time; but if he attempts to write quickly, there is a marked tremor which renders the letters sometimes almost illegible. The up strokes show the most tremor. There is no festination, no change in voice, no loss of power over the sphincters, and no loss of reflexes; the reaction to the galvanic current is normal.
Case II.—W. H——, æt. 58, male. For fifty years the patient has been a hard writer, first as an editor and later as a cashier. In 1882 he noticed difficulty in raising arm to put away papers in pigeon-holes above his head; this movement caused pain in shoulder and arm. Shortly after this he found that his hand became tremulous when he attempted to write, and later any voluntary effort was sufficient to cause the tremor. There has been no cramp. The grip of both hands is good, nor is there any wasting of the muscles. Standing with eyes closed causes no swaying, although there are occasional vertiginous attacks. While walking he has noticed that the right arm does not swing with its usual freedom. No ataxic pains are present. Reflexes of right arm and shoulder are very much exaggerated; there are no changes in nutrition or sensation. Galvanic reaction normal and alike in both arms. The urine is non-albuminous.
The following case is in all probability one of diffused sclerotic changes in the right lateral half of the cord, where the disease has apparently ceased advancing:
Case III.—T. L——, æt. 45. In 1880, three years ago, patient noticed occasional formication in various parts of the right face, hand, and leg, which ceased after he suspended the use of tea and coffee; soon after this he noticed that his writing began to lack ease and that the letters became crowded toward the end of the line; later, a fine tremor appeared in the fingers of the right hand; crampy sensations then appeared in the hamstring muscles of right leg, chiefly while sitting with the knee bent at right angles; writing with the right hand was sufficient to cause, or at least aggravate, this. In 1882 the right arm lost its automatic swing during walking, although holding the left arm still would enable the right arm to swing automatically. Lately the symptoms have ceased advancing, and some seem to improve. His present condition is an inability to write with right hand without paying great attention and making each letter separately, and a trembling of fingers during excitement of any kind. Coarse movements of co-ordination can, as a rule, be well performed; there is no increase of reflexes, nor are they absent; there is no ataxic gait, and there are no trophic changes. Galvanic reaction is normal, and alike on both sides. There is no history of hereditary disease or of venereal taint.
In this connection it is proper to mention tremor mercurialis and [p. 526] tremor saturninus, which might possibly lead to mistake should proper attention not be paid to the history and to the symptoms. Paul51 reports a case of the former affection, and gives a specimen of the handwriting of the patient.
51 C. Paul, Bull. et Mém. de la Soc. de Thérap., Paris, 1881, xiii. pp. 129-131.
Traumatisms, etc. of the various nerves of the arm usually interfere with the proper play of the muscles supplied by them, and although certain of the milder forms of inflammation or of congestion, as previously mentioned, are sometimes present in cases of copodyscinesia, it is manifestly improper to include all cases of impairment of hand-and-arm movement from nerve-injury under this head.
Palsy from pressure, as from sleeping with the head resting upon the arm or with the arm hanging over the back of a chair, is a frequent cause of paresis or paralysis of the muscles supplied by the musculo-spiral.
Tumors pressing upon the nerves in any part of their course, or neuromata, may be mentioned among the more ordinary affections that possibly might mislead.
Tenosynovitis which is described by Hopkins52 as a congestion of the tendinous sheaths in the forearm, with insufficient lubrication of the same, causing pain and interfering with motion, might be mistaken for the disease in question, especially as it occurs in many of the same occupations which furnish cases of copodyscinesia.
52 Wm. Barton Hopkins, “Tenosynovitis,” Med. News, Philada., July 15, 1882.
The exciting cause of tenosynovitis is “usually the resumption of work to which the individual is thoroughly accustomed after a shorter or longer interval when he is out of practice,” and not the monotonous repetition of the same act. The differential diagnosis should occasion no difficulty, as there is soreness amounting to positive pain upon motion or pressure along the course of the affected tendons, and the peculiar creaking which is communicated to the finger on palpation.
PATHOLOGY AND MORBID ANATOMY.—Unfortunately for correct determination of the pathological conditions underlying these neuroses, there have been no reported examinations of the spinal cord and nerves in subjects affected with copodyscinesia dying from intercurrent diseases, although it is probable that no macroscopic lesion would be discovered.
Solly53 reports the post-mortem appearance in a case of impaired writing-power in which he found a granular disintegration of the cervical portion of the cord; but this case, from his description, was evidently one in which the impairment of power was merely one of the numerous symptoms dependent upon disease of the cervical cord from degenerative changes, and not a true case of writers' cramp. If such a condition underlaid these neuroses, the cures occasionally reported and the relief frequently felt after the use of the galvanic current could not be explained.
53 London Lancet, vol i. p. 113.
In default, then, of positive information upon this point, conclusions must be drawn from a study of the symptoms, the course, and the behavior of these diseases under treatment. An affection of such protean aspect is not likely to have one settled pathological condition underlying it.
Many affections considered hitherto purely functional have under our [p. 527] more advanced knowledge been found to have as a basis a positive organic change.
On the subject of fatigue, Poore54 concisely states that the symptoms “are referable to the muscles, but we must always bear in mind that muscles and motor-nerve are one and indivisible, and that recent experiments have given great probability to the idea that every muscle is connected with a definite spot in the brain; when, therefore, we speak of a sense of fatigue, we must necessarily be in doubt, notwithstanding the fact that the symptoms are referred to the muscles, whether brain, nerve, or muscle, one or all of them, be really at fault.”
54 “On Fatigue,” London Lancet, vol. i., 1875, p. 163.
There is a certain limit to which exercise of a given group of muscles may be carried without producing fatigue and local congestion, or perhaps even inflammatory results; this varies greatly in different individuals, but if it is continually and uninterruptedly overstepped, and insufficient time given for rest and recuperation, the centres in the spinal cord which regulate the action of the various muscles implicated become overstimulated, and the result is an undue amount of nervous energy induced by the peripheral excitation, or there is a distortion of the central impulses in passing through these centres: a perturbation of the co-ordinating power ensues and inco-ordination is the result. Under rest and appropriate treatment these symptoms may pass away, but if the part is continuously used it is highly probable that nutritive changes will be produced in that part of the spinal cord from which the nerves supplying the overtaxed muscles proceed.
In some cases of hemiplegia there is produced during gaping and sneezing an automatic movement of the paralyzed arm; this was noticed as early as 1834 by Marshall Hall,55 and in 1872, Onimus56 noticed that movements of the hand and fingers of the non-paralyzed arm produced similar movements in the paralyzed side.
55 Quoted by Charcot, Diseases of Spinal Cord, transl. by Comyges, Cincinnati, 1881, p. 110.
56 Ibid.
Erb57 states that these movements in certain spinal troubles are partly owing to the establishment of conditions of irritation in the neighborhood of the lesion.
57 Ziemssen's Cyclopædia, Amer. ed., vol. xi. p. 409.
Hitzig58 states that in certain pathological conditions where the ganglionic elements (in the cord) are superexcitable, the least disturbance produced on one side, and which determines there a voluntary movement, may be communicated to the other side, and provoke, according to the case, either movements similar to a voluntary one or a spasmodic movement which is really a contraction; and also in certain cases relations of the same nature may be established among cellular groups quite distant from each other; and we can comprehend that in these cases the voluntary movements executed by the sound side may be re-echoed in that which is diseased.
58 Quoted by Charcot, loc. cit., p. 124.
This apparent digression bears an important relation to the pathology of copodyscinesia, and lends force to the view that the associated movements which occur in the well arm, or in the affected arm when the sound side is used, or even in the face and legs, and which are quite often seen in these affections, are due to the fact that there is a central change.
Mitchell,59 in speaking of functional spasms, states that it will be found [p. 528] in all these cases that when an ordinary functional motor act gives rise to spasms elsewhere, these occur in muscles which have physiological, and therefore anatomical, relations to the muscles which by their normal use give rise to the morbid activities. He considers that there is a hypersensitizing of the sensory centre which takes record of the activities of the affected muscles.
59 “Functional Spasms,” Amer. J. Med. Sciences, Oct., 1876.
The fact that the left hand becomes implicated in some cases where it is used to relieve the right should be mentioned in this connection as lending weight to this hypothesis, especially as in a few cases of telegraphers' cramp the left hand has been found implicated in the very first attempt to use it in telegraphing.
Poore60 considers this transfer as no evidence that the change is central, and is one of the few who consider the pathological conditions as purely peripheral in character. Hamilton61 and De Watteville62 also consider the peripheral hypothesis the correct one.
60 Loc. cit.
61 Nervous Diseases, Philada., 1881.
62 “The Cure of Writers' Cramp,” Brit. Med. Journ., 1885, vol. i. pp. 323-325.
Fritz63 (and after him Poincaré64) considers the disease a reflected neurosis, due to a perversion of the muscular sense. Onimus and Legros65 incline to the same opinion.
63 Oesterr. Jahrb., März u. April, 1844.
64 Le Système nerveux-péripherique, Paris, 1876.
65 Traité d'Electricite médicale, Paris, 1872, p. 327.
The older theory that the disease is solely central in its pathology is advocated by Duchenne,66 Solly,67 Reynolds,68 Althaus,69 Wood,70 Vance,71 Erb,72 Dally,73 Axenfield,74 Whittaker,75 Waller,76 Gowers,77 Hammond,78 Romberg,79 Cederschjöld,80 Robins,81 Ross,82 and some others. Roth83 considers that there are two entirely separate classes, the central and the peripheral or local.
66 De l'Électrisation localisée, 3d ed., pp. 1021 et seq.
67 London Lancet, Jan. 28, 1865.
68 System of Medicine.
69 Julius Althaus, London Mirror, vol. vii., Aug. 1, 1870; also, pamphlet, Scriveners' Palsy, London, 1870.
70 Practice of Medicine.
71 Reuben A. Vance, Bost. Med. and Surg. Journal, vol. lxxxviii. p. 261.
72 Ziemssen's Cyclopædia, vol. xi. p. 355.
73 Journal de Thérapeutique, Paris, 10 Fév., 1882.
74 Des Névroses, Paris, 1864.
75 Cincinnati Lancet and Clinic, 1880, N. S., vol. iv. p. 496.
76 Aug. Waller, Practitioner, 1880, vol. ii. p. 101.
77 W. R. Gowers, Med. Times and Gaz., 1877, vol. ii. p. 536.
78 Treatise on Dis. of Nervous System, 6th ed., New York, 1876.
79 Manual of Nervous Dis. in Man, Sydenham Society, vol. i.
80 Gustaf. Upsala läkarefören, förhandl. xv., 3 och. 4, S. 165, 1880, review in Schmidt's Jahrb., Bd. clxxxvii., 1880, p. 239.
81 “Writers' Cramp,” Amer. Journ. Med. Sci., April, 1885, pp. 452-462.
82 A Treatise on Diseases of the Nervous System, London, 1881, vol. i. pp. 464-469.
83 The Treatment of Writers' Cramp, by Roth, London, 1885.
The later theory, that the disease is at first peripheral, but that by abuse may become central (spinal), is advocated by Beard,84 Liebman,85 Bartholow,86 Frazer,87 and a few others. The latter theory, and not the idea that it is a disease of the co-ordinating centres in the brain or of the spinal centres only, best explains, in my opinion, the various symptoms encountered.
84 New York Med. Record, 1879, p. 244.
85 Maryland Med. Journ., June, 1880-81, vol. vii.
86 Medical Electricity.
87 Glasgow Med. Journ., 1881, vol. xv. p. 169.[p. 529]
Many others have written upon this subject, but upon the probable pathology they have been silent.
The experiments recently made by Dercum and Parker88 on the artificial induction of convulsive seizures are of considerable interest, and certainly tend to throw light on the point in question. These convulsions were produced by subjecting a group of muscles to a constant and precise effort, the attention being at the time concentrated upon some train of thought. The position most frequently adopted was to cause the arms to be held so that the tips of the fingers barely touched the surface of the table before which the subject was seated, the fingers not being allowed to rest upon the table, but maintained by a constant muscular effort barely in contact with it. After this position was maintained for a variable length of time tremors commenced in the hands; a little later these tremors became rapidly magnified into rapid movements of great extent sometimes to and fro, sometimes irregular; if the experiment was carried still farther, the muscles of the arms, shoulders, back, buttocks, and legs become successively affected, and the subject was frequently thrown violently to the ground in a strong general convulsion, the consciousness being always retained.89 The more frequently these experiments were performed, the more readily the seizures were brought on, and, other things being equal, with successively increasing intensity. One subject thus experimented upon became so susceptible that the jar of a passing wagon sufficed to induce a partial seizure. These experiments throw a new light upon the associated movements previously mentioned, and show how easily the phenomena noticed in one part may pass to another having physiological relationship with it. It is highly probable that some nutritional change in the cord would follow the too frequent repetition of these experiments.
88 “The Artificial Induction of Convulsive Seizures,” Dercum-Parker, The Polyclinic, Philada. 1884, vol. ii. pp. 95-97.
89 These experiments were subsequently repeated before the Philadelphia Neurological Society in 1885.
Peripheral pathological conditions undoubtedly exist in many cases of copodyscinesia; these may be so slight that they can scarcely be demonstrated, or, on the other hand, they may be marked, and even present a well-marked inflammation of one or more of the nerves of the arm, as evidenced by pain on motion, tenderness on pressure, and sensory and nutritive disturbances in the areas which they supply.
There are some cases where the disability is pronounced, and yet the most careful examination fails to reveal peripheral changes of sufficient gravity to account for the severity of the symptoms; these, in my opinion, are best explained by supposing a hyperexcitability of the spinal centres, as previously expressed.
The electrical reaction in many cases tends to prove an irritable condition of the spinal centres. In most of the cases of the spastic group there will be found a quantitative increase in the reaction of both nerve and muscle to the galvanic current. Gowers90 states that he has found such an increase in diseases regarded as functional, as paralysis agitans and chorea, and considers it an interesting proof of the molecular changes which underlie or result from functional maladies. He previously [p. 530] remarks91 that such a condition of exalted irritability is to be ascribed to a corresponding change in the nutrition of the nerve-cells of the spinal cord, secondary to the irritative influence which caused it.
90 Dis. of Spinal Cord, 2d ed., Philada., 1881, p. 40.
91 Med. Times and Gaz., London, vol. ii., 1877, p. 536.
Erb92 also considers that quantitative increase in the electrical reaction points to central lesion. Buzzard93 quotes several authors upon tetany—which some cases of copodyscinesia closely resemble—who state that the electrical reactions are increased quantitatively in that affection, and considers, himself, that the change is due to central lesion.
92 Loc. cit.
93 Thomas Buzzard, Dis. of the Nervous System, London, 1882.
It must be borne in mind, however, that in those cases of congestion of the nerves, or neuritis, previously mentioned a quantitative increase may be found, indicating a hypersensitiveness of the peripheral nerve, and not necessarily of the spinal centres.
Poore94 states: “Thus we see that alterations of irritability” (he especially alludes to depressions) “accompany many conditions, both central and peripheral,” and “there is no necessity for assuming that central change exists in every case of altered irritability, and we have no warrant for such an assumption in the absence of independent evidence of central change.”
94 “Impaired Writing-power,” loc. cit.
Exactly what the alteration in the condition of the spinal cord is which probably occurs in many of these cases it is impossible to state, but the view that it is a nutritive change of the upper dorsal and lower cervical portion of the spinal cord (that is, when the arm is the part affected, as it is in all but the rarer cases) is quite attractive, the condition being secondary to a peripheral irritation in many cases.
Althaus95 considers that there is a “constriction of the small arteries, dilatation of the veins, and slight serous effusions compressing the nervous matter in the cervical spinal cord.”
95 Loc. cit.
Pain in the cervical and dorsal spine during work may be mentioned here as an evidence that some of the symptoms are due to central alterations.
Those few cases that exhibit great difficulty in performing one set of movements that requires a certain combination of muscles, but are able to use those same muscles in combination with others with ease, are difficult of explanation by the peripheral theory of the disease alone; but less difficulty is encountered if a superexcitability of the spinal centres is supposed to exist, for here we can imagine that when all the centres so affected are called into use, and only then, there will be an undue amount of nervous energy transmitted to the periphery, and disordered movement be the result.
The explanation offered by those who believe in the peripheral theory is, that the affected muscle is always imperfect in its action, but that this imperfection is masked in other combinations by the action of the healthy muscles, so that it is no longer noticeable.
PROGNOSIS.—The prognosis in these affections varies with the conditions found and with the previous duration of the disease.
A favorable prognosis may generally be given where the case is an acute one, and where the disability can be proved to be due to some one of the peripheral conditions previously mentioned. When the condition is in the forming stage, when fatigue, stiffness, tremor, tingling, aching, [p. 531] sense of heat, coldness, or powerlessness are the only symptoms which exist, the disease is quite amenable to treatment and a good prognosis may be given; but, unfortunately, patients are loath to believe that these trivial symptoms, which do not prevent their work, are precursors of any serious trouble, and therefore pay but little attention, if any, to them, so that the physician is seldom consulted during this period.
When positive cramp has made its appearance, it is an evidence of a more advanced stage of the malady, and the prognosis becomes less hopeful, although still the symptoms may be greatly ameliorated, or a complete cure even be effected.
When the cramp has existed for years and is present in many of the finer acts of co-ordination, the case becomes almost hopeless as far as cure is concerned; and even though the part is rested, so far as the disabling occupation is concerned, for months or even years, it will be found to return upon resumption of the old work. Roth96 considers those cases due to central changes totally incurable.
96 Loc. cit.
When a congestion of the nerves or a well-defined neuritis is discovered to be the cause of the trouble, the probability of a favorable termination is rather more hopeful.
Paralysis is to be looked upon as an unfavorable symptom, pointing as a rule to a late stage of the disease.
It may be stated with positiveness that when the premonitory symptoms are neglected and constant work persevered in, the case will go on from bad to worse: periods of amelioration, it is true, may occur, but cramp usually supervenes, and the affection becomes gradually progressive as group after group of muscles becomes implicated, until the part becomes useless for all delicate work.
The probability of the left hand escaping, should it be used to relieve or replace the right, is slight; and for two reasons: 1st. The same predisposition which favored the trouble in the right arm still exists; and, 2d. The proximity of the spinal centres for the two arms is such that the morbid process may easily be conveyed from one to the other, as was shown while considering associated movements.
Poore disbelieves in the possibility of such a transfer, and with Gowers is of the opinion that the liability of the left hand to suffer has been overestimated.
In my experience, as regards telegraph operators, the majority who use the left arm soon notice symptoms of the disability in it. Of 43 cases of this form of copodyscinesia which have come under my observation, in 21 the left arm was implicated; in 12 there was no such implication, although the arm was used; of the remaining 10, 8 had never tried to telegraph or write with the left arm; 1 had only one arm, the left; and 1 was doubtful. Throwing out of consideration the last 10, 21 out of the 33 had this symptom, equivalent to 63.63 per cent.
PROPHYLAXIS.—The only prophylactic measures are the observance of the most easy and least fatiguing method of performing the act which it is feared will bring on the trouble, and the avoidance of overwork.
Tobacco and alcohol generally act injuriously, and therefore should be avoided as much as possible by those who are predisposed by occupation or otherwise to these disorders.
[p. 532]In writing it is advisable to avoid an awkward manner of holding the pen-holder, which should be of good size; large, moderately soft pens and paper of good quality should be used.
It is also important that the table or desk upon which the writing is done should be of a convenient height, with plenty of room for the arrangement of the paper; otherwise an awkward manner is inevitable.
As regards the position of the paper, R. Berlin97 (Stuttgart) states substantially as follows: In writing the head is almost invariably held so that the line passing through the two eyes, if projected upon the paper, shall cross at right angles the oblique line of the writing: when the paper is placed to the right and parallel to the edge of the table, as generally directed by teachers, the tendency is to twist the spine and incline the head to the right in order to conform to this rule, and a cramped position is the result; but by placing the paper in an oblique position directly in front of the writer—i.e. turned toward the left—this cramped position is avoided, and the least fatigue, both to the muscles of the spine and arm, produced. Tight sleeves or anything that might possibly impede the free play of the muscles or cause pressure upon the nerves should be discarded.
97 “Physiology of Handwriting,” Von Graefe's Archiv, xxviii. p. 259, review in Ophth. Review, London, vol. i. No. 14, Dec., 1882, and Jan. 1, 1883.
It is now almost universally conceded that the conjoint movement in writing—that is, the arm movement for all the small letters, and the finger movement only to assist in making the long ones—is least likely to produce fatigue.
It has been stated, and quite generally believed, that the slighter degrees of scriveners' palsy are relieved by avoiding contact with the metallic portion of the pen-holder,98 and one of the methods taken to avoid this contact, especially among telegraph operators, is to slip a piece of rubber tubing over the pen-holder; this certainly does relieve the fatigue slightly, but the cause is not the avoidance of contact with metal or the insulation, etc., but simply that the holder is thus made larger and softer for the fingers, and thus takes the place of a cork pen-holder, which for some time has been in use for this purpose.
98 W. Bathurst Woodman, St. Andrews Grad. Ass., 1872-73.
Holding the pen-holder or pencil between the different fingers is another prophylactic measure, and relieves fatigue considerably; for instance, when it is placed between the index and middle fingers there is much less effort at pen-prehension, and the fingers may be temporarily rested without any effort to hold the pen-holder, as the friction between the fingers keeps it in position. This method is frequently adopted by stenographers.
The stylographic and Mackinnon pens, although they destroy much of the originality in handwriting, are easier to write with than a pen, as less pressure is needed and no particular angle is required to be maintained between the point and the paper.
The type-writer is one of the newer inventions destined to come into extended use for the purpose of relieving the fatigue of writing, which it does to a marked degree, besides having other merits; and although one of these is said to be the immunity of its users from writers' cramp, [p. 533] I venture to assert that cases of this class of trouble will ensue from its over-use, exactly as they do in piano-playing.99
99 To print this article by this machine would require nearly one hundred and fifty thousand separate flexions of the fingers.
Thurber's kaligraph, which was invented before the type-writer, has never come into general use: it works upon the principle of a pentagraph, and all finger movements are done away with and the arm movement used exclusively, the motions of writing being much coarser than ordinary. This instrument is not as well adapted for prophylaxis in these troubles as it is for use in some deformities of the hand hindering pen-prehension, as rheumatoid arthritis, contractions after burns, etc.
In regard to the means to be taken to avoid the occurrence of telegraphers' cramp, but little can be said, except that if any of the premonitory symptoms of the neurosis should occur (fatigue, pain, tingling, numbness, flushing, associated movements, etc.) after performing the amount of work which previously caused no discomfort, it should be taken as a warning that the operator is attempting more work than can be done without detriment, and that a curtailment of the work is absolutely necessary if he or she wishes to avoid the disease.
Onimus100 has said that if further investigation proves that the operators upon the Morse instrument are more liable to suffer than those using other systems, it should be the duty of those in authority to abolish that system and adopt some other: he suggests for this object the Hughes, which is a printing instrument. That the operators upon the Morse are more liable to suffer than any others is self-evident after a very slight inquiry, and because of the very general introduction of that machine. This instrument is far more practical, takes up less room, and is less likely to get out of order, than any other yet invented, and no other, it is probable, will be introduced so generally. The telephone has not diminished the amount of work for the telegraph operator, but has given rise to a new industry. In all of the systems the instruments are manipulated at least in part by the fingers, so that all are liable to cause this disease.
100 Loc. cit.
The telegraph key should be placed some distance from the edge of the table, so that the forearm may have sufficient support, resting upon the bellies of the flexor group of muscles, and thus relieve the shoulder-muscles, which otherwise would have to support the weight of the arm. Some operators prefer to hold the arm raised from the table, but this method is more liable to cause fatigue.
Several keys have been invented for the purpose of lessening the amount of force needed to manipulate them, and to avoid the jarring caused by the metallic contact; and, although everything that lessens the amount of labor should be adopted, the movements of telegraphing must remain the same no matter which key is used.
Tapping upon the key or attempting to operate by flexing the fingers while the wrist is held still should be avoided.
It is needless to enumerate the other forms of copodyscinesia, as the same general principles apply to the prophylaxis of all.
TREATMENT.—Rest.—It is an assured fact that as long as the patient continues without curtailment the amount of work he was performing [p. 534] when the symptoms of this trouble appeared, treatment will be negative in its results. Rest in itself is powerless to cure, except in the very earliest stages of the disease, for many sufferers have found, to their dismay, that after having given the arm complete rest, as far as the disabling occupation was concerned, for months at a time, the symptoms reappear upon returning to the accustomed work.
During treatment rest is essential, but this need not of necessity be complete; a curtailment of the work will often be all that is needed in the lighter cases. This may be effected by using the unaffected arm for a part of the work at least, but great care must be exercised lest the symptoms appear on this side also, as the left arm, from want of use, is wanting in strength and dexterity, and is more liable to be overtaxed by an amount of work that could be performed without fatigue by the right; for should this happen the end sought for is defeated, and the condition of the patient rendered far worse than before.
In writers' cramp the type-writer, as mentioned under Prophylaxis, is an important adjuvant in the treatment; unfortunately, it is not applicable to much of the work done by clerks.
The other means described in the last section are also useful in the treatment as affording temporary rest to the affected muscles. Hamilton101 has seen occasional benefit from forced rest by fastening the hand upon a splint.
101 Loc. cit.
In telegraphing, besides using the left arm, the key may be grasped in a different manner, or if the operator has been holding his arm raised from the table, let him rest it upon the latter, or vice versâ.
These remarks only apply to those who are compelled to continue moderate work during treatment.
Electricity.—The majority of the later writers unite in considering electricity as one of the most important agents in the treatment of these affections: the form and the manner in which it is applied are, however, all important.
The faradic or secondary current has often been tried in undoubted cases of copodyscinesia, and in the majority has failed. It may be of great service in the paralytic group, where the affected muscle shows signs of atrophy and of being temporarily deprived of nerve-influence; it may be also of service in those apparent cases of the spastic group due to contracture of the unopposed muscles, but in the vast majority, where there is a true spasm of the affected muscles or a tendency in that direction, as evinced by rigidity more or less pronounced during work, or even where there is only a quantitative increase to either current (faradic or galvanic), the application of this form of electricity is contraindicated, as the muscular contraction is already excessive, and should this extra stimulus be applied the muscle may be exhausted, for we know how readily this effect may be produced by a too strong or a too lengthy application in a perfectly healthy subject.
It is hardly necessary to mention that the manner of applying electricity so often followed by individuals—viz. holding the electrodes in the palms of the hands—is unscientific and productive of no good. The proper method of application in the suitable cases is to place one electrode of the secondary coil (preferably the negative, so called) over [p. 535] the muscle that is weakened or over its nerve-point, and the other in some indifferent position, using a current that is just strong enough to cause a fair contraction, and employing a slow interrupter, which breaks the current from one to four times a second. The application should be short, five to ten good contractions of each muscle being sufficient.
Buzzard102 has used this current with success in two cases of impaired writing-power, one of these depending upon a local paralysis. Zuradelli,103 Meyer,104 and Haupt105 have also seen good results by this method. Duchenne106 states that he has “not even seen one success obtained by those who have praised this method of treatment.” The majority of the later writers coincide with this last opinion as regards the spastic form at least.
102 “Two Cases of Impaired Writing-power,” Practitioner, Aug., 1872.
103 Quoted by Erb and Poore, loc. cit.
104 Ibid., loc. cit.
105 Der Schreibekrampf mit Rücksicht auf Path. u. Therap., Wiesbaden, 1860, review in Schmidt's Jahrbucher, Bd. cxv. 3, 136, 1862.
106 Loc. cit.
The galvanic current has of late been considered one of the most important agents in the treatment of these affections, but there is considerable variance among authorities as to how it should be applied. The most efficacious method is the descending current (anode on the spine and the cathode at the periphery), as this has been found to be more soothing in its effects than the reverse. The anode should be placed upon the spine over the cervical cord, and the cathode in the hand of the affected side or over the affected muscles or nerves.
A stabile current—i.e. where the poles are not moved about—is to be preferred to a labile current—i.e. where the poles are moved constantly—as this is more stimulating than the former; but if a current of proper strength is used, one that can be plainly felt when the circuit is made and broken only, the importance of the stabile over the labile does not obtain.
The treatment should not be prolonged for more than fifteen or twenty minutes, and may be repeated three times a week or every other day.
Onimus and Legros107 recommend this mode of treatment, but from a different pathological standpoint, as they consider the neurosis to be an excitability of the sensitive nerves of the muscles, and employ the descending current to allay this.
107 Loc. cit.
All sudden shocks or reversals of the current should be avoided in the treatment, although this may be necessary in using the galvanic current for diagnosis.
As the seat of the trouble in many cases is probably in the cervical cord, it is well that special treatment should be applied to this part, and for this purpose Althaus108 recommends that the anode be placed, as previously mentioned, over the cervical cord, and the cathode in the depression between the angle of the lower jaw and the sterno-cleido-mastoid muscle, which position corresponds to the superior cervical ganglion of the sympathetic. The current should be allowed to flow from three to five minutes at a time; it should be a mild one, and not be broken or increased or diminished suddenly, as vertigo may be produced. Both sides should be treated should the left hand be suffering also. A reversal of this method—i.e. cathode to spine—does little if any good, according to the same author.
108 Loc. cit.[p. 536]
Poore109 employs the descending stabile current of a strength just short of producing muscular contraction when the current is broken, but at the same time he employs rhythmical movements of the muscles supplied by the nerve upon which the cathode is placed during the flow of the current.
109 Loc. cit.
A novel mode of applying the galvanic current in scriveners' palsy has been recommended by Imlach.110 He has an electric desk so constructed that when the patient makes the movements of writing the extensors and flexors are alternately galvanized, the muscles being thus assisted in their movements. While this might be of service in some cases, it is entirely too complicated for practical use. He reports one case benefited by its use.
110 Francis Imlach, “Automatic and Other Medical Electricity,” Practitioner, vol. ii. p. 270, 1879.
Franklinic or Static Electricity.—This form of electricity is now being much used, especially abroad, in the treatment of nervous affections, but does not appear to have been employed in the different copodyscinesiæ, as but few reports of such treatment have found their way into current literature. Romain Vigouroux111 states that he has cured one case by statical electricity. Another case is reported by Arthuis112 as rapidly cured by this treatment after many other means, carried on during a period of five years, had failed; but his brochure contains too many reports of cures of hitherto incurable diseases to be relied upon.
111 Le Progrès médical, Jan. 21, 1882.
112 A. Arthuis, Traitement des Maladies nerveuses, etc., Paris, 1880, 3me ed.
Gymnastics and Massage.—As those suffering from copodyscinesia are generally compelled by their vocation to be more or less sedentary, exercise in the open air is indicated, inasmuch as it tends to counteract the evil effects of their mode of life; but the use of dumb-bells or Indian clubs, riding, rowing, and similar exercises do not ward off the neuroses in question or diminish them when they are present.
Such is not the case when rhythmical exercises and systematic massage of all the affected muscles are employed, as marked benefit has followed this method of treatment. The method employed by J. Wolff, a teacher of penmanship at Frankfort-on-the-Main, which consists of a peculiar combination of exercise and massage, appears to have been wonderfully successful, judging from his own statements and editorial testimonials of such eminent men as Bamberger, Bardenleben, Benedikt, Billroth, Charcot, Erb, Esmarch, Hertz, Stein, Stellwag, Vigouroux, Von Nussbaum, Wagner, and De Watteville. The method is described by Romain Vigouroux113 and Th. Schott,114 the latter claiming priority for himself and his brother, who employed this method as early as 1878 or 1879. Wolff,115 however, states that he had successfully treated this disease by his method as early as 1875. Theodor Stein,116 having had personal experience in Wolff's treatment, also describes and extols it: 277 cases of muscular spasms of the [p. 537] upper extremities were treated; of these, 157 were cured, 22 improved, while 98 remained unimproved; these comprised cases of writers', pianists', telegraphers', and knitters' cramp.
113 Le Progrès médical, 1882, No. 13.
114 “Zur Behandlung des Schreibe- und Klavierkrampfes,” Deutsche Medizinal Zeitung, 2 März, 1882, No. 9, Berlin; also “Du Traitement de la Crampe des Écrivains, reclamation de Priorité, Details de Procedes, par le Dr. Th. Schott,” Le Progrès médical, 1re Avril, 1882.
115 “Treatment of Writers' Cramp and Allied Muscular Affections by Massage and Gymnastics,” N. Y. Med. Record, Feb. 23, 1884, pp. 204, 205.
116 “Die Behandlung des Schreibekrampfes,” Berliner klinische Wochenschrift, No. 34, 1882, pp. 527-529.
It must be borne in mind that Wolff, not being a physician, can refuse to treat a case if he thinks it incurable; and in fact he does so, as he has personally stated to the writer, so that his statistics probably show a larger percentage of cures than otherwise would be the case.
His method may be described as follows: It consists of a combined employment of gymnastics and massage; the gymnastics are of two kinds: 1st, active, in which the patient moves the fingers, hands, forearms, and arms in all the directions possible, each muscle being made to contract from six to twelve times with considerable force, and with a pause after each movement, the whole exercise not exceeding thirty minutes and repeated two or three times daily; 2d, passive, in which the same movements are made as in the former, except that each one is arrested by another person in a steady and regular manner; this may be repeated as often as the active exercise. Massage is practised daily for about twenty minutes, beginning at the periphery; percussion of the muscles is considered an essential part of the massage. Combined with this are peculiar lessons in pen-prehension and writing.
The rationale of this treatment is not easy, but any method which even relieves these neuroses should be hailed with pleasure, as they heretofore have been considered almost incurable.
The method employed by Poore, as mentioned under Electricity, of rhythmical exercise of the muscles during the application of the galvanic current, is worthy of further trial, as it combines the two forms of treatment hitherto found most successful.
Internal and External Medication.—Generally speaking, drugs are of comparatively little value in the treatment of these affections. This statement does not apply to those cases where the symptoms are produced by some constitutional disorder, or where there is some other well-recognized affection present which does not stand in relation to these neuroses as cause and effect.
In any case where an accompanying disorder can be discovered which is sufficient in itself to depress the health, the treatment applicable to that affection should be instituted, in the hope, however unlikely it is to be fulfilled, that with returning health there will be a decrease of the copodyscinesia. In the majority of cases no constitutional disease can be detected, and it is in these that internal medication has particularly failed.
The following are some of the remedies that have been employed: Cod-liver oil, iron, quinine, strychnia, arsenic, ergot, iodoform, iodide and bromide of potassium, nitrate of silver, phosphorus, physostigma, gelsemium, conium, and some others.
Hypodermic Medication.—Atropia hypodermically, as first suggested by Mitchell, Morehouse, and Keen117 in the treatment of spasmodic affections following nerve-injury, has been used with good effect in those cases where there is a tendency to tonic contraction; it should be thrown into the body of the muscle. Vance118 speaks very favorably of one-sixtieth [p. 538] of a grain of atropia used in this manner three times a week. Morphia, duboisia, and arsenic in the form of Fowler's solution have been used hypodermically with but little effect. Rossander119 reports a cure in one month of a case of two years' duration by the hypodermic use of strychnia. Onimus and Legros120 used curare in one case without effect.
117 Gunshot Wounds and Other Injuries to Nerves, Philada., 1864.
118 Reuben A. Vance, M.D., “Writers' Cramp or Scriveners' Palsy,” Brit. Med. and Surg. Journal, vol. lxxxvii. pp. 261-285.
119 J. C. Rossander, Irish Hosp. Gazette, Oct. 1, 1873.
120 Loc. cit.
Local Applications.—The apparent benefit following the local application of lotions, etc. to the arms in some cases appears to be as much due to the generous kneading and frictions that accompany them as to the lotions themselves. Onimus and Legros, believing the lesion to be an excitability of the sensitive nerves at the periphery, employed opiated embrocations, but report amelioration in one case only.
When there are symptoms of congestion of the nerves or of neuritis, then the proper treatment will be the application of flying blisters, or the actual cautery very superficially applied to the points of tenderness from time to time, so as to keep up a continual counter-irritation. This treatment may be alternated with the application of the galvanic current (descending, stabile, as previously mentioned) or combined with it. As these conditions are often found in nervous women, care should be taken lest this treatment be too vigorously carried out.
Considerable relief has been reported from the use of alternate hot and cold douches to the affected part—a procedure which is well known to do good in some cases of undoubted spinal disease; the application peripherally applied altering in some way, by the impression conveyed to the centres, the nutrition of the spinal cord.
Tenotomy.—Tenotomy has been but little practised for the cure of these affections. Stromeyer121 cut the short flexors of the thumb in a case of writers' cramp without any benefit, but in a second case, where he cut the long flexor of the thumb, the result was a cure. Langenbeck122 quotes Dieffenbach as having performed the operation twice without success, and states that there has been but one observation of complete success, and that was the one of Stromeyer. Aug. Tuppert123 has also performed this operation, and Haupt124 advises it as a last resource.
121 “Crampe des Écrivains,” Arch. gén. de Méd., t. xiii., 1842, 3d Series, p. 97.
122 Ibid., t. xiv., 1842, 3d Series.
123 Quoted by Poore, loc. cit.
124 “Der Schreibekrampf,” rev. in Schmidt's Jahrbuch, Bd. cxv., p. 136, 1862.
Very few would be willing to repeat the experiment in a true case of copodyscinesia after the failures above enumerated, for the temporary rest given the muscle does not prove of any more service than rest without tenotomy, which has failed in all the more advanced cases, which are the only ones where tenotomy would be thought of.
Nerve-Stretching.—It is curious that no cases have been reported (at least I have not been able to discover them) of nerve-stretching for aggravated cases of copodyscinesia, as the operation has been performed in several cases of local spasm of the upper extremity following injuries to the nerves.
Von Nussbaum125 alone mentions the operation, and states that it has been of no avail, but gives no references; he previously126 stretched the ulnar nerve at the elbow and the whole of the brachial plexus for spasm [p. 539] of the left pectoral region and of the whole arm, following a blow upon the nape of the neck; the patient made a good recovery.
125 Aerztliches Intelligenzblatt, Munich, Sept. 26, 1882, No. 39, p. 35.
126 London Lancet, vol. ii., 1872, p. 783.
This operation, according to an editorial in the American Journal of Neurology,127 has been performed seven times for spastic affections of the arm with the following results: 2 cures (1 doubtful), 3 great improvement, and 2 slight relief.
127 Am. Journ. of Neurology and Psychiatry, 1882.
This procedure would seem to be indicated in those cases of copodyscinesia where spasms are present which have a tendency to become tonic in their character, where other means of treatment have failed. One such case has fallen under the writer's notice, which, on account of its singularity and the rarity of the operation, seems worthy of record. The patient is a physician in large practice, and his account, fortunately, is more exact than it otherwise would be:
—— ——, æt. 36. Paternal uncle had a somewhat similar trouble in right arm, father died of paralysis agitans, and one brother has writers' cramp. From nine to twelve years of age he was considered an expert penman, and was employed almost constantly, during school-hours, writing copies for the scholars. At the age of eleven he began to feel a sense of tire in right forearm and hand when writing; soon after this the flexors of right wrist and hand began to contract involuntarily and become rigid only when writing. He remembers being able to play marbles well for two years after the onset of the first symptoms. The trouble gradually increased until every motion of the forearm became involved. At the age of nineteen he became a bookkeeper, using his left hand, but at the end of one year this became affected also. Since then both arms have been growing gradually worse, and at one time exhaustion would bring on pain at the third dorsal vertebra. At the age of thirty a period of sleeplessness and involuntary contractions of all the muscles of the body came on, accompanied by difficulty in articulation from muscular inco-ordination. After persistent use of the cold douche to spine these symptoms ameliorated, but the general muscular twitching sometimes occurs yet, and overwork brings on spasm of the extensors of the feet. The condition of his arms in December, 1882, was as follows: At rest the right forearm is pronated, the wrist completely flexed and bent toward the ulnar side, the thumb is slightly adducted, and the fingers, although slightly flexed, are comparatively free, enabling him to use the scalpel with dexterity. This contraction can be overcome by forcibly extending the fingers and wrist and supinating forearm, but if the arm be now placed in supination the following curious series of contractions occur, occupying from one to two minutes from their commencement to their completion: gradually the little finger partially flexes, then the ring, middle, and fore finger follow in succession; the wrist then slowly begins to flex and to turn toward the ulnar side, and finally the arm pronates, in which position it will remain unless disturbed. The contraction is accompanied by a tense feeling in the muscles, but is painless. The left arm behaves in a somewhat similar manner, and if this is placed in supination a gradual pronation of the arm begins; then follows the flexion of the fingers, commencing with the little finger and ending with the thumb; the wrist also flexes, but not as much as the right, although the flexion of the fingers is more marked. There is no pain on pressure over [p. 540] muscles or nerves. The extensor muscles of both arms, although weaker than normal, are not paralyzed, those of the right responding more readily to both faradic and galvanic currents than do the left. There is no reaction of degeneration. The flexors respond too readily, the right showing the greatest quantitative increase.
In 1879, while abroad, his condition being essentially as above described, he consulted Spence of Edinburgh, who as an experiment stretched the left ulnar nerve at the elbow; immediately after the operation the muscles were paralyzed and the arm remained quiet; in twenty-four hours the nerve became intensely painful, and remained so, day and night, for three weeks; this gradually subsided, and ceased with the healing of the wound two weeks later. Forty-eight hours after the operation the spasm of the muscles returned, and in a short time became as bad as ever, proving the operation to have been a failure.
An interesting point to decide in this case is whether the symptoms point to an abnormal condition of the nerve-centres, first manifesting itself in difficulty of writing, or whether the constant writing induced a superexcitability (for want of a better term) of the spinal cord in a patient markedly predisposed to nervous troubles. This last hypothesis I believe to be the correct one.
It might be considered at first sight that the symptoms presented by this patient were due to a paralytic condition of the extensors, and not a spasm of the flexors, or at least that the latter was secondary to the former. While the extensors are somewhat weaker than normal from want of use, a careful study of the mode of onset of this affection and the symptoms presented later prove this idea to be erroneous.
In regard to the operation and its results, it seems that a fairer test of the efficacy of nerve-stretching in this case would have been made if the median and not the ulnar nerve had been stretched, as the latter only supplies in the forearm the flexor carpi ulnaris and the inner part of the flexor profundus digitorum, while the former supplies the two pronators and the remainder of the flexor muscles.
Of the mode of action of this operation we are still much in the dark, but it would seem to be indicated in any case where the contractions are very marked and tonic in their nature—not, however, until other means have failed to relieve.
In the ordinary forms of copodyscinesia, it is needless to say, the operation would be unjustifiable.
Mechanical Appliances.—Most of the prothetic appliances have been devised for the relief of writers' cramp, the other forms of copodyscinesia having received little if any attention in this direction. The relief obtained by their use is usually but temporary, especially if the patient attempts to perform his usual amount of work, which is generally the case.
These instruments are of undoubted benefit when used judiciously in conjunction with other treatment, as by them temporary rest may be obtained, or in some cases the weakened antagonists of cramped muscles may be exercised and strengthened. They all, without exception, operate by throwing the work upon another set of muscles, and failure is almost sure to follow their use if they alone are trusted in, as the new set of muscles sooner or later becomes implicated in the same way that the left hand is apt to do if the whole amount of work is thrown upon it.
[p. 541]To accurately describe these instruments is out of place in this article: those wishing to study this branch of the subject more fully are referred to the article by Debout,128 where drawings and descriptions of the most important appliances are given.
128 “Sur les Appareils prothetiques, etc.,” Bull. de Thérap., 1860, pp. 327-377.
Their mode of action may be considered under the following heads:
I. Advantage is taken of muscles as yet unaffected, which are made to act as splints (so to speak) to those affected, greater stability being thus given and cramp controlled when present.
Under this head may be mentioned the simple plan of placing a rubber band around the wrist, wearing a tight-fitting glove, or applying Esmarch's rubber bandage with moderate firmness to the forearm. Large cork pen-holders, by distributing the points of resistance over a larger surface, are thus much easier to hold than small, hard pen-holders.
Two of the instruments devised by Cazenave—one, consisting of two rings joined together in the same plane (to which the pen-holder is attached), and through which the index and middle fingers are thrust as far as the distal joints; and another consisting of two rings of hard rubber, one above the other, sufficiently large to receive the thumb, fore and middle fingers, which are thus held rigidly in the writing position—act in this manner, and are used when the cramp affects the thumb or fore finger.
II. The cramp of one set of muscles is made use of to hold the instrument, the patient writing entirely with the arm movement.
The simple plan of grasping the pen-holder in the closed hand, as previously described, or of thrusting a short pen-holder into a small apple or potato, which is grasped in the closed hand, occasionally affords relief and acts in this way. The instruments of Mathieu, Velpeau, Charrière, and one by Cazenave are based upon this principle. The first consists of two rings rigidly joined together about one inch apart, one above the other, through which the fore finger is thrust, and of a semicircle against which the tip of the thumb is pressed; the pen-holder is attached to a bar adjoining the semicircle and rings. Velpeau's apparatus consists of an oval ball of hard rubber carrying at one extremity the pen-holder at an angle of 45°; the ball is grasped in the closed hand, and the pen-holder allowed to pass between the fore and middle fingers. Charrière's instrument is a modification of the last, having in addition to the ball a number of rings and rests for the fixation of the fingers. The latter has also devised an instrument consisting of a large oval ball of hard rubber; this is grasped in the outstretched palm, which it fills, and is allowed to glide over the paper; the pen-holder is attached to one side. Cazenave's instrument is simply a large pen-holder with rest and rings to fix the fingers.
III. The instrument prevents the spasm of the muscles used in poising the hand from interfering with those used in forming the letters.
One of the instruments devised by Cazenave acts in this way: it consists of a small board, moving upon rollers, upon which the hand is placed; lateral pads prevent the oscillations of the arm due to spasmodic action of the supinators. The pen-holder is held in the ordinary manner.
IV. The antagonistic muscles to those affected by cramp are made to hold the instrument, while the cramped muscles are left entirely free.
[p. 542]But one instrument acts in this manner—viz. the bracelet invented by Von Nussbaum,129 which consists of an oval band of hard rubber to which the pen-holder is attached. The bracelet is held by placing the thumb and the first three fingers within it and strongly extending them.
129 Aerztliches Intelligenzblatt, Munich, 1883, No. 39.
The inventor claims great success by its use alone, as the weakened muscles are exercised and strengthened and the cramped muscles given absolute rest.
Résumé of Treatment.—In the complicated cases of copodyscinesia rest of the affected parts, as far as the disabling occupation is concerned, must be insisted upon: this should be conjoined with the use of the galvanic descending stabile current, combined with rhythmical exercise of the affected muscles and of their antagonists, and massage. Where there is evidence of a peripheral local congestion or inflammation, this must be attended to; for instance, if there is congestion of the nerves, or neuritis, flying blisters or the actual cautery should be applied over the painful spots, followed by the galvanic current. Where there is paralysis of one or more muscles, with evidence of interference of nerve-supply, the faradic current may be used with advantage.
Evidences of constitutional disease should lead to the employment of the treatment suitable for those affections.
| Age at time of onset: | |||
| Under 20 years | 7 | ||
| Between 20 and 30 | 25 | ||
| Between 30 and 40 | 7 | ||
| Doubtful | 4 | —43 | |
| Average age | 23.94 years. | ||
| Average age of males | 24.22 years. | ||
| Average age of females | 20.66 years. | ||
| Average length of time before the disease appeared after the commencement of telegraphing was— | |||
| In males | 7.27 years. | ||
| In females | 4 years. | ||
| The shortest period being | 6 months. | ||
| The longest period being | 20 years. | ||
| Left arm implicated in | 21 | ||
| (Not counting case with amputation of right arm) | 1 | ||
| Never used left arm | 8 | ||
| Left arm not affected, although used | 12 | ||
| Doubtful | 1 | —43 | |
| Percentage with left arm implicated | 63 | .63 | |
| No. of cases with difficulty in telegraphing only | 9 | ||
| No. of cases with difficulty in writing only | 0 | ||
| No. of cases with difficulty in telegraphing most | 22 | ||
| No. of cases with difficulty in writing most | 11 | ||
| No. of cases with difficulty in both alike | 1 | —43 | |
| Use of tobacco or alcohol: | |||
| No effect in | 14 | ||
| Bad effect in | 16 | ||
| Good effect (in moderation) in | 3 | ||
| Don't use either | 10 | —43 | |
| [p. 543] | |||
| Flushings in arm or face during work in | 22 | ||
| Brittleness of nails in | 5 | ||
| Emotional factor present in | 29 | ||
| Sympathetic movements in other parts in | 9 | ||
| Pain in back during work in | 18 | ||
| Trouble in performance of other acts in | 19 | ||
| Pain on pressure over nerve or muscle in | 13 | ||
| Cramp of flexor group of muscles: | |||
| In writing only | 0 | ||
| In writing most | 3 | ||
| In telegraphing only | 1 | ||
| In telegraphing most | 5— 9 | ||
| Cramp of extensor group of muscles: | |||
| In writing only | 0 | ||
| In writing most | 0 | ||
| In telegraphing only | 4 | ||
| In telegraphing most | 7—11 | ||
| Doubtful as to character of cramp | 11 | ||
| No cramp | 12 | —43 | |
| Manner of telegraphing: | |||
| Arm resting on table | 22 | ||
| Arm raised from table | 12 | ||
| Alternating one with the other | 7 | ||
| Doubtful | 2 | —43 | |
| Manner of writing: | |||
| Arm movement | 13 | ||
| Finger movement | 6 | ||
| Combination of the two | 24 | —43 | |
Tetanus (τεινω, to stretch) is a morbid condition characterized by tonic contraction of the voluntary muscles, local or general, with clonic exacerbations, occurring usually in connection with a wound. Cases of it may be classified according to cause (traumatic or idiopathic); to age (of the new-born and of those older); to severity (grave and mild); or to course (acute and chronic), this latter classification being the one of greatest value.
Though known from the earliest times, it is in the civil practice of temperate regions of comparatively rare occurrence, and even in military surgery has in recent periods only exceptionally attacked any considerable proportion of the wounded.
Occurring in individuals of all ages, the great majority of the subjects of it are children and young adults. Women seem to be decidedly less liable to it than men. That this is due to sexual peculiarity may well be doubted, since the traumatic cases are by far the most numerous, and females are much less often wounded than males. The traumatisms of childbed are occasionally followed by it (puerperal tetanus).
That race has a predisposing influence would appear to be well established; the darker the color, the greater the proportion of tetanics. Negroes are especially likely to be attacked with either the traumatic or idiopathic form.
Atmospheric and climatic conditions, beyond question, act powerfully in, if not producing at least favoring, the development of tetanus. Places and seasons in which there is great difference between the midday and the midnight temperature, the winds are strong, and the air is moist, are those in which the disease is most prevalent; and it is because of these conditions that the late spring and early autumn are the periods of the year when cases are most often seen.1
1 In his account of the Austrian campaign of 1809, Larrey wrote: “The wounded who were most exposed to the cold, damp air of the chilly spring nights, after having been subjected to the quite considerable heat of the day, were almost all attacked with tetanus, which prevailed only at the time when the Reaumur thermometer varied almost constantly between the day and the night by the half of its rise and fall; so that we would have it in the day at 19°, 20°, 21°, and 23° above zero (75°–84° F.), while the mercury would fall to 13°, 12°, 10°, 9°, and 8° during the night (50°–61° F.). I had noticed the same thing in Egypt.”
Cold has, from the time of Hippocrates, been regarded as a great predisposing if not exciting cause, and the non-traumatic cases have been classed together as those a frigore. It is not, however, the exposure to simply a low temperature that is followed by the disease, but to cold combined with dampness, and quickly succeeding to a temperature decidedly [p. 545] higher, as in the cool nights coming on after hot days in tropical regions, or in the spring and fall seasons of temperate latitudes, or in the cold air blowing over or cold water dashed upon a wound or the heated skin. That such cold, thus operating, does most usually precede the attack of tetanus is unquestionable; and it has by many been held that without it no traumatism will be followed by the disease. Observers generally are agreed, with Sir Thomas Watson, that “there is good reason for thinking that in many instances one of these causes (wound and cold) alone would fail to produce it, while both together call it forth.”
In the low lands of hot countries (as the East and West Indies) the disease is very frequently met with, at times prevailing almost epidemically; and, on the other hand, it is rare in dry elevated regions and in high northern latitudes, as in Russia, where during a long military and civil experience Pirogoff met with but eight cases. Trismus nascentium would seem to be an exception to the general rule of the non-prevalence of tetanus in places far north, since, e.g., it has been at different periods very common in the Hebrides and the small islands off the southern coast of Iceland. But these localities, from their peculiar position, are not extremely cold, and their climate is damp and variable; so that, even if the lockjaw of infants be accepted as a variety of true tetanus, the geographical exception indicated is but an apparent one.
Traumatic cases are greatly more numerous than idiopathic, and no class of wounds is free from the possibility of the supervention of tetanus. Incised wounds are much less likely to be thus complicated than either of the other varieties, though operation-wounds of all sorts, minor and major, have been followed by this affection. So frequently has it been associated with comparatively trivial injuries that it has become a common belief that the slighter the traumatism the greater the danger of tetanus. That this is not true the records of military surgery abundantly show. Wounds of the lower extremity are much graver in this respect than those of the upper. Injuries of the hand and feet, especially roughly punctured wounds of the palmar and plantar fasciæ (as, e.g., those made by rusty nails), have long been regarded as peculiarly liable to develop the disease, and accidents of this nature always give rise to the fear of lockjaw. Though there can be no question but that more than one-half of the cases of tetanus in civil life are associated with wounds of these localities, yet the number of such injuries is so much greater than of those of other parts of the body that the special liability of the subjects of them to become tetanic may well be questioned. In this connection it is a significant fact that during our late war of perhaps 12,000 or 13,000 wounds of the hand, only 37 were followed by tetanus, and of 16,000 of the foot, but 57. A few years ago numerous cases of tetanus were observed in our larger cities complicating hand-wounds produced by the toy pistol—injuries that were often associated with considerable laceration of the soft parts, and generally with lodgment of the wad.
Not even the complete cicatrization of a wound altogether protects against the occurrence of the disease, the exciting cause of which, under such circumstances, is probably to be found in retained foreign bodies or pent-up fluids.
ETIOLOGY.—Almost universally regarded as an affection of the central nervous system, inducing a heightened state of the reflex irritability, [p. 546] though some have maintained that the reflex excitability of the medulla and the cord is actually lessened, how such affection is produced is unknown; and it is an unsettled question whether it is through the medium of the nerves or the vessels, whether by ascending inflammation, by reflected irritation, or by the presence of a septic element or a special micro-organism in the blood.
That the disease is due to ascending neuritis finds support in the congested and inflamed state of the nerves leading up from the place of injury (affecting them in whole or in part, it may be in but a few of their fibres), and in the inflammatory changes discoverable in the cord and its vessels. But time and again thorough and careful investigation by experienced observers has altogether failed to detect any alterations in the nerves or pathological changes in the cord, other than those that might properly be attributed to the spasms, the temperature, or the drugs administered. The symptoms of acute neuritis and myelitis (pain, paralyses, and later trophic changes) are not those which are present in cases of tetanus. The evidences of inflammation of the cord are most apparent, not in that portion of it into which the nerves from the wounded part enter, but, as shown by Michaud, so far as the cellular changes in the gray matter are concerned, always in the lumbar region, no matter where the wound may be located.
The much more generally accepted theory of reflex neurosis is based upon the association of the disease with “all forms of nerve-irritation, mechanical, thermal, chemical, and pathological;” upon the direct relation existing between the likelihood of its occurrence and the degree of sensibility of the wounded nerve;2 in the, at times, very short interval between the receipt of the injury and the commencement of the tetanic symptoms; in the local spasms unquestionably developed by nerve-pressure and injury; in the primary affection of muscles at a distance from the damaged part; in the already-referred-to absence of the structural lesions of inflammation; and in the relief at times afforded by the removal of irritating foreign bodies, the temporary cutting off of the nerve-connection with the central organs, or the amputation of the injured limb. But that something more than irritation of peripheral nerves is necessary to the production of tetanus would seem to be proved by the frequency of such irritation and the rarity of the disease; by the not infrequent prolonged yet harmless lodgment of foreign bodies, even sharp and angular ones, against or in nerves of high sensibility;3 by the primary affection of the muscles about the jaws, and not those in the neighborhood of the wound; by the almost universal failure to produce the affection experimentally, either by mechanical injuries or by electrical excitations; by certain well-attested instances of its repeated outbreak in connection with a definite locality, a single ship of a squadron, a particular ward in a hospital, or even bed in a ward; by the usual absence of that pain which is the ordinary effect of nerve-irritation; and by the small measure of success which has attended operations, even when early performed, [p. 547] permitting the taking away of foreign bodies pressing upon or resting in a nerve, interrupting the connection with the cord, or altogether removing the wound and its surroundings. Even in the idiopathic cases—many of which, it would at first sight appear, can be due only to reflected irritation—another explanation of the mode of their production may, as we will see, be offered.
2 According to Gubler, the danger is greatest in wounds of parts containing numerous Pacinian corpuscles.
3 Heller has reported a case in which a piece of lead was lodged in the sheath of the sciatic nerve. Though chronic neuritis resulted, the wound healed perfectly. Two years later, after exposure while drilling, the man was seized with tetanus and died of it.
The so-called humoral theory would find the exciting cause of the disease in a special morbific agent developed in the secretions of the unbroken skin or the damaged tissues of the wound, or introduced from without and carried by the blood-stream to the medulla and the cord, there to produce such cell-changes as give rise to the tetanic movements. It finds support in the unsatisfactory character of the neural theories; in the strong analogy in many respects of the symptoms of the disease to the increased irritability and muscular contractions of hydrophobia and strychnia-poisoning, or those produced by experimental injections of certain vegetable alkaloids; in the recent discoveries in physiological fluids, as urine and saliva, of chemical compounds,4 and in decomposing organic matter of ptomaïnes capable of tetanizing animals when injected into them; in the rapidly-enlarging number of diseases known to be, or with good reason believed to be, consequent upon the presence of peculiar microbes; in the more easy explanation by it than upon other theories of the ordinary irregularity and infrequency of its occurrence, its occasional restriction within narrow limits, and its almost endemic prevalence in certain buildings and even beds; in the extreme gravity of acute cases and the protracted convalescence of those who recover from the subacute and chronic forms; in the very frequent failure of all varieties of operative treatment; and in the success of therapeutic measures just in proportion to their power to quiet and sustain the patient during the period of apparent elimination of a poison or development and death of an organism.
4 Paschkie in some recent experiments found that the sulphocyanide of sodium applied in small quantities caused a tetanic state more lasting than that caused by strychnia.
This theory is as yet unsupported by any positive facts. Neither septic element nor peculiar microbe has been discovered.5 Failure has attended all efforts to produce the disease in animals by injecting into them the blood of tetanics. There is no testimony worthy of acceptance of the direct transmission of the disease to those, either healthy or wounded, coming in contact with the tetanic patient; nor can much weight be attached to such reports as that of Betoli of individuals being attacked with it who had eaten the flesh of an animal dead of it.
5 Curtiss of Chicago thought that he had found a special organism, but further investigation showed that it was present in the blood of healthy members of the family and in the water of a neighboring pond.
The ordinary absence of fever has been thought to prove the incorrectness of this theory, but increased body-heat is not a symptom of rabies or strychnia-poisoning, of the tetanic state following the injection of ptomaïnes, or of cholera—a disease very probably dependent upon the presence and action of a bacillus. Martin de Pedro, regarding the affection as rheumatic in character, located it in the muscles themselves, there being produced, through poisoning of the venous blood, a muscular asphyxia.
[p. 548]MORBID ANATOMY.—The pathological conditions observed upon autopsy in the wound, the nerves, the central organs, and the muscles, have been so various and inconstant that post-mortem examinations have afforded little or no definite information respecting the morbid anatomy of the disease. Many of the reported lesions have unquestionably been dependent upon cadaveric changes or defective preparation for microscopic study. The wound itself has been found on the one hand healthy and in due course of cicatrization,6 on the other showing complete arrest of the reparative process (“the sores are dry in tetanus,” wrote Aretæus),7 or even gangrenous, with pus-collections, larger or smaller, in its immediate vicinity, usually in connection with retained foreign bodies.
6 Of one of Hennen's cases it is reported that “the life of the patient and the perfect healing of the wound were terminated on the same day.”
7 Morrison seventy years ago wrote: “Wounds from which there is a copious discharge of bland pus are seldom or never followed by this disease;” and as a rule this is true.
The nerves in and about the injured area have often been found reddened and swollen, their neuroglia thickened and indurated, and blood extravasated at various points. At times, even when to the naked eye healthy, microscopic examination has shown one or a few of the constituent bundles inflamed. But repeatedly the most thorough search has failed to find any departure from the normal state, and the same appearances of congestion and inflammation are not seldom observed when there has been no tetanic complication. In an interesting case reported by Michaud the sciatic in the uninjured limb presented the same neuritic lesions as that of the wounded side.
In the cord and the medulla vascular congestion has been the condition most generally seen, associated not infrequently with hemorrhages and serous effusions—a condition occasionally absent, and when present due, it is probable, in great measure, perhaps wholly, to the muscular spasms, or consequent in part upon post-mortem gravitation of the fluids. Increase in the amount of the connective tissue of the white columns of the cord (thought by Rokitansky to be the essential lesion of the disease); disseminated patches of granular and fluid disintegration (to which Lockhart Clarke called attention in 1864); atrophy of the cells, especially those of the posterior gray commissure; nuclear proliferation; changes in the color, form, and chemical reaction of the ganglion-cells; dilatation and aneurismal swellings of the vessels, with development of granulation-masses in their walls; and changes in the sympathetic ganglia,—such have been the reported lesions. But each and every one has at times been absent—at times been discovered in the bodies of those dead of other diseases. Some of the changes have without doubt been produced after death; some perhaps have been but errors of observation.
The muscles have been found healthy in appearance and constitution; discolored, softened, and the seat of blood-extravasations large and small; undergoing the vitreous degeneration; and ruptured, the laceration affecting a few fibres or the entire thickness of one or more muscles, as the rectus abdominis, the muscles of the neck, those in the vertebral gutter, and even the heart. The rigor mortis appears at once or very soon, thus confirming Brown-Séquard's observation, that cadaveric rigidity is “quick in coming on and quick in passing off in direct proportion to the amount [p. 549] of long-continued violent action which preceded death.” The visceral congestions that have been observed cannot be regarded as in any way peculiar, but as due simply to the muscular spasms and the mode of dying.
It is probably by chemical and microscopical examinations of the blood, and, much more, the solids and fluids of the damaged part or the secretions of the skin in the non-traumatic cases, that the cause of this obscure affection is to be discovered, and not from study of the nerves, the cord, and the brain; which study up to the present time has only shown that “tetanus has no morbid anatomy, except perhaps its traumatic cause and the asphyxial congestions resulting from it.”
SYMPTOMS.—Following the receipt of a wound, tetanus may be developed quickly or only after many days, cases of more or less credibility being on record of immediate appearance, and of an elapsed interval of one, two, three, even seven months (in a case occurring during our late war). Doubt, however, may very properly be entertained as to the true tetanic character of some at least of these very long-delayed cases, or of their dependence upon the previous traumatism. The very common belief that after the lapse of three weeks no fear of the disease need be entertained is unquestionably an erroneous one, but the danger certainly is slight when the wounded person has escaped for twenty-two entire days. In by far the larger proportion of cases the outbreak occurs between the fifth and fifteenth days after injury—in about two-thirds, according to Yandell's, or about four-fifths, according to Joseph Jones's and Otis's statistics.
Not infrequently for a day or two before any distinct evidences of the disease are manifested there is prodromal malaise, associated at times, but by no means constantly, with unusual sensitiveness, or even positive pain, in the wound and slight muscular twitching in its vicinity. In the larger number of cases the first symptoms noticed are stiffness about the jaw, more or less difficulty in opening the mouth, and perhaps slight interference with deglutition, the patient feeling as if he had taken cold; such symptoms often appearing early in the morning after waking from the night's sleep. With more or less rapidity well-marked trismus comes on, the jaws being locked, the corners of the mouth retracted, and the lips either firmly closed or separated so as to uncover the teeth, producing the peculiar grin long known as the risus sardonicus.
In rare cases it is the depressors, and not the elevators, of the lower jaw that are in a state of contraction, the mouth consequently being kept wide open. The forehead is wrinkled, the eyes staring, the nose pinched, and not seldom there is the facial expression of old age. The voice is altered and swallowing is difficult. Occasionally the spasms of the muscles of deglutition are so intense as to be the principal tetanic symptom, such dysphagic or hydrophobic (Rose) tetanus very generally proving fatal. In a few cases, after wounds of the face and head, these violent spasms have been found associated with facial paralysis, almost always, if not always, on the injured side; such paralysis having been present in at least one case (Bond's) in which throat-spasm was wanting, the wound being in the temporo-parietal region. Often there is early felt in greater or less intensity pain, as from pressure, in the epigastrium, piercing through to the back—a symptom by some regarded as pathognomonic, and due without doubt to contraction of the diaphragm.
[p. 550]From the region of the jaw the disease passes on to successively attack the muscles of the neck, the back, the abdomen, the chest, the lower, and, last of all, the upper, extremities, those of the forearm long after those of the arms. The muscles of the fingers, of the tongue, and those of the eyeball are very late if at all affected, the tongue probably never being tonically contracted. The anterior abdominal wall is broadened, depressed, and hard. In the fully-developed acute cases the whole body is rigid, remaining perfectly straight (orthotonos), arched backward (opisthotonos), forward (emprosthotonos), or laterally (pleurosthotonos), according as the muscular tension is balanced or greater on one side than another. The action of the extensors being usually the more powerful, backward bending (opisthotonos) to a greater or less extent is the ordinary condition; but only in rare and extreme cases is the contraction such as to curve the body like a bow and keep it supported upon the occiput and heels. Frequently the bending is not specially noticeable except in the neck. Emprosthotonos is rare, and pleurosthotonos has been so seldom observed that its very existence has been denied. Occasionally, in well-marked cases of opisthotonos, there is some associated lateral arching, due rather to voluntary efforts on the part of the patient (for the purpose of obtaining relief) than to tetanic contraction. Larrey's opinion that the location of the wound (behind, in front, or on the side) determined the direction of the curving has been proved to be incorrect. Except in a small proportion of cases to the persistent tonic spasm8 there is added convulsive seizures of the affected muscles, developed upon any, even the slightest, peripheral excitation of the reflex irritability, as by a movement, a touch, a draft of air, a bright light, a sudden noise, an attempt at swallowing, etc. The frequency of these clonic exacerbations and their intensity vary much, being severer and coming on closer together in the grave acute cases and in the later stages of those terminating fatally. They may occur only once in several hours or four, five, or more times in a single hour, each spasm lasting from but a few seconds to a minute or two. During its continuance the suffering is intense, both from the pain of the contraction and the experienced sense of suffocation. Between the paroxysms there is usually but little pain, the sensation being rather one of tension or pressure. Occasionally cessation of spasms and complete relaxation of all muscular contraction suddenly take place six, eight, or twelve hours before death, the patient quickly passing into a state of collapse.
8 This is not, in reality, a state of uninterrupted spasm, but one of very numerous, quickly-repeated muscular contractions, as many even as six hundred and sixty per minute (Richelot).
Throughout the whole course of the disease the mind remains clear,9 except in the later stages of a few cases; and then the existing delirium or coma is often, it is probable, an effect of the treatment that has been employed. Except in the more chronic cases the patient is generally unable to sleep, and even when fortunate enough to do so the tonic spasm may not relax. In other than the mildest attacks there is usually noticed a marked increase, local or general, of the perspiration; such sweating [p. 551] being a much more prominent symptom of the disease as met with in tropical than in temperate regions.
9 “The brain alone in this general invasion has appeared to us to constantly preserve the integrity of its functions down to the very last moment of existence, so that the unfortunate subject of this disease is, as it were, an eye-witness of his own death” (Larrey).
The pulse, which is normal in the earlier stages, may later be but little increased in frequency (except during the exacerbations, when, small and compressible, its beats may run up to 140, 160, or even 180 per minute), or it may become progressively feebler and more rapid as the case advances toward the fatal termination. The irregularity often noticed during the convulsive seizures is doubtless owing to the muscular contractions so compressing the vessels as to hinder the passage of the blood through them. That the heart itself is not tetanically contracted would seem to be proved by its regular quiet action during anæsthesia.
The body-heat varies greatly in different cases, the temperature being oftentimes normal, or even subnormal, until toward the very last. Not infrequently, even in severe and fatal cases, it is not increased more than two or three degrees, and quite rarely, except just before death, does it rise much above 103° F. Exceptionally, very high temperatures have been observed; I have myself seen one of 108° F. an hour before death. Prévost had a patient whose axillary temperature was 110¾° F. Lehmann reports a heat of 111.9° F. just before death, and in one of Wunderlich's cases the temperature (that three hours earlier was 103.5° F.) fifteen minutes before death was 110.1° F., and at death 112.5° F., with a further post-mortem rise of more than a degree (113⅔° F.)—a phenomenon that has been observed in a number of cases. This increased temperature of tetanus is not of inflammatory origin (except as a part of it, at times, may be due to intercurrent affections, especially a broncho-pneumonia), but depends doubtless upon a combination of causes, among them the violent muscular spasms, and, more particularly, the disturbance of the regulating heat-centre or centres from the alterations of their blood-supply in quantity and quality.
The bowels are usually constipated, because of the little food taken, the profuse sweating, the tonic spasms of the abdominal muscles, and the contraction of the external sphincter and the levator ani, the muscular coat of the bowel, like all the other involuntary muscles, remaining unaffected.
Micturition, generally infrequent because of scanty secretion, may or may not be disturbed. In many cases it is true, as written by Aretæus, "the urine is retained so as to induce strong dysuria, or passes spontaneously from contraction of the bladder,” though it is the external muscles, and not the bladder itself, the contraction of which produces the retention or the discharge; which latter is of rare occurrence.
DIAGNOSIS.—When fully developed, with all its characteristic symptoms present, tetanus cannot, or at least ought not to, be mistaken for anything else; yet a study of reported cases will show that errors of diagnosis have been made, and because of such errors various methods of treatment have been given undue credit as curative measures. Wound-spasms, clonic in character, of different degrees of severity, beginning in and confined to the muscles of the injured part or limb (even of the lower segment of the upper extremity), have not seldom been regarded as tetanic, which they certainly are not; and recovery having taken place, it has been attributed to the adopted treatment, operative or therapeutic. The comparatively few cases in which, primarily located in the vicinity [p. 552] of the wound, these traumatic spasms have become generalized in strict accordance with Pflüger's laws, or, much more rarely, passing over the intervening parts of the body, have seized upon the muscles of the jaw and neck, may perhaps, for want of accurate knowledge of the essential nature of tetanus, be regarded as a variety of the disease; but it is much to be regretted that observers and reporters have not clearly separated them from the cases of true tetanus (or the commonly met-with variety of tetanus) in which the first or first important symptoms are always in connection with the muscles whose nerves take origin in the medulla oblongata, no matter where the wound may be located or whether there is any wound at all. Not a few of the idiopathic cases may justly be regarded as of tetany, that “little tetanus” in which the spasms always proceed from the periphery toward the centre; are especially likely to affect the forearms and the fingers, forming in their contractions the obstetrical hand; are followed by periods of complete relaxation; can be brought on by compression of the main artery or nerve of the limb, or by light tapping of the affected area; may cause a rigid state of the trunkal muscles or even well-marked opisthotonos; are associated with impairment or paralysis of sensation; may last for a few minutes or for hours; and sooner or later spontaneously cease, a fatal termination of the affection being exceedingly rare.
Hysterical spasms may strongly simulate those of tetanus, and such attacks have without doubt been wrongly diagnosticated, the cases going to swell the number of those successfully treated by one remedy or another. They ought, however, to be readily recognized if due consideration be had of the age and character of the patients, the history of the attack, and the order and nature of the symptoms themselves, especially their frequent limitation to one member (preferably a leg), the absence of consciousness during the attacks, the long and uninterrupted rest at night, their more or less often and prolonged complete intermissions.
Cerebro-spinal meningitis, because of the developed stiffness of the neck and retraction of the head, the orthotonos, or even well-marked opisthotonos, the epigastric pressure-pain, the occasional trismus, and rigidity with reflex convulsive movements of the muscles of the extremities, may, and doubtless has been, mistaken for tetanus; but its generally epidemic prevalence, the headache, the cutaneous hyperæsthesia, the temperature, and the other well-known symptoms of the disease ought to suffice for its ready determination.
Strychnia-poisoning has many symptoms in common with tetanus, but there is an absence of the wound which is generally associated with the latter affection, a much more rapid development of severe convulsions, and a quickly-appearing opisthotonos. The spasms from the commencement affect the extremities, producing early contractions of the muscles of the hands and feet, and only later those of the jaw. Complete intermissions of greater or less length usually occur, and either death or marked amelioration of pain and spasm follows in a comparatively short time.
Hydrophobia, the dysphagic symptoms of which are like those at times observed in tetanus, has its peculiar wound of origin and protracted period of incubation, its absence of trismus or general tonic muscular contractions, its usual dread of water and inability to swallow fluids, its attendant restlessness, and its frequently-observed delirium, the entire [p. 553] aggregation of symptoms being characteristic of itself and nothing else except the simulating nervous affections occasionally developed in individuals bitten by rabid or supposed rabid animals.
PROGNOSIS.—As declared by Hippocrates, “the spasm that comes on after the receipt of a wound is a frequent cause of death.” Violent acute cases, developing early, are excessively dangerous; and there is much truth in Poland's declaration that “there is scarcely a well-authenticated instance of recovery on record.” Taking all the traumatic cases together as met with in military and civil hospitals, the death-rate may safely be placed at not less than 80 per cent. Of 1332 cases reported from the wars of the last thirty years, and occurring in six large hospitals during the last twenty years, 1060 proved fatal—i.e. 79.6 per cent.10
10 Crimean war, 23—21, 91 per cent.; Confederate army, (Sorrel), 66—60, 91 per cent.; U. S. army, 505—451, 89.3 per cent.; Italian war (Demme and Chenu), 176—162, 91 per cent.; Franco-German war (Poncet), 316—181, 57.28 per cent. (omitting Richter's 224 cases with only 107 deaths, the mortality of the remaining 92 cases (74) was 80 per cent.); St. Thomas's Hospital, 43—24, 55.8 per cent.; St. George's Hospital, 30—21, 70 per cent.; St. Bartholomew's Hospital, 63—47, 74.6 per cent.; Guy's Hospital, 60—51, 85 per cent.; Pennsylvania Hospital, 26—20, 76.9 per cent.; Boston City Hospital, 24—22, 91.6 per cent. The mortality-rate at Guy's (85 per cent.) is almost the same as that given by Poland for the period from 1825 to 1858 (86.1 per cent.).
As met with in private practice, under favorable hygienic surroundings, a decidedly larger percentage of recoveries probably takes place—how much larger cannot be even approximately determined, since, as a rule, only those cases which get well are reported, but few patients come under the care of any single observer, and the chances of error in diagnosis are much greater than in a large general hospital. The mortality rate of the idiopathic cases is very much lower (not exceeding perhaps 25 or 30 per cent.), localized trismus being “never mortal, though it may last for a number of weeks” (Poncet). That recovery should take place much more frequently in cases of this variety than in those associated with wounds might be anticipated, since, as a rule, they are more chronic in their course; the attacks are less frequent; if generalized, the spasms do not involve all the muscles at once, but by progressive seizures and relaxations; and they less often and less severely affect the muscles of respiration. The earlier the disease shows itself after the receipt of a wound (other things being equal), the stronger the likelihood of a fatal termination; and, for obvious reasons, the more powerful, more general, and more quickly repeated the spasms, the greater is the danger. The larger part of the deaths occur within the first week, a majority by the fifth day; all experience tends to show that there was much truth in the Hippocratic observation, that “such persons as are seized with tetanus die within four days, or if they pass these they recover.” From the end of the first week on, the chances of recovery rapidly increase day by day, and after the second week there is but little danger of a fatal termination, though death may take place (from exhaustion usually) after the lapse of several weeks, six or more.11 I have myself seen it occur on the thirty-seventh day.
11 Of the 358 cases reported in the Medical and Surgical History of the War of the Rebellion, the duration of which was known, 64.8 per cent. died within five, and 83.5 per cent. within ten days. Of 327 cases reported by Poland and Hulke, 56 per cent. died within the earlier, and 83.5 per cent. the later, period. Of Richter's cases, 76.6 per cent. died within five days. Of 170 cases tabulated by Yandell, 53 per cent. died within the first four days, and 77 per cent. within nine days.[p. 554]
Recovery is usually slow. Even in the non-traumatic cases the period of convalescence very seldom is less than two months, and, as has been truly said, “it is a very mild case that the patient is well of in thirty days.” More or less stiffness of the muscles usually continues for many weeks; in one case (Currie's) “his features retained the indelible impression of the disease;” and Copland reports having seen a man who had had tetanus nine years before, whose jaws were still permanently locked. Relapses may easily be brought on by exposure or slight imprudences, and such secondary attacks not infrequently prove fatal. The earlier and more severely dysphagic symptoms are manifested, the more grave the prognosis; and the sooner disturbances of respiration are shown, the speedier the death, since spasm of the respiratory muscles, in the words of Aretæus, “readily frees the patient from life.” Generally stated, “the more powerful the contractions, the greater the irritation and the danger;” and the longer the delay of involvement of the respiratory muscles, the more favorable the prognosis. The occurrence of strabismus is of grave import (Wunderlich), as might be expected, since only in very severe cases or in the later hours are the deep muscles of the eye affected by spasm. The manifestation of delirium (which is rare, and sometimes, if not generally, due to over-medication) indicates with almost absolute certainty a speedy death.
The pulse-rate and temperature, especially the latter, afford prognostic indications of value.
A rapid pulse is an unfavorable symptom; and if at the same time it is feeble and irregular, the probabilities of an early death are very great.12 Though, as has already been stated, the temperature often varies but slightly from the normal, even in acute and rapidly fatal cases, yet when the thermometer does not indicate a body-heat of over 100° F. the prognosis is unquestionably more favorable than when it is two or more degrees higher; and there is certainly much truth in the opinion (Arloing and Tripier) that as long as the rectal temperature is not above 1002/5° F. (38° C.) the prognosis is favorable; whereas when it rises the prognosis at once becomes much more grave, few patients recovering in whom it reaches 103° F. Oscillations of temperature are of no prognostic value, good or bad.
12 Few at the present time share Parry's belief, that “if in an adult the pulse by the fourth or fifth day does not reach 100 or perhaps 110 beats in a minute the patient almost always recovers,” and “if, on the other hand, the pulse on the first day is 120 or more in a minute, few instances will be found in which he will not die.”
Death usually occurs suddenly, from spasm of the external respiratory muscles or of those of the larynx, but it may be consequent upon a slow strangulation, upon exhaustion (as it frequently is in the chronic cases), or even upon heart rupture, as in a patient of Dujardin-Beaumetz.
How far the age of the patient affects the prognosis cannot be very definitely stated. The prevalent opinion (entertained as long ago as the time of Aretæus), that the disease is less dangerous in the middle part of life than as either extreme is approached, is probably an erroneous one. Yandell, from the analysis of the cases he had collected, found that the mortality was greatest in children under ten, and least in individuals between ten and twenty years old. Kane's statistics would place the time of greatest danger in the early adult period, from the age of twenty to that of thirty-five or forty.
[p. 555]In traumatic cases the location of the wound does not seem to materially influence the death-rate. As occurring during our late war, those associated with injuries of the upper extremity were the least, and of the head, face, and neck the most, fatal, but the difference in the mortality rates was but 8.4 per cent. (86.8:95.2 per cent.). It has long been believed that wounds of parts supplied by the cranial nerves are not only less often followed by tetanus than those of other regions, but that the disease when present is of a less fatal character. Of the 10 cases of the peculiar head-tetanus already referred to, collected by Bernhardt, 6 died (60 per cent.).
TREATMENT.—For the relief of tetanus agents of most diverse action and power have been employed, intended to control inflammation, allay nervous irritability, arrest spasm, and sustain the general strength; and operations have been performed with the view to destroy nerve-conduction, remove external irritants, change the character of the associated wound, or take away the originally damaged part. Much of the confusion and uncertainty that have prevailed respecting the therapeutic treatment has doubtless arisen from the want of distinct separation of the idiopathic from the traumatic cases, because of incorrect diagnosis, or through an unwarranted assumption of the general applicability of a method of medication found advantageous in individual cases of perhaps rheumatic, malarial, or meningeal disease.
Regarding the affection as inflammatory, the older surgeons treated it antiphlogistically, and until within comparatively recent times bloodletting and mercury were largely employed. General and local bleedings, resorted to as far back as the time of Hippocrates, were not seldom made in excessive amounts,13 the patient occasionally surviving both the disease and the treatment. The mercurials were pushed until profuse ptyalism was produced—a condition which could but add to the distress (because of the great difficulty experienced in clearing the throat and mouth), and likely to induce and increase the severity of the convulsive seizures. Combined with opium, calomel was formerly held in high repute, and numerous recoveries have been attributed to such treatment—recoveries, however, almost always of cases of chronic character and no great severity. Should the mycotic origin of the disease ever be demonstrated, there will be good reason, in its well-known destructive action upon minute organisms, for the administration of the mild or corrosive chloride of mercury. Cold baths and affusions have sometimes caused entire relaxation of the spasms, leaving the patient as supple as a glove, and not seldom have been followed by muscular ruptures or sudden death.14 The local application of ice to the spine has been credited with many cures, particularly of cases of the non-traumatic variety, and benefit has seemed to follow the employment of ether or rhigoline spray. Hot baths, water [p. 556] or air, general or local, have been largely used from the time of Paré down, and the induced free perspiration has in some instances seemed to have been of service, as have the medicinal agents acting as sudorifics, of which jaborandi has of late been the one ordinarily employed. “To relieve the contractions and provoke sweating are the two principal bases of treatment,” wrote Martin de Pedro. But it should not be forgotten that in many of the more severe and rapidly-fatal attacks profuse sweating is characteristic of the disease.
13 In a case of Lisfranc's, in twenty-six days venesection was made nineteen times, and seven hundred and seventy-two leeches were applied.
14 An interesting and frequently-mentioned case is reported by Sir James McGrigor. A soldier having tetanus (unusually severe) was “during the first part of the day drenched with rain, the thermometer standing at 52°, but after ascending one of the highest mountains in Galicia the snow was knee-deep and the thermometer below 30°. The patient was exposed to this inclement weather from six o'clock in the morning till ten at night, when he arrived half starved to death, but perfectly free from every symptom of tetanus.”
All violent depleting measures should be abstained from, since in the acute attacks they can do no good, and in the more chronic ones can only increase the general debility; and it is from exhaustion that the subjects of these latter usually die.
To lessen the reflex irritability, to quiet the muscular spasms, and support the patient are the prime indications; to fulfil which every agent in the materia medica that has, or has been supposed to have, any sedative action upon the nervous system has been employed, as well as remedies directly controlling muscular movements. Of the greater number of such it may be truly said, “They have the same value, and the best of them is good for nothing” (Giraldes).
At the present time the medicinal agents that are deserving of consideration are tobacco, the anæsthetics, curare, conium, cannabis indica, calabar, opium, chloral, and the bromides.
Tobacco, that in virtue of its depressant action so powerfully relaxes the muscles, was until the introduction of the anæsthetics largely employed and regarded with much favor, but of late years has rarely been used, inhalations of chloroform or ether securing more rapid and complete relaxation, with far less danger to the patient. Nicotine, in doses of from a fraction of a minim to a full minim (6/10 gr.) by the mouth, or two by the rectum (Houghton), has been given instead of the tobacco infusions with equally good effects, and of course the same dangers of producing fatal collapse.
The anæsthetics, chloroform and ether, have been frequently administered, but although muscular relaxation and sleep have been thereby secured, the natural progress of the disease toward a fatal termination has not been materially affected: death has at times been directly and suddenly produced, and not infrequently, though the inhalations have lessened suffering, they have seemed to hasten the end.
Curare, which “powerfully impairs and destroys the conductivity of motor nerves,” and of which, consequently, much was hoped at one time, has proved to be of but little value.15 In order that benefit may follow its administration the agent must be given in large doses and until a decided impression is made upon the innervation of the muscles of respiration, great danger meanwhile existing of producing asphyxia, for the relief of which artificial respiration must be instituted. McArdle of Dublin, in reporting recently a successful case of the acute variety in which gr. ⅔ was given every fifth hour, suggested the combination of curare and pilocarpine, “in the hope that the cardiac and respiratory trouble produced by the former might be prevented by the latter.” Uncertain in composition, cumulative in action, “dangerous, difficult to manage, [p. 557] and variable in its effects,” curare is not, so far as has as yet been determined, an agent to be recommended in the treatment of tetanus.
15 Of Demme's 22 cases, 14 died (63.6 per cent.); of Busch's 11 cases, 6 died (54.5 per cent.); and in 51 cases collected by Knecht the mortality-rate was 49 per cent.
Conium, the action of which is much akin to that of curare, and which primarily is upon the terminal portions of the motor nerves, has been occasionally employed—successfully in two cases by Christopher Johnson of Baltimore, who gave it hypodermically in doses of from 1/6 to 2 minims every one, two, or three hours. In two other cases under the care of the same surgeon death took place, but the remedy seemed to have acted beneficially in relieving the spasms and relaxing the tonic rigidity.
Calabar bean—which produces a paralyzing action on the spinal cord, abolishing its reflex functions, and later “diminishes and destroys the conductivity of the motor nerves”—though apparently of service in certain cases (almost all of them, however, in young subjects and of chronic character), has proved to be of little or no more value than other less dangerous agents. It was first clinically employed by Vella in the Italian war of 1859. Of the 39 cases in Yandell's table, 39 per cent. recovered; of the 60 in Knecht's, 45 per cent.; and of the 60 collected by H. C. Wood, 55 per cent. It may be administered by the mouth, the rectum, or subcutaneously in doses (of the extract) of from ⅓ gr. to 2 grs. every quarter hour, half hour, hour, or two hours (Ringer gave 4 grs. in an hour),16 according to the violence of the symptoms, being stopped when there is produced “vomiting, diarrhœa, or a rapid small pulse and clammy sweat.” Yet its beneficial action in severe cases is only manifested when it has been “pushed to the extent of rendering the patient collapsed, the temperature of his body falling perhaps to 94° or 95° F., the pulse being hardly perceptible at the wrist” (Macnamara); under which circumstances there is about as great risk of death from the treatment as from the disease itself. Always, fever is a contraindication to its employment.
16 E. Watson gave to a patient in the course of forty-three days the equivalent of 1026 grs. of the solid extract, a tincture of the powdered bean being largely employed.
Cannabis indica, originally used by the East Indian surgeons, and believed by them to have a powerful influence in controlling the tetanic spasms, has proved much less efficacious in cases occurring in Europe and this country, perhaps because of the unreliable character of the extract used; though of 42 cases of the traumatic variety treated in the Chadnie Hospital at Calcutta in five years (1865-69), 62 per cent., and of 39 idiopathic cases 40 per cent., died, and of Chuckerbutty's 13 cases in India, 6 (i.e. 46 per cent.) died. Of the 25 cases in Yandell's table, the mortality-rate was 36 per cent. If given, it should be in doses of from ½ to 2, or even 4, grs. of the extract, or minim 15 to drachm j of the tincture, every two or three hours. Having a strong hypnotic action, it is to this probably that the beneficial effects of its administration are due, rather than to its secondary influence upon sensation and muscular movements.
Of all the sedatives and narcotics, opium has been longest and most often used, and in so far as it relieves pain and causes sleep it is of service. Like the other agents, it must be administered in large doses, reference being had to the effect produced and not to the number of grains given. The difficulty of swallowing even the liquid preparations has of late years made the hypodermic injections of morphia the favorite mode of administering the drug. Demarquay has advised that the solution (1 part to 50 of water) should be thrown deeply into the substance [p. 558] of the affected muscles, as near as possible to the place of entrance of their supplying nerves; the result being to especially relieve the trismus and allow of the taking of food. Fayrer in India found opium-smoking of advantage. The mortality-rate of the 185 cases tabulated by Yandell treated with opium was 43 per cent., but, as is true of the other drugs that have been referred to, it is chiefly if not wholly in the mild and chronic cases that the beneficial effects have been observed.
So far as has yet been determined, chloral is our most valuable drug in the treatment of tetanus, as it is in that of the allied condition of strychnia-poisoning—not because of any direct antidotal action, but by reason of its producing sleep, lessening the reflex irritability of the spinal cord, and diminishing the violence and frequency of the muscular spasms, thus enabling the patient to keep alive until the morbid state can spontaneously disappear. Given usually by the mouth or the rectum, it has been administered hypodermically (as much as 5 grs. at a time by Salter) or, as proposed by Oré, thrown directly into a vein. If it is true, as has been claimed, that its beneficial effect is due entirely to the sleep secured (not infrequently after waking up the spasms return with increased violence), the drug should be administered in doses sufficiently large and repeated to maintain a continuous slumber. Verneuil (whose therapeutic formula has three terms, rest, warmth, sleep) has found that while with certain patients a drachm a day is enough, to others four times as much must be given, and directs that the chloralic coma be continued for about twenty days. Further experience may show that small doses may suffice to secure the needed quiet—as, e.g., the 40 grs. at bedtime, with, if necessary, 30 grs. more at midday, recommended by Macnamara. Such small doses are far safer than the enormous ones that have at times been employed,17 since chloral can exert a powerful toxic influence upon the circulatory and respiratory centres, death being almost always due to arrest of respiration, though in tetanic cases it may be the effect of slight spasm upon a heart the enfeebled state of which is indicated by a very rapid and thready pulse. The intravenous injections expose the patient further to the risk of the formation of clots and plugging of the pulmonary artery, several instances of which accident have already been reported, though this method of treatment has but seldom been employed. The death-rate of those treated by chloral alone was 41 per cent. in the 134 cases analyzed by Knecht, and 41.3 per cent. of the 228 tabulated by Kane.
17 Beck is reported to have given 420 grs. in three and a half hours, and Carruthers 1140 grs. in six days; both patients recovered—Beck's after a continuous sleep of thirty hours. In one case the chloral sleep was maintained without interruption for eight days, from 250 to 300 grains a day being given; and in another, which also recovered, over 3000 grs. were taken in the course of thirty-eight days.
Of late years use has been made, either alone or in combination with opium or chloral, of the bromides, especially that of potassium, which in full dose unquestionably diminishes reflex irritability, lessens the sensibility of the peripheral nerves, and moderates excessive body-heat. Under its influence mild cases of tetanus have recovered and more severe ones been somewhat relieved, and it has the decided advantage over the other drugs that have been noticed of not being a direct cause of death even when given in large dose—as much in some instances as six, seven, or nearly eight drachms a day. Knecht found that of 10 [p. 559] cases treated with chloral and the bromide, 9 got well; and Kane, of 21 to whom such a combination was given, only 5 died (23.8 per cent.); but the number of cases is too small to make conclusions deduced therefrom of any special value. Voisin reports a case (in which it should be noted the spasms began in parts near the wound, and that on the fourteenth day after the receipt of the gunshot injury of the right thigh) that had for eleven days been treated without effect with chloral in large quantity, which at the end of that time was put upon drachm ij doses of the bromide, with three hypodermics a day of about ½ gr. of morphia each: in three days decided improvement had taken place, and in four days more the patient was well.
The sedative and sustaining action of alcohol has many times been taken advantage of in the treatment of this affection. The administration of wines or spirits in large amounts has certainly been found of much service, though it will seldom or never be necessary to give wine, as Rush advised, “in quarts, and even gallons, daily.” 80 per cent. of recoveries appear to have taken place in the 33 cases that Yandell found to have been treated with stimulants; but, on the other hand, of Poland's 15 cases treated with wine, 75 per cent. died: here, again, the numbers are too few to make any deduced conclusions of much value.
As tetanus (or at least tetanoid spasm) has at times been observed as a consequence of malarial poisoning, and successfully treated with quinine, this remedy has occasionally been employed in cases not dependent upon paludism, but very generally to no purpose.
Fowler's solution of arsenic in doses of from 5 to 20 minims every two, three, or four hours has been believed by certain of our American surgeons (Hodgen, Prewitt, Byrd) to be of service.
Because of the supposed origin of the disease in peripheral nerve-inflammation or irritation, operative procedures have many times been adopted to interrupt the conduction or remove the part.
Amputation, which was so highly commended by Larrey, is now recognized as of no service in the severer and more acute cases, and as unnecessary mutilations in the chronic ones; and if performed in those of intermediate severity, when recovery takes place it will generally be difficult or impossible to determine of how much benefit the operation really was, and in some at least of the fatal cases the result can fairly be attributed to the amputation itself. When the disease is associated with an extensive lesion of an extremity, there can be no objection to the removal of the damaged part (if performed early), except that it may by the added shock still further weaken the patient and render him less able to hold out against the tetanus. In cases of severe spasms limited to the muscles of the injured limb (and such are frequently said to be of tetanus) amputation is often strongly indicated, and not seldom is the only treatment that will afford relief. During our late war “amputation was resorted to in 29 instances after incipient tetanic symptoms; 10 of the cases resulted favorably, and in several instances it is noted that the symptoms ceased after the operation.”18 Of Yandell's 17 cases, 60 per cent. recovered.
18 Medical and Surgical History of the War of the Rebellion.
As there is here, apparently, recovery in 34.5 per cent. of the gunshot cases treated by amputation (nearly one-fifth of all the non-fatal cases reported)—a very gratifying degree of success, and one that might properly encourage the resorting to this method of treatment—somewhat careful analysis may well be made of the 7 cases the histories of which are given. In 2, shell wounds of the foot, operated upon by the same surgeon, the disease appeared while the men were still upon the field. Of one of them it is stated that “there was but little hemorrhage, but the shock was excessive and tetanic symptoms were present;” and of the other, that “the peculiarities in the case were that symptoms of tetanus were quite marked, with great exhaustion.” There are certainly good reasons for believing that these two cases were not of tetanus, but of simple convulsive movements from shock and anæmia. Of the remaining 5 cases, the symptoms manifested themselves on the fourteenth, nineteenth, twenty-first, thirty-fifth, and fifty-fourth day after the receipt of the wound. One of the patients (in whom the disease was longest delayed), having a much inflamed and suppurating compound fracture of the bones of the forearm, “was suddenly seized with a chill followed by threatening tetanus,” and amputation was made the following day. In another (thirty-fifth day case) the “arm became much swollen and symptoms of tetanus ensued, including stiffening of the jaws, great pain and restlessness, and irritable pulse;” two days later the limb was removed, and “all symptoms of tetanus disappeared after the operation.” In another (twenty-first day) the man when admitted into hospital, one month after the date of the injury, stated that “he was first taken with trismus about a week before.” “As he was certainly getting worse every day,” the forearm was removed forty days after the receipt of the wound and nearly three weeks after the commencement of the tetanic symptoms. Other remedies employed after the operation (brandy, chloroform, and blisters to the spine) doing no good, drachm ss doses of the tr. cannabis indica were given every two hours, “under which the patient slowly improved.” In another case (nineteen days) the symptoms were those of tetanus; the amputation was made on the following day; twenty-four hours later “rigidity of the muscles had partly disappeared, and improvement continued until the patient was entirely relieved.” In the remaining case (fourteen days) the first symptoms of tetanus “were relieved by active purgatives, calomel, etc. Three days later the symptoms returned,” and on the next day “tetanus supervened in its usual form.” Five days afterward “the leg was amputated at the middle third, after which the tetanus subsided and the patient made a rapid and good recovery.”
In all of these five cases the disease appeared so long after the receipt of the wound that the chances were that if it was tetanus recovery would take place without regard to the treatment adopted; and of two some doubt may properly be entertained as to their real nature, there being present in both much inflammation—in one an initial chill, and in the other restlessness, great pain, and an irritable pulse. If the unpublished histories of the other three cases are similar to those given, these reported ten successful amputations can affect but little, or not at all, the previously entertained opinion of the real value of this method of treatment—that it is destructive to part, dangerous to life, and only very exceptionally, if ever, curative of the disease.[p. 560]
Nerve-section, first made by Hicks in 1797, and nerve-stretching, first performed by Vogt in 1867—reason for which can be found only in the neuritis (or, much more strongly, the reflex-neurosis) theory of the disease—has not been followed by relief in any unusually large proportion of cases,19 and should be practised only when the affected nerve is clearly indicated, when there is much pain in the wound, or when a distinct aura proceeds therefrom. In determining what nerve shall be divided or stretched regard may with advantage be had to Wood's symptom—to wit, the development of pain when pressure is made upon the nerve-trunk, branches from which terminate in the wound.
19 Of section, 21 cases, 10 deaths—i.e. 47 per cent. (Poncet); of stretching, 46 cases, 36 deaths—i.e. 78.2 per cent. (Harte).
Arloing and Tripier strongly advised total neurotomy (i.e. division of all the nerves going to the damaged part), and that high up—an operation that must be followed by extensive paralysis; not, however, permanent, they claim; in six months, at the latest, the power of motion being regained. This period is altogether too limited, as has been proved more than once. Fayrer reports having seen a case in which the hand was permanently crippled. It is to be noted that in most of these nerve-operation cases that terminate in recovery the tetanic spasms in the other parts of the body do not cease at once, but often quite slowly, and in the [p. 561] larger number of them internal medication of some kind is steadily employed. The removal of foreign bodies from the wound, the freeing of nerves from constricting ligatures, the division of the parts around containing nerve-fibres, and cauterization of the unhealed surface—each has at times proved beneficial, and the first two should always be early resorted to if the necessity therefor exists, no matter what views may be entertained respecting the nature and cause of the disease.
Tracheotomy, first proposed by Physick and later advised by Marshall Hall, has rarely proved of service, since the dyspnœa generally depends upon causes other than spasm of the laryngeal muscles. Verneuil, however, has recently stated that he has saved several lives by this operation.
Careful analysis of reported cases clearly indicates that neither in drug nor operation has a cure for tetanus as yet been found. Almost without exception “in the fully-developed cases all remedial measures fail, and the cases run on unchecked to a fatal termination;” and with the subjects of such acute attacks the physician, in the words of Aretæus, “can merely sympathize.” If not quickly overpowered by the violence of the seizure, and if he can be sufficiently supported, the patient may recover; and if there is late appearance, slow development, and infrequent and limited spasms, he probably will do so, whatever may be the treatment adopted.
“The first indication,” wrote John Hunter, “should be to strengthen the system;” and in the fulfilment of this indication food is of prime importance:20 “many patients perish from too much medication and too little feeding” (Agnew). Stimulants and hypnotics indirectly yet powerfully sustain the strength, and the removal of sensory irritants, as light and noise, by lessening the frequency of the spasms contributes to the production of the desired result, since in the convulsed muscles themselves there are developed substances that cause contraction. “Quiet and warmth are indispensable.” Fecal accumulations can but irritate, and therefore an early action through enema or mild drug should, if possible, be secured. As has been happily said by Labbé, “one must treat the tetanics, not tetanus.”
20 If necessary, fluids may be administered by means of a tube passed through the nose, or given by the rectum.
If little can be done to cure, much can be done to prevent. The influence of predisposing causes (anxiety, care, excesses, paludism) is to be counteracted as far as may be; the hygienic surroundings of the wounded are to be rendered as favorable as possible; especially is proper ventilation to be secured, and exposure to cold and rain avoided. Whether or not one believes with Rose that the disease depends not on the kind of wound, but on its treatment (“the earlier it is treated in the most careful manner the less frequently do we have tetanus”), there can be no question as to the great advantage to be derived from the thorough cleansing of the wound, the removal of irritating foreign bodies, the securing of free drainage, and the lessening of the amount of inflamed and dying tissue. The marked diminution in the number of cases observed in the last thirty years, as compared with that of a century or three-quarters of a century ago, is the direct result, we may well believe, of improved treatment of wounds and the wounded. The greater danger of slight injuries very possibly lies in their liability to be neglected or mistreated, [p. 562] and the special gravity of punctured wounds of the hand and foot in the anatomical obstacles presented to the ready outflow of blood, serum, or pus. In the exceedingly fatal toy-pistol wounds is it not in the decomposing débris of the lacerated tissues, or in the retained wad saturated with the secretions, that the danger lies of the development of tetanus, and not in nerve-irritation or any peculiar character of the injury? Certainly in the only case I have myself seen, in which the disease was not developed, the damaged hand was kept under hot water from the time it was hurt until healing was complete, and free drainage was from the first maintained.
Tetanus is reported to have appeared notwithstanding the associated injury was antiseptically dressed; but in modern wound-treatment, with its cleanliness, its protection of the damaged part, its infrequent manipulations, and its power to diminish inflammation and prevent decomposition, lies, we may well believe, the means of reducing to a minimum the danger of occurrence of those spasms that, once developed, are of “exceedingly painful nature, very swift to prove fatal, but not easy to be removed” (Aretæus).
As met with after abortion or labor at term, tetanus presents no special peculiarities in course, treatment, or termination. Of very rare occurrence in temperate regions, it is often met with in hot countries in women of the darker-colored races. Grief, anxiety, overwork, and profuse hemorrhage predispose to it, as do obstetrical operations and the retention of pieces of the placenta. Unlike the ordinary puerperal affections, it is more common in the country and in private practice than in cities and hospitals. Rather elderly women are more often attacked than are those younger. First and second pregnancies are the more dangerous if completed; later ones if abortion occurs. Abortion in the earlier months, especially in the third, is most likely to be followed by the disease (Garrigues). Ordinarily manifesting itself within ten days after labor, it has been known to occur after an interval of a month.
Hysteria, eclampsia, and especially tetany, may be mistaken for it. The latter affection, which generally attacks young women, may occur at any time during pregnancy or lactation—tetanus only within a comparatively few days after delivery.
Its TREATMENT is the same as that of ordinary tetanus, care being taken to remove from the uterus as speedily as possible any contained foreign body. Antiseptic irrigations may prove of service, though it is doubtful if their employment can accomplish much after the commencement of the spasms. Aveling has thought that transfusion might perhaps be of benefit.
The occurrence of intracranial congestions, hemorrhages, and venous thrombosis21 will, almost of necessity, render any medication of no value.
21 Such as were found upon autopsy in the case reported by Macdonald, and believed by him to be the essential lesions of the disease.
Under all circumstances the PROGNOSIS is exceedingly grave. The [p. 563] mortality-rate of the cases after abortion collected by Garrigues was 92 per cent. (25—23), and of those after labor 84.37 per cent. (32—27).22
22 As indicating the extreme gravity of tetanus occurring in connection with a wound of the genital tract, it may be noticed that of 17 cases after ovariotomy collected by Parvin, 16 died, 94.1 per cent., and of 24 cases tabulated by Olshausen, 23 died, 95.83 per cent.
From the earliest times it has been known that newly-born children are occasionally the subjects of trismus and generalized spasms, and that those thus affected usually die.
More common among the darker races23 and in warm countries (though some of the southern races and tribes are almost or altogether free from it), it has been for years together endemic in places far north (e.g. the islands of Heimacy and St. Kilda), and a veritable scourge in certain lying-in hospitals (e.g. Dublin, Stockholm, St. Petersburg). Occasionally it has prevailed epidemically.
23 Wallace, however, found that in the Medical College Hospital at Calcutta the disease occurred proportionably more frequently in the children of European than of native mothers, though the actual number of cases among the latter was very much the greater.
Attacking usually the children of the poor, others have not been altogether exempt from it, though unquestionably “it is most often seen where the mothers of the children are very young or very poor or very worthless” (Mosely). Rarely appearing before the third day, it as rarely occurs after the twelfth, generally manifesting itself within the first week.
Its cause has been thought to be navel-string injuries; inflammation of the umbilical arteries or vein; reflected irritation from the skin, the bowels, or the external genitals; uræmic encephalopathy; cold and dampness; defective ventilation; and indirect pressure upon the cerebellum and the medulla.
The supposed causative umbilical lesions have time and again been found in young infants presenting none of the symptoms of the disease; and the same is true of the vessel inflammations24 and of the reflex irritations. Atmospheric and climatic states and the hygienic condition of the child and its surroundings, however much they may contribute to the development of the affection, cannot be regarded as directly producing it; though experience has shown (as in the lying-in hospitals before referred to) that by securing proper care of the children, by improving the ventilation, and by preventing overcrowding, its prevalence may be very greatly diminished.
24 Mildner of Prague reports that in 46 fatal cases of inflammation of the umbilical vein, convulsions occurred in but 5, and in these the spasms were not like those of tetanus.
Forty years ago Marion Sims believed that he had discovered the exciting cause in “pressure exerted on the medulla oblongata and its nerves, the result most generally of an inward displacement of the occipital bone,” occasionally, though rarely, of the parietal. That intracranial pressure may give rise to tetanic symptoms is beyond question, seizures identical with those of tetanus having been observed in connection with tumors of the cerebellum (Hughlings Jackson), as also trismus, confined even to one side (Wernicke).
[p. 564]In some cases without doubt the occipital depression is secondary, the result of intracranial shrinkage; and even if primary, there may be no lockjaw.25
25 H. G. Lyttle of New York recently reported the case of a child two months old whose occipital bone was depressed and overlapped by the parietals, in which there had been no trismus, though the child had slight convulsive movements of the hands and rolling of the eyes.
Parrot regarded the disease as a form of eclampsia, the uræmic encephalopathy manifesting itself as one or other of the three varieties recognized (by Cederschjöld) a half century ago—viz. trismus, tetanus, and ordinary eclampsia. The articular rigidity, especially noticeable in the temporo-maxillary joint, he held to be largely independent of the convulsive tonicity of the muscles, and due in no small measure to induration of the overlying soft parts, such hardening being the result of that loss of fluid which, as it affects the body in general, produces the rapid and extreme emaciation which is so characteristic of the disease.26
26 Parrot adds: “In the new-born in a state of health great difficulty is experienced in separating the jaws, the muscles that bring them together having, relatively, considerable power, and the infants making quite an active resistance when one attempts to separate them. It follows that when a pathological state exaggerates this tendency it may be thought that we have to do with a veritable trismus.”
Though there is at times a prodromal period of restlessness and fretfulness, usually the disease is first indicated by an inability to nurse, the nipple being eagerly seized upon, but quickly dropped—an action that may be regarded as almost pathognomonic. Swallowing, difficult from the first, soon becomes impossible. The lower jaw in the earlier hours in many cases is dropped, but nearly always well-marked trismus is more or less quickly developed, at first intermittent, but later persistent. Opisthotonos in some degree is almost certain to be present, and in a large proportion of cases the tetanic convulsions become generalized, clonic exacerbations occurring as often as every half hour or hour, and capable of being induced at any time by pressure upon the abdomen (Morrison), or indeed by any external irritation, noise, touch, draft of air, etc.
All observers have noticed the peculiar cry, or rather whine, of the little patient. The bowels have in some cases been constipated, in others diarrhœa has been present. The temperature is generally decidedly elevated, and has been known to reach 111.2° F. Usually in from twelve to twenty-four or thirty-six hours collapse occurs, and the child speedily dies; though the fatal result may be deferred for a number of days or suddenly produced at any moment by spasm of the respiratory muscles.
Upon autopsy there has generally been found hyperæmia of the brain and cord with extravasations (commonly perithecal) in the spinal canal, occasionally in the meninges of the brain and in the ventricles. Very probably, as in true tetanus, these vascular conditions are the effect, and not the cause, of the spasms; and sometimes, doubtless, they are hypostatic.
As usually observed and commonly treated, the PROGNOSIS is very bad. Whether occurring in India or in Iceland, in the Rotunda Hospital in Dublin or in the Foundling Hospital in St. Petersburg, in the negro cabins of our Southern States or in New York or Washington, the subjects of it almost always die, generally in from six to forty-eight hours.27 It has been very exceptional to have 20 per cent.28 of [p. 565] recoveries, or even 15;29 and the non-fatal cases have almost invariably been those in which the disease appeared late and in mild form.
27 80 per cent. of the cases collected by Hartigan (207—165).
28 8 out of 40 cases tabulated by Smith; 8 out of 42 in the Stockholm Lying-in Hospital in 1834. It is very probable that these latter were cases of infantile meningitis.
29 5 out of 34 cases reported by Wallace from the Medical College Hospital of Calcutta.
When treated by manipulation and position, as recommended by Marion Sims, the chances of recovery seem to be very much greater. Even in the acute cases under the care of Sims, of Wilhite, and of Hartigan, death occurred only in those seen late, after extravasations had taken place.
The Sims's method consists simply in releasing the overlapped occipital bone by manipulation (or, if that fails, by an operation), and then placing the child so that the head shall rest flat upon its side, the face looking directly toward the horizon. The success attending this postural treatment has been so remarkable that the practitioner cannot be justified in failing to determine the relative positions of the occipital and parietal bones and to keep the head resting upon its side.
Of the medicinal agents that have been administered (the same as those employed in ordinary tetanus), calabar and chloral have of late years been the favorites, chloral to-day standing highest in professional estimation. Calabar is best given hypodermically in doses of from 1/12 to 1/6 gr. of eserine; chloral, either by the mouth (½ to 1½ or 2 grs.) or preferably by the rectum (2 to 4 grs.), either drug being pushed until relaxation takes place and sleep is secured, or toxic symptoms become so grave as to compel suspension of the treatment. Though favorable results have rarely followed such medication,30 and (with but few exceptions) only in late-developed and mild cases that very possibly would have gotten well of themselves; yet as recovery from an acute attack has occasionally been reported, at least the chloral treatment should be instituted in every case not found to be promptly relieved by change of position of the head.
30 Monti, however, reported 11 recoveries out of 16 cases treated with calabar (68.75 per cent.), 3 out of 5 in his own practice; and Widerhofer was credited in 1871 with 6 recoveries in the 10 or 12 cases that he treated with chloral.
Whatever views may be entertained as to cause or nature, it is to measures that will prevent development that we must chiefly look for relief from this lockjaw of infants, that even in our own country annually carries off a great number of children—25,000, as estimated by Hartigan. If mechanically produced, its occurrence should be rendered impossible by having the child's head from the time of birth properly placed, and at regular intervals changed in position. If defective hygiene, personal and social, is the one common and constant condition wherever the disease prevails, then due regard should be had to dressing the umbilical (and perhaps the preputial) wound; to bathing, clothing, and keeping quiet31 the child; to thoroughly airing,32 warming, and disinfecting the lying-in room; and to overcoming, as far as may be possible, the evil influences of unfavorable atmospheric and climatic conditions.
31 In these new-born children, though the reflex irritability is less than in those older, the response to irritation is very much greater, because of the lessened inhibitory power at this age (Soltmann).
32 By increasing the air-supply and lessening the number of beds the mortality at the Rotunda was in seven years reduced from about 1 in 7 to about 1 in 19 of the children born.
The study of speech, a complex function, enlisting at once the activities of mind and body, invites the physician to enter alike the domains of the psychologist and physiologist.
Distinguishing man from beast, articulate expression has its foundation in purely mental phenomena; its successful accomplishment requires the reflex mechanism common to man and beast.
Let us consider as concisely as possible the physiology of speech.
DEVELOPMENT OF SPEECH IN THE INDIVIDUAL.—The earliest observation has noted in the common name of the new-born child its speechless condition; it is the infant, or not-speaking being. Born with a nervous system in a highly unstable condition, the babe is a most favorable recipient of the many impressions which stream upon it from all sides. With sight and hearing undeveloped, the field of early infantile impressions is limited to hunger, need of sleep, and cutaneous impressions. Speech under such conditions is inarticulate, an animal cry, unconscious and without intelligence. But with the growth of the cerebrum the child's environment suggests to the embryonic intelligence its primal impression. The parental relation is dimly apprehended, and designations of the father and mother are uttered in scarcely articulate sounds.
Sight and hearing open extensive fields of sensation, and with their development begin the primal, physical impressions from which proceed the emotions. The acoustic and optic centres of perception become established, and the mental formation of symbols and signs, an imitative process, marks the stage of childish cerebration, beyond which the savage often does not proceed. The symbolic function is the basis of language and of pictorial representation; as man requires the trade medium of the symbol for the interchange of his ideas, so his legal tender appears with the first emergence of mental enterprise. The hieroglyphic and the onomatopoetic word are as old as humanity.
The co-ordinating mechanism of speech is of equal development. With the growth of the child the varied impressions of education, of surroundings, of heredity, all are influencing speech. With mental growth, stimulated by these numerous impressions, comes the gradual mental habit of forming ideas after certain models—of trading, so to speak, in the coin of the country, of making and using a vocabulary. Intuition, [p. 567] induction, and deduction are established, the general nervous function of memory develops, observations are made, and mind and body, master and instrument, enter upon full activity.
PHYSIOLOGY OF NORMAL SPEECH IN THE ADULT.—Let us consider normal speech in the adult. From a purely mental aspect speech is not included in the nervous reflexes. The conception before the individual may arise without sight or sound, it may be the object of the mental processes only; but if it is to be communicated, or transferred from the subjective to the objective, it calls into play the denotative faculty or facultas signatrix.
As we are cognizant through the senses of phenomena only, so we communicate only phenomena, or more particularly symbols; the spoken or written word, the gesture, are necessary to make ideas tangible to another mind. The symbolic faculty, then, is the mental faculty most concerned in speech.
Cerebral localization has not included this faculty in its areas; it is assigned to the anterior cortex, which as yet is the indiscriminate site of the formation of ideas. The idea conceived, the symbol formed, the motor area whose integrity is essential, is found in the region commonly known as Broca's convolution, the posterior third of the left third frontal convolution. This region is especially connected with the corona radiata coming from the corpus striatum, with the corpus striatum and the anterior portion of the internal capsule: like the anterior, or motor, cornua of the spinal cord, it possesses giant, or branching, nerve-cells; its anatomy would assign to it a motor function. Its blood-supply is derived through the inferior frontal branch of the Sylvian vessel, whose occlusion in a case cited by Charcot was followed by complete aphasia.
Ferrier distinguishes just adjacent to this centre the motor centres for the tongue and mouth and upper extremities, showing an anatomical association of the processes of articulate and written speech.
But purely motor impulses comprise only a portion of the phenomena of speech. The external world must be brought into relation with the mind, and this is done through the perceptions. We may say that perceptions are apprehended sensations, and this apprehension demands a localized field of cerebral activity, as well as the motor energies. It seems natural enough that experiment should have located (Ferrier) perceptive, visual, and acoustic centres in the posterior cortical areas and temporo-sphenoidal lobes—that the motor and perceptive areas should be contiguous and sharing a common blood-supply.
The perceptive visual centre is found to occupy the occipital lobes, while the acoustic centre occupies the whole length of the first temporo-sphenoidal convolution.
As motor impulses found a path to the motor ganglia, and finally to the cord, so the course of sensory perceptive impressions can be traced back through the posterior internal capsule and through the optic thalami to the sensory columns of the medulla and cord.
Intuitive and sense perception, even when reinforced with motor power, cannot result in articulation. The mechanism of speech requires a co-ordinating centre, and this basal phonic centre of Kussmaul is located in the medulla near the origin of the hypoglossal and facial nerves. From the medulla proceed the nerves supplying the machinery of [p. 568] phonation, the superior laryngeal nerve to the mucous membrane of the larynx and to the crico-thyroid muscle, the most important muscle of phonation. The remaining laryngeal muscles are supplied by the recurrent laryngeal; the motor processes of articulation are guided by the hypoglossal, facial, and fibres of the glosso-pharyngeal.
The larynx is a reed, with the addition of numerous resonance-cavities producing abundant overtones. It may be considered as a box composed of two segments, the lower of which has vertical motion upon the joint at the posterior junction of the superior and inferior segments. By this motion the tongue of the reed (vocal cords, stretching antero-posteriorly from lower segment to junction with upper segment) is tightened or relaxed, the vibratory blast of air coming through the trachea from the lungs. The superior aperture of the tube is guarded by the epiglottis and false vocal cords. As auxiliaries are the pharyngeal, oral, and nasal cavities, with the associated bony cavities of the skull, the soft palate acting as a movable partition or switch, the hard palate as a sounding-board or resonance-surface. The reed is applicable to the production of musical sounds; the tongue, lips, and teeth are required for the checks in those sounds, constituting the consonants or division utterances.
The curious phenomenon of the falsetto voice is thought by Helmholtz to be produced by the attenuation of the true cords and the vibration of their thinned edges.
DEVELOPMENT OF LANGUAGE.—The study of language demonstrates its origin to have been largely in exclamations and imitative sounds, from which our vowels can easily have arisen. The growth of all synthetic language illustrates the aggregation of accessory sounds about the primitive root-sound, while the common tendency to the insertion of consonants shows their addition to the primitive vowels. That the long vowels should have undergone countless modifications from the physical peculiarities and environment of those speaking them is but natural, for the number of vowels remaining in actual use in any language is not large. Consonants serve to make more clear by their separation of vowel-sounds the meaning to be conveyed; their development resulted from vowel changes, and their number is small.
The written characters of language represent only the usage of the majority. Individual speech and pronunciation vary as greatly as do languages themselves, and it is evident that the speech of any individual is as truly peculiar as his physical conformation.
To recapitulate, we find ideas, the material of speech, formed in the cerebral cortex. Speech-volition becomes motor impulse at Broca's convolution; such impulse passes along the internal capsule to the corpus striatum, where it is co-ordinated probably in the formation of syllables, thence to the medulla, whence the mechanism of the larynx receives its co-ordinated stimulation.
The classification of the disorders of speech should depend on the anatomical site of the lesions by which they are occasioned. Broadly [p. 569] speaking, speech disorders resolve themselves into those of the formative apparatus for ideas and symbols and those of the purely co-ordinating and conducting mechanism. Abbreviating the schedule of Potter, we may say that the disorders of speech may be included in three classes—alalia, or lack of speech; paralalia, defective speech, the stammering of most observers; and dyslalia, difficult speech or stuttering.
The anatomy of the blood-supply of the speech-centres affords some explanation of alalia. The Sylvian artery will be remembered as the feeder of the speech-centres—an artery often the source of hemorrhage, as Charcot suggests, from the angle at which it leaves the carotid. Ducrot explains the frequency of left-sided softening and hemorrhage from the manner of origin of the left carotid, its axis being more nearly that of the ascending aorta and furnishing a ready channel for cardiac clots. In regard to the relative frequency of peripheral and central hemorrhage, Andral and Durand-Fardel cite 119 cases, of which but 17 were in the anterior or posterior lobes. It is admitted that cerebral lesions are largely those of the circulatory system, and the fact that such lesions result in the suspension of the activity of restricted areas is due to the circumstance that the cerebral arteries are terminal vessels giving off no anastomosing branches and supplying restricted areas only. With blood-supply so arranged it is not difficult to understand how the different portions of the motor centres may be separately involved, and thus the motor functions of speech may become singly at fault.
Inability to remember words and inability to form the motor impulses necessary for speech or writing are the common forms of alalia or aphasia, the former being known as amnesic, the latter as ataxic, alalia. In addition, we may cite the failure of cerebral power occurring in general softening, in microcephalic brains, and the curious instances of voluntary silence from some strong belief or prejudice. Instances of the gradual resumption of cerebral function after its loss are not wanting; and, occurring where subsequent post-mortem examinations reveal a limited area of destruction of brain-tissue, they afford examples of the vicarious performance of cerebral functions by contiguous areas.
The phenomena of amnesic alalia are commonly seen in cases of recovery from cerebral hemorrhage, cerebral injury, and severe febrile affections. Numerous cases are recorded where the memory of things themselves remained, but the faculty of denoting them had been destroyed.
Kussmaul distinguishes here two conditions: 1st, where the word is entirely effaced from memory, 2d, where it still remains, but its association with that which it represents is suppressed. Cases of the second class are the most frequent, the fundamental part which the association of ideas plays in mental activity and the extent to which memory is dependent on association explaining this fact. A marked example of the failure of the denotative faculty lies in the cases of forgetfulness of one's own name, as described by Crichton in the case of an ambassador at the Russian court, who was obliged to say to his companion, when visitors asked his name, “For Heaven's sake, tell me what I call myself!” Piorry mentions the case of an aged priest who after right-sided paralysis lost entirely the use of substantives; wishing to ask for his hat, the word hat failed him utterly, and he was obliged to express himself in the remaining parts of speech: “Give me that which I place upon the [p. 570] ——;” but the word head, denoting the object most commonly in relation with the hat, was wanting also. When either hat or head was mentioned he spoke the word without difficulty.
Instances of failure in linguistic faculty are not uncommon. Witness a case, reported by Proust, of an Italian who after long residence in France, though understanding his native tongue, could speak only in French. Cases in which after acute disease one language is gone entirely while several others are retained are not wanting. A striking case of amnesic alalia was that of Lordat, a French physician, who thus described his malady: “I find myself deprived of the value of all words. If any words remain to me, they become useless, because I can no longer remember the manner in which I must co-ordinate them to express my thoughts. I am conscious that I recognize all ideas, but my memory does not suggest a word. In losing the memory of the meaning of spoken words I have lost that of their visible signs.”
Fortunately, these cases are among the more tractable of cerebral disorders. Bristowe has reported a case wherein elementary instruction in speech-formation was tried with marked success. The patient, aged thirty-six, after a violent cerebral disturbance without traumatism became paraplegic, speechless, and deaf. Gradual recovery ensued until, seven months after his first illness, he was admitted into St. Thomas's Hospital in the following condition: Numbness and paresis in left leg, less in left arm; special senses healthy; no incontinence; some pain about head and neck; complete loss of speech. It was found that the patient was very intelligent, wrote legibly, could make all kinds of voluntary movements with lips, tongue, and teeth, and was capable of vocal intonation; articulation alone was lacking.
The law of the evolution of language designates as primitive forms of word-signs those words affirming qualities, while those denoting relative positions are of secondary formation (Whitney.) Remembering, also, the fact that amnesia in general “is a regression from the new to the old, from the complex to the simple, from the voluntary to the automatic, from the least organized to the best organized,”1 we are able to understand the cause of amnesic alalia, and also the steps of the process of recovery, in which the inverse order is observed.
1 Ribot, Diseases of Memory.
Amnesic alalia can hardly be regarded as susceptible of treatment other than as a general neurasthenia. Though we may develop memory by cultivating the association of ideas and by repetition, yet, regarding it as a general function of the nervous system, it is evident that recovery from its disorders is conditioned by the general vigor of the nervous centres. A partial recovery usually occurs in such cases; complete recovery is more infrequent.
Ataxic alalia, the failure of the motor powers of speech, occurs in all forms of general paralysis, most typically in bulbar paralysis. This disease is fully described in the standard works on neurology. Ataxic alalia will also occur in disseminated sclerosis, posterior spinal sclerosis, dementia paralytica, and cretinism. It forms in general disorders an instructive symptom, and is to be distinguished by a tremulous utterance and by facial spasm from the hesitation of the stammerer and from the convulsive utterance of the stutterer.
[p. 571]Paralalia embraces all abnormalities of speech, from trivial mannerisms to difficulties in the utterance of certain letters, including those painful defects which depend upon physical malformations.
The free discussion of paralalia would cover the domain of elocution; the physician is called upon to advise in those cases only where either a physical malformation is evident or the difficulty experienced by the patient in enunciating certain letters has led to a suspicion of the existence of malformation. The former cases lie in the province of the surgeon; the latter come within the scope of those elocutionists, speech-trainers, and instructors who hope to cure stammering and stuttering.
Discrimination between stammering and stuttering will give the physician a basis for judgment from which he can reasonably offer encouragement in many cases and avoid the creation of false hopes in others. As a cardinal point of difference, it will be remarked that in the case of the stutterer the muscles of phonation are thrown into a state of spasm when speech is attempted, while in the stammerer their movements are merely lacking in proper co-ordination. It may also be observed that the respiration of the stammerer is marked by irregular contractions of the diaphragm, which render the expiratory blast of air irregular in its delivery. In the stutterer the spasm is pronouncedly laryngeal and facial. The nervous embarrassment of the stutterer is proverbial, and is increased by excitement, while a moderate degree of excitement, stimulating respiration, greatly improves the speech of the stammerer.
Whispering, a difficult respiratory act, exaggerates the stammerer's fault, but the spasm of the stutterer is often relaxed by the diminished pressure of whispered breath.
As articulation is effected by the larynx and the oral organs, the stutterer makes his spasmodic articulation particularly noticeable, while the stammerer finds little difficulty in the utterance of words. R, L, S, and other letters whose enunciation demands the continued expiratory blast, are imperfectly uttered by the stammerer, while these letters when joined to a long vowel-sound occasion little or no difficulty for the stutterer.
TREATMENT.—It follows that if stammering is recognized as inco-ordinate enunciation, owing largely to irregular action of the diaphragm, any training of the respiratory muscles which will ensure a regular delivery of the expiratory air will improve this defect. It follows, then, that the treatment of stammering resolves itself into careful attention to general hygiene, associated with such persistent respiratory and vocal gymnastics as shall effectually develop regularity, depth, and co-ordination of action on the part of all the muscles concerned in the act of respiration. Drugs will be of service only as aids to the correction of errors in the essential physiological functions. In the child the powers of imitation may be enlisted to effect a cure, and the familiar fact that the habits of childhood are easily formed would indicate this as the best time for treatment.
Childhood once passed, however, the steadiness of purpose of the adult is requisite to break up a confirmed habit, and active treatment should be deferred until after adolescence. Most important in all cases are judicious moral influences exerted by those about the patient, the ridicule so often visited upon the unfortunate stammerer being most harmful in its consequences. The many tricks and devices so often employed in these [p. 572] cases are of use simply by varying the monotony of vocal drill; they may be employed or abandoned as the judgment of the physician may dictate.
Regarding the prognosis in these cases, it follows that with a fairly developed and healthful nervous system, reinforced by proper mental and physical hygiene, the stammerer's case is far from hopeless in the hands of a patient and intelligent physician.
An unfavorable prognosis would be demanded by hereditary defects and vices of the nervous system, by the lack of general nervous vitality, by enfeeblement of the will and the mental tone of the individual, by advanced age, and by irremediable hygienic conditions. Under favorable conditions recovery should be the rule.
DYSLALIA OR STUTTERING.—Recalling to mind the points of difference between stuttering and stammering, it becomes evident that while the prospect of success in the treatment of the stammerer is often favorable, the case of the stutterer presents such difficulties as render it too frequently hopeless.
We may liken the confirmed stutterer to those rare cases of chorea which defy treatment, and to those cases of hereditary deterioration of the nervous system where the most patient and painstaking care fails to overcome the defect. The laryngeal and facial spasms depend upon no malformation for their exciting cause; hence surgery fails to remedy the defect. Drugs which are given with hope of invigorating the nervous system have only a general tonic influence, while the motor depressants and antispasmodics find but partial success. We must again rely upon hygiene, and also upon those aids to enunciation which come from rhythmical associated movements, such as stamping with the foot, beating time with the hand, the employment of a sing-song tone, or other modes of specially rhythmic enunciation. The sing-song mode of utterance is a familiar resource with parents in attempting to aid a stuttering child, and the measured forms of articulation offer the only vocal drill that possesses any permanent value. It is especially essential in the stutterer's case that the patient be protected from ridicule and from all disturbing emotions: the burden of difficult speech is sufficient to greatly depress the nervous system without the added suffering of emotional distress. It is evident that childhood, characterized as it is by especial instability of the nervous system, is the period when we can hope for the best results from care and training; the long-formed habits of the adult are rarely broken.
We have thus traced the disorders of speech to their origin as symptoms of grave central lesions of the nervous system, as results of heredity or of a general neurasthenic condition; very rarely are they dependent upon malformations of the organs of speech.
The treatment of such malformations, when they occur, is largely unsatisfactory and is seldom curative.
The thorough treatment of those speech disorders that are not susceptible of surgical aid would embrace such mental and physical hygiene and training as should ensure the formation of a thoroughly conceived vocabulary and its co-ordinated expression by words either spoken or written. The study of expression in its highest forms would necessarily conduct the investigator far into the realm of the plastic, harmonic, and literary arts.
DEFINITION.—Alcoholism is the term used to designate collectively the morbid phenomena caused by the abuse of alcohol.
SYNONYMS.—Alcoholismus, Ebrietas, Ebriositas, Temulentia, Drunkenness, Delirium potatorium, Mania potatorium, Delirium tremens, Chronic alcoholic intoxication, Dipsomania; Ger. Trunkenheit, Trunksucht; Fr. Ivresse, Ivrognerie.
These terms are in common use to describe such conditions and outbreaks in alcoholic individuals as amount to veritable morbid states or attacks of sickness, but they are not interchangeable, nor are they all sufficiently comprehensive to constitute true synonyms. They are names applied to various conditions due to acute or chronic alcohol-poisoning properly and distinctively comprehended under the general term alcoholism.
CLASSIFICATION.—It was formerly the custom to restrict this term to affections of the general nervous system induced by continued excesses in the use of alcoholic drinks.1 But the nervous system bears the brunt of the attack and suffers beyond all others alike in transient and in continued excesses. The artificial restriction of the term to the cases caused by continued excesses was therefore illogical in itself, and has been productive of much needless difficulty in the treatment of the subject and in the classification of the cases. The use of the term chronic alcoholism to denote an established condition, and of acute alcoholism to describe outbreaks of various kinds which occur in individuals subject to that condition, has also proved a source of embarrassment to the student. Not less vague has been the employment of such terms as delirium tremens, mania-a-potu, and the like, which are unsatisfactory in themselves, and tend to exalt symptoms at the expense of the morbid condition of which they are only in part the manifestation. I am of the opinion—which is at variance with established usage—that the systematic discussion of alcoholism requires that all forms of sickness, including drunkenness, due to that poison must receive due consideration, and that the term acute alcoholism, hitherto used in a sense at once too comprehensive and too variable, should be reserved for those cases in which the sudden energetic action of the poison is the occasion of like sudden and intense manifestations of its effects. Furthermore, the uncertainty and lack of precision in the use of the terms acute and chronic alcoholism are due to errors of theory formerly almost universal in medical [p. 574] writings and popular belief concerning the disease. The chief source of these errors was the recognition only of the more acute nervous affections caused by alcoholic excess—delirium tremens, maniacal excitement, and terrifying hallucinations—and the belief that these conditions occurred only after a temporary abstinence in the course of habitual or prolonged indulgence. It has now long been known that abstinence from drink by no means necessarily precedes the outbreak of mania or delirium, and modern researches have established the existence of a chronic alcoholic intoxication of long duration extending over a period of months or years, in which such outbreaks merely exhibit the full development of symptoms that have already been occasionally and partially recognizable.
1 Anstie, Reynolds's System of Medicine, vol. ii., 1868.
The following arrangement of the topics will facilitate the discussion of the subject in the present article, and serve, I trust, a useful purpose for the classification of cases in accordance with existing knowledge:2
I. Acute Alcoholism: Drunkenness, Debauch.
A. Ordinary or Typical Form.
B. Irregular Forms.
1. Maniacal;
2. Convulsive;
3. In persons of unsound mind.
C. Acute Poisoning by Alcohol: Lethal doses.
II. Chronic Alcoholism.
A. Visceral Derangements.
1. Local disorders:
a. Of the digestive system;
b. Of the liver;
c. Of the respiratory system;
d. Of the circulatory system;
e. Genito-urinary system.
2. Disorders of special structures:
a. Of the locomotor apparatus;
b. Of the skin.
3. General disorders:
a. The blood;
b. Obesity;
c. Cachexia.
B. Derangements of the Nervous System: Cerebro-spinal Disorders.
1. Cerebral disorders.
2. Spinal disorders.
3. Disorders of the peripheral nerves.
4. Disorders of the special senses.
C. Psychical Derangements.
1. The moral sense.
2. The will.
3. The intellect.
4. Alcoholic delirium in general.
5. Delirium tremens.
6. Alcoholic insanity:
a. Melancholia;
b. Mania;
c. Chronic delirium;
d. Dementia;
e. Paretic dementia.
III. Hereditary Alcoholism.
IV. Dipsomania.
2 This classification is in part based upon that of Lentz, De l'Alcoholism et de ses Diverses manifestations, etc., Bruxelles, 1884—a prize essay.
HISTORY.—The history of the abuse of alcohol would be the history of society from the most remote period until the present time, not only among civilized but among barbarous races of men, for the abuse of narcotics, of which alcohol is at once the most important and the most widely used, forms a dark background to the broad picture of healthful human progress. In truth, the most sketchy account of our knowledge of the effects of alcoholic excess, as manifested in the individual and in society at large, interesting as it might prove to the general reader, would be out of place in this article. To be of real [p. 575] value it would necessarily embody a record of experiences so vague, facts so indeterminate, opinions so at variance, and citations so numerous, that they would require for their mere presentation a volume rather than an article. The object of the writer in the following pages shall be, therefore, to present the subject in its present aspect, without reference, beyond that which is absolutely necessary, to considerations of mere historical interest. This being the case, he considers further apology for the lack of laborious historical studies unnecessary.
ETIOLOGY.—A. Predisposing Influences.—We are at this point confronted with a series of problems the complex nature and grave importance of which appeal with peculiar urgency to all thoughtful physicians. Their discussion, however, involving as it does unsettled questions of great moment in social science, is beyond the scope of the present article. A few practical points only can occupy our attention.
The influences which predispose to alcoholism arise from unfavorable moral, social, and personal conditions.
Among the unfavorable moral conditions may be mentioned a want of wholesome public sentiment on the subject in communities. This arises too often, but by no means exclusively, from poverty and its attendant evils ignorance and vice. Rum is at once the refuge and the snare of want, destitution, and sorrow. To the vacant and untrained mind it brings boons not otherwise to be had—excitement and oblivion. That both are brief and bought at a ruinous cost exerts little restraining influence. Of equal if not greater importance are the influences which spring from ill-regulated and demoralizing domestic relations, and the absence of motive and the contentment which properly belong to the family as an organization. Everywhere also do we find in example a potent influence. In the individual, in addition to hereditary propensities, the evil results of a lax, over-indulgent, or vicious early training, as shown in a want of power of application, of moral rectitude, in self-indulgence, craving for excitement, and a weak will, powerfully predispose to the temptations of alcoholic excess.
Among social conditions which must be regarded as predisposing influences occupation takes the first rank. The occupations which render those pursuing them especially liable to alcoholism may be divided into two classes—those in which the temptation to drink is constantly present, and those in which the character of the work begets a desire for stimulation, while the opportunities for the gratification of the desire are but little restricted.
To the first of these groups belong all classes of workmen in distilleries, breweries, and bottling establishments; keepers and clerks of hotels, public houses, and restaurants; the barmen and waiters in the same trades; the salesmen who travel for dealers in wines and spirits. To this group must also be referred the professional politician of the lowest order. These occupations have furnished by far the larger number of cases that have come under my care, both in hospital and in private practice.
To the second class belong occupations involving great exposure to the inclemency of the weather. We frequently find cabmen, expressmen, coal-heavers, hucksters, and street-laborers habitually addicted to excesses in alcohol. The stringent regulations of corporations exert a powerful [p. 576] protective influence in the case of men employed on railways, ferry- and other steamboat service, and in and about dépôts and stations. Exhausting toil under unfavorable circumstances as regards heat and confinement predisposes to drink, as in the case of foundrymen, workers in rolling-mills, stokers, and the like. The men-cooks who work in hotels and restaurants are especially liable to alcoholism. Monotony of occupation, as in the cases of cobblers, tailors, bakers, printers, etc., especially when associated with close, ill-ventilated workrooms and long hours of toil, exerts a strong predisposing influence. Persons following sedentary occupations suffer from excesses sooner than those whose active outdoor life favors elimination. To the monotony of their occupations may be ascribed in part, at least, the disposition of soldiers, ranchmen, sailors, etc. to occasional excesses as opportunities occur. Irregularity of work, especially when much small money is handled, as happens with butchers, marketmen, and hucksters, also often leads to intemperance.
The lack of occupation exerts a baleful influence. Men-about-town, the frequenters of clubs, dawdlers, and quidnuncs often fall victims to a fate from which occupation and the necessity to work would have saved them. In this connection it may be permitted to call attention to the custom of treating as enormously augmenting the dangers to which such persons are habitually exposed in the matter of alcoholic excesses. The occasional moderate use of alcohol in the form of wine with food and as a source of social pleasure is not fraught with the moral or physical evils attributed to it by many earnest and sincere persons. It is, on the contrary, probable that the well-regulated and temperate use of sound wines under proper circumstances and with food is, in a majority of individuals, attended with benefit. Those who suffer from the effects of excesses do not usually reach them by this route, nor would they be saved by any amount of abstinence on the part of temperate and reasonable members of society.
When we turn our attention to the unfavorable personal conditions which predispose to alcoholism, we at once enter upon the familiar field of work of the practical physician. Numerous influences having their origin in the individual himself, some occasional, others constant, all urgent, demand our careful consideration. Some of the conditions out of which these predisposing influences spring are tangible and easy of recognition; others are elusive and uncertain. To point them out is, unfortunately, not to remedy them. As a rule, they have wrought their evil effects long before the individual has cause to regard himself in the light of a patient.
First in importance is heredity. A peculiar inherited constitution of the nervous system is as influential in leading to alcoholic excess and in aggravating its disastrous effects as any other cause whatsoever. A considerable proportion of individuals who suffer from alcoholism are found upon inquiry to come of parents who have been addicted to drink. A still greater number belong to families in which nervous disorders, and in particular neuralgia, epilepsy, and insanity, have prevailed. Others, again, are the offspring of criminals. It can no longer be doubted that particular causes of nervous degeneration in one or both parents may lead to the hereditary transmission of a feeble nervous organization, which, on the one hand, renders its possessor peculiarly liable to neuroses [p. 577] of every kind, and, on the other hand, an easy prey to the temptation to seek refuge from mental and physical suffering in occasional or habitual narcotic indulgence. Thus, as Anstie pointed out, “the nervous enfeeblement produced in an ancestor by great excesses in drink is reproduced in his various descendants, with the effect of producing insanity in one, epilepsy in another, neuralgia in a third, alcoholic excesses in a fourth, and so on.” When it is possible to obtain fairly complete family histories, covering two or three generations, in grave nervous cases, facts of this kind are elicited with surprising frequency. The part which heredity plays in many of the more inveterate and hopeless cases of alcoholism is wholly out of proportion to the obvious and easily recognizable part played by momentary temptation. To the failure to recognize the real agency at work in such cases must be ascribed the disappointment of too many sanguine and unsuccessful social reformers.
Various forms of disease exert a predisposing influence to alcoholic excesses. In the first place, bodily weakness and inability to cope with the daily tasks imposed by necessity impel great numbers of persons of feeble constitution, especially among the laboring classes, to the abuse of alcohol.
In the second place, many conditions of chronic disease attended by suffering are susceptible of great temporary relief from the taking of alcohol. Especially is this the case in the neuralgias, in phthisis, in dysmenorrhœa and other sexual disorders of women, in the faintness and depression of too-prolonged lactation, in the pains and anxieties of syphilis, and in the malaise of chronic malaria. When the patient has learned that alcohol is capable of affording relief from suffering, it is but a short step through ignorance or recklessness to habitual excess.
The administration of alcohol during convalescence from attacks of illness is not unattended by the danger of subsequent abuse. It is well for the physician to inform himself of the hereditary tendencies and previous habits of the patient before assuming the responsibility of continuing alcohol beyond the period of acute illness under these circumstances; and it is a rule never to be disregarded that the stimulant ordered by the physician is to be regulated by him in amount, and discontinued when the patient passes out of his care.
Irregularities of the sexual functions in both sexes, and especially sexual excesses, strongly predispose to alcoholism. The custom of administering to young women suffering from painful menstruation warming draughts containing gin, brandy, or other alcoholic preparations in excessive amounts is a fertile cause of secret tippling.
The abuse of tobacco, to the depressing effects of which alcohol is a prompt and efficient antidote, must be ranked as an important predisposing influence.
Depressing mental influences of all kinds tend strongly to drinking habits. This is true of persons in all classes of society.
Habit constitutes an influence the importance of which can scarcely be over-estimated. Much of the drinking done by active business-men has no other cause than this. Alcohol, like opium and other narcotics, exerts its most pernicious influence through the periodical craving on the part of the nervous system for the renewal of the stimulating effects which it causes, while it progressively shortens the period and diminishes the [p. 578] effect by its deteriorating action upon the nutrition of the peripheral and central nervous tissues.
B. The Exciting Cause.—Alcohol, or ethyl hydrate, is the product of the fermentation of solutions which contain glucose or a substance capable of transformation into glucose. Other alcohols, as propyl, butyl, and amyl alcohol, etc., are also formed in small quantity in the fermentation of saccharine liquids. Ethyl alcohol is the type of the series, and forms the normal spirituous ingredient of ordinary alcoholic beverages. The others when present, except in minute quantities, constitute impurities. Their toxic effects are much more pronounced than those of ethyl alcohol.
Alcohol is a colorless mobile liquid having an agreeable spirituous odor and a pungent, caustic taste, becoming fainter upon dilution. It mixes with water and ether in all proportions.
Alcoholic beverages form three principal groups: 1, spirits, or distilled liquors; 2, wines, or fermented liquors; and 3, malt liquors.
1. The various spirituous liquors, as whiskey, gin, rum, brandy, etc., contain, in addition to the ethyl alcohol and water common to them all, varying minute proportions of ethereal and oily substances to which each owes its peculiar taste and odor. These substances are œnanthic, acetic, and valerianic ethers, products of the reaction between the corresponding acids and alcohol, and various essential oils. Traces of the other alcohols are also present. Amyl alcohol, the so-called fusel oil, is present in new and coarse spirit, but especially in that derived from potatoes, in considerable amounts. It is to this ingredient that potato spirit owes its peculiarly deleterious properties. Richardson3 experimentally produced with amyl alcohol phenomena analogous to delirium tremens in man. Spirits also frequently contain sugar, caramel, and coloring matters derived from the cask, to which certain products of the still also owe in part their flavor. These liquors are of varying strength, and contain from 45 to 70 per cent. of absolute alcohol by volume.4
3 On Alcohol, Lond., 1875.
4 Vide Baer, Der Alcoholismus, Berlin, 1878.
Liqueurs (anise, kümmel, curaçoa, Benedictine, etc.) are the products of the distillation of alcohol with various aromatic herbs, sweetened, or of its admixture with ethereal oils and sugar. These compounds contain a very high percentage of alcohol. Two of them, absinthe and kirsch, by reason of their peculiarly dangerous properties deserve especial mention.
Absinthe is an alcoholic distillate of anise, coriander, etc. with the leaves and flowers of the Artemisia absinthium, which yields a greenish essence. This liqueur contains from 60 to 72 per cent. of alcohol, and exerts a specific pernicious effect upon the nervous system, largely due to the aromatic principles which it contains.5 Kirsch, which owes its [p. 579] peculiar flavor to the oil of bitter almonds and hydrocyanic acid which it contains in varying and often relatively large proportions, is still more dangerous. The toxic effects produced by these liqueurs are of a very complex kind, and scarcely fall within the scope of this article.
5 As early as 1851, Champouillon (referred to by Husemann, Handbuch der Toxicologie) called attention to the fact that the French soldiers in Algiers, in consequence of excessive indulgence in absinthe, suffered especially from mania and meningitis. Decaisne (La Temperance, 1873, Étude médicale sur les buveurs d'absinthe) found absinthe in equal doses and of the same alcohol concentration to act much more powerfully than ordinary spirits, intoxication being more rapidly induced and the phenomena of chronic alcoholism earlier established. Pupier (Gazette hébdom., 1872) found in those addicted to the use of absinthe marked tendency to emaciation and to cirrhosis of the liver; and Magnan (Archives de Physiol., 1872) asserts that the chronic alcoholism due to this agent is characterized by the frequency and severity of the epileptic seizures which accompany it. There is reason to believe that the consumption of absinthe in the cities of the United States is increasing.
2. Wines are the product of the fermentation of the juice of the grape. Their chemical composition is extremely complex. They owe their general characteristics to constituents developed during fermentation, but their special peculiarities are due to the quality of the grape from which they are produced, the soil and climate in which it is grown, and the method of treatment at the various stages of the wine-making process. So sensitive are the influences that affect the quality of wine that, as is well known, the products of neighboring vineyards in the same region, and of different vintages from the same ground in successive years, very often show wide differences of flavor, delicacy, and strength.
The most important constituent of wine is alcohol. To this agent it owes its stimulating and agreeable effects in small, its narcotic effects in large, amounts. The proportion of alcohol, according to Parkes, Bowditch, Payen, and other investigators, varies from 5 to 20 per cent. by volume, and in some wines even exceeds the latter amount. The process of fermentation, however, yields, at the most, not more than 15 to 17 per cent. of alcohol, and wines that contain any excess of this proportion have been artificially fortified.
Further constituents of wine are sugar, present in widely varying amounts, and always as a mixture of glucose and levulose—inverted sugar; traces of gummy matter, vegetable albumen, coloring matters, free tartaric and malic acid, and various tartrates, chiefly potassium acid tartrate, or cream of tartar. In some wines there are found also traces of fatty matters. Tannin is likewise found. Small quantities of aldehyde and acetic acid are due to the oxidation of alcohol. The acetic acid thus formed further reacts upon the alcohol, forming acetic ether. To the presence of traces of compound ethers, acetic, œnanthic, etc., wines owe their bouquet. Carbon dioxide, produced in the process of fermentation, is retained to some extent in all wines, and is artificially developed in large quantities in champagnes and other sparkling wines.
Much of the stuff sold as wine, even at high prices, in all parts of the world, is simply an artificial admixture of alcohol, sugar, ethereal essences, and water. The wines rich in alcohol are especially liable to imitation.
Wine is the least harmful of alcoholic drinks. In moderate amounts and at proper times its influence upon the organism is favorable. In addition to its transient stimulating properties, it exerts a salutary and lasting influence upon the nutrition of the body. Only after prolonged and extreme abuse, such as is sometimes seen in wine-growing countries, does it lead to alcoholism.
3. Malt liquors—beer, ale, porter, stout, etc.—are fermented beverages made from a wort of germinated barley, and usually rendered slightly aromatic by hops. This process is known as brewing. Malt liquors, of which beer may be taken as the type, contain from 3.75 to 8 per cent. by volume of alcohol, free carbon dioxide, variable quantities of saccharine matters, dextrin, nitrogenized matters, extractive, bitter and coloring matters, essential oil, and various salts. Much importance has [p. 580] been ascribed to the quantity of malt extractive in beer: it has even been seriously spoken of as fluid bread. But, granting the nutritive value of the malt extractives, it is, as compared with the nutritive value of the grain from which they are derived, so small that beer must be regarded as a food of the most expensive kind.
Sound beer is wholesome and nutritious, and serves a useful purpose in the every-day life of a considerable part of the earth's population. But it is wholesome only in moderate amounts. Its excessive consumption results in progressive deterioration of mind and body. Undue accumulation of fat, diminished excretion of urea and carbon dioxide, are followed by disturbances of nutrition. Incomplete oxidation of the products of tissue-waste leads to the abnormal formation of oxalates, urates, etc., to gout, derangements of the liver, and gall-stones. In long-continued excesses in beer one of the effects of the lupulin is to enfeeble the powers of the reproductive organs. The inordinate consumption of beer induces intellectual dulness and bodily inactivity, and lessens the powers of resistance to disease. The dangers of acute and chronic alcoholism are obvious. Five glasses of beer of 5 per cent. alcohol strength contain as much alcohol as half a beer-glassful of spirits of 50 per cent.
The moderate consumption of beer in communities is to some extent a safeguard against alcoholism. To secure this end, however, the beer must be sound and of light quality. The stronger beers, and especially those which are fortified with coarse spirits, besides the direct dangers attending their use, tend rapidly to the formation of spirit-drinking habits.
The action of alcohol varies according to its degree of concentration, the quantity ingested, and its occasional or habitual use. On the one hand, when well diluted, taken in small amount and occasionally only, it may be without permanent effect upon any function or structure of the body; on the other hand, its frequent administration in large doses and but little diluted is, sooner or later, surely followed by widespread tissue-changes of the most serious kind.
The Physiological Action of Alcohol.—Alcohol is very rapidly taken up by absorbent surfaces. According to Doziel,6 it has been detected in the venous and arterial blood and in the lymph of the thoracic duct a minute and a half after its ingestion. It is very slightly if at all absorbed by the unbroken skin. Denuded surfaces and extensive wounds permit its absorption, as in the case of surgical dressings, and instances of intoxication from this cause have been recorded. It is also freely absorbed in the form of vapor by the pulmonary mucous surfaces. Some surfaces, as the pleura and peritoneum, absorb it, as has been demonstrated by the effects following its injection into those cavities. Its constitutional effects are also rapidly developed after hypodermic injection. Under ordinary circumstances, however, it is by the way of the absorbents and veins of the gastric mucous membrane that alcohol finds its way into the blood. It is probable that the greater part of the alcohol taken into the stomach undergoes absorption from that organ, and that very little of it reaches the upper bowel. Alcohol is readily absorbed by the rectal mucous membrane. Having entered the blood, [p. 581] it reaches all the organs of the body, and has been recovered by distillation not only from the blood itself, but also from the brain, lungs, liver, spleen, kidneys, and various secretions.7
6 Pflüger's Archiv für Physiologie, Band viii., 1874.
7 Strauch, De demonstratione Spiritus Vini in corpus ingesti, Dorpati, 1862.
Lentz and other observers believe that certain organs have a special affinity for alcohol. The author named and Schulinus place the brain first in this respect, and in the next rank the muscles, lungs, and kidneys. But Lallemand and Perrin regard the liver and the brain as having an equal affinity for alcohol. The opinion of Baer, who rejects the view that alcohol has an especial predilection for particular organs, is more in accordance with known physiological law. This observer holds that alcohol, having found its way into the blood, circulates uniformly throughout the whole organism, and explains the greater amount recoverable from certain organs as due to the fact that these organs contain more blood than others.
The elimination of alcohol is at first rapid, afterward very gradual. It begins shortly after ingestion, and in the course of two or three hours one quarter, and perhaps much more, of the amount passes from the organism. Nevertheless, after the ingestion of large amounts traces of alcohol were discovered on the fifth day in the urine by Parkes and Wollowicz, although the elimination by the lungs had entirely ceased.
Elimination takes place for the most part by way of the kidneys, the lungs, and the skin; alcohol has been recovered also from the bile, saliva, and the milk.
Whatever may be the affinity of certain organs for alcohol, whatever the channels by which it is eliminated, the general belief is that some portion of it undergoes chemical decomposition within the body. The steps of this process and its ultimate results are as yet unknown; nor, indeed, are the proportional amounts decomposed and eliminated established. Some observers regard the amount eliminated as less than that decomposed. Others suppose that the amount consumed within the body is relatively very small as compared with that disposed of by elimination. It is, however, established that the sojourn of alcohol in the body, unlike that of many other toxic substances, is transient, and that in the course of from twenty-four to forty-eight hours after the ingestion of a moderate amount there remain only traces of this substance.
The local action of alcohol upon organic tissues depends upon its volatility, its avidity for water, its power to precipitate albuminous substances from solution and to dissolve fats, and, finally, upon its antiseptic properties.
Applied externally and permitted to evaporate, it produces a fall of temperature and the sensation of cold; if evaporation be prevented, a sensation of warmth is experienced, the skin reddens, and, if the action be prolonged, desquamation results. The sensation produced when diluted alcohol is applied to mucous surfaces is burning and stinging; when concentrated, it may excite inflammation.
Dilute alcohol has been much employed as a surgical dressing for wounds and ulcerated surfaces. Its value for this purpose depends on its stimulating properties, by virtue of which it exerts a favorable influence upon granulating surfaces; and on its antiseptic qualities, which are, however, much inferior to those of salicylic and carbolic acids among organic substances and to the chlorides among the inorganic salts.
[p. 582]The direct action of alcohol upon the mucosa of the digestive system depends upon the quantity ingested and degree of concentration. In moderate amounts and diluted to the extent of 50 per cent. or more, it produces a sensation of warmth in the tissues over which it passes. This sensation is due in part to the impression upon the nerve-endings, and in part to reflex hyperæmia, which is at once excited. In individuals unaccustomed to its use reflex contractions of the constrictor muscles of the pharynx, with gagging, are sometimes provoked. The secretion of saliva and of the gastric juice is increased, diluted alcohol being, in respect to its physiological effect in stimulating the buccal and gastric mucous glands, inferior to no other agent. This action is due as much to reflex as to local action, as has been shown experimentally by the application of a few drops of alcohol to the tongue of a dog with gastric fistula, increased secretion of gastric juice immediately resulting.
It is in consequence of this action that moderate doses of diluted alcohol exert a favorable influence upon the appetite and digestion. Increased amounts of food are well borne; fats especially are more tolerable and better digested; and a more energetic peristalsis favors the absorption of the food solutions. In those habituated to the use of alcohol these effects do not always follow; and if the amount be increased or the repetition become frequent, some part of the alcohol undergoes in the stomach, with the food, acid fermentation, and acid eructations or vomitings occur. With these phenomena is associated gastro-hepatic catarrh with its characteristic symptoms—loss of appetite, feeble digestion, diarrhœa alternating with constipation, sallowness, mental depression, and headache. In still greater amounts and little diluted, alcohol is capable of exciting acute gastritis or congestion and catarrhal inflammation of the liver.
When we come to study the action of alcohol upon the circulatory system, we find that in small doses it has little or no influence either upon the action of the heart or the condition of the vessels. In augmented amounts it increases the action of the heart both in force and frequency, and the arterial blood-pressure. After large doses these effects quickly pass away, and the circulation becomes depressed. The heart's action grows feebler, often slower, the pulse weaker; blood-pressure sinks and arterial tension is diminished. Its physiological action is that of a direct stimulant to the heart and the pneumogastric nerve; its toxic action, that of a depressant. Upon the vaso-motor system the action is from the first that of a depressant. Dilatation of capillary vessels and increased afflux of blood manifest themselves in the flushed face, brilliant eyes, and warmth of surface which are familiar phenomena. Frequent repetition tends to permanently impair the activity of the peripheral circulation. Hence the visible vascular twigs and rubicund nose that characterize the physiognomy of the habitual drinker.
This congestion no less affects the internal organs, setting up, by interference with their functions, chronic derangements of nutritive processes on the one hand, and on the other the liability to acute local diseases and complications.
The reactions which take place between the blood and alcohol remain, notwithstanding the energy devoted to their investigation, among the unsolved problems of physiological chemistry. It were a profitless task to here review the researches into this subject or to set forth their [p. 583] conflicting results. It may be stated that conclusions based upon the reactions between blood drawn from the vessels and tested with alcohol in the laboratory are wholly inapplicable to the inquiry. While it is generally conceded that some part of the alcohol ingested undergoes decomposition within the organism, what the steps of the process are and what the products are have not yet been demonstrated. Rossbach and Nothnagel8 state that it has not yet been possible to detect in the organism the products of the oxidation of alcohol—namely, aldehyde, acetic acid, and oxalic acid; nevertheless, acetic acid formed in the economy by the general combustion of alcohol may form acetates, which, undergoing decomposition, are transformed into carbonates and water, and are eliminated as such in the urine.9 This view is also held by Parkes.10
8 Cited by Peeters, L'Alcool, physiologie, pathologie, médecine légale, 1885.
9 Henri Toffier found in the brain of a man who died of acute poisoning by alcohol not only alcohol, but also aldehyde: Considerations sur l'empoisonment aiqu par Alcohol, Paris, 1880.
10 Journal of Practical Hygiene, 4th ed., Lond., 1873.
According to Peeters, the action of alcohol upon the blood may be summed up as follows: That portion of the ingested alcohol which undergoes decomposition takes from the blood some part of its oxygen for this purpose, with the result of a diminished amount of oxygen and an increase of carbon dioxide, the blood thus being made to resemble venous blood. A part of the oxygen destined for the oxidation of waste products being thus diverted, these substances are not completely transformed. In this respect also blood charged with alcohol resembles venous blood. Alcohol even when diluted is capable of retarding the combustion of oxidizable organic substances, and there is no reason to doubt that this agent has in the blood the same chemical properties that it elsewhere possesses.
The exhalation of some part of the alcohol circulating in the blood by the way of the pulmonary mucous membrane interferes with the elimination of carbon dioxide, with the result that the latter agent further tends to accumulate in the blood.11
11 David Brodie, Medical Temperance Journal, October, 1880.
Alcohol must act, to some degree at least, directly upon the water of the blood and upon its albuminoid principles. The products of the reactions normally taking place within the corpuscles pass with greater difficulty into serum containing alcohol as the current of osmosis tends rather from the serum to the corpuscles. It is in accord with this fact that the corpuscles of alcoholized animals have been found relatively large.
The blood of individuals who have died in a state of alcoholic intoxication has been frequently found to contain an unusual amount of fatty matter in a fine state of subdivision.
Upon the respiration the influence of alcohol is twofold: it modifies the respiratory movements and the results of the respiratory processes. After moderate doses the movements are accelerated without disturbances of rhythm; after large doses the respiratory acts become embarrassed, feeble, irregular, finally wholly diaphragmatic.
Alcohol modifies the results of respiration in a constant manner and in all doses. This modification consists in a decrease in the amount of oxygen absorbed and carbon dioxide exhaled. This effect is usually more marked when alcohol is taken fasting than during digestion.
[p. 584]The influence of alcohol upon the renal secretion is that of a diuretic, but the fact must not be overlooked that this tendency is much increased by the large amount of water which alcoholic drinks necessarily contain. But that alcohol acts as a diuretic, even in small doses and altogether independently of the water with which it is taken, does not admit of doubt. The changes in the urine are qualitative as well as quantitative. The amount of urea, uric acid, and other solids is always notably diminished. The diminution of the amount of phosphoric acid is even greater than that of the nitrogenized substances, especially during the period of excitation.
The diuretic effect of alcohol is dependent upon its direct action on the parenchyma of the kidneys, the qualitative changes in the urine upon its influence on nutrition.
Upon the temperature of the body alcohol has a marked effect. The sensation of warmth experienced after moderate doses is chiefly subjective, and is accompanied by a very slight actual rise in temperature, amounting to some fraction of a degree Fahrenheit, and of but short duration. This rise is followed by a rapid fall, amounting to a degree or more below the norm. This effect is manifested within the course of an hour after the administration, and is of comparatively brief duration, being largely influenced by the condition of the individual at the time as regards mental or physical exercise, digestion, and the like. It is in part due to the increased loss of heat from the surface of the body, favored by more active cutaneous circulation, but chiefly to the action of alcohol in retarding oxidation and the activity of nutritive changes. Toxic doses are followed by marked fall of temperature. The influence of alcohol upon the temperature is more pronounced in febrile conditions than in health.
The influence of physiological doses of alcohol upon the nervous system is, among all its effects, the most marked and the most difficult to describe with exactitude. It is usual to regard this agent as a stimulant and to separate the period of its direct effects into two stages—that of excitement and that of depression. John Hunter defined stimuli as agents which increase some natural action or tendency, in contradistinction to irritants, which produce actions altogether abnormal. Anstie12 sought to restrict the use of the term stimulant to agents which by their direct action tend to rectify some deficient or too redundant natural action or tendency. Without entering upon the discussion of the doctrine of stimulation, I may say that the views of Anstie have served a useful purpose in making clear some vexed questions. In accordance with these views, the physiological action of alcohol is followed neither by excitement nor by depression, and when its administration is followed by these conditions, its action is not truly physiological, but narcotic or toxic.
12 Stimulants and Narcotics, Lond., 1864.
The effects of this agent upon the nervous system vary within very wide limits according to innumerable conditions which relate to the temperament, health, habits, occupation of the individual, season, climate, social circumstances, and the quantity, kind of alcoholic drink, and its mode of administration. Its first action in moderate doses and under circumstances free from complications is to increase the functional [p. 585] activity of the brain: the ideas flow more easily, the senses are more acute, speech is fluent, and movement active. These effects accompany the increase in the heart's action, the slight rise in temperature already described, and increased activity of the organism in general. They appear to be in part due to the direct action of the substance upon the cerebrum, and in part to increased activity of the circulation. The effect upon the nervous system has been compared by Nothnagel to the effect, in a higher sphere, of strong moral impulses. Without otherwise modifying existing traits of character, such impulses call them into action, and lead to the accomplishment of deeds quite impossible under ordinary circumstances. To a man worn out by some prolonged task which from sheer fatigue he despairs of finishing, let there be announced some joyful news; he at once feels refreshed, applies himself with renewed energy to his work, and perhaps finishes it with ease. In kind at least this is the effect also of alcohol.
But the limits of the physiological effects are easily transcended, and the manifestations then become those of its toxic influence, between the slightest grades of which and drunkenness the difference is one rather of degree than of kind. These effects must therefore be described under the heading Acute Alcoholism.
Passing to the influence of alcohol upon nutrition, we recognize two modes of action. Of these the first is direct and in part local, and results from the stimulation of the glandular apparatus of the mucous membrane of the mouth and stomach, from increased activity of the circulation, and from direct stimulation of the pneumogastric nerve. Hence increased secretion of the digestive juices, augmented appetite, more active peristalsis, and improved digestion, to which, indeed, the direct action of alcohol upon the cerebrum doubtless contributes. It is to these effects that the favorable influences of this agent in the extremes of life, when it is so well borne and so useful, must be largely attributed.
The second mode of action is indirect and general. It has been shown that alcohol diminishes the amount of carbon dioxide expired and of oxygen inspired, that it diminishes the quantity of urea excreted, and that it lowers the temperature of the body. It follows that normal oxidation goes on more slowly—that there is diminished tissue-change. Alcohol supports the body, not by nourishing it as a food, but by curtailing waste; it favors nutrition, not by augmenting the receipts, but by cutting down the expenses of the organism. But nutrition and waste are in health correlated and complementary. They are, in fact, essential and associated processes of life, of which one is not more necessary than the other to the maintenance of health. In various pathological states the arrest of waste is a cardinal indication, and for this purpose alcohol holds the first place. But in health this action itself is pathological, and the beginning of evil. The fat accumulation of the drunkard is due in part to the sugar and starchy matter taken in malt liquors, but much more to this control of waste, as is shown by the fact that spirit-drinkers who have sufficient food also often become fat. Alcoholic excesses tend not only to fat accumulation, but also to fatty degeneration of the tissues. The opinion that alcohol in any dose or under any circumstances is a food in the ordinary acceptation of the term is no [p. 586] longer tenable. Chauffard has well said: “Not only is alcohol not an aliment; it is the very reverse. Not only does it not contribute to the nutrition of the body; it opposes it and destroys it little by little.”13
13 This opinion is at variance with the views generally entertained by English and American writers upon materia medica. T. Lauder Brunton (Textbook of Pharmacology, Therapeutics, and Materia Medica, Am. ed., 1885) regards “all the evidence as pointing to the fact that alcohol is a food, and in certain circumstances, such as febrile conditions, may be a very useful food; but in health, when other kinds of food are abundant, it is unnecessary, and, as it interferes with oxidation, it is an inconvenient form of food.”
In accordance with the classification laid down at the beginning of this article, the term acute alcoholism is here used to denote the various forms of primary alcoholic intoxication in contradistinction to the conditions which are brought about by the gradual but long-continued action of the poison, and to the violent and sometimes abrupt outbreaks which are secondary to these conditions. From this point of view, which is at variance with the established usage of writers upon alcoholism, but which is here adopted in the hope that it will tend to simplify the treatment of a subject at present in much confusion, acute alcoholism includes all forms of drunkenness, from mere transient derangement of the normal functions of life, scarcely amounting to tipsiness, to profound intoxication. It includes also poisoning by lethal doses. Chronic alcoholism may be the outcome of frequent repetitions of acute alcoholism at short intervals, or it may result from the constant abuse of alcohol in doses so small that the evidences of its poisonous effects are at no time actively manifested. I hope to be able to show that the seemingly acute outbreaks, the symptoms of which chiefly relate to the nervous system, that occur after the condition of chronic alcoholism is fully established, are commonly preceded for a longer or shorter period by imperfectly developed symptoms of an analogous character, and that these outbreaks differ in essential particulars from acute alcoholism in all its forms.
That persons suffering from some degree of chronic alcoholism may, and as a matter of common occurrence do, after excessive doses suffer from acute alcoholism—in other words, get drunk—is too obvious to demand more than passing consideration at this point; but it is scarcely necessary to point out to those who are familiar with the life-history of such individuals that the time comes when no degree of excess will produce the ordinary manifestations of transient intoxication. It is then that phenomena of another and more serious kind are apt to occur. The difference is that between the reactions of normal or as yet quasi-normal tissues and alcohol on the one hand, and on the other the manifestations induced by the supersaturation of tissues previously alcoholized to the point of an acquired tolerance. This tolerance of the nervous system is in a high degree a pathological condition, and is therefore in an equally high degree [p. 587] unstable and liable to be overthrown by accidents of various kinds as well as by extraordinary excess in alcohol.
The variety of forms and admixtures in which alcohol is taken is so great, and the susceptibility of individuals to its action so different, that it would be a hopeless task to attempt to describe the manifold phases of acute alcoholism. Unfortunately, most of them are too familiar. The following description embraces the more important phenomena, and is intended to serve as a type:
A. THE ORDINARY OR TYPICAL FORM.—The physiological effects of alcohol in moderate doses are followed by no reaction, but they are evanescent. When, however, the dose is repeated at short intervals and the effect is sustained, the condition by its continuance becomes pathological, and the subject enters upon the prodromic period of acute alcoholism. From this condition to that in which the poison manifests its distinctly toxic effects the transition is a speedy one. The face becomes flushed, the eyes brilliant; the heart's action increases in force and frequency; muscular force seems augmented; there is excitation of the mental processes; intelligence seems more active; ideas flow readily; preoccupation ceases; anxieties are forgotten. The future is full of hope, the past has lost its sorrows, its regrets. The powers of expression are brought into fullest play; conversation becomes animated, brilliant, often sparkling and keen. Reason is thrown aside, the judgment relaxed; vanity, pride, rashness, assert themselves. Emotions, sentiments, habitually repressed, are manifested without reserve, often with emphasis and insistance. Hence the proverb, In vino veritas.
Then speech degenerates into loquacity; improper confidences are made, indiscretions committed; the bent of disposition is made clear; he who is by nature sad grows sombre, melancholy; he who is irritable becomes cross and quarrelsome; the generous man grows lavish, and a good-natured fellow is everybody's friend. But this intensification of normal characteristics is by no means invariable. Not seldom do we see the timid man become in his cups violent and aggressive, the refined coarse, and the gay melancholy. The sensation of increase in muscular force manifests itself in unusual activity. Gesticulation is frequent, energetic, and apt; there are bodily restlessness and desire to move about. Shouts of laughter, bursts of song, are followed by a disposition to easily-provoked quarrels. At this stage there are evidences of some degree of cerebral congestion. The temples throb, the heart is full, and dizziness is felt. The skin is moist, the mouth pasty, thirst is experienced, and there is frequent desire to pass water. There yet remains some degree of self-control. The phenomena which characterize this condition are more or less transient, and if alcohol be now discontinued they speedily cease, commonly in sleep, sometimes without it, and are followed by sensations of weariness and fatigue, with headache, gastric disturbances, and temporary loss of appetite.
If, however, the influence of alcohol be pushed beyond this point, the manifestations of mere exaltation of function give place to grave perversion of the processes of life. A gradually increasing vertigo is associated with obscured intelligence, dulled imagination, blunted and confuted perception, disjointed ideation, and incoherent speech. The recollection grows indistinct, the will purposeless. Now the baser [p. 588] passions are aroused; evil impulses and illusions of all kinds sway the drunken man. All control of conversation and action is lost. Reason is replaced by delirium, and he becomes a maniac, dangerous alike to himself and to others, liable upon some sudden impulse to commit the most atrocious crimes.
The countenance betrays the profound disturbance of the intellectual and moral nature: its expression is changed, its lines are blurred; the flush deepens, the veins are distended, the arteries pulsate visibly, the gaze is staring, the pupils contracted. The respiration, at first quickened, becomes irregular. The heart's action is rapid and bounding, and sometimes there is palpitation. Somnolence soon deepens into an invincible desire to sleep. At this point great muscular relaxation not infrequently occurs in connection with vomiting, profuse sweating, and dilatation of the pupils.
Muscular movements are irregular and uncertain, the gait vacillating and staggering; the movements of the superior extremities, wanting in precision, become trembling and awkward. At the same time speech becomes embarrassed. Articulation is difficult and imperfectly executed. At length standing becomes impossible; the drunkard, profoundly poisoned, sinks helplessly to the ground, and not infrequently the control of the sphincters is lost. The development of this condition is accompanied by a gradual perversion of general and special sensibility. Dull headache, ringing in the ears, phosphenes, and other disturbances of vision, hallucinations of taste and smell, are followed by abrogation of the special senses. Loss of cutaneous sensibility, beginning at the extremities, invades the whole body, and finally the subject sinks into more or less profound coma, from which it is no longer possible to arouse him. Muscular resolution is complete, sensation is lost; the face is now bloated, deeply flushed, sometimes livid, sometimes ashy pale; the pupils are dilated; the temperature below normal; the respiration stertorous and accompanied by abundant mucous râles. The pulse is feeble, fluttering, the surface covered with sweat, and involuntary evacuations take place.
VARIETIES.—Three varieties of acute alcoholism are recognized by Lentz—the expansive, the depressive, and the stupid. The first is characterized by gayety, self-satisfaction, and content. The drunkard, smiling and happy, is satisfied with the present and full of hope for the future. The second variety is characterized by sadness and melancholy. The drunkard becomes sombre and taciturn; if he talk at all, it is to bewail his misfortunes and to recount his mishaps. In the third variety the period of excitement is wanting and the drunkard passes rapidly into a condition of stupor.
Great as are the modifications of the course of acute alcoholism under different circumstances and in different individuals, it is evident, upon close investigation, that its phenomena—and especially those which relate to the nervous system—manifest themselves in a progressive series more or less constant in the majority of persons. This series includes three well-characterized periods: 1. The stage of functional exaltation of the nervous system; 2. The stage of functional perversion; 3. The stage of depression.
We may, then, recognize the degrees of acute alcoholism corresponding [p. 589] to these stages.14 Of these, the first scarcely goes beyond the stage of excitement already described, and if the dose have been moderate or its repetitions not too long continued, the symptoms gradually subside, leaving perhaps no sequels beyond slight headache, tinnitus aurium, some degree of muscular relaxation, and mental depression.
14 These stages correspond to the three degrees of alcoholic intoxication recognized and described by German writers as Rausch, Betrunkenheit, and Besoffenheit. To these may be added the prodromic period, designated as Weinwarme Zustand. These three degrees are known to the French as l'ivresse légère, l'ivresse grave, and l'ivresse suraiguë.
The second degree is characterized by partial abolition of intelligence, of general and special sensation, and of motor power. Hence incoherent speech, extravagant actions, blunted perceptions, hallucinations and delusions, inco-ordination of movements, a reeling gait, and not rarely vomiting and involuntary discharges of urine and feces. This degree of acute alcoholism usually ends in deep sleep with abundant perspiration, to which succeed great lassitude and depression, accompanied by much gastro-intestinal derangement, of which the symptoms are inability to take food, coated tongue, viscid mouth, foul breath, repeated vomiting, and occasionally diarrhœa. These sequels are less serious in those individuals accustomed to excesses than in others.
In the third degree the subject falls by gradual stages or abruptly into more or less profound coma. The abolition of intelligence, sensation, and motion is complete. The face is now swollen, livid, or pale, the pupils dilated, the respiration stertorous, the pulse feeble, often slow, sometimes imperceptible, the surface cool and often bathed in sweat. The man is dead drunk. The symptoms are now of the gravest kind. It is no uncommon occurrence for this condition to end in death.
Well characterized as these three degrees of alcoholic intoxication are, they are not, when occurring successively in the same individual, separated by abrupt lines of demarcation. On the contrary, the evolution of the symptoms is from the beginning to the close a gradual and progressive one.
While the scope of this article precludes extended discussion of the symptoms of acute alcoholism—which, indeed, present an almost endless variety in their intensity and combination—yet it seems necessary to the elucidation of the subject to point out some of the more prominent modifications due to variations in the conditions under which alcohol acts upon the organism.
First among these are differences in the nature and composition of the drink. Here we have to do not only with the well-known differences in alcoholic beverages, as spirits, wines, and malt liquors, and their quality and grades, but also with differences in the chemical nature of the alcohols themselves which enter into their composition. The principal of these alcohols are—
| Methyl alcohol, | CH3OH. |
| Ethyl alcohol, | C2H5OH. |
| Propyl alcohol, | C3H7OH. |
| Butyl alcohol, | C4H9OH. |
| Amyl alcohol, | C5H11OH. |
Richardson was the first to call attention to the differences in the physiological and pathological action of the members of this series. Other [p. 590] observers, among whom may be named Dujardin-Beaumetz and Andigie,15 and Rabuteau,16 have also investigated the subject. The researches of these observers have established the fact that the effects of the different alcohols in depressing the temperature of the body and in paralyzing sensation and motion are exactly the same, but that their narcotic influence upon the nervous system increases, dose for dose, in proportion to the amount of carbon which they contain. Ethyl alcohol is, with the exception of methyl alcohol or wood-spirit, the least rich in carbon and the least dangerous to health.17 The increased consumption of alcohol, both as a beverage and in the arts, the demand for cheap, coarse spirits producing their primary narcotic effects with promptness, and the cupidity of manufacturers, have led to the almost universal adulteration of the liquors of commerce with the more dangerous alcohols.18 So extensive has this substitution of the high-carbon alcohols for ethyl or ordinary spirit of wine become that it has been suggested that alcoholism should be divided into ethylism, amylism, propylism, and butylism—not so much for clinical reasons as to direct attention to the composition of alcoholic drinks and to their deleterious properties.19
15 Recherches expérimentales sur la Puissance toxique des Alcools, Paris, 1879.
16 “Contributions à l'Étude des Effets physiologiques et therapeutiques d'Alcool,” Compt. rend. Société de Biologie, 1870-71.
17 “Methylic alcohol is the safest of the series of bodies to which it belongs” (B. W. Richardson, Lectures on Alcohol).
18 M. Girard, chief of the municipal laboratory in Paris, has recently called attention to the enormous diminution in the production of alcohol by the natural method—that is to say, by the distillation of wine. The falling off he ascribes to the ravages of the phylloxera. This loss is made up by the substitution of spirits obtained by the distillation of various fermented grains, potatoes, beets, molasses, etc. To give some idea of the extent to which the alcohols of industry at present replace the alcohols of wine, he cites the following figures: From 1840 to 1850 the mean annual production of alcohol in France was 891,500 hectoliters, of which the alcohols of wine amounted to 715,000 hectoliters. In 1883 the product reached 1,997,280 hectoliters, of which alcohols obtained by the distillation of wine amounted to only 14,678 hectoliters.
19 Peeters, L'Alcool, 1885.
The effects of propyl, butyl, and amyl alcohols upon the nervous system are not only more marked than those of ethyl alcohol, but they are more rapid. The stage of excitement is speedily induced, and its manifestations are intense. Hence the preference often manifested by drunkards for cheap, coarse spirits. On the other hand, the stage of depression quickly follows, and is itself of relatively shorter duration than that induced by ethyl alcohol, probably for the reason that the amount required to bring it about is smaller. Muscular resolution soon becomes general and complete; insensibility speedily succeeds; the fall of temperature is rapid; vomiting, occasionally absent in the intoxication produced by ethyl alcohol, is the rule, and is frequently repeated. Muscular tremor—and especially is this true of amyl alcohol—comes on earlier, is more general and more marked, and lasts longer than that which occurs in consequence of excess in ethyl alcohol. Richardson states that the complex alcohols are more slowly eliminated than ethyl alcohol, but the French observers are of a different opinion.
But these differences in action are probably rather differences in degree than in kind. Peeters says: “Ethyl alcohol is less dangerous than the more complex members of the series. It is less irritating, less charged with carbon, its specific gravity is less, its fumes are less dense and escape [p. 591] more readily from the economy; its action ought to be less profound, less prolonged, than that of butyl, propyl, and amyl alcohol, but it is of the same nature. It is not qualitatively but quantitatively different. I suspect that the effects of liquors containing ethyl alcohol are, as a rule, less decidedly injurious, by reason of the more favorable surroundings of those who can afford to use them.”
The three principal groups of the alcoholic drinks of commerce produce, independently of the properties of the different kinds of alcohol which they contain, forms of acute alcoholism which differ in important respects.
The intoxication induced by the exclusive use of malt liquors is dull and heavy, slow in coming on, and of long duration. The stage of excitement is relatively brief, not often characterized by gayety, often brutal; drowsiness soon supervenes and deepens slowly into unconsciousness. The after-effects are disagreeable and prolonged. The enormous quantity of fluid and the large amount of malt extractives cause gastro-hepatic derangements of a more or less distressing kind. To the hops must be ascribed the prolonged dulness which is so characteristic of the after-effects of beers and ales. The influence of the various substances used in the adulteration of beers without doubt modifies the symptoms of the alcoholism which these beverages cause when impure. These substances consist of glucose, various vegetable bitters, and salt—articles not necessarily hurtful in small amounts, but capable of exerting deleterious action when taken in excess and in connection with the normal ingredients of beer.
The intoxication produced by pure wines is, as a rule, characterized by a bodily and mental activity strongly in contrast with the drunkenness produced by malt liquors. The drunkard is usually gay and vivacious—at all events, lightly merry or not hopelessly despondent. His mood is variable, changing from grave to gay. The first stage is prolonged, and the manifestations of the later stages less grave, nor are the sequels apt to be so severe. The action is that of ethyl alcohol and certain ethereal substances, the latter being present, however, only in minute amounts. The rapidity of the effects depends upon the proportion of alcohol which the wine contains, which varies from about 7 per cent. in the clarets to 15, to 18, or even to 20 per cent. in port and madeira. The sparkling wines, moselle and champagne, produce more transient effects than the still wines—a fact probably to be explained by their greater and more prompt diuretic action.
The foregoing remarks apply only to pure wines. The intoxication which follows the use of artificial compounds sold in all parts of the world as wines betrays in its course and symptoms the high percentage and toxic characters of the mixed alcohols which form their essential ingredients.
The intoxication which follows excesses in the various spirits of commerce presents no special characters. Its symptoms are determined to a considerable extent by the relative purity—that is, freedom from admixture with the various complex alcohols—of the liquor by which it has been produced. Potato spirit causes drunkenness which is profound, overwhelming, and preceded by a brief period only of excitement.
Even more important than the kind of liquor is its quantity. Here, [p. 592] however, it is impossible to formulate precise statements. A few glasses of wine will produce effects in some persons more decided than much strong spirits in others. Those conditions which favor the absorption of alcohol hasten the production and augment the intensity of alcoholism; and the contrary is true. Thus, alcohol taken while fasting does much more harm than the same amount taken with a meal. Intense excitement, anger, mortification, or other violent emotion is said by Lentz to increase the effects of alcohol. Sudden transition from a warm to a cold atmosphere intensifies the action. That this effect of cold is due to suppression of perspiration, and the consequent interference with one of the elements of elimination, is much less likely than that it is due to the further depressing influence of cold upon the nervous system, already depressed by the alcohol imbibed. Occupation has in an indirect way much to do with the facility with which alcohol is borne. Hard work, requiring great and continuous muscular effort, especially in the open air, diminishes the liability to acute alcoholism, while sedentary occupations and confinement strongly predispose to it. These well-recognized facts are to be accounted for by the influence of different occupations and modes of life upon the elimination of the poison. Persons who are debilitated by chronic disease or are convalescent from acute maladies, and the otherwise feeble and anæmic, are peculiarly obnoxious to the action of alcohol. Previous custom and hereditary peculiarities of organization exert an influence upon the liability of individuals to acute alcoholism, and upon its nature when induced.
Persons of an impressible nervous organization are peculiarly prone to the evil effects of drink. With such persons slight excess is often followed by serious consequences; the intellectual disturbance is early developed and out of proportion to the derangements of motility and sensation. The effects of alcohol are manifested more promptly and more intensely in children and women than in men or in the aged. Drunkenness is induced more rapidly and with smaller quantities of alcohol in summer than in winter, in warm than in cold countries.
B. IRREGULAR FORMS OF ACUTE ALCOHOLISM.20—1. The Maniacal Form.—The outbreak is usually sudden, sometimes occurring after the ingestion of comparatively small quantities of alcohol; at others after excesses which in a certain proportion of the cases have already ceased. The transition from a condition apparently normal, or marked at most by mental concentration, restlessness, and some degree of irritability, to furious mania is sometimes almost instantaneous, and the subsidence of the latter no less swift. More commonly there are prodromic symptoms, among which are general malaise, præcordial distress, palpitations, flushing of the face, vertigo, tinnitus aurium, phosphenes, and dull, throbbing headache. The attack is characterized by maniacal excitement, usually of a furious kind. The restlessness is, however, far from being aimless and purposeless. On the contrary, impelled by the wildest passions, transported with rage, the patient seeks the destruction of life and property, and wreaks his fury alike upon animate and inanimate objects. So great is his strength for the time being that several strong men may be scarcely able to restrain him. He pours forth a torrent of commingled threats and curses, in which may be heard unintelligible, and often [p. 593] inarticulate, sounds. He is beside himself, yet, so far as can be learned, there are neither hallucinations nor delusions by which his fury can be explained. In this respect the condition is wholly unlike that form of alcoholic mania in which the actions are explained by the imaginary surroundings and circumstances of the patient. In the maniacal form of acute alcoholism the most trifling incident, a word, a look, are sufficient to produce a tempest of rage that may end in scenes of violence. Nevertheless, the patient yet retains for a time some notion of his surroundings. At length, however, he falls into a state of complete unconsciousness, and the delirium is like that of fever, of the delusions of which no recollection afterward remains. This form of acute alcoholism is almost invariably associated with the symptoms of a high degree of cerebral hyperæmia. The hands are hot, the eyes injected, the pupils dilated or contracted, the expression eager. There are abundant secretion of saliva, frequent and irregular respiration, a rapid pulse—often exceeding 100—throbbing arteries, distended veins, and a hot skin, often bathed with sweat. The urine is scanty and constipation usual. There is, as a rule, increased sensibility to light and sound. The attack is liable to come to a tragic close in murder or suicide.
20 Ivresses anormales ou pathologiques of the French writers.
The termination of the paroxysm is as abrupt as its onset. Some abatement of its violence is quickly followed by signs of mental and bodily exhaustion; this deepens into profound sleep, which often lasts from twelve to twenty-four hours, and from which the patient awakes clear, tranquil, and as if nothing had happened, or dimly recollecting the occurrences that have passed as a hideous dream. In a small proportion of the cases the sleep deepens into coma which ends in death.
2. The Convulsive Form.—The analogy to the form just described is very close. Here, however, the morbid manifestations directly relate to the muscular system. The attack is commonly sudden, often abrupt. When prodromes occur, they are such as have been described as preceding the maniacal form—mental irritability, headache, præcordial distress, etc. The attack is thus described by Lentz: “The phenomena consist not in ordinary convulsions, but in convulsiform movements of remarkable disorder, only to be compared with the extraordinary convulsive movements of grave hysteria. We have happened to see several cases during the attack. These patients threw themselves to the ground, giving themselves up to the most irregular and disorderly contortions, rolling from side to side, throwing the body into the air, striking out with the legs and arms, kicking at random, biting at persons and things—now knocking the head against the floor, again rising for a moment, only to fall back and commence again the same contortions. Their movements are energetic and violent. There are madmen whom it is dangerous to approach by reason of the violence of their movements, but they are certainly much less dangerous than those suffering from the maniacal form of acute alcoholism, for their morbid motility has no tendency to take the shape of co-ordinated actions. It is movement wasted in pure loss. Their muscular energy is excessive; it is difficult to restrain them. To resume: the peculiarity of these movements is this, that they are not intentional, but that they are rather purely convulsiform, automatic.
“Another phenomenon of this form, one of its characteristic symptoms, is the state of intellectual enfeeblement which accompanies it. The loss [p. 594] of consciousness is complete, and were it not for the movement produced by the convulsions the patient would be plunged into a condition of profound coma. He has not the least knowledge of himself; not even delirium denotes intellectual activity; only an occasional harsh cry or inarticulate sound indicates the existence of mind.”
The other symptoms differ but little from the maniacal form. The duration of the attack varies from a few hours to half a day; its termination is usually abrupt, the patient falling into a condition of extreme exhaustion with stupor, or into a deep and prolonged sleep, from which he awakens without the slightest recollection of the attack through which he has passed.21
21 Consult also Dict. des Sciences méd., t. xxvi.
3. Acute Alcoholism, in Persons of Unsound Mind.—The insane, imbeciles, epileptics, and persons suffering from nervous diseases are, as a rule, abnormally susceptible to the action of alcohol, and present more or less striking peculiarities in the symptoms which it causes. Brief notice of certain of these peculiarities is in accordance with the scope and plan of this article.
In general paralysis propensity to alcoholic excesses is not rarely an early symptom. The subject is very susceptible to the action of alcohol, and under its influence rapidly passes into a state of intense excitement, characterized by incoherence, delirium, excessive restlessness, and unwillingness to seek repose until exhaustion is complete. It is under the influence of this easily-provoked alcoholic excitement that the vagabondage, quarrels, thefts, robberies, incendiarisms, and other grave crimes observed during the first stage of this form of insanity are often committed.
Imbeciles and idiots are likewise quickly, and often intensely, excited by alcohol. They are then apt to be quarrelsome, perverse, and ungovernable, defiant of authority, and capable of shocking crimes, often evincing latent vicious tendencies previously wholly unsuspected.
Epileptics are easily affected by alcohol, and usually violent in the stage of excitement; not rarely this period terminates in a true epileptic seizure.
The drunkenness of the dipsomaniac is characterized by a prolonged, uninterrupted stage of excitement without the stage of depression. Such individuals are capable of consuming in their periodical excesses large amounts of drink without the evolution of the ordinary successive phenomena of acute alcoholism.
Persons of unsound mind are, as a rule, so susceptible to the influence of alcohol, and suffer so promptly and intensely from its primary effects, that they are rarely able or permitted to consume a sufficient quantity to bring about a comatose state.
The irregular forms of acute alcoholism are only to be explained by the inherited or acquired constitutional peculiarities of individuals. To attempt to explain them in any case by the quality of the alcohol by which they are induced meets with the difficulty indicated in the fact that they are isolated and comparatively rare, even where the coarser spirits are habitually consumed. They occur in individuals who habitually commit excesses, but they cannot be viewed as manifestations of chronic alcoholism, for the reason that they also occasionally occur in those who are [p. 595] not habitual drinkers, and even in persons who have not for a long time previously tasted strong drink. Furthermore, as has been pointed out, they are not only occasionally, but indeed even as a rule, induced by relatively small amounts of alcohol. They are then the manifestations of idiosyncrasy. One of the striking peculiarities of this peculiar bodily organization is this very susceptibility to the action of alcohol in doses smaller than are taken with impunity by ordinary individuals. It is also characterized by a special tendency to delirium in febrile states, to hallucinations, to disturbances from trifling changes in climate, food, or manner of life, to irritability of the nervous system, and in particular of the vaso-motor system, and by a tendency to convulsions. With these tendencies is associated an unstable mental and moral character. Such persons are liable to headaches, vertigo, and epistaxis—signs of cerebral hyperæmia, which is easily induced—and their family histories indicate strong hereditary tendencies to neurotic disorders, and not rarely addiction to alcohol on the part of one or several ancestors.
But this idiosyncrasy is by no means always an inherited one. It is acquired as one of the results of profound disturbance of the nervous system, such as is produced by moral causes, by temporary or recurrent insanity, by wounds and injuries of the head, by the infectious diseases, especially syphilis, enteric and typhus fever, and small-pox, and by inflammations of the meninges.
What may be the precise mode of action of alcohol in the production of its acute effects yet remains a matter of conjecture. It cannot be doubted that its primary and direct action is upon the nervous system, and that the circulation is secondarily but rapidly implicated. But it is quite impossible to say, in the present state of knowledge, what this action is. It has been suggested that certain chemical modifications of alcohol in the blood, or of the blood itself in the presence of alcohol, cause these phenomena; that aldehyde is the active agent in their production; that the chemical changes by which alcohol is transformed into aldehydes, acetic acid, and finally into carbon dioxide, deprive the blood of the oxygen necessary for the proper performance of the functions of the nervous system. Unfortunately for these views, neither the presence of aldehydes in the blood in acute alcoholism, nor these transformations themselves, have yet been demonstrated, and a high degree of deoxygenation of the blood is frequently observed in asphyxia, the inhalation of nitrous oxide, etc., without the train of symptoms characteristic of the condition now under consideration.
It is more than probable that varying conditions of the cerebral circulation, secondary in themselves, have much to do in the causation of certain symptoms. The experimental investigations of Bernard and others have established the fact that during the period of excitement there is actual congestion of the meninges. This condition is transient, and reproduced after each repetition of the dose. After a time, or if the dose at first be excessive, the congestion is succeeded by anæmia.
PATHOLOGICAL ANATOMY.—Upon the examination of the bodies of persons who have died by accident while drunk or in consequence of drunkenness itself, deep congestion of the cerebral meninges, and especially of the pia, has been almost constantly observed. In the pia effusions of blood are occasionally encountered. The condition of the cerebral [p. 596] substance is not always the same. It is in a majority of the cases more or less deeply congested, yet it presents in other instances no appreciable departure from the normal state, and in a smaller number still there is actual anæmia.
The sinuses and choroid plexuses are distended with dark blood; the cerebro-spinal fluid is increased, and often tinged with blood; the ventricles are distended with fluid, which not rarely has an alcoholic odor. Occasionally the ventricles contain blood, and hemorrhage into the substance of the brain has been observed.
The condition of the elementary nervous tissues after death from acute alcoholism is not yet known.
The lungs are deeply congested, with small extravasations of blood into their substance, and often œdematous. Congestion of the liver, spleen, and kidneys in varying degrees of intensity is also seen. The pancreas is usually deeply injected, occasionally the seat of large extravasations of blood. The mucous membrane of the stomach is invariably deeply injected when the alcohol has been introduced into the organism in the ordinary manner. The observation of Caspar that post-mortem decomposition takes place with diminished rapidity has been denied by Lancereaux and others.
Other post-mortem conditions appear to be neither constant nor characteristic. The stomach usually contains partially digested food and alcohol. Lallemand, Perrin, and Du Roy observed, both during life and after death, in the blood of animals subjected to experiments, great numbers of minute glistening points, which upon microscopic examination proved to be fat-globules. The same condition has been observed in man, not only when death has taken place owing to acute alcoholism, but also when it has occurred during the digestion of a hearty meal without alcohol. The blood itself is often fluid and dark-colored; the heart sometimes empty, sometimes containing a few soft clots. Tardieu22 states that in sudden death during drunkenness pulmonary apoplexy and meningeal apoplexy, if not constant lesions, are at least extremely frequent, and almost characteristic. Baer, on the other hand, denies the occurrence of specific or characteristic lesions.
22 “Observationes médicales sur l'Etát d'Ivresse,” Annales d'Hygiene publique et de Médecine légale, tome xl.
C. ACUTE POISONING BY ALCOHOL IN LETHAL DOSES.—The symptoms are much modified when overwhelming doses of strong alcohol are introduced into the organism at once or in the course of a short time. Here alcohol produces death as an acute poison. The cases may be arranged in two groups:
1. Corrosive Poisoning.—These cases are very rare. They are caused only by undiluted alcohol, and depend upon the action of this agent in coagulating albumen and disorganizing the tissues with which it comes in contact by its affinity for the water which they contain. Absolute alcohol is a powerful corrosive poison. It produces intense phlegmonous inflammation of the œsophagus and stomach, with erosion of the mucous membrane, accompanied by vomiting, diarrhœa with bloody stools, prostration, and stupor. Death occurs by heart-failure. Among the direct effects of large doses somewhat less concentrated are acute and subacute gastritis with characteristic symptoms.
[p. 597]Percy23 injected by means of an œsophageal tube 90 grammes of absolute alcohol into the stomach of a dog. Death followed in the course of eight hours in consequence of violent gastro-intestinal inflammation with ulceration. Dujardin-Beaumetz and Andigie found the gastric and intestinal mucous membrane of dogs poisoned by alcohol, red, deeply injected, and “presenting at certain points a black coloration due to effused blood.” This fact they regard as worthy of note, because in their experiments the toxic agent was introduced, not by the mouth, but hypodermically, and they explain it by the supposition—which appears to me warrantable—that it is due to elimination by the mucous glands. Hence the congestion, softening, and hemorrhage.24 These observers also found that the symptoms were more acute and the lesions more marked when poisoning was caused by propyl, butyl, or amyl alcohol than when it was produced by ethyl alcohol.
23 An Experimental Inquiry concerning the Presence of Alcohol in the Ventricles of the Brain after Poisoning by that Liquid, together with Experiments illustrative of the Physiological Effects of Alcohol, London, 1839.
24 Chatin and Gublier have emphasized the fact that certain poisons introduced by intravenous injection or by absorption through the respiratory tract are eliminated by the intestines, with the production of the same local symptoms as when administered by the mouth (Bulletin de l'Académie de Médecine, Séance du 6 Novembre, 1877).
2. Acute Narcotic Poisoning.—Much more common are the cases in which death is rapidly produced by excessive doses of ordinary diluted alcohol taken at once or rapidly repeated. This happens under various circumstances, as when a drunkard avails himself of some favorable opportunity to gratify to the full a bestial appetite, or upon a wager drinks a number of glasses of spirits in quick succession or a given quantity down, or when a man already drunk is plied by his companions for pure deviltry. Suicide by this means is, in the ordinary sense of the term, rare, and murder still more so. The latter crime has, as a rule, been committed upon infants and children. Blyth25 estimates the fatal dose of absolute alcohol, diluted in the form of ordinary whiskey, gin, etc., at from one to two fluidounces for any child below the age of ten or twelve years, and at from two and a half to five ounces for an adult. In the instance recorded by Maschka26 two children, aged respectively nine and eight years, took partly by persuasion, afterward by force, about one-eighth of a pint of spirits of 67 per cent. strength—about 1.7 ounces of absolute alcohol. Both vomited somewhat, then lay down. Stertorous breathing at once came on, and they quickly died. Taylor relates a case in which a quantity of brandy representing about two fluidounces of absolute alcohol produced death in a child seven years old.
25 Poisons, their Effects and Detection, Am. ed., New York, 1885.
26 Cited by Blyth.
The symptoms are uniformly the same. The period of excitement is transient or absent altogether; occasionally the patient falls at once to the ground while in the act of drinking or immediately thereafter; complete coma, interrupted by shuddering convulsions, may terminate in the course of a short time in death. If the fatal issue be delayed, there are vomiting and involuntary discharges; the respiration becomes slow, embarrassed, stertorous; the heart's action is feeble and irregular, the pulse almost or wholly imperceptible; the temperature rapidly falls several degrees: 90° F. has been observed. The pupils are dilated; insensibility and muscular resolution are complete. The face is bloated, cyanotic; the [p. 598] surface bathed in a clammy sweat; the mucous membrane of the mouth often swollen and blanched. Vomiting is usual, but not constant, and there is occasionally thin mucous diarrhœa, the stools being mixed with blood. If the patient survives any considerable length of time, acute superficial gangrene of the parts most exposed to pressure is liable to take place. Recovery is rare; its possibility is, however, increased in proportion as the subject is of vigorous constitution, previous sound health, beyond the period of childhood, not yet approaching that of physiological decadence, and as treatment is early instituted and carried out with judgment.
The diagnosis is difficult, almost impossible, in the absence of witnesses: it is rendered still more obscure by the fact that this, as other forms of alcoholic coma, may be complicated by cerebral or meningeal hemorrhage and by cerebral congestion, in themselves fatal—lesions the onset of which may have been the cause of mental aberration leading to the commission of impulsive alcoholic excesses.
The prognosis, in the highest degree unfavorable in all cases, is rendered yet more so by the occurrence of intense cerebral and pulmonary congestions.
The lesions found post-mortem are those of acute alcoholism, already described. As this form of alcoholic poisoning frequently occurs in the subjects of chronic alcoholism, the lesions of that condition are often encountered, and must be distinguished from those due to the lethal dose. Nor must we overlook the fact that in the action of alcohol just described we have to do with a process differing from ordinary acute alcoholism in degree rather than in kind—a consideration which tends to simplify our notions of the pathology of alcoholism in general.
The prolonged abuse of alcohol brings about a series of changes which affect alike the organism at large and its various structures. The changes thus brought to pass are of the most varied kind, and depend upon individual differences too manifold and complex for enumeration and classification. Among the more important of these individual peculiarities are those which relate to temperament, constitution, hereditary predisposition, occupation, social position, personal habits, tendency to or already-existing disease of particular organs and systems, and the like. The degree of the pathological change is determined by the strength and quantity of alcohol consumed and the duration of habitual excess. The human body is capable of adapting itself to the habitual consumption of large quantities of alcohol, just as to other directly acting agents of an injurious nature, such as foul air, bad drinking-water, and unwholesome food, or even to the action of substances dangerous to life, as opium or arsenic, and yet presenting for a considerable time the appearance at least of health. Degeneration of the tissues of the body and disorders of its functions are nevertheless surely produced. These alterations are not the less dangerous to health and life because they are insidious and remain for a time latent. Furthermore, like the habit of which they are begotten, they are progressive, and sooner or later declare themselves in open disease.
[p. 599]The condition, whether latent or manifest, that is produced by prolonged habitual alcoholic excess is designated chronic alcoholism.27
27 The writer, although fully aware of its imperfections, regards the above definition of the term as more in accordance with the present state of our knowledge of the subject, and therefore more useful, than any other that he has been able to find. It is scarcely necessary to repeat here that the restriction of the term chronic alcoholism to accidental or occasional manifestations of a permanent state is misleading and unscientific. The same criticism is applicable to the attempt that has been made to establish this condition as a substantive disease, chronic, progressive, and characterized anatomically by inflammatory, sclerotic, and steatogenous processes.
The symptoms of this condition, when fully established, differ within wide ranges in kind and degree. They are the manifestations of derangements of the viscera, of the nervous system, and of the mind. Varying among themselves according as the stress of the pathological action has fallen upon one organ or another, forming combinations at once curious and inexplicable, developing quietly, without event, almost imperceptibly at one time, breaking into the most furious paroxysms at another, they present for our study perhaps the most complex of chronic morbid conditions. The chronic alcoholism which is latent is not, therefore, always without symptoms. They are, however, often slight and escape observation, or when manifest they are not infrequently ascribed to other causes; or, again, their etiological relations being concealed or overlooked, they are exceedingly obscure and puzzling. This is especially the case in the chronic alcoholism produced by the secret tippling of otherwise respectable persons, and especially women.
To facilitate description, we shall consider the derangements of the viscera, the nervous system, and the mind in regular order, according to the scheme on p. 574. But the reader will observe that whatever may be the prominence of particular symptoms or groups of symptoms in any given case, all parts of the organism are involved, and that there is no such thing as chronic alcoholism restricted to any particular viscus or group of viscera, to the nervous system, or to the mind.
A. VISCERAL DERANGEMENTS.—There is nothing specific in the lesions of chronic alcoholism. The chronic hyperæmia, steatosis, and sclerosis induced by alcoholic excesses differ in no respect from those conditions brought about by other causes. That which is specific is the evolution of a series of morbid changes in the different structures of the body under the influence of a common and continuously acting cause. The digestive system is affected, as a rule, long before the vascular or the nervous system.
1. Local Disorders.—a. Disorders of the Digestive System.—The Mouth and Throat.—The action of insufficiently diluted alcohol upon the mucous tissues is that of an irritant. The habitual repetition of this action causes subacute or chronic catarrhal inflammation. The condition of the tongue varies with that of the stomach. The mouth in acute alcoholism is apt to be pasty and foul, the tongue slightly swollen and coated with a more or less thick yellow fur; there is often also an increase of saliva; in chronic alcoholism the tongue is usually small, sometimes red, sometimes pale, often smooth from atrophy of the papillæ, not rarely deeply fissured. In a word, the condition of this organ is that seen in the various forms of subacute or chronic gastritis. The salivary secretion is often notably diminished, the sense of taste impaired. Relaxation of the throat and [p. 600] uvula and granular pharyngitis are common. Those who, whilst leading a sedentary life, are inclined to the pleasures of the table and a free indulgence in spirituous liquors often suffer from these affections. Mackenzie28 states that the worst cases of chronic catarrh of the throat generally arise from the habitual abuse of the stronger forms of alcohol. The associated influence of tobacco in the causation of this group of affections is not to be disregarded.
28 Diseases of the Pharynx, Larynx, and Trachea, 1880.
Lancereaux encountered ulceration of the œsophagus, and Bergeret a case of narrowing of that organ, in chronic alcoholism.29
29 Peeters regards it as probable that the connective-tissue hyperplasia and resulting stenosis seen in the stomach as a result of the action of alcohol may also occur in the œsophagus.
The Stomach.—In addition to functional dyspepsia, which is scarcely ever absent in chronic alcoholism, all forms of gastritis, from simple erythematous inflammation of the mucous membrane to sclerosis and suppurative inflammation of the stomach, are encountered. Armor30 assigns to the habit of spirit-drinking, especially to the habit of taking alcohol undiluted on an empty stomach, a high place among the causes of indigestion. He regards this habit as a prominent factor in the production of chronic gastric catarrh—a condition very frequently present in indigestion. This observer also regards the excessive use of alcohol as the most frequent among the direct exciting causes of gastric inflammation in this country, exclusive of acid or corrosive poisons. Next to errors in diet as a cause of chronic gastritis he places the immoderate use of alcohol, especially by persons whose general health and digestive powers are below a healthy standard. The primary lesions are vascular dilatation and hyperæmia. The mucous membrane is discolored, red or bluish, in scattered patches of varying size, with occasional ecchymoses of a bluish hue or spots of pigmentation. These patches occupy more commonly the region of the cardia and the lesser curvature. Vascular injection is conspicuous; the veins are dilated, tortuous; the mucous glands hypertrophied; the surface covered with thick, ropy, acid-smelling mucus. After a time permanent changes in the mucous membrane are set up. It undergoes atrophy or softening; or, again, it becomes hardened, thickened, and contracted, its rugæ more prominent, its surface mammilated—sclerosis. Grayish-brown pigmentation, the remains of former blood-extravasations, is seen at many points. Minute retention-cysts are formed in consequence of the occlusion of the ducts of certain glands. The submucous connective tissue and the muscular coat occasionally undergo, in consequence of prolonged gastritis, local hypertrophy.
30 See this System of Medicine, Vol. II. pp. 446, 464, 470.
Acute suppurative inflammation of the stomach, with purulent infiltration of, or the formation of abscesses in, the submucous tissue, has been met with in drunkards. It is extremely rare, and results from the violent irritant action of large doses of strong alcohol in subjects debilitated by previous excesses.
Gastric ulcer is much more common. The abuse of alcohol is regarded as an indirect cause of this lesion by the majority of writers. In the present state of knowledge alcohol as usually taken can scarcely be regarded as a direct cause of ulceration. Nevertheless, gastric ulcer is relatively [p. 601] common in alcoholic subjects. Leudet31 found gastric ulcer in 8 of 26 necropsies of drunkards. Baer and Lentz also regard the abuse of alcohol as a very common cause of ulceration. The ulcers are usually superficial, occupy by preference the neighborhood of the cardia and the lesser curvature, and are apt to be multiple. In these respects they differ from simple gastric ulcer. The latter lesion is also probably as frequent, if indeed not more frequent, in individuals dying of chronic alcoholism than in others.
31 Clinique médicale de l'Hôtel Dieu à Rouen, 1874.
The view formerly entertained that alcohol was an important cause of cancer of the stomach has been shown by Kubik, Magnus, Huss, Engel, and others to be untenable. Carcinoma ventriculi is rarely associated with chronic alcoholism.
The dimensions of the stomach are rarely normal. Dilatation is usually present in the early stages, and in beer-drinkers throughout; in the advanced course of alcoholism due to spirit-drinking the organ undergoes, in consequence of changes secondary to prolonged inflammation, more or less contraction, which is in many cases irregular.
Dyspeptic symptoms are common: the appetite is variable, irregular, and at length wholly lost. There is especially distaste for food in the morning. This, together with the disordered state of the secretions of the mouth and a feeling of nervous depression on rising, leads to the disastrous habit of taking spirits early in the day. Gastric digestion is performed with difficulty; it is accompanied by sensations of distension and weight, by flatulence and acid eructations. Heartburn is a common symptom. The drunkard is not rarely tormented by an uneasy craving or sense of emptiness in the region of the stomach, which he temporarily allays by nips and pick-me-ups and morsels of highly-seasoned foods at odd times, with the result of still further damage to his digestion and the complete loss of appetite for wholesome food at regular hours. In the course of time the characteristic morning sickness of drunkards is established. On arising there is nausea, accompanied by vomiting—sometimes without effort or pain, at others attended by distressing retching and gagging. The matter vomited consists usually of viscid mucus, at first transparent, then flaky, and at length, if the efforts be violent, of a green or yellow color from the admixture of bile. These symptoms ordinarily do not recur until the following day. In other cases vomiting is more frequent, recurring at irregular periods during the day, and not uncommonly an hour or two after the ingestion of food. When gastric ulcer is present, portions of the vomited matter are often dark and grumous like coffee-grounds or the settlings of beef-tea, and are found upon microscopic examination to contain blood-corpuscles. Actual hæmatemesis may also occur under these circumstances, and be repeated from time to time. The quantity of blood thrown up is frequently small; at times, however, it is excessive, and occasionally so great as to cause death.
Common as are the evidences of gastric disturbance in chronic alcoholism, they are far from being constant, and it is worthy of note that in proportion to the number of the cases serious gastric affections are, except in the later stages, relatively infrequent.
The Intestines.—Lesions of the small intestine due to alcoholism are [p. 602] extremely rare. Even when simple or ulcerative inflammation of the stomach is localized at, or extends to, the pylorus, it rarely passes any great distance into the gut. The large intestine is, on the contrary, frequently the seat of chronic inflammatory processes. Here we find vascular engorgement, patches of pigmentation, localized thickening of the mucous and submucous tissues, enlargement of the solitary glands, and an excessive secretion of viscid mucus. The tendency to permanent vascular dilatation, which is a characteristic result of alcoholic habits, constitutes a powerful predisposing influence in the causation of hemorrhoids, which are common. Alcohol acts directly upon the hemorrhoidal plexus of veins, and indirectly by causing permanent congestions of more or less intensity in the greater number of the abdominal viscera. When a prolonged course of excesses in alcohol has led to chronic congestion with hypertrophy, cirrhosis, or other structural change in the liver which is capable of causing permanent mechanical obstruction of the portal circulation, hemorrhoids constitute a very common affection in the group of morbid entities secondary to these conditions.
The symptoms of intestinal derangement are in the beginning, as a rule, slight and occasional. They consist of uneasy sensations or colicky pains in the abdomen, a feeling of fulness with or without tympany, and constipation alternating with diarrhœa: in a word, they are the symptoms of acute or subacute intestinal indigestion terminating in an attack of intestinal catarrh. Attacks of this kind repeat themselves in a considerable proportion of the cases with variable but increasing frequency, until at length the conditions of which they are the expression become permanent, and the patient suffers, among other distressing symptoms hereafter to be described, from chronic diarrhœa. The stools are now of the most variable character—occasionally bilious, sometimes containing small dark scybalous masses, rarely formed, but usually containing more or less abnormal mucus, too much fluid, and traces of blood. Indeed, at this stage several causes—among which I may mention visceral congestions, local inflammation of the intestinal mucous membrane, dilatation of the hemorrhoidal veins, and structural changes in the liver—conspire to determine blood toward the interior of the intestinal tube. Traces of blood in the stools are therefore frequent, and actual hemorrhage and the appearance of the dark, tarry, and altered blood formerly described under the term melæna are by no means rare. Colliquative diarrhœa and dysenteric attacks also occur, and at length an intense enteritis with uncontrollable diarrhœa may end the life of the patient. The conditions just described lead to rapid emaciation, and contribute when present to the establishment of the cachexia so marked in many cases of chronic alcoholism.
The Glands.—The salivary glands were found by Lancereaux32 to have undergone softening, with granulo-fatty changes in their epithelium. If such changes are among the usual effects of alcohol, they are doubtless productive of alterations in the saliva, which explain, in part at least, the dryness of the mouth so frequent among drunkards.
32 Dictionnaire de Médecine, art. “Alcoholism.”
The pancreas is, as the result of interstitial inflammation, the seat of similar changes. It is sometimes enlarged and softened, sometimes atrophied, shrivelled, or cirrhotic. In the latter condition its consistence is [p. 603] firm, its surface uneven, its color deep yellow, brown, or pale. Hyperplasia of the interacinous connective tissue, with subsequent contraction and atrophy and destruction of the glandular tissue, characterizes the more chronic forms of pancreatitis, and the organ is frequently the seat of scattered minute blood-extravasations. I have already alluded to the enlargement of the solitary glands which constitutes a feature of the condition of the large intestine. The solitary glands and Peyer's patches of the small intestine are rarely altered.
b. Disorders of the Liver.—Next in order to the stomach, the liver is more directly exposed to the action of alcohol than any other viscus. For this reason lesions of the liver are frequent and grave. It is worthy of note, however, that in a small proportion of cases of chronic alcoholism terminating fatally, with widespread evidences of the destructive action of alcohol upon the other organs of the body, the liver has been found, both in its macroscopic and microscopic appearances, wholly normal. Absorbed by the gastric vessels, alcohol passes directly, by way of the portal vein, into the parenchyma of the liver, there giving rise to various disturbances, the nature of which is determined by the tendencies of the individual on the one hand, and on the other hand by the character of the alcohol consumed. The danger of hepatic disease is in direct proportion to the amount and the concentration of the alcohol habitually taken. The steady drinkers of spirits of whatever kind, whether gin, brandy, whiskey, or rum, present the largest proportion of diseases of the liver. These affections are far less common among beer-drinkers, and infrequent among wine-drinkers in wine-growing countries. In this connection it is to be borne in mind that the presence of food in the stomach retards to some degree the absorption of the alcohol ingested, and to a certain extent constitutes a means of dilution.
Hepatic disorders due to alcohol may be arranged in two groups: first, congestion and inflammation; second, fatty infiltration or steatosis; and the inflammatory process may affect chiefly the interstitial connective tissue on the one hand, giving rise to sclerosis, or on the other the glandular substance, constituting a true parenchymatous inflammation.
Congestion.—Congestion of the liver is an early lesion. It is brought about by the direct irritant action of the alcohol itself in part, and in part by the extension of inflammation from the stomach by continuous mucous tracts. Its development is insidious. Anatomically, the condition is characterized by vascular dilatation, moderate tumefaction, slight increase in the consistence of the organ; the surface is of a deeper red than normal; on section the color is more intense and the oozing more abundant. At a later period we have, as the result of chronic congestion, the cyanotic liver; the color is brownish or violet, mottled, and on section the surface is granular and the lobules distinct. The organ may now be somewhat diminished in size, but it lacks the firmness of sclerosis and the hobnail appearance due to the contraction of the interlobular connective tissue in that condition.
The symptoms of congestion of the liver are the familiar symptoms of gastro-hepatic catarrh, varying from the transient disturbance known as biliousness to serious sickness, characterized by acute gastro-intestinal phenomena, with vomiting, headache, and other derangements of the nervous system—constipation, succeeded by diarrhœa and by more or less [p. 604] distinct jaundice. The graver forms of hepatic congestion are characterized by intense nausea, frequent vomiting, pain and soreness in the epigastrium and right hypogastrium, the physical signs of augmentation of the volume of the liver, and well-marked yellow discoloration of the conjunctivæ and skin. These attacks are usually afebrile: the pulse is slow; there is considerable nervous and mental depression, a tendency to vertigo, and occasional syncope. The urine is scanty and high-colored, and presents the reactions of bile-pigment. Muscular tremor, especially marked in the extremities and tongue, is often present, but is to be attributed rather to the direct action of alcohol upon the nervous system than to the condition of the liver.
Hepatitis.—There are two principal forms of inflammation of the liver induced by alcohol—parenchymatous hepatitis and interstitial hepatitis or sclerosis.
Several varieties of parenchymatous hepatitis have been described. The anatomical discrimination of these varieties is attended with less difficulty than their clinical diagnosis. One of the more serious is diffused parenchymatous hepatitis or acute yellow atrophy. Alcoholic excesses appear to constitute a predisposing influence to this grave disorder (Lentz). In several cases prolonged and repeated excesses have preceded its development. It is a true parenchymatous inflammation, in which the glandular elements of the organ undergo disintegration. The liver is diminished in volume in all its diameters. It is of a uniform yellow color; its tissue is soft and friable; upon section the hepatic cells are found to be replaced by a granular detritus mingled with globules of coloring matter and a greasy, grayish-yellow liquid exudation.
The symptoms of this affection are those of an acute parenchymatous hepatitis of the gravest kind. In the early stages there is intense jaundice, gastro-intestinal disturbance, and fever, followed by speedy evidences of profound toxæmia. The patient rapidly falls into the so-called typhoid state, with a tendency to coma. The prognosis is, in the greater number or cases, a fatal one. So close is the resemblance between acute yellow atrophy of the liver and the phenomena of acute phosphorus-poisoning that by many observers these two conditions are held to be identical.33
33 Consult this System of Medicine, Vol. II., article “Acute Yellow Atrophy of the Liver.”
There is little doubt that the view now generally held, that acute yellow atrophy is due to the action of some unknown toxic principle, is correct. Alcoholic excess must therefore be regarded merely in the light of a predisposing influence. Acute yellow atrophy of the liver is an exceedingly rare disease.
Suppurative Hepatitis.—Abscess of the liver is in temperate climates infrequent as the direct result of alcoholic excess. It is frequently ascribed, however, to improper alcoholic indulgence, especially when combined with the eating of large quantities of improper food, in tropical and subtropical climates. A form of hepatitis has been described by Leudet under the head of chronic interstitial hepatitis with atrophy. The symptoms are for the most part not very well marked, and consist chiefly in general malnutrition, which may in fact be dependent upon the associated gastric disturbance. Chronic jaundice is usually present.
Interstitial Hepatitis.—Cirrhosis of the liver is in a large proportion of cases directly attributable to alcoholic excess. In this view the greater [p. 605] number of observers coincide. But that alcohol is not the sole cause of chronic interstitial hepatitis has been abundantly established. As long ago as 1868, Anstie34 wrote as follows: “Considering the enormous quantities of spirituous liquors which are drunk by many of the patients who apply for relief from the consequences of chronic alcoholism, it would be natural for the reader who holds the usual opinion as to the origin of cirrhosis of the liver to expect that serious symptoms produced by the latter disorder must often complicate cases of the former. The case is, however, far otherwise in my own experience. Of the immense number of patients in whom the nervous disorder has been clearly identified, I have only seen thirteen cases in which the symptoms of cirrhotic disease called for any special treatment, although a certain degree of cirrhosis was doubtless present in many of the others; and I cannot avoid the conclusion that some very powerful element over and above the influence of alcoholic excess is needed to produce the severe type of that disease.” Formad35 states as the result of his investigations as coroner's physician of the city of Philadelphia that cirrhosis of the liver is much less common in alcoholic subjects than has been generally thought. My own experience during eleven years as attending physician at the Philadelphia Hospital leads me to endorse this opinion.
34 A System of Medicine, Reynolds, vol. ii. p. 74.
35 Proceedings of the Pathological Society of Philadelphia, Dec., 1885.
The anatomical lesions of chronic interstitial hepatitis consist essentially in hyperplasia and hypertrophy of the connective tissue of the organ. The progress of the affection is insidious and gradual; some degree of enlargement, due in part to congestion and in part to interstitial exudation, is followed by gradual diminution, with retraction of the new connective tissue. When the connective-tissue new formation is excessive, and retraction fails to take place, the organ remains permanently enlarged (hypertrophic cirrhosis). During the first period the volume of the organ is increased, its consistence is more firm, and its surface is slightly granular. The second period is characterized by induration, with diminution of the volume of the organ and alteration of its form. The surface is uneven, deeply granular, and usually of a mottled yellow color. The tissue is firm, creaking under the knife. The connective tissue is enormously increased, the glandular elements being proportionately atrophied.
The contracting connective tissue exercises at the same time a compressing influence upon the hepatic cells and upon the vascular supply throughout the organ; the radicals of the portal vein and the branches of the hepatic artery are alike compressed, and in part obliterated. The same is true of the bile-ducts. The functional activity of the liver, at first diminished, is finally, to a considerable extent, arrested. In consequence of these physical alterations in the structure of the organ, the symptoms, which are at first insignificant, become progressively more grave, until at length they constitute complications of the most serious kind.
It can be no longer asserted that the interstitial hepatitis produced by alcohol presents specific characters. It nevertheless differs in many respects from that form due to valvular lesions of the heart, in which there are induration, usually augmentation in the volume of the organ, [p. 606] and persistent congestion. Congestion, in truth, is the chief characteristic of the latter form, in which the surface is smooth and glistening, of a deep brown or violet hue, and on section yellowish or brown—a condition which has been well described under the term cyanotic liver.
Sclerotic changes due to alcohol usually affect the organ throughout. In this respect alcoholic cirrhosis differs from that form due to syphilis in which the lesions are irregularly distributed.
The functional disturbances due to cirrhosis are, in the beginning, obscure in themselves and masked by the concomitant gastric derangement. Later, ascites constitutes the chief as well as the most constant symptom. It is rarely altogether absent. Emaciation is also a prominent symptom. No affection, not even diabetes or phthisis, produces loss of flesh so rapid, so marked, and so significant as cirrhosis of the liver in chronic alcoholism. Not only do the adipose tissues waste, but the muscles themselves undergo rapid atrophy. This fact is not surprising when we consider that the lesions of the liver give rise to grave interference with every function of that organ. In addition to the more common gastric symptoms, there is constipation, not rarely alternating, without assignable cause, with serous and sometimes bloody diarrhœa. Epigastric distress, epistaxis, and hemorrhages from other mucous surfaces are common, and are due in part to the disturbance of the general circulation, and in part to alterations in the character of the blood itself. The physical signs indicate in the early stages increase, and afterward diminution, in the volume of the liver. Enlargement of the superficial abdominal veins is a characteristic sign. Cirrhosis of the liver is a grave affection, the course of which, at first slow, afterward more rapid, almost invariably leads to a fatal termination.
Fatty Degeneration of the Liver.—Steatosis of the liver is of extremely common occurrence in the advanced stages of alcoholism. The anatomical changes consist in accumulation of fat-globules in the liver-cells. French writers distinguish two varieties of hepatic steatosis: first, that in which the cellular elements undergo no change beyond that of an accumulation of fat-globules within their substance; and second, that in which the liver-cells undergo an actual disintegration, in the course of which fat-granules are formed, and which is, as a matter of fact, a true fatty degeneration. The first of these conditions is not incompatible with the functional integrity of the organ, and is in many instances unattended by symptoms, being discovered only upon examination after death. Its occurrence is to be explained by the imperfect oxidation of waste products due to the constant presence of alcohol in the blood, and by the habitual excess of fat in the latter fluid. When fatty infiltration is of moderate amount there are no changes in the volume or the contour of the organ, and the condition is recognized only on microscopical examination. At a later stage the organ becomes enlarged, particularly in its antero-posterior diameter. The surface is now smooth and glistening, its color yellow or reddish-yellow; upon section it is anæmic, of a yellowish color, with patches of a reddish hue, and its consistence is diminished. The indentation caused by pressure of the finger persists. Under the microscope the hepatic cells are enlarged, rounded, packed with fat-globules of varying size. In some of the cells these globules coalesce and form more or less extensive drops of fat. The bile which is [p. 607] secreted in this condition presents in most instances the normal characteristics.
Disorders of digestion do not occur in consequence of the fatty change in the liver until the lesion has reached an advanced stage; nevertheless, they constitute the earliest symptoms of this condition. Imperfect digestion, accompanied with flatulence, distension of the belly, epigastric tenderness, with light-colored stools, and constipation alternating with diarrhœa, are common symptoms. There is no pain properly referable to the region of the liver. Whilst icterus does not occur, there is, nevertheless, a peculiar earthy pallor of the complexion and persistent greasiness of the skin—conditions, however, which are not in themselves sufficiently marked to possess, in the absence of other signs, clinical value.
The second form of fatty degeneration, in which the liver-cells undergo actual and destructive metamorphosis, accompanied by the production of fat, is of a much more serious character. It appears to constitute the stadium ultimum of various forms of interstitial hepatitis, and is manifested by symptoms of the gravest character, in many particulars much like those met with in acute yellow atrophy—namely, visceral congestions, hemorrhages from mucous surfaces, serous effusions, profound and rapidly developing anæmia, nervous depression, and coma.
Biliary Catarrh.—The biliary ducts are usually the seat of catarrhal inflammation, due less perhaps to the direct irritant action of the alcohol than to the extension of the inflammation of the gastric mucous membrane in the form of gastro-duodenal catarrh. Gall-stones are not common in alcoholism.
The spleen is, as a rule, enlarged, soft, and friable; occasionally it is small and shrivelled. No characteristic changes in its contour and structure have been recorded.
The great omentum and mesentery are loaded with fat, very often to an extreme degree. This condition is more marked in the chronic alcoholism of beer-drinkers than in that of spirit-drinkers. Not infrequently there are found evidences of chronic peritonitis, which has been attributed by Lancereaux, in the absence of other assignable cause, to the effect of alcohol itself. The symptoms of this condition are usually obscure, consisting of diffused dull pain, augmented upon pressure, diarrhœa, digestive troubles, and abdominal distension, sometimes voluminous, often irregular.
c. Disorders of the Respiratory System.—The Larynx.—Catarrhal inflammation of the mucous membrane of the air-passages is common in drunkards. Some degree of subacute or chronic laryngitis is an early symptom of chronic alcoholism. It may result from repeated attacks of acute alcoholism, or it may be among the first signs of excesses that are continuous, without at any one time being extreme. In the production of this local trouble the direct action of alcohol is reinforced by the foul and smoke-laden air of the apartments in which tipplers spend much of their time and by heedless exposure to the vicissitudes of the weather. The anatomical changes are those of chronic laryngitis in general, hyperæmia of the mucous membrane with minute ecchymoses, local destruction of epithelium with superficial ulcerations or granulating surfaces. The mucus is often thick, opaque, and adherent.
[p. 608]These lesions are accompanied by more or less decided impairment of function. The voice is hoarse and husky; there is fatiguing laryngeal cough, usually harsh and grating in character, and attended by scanty muco-purulent expectoration. This cough is often paroxysmal; especially is it apt to be so on rising, and it then provokes the vomiting previously described.
The Bronchi.—After a time similar anatomical changes are brought to pass in the bronchial tubes. Subacute bronchitis is little by little transformed into the chronic form, characterized by hyperæmia and thickening of the mucous membrane, extending to the finer twigs, with submucous infiltration and implication of the connective-tissue framework of the lung. The exudation, tough and adherent or fluid and copious, occasions more or less frequent cough, and interferes with the function of respiration. Hence it is common to encounter in the subjects of chronic alcoholism bronchiectasis, pseudo-hypertrophic emphysema, easily excited or permanent dyspnœa, asthmatic seizures, and some degree of cyanosis. These local affections, interfering with the circulation of the blood and its proper aëration, react unfavorably upon the nutrition of the organism at large, and largely contribute to the production of the ultimate dyscrasia.
The Lungs.—Pulmonary congestion and œdema are of common occurrence. Favored by the action of alcohol upon the vaso-motor system, they are readily excited by the careless habits and frequent exposures of the subject. The lesions occupy by preference the lower and posterior parts of the lungs, and consist in relaxation of the parenchyma, with vascular dilatation and serous infiltration. The vesicles are capable of distension, but contain little air. The tissue is friable, deep-red or brownish in color, and floats upon water. The symptoms of this condition are sometimes obscure: usually they consist in a sensation of constriction of the thorax, more or less dyspnœa, mucous expectoration, sometimes streaked with blood, and lividity of the countenance and finger-tips. The chief physical signs are impaired percussion resonance and mucous, subcrepitant, and occasionally a few scattered crepitant râles.
Pulmonary Apoplexy.—When the congestion is extreme, blood may escape into the parenchyma of the lung with laceration of its substance. This lesion is more frequent in intense acute alcoholism than in the chronic form.
Pneumonia.—Habitual alcohol-drinkers are far more liable to pneumonia than others. It has even been asserted that alcohol is of itself capable of acting as an efficient exciting cause. Whilst it is indisputable that the action of this agent upon the pulmonary blood-vessels and in favoring pulmonary congestion constitutes a powerful predisposing influence, it cannot be admitted, regard being had to the fact that it is largely eliminated by the lungs, that alcohol can, in the absence of a specific cause, ever produce a specific acute febrile disease, such as croupous pneumonia. The pneumonia of alcoholic subjects, like that of aged persons and that occurring in the convalescence from acute diseases, is apt to be latent. The exudation is often of limited extent; the symptoms are insidious, and the striking clinical features of the ordinary frank form of the affection are not rarely absent altogether. It is no infrequent occurrence that pneumonia is overlooked in the delirium tremens which it has induced.
The anatomical changes are those of the ordinary form. The prognosis [p. 609] is always grave. When recovery occurs resolution is often tedious and prolonged.
Catarrhal pneumonia is also common. It is marked by its usual phenomena.
The most striking fact in the pneumonia of alcoholic individuals is the contrast between the local and the constitutional symptoms. The former are in the greater number of the cases insignificant and easily overlooked. Even the physical signs, when sought for, are often obscure and indeterminate: relative dulness, enfeebled or absent vesicular murmur, faint scattered crepitation masked by mucous râles, and a bronchial respiratory sound scarcely appreciable, are all that can be detected upon physical examination. In strong contrast to this almost negative picture is that of the constitutional disturbance, which is commonly of the gravest kind. The prostration is extreme; there is delirium with tremor, restlessness, sleeplessness, mental agitation, profuse sweating, feeble action of the heart, gastro-intestinal irritation, with vomiting and often complete inability to retain food. The temperature-curve lacks the characters of pneumonia of the ordinary form. Not seldom is febrile movement absent altogether.
The view that alcohol, independently of and in the absence of other lesions, occasionally produces changes in the lungs analogous to the chronic interstitial inflammatory processes of cirrhosis of the liver—i.e. fibroid phthisis—is not borne out by clinical or pathological investigation, and appears to be wholly without foundation in fact.
Pulmonary Phthisis.—The question whether or not chronic alcoholism exerts any influence in the production and evolution of pulmonary phthisis has been the subject of no little fruitless controversy. There are medical men of experience who do not hesitate to affirm that the abundant use of alcohol constitutes in certain cases an actual prophylaxis, while there are others who insist with equal positiveness that alcoholic excesses favor the development of this affection. Whatever may be the influence of alcohol in depressing the forces of the body and in the production of serious lesions of pulmonary structures, and thus predisposing the subject to phthisis, it can be asserted with confidence that it does not directly cause any form of phthisis whatever. The alcoholic phthisis of Lancereaux, Richardson, Drysdale, and others cannot be now regarded as a distinct, independent affection. The process of exclusion by which alcohol was made to seem the real cause of the disease in 36 of 2000 of the cases examined by Richardson was not sufficiently rigid to meet the requirements of our present knowledge. There is reason to believe that by its favorable influence upon the appetite and digestion, its power to reduce temperature, its retarding influence upon tissue-waste, alcohol in moderate quantities is of great use in the management of this affection. That phthisical subjects occasionally seem to derive benefit from, and to lengthen their lives by, excesses in alcohol is capable of explanation—first, by the fact that an extraordinary tolerance for alcohol is natural to or acquired by certain individuals; and, second, by the favorable influence of alcohol upon ulcerative and suppurative processes, and in determining connective-tissue new formation—a process by which certain inflammatory products, including tubercle, are capable of being rendered inert. The foregoing remarks are applicable to all forms of pulmonary phthisis.
[p. 610]The Pleuræ.—The pleura is sometimes the seat of patches of fibrinous exudation of varying extent and thickness, which are, according to Lentz, the expression of the formative action which constitutes one of the modalities of alcoholism, and which are of the same nature as the fibrinous exudations which occur in the peritoneum and the dura mater. These false membranes cause pleural adhesions, and occasionally contain within their meshes a turbid serous fluid.
d. Disorders of the Circulatory System.—The Heart.—This organ is usually implicated to a greater or less extent in the course of chronic alcoholism. Lesions of the muscular substance are more common than those of the valvular apparatus.
Hypertrophy is common. It affects usually both sides of the heart—the left, however, more than the right—and is associated with some degree of dilatation. The part played by alcohol in the production of cardiac hypertrophy is a dual one: first, that of constantly-repeated direct stimulation of the heart; second, that of the indirect stimulation to over-action caused by the necessity to overcome the obstacles which the lesions of the viscera interpose to the circulation of the blood in the later periods of the disease. Nor are the lesions of the blood-vessels themselves, hereafter to be described, without influence in inducing hypertrophy. Bollinger and Schmidbauer have shown that the habitual consumption of beer in excessive quantities leads to cardiac hypertrophy of characteristic form. Both sides of the heart participate in the overgrowth: there is enormous increase in the volume of the primitive muscular elements, with enlargement of the nuclei. Whether or not actual numerical increase in the muscular fibres takes place cannot be determined. This form of enlargement of the heart occurs in the absence of lesions of the valves, disturbances of the pulmonary circulation, arterial sclerosis, atheroma, or granular kidneys. Some few of these cases of so-called idiopathic hypertrophy are perhaps due to prolonged excessive bodily effort and bodily strain. But the greater number are only to be explained by habitual excesses in beer-drinking, as shown by carefully worked-out personal histories of the patients. Neither fatty degeneration nor myocarditis enters into the pathological process under consideration. The hypertrophy is due to the direct action of the alcohol consumed, to the enormous amount of fluid introduced into the body, and to the easily-assimilated nutritive constituents of the beer itself. Furthermore, such habits are often associated with great bodily activity and a relatively luxurious manner of life. The greater number of alcoholic subjects who suffer from this form of hypertrophy perish after brief illness with symptoms of heart-failure. At the necropsy are discovered moderate dropsy, congestion and brown induration of the lungs, congestion of the liver, spleen, kidneys, and other organs, bronchitis and moderate serous effusions or general anasarca. Death is probably due to paralysis of the cardiac nerves and ganglia. This form of hypertrophy is of course much more common among men than among women. It is much less common in this country than in Germany, but is occasionally met with among brewers' employés.
Fibroid Degeneration.—This condition has been ascribed to a number of causes, among which long-continued excess in alcohol is unquestionably an important one. Bramwell holds the opinion that in a certain [p. 611] proportion of cases of this description, in which fibroid degeneration of the heart is connected with similar changes in the kidneys (sclerosis), the lesions of both organs are due to alcoholism. Alcoholic fibrosis differs in no respect from that due to other causes. The condition may escape recognition by the unaided eye if it be disseminated throughout the muscle and the change consist in thickening of the perimysia around undivided fibres. The heart is larger than normal, perhaps a little paler, and its consistency a little more firm. When, as is more commonly the case, the fibroid change is localized, and masses of new tissue are developed in and around the muscular fibres, the heart assumes a flecked or streaked appearance, due to the contrast between the yellowish-white fibroid tissue and the brownish-red muscular structure. The microscope shows excessive development of fibrous tissue, with atrophy of muscular fibres. The effect is to weaken the force of the heart's action, and to weaken the walls of the cavities at the affected parts in such a manner as to cause local bulgings or cardiac aneurisms.
The symptoms and physical signs of fibroid degeneration of the heart are very obscure and indefinite, and the diagnosis is always attended with difficulty, and in many cases is impossible. Jubel-Renoy, however, regards the diagnosis as having already attained some clinical exactitude, and regards as important the association of the following diagnostic data: first, feebleness of the systole and the pulse, with augmentation of the frequency without irregularity; second, moderate enlargement, varying within considerable limits; and third, absence of murmurs in the greater number of the cases. Death is apt to occur suddenly. Welch, upon investigation of the clinical histories of cases in which fibroid degeneration of the heart was found after death, concluded that they might be clinically grouped as follows: first, cases in which there is no symptom of heart disease; second, cases of sudden death without previous heart symptoms; third, sudden death preceded by one or more attacks of angina pectoris; fourth, after cardiac insufficiency of a few days' standing; and fifth, in cases of old heart disease.
Fatty Heart.—Under the term fatty heart two distinct pathological conditions are comprised. Of these the first is fatty infiltration, which consists in an excessive development of the normal subpericardial fat, with a deposition of fat-cells in considerable number between the muscular fibres of the myocardium. This condition occurs chiefly in individuals suffering from general obesity, and is particularly apt to occur in alcoholic obesity. Large masses of fat fill the grooves and furrows of the organ, the surface of which is covered with a thick layer of yellowish fat. The right heart is first and most affected, but in advanced cases the whole heart may be encased in a thick fatty layer. When the fat-cells infiltrate the intermuscular spaces, they exert pressure which may produce atrophy and degeneration of the muscular elements. This condition may exist to a certain extent without symptoms, but it is, however, apt to be manifested by a certain amount of cardiac dyspnœa and inability to endure excessive strain or acute illness. In cases in which the fatty infiltration attains a high grade, inducing by mechanical pressure degenerative changes in the muscular substance of the heart, there are signs of embarrassment of the circulation. The precise diagnosis is usually difficult, often impossible.
[p. 612]The second form of fatty heart is known as fatty degeneration, and consists in changes in the muscular fibres by which the albuminoid constituents are broken up and replaced by microscopic particles of fat. After a time the transverse striæ disappear, and the functional activity of those muscular fibres which are affected is completely lost. All conditions which interfere with the supply of oxygen to the muscular tissue or which seriously derange its nutrition are capable of producing fatty degeneration. Among these are alcoholic excesses. The color of the heart is paler than normal, usually fawn or pale buff. It has been described as the faded-leaf color. The consistence is softer than normal, the wall of the heart in many instances being readily broken down by the pressure of the finger. The left ventricle is the part most likely to be affected, the papillary muscles being often profoundly altered. Next in order the right ventricle is involved, then the left auricle, and finally the right auricle. When this form of degeneration is due to disease of the coronary arteries, the lesion is usually localized, sometimes limited to the distribution of the branch of the artery which is affected.
Upon microscopical examination the affected muscular fibres are found to contain minute molecules of fat, often of a uniform size, sometimes arranged in rows, but commonly distributed irregularly throughout the substance of the fibre. The transverse striæ are indistinct, and sometimes wholly absent. The functional activity of the affected fibres is seriously interfered with or wholly lost, and as a result the force of the circulation is greatly weakened. These two forms of fatty change are occasionally associated. Among the more common symptoms are shortness of breath upon exertion, with dry hacking cough. In advanced cases the dyspnœa may become constant. The fatal issue is sometimes preceded by the Cheyne-Stokes respiration. Other symptoms are due to cerebral anæmia. The memory is impaired, the patient becomes wayward and irritable, and is apt to become faint upon suddenly changing from the recumbent to the erect posture, and in most instances is incapable of concentrated mental effort or active bodily exertion.
The Blood-vessels.—Capillary dilatation is one of the earliest and most persistent effects of alcohol. The visceral congestions which constitute so important a factor in the pathology of alcoholism are in part the result of the paralyzing action of alcohol on the vaso-motor system, and in part of the degenerative changes in the unstriped muscular fibres of the arterial walls.
Atheroma.—Alcoholic excesses play an important part in the etiology of atheromatous degeneration of the arterial walls, not so much by the direct action of the alcohol itself, as by its indirect action in increasing the tension in the main trunks, and in leading to an irregular life in which excitement, sudden and severe exertion, exposure to cold, and depressing influences of all kinds play a part.
Valvular lesions of the heart do not occur as a direct result of the action of alcohol.
e. Disorders of the Genito-urinary Apparatus.—The Kidneys.—Alcohol, as has been shown above, is a diuretic. In large doses it produces renal congestion. Ollivier36 observed acute transient albuminuria resulting from the influence of excessive doses of alcohol.
36 Essai sur les Albuminuries produites par l'Elimination des Substances toxiques, Paris, 1863.[p. 613]
Much difference of opinion exists as to the part played by alcohol in the causation of the various forms of Bright's disease. It was at one time thought that a large proportion of the cases were due to the abuse of this substance. Bright held this view, and Christison attributed from three-fourths to four-fifths of all cases of granular degeneration of the kidneys to the abuse of spirits. The latter considered that not alone in notorious drunkards was this result likely to occur, but even in those accustomed to the moderate daily consumption of spirits with only occasional excesses. This opinion for a long time largely prevailed among English writers. Of late years, however, in consequence partly of the teachings of Anstie and Dickinson, partly of more precise methods of reasoning, the direct causative relation between chronic alcoholism and disease of the kidneys has come to be questioned. Nevertheless, many teachers of authority adhere to the former view. It is, however, more than probable that the action of alcohol is not of itself capable of producing these effects in the absence of other causes, among which are insufficient or improper diet, irregular living, damp dwelling-places, occupations necessitating great or prolonged exposure to cold and wet or such exposure from accidental causes—circumstances to which those who, especially among the poorer classes, are addicted to drink are peculiarly liable. Nor must we overlook the influence of exposure to paludal poison, of lead, and of heredity in the causation of diseases of the kidneys. While alcohol cannot be regarded as the direct exciting cause of acute or chronic nephritis, chronic alcoholism acts as an influence predisposing to the development of these affections in persons otherwise liable to them.
Congestion of the Kidneys.—The general action of alcohol in inducing visceral hyperæmia is aided by its special diuretic action in causing chronic congestion (cyanotic kidney). The kidney is of a dark violet-red hue, slightly enlarged, especially in its transverse diameter, of a consistence firmer than normal, and bleeds freely upon section.
Acute parenchymatous nephritis is of rare occurrence in chronic alcoholism. Of chronic parenchymatous nephritis Bartels37 writes: “I may say that alcoholic excesses, to which the disease is by many attributed, cannot be charged with being the cause of it. None of the cases treated by me occurred in drunkards, and in no instance have I encountered the large white kidney at the autopsies of notorious drinkers, of which I have made a not inconsiderable number during my many years' active hospital service.” The same author in discussing the etiology of chronic interstitial nephritis (contracted kidney) enters a protest against the view which is widespread in England that the abuse of spirituous liquors favors the development of the genuine contracted kidney. He says: “In the first place, among all the patients whom I have treated, three only were brandy-drinkers to any notorious excess, while by far the greater number who were affected with this complaint had lived remarkably abstemious lives. In the second place, throughout my twenty-five years of active service as a hospital physician I have had the most abundant opportunity of watching the consequences of intemperance, both at the bedside and upon the post-mortem table; yet these three cases have hitherto been the only ones in which I have found atrophied [p. 614] kidneys in the bodies of habitual drunkards.” Baer also testifies to the infrequency of contracted kidneys among drunkards.
37 Ziemssen's Cyclopædia of Medicine.
Fürstner detected by very exact testing a trace of albumen in the urine of almost all cases of delirium tremens examined. Its presence was, however, transient, and appeared to be not associated with structural changes in the kidneys.38
38 Berliner klin. Wochenschrift, 1876, No. 28.
Fatty infiltration and fatty degeneration of the kidneys occur in chronic alcoholism, the former as part of the general fat accumulation, the latter as a result of the general nutritive disturbances.
Amyloid degeneration is rare, and can in no case be ascribed to the direct action of alcohol.
Griesinger saw excessive diabetes insipidus follow a prolonged and severe attack of acute alcoholism in a man twenty-eight years old, and terminate fatally in the course of four months. Ebstein attributes the polyuria of acute alcoholism to lesions of the brain.
Glycosuria is rare among drunkards.
The Bladder.—Catarrh of the bladder is not rare in chronic alcoholism, especially in that form originating from excesses in malt liquors. This condition, however, scarcely occurs with sufficient frequency to be regarded as in any sense a symptom of alcoholism.
The Genital Organs.—The subjects of alcoholism are especially prone to sexual disorders of all kinds—a fact to be explained by the influence of alcohol on the imagination, and especially upon the sexual appetite, its debasing effect on the moral sense and upon the judgment, and the indifference to the consequences of exposure which it begets. In the later stages of chronic alcoholism sexual power is apt to be greatly enfeebled or wholly lost. This condition, which is usually attended also by loss of sexual desire, is to be attributed to the action of alcohol upon the nervous system rather than upon the sexual organs themselves. It has nevertheless been established that long-continued alcoholic excesses are apt to be followed by atrophy of the testicles. Lancereaux has described a condition of these organs resembling in all respects senile atrophy. On the other hand, Huss attributed the impotence of alcoholic subjects to loss of nervous tone. In the female, alcoholism produces disturbances of menstruation and premature menopause. Alcoholic excesses are said also to produce a liability to abortion, and Lancereaux has observed atrophy of the ovaries in alcoholic subjects.
2. Disorders of Special Structures.—a. Disorders of the Locomotive Apparatus.—The muscles at large, like the heart, are liable to fatty infiltration and degeneration. Fatty infiltration, frequent at some period in the course of the affection, is apt to be widespread. The muscles are paler than normal, softer in consistence, and streaked with fat. True fatty degeneration is less frequent, and apt to be localized. Here the muscular fibres lose their striation, and present within the myolemma minute fatty deposits in the form of granules. This change is accompanied by atrophy. The symptoms consist in feebleness and difficulty in movement and in locomotion.
Changes in the bones, notably enlargement of and increase in the contents of the medullary canal in the long bones, and arthropathies of various kinds, have been observed in alcoholic subjects.
[p. 615]b. Disorders of the Skin.—Alcohol is a sudorific, and is largely eliminated by the skin. This effect is purely physiological; therefore the moderate and occasional use of alcohol exerts an influence rather favorable than otherwise upon the tegumentary structures, but in repeated excesses it gives rise to more or less cutaneous irritation. The skin, partly for this reason, and partly because it shares in the general disturbance of nutrition, becomes dry, harsh, and scaly; after a time the face, and especially the nose and neighboring parts, assumes in many instances a violaceous hue, the minute superficial cutaneous veins are enlarged, and acne is common. The resulting appearance is almost characteristic of the habits of the individual. Alcoholic subjects frequently suffer from pruritis, urticaria, and eczema. In certain cases the skin, instead of being dry and harsh, is soft and unctuous, and in others, especially in the more advanced cases, it becomes slightly yellow or earthy in hue. Owing in part to changes in the nutrition, and in part to vascular dilatation, the skin of the extremities is not rarely mottled and cyanotic. In certain forms of alcoholism of the nervous system, and particularly in alcoholic paralysis, in which we have to do with multiple peripheral neuritis, the skin of the affected parts, especially that overlying the atrophied muscles, becomes, in consequence of trophic changes, dusky in color and hard, smooth, and glossy. It has been stated that chronic alcoholism is a cause of pellagra, and numerous observations have been advanced in support of this view (Hardy). The excessive rarity of this condition in countries in which the abuse of alcohol is most common renders it probable that the occasional association of these affections is accidental rather than causal. Chronic alcoholism predisposes to gangrene of the skin and to bed-sores; slight wounds readily inflame and are slow to heal; alcoholic subjects are especially predisposed to erysipelas, while the enfeeblement of the circulation and the lowered tone in the later stages of chronic alcoholism often result in œdema of the inferior extremities.
3. General Disorders.—In addition to the various local disorders thus far described, the prolonged excessive indulgence in alcohol leads to profound disturbances of the processes of nutrition, which are manifested in alterations in the blood, in excessive accumulation of fat, and in a well-marked cachexia.
a. The Blood.—The alterations in the blood, although sufficiently manifest in disorders of nutrition, have not yet been studied with satisfactory results. In chronic alcoholism the proportion of water is increased, while that of fibrin is diminished. After death the blood remains fluid. The red globules are diminished in number. The blood also contains free fat, to which it owes its pale, opalescent, and sometimes almost milky hue. The presence of fat has been demonstrated after the injection of alcohol into the veins of animals.
b. Obesity.—Fat-infiltration and fat-accumulation must be regarded as among the most characteristic disturbances produced by alcohol. Fat is abundantly stored up in the subcutaneous tissues. The anterior abdominal wall is especially liable to its accumulation. The heart, kidneys, omentum, and mesenteries are also not infrequently the seat of abnormally large accumulations of fat. Fat also collects in the muscles and in the intermuscular planes, but to a less extent. Obesity is not, however, so frequent in the advanced stages of alcoholism as it is while the subject [p. 616] has not yet lost the appearance of health, and in a large proportion of the individuals it does not manifest itself at all. It appears to depend largely upon the character of the drink, and is especially frequent among those addicted to excesses in beer. It is less common among wine-drinkers, and relatively infrequent and of moderate degree in those who confine themselves to spirits. A sedentary life, and perhaps also an hereditary tendency, exerts an important influence upon the development of obesity in alcoholism.
c. Alcoholic Cachexia.—The action of alcohol in excessive amounts upon the nutrition of the body at large, and in particular upon the nutrition of the nervous system, is radically unfavorable. This unfavorable influence manifests itself from the beginning, while the subject yet presents the appearance of health, and long before the occurrence of either the symptoms or physical signs of organic disease. The powers of resistance to unfavorable influences of all kinds are diminished; the ability to endure hardships, privations, and fatigue is lessened; sickness and injuries are badly borne; complications are frequent and grave; and convalescence is apt to be tardy and insecure. It is among the more striking peculiarities of the alcoholic subject that blood-losses are badly borne and slowly repaired. It is this want of tone, often latent for a long time under ordinary circumstances, which unfits those addicted to alcohol for Arctic and exploring expeditions and for military and scientific enterprises involving prolonged hardship and exposure. In the course of time disorders of the digestion, of hæmatosis, of circulation, increase the difficulty and render it more apparent. The fat now rapidly diminishes; anæmia develops; the complexion becomes dull, earthy, or slightly jaundiced, the tissues flabby. Then follow diarrhœa, hemorrhages from mucous surfaces, serous effusions, visceral congestions of high degree, hypostasis, œdema, and progressive deterioration of all the powers alike of the body and the mind until the dyscrasia is complete.
The subjects of chronic alcoholism are especially prone to affections of the respiratory tract and to the infectious diseases. They furnish, as a rule, the earliest victims in epidemics. They not rarely die of pneumonia. They develop troublesome delirium in simple maladies, and in all acute affections the prognosis is unfavorable as compared with that in persons of sober habits. As Clouston well says, “The whole organism suffers sanative and mental lowering, alteration of functions and of energizing.”
B. DERANGEMENTS OF THE NERVOUS SYSTEM: CEREBRO-SPINAL DISORDERS.—The disorders of the central nervous system in chronic alcoholism are even more numerous and more important than those already described. Many transient and permanent disturbances of function occur without anatomical lesions recognizable by existing methods of examination; many others are associated with readily-discoverable changes of structure. These changes are encountered in the blood-vessels, the meninges, the substance of the cerebro-spinal axis, and in the peripheral nerves. Much as they differ in appearance and in their clinical manifestations, they may all be referred to three processes: (a) congestion and inflammation; (b) sclerosis; and (c) stentosis.
1. Cerebral Disorders.—The Cranium.—The bones of the skull are often thicker and more dense than normal. This change implicates the [p. 617] diploë and the outer and inner tables. The last is then deeply channelled for the blood-vessels and deeply indented for the Pacchionian bodies, which are commonly hypertrophied.
The Vessels.—Disturbances of the cerebral circulation are among the earliest and most important symptoms. Due primarily to the increased action of the heart and vaso-motor dilatation of the blood-vessels excited by repeated large amounts of alcohol, and secondarily to permanent enlargement of the vessels in consequence of fatty or atheromatous degeneration of their walls, some degree of active or passive congestion is almost always present. It is probable also that in consequence of irregular and complex disturbances of the circulation secondary localized ischæmia occurs. Lentz states that anæmia is more common in the cerebral substance than in the membranes.
The capillaries are usually much altered—sometimes uniformly dilated to a considerable extent, sometimes forming capillary aneurisms. They are more sinuous than normal, their walls show evidences of fatty degeneration, and they sometimes contain minute thrombi. Extravasated blood, in the form of circumscribed collections, of diffuse layers, or finally of capillary hemorrhages, also occurs. These collections are sometimes free, sometimes encysted.
The Meninges.—The dura mater is congested; occasionally it shows more or less extensive areas of inflammation with exudation of lymph. Purulent exudation in the absence of traumatism is rare. The lymph may be deposited in the form of patches of varying extent, or it may form more or less extensive false membranes. These accumulations are of variable, often considerable, thickness, and constitute the condition described as pachymeningitis hæmorrhagica interna, or, from the large amount of blood which they contain, hæmatoma of the cerebral meninges. They occupy the convexity of the brain, and are developed upon the inner surface of the dura; they are usually nearly symmetrical in outline, but of different thickness upon the two sides. They consist of superimposed layers of lymph, between which, or within the substance of which, are more or less extensive blood-extravasations, either fluid, coagulated, or undergoing resorption. More frequently the exudation consists of mere shreds of lymph within the cavity of the arachnoid.
The arachnoid is almost invariably altered. Upon the convex surface of the hemispheres, especially along the median fissure, it is thickened and opaque. This condition may be uniform or distributed in patches, and is apt to follow the line of the blood-vessels.
The pia mater is congested, often œdematous, not rarely the seat of blood-effusions of greater or less extent.
The cerebro-spinal fluid is usually more abundant than normal, of a deeper color, cloudy, sometimes tinged with the coloring matter of the blood.
The Brain.—The intimate lesions of the substance of the brain are not yet known. The volume of the encephalon, as a rule, undergoes no change. Occasionally it appears to be swollen, and protrudes with some degree of force through the incision first made in the membranes. More commonly, the brain is throughout or in certain parts atrophied or shrivelled, its convolutions flattened, its surface retracted. This is sometimes the result of the pressure of collections of hemorrhagic or inflammatory products.
[p. 618]The consistence of the cerebral mass is sometimes increased; it becomes harder, more resistant to pressure, and preserves its form when removed from the cranium better than the normal brain. This condition may be present throughout the brain or it may be localized. In the latter case it is usually due to patches of sclerosis. Softening in more or less extensive areas may occur in the advanced stages of the more severe forms of chronic alcoholism. It is found chiefly in the gray substance, where the vessels are more numerous, especially in the cortex and central ganglia. In this as in other affections cerebral softening is the result of obstruction of the circulation in consequence of atheroma, thrombosis, or other change in the arteries. It varies from simple diminution in consistency to diffluence.
The nervous substance of the brain doubtless undergoes changes proportionate to the degree and duration of its exposure to an alcohol-charged blood. What these changes are has not yet been fully determined. The nerve-cells of the cortex have been found rounded and contracted, so that instead of being surrounded by a small lymph-space they seem to be lying in large cavities, and so granular that the nucleus can hardly be made out. Slight increase in the number of the small round cells in the cortex and in the adjoining parts of the white matter has also been observed (Hun). These changes are not, however, constant. Not only has the microscopical morbid anatomy of the lesions of nerve-substance peculiar to chronic alcoholism not yet been worked out, but even macroscopic changes adequate to account for symptoms that were during life serious, persistent, and apparently referable to well-defined lesions, are sometimes absent altogether.
It is important to distinguish the disorders due to the direct action of alcohol, which are often functional or dependent upon lesions too subtle for recognition, from those which are secondary and dependent for the most part upon coarser changes of structure.
In consequence of hyperæmia of the brain and its membranes there not infrequently occur a sense of confusion or dulness, increasing to headache, which may become almost unbearable, mental disturbances of the most varied character, disorders of movement and sensation, and disorders of the special senses.
Cerebral hemorrhage, to which the subjects of chronic alcoholism are, in consequence of the vascular lesions already described, peculiarly prone, manifests itself by the usual primary and secondary phenomena. Meningeal hemorrhage, save in the form of hæmatoma, is rare except in the advanced stages of paretic dementia.
The blood in alcoholic dyscrasia undergoes changes which favor its transudation through the walls of the vessels; hence a tendency to œdema and to accumulations in serous sacs. This tendency implicates the structures of the nervous system in common with the organism at large. The ventricles of the brain become distended with fluid, and the brain-substance itself and the meninges not rarely become œdematous in the last stage of chronic alcoholism, in consequence of grave disturbances of the circulation or as complications of affections of the lungs, heart, or kidneys. These conditions are attended by mental obscuration, somnolence alternating with sleeplessness, delirium, maniacal paroxysms, impairment [p. 619] of muscular power, of general and special sensibility, impaired reflexes, inability to speak, deepening stupor, and death.
2. Spinal Disorders.—Lesions of the spinal cord or its membranes have been rarely discovered. When present they have been invariably associated with similar or corresponding lesions of the brain or its envelopes. Leyden39 states that not only do the cerebral meninges present inflammatory changes in chronic alcoholism, but the meninges of the cord are sometimes found in an analogous condition; that pachymeningitis hæmorrhagica interna spinalis has also been observed, as well as other forms of spinal meningitis, with thickening and discoloration of the pia and dura; and that œdema of the pia has been especially noted. While anatomical lesions of the cord are less frequent than lesions of the brain, nutritive and functional disturbances, as manifested in the general symptomatology, are quite as common in one as in the other.
39 Klinik des Rückenmarkskrankheiten.
3. Disorders of the Peripheral Nerves.—Magnus Huss found no change in the peripheral nerves in five cases in which they were carefully examined. Lancereaux discovered degenerative changes in the peripheral filaments in alcoholic paralysis. Leudet found hypertrophy of the neurilemma and alterations in the cubital nerve in an individual suffering from chronic alcoholism in whom this nerve was paralyzed. Dejerine40 observed in two fatal cases of alcoholic paralysis neuritis of peripheral nerves with integrity of the nerve-roots, the spinal ganglia, and the cord. In one of Dreschfeld's cases of alcoholic paralysis,41 in which the cord was found perfectly normal, the “sciatic appeared thin and grayish, and was surrounded by a great deal of adipose tissue. Vertical sections showed, when treated with perosmic acid and stained afterward with picro-carmine, a moniliform appearance of the nerve-tubes, due to breaking up of the myelin; the nuclei were increased, and there was also some interstitial cell-infiltration. Transverse sections showed in some few places an increase in the diameter of the axis-cylinder, and again the interstitial infiltration.”
40 Archives de Physiologie nerv. et patholog., No. 2, 1884.
41 Brain, Jan., 1886.
Disorders of General Sensibility.—Disorders of general sensibility are among the earliest of the nervous phenomena of chronic alcoholism. They occur in the following order: hyperæsthesia, dysæsthesia, and anæsthesia. Disturbances of sensibility manifest themselves, quite independently of hallucinations, as sensations of malaise, of discomfort, of chilliness, of cramps, or of abnormal warmth or cold. Sometimes they amount merely to momentary discomfort, at other times to extreme pain. They are usually limited, often to the feet and legs, sometimes to the hands and arms; again, they are experienced in the trunk, and especially in the back. They are most common during the evening; less frequently they are induced by the warmth of the bed; and, again, they are experienced on rising. They are apt to be associated with occipital or frontal headache.
Among the most frequent nervous phenomena of chronic alcoholism are disturbances of sleep. Sleep is light, uneasy, and disturbed, difficult to obtain, troubled with dreams, and unrefreshing. More or less complete insomnia is by no means rare. It is more apt to occur, however, after acute exacerbations of alcoholism than in the ordinary chronic condition.
[p. 620]Hyperæsthesia manifests itself as an increased sensibility to pain, to mere contact, to temperature, and in an exaggeration of the muscular sense. Two general forms may be distinguished—the superficial and deep. The former usually manifests itself by an exaggerated sensibility of the skin, especially along the course of the superficial nerves and at their points of emergence from the deeper structures. The latter consists in a more or less intense sensation of pain, often diffuse, sometimes almost unbearable, and associated with a sensation of heat or cold, which is most commonly experienced in the lower extremities. It is often referred by the patient to the deeper muscles or to the bones and joints, and is increased by movement or pressure.
Anæsthesia is a much more common occurrence. It is usually developed during the later period of chronic alcoholism, and may implicate the skin, the mucous tissues, or the deeper structures. It presents all degrees from mere impairment to absolute loss of sensation. In the latter case, contact, pain, temperature, and electrical stimulation equally fail to excite sensation. In the deep anæsthesia of alcoholism pressure and electro-muscular sensibility are alike impaired. The muscular sense is also enfeebled or abolished. The regions which are the seat of anæsthesia are, as a rule, of a lower temperature than those in which sensation is normal. The anæsthesia may extend to the conjunctiva, and even to the cornea and to the mucous membrane of the mouth and throat. It has also been observed in the mucous membrane of the genitalia and at the verge of the anus.
Disorders of Motion.—Disorders of motion consist of tremor, subsultus, spasm, convulsions, muscular paresis, and palsies. Tremor is a very frequent phenomenon in chronic alcoholism. It consists generally of a series of rapid rhythmical movements. Sometimes the extent of the movement is increased and their rhythm irregular. They are then choreiform. The tremor may be continuous; much more frequently it only appears in the morning. The subject has then some difficulty in dressing himself, particularly in buttoning his clothing, in shaving himself, and in raising a cup to his lips. This symptom commonly ceases after the ingestion of a certain quantity of alcohol, only to return on the following morning or after a considerable period of abstinence. Voluntary movements intensify the tremor. It most commonly affects the upper extremities, next in frequency the muscles of the face, and finally the lower extremities. In rare cases it affects the muscles of the whole body. Alcoholic tremor affecting the hands and arms renders the subject awkward and interferes with his ability to work; affecting the lower extremities, it gives rise to an embarrassing, irregular gait; affecting the lips and tongue, it produces hesitation of speech or stammering, and when it is of a high degree articulation may be so imperfect that conversation is impossible; affecting the muscles of the eyes, it gives rise to nystagmus. Tremor is not infrequently associated with subsultus tendinum, spasmodic contractions, and cramps. These phenomena are usually localized, and affect by preference the muscles of the face and those of the lower extremities.
Loss of muscular power, which may pass, little by little, into complete palsy, also occurs. It is, however, neither constant nor proportionate to the gravity of the case in other respects. Whilst, as a rule, it is developed insidiously, it occasionally shows itself with suddenness. In the latter [p. 621] case it is usually preceded by some acute complication, and may disappear as quickly as it came. At first it is a mere feebleness, which, beginning in the fingers, extends to the hands and arms. It may after a time manifest itself in the feet. More or less muscular paresis is invariably associated with the tremor above described.
Alcoholic Paralysis.—The earliest account of alcoholic paralysis is that of James Jackson,42 who designated the disease, from its most prominent symptom, arthrodynia. He attributes it to ardent spirits, and chiefly observed it among women. “This arthrodynia comes on gradually. It commences with pain in the lower limbs, and especially in the feet, and afterward extends to the hands and arms. The hands may be affected first in some instances, but in all cases in the advanced stage of the disease the pain is more severe in the feet and hands than in the upper limbs. The pain is excruciating, and varies in degree at different times. It is accompanied by a distressing feeling of numbness. After the disease has continued a short time there take place some contraction of the fingers and toes and inability to use these parts freely. At length the hands and feet become nearly useless. The flexor muscles manifest, as in other diseases, greater power than the extensors, and the whole body diminishes in size, unless it be the abdomen; but the face does not exhibit the appearance of emaciation common to many visceral diseases. The diminution is especially observable in the feet and hands. At some time the skin of these parts acquires a peculiar appearance. The same appearance is noticed in a slighter degree in the skin of other parts. This appearance consists in great smoothness and shining, with a sort of fineness of the skin. The integument looks as if tight and stretched, without rugæ or wrinkles—somewhat as when adjacent parts are swollen. The skin is not discolored. In this disease there is not any effusion under the skin, and the character which it assumes arises from some change in the organ itself.”
42 New England Journal of Medicine and Surgery, vol. xi., 1822, “On a Peculiar Disease resulting from the Use of Ardent Spirits.”
Since Jackson's day, Huss, Lancereaux, Leudet, and others have described various forms of paralysis due to alcohol. Wilks43 under the term alcoholic paraplegia described a form of alcoholic paralysis of which he had seen numerous cases, especially in women addicted to alcoholic excesses. The symptoms are severe pain in the limbs, especially the lower ones, with wasting, numbness, anæsthesia, only slight power of movement or total inability to stand. The symptoms are not unlike those of ataxia. Wilks regarded the disease as due to degeneration of the cord and thickening of the membranes. Several of the cases terminated in recovery in a comparatively short time after the abrupt and complete withdrawal of alcohol. Since that time a number of cases have been reported by various observers.44
43 Lancet, 1872, vol. i. p. 320.
44 See, in particular, Hun, American Journal of the Medical Sciences, April, 1885, “Alcoholic Paralysis.” This paper contains a valuable résumé of the reported cases up to that time. Consult also Dreschfeld, Brain, July, 1884, and January, 1886.
Hun concludes that alcoholic paralysis may be regarded as a special form of disease with the following symptoms: “Neuralgic pains and paræsthesiæ of the legs, gradually extending to the upper extremities, and accompanied at first by hyperæsthesia, later by anæsthesia, and [p. 622] in severe cases by retardation of the conduction of pain. Along with these symptoms appears muscular weakness, which steadily increases to an extreme degree of paralysis, and is accompanied by rapid atrophy and great sensibility of the muscles to pressure and to passive motion. Both the sensory and motor disturbances are symmetrically distributed. The paralysis attacks especially the extensor muscles. In addition to these motor and sensory symptoms, there is also a decided degree of ataxia. The tendon reflexes are abolished, and vaso-motor symptoms, as œdema, congestion, etc., are usually present. Symptoms of mental disturbance are always present in the form of loss of memory or transient delirium.”
Lesions of the cord are absent, but degenerative processes in the peripheral nerves have been discovered in a number of cases. The symptoms are those of multiple neuritis, and the essential lesions consist in degenerative changes in the peripheral nerve-fibres. The associated mental derangement, tremor, and ataxia have been ascribed to changes in the cerebral cortex.
Dreschfeld has divided the cases, according to the more prominent symptoms, into two clinical groups—alcoholic ataxia and alcoholic paralysis.
The ataxic form represents a milder type. The symptoms are lancinating and shooting pains in the lower extremities, sometimes in the upper, with areas of anæsthesia and retarded sensibility. The muscles are painful upon pressure, and atrophy may be moderate or absent altogether. Inco-ordination is marked. The tendon reflexes are absent. Shooting pains down the legs to the toes of a paroxysmal character, and followed by a sense of numbness, also occur. Eye symptoms are wanting.
The paralytic form is usually associated with atrophy, affecting chiefly the extensors of the fingers and toes. The paralysis and atrophy in some cases come on acutely, in others more slowly. When the patients come under observation they are usually unable to stand or walk, and it is therefore not easy to make out whether or not the paralytic stage has been preceded by a stage of ataxia. As the sensory phenomena in these cases are the same as in the first group, it is probable that pseudo-ataxic symptoms have preceded the slowly oncoming paralysis. Paralysis and atrophy of the extensors of the fingers and toes, with paresis of the other muscles, are associated with the sensory phenomena above described. Tendon reflexes are absent; the superficial reflexes are much diminished. Recovery takes place in a considerable proportion of the cases upon the withdrawal of alcohol. The atrophy and paralysis pass away altogether, the tendon reflexes are restored, and the disturbances of sensation disappear. In the greater number of these cases persistent delusions are present.
Lancereaux45 describes alcoholic paralysis as symmetrical, affecting either the upper or lower extremities and gradually extending toward the trunk. The lower extremities are invariably more affected than the upper, and the extensor than the flexor muscles. There is diminished reaction to electricity, and anæsthesia is present. The brain and spinal cord are normal, but the peripheral nerves show extensive degenerative changes.
45 Gazette des Hôpitaux, No. 46, 1883.
4. Disorders of the Special Senses.—a. The Sight.—Disorders of vision [p. 623] are among the most frequent and the earliest symptoms of chronic alcoholism. Phosphenes, scintillations, sensations of dazzling, muscæ volitantes, and streams of light are often complained of. These phenomena may be constant or transient. Diplopia and other visual disturbances of the most irregular and annoying character also occur. Sometimes there is dyschromatopsia; the colors are confounded: red appears brown or black, and green appears gray, etc. In the more advanced stages amblyopia may occur. The acuity of vision rapidly diminishes, sometimes to the point that the patient with difficulty distinguishes the largest print. Objects appear as seen through a fog, and their outlines are distinguished only after repeated and close effort. Again, blindness almost absolute occurs for the course of some minutes—passes away rapidly, only to return again at intervals. Not infrequently the sight is better in the morning and evening than during the day. Achromatopsia, characterized by enfeeblement, and not infrequently by the momentary loss of the power to recognize colors, and particularly the secondary tints, also occurs. Cases of Daltonism occasionally seem to depend, to some extent at least, upon alcoholic disturbances of vision. Impairment of the power to distinguish colors must not, however, be confounded with the difficulty experienced by many alcoholic subjects in recognizing different colors successively presented to the eye with some degree of rapidity. Such individuals are able to distinguish colors when sufficient time is permitted them. Their difficulty depends upon tardiness of perception, such as is often experienced by neurasthenic subjects in recognizing faces in a crowd, rather than upon any failure in the power of recognizing colors. As a rule, the disorders of vision are not permanent, at least in the beginning. Later, they are of longer duration, and alcoholic amblyopia occasionally degenerates into irremediable amaurosis. Ophthalmoscopic examination reveals at first no appreciable lesion, and the disturbance of circulation, venous stasis, and peri-papillary infiltration thus observed appear to be inadequate to explain the visual disturbance. Atrophy of the optic nerve occasionally occurs as a direct result of alcoholism. Nystagmus has been frequently observed. The state of the pupils is variable and without constant relation to the acuity of vision. The pupils are not infrequently uniformly dilated, contracting slowly under the influence of light. More rarely they are permanently contracted; occasionally they are unequal. These modifications are often without demonstrable relation to anatomical lesions.46
46 Vide this System of Medicine, Vol. IV. p. 803.
b. The Hearing.—The disturbances of hearing encountered in chronic alcoholism are in many respects analogous to those of sight. Patients complain of curious subjective sensations, which are described as humming or whistling sounds, the ringing of bells, music, or the murmur of a crowd. At times the sense of hearing is so exquisite that the least noise causes pain. On the other hand, hearing may be greatly impaired, diminishing by degrees until it becomes in some cases, without recognizable lesion, almost or completely lost.
c. The Taste.—As a rule, the sense of taste is impaired in chronic alcoholism; occasionally it is wholly lost.
d. The Smell.—The sense of smell is in most cases to some extent, and in many cases greatly, impaired, the most powerful odors being scarcely perceived by old topers.
[p. 624]Alcoholic Epilepsy.—Alcohol, and especially that combination of alcohol with oil of wormwood and aromatics known as absinthe, is capable of producing convulsive seizures resembling epilepsy. Certain forms of alcoholic convulsions can scarcely be distinguished from ordinary epilepsy. Acute alcoholism may be an exciting cause of the convulsive seizures in an epileptic. Alcoholic epilepsy is, however, peculiar to chronic alcoholism, and particularly in individuals in whom there is an hereditary tendency to nervous disorders. Once established, alcoholic epilepsy may continue even after the alcoholic habit has been discontinued. The attack is usually followed by marked mental disturbances. These vary from profound dulness to stupor or mania; they last from some hours to several days, and present the characters of similar conditions following non-alcoholic epileptic paroxysms.
C. PSYCHICAL DERANGEMENTS.—Yet more important than the visceral and nervous lesions of chronic alcoholism are the indications which it affords of a progressive debasing influence upon the mind. The moral sense, the will, and the intellect are involved successively in a process of deterioration, which, manifesting itself only in part and by little at first, becomes after a time general and plain to all the world, and ends at length in ruin more complete and more hopeless than that of the body. Indeed, it not infrequently happens that while the general health appears to be good and the nervous system, save in transient disturbances of function, presents no evidence of the toxic action of alcohol upon its tissues, serious psychical disorders are established. The alcoholic subject develops propensities, otherwise latent, that tend to refer him to the criminal or the insane classes of society. The psychical debasement, of which these propensities are the outcome, is, like the alcohol habit itself, progressive. This fact cannot be too strongly insisted upon. Like the loss of vascular tone, the sclerosis, the steatosis which alcohol induces in the body, this mental deterioration is cumulative and destructive. It is to its psychical manifestations that alcoholism owes its chief importance, not only as a study in pathology, but also as a problem of the gravest moment in social science.
1. The Moral Sense.—Deterioration of the sense of moral obligation is among the earlier of the mental phenomena of alcoholism. The moral sense is perverted and enfeebled. Sentiments of honor, of dignity, of reputation, and of decency are no longer cherished or regarded. The amenities of social life and the proprieties of personal conduct are disregarded or set at naught. He who was punctilious, considerate, and thoughtful becomes negligent, selfish, and indifferent to sentiments of honor and emulation; he gives himself up to indulgences formerly considered unworthy; his reputation and that of his family are no longer matters of concern to him; respect for public opinion is replaced by cynicism. Little by little the conception of duty, of justice, of honor are lost to him, or if he regards them at all it is rather as subjects for idle and purposeless discussion than as motives to regulate his life. These changes are gradual and progressive, their evolution being largely influenced by the hereditary traits and previous moral culture of the individual. The deterioration of the sense of right, and the coincident exaltation of those passions which are normally under its control, lead to the commission of the crimes peculiar to the early period of alcoholism. [p. 625] Indifference is another characteristic of this period—indifference not incompatible with a selfishness of the most intense kind. The sense of obligation to the family is forgotten, and the responsibility of providing for and caring for others is unfelt. If the drunkard's own wants, and especially his craving for drink, are gratified, the necessities of those formerly dear fail to move him. The affections are not only enfeebled, but they are also perverted; not rarely they are replaced by aversion, disdain, and hatred. The individual who has been calm, reasonable, and patient becomes excitable, perverse, and intolerable of contradiction or opposition. Prone to acts of sudden violence, he becomes gloomy, taciturn, and preoccupied. He is disturbed by fixed tormenting ideas or by vague pursuing terrors. He thus becomes self-conscious, irritable, fault-finding, and easily provoked to passion. The character, after a time, undergoes still more decided change: alternations of indifference and irritability characterize his varying moods. After a time the joys and the sorrows of life alike fail to provoke real feeling. At length the confirmed sot manifests moral traits that are simply infantile; he laughs without motive, he weeps without cause.
2. The Will.—At the same time the will undergoes an enfeeblement even more marked. Except in paroxysms of transient excitement it is feeble and uncertain. The subject of chronic alcoholism scarcely knows his own mind under ordinary circumstances. Aware of his duties and his obligations, he is unable to discharge them. Especially does he lack the power to say No. Vacillation, indecision, and dependence upon others become characteristic traits. This loss of moral energy, combined with the loss of physical power brought about by continued and repeated excesses, begets at once a distaste for the ordinary occupations of life and an inability to perform them.
3. The Intellect.—Loss of intellectual power comes last. In some cases it shows itself only after the most prolonged excesses, when the body itself is becoming thoroughly broken down. Exceptionally, fitful intellectual power is curiously sustained to the last. The first evidence of intellectual failure consists in diminution of vivacity and readiness. The intellectual state is marked by apathy, obtuseness, and indifference; mental processes are performed slowly and with difficulty. This is perhaps one of the causes of the mental indolence characteristic of alcoholism. After a time the drunkard becomes timid, loses confidence in himself, and is unwilling to engage in enterprises demanding mental effort. Some tardiness of appreciation then shows itself; conversation becomes difficult; ideas are not spontaneous, but must be sought for; replies are not made with the usual promptness; it is difficult to arouse and fix the attention. The sense of self-respect is now lost, and it is almost impossible to make the subject comprehend his degradation. The intellectual deterioration becomes more and more marked. The memory fails little by little and becomes treacherous. Names and dates are recalled with difficulty. The conversation is interrupted by an inability to choose the proper words with precision, hence hesitancy, interruptions, and various forms of circumlocution. The power of argument and of reasoning is now much impaired, the judgment is uncertain, the association of ideas is inexact, and at length the intellectual degradation attains a degree that unfits the subject for the ordinary relations of life.
[p. 626]The above-described derangements of the viscera, of the nervous system, and of the mind are the morbid phenomena induced by long-continued excesses in alcohol. Whether merely functional or dependent upon recognizable anatomical lesions, they indicate pathological changes in the organism which are radical, and which under the influence of the continuously acting cause are progressive. Taken together, they constitute the condition known as chronic alcoholism. In view of the familiar experiences of every-day life, it is hardly necessary to repeat that these derangements are manifested in all degrees of intensity and in the most variable and complex combinations. The specific nature of chronic alcoholism is, in truth, due not to the derangements themselves, the greater number of which are such as we may encounter in morbid states not occasioned by alcoholic excesses, but to the combinations in which they occur in consequence of the action of the specific cause upon the organism as a whole. The prominence of particular symptoms or groups of symptoms in any given case is to be accounted for largely, if not wholly, by individual peculiarities.
Chronic alcoholism, however latent it may be, however sedulously concealed, warps the life of the individual in all its relations. In its advanced degrees it amounts to mental and physical dyscrasia. Between these extremes is every grade of incapacity and degradation. It is beyond the scope of this article to discuss the moral, social, or medico-legal bearings of this condition. Its purely medical relations are sufficiently obvious from what has gone before. It has been the writer's aim to make clear the existence and nature of the continuing condition.
It remains to describe certain other psychical disturbances which occur in chronic alcoholism, and which require separate consideration for the reason that they are accidental rather than essential, many cases running their course without their manifestation.
4. Alcoholic Delirium in General.—True alcoholic delirium, presenting the traits about to be described, is never the result of the direct primary action of alcohol upon the nervous system. Transient excesses produce acute alcoholism, drunkenness, which, varied as its manifestations are, differs essentially from that peculiar delirium which occurs only in individuals in whom the nervous system has undergone those nutritive changes that are brought about by prolonged alcoholic saturation.
The most striking peculiarity of this delirium relates to the hallucinations which attend it. These are almost invariably visual; occasionally they are also auditory. Their objects, whether men, animals, or things are in constant and unceasing motion, appearing and disappearing, coming and going, and changing from place to place with extreme rapidity. In this respect they differ from the hallucinations of other forms of delirium, of which the objects are fixed and more or less permanent. As a result of this peculiarity, the objects of alcoholic delirium are almost invariably multitudinous, as swarms of vermin, herds of animals, multitudes of demons, and the like.
A second peculiarity is the restlessness of the delirium. The patient is invariably uneasy, apprehensive, always on the alert, declaring that some calamity threatens him or that some evil is about to befall him. In consequence of these apprehensions even momentary repose is wanting. If he lies down for a moment, it is only to rise again and peer under the bed [p. 627] or into the corners, turning his head from side to side in search of some realization of the fears that torment him. This sense of apprehension impels the patient to hurry ever onward from place to place in search of the repose which he nowhere finds. It is increased to positive terror by the ever-varying and constantly-renewed hallucinations which torment him, and from which he seeks to escape, no matter how great the obstacles to be overcome.
A third peculiarity of alcoholic delirium is insomnia. This condition is of the must marked and stubborn character, even continuing for several days in succession.
5. Delirium Tremens.—This is the characteristic form of alcoholic delirium, and, as is indicated by the name, is invariably accompanied by tremor. It must be looked upon as an episode or epiphenomenon of chronic alcoholism. It is rare that even prolonged temporary excesses in persons ordinarily sober are followed by delirium tremens. Such excesses in the subjects of chronic alcoholism are, however, perhaps the most common cause of this condition. Orgies, especially when associated with venereal excesses, very frequently terminate in delirium tremens. Occasionally also, but much less frequently than was formerly supposed, the abrupt discontinuance of alcohol is followed by the outbreak. Other exciting causes are violent emotions, as anger or fright; hardships, such as prolonged hunger, over-exertion, or watching; acute maladies, as pneumonia, dysentery, erysipelas, the exanthemata, or rheumatism; finally, serious traumatisms, with or without great loss of blood. Delirium tremens usually occurs in those addicted to the abuse of spirits, less frequently in beer-drinkers, and comparatively rarely in those whose excesses have been restricted to wine. The attack does not, as a rule, begin abruptly; its prodromes usually consist in an exaggeration of the previously existing symptoms of chronic alcoholism. The patient complains of malaise, restlessness; he becomes depressed, morose, anxious without cause, apprehensive of some calamity, or he is more impatient and choleric than before. The ability to apply himself to his ordinary occupations is lost. He complains of vertigo, ringing in the ears; sleep is disturbed, or there is already insomnia. At the same time the stomach is deranged, appetite is lost, the tongue is covered with a thick yellowish-white fur, and there is constipation or diarrhœa. The period of prodromes may last from a few days to a week.
The outbreak is characterized by delirium, without, at least in the greater number of cases, absolute loss of consciousness. That is to say, it is possible by addressing the patient with energy or by strongly arousing his attention to interrupt the delirium and for a moment recall the patient to himself. In the graver cases, however, loss of consciousness appears to be complete. The subjective impression of the delirium, as recollected at the termination of the attack, is that of a sense of overwhelming confusion and inability to recollect or co-ordinate the ideas that were crowding upon the brain. The hallucinations, as has already been indicated, relate almost exclusively to the organ of sight, more rarely to the hearing; also, and exceptionally, to the other organs of sense. They are almost always either terrifying or repugnant. The objects of the hallucinations of the sight have already been described. They consist of animals, serpents, and monsters, which crowd into the apartment, coming [p. 628] usually toward the patient, disappearing in the walls, in the floor, under the bed, or among the bed-clothing. These visions are usually aggressive, threatening the patient, throwing themselves upon him, striking him, or tearing at his vitals. They are sometimes replaced by phantoms, spectres of the most horrible character, skeletons, death's-heads, or by flames which surround the patient and threaten to consume him. Sometimes the hallucinations relate to the daily occupation of the patient, and he pursues his tasks with a feverish and distressing anxiety. These hallucinations are almost invariably of the most fleeting, incoherent, and variable kind.
Auditory hallucinations occur usually in individuals of marked neurotic tendencies. They are apt to be more coherent than the hallucinations of vision, and are often of the nature of those which occur in the delirium of persecution. Sometimes they consist of cries, of chiding, of menacing voices, of the repetitions of obscene words and suggestions; sometimes they are cries of horror or the roars of animals, sometimes explosions or the discharge of firearms; or, again, they are terrifying threats. Hallucinations of taste and smell are much more rare, and occur in the subacute forms of delirium tremens. The patient complains of annoying odors or disagreeable tastes, either constantly present or upon the taking of food or drink. Disturbances of general sensibility show themselves in hallucinations in regard to sensations of pricking, burning, or tearing of the surface of the body, or of animals or vermin crawling over the patient. Hallucinations relating to the sexual instinct are far from rare. The hallucinations of every form are apt to be more frequent and more troublesome during the night than during the day.
Restlessness, fear, and anxiety are characteristic phenomena of delirium tremens. The patient is not only terrified by the imaginary objects which surround him, but often in their temporary absence he experiences an equal degree of fear for which he can assign no cause. It is to this condition of apprehension that is due the desire to escape from his present surroundings which is so characteristic of the delirium in question. Under its influence the patient occasionally commits acts of violence of the most serious kind. Sometimes the delirium is more quiet: the patient converses with individuals whom he supposes to surround him; he busies himself with his familiar occupations, giving orders, directing work, dictating letters, and arranging his affairs. At other times the delirium takes the form of apprehension of poisoning, and food and medicine are alike stubbornly refused.
The countenance, as a rule, is animated, the eyes brilliant and injected, the look fixed or peering, but always eager, or the expression may be haggard and agitated. The physiognomy, although largely influenced by the character of the delirium, may be said to be in most cases characteristic.
Sensation is usually impaired; especially is this true of sensibility to pain.
Tremor, although occasionally slight, may be said to be never wholly absent. Sometimes it affects the muscles of all parts of the body; more commonly it is limited to the hands, arms, tongue, and lips; less frequently it manifests itself in the lower extremities. Slight tremor may be increased by causing the patient to hold his hands extended with the [p. 629] fingers separated. The movements of the hands consist of rapid rhythmical oscillations of nearly equal extent and duration. The tongue is protruded with a rapid jerking movement, and withdrawn with equal suddenness. It shows fibrillar trembling. The trembling is increased by voluntary movement, and is ordinarily associated with some loss of motor power. The gait is often hesitating and awkward; movements of the upper extremities are executed with difficulty, and speech is irregular and interrupted. The motor disturbances are occasionally associated with choreiform movements or actual epileptic convulsions.
Insomnia is a constant condition. It usually persists throughout the attack, and occasionally proves troublesome for several weeks after convalescence is in other respects complete.
In the absence of pulmonary complications the respiration is not disturbed, save as a result of the restlessness and physical effort which sometimes quicken it. The same statement is true of the pulse. The action of the heart is usually enfeebled, and the first sound weak. The temperature is normal. The skin is frequently bathed in copious perspiration. There is complete loss of appetite, and in most cases inability to retain food. Thirst is constant, often tormenting. The tongue is sometimes moist, and coated with thick white or yellow fur; sometimes hard and dry, sometimes red. The urine is scanty, dark-colored, and sedimentary. It occasionally shows traces of albumen. Constipation is the rule.
The duration of delirium tremens is from three to seven, or even ten or twelve, days. The course of the attack is paroxysmal or remittent. The symptoms usually undergo some improvement during the day, only to become more urgent at night. The periods of remission are occasionally marked by transient slumber; the recovery by prolonged and deep sleep. But this is by no means the rule. Several varieties of delirium tremens have been described by writers upon the subject. These are—the grave form, characterized by violence of the motor disturbances, aggravated delirium, and gravity of the general condition; the febrile form, in which after the third or fourth day the temperature, without pulmonary or other discernible complications, suddenly rises to 104° F. or beyond that point, with great aggravation of the general symptoms; the adynamic form, marked by failing heart-power, feeble or imperceptible pulse, profuse sweats, collapse, stupor, which deepens into coma and ends in death; and finally, the subacute form. Here the patient is quiet, but restless. The delirium scarcely passes beyond the limits of occasional wandering, and relates chiefly to matters connected with the daily interests and occupations of the patient. Tremor is more or less marked, and sleeplessness is stubborn.
The termination of delirium tremens is in—1, recovery; 2, in death; 3, in the chronic form; and 4, in other forms of insanity.
1. Recovery.—Except in the grave forms recovery may be said to be the rule. Occasionally ushered in by a prolonged, almost critical, sleep, more frequently it takes place by gradual improvement. In the latter case the remissions are more and more prolonged, and attended by increasing repose alike of body and of mind, and by tendency to sleep. The hallucinations become feebler and less tormenting, at length recurring only in the evening or at night, and especially as the patient is about [p. 630] falling asleep. The anxiety and restlessness grow less urgent, consciousness becomes more secure, the trembling diminishes, and recovery is slowly established. The tremor is apt to persist some days into convalescence.
2. Death.—This mode of termination is not very common in the ordinary forms of delirium tremens. In the grave forms it is usual, sometimes occurring suddenly, sometimes gradually from intensification of the symptoms and failure of nervous power; or it may occur in consequence of pulmonary, cerebral, or renal complications; finally, the fatal termination is often due to the acute disease or the traumatism by which the delirium tremens has been excited, and of which it is, in fact, a complication.
3. Chronic Delirium Tremens.—This mode of termination, described by Lentz, is rare. The acute phenomena subside; the restlessness and the mental agitation diminish. Insomnia gives place to sleep, which is light and disturbed by dreams and nightmare; most of the hallucinations lose their activity and frequency, and finally disappear. The changing delirium settles into a fixed delirium of persecution; the tremor, while it becomes fainter, persists, and the condition is permanent.
4. Other Forms of Insanity.—This mode of termination has been studied especially by Magnan, who has classified the cases of delirium tremens into three different groups, according to their tendency to recover or to the development of mental alienation. The first group includes those cases which run a favorable course and terminate in complete convalescence; the second group, those cases in which the convalescence is prolonged and characterized by repeated relapses; the third group is composed of cases which likewise show a strong tendency to relapse, but in which the delirium continues after the other active symptoms have subsided. This form shows itself most frequently among the subjects of hereditary alcoholism. After repeated attacks the delirium becomes chronic. Morbid mental phenomena replace or accompany symptoms more directly referable to organic disturbances of the nervous system. Tremor gradually diminishes and disappears, the gastric symptoms subside, insomnia passes away, even hallucinations disappear, or at all events become infrequent; but the delirium which developed coincidently with these symptoms continues, and finally becomes chronic, losing to a great extent its original characteristics and constituting a form of insanity. Finally, dementia constitutes an occasional mode of termination in delirium tremens. It does not often develop immediately, although cases of this kind have been recorded. More commonly, the alcoholic subject, losing little by little his mental activity after each attack of delirium tremens, subsides by degrees into absolute and irremediable dementia. Paretic dementia may also develop after prolonged alcoholic excesses characterized by repeated attacks of delirium tremens.
The anatomical lesions after death from delirium tremens shed no light on the pathogenesis of the condition. Meningeal congestion, œdema of the pia mater and of the cortical substance of the brain, scattered minute extravasations of blood, and some augmentation of the cerebro-spinal fluid have been observed. In the greater number of cases no lesions whatever beyond those characteristic of chronic alcoholism have been discovered.
[p. 631]6. Alcoholic Insanity.—Among the psychical derangements, it remains to notice briefly the more prominent forms of insanity which develop in the course of chronic alcoholism, in consequence either of hereditary or of acquired morbid mental tendencies. These are—a, melancholia; b, mania; c, chronic delirium; d, dementia; e, paretic dementia.
Alcohol is the most common of all the causes of insanity. Clouston47 estimates that from 15 to 20 per cent. of the cases of mental disease may be put down to alcohol as a cause, wholly or in part. Those forms of insanity in the production of which alcohol is merely an occasional cause are not, however, properly included in the group of alcoholic insanities. Still less are we to include in this group cases of symptomatic dipsomania; that is to say, cases of insanity in which morbid impulse to drink constitutes a prominent symptom of the prodromic or fully-developed periods of various forms of mental disorder.
47 Clinical Lectures on Mental Diseases, Am. ed., 1884.
Alcoholic insanity manifests itself as an outcome of chronic alcoholism, just as epileptic and hysterical insanity show themselves as the outcomes of epilepsy and hysteria. This group properly includes various forms of mania-a-potu, especially the maniacal form of acute alcoholism, delirium tremens, and other transitory psychoses which occur in acute and chronic alcoholism.
In truth, the mental derangements of ordinary drunkenness constitute in many cases a form of transient insanity. These forms, have, however, already been considered at sufficient length. Dipsomania, for reasons already stated, cannot be regarded, either in its symptomatic form or in its essential form, as belonging to the group of alcoholic insanities.
a. Melancholia.—Melancholia is the most frequent form of true alcoholic insanity. It may begin abruptly or gradually, with changes of character, vague disquietude, great irritability, and disturbances of sleep amounting in many cases to insomnia. Hallucinations of hearing are characteristic. In this respect the morbid mental condition in question is in strong contrast with delirium tremens, in which the hallucinations are principally visual. The hallucinations of hearing usually consist of accusing or threatening voices. These voices inform the patient that he is to be poisoned, assassinated, murdered, or that outrages of all kinds are to be committed upon him; they accuse him of murder, of robbery, of rape, and of other shameful crimes. Præcordial distress is also apt to be present. In consequence of these hallucinations of hearing the patient falls into a profound melancholia, often characterized by suicidal impulses which are sometimes the direct outcome of hallucination, at other times blind and unreasoning. There is apt to be cephalalgia and insomnia. Trembling is not usually a marked symptom. Local anæsthesia and hyperæsthesia, if they occur, are transient. The ordinary duration of this form of alcoholic melancholia is much longer than that of delirium tremens, sometimes extending throughout several months. The termination usually is in recovery, less frequently in chronic delirium.
b. Mania.—This form of alcoholic insanity is characterized by various hallucinations which present peculiar characters. Thus, the hallucinations of vision commonly relate to supernatural apparitions, attended with luminous phenomena of various kinds. These visions may be [p. 632] occasional or they may be frequently repeated, or the hallucinations may consist of images of emperors, kings, princes, and potentates, or of military chieftains, in the midst of whom the patient passes his existence. Or, again, the hallucinations may be made up of historical scenes, pageants, the movements of armies, battles, and the coronations of kings, or they may be landscapes pleasant to the eye—snow-clad mountains, valleys filled with flowers, magnificent forests, and the like. These phantasmagoria are by no means fixed; on the contrary, they are of the most shifting character.
Auditory hallucinations are even more frequent, and quite as changeable. They bear a more or less well-defined relationship to the hallucinations of vision. They consist not rarely of promises of money, honors, titles, and the like. Sometimes they are voices from heaven, even the voice of God himself, commanding the patients to perform definite acts and promising in return equally definite blessings.
Hallucinations of general sensibility occur much less frequently. When present, they consist of various painful sensations, giving rise to the delusions of blows, stabs, bites of animals, electrical discharges, etc. In consequence of these hallucinations the delusions are often of a grandiose character. Patients believe themselves to be God, the pope, or some great potentate, or enormously rich, etc.
The somatic condition depends upon the degree of chronic alcoholism existing at the time of the manifestation of the mania. There are usually marked tremor, hesitation and uncertainty of speech, stubborn sleeplessness. Acute mania may show itself abruptly, attaining its full development in the course of a few days, or the development may be gradual. The prognosis in alcoholic mania is unfavorable; recoveries are rare. The fatal termination is sometimes the result of the maniacal condition itself, and sometimes the result of visceral complications. This form of insanity occasionally terminates in chronic delirium.
c. Chronic Delirium.—This form of alcoholic insanity is one of the terminations of acute alcoholic melancholia and of acute alcoholic mania. It is also one of the results of repeated attacks of delirium tremens. Finally, it may develop independently of these affections.
Developing independently, chronic delirium is usually of rapid invasion, and is characterized by the prodromes common to the various forms of alcoholic insanity—irritability, headache, vertigo, insomnia, etc. Hallucinations of hearing are very common, and relate principally to the sexual life of the patient. Voices taunt him with the fact that he is maimed or impotent; he hears persons whispering that he is about to be castrated or that he is the subject of loathsome venereal diseases, or they declare that he is known to be addicted to vile crimes and bestiality. Hallucinations of sight are much less common; those of the other special senses occasionally occur. The delirium takes the form of delusion of persecution. The patient believes himself the object of plots and conspiracies; his enemies are seeking to ruin his good name, to tarnish his reputation, to poison him. They put filth in his food or charge him with electricity; they steal away his vital force or his sexual power; they taunt him; they mock him; they beat him and rob him.
A delusion so frequent as to be almost characteristic of chronic [p. 633] alcoholic delirium relates to marital infidelity.48 The patients cherish unjust and often absurd suspicions of the virtue of their wives. These delusions arise independently of hallucinations either of sight or hearing, and are of the greatest importance, because they supply logical motives for the most appalling and brutal crimes.
48 “The combination of a delusion of mutilation of the sexual organs with the delusion that the patient's food is poisoned, and that his wife is unfaithful to him, may be considered to as nearly demonstrate the existence of alcoholic insanity as any one group of symptoms in mental pathology can prove anything” (Spitzka, Insanity, N. Y., 1883).
Alcoholic delirium differs in the transitory and incoherent character of its delusions from ordinary chronic delirium, in which the delusions are much more apt to be fixed and permanent.
d. Dementia.—This is a common terminal condition of alcoholism. It may develop, without the intervention of other forms of mental disease, in the course of chronic alcoholism as a mere intensification of the intellectual and moral degradation of that condition. This is especially liable to occur in hereditary alcoholism. Dementia also closes the scene in a considerable proportion of cases characterized by repeated attacks of delirium tremens. It likewise constitutes the terminal condition in other forms of alcoholic insanity.
The symptoms are sometimes so slight as to escape ordinary observation. More commonly they are fully developed. As compared with ordinary dementia, they present but little that is characteristic. Alcoholic dements are perhaps more filthy and more difficult to manage, duller and more mischievous, than others. Their somatic disorders are more marked. In them hyperæsthesias are replaced by anæsthesias; sleep is apt to be irregular and disturbed; the hallucinations characteristic of the antecedent alcoholic psychosis now and then reappear. Slowly-developing failure of intellect, forgetfulness, stupor, end in more or less complete loss of mental power. Nevertheless, a small proportion of the milder cases are capable of arrest under treatment.
e. Paretic Dementia.—Alcoholism is an important etiological factor in the production of this condition. The intellectual disorders and motor disturbances which characterize it, varied as they are, are associated with cerebral lesions, and especially with lesions of the cortex equally varied—lesions which are common in chronic alcoholism. These lesions vary from meningeal congestion and inflammation to profound inflammatory and degenerative alterations in the cerebral substance.
Paretic dementia may develop after long-continued excesses without previous appreciable mental or cerebral symptoms. In such cases it presents no specific indications of its alcoholic origin. The difficulty of determining the influence of alcohol in its causation is increased by the fact that alcoholic excesses—symptomatic dipsomania—are frequent in the prodromic and early stages of this form of mental disease. Paretic dementia may also develop after repeated attacks of delirium tremens. Here the early attacks end in recovery apparently complete; later, the convalescence is unsatisfactory and prolonged, leaving some indications of intellectual enfeeblement, which, after renewed attacks, increases, and is accompanied by delusions of grandeur, embarrassment of speech, unequal dilatation of the pupils, and general paresis. The prognosis is practically hopeless.
This term has been used in a somewhat vague manner to designate the morbid tendencies and pathological conditions directly transmitted by alcoholic subjects to their offspring. Chronic alcoholism on the part of one or both parents may be followed by morbid manifestations in the child. The hereditary transmission of the effects of alcoholism has been recognized from remote antiquity. Aristotle believed that a woman given to drunkenness would bear children with the same tendency. Plutarch affirms that the children of drunkards will abandon themselves to the same vice. Hippocrates speaks of the distressing effects of drunkenness upon the product of conception. Bacon states that many idiots and imbeciles are born of drunken parents. In more recent times the fact has been generally recognized that many maladies caused by the abuse of alcohol are liable to be transmitted to succeeding generations, and that alcoholism may in this way, in the course of two or three generations, lead to the complete extinction of families. Alcoholism on the part of the parents certainly exerts an unfavorable influence upon the health of their children, who are especially disposed to cerebral congestion, hypochondriasis, intellectual feebleness, and insanity. Two forms of hereditary alcoholism have been recognized: First, that in which the disease or defect of the parent is transmitted to the offspring; and second, that in which the disease or defect is not directly transmitted to the offspring, but a morbid tendency which manifests itself in diseases or defects of a different kind.49
49 1. Heredite de similitude, Alcoolisme hereditaire homotype; 2. Heredite de transformation, Alcoolisme hereditaire heterotype.
1. The appetite for strong drink is frequently transmitted from parents to the children, just as other traits of the mind or body. Sometimes it develops early, sometimes late in life; as a rule, however, this hereditary propensity shows itself at an early age, and is apt to be intensified at the time of puberty and the menopause. Objections have been urged against the theory of hereditary alcoholism. Among these the strongest is perhaps that the taste for drink in the offspring of alcoholic subjects is the result rather of opportunity and example than of heredity. The frequency with which alcoholic tendencies develop themselves in children reared and educated away from their parents, and the number of cases in which these tendencies show themselves only at an advanced period of life, long after the influence of example in childhood has ceased, sufficiently disprove this assumption. The hereditary influence does not, however, invariably manifest itself in the desire for drink. On the contrary, not rarely it consists in feebleness of nervous constitution, characterized by irritability, want of mental repose, or a restless or vicious disposition which demands constant excitement. Hence such individuals, although intellectually well developed, are often scarcely more than moral imbeciles, in whom the passion for drink may be replaced by the opium habit, addiction to gaming and to other vices, and whose career is shaped largely by an inordinate and insatiable craving for excitement of all kinds. Hereditary alcoholism follows the laws of heredity in general. The tendency may be transmitted directly from one generation to another, [p. 635] or may skip one or more generations, taking in the intermediate periods some different form.
2. The second variety is that in which the symptoms of chronic alcoholism are manifested in the offspring in the absence of the direct action of alcohol; that is to say, not the taste for alcohol, but the results of the gratification of that taste are transmitted, just as epileptic or hysterical patients may transmit to their offspring epilepsy or hysteria; thus it is not rare to encounter in the descendants of alcoholic parents perverted sensation, both general and special, hyperæsthesia, anæsthesia, flying neuralgias which do not always follow the course of particular nerves, but frequently affect in a general way the head or the members or manifest themselves as visceral neuralgias. These persons are much troubled with headache from slight causes and with migraine. Nor are disturbances of vision rare, nor vertigo. Insomnia is also frequent in such individuals, and augments the other symptoms. Digestive troubles also frequently occur, notwithstanding a regular and perfectly temperate life. Such persons are often subject to hallucinations of sight and hearing, and are liable to have delirium in trifling illnesses.
The second form of hereditary alcoholism manifests itself in a wholly different manner. The descendants, without a special appetite for strong drink, and in the absence of the special morbid manifestations above described, are singularly liable to mental and nervous diseases of various kinds. Among these convulsions and epilepsy are especially frequent; hysteria and various forms of insanity also occur. In this group of cases we find every degree of arrest of intellectual development, from mere feeble-mindedness to complete idiocy. As manifestations of the influence of alcoholism upon the offspring may be cited certain moral peculiarities otherwise inexplicable, such as are seen in children who at a very tender age show themselves vindictive, passionate, and cruel, to whom the sufferings of others afford pleasure, who torment their companions and torture their pets, and show precocious vicious tendencies of all kinds. Later in life these persons become lazy, intolerant of discipline, vagabonds, unstable of character, without the power of application and without moral sense. Given to drink, defiant of law, they constitute the great body of tramps, paupers, and criminals. The children of alcoholic subjects are often feeble and puny, pale, badly nourished, and curiously subject to morbid influences.
Dipsomania, which has also been described under the term oinomania, is rather a form of insanity than of alcoholic disease. The characteristic symptoms are, however, in the greater number of instances, due to indulgence in alcohol. The subjects of this affection usually belong to families in which insanity, and especially this particular form of insanity, is hereditary.
There are two forms of dipsomania—the essential and the symptomatic. Of these, the latter is the more frequent. Its consideration requires in this connection very few words. It manifests itself by an irresistible desire on the part of many insane people for alcohol. It occurs both in [p. 636] the prodromic and in the fully-established periods of insanity. It is especially common in various forms of mania and in the prodromic periods of general paralysis. The dominating influence in essential dipsomania is heredity. Occasional causes may bring on particular attacks, but their influence is secondary. Dipsomania cannot be looked upon as a distinct recurrent affection in an otherwise healthy person. At some period in their lives, and often long before the occurrence of characteristic paroxysms, dipsomaniacs show peculiarities indicating defects of mental organization. Certain symptoms of dipsomania are often mistaken for its cause. Thus, dyspepsia is more frequently an effect than a cause of the alcoholic excesses. The despondency, irritability, restlessness, hysterical manifestations, and insomnia which precede the attack are not the cause of it: they are its earliest symptoms.
The affection usually begins insidiously and is progressive. As a rule, although not always, it begins in early adult life. The manifestations of this disease are essentially intermittent and paroxysmal, but the impulse to drink must be regarded as a symptom which may be replaced by other irresistible desires of an impulsive kind, such as lead to the commission and repetition of various crimes, as the gratification of other depraved appetites, robbery, or even homicide. The paroxysms are at first of short duration, and are followed by return to the previous regular and decent manner of life. They become, however, by degrees, more violent and more prolonged. At first lasting for a few days or a week, by and by they extend to periods of a month or six weeks, the attack wearing itself out, and recurring with a periodicity sometimes variable and sometimes constant. In the intervals of these attacks for a considerable time the patients very often lead sober, chaste, and useful lives. At length, however, evidences of permanent mental trouble are manifested, and the case settles into confirmed insanity. The attack is usually preceded by evidences of mental derangement; the patient becomes restless and irritable; sleep is irregular and unrefreshing; he complains of general malaise, and is anxious, troubled by vague apprehensions. He presently abandons his usual occupations and gives himself up to disordered impulses, among which alcoholic excesses are the most frequent and the most easily gratified. Sometimes the patient passes his time at taverns drinking with all comers; at others he shuts himself up in a chamber and gratifies his desire for drink to the most extreme degree alone. Dipsomaniacs not rarely leave their homes and associates without warning or explanation, and pass the period of the paroxysm among associates of the most disreputable character. The desire for drink is gratified at all costs, and not infrequently they return to their friends without money and without sufficient clothing, most of it having been sold or pawned in order to purchase drink. The paroxysm is succeeded by a period of more or less marked mental depression, during which the patient not rarely voluntarily seeks admission to some asylum.
The true nature of dipsomania is frequently overlooked. As a symptom of hereditary insanity it is in striking contrast with the habitual propensity to drink which occurs in the ordinary alcoholic subject. The latter seeks occasions to drink. He renews his excesses not intermittently, but habitually. If in consequence of disgrace or misfortune or under strong moral suasion he is for a time abstemious, it is only to renew and to [p. 637] continue his indulgence upon the first favorable occasion. On the contrary, the true dipsomaniac recognizes his malady and struggles against it. Even more: for a time he shows much skill in concealing it. He avoids occasions to drink, and, reproaching himself for his mad and unreasonable desire, seeks by every means to overcome his impulse to it. The ordinary drunkard may become insane because he drinks; the dipsomaniac drinks because he is insane.50
50 Magnan, Le Progrès médical, 1884.
Dipsomaniacs are apt to manifest precocious or retarded intellectual development. They are from infancy or childhood especially prone to convulsive or other paroxysmal nervous phenomena. They are often choreic, often hysterical. This association with instability of the nervous system is related to the fact that dipsomania is more common in women than in men.
DIAGNOSIS.—1. Acute Alcoholism.—The diagnosis of the ordinary form of acute alcoholism, with the exception of alcoholic coma, requires no consideration. The diagnosis of alcoholic coma from profound coma due to other conditions is, in the absence of the previous history of the case, always attended with difficulty, and is in certain cases quite impossible. It is therefore of great practical importance to obtain the history where it is possible to do so. The odor of alcohol upon the breath is of less positive diagnostic value than would at first thought appear. In the first place, sympathetic bystanders may have poured alcoholic drinks down the throat of one found unconscious, or, in the second place, individuals who have taken a certain amount of drink may be, and not unfrequently are, seized with apoplexy in consequence of the excitement thereby induced. The more common conditions with which alcoholic coma is confounded are apoplexy from cerebral hemorrhage and narcotic poisoning, especially opium-poisoning. To these may also be added uræmic coma and, under exceptional circumstances, sunstroke. In all these cases the circumstances under which the individual has been found are of diagnostic importance.
In alcoholic coma the pupils are more commonly dilated than contracted, the heart's action feeble, the respiration shallow, the muscular relaxation symmetrical, and the temperature low. There is a strong odor of alcohol upon the breath.
In apoplexy from cerebral hemorrhage the condition of the pupils will depend upon the location of the clot. They may be moderately dilated, firmly contracted, or unequal. The enfeeblement of the heart's action is, as a rule, less marked than in profound alcoholic coma. The pulse may be small or full and slow or irregular. It is usually slow and full. The respiration is often, although not invariably, slow and stertorous. Not uncommonly, the eyes and also the head deviate from the paralyzed side. If the coma be not absolute, the muscular relaxation is unilateral. The temperature is at first slightly below the normal, but less, as a rule, than in alcoholic coma; after several hours it rises to or above the normal.
In complete opium narcosis the insensibility is profound; the heart's action is slow or rapid, but feeble; the respirations slow and shallow or quiet or stertorous; the face at first flushed, afterward pallid and cyanosed; the pupils minutely contracted or dilated as death approaches; [p. 638] and the muscular relaxation complete, with abolition of reflex movements. In cases of doubt it is important to use the stomach-pump.
Uræmic coma is apt to be preceded by or alternate with convulsions. The pupils are more commonly slightly contracted than dilated, but are without diagnostic significance. The temperature is not elevated; it may even be low. The face may be pallid, pasty, and puffy, and there may be general anasarca if the nephritis be parenchymatous. On the other hand, in interstitial nephritis there is hypertrophy of the heart, without evidence of valvular disease, and some degree of puffiness of the lower extremities. In doubtful cases the urine should be drawn by a catheter and subjected to chemical and microscopical examination.51 Diabetic coma occurs suddenly without convulsions. This condition may be suspected when the emaciation is extreme or upon the recognition of sugar in the urine.
51 The following is the method recommended by Green (Medical Chemistry, Philadelphia, 1880) for the detection of alcohol in the urine: If its reaction be acid, the urine is exactly neutralized by potassium acid carbonate. It is then distilled on a water-bath in a flask or retort connected with a condensing apparatus. When about one-sixth of the liquid has passed over the distillate will, if alcohol be present, present the following characteristics: first, the peculiar alcoholic odor; second, a specific gravity lower than water; third, upon being mixed with dilute sulphuric acid and treated with a few drops of potassium bichromate solution the liquid becomes green, owing to the separation of chromic oxide; the odor of aldehyde may at the same time be observed. This reaction is not characteristic, but may serve to confirm other tests. Fourth, if dilute alcohol be shaken with an excess of solid and dry potassium carbonate in a test-tube, the greater part of the water will be appropriated by the potassium carbonate, and two layers of liquid will be formed. The alcohol constitutes the upper layer, and if sufficiently concentrated will burn upon the application of a flame. Finally, a small trace of alcohol may be separated from the urine without difficulty after the ingestion of alcoholic liquids by means of a good fractionating apparatus. Less than 1 per cent. of alcohol cannot be detected.
Sunstroke is characterized by dyspnœa, gasping respiration, jactitation, and intense heat of the skin. The pulse varies. It may be full and labored or feeble and frequent. The face is usually flushed. The pupils, at first contracted, are afterward dilated. The coma is apt to be interrupted by transient local or general convulsions.
It is impossible to lay down any rules by which the maniacal form of acute alcoholism may be at once diagnosticated from acute mania from other causes. For the characteristics of the convulsive form of acute alcoholism and those forms which occur in persons of unsound mind the reader is referred to the descriptions of those conditions. The diagnosis of acute poisoning by alcohol in lethal doses can only be established during life by investigation of the history of the case.
II. Chronic Alcoholism.—The lesions of chronic alcoholism, as has already been pointed out, are not in themselves peculiar to that condition. Many of them occur with more or less frequency in morbid states not induced by alcohol. It is their association and progressive character which gives to chronic alcoholism its individuality. The occasional prominence of certain symptoms or groups of symptoms may thus in particular cases lead to some confusion of diagnosis, especially where the history is unknown or the habits of the individual are concealed. In the greater number of cases, however, the association of symptoms is such as to render the diagnosis, even in the absence of a direct history, a comparatively easy one.
Chronic alcoholism is a condition rather than a disease—a condition [p. 639] characterized by varying lesions of the viscera and nervous system, by profound disturbances of nutrition, and by grave mental and moral derangements. This fact being recognized, the cardinal error of diagnosis to be guarded against is that of overlooking the condition upon which the disease itself with which we have to do depends or is associated. Congestion, inflammation, sclerosis, and steatosis affect the various organs of the body and produce their characteristic symptoms. Profound and lasting disturbances of nutrition demand our attention. Psychical derangements of all grades, from mere moodiness to confirmed and hopeless insanity, take place. These affections must be diagnosticated for themselves here as elsewhere in clinical medicine. The recognition of the underlying condition can, however, alone supply the key to their true pathology.
Delirium tremens is occasionally diagnosticated with difficulty from some forms of insanity not caused by drink. Here transitory and fixed delusions, not mere terrors and hallucinations, are of importance, not less than the absence of the varied and complex associations of symptoms which are characteristic of alcoholism. The delirium of the acute infectious diseases may be mistaken for delirium tremens. Pneumonia, typhoid fever, and the exanthemata occasionally begin with delirium resembling in some respects delirium tremens. Here the history of the case, the pyrexia, and the general condition of the patient are sufficient to establish the diagnosis if the danger of error be borne in mind.
III. Hereditary Alcoholism.—The diagnosis of this condition can only be established by careful investigation of the family history and systematic study of the stages of progression by which the morbid condition presented by the patient has been reached.
IV. Dipsomania.—The diagnostic points are the hereditary transmission of this or other forms of insanity—the mental instability of the patient in early life and in the intervals of the paroxysms, the intermittent or cyclical recurrence of the attack, the morbid impulses of a different kind associated with the impulse to drink, and the struggle of the patient against his recurring impulses to uncontrollable excesses.
PROGNOSIS.—The prognosis in acute alcoholism of the ordinary form is favorable, so far as the immediate attack is in question. The prognosis in rapidly-developing, overwhelming coma from enormous doses of alcohol is in the highest degree unfavorable. Acute coma from moderate doses usually passes off in the course of some hours. It occasionally, however, terminates in fatal pneumonia.
The prognosis in delirium tremens of the ordinary form is favorable. It becomes, however, more and more grave with each recurring attack. Delirium tremens in patients suffering from advanced disease of the heart, lungs, liver, or kidneys, or complicated by acute diseases of these organs, is apt to prove fatal.
The prognosis of chronic alcoholism is gloomy. If the lesions be not advanced, permanent discontinuance of alcoholic habits may be followed by restoration of health, but, unfortunately, the discontinuance is too often merely temporary, the habit being too strong to be permanently broken off.
The prognosis in hereditary alcoholism is unfavorable, both as regards the alcoholic habit and as regards the development of serious diseases of [p. 640] the nervous system under adverse circumstances, even in the absence of the direct action of alcohol.
The prognosis in dipsomania is unfavorable. The paroxysm may recur many times without apparent serious result; the patient in the course of some days or weeks recovers, abandons his evil courses, and resumes his usual occupations. After a time, however, the insanity of which the dipsomania is the recurring manifestation declares itself as a more or less permanent state. The outbreaks become more frequent and more prolonged, the mental condition in the intervals progressively more morbid, until the patient lapses by degrees into confirmed insanity.
The prognosis in all forms of alcoholism, both acute and chronic, is rendered in a high degree uncertain by the psychical disorders which characterize so many of its phases. In consequence of some of these conditions the patient loses at once his appreciation of bodily dangers and his power to avoid them; by reason of others, to escape imaginary evils he plunges into real ones; and finally some of them are of such a nature that they impel him to the blind and unreasoning commission of the most grievous crimes, including suicide and homicide.52
52 “I believe that more suicides and combined suicides and homicides result in this country from alcoholism in its early stages than from any other cause whatsoever” (T. S. Clouston, Clinical Lectures on Mental Diseases, Am. ed., 1884).
TREATMENT.—The prophylaxis of alcoholism has regard to communities at large and to individuals. The prevention of the evils of excess by the control of the sale of drink constitutes one of the more important objects of state medicine. At the same time, the traffic in alcohol is curiously evasive of legal enactments. The difficulties attending the enforcement of sumptuary laws are well known. Restrictive laws concerning the making and sale of alcoholic drinks, while partaking of the nature of sumptuary laws are of more comprehensive character, being obnoxious to powerful commercial interests and to the sense of personal liberty of large numbers of persons of all classes. As a result of organized opposition and individual violation they are to a great extent inoperative as regards the prevention of alcoholism.
Aside from the question of revenue from taxation, the practical influence of law is in this matter somewhat limited, being confined chiefly to the prevention of the sale of liquors to minors and persons already intoxicated, and to ineffectual attempts in certain countries to regulate the quality of the drink sold. The penalties for personal drunkenness which does not lead to overt acts are, as a rule, wholly inadequate to restrain it. The best results upon anything like an extended scale have been obtained by the co-operative action of philanthropic individuals in endeavoring to influence the moral tone, especially among workingmen, to diminish temptations, and to provide for leisure hours, in the absence of drink, reasonable amusements and occupation to occupy the time ordinarily spent in taverns and similar places.
The decrease in the consumption of alcoholic drinks in the United States within recent years is doubtless due in part to increasing popular knowledge concerning the dangers of alcoholic excess and to the growth of a more wholesome public sentiment. It is, however, in part also due to poor wages among workingmen.
As regards the individual, prophylaxis against alcoholism consists [p. 641] either in total abstinence from, or in the most guarded indulgence in, alcoholic beverages. It is unfortunate that individuals whose moral and physical organization is such as renders them most liable to suffer from the consequences of alcohol are by that very fact most prone to its temptations, and hence contribute largely to the subjects of alcoholism. These individuals are found among the ignorant, the very poor, and especially among neurotic subjects of all classes of society. Due consideration of this fact cannot fail to establish the responsibility of those fortunately not belonging to these classes, in two respects: first, that of example; and second, that of personal restraint from the standpoint of heredity. The influence of heredity among races addicted to alcohol has not yet attracted the attention it deserves. It is probable that much of the tolerance for alcohol exhibited by individuals, families, or even nations, is to be accounted for by heredity. Still more probable is it that most of the evils and crimes that befall alcohol-drinking communities and individuals are due directly or indirectly to the abuse of this agent. No argument against the indulgence in narcotics can be more potent than that derived from a consideration of the laws of heredity.
I. The Treatment of Acute Alcoholism.—The medical treatment of mere drunkenness requires no consideration. The rapid elimination of alcohol, and the transient nature of its pathological effects in excesses which are not repeated or prolonged, explain the spontaneous recovery, which is usually sufficiently prompt and permanent. The physical suffering and mental distress following unaccustomed excesses are of salutary influence. Under certain circumstances a powerful effort of the will is sufficient to control, at all events for a time, the more moderate effects of alcohol. A similar result follows the use of cold douches, the Turkish bath, and full doses of certain preparations of ammonium, particularly the officinal solution of the acetate of ammonium. In alcoholic stupor of an acute kind the patient may be left to himself, care being taken that the clothing is loosened and that the position is such as to prevent local paralysis from the nerve-pressure. Alcoholic coma, if of moderate intensity, may be managed in the same way. Profound alcoholic coma requires, however, more energetic measures. Frictions, artificial warmth, stimulating enemata, as of turpentine or of hot salt and water, an ounce to the pint, hypodermic injections of strychnia or atrophia in minute doses and occasionally repeated, inhalations of ammonia, and occasional cold affusions, followed by brisk frictions with warm flannel and faradism of the respiratory muscles, may be needed to tide over the threatened fatal collapse. The stomach should be at once washed out with hot coffee.
In the convulsive form of acute alcoholism chloral in twenty-grain doses, repeated at intervals until sixty grains have been given, usually serves to arrest, or at all events to moderate, the paroxysm. It may be administered by the mouth or in double doses by the rectum. If chloral be inadmissible by reason of weakness of the circulation, paraldehyde may be substituted in doses of from half a drachm to one drachm, repeated at intervals of from one to two hours until quietude is produced. Where the convulsive paroxysms are of great violence it may be necessary to control them by the cautious administration of ether by inhalation.
The mania of acute alcoholism calls for energetic management. To [p. 642] avert injury to the patient himself or to those about him he must be confined, if practicable, in a suitable apartment in a hospital; if not, in his own house and carefully watched. Here, as a rule, paraldehyde, chloral, or large doses of the bromides constitute our most efficient means of medication.
In all forms of acute alcoholism it is a rule admitting of no exception to at once withhold alcohol in every form and all doses. If, under exceptional circumstances, great nervous depression or flagging circulation seems to call for the use of alcohol in small amounts, it is far better to substitute other drugs. The frequently repeated administration of hot beef-tea or rich broths in small doses, with capsicum and the use of the various preparations of ammonia, or small doses of opium with or without quinia and digitalis, proves useful in proportion to the skill and discrimination with which they are selected and repeated. It is a good plan to commence the treatment with an active purge.
In the acute collapse following excessive doses—lethal doses—the stomach is to be immediately emptied by the tube or pump and washed out with warm coffee. In the absence of the stomach-tube emesis may be provoked by the use of mustard or sulphate of zinc or by hypodermic injection of apomorphia. The patient must be placed in the recumbent posture and surrounded with hot blankets. The cold douche may be occasionally applied to the head and face, and the muscles of respiration may be excited to action by faradism. Artificial respiration and friction of the extremities may also be required. Inhalations of ammonia may be used. The flagging heart may be stimulated by occasionally tapping the præcordia with a hot spoon—Corrgan's hammer. Hypodermic injections of digitalis may also be employed. Overwhelming doses of alcohol, leading promptly to collapse, usually prove fatal despite all treatment.
II. The Treatment of Chronic Alcoholism.—Whatever may be the prominence of particular symptoms or groups of symptoms, whether they indicate derangement of the viscera, of the nervous system, or of the mind, whatever their combination, the fundamental therapeutic indication in chronic alcoholism is the withdrawal of the poison. The condition is directly due to the continuous action of a single toxic principle: its relief when practicable, its cure when possible, are only to be obtained by the discontinuance of that poison. This is a matter of great, often of insurmountable, difficulty. The obstacles are always rather moral than physical. Occasional or constant temptation, the iron force of habit, the malaise, the faintness, the craving of the nervous system, and, worse than all, the enfeebled intellectual and moral tone of the confirmed drunkard, stand in the way. Even after success seems to have been attained, and the patient, rejoicing in improved physical health and in the regained companionship and consideration of his family and friends, feels that he is safe, it too often happens that in an unguarded moment he yields to temptation and relapses into his old habits. A patient of the writer, after seven years' abstinence from drink, again became its victim in consequence of the incautious suggestion of a young medical man, met at a summer hotel, to take brandy for some transient disorder, and died after eight months of uncontrollable excesses. It is necessary to guard the patient against the temptation to drink. To secure this he may he sent as a voluntary patient for a length of time to a suitable institution, [p. 643] or, still better, he may place himself under the care of a conscientious, clear-headed country doctor in a sparsely-settled region, preferably in the mountains or at the seaside. The malaise, depression, insomnia, and other nervous symptoms when of moderate degree are best treated by abundance of nutritious and easily-assimilable food, taken often and in moderate amounts. To this end gastro-intestinal disturbances may be practically disregarded, except in so far as they regulate the selection of a highly nutritious diet. As a matter of fact, in the early periods of chronic alcoholism, while visceral lesions of a grave character are yet absent, appetite and digestion alike improve in the majority of cases upon the withdrawal of alcohol, provided a sufficiently abundant and easily assimilable dietary is insisted upon. Grave visceral lesions characterize a more advanced alcoholic cachexia and necessarily complicate the treatment. Nevertheless, even here the indication is the withdrawal of the poison. The nervous symptoms require special medication. The whole group of tonics, from simple bitters to quinia and strychnia, is here available. It is impossible to lay down rules for the treatment of particular cases except in the most general manner. In the absence of conditions calling for special treatment, such as gastritis, hepatic or pulmonary congestion, fatty heart, etc., good results follow the frequent administration of small doses of quinia and strychnia; thus, the patient may take one grain of quinia six or eight times a day, or a little gelatin-coated pill containing 1/200–1/100 of a grain of strychnia every hour during the waking day, amounting in all to one-twentieth, one-tenth, or one-fifth of a grain in the course of twenty-four hours. This treatment is often followed by the relief of tremor, the quieting of nervous irritability, and the production of good general results. The malaise, the general depression, and especially the sinking feeling at the pit of the stomach so often complained of by patients, are best relieved by food. Fluid extract of coca is also useful in these conditions. The value of cocaine in the management of the nervous symptoms of chronic alcoholism, and in particular as a temporary substitute for alcohol, is doubtful. The writer, having used it in a number of cases by the mouth and hypodermically in doses of ¼–1 grain, has had variable results. In some cases it temporarily relieved the craving and concomitant symptoms; in others it failed wholly: in one instance one-fourth of a grain was followed by great nervous depression. It is desirable not to inform the patient of the nature of the remedy, especially if its use be followed by good results, lest the cocaine itself supplant alcohol as an habitual narcotic. Cold or tepid sponging, the occasional hot bath at bedtime, and the Turkish bath are useful adjuvants to the treatment. As a rule, opium is contraindicated. Sleep often follows the administration of a cupful of hot broth or milk at bedtime. Lupulin is here useful, and the writer has come to regard an ethereal extract of lupulin in doses of from one to three grains as a valuable and harmless hypnotic. If necessary, hypnotic doses of chloral or paraldehyde may be used, but care is required in their administration, and their early discontinuance is advisable. If anæmia be profound, chalybeate tonics do good, and among the preparations of iron pills of the dried sulphate with carbonate of potassium (Blaud's pills) are especially useful.
The obesity of drunkards, as a rule, diminishes on the withdrawal of alcohol. Under circumstances of partial or complete abstinence from [p. 644] drink measures to reduce the weight of such patients are wholly inadmissible.
In conditions characterized by failure of mental power, in beginning dementia or threatened insanity, the syrup of the hypophosphites, the compound syrup of the phosphates, or cod-liver oil should be administered. These remedies are likewise useful in various forms of alcoholic paralysis, as are also faradism and galvanism employed secundum artem. The various forms of alcoholic insanity require special treatment, only to be had in institutions designed for the care of patients suffering from mental diseases in general.
Whilst it is desirable in the treatment of all forms of chronic alcoholism to secure the permanent discontinuance of the alcoholic habit, the skill, judgment, and experience of the physician must determine the degree of rapidity with which this, when practicable, is to be done. The number of cases in which alcohol can be discontinued at once and finally is limited; those in which it can be wholly given up in the course of a few days constitute the largest proportion of the cases; finally, in a small number of cases alcohol can only be withdrawn cautiously and by degrees.53 Whilst it is in most cases essential to remove the patient from his customary surroundings and companionships, it is in the highest degree important to provide for him mental occupation and amusement. To this end a wholesome open-air life, with sufficient daily exercise to induce fatigue, is highly desirable, as indeed is the companionship of interested and judicious friends.
53 It must be borne in mind that in chronic alcoholism acute maladies of all kinds, including traumatism, both accidental and surgical, act as exciting causes of delirium tremens. The part played by the abrupt diminution or withdrawal of alcohol under such circumstances is often an important one. It is the opinion of the writer that a certain amount of alcohol should be administered for a time at least in the accidental injuries and acute sicknesses of alcoholic subjects, and that the reduction should be gradually made.
The Treatment of Delirium Tremens.—The patient should be confined in a large, well-aired apartment, without furniture except his bed, and when practicable he should have a constant attendant. The favorable influence of a skilful nurse in tranquillizing these patients is very great. The custom of strapping them to the bed by the wrists and ankles is to be deprecated. If the case be a mild one, and especially during convalescence, open-air exercise in the sunshine with an attendant is of benefit; care must, however, be taken to guard against the danger of escape.
Under no circumstances should visitors be permitted to see the patient. In young persons the treatment may be preceded by an active saline or mercurial purge. In elderly persons, those suffering from cachectic conditions, or in cases characterized by marked debility and feeble circulation—conditions frequent in persons who have had repeated attacks—it is not desirable to purge. Alcohol should be either wholly withdrawn or more or less rapidly diminished. It must be replaced by abundant food in the form of concentrated broths or meat-extracts. In cases of vomiting these must be given hot and in small doses frequently repeated. Bitter infusions may also be given, or milk or equal parts of milk and Vichy water. If there be thirst, the effervescent waters may be given freely. Patients often drink with satisfaction and apparent benefit hop tea, which may be made simply with water or with equal parts of water and porter.
[p. 645]The medicinal treatment will depend to a large extent upon the peculiarities of the case. In mild cases a combination of the watery extract of opium in small doses, not exceeding a quarter of a grain, with quinia and digitalis, repeated every four or six hours, is often useful. Although the view once entertained that the graver symptoms were the result of prolonged sleeplessness is no longer tenable, the induction of sleep, or at all events of mental and physical repose, is among the more important therapeutical indications. For this purpose hypnotic doses of opium are not only not desirable, but are even, in the majority of instances, attended with danger. The sleep which follows repeated and increasing doses of opium in delirium tremens has too often terminated in coma deepening into death. As calmatives, extract of cannabis indica, hyoscyamus, or the fluid extract of piscidia are useful. As hypnotics, the bromides, chloral, and paraldehyde yield, in the order here given, the best results. The bromides are better in large single doses than in small doses often repeated, better in combination than singly. Chloral, either by the mouth or by the rectum, in doses of from twenty to forty grains, is often followed by beneficial sleep. It is contraindicated where the heart's action is much enfeebled. Paraldehyde, in doses of half a drachm to one drachm, repeated at intervals of two or three hours until sleep is induced, is still more efficient. This drug may be administered without the fear of its exerting a depressing influence upon the heart. The depression characteristic of grave delirium tremens may be combated by repeated small doses of champagne or by carbonate of ammonium in five- or ten-grain doses; the vomiting, by withholding food and medication by the mouth, and giving them for some hours wholly by the rectum or hypodermically. Excessive restlessness is sometimes favorably influenced by cold affusion, followed by brisk friction and warm blankets with continuous artificial heat. The cold pack has proved useful.
Digitalis may be employed, ex indicatione symptomatica, but the enormous doses of tincture of digitalis used by the late Jones of Jersey and others are here mentioned only to be condemned.
To sum up, the chief indications for treatment are complete isolation, the withdrawal of alcohol, abundant, readily assimilable, nutritious food, and control of the reflex excitability of the nervous system.
III. Hereditary Alcoholism.—The treatment of the vicious propensities of the descendants of alcoholic parents does not fall directly within the province of the physician. It is among the most difficult problems of education. The recognition of the cause of evil traits manifested in childhood and youth may do something to avert dangers commonly unsuspected. All things considered, the outlook is not hopeful. The recognition, on the part of the physician, of the influence of hereditary alcoholism in cases of arrested development, feeble organization, or declared disease of the nervous system will perhaps do less to aid his treatment in many cases than to reconcile him to its want of full success. The cry of warning is to those who are eating sour grapes that the teeth of their children will be set on edge.
IV. Dipsomania.—The general indications for the treatment of dipsomania are two: first, the management of the paroxysm; second, the control of the general condition itself.
First, then, during the paroxysm the patient must be saved, in so far [p. 646] as is possible, from the danger of injuring himself or others and from squandering his property. If the excesses are of such a degree as to render it practicable, the same treatment must be carried out as in cases of acute alcoholic mania and delirium tremens—namely, confinement in a suitable apartment under the care of an experienced nurse and the control of the doctor. Unfortunately, this plan is not always practicable in the early days of the outbreak. Here tonics, coca, and repeated small doses of quinia and strychnia are of advantage. Courses of arsenic at the conclusion of, and in the intervals between, the paroxysms are of use, on account of the excellent influence they exert on the general nutrition. These may be advantageously alternated with iron, cod-liver oil, and the compound syrup of the phosphates or of the hypophosphites. Hydrotherapy may also be used with advantage, and the influences of a well-regulated hydropathic establishment are much more favorable than those of institutions specially devoted to the treatment of alcoholic subjects. In the latter the moral atmosphere is apt to be bad; the patients support each other, and too often conspire to obtain in secret that which is denied them openly, or, if the discipline be too strict for this, they sympathize with each other in their restraint, react unfavorably upon each other in the matter of shame and loss of self-respect, and plot together to secure their liberty.
Few dipsomaniacs in the earlier periods are proper subjects for treatment in hospitals for the insane. If cerebral excitement or sleeplessness persist after the paroxysms, chloral, paraldehyde, or the bromides in large doses may be used to secure sleep. Various combinations of the bromides are often of use where the single salts fail. It must not be forgotten that during the paroxysm there is great danger lest the patient do himself or others harm. When there are indications of an impending attack, and during the period of depression following the attacks, benefit is derived from the daily use of bitter infusions. As a matter of fact, however, the management of these cases is among the most unsatisfactory of medical undertakings. The difficulty is increased by the latent character of the mental disorder in the intervals between the attacks. Even when such patients voluntarily enter hospitals for the insane, they cannot be retained there sufficiently long to derive any permanent benefit. What we want is, in the words of Clouston, “an island where whiskey is unknown; guardianship, combined with authority, firmness, attractiveness, and high, bracing moral tone; work in the open air, a simple natural life, a return to mother Earth and to Nature, a diet of fruits, vegetables, bread, milk, eggs, and fish, no opportunity for one case to corrupt another, and suitable punishments and deprivations for offences against the rules of life laid down. All these continued for several years in each case, and the legal power to send patients to this Utopia for as long a period as medical authority determines, with or without their consent.”
Next in order to alcohol, opium and morphine are habitually abused to a greater extent than any other narcotic. Chloral is used in the same way by a large number of individuals. Paraldehyde, cannabis indica, ether, chloroform, and cocaine are also used to a less extent. The scope of this article does not include the consideration of acute poisoning by these drugs.
The habit of taking narcotics, whether medicinally or as a mere matter of indulgence, is apt speedily to become confirmed. The physiological dose more or less rapidly loses its power to affect the nervous system in the ordinary way. Tolerance increases with increasing doses, and in a comparatively short space of time poisonous doses are taken with impunity as far as immediate danger to life is concerned. The toxic effects of the poison are shown in characteristic perversion of the functions of the nervous system and of the mind. A condition is established in which the ordinary functions of life are properly performed only under the influence of the habitual narcotic, and in which its absence results in languor, depression, and derangement of bodily and mental processes. The habit, once established, thus makes for itself a constantly recurring plea for its continuance. Especially is this true of opium and morphia.
Opium-eating is chiefly practised in Asia Minor, Persia, and India. It is also prevalent in Turkey. It has been practised in India from very ancient times. The prevalence of this habit in the East is probably largely due to the restrictions placed upon the use of alcoholic beverages among the Mohammedans, and to some extent also to the long religious fasts observed by the Buddhists, Hindoos, and Moslems, during which opium is often used to allay the pangs of hunger. The prevalence of the opium habit in India is shown by the fact that the license fees for a single year amounted to nearly five hundred thousand pounds sterling. It is stated that in Samarang, a town of 1,254,000 inhabitants, the average quantity of opium consumed monthly is 7980 pounds. The town of Japava, with 671,000 inhabitants, consumed in fifteen days 5389 pounds [p. 648] of opium. In 1850, 576,000 pounds of opium were imported into Java, besides an unknown quantity smuggled.1
1 Archiv für Pharmazie, 1873, cited by Von Beck, Ziemssen's Cyclopædia, vol. xvii.
The habit is not confined to Oriental countries, but is also practised in various forms in the West. It is by no means rare on the continent of Europe. In certain districts of England, especially in Lincolnshire and Norfolk, more opium is consumed than in all the rest of the United Kingdom. Shearer2 states that the increase in the practice of opium-eating among the workpeople of Manchester is such that on Saturday afternoons the druggists' counters are strewed with pills of opium of one, two, and three grains, in preparation for the known demand of the evening. The immediate occasion is said to be the lowness of wages, opium being used as a cheap substitute for alcohol or as a food substitute, or with the view of removing the effects of disease and depression. According to the same observer, laudanum is more or less in use as a narcotic stimulant in the cotton-spinning towns, where female labor is in requisition and is well paid. Children are accustomed to it from their earliest infancy. Their parents drug them with daily potions of Godfrey's cordial, Dalby's carminative, soothing syrup, and laudanum itself, during the long hours of their absence from home. While the habit of opium-eating cannot be said to be generally prevalent in any part of the United States, instances of it are frequently encountered in all classes of society, and particularly among people of means and refinement. The preparations employed in this country are crude opium, tincture of opium or laudanum, camphorated tincture of opium or paregoric, McMunn's elixir, Dover's powder, and the salts of morphia. All of these preparations are used by the mouth; opium is very frequently, especially among women of the better classes of society, habitually taken in the form of suppositories; finally, the acetate and sulphate of morphine are used by means of the hypodermic syringe. While it will be necessary to point out some differences in the effects of these drugs due to the preparation used or to the method in which it is employed, the distinction between the opium habit and the morphine habit, in itself an artificial one, will not be regarded in the course of the present article.
2 Opium-smoking and Opium-eating, their Treatment and Cure, by George Shearer, M.D., F. R. S.
Opium-smoking is chiefly practised by the inhabitants of China and of the islands of the Indian Archipelago. It has been imported into those countries where Chinese labor is largely employed. The Chinese have transmitted it, to an extent which is fortunately very limited, to the inhabitants of certain of our cities. Opium-smoking is habitually practised in this country only among the more debased orders of society.
SYNONYMS.—Opiophagia, Morphiopathy, Morphinism, Morphinomania, Morphiomania, Morpheomania, are terms occasionally employed to designate the opium or morphia habit.3 Landowski, Levinstein, Jouet, and others use the term morphinism to denote the condition of the body; morphinomania, the condition of the mind in chronic morphine-poisoning. This distinction may be misleading. In effect, the pathological condition is complex, including derangements both somatic and psychical.
3 The word morphiomania, used by writers, is contrary to all etymological rule (Zambaco, De la Morphéomania, Paris, 1883).[p. 649]
ETIOLOGY.—A. Predisposing Influences.—Pain holds the chief place among the influences which predispose to the formation of the opium habit. By far the greater number of cases have taken origin either in acute sickness, in which opium administered for the relief of pain has been prolonged into convalescence until the habit has become confirmed, or in chronic sicknesses, in which recurring pain has called for constantly repeated and steadily increasing doses of opiates. In view of the frequency and prominence of pain as a symptom of disease, and the ease and efficiency with which opium and its preparations control it, the remote dangers attending the guarded therapeutic use of these preparations are indeed slight. Were this not so, the number of the victims of the opium habit would be lamentably greater than it is. In a considerable proportion of cases of painful illness the relief afforded by opiates is attended by at least some degree of malaise, nausea, vomiting, and vertigo—symptoms which render the speedy discontinuance of the remedy scarcely less desirable than the control of the pain for which it was administered. Occasionally these symptoms are so distressing as to render opium wholly inadmissible. In other instances each successive dose is attended by an aggravation of the distress. More commonly, especially in acute illnesses, decreasing pain may be controlled by diminishing doses, thus rendering practicable entire discontinuance of the drug before those modifications of the nervous system, and especially before that tolerance for large doses, which constitutes the beginning of the opium habit, are established. For these reasons the use of opiates in acute sickness, if properly regulated, is attended with but little danger. Far different is it, however, in chronic painful illnesses. Here to procure relief by opium is too often to pave the way not only to an aggravation of the existing evils, but also to others which are often of a more serious kind. Opium is at once an anodyne and a stimulant. The temptations to its use are of a most seductive character. To the overworked and underfed mill-operator it is a snare more tempting than alcohol, and less expensive. It allays the pangs of hunger, it increases the power of endurance, it brings forgetfulness and sleep. If there be myalgia or rheumatism or neuralgia, and especially the dispiriting visceral neuralgias so common and so often unrecognized among the poorer classes of workpeople, opium affords temporary relief. The medical man suffering from some painful affection, the worst symptoms of which are relieved by the hypodermic injection of morphine, falls an easy prey to the temptation to continue it—a danger increased by the fact that he is too often obliged to resume his work before convalescence is complete. Indeed, the self-administered daily doses of physicians sometimes reach almost incredible amounts. To women of the higher classes, ennuyée and tormented with neuralgias or the vague pains of hysteria and hypochondriasis, opium brings tranquillity and self-forgetfulness.
Of 100 cases collected by Jouet,4 the habit followed the therapeutic use of morphine in 32 cases of ataxia, 24 of sciatica and other neuralgias, 8 of asthma, 2 of dyspepsia, 4 of hypochondriasis, 2 of madness, 9 of painful tumors, 2 of prostatic inflammation, 7 of nervous conditions (not specified), 1 of peritonitis, 2 of periostitis, 1 of gastro-enteralgia, 4 of pleuritic pains, 1 of contracture, and 1 case of hæmoptysis.
4 Étude sur le Morphinism chemique, Thèse de Paris, 1883.
The responsibility of the physician to his patient becomes apparent [p. 650] when we reflect that with very few exceptions the opium habit is the direct outcome of the use of the drug as a medicine.
The decade of life at which the opium habit is most common is between thirty and forty. But it may be developed at any age. Even infants are not rarely made the subjects of chronic opium narcotism by the use of soothing syrups and other poisonous nostrums.
Sex in itself exerts very little influence as a predisposing cause. Owing to collateral circumstances, the number of women addicted to opium is greater than the number of men. Kane5 states that females more frequently fall victims to these drugs than males, in the proportion of three to one, and attributes this excess to the fact that women more often than men are afflicted with diseases of a nervous character in which narcotic remedies are used for long periods. This observer suggests as an additional explanation the occasional preference on the part of women for opium as a stimulant in place of alcohol, its effects being less noticeable and degrading. On the other hand, Levinstein observed in 110 cases 82 men and 28 women. He does not, however, regard the conclusion that the use is more common among men as warranted by these figures. The habit resulted in these 110 cases from the following causes: In 20 men and 6 women after acute affections; in 46 men and 17 women after chronic affections, these diseases being in each instance accompanied by great pain. One man began to use morphine as an antiaphrodisiac. Either to produce mental excitement simply or to cause forgetfulness of the ordinary cares of daily life, 15 men and 5 women indulged to an uncontrollable extent.
5 Drugs that Enslave, Philadelphia, 1881. I refer with pleasure to the early labors of this observer. His later publications tell their own story.
Occupation has in some respects much to do in favoring the development of the opium habit. Familiarity with the use of drugs exerts a powerful influence. Of Levinstein's 110 cases, 47 occurred in persons belonging to the medical profession or dependent upon it; thus, 32 physicians, 8 wives of physicians, 1 son of a physician, 4 nurses, 1 midwife, and 1 student of medicine.
A predisposing influence of more importance than would at first sight appear is found in sensational popular writings upon the subject. As Kane has well said, “At the time in which De Quincey, Coleridge, and Southey lived the people and the profession knew little of the opium habit save among foreign nations. The habitués were few in number, and consequently when De Quincey's article appeared it created a most decided impression upon the popular mind—an impression not yet effaced, and one which bore with it an incalculable amount of harm. Men and women who had never heard of such a thing, stimulated by curiosity, their minds filled with the vivid pictures of a state of dreamy bliss and feeling of full content with the world and all about, tried the experiment, and gradually wound themselves in the silken meshes of the fascinating net, which only too soon proved too strong to admit of breaking.” There can be no question that a percentage of cases of the opium habit, small though it be, is even in our day to be attributed to this cause.
Somewhat analogous in its etiological importance is the influence of example upon persons of idle and luxurious habits. Nowhere in Western countries, with the exception of the opium-smoking dens of the [p. 651] Chinese and their depraved associates, are there public places of resort devoted to the practice of the opium and morphine habits, as there are in Turkey and the East. According to Jouet—whose statements are corroborated by occasional statements in French newspapers—the habitual injection of morphine is to-day, in France at least, almost a matter of fashion. Landowski states that friendship is occasionally pushed to the extent of the exchange of pretty syringes in silver cases as presents, and that a patient received upon his birthday a hypodermic syringe as a present from his sister. Zambaco, whose observations were made at Constantinople, states that among the Moslems the opium habitués prefer the crude drug, either alone or associated with certain aromatic substances, such as ambergris, canella, or saffron, which are used for their aphrodisiac effect. These mixtures are prepared openly in the family, and carried upon the person in the form of pills in rich boxes of gold and enamel among the better classes. This observer further says that the ladies of the better classes carry jewelled cases containing hypodermic syringes and artistic flaçons for the seductive solution, and that they avail themselves of favorable opportunities to take an injection of morphine even when together.
In addition to the predisposing influences already mentioned, it has been customary to regard insanity as a cause of the opium habit. Laehr6 and Fidler7 have gone so far as to class the morphine habit among the psychoses. This view appears to be no longer tenable. The opium habit must be classed with the taste for alcohol, gambling, avarice, and lust as among human passions. That nervous subjects, invalids, and individuals wanting in moral and physical tone are specially prone to it is obvious. It constitutes in these cases, however, an expression of the morbid constitution rather than a substantive affection in itself. In the same manner, the opium habit in insane persons must be looked upon as an epiphenomenon of the morbid mental condition.
6 Allgemeine Zeitschrift für Psychiatrie, 1872.
7 Jahresb. der Gesellschaft für Natur und Heilkunde, Dresden, 1876.
Levinstein has with reason insisted upon the essential difference between the disturbances resulting from chronic poisoning by alcohol, lead, arsenic, etc., and that produced by morphine. In the former group the mental conditions are expressions of physical and chemical alterations of the central nervous system, which, once established, persist for an indefinite period, whereas in morphinomania the troubles of the nervous system are chiefly functional and of a transitory character. He regards the nervous disorders developed from the prolonged use of morphine as the result simply of depression of the nervous system, and the extreme suffering experienced on the withdrawal of the regular dose to which the subject has been accustomed as a trouble of innervation rather than as a psychical derangement. This physical suffering and the mental depression which accompanies it have their analogues in the angina occasionally seen in paroxysmal affections of the heart, the blood-vessels, and the respiratory organs. Certain it is that individuals addicted to opium and morphine excesses in a high degree not only frequently retain full possession of their intellect, but occasionally achieve and maintain great distinction in professional and scientific life. Furthermore, subjects of the opium habit, notwithstanding the gravest mental disturbance manifested during the [p. 652] continuance or upon the cessation of the habit, usually exhibit when cured no further indication of mental disorder.
B. The Exciting Cause.—In addition to the usual constituents of vegetable substances, mucilage, albumen, proteids, fat, volatile substances, and salts of ammonium, calcium, and magnesium, opium contains a number of alkaloids, two neutral substances, and meconic acid. Some of the alkaloids are probably derivatives from morphia. The three most important alkaloids are morphine, codeine, and thebaine. The neutral substances are meconin and meconiasin. Morphinæ hydrochloras, acetas, and sulphas, codeina, and apomorphinæ hydrochloras are officinal in the United States Pharmacopœia. Opium and its alkaloids act principally on the central nervous system, and in mammals on the brain. The functions of the nervous system, as Brunton has pointed out, are abolished in the order of their development, the highest centres being the first affected. In man the action of opium is chiefly manifested upon the brain. With small doses a stage of excitement, attended by increased activity of the circulation, augmented nervous energy, and under favorable circumstances an agreeable languor, followed by quiet sleep, constitute the effects of the drug; with larger doses, of from one to two grains, the transient stage of excitement is followed by deep sleep, the awakening from which is marked by headache, nausea, and evidences of gastro-intestinal catarrh; with still larger doses, of three grains or more, deep sleep is produced, which speedily passes into coma. The drug has an especial action on the vaso-motor system, which is manifested in its power to diminish congestion and relieve inflammation. With the exception of the urine and the sweat, the secretions of the body are diminished by opium. The action of the drug upon the intestines varies with the dose. In moderate doses it diminishes peristalsis and causes constipation; in very small doses it increases peristalsis; in large doses peristaltic action ceases. Morphine is eliminated unchanged by the kidneys. It is eliminated also by the gastro-intestinal mucous membrane, having been found in the stomach after hypodermic injection. The action of opium and its derivatives, as that of other narcotics, is much influenced by habit. In those accustomed to the drug large (and sometimes enormous) quantities are required to induce the characteristic manifestations. Not rarely these manifestations are much retarded. The enormous amount of two pints of tincture of opium has been taken in the course of a day; a female patient afterward successfully treated by the writer took habitually for a long period of time from ten to twelve grains of morphine per diem, hypodermically. Diedriech8 assumes that a portion of the morphine introduced into the organism is converted into oxydimorphine or other analogous substances which have the property of counteracting to some extent the toxic effects of the morphine.
8 Ueber oxydimorphine, Inaug. Diss., Göttingen, 1883.
Levinstein concludes as a result of experiments upon animals that morphine, besides its influence upon the nervous system, exerts an especial action upon two sets of organs: first, upon the digestive tube; and second, upon the sudoriferous glands. Taken by the mouth, it irritated the gastric mucous membrane. Whether taken by the mouth or hypodermically, it diminishes the secretion of gastric juice and the peristaltic movements of the intestine. These disturbances serve to explain not [p. 653] only certain of the phenomena of the opium habit itself, but even more fully some of the symptoms manifested upon its discontinuance. The nausea, vomiting, and constipation occurring during the continuance of the habit must be looked upon as a result of the derangement of function of the gastro-intestinal glandular apparatus and the chronic catarrh which accompanies it. The abrupt discontinuance of the drug is followed by the sudden return of functional activity, hence salivation, persistent vomiting, anorexia, and diarrhœa.
The effects of habitual excesses in opium and morphine upon the nervous system are in essential particulars the same. Upon the functions of the digestive system and upon nutrition they differ to a considerable extent. Opium, as a rule, soon produces gastro-intestinal derangements of a marked kind. These derangements consist in loss of appetite, enfeebled digestion, nausea, vomiting, and constipation alternating with occasional diarrhœa. The anorexia is usually persistent and of a high degree, and has much to do with the development of the wasting which is so common and so marked. The occasional excessive appetite for food manifested by opium-eaters is of brief duration. Its gratification aggravates the functional disturbances, provokes gastro-intestinal catarrh, and thus tends to increase the general malnutrition. On the other hand, morphine is much better borne. At the present time almost all morphine habitués use the hypodermic syringe, and, notwithstanding the elimination of the drug in part by the gastric mucous membrane, thus escape in part its evil effects upon the organs of digestion, and remain for a long time, often despite enormous excesses, free from the nutritive disturbances which are almost characteristic of the habitual abuse of crude opium.
SYMPTOMATOLOGY.—The symptoms of the confirmed opium habit may be divided into two principal groups: first, the symptoms of chronic opium- or morphine-poisoning; and second, the symptoms due to the withdrawal of the drug.
I. Symptoms of Chronic Poisoning.—A considerable percentage of the individuals addicted to the opium habit preserve for a longer or shorter period of time the appearance of health; indeed, it is possible for very large doses of opium to be occasionally taken by certain individuals without appreciable impairment of the functions either of the body or the mind. These cases must, however, be looked upon as exceptional. It is estimated that from one-fourth to three-tenths of the entire population of China are addicted to the habit of opium-smoking. The statements of travellers concerning the effect of this habit are somewhat conflicting. When practised within bounds it appears to resemble in its effects the moderate use of alcoholic stimulants, increasing the ability to endure fatigue and diminishing for a time the necessity for food. In moderation it appears to have little injurious effect upon the general health. On the other hand, in the greater number of individuals the confirmed opium habit causes in a variable period of time symptoms of the most decided character; the appetite and general nutrition fail; emaciation is often rapid, commonly marked, and sometimes extreme. There are thirst and anorexia; a little later the patient begins to suffer from nausea with occasional vomiting. At this time a loathing for food alternates with boulimia. These occasional excesses in food are followed by epigastric [p. 654] distress, heartburn, and great mental depression. The skin becomes relaxed, inelastic, and dull. Exceptionally, especially in women who use morphine hypodermically, embonpoint is preserved and the skin retains its normal tension and appearance. The countenance is pale, muddy, and sometimes slightly cyanotic. There is increased tendency to perspiration. Acne and urticaria are common. Herpes zoster is encountered with considerable frequency among opium subjects. In cases in which morphine is administered by means of the hypodermic syringe the resulting lesions of the skin are of importance. If the habit be concealed or denied, they are of diagnostic value. Not rarely they constitute serious affections in themselves. They are of all grades, from mere inflammatory points to coarse infiltration and ulceration. The wounds are frequently so thick set over the greater part of a limb as to present the appearance of a continuous eruption. In other cases scattered points of ulceration occur or extensive surfaces are occupied by a series of ulcerations varying in size from a split pea to an inch or more in diameter. Purulent inflammation of the subcutaneous tissues, with burrowing, also occurs. Numerous scars bear witness to the duration and extent of the habit. These lesions are usually due to unclean needles and impure solutions; in certain cases they are to be explained by the peculiarities of the individual as regards the tendency to inflammation of the integumentary structures; finally, instances are related in which immunity from skin lesions has existed in spite of rusty needles and carelessly kept solutions.
The expression of the countenance is sometimes dull, much more frequently furtive and timid. The repetition of the dose renders it eager and bright. The pupils are commonly contracted, sometimes enlarged, and occasionally unequal. Diminished power of accommodation is common, and diplopia has been occasionally observed.
The action of the heart is often irregular and weak. Disturbances of the vaso-motor system give rise to flushing of the face, irregular sensations of heat over the body, and sweating. It is probable that the albuminuria hereafter to be described is due to disturbance of the circulation in the kidneys. The pulse is variable; it is sometimes tense and full, sometimes small and thready, often irregular. The volume, tension, and rhythm of the pulse depend largely upon the state of the vaso-motor and general nervous systems. They vary according to the periods of stimulation, following doses or the periods of depression characterizing the intervals between the doses. Palpitations occasionally occur. Respiration is, as a rule, normal. Transient dyspnœa sometimes occurs after doses a little larger than usual. Subacute bronchitis is common. The urine is often diminished in quantity. Its specific gravity varies within extreme limits, being influenced rather by collateral circumstances than by the dose of opium or morphine consumed. In grave cases albuminuria occurs. Casts of various kinds are also encountered. As Levinstein9 has pointed out, these changes in the urine are often transitory, disappearing upon the suppression of the opium habit.
9 La Morphiomanie, 2d ed., Paris, 1880.
In confirmed cases uric acid is increased and urea diminished. The chlorides are also diminished in amount. Vesical irritation is likewise common. It is apt to be accompanied by neuralgia of the urethra and [p. 655] of the rectum. Strangury and retention of urine also occur in old cases. These complications are often followed by vesical catarrh.
Derangements of the central nervous system are constant and serious. The disorders which originally led to the use of opiates are in many instances intensified. The temper is capricious, fanciful, and discontented. There are giddiness, headache, and vertigo. Disturbed sleep, irregular flying neuralgic pains, and hyperæsthesia also occur. Spinal tenderness is occasionally encountered, with characteristic painful spots. Reflex excitability is augmented, but in aggravated cases the tendon reflexes are often impaired. Itching is common and troublesome. It may be local or general. Trembling of the hands and of the tongue also occurs. This tremor resembles in all particulars the tremor of chronic alcoholism, and, as many individuals addicted to the opium habit also abuse alcohol, it is not always easy to say to which of these poisons the symptom in question is to be referred: it may be due to their combined action. Disturbances of speech are not very uncommon. Sleeplessness is troublesome, but absolute insomnia is rare. The sleep which is obtained is late, irregular, and unrefreshing. In several cases that have occurred under the observation of the writer there has been habitual inability to sleep during the night, the patients wandering about, occupying themselves in attempts to read or write until toward morning, and then, under the influence of repeated doses, falling into a more or less profound slumber, which has often been prolonged till after midday. The effects of the dose upon the mind are in the early periods of the habit agreeable exhilaration, increased activity of imagination, and stimulation of the powers of conversation. These effects are sometimes manifested for a long period, and in many instances the most brilliant conversation, and among professional men and public speakers the ablest efforts, have followed the taking of large doses of opiates, and been followed in turn by periods of the most profound physical and mental depression. In the absence of the necessity for intellectual effort, and in individuals incapable of it, the mental condition produced by the dose is one of profound revery, largely influenced by the mental organization of the subject. This state is described, and in many particulars much exaggerated, in the writings of De Quincey, Coleridge, and others.
The voluptuous play of the imagination ascribed to the action of the drug by Orientals is for the most part absent among opium-takers in this country. If present at all, it occurs only to a limited degree. The corresponding fact is also worthy of note—namely, so long as the habit is continued the depression between the doses is less profound than that described as occurring in the East. One of the mental peculiarities of individuals addicted to the opium habit is secretiveness concerning their vice. Not infrequently, the real cause of the grave derangements of health thus produced is wholly unsuspected by the family or friends of the patient. When the habit is suspected or admitted, the amount and frequency of the dose are rarely fully known, patients almost invariably deceiving their friends in regard to the particulars of their indulgence. Individuals above reproach in other matters, and previously of unquestioned veracity, lie without any hesitation in this matter. A patient under my care who had secreted in her room a quantity of morphine when about to undergo treatment, denied either having taken or then having [p. 656] in her possession any opium or morphine whatever, using the expression, “I call God to witness that I neither now have, nor have had since I began the treatment, any preparation of opium or morphine whatever.” Within ten minutes sixty quarter-grain pills of morphine were discovered secreted under the bolster. This patient was a devout, refined, and, in regard to other matters, a trustworthy person.
The functions of the reproductive organs both in the male and in the female are seriously deranged. In the male sex enfeeblement of the sexual function is manifested in all degrees, even to complete loss of sexual desire and sexual power. In certain individuals opium and morphine in moderate doses produce some increase of sexual desire and power, which is, however, speedily lost on the continuance of the habit. Some doubt exists whether this is of psychical or physical origin—a question at once difficult to decide by reason of the reticence of opium-habitués upon this subject, and unimportant in itself. Levinstein makes the interesting statement that in no cases coming under his observation did the wives of morphomaniacs who had injected as high as fifteen grains of morphine a day reach the full term of pregnancy for two years prior to the treatment, notwithstanding the fact that they were still young, that they had borne children before their husbands had become addicted to morphine, and that they had not, up to the time of the formation of the habit by their husbands, suffered from premature accouchements.
Among women the morphine habit invariably produces derangement of the menstrual function. Menstrual irregularity, both as regards time and amount, is succeeded after a time by amenorrhœa. Vicarious hemorrhages do not occur. Complete amenorrhœa is sometimes established abruptly, and married women not infrequently suspect for this reason that they have conceived. In several cases of this kind under the observation of the writer the absence of enlargement of the breasts, of alteration of the areola, and of softening of the os after several months, indicated the improbability of these fears, notwithstanding the irregular appetite, the morning vomiting, the occasional palpitations and faintness, the hysterical condition, and the mental peculiarities of the individuals—phenomena unquestionably due to the action of the morphine itself. The amenorrhœa of the morphine habit is associated with sterility—a fact that renders probable the supposition that it is dependent upon absence of ovulation. Women addicted to the opium habit are capable of conceiving so long as menstruation persists, those only, however, going to full term who use very moderate quantities. In women using large doses abortion invariably occurs. The functional integrity of the reproductive system is re-established upon the permanent cessation of the habit. Women who are cured may again menstruate regularly and may again bear children. Morphine in women, as in men, is said to increase, when first habitually taken, the capacity for sexual pleasure.
Levinstein and others have described certain febrile conditions observed in individuals addicted to morphine. First, a form of intermittent fever closely resembling malarial fever. This fever of intermittent type occurs in individuals neither living in malarious regions nor previously exposed to malaria. In addition to periodicity, it presents other points of resemblance to malarial intermittent. The earlier paroxysms cease after the [p. 657] administration of quinine. They are favorably influenced by change of residence, and recur with intensity after over-exertion, exposure, and upon the occurrence of acute maladies. The favorable influence of quinine is only transient; the febrile paroxysms recur after a time, notwithstanding the continued use of the medicament. This fever disappears without special treatment upon the discontinuance of the habit. It is more frequently of the tertian than of the quotidian type. Its paroxysms are marked by the symptoms of paludal intermittent. Neuralgias of various kinds, especially supraorbital, intercostal, and præcordial neuralgias, are apt to occur. The temperature during the paroxysm ranges from 102.5° to 104°. The area of splenic dulness is increased. More or less mental and physical depression follows the paroxysm, continuing in most cases through the period of apyrexia. These observations require further confirmation. Secondly, confirmed opium-habitués are peculiarly liable to transient febrile disturbances from slight causes. Finally, ephemeral fever, ushered in by chills or rigors and accompanied by headache, vertigo, thirst, malaise, restlessness, and even mild delirium, and terminating with profuse perspiration, occasionally occurs immediately after the injection of large doses of morphine.
The course of the opium habit, when once established, is, notwithstanding its occasional transient interruptions, gradual and progressive. Certain individuals endure enormous doses of opium or morphine for years without serious symptoms. In others moderate doses give rise in the course of a few months to anorexia, disturbances of nutrition, neuralgias, fitful and difficult sleep, and serious mental derangement. These symptoms are usually controlled by increasing doses and diminution of the intervals. Finally, however, the drug fails to produce either excitement or repose, and enormous doses are taken with but insignificant relief. This is the period of grave derangement of the mental and physical functions and of nutrition amounting to a true dyscrasia. The phenomena are analogous to those produced by the withdrawal of the dose. They are the symptoms of inanition, which in the absence of well-directed and energetic treatment speedily terminates in death.
II. Symptoms Due to the Withdrawal of the Drug.—Opium-habitués, differing as they do among themselves in the manifestations of the effects of the drug so long as it is freely taken, all alike develop characteristic symptoms upon its speedy or gradual withdrawal. The apparent immunity exceptionally observed now comes to an abrupt termination. The nervous system, whether it has been accustomed for months merely or for years to the influence of opiates, is upon their withdrawal forthwith thrown into derangement of the most serious and widespread kind. In the course of a few hours after the last dose the steadying influence of the drug disappears. General malaise is associated with progressive restlessness; the ability to perform the ordinary duties of life gives way to profound depression and indifference; præcordial distress, accompanied by cough, is followed by insomnia, hallucinations, and sometimes by mania. The habitual pallor of the face is replaced by deep flushing or cyanosis. The heart's action becomes excited and irregular, then feeble; the pulse, at first tense, becomes slow, thready, and irregular. Colliquative sweats appear. Attacks of yawning and sneezing are followed by convulsive twitching and trembling of the hands. Speech becomes hesitating, drawling, and [p. 658] stuttering. Troubles of the accommodation and even diplopia occur, often accompanied by excessive lachrymation. Transient and varying differences in the pupils are very frequent. Retinal hyperæsthesia may occur. In the amblyopia occasionally observed in subjects of the opium habit the ophthalmoscope reveals persistent anæmia of the retina. These phenomena are associated with a sense of perfect prostration which obliges the patient to take himself to his bed. Pain in the back and limbs, followed by neuralgias, now occurs. Complete anorexia, with easily-provoked or even causeless vomiting and persistent nausea and diarrhœa difficult to control, adds to the gravity of the condition. The abrupt discontinuance of the drug is followed in many individuals by mental phenomena of a marked character: hallucinations, illusions, and delirium continue for several days. The hallucinations relate to all of the senses, but especially to those of sight and hearing. The sense of smell is also occasionally affected, that of taste rarely. Syncopal attacks occur. These are usually transient; occasionally, however, profound syncope calls for the active interference of the physician. Epileptiform seizures also take place. Women who have previously suffered from hystero-epilepsy are prone to the recurrence of severe paroxysms. Trembling of the limbs, and especially of the lower extremities, rhythmical in time and often violent, must be ranked among the more characteristic phenomena produced by the abstinence from the drug. Sweating, although by no means constant, is among the earlier and more persistent phenomena. Urticaria occurs. Dyspnœa is common. Sometimes it is provoked by exertion; sometimes paroxysmal shortness of breath occurs spontaneously. Irritable cough is frequent. It is in many cases unattended by râles. Pre-existing bronchitis is of course accompanied by its characteristic signs and symptoms. Præcordial distress, with palpitation and a sense of oppression, is common. During the earlier days of abstinence the evidences of cardiac failure are marked. Enfeeblement of the first sound, irregularity of the heart's action, and intermission are common. The pulse phenomena correspond to the heart's action. Thirst is a very frequent symptom. It is often out of proportion to the loss of fluid by perspiration and diarrhœa. The urine does not contain sugar. Salivation is rare and of moderate degree. Nausea is persistent. Œsophageal spasm, provoked by every effort to swallow, occasionally occurs and constitutes a distressing symptom. Many patients also complain of spasmodic contraction of the anus. Neuralgia of the testicles also occurs. The cure of the opium habit is followed by rehabilitation of the sexual power in the male and by menstrual regularity and fecundity in the female. Levinstein has observed sexual hyperæsthesia during the first weeks of abstinence in both sexes. Albuminuria occurs in a large proportion of the cases. The albumen shows itself, as a rule, from the third to the sixth day after the discontinuance of the morphine, and disappears in the course of a very few days. It is usually of slight amount.
The behavior of patients undergoing the suffering attendant upon the abrupt, or even the gradual, withdrawal of the drug is variable. It depends upon the mental and physical organization of the different individuals and upon their ability to endure pain. Some rest quietly in bed, enduring with fortitude suffering from which there is no escape; others, silent, uncomplaining, and apathetic, present the [p. 659] appearance of utter despair; a few, more fortunate than their fellows, lapse into a condition of almost continuous drowsiness. In the greater number of cases, however, these states of repose are but momentary or absent altogether. Restlessness is continuous, and very often intense; the patients are with difficulty kept in bed; if left to themselves they move frantically about the room, moaning, bewailing their condition, and begging the attendants for that which alone is capable of relieving their distress. This condition gradually subsides, giving way to a state of the most profound exhaustion. The exhaustion due to the reaction of the nervous system deprived of the stimulus of the drug is, on the one hand, favored by pre-existent derangement of the nutritive processes, and on the other increased by the pain, wakefulness, diarrhœa, and vomiting which accompany it. The appearance of the patient is now most pitiable; the countenance is blanched and pinched, the body occasionally drenched with sweat; the heart's action is feeble, and the pulse thready and irregular. This condition of collapse is usually of short duration, disappearing in favorable cases under the influence of appropriate nourishment administered in small quantities and with regularity. Where, however, the gastric irritability is unmanageable, an increasing tendency to collapse may threaten life. In rare cases suddenly-developed fatal collapse has occurred at a later period in the treatment, even after the patient has become able to take and retain food. The restlessness does not, however, always subside in this manner. In a considerable proportion of cases it increases. Hallucinations and delusions occur, and a condition of delirium tremens, scarcely differing from the delirium tremens of chronic alcoholism, is established. Tremor is a constant phenomenon of this condition. Sometimes the gravest symptoms of the suppression of the drug are developed with great rapidity. Jouet relates a case of a patient at the Salpêtrière who during a temporary absence from the hospital forgot her syringe and solution; her return being delayed from some cause, she, notwithstanding her struggles against the symptoms caused by the want of her habitual dose, suddenly fell in the street, her countenance haggard and anxious, her hands shrivelled, and her whole body bathed in drenching sweat. She immediately became maniacal, and demolished the glass and lamps of the coupé in which she was taken to the hospital. No sooner had she received her ordinary hypodermic dose than she recovered her usual quietude. This patient was neither hysterical nor had she previously suffered from nervous paroxysms. She was, however, accustomed to administer to herself at four o'clock every day a large hypodermic dose of morphine, and it was at a few minutes past four that the above-described seizure occurred.
DIAGNOSIS.—The diagnosis of the opium habit is in many cases attended with considerable difficulty. Many habitués, it is true, do not hesitate to admit the real cause of their symptoms; others, while seeking to conceal it, do so in such an indifferent manner that detection is not difficult; but the greater number for a long time sedulously conceal their passion, not only from their friends, but also from the physician whom they consult voluntarily or at the solicitation of those interested in them. If inquiries be made upon the subject, they deny the habit altogether, often with vehement protestations. If forced to admit it, they are very apt to misstate the amount employed or the frequency of the repetition of the dose. As a rule—to which there are, however, not infrequent [p. 660] exceptions—emaciation is marked, appetite is diminished and variable, the pulse is small, the circulation feeble, the respiration shallow and occasionally interrupted by long-drawn sighs, the pupils are as a rule contracted, constipation is present, often alternating with diarrhœa. When to these conditions, for which no cause can be found upon careful examination, there are added marked change in disposition, periods of unaccountable dulness and apathy alternating with unusual vivacity and brightness, especially when insomnia alternates with periods of prolonged and heavy sleep, the abuse of morphia may be suspected. If the hypodermic syringe be used the wounds made by the needle confirm the diagnosis. These punctures are usually found in groups upon the thighs, legs, arms, and abdomen. Close inquiry into the habits of the patient, who either goes himself or sends at short intervals for unusual quantities of opium or morphia to some neighboring apothecary, is sometimes necessary to confirm the diagnosis. Finally, the presence of morphine in the urine10 renders the diagnosis positive, notwithstanding the most vehement assertions of the patient as regards his innocence of the habit and the extreme cunning with which it is concealed.
10 “According to Bouchardat, morphine, when taken in the free state or under the form of opium, speedily appears in the urine, and may be detected by the liquid yielding a reddish-brown precipitate with a solution of iodine in iodide of potassium. Since, however, as we have already seen, this reagent also produces similar precipitates with most of the other alkalies and with certain other organic substances, this reaction in itself could by no means be regarded as direct proof of the presence of the alkaloid. Moreover, we find that the reagent not unfrequently throws down a precipitate from what may be regarded as normal urine, while, on the other hand, it sometimes fails to produce a precipitate even when comparatively large quantities of the alkaloid have been purposely added to the liquid” (Wormley, Micro-chemistry of Poisons).
The presence of meconic acid or morphine in the urine can only be positively determined by elaborate chemical analysis. In cases of doubt the urine should be submitted to a competent analyst. To make sure that opium or its derivatives are not being taken, the feces must also be examined.
PROGNOSIS.—The prognosis is favorable as regards the discontinuance of the habit for a time, doubtful as regards a permanent cure. Relapses are apt to occur. They are more common in men than in women, in the aged than in middle life, and in persons of feeble physical and mental organization than in those who are possessed of bodily and mental vigor. Relapses also occur more frequently in those individuals addicted to alcohol, and in those who are habitually subjected to temptation by reason of their avocation, such as doctors, nurses, and apothecaries, than in others. The danger of relapse is greater where the habit has been formed in consequence of chronic painful affections than where it has been rapidly developed in the course of acute illnesses. Of 82 men treated by Levinstein, relapses occurred in 61; of 28 women, in 10; of 38 physicians, in 26. The danger of relapse diminishes with the lapse of time; nevertheless, a single dose of morphine or a hypodermic injection may, after an abstinence of months, precipitate a relapse. Indeed, the return of the habit is in the majority of instances caused by the thoughtlessness of medical men in prescribing in these cases opiates for maladies which are often in themselves insignificant.
The prediction made by B. W. Richardson, within two years of Liebreich's announcement of the medicinal properties of chloral, that its [p. 661] abuse would become widespread, has been abundantly fulfilled. The consumption of this substance as a narcotic has reached an extent in certain classes of society which raises it, after alcohol and opium, to the third place among such agents.
SYNONYMS.—The Chloral habit, Chloralism.
ETIOLOGY.—A. Predisposing Influences.—Age exerts but little predisposing influence. Cases occur almost exclusively in adults, and the greater proportion of these are in middle life. The abuse of chloral is relatively somewhat more common among males than among females. Individuals addicted to this habit usually belong to the refined and educated classes of society; the fascinations of chloral remain thus far unknown to the great mass of the people. Professional men and those engaged in literary work form a very considerable proportion of the cases. Chloral is occasionally used by hospital nurses, and very frequently by prostitutes. Chronic alcoholism is an important predisposing element in the formation of the chloral habit; in fact, morbid conditions attended by insomnia from whatever cause tend to the formation of this habit.
B. The Exciting Cause.—Chloral is a powerful hypnotic, usually without unpleasant after-effects. In full doses it is a depressant to the nerve-centres at the base of the brain and to the spinal cord. It enfeebles the action of the heart, depresses respiration, and lessens reflex activity. It has no action on the secretions except that of the kidneys, which it frequently augments.
The habit has in some few instances been developed in consequence of the indulgence in a morbid desire to experience the effects of the drug. In a majority of instances it is due to the continuance of the medicine indefinitely after the sickness in which it was originally prescribed has ceased. I have known apothecaries to renew prescriptions of chloral often enough to supply a daily dose of from forty to sixty grains for years—in one instance for more than four years.
The dose taken by victims of the chloral habit varies greatly. Thirty or forty grains daily is a moderate amount. Not rarely this quantity is repeated twice or oftener within the space of twenty-four hours. The tolerance after a time exhibited by the organism for enormous doses of alcohol and opium is not established, as a rule, in regard to chloral. The victim of the latter after a little time discovers the average dose required to produce narcotic effects, and, while he may vary it within limits, he is liable to acute toxic effects if it be greatly exceeded. Death from such excesses is not uncommon.
SYMPTOMATOLOGY.—I. Symptoms Due to Habitual Excesses.—The habitual use of chloral, notwithstanding its ruinous consequences in a certain proportion of the cases, is less dangerous than that of opium or morphine. Many individuals take chloral in considerable doses for years without obvious ill effect. The craving for it is much less intense than that for opium or morphine, and is readily satisfied by other drugs. In point of fact, persons addicted to chloral very frequently exchange it for other narcotics. For these reasons the chloral habit is more easily cured.
Derangements of the digestive system are common, but by no means constant. They are (1) primary, and due to the direct irritant action of the drug upon the mucous tissues of the month and stomach; and (2) secondary, due to its effects upon the nervous system and the circulation. [p. 662] Irritation of the mucous membranes is very common. This not rarely amounts to gastro-duodenal catarrh with its characteristic symptoms. Jaundice is common, sometimes intense. A sense of fulness with pain and tenderness in the hepatic region is frequent. Constipation, with clay-colored stools, is the rule. It occasionally alternates with diarrhœa. The tongue is often coated and the breath foul. On the other hand, in a fair proportion of the cases the digestive organs are not affected. Chloral has been said to occasionally exert even a favorable influence upon appetite and digestion when taken before meals. The recent observations of Fiumi and Favrat11 in a man suffering from a gastric fistula and insomnia have shown that chloral hydrate in twenty- or forty-grain doses, administered before or at the beginning of a meal, retarded digestion by increasing the secretion of mucus in the stomach. The acidity of the gastric juice is diminished temporarily. The secretion of pepsin is not changed. Taken two hours after meals, doses not exceeding forty grains caused no derangement of gastric digestion.
11 Archives Ital. de Bioloqie, vol. vi. No. 3.
Persons not habituated to chloral usually experience a sense of constriction upon swallowing it, and a disagreeable after-taste.
The circulation is much affected. Chloral weakens, and finally paralyzes, the vaso-motor centre, and thus dilates the vessels; it at the same time weakens the action of the heart. Its habitual use is attended by flushing of the face, congestion of the eyes, and fulness of the head. The heart's action is weak, intermittent, irregular; palpitation occurs; the pulse is full and compressible or small and weak. It is usually slow.
The blood undergoes changes corresponding to the general disturbances of nutrition. What the special changes in its composition may be is not known. Many of the cases, even after the prolonged use of the drug in considerable doses, show few evidences of malnutrition or of anæmia. In the greater number, however, wasting is marked, and the physical signs and rational symptoms of profound anæmia are present. Deterioration in the composition of the blood is further indicated by petechiæ, hemorrhage from mucous surfaces, sponginess of the gums, and serous effusions.
The respiration is not permanently affected, save in grave cases. It is then slow, irregular, and shallow. Dyspnœa is common and easily provoked. It is usually accompanied by cough and abundant frothy expectoration. These symptoms vanish upon the discontinuance of the drug. In a fatal case of chloral-poisoning seen by the writer, in which the daily use of the narcotic in non-poisonous amounts had been for a long time varied at intervals of five or six weeks by doses sufficient to induce prolonged coma, death was preceded by Cheyne-Stokes respiration. This patient was a retired dentist, and kept the solution of chloral in a large unlabelled bottle. The actual doses taken were not ascertained.
The muscular system shares in the general malnutrition. The muscles become flabby and wasted. Persons addicted to chloral are very frequently of nervous organization and sedentary habits, and hence of poor muscular development prior to the use of the drug.
The kidneys show no constant derangement. In a certain proportion of the cases chloral acts as a diuretic, largely increasing the urinary excretion. Albumen is present in a certain proportion of the graver [p. 663] cases, when it is apt to be associated with anæmia, serous effusions, and a tendency to hemorrhages from mucous tracts. The occurrence of casts and the persistence of albuminuria after the discontinuance of chloral suggest an antecedent or coincidently developed nephritis. The reducing substance present in the urine after small doses of chloral is uro-chloralic acid (Mering and Musulus). It gives the reaction of sugar with the copper and bismuth tests, but is levogyrate. Glycosuria is occasionally encountered.
Vesical and urethral irritation occurs in a small proportion of the cases. When these symptoms vanish upon the discontinuance of the drug and recur upon its resumption, it may be fairly assumed that they are due to its action. A great number of morbid phenomena relating to the genito-urinary tract and to the urine, that have been ascribed to the action of chloral in those addicted to its use, are due to associated conditions rather than to the drug itself.
It has been claimed upon evidence that does not appear to the writer adequate that chloral sometimes acts upon the sexual system as an aphrodisiac, sometimes as the reverse. More or less complete impairment of sexual power and appetite is the rule in individuals addicted to great excesses in narcotics of all kinds. Menstruation is not arrested by chloral as by morphine, nor does it necessarily cause sterility in the female.
The skin undergoes nutritive disturbances of a marked kind. As a result of individual peculiarity, single doses or medicinal doses continued for brief periods of time have occasionally caused erythematous, urticarious, papular, vesicular, and pustular eruptions. Of these, the first named is of most frequent occurrence. The habitual abuse of chloral causes in many individuals chronic congestion of the face, neck, and ears. This redness is often very striking. It is increased by the use of alcohol. Erythematous patches upon the chest, in the neighborhood of the larger articulations, and upon the backs of the hands and feet, also occasionally occur. They are often associated with urticaria. General eruptions resembling measles, scarlatina, and even mild variola, are said to have been observed after large doses of chloral. Purpura is by no means rare in old cases, and falling of the hair and atrophy and loss of the nails occur.
The nervous system bears the blunt of the disturbance, and the more significant symptoms relate directly to it.
The hypnotic effect is usually preserved. Hence the chloral habitué is dull, apathetic, somnolent, disposed to neglect his ordinary duties and affairs. He passes much of his time in a state of dreamy lethargy or in deep and prolonged sleep, from which he awakes unrefreshed and in pain. In one of my cases, however, even larger doses than usual at length failed to induce more than fitful slumber, and the insomnia which led to the formation of the habit finally reasserted itself, reinforced by the unutterable miseries of chloralism.
Headache is a frequent symptom. It is usually general, sometimes frontal, often referred to the top of the head. It is commonly severe, not rarely agonizing, and is described as a pressure, weight, or a constricting band. It is associated with injection of the eyes, flushing of the face, confusion of thought, inability to converse intelligently or to articulate distinctly, and other evidences of cerebral congestion. Vertigo is common.
[p. 664]Sensory disturbances are frequently present. They consist in local areas of hyperæsthesia, more frequently of anæsthesia, numbness of the hands and fingers or of the feet, formication of the surface of the body and limbs, and burning or neuralgic pains in the face, chest, and extremities. The pains in the limbs are almost characteristic. They are acute and persistent, neuralgic in character, but not localized to particular nerve-tracts. They are more common in the legs than in the arms, and occupy by preference the calves of the legs and the flexor muscles between the elbows and the wrists. They do not implicate the joints, are not aggravated to any grave extent by movement, and are often temporarily relieved by gentle frictions. The pains of chloralism have been described as like encircling bands above the wrists and ankles.
Sensations of chilliness alternating with flashes of heat are experienced. The temperature is, in the absence of complications, normal. Excessive doses are followed by a reduction of one or more degrees Fahrenheit, lasting several hours.
Among the motor disturbances are the following:
Tremor.—This symptom is not common. It is neither so pronounced nor so distinctly rhythmical as that of alcoholism or the opium habit. It is increased upon voluntary effort. It affects chiefly the hands and arms and the tongue.
Palsy.—Loss of power in the lower extremities has been observed in a number of instances. It varies in degree from paresis to complete paraplegia. Its occurrence may be gradual or sudden. It passes away upon the discontinuance of the habit. In many respects this condition resembles alcoholic paraplegia.
Impairment of Co-ordinating Power.—Ataxic phenomena are sometimes present. The patient has difficulty in walking in the dark, cannot stand with his eyes closed, has trouble in buttoning his clothes, and the like.
Impairment or Abolition of the Knee-jerk.—In a man aged fifty, who had taken thirty to sixty grains of chloral hydrate at night for eighteen months, the writer observed complete loss of the knee-jerk, which, however, reappeared in the course of a few weeks after the discontinuance of the drug.
In rare cases epileptiform seizures have occurred.
Chloral produces in certain individuals, even as the result of a single dose, congestion and irritation of the conjunctiva. Apart from this idiosyncrasy, its habitual use not infrequently causes conjunctivitis. This affection is occasionally of a severe grade and accompanied by œdema of the eyelids and great photophobia. Retinal congestion has been noted by several observers. Amblyopia, disappearing upon the cessation of the habit, has also been observed.
Psychical Derangements.—The mental and moral perversion caused by immoderate chloral-taking shows itself rapidly. The transient stimulating effects of the dose of opium or morphine in those accustomed to these drugs are seen not at all or to a very slight extent in chloralism. Hence the mental state is characterized by dulness, apathy, confusion, and uncertainty. These conditions alternate with periods of irritability and peevishness. The physical sufferings of the chloral-taker in the daily intervals of abstinence are greater than those of the [p. 665] morphine-taker; his mental depression less. The one is tormented by the agony of pain, the other by the anguish of craving. To the former repetition of the dose brings stupor and sleep, to the latter exhilaration and activity. In certain respects, however, the effects of these drugs upon the mind are similar. They alike produce intellectual enfeeblement, inability to concentrate the mind, habitual timidity, and impairment of memory. In the worse cases of chloralism hallucinations, delusions, and delirium occur. Acute mania may occur, and dementia constitutes a terminal state.
II. Symptoms Due to Abstinence from Chloral.—The symptoms occasioned by the abrupt discontinuance of even large habitual doses of chloral are not, as a rule, severe. In this respect the difference between this drug and opium and its derivatives is very marked. The chloral-taker not infrequently substitutes some other narcotic, as alcohol or opium, for his usual doses without discomfort, and in many instances voluntarily abstains from the drug, without replacing it by others for periods of weeks or months.
The more important of the symptoms induced by sudden discontinuance relate to the nervous system. Insomnia is usual. It is not always readily controlled, and constitutes one of the principal difficulties in the management of these cases. Headache is rarely absent; it is in many cases accompanied by vertigo. Occipital neuralgia frequently occurs, and is often severe. Neuralgias of the fifth pair also occur. Darting pains in the limbs are usual, and the fixed aching pains already described as peculiar to habitual chloral excess are present, and often persist for a long time after the withdrawal of the drug.
Irregular flushes of heat, nervousness, restlessness, inability to fix the attention, formication, burning sensations in various regions of the surface of the body, are unimportant but annoying symptoms.
In a considerable proportion of the cases delirium occurs. It is commonly associated with tremor, great prostration, complete insomnia, sweating, inability to take food, and vomiting, and resembles in every particular the delirium tremens of alcoholic subjects. In the absence of this condition gastric derangements are not of a grave kind. The nausea, vomiting, epigastric pain, and diarrhœa which are induced by the discontinuance of opium are absent, or if present at all only to a slight degree. As a matter of fact, the functions of the digestive system are in a very short time much more perfectly performed than before. Hemorrhage from the stomach, bowel, or urinary tract may also occur.
The conjunctivitis and cutaneous eruptions usually disappear with promptness as soon as the influence of the habitual chloral excesses passes away.
DIAGNOSIS.—The diagnosis of the chloral habit is attended with much less difficulty than that of the morphine habit. In the first place, there is general and often serious derangement of health without adequate discoverable cause. The appetite is poor and capricious, the digestion imperfect and slowly performed; jaundice of variable intensity, often slight, sometimes severe, occurs in many cases; the bowels are not, as a rule, constipated. Dyspnœa upon slight exertion is, in the absence of pulmonary, cardiac, or renal cause, of diagnostic importance. The circulation is, as a rule, feeble. Disorders of the skin, persistent or easily provoked conjunctivitis, puffiness about the eyelids, and a tendency to hemorrhage [p. 666] from mucous surfaces also occur. When with these symptoms, irregularly grouped as they are, we find a tendency to recurring attacks of cerebral congestion, persistent or frequently recurring headaches, and the characteristic pains in the legs, the abuse of chloral must be suspected. This suspicion becomes the more probable if there be a history of protracted painful illness or of prolonged insomnia in the past. The adroitness of these patients in concealing their vice, and the astonishing persistency with which they deny it, are remarkable. In the absence of the characteristic association of pains, conjunctivitis, and affections of the skin the diagnosis is attended with considerable difficulty. It becomes probable from the association of chronic ill-health, not otherwise explicable, with perversion of the moral nature, enfeeblement of the will and of the intellectual forces. It is rendered positive, notwithstanding the denials of the patient, by the discovery of the drug or the prescription by means of which it is procured.
PROGNOSIS.—If the confirmed chloral habitué be left to himself, the prognosis, after excessive doses or the stage of periodical debauches has been reached, is highly unfavorable. The condition of mind and body alike is abject. There is danger of sudden death from cerebral congestion or heart-failure—a mode of termination by no means rare.
On the other hand, the prognosis under treatment may be said to be favorable. The habit is much more readily broken up, and the danger of relapse is far less, than in cases of confirmed opium or morphine addiction. Nevertheless, the underlying vice of organization which impels so many individuals to the abuse of narcotics precludes a permanent cure in a certain proportion of the cases of chloralism. Sooner or later relapse occurs—if not relapse to chloral, relapse to opium, morphine, or alcohol, or into that wretched condition in which any narcotic capable of producing excitement and stupor is taken in excess as occasion permits.
The use of this hypnotic is not unattended with danger. In a single case afterward under the observation of the writer paraldehyde was used in large and increasing doses for the sake of its narcotic properties. The patient, a young married woman whose family history was bad, her mother having died insane, contracted the chloral habit after an acute illness. After some months a cure was effected without great difficulty. She relapsed into chloralism after a second sickness which was attended with distressing insomnia. The habit was again broken up. In consequence of over-exertion in social life during a winter of unusual gayety insomnia recurred. For the relief of this condition paraldehyde was prescribed with success. Notwithstanding its disagreeable and persistent ethereal odor, and the precautions taken by the physician, this lady managed to secure paraldehyde at first in small quantities, afterward in half-pound bottles from a wholesale druggist, and took it in enormous amounts, with the result of producing aggravated nervous and psychical disturbances corresponding to those produced by chloral, but without the disturbances of nutrition attendant upon the abuse of the latter drug. The patient remained well nourished, retained her appetite and digestion, and was free [p. 667] from disorders of the skin and the intense neuralgia which had been present during both periods of chloral abuse. She suffered, however, from a persistent binding headache, disturbances of accommodation, phosphenes, and brow-pains. Under the influence of moderate doses she was enabled to take part in social life with some of her old interest and vivacity. The brief intervals of abstinence which occasionally occurred were characterized by distressing indifference to her friends and surroundings and by apathy and depression. At frequently-recurring intervals the indulgence in excessive doses, constituting actual paraldehyde-debauches, was followed at first by maniacal excitement of some hours' duration, later by profound comatose sleep lasting from one to three days. Upon the complete withdrawal of the drug this patient manifested the symptoms produced by complete abstinence in the confirmed morphine habit—yawning, anorexia, epigastric pains, vomiting, diarrhœa, absolute sleeplessness, extending over several days, heart-failure, collapse, colliquative sweating, and finally well-characterized delirium tremens. At the end of a week, under the influence of repeated small doses of codeine, sleep was secured, and within a month convalescence was complete. This person now continues free from addiction to any narcotic, in good health, and able to sleep fairly well, after the lapse of several months since the complete discontinuance of paraldehyde.
These drugs are habitually used as narcotic stimulants by a limited number of individuals. Cannabis indica, or Indian hemp, the hashhish of the Arabians, is said to be largely used in India and Egypt. It is occasionally taken by medical students and other youths of an experimental turn of mind, but no case of habitual hashhish addiction has come under the observation of the writer.
The use of ether as a narcotic stimulant is occasionally observed among druggists, nurses, and other hospital attendants, but does not give rise to clinical phenomena sufficiently marked or distinctive to demand extended consideration in this article. The same remark may be made of chloroform, which is also used in the same way to a considerable extent among women suffering from neuralgia and other painful or distressing affections of the nervous system. The fact that individuals are every now and then found dead in bed with an empty chloroform-bottle by their side serves to indicate the extreme danger attending the vicious use of this substance.
Cocaine, within the short time that has elapsed since its introduction into therapeutics, has unquestionably been largely abused, both within the ranks of the profession and among the people. Highly sensational accounts of the disastrous effects resulting from its habitual use in excessive doses have appeared in the newspapers and in certain of the medical journals. No case of this kind has fallen under the observation of the writer, and it would appear premature to formulate definite conclusions concerning the effects of cocaine upon the data thus far available.
The treatment of the opium habit and kindred affections is a subject which derives its importance from the following facts: First, the gravity of the disease, as regards the functions both of the body and of the mind; second, the enormous suffering and misfortune, alike on the part of the patient himself and on the part of those interested in him, which these affections entail; third, the fact that they are not self-limited, and therefore cannot be treated with indifference or upon the expectant plan, but are, on the other hand, progressive and gradually destructive of all that makes life worth living, and at last of life itself; and finally, because they are capable at the hands of skilful and experienced physicians of a cure which in a considerable proportion of the cases may be made permanent.
The treatment of these affections naturally arranges itself under two headings: (a) the prophylactic, (b) the curative treatment.
a. Prophylaxis.—It is impossible to overrate the importance of a true conception of the duty of practitioners of medicine in regard to the prophylaxis of the opium habit and associated affections. In communities constituted as are those in which the physicians practise into whose hands this volume is likely to fall, a large—I may say an enormous—proportion of the cases of habitual vicious narcotism is due to the amiable weakness or thoughtlessness of medical men. A majority of the cases occur either in chronic painful affections attended or not by insomnia, or as a result of acute illness in which narcotics have been employed to relieve pain or induce sleep. The chronic affections constitute two classes: First, those manifestly incurable, as visceral and external cancer, certain cases of advanced phthisis, confirmed saccharine diabetes, and tabes dorsalis. In such cases the use of morphine in large and often-repeated doses, although attended with evils and likely to shorten life, amounts to a positive boon. It is neither practicable, nor would it be desirable, to interfere with it. To this class may be added those cases of grave valvular or degenerative disease of the heart where the patient has become addicted to the habitual use of narcotics. Here, notwithstanding the evils resulting from these habits, among which the likelihood of shortening the period of life must unquestionably be counted, the dangers of the withdrawal of the drug are so great that it must be looked upon as neither desirable nor feasible. Attention must, at this point, be called to the fact that great caution is required in the management of pregnant women addicted to narcotics. Incautious attempts to withdraw the habitual drug are almost certain to be followed by speedy loss of the fœtus; and it is to my mind questionable whether anything more than the most guarded reduction of the daily dose should be attempted while the pregnancy continues.
The second class of chronic cases includes individuals suffering from diseases which are remediable or capable of decided or prolonged amelioration. Among these affections are painful diseases curable by surgical procedures, such as certain obstinate and intractable localized neuralgias, painful neuromas, irritable cicatrices, pelvic and abdominal tumors, and surgical affections of the joints and extremities. Here, either before or after radical surgical treatment, an effort to relieve the patient from the bondage of habitual narcotism should be made. For reasons that are [p. 669] obvious, measures having this end in view should be instituted by preference subsequently to surgical treatment. To this class also belong certain painful affections occupying the border-region between surgery and medicine. These are floating kidney, renal and hepatic abscess, calculous pyelitis, cystitis, impacted gall-stones, and thoracic and abdominal aneurism. In these cases the possibility of a cure renders it in the highest degree desirable that the opium habit should be stopped. Whether this attempt should be made while the patient is under treatment for the original affection, or deferred until relief has been obtained, is a question to be decided by the circumstances of the particular case under consideration. Finally, we encounter a large group of chronic painful affections coming properly under the care of the physician in which the opium habit is frequently developed. This group includes curable neuralgias of superficial nerves, as the trigeminal, occipital, brachial, intercostal, crural, and sciatic, and visceral neuralgias, as the pain of angina, gastralgia, enteralgia, and the pelvic and reflex neuralgias of women. Here also are to be mentioned the pains of neurasthenia, hypochondriasis, and hysteria. In this group of affections the original disease constitutes no obstacle to the attempt to break up the habit to which it has given rise.
The practice of using narcotics, especially the preparations of opium, in large and increasing doses for the relief of frequently-recurring pains, especially in neurotic individuals, is a dangerous one. When necessary at all, the use of these drugs should be guarded with every possible precaution. In the first place, in so far as is practicable, the patient should be kept in ignorance of the character of the anodyne used and of the dose. In the second place, the physician should personally supervise and control, in so far as is possible, the use of such drugs and the frequency of their administration, taking care that the minimum amount capable of producing the desired effect is employed. In the third place, the occasional alternation of anodyne medicaments is desirable. Fourthly, an effort—which, unfortunately, is too often likely to be unsuccessful—should be made to prevent repeated renewals of the prescription without the direct sanction, or indeed without the written order, of the physician himself. Finally, the danger of yielding to the temptation to allow a merely palliative treatment to assume too great importance in the management of painful affections must be sedulously shunned. Too often these precautions are neglected, and the patient, betrayed by a dangerous knowledge of the drug and the dose by which he may relieve not only physical pain, but also mental depression, and tempted by the facility with which the coveted narcotic may be obtained, falls an easy victim to habitual excesses. The lowered moral tone of convalescence from severe illness and of habitual invalidism increases these dangers. Yet more reprehensible than the neglect of many physicians in these matters is the folly of the few who do not hesitate to fully inform the patient in regard to the medicines given to relieve pain or induce sleep, and to place in his hands designedly the means of procuring them without restriction for an indefinite period of time. Almost criminal is the course of those who entrust to the patient himself or to those in attendance upon him the hypodermic syringe. No trouble or inconvenience on the part of the physician, no reasonable expense in procuring continuous medical attendance on the part of the patient for the sake of relief from pain, can ever offset, save in cases of the final stages [p. 670] of hopelessly incurable painful affections, the dangers which attend self-administered hypodermic injections.
The uniform and efficient regulation of the sale of narcotic drugs by law would constitute an important prophylaxis against habitual narcotism. Unfortunately, the existing laws relating to this subject are a dead letter. They are neither adequate to control the evil nor is their enforcement practicable. Nostrums containing narcotics, and particularly opium and morphine, in proportions that occasionally produce fatal results are freely dispensed at the shops to all comers. Prescriptions calling for large amounts of opium, morphine, codeia, chloral, cannabis indica, etc. are dispensed to the same individuals at short intervals over the counters of apothecaries for months or years after the illness in which they were originally prescribed is over. Yet more, occasional cases come to light which serve to indicate the appalling frequency with which opium, its tincture, morphine, and solutions of chloral are directly sold to unauthorized individuals. If the evil thus accomplished were better understood, the paltry profit realized from such nefarious trading would rarely tempt men to the commission of the crime which these practices constitute.
Finally, the dissemination of a wholesome knowledge of the methods by which the opium habit and kindred affections are induced, of the serious character of these affections, and of the dangers attendant upon an ignorant and careless employment of narcotics, would constitute an important measure of prophylaxis. I am fully aware of the evils resulting from the publication of sensational writings relating to this subject. Notwithstanding these dangers, I am convinced that a reasonable and temperate presentation of the facts in the popular works upon hygiene used in schools and in the family would exercise a wholesome influence in restraining or curing the tendency to the practice of these vices.
Where these habits have resulted in consequence of the medicinal abuse of narcotics in acute cases from which the patient has long recovered, a determined effort to break them up should at once be instituted.
b. The Curative Treatment.—The responsibility assumed by the physician in attempting to cure patients suffering from the confirmed abuse of narcotics is often a serious one. Much judgment must be exercised in the selection of cases. The responsibility of the physician, beginning as it does with the judicious selection of the cases, does not cease with the active management of the patient until the habit has been completely broken up, but involves for a considerable period of time such continued personal influence and supervision as is needed to avert relapse. It is needless to say that such supervision and influence must, after a more or less extended period, in nearly every case come to an end, but the important fact is to be borne in mind that the danger of relapse becomes less and less with the progress of time; therefore, the more extended the period during which the personal control of the physician may act as a safeguard to his patient the better.
The question as to whether the cure should be attempted in the patient's own home or away from it does not appear to the writer to admit of discussion. Some trustworthy observers12 have reported successful cases not only [p. 671] of the home-treatment of opium-addiction, but even under circumstances in which the patients have been permitted to go at large. Many physicians do not hesitate to undertake the treatment with certain precautions at the home of the patient. On the other hand, those whose experience in the management of these cases is most extended look upon attempts of this kind as likely to be unsuccessful in the great majority of the cases of the opium or morphine habit. In cases of chloralism and the abuse of less formidable narcotics, as cannabis indica, paraldehyde, etc., the home-treatment, if judiciously carried out, usually succeeds, but the cases in which the home-treatment proves successful in curing the confirmed addiction to opium or morphine must be looked upon as exceptional. The reasons for this are obvious. They relate to a variety of circumstances which tend to weaken the mutual relations of control and dependence between the physician and his patient. The doubts, criticisms, remonstrances, even the active interference, of the patient's friends tend to weaken the authority of the physician and to hamper him in the management of the case; the discipline of the sick-room is maintained with greater difficulty; the absolute seclusion of the attendant with his patient is a practical impossibility. Affectionate but foolish friends come with sympathy at once disturbing and dangerous. Some devoted and trusty servant cunningly conveys from time to time new supplies of the coveted drug, or, if these accidents be averted, the very consciousness of the separation which amounts to a few feet of hall-way only is in itself a source of distress to the patient and his friends alike. Furthermore, the period of convalescence following the treatment is attended with the greatest danger of relapse—a danger which is much increased by the facility of procuring narcotics enjoyed by the patient in his own home as contrasted with the difficulties attending it away from home under the care of a watchful attendant. The desirability of undertaking the treatment away from the patient's home can therefore scarcely be questioned. That this plan is more expensive, and that it involves a radical derangement of the ordinary relations of the patient's life, are apparent rather than real objections to it. The very expense of the cure within the limits of the patient's ability to pay, and the mortification and annoyance of temporary absence from usual occupations and seclusion from friends, are in themselves hardships that enhance the value of the cure when achieved, and constitute, to a certain extent, safeguards against relapse. Whether the treatment can be more advantageously carried out in a private asylum designed for the reception of several such cases, or in a private boarding-house, or at the home of the physician himself, is a question to be determined by circumstances. The writer is of the opinion that with well-trained and experienced attendants, well-lighted, airy rooms in the upper part of a private house are to be preferred on account of the seclusion thus secured.
12 See, for example, Waugh, “A Confirmed Case of Opium-addiction treated Successfully at the Patient's Home, with Remarks upon the Treatment, etc.,” Philadelphia Medical Times, vol. xvi., March 20, 1886.
In general, two methods are recognized: (a) that of the abrupt suppression of the drug, and (b) that of the gradual diminution of the dose. Both of these methods demand the isolation of the patient, and to some extent at least the substitution of other narcotics. The isolation of the patient under the care of skilled and experienced attendants may be secured in a suitable private boarding-house, in the home of a physician, or in a private room of a well-appointed general or special hospital. Favorable opportunities are also afforded in private institutions devoted [p. 672] to this purpose. The apartment occupied by the patient should be so arranged as to guard against attempts at suicide, and the furniture should be of the simplest character. The heating and lighting arrangements must be such as to render any accidental injury to the patient during paroxysms of sudden maniacal excitement quite impossible. From the beginning of the treatment the patient must under no circumstances be left alone. Two attendants are required, one for the day and one for the night. They should be not only skilful and experienced, but also patient and firm; and, as a considerable proportion of the patients are persons of education and refinement, intelligence and good manners are desirable on the part of those who must be for a length of time not only the nurses, but also the companions, of the sufferer. It is desirable that the separation of the patient from his family and friends should be made as complete as possible. During the continuance of the active treatment no one should be admitted to the patient except his physician and regular attendants. Communication with his friends by letter should be interdicted. The enforcement of this rule must be insisted upon. So soon as the acute symptoms caused by the withdrawal of the drug subside and convalescence is fairly established, brief visits from judicious members of the family in the presence of the nurse may be permitted. At the earliest possible moment open-air exercise by walking or driving must be insisted upon, and change of scene, such as may be secured by short journeys or by visits to the seashore, is useful. These outings require the constant presence of a conscientious attendant.
The Treatment of the Opium and Morphine Habit.—a. The Abrupt Discontinuance of the Drug: the Method of Levinstein.—This method is thus described by the observer whose name it bears: Directly upon admission the patient is given a warm bath, during which time careful examination of his effects is made by a responsible person for the purpose of securing the morphine which the patients, notwithstanding their assertions to the contrary, frequently bring with them. These measures of precaution are by no means unnecessary. An officer had saturated his cigarettes and cigars with a solution containing opium, and smoked for twenty-four hours almost without interruption. Another officer had slipped morphine between the soles of new slippers. Other individuals concealed immediately after their arrival morphine in powder in the upholstery of the sofa, upon the canopy and in the ventilators of the windows. Other patients enclosed morphine in envelopes of thin paper, which were placed between the leaves of their books, stitched it in the folds and lining of their garments, etc.
The first symptoms of the withdrawal of the drug show themselves in delicate individuals at the end of three or four hours, and in robust persons about fifteen hours, after the last dose. These symptoms consist of malaise, restlessness, a sense of muscular tension, chilly sensations, and the like, but do not demand treatment. As soon as shivering commences the patient must be put to bed—a measure to which, as a rule, he readily assents on account of the sense of muscular fatigue now experienced. For the relief of the headache, which is rarely absent, applications of cold water or of ice or ether-douches to the forehead may be employed. For the distressing gastralgia compresses moistened with chloroform may be applied to the epigastrium. The colic, which is often distressing, [p. 673] may be treated by sinapisms or hot compresses. The nausea and vomiting and epigastric distress, which are apt to continue for several days, may be treated by a solution of bicarbonate of sodium with tincture of nux vomica and essence of mint. If the vomiting be excessive, recurring twenty or thirty times in the course of twenty-four hours, small doses of morphine by the mouth must be given. If by reason of the continued vomiting and inability to retain nourishment dangerous exhaustion develops, nutritive enemata must be administered. The diarrhœa requires little treatment during the early days. If, however, it be excessive and persists beyond the third or fourth day, large enemata of warm water of a temperature of 98° F., repeated two or three times during the day, are attended by excellent results. The insomnia, which constitutes a most distressing symptom, defies every kind of treatment during the first three or four days. During this time prolonged baths are not well borne, and even when they are employed they scarcely produce more than half an hour or an hour of sleep. Chloral is also, under these circumstances, inadmissible, whether administered by the stomach or by the rectum. It does not induce sleep, and its employment is very often followed by a high degree of excitement. After the fourth day it is well borne by many persons, and manifests its usual hypnotic property. Warm baths of five minutes, followed by cold affusions, exert an excellent influence upon the general debility and mental depression of the first days. The objections of patients to these baths cease after they have experienced the excellent results which follow their use. During the bath stimulants, such as champagne, port, and hot bouillon, may be given. Care must be paid to the alimentation from the very beginning of the treatment. During the first days liquid nourishment should be given, and abundance of wine and other alcoholic beverages according to the previous habits of the patient. Some nourishment is to be given every hour or every two hours. Many patients experience an intense craving for alcoholic drinks; others, on the other hand, are unable to take them. To the former wine, beer, etc. may be given freely during the first three or four days; to the latter a restricted milk diet may be given, one to two quarts in the course of twenty-four hours. Such is the method of Levinstein, to which he adds, however, important modifications for those—and their number is large—who are unable to bear the abrupt withdrawal of the drug.
This method is attended in all cases by indescribable sufferings, and in many by serious dangers. Among the last, collapse and delirium tremens demand special consideration. The collapse which occurs in a certain proportion of the cases requires prompt and energetic treatment. The pulse becomes feeble, small, gradually or suddenly diminishes in frequency; the countenance is pale; the previous agitation gives place to an ominous calm; there is a tendency to syncope, accompanied by persistent somnolence and slowing of the respiration. Inhalations of ammonia and the administration of aromatic spirits of ammonia, champagne, brandy, or hot coffee, with frictions of the surface and cold applications to the head, may occasionally produce reaction. As a rule, however, it is necessary to administer a hypodermic injection of morphine. This condition of collapse, once having shown itself, is apt to recur upon the same or the following day. The treatment of the delirium tremens [p. 674] consists in isolation, the administration of abundant nourishment, the use of the bromides, chloral, or paraldehyde, with alcoholic stimulants. As this complication is unattended by danger to life, and usually disappears in the course of a few days, the administration of morphine is not required.
The modifications of this method suggested by Levinstein for those who are unable to bear the abrupt suppression of the drug are as follows: The patient is isolated and guarded; for two or three days his habitual dose is administered, this duty being performed by the physician himself. The drug is then abruptly discontinued. At the end of twenty-four hours the phenomena of abstinence are manifested; the pulse loses its regularity, distressing diarrhœa and vomiting occur, etc. These symptoms are controlled by the injection of morphine, the dose being much smaller than that to which the patient has been accustomed. By this means the sufferings of the patient are ameliorated, and the dangers attendant upon the rapid suppression of the drug are averted. At the end of twenty-four hours it becomes necessary to again administer the drug, but in diminished dose. After a time it is discontinued altogether.
b. The Gradual Diminution of the Dose.—This method is now generally employed. It consists in isolation of the patient with proper attendants and the progressive diminution of the dose. The drug should always be administered by the physician himself. The rapidity with which it is suppressed will be determined by the circumstances of the individual case. The time occupied should not exceed ten days. In the majority of cases it will be much shorter than this. If the administration of morphine to correct urgent symptoms be at all required after this time, it will be at most on one or two occasions at intervals of twenty-four or forty-eight hours. When the process of reducing the dose is too greatly prolonged, the sufferings of the patient are unnecessarily aggravated. As the diminution progresses the relief produced by each dose is followed by distressing reaction. The anticipation of smaller doses from time to time or from day to day is a matter of great distress to patients. After a while their courage and endurance fail them, and they seek by every possible means to secure at least one good dose of the coveted drug.
The symptoms produced by the suppression of the drug speedily show themselves, increasing in intensity as the dose diminishes. Temporary amelioration is, however, produced by each of the successively diminishing doses of the drug. Whatever may have been the method followed by the patient, the hypodermic injection of morphine is to be preferred in the treatment. The disturbances of the digestive system which speedily appear require but little special medication. The danger of inanition which attends the complete loss of appetite, the inability to take ordinary food, and the frequent often uncontrollable vomiting, are best met by the systematic administration of easily assimilable liquid diet, consisting of lime-water and milk, milk and Vichy water, pancreatized milk, koumiss, concentrated broths, the expressed juice of fresh partly-cooked beef, and the various commercial foods used in the artificial feeding of infants. Vomiting rarely occurs immediately after the ingestion of articles of this kind. If it takes place in the course of an hour, some degree of digestion and absorption will have taken place. Should, however, all food be rejected by the stomach, efforts at rectal [p. 675] alimentation must be attempted. Efforts to control the vomiting by medicines other than the administration of opium or morphine in some way are not usually attended by success. The diarrhœa is usually frequent, the stools being liquid, sometimes small, often copious, and amounting in number from eight or ten to thirty or more in the course of twenty-four hours. They are not usually attended by pain. Some relief to this symptom follows the administration for a time of large doses of bismuth subnitrate (grs. xx to xxx) every second, third, or fourth hour. The sinking feeling at the pit of the stomach and the epigastric pain are to some extent alleviated by external applications. Hot fomentations or compresses containing a few drops of chloroform or turpentine are also useful.
The derangement of the respiratory system, which consists usually in a certain amount of bronchitis with more or less cough and some dyspnœa aggravated by exertion and movement, does not usually require special treatment.
Disturbances of the circulation constitute a very important group of symptoms, and require close watching always, active interference frequently. For the relief of the phenomena due to flagging action of the heart the recumbent posture, external warmth, friction of the extremities, the application of turpentine stupes or mustard to the præcordial and epigastric regions, the inhalation of ammonia or the administration of preparations of ammonia, and sometimes digitalis, which may be given either by the mouth or hypodermically, will be required. Alcohol, however, will prove in the greater number of cases a most useful remedy—in many an indispensable one. It may be given in the form of milk-punch, hot toddy, or of port, champagne, etc., according to the requirements of the case. Failure of the circulation may, notwithstanding every effort to control it, reach such a degree as to jeopardize the patient's life. Under such circumstances the treatment must be interrupted by the immediate administration of small but efficient doses of morphine, which, if necessary, must be repeated. As diarrhœa increases the quantity of urine excreted rapidly diminishes. It may not exceed eight or ten fluidounces in the course of twenty-four hours. After the third or fourth day of the treatment the urine in a considerable proportion of cases contains albumen and occasionally casts. The oliguresia is largely due to the excessive loss of fluid by the bowel, and does not require treatment. Nor, indeed, is active treatment demanded by the albuminuria, which usually spontaneously subsides in the course of a few days, although it sometimes persists for some weeks or months. Persistent albuminuria requires appropriate treatment.
The nervous symptoms, which constitute a most important group, are favorably influenced by methodical alimentation and the free use of alcoholics. Care must be taken to reduce the amount of alcohol administered as convalescence progresses. With the re-establishment of the normal functions of the body, the disappearance of insomnia, and improved nutrition, alcohol may in the majority of cases be rapidly diminished or wholly withdrawn. This course, favored by the regular life which the patient should be obliged to lead on becoming convalescent, and the feeling of general bienaise which is gradually developed as the cure progresses, is rendered especially important by the fact that a considerable proportion of opium-habitués are individuals of unstable nervous organization, which in itself constitutes a powerful predisposing influence to alcoholism.
[p. 676]It seems hardly necessary to describe in detail the treatment demanded for the relief of the varied disturbances of the nervous system. The use of coca in the form of a good preparation of the wine or fluid extract in appropriate doses, to which may be added tincture of cannabis indica, exerts a favorable influence. The administration of cocaine by the mouth and hypodermically has in some instances seemed to me to be followed by favorable results. It is not, however, to be adopted as a routine practice, by reason of its occasional depressing effect and the possible danger of replacing the opium habit by a craving for cocaine. Lupulin, and in particular an ethereal extract of lupulin, exerts a favorable but not very powerful influence in tranquillizing the nervous system. With the view of controlling to some extent the insomnia, the hypodermic injections should, during the early part of the treatment, be so timed that the period of sleep or drowsiness which they produce should occur during the night. As soon as the number of injections is reduced to one daily, that one should be administered at the latest convenient hour before midnight. For twenty-four or forty-eight hours after the final discontinuance of morphine but little effect may be expected from ordinary doses of other sleep-inducing drugs. Chloral in single large doses (grs. xx to xxx), either alone or associated with a corresponding large dose (grs. xl to lx) of one of the bromides, administered on the second or third night after total suppression, is very often followed by prolonged, tranquil, and refreshing sleep. Caution must be observed, however, in administering chloral so long as the indications of feeble circulation persist. Paraldehyde, although less certain, is a less dangerous hypnotic under such circumstances. Massage, hot baths, and the cold pack are all useful adjuvants to the treatment. The sweating when copious and distressing is favorably influenced by sponging with hot alcohol.
The abject mental state of the patient calls for much firmness, gentleness, and tact on the part of the physician and attendants. Every effort should be made to inspire courage and hope. Neither the importance of the symptoms nor the intensity of the sufferings of the patient should be underrated; nevertheless, the ordeal is a limited one. In the majority of instances, to get rid of the opium means to get well, because opium, unlike alcohol, does not leave permanent structural lesions of any organ. The expectation of a radical cure must therefore be confidently presented to the patient as a consolation in his sufferings.
With the return of convalescence sexual power is restored and menstruation is re-established. Insomnia and muscular weakness usually persist into the convalescence for some weeks, and only gradually yield to careful regulation of the daily life of the patient, with abundant nutritious food, open-air exercise, and change of scene. The insomnia of this period constitutes a serious symptom, for the reason that it constantly subjects the patient to the temptation to return to the use of hypnotics. In the course of time, however, the normal physical and mental condition is regained, and the patient may be permitted to return to his former pursuits and associations.
The Treatment of the Chloral Habit.—That which has been said in the foregoing pages concerning the prophylaxis against the opium habit applies with equal force to chloral and other narcotics. The curative treatment of habitual addiction to chloral is attended neither by the [p. 677] difficulties nor the dangers which are encountered in the management of the opium habit. The symptoms attending the discontinuance of chloral are less severe and less persistent; in fact, individuals accustomed to the taking of large doses of chloral not infrequently voluntarily discontinue its use for considerable periods of time. As a rule, the treatment may be carried out at home, the patient, however, being isolated and cared for by a watchful attendant. The drug should be stopped at once. For the first few days alcoholic stimulants should be freely given. Systematic feeding, pepsin, full doses of quinine, followed after a time by strychnia, and, as soon as the condition of the digestive system will permit of it, by iron, fulfil the general indications. Cod-liver oil and malt extracts may be given with advantage. Cardiac failure, collapse, and delirium tremens are to be treated in the same manner as similar complications occurring in the treatment of the opium habit. Vomiting is much less likely to occur, and when present is less persistent and less difficult of management. Diarrhœa does not usually prove troublesome, the bowels, on the contrary, being constipated. The latter condition yields to mild laxatives or to simple enemata. Hemorrhages from the various mucous tracts may be controlled by fluid extract of ergot, the hypodermic injection of solution of ergotin, minute doses of wine of ipecac, or fluid extract of hamamelis. The conjunctivitis which is occasionally present usually subsides spontaneously upon the discontinuance of chloral. It may be treated by instillations of a 2 per cent. solution of cocaine and mild borax lotions (grs. v to fluidounce j). The after-treatment must be carefully carried out. Relapses are less frequent than after the opium habit.
The Treatment of Habitual Addiction to Paraldehyde, Cannabis indica, Ether, Chloroform, etc. must be based upon the general principles indicated in the foregoing pages. Cases of the habitual abuse of these drugs are comparatively infrequent on the one hand, and on the other do not often present the serious and progressive symptoms produced by excesses in opium and chloral; hence they come but rarely under the care of the physician, except in those unhappy individuals in whom the propensity to vicious narcotism is such that any drug capable of producing excitement and oblivion is made the means of gratification, and all are used by turns as the opportunity occurs.
DEFINITION.—The term chronic lead-poisoning is used to designate the morbid phenomena induced by the gradual accumulation of lead in the organism.
SYNONYMS.—Plumbism, Saturnism, Morbus plumbeus, Molybdosis, Molybdonosus, Intoxication saturnine, Bleivergiftung.
CLASSIFICATION.—Chronic lead-poisoning manifests itself in serious disorders of nutrition which are widespread and implicate all the tissues of the body; but for the reason that its more striking and characteristic symptoms relate to the nervous system, it has been classed among disorders of that system as a toxic neurosis.
Acute poisoning by lead is an entirely different affection. It depends upon the power of the salts of lead to coagulate albumen. Its symptoms are those of acute corrosive gastritis; derangements of the nervous system are secondary. It does not fall within the scope of the present article.
HISTORY.—Chronic lead-poisoning must have existed from the infancy of the arts in which the metal is employed. It does not, however, appear to have been recognized until after the time of Hippocrates. Celsus was aware of the danger attending the administration of lead. Nicander, Dioscorides, Aretæus, and Paul of Ægina recognized lead colic and the paralysis resulting from its long-continued introduction into the stomach. Among Arabian physicians, Rhazes and Avicenna accurately describe the effects of the preparations of lead. No considerable addition to the knowledge of the subject was made until the seventeenth century. In 1616 was printed at Poitou the famous work of Citois, De novo et populari apud Pictones dolore Colico bilioso Diatriba. The epidemic colic described by this author was caused, although he little suspected it, by the common use of wine which had been treated by lead to remove its acidity. This practice, which is of very ancient date, and is described in the writings of Cato, Pliny, and Columella, was at one period very general in Europe, and had been forbidden by imperial ordinances as early as 1437.1 It remained for Stockhausen, in a treatise published at Goslar in 1656, and entitled De Lythargyrii Fumo, noxio, morbifico ejusque metallico frequentiori morbo vulgo dicto Hutten-Katze, to demonstrate that Poitou colic was produced by lead in particles in [p. 679] emanations, and for Wepfer in 1671 to first clearly point out the fact that the epidemic colic so often described was usually caused by lead in wine. During the eighteenth century the epidemic colic attracted much attention among medical men, and its etiology was made clear. Henkel called the affection founder's colic, and showed how it was produced in those engaged in casting lead; Huxham, in his work on Fevers (1745), described the disease as it prevailed in Devonshire, and several English observers conclusively proved that the epidemics of colic frequently appearing in certain districts were caused by the presence of lead in cider, and that it was due to the action of the apple-juice upon lead used in the construction of the presses and implements employed in the manufacture of that popular beverage.
1 Vide Tanquerel des Planches, Lead Diseases, translation by S. L. Dana, M.D., LL.D., Lowell, 1848.
During the current century the closer study of the etiological relations of disease has revealed many unsuspected sources of lead-poisoning in the arts, and of lead contamination, both accidental and intentional, in articles of food, drink, and luxury. Hence the literature of the subject has assumed very extensive proportions. The French physicians have devoted much attention to this subject. The great work of Tanquerel des Planches, to which reference has already been made, remains to this day the most complete and comprehensive authority. Quite recently valuable additions to existing knowledge have appeared in some of the Paris theses.2
2 Vide Capelle, De l'Intoxication saturnine, Paris, 1883; Séguin, Ch., De l'Albuminurie transitoire des Saturnins, Paris, 1883; Goudot, Étude sur la Goutte saturnine, Paris, 1883; Verdugo, Contribution à l'Étude de la Goutte saturnine, Paris, 1883; and Coutard, La Colique du Poitou considérée comme Intoxication saturnine, Paris, 1884.
ETIOLOGY.—A. Predisposing Influences.—Individuals exposed to lead and its compounds are not all equally prone to its effects. The degree of liability is to some extent dependent upon individual susceptibility, and to a much greater extent upon circumstances which are determined by the season, climate, age, sex, diet, and mode of life of different persons. It will be convenient to consider the predispositions which arise from occupation under the head of the Exciting Cause.
Variations in the degree of susceptibility to chronic lead-poisoning appear to be explicable in a majority of the cases solely upon the theory of idiosyncrasy. While a large proportion of the cases are in well-developed, strong, and previously healthy adults, individuals of feeble constitutions do not escape. Those occupations which involve the greatest exposure to the danger of contracting this affection at the same time demand the powers of a robust frame. Habitual recognition of these dangers, such as begets the habitual exercise of reasonable precautions against them, diminishes to some degree the liability of a few workmen.
Season.—Due allowance being made for the difference in the number of workmen employed in manufactures which involve exposure to lead, and especially in the making of white lead, at different seasons of the year, it has been found that attacks of lead colic and of lead palsy are more common in warm than in cold weather. Heat predisposes to the attack, either by favoring the dissemination of the lead compounds or by facilitating their absorption by various channels, especially by the skin, which is more freely exposed in summer, and at the same time more or less bathed in sweat in which the dust of lead salts may be dissolved.
[p. 680]Climate.—In the absence of definite statistics upon the subject, it appears probable that the dangers of chronic lead-poisoning would be greater in warm than in cold climates. The clinical features of the affection are alike in all parts of the globe.
Age.—The majority of individuals attacked are adults. Nevertheless, children employed in occupations involving exposure to lead are attacked with great frequency—so much so that it may be concluded that their liability is in fact greater than that of adults.
Sex exerts a decided influence, women being, under nearly similar circumstances, less frequently attacked than the men employed in the same factories—a fact to be explained only by their greater willingness to exercise the recognized precautions.
Diet does not constitute a predisposing influence. It is nevertheless probable that a deficient diet favors the development of the affection. Excesses in food, and especially excesses in drink, predispose to lead colic.
The mode of life is important. Those who lead sober, regular, and, above all, cleanly lives are less liable to the affection than the intemperate, irregular, and careless. Particularly are the dangers in factories increased by neglect of ventilation. Persons suffering from affections of the digestive tract are not, among lead-workers, more prone to lead colic than their comrades who are free from such diseases.
B. The Exciting Cause.—Metallic lead is probably inert, but, owing to the ease and rapidity with which it oxidizes and forms salts, lead in any form, if introduced into the body continuously for a length of time, produces characteristic toxic effects. The oxides, acetates, and carbonate of lead, being soluble in the gastric juice, act more surely.3 But the sulphate, the least soluble of the lead compounds, may also have this effect (Gasserow).
3 Naunyn, Ziemssen's Encyclopædia, vol. xvii.
The channels by which lead is introduced into the body are the alimentary canal, the respiratory tract, and the cutaneous surface. Hence the modes of introduction are of almost endless variety. The conveyance of lead into the stomach constitutes the most common as well as the most important means of access to the organism. This may be in the form of medicine, as the acetate, the unduly prolonged use of which, even in moderate doses, sometimes produces chronic poisoning. Articles of diet are not infrequently contaminated by lead derived from different sources, of which the most common is the lead glaze of earthenware vessels, which is soluble in acid fluids. According to Naunyn, beer drawn through lead pipes may cause chronic lead-poisoning, which has also been frequently ascribed to the use of shot in cleaning bottles used for wine and malt liquors. Drinking-water is occasionally contaminated with lead derived from pipes made of this metal and cisterns painted with lead colors. Pure water, freed from gases, does not act upon lead when the air is excluded. In the presence of air, however, an oxide of lead is formed which is partially soluble in water. If nitrates, nitrites, and chlorides, such as constitute ingredients of sewage, are also present, they form soluble compounds with lead and increase the proportion of lead salts soluble in the water. For this reason water contaminated by sewage is rendered decidedly more dangerous if carried in leaden pipes. On the [p. 681] other hand, the purer the water the greater the danger. Hence rain-water and pure spring-water cannot safely be stored in cisterns painted with lead colors nor conveyed in leaden pipes, nor can lead covers be used for cisterns, because of the condensation of the vapor of water, which drops back, holding lead salts in solution. The sulphates, phosphates, and carbonates usually found in river-waters form insoluble lead compounds, which, being deposited upon the interior of the pipes, act as protectives and prevent further chemical changes.
Still more common is the accidental conveyance of lead dust and lead compounds to the mouth in consequence of their adhering to the hands or settling from the atmosphere upon articles of food and drink, in the case of workmen engaged in the various arts in which lead is freely used. As a rule, to which the exceptions are rare, the more severe cases of chronic lead-poisoning occur only among workers in lead, as miners, those employed in white-lead factories, painters, typesetters, plumbers, and lapidaries.
Potters engaged in the glazing of common pottery and tiles, workmen in file-factories, workers on colored papers and in enamels, especially in glass enamels, brushmakers for the reason that the bristles are sometimes colored by lead preparations, and those engaged in sewing coarse goods because the thread is sometimes treated with a preparation of lead in order to add to its weight, are likewise liable to chronic lead-poisoning. The introduction of lead into the body through the respiratory tract is a subject of the greatest importance in the trades. Inadequate ventilation of working-rooms, living or sleeping in apartments connected with or contiguous to factories in which lead is largely used, and particularly in lead-factories, is attended with serious dangers, as is also the habit of eating food in such apartments or drinking water that has been standing in them. The possibility of lead-poisoning by way of the respiratory tract has been questioned. In view of existing knowledge as to the readiness with which carbon in minute states of subdivision finds its way into the connective lymph-channels of the lung, there can be no doubt that the habitual respiration of an atmosphere loaded with the dust of lead or its preparations in a minute state of subdivision may give rise to chronic lead-poisoning. At the same time, the experiments of Hassel4 render it probable that less absorption takes place directly by means of the pulmonary mucous membrane than by way of the mucous membrane of the mouth and throat. It must be borne in mind that none of the preparations of lead are volatile. This affection is also occasionally observed in clowns and others upon the stage or elsewhere, who habitually use cosmetics containing lead. The use of cheap tinfoil, into the composition of which lead enters largely, as a wrapper for tobacco and snuff is said to occasionally produce chronic lead-poisoning. It is stated by Naunyn that mattresses filled with horse-hair died black by lead compounds have occasioned this affection. The same authority states that a proof-reader was poisoned by reading printed proof for many years. Chronic lead-poisoning is pre-eminently a disease of the industrial arts. The means of obviating or diminishing the dangers of those exposed by their occupation to the preparations of lead will be considered under the head of Prophylaxis. [p. 682] The quantity of lead absorbed is of less importance than is its continuous introduction. As stated in the definition, the phenomena of chronic lead-poisoning are those brought about by the gradual accumulation of lead in the system, the amount absorbed into the blood in any given cases being comparatively small, even where large quantities are ingested. Hence prolonged exposure to small amounts of lead is attended with greater danger than a comparatively brief exposure to larger quantities. It is stated that the members of the household of Louis Philippe at Claremont manifested the symptoms of chronic lead-poisoning after the lapse of seven months in consequence of drinking water which contained a mere trace of lead. On the other hand, several grains of acetate of lead may often be administered medicinally to patients for a week at a time without inducing the phenomena of this affection, although, in view of the idiosyncrasy of many individuals, the exhibition of lead preparations for prolonged periods is not advisable.
4 The Inhalation Treatment of the Diseases of the Organs of Respiration, including Consumption, London, 1885.
According to Heubel,5 the blood and internal organs contain but very small amounts of lead—.02 per cent. in the maximum. It is probable, therefore, that the more insoluble of the lead compounds may yield a sufficient amount of absorbable lead to produce the characteristic constitutional effects.
5 Pathogenese und Symptome der Chronic Bleivergiftung, Berlin, 1871.
So long as the urine remains free from albumen, it serves for the elimination of a mere trace of lead. In albuminous urine the amount is larger. Lead is found in the bile and feces in small quantities.
SYMPTOMATOLOGY.—The general description of chronic lead-poisoning must include a great number of symptoms that do not always occur in regular order or sequence. According to the prominence of certain of these symptoms in particular cases the specific effects of lead may be grouped under the following five heads: (1) disturbances of nutrition; (2) the colic; (3) the arthralgia; (4) the paralysis; and (5) lead encephalopathy.
1. Disturbances of Nutrition—After the long-continued introduction of lead into the system the signs of impaired nutrition manifest themselves in almost all cases. The appearance of the patient is changed; he becomes thin, anæmic, and of a somewhat peculiar yellowish complexion. This hue of the skin, to which the term icterus saturninus has been applied, is not due to the deposition of bile-pigments. The wasting of the tissues of the body seems to implicate the muscular to a much greater extent than the adipose tissues. In the majority of cases a dark or bluish-black line is observed at the border of the gums. This line is more strongly marked in the upper than in the lower jaw. It is, as a rule, more plainly developed in persons of careless habits, whose teeth are the seat of deposits of tartar, but the teeth in such individuals are often discolored and appear to be elongated in consequence of the retraction of the edge of the gums. This bluish or violet-black gingival line is due to the deposit of particles of sulphide of lead in the substance of the gum, in consequence of the reaction between the sulphuretted hydrogen formed by the decomposition of particles of food and the lead particles present in the mouth. According to Tanquerel, this color may extend over the greater part of the gum or even to the mucous membrane of other portions of the mouth. If due care be exercised, there is little danger [p. 683] of confounding the lead-line with the livid border of the gums frequently seen in people whose teeth are in bad condition. The occasional absence of this line in otherwise well-characterized cases of chronic lead-poisoning is to be noted. It does not occur when the teeth have been lost, and is slight if they are kept clean.
Patients complain of habitual dryness of the mouth and of an insipid, mildly astringent, sweetish, or faintly metallic taste; the tongue is coated, the breath fetid. There are nausea and occasional vomiting. Constipation is common. The patient is now liable to attacks of lead colic, joint trouble, and the specific palsy, or to cerebral disturbances of grave character. Of these affections, colic is the most frequent; the joint affection is next in order; the paralysis far less common, and the cerebral disturbances comparatively rare. Continued exposure results after a time in an intensification of the malnutrition, either with repeated attacks of colic or the other specific disturbances, or occasionally in their absence, although at length the positive lead dyscrasia is established, characterized by obstinate dyspepsia, constipation, and intensification of the curious earthy or yellowish color of the skin, which is succeeded by the pallor of profound anæmia. Loss of muscular power with transient œdema now shows itself. The patient becomes apathetic, irritable, and morose. As the condition of cachexia deepens muscular tremor occasionally shows itself. After a prolonged period of profound ill-health the patient succumbs to some complication, among the more frequent of which are tuberculosis, pneumonia, and chronic interstitial nephritis. Gout is a very common complication of chronic lead-poisoning.
2. Lead Colic; Colica saturnina; Colique de plomb; Bleikolik.—This affection is also known as painter's colic, Devonshire colic, colica pictonum, the last term being derived from Poitou. It occasionally develops abruptly without previous symptoms. In the majority of cases, however, the earlier disturbances of nutrition before pointed out precede the attacks, often by a period of weeks or months. An increased tendency to constipation with transient recurrent abdominal pains, occurring sometimes immediately after food, more frequently at irregular intervals, often characterizes the prodromic period. There is, moreover, an intensification of the other symptoms of chronic lead-poisoning. The appetite is decidedly impaired, so also are the powers of digestion; the foul condition of the mouth becomes more annoying, and the peculiar taste alluded to more persistent and more marked. Constipation occasionally alternates with diarrhœa. The colicky pains which constitute the attack are of variable intensity, but usually severe. They are of the nature of true colic. Pressure over the seat of pain almost invariably gives relief, particularly in severe attacks. During the remission pressure is grateful to the patient. The position of the pain varies. Its most common seat is in the region of the umbilicus. It may occupy the epigastric and hypochondriac regions or the lower part of the abdomen, extending from side to side above the level of the pubic bone. These colics are of some minutes' duration, recurring after short intervals, which are characterized by a certain amount of continuous cramp. Tenesmus is frequent. It may be accompanied by strangury or retention of urine, with pain in the course of the ureters, the spermatic cord, or in the penis. Shooting pains in the breast also occur. The abdomen [p. 684] is retracted, and scaphoid to such an extent in some instances that the prominence caused by the bodies of the vertebræ is apparent in the median line of the abdomen. It occasionally happens, however, that retraction does not occur, the belly, on the other hand, remaining prominent. As a rule, to which there are few exceptions, the bowels are constipated. This condition is often stubborn. In rare cases, however, the colic is accompanied by diarrhœa. Nausea is of common occurrence. Vomiting is sometimes violent and distressing, being ushered in by repeated attacks of retching. The vomited matters are usually discolored by bile, and icterus of slight degree usually occurs. The pulse is invariably diminished in frequency, sometimes as low as 40 or even 30, per minute. It is at the same time full and tense. The pulse-frequency is occasionally variable within comparatively brief periods of time. Respiration is increased in frequency during the attack. The urine is small in quantity and of high specific gravity, and frequently contains small amounts of albumen. It is sometimes entirely suppressed. Fever is absent, and the slight increase of temperature occasionally observed is attributable to the restlessness of the patient. The intellectual condition usually remains clear, but in violent cases it is characterized by excitement. The paroxysms of pain are more severe in the latter part of the day and during the night. The course of the attack is irregular. Relapses, which may occur in the course of some days or even weeks, are frequent. The duration of the attack does not, as a rule, exceed a week, but the illness is often protracted by repeated relapses, and in continued exposure to the cause the tendency to colic may become chronic. The termination of the attack is in most instances as abrupt as its onset, and with the cessation of the colic the associated symptoms, such as retraction of the abdomen, constipation, vomiting, and diminished frequency of the pulse, rapidly subside. Lead colic is not unfrequently associated with the other affections of chronic lead-poisoning. The prognosis is favorable, the mortality being about 2 per cent.
3. The Arthralgia; Arthralgia saturnina.—The tissues entering into the formation of the joints and the muscular masses contiguous to them are frequently the seat of intense paroxysmal pains, which appear more or less suddenly, either with or without prodromes, and run a course similar to that of lead colic, exhibiting violent exacerbations and occasional more or less complete remissions. These pains are accompanied by painful contractions of the muscles. They are somewhat relieved by pressure and friction and aggravated by exercise and exposure to cold. Swelling and redness over the affected joints, ligaments, and tendons are absent. These pains do not follow the course and distribution of the nerve-trunks, and lack the tender pressure-points of true neuralgias. They are more common in the lower extremities, the knee being especially apt to be affected. When they affect the upper extremity the elbow and shoulder suffer more frequently than the other joints. The flexor muscles are much more frequently attacked than the extensors. The muscles of the back, especially the great masses of long muscles in the lumbar region, whose function is to sustain the equilibrium of the body, are frequently implicated. The intercostal muscles and the muscles of the neck are also frequently affected. The small joints and the muscles of the hands and feet as a rule escape. The pain is tearing and burning in [p. 685] character, and very often severe. It is occasionally associated with tremor. The derangement of the alimentary canal, especially constipation, which is so characteristic of lead colic, is often absent. Fever does not occur.
A careful study of these cases establishes the fact that in a considerable proportion of them the morbid condition is myalgic. Whether it be due to simple muscular malnutrition or to some specific action of lead upon the muscle-substance is not determined. The analogy between these muscular pains and lead colic renders it probable that in a large majority of the cases the latter view is correct. These pains are frequently associated with the attack of lead colic; sometimes, however, they precede the colic, while at other times they follow it. After a series of remissions and exacerbations the pain often ceases as suddenly as it began. As in other lead affections, relapses are frequent. The prognosis is favorable.
The English physicians, and especially Garrod,6 Todd,7 and Bence Jones,8 have insisted upon the frequency of gout in chronic lead-poisoning. Murchison,9 Wilks,10 and others regard this association as causative. This view has not found general acceptance in France. Lancereaux11 in particular, after a comparative study of the lesions of the kidney and of the joints in saturnine cachexia and the corresponding lesion of gout, concludes that the gouty kidney and the kidney of lead-poisoning have the same appearance, and are simply varieties of interstitial nephritis, and that the articular and arterial lesions in both affections are identical. So-called saturnine gout differs in no respect, either in its clinical or anatomical characters, from ordinary gout. It would therefore appear superfluous to describe saturnine gout. At the same time, it must be insisted upon that chronic lead-poisoning exercises an important influence in the production of gout—a causal relation due to the fact that lead diminishes the excretion of uric acid.
6 Medico-Chirurg. Transactions, 1854, vol. lvi.
7 Clinical Lectures, London, 1856.
8 Transactions of the Pathological Society, London, 1856.
9 Lancet, 1868.
10 British Medical Journal, 1875.
11 “Nephritis et Arthrites saturnines: coincidence de ces Affections paralleles avec la Nephrite et l'Arthrite goutteuse,” Arch. gén. de méd., Decembre, 1881.
4. Lead Palsy; Lead Paralysis; Paralysie Saturnine; Bleilähmung.—This condition is fourth among the affections due to chronic lead-poisoning, both in frequency and in the order of succession. Nevertheless, like each of the others, it may be the first in the order of appearance after disturbances of nutrition which are in some rare cases of very slight degree. As a rule, however, the paralysis has been preceded by colic or by joint affection, or by both. Tanquerel12 found that in 88 cases of lead palsy 25 had been preceded by an attack of colic, 15 by two attacks, 3 by ten attacks, 1 by fifteen attacks, and that in single cases as many as twenty, and even thirty, attacks of lead colic had occurred before the appearance of paralysis.
12 Loc. cit.
The length of time over which habitual exposure to lead without the development of palsy may extend was found by the same observer to vary from eight days to ten, twenty, or even twenty-five years. One individual first suffered from paralysis after fifty-two years of exposure.
Without dwelling upon the sources of error in statistics of this kind, [p. 686] it must be conceded that they establish in a general way the extraordinary differences in the susceptibility of individuals. There are persons who every time they are attacked with colic, of whatever degree of severity, suffer also from paralysis. Others, on the contrary, suffer from repeated attacks of violent colic without the development of paralysis.
Lead palsy is an affection of adult life. Of 102 cases, 2 only occurred in individuals below twenty years of age.
Like the other specific lead affections except the encephalopathy, palsy is more common in the summer than at any other season.
Those who have once suffered are very liable to successive attacks. Tanquerel and Maréchal have observed many returns of paralysis, presenting the characters of the original attack, many years after the patient had withdrawn from exposure to lead.
Perverted sensations of the parts about to be affected, such as coldness, numbness, and hyperæsthenia, may precede the attack. Impairment of motor-power, manifested by feebleness, stiffness, or awkwardness and tremor, also appears in the prodromic period. This trembling consists in slight agitation of the muscles, rather than in well-marked rhythmical contractions. These precursors may indeed constitute the attack, which occasionally, and especially under treatment, terminates at this point. The prodromic symptoms are less severe during the day, while the patient is at work; at night they are aggravated. After some days they end in the characteristic paralysis. Colic is a common precursor. After the attack some stiffness of the muscles is experienced, which terminates by rapid loss of power or abruptly in actual palsy. Occasionally encephalopathy precedes the paralysis. It is rare that prodromes are wholly absent.
In the great majority of the cases the upper extremities and the extensor muscles are first attacked. If the paralysis be slight other muscles may escape. The characteristic form of lead paralysis consists in loss of power in the extensors of the hands and fingers, especially of the extensor communis, without implication of the supinator longus. The muscles affected are in the region of distribution of the musculo-spinal nerve. The deformity is known as wrist-drop. Next in order, the triceps and deltoid are most frequently attacked. The lower extremities commonly escape for a considerable time. When attacked, the extensor muscles of the feet and toes are the first to suffer.
Paralysis of the dorsal muscles occurs in rare instances. It gives rise to a peculiar stooping, uncertain, and tottering gait. Paralysis of the intercostal and laryngeal muscles was observed by Tanquerel. Paralysis of the muscles of the face or of those of the eye has never been observed in consequence of lead-poisoning. The loss of power never corresponds strictly to the distribution of the branches of a single nerve-track.
The paralysis, as a rule, affects both sides, and frequently the corresponding muscles of the two extremities. Sometimes, however, the affected muscles of the two sides are not the same, and it occasionally happens that the affection is limited to one side. In very rare cases, the arm and leg on the same side being paralyzed, the affection resembles hemiplegia.
Local paralysis may be limited to the extensor muscle of a single finger [p. 687] or may involve all the muscles of a limb. There may be slight impairment of power in the flexor muscles. The enfeeblement of certain flexor muscles, especially of those of the fingers, may, Naunyn suggests, be only apparent, the position of the hands being in pure extensor paralysis unfavorable to the exercise of the flexors and limiting their function.
Sensation is not, as a rule, affected in lead paralysis. Pains in the paralyzed muscles, in neighboring muscular masses, and in the structures about the joints often precede the attack of paralysis. Anæsthesia of the skin is rare. When present, it is usually of slight degree, and corresponds to the region of the paralysis. Deep anæsthesia has also been observed.
Atrophy of the paralyzed muscles is constant and rapid. It frequently reaches a high degree, causing characteristic deformities, which are rendered more marked by the fact that the adjacent non-paralyzed muscles preserve to a great extent their original state of nutrition. As the neuro-muscular lesion progresses other deformities arise, in consequence of derangements of the balance of force between opposing muscles and from other causes. Among these deformities are partial or complete dislocations of the more movable joints, as the shoulder and phalanges, with the formation of tumors, which, when they occupy the dorsum of the hand, might be carelessly mistaken for the nodosities of gout. It is to be noted that the latter are occasionally present as complications.
There is rapid diminution, and finally complete loss, of the reaction to the faradic current. With the galvanic current the reaction of degeneration is usually well marked. The reaction of degeneration may be demonstrated in the extensors of the limbs in lead-poisoning before wrist-drop has occurred.
The course of lead palsy is very variable. In a few cases it is progressive. When local emaciation or atrophy arrives at the last degree of marasmus, the skin seems glued to the bones, to such an extent are the paralyzed parts wasted; the muscles especially are so thinned that the contour of the bones is easily distinguished. If the paralysis attack the whole of the limb, then this organ, abandoned to its own weight, stretches the ligaments and permits the head of the bone to leave its cavity. In other rare instances the paralysis remains stationary for long periods of time, only to grow worse after each new attack of lead disease. Much more frequently lead paralysis disappears spontaneously or under treatment in the course of some days or weeks. The convalescence is gradual, and usually rapid, when the gravity of the lesion is considered; occasionally it is complete in the lapse of a few days.
The prognosis depends upon the degree of lead cachexia present, the possibility of withdrawing the patient from the exposure, and finally upon the degree and extent of the paralysis and of the atrophy. It is rendered unfavorable by the necessity of the prolonged exposure of the patient to lead, by a high degree of disturbance of the general nutrition of the patient; and by the fact of his having presented for a considerable period the evidences of lead disease, with occasional attacks of colic or arthralgia; by the complete loss of power and electrical reactions in the affected muscles; and, finally, by absolute wasting of the muscular masses. The prognosis is less favorable in relapses than in the primary attack.
[p. 688]Progressive muscular atrophy has been frequently observed in patients suffering from lead disease (Naunyn).
5. The Encephalopathy; Encephalopathia Saturnina.—This term was suggested by Tanquerel to designate collectively the various morbid cerebral phenomena produced by chronic lead-poisoning. It embraces, therefore, those affections due to the action of lead upon the central nervous system, and occasionally described as lead insanity, delirium, convulsions, epilepsy, coma, etc. It is, of all the disorders produced by lead, the most rare. Tanquerel met with seventy cases only. It occurs only in those individuals who are exposed to large quantities of lead, and in such a manner as to favor the absorption of the metal and its compounds by the digestive and respiratory tract. Hence house-painters and the workers in lead-factories supply the greater number of cases. The time of exposure elapsing before the manifestations of the special morbid action of the poison upon the nervous system show themselves varies from a few days to many years. In a large proportion of the cases the time has been less than one year.
Women are much less liable than men—a fact clearly due to the nature of their occupations even when involving exposure to lead.
The majority of the cases have occurred between the ages of twenty and fifty. Alcoholic habits, insufficient and unwholesome diet, privations, exposure, and an irregular life especially predispose those working in lead to the affection. Lead encephalopathy has developed with nearly equal frequency in warm and in cold weather. Relapses are frequent.
Among the prodromes are headache, vertigo, agitated and interrupted sleep marred by distressing dreams, and troublesome insomnia; derangements of the special senses, dimness of vision, alterations of the pupils, tinnitus aurium; dysphagia and a sense of constriction of the pharynx have also preceded the attack of cerebral disorder. It is usually preceded likewise, and often by a considerable lapse of time, by the other lead affections above described—namely, colic, arthralgia, and palsy. Psychical derangements—stupor, apathy, or excitement—also precede the attack. In a small number of cases lead encephalopathy has occurred abruptly without prodromes.
The symptomatology is exceedingly variable and irregular. Three forms, the delirious, the comatose, and the convulsive, have been described. These conditions may succeed each other in the same attack. The delirium is variable in kind. It is apt to be at first tranquil; after some time it becomes paroxysmal and furious. It is broken by intervals of somnolence. At length true sleep supervenes, and the patient awakes restored almost completely to his reason.
Coma may develop suddenly, even instantaneously. In a very few cases the comatose form has developed itself alone during the course of chronic lead-poisoning. As a rule, however, it is preceded by delirium or convulsions.
The convulsive form is the most common. The convulsions may be partial, involving the face or the one side of it, a single limb, or one side of the body. They may be general, without loss of consciousness. These incomplete attacks are apt to be followed, after a period of dulness or unconsciousness, by acute eclampsia. Epileptiform attacks may now follow each other in rapid succession, ending in more or [p. 689] less profound coma. The attacks are sometimes separated by intervals of uneasiness, restlessness, or delirium. These attacks continue several days. If they are very violent and frequent death may rapidly supervene. In favorable cases consciousness is gradually restored, or the patient may awaken suddenly from his drowsiness after some hours or a day.
These attacks are not preceded by an aura.
Amaurosis is among the more important of the symptoms produced by the action of lead upon the nervous system. It is usually accompanied by dilatation of the pupils. The amaurosis gradually disappears as the other symptoms subside, and with the improvement in sight the pupils contract. Recovery is frequently complete. Occasionally vision does not return with the improved general condition. Norris13 saw, in two cases of lead-poisoning due to the use of white lead as a cosmetic, marked choking of the discs in connection with severe cerebral symptoms. The terminal condition, when recovery does not take place, is that of nerve-atrophy.
13 See this System of Medicine, Vol. IV.
Albuminuria is common in this as in other lead affections. It may be of moderate amount and due to the rapid breaking-down of the blood-corpuscles which marks the exacerbation of the general condition. Albuminuria may be a direct consequence of the eclampsia. Finally, it may be due to coexisting nephritis.
The prognosis is in a high degree unfavorable.
MORBID ANATOMY AND PATHOLOGY.—There are no well-characterized anatomical lesions in chronic lead-poisoning. Lead has been found in almost every organ and tissue in the body. It exists in combination with the albumen of the tissues. The changes in the nervous system that have thus far been described are neither constant nor characteristic. The same is true of the lesions of the intestines. The paralyzed muscles are found to have undergone atrophy, with loss of the striæ and increase of connective tissue. The nerve-trunks are also the seat of atrophic degeneration.
The mode of action of lead is not yet determined. The view of Henle, that lead acts chiefly upon the unstriped muscular fibre, was at one time generally accepted, and served to explain many of the characteristic phenomena of the disease. On the other hand, there is much in the clinical history to support the opinion of Heubel, that its primary action is upon the nervous system. Whether the peripheral degeneration by which the paralysis is to be explained is primary or secondary to central degeneration in the anterior cornua of the gray matter of the spinal cord, is yet in dispute. Some of the forms of encephalopathy are doubtless due to the nephritis which is found in many cases of chronic lead disease, and are, in fact, symptoms of uræmia. In the great majority of the cases this is not the case. The morbid condition must be explained by the direct toxic action of lead upon the central nervous system. No theory adequate to account for all the cerebral manifestations has yet been suggested. Naunyn has pointed out the resemblance between the nervous and psychical derangements in lead encephalopathy and those which characterize chronic alcoholism, and suggests that lead, like alcohol, produces these effects not as a direct poison, but indirectly in consequence of abnormal nutrition of the whole system, brought about [p. 690] by the continued circulation of a foreign poisonous material in the blood.
Chronic Lead-Poisoning in Animals.—Animals exposed to lead under conditions favorable to the development of the lead affections in man suffer in like manner. Instances of this kind are of frequent occurrence in and about large lead-factories. The drinking of water containing lead also gives rise to these affections in animals. Horses, dogs, cats, and fowls have frequently suffered from lead colic. Horses used in lead-factories suffer from a form of laryngeal obstruction due to lead paralysis of the muscles of the larynx. Relief has followed tracheotomy and the introduction of a canula, and removal to an atmosphere free from lead has resulted in recovery. Cats who spend some time in red-lead workshops frequently are paralyzed. Even the rats in lead-factories become paralytic (Tanquerel).
DIAGNOSIS.—The diagnosis of the affections due to chronic lead-poisoning is, as a rule, unattended with difficulty. The malnutrition, anæmia, poor digestion, foul mouth, stubborn constipation, and the gingival line, considered in connection with the history of prolonged or habitual exposure to lead, would warrant the assumption that the relation between this poison and the symptoms is a causal one. When there is added colic, arthropathies, and paralysis, or the cerebral states having the characters above described, the assumption becomes a certainty. The absence of any one of the ordinary phenomena, such as the blue line or constipation, would still leave the clinical picture sufficiently full to justify the diagnosis. The reaction of degeneration, which is usually marked in saturnine wrist-drop, with the escape of the supinators, distinguishes it from pressure paralysis of the musculo-spiral.
TREATMENT.—A. Prophylaxis.—Free ventilation and scrupulous cleanliness constitute, in general terms, the most efficient safeguards for those whose occupations involve prolonged exposure to lead. Workmen employed in lead-factories and those otherwise exposed to lead should be compelled to wash their hands and change their outer clothing before eating; they should also bathe regularly every day on leaving work; under no circumstances should they be suffered to eat or sleep in or near the workshops. As all kinds of work in the manufacturing of lead preparations are not attended with equal risk, the workers should from time to time be transferred from one department to another or from in-door to out-door work. In order to prevent the constant rising of dust, the floors are to be kept constantly sprinkled or covered with moist sawdust. It is unnecessary to go into further details in regard to the hygiene of the subject. It is probable that towels and sponges worn over the mouth, or other forms of respirators, because of the inconvenience which they occasion and the false sense of security which attends their use, are of less value than has been generally supposed.
It appears scarcely needful to here insist upon the avoidance of cosmetics and hair-dyes containing lead, or upon the exercise of reasonable prudence in the matter of the manufacture, sale, and use of articles of food or drink which are liable either by accident or design to become adulterated with lead compounds.
The use of sulphuric-acid lemonade is a measure of prophylaxis of less real value than was at one time supposed, seeing that the sulphate of lead [p. 691] is in itself capable of producing the disease. Occasional doses of magnesia sulphate are of use where a tendency to constipation exists. Workmen who begins to show signs of chronic lead-poisoning should without delay abandon their work and seek some occupation free from its peculiar dangers.
The precautions against the use of water contaminated with lead have been pointed out under the heading Etiology.
B. Curative Treatment.—When the disease shows itself, no matter in what form, the primary indication is the discontinuance of exposure to lead. Chronic cases of malnutrition, constipation, functional nervous disorder, will occasionally be found upon careful search to depend upon long exposure to lead in some unsuspected way. The cause being removed, such cases often promptly recover.
Measures aimed first at the separation of the lead from the tissues, and then at its elimination from the body, constitute a rational treatment. Sulphur baths and the internal administration of sulphur may be employed with a view of converting the lead eliminated by the skin and mucous membranes into an insoluble sulphide, and thus preventing its resorption. Repeated laxative doses of castor oil will remove unabsorbed lead from the intestinal canal. The plan of treatment at present in general favor consists in the combined use of potassium iodide and magnesium sulphate. From five to twenty grains of the iodide are to be given in not less than six or eight fluidounces of water three times daily, the stomach being empty: two hours after each dose one or two drachms of the magnesium sulphate are to be taken; after this dose an ordinary meal.
This treatment is designed to dissolve the lead deposited in the tissues, and cause its elimination by the mucus of the alimentary canal in part, and to a slight extent also by the urine. The magnesium sulphate tends to remove such lead as finds its way into the alimentary canal thence with all possible rapidity. These measures, together with the removal of the patient from further exposure, exert of themselves a favorable influence upon the malnutrition and anæmia. Quinine, strychnine, iron, cod-liver oil may be advantageously administered as the toxic effects of the lead pass away.
The colic demands the administration of opium or its derivatives to relieve the pain, which is commonly excruciating. For this purpose the hypodermic injection of morphia is our most efficient remedy. Alum in doses of twenty to thirty grains every four or six hours is useful in lead colic.
For the relief of the local paralytic affections local as well as general treatment is necessary. Massage is of great use, especially when combined with passive movements. Galvanism, one large electrode being applied to the cervical vertebræ, the other to the extensor surface of the affected limbs, is followed by excellent results. Labile currents of fifteen or twenty cells should be thus applied, the poles being changed several times at each sitting. As the nutrition of the muscles improves faradic currents may be occasionally substituted. Persevering treatment is necessary to obtain the best results.
For the present relief of the arthralgia gentle frictions with or without anodyne liniments must be employed. The hypodermic use of morphine [p. 692] may become necessary in cases in which the pain is urgent. It is, however, here as elsewhere, to be if possible avoided. The tendency to recurrent joint-pains rapidly disappears as the poison is eliminated from the organism.
For the relief of the severe cerebral symptoms which are described under the term Encephalopathy special treatment is of little avail. All observers agree in recommending an expectant plan. The measures of treatment directed against the general condition, as above described, must be steadily continued. The influence of chronic lead-poisoning upon pregnancy is very deleterious. Constantine Paul14 and others have shown that the early death of the fœtus very constantly occurs. The prompt removal of women who have become pregnant, from all exposure to lead, and energetic medicinal treatment, are needed to obviate the danger of abortion.
14 Arch. gén. de Méd., vol. xv., 1860.
DEFINITION.—Progressive unilateral facial atrophy is a disease characterized by progressive wasting of the skin, connective tissue, fat, bone, and more rarely muscles of one side of the face.
SYNONYMS.—Progressive facial hemiatrophy, Neurotic atrophy of the face (Virchow), Facial trophoneurosis (Romberg), Prosopodismorphia (Bergson), Atrophy of the connective tissue of the face or Laminar aplasia (Lande).
HISTORY AND LITERATURE.—This disease has been known to the medical profession since 1825, when, according to Eulenburg, it was first described by Parry. The Index Catalogue contains references to thirty books and articles on the subject in various languages. Eulenburg gives a bibliography which contains thirteen references not given in the Index Catalogue. One personal case, which will be detailed later, has fallen under observation. In all, I have collected from fifty to sixty cases. The number of reported cases is slowly increasing; nevertheless, the disease must still be regarded as rare. Carswell,1 according to Lasègue,2 first arranged scientifically the various lesions which might arise in consequence of a retardation and arrest, or even inverted action, in nutrition, and at the same time that he assigned their causes pointed out the several forms of atrophy. Aran3 has written a contribution on the subject, furnishing valuable material for classifying atrophies. Romberg called general attention to the disease in his clinical researches, published in 1846. He described the disease under the name of a new form of atrophy of the face, and took the position that it was a primary trophoneurosis. Of contributions by American writers, a paper by Bannister4 is the most complete and valuable. This not only contains two fully and carefully reported cases, but also a thorough discussion of special symptoms and the pathology of the disease. The chapter of Eulenburg5 contains an excellent sketch of the disease, and is especially valuable for the discussion of the various theories as to its nature.
1 Illustrations of the Elementary Forms of Disease, 1836.
2 Archives générales de Médecine, May, 1852, p. 71.
3 Ibid., Sept. and Oct., 1850.
4 Journal of Nervous and Mental Disease, vol. iii., No. 4, Oct., 1876, p. 539.
5 Ziemssen's Cyclopædia of the Practice of Medicine, vol. xiv., 1877.
ETIOLOGY.—The disease is of much more frequent occurrence among females than males. Out of 25 cases which I have been able to classify, [p. 694] 9 were in men and 16 in women. It is an affection of comparatively early life. The following were the ages of 25 patients: under ten years, 7; from ten to twenty years, 11; from twenty to thirty years, 6; over thirty years, 1.
Graefe6 reports a case due to syphilis, in which there was also paralysis of the left oculo-motor externus and trigeminus. In one of Bannister's cases the patient had suffered repeatedly from slight frost-bites. Among the causes which seem to be thoroughly established traumatism holds the first place. The affection could be traced to injury in a fair number of the published cases. A case is reported by Maragliano7 of a child who had a fall in which she struck the left half of her face, and in consequence of which a circumscribed swelling appeared near the external angle of the left eye and remained for a few days. Shortly after this the left half of the face began to grow smaller than the right. Schuchardt8 speaks of a fall on the head which left a cicatrix on the right parietal bone below the coronary suture, the injury being followed by facial atrophy. Panas9 reports a case in which the wasting of the face followed a fracture of the lower jaw. In one of two cases reported by Bannister,10 a man, aged forty-two, is stated to have been thrown from a stage-coach, falling on his head, and not losing consciousness, but receiving a scalp wound over the coronal suture. Subsequent to this time he had cerebral symptoms, physical and mental, and unilateral facial atrophy developed.
6 Quoted by Rosenthal.
7 Note di Clinica Medica, Genoa, 1881, translated by Joseph Workman, M.D.—Alienist and Neurologist, vol. ii. No. 2, April, 1881, p. 146.
8 Quoted by Eulenburg.
9 Bull. Soc. de Chir. de Par., 1869, 1870, 2d S. ex., 198, and Gaz. des Hôpitaux, 1869.
10 Journ. Nerv. and Ment. Dis., Chicago, 1876, iii. pp. 539-560.
SYMPTOMATOLOGY.—Before discussing the symptomatology I will give brief notes of the following case, which has not been before reported, and which was observed by me while in charge of the Nervous Dispensary of the Hospital of the University of Pennsylvania several years since.
C——, aged seventeen, white, a mill-operative, had a good family history. Three years before coming under observation a white spot appeared in the skin over the right malar prominence, and since that time this side of the face had gradually atrophied. When this patient was first examined the skin had a mottled appearance. Close examination showed that the skin, connective tissue, and bone were decidedly wasted, and there seemed also to be some loss of substance in the muscles of the right side of the face. The mouth, however, could be closed properly, the lips showing no puckering or drawing to one side. The right half arches of the palate were atrophied. The uvula was drawn slightly but positively to the left. Careful examination of the membrane of the drum of the right ear showed it to be atrophied. An ophthalmoscopic examination of both eyes was made, but no changes were discovered. No changes were noted in the hair of the patient on the affected side. He was able to perform all movements with the facial muscles, but the creases and contours of the face in repose and in motion were less marked on the right side than on the left. The skin of the right side of the face seemed to be bound closely to the bone. The muscles on the same side responded well to [p. 695] the faradic and galvanic current. The patient had at times a peculiar sensation of stinging in the atrophied half of the face. He was treated with electricity, local massage, and tonics, and did not improve, but did not get worse while under observation, a period of several months.
At the Hospital of the University of Pennsylvania I also observed one well-marked case of unilateral atrophy of the tongue without atrophy of the face, of which, unfortunately, I have not preserved the notes. The patient was a middle-aged man with a syphilitic history. The atrophy in the reported cases has occurred much more frequently upon the left than upon the right side of the face.
Changes in the skin are among the most constant and striking phenomena. By some dermatologists the disease is regarded as a form of morphœa, the keloid of Addison. Morphœa as described by Duhring11 occurs in the form of patches, rounded, ovoid, or irregular in outline, small or large, tough or leathery, smooth or shiny, and may also manifest itself in the form of atrophic pit-like depressions in the skin. The skin alterations differ somewhat in character; frequently one of the first signs of the disease is the appearance of a white spot on the cheek. This was the first noticeable phenomenon observed in the above case. After a time this spot or patch may change in color, becoming of a yellowish or brownish hue. A number of spots appearing and undergoing change, the skin after a time assumes a mottled appearance. In some of the reported cases a yellowish, or yellowish-gray, or brownish appearance is recorded as having been present. In these the observations were probably made after the affection had existed for some time, and in them the white spots or patches were probably at first present. In one of Romberg's cases, first recorded when the patient was nine and a half years of age, he noted the deposit of a yellowish-gray pigment which began at the median line and extended to the angle of the jaw across the lower half of the face and neck, divided here and there by portions of healthy skin. Discoloration, varying in intensity, also existed in irregular patches on the upper part of the face and on the forehead. The discolored tissues were glossy and greasy-looking. The skin adhering to the bone often gives the patient an aged appearance. Pruritus has been several times observed.
11 Medical News, vol. xlv. No. 4, July 26, 1884, p. 85.
Changes take place in the hair. Sometimes it simply changes color; at other times it falls out or ceases to grow. The beard or hair of the head will thus be gray or white upon one side, or in one or two locations of one side and not of the other; or the hair may be absent or simply thinned out. Peculiar limitations in the extent to which the hair is affected are sometimes observed. In one of Romberg's cases, for example, complete absence of the eyelashes from the inner angle of the eye to the middle of the lids was noted; the hair was very thin, and in some parts altogether wanting, and the left eyebrow was almost entirely devoid of hair. The changes which take place in the color of the hair in some severe cases of chronic trigeminal neuralgia will be recalled in this connection. I have known of several instances in which a few locks of hair were turned gray or white on the neuralgic side. Anstie, author of the work on Neuralgia, was a sufferer from supraorbital neuralgia, and the eyebrow of the same side contained a white tuft. Facts of this kind [p. 696] serve to corroborate and emphasize the view that unilateral facial atrophy is a tropho-neurosis.
Anidrosis, or absence of perspiration, on the atrophied side of the face is a nearly constant phenomenon. In one of Bannister's cases, a printer, attention was first called to the patient by the fact that in working a hand printing-press in the hot weather he perspired only on the right side of his face. The left side remained perfectly dry, no matter how warm the temperature or hard the labor. This hemidrosis, or unilateral sweating, was confined only to the right side of the forehead, the right cheek, side of the nose, and lip. On the chin it encroached a little on the left. Under the chin and in the throat there was a little excess of perspiration on the right side; on other portions of the body no difference was noted. Nicati12 considers a combination of symptoms, several of which were present in a recorded case—namely, lowered temperature, stoppage of perspiration, and wasting of the side of the face—as indicating a paralysis of the sympathetic nerve in what he calls its second or more advanced stage. In true facial hemiatrophy, however, other phenomena of such paralysis are wanting. Brunner13 gives a case in which perspiration, tears, mucous secretions, and temperature were all diminished on the affected side, and in which were also present exophthalmos and dilatation of the pupil. The cervical sympathetic in this case was irritated by a tumor. I agree with Bannister, however, that while we cannot exclude the possibility of the participation of the sympathetic in hemiatrophy of the face, the evidence is not sufficiently positive. Mechanical interference with the sweat-glands by pressure or otherwise has been suggested. The true view to take would seem to be that the perspiratory disorder is due to the same central or peripheral neurotic affection which gives rise primarily to the atrophy. Eulenburg says that the secretion of the sebaceous follicles is in most cases diminished or stopped on the atrophied side, while the sweat-glands often act in a normal manner; but his experience does not seem to correspond with that of the majority of other observers.
12 Sur Paralysie du Nerf sympathetique-cervical, Lausanne, 1873, quoted by Bannister.
13 St. Petersburger Med. Zeitschr., ii., 1871, quoted by Bannister.
Seguin, Dreschfeld, and others have found no notable differences in surface temperature between the two sides of the face. In one of Bannister's cases the temperature was tested in both ears, and a difference of six-tenths of a degree Fahrenheit in favor of the ear of the unatrophied side was found, that of the left ear being 97.6°, and that of the right 98.2°. This examination was repeated on another occasion with nearly the same result.
Weakness of pulsation in the carotid of the affected side has been observed. Sometimes the power to blush is lost on the affected side, but this may return. In one instance the cheek, having been reddened by electrical stimulation, so remained for an hour or more.
Paræsthesiæ, such as pain, numbness, and stinging sensations, are not uncommon. A diminution of the general tactile sensibility of the skin of the affected side has been observed by Tanturri14 and by Vulpian,15 and perhaps by others, but anæsthesia is not commonly present.
14 Il Morgagni, 1872, quoted by Bannister.
15 L'Appareil vaso-moteur, ii. p. 430.
Eulenburg and Guttmann found atrophy of the muscles supplied by the motor branch of the fifth nerve—namely, the masseter and temporal. [p. 697] The changes which take place in the muscles of the affected side are, so far as can be judged, not of the character of fatty degeneration. Probably a general and uniform shrinkage of calibre of muscular fibres and bundles occurs. Certainly, this would seem to be true of the muscles supplied by the portio dura. The muscles on the atrophied side respond to both the faradic and galvanic currents, reactions of degeneration not being present. The absence of the reactions of degeneration in the facial muscles shows that normal muscular fibres remain. In one reported case the facial muscles seemed at first to react more readily than in normal conditions. The muscles of the upper lip sometimes appear to have wasted, preventing full closure of the mouth on this side. Fibrillary twitchings have been observed only very rarely. Voluntary control over the muscles of the affected side is not impaired.
In one of Bannister's cases the first upper molar of the left side sometimes ached, and the gum and bone were so wasted as to expose its roots for a considerable distance. Falling out of the teeth has been observed in a few other cases.
Atrophy of the tongue is associated with the facial wasting in a certain percentage of cases, and the uvula and soft palate are also sometimes wasted. On the other hand, atrophy of the tongue has been observed as an isolated phenomena.
Atrophy of the bones of the face is frequently present, and has been determined by careful measurements. It will show to a greater or lesser extent according to the age of the patient. When the disease arises after the bony development has been fully acquired, there will be little external evidence of osseous involvement; when it begins during the time of active growth of the bone, as it does not infrequently, the arrest in the skeleton will be very apparent. Thus in a number of cases beginning in early childhood bone atrophy has been a very marked feature.
Eulenburg says that the functions of taste, smell, hearing, and seeing are not interfered with in any of the reported cases; but Bannister reports impairment of the sense of taste in both of his cases. In one the whole left half of the tongue was involved, in the other only the left posterior third. In the first of these, in which the whole left half of the tongue was involved, both the glosso-pharyngeal and the chorda tympani nerves were affected. According to Bannister, the significance of this observation is that either the glosso-pharyngeal and fifth nerves are both involved, or that the taste-fibres for the base as well as tip of the tongue are derived from the last-named nerve. In this case, however, which was due to a severe injury, the headache, mental confusion, loss of hearing, etc. more probably indicated a widespread intracranial lesion, affecting to some degree the nucleus of the glosso-pharyngeal. In the other case, which was apparently a typical one of unilateral facial atrophy in its early stage, no history of traumatism was present, and the sense of taste, which was carefully tested several times, was seriously impaired over the left posterior third of the tongue.
Bannister discusses the probable cause of impairment of taste in each case, as follows: “The atrophy seemed to involve the region supplied by the second division of the fifth nerve as much as, or more than, the other divisions; and on this is situated the spheno-palatine ganglion which gives off the Vidian nerve, the upper division of which, the superior [p. 698] superficial petrosal nerve, is supposed by Schiff to contain the taste-fibres, which return from the lingual nerve through the chorda tympani. The usual theory of this disease is that it depends upon an affection of the trophic fibres contained in the fifth nerve or one or more of its divisions. Accepting this theory, Baerwinkel,16 noticing a case of unilateral atrophy of the face affecting only the second division of the fifth, and, as he held, indicating trouble with the spheno-palatine ganglion, its trophic centre, mentions the fact that there was no impairment of taste in the anterior portions of the tongue as rather against the hypothesis of Schiff as to the course of the taste-fibres. At the same time he gives two other observations of lesions of the trifacial and the seventh nerve that favor it. In our patient I should have expected a priori to have found the taste affected in the anterior portion of the tongue, if anywhere, but the reverse was the fact. It is difficult to suppose an accidental lesion of the glosso-pharyngeal coexisting with the one of the trigeminus that produces the atrophy when there are no more signs of nervous disorder than there were in this case. On the other hand, the taste-fibres of the glosso-pharyngeal are not generally supposed to have such connections with the fifth nerve as to be involved in its disease, while those of the chorda tympani, of the connections of which with the trigeminus there is much more physiological evidence, escape. The observation is a contradictory one, and I cannot at present explain it.”
16 Deutsch. Archiv f. klin. Med., xvii. 1, 1875.
So far as I know, ophthalmoscopic changes have never been noted. In a few cases enophthalmos, or sinking in of the eye, doubtless due to the disappearance of orbital fat as the disease advances, has been recorded.
Defects of hearing, and even partial deafness, have been reported in a very limited number of cases, making it questionable whether this symptom is a coincidence or a complication. In the case reported by me careful examination of the membrane of the tympanum by W. Ziegler of the ear department of the Hospital of the University of Pennsylvania showed atrophy of this membrane.
Eulenburg speaks of one case in which the external atrophy had reached as far as the larynx, and in which the pronunciation of the letter r was somewhat impeded. Beverly Robinson,17 reports a case accompanied with slight paralysis of the adductors of the vocal cords. The laryngeal paralysis in this case improved under treatment, which led Robinson to believe that the relation between the two affections might have been only one of coincidence.
17 Am. Journ. Med. Sci., October, 1878, p. 437.
Flascher18 has described a unique case of bilateral facial atrophy occurring in a woman twenty-three years old. When an infant she fell and injured her forehead, and soon afterward had an attack of measles without eruption. Shortly afterward the atrophy appeared. Tactile sensibility was diminished and the secretion of sweat absent. The masseter, temporal, and facial muscles and bones were atrophied. External strabismus of the left eye was present; the pupil of this eye was dilated, irregular, and non-reactile; sight was diminished, the optic disc atrophied. This case would appear to differ somewhat from true facial hemiatrophy. It was probably a peripheral nerve affection following measles.
18 Berliner klin. Wochenschr., 1880, No. 31.[p. 699]
Mitchell19 has reported a case of absence of adipose matter in the upper half of the body. I had an opportunity of examining this patient, who was exhibited at a meeting of the Philadelphia Neurological Society, and noticed that both sides of the face presented a striking similarity to the affected side in cases of unilateral atrophy. The muscles were apparently not affected. Mitchell suggests the possibility of separate centres capable of restraining deposits of adipose tissue.
19 Am. Journ. Med. Sci., July, 1885.
DURATION AND TERMINATION.—The disease pursues a slow but generally progressive course. In a few instances, after having attained a certain development, it seems to have remained stationary for many years. Nothing could better illustrate the slow progress or stationary character of this affection than the study which Virchow made in 1880 of a patient whose case had been described by Romberg more than twenty years before. After comparing the patient's present condition with that described in notes taken twenty-one years before, Virchow was not able to convince himself that any material alteration had occurred in the atrophic parts; in fact, he regarded the disease as having long ago become stationary. Cases reported by Tanturri, Baerwinkel, and others bear out the same view as to the stationary character of the affection in some cases.
COMPLICATIONS.—In a case of Virchow's, in addition to the facial atrophy the patient presented atrophy which, commencing in the distribution of some of the dorsal cutaneous nerves of the scapular region, affected the musculo-spiral nerve from its origin downward, most markedly in the forearm and head. Mendel20 describes a case of facial hemiatrophy occurring in a monomaniac, the diagnosis being complicated by the somatic signs of degeneracy—congenital facial and bodily asymmetry. The patient was twenty-eight years old, and the disease could be traced back to the seventh year. In several reported cases the disease has followed or has been associated with epileptic seizures. Buzzard21 has published a case in which the affection came on in a girl aged thirteen in the course of a second attack of chorea. In another it followed typhoid fever. In a case reported by Parry22 left hemiplegia with temporary disturbance of intelligence preceded the disease by about two years. In another, observed by Axman and Hueter, the patient, a man aged thirty-two, had suffered from irregular contractures of the left masticator muscle, which commenced in the seventh year. These spasms were associated with an increased delicacy of sensation in the region of the left trigeminus. Neuralgia is sometimes a complication. In a case reported by Holland,23 the patient for several years suffered from paroxysms of fronto-temporal neuralgia.
20 Neurologisches Centralblatt, June 15, 1883, quoted in Journal of Nervous and Mental Disease, 1883, x. p. 571.
21 Transactions of the Clinical Society of London, vol. v., 1872, p. 146.
22 Eulenburg.
23 American Practitioner, vol. xxxi. No. 182, Feb., 1885, p. 72.
PATHOLOGY.—Up to the present time, so far as I have been able to learn, not a single autopsy in a case of typical progressive unilateral facial atrophy has been made. Conclusions as to pathology can therefore only be drawn from an analysis and study of symptoms and from comparisons with other degenerative affections. Most authorities hold that it is neurotic in origin. [p. 700] Lande, however, regarded it as having its origin in the connective tissue, affecting the nutrition of the other tissues by interfering with the circulation.
Different views have been held by those who have believed in its neurotic origin. Moore regarded it as a form of progressive muscular atrophy attacking the muscles supplied by the portio dura, but what has already been shown with reference to the symptomatology is sufficient to show that this is an erroneous hypothesis. The muscles supplied by the facial nerve may diminish in volume, but they do not undergo a true degeneration.
Brunner attributed the affection to continued irritation of the cervical sympathetic by some continuing lesion. Irritation of such a lesion, according to him, causes vascular spasms, diminishes blood-supply, and thus leads to the gradual development of the atrophy. This view, to say the least, has not been made out.
Virchow holds that the affection is peripheral, and not central. He believes, however, that a primary process being once set up in the nerve-trunks, owing to inflammations of the surrounding tissues it may then extend upward to the spinal and basal ganglia. The disease, according to this view, has some analogy to herpes zoster. The manner in which nerve-districts are unequally attacked is similar to what is observed in the various forms of lepra and in morphœa. The doctrine of a tropho-neurosis is the one that is best upheld by clinical facts. In the first place, various arguments can be adduced to show that the disease is neurotic in origin. It is limited to one side of the face and to special nerve-distributions. Affections of sensibility in the domain of the trigeminal nerve are frequently present. In the case given under Symptomatology, although anæsthesia was absent, the patient complained of peculiar paræsthesia in the form of stinging sensation. Either trophic centres or trophic fibres, which have the same connection and course as the trigeminal, are affected by a degenerative process. Whether nuclei, ganglia, or peripheral fibres are primarily affected has not yet been satisfactorily determined.
The case of Romberg, observed by Virchow twenty years after, was considered by the latter to entirely overthrow the vaso-motor theory, owing to the condition of the blood-vessels. While the surrounding tissues from the skin inward were wasted and shrunken, the veins and arteries of the parts appeared absolutely unchanged, the larger even projecting above the surface of the skin. Under stimulation the vessel dilated as in a normal individual, appearing to take no part in the atrophy.
DIAGNOSIS.—The chief affections from which progressive unilateral facial atrophy are to be diagnosticated are congenital asymmetry of the face and head, facial paralysis, progressive muscular atrophy, and hypertrophy of the opposite side of the face.
Congenital asymmetry of the face is observed in institutions for the idiotic and feeble-minded. Such asymmetry, however, is usually associated with corresponding defects of other parts of the body, as of the head and limbs. In the nervous wards of the Philadelphia Hospital is now, for instance, a patient the entire right half of whose body is very decidedly wasted, the case being one of epileptic idiocy with paralytic and choreic manifestations which point to atrophy of the opposite half [p. 701] of the cerebrum. At the Pennsylvania Training-School for Feeble-minded Children want of development of one-half of the head is often observed, but in these and in other congenital cases the special changes in nutrition, in the skin, in the color and growth of the hair, and in sensation, are absent. In some cases of congenital asymmetry of the head atrophy of the face or limbs, if present, will be upon the opposite side of the body; and this is what might be expected, as arrested development of the cranial vault will probably correspond with arrested development of the cerebrum of the same side and bodily defects of the opposite side.
Eulenburg, Maragliano, and others refer to an acquired want of symmetry of the face sometimes observed in cases of wry neck or scoliosis with deviation of the spinal column. Eulenburg especially speaks of the so-called habitual scoliosis, where a curve in the dorsal region in one direction has a compensatory cervical curve, the side of the face which corresponds to the dorsal curve being often smaller than the other. This asymmetry is supposed to result from compression of the vessels and nerve-roots in the concavity of the cervical curve. Here, again, the absence of special nutritional changes will assist in the diagnosis. A study of the spinal curvature will also be of value. Indeed, only the most careless observation would allow this mistake in diagnosis to be made.
Facial paralysis—Bell's palsy of the usual type—would not be likely, except by a careless observer, to be confounded with the disease under consideration. When the muscles in the facial distribution are involved, it is only in a very slowly progressive deterioration, which may be due to mechanical causes, as compression by the contracting skin. Moore,24 as already stated, was wrong in speaking of the morbid changes as entirely confined to the portio dura of the left side. It is the fat, the connective tissue, and the skin which are first and chiefly affected. In unilateral facial atrophy no true paralysis of the facial muscles is present; consequently, the forehead can be wrinkled, the eye closed, the mouth drawn up or down, or sideways, etc.; in short, all the movements of the face are possible. The opposite of this, it goes without saying, is present in general facial paralysis. The drawing of the face to the side opposite the paralysis in Bell's palsy is not here observed; the mouth is sometimes drawn upward slightly on the atrophied side. In facial paralysis of any severity reactions of degeneration are present. In unilateral facial atrophy, as in progressive muscular atrophy, the muscles respond both to faradism and galvanism. As minor aids in making the diagnosis, the absence of loss of taste in one-half of the tip of the tongue, and of deflection of the tongue and uvula, are in favor of facial atrophy.
24 Dublin Journal of Medical Science, vol. xiv., August and Nov., 1852, p. 245.
It is possible that a case of progressive muscular atrophy might begin in almost any muscle or group of muscles in the body. In progressive muscular atrophy, however, the appearance of the skin is different; it is not mottled; it is not thin, as can be demonstrated by manipulation of it; it can be raised by the fingers; it is soft and flaccid. In progressive muscular atrophy also first one muscle and then another, just as likely as not at some distance from each other, are attacked by the wasting process; in unilateral facial atrophy the affection spreads uniformly and regularly [p. 702] over one-half of the face. According to Duchenne of Boulogne, when progressive muscular atrophy first appears in the face the orbicularis oris is the muscle most likely to be attacked, causing the lips to appear enlarged and pendent, and giving a stupid look to the patient. In unilateral facial atrophy this appearance is not present. Progressive muscular atrophy commonly begins at a later age than unilateral facial atrophy.
Hypertrophy of the opposite side of the face is suggested by Eulenburg as a possible source of mistake; but a little study, however, will suffice to exclude this affection.
The following points are given by Eulenburg with reference to vitiligo and porrigo decalvans: “In vitiligo we find the same white decoloration of the skin, the cicatricial feel, the turning gray and falling out of the hair, but not the loss of volume, which is the special characteristic of this disease. In porrigo decalvans inflammatory symptoms and œdema of the skin come first; the disease first appears in regular circular spots; the hairs fall out without previous loss of color; and finally, the disease is contagious, and fungi can be demonstrated (microsporon Audouini).”
PROGNOSIS.—The prognosis as to recovery is bad, but, as already shown, the disease may long remain stationary.
TREATMENT.—No well-authenticated case of cure under any method of treatment has yet been reported. Electricity, either in the form of galvanism or faradism, has been resorted to in a majority of cases. In most of these temporary benefit has been produced by the employment of these agencies. Baerensprung reports two cases as having been greatly benefited by faradism. In Moore's case it also produced temporary improvement. Carefully administered massage should be tried. With reference to friction or massage, however, it is well, as advised by Eulenburg, to be cautious, as excoriations are easily produced. Measures directed to building up the nervous centres are indicated—such medicinal agents, for instance, as the salts of silver, gold, zinc, and copper, arsenical preparations, strychnia, and iron.
The membranes or envelopes of the brain and cord were formerly reckoned as three in number: the dura mater, lying next to the inner surface of the bones of the cranium and spinal column, forming an internal periosteum; the pia mater, which is in immediate contact with the brain and cord; and the arachnoid, which was described as a distinct membrane loosely attached to the pia mater, but more firmly united to the dura, and constituting a closed sac or serous cavity called the cavity of the arachnoid. This view is now abandoned by most anatomists, who regard the external arachnoid as simply a pavement epithelium covering the internal surface of the dura, and the visceral arachnoid as constituting the external layer of the pia. The term cavity of the arachnoid has, however, been generally retained for the sake of convenience; and it gives rise to no obscurity if we remember that by it we simply mean the space between the dura and the pia.
The diseases of the membranes which I shall consider are—congestion and inflammation of the dura, including hæmatoma; congestion and simple and tubercular inflammation of the pia; and meningeal apoplexy.
The membranes of the brain and those of the cord may be separately diseased, or both may be affected at the same time. Simultaneous inflammation of the cerebral and spinal meninges is apt to occur epidemically, and is supposed to be zymotic in its origin. This is described in another article. (See EPIDEMIC CEREBRO-SPINAL MENINGITIS, Vol. I. p. 795.)
SYNONYM.—Pachymeningitis. Either surface of the dura may be inflamed separately, and in many cases the symptoms are sufficiently definite to render it possible to diagnosticate the situation of the disease in this respect during life, especially when taken in connection with the causes. For this reason it is usual to speak of external and internal pachymeningitis. A peculiar form of the latter is accompanied by the effusion of blood upon the arachnoidal surface, which sometimes forms a tumor called hæmatoma. Congestion is also sometimes included in the diseases of the dura mater, but is rarely alluded to by writers on pathology or clinical medicine.
Except as the first stage of inflammation, congestion of the dura can hardly exist unless in connection with the same condition of the pia or of the brain. Its causes are either local, such as thrombosis of the sinuses, syphilitic or other growths in the membranes; or remote, the principal being obstructions to the general circulation, including valvular disease of the heart, emphysema and other affections of the lungs, renal disease, compression of the superior cava or jugulars by aneurism and other tumors, delayed or suppressed menstruation, etc. The symptoms cannot be distinguished from those of congestion of the pia or of the brain—namely, headache, a sensation of throbbing, pressure, or weight in the head, somnolence, etc. The absence of fever would serve to distinguish the affection from an inflammatory condition of the membranes or brain.
SYNONYM.—External pachymeningitis.
ETIOLOGY.—The most frequent causes of external pachymeningitis are injuries to the cranial bones from violence, caries and necrosis of the same, and concussion from blows on the head. Next in order of frequency, if not even more common, comes the propagation of inflammation from disease of the inner ear and of the mastoid cells. It is only of late years that this important subject has been brought prominently forward and the danger of ear diseases in this respect fully pointed out. The channels of communication, as indicated by Von Tröltsch1 in his valuable article on diseases of the ear, are along the arteries and veins which pass from the skin of the meatus and the mucous periosteal lining of the middle ear to the contiguous bone, while the capillaries of the petrous bone are in direct connection with the dura mater, so that the vessels of the latter are in communication with the soft parts of the external and middle ear. The vessels of the ear and the membranes of the brain are also directly connected through the diploëtic veins of the temporal bone, which discharge into the sinuses of the dura, as well as through the venæ emissariæ, which, arising from the sinuses, pass through the bone and discharge their contents into the external veins of the head. Von Tröltsch also points out that the extension of an inflammatory process may occur along the sheath of the facial nerve, the canal of which (canalis Fallopii) is a branch of the internal auditory canal and is lined by the dura mater. The latter is separated from the mucosa of the tympanum only by a thin, transparent, and often defective plate of bone. Inflammation may also be transmitted from the scalp by means of the vessels which pass through the bones of the skull. In this way erysipelas and other diseases of the integument sometimes give rise to external pachymeningitis.
1 “Die Krankheiten des Gehörorganes,” von Anton von Tröltsch, in Gerhardt's Handb. der Kinderkrankheiten, Tübingen, 1879, 5 B., ii. Abt., p. 150; also English translation of the same, by J. O. Green, M.D., New York, 1882, p. 107.
SYMPTOMS.—There are no known symptoms which are characteristic of inflammation of the external surface of the dura. In cases of death [p. 705] from other diseases an autopsy may show traces of previous inflammation, such as thickening of the membrane and its firm adhesion to the cranial bones, which were not manifested during life by other symptoms than those which accompany meningeal disease in general; and in some instances none at all were known to have occurred. At a variable time after the receipt of an injury to the head the patient may complain of headache, followed by a chill, with high fever, vomiting, vertigo, delirium, unconsciousness, convulsions, etc., arising from compression by the products of inflammation. The same phenomena may follow the transmission of inflammation to the dura from caries or other disease of the bones, or from otitis medea purulenta. These symptoms usually continue without interruption, though there is sometimes more or less complete remission of the pain, and the patient may recover his consciousness for a time, thus giving rise to fallacious hopes. In a large proportion of cases the disease extends to the inner surface of the membrane and to the pia, without any noticeable change in his condition other than coma. In chronic external pachymeningitis the principal symptom is pain in the head, which may persist for weeks or months without other manifestations except drowsiness. Sometimes, on the contrary, there is obstinate vigilance. Mental symptoms, such as loss of memory, hallucinations, dementia, or mania, are sometimes noticed, ending, as in the acute form, in coma.
PATHOLOGICAL ANATOMY.—In chronic cases often nothing is found but thickening of the membrane, which generally becomes firmly united to the inner surface of the cranium. Indeed, these appearances are not unfrequently observed, to a limited extent, when there has been no history of disease to account for them. In other chronic cases the connective tissue of the membrane is found to be in part ossified, and the osteophytes of the cranium sometimes found in pregnant women and in patients with rheumatic cachexia are supposed to be due to a chronic inflammatory process of the dura. The first changes observed in acute external pachymeningitis are increased vascularization, shown by red lines corresponding to the blood-vessels, with punctiform extravasations, swelling, and softening of the tissue. Later, there is thickening of the membrane from new formation of connective tissue, and exudation of lymph, and sometimes of pus, which latter may accumulate between the dura and the cranial bones, or in traumatic cases may escape through openings in the skull. The dura and the pia become united in most cases of acute inflammation. The lateral sinuses frequently contain thrombi, which, when ante-mortem, are firm in structure, reddish-brown in color, often closely adherent to the walls of the vessel, and may extend to other veins, sometimes reaching as far as the jugulars. When purulent inflammation of a sinus occurs, its walls are thickened, softened, and discolored, and the inner surface is roughened. The thrombus becomes more or less purulent or sanious, disintegrates, and the infecting particles are carried into the circulation, giving rise to embolism and disseminated abscesses of the lungs, kidneys, liver, or spleen. Other lesions, such as injury or caries of the cranial bones and purulent inflammation of the middle ear and of the mastoid cells, are frequently found in conjunction with pachymeningitis, to which they have given rise. When the disease of the dura extends to the pia, the adjacent portion of the brain is often found implicated in the [p. 706] inflammation. In traumatic cases the dura may be detached from the bone and lacerated to a greater or less extent.
DIAGNOSIS.—The existence of external pachymeningitis may be suspected from cerebral symptoms following traumatic injury of the skull, erysipelas, or suppurative otitis medea, but apart from the etiology it would not be possible to distinguish it from internal inflammation of the membrane, or even from leptomeningitis.
PROGNOSIS.—In cases of suspected external pachymeningitis the prognosis will depend upon the evidence of effusion of pus or blood between the dura and the skull, and the possibility of their removal. A large proportion of cases are fatal, especially those arising from caries of the cranial bones and from the propagation of disease from the middle ear, the mastoid process, or the external surface of the skull, the inflammation extending through the membrane to the arachnoid surface of the dura, and also to the pia mater. This would be shown by a high temperature, rapid pulse, pain, and delirium, followed by coma and perhaps convulsions. The frequency with which external pachymeningitis occurs in connection with diseases of the ear should put the physician on his guard in cases of otorrhœa or pain in the ear, that he may warn the patient or his friends of the possibility of danger, and may employ an appropriate treatment.
TREATMENT.—In all cases of injury to the skull or of severe concussion the possibility of subsequent external meningitis should be borne in mind. The patient should be confined to the bed and be carefully secluded from excitement. Cold applications should be made to the head, the diet should be simple and somewhat restricted, and the bowels kept free without active purging. If there be evidence or suspicion of the presence of pus or of blood between the dura and the skull, means should be taken to evacuate the effusion. In case of inflammatory symptoms leeches should be applied behind the ears, and a stimulating liniment or croton oil rubbed on the scalp. There is no specific treatment. Pain and sleeplessness must be relieved by opiates and sedatives, and the strength must be sustained by nourishing diet and stimulants.
Internal pachymeningitis is of two kinds: 1st, simple inflammation, which may be accompanied by purulent exudation and by a corresponding affection of the pia mater: 2d, hemorrhagic inflammation or hæmatoma of the dura mater. Simple inflammation of the internal or lower surface of the dura, without the coexistence of external pachymeningitis is rarely found in the adult. The morbid appearances differ but little from that of the external form, and the causes and the diagnosis are also similar. In children, however, it is not uncommon, according to Steffen.2 The pus may discharge itself spontaneously through the fontanels or the sutures, or caries of the cranial bones may open a passage for its exit. It has also been evacuated artificially when the symptoms have indicated its presence. In other cases more or less extensive firm adhesions [p. 707] between the dura and pia mater have shown the previous existence of inflammation, but it would be difficult to say in which membrane it began. In some instances no symptoms are observed during life; in others the coexistence of inflammation of the pia, effusion into the ventricles, etc. prevent an exact diagnosis.
2 “Die Krankheiten des Gehirns in Kindesalter,” von Dr. A. Steffen, in Gerhardt's Handb., 5 B., i. Abt., 2te Hälfte, p. 380.
The TREATMENT does not differ from that of inflammation of the external layer of the pia.
SYNONYM.—Hemorrhagic pachymeningitis.
DEFINITION.—A chronic inflammation of the dura mater, resulting in the formation upon its inner surface of successive layers of false membrane, into and between which there is usually an effusion of blood, the whole sometimes forming a large solid mass between the dura and the cavity of the arachnoid.
ETIOLOGY.—Hemorrhagic pachymeningitis never occurs in healthy persons except from traumatic causes. It is most frequently observed in advanced life, and especially in the male sex. In a large number of cases the blood is in an unhealthy condition, and hence the disease is seen in alcoholism, in scurvy, in acute articular rheumatism, and in the acute febrile affections, as typhoid fever, pleuro-pneumonia, and pernicious anæmia, of which last, according to Huguenin,3 it complicates one-third of the cases. It is frequent among the chronic insane. It is occasionally met with in young children, but with them its causes are mostly unknown; according to Steffen,4 they may consist in alterations of the blood resulting from insufficient nourishment or from the infectious diseases, and from abnormal blood-pressure, as in whooping cough, asthma, etc., as well as from blows on the head.
3 G. Huguenin, “Acute and Chronic Inflammations of the Brain,” in Ziemssen's Encylop., Am. translation, New York, 1877, vol. xii. p. 401 et seq.
4 Op. cit., p. 386.
SYMPTOMS.—Many cases of hemorrhagic pachymeningitis complicating other cerebral diseases can be distinguished by no special symptom from the original malady. Thus, in cases of chronic insanity its existence may not be suspected during the lifetime of the patient. Steffen quotes5 the case, reported by Moses, of a child seven months old who died of catarrhal pneumonia, and who exhibited no symptom which could suggest any disease of the brain or its membranes. The autopsy revealed a pachymeningitic cyst extending over the anterior half of the right hemisphere. When symptoms are present they vary in different cases according to the acuteness of the inflammatory process, the amount and situation of the effusion, and the participation of the pia mater and brain in the disease. In the beginning they are usually indefinite, headache being the most common and often the only complaint. This may continue for weeks without any other indication of disease, but it is frequently accompanied by tinnitus aurium, vertigo, muscular weakness, and contraction of the pupils. Wakefulness and restlessness at night and slight twitching of the facial muscles or of the limbs sometimes occur. There may be no change in the condition of the patient for a [p. 708] considerable length of time (weeks or months), or he may improve to some extent, owing to the absorption of the serous portion of the effusion or to the tolerance of the foreign body acquired by the brain. Sooner or later a fresh hemorrhage is followed by a recurrence, and usually an aggravation, of all the symptoms. Sometimes the patient becomes comatose, and dies speedily with apoplectic symptoms, but this is not common at an early period. The extravasation of blood generally takes place in small quantities at a time, without giving rise to unconsciousness or paralysis. After a period of uncertain duration, when the tumor has attained considerable dimensions a condition of somnolence may take place, the patient sometimes sleeping twenty-four hours or longer at a time. Distinct paralysis rarely occurs, though hemiplegia is sometimes seen, and the paralysis has been observed on the same side with the lesion. When symptoms of compression appear the pupils become dilated. Toward the end of life the patient is usually in a state of profound coma, the pulse is slow and irregular, and the sphincters are relaxed.
5 Op. cit., p. 394.
The distinctive features of internal pachymeningitis, therefore, so far as they are at present known, are those which would depend upon a primary cerebral irritation, followed by those of compression of the brain—persistent, often severe, headache, with contracted pupils, and occasionally motor and sensory disturbances; afterward, coma, dilated pupils, and involuntary discharges from the bowels and bladder.
The DURATION of the disease is exceedingly variable, extending from a few days to more than a year. According to a table made from carefully observed cases by Huguenin, 74 per cent. of patients die within thirty days; 18 per cent. live from one to six months; 4 per cent. live from six months to one year; and 4 per cent. live over one year.
PATHOLOGY.—A difference of opinion has existed among pathologists concerning the true nature of hemorrhagic effusions of the inner surface of the dura mater, especially as to whether the membrane in which they are enclosed is formed by a deposit of fibrin from the effused blood itself, or whether the disease consists essentially in an inflammation of the dura, followed by a pseudo-membranous deposit into which blood is afterward extravasated. The latter explanation, offered by Virchow, has been generally accepted, but Huguenin, whose opportunities for observing the disease were unusually good, believes that the first stage of hæmatoma is not the formation of connective tissue, but simply an extravasation of blood.
The disease begins with hyperæmia of the dura mater in the area of distribution of the middle meningeal artery, followed by the formation upon its inner surface of an extremely delicate membrane in small patches of a yellowish color and studded with innumerable bloody points. If the membrane be carefully raised, it is found to be connected with the dura by very delicate blood-vessels, and to contain an immense number of very wide and thin-walled vessels, much larger than ordinary capillaries.6 At a later stage we find the membranes to be made up of several distinct layers, of which the innermost exhibits the character of the primary deposit, being thin and abundantly supplied with blood-vessels, while those of older formation have become successively thicker and are [p. 709] composed of tough, lustrous fibres of connective tissue almost as dense as that of the dura mater itself. The delicate structure of the false membranes and of the vessels which they contain leads almost inevitably to the effusion of blood, which increases in quantity with the thickness of the whole growth, so that in an advanced stage it is not uncommon to find large pools of blood, partly clotted and partly fluid, constituting what is called hæmatoma of the dura mater. The small bloody points are within the substance of the false membrane; the extravasations are interstitial, the largest being always found between the youngest membrane and the older layers. In some cases serous transudations also occur between the false membranes. In still rarer instances no blood or serum is found between or beneath the layers. Occasionally small quantities of blood escape by leakage through the delicate membrane into the cavity of the arachnoid.
6 See Rindfleisch's Manual of Pathological Histology, New Sydenham Soc.'s translation, 1873, vol. ii. p. 302.
The usual situation of internal pachymeningitis is the vault of the cranium, near the median line, the upper or external layer of the tumor being in relation with the dura mater, to which it is adherent, and the lower or internal with the arachnoid and pia mater. If the effusion be extensive, it spreads downward over the frontal and occipital lobes of the brain, and laterally toward the fissure of Sylvius. In the majority of cases the disease occupies both sides of the median line symmetrically, but it may be limited to one side only. According to Huguenin, 56 per cent. of the cases embrace the surfaces of both hemispheres; 44 per cent., that of one only. Hæmatoma very rarely occupies the base of the cranium. The thickness and consistency of the deposit vary in different cases, depending upon the number of successive exudations, and hence are most marked in cases of the longest duration.
Hemorrhagic pachymeningitis is occasionally met with in young children, but much more rarely than in adults. The disease is usually more acute than in older persons, but the anatomical appearances are essentially the same.7
7 For an able description of the lesions of hemorrhagic pachymeningitis in children see the third edition of Rilliet and Barthez's Maladies des Enfants, by Barthez and Sanné, Paris, 1884, vol. i. p. 152.
PROGNOSIS.—The great majority of cases end fatally. A few instances of recovery are reported in which the diagnosis seems justified by the symptoms. Moreover, it is not very rare to find, on post-mortem examination of those who have died of other diseases, evidence of the former existence of hemorrhagic pachymeningitis. According to Steffen, while the prognosis of simple pachymeningitis in children is frequently good, owing to the favorable conditions for the exit of pus through the open fontanels and sutures, in hemorrhagic pachymeningitis recovery is rare.
DIAGNOSIS.—In a disease whose symptoms are so vague the diagnosis must of necessity be difficult and often impossible. The chief elements for the formation of the diagnosis are the slow and interrupted progress of the affection, persistent headache, tendency to prolonged slumber, and final coma; the absence of paralysis of the cranial nerves, of vomiting, and of general convulsions; the age of the patient, the coexistence of alcoholism, chronic insanity, or acute rheumatism, and traumatism. The diseases for which hæmatoma would be most likely mistaken are acute inflammation of the meninges, apoplexy from cerebral hemorrhage, tumor in the substance of the brain, and necrobiosis from thrombus or embolus. [p. 710] The absence of symptoms characteristic of these affections might lead to a probable diagnosis by exclusion, but in many cases the existence of the disease cannot be determined with certainty. In children it is most likely to be confounded with tubercular meningitis, from which it may be distinguished by the fact that it is most common under the age of two years, the other being rare before that period, and that the characteristic symptoms of tubercular meningitis (prodromic period, vomiting, irregularity of pulse, etc.) are wanting. But the tubercular disease in young infants may closely resemble hæmatoma, a profound coma replacing all other symptoms. Here the existence of tuberculous disease in the parents or other near relatives would point strongly to tubercular meningitis, while the absence of such antecedents would suggest hæmatoma.
TREATMENT.—If the disease be a complication of alcoholism, anæmia, scurvy, rheumatism, etc., the treatment appropriate to those affections should be employed, along with remedies addressed to the local disease. For the early symptoms of irritation, perfect rest in bed, cold to the head, bromide of potassium internally, sinapisms to the back of the neck, together with simple and nutritious diet, are the most efficient means. The bowels must be regulated, but purging is not necessary. The abstraction of blood from the head by leeches to the temples or behind the ears, or by cupping, is recommended by most authorities, especially if there be much heat of the head. Mercury may be tried, care being taken not to salivate the patient. It is obvious that this treatment, in order to be of any avail, must be instituted at the earliest stage of the disease. After the probable formation of the hæmatoma an effort should be made to promote its absorption, which sometimes actually takes place, as is proved by the autopsies of patients who, having previously suffered from this affection, have died from other causes. The iodide of potassium or the iodide of sodium should be employed perseveringly for this purpose, in the dose of from ten to thirty grains three times daily. The bromide should also be continued if necessary. The acne which sometimes accompanies the continued use of these remedies may be prevented or cured by the use of three to five drops of the liquor potassæ arsenitis, given once or twice daily after meals. Counter-irritation to the scalp by means of stimulating liniments or croton oil, and small blisters to the temples, are likely to do good. In alcoholic subjects the amount of wine or spirit taken should be regulated by allowing enough to support the strength, without too suddenly withdrawing the accustomed stimulant. In the stage of coma the treatment must be purely expectant. The state of the bladder must be regularly examined, and the catheter employed when necessary. Liquid nourishment should be carefully given as long as the patient is able to swallow.
SYNONYM.—Meningeal apoplexy of the brain. Hemorrhage of or upon the membranes of the brain is closely connected with intracerebral hemorrhage. Both arise from similar causes, and the former may result directly from the latter. It is for convenience of arrangement that the two subjects are treated separately in this work.
[p. 711]ETIOLOGY.—The causes of meningeal apoplexy are predisposing and immediate. The most important predisposing cause consists in disease of the cerebral vessels, especially the arteries, which favors the formation of so-called miliary aneurisms, as demonstrated by Charcot and Bouchard in the case of cerebral apoplexy. Disease of the vessels in its turn arises from various conditions, among which alcoholism in adults holds a prominent place from its tendency to favor a fatty degeneration of the vascular walls. In subjects of purpura or hæmophilia (the so-called bleeders), in whom, from an inherent weakness of the capillary vessels or a deficiency of the fibrin of the blood, or both combined, there is a tendency to extravasation of the blood in various parts, hemorrhage into the arachnoid cavity may occur.8 A new-born child under my observation had bleeding at the navel and ecchymoses in various parts of the body. Suddenly it became comatose, and it died with signs of cerebral compression. There was no autopsy, but it seems probable that hemorrhage into the cavity of the arachnoid had taken place. A sister of the patient had also had spontaneous hemorrhage from the navel and from other parts shortly after birth, but recovered. Chronic general arthritis and gout also probably predispose to the affection, as well as old age, which is accompanied by atrophy of all the tissues. The disease is most frequently met with in the two extremes of life; according to Durand-Fardel,9 in adults the largest number of cases occurs between the ages of seventy and eighty years.
8 A case of this kind is cited in the article “Pathologie des Méninges” in Nouv. Dict. de Méd. et de Chirurg. pratiques, Paris, 1876, vol. xxii. p. 101.
9 Traité clinique et pratique des Maladies des Vieillards, par M. Durand-Fardel, Paris, 1854, p. 283.
The exciting causes comprise injuries to the head, both with and without fracture; strong muscular effort, as in lifting, straining at stool or in labor; powerful action of the heart in cases of hypertrophy. An interesting case is reported10 by S. G. Webber of Boston, in which the effusion was evidently caused by vomiting; a clot of blood covered the greater part of the posterior two-thirds of the right hemisphere. Sometimes meningeal hemorrhage may arise from the bursting of an intracerebral apoplexy into the arachnoid cavity, as in a remarkable case occurring in the practice of Morris Longstreth of Philadelphia, of bilateral effusion.11 Outside the dura, corresponding with the left middle cerebral lobe, was a considerable amount of blood connected with a fracture of the skull, and on the right side a large quantity of blood in the cavity of the arachnoid, originating in the middle lobe, which was torn up. The patient had fallen in the street; he was stupid, there was no paralysis, active delirium came on, followed by coma and death in twenty-four hours. Here was cerebral apoplexy bursting into the cavity of the arachnoid on the right side, and causing the fall, which was the occasion of the fracture and hemorrhage on the left side.
10 Boston Med. and Surg. Journal, Jan. 17, 1884.
11 Ibid., Dec. 28, 1882.
In young children, especially in the new-born, meningeal hemorrhage may follow difficult and instrumental labor, either from injury to the skull or from delay in the establishment of respiration, as in breech presentation, though it sometimes occurs in cases in which the labor has been normal. In a case of breech presentation under my care in 1873 [p. 712] the child, a female weighing nine pounds, did not cry or breathe for some minutes after birth, although delivery had not been much delayed. Soon afterward it was noticed that it did not move the right arm, although it moved the hand and the fingers. In the course of twenty-four hours, during which time it cried much more than usual, it became comatose, and remained so until its death, three days after birth. The whole surface was livid, and the child had two or three short convulsions. At the autopsy a clot about the size of a grape was found in the pia mater on the upper surface of the cerebellum, in the immediate vicinity of the pons Varolii. The brain was so soft that the amount of injury received by the cerebellum could not be exactly ascertained, but it was probable that the clot extended into the fourth ventricle.
Thrombus of the sinuses of the dura mater, and less frequently of the cerebral arteries, is the origin, in a considerable number of cases, of meningeal hemorrhage in children, in consequence of pressure upon the delicate vessels of the membranes caused by the obstructed circulation. Bouchut12 reports an observation of hemorrhage produced in this way.
12 E. Bouchut, Clinique de l'Hôpital des Enfants maladies, Paris, 1884, p. 263. See, also, Steffen, op. cit., p. 352.
SYMPTOMS.—In some cases the attack is preceded by indications of congestion, such as headache, vertigo, staggering, confusion of ideas, noises in the ears, feeling of weight in the head, delirium, stupor. At the time of the attack the patient frequently complains of severe pain in the head, just as in cerebral hemorrhage, and then falls to the ground with complete loss of consciousness. Sometimes the symptoms come on gradually. Hemiplegia occurs in a notable proportion of cases. Convulsions may occur at any time after the attack. In Webber's case, already referred to, the first symptom was sharp pain in the head and neck; this was followed by very severe headache and pain on motion of the head. Intelligence gradually diminished; on the sixth day there was almost no consciousness, and the patient died in about eight days. She had occasional spasms, in which both eyes were turned toward the left in extreme conjugate deviation, and the left side of the face was distorted. The spasms were followed by suspension of respiration for nearly a minute, cyanosis, and paralysis of the left hand and leg. Both the nature of the lesion and its seat were correctly diagnosticated during the patient's lifetime.
As a rule, the condition of unconsciousness continues up to the time of death, but in some cases there are intermissions during which the patient responds to questions more or less promptly. Death takes place at a period varying between a few hours and several days. Durand-Fardel13 reports a case in which the patient lived a month from the first attack, with preservation of the intellect and of motion. An inmate of the Home for Aged Women in Boston, eighty-eight years old, previously in good health, complained of severe pain in the head one morning before rising. She took her breakfast in bed, and immediately afterward vomited copiously. From that moment she became insensible, and remained so until her death, seven days and three hours afterward. During this time there was no stertor. No decided paralysis could be discovered, but there was some rigidity of the left arm. At the autopsy an effusion of [p. 713] blood was found in the arachnoid cavity extending from below upward on each side to a level with the top of the ear. There was a large amount of blood at the base of the brain, and both lateral ventricles were distended with bloody serum. The vessels were generally in an atheromatous condition. There was no laceration of the brain. The source of the hemorrhage could not be ascertained. In such a case the condition of the patient in respect to power of movement often cannot be ascertained with certainty, in consequence of the abolition of consciousness. Complete muscular resolution is most common when the effusion is bilateral, but when the hemorrhage is limited to one side more or less paralysis of the opposite limbs may exist. Should the blood make its way into the spinal canal, it might give rise to special symptoms, but this is not probable in view of the large amount of the cerebral effusion under the circumstances, which would produce complete insensibility or speedily cause death by pressure on the medulla.
13 Op. cit., p. 202.
The temperature of the body immediately after a copious cerebral or meningeal hemorrhage falls below the normal point, and remains so for several hours, after which it rises, its degree varying according to circumstances. In fatal cases the elevation is extreme, and remains so until death. If the patient recover, it gradually returns to the normal standard.
Vomiting is a frequent symptom at the beginning of the attack, just as in intracerebral hemorrhage, owing probably to compression of the pneumogastric by the effusion at the base of the brain. In Webber's case the vomiting was evidently the cause of the hemorrhage, and not its consequence, since it had been a frequent symptom for several days before the attack, and was probably due to the presence of a calculus in the pelvis of the right kidney, which was found at the autopsy, and there was no blood at the base of the brain.
PATHOLOGICAL ANATOMY.—The chief points of interest in the morbid anatomy relate to the seat and source of the effusion, the amount and condition of the blood, the state of the vessels and that of the brain, including the ventricles. In respect to the seat, the hemorrhage may occupy the space between the cranial bones and the dura mater; it may be found on the lower surface of the latter, in the arachnoid cavity, or in the meshes of the pia mater, the so-called subarachnoid space. Blood found upon the outer surface of the dura, between that membrane and the bones, is almost always the result of traumatic causes, such as blows or other injuries, with or without fracture, or of caries of the skull. If below the dura, but between that and the so-called parietal layer of the arachnoid, the lesion comes under the title of pachymeningitis interna, already described as an inflammatory disease of the dura with hemorrhagic effusion. The arachnoid cavity and meshes of the pia are by far the most common situations in which the blood is found in meningeal hemorrhage. The origin of the effusion is either the rupture of a capillary aneurism of one of the arterioles of the membrane or of one of the vessels themselves in consequence of atheromatous or other degenerations of its walls. On account of the minute size of the vessels it is seldom possible to discover the exact point at which the rupture took place. In rare instances the source of the hemorrhage is within the brain, the blood being forced through the cerebral tissue, either into the meshes of the pia [p. 714] or upon the surface of that membrane. The amount of hemorrhage varies according to conditions which are mostly unknown, but is probably dependent upon the size of the ruptured vessel and the conditions under which the accident occurs, such as muscular effort, cardiac action, etc. In some cases it is so small as to give rise to no definite symptoms, as is evident from post-mortem examinations of those who have died from other causes. In these cases there may be either a single effusion or several. The amount is largest when the arachnoid cavity is the seat of the extravasation. The blood, which may be either liquid or more or less coagulated, according to the time which has elapsed since the hemorrhage, is usually found upon the convexity of the hemispheres, most frequently on one side only, and oftenest on the left. But if the rupture have taken place at the base, it often ascends on each side, as in a case mentioned above. Where a large vessel has given way, its contents may cover a great part of the surface of the brain. The coagulum is found in a thin layer, which at the end of a few days is covered with a transparent envelope, evidently composed of a deposit or separation of fibrin. Should the patient survive long enough, this membrane may become organized, receiving vessels from the adjacent pia, and in turn become the seat of new hemorrhages, exactly as in the hæmatoma of internal pachymeningitis. In cases in which absorption of most of the fluid part of the effusion takes place, the membrane remains more or less dense and vascular, and usually contains a small quantity of recently-effused blood within its meshes. Small cysts, containing transparent or reddish-brown serum, are also occasionally observed enclosed between the layers of the membrane. In very young children, whose fontanels are not yet ossified, these cysts sometimes attain to a large size, containing several pints of fluid, which is more or less limpid from absorption of the coloring matter of the blood, constituting the so-called dropsy of the arachnoid.14 The convolutions of the brain are more or less flattened according to the amount of the effusion, and the cortical substance is correspondingly anæmic from pressure. The blood may make its way, if extravasated in large quantities, into the ventricles, over the medulla, into the spinal arachnoid cavity, or even into the central canal of the spinal cord. The arteries of the brain, especially at the base, are frequently in a state of atheromatous degeneration, and thrombi often occupy the sinuses of the dura mater.
14 Charles West, M.D., Lectures on the Diseases of Childhood and Infancy, 6th ed., London, 1874, p. 62. These large cysts are much more frequently (perhaps solely) found in cases of hemorrhagic pachymeningitis. (See Barthez and Sanné, op. cit., vol. i. p. 157.)
DIAGNOSIS.—The distinction between meningeal hemorrhage and cerebral apoplexy is always difficult, and in the majority of cases impossible. Sudden pain in the head, vomiting, and lowering of the bodily temperature (the thermometer should be placed in the rectum), followed by loss of consciousness, are strongly suggestive of hemorrhage within the cranium, either cerebral or meningeal. If these symptoms are followed by coma and resolution without obvious paralysis, the diagnosis would be almost impossible between intra- and extra-cerebral extravasation. If the loss of consciousness be not complete, so that the presence or absence of paralysis can be ascertained, we can sometimes distinguish the situation of the hemorrhage. Right-sided hemiplegia, with paralysis of the face or tongue, or with aphasia, is most probably owing to hemorrhage or [p. 715] embolism somewhere in the left motor tract, and hence within the brain. If the absence of paralysis can be certainly ascertained, the probabilities are in favor of meningeal apoplexy. Convulsions affecting the face or limbs of one side would point to irritation of the cortical centres of those parts, and so far to extravasation on the surface of the brain (on the opposite side), as in Webber's case. Where the amount of hemorrhage is small it furnishes no diagnostic indications. In the case of new-born children the presumption is in favor of meningeal effusion.
PROGNOSIS.—If the effusion be considerable in amount, as indicated by prolonged coma with resolution, the issue is almost inevitably fatal, though life is occasionally prolonged for a surprising length of time. Slight hemorrhages are doubtless recovered from, but there are no means for their certain diagnosis.
TREATMENT.—The treatment, which is essentially the same as that for cerebral congestion, has for its object the arrest of the hemorrhage, and, if that can be effected, the absorption of the effused blood. In view of the former, the patient's head should be elevated and kept cool by the application of ice. Unless the bowels have previously been freely moved, saline laxatives, followed by enemata if necessary, must be given. The state of the bladder must be carefully attended to. Liquid nourishment alone, in moderate quantities at regular intervals, is permissible, with stimulants if there be signs of exhaustion. For the absorption of the effusion mild counter-irritation to the scalp and the administration of the iodide of potassium may be employed.
The pia mater consists of two layers, separated by a loose connective tissue. The outer layer, being that which was formerly called the visceral layer of the arachnoid, is stretched smoothly over the convolutions of the brain without dipping into the sulci; the inner layer is closely connected with the surface of the brain, whose inequalities it follows. The two layers are more firmly united together over the convolutions than between them; in the latter situation the connection is loose, and the space which separates the surfaces is called the meshes of the pia. The membrane extends into the ventricles, investing the ependyma and the choroid plexuses, and over the medulla oblongata and spinal cord. In the normal condition it is loosely attached to the brain, from which it can be stripped off without loss of substance. The meshes of the pia, together with the ventricles, constitute a series of cavities connected with each other, containing a variable amount of cerebro-spinal fluid, and they communicate with the lymph-spaces surrounding the blood-vessels. Pressure within the cranial cavity, from congestion of the vessels or from the products of inflammation, is thus relieved in a measure by displacement of the cerebro-spinal fluid, which is driven out through the perivascular lymph-spaces.
Congestion or hyperæmia of the pia mater probably never occurs independently of that of the external surface of the brain, on account of the intimate vascular connection of the two. In the adult it can only exist to a limited extent, on account of the unyielding nature of the cranial [p. 716] walls and of the limited compensatory action of the cerebro-spinal fluid. In young children the incomplete ossification of the skull and the delicate structure of the vessels are more favorable to congestion.
ETIOLOGY.—The causes of hyperæmia of the pia mater are in the main the same as those of congestion of the dura.
SYMPTOMS.—Since congestion of the pia always coexists with that of the corresponding part of the external portion of the brain, it is impossible to separate the symptoms belonging to each. They are therefore usually included under the head of Cerebral Congestion, to which article the reader is referred.
PATHOLOGICAL ANATOMY.—Arterial hyperæmia of the pia is seldom discovered after death, the elasticity of the vessels causing transudation of the fluid part of the blood through their walls. Venous congestion of the pia is more frequently noticed, usually in connection with that of the dura, the sinuses with their accompanying veins being distended with blood, and in cases of long standing often containing thrombi. Simple hyperæmia of the pia being rarely or never fatal of itself, these appearances are usually accompanied by those of inflammation of the membrane or of the cortical layer of the brain (effusion of lymph or pus), or by hemorrhage.
TREATMENT.—In a case of suspected congestion of the pia the treatment would be the same as that of cerebral congestion.
SYNONYMS.—Meningitis, Leptomeningitis, Acute non-tubercular hydrocephalus.
Meningitis (by which is generally understood inflammation of the pia) appears under an acute, a chronic, and an epidemic form. The latter, being a zymotic disease, is described in a separate article, to which the reader is referred.
ETIOLOGY.—Meningitis occurs both as a primitive disease and as secondary to other affections. The former is rare, the latter is more frequent. The causes of idiopathic meningitis are for the most part unknown. Exposure to the sun's rays and excessive indulgence in alcoholic liquors are thought to excite it in some instances. It has been known to follow blows and falls on the head which have produced no injury to the skull. It is rather more commonly observed in early manhood than at other periods of life. Secondary meningitis may follow injury or disease of the cranial bones or of the dura, and of the brain. A frequent cause is extension of disease of the ear to the membranes and substance of the brain. The reader is referred to the article on MEDICAL OTOLOGY for information concerning the symptoms of that formidable complication. Certain diseases are known to be occasionally complicated with meningitis—acute articular rheumatism; erysipelas of the scalp and of the face; Bright's disease, especially the chronic interstitial form; peritonitis; ulcerative endocarditis; pyæmia; the eruptive fevers; the puerperal state; and syphilis. Meningitis following or complicating acute rheumatism is generally supposed to be not uncommon, but the number of cases in which the existence of inflammation of the meninges has been [p. 717] proved by autopsy is small. Fuller,15 along with three cases in which dissection showed suppurative inflammation of the pia, cites several others in which no cerebral disease was found after death, although the symptoms gave every indication of it. True meningitis is rare in chronic Bright's disease, the symptoms resembling it being caused, in the majority of cases, by uræmia. Meningitis complicating pneumonia is also rare, although cerebral symptoms are common enough in that disease, especially in young children with inflammation of the upper lobes. C. Neuwerk16 reports seventeen cases of purulent meningitis complicating acute pneumonia. It was more frequent in men, especially in alcoholic subjects, than in women. The meningitis was generally total. The lungs were in a state of gray or yellow hepatization.
15 H. W. Fuller, M.D., On Rheumatism, Rheumatic Gout, and Sciatica, 3d ed., Philada., 1864, p. 271. See also E. Leudet, Clinique médicale de l'Hôtel Dieu de Rouen, Paris, 1874, p. 133.
16 Deutsches Archiv für klin. Med., xxix., 1881, p. 1; and Schmidt's Jahrbücher, Band cxcviii., 1883, Nov. 5.
SYMPTOMS.—The symptoms of acute leptomeningitis vary much in the course of the disease. This is readily explained by the complex character of the functions of the parts involved in the inflammation. It may be assumed that the cortical layer of the brain is implicated in every case unless of the most transient and limited kind; the substance of the brain, cerebellum, and medulla are subjected to pressure from the afflux of blood, from the effused lymph and pus, and from the accumulation of serum in the ventricles; the cranial nerves are exposed to pressure from the deposit of lymph, which may give rise to irritation or to suspension of function or both; parts at a distance from the seat of lesion may be functionally disordered by reflex action through communicating filaments. Finally, the general system suffers from the effects of the high fever upon the blood and the nutrition.
It is customary to speak of a stage of excitement followed by one of depression as characteristic of the course of the disease; but although active symptoms generally prevail in the early period, to be succeeded later by coma and paralysis, this disposition is by no means uniform. Sometimes sopor and paralysis constitute almost the only symptoms throughout the disease—this is especially noticed in infants—or active delirium and convulsions may persist until the fatal termination. More frequently the two conditions alternate several times with each other. A prodromic period of short duration, a few hours or a day or two, is sometimes observed in primitive meningitis, the patients complaining of headache, vertigo, vomiting, restlessness, or lassitude. Infants are irritable or drowsy, with heat of the head, quick pulse, and occasional vomiting. In secondary meningitis this period is usually masked by the symptoms of the primitive disease. In the majority of cases the beginning of acute meningitis is abrupt. Rigor is sometimes the first symptom observed, and in children is usually represented by a convulsion. More commonly, however, the disease is ushered in by severe headache, which is often referred to the forehead. The head is hot, the face is flushed, the eyes are brilliant, the pupils are contracted, the pulse is quick and hard, the temperature high (104° F. or upward). The patient is wakeful, restless, and irritable, sensitive to light and to sound. The skin is hyperæsthetic, [p. 718] especially that of the legs. There may be wandering or even active delirium. Vomiting is not unfrequent. There is thirst, but no desire for food. The urine is scanty and high-colored, the bowels constipated. These symptoms gradually increase in intensity, especially the pain in the head and the delirium, and in many cases they are followed by convulsions, at first in the form of twitchings of the facial muscles or of the limbs, grinding the teeth, etc., which give place to tonic contractions of the limbs or of the trunk, often confined at first to one or both members of the same side, but afterward becoming general; the flexors of the forearms and of the legs are most usually affected. The upper dorsal muscles may become contracted, so that the head is drawn backward, and more rarely trismus occurs.
A diminution in the rapidity of the pulse, which may fall to the normal rate, or even below that, notwithstanding the persistence of the high temperature, indicates the beginning of the stage of depression. This change is sometimes sudden, though more often gradual in its approach. The activity of the delirium subsides, giving place to a somnolence which may seem to the inexperienced observer a favorable indication, but which soon deepens into coma. The face becomes pale, the features are sunken. Only an occasional grimace or a movement of the hand to the head shows that the patient is to some extent conscious of suffering. This condition may alternate with the previous one from time to time, the comatose state being interrupted by noisy delirium and tonic or clonic convulsions, or even a partial return of consciousness, giving rise to fallacious hopes on the part of the friends, and sometimes deceiving the physician himself into a belief that a favorable issue is at hand. Before long, however, the symptoms of brain-compression become permanent. The rigidity of the limbs gives place to complete resolution. The patient lies absolutely unconscious, with dilated pupils. The pulse becomes again rapid in consequence of compression of the medulla, and thread-like and irregular; for the same reason the respirations increase to 40, 50, or 60 in the minute. The sphincters are relaxed, and the patient dies without any recurrence of the active symptoms. In rare cases recovery takes place, although almost never after the symptoms of compression have continued without interruption for any considerable length of time. Moreover, it is seldom that recovery takes place in the adult without leaving some traces of permanent damage, such as general debility, paralysis of one or more limbs, deafness, mental weakness, epilepsy, etc. Many cases of general paralysis of the insane and other forms of so-called mental disease are the result of meningitis.
DURATION.—In the adult usually the disease lasts about a week or ten days; exceptionally, it may last two or three weeks.
COURSE.—In young children the course of meningitis differs somewhat from that which is observed in adults, though the symptoms are essentially the same. It is more sudden in its onset and shorter in its duration. The prodromal stage may be brief or hardly noticeable; but in older children restlessness, sensitiveness to light and sound, wakefulness, slight twitchings of the features or of the limbs, a half-open condition of the eyelids during sleep, occasional vomiting, etc., are more commonly noticed. Convulsions are more common than in the adult, and sometimes constitute the chief symptom. They may be confined to a single extremity, but in [p. 719] general they shift from one limb to another. The muscles of the eyeball are usually implicated, causing strabismus. Retraction of the head is rarely absent, especially in young infants. These convulsions are almost always tonic, but occasionally they alternate with clonic ones. Distension and increased pulsation of the anterior fontanel is always observed in infants a few months old affected with this disease. When meningitis is secondary to some other disease, the first symptom noticed in children is apt to be vomiting, with delirium. According to Steffen, pneumonia is the disease most frequently complicated with meningitis in children. As in tubercular meningitis, the most prominent symptom may be mere sopor, sometimes with intervals of intelligence. Simple meningitis in children is generally a rapid disease, proving fatal in most cases within a week, and sometimes even in a few hours. Exceptionally, it may last much longer. A case occurring in a girl six years old, the duration of which was fifty-five days, is reported by J. Bokai, Jr.;17 the diagnosis was substantiated by autopsy. Another case, which recovered after seven weeks, is mentioned by Henoch.18
17 Jahrb. f. Kinderkrankheiten, N. F., xviii. 1, p. 105; and Schmidt's Jahrb., 1882, No. 6, p. 269.
18 Eduard Henoch, Vorlesungen über Kinderkrankheiten, Berlin, 1881, p. 277.
PATHOLOGICAL ANATOMY.—The lesions, which are rarely general, may occupy a greater or less extent of the membrane. They are usually disposed symmetrically with regard to the two hemispheres, or occupy corresponding regions of the base. The vessels are in the beginning of the disease distended, the finest ramifications being injected, giving a red color to the membrane, which varies in different places from crimson to light pink. The perivascular spaces of the larger vessels are filled with a grayish or yellowish fluid composed of extravasated liquor sanguinis and white blood-corpuscles. The meshes between the two layers of the pia are soon infiltrated with pus, and the thickened membrane can be stripped off from the surface of the brain, which is, however, adherent to it in places and is torn in the process. Sometimes a thin layer of pus, which can be scraped off with the knife, is found upon the surface of the pia. The extent of the lesion varies much in different cases. It may be confined to a limited region of the hemispheres, or it may spread to the fissure of Sylvius, where two surfaces become adherent. Sometimes the concrete pus and fibrin are deposited in thick masses upon the base of the brain, often completely surrounding the cranial nerves, and even the medulla. The inflammation may extend to the lateral ventricles, which become filled with a turbid fluid containing pus-cells, and sometimes wholly purulent. The choroid plexuses are often covered with flecks of pus. When the distension of the ventricles is very great, the gyri of the brain are more or less flattened by compression against the cranium, and the outer layer of the cerebral substance is bloodless and œdematous. The cerebral sinuses are distended with blood, and frequently contain thrombi due to an early stage of the inflammatory process, besides recent coagula.
DIAGNOSIS.—The diagnosis of acute meningitis is often difficult, and sometimes impossible, especially in the early stages, when the line between congestion and inflammation cannot be drawn, and in complicated cases. The typical symptoms are sudden and acute pain in the head, with [p. 720] sensitiveness to light and sound, contracted pupils, rapid pulse, and vomiting, followed by delirium, convulsions, and coma. If these symptoms were observed in an individual previously in good health, they would be strongly suggestive of the disease, and yet many of them are often present in the beginning of pneumonia, erysipelas, typhoid, typhus, and other eruptive fevers, uræmia, and poisoning from narcotic substances. Hence it is important to eliminate these sources of error before coming to a conclusion, and a neglect of this precaution is a not infrequent source of error in the diagnosis. A careful examination of the urine will generally enable us to exclude uræmia. The presence or absence of the eruptive fevers can usually be determined by the attendant circumstances, and yet cases of scarlatina, typhoid fever, variola, etc., beginning with active cerebral symptoms, are sometimes hastily pronounced to be meningitis by inexperienced observers. In poisoning by narcotics the history will often aid us in the diagnosis; moreover, except in the case of opium, the pupils are dilated instead of being contracted. In traumatic cases, with fracture of the cranial bones, it is always difficult, and often impossible, to distinguish between the symptoms of meningitis and those due to other lesions. In concussion without fracture we must be guided in our diagnosis by the same rules as in idiopathic cases. The distinction between extreme congestion of the pia mater and meningitis must be based chiefly upon the duration of the symptoms. The former is usually brief in its course; the latter lasts one or two weeks, and in cases which recover is often followed by after-effects which are more or less permanent in their duration, such as paralysis or rigidity of the limbs, mental defects, etc. Rapid recovery from the acute symptoms would be strongly suspicious of congestion, and doubtless in many such cases the treatment has been credited with a success to which it was not entitled. The diagnosis from tubercular meningitis will be reserved for the article on that disease.
PROGNOSIS.—Acute meningitis is fatal in the majority of cases, though recovery is possible. A gradual diminution of the severity of the symptoms, especially in respect to temperature, pulse, pain in the head, and other cerebral phenomena, would afford encouragement, but we must not trust too much to the brief appearances of amendment so often observed.
TREATMENT.—The indications for treatment are threefold: 1st, to prevent or arrest the inflammation; 2d, to modify its violence and shorten its duration when arrest is no longer possible; and 3d, to place the patient in the best condition to withstand the violence of the disease and to recover from its effects. It is only by prompt action that we can hope to attain the first object, that of preventing the passage of hyperæmia into inflammation. The patient should be placed in a cool and well-ventilated apartment of good size, from which a bright light is excluded. His head, moderately raised, should be kept cool by means of pounded ice enclosed in a rubber bag or a bladder. One or more leeches, according to his age, should be applied behind the ears, or blood may be drawn from the temples or back of the neck by means of cupping. The bleeding should be encouraged by poultices if necessary, but with young children the abstraction of blood should be done with caution. An active purge should be given, such as ten grains each of calomel and jalap, followed by castor oil or infusion of senna; for [p. 721] children, from three to six grains, according to age, followed by oil, would be sufficient. The medicine should be repeated in a few hours if there be no effect. Counter-irritation by means of blisters is recommended by most authorities as a valuable aid in the first stage of the disease. Unless the application be very extensive, it is not likely to be of any avail, and extensive blistering would hardly fail to greatly reduce the strength of the patient, and also is likely to irritate the kidneys. There are no medicines which can be relied upon to arrest the inflammatory process. Nevertheless, the tincture of aconite-root, in the dose of from one to three drops, according to the age of the patient, every two hours, might be given early, with the view of fulfilling the second indication by its sedative property. The bromide of potassium or of sodium, combined with small doses of chloral hydrate or of sulphate of morphia, will also calm the excitement and pain, and diminish convulsions. The success which sometimes follows the employment of ergot in the epidemic cerebro-spinal meningitis warrants its trial. Bartholow recommends the wet sheet two or three times a day if the temperature is high. Steffen advises four grains of sulphate of quinine with one grain of salicylate of soda, from two to four times daily, for young children, and in double these doses for older ones. The alimentation of the patient should be carefully attended to during this stage. Nourishing liquid food, such as milk, gruel, broth, eggs, with stimulants if indicated, should be given at proper intervals, care being taken not to overload the stomach, as is frequently done. When the patient can no longer swallow the food must be given by the rectum. During the stage of compression it is useless, in the present state of our knowledge, to expect any benefit from the further administration of drugs, and the treatment then consists mainly in giving small quantities of food at regular intervals, and in such external applications as the bodily temperature may require. The bladder must be relieved by the catheter when necessary. Simple enemata are generally sufficient to prevent constipation.
Chronic inflammation of the pia mater rarely follows the acute form, but is generally secondary to other conditions, such as inflammation and tumors of the dura, tumors and abscess of the brain, disease of the vessels of the brain, suppurative otitis, and to constitutional diseases, especially alcoholism, syphilis, and pulmonary tuberculosis. It is one of the most common lesions found after death from general paralysis of the insane. As a distinct affection, unconnected with constitutional disease, it is extremely rare, though less so, according to Flint,19 than the acute form. He cites a case in which the symptoms were intermittent. The patient, fifteen years old, died after a month's illness. The autopsy showed cerebral hyperæmia, lymph at the base of the brain, and distension of the ventricles with transparent fluid. There were no tubercles. In most cases in which the results of chronic meningitis are found after death the cortical substance of the brain is involved in the disease; hence [p. 722] the difficulty in defining its symptoms, which are usually extremely vague, and not always distinctive of cerebral disease. The principal are pain in the head, vertigo, vomiting, impairment of the memory, mental apathy, drowsiness, and muscular weakness. The anatomical changes are thickening and opacity of the membrane by the deposit of lymph upon its surface and into the connective tissue, adhesions to the dura and to the cortical substances of the brain, together with hyperæmia of the latter. These appearances are usually distributed in irregular patches of greater or less extent.
19 Austin Flint, M.D., Principles and Practice of Medicine, 5th ed., Philada., 1881, p. 701.
The DIAGNOSIS of chronic meningitis is often obscure or impossible. Long-continued pain in the head, accompanied by vertigo, impairment of memory, drowsiness, mental apathy, etc., without paralysis, would be suggestive of it, especially if there were occasional intermissions of the symptoms. The probability would be greatly increased if the patient had a syphilitic or alcoholic history. The diagnosis should exclude tumor of the brain, chronic pachymeningitis, and chronic hydrocephalus, but as these diseases are often complicated with chronic meningitis, the distinction might be very difficult. As already stated, chronic meningitis is almost a constant lesion in general paralysis, as well as in other forms of chronic insanity, but there are no special symptoms by which its presence can be ascertained during life.
TREATMENT.—Our aim should be to relieve pain, diminish congestion, and favor absorption. Counter-irritation to the head and nucha by means of small blisters or croton oil should be employed with moderation. Bromide of potassium, or, if necessary, small doses of morphia, may be given if the pain be severe. Should there be symptoms of cerebral congestion, such as acute delirium, flushing, and heat of head, an ice-bag should be applied to the head and leeches behind the ears, or blood may be drawn from the temples or nucha by cupping. As an absorbent the iodide of potassium is much recommended, but it is not likely to be effectual, except in syphilitic cases. The bowels should be kept free, but without active purging. The general health of the patient should be promoted by suitable diet and regimen, by relief from excitement and fatigue, or by change of scene and of climate. For the treatment of chronic meningitis complicating syphilis, alcoholism, and tuberculosis, the reader is referred to the articles treating of those diseases.
DEFINITION.—Inflammation of the pia mater of the brain, with effusion of lymph and pus, caused by the deposit of miliary tubercles upon its surface or into its substance.
SYNONYMS.—Scrofulous meningitis, Granular meningitis, Basilar meningitis, Acute hydrocephalus, Dropsy of the brain.
HISTORY.1—It is only within a comparatively recent time that tubercular meningitis has been distinguished from other cerebral diseases. Up to the eighteenth century the term hydrocephalus was employed not only for the dropsical diseases of the head, including internal and external hydrocephalus, but also for meningeal inflammations, both simple and tubercular, and for congestion of the brain and of the membranes; the accumulation of water in the ventricles or between the membranes being looked upon as the disease, and not as one of its consequences. The term was even applied to external tumors, as cephalæmatoma and caput succedaneum. We owe the first accurate account of the symptomatology of acute hydrocephalus, or ventricular dropsy, to Robert Whytt of Edinburgh, whose remarkable monograph, entitled Observations on the Dropsy of the Brain, first published in 1768, after his death, was founded upon the study of 20 cases with 10 autopsies. No addition of importance has been made by later observers to his graphic description of the disease or to his rules for its diagnosis. Whytt, however, had no clear notion of its pathogeny, and it was not till 1815 that Gölis pointed out that acute ventricular dropsy was a secondary condition depending upon previous inflammation of the membranes or vessels of the brain.
1 See W. Hughes Willshire's valuable paper, entitled “Historic Data on Scrofulous Meningitis,” in Brit. and For. Med.-Chir. Review, Oct., 1854.
In 1827, Guersant remarked that the inflammation of the meninges constituting acute hydrocephalus presented such peculiarities as led him to denominate it granular meningitis. He did not, however, connect the granular deposit with tubercle. This was left for Papavoine to effect, who in 1830 published two cases of tuberculous arachnitis, in one of which effusion into the ventricles, or hydrocephalus, existed. The meningeal granulations or tubercles were described with care, and their coincidence with tuberculous deposit elsewhere was remarked upon, as also the apparent occurrence of the former previous to the inflammatory action in the meninges, and in one case the existence of the tuberculous granules without the sequence of inflammation. The important pathological element of acute hydrocephalus thus clearly pointed out by Papavoine [p. 724] now became apparent to observers, and obtained almost universal assent. The attention of the profession in this country was first called to it by W. W. Gerhard of Philadelphia in 1833, in an admirable paper published in the American Journal of the Medical Sciences,2 containing the reports of thirty-two cases with autopsies. In every case but two tubercles were found in other organs besides the meninges. In one of these two, gangrenous cavities were found in the lungs without tubercles, though perfectly characterized miliary tubercles existed in the membranes; in the other case the lungs were not examined with care, Gerhard not being present at the autopsy.
2 Vols. xiii. and xiv., 1833-34.
Finally, the distinction between tubercular and simple meningitis was pointed out by Guersant in 1839, and clearly established by Barthez and Rilliet in 1843 in their systematic work on the diseases of children; and it was further elucidated by Rilliet in 1847.
ETIOLOGY.—The causes of tubercular meningitis are predisposing and exciting. Among the former are hereditary tendency to tuberculosis and to the so-called scrofulous diathesis; the previous existence of tubercle in any part of the body, especially in the lungs; and the presence of caseous degeneration in the bronchial, the mesenteric, and other glands, or in the parenchyma of various organs, as the lung, the testicle, the liver, the spleen, etc. The dependence of miliary tuberculosis of the pia upon previously-existing caseous or other inflammatory deposits in some part of the body is acknowledged by most modern pathologists. Seitz3 states that out of 130 cases, with autopsies, of adults, upon which his work is based, such deposits were found in 93.5 per cent. General constitutional weakness, either congenital or resulting from grave disease or from overwork, from insufficient or unwholesome food, and from bad hygienic surroundings, also favors the deposit of tubercle in the meninges. Sometimes two or more predisposing causes exist at once. Thus, a child born of tuberculous parents may be fed with artificial diet instead of being nursed, or may live in a house whose sanitary condition is bad. Hence the disease is common among the poor, although by no means rare in the higher classes of society. In some cases it is difficult or impossible to assign any predisposing cause. A single child out of a numerous family may be stricken with the disease, while the rest of the children, as well as the parents and other ascendants, are healthy. For instance, while writing this article I had under observation a little boy six years old whose parents are living and healthy, with no pulmonary disease in the family of either. The only other child, an older brother, is healthy. While apparently in perfect health the child was attacked with tubercular meningitis, and died in seventeen days with all the characteristic symptoms of the disease. At the autopsy there was found much injection of the cerebral pia everywhere, a large effusion of lymph at the base of the brain and extending down the medulla, abundance of miliary tubercles in the pia and accompanying the vessels in the lateral regions of the hemispheres, lateral ventricles distended with nearly clear fluid, ependyma smooth, choroid plexuses covered with granulations, convolutions of brain much flattened. Careful investigation, however, will usually [p. 725] enable us to detect some lurking primary cause, either in the family predisposition or in the history of the patient himself.
3 Die Meningitis Tuberculosa der Erwachsenen, von Dr. Johannes Seitz, Berlin, 1874, p. 317.
Season appears to have but little influence on the production of the disease. The largest number of cases is observed during winter and spring, owing doubtless to the influence of the temperature and weather, and to the exclusion from fresh air, in favoring the development of tubercle and the scrofulous diathesis. Males, both children and adults, are somewhat more frequently attacked than females.
In regard to the exciting causes it may be said that where a disposition to the deposit of tubercle exists, anything which tends to lower the vitality of the individual is likely to hasten the event. In infants with hereditary tendency to tubercle, an improper diet is especially liable to develop meningeal tubercle. In older children, besides unwholesome or insufficient food and unfavorable hygienic surroundings, the acute diseases common to that period of life, such as the eruptive fevers, intestinal disorders, whooping cough, etc., often act as immediate causes. Sometimes the development of the disease may be traced to over-stimulation of the nervous system by excessive study, often aided by imperfect ventilation or overheating of the school-room. Caries of the temporal bone from disease of the middle ear may act as an immediate cause of tubercular meningitis, although simple meningitis is of course a more frequent result of that condition. The disease has been known to follow injuries of the head from blows or falls. In a larger number of cases the exciting cause is not discoverable, especially when the meningeal affection is simply an extension of the disease from some other part of the body, as the lungs, the bronchial or mesenteric glands, etc. This is often the case, both in adults and in children, when tubercular meningitis complicates pulmonary consumption.
SYMPTOMS.—The disease is most frequently observed in children between the ages of two and seven years. It is much less common in adults, who are generally attacked between the ages of twenty and thirty years. In the majority of cases the invasion of the malady is preceded by a prodromic stage, usually occupying from a few days to several weeks, though sometimes extending over a considerably longer period. This stage probably represents the process of deposit of miliary tubercles in the pia mater before their presence has given rise to much structural change in the tissue. The characteristic symptoms of the prodromic stage consist chiefly in an alteration of the character and disposition of the patient, varying in extent in different cases. In general, it may be said that he becomes sad, taciturn, apathetic, irritable, indisposed to play, often sitting apart from his companions, gazing in a strange way into vacancy. There is diminution or loss of appetite and some emaciation. He is restless at night, is disturbed by nightmare, or grinds his teeth. The digestion is deranged. Usually there is constipation, but occasionally diarrhœa, or these conditions may alternate with each other. Squinting and twitching of the facial muscles are sometimes noticed. Headache may occur early in this stage, but it is usually observed later, and it then forms a prominent symptom. Vomiting is also frequent, usually not preceded by nausea, sometimes provoked by sudden movement, as in sitting up in bed, and is apt to occur when the stomach contains little or no food. These symptoms vary much in degree, and they are often so slight [p. 726] that they pass unnoticed by the parents or friends. Occasionally the patient, if a child, will manifest a strange perversity or an unusual disobedience, for which he is perhaps punished under the belief that his misconduct is intentional. In older children and in adults delirium, especially at night, sometimes followed by delusions which may be more or less permanent, is frequent at this stage. The above symptoms often remit from time to time, and during the interval the patient may seem to have recovered his health. The prodromic symptoms are rarely altogether wanting in children, although they may have escaped notice from lack of opportunity of observation on the part of the physician. On the other hand, as Steffen4 justly observes, the most characteristic symptoms may be present, and lead even an experienced observer to a confident diagnosis of tubercular meningitis during the early stage of a case of typhoid fever or of cerebral congestion without tuberculosis.
4 “Meningitis Tuberculosa,” by A. Steffen, in Gerhardt's Handb. der Kinderkrankheiten, 5 B., 1ste Abth., 2te Hälfte, p. 465.
For convenience of description it is customary to divide the disease proper, after the prodromal period, into three stages—viz. of irritation, compression, and collapse. In some cases it is not difficult to observe these divisions, but it must be borne in mind that in others the symptoms do not follow any regular sequence, so that no division is possible. In infants profound slumber may be the only morbid manifestation throughout the entire disease. Steffen records such a case, and I have seen two similar ones.
First Stage: The interval between the prodromic period and the first stage is usually so gradual that no distinction between the two can be detected. In other cases the disease is ushered in suddenly by some striking symptom, such as an attack of general convulsions, with dilated pupils and loss of consciousness. This is not often repeated, though partial twitchings of the limbs or of the muscles of the face may follow at intervals. In young children a comatose condition, with unequal pupils, is apt to take the place of these symptoms. The principal phenomena of the first stage are headache, sensitiveness to light and sound, vomiting, and fever. The latter varies much in intensity from time to time, but is not usually high, the temperature seldom rising above 103° F., and usually, but not always, higher at night than in the morning; but there is no characteristic curve. The pulse varies in rate, but is usually slow and irregular or intermittent. The respiration is irregular, with frequent sighing. The tongue is dryish and covered with a thin white coat. The bowels are costive. Delirium is frequent at night, and the sleep is disturbed, the patient tossing about and muttering or crying out. The eyes are half open during sleep. These symptoms become more marked from day to day. The pain in the head is more frequent and severe; the patient presses the hands to the forehead or rests the head against some support if sitting up. During sleep he occasionally utters a loud, sharp cry, without waking. There is increasing apathy, and some intolerance of light, shown by an inclination to turn toward the wall of the room or to lie with the face buried in the pillow. The appetite is lost, the constipation becomes more obstinate, the slowness and irregularity of the pulse persist. With the rapid emaciation the belly sinks in, so that the spinal column can be easily felt. Soon the child falls into a state of almost [p. 727] continual somnolence, from which, however, he can be awakened in full consciousness, and will answer correctly, generally relapsing again immediately into slumber. His restlessness diminishes or ceases altogether, and he lies continuously on the back with the head boring into the pillow. He becomes more passive under the physician's examination, in strong contrast to his previous irritability. At the end of a week or more from the beginning of this stage symptoms of irritation of some of the cerebral nerves begin to show themselves, in consequence of pressure from the increasing exudation at the base of the brain and into the ventricles. Strabismus (usually convergent), twitching of the facial muscles and grimaces, grinding of the teeth, or chewing movements of the mouth are noticed. The somnolence deepens into sopor, from which it becomes more and more difficult to arouse the patient, who gradually becomes completely insensible.
Notwithstanding the alarming and often hopeless condition which this assemblage of symptoms indicates, intervals of temporary amendment not unfrequently take place. The child may awake from his lethargy, recognize those about him, converse rationally, take his food with relish, and exhibit such symptoms of general improvement that the parents and friends are led to indulge in fallacious hopes, and sometimes the physician himself ventures to doubt the accuracy of his diagnosis. Such hopes are of short duration; the unfavorable symptoms always return after a brief interval. The duration of the first stage may be reckoned at about one week.
Second Stage: This period is not separated from the preceding one by any distinct change in symptoms. The patient lies in a state of complete insensibility, from which he can no longer be aroused by any appeal. The face is pale or of an earthen tint, the eyes are half closed. If the anterior fontanel be still open, the integument covering it is distended by the pressure beneath. Often one knee is flexed, the opposite leg extended; one hand applied to the genitals, the other to the head. Sometimes one leg or arm is alternately flexed and extended. The head is apt to be retracted and bores into the pillow. The pupils are dilated, though often unequal and insensible to light: the sclerotica are injected; a gummy exudation from the Meibomian glands forms on the edges of the lids. The patient sighs deeply from time to time, and occasionally utters a loud, piercing cry. Paralysis, and sometimes rigidity of one or more of the extremities, are often observed, and occasionally there is an attack of general convulsions. The pulse continues to be slow and irregular, the emaciation progresses rapidly, and the abdomen is deeply excavated. The discharges from the bladder and rectum are involuntary. The average duration of the second stage is one week.
Third Stage: No special symptoms mark the passage of the second stage into the third, which is characterized by coma, with complete resolution of the limbs. The constipation frequently gives place to moderate diarrhœa. The distended fontanel subsides, and often sinks below the margin of the cranial bones. A striking feature of this stage is a great increase in the rate of the pulse, the heart being released from the inhibitory influence of the par vagum in consequence of the complete paralysis of the latter from pressure. The pulse varies in rapidity from 120 to 160 or more in the minute. For the same reason the respiration also [p. 728] increases in frequency, though not to the same degree. The eyelids are widely open; the pupils are dilated and generally motionless, even when exposed to a bright light. The eyes are rolled upward, so that only the lower half of the iris is visible; the sclerotica is injected from exposure to the air and dust. Convulsions may occur from time to time. Death terminates the painful scene, usually in from twenty-four to forty-eight hours, but sometimes the child lives on for days, unconscious, of course, of suffering, though the afflicted parents and friends can with difficulty be brought to believe it.
Certain points in the symptomatology of tubercular meningitis demand especial consideration.
I have already observed that the division of the disease into definite stages is purely arbitrary, and is employed here merely for convenience of description; in fact, few cases pursue the typical course. A period of active symptoms and another of depression can often be observed, but these frequently alternate. Stupor and paralysis may characterize the early stage, and symptoms of irritation, with restlessness, screaming, and convulsions, predominate toward the end. Certain characteristic symptoms may be wholly or in part wanting, such as vomiting, constipation, or stupor.
The temperature shows no changes which are characteristic of the disease. Throughout its whole course it varies from time to time, without uniformity, except that it usually rises somewhat toward night. It seldom exceeds 102° or 103° F., unless shortly before death, when it may rise to 104° F., or even higher, and may continue to rise for a short time after death.
During the premonitory stage the pulse offers no unusual characteristics. Its frequency is often increased, as is usual in any indisposition during the period of childhood, but it preserves its regularity. Toward the close of this period, and especially during the first stage of the disease proper, a remarkable change takes place. It becomes slow and irregular, the rate often diminishing below that in health. The irregularity varies in character; sometimes the pulse intermits, either at regular or irregular intervals. An inequality in the strength of different pulsations is also observed. These peculiarities of the circulation are due to the irritation of the medulla and the roots of the par vagum, by which the inhibitory function of that nerve upon the action of the heart is augmented. During the last period, on the other hand, the increasing pressure on the vagus paralyzes its function, and the heart, freed from its control, takes on an increased action, the pulse rising to 120 beats, and often many more, in the minute. Robert Whytt, in his interesting memoir,5 dates the beginning of the second stage from the time that the pulse, being quick but regular, becomes slow and irregular; the change again to the normal frequency, or beyond it, marking the commencement of the third stage.
5 “An Account of the Symptoms in the Dropsy of the Ventricles of the Brain,” in the Works of Robert Whytt, M.D., published by his son, Edinb., 1768, p. 729.
In the early stage the respiration presents nothing abnormal, but when the pulse becomes slow and irregular the breathing is similarly affected. Sighing is very common in the prodromal period and first stage. Toward the end of the second stage the increasing paralysis [p. 729] of the respiratory centre gives rise to the phenomena known as the Cheyne-Stokes respiration, consisting of a succession of respiratory acts diminishing in force until there is a complete suspension of the breathing, lasting from a quarter to three-quarters of a minute, when the series begins again with a full inspiration. In general, the variations in the rate of the respiration follow those of the pulse, though the correspondence is not always exact.
In the early stage of the disease the pupils are usually contracted and unequal. They are sluggish, but still respond to the stimulus of light. At a later period they become gradually dilated, and react even more slowly to light or not at all, the two eyes often differing in this respect. Ophthalmoscopic examination frequently shows the appearance of choked disc and commencing neuro-retinitis. In rare cases tubercles are seen scattered over the fundus of the eye. They are about the size of a small pin's head, of a yellowish color, and of sharply-defined contour. Neuro-retinitis and choked disc are not, of course, pathognomonic of tubercular meningitis, and choroidal tubercles are so rarely seen as to be of little avail in diagnosis. In fact, they are less frequent in this disease than in general tuberculosis without meningitis. In twenty-six cases of tubercular meningitis examined by Garlick at the London Hospital for Sick Children they were found only once.6 The effect upon the conjunctiva of the unclosed lids has been already described.
6 W. R. Gowers, M.D., Manual and Atlas of Medical Ophthalmoscopy, Philada., 1882, p. 148. See, also, Seitz, op. cit., p. 347; Steffen, op. cit., pp. 452 and 472; and “Tubercle of the Choroid,” Med. Times and Gazette, Oct. 21, 1882, p. 498.
The tongue is somewhat coated soon after the beginning of the disease, and the breath is offensive. The appetite is lost, and there is decided emaciation in many cases during the prodromic period. The thirst is usually moderate. Vomiting is one of the most constant symptoms during the first period, and its occurrence on an empty stomach is characteristic of tubercular meningitis. It is not usually preceded by nausea, and often takes place without effort, by mere regurgitation, the rejected fluid consisting chiefly of bile mixed with mucus. Although constipation is the most common condition in the early stage, and is often rebellious to treatment, yet in some cases diarrhœa is observed, which may mislead the physician in respect to the diagnosis. From the beginning of the second stage, and sometimes earlier, the discharges from the bowels and the bladder are involuntary.
DURATION.—The duration of tubercular meningitis, apart from the prodromic period, which often can hardly be determined, averages from two weeks to two weeks and a half. In exceptional cases death may take place in a few days or a week, and occasionally a patient may linger for several weeks,7 the difference being apparently due to the rapidity of the tubercular deposit and of the resulting inflammation and exudation. The patient usually takes to his bed at the beginning of the first stage, but he may be up during a part of the day until the beginning of the second. In rare instances the child will be about, and even out of doors, until a few days before death.
7 Such a case is reported by Michael Collins in the London Lancet, March 8, 1884.
PATHOLOGICAL ANATOMY.—The essential lesion of tubercular [p. 730] meningitis consists in a deposit of miliary tubercles in the pia mater of the brain, giving rise to inflammation of that membrane and exudation of serum and pus. In the early stage both surfaces of the pia are reddened and more or less thickened, and present an opaline appearance, while between them—that is, in the meshes of the pia—we find a colorless and transparent fluid which is effused in greater or smaller amount, resembling jelly when viewed through the arachnoid. These conditions are sometimes observable on the convexity of the hemispheres, but are much more abundant on the lateral surfaces, and especially at the base. More distinct evidence of inflammation is shown by the presence of a yellowish or greenish-yellow creamy deposit on the surface of the pia, consisting chiefly of pus, which is also much more abundant at the base than elsewhere, especially about the optic commissure, infundibulum, pons Varolii, and the anterior surface of the medulla. The cranial nerves may be deeply imbedded in the deposit, which often extends into the fissure of Sylvius, gluing together the adjacent surfaces of the lobes, and accompanies the vessels, forming narrow streaks along the sides of the brain up to the convexity.
The miliary tubercles or granulations consist of semi-transparent bodies, grayish or whitish in color, varying in size from that of the head of the smallest pin, indeed almost invisible to the naked eye, to that of a millet-seed (whence their name). Larger masses are frequently seen, formed by the aggregation of smaller granulations. The tubercles are usually found on the inner surface of the pia, always in the immediate neighborhood of the blood-vessels, which they accompany in their ramifications, and are also scattered, in greater or less numbers, throughout the purulent exudation from the surface of the pia. They are most abundant at the base of the brain, ascending the sides along the course of the vessels. Sometimes, though rarely, they are more abundant on the convexity. The total number varies; it is usually very large, but sometimes only a limited number exists, even in well-marked cases, and along with intense inflammation of the pia. The granulations are found in different degrees of development—sometimes all of them similar in color, size, and consistency, at others in various stages of fatty degeneration. The distribution may be symmetrical in the two hemispheres or irregular. Under the microscope (after suitable preparation of the part) the bacillus tuberculosus in considerable numbers may be found in the pia, in places adjacent to the arterioles.8
8 See a case reported by Y. Dawson in the London Lancet, April 12, 1884, in which tubercles were visible only by the microscope with numerous bacilli.
The ventricles of the brain are usually distended with a clear or opalescent, rarely bloody, fluid, the amount of which generally corresponds to the intensity and extent of the meningeal inflammation, although sometimes it is not above the normal quantity. The two lateral ventricles are affected in an equal degree; the third and fourth ventricles are more rarely implicated. According to Huguenin,9 it is doubtful whether acute inflammation of the ependyma takes place in tubercular meningitis. Steffen also10 says that the ependyma is not inflamed, and that it is not the seat of the deposit of tubercles. This latter statement is denied by other authorities, and Huguenin is inclined to believe that they may exist [p. 731] in that membrane. In the following case, under my care, abundant granulations were found on the surface of the ependyma:
9 G. Huguenin, op. cit., p. 499.
10 Op. cit., p. 449.
Olaf M—— (male), æt. 8 years, born in Denmark, entered Massachusetts General Hospital Sept. 13, 1881. Maternal grandmother died of consumption; paternal grandfather lived to the age of ninety-five years. One brother had some disease of hip. Patient was the child of poor parents and lived in an unhealthy suburb of Boston. During the two preceding winters he had a bad cough. He was apparently well till four weeks before his entrance, when he complained of bellyache, and became listless, but he was out of doors ten days before he came to the hospital. It was noticed that he was sensitive to sound. No vomiting, no diarrhœa, no epistaxis, no cry; some cough. He had been somnolent, and was observed to swing his arm over his head while asleep. June 14, when first seen by me, he was lying on his back, unconscious, eyes half closed, pupils dilated, jaw firmly closed, much emaciated, belly retracted, left leg occasionally flexed and extended. No priapism. The optic discs were reddened. June 15, there is some intelligence, he answers questions; keeps one hand on the genitals. June 16, pupils contracted, does not swallow. June 18, left eye divergent, conjunctiva injected, whole surface livid, cries out occasionally. Died at midnight.
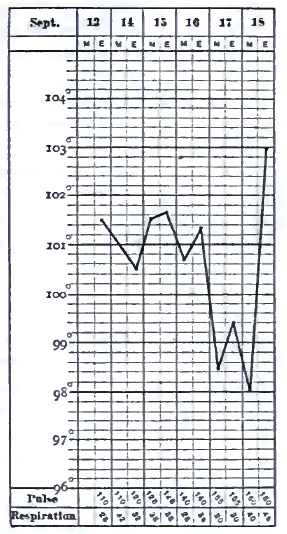
Autopsy.—General lividity of surface, much emaciation. Much fine arborescent injection on outer surface of dura mater. Numerous Pacchionian bodies. Yellow matter beneath arachnoid along course of vessels on each side of anterior lobes. Abundant fine granulations along course of vessels on each anterior lobe, on upper margins of median fissure, along fissure of Sylvius, and on choroid plexuses. Very little lymph at base of brain. Six or eight ounces of serum from lateral ventricles, and abundant fine transparent granules over ependyma of both. Numerous opaque granulations in pia mater of medulla oblongata. Surface of right pleura universally adherent. Mucous membrane of bronchia much injected; a considerable amount of pus flowed from each primary bronchus. No tubercles in lungs nor in peritoneum. No ulcerations in intestines. No other lesions.
The choroid plexuses are generally involved in the inflammatory process, and are sometimes covered with yellow purulent exudations. As in the above case, large numbers of tubercles may be found in them, notwithstanding the opinion of Huguenin that their number is always small.
The substance of the brain in the vicinity of the tubercular deposit is generally found in a more or less œdematous condition, owing to the obstruction of the circulation resulting from compression of the vessels [p. 732] by the tubercles and effused lymph. Softening, sometimes even to diffluence, not unfrequently occurs in the neighborhood of the deposit, probably from ischæmia (necrobiosis). If there be any considerable amount of exudation in the ventricles, the convolutions are flattened by compression against the cranial bones.
The above-described lesions are not confined to the brain, but may extend to the cerebellum, the pons, the medulla, and the spinal cord. If examinations of the latter were more frequent in autopsies of this disease, we should doubtless find, as has been done in some instances, that the membranes often show the characteristic alterations of tubercular meningitis, and even the presence of granulations in the cord itself. The lesions may extend throughout the cord, and are especially noticed in the dorsal region and in the vicinity of the cauda equina. Their presence explains some of the symptoms evidently due to spinal origin, such as retraction of the head with rigidity of the neck and of the trunk, contractions of the limbs, tetanic spasms, priapism, paralysis of the bladder and rectum, etc., which are common in simple spinal meningitis.
The deposit of miliary tubercles in the pia mater, with little or no accompanying meningitis, is met with in rare instances. The tubercles are few in number, but vary in dimensions, being sometimes united together in masses of considerable size, which are frequently encysted. Beyond thickening and opacity of the membrane, their presence seems to excite but little inflammatory reaction, but they are generally accompanied by ventricular effusion which by its pressure gives rise to characteristic symptoms.
The principal lesions found in other organs of the body consist of tubercle in various stages of development, caseous matter, diseases of the bones, etc. Miliary granulations are chiefly seen in the lungs, peritoneum, intestinal mucous membrane, pleura, spleen, liver, and kidneys. The bronchial and mesenteric glands often contain caseous masses, some of which are broken down and suppurating. The testicles sometimes present the same appearances. In adults, the most frequent lesion which is found external to the brain is pulmonary tuberculosis in a more or less advanced stage. Tubercles are also sometimes present in the eye. Angel Money11 states that out of 44 examinations made at the Hospital for Sick Children, London, the meninges were the seat of gray granulations in 42. The choroid (one or both) showed tubercles 14 times (right 3, left 5, both 6), and 11 times there were undoubted evidences of optic neuritis. Twice the choroid was affected with tubercle when the meninges were free; in one of these instances there was a mass of crude tubercle in the cerebellum; in the other, although there were tubercles in the belly and chest, there were none in the head. So that 12 times in 42 cases of tubercles in the meninges there were tubercles in the choroid—i.e. about 31 per cent.
11 “On the Frequent Association of Choroidal and Meningeal Tubercle,” Lancet, Nov. 10, 1883.
DIAGNOSIS.—In many cases tubercular meningitis offers but little difficulty in the diagnosis. Although the symptoms, taken singly, are not pathognomonic, yet their combination and succession, together with their relation to the age, previous health, and antecedents of the patient, are usually sufficient to lead us to a correct opinion. The prodromic period [p. 733] of altered disposition (irritability of temper or apathetic indifference), headache, constipation, vomiting, and emaciation, followed by irregularity and slowness of the pulse, sighing respiration, sluggishness and irregularity of the pupils; the progress from somnolence to unconsciousness and coma; the sudden lamentable cry; the convulsions and paralysis; the return of rapid pulse and respiration in the last stage,—are characteristic of no other disease. Our chief embarrassment arises during the insidious approach of the malady, before its distinctive features are visible or when some important symptom is absent. Its real nature is then apt to be overlooked, and, in fact, in some cases it is impossible to decide whether the symptoms are indicative of commencing cerebral disease, or, on the other hand, are owing to typhoid fever, to a simple gastro-intestinal irritation from error in diet, to worms in the alimentary canal, to overwork in school, or to some other cause. Under these circumstances the physician should decline giving a positive opinion until more definite signs make their appearance. It must be remembered that very important symptoms may be absent in cases which are otherwise well marked. In all doubtful cases the family history should, if possible, be obtained, especially whether one or both parents or other near relatives have been consumptive or have shown symptoms of scrofula or tuberculosis in any form, and whether the patient himself has signs of pulmonary tuberculosis, of enlarged or suppurating glands, or obstinate skin eruptions. The presence or history of those conditions would add greatly to the probability of tubercular meningitis.
The diseases for which tubercular meningitis is most liable to be mistaken are acute simple meningitis, typhoid fever, acute gastro-intestinal affections, eclampsia of infants and children, worms in the intestines or stomach, the hydrencephaloid disease of Marshall Hall, and cerebro-spinal meningitis.
Acute meningitis is distinguished from the tubercular disease by its sudden invasion without prodromatous stage, by the acuteness and intensity of the symptoms, the severity of the headache, the activity of the delirium, the greater elevation of the temperature, and by its brief duration, which rarely exceeds one week. In those exceptional cases of tubercular meningitis in which the prodromal period is absent or not observed and the course is unusually rapid, it would be perhaps impossible to distinguish between the two diseases. A family history of tubercle, or the discovery of the granulations in the choroid by ophthalmoscopic examination, might save us from error under such circumstances. The great rarity of idiopathic simple meningitis should be remembered. Meningitis from disease of the ear sometimes resembles the tubercular affection, but the history of the attack, usually beginning with local pain and otorrhœa, will in most cases prevent any confusion between the two forms of disease.
The early period of typhoid often bears considerable resemblance to that of tubercular meningitis. Headache, languor, restlessness, and mild delirium are common to both. Typhoid can be distinguished by the coated tongue, the diarrhœa, the enlargement of the spleen, the tympanites, abdominal tenderness and gurgling, the eruption, and, above all, by the characteristic temperature-curve, which, if accurately observed, is conclusive. The course of typhoid fever is comparatively [p. 734] uniform, while that of tubercular meningitis is often extremely irregular. It should not be forgotten that the two diseases may coexist.
The presence of worms in the alimentary canal may cause symptoms somewhat like those of tubercular meningitis, and the symptoms of the latter disease are occasionally erroneously attributed to those parasites. The administration of an anthelmintic, which should never be omitted in doubtful cases, will clear up all uncertainty.
Cerebro-spinal meningitis is usually an epidemic, and therefore not likely to be confounded with the tubercular disease. In sporadic cases it can be recognized by its sudden onset and acute character, by the eruption, and by the prominence of the spinal symptoms.
The so-called hydrencephaloid disease of Marshall Hall is a condition of exhaustion and marasmus belonging to infancy, caused by insufficient or unsuitable nourishment, by diarrhœa, and by the injudicious depletive treatment so much in vogue in former times, when the affection was much more common than at present. Some of its symptoms, such as sighing respiration, stupor, pallor, and dilated pupils, bear a certain resemblance to those of tubercular meningitis, though it would be more easily confounded with chronic hydrocephalus. The absence of constipation, headache, convulsions, and vomiting, and the favorable results of suitable nourishment and stimulants, serve to distinguish it from cerebral disease.
Eclampsia, or sudden convulsion, is common in infants and young children, and, since the occurrence of a fit may be the first or the most striking symptom in tubercular meningitis, it is important to ascertain its origin. In the majority of cases convulsions in children arise from some peripheral irritation, such as difficult dentition, worms in the alimentary canal, constipation, fright, etc., acting through the reflex function of the spinal cord, which is unusually sensitive in the early period of life. The absence of previous symptoms, and the discovery of the source of the irritation, with the favorable effect of its removal by appropriate treatment, will in most cases suffice to eliminate structural disease of the brain. In others we must withhold a positive opinion for a reasonable time in order to ascertain whether more definite symptoms follow. Convulsions also occasionally form the initial symptom of the eruptive fevers, especially scarlatina. Here the absence of prodromal symptoms, and the speedy appearance of those belonging to the exanthematous affection, will remove all sources of doubt. Convulsions, with or without coma, occurring in the early stage of acute renal inflammations, may simulate the symptoms of tubercular meningitis. An examination of the urine will show the true nature of the disease.
In addition to the above diseases there are some cerebral affections of uncertain pathology which resemble tubercular meningitis, but which are not generally fatal. As Gee justly remarks,12 “Every practitioner from time to time will come across an acute febrile disease accompanied by symptoms which seem to point unmistakably to some affection of the brain, there being every reason to exclude the notion of suppressed exanthemata or analogous disorders. After one or several weeks of coma, delirium, severe headache, or whatever may have been the prominent symptom, the patient recovers, and we are left quite unable to say what has been the [p. 735] matter with him. To go more into detail, I could not do otherwise than narrate a series of cases which would differ from each other in most important points, and have nothing in common excepting pyrexia and brain symptoms. There is, generally, something wanting which makes us suspect that we have not to do with tubercular meningitis. Brain fever is as good a name as any whereby to designate these different anomalies; cerebral congestion, which is more commonly used, involves an explanation which is probably often wrong, and certainly never proved to be right.” No doubt such cases are occasionally cited as examples of recovery from tubercular meningitis.
12 “Tubercular Meningitis,” by Samuel Jones Gee, M.D., in Reynolds's System of Medicine, Philada., 1879, vol. i. p. 832.
PROGNOSIS.—Although there are on record undoubted instances of recovery from tubercular meningitis, yet their number is so small that practically the prognosis is fatal. It is safe to say that in almost all the reported cases of recovery the diagnosis was erroneous.13 Even should the patient survive the attack, he is usually left with paralyzed limbs and impaired mental faculties, and dies not long afterward from a recurrence of the disease or from tuberculosis of the lungs or other organs.
13 Hahn, “Recherches sur la Méningite tuberculeuse et sur le Traitement de cette Maladie” (Arch. gén. de méd., 4e Série, vols. xx. and xxi.), claims to have cured 7 cases, but of 5 of them there is no evidence that they were examples of tubercular meningitis at all. The subject of the curability of tubercular meningitis is ably treated by Cadet de Gassicourt (Traité clinique des Maladies de l'Enfance, vol. iii., Paris, 1884, p. 553 et seq.). His conclusion is that most of the alleged cures are cases of meningitis of limited extent, arising from the presence of tubercular tumors, syphilitic gummata, cerebral scleroses, and neoplasms of various kinds.
TREATMENT.—In view of the fatality of the disease, and of its frequent occurrence in childhood, the prophylactic treatment is of great importance. Every effort should be made to protect children whose parents or other near relatives are tuberculous or scrofulous, and who are themselves delicate, puny, or affected with any constitutional disorder, from tubercular meningitis, by placing them in the best possible hygienic conditions. Pure air, suitable clothing, wholesome and sufficient food, and plenty of out-of-door exercise are indispensable. Sedentary amusements and occupations should be sparingly allowed. Especial pains should be taken to prevent fatigue by much study, and school-hours should be of short duration. The hygiene of the school-room is of paramount importance, and if its ventilation, temperature, and light are not satisfactory, the child should not be permitted to enter it. The bed-chamber should be well ventilated night and day. A sponge-bath, cold or tepid according to the season or to the effect on the patient, should be given daily, followed by friction with a towel. The bowels must be kept regular by appropriate diet if possible, or by simple laxatives, such as magnesia or rhubarb. For delicate, pale children some preparation of iron will be useful. The choice must be left to the practitioner, but one of the best in such cases is the tartrate of iron and potassium, of which from two to six grains, according to the age, may be given three times daily after meals. Cod-liver oil is invaluable for scrofulous patients or where there is a lack of nutrition. A teaspoonful, given after meals, is a sufficient dose, and it is usually taken without difficulty by children, or if there be much repugnance to it some one of the various emulsions may be tried in proportionate dose. Along with this, iodide of iron will in many cases be found useful or as a substitute for the oil when the latter cannot [p. 736] be borne. It is best given in the form of the officinal syrup, in the dose of from five to twenty drops. Change of air is useful in stimulating the nutritive functions, and a visit to the seashore or mountains during warm weather will often be followed by general improvement.
Since it is not possible to arrest the disease when once begun, the efforts of the physician must be directed toward relieving the sufferings of the patient as far as possible. In the early period the restlessness at night and inability to sleep will call for sedatives, such as the bromide of sodium or of potassium, in the dose of ten or fifteen grains at bedtime or oftener. This should be well diluted with water, sweetened if necessary. The addition of five to twenty drops of the tincture of hyoscyamus increases the effect. Sometimes chloral hydrate, either alone or combined with the bromide when the latter fails, will procure quiet sleep. From five to ten grains may be given at a dose, according to the age. Compresses wet with spirit and water or an ice-cap may be applied to the head if there be much pain in that region, or it may be necessary to give opium in some of its forms by the mouth, such as the tincture or fluid extract, in doses of from one to five drops. Constipation is best overcome by means of calomel in three- to five-grain doses, to which may be added, when necessary, an equal amount of jalap powder, or an enema of soapsuds may be administered. Active purging should be avoided. Liquid nourishment, such as milk, gruel of oatmeal, farina, or barley, beef-tea, broths, etc., must be given in moderate quantities at intervals of a few hours so long as the patient is able to swallow. Occasional sponging of the whole surface with warm or cool water, and scrupulous attention to cleanliness after defecation, especially when control of the sphincters is lost, will add to his comfort. He should occupy a large and well-ventilated chamber, from which all persons whose presence is not necessary for his care and comfort should be excluded. He should be protected from noise and from bright light, and should lie on a bed of moderate width for convenience of tending.
There is no specific treatment at present known which is likely to be of any benefit in this disease, any more than in tuberculosis of other organs than the brain. Common experience has shown that mercury, which formerly had so high a reputation in the treatment of cerebral diseases of early life, not only fails completely, but adds to the sufferings of the patient when pushed to salivation. The iodide of potassium is recommended by almost all writers, but, so far as I know, there is no proof that it possesses any virtue in meningeal tuberculosis. It has the high authority of Charles West,14 however, who thinks the remedy is more encouraging than any other, and who mentions one instance in which recovery took place under its employment. He recommends that two grains be given every four hours to a child three years old, the bowels being kept free. Most authorities recommend much higher doses, such as ten or fifteen grains, three or four times daily.
14 Op. cit., p. 102.
Counter-irritation to the head or back of the neck was formerly much employed, but is now generally abandoned, as giving rise to much discomfort without obvious beneficial effect. In the cases reported by Hahn, already alluded to under the head of Prognosis, recovery is attributed to the energetic application of tartar-emetic ointment to the scalp, [p. 737] producing extensive ulceration, which in one of them lasted more than ten months before cicatrization took place. A careful examination of the reports of these cases satisfies me that but two out of the seven were really examples of tubercular meningitis. How far the recovery in the successful cases is to be attributed to the treatment is very doubtful. Small blisters applied to the vertex or back of the neck are alluded to favorably by West, but he quotes no observations in which they were followed by benefit.
Tubercular meningitis may occur at any age, but after the period of childhood it is most frequent between the ages of sixteen and thirty years. About 75 per cent. of the patients are males, and 25 per cent. females.15 The disease does not differ essentially in its course and symptoms from that in children. A family history of tuberculosis is common, or the patient may be already suffering from phthisis, scrofulous glands, cheesy deposits in various organs, caries of the bone, syphilis, or other constitutional affections. According to Seitz, in 93.5 per cent. out of 130 cases with autopsies chronic inflammatory conditions or caseous deposits were found in various organs of the body. Many cases are examples of acute tuberculosis in which the brunt of the disease has fallen upon the brain rather than the other organs.
15 Seitz, op. cit., p. 9.
When cerebral symptoms supervene upon acute disease, such as typhoid fever, pericarditis, acute rheumatism, pneumonia, the exanthemata, etc., the diagnosis between tubercular and simple meningitis is important, because the latter is not necessarily fatal, while the former is almost never recovered from. If the patient were previously healthy and presumably free from tubercular disease, the chances would be in favor of the simple form. A rapid course of the disease would also speak for acute meningitis, and recovery would almost certainly preclude tubercular meningitis. In some cases the diagnosis is difficult or impossible in the beginning.
In cases beginning without acute antecedents—in adults as in children—there is no pathognomonic symptom, but the combination and succession of the phenomena are usually sufficient for the diagnosis. Headache, depression or irritability of temper, delirium, half-closed eyes, ptosis of one lid, squinting, inequality and sluggishness of the pupils, moderate fever, sunken belly, vomiting, constipation, slow and irregular pulse, sopor gradually deepening to coma, with occasional convulsions or paralysis of the limbs, followed in the course of two or three weeks by death, especially if occurring in a patient who has already presented signs of tuberculosis in other organs, point almost unmistakably to tubercular meningitis. Some of the symptoms may not be strongly pronounced, one or two may be absent, but the general picture will suggest no other disease. According to Seitz, tubercle of the choroid is rare in tubercular meningitis of the adult. It is usually associated with tuberculosis of other organs, the pia being free. The subjoined cases are illustrations of the disease in adolescence and adult life:
Case I.—A lad sixteen years old, always somewhat delicate, with a [p. 738] cough and morning expectoration of some months' standing, exerted himself immoderately in gymnastic exercise on the afternoon of Sept. 24, 1875. That night he was awakened by cough and hæmoptysis. Signs of consolidation were found at the apices of both lungs. In three months there were swelling, induration, and suppuration of one testicle. Some months later, pain in the right arm, stiffness of the shoulder-joint, and an abscess communicating with the joint, from which small spicula of bone were discharged. He was about, and even attended school, for more than a year from the time of the attack of hæmoptysis. About Jan. 1, 1877, he began to complain of severe pain in the forehead, with nausea (but no vomiting) and constipation. Jan. 27th he took to his bed, complaining chiefly of pain in the forehead and eyes. Feb. 1st he was drowsy, irritable, and delirious. Feb. 3d incontinence of urine and constant delirium. Up to this time the pulse had not been above 76 in the minute, and on this day it was 64. The next day, Feb. 4th, he was wholly unconscious; pulse 96, pupils dilated. Feb. 5th, left hand in constant motion; pulse 112. From this time the pulse steadily increased in frequency. Feb. 6th he swallowed food, notwithstanding his stupor. Feb. 7th he answered questions; there was oscillation of the eyeballs, and epistaxis from constant picking of the nose. He died Feb. 9th, the pulse being 144 and the respirations 60 in the minute for several hours previous. The temperature never rose above 101.7° F. There was never any vomiting. The duration of the case was thirteen days, in addition to the prodromic period of twenty-seven days.—Autopsy by R. H. Fitz: The pia of the base of the brain from the medulla to the optic thalamus contained a large number of gray miliary tubercles, old and recent, and the same condition was found in the surfaces of the fissure of Sylvius. Ventricles distended with fluid, ependyma thick and translucent. A moderate-sized cavity in the apex of the left lung, with cheesy contents. Both lungs contained an abundance of hard, gray, miliary tubercles. Left kidney contained a wedge-shaped, cheesy mass of the size of a walnut, with numerous tubercles. Left testicle contained a cheesy mass of the size of a walnut; both epididymes were cheesy. The mucous membrane of the bladder contained tubercles near the neck. The vesiculæ seminales contained softened cheesy masses with openings into the urethra. There was a fistulous opening into the right shoulder-joint.
Case II.—Emeline K. L——, 32 years old, single, nurse, had become much exhausted by taking care of a difficult case, and entered Massachusetts General Hospital March 6, 1883, complaining since four days of a little cough, slight expectoration, and chilliness, but no rigor. She seemed hysterical. There was complaint of severe pain in the head, chest, and abdomen. A slight systolic murmur was found at the apex of the heart, and a few moist râles at the base of the chest on both sides behind. The urine was normal. Temperature, 103° F. Three weeks after entrance she began to be delirious, especially at night. April 13th, five weeks and three days after entrance, she was semi-conscious, but would put out her tongue and open her eyes when requested to do so; the abdomen was distended, the pupils were dilated and unequal; there was twitching of the muscles of the right side of the face. Careful examination only disclosed occasional fine râle at the base of right chest. [p. 739] She died April 16th, having been completely unconscious for twenty-four hours. There was no vomiting throughout the case. The temperature was very irregular, ranging between 100° and 103° F., and once as high as 104° F.; it was usually one or two degrees higher at night than in the morning. Pulse, generally from 100 to 110; it rose steadily during the last few days to 160 at the time of death.—Autopsy: Pia mater of brain œdematous, slightly opaque; its lower surface, especially at the base of the brain, showed numerous minute gray tubercles; enlarged cheesy glands at the base of the neck; small, opaque, gray tubercles scattered rather sparsely throughout both lungs. There was also miliary tuberculosis of the liver, spleen, and kidneys.
SYNONYMS.—Dropsy of the brain, Dropsy of the head.
DEFINITION.—A gradual accumulation of serous fluid in the brain, occupying either the ventricles or the cavity of the arachnoid, or both, occurring chiefly in infants or very young children.
The term hydrocephalus, which was applied by the older writers to accumulations of serous fluid both within and also without the cranium, termed distinctively internal and external hydrocephalus, is now restricted to dropsical effusions either between the meninges or within the ventricular cavities. These may be acute or chronic, and they arise from the same conditions which are followed by the effusion of serum in other parts of the body; that is to say, from an alteration in the serous membrane lining a cavity, from an obstruction in the capillary circulation with increased tension in the larger vessels, from an altered condition of the blood, etc.
Chronic hydrocephalus is almost entirely confined to young children, and is probably due to an arrested development of the brain, as shown by its being usually congenital, by the dwarfed intellectual condition of the patient, and by its frequent association with spina bifida. The pathogeny of the disease is, however, still obscure. Whether the abnormal accumulation of serous fluid is to be ascribed to a chronic alteration of the ventricular walls or of the choroid plexuses, allied to inflammation, such as occurs in the pleura, for example, causing an increased secretion, or to a closure of the communication between the ventricles and the spinal cavity, as suggested by the late John Hilton, resulting in dropsy by retention, or to some other cause, is not yet determined. Hilton says:1 “In almost every case of internal hydrocephalus which I have examined after death I found that this cerebro-spinal opening [between the fourth ventricle and the spinal canal] was so completely closed that no cerebro-spinal fluid could escape from the interior of the brain; and, as the fluid was being constantly secreted, it necessarily accumulated there, and the occlusion formed, to my mind, the essential pathological element of internal hydrocephalus.” Sieveking, commenting upon Hilton's theory, says:2 “While giving these facts due weight, it must be pointed out that we are yet far from understanding either how the fluid is poured into the cerebral cavities or how it is removed, and that we do not positively know that the spinal canal has any better means of getting rid of an excess of [p. 741] fluid than the cerebral cavities have.” An arrest of the growth of the brain is supposed by some pathologists to account for ventricular as well as arachnoidal dropsy by the creation of a vacuum in the cavity of the cranium, which is filled by exudation of the more fluid portion of the blood from the vessels or of lymph from the lymphatics.
1 John Hilton, Lectures on Rest and Pain, etc., 2d ed., New York, 1879, p. 22.
2 Jones and Sieveking's Pathological Anatomy, 2d ed., London, 1875, p. 248.
ETIOLOGY.—That chronic hydrocephalus in young children is in a large proportion of cases an hereditary disease is shown by the fact that it is frequently congenital, that more than one child in a family is occasionally affected by it, and that while one child is hydrocephalic others may be idiotic. A scrofulous taint in the family history is noticeable in many cases, the evil effect of which is frequently enhanced by unfavorable sanitary conditions of life, especially by residence in dark, damp, ill-ventilated, and badly-drained apartments and by insufficient or unwholesome food. Hence the disease is more frequently met with among the poor than in the well-to-do classes of society. There is a difference of opinion as to whether it ever arises in consequence of external violence, such as a blow on the head, or of some strong impression, like fright or grief, acting on the mother of the child during pregnancy. The probability is that such causes would not be efficient except in cases where a predisposition to hydrocephalus had already existed. West3 mentions the case of a healthy child five months old who fell out of the arms of her nurse, and was taken with a fit the same day. She apparently recovered, but when a year old had frequent returns of convulsions. At the age of fifteen months the head began to enlarge, and it continued to increase in size until she was three years old, when she was attacked by measles, and died in a few days with convulsions and coma. The symptoms, both bodily and mental, were typical of hydrocephalus, and the diagnosis was fully confirmed by the autopsy.
3 Op. cit., p. 127.
The causes of chronic hydrocephalus in older subjects and in adults are, in addition to the above mentioned, chiefly mechanical. Any lesion which hinders the exit of venous blood from the cranium may be followed by dropsy of the arachnoid cavity or ventricles. The principal ones are tumors of the brain or its membranes, the effusion of lymph in the neighborhood of veins, thrombosis of the cerebral sinuses, compression of numerous small vessels by tubercular granulations, obstructions outside the cranium, including tumors of the neck, aneurisms, obstructive disease of the heart, emphysema and cirrhosis of the lungs, besides diseases giving rise to general dropsy, as the different forms of nephritis, marasmus, the various cachexiæ, etc.
SYMPTOMS.—When the disease is already somewhat advanced before birth, the head is often abnormally large, the cranial bones are separated, the fontanels are distended and fluctuating, and it occasionally happens that delivery of the distended head can only be effected after the fluid has been evacuated by puncture. Even when there is no abnormal increase in the size of the head, indications of cerebral disturbance are sometimes apparent from birth, such as strabismus or convulsions recurring with more or less frequency, along with signs of failure of the general health. In the course of some weeks, or, it may be, months, the attention of the parents is attracted to the prominence of the child's forehead, strongly contrasting with the comparatively diminutive size of [p. 742] the face. Soon an enlargement of the fontanels is perceived, the sutures between the cranial bones become broader, and the head assumes a globular shape from the pressure of the contained fluid. The separation of the bones at the vertex of the skull causes the os frontis to protrude forward, the parietals backward and outward, and the occipital backward and downward. The orbital plates of the frontal bone yield to the pressure of the fluid behind them, and from a horizontal position tend to assume a vertical one, protruding the eyeballs, which have a peculiar downward direction. The sclerotica is visible above the iris, and the latter is partially covered by the lower eyelid. The enlargement of the head is progressive, though not uniformly so, there being pauses of weeks or months during which it is arrested. If it be considerable, the cranial bones are usually thinned, so that the skull becomes translucent when opposite a bright light. When there is a wide separation of the bones there is an unusual development of ossa triquetra in the sutures.
In cases in which the ossification of the cranium is considerably advanced before the beginning of the disease, the enlargement of the head is apt to be correspondingly less. If all the sutures are consolidated, there may be no increase in size, and this is especially true of the mechanical dropsy of adult life. The dropsical effusion, which is then moderate in amount, finds room through compression of the brain-substance, and part of it escapes into the spinal canal.
The size of the hydrocephalic head varies considerably. Where there has been an early arrest of the disease it may be but slightly above the normal. On the other hand, the dimensions are sometimes enormous. In the Warren Museum of Harvard University is a cranium which measures 27½ inches in its greatest circumference, and 20½ inches from one auditory foramen to the other over the top of the head. Its internal capacity is 257 cubic inches. The patient, who died at the age of three years, was never able to sit up and support the head, or even to turn it from the left side, on which she continually lay; she never spoke, and seemed to have no intelligence. The skull of the celebrated James Cardinal measured 32¼ inches in its largest circumference.4 Even more remarkable instances are on record. The dimensions of the fontanels, particularly the anterior, usually correspond with those of the skull in general. During any strong muscular effort on the part of the patient the membrane covering them is seen to be bulged out by pressure from the fluid beneath. The enlargement is not always uniform; it may be in part or wholly confined to one side, owing to consolidation of the sutures of the opposite side, or because only one of the lateral ventricles is affected. The scalp is traversed by numerous distended veins. The hair is very scanty. The head has a soft, fluctuating feel, and the walls sometimes seem to crackle beneath the fingers, like parchment.
4 Reports of Medical Cases, etc., by Richard Bright, M.D., London, 1831, vol. i. p. 431.
In cases of moderate severity there may be few or no symptoms of active cerebral disturbance, such as convulsions or paralysis, but the child does not learn to talk, to walk, or to control the sphincters even at the age of three or four years, and the signs of imperfect mental development are evident. He is apt to be irritable or mischievous, and even when not actually idiotic is very backward in evincing signs of intelligence. There are, however, not a few exceptions to this, and some [p. 743] children with large hydrocephalic heads are intelligent and amiable. The cranium of a girl who died at the age of sixteen years is preserved in the Warren Museum. It measures 24¼ inches in circumference and 17¼ inches from one auditory meatus to the other over the vertex, and the bone is in no place more than one-eighth of an inch in thickness. The child was an inmate of a house of industry, where she was instructed in the usual branches of knowledge taught in our common schools, until at length, such was her capacity, she was entrusted with the teaching of the other pauper children, and she had an excellent character for intelligence and moral worth. She died of phthisis. On post-mortem examination “the brain was found floating, as it were, in a large collection of water.” As in other chronic diseases, there are often pauses, from time to time, of variable duration, in which there is some improvement in the condition of the patient, as well as a temporary arrest in the enlargement of the head. The growth of the child in stature is often retarded, and when life is prolonged the individual is more or less dwarfed. In some cases there is a considerable increase in the amount of adipose tissue, and the appetite is often voracious. L. Fürst reports5 the case of a hydrocephalic girl, sixteen years old, whose height (or, rather, length, for she was unable to stand) was 81 centimeters (nearly 32 inches), corresponding to the stature of a child between three and four years old. The periphery of the head measured 511/5 centimeters (20¼ inches). The anterior fontanel was still open. The age was verified by reference to the registry of birth at the police-office.
5 “Exquisite Wachsthumshemmung bei Hydrocephalus chronicus,” von Dr. Livius Fürst, Virchow's Archiv, June, 1884.
The symptoms of cerebral disturbance in chronic hydrocephalus are much less striking than one would expect, doubtless because the increase of pressure upon the brain is so gradual. Actual paralysis, especially of the limbs, is rare, but convulsions are not infrequent, as is the spasmodic constriction of the glottis known as laryngismus stridulus or spasmodic croup. A general state of uneasiness and restlessness is common. Vision is often impaired and sometimes wholly lost. Strabismus is frequently present, or there may be an involuntary rolling movement of the eyeballs. The pupils are often dilated and insensible to light. In consequence of the increased weight of the head, the child is unable to support it, and in most cases is compelled to keep the bed. Vomiting is common. The digestive functions are disturbed. Constipation is an almost constant symptom, and the sphincters are relaxed in the advanced stages of the disease. Although in some cases, as already stated, the child may grow fat, the reverse of this is the rule; there is usually progressive emaciation, especially of the lower extremities.
The duration of the disease varies much in different cases. The earlier the characteristic symptoms manifest themselves the more rapid is its course. Most children born hydrocephalic survive but a few days or weeks. In cases which are more slow in their development the patient may live some years, and in rare instances attain adult life. But his feeble vitality usually makes him an easy prey to the ordinary complaints of childhood, and a large proportion of cases succumb to inflammation of the lungs or of other organs, to diarrhœa, whooping cough, or the eruptive diseases. Most of those who escape these intercurrent maladies [p. 744] perish from defective nutrition, the result of malassimilation of food, or else are cut off by acute cerebral inflammation, with convulsions, etc.
PATHOLOGICAL ANATOMY.—It is rarely that a large amount of serum is found in the cavity of the arachnoid unless a free communication has been established between it and the ventricles by the destruction of cerebral tissue. In the pia the quantity may be more abundant than normal, filling the subarachnoid spaces, separating the convolutions from each other, and occasionally forming little sac-like elevations on the surface of the membrane; but it should be borne in mind that a certain amount of serous infiltration of the tissue of the pia is by no means rare in cases of death from various diseases, owing to the obstruction to the circulation during the last hours of life, and should not be considered pathological unless it exceed the usual limits. The amount of effusion into the ventricles varies between very wide limits, from some ounces to two or three pints. It may be transparent, or turbid from particles of cerebral tissue or epithelial or pus-cells, and is occasionally slightly tinged with blood. Its specific gravity is nearly identical with that of water, and it contains a trace of albumen. The effusion usually occupies the two lateral and the middle ventricles. Less frequently the dropsy is unilateral, in consequence, apparently, of an obliteration of the foramen of Monro. The tissues composing the walls of the ventricles are compressed and hardened. The ependyma of the walls and of the plexus is thickened and roughened by the formation of minute elevations, which the microscope shows to be composed of proliferated and sclerosed connective tissue. The brain in cases of large effusion is reduced to a membranous sac, flattened, with hardly any trace of its original structure at first sight apparent. In the case of James Cardinal, before alluded to, Bright says, “The brain lay at its base [of the skull] with its hemispheres opened outward like the leaves of a book.” Closer inspection shows that all the parts are present, although atrophied by pressure. The convolutions are flattened and the brain-substance is pale and softened. The cranial nerves are often softened and flattened.
In the dropsy of the head in adults which is the result of mechanical pressure or of cachexia the appearances are widely different. The effusion may occupy the cavity of the arachnoid, and even the space between the dura and the skull, as well as the ventricles. The amount of fluid is much less than in the chronic hydrocephalus of children. The ventricular walls present no signs of inflammatory changes.
DIAGNOSIS.—Chronic hydrocephalus is usually recognized without difficulty. The chief points of diagnostic importance are the progressive enlargement of the head, the separation of the cranial bones, with their peculiar change of position, as already described, and the evident signs of arrested intellectual development. If the head be but little enlarged, the case might be mistaken for that of chronic hypertrophy of the brain, but this is a very rare disease, and is not accompanied with defective mental development.
PROGNOSIS.—The elements of prognosis include the size of the head at birth, its rate of enlargement, the general condition of the child, both physically and intellectually, his hereditary antecedents, and the hygienic influences to which he may be subjected. A large proportion of children born hydrocephalic live but a short time; a few survive one or more [p. 745] years. The number of those who reach adult life is extremely small. The favorable indications are a tardy appearance of the dropsy and its slow progress, without marked evidence of defective mental and bodily development.
TREATMENT.—The treatment of chronic hydrocephalus is general and local, the first being the most important, although in many cases it is difficult to enforce it, from lack of intelligence and of means on the part of those in charge of the patient. Proper ventilation, good drainage, and cleanliness are essential. The child should be bathed daily, and should be protected against changes in temperature by suitable clothing. If his strength allow, he should be taken into the open air daily in fine weather. A wet-nurse should be provided for infants whose mothers are unable to suckle them. Older patients should take milk, cream, animal broths, farinaceous substances, etc., with wine or brandy. Tonics, especially cod-liver oil, hypophosphite of lime, and some preparation of iron or of the iodide of iron, are important, the choice being determined by the effect apparently produced. The internal and external employment of mercurial preparations, once in vogue, is now almost entirely abandoned by the best authorities. The evacuation of the fluid by puncture, followed by compression of the head by bandaging, has been occasionally resorted to, and in a few instances with success, but the cases in which it is indicated are rare. Thomas Young Thompson6 reports a case in which puncture was followed by recovery. The child, fourteen days old, fell, apparently without ill effects, but three weeks afterward a protuberance appeared on the crown of the head which continued to enlarge, and the signs of chronic hydrocephalus were unmistakable. In three months the circumference over the parietal eminences measured 20 inches, and a year afterward 24½ inches. In spite of energetic internal and external treatment the enlargement continued to progress, until the head was punctured, and about three hundred grammes of a clear, transparent fluid, free from albumen, were evacuated. Five weeks later a second puncture was made, and sixty grammes of a milky fluid withdrawn. The child recovered, and two years later was in good health, the head not being disproportioned to the rest of the body. West considers the cases in which the effusion is apparently external—that is, confined to the arachnoid cavity, rather than ventricular, and in which there are no indications of active cerebral disease—to be the most favorable for the operation. The proper situation for the puncture is the coronal suture, about an inch or an inch and a half from the anterior fontanel. A few ounces of fluid only should be withdrawn at a time, and compression should be carefully applied both during the escape of the fluid and afterward.
6 Med.-Chir. Transactions, vol. xlvii., 1864.
The blood-vessels of the spinal membranes communicate freely with the general circulation, and there is less opportunity for their obstruction than in the case of the meninges of the brain. Hyperæmia of the dura and pia mater is therefore seldom met with, except in connection with disease of the cord; and, indeed, but little is known on the subject, which is only alluded to as possible by authorities of the present day, although the affection was formerly supposed to be a common one, giving rise to various symptoms, such as numbness and formication of the extremities, muscular weakness, and even paraplegia—symptoms which are now known to be caused by structural diseases of the cord only. As Erb1 remarks, “It is hardly possible that any considerable hyperæmia of the meninges should exist without a similar condition existing in the cord also, as the vascular supply of both is the same.”
1 “Krankheiten des Rückenmarks,” von Wilhelm Erb, in Ziemssen's Handbuch, Leipzig, 1876; Am. trans., vol. xiii. p. 99.
ETIOLOGY.—Hyperæmia of the spinal membranes is found after death from convulsions, especially in cases of tetanus, hydrophobia, eclampsia, strangulation, poisoning from narcotics, etc., in which the effect is evidently due to asphyxia. An interesting case of extensive hyperæmia of the spinal membranes, as well as of those of the brain, complicating mania, is reported by M. R. G. Fronmüller.2 A girl of eighteen years, previously well, being accused of theft, fell into a state of melancholia, passing into mania, with frequent convulsions, screaming, etc. There was no spinal tenderness. The urine contained no albumen. The temperature was never elevated. No opisthotonos. The sphincters became relaxed, and she died at the end of about three weeks. The dura was found to be normal, but the pia mater of the brain, cerebellum, medulla oblongata, and cord was strongly injected. The brain and cord were normal; no ventricular effusion. Here the meningeal hyperæmia was doubtless caused by asphyxia resulting from the convulsions.
2 See Schmidt's Jahrbücher, 1883, No. 7.
Congestion of the spinal membranes has been attributed to sudden suppression of the menstrual flow or of hemorrhoidal bleeding, and to portal obstruction, but the evidence of this is very meagre. Exposure [p. 747] to cold and wet, as from sleeping on the damp ground, is an alleged and plausible cause.
The SYMPTOMS attributed to hyperæmia of the spinal membranes are pain in the back extending to the legs, with numbness and tingling of the toes, sensation of weight in the limbs, muscular weakness, appearing suddenly without fever and usually of transient duration. There is no evidence that it gives rise to paralysis. Considering that temporary congestion of the membranes must occasionally happen from convulsions, as in epilepsy, etc., it is remarkable that no symptoms attributable to it have been observed under these circumstances.3
3 See Epilepsy and other Chronic Convulsive Diseases, etc., by W. R. Gowers, M.D., London, 1881, p. 106.
MORBID ANATOMY.—We must be careful not to mistake post-mortem staining of the tissues from imbibition of the coloring matter of the blood—the result of decomposition aided by the position of the body—for true congestion. The latter is recognized by fine vascular arborization covering the surface of the dura or pia, often accompanied with small punctate hemorrhages. More extensive extravasations in the connective tissue, surrounding and between the membranes, are sometimes found. The spinal fluid is usually increased in amount, and often tinged with red. On account of the free vascular connection between the membranes and the cord the latter almost always partakes of the congestion.
DIAGNOSIS.—From what has been said it follows that simple hyperæmia of the spinal membranes can hardly be distinguished from that of the cord. (See the article on DISEASES OF THE SUBSTANCE OF THE BRAIN AND SPINAL CORD.) When the symptoms are unaccompanied by fever, are of very moderate severity, and of short duration, we may perhaps infer that the lesion is confined to the membranes.
The TREATMENT is the same as that for congestion of the spinal cord.
SYNONYM.—Acute spinal pachymeningitis.
Acute inflammation of the spinal dura mater is chiefly confined to the outer surface of the membrane (peripachymeningitis), and is almost always consecutive to either injury or disease of the vertebræ (fracture, dislocation, caries), to wounds penetrating the spinal cavity, or to suppurative disease in neighboring organs or tissues, which makes its way into the peridural space through the intervertebral openings. The symptoms are complex—in part caused by the original disease, and in part by the pressure of the products of inflammation exercised upon the nerve-roots, and even upon the cord itself. Pain in the back, corresponding to the seat of the disease, is rarely absent, and all movements of the trunk are extremely painful. When the exudation is sufficient to compress the nerve-roots, the pain will extend to the trunk and the limbs, and other signs of irritation, such as a feeling of constriction by a tight girdle, and tingling, numbness, and cutaneous hyperæsthesia in the limbs, will be observed, varying in situation according to the seat of the lesion. In some cases the compression of the cord may be sufficient to cause paraplegia. General symptoms will vary according to the complications of the [p. 748] case. Severe injury or extensive disease of the vertebræ will be accompanied with high fever; but if the external inflammation be moderate and the meningeal complication be limited in extent, the fever may be subacute.
MORBID ANATOMY.—The connective tissue between the dura and the bone is the seat of inflammatory exudation, usually purulent, of greater or less extent, and more abundant in the posterior than the anterior part of the spinal cavity, owing to the position of the patient. A more or less abundant exudation, either of pus or of dry caseous matter, is found upon the outer surface of the dura or infiltrating the connective tissue between it and the bony walls. The dura is thickened, and sometimes the exudation is seen upon its inner walls, but the pia is seldom involved in the inflammation. The cord may be compressed or flattened when the amount of exudation is large, and may in consequence show signs of inflammation in its vicinity. The spinal nerves likewise are sometimes compressed, atrophied, softened, and inflamed. The disease rarely occupies the cervical region, on account of the close union of the dura with the bones of that part; hence there is an absence of pain in the neck and of retraction of the head.
DIAGNOSIS.—The diagnosis is founded on the presence of general symptoms of spinal disease—pain in the back, but not extending to the neck, increased by movements of the trunk; cutaneous hyperæsthesia, tingling, or numbness in various parts of the surface of the body; paresis or paralysis of the lower extremities in severe cases; along with a history of vertebral disease or injury or of suppurative disease in the neighborhood of the spine. The history of the case will generally be sufficient to exclude myelitis, tetanus, or muscular pain (rheumatism, lumbago). From acute leptomeningitis the diagnosis must also be made by the history, but it should be borne in mind that the pia may be involved at the same time with the dura.
PROGNOSIS.—In complicated cases the prognosis is grave if the spinal symptoms are well marked and severe, especially when there is evidence of much pressure on the cord (paraplegia). If the signs of spinal irritation were moderate, the danger would depend upon the nature and extent of the external lesion.
TREATMENT.—This would be addressed mainly to the primitive disease. For the spinal symptoms the treatment would not differ materially from that of inflammation of the spinal pia mater.
This affection generally coexists with chronic inflammation of the pia. Like the acute inflammation of the dura, it is seen in connection with disease or injury of the vertebræ, and it may also arise from tumors of the membrane (chiefly syphilitic) and from myelitis. It is frequent among the chronic insane, and in them is sometimes associated with hemorrhagic effusions analogous to the hæmatoma of the cerebral dura mater. Chronic inflammation of the spinal dura is of unfrequent occurrence, and but little is known of its history and pathology. In a case reported by Wilks4 the membrane was thickened to nearly its whole [p. 749] extent, and in the cervical region presented numerous bony plates. The pia was also thickened at this part and adhered closely to the dura. The symptoms, which seemed chiefly due to disease of the cord from compression, were retraction of the lower limbs and violent jerking from excessive reflex action.
4 Transactions of the Pathological Society of London, vol. vii., 1856.
A special form of the disease, occupying chiefly the cervical region, was first described by Charcot.5 The membrane is thickened by a deposit of successive layers of fibrin, compressing the cord, which is flattened from before backward and inflamed. The nerve-roots are also more or less compressed. The course of the disease may be divided into two stages: First, that of irritation of the spinal nerves, with pain in the back part of the neck, extending to the head and along the upper limbs. The pain is permanent, but liable to exacerbations, and is accompanied with stiffness of the neck and a feeling of numbness and tingling, with muscular weakness of the arms. Sometimes the skin of the arms is the seat of trophic changes, as shown by the presence of bullæ or pemphigus. The second period is that of extension of the disease to the cord. The pain ceases, and is followed by paralysis or muscular atrophy, especially in the domain of the ulnar and median nerves, resulting in extension of the hand on the forearm, with flexion of the fingers toward the palm, giving rise to a claw-like appearance (main en griffe). In some cases an upward extension of the disease implicates the root of the radial nerve, and the hand then assumes a prone position from paralysis of the extensor muscles. The lower portion of the cord may also become involved, with similar results in the lower extremities. Although the disease is generally progressive, it is not always so, and Charcot cites one case in which great improvement took place in the course of some years, though not apparently in consequence of any special treatment.
5 Leçons sur les Mal. du Syst. nerv., par J. M. Charcot, Paris, 1875, vol. ii. p. 246. See, also, Maladies du Syst. nerv., par A. Vulpian, Paris, 1879, p. 127; and Clinique méd. de l'Hôpital de la Charité, by the same.
SYNONYM.—Leptomeningitis spinalis acuta.
By the term spinal meningitis is usually meant inflammation of both the arachnoid and the pia, the two being, as already stated, in reality one membrane. In connection with meningitis of the brain it constitutes a distinct disease which is usually epidemic, and probably zymotic in its origin. (See EPIDEMIC CEREBRO-SPINAL MENINGITIS.) Sporadic spinal meningitis is a rare disease. It may be acute or chronic.
ETIOLOGY.—Among the causes of acute spinal meningitis are injuries to the vertebral column, such as fracture and dislocation from falls, blows, etc.; wounds by stabbing or shooting; violent bodily effort, as in lifting heavy weights, etc. Other causes are local exposure to wet and cold, as from sleeping on the wet ground or standing long in water while at work. Like cerebral meningitis, it may complicate constitutional diseases, as rheumatism, pyæmia, etc., but less frequently than the former. Syphilitic inflammation of the spinal membranes is, however, not unfrequently met with, but chiefly of the chronic form. (See the article on SYPHILIS [p. 750] OF THE BRAIN AND SPINAL CORD.) In tubercular meningitis of the brain the pia mater of the cord is often implicated in the disease. Acute spinal meningitis is most frequently met with in young persons, and is more common in men than in women.
SYMPTOMS.—The onset of the disease is generally sudden, and it is rarely preceded by the usual inflammatory symptoms of chilly sensations, restlessness, headache, etc. A sharp rigor is the first indication of disease in most cases. This is followed by fever, with high temperature and a quick, full, hard pulse. Pain in the back follows, either confined to a limited region or extending throughout the whole extent of the spine, soon becoming acute, and aggravated by any movement of the trunk or even of the limbs. There is usually but little tenderness on pressure upon the spinous processes, and often none at all. The pain extends around the body and throughout the limbs. In the course of a few hours muscular contraction in the region of the back, and also of the limbs, is observed. When the disease is situated in the cervical region, the head is drawn backward, and cannot be moved without severe pain. If it occupies a considerable extent of the spine, the dorsal muscles become rigidly contracted and the body is arched forward (opisthotonos), as in tetanus, so that the patient may even rest upon his occiput and sacrum. Owing to the implication of the muscles of respiration, more or less dyspnœa is common, and may even cause death by asphyxia. There is no paralysis of the limbs, unless there be complication of myelitis, but the patient abstains as far as possible from any movement from dread of pain. Reflex irritability is exaggerated. Retention of urine and constipation are common, probably for the same reason. Hyperæsthesia of the surface of the body in limited areas is sometimes noticed, owing to the irritation of the posterior spinal roots. Provided the extent of the inflammation be comparatively limited, recovery is possible, though rare, at this stage of the disease.
When the course of the disease is unfavorable, symptoms of paralysis appear, from compression of the cord by the products of inflammation. The hyperæsthesia of the skin gives place to insensibility; the muscles lose their reflex function and their reaction to electricity; the bladder and rectum become paralyzed. The invasion of the medulla by the disease, which is announced by paralysis of the muscles of the œsophagus and of the tongue, is a fatal complication. The pulse and the respiration become rapid and irregular from compression of the vagus, the temperature rises to 106° or 108° F., and death ensues through asphyxia or failure of the heart.
The course of acute spinal meningitis is rapid. It sometimes terminates fatally within two or three days, and the average duration of fatal cases is about a week, but exceptionally the disease may last for several weeks or even months. Even then complete recovery may take place, though permanent effects are usually left behind, such as paresis or paralysis of the lower extremities, muscular contractions, muscular atrophy, etc., from injury to the nerve-roots or the cord.
The mind is generally clear in the early stage; afterward there may be delirium, especially along with cerebral complication.
MORBID ANATOMY.—It is rarely that the pia mater is the only tissue involved in the inflammation. Frequently the inner surface of the dura [p. 751] is the seat of a fine injection, with delicate false membranes, and the cord itself—at least its exterior portions—probably always participates more or less in the congestion. The pia is reddened and thickened, the surface showing small bloody extravasations, and the space between its two layers is the seat of a fibro-purulent deposit. The spinal fluid is turbid and flocculent. The seat and extent of the morbid appearances vary in different cases; they are always more abundant in the posterior than the anterior part of the cord, and may be confined to a limited space or extend throughout its whole length. It is remarkable that the region of the medulla oblongata is generally free or only slightly affected; but since bulbar symptoms are often prominent in grave cases, Leyden6 accounts for it by supposing that the exudation is washed away by the constant movement of the cerebro-spinal fluid. If the cord be involved in the inflammation, it is softened and injected, the nerve-sheaths are destroyed, and the axis-cylinders swollen in places. The nerve-roots show hyperæmia, infiltration of the interstitial tissue with round cells, and destruction of the nerve-sheaths.
6 Klinik der Rückenmarks-krankheiten, von E. Leyden, Berlin, 1874, vol. i. p. 407.
DIAGNOSIS.—Spinal meningitis is easily recognized in most cases by its sudden onset and the severity of its symptoms. The distinguishing symptoms are sudden and acute pain in the back, extending around the body and into the limbs, which is increased by every movement of the trunk, rigidity of the back, hyperæsthesia of the skin, retraction of the head, with difficulty of breathing and of swallowing. The diseases from which it must be distinguished are muscular rheumatism (so called), tetanus, and myelitis. In rheumatism of the dorsal muscles the pain is confined to the back, does not extend to the limbs, and is only excited by movement. The fever is moderate or absent; there are no symptoms of spinal complication, such as cutaneous hyperæsthesia, retraction of the head, paresis of the limbs, etc.; and the result is uniformly favorable. Tetanus is almost always due to some well-marked traumatic cause; the muscles of the jaw are usually first implicated (trismus); and the attacks of general muscular spasm are easily excited by peripheral irritation. Myelitis can be distinguished by the absence of pain in the limbs and by paraplegia, but it must be borne in mind that myelitis and spinal meningitis may coexist.
PROGNOSIS.—Acute spinal meningitis is always a grave disease, hence a guarded opinion should be given even in apparently favorable cases. General mildness of the symptoms, with no indication of extension to the medulla oblongata, would afford ground for encouragement. The unfavorable symptoms are those showing compression or inflammation of the cord, such as paresis, paralysis, twitching of the limbs, muscular contractions, cutaneous anæsthesia, etc. The extension of the disease to the medulla, as shown by difficulty of swallowing, speaking, or breathing, is almost necessarily fatal.
TREATMENT.—During the first stage of the disease an effort should be made to reduce the hyperæmia of the membranes by the local abstraction of blood. This is best effected by cupping along each side of the spine and by the application of leeches to the anus; the bleeding should be promoted by poultices. Free purging is likely to be of service, and is best obtained by means of ten grains each of calomel and jalap (for an [p. 752] adult), followed by saline laxatives. Counter-irritation to the back may be induced by the application of blisters or by painting the skin with a strong tincture of iodine (one or two drachms of iodine to an ounce of sulphuric ether). After the effusion of lymph and pus, as shown by symptoms of compression of the nerve-roots and cord, absorbents should be tried, of which the iodide of potassium, in doses of five to ten grains, four times daily, is most likely to be of benefit. Pain must be relieved by opium or morphia and chloral hydrate. The latter, either alone or combined with hyoscyamus and bromide of potassium, will be useful to allay spasmodic twitching, opisthotonos, or muscular contraction. The patient should be enjoined to lie on each side alternately, or on the face if possible, in order to equalize the hyperæmia of the membranes and cord. Liquid nourishment must be freely administered, such as milk, broths, gruel, etc., together with wine and other stimulants in case of exhaustion and threatening of collapse. During convalescence the patient should be carefully protected against cold and fatigue, and the strength must be supported by quinine and iron with suitable diet.
SYNONYMS.—Chronic inflammation of the pia mater of the spinal cord, Chronic spinal leptomeningitis.
Chronic spinal meningitis may follow the acute form, or it may arise from chronic disease of the vertebræ or of the cord, especially myelitis and sclerosis. It is most apt to accompany sclerosis of the posterior columns, and it is often difficult to say in any particular case whether the meningeal affection preceded or followed that of the cord. Probably some cases of chronic myelitis, especially of the disseminated form, owe their origin to chronic meningitis.7 It has been thought to follow blows on the back, and also to arise from general concussion without traumatism, and has been considered as a frequent result of accidents from railroad collisions, etc. This view has been disputed by Herbert W. Page,8 who says: “Of the exceeding rarity of spinal meningitis as an immediate result of localized injury to the vertebral column we are well assured.... And we know of no one case, either in our own experience or in the experience of others, in which meningeal inflammation has been indisputably caused by injury to some part of the body remote from the vertebral column.” Chronic alcoholism and syphilis, especially the latter, predispose to the disease. In many cases no adequate cause can be assigned.
7 Leyden, op. cit., vol. i. p. 442.
8 Injuries of the Spine and Spinal Cord, without Apparent Mechanical Lesion and Nervous Shock, in their Medico-legal Aspects, London, 1883, p. 128.
SYMPTOMS.—Gowers9 remarks that a large number of symptoms formerly assigned to chronic spinal meningitis have nothing to do with that pathological state, but are now known to be owing to alterations within the cord which are frequently associated with it. The symptoms which are really due to the meningeal inflammation—namely, those [p. 753] arising from interference with the nerve-roots in their passage through the thickened membranes—do not differ essentially from those of chronic pachymeningitis of the spine; the principal are pain in the back, especially on movement, extending to the trunk and limbs, hyperæsthesia of the skin in various regions within the domain of the irritated sensory roots, with diminution or loss of the knee-jerk, and areas of anæsthesia due to their more complete compression. The compression of the motor roots gives rise to symptoms which are similar to those of disease of the anterior cornua, consisting chiefly of muscular wasting, with impairment of motion in corresponding regions, without fever.
9 The Diagnosis and Diseases of the Spinal Cord, by W. R. Gowers, M.D., 2d ed., Philada., 1881, p. 73.
The anatomical appearances, which are most pronounced in the posterior aspect of the cord, and diminish from below upward, are often of considerable extent. The membrane is thickened, opaque, and often adherent to the cord. On the inner surface are seen numerous small bodies composed of proliferating connective tissue.10 These, according to Vulpian, are chiefly found in the lower dorsal and lumbar region and on the cauda equina. The dura is very frequently involved in the inflammation; it is thickened, and its inner surface is adherent to the pia, often showing numerous miliary bodies similar to those found in the pia.
10 Leyden, op. cit., vol. i. p. 144; A. Vulpian, Mal. du Syst. nerv., Paris, 1879, p. 126.
DIAGNOSIS.—Chronic spinal meningitis so rarely exists apart from disease of the dura or of the cord that its separate diagnosis must be mainly a matter of conjecture. Leyden justly says we must usually be content to diagnosticate chronic meningitis without attempting any further distinction, except in cases which originate in disease of the vertebræ or of their neighborhood, and afterward penetrate into the spinal canal, and which would probably give rise to pachymeningitis. The diseases with which chronic meningitis of the spine is most likely to be confounded are posterior sclerosis (locomotor ataxia) and chronic degeneration of the anterior cornua (progressive muscular atrophy).11 From the former it is distinguished by the absence of ataxia; from the latter, by the irregular distribution of the symptoms; and from both, by the existence of limited areas of anæsthesia and of extensive spinal pain. It must be remembered that inflammation of the cord complicating that of the meninges, or pressure upon the cord by the thickened membranes may give rise to mixed symptoms. The latter is especially observed in syphilitic cases.
11 Gowers, op. cit., p. 74.
PROGNOSIS.—Simple chronic spinal meningitis is rarely if ever fatal. How far it is capable of amelioration or of cure is not, in the present state of our knowledge, known. When complicated with disease of the cord the prognosis will depend upon that of the latter. Syphilitic chronic meningitis is to a certain extent amenable to appropriate medication.
TREATMENT.—The treatment should have for its object (1st) to relieve pain; (2d) to arrest the progress of the inflammation, and especially to prevent it from extending to the cord; (3d) to promote the absorption of the exudation. For the first object the internal or hypodermic employment of morphia should be combined with external applications, such as fomentations, liniments, ice, etc. Counter-irritation by means of dry cupping, blisters, iodine, etc., with leeches, shampooing, and douches of hot water, may be of some use in retarding the progress of the [p. 754] inflammation, and should be aided by the administration of mercurials and the preparations of iodine. The biniodide of mercury would be useful for this purpose in the dose of one-sixteenth to one-eighth of a grain three times daily, its effect being carefully watched in order to prevent salivation. The same means will also aid in favoring the absorption of lymph. In syphilitic cases an appropriate specific treatment is indicated.
SYNONYMS.—Spinal meningeal apoplexy, Hæmatorrhachis.
Spinal meningeal hemorrhage may take place between the dura mater and the walls of the vertebral canal, or between the dura and the pia mater—i.e. into the arachnoid space.
ETIOLOGY.—Penetrating wounds, injuries to the vertebræ, fractures and dislocations, and violent blows are apt to give rise to more or less hemorrhage into the spinal canal. Violent convulsions, as in tetanus, epilepsy, uræmic eclampsia, hydrophobia, may be followed by meningeal hemorrhage, owing to the disturbance of the circulation from asphyxia; and excessive muscular effort, as in lifting heavy weights, etc., has been said to cause it. In cerebral meningeal hemorrhage and in effusion into the substance of the brain the blood sometimes escapes into the spinal canal. An aneurism of the aorta has been known to communicate with the canal; such a case was reported by Laennec.12 In certain diseases with hemorrhagic tendency, as purpura and scurvy, spinal extravasation is occasionally observed.13
12 Traité d'Auscultation médiate, 4th ed., Paris, 1837, vol. iii. p. 443.
13 A case of scorbutic spinal hemorrhage is reported in the British Med. Journal, Nov. 19, 1881.
SYMPTOMS.—These vary according to the conditions under which the hemorrhage is produced and to the amount of bleeding. In traumatic cases the signs of hemorrhage are often completely overshadowed by those of the injury of the vertebræ, the membranes, or the cord, and are undistinguishable. When a large amount of blood is suddenly introduced into the spinal canal, it usually gives rise, by pressure on the cord, to paraplegia, which, however, is sometimes of only short duration. Thus in Laennec's case the bursting of an aneurism into the spinal cavity was signalized by a sudden paraplegia, but in half an hour the power of movement returned, though sensation did not. The patient died in a few hours from hemorrhage into the left pleural cavity. The amount of blood in the spinal cavity is not stated, and, in fact, it would appear that the spine was not opened. When the amount of blood is smaller the symptoms indicate irritation of the spinal nerves and of the cord. Pain in the back is always present, extending into the limbs, and is sometimes severe. Its seat corresponds to that of the effusion. There may be a feeling of tingling and numbness in the lower extremities, with anæsthesia or hyperæsthesia of the skin and more or less paresis. A feeling of constriction around the waist or the chest is sometimes complained of. In slight effusions the symptoms may be limited to numbness and formication of the extremities, with slight paresis. There is rarely fever in the early stages, unless the amount of blood is [p. 755] sufficient to give rise to inflammatory conditions of the cord or membranes. If the extravasation be moderate it is generally absorbed, with relief to the symptoms, although slight numbness and paresis of the extremities may continue for a long time.
PATHOLOGICAL ANATOMY.—In hemorrhage outside the dura the loose cellular tissue between the membrane and the bony canal contains more or less coagulated blood according to the circumstances of the case, especially in the posterior region of the canal and covering the nerve-roots. The dura is reddened by imbibition of the coloring matter of the blood. When the amount of the effusion is large, as in traumatic and aneurismal cases, or where cerebral hemorrhage has extended into the spine, the cord may be compressed by it. Hemorrhage into the arachnoid sac, except in cases of violence, etc., is usually of limited amount, sometimes only in the form of drops of blood upon the surface of the dura or pia. When more abundant it may surround the cord more or less completely, but in most cases it is limited in longitudinal extent, being confined to the space of one or two vertebræ. The cord may be more or less compressed, reddened, and softened. In all cases the spinal fluid is discolored and reddened in proportion to the amount of the hemorrhage.
DIAGNOSIS.—When the complications are such that symptoms attributable to hemorrhage are not observed, the diagnosis of spinal hemorrhage is impossible. This may happen in the case of wounds and injuries of the vertebræ and of the passage into the spinal canal of blood from an apoplectic effusion of the brain. In the convulsions of tetanus, epilepsy, etc. the amount of the hemorrhage is rarely sufficient to give rise to distinctive symptoms. In idiopathic and uncomplicated cases the chief diagnostic marks are suddenness of the attack; pain in the back, usually at the lowest part; disturbances of sensation in the extremities (anæsthesia, formication, etc.); paresis or paralysis of the legs; the absence of cerebral or spinal inflammatory symptoms; and, in many cases, the favorable course of the disease. Sometimes an ostensible cause, such as scurvy, purpura, suppressed menstruation, or hemorrhoidal flux, will aid in the diagnosis. The disease for which spinal hemorrhage is most likely to be mistaken is acute myelitis, but this is not sudden in its onset, is accompanied with fever, and gives rise to paralysis both of motion and sensation, and to loss of control over the sphincters, to bed-sores, etc. Hemorrhage of the cord would be accompanied by paraplegia and loss of sensation in the lower extremities and slight tendency to spasmodic manifestations; it is fatal in the majority of cases, or else is followed by permanent paralysis. Hysteria might be confounded with spinal hemorrhage, but the history of the case and the transient duration of the symptoms would clear up all obscurity.
PROGNOSIS.—In traumatic cases the hemorrhage is usually only one element in the gravity of the situation, which depends chiefly upon the character and extent of the original injury. In idiopathic and uncomplicated cases the prognosis, which must always be doubtful, will vary according to the severity of the symptoms as corresponding to the amount of the effusion. The danger is greatest during the first few days; if there should then be diminution of the more important symptoms, an encouraging opinion may be given. The immediate effects may, however, be [p. 756] less grave than the remote, such as bed-sores, cystitis, etc. Except in the very mildest cases the patient is likely to be confined to bed for several weeks. In more severe ones the convalescence may be very protracted, and permanent lameness, etc. may result.
TREATMENT.—In the early stage absolute rest in bed, with cold applications to the back and moderate purging, should be employed. Large doses of ergot are recommended, but there is little evidence of benefit from this medicine. In traumatic cases no rules for treatment of the hemorrhage can be laid down. If the extravasation evidently depends upon a constitutional diathesis, as in purpura, scurvy, etc., the remedies appropriate for these diseases should be employed, especially tonics and astringents, such as the tincture of the chloride of iron, in doses of from fifteen to thirty drops three times daily, quinine, and the vegetable acids. Should there be evidence of blood-pressure from suppressed discharge, as in amenorrhœa, arrested hemorrhoidal flow, etc., leeches should be applied to the anus, and blood may be taken from the region of the spine by cupping. In the later stages an attempt may be made to aid the absorption of the effused blood by the administration of the iodide of potassium or the protiodide of mercury, and by the application of blisters or strong tincture of iodine to each side of the spine. Pain must be relieved and sleep obtained, when necessary, by means of opium, chloral hydrate, or other anodynes. Electricity, rubbing, bathing, etc. will be useful for combating the paralytic symptoms which may remain after the disease itself is relieved.
DEFINITION.—By the term spina bifida is meant a congenital malformation of the vertebral column, consisting in the absence of a part—commonly the spinous processes and laminæ—of one or more of the vertebræ, and thus permitting a protrusion of the spinal meninges, which, with their contents, form a tumor of variable size and shape, usually in the lumbo-sacral region.
SYNONYMS, ETC.—Of the various names which have been proposed for this affection, most are objectionable, as not expressing with sufficient definiteness what is meant. Thus, hydrorachis (the term generally employed by French writers), hydrorachitis, spinal hydrocele, etc., convey merely the notion of an accumulation of fluid within the spinal canal, and are as applicable to simple serous effusions in that part, whether occurring as a complication of hydrocephalus or as the result of injury, as to the special affection under consideration. Again, myelochysis—pouring out or protrusion of the spinal marrow—would imply that the cord itself was necessarily involved in the tumor, which is certainly not always the case. The terms schistorachis (cleft spine) and atelorachidia (defective spine—a name suggested by Béclard) would be preferable, and are really more accurate than the name spina bifida, since, as a matter of fact, the spinous processes are, as a rule, not bifid, but totally deficient. The latter term, however, has the advantage of being more familiar, and may be retained simply as a matter of convenience. It is said by Itard to have been first employed by the Arabian physicians.
HISTORY.—Spina bifida does not appear to have been known to the ancients, the earliest recorded observations of the affection being found in the writings of Bauhinus (1560-1624), of Tulpius (1593-1674), of Bonetus (1620-89), and of Ruysch (1638-1731). Good accounts of the affection may be found in the Dictionnaire des Sciences médicales (tome xxii., Paris, 1818), and particularly in Holmes's Surgical Treatment of the Diseases of Infancy and Childhood (2d ed., London, 1869), in Follin and Duplay's Traité de Pathologie externe (tome iii.), and in Treves's article on “Malformations and Injuries of the Spine” in the International Encyclopædia of Surgery (vol. iv., New York, 1884).
ETIOLOGY.—There are two conditions essential to the formation of a spina bifida: (1) an arrest of development, or at least a defective closure, of the vertebral arches; and (2) a dropsical condition either of the central canal of the spinal cord or of the subarachnoid spaces; but which [p. 758] of these is the antecedent condition it is, as justly remarked by Erb, impossible to decide. Spina bifida often occurs as a complication of hydrocephalus, and is itself often complicated with an atrophic and deformed condition of the lower extremities—a circumstance which led Tulpius to suggest that the malformation was caused by a malposition of the fœtus in utero, an explanation which it seems hardly necessary to waste time in considering. Salzmann observed spina bifida in two children born of the same mother, and Camper noticed it in twins.
SYMPTOMATOLOGY.—Spina bifida forms a tumor—or, more rarely, several tumors—in the region of the vertebral column, usually discovered at birth, but occasionally not noticed until a later period. Thus, Lancisi mentions a case in which the tumor first made its appearance in a hydrocephalic child at the age of five years, and J. L. Apin one in which the patient reached the age of twenty before any swelling was manifested. If these records are accepted as authentic, the only satisfactory explanation is that of Itard—viz. that the bony deficiency existed from the time of birth, and that the dropsical protrusion did not occur until afterward: this seems to me more reasonable than the suggestion of the younger Andral, that the vertebræ underwent a process of secondary softening and absorption. The part most frequently affected is the lumbar region, but cases are not wanting of the occurrence of spina bifida in the cervical, dorsal, and sacral regions, and even, in at least one case (Genga's), in the coccyx. The tumor almost invariably occupies the median line, and projects directly backward: in at least four cases, however, recorded by Bryant, Emmet, and Thomas, the tumor protruded anteriorly from deficiency of the vertebral bodies.
The size of a spina bifida varies from that of a walnut to that of a child's head, or even larger: in some rare instances, such as those recorded by Lezelius and Richard, the whole spinal column has been cleft, and the tumor has extended from nucha to sacrum; but cases of this kind seldom come under the surgeon's observation, as children with such extensive deformity usually perish shortly after birth. The shape of the swelling is rounded, or more often oval; it is commonly sessile, but occasionally pedunculated; and it is sometimes lobulated, the lobules being separated by more or less distinct sulci. The skin covering the tumor is in some cases normal, with more or less fat in the subcutaneous connective tissue, but more often thin, tightly stretched, red, shining, and occasionally ulcerated; more rarely it is thickened and leathery, as in a case referred to by Sir Prescott Hewett. Sometimes a navel-like depression is found at some part of the surface, corresponding, as pointed out by Follin and Duplay, and by Erb, to the place of attachment, on the interior of the sac, of the terminal extremity of the spinal cord. The cutaneous investment is sometimes altogether wanting, the spinal dura mater itself forming the external covering of the tumor. It is in these cases especially that ulceration and rupture are apt to occur.
Spinæ bifidæ are usually soft and fluctuating, and occasionally partially reducible; their tension and elasticity are increased when the child is in the upright position or during the acts of expiration and crying, and are diminished during inspiration or when the child is laid upon its face. When the part is relaxed a bony prominence can be felt on either side, and the aperture in the vertebral column can be more or less distinctly [p. 759] outlined. The swelling is apt to be painful on pressure. If the tumor is of moderate size and covered with healthy skin, there are usually no constitutional symptoms, and, even where ulceration and rupture occur, the opening may heal and a spontaneous cure may possibly ensue. More often, as the tumor increases in bulk—or at any time if pressure be made upon it—various nervous symptoms are observed: drowsiness, muscular twitchings, convulsions, and often paraplegia and paralysis of the sphincters. Rupture is usually followed by the development of spinal meningitis, or may prove directly the cause of death by the loss of cerebro-spinal fluid which it causes; in other instances, however, if the rupture be a small one, healing may occur (as already mentioned) or a fistulous opening may persist; in rare cases the fluid may escape by a process of transudation without rupture, as in an example recorded by Laborie.
As may be inferred from what has already been said, the course of spina bifida is usually rapid and toward a fatal termination. In some instances, however, as in cases observed by Holmes, and more recently by Lithgow, spontaneous recovery has followed the obliteration of the channel which unites the sac with the cavity of the spinal membranes; and in other instances, without a cure having been effected, life has been prolonged for very many years. Thus, Behrend reports a case in which a patient with spina bifida lived to the age of fifty, and Holmes refers to another in which death resulted from an independent disease at the age of forty-three. But a still more remarkable case was recorded by Callender, the patient in this instance having reached the age of seventy-four.
PATHOLOGY AND MORBID ANATOMY.—The most important points for consideration in respect to the anatomy of spina bifida are the relations which the spinal cord and spinal nerves bear to the sac, and the nature of the contained fluid. It is ordinarily said that the spinal cord itself commonly enters the sac of a spina bifida—the report of the London Clinical Society's committee gives the proportion of cases in which it does so at 63 per cent.—and Holmes figures a specimen from the museum of St. George's Hospital, London, in which this condition is obviously present; on the other hand, Mayo-Robson in eight operations only once found the cord implicated; and the late John B. S. Jackson of Boston—whose name will be recognized as one of high authority in regard to all questions of morbid anatomy—once assured me that he had made very many dissections of spinæ bifidæ, and that he had invariably found that the cord stopped short of the sac, and that only the nerves entered the latter: this, as negative evidence, cannot of course contravene such positive evidence as that of the specimen referred to by Holmes, but it would seem to show that the condition was a less common one than is generally supposed, and that in at least a fair proportion of cases the cord itself did not form part of the sac contents. This remark applies especially to those cases in which the fluid is accumulated in the subarachnoid space, and in which, as pointed out by Sir P. Hewett, the cauda equina or spinal nerves are pushed by the vis a tergo into the sac; but when the dropsical effusion occupies the central canal of the cord, this is apt to be flattened and spread out like a thin lining to the sac, just as the brain is spread over the inner wall of the skull in cases of internal hydrocephalus; and, on the other hand, when the accumulated fluid fills the cavity of the arachnoid the cord is apt to be pushed forward, and the [p. 760] sac may be entirely devoid of all nerve-structures. Such, too, according to Giraldès, is the case in spina bifida of the cervico-dorsal region.
The committee of the London Clinical Society classify cases of spina bifida in three divisions: (1) Those in which the membranes only protrude (spinal meningocele); (2) those in which the protrusion involves both the cord and membranes (meningo-myelocele); and (3) those in which the central canal of the cord itself forms the cavity of the sac (syringo-myelocele). The last variety is the rarest, as the second is the most common. In meningo-myeloceles the spinal cord with its central canal is continued within the median, vertical portion of the sac, and at this part there is no covering of true skin; the nerve-roots which traverse the sac arise from this intramural portion of the central nervous system.
Humphry of Cambridge, England, makes a somewhat similar classification of spinæ bifidæ, recognizing as the most common variety the hydrorachis externa anterior, in which the fluid occupies the subarachnoid space in front of the spinal cord, and in which “the cord and the nerves are stretched backwards and outwards upon the sac, and are there confluent, together with the arachnoid, pia mater, and dura mater, or their representatives, in the thin membrane which forms the hindmost part of the wall of the sac;” rarer forms are the hydro-meningocele, or hydrorachis externa posterior, in which the fluid accumulates behind the cord, which does not enter the sac, and the hydro-myelocele or hydrorachis interna, in which the fluid occupies the central spinal canal.
The theory which, according to the Clinical Society's committee, best explains the pathological anatomy of spina bifida is that which assumes a primary defect of development of the mesoblast from which the structures closing in the vertebral furrow are developed.
The fluid of spina bifida appears to be identical in character with the cerebro-spinal fluid. Bostock found that it was very slightly clouded by the application of heat, and that it contained, in 100 parts, 97.8 of water, 1.0 of chloride of sodium, 0.5 of albumen, 0.5 of mucus, 0.2 of gelatin, and some traces of lime. Five specimens more recently analyzed by Hoppe-Seyler gave an average of 98.8 parts water, 0.15 parts proteids, and 1.06 extractives and salts. Turner found a reaction somewhat similar to that of grape-sugar, as had been previously found by Bussy and Deschamps in cerebro-spinal fluid itself, but in two specimens analyzed by Noad for Holmes it was at least very doubtful whether sugar was actually present. “The first specimen was found to be completely neutral; its specific gravity was 1.0077; it contained phosphates, but no reaction could be obtained resembling that of sugar. The second specimen ... did give a reaction with copper like that of sugar, but no trace of fermentation could be obtained.” Three analyses, however, made by Halliburton for the London Clinical Society's committee showed uniformly a decided trace of sugar, with a diminution in the quantity of proteids, which appeared to consist entirely of globulin.
In some cases the sac of a spina bifida contains, besides nerve-structures and cerebro-spinal fluid, both fibrous and fatty tissues.
DIAGNOSIS.—Ordinary fatty tumors have been mistaken for spinæ bifidæ, but such an error could only be committed through carelessness: more difficult is the diagnosis from certain forms of congenital cyst, occupying the median line of the back, and still more difficult the [p. 761] diagnosis from the several affections known as false spina bifida. In the former case the distinction might be made by noting the irreducibility, constant shape, and unchanging tenseness of the cyst, and perhaps, as suggested by T. Smith, by tracing the line of spinous processes beneath it; some information, too, might perhaps be gained by chemical examination of the fluid obtained by puncture. Under the name of false spina bifida Holmes includes three distinct conditions: these are—(1) a true spina bifida, in which the connection with the spinal membranes has in some way been obliterated, the sac then communicating with the vertebral canal, but not with the theca; (2) a congenital, cystic, or fatty tumor, taking its origin within the vertebral canal, and projecting through an opening caused by a gap in the laminæ; and (3) a tumor containing fœtal remains, and properly regarded as an example of included fœtation. In any of these cases a positive diagnosis might be impossible, and the probable nature of the tumor could only be inferred by noting the absence of one or more of the characteristic symptoms of true spina bifida.
PROGNOSIS.—The prognosis of spina bifida is without question unfavorable; at the same time the affection is by no means to be considered, as it was formerly, one of an invariably fatal character, for, apart from the fact already mentioned that several cases are on record in which patients with untreated spina bifida have reached adult life, and even old age, the modern method of treatment has proved so much more successful than those formerly employed that in favorable cases surgical interference affords at least a reasonable prospect of recovery. The circumstances which especially furnish grounds for an unfavorable prognosis are the rapid growth of the tumor, the thinning or ulceration of its coverings, and the occurrence of nervous symptoms, and particularly of paralysis or convulsions.
TREATMENT.—This may be either palliative or radical. If the tumor be not increasing materially in size, the surgeon may properly content himself with palliative measures—applying equable support and perhaps slight pressure by the use of a well-padded cap of gutta-percha or leather, an air-pad, or, as advised by Treves, a simple pad of cotton smeared with vaseline, and a bandage; if the tumor be small and covered with healthy integument, painting its surface with collodion may be of service through the contractile property of that substance. Radical measures are only indicated when the child, otherwise healthy, seems to have his life threatened by the rapid growth of the tumor, causing risk of ulceration and rupture, or giving rise to convulsions or paralysis. The principal modes of treatment to be considered under this heading are—(1) simple tapping or paracentesis; (2) injection of iodine; (3) ligation of the neck of the sac; and (4) excision.
(1) Paracentesis, a simple evacuation of the fluid contents of the sac, is the only operation ordinarily justifiable in cases attended by paralysis or other grave nervous manifestations. The puncture should be made in the lower part of the sac and at a distance from the median line (in the course of which the nerve-structures are particularly distributed), and only a small quantity of fluid—a few drachms or at most one or two ounces—should be removed at a time, the instrument being at once withdrawn if convulsions follow, and the wound being instantly closed with lint dipped in compound tincture of benzoin. Either an aspirator-tube or a [p. 762] small trocar may be used, and the operation may be repeated if necessary, pressure being maintained during the intervals. Paracentesis has occasionally though not often proved curative.
(2) Injection of Iodine.—This mode of treatment was introduced about the same time by Velpeau and by Brainard of Chicago. The latter surgeon's method consists in injecting, after only partially emptying the tumor, a solution of iodine with iodide of potassium (iodine, 5 grs.; iodide of potassium, 15 grs.; water, 1 fl. oz.), allowing it to flow out again, washing out the sac with water, and finally reinjecting a portion of the cerebro-spinal fluid originally evacuated; and the former's, in completely evacuating the tumor, and then injecting a mixture of iodine and iodide of potassium, each one part to ten parts of water. Each of these plans has met with a fair measure of success;1 but the modification introduced by James Morton of Glasgow is a great improvement, and affords what is actually the most successful mode yet devised for dealing with spina bifida. Morton employs a solution of iodine in glycerin (iodine, 10 grs.; iodide of potassium, 30 grs.; glycerin, 1 fl. oz.), which has the advantage of being less diffusible than the aqueous solution, and therefore less liable to enter the spinal canal. The tumor is about half emptied, and a small quantity—from fluid drachm ss to fluid drachm iij of the solution—is then slowly injected, and allowed to remain. The operation is repeated after a few days if necessary. Of 50 cases known to Morton as having been treated in this way up to May, 1885, 41 were regarded as successful; but of 71 cases collected by the London Clinical Society's committee, only 39 had been benefited by the operation.
1 In a case recently recorded by Woltering, however, iodine injection was followed by death within half an hour.
The introduction of iodine into the sac of a spina bifida is, according to Morton, only justifiable in cases unattended by paralysis; under opposite circumstances I should be disposed to try a plan recently employed with success by Noble Smith in a case of meningocele—viz. injecting the iodo-glycerin solution into the coverings of the sac, and as close to it as possible without perforating it.
(3) and (4). Ligation and excision have each occasionally effected a cure, but more often have but helped to precipitate a fatal issue. A successful case of ligation followed by excision has been recently recorded by Löbker. The elastic ligature, applied around the neck of the sac (if this be pedunculated), has been employed by Laroyenne, Ball, Colognese, Baldossare, Mouchet, and other surgeons, and of 6 cases collected by Mouchet, 3 ended in recovery. Another success has been recently recorded by Turretta. The écraseur has been used, but its employment cannot be recommended. Compression by clamps is advised by Schatz of Rostock. Ligation is best adapted to cases occurring in the cervical and dorsal regions, in which, as pointed out by Giraldès, nerve-elements are less likely to be involved. Excision, supplemented by transplantation of a strip of periosteum from a rabbit, has been successfully resorted to by Mayo-Robson and by R. T. Hayes of Rochester, N. Y.; and simple excision, with suture in separate lines of the sac and integuments, by Mayo-Robson, Atkinson, and Jessop. The Clinical Society's committee in all refers to 23 cases treated by excision, 16 of which are said to have been successful.
Up to within a few years it was a favorite mode of explaining the results of the administration of certain narcotic and stimulant drugs, and certain of the active symptoms of mental derangement, to attribute them to an increased blood-supply of the nerve-centres. This view seemed to harmonize so thoroughly with the physiological dictum that functional activity depends on the supply of oxygenated blood that the first attempts at questioning it were treated as heresies. To-day, however, few authorities can be found to adhere unreservedly to this once-popular and easy explanation. The drift of physiological and medical opinion is in the direction of regarding some subtle molecular and dynamic state of the nerve-elements as the essential factor in intoxications as well as in maniacal and other forms of insane excitement: if they be complicated by active or passive congestions, this is probably a secondary occurrence of modifying but not of intrinsic determining power. While this change in our views is the natural result of progress in experimental pharmacology and pathology, it does not justify the extreme assertion that there is no disorder of the brain functions deserving the name of congestion and hyperæmia. This assertion seems to have been provoked by the careless manner in which these terms have been employed to designate conditions which are in reality the most different in nature that can be well conceived. No one familiar with the extent to which the term “congestion of the base of the brain” has been abused in this country will marvel that the reaction provoked by it has overstepped the boundaries of cautious criticism. That there are physiological hyperæmias of the brain is now universally admitted; the most recent experimental observations, indeed, conform most closely to the claims of the older investigators. It naturally follows that pathological hyperæmias are both possible and probable, and even if the observations in the dead-house do not strongly sustain the existence of pathological hyperæmias and congestions independently of gross disease, clinical analysis and the gratifying results of appropriate treatment justify us in retaining these designations in our nomenclature with the limitation here implied.
One great difficulty in determining the precise nature of the disorders which the physician is called upon to treat on the theory of hyperæmia lies in the number of factors which may contribute to or modify its [p. 764] development. If, for example, the action of the heart be increased through hypertrophy, the result to the cerebral circulation will obviously be different in a plethoric and in an anæmic person; it will be also very much different in the event of the stimulation of the centres which contract the calibre of the cerebral blood-vessels from what it would be if there were a state of vascular relaxation. Should the cardiac hypertrophy be associated with renal disease, other disturbing elements may be introduced, such as arterio-fibrosis, or the presence in the blood of certain toxic substances having direct effects of their own on the nerve-elements. The picture may be still more complicated by variations in the intracranial pressure. It is impossible to prove, either by direct or indirect evidence, that there is such a pathological state as a simple cerebral hyperæmia; indeed, there is one fact which militates strongly against, if it be not fatal to, such an assumption. Were a physiological hyperæmia to become intensified to a pathological degree, we should have corresponding clinical phenomena. In other words, the culmination of the morbid process should be preceded by an exaggerated physiological excitation similar to that observed with intoxications. But this is rarely the case, and we accordingly find that the more cautious writers, like Nothnagel,1 do not commit themselves to the view that the results of mental overstrain2 are to be classed as simple cerebral hyperæmia. Similar restrictions are to be made regarding the established congestive states, such as those following sunstroke. It has been usually supposed that insolation directly produces cerebral hyperæmia, even to the degree of engorgement, and that the after symptoms in persons who recover are due to the non-return of the meningeal and cerebral blood-vessels to their normal calibre, and to other more remote results of vascular stasis. The latter half of this proposition is in part correct; the former is contradicted by numerous pathological observations. Thus, Arndt,3 who had the opportunity of studying over one hundred cases occurring in the course of a forced march of a division of infantry from Berlin to Pankow, many of which terminated fatally, found almost uniformly a pale brain, with peculiar color-changes, denoting rather structural than circulatory trouble.4 The [p. 765] whole list of causes of what is commonly designated cerebral hyperæmia, congestion, and engorgement may be gone through with and similar modifying statements be found to apply to them. The nearest approach to an ideal cerebral congestion is that found with acute alcoholic intoxication. This is at first accompanied by cerebral hyperæmia, which, with the comatose climax, becomes an engorgement; accordingly, many of the results of acute alcoholic intoxication are attributed to the circulatory condition alone. The congestive troubles due to alcoholism which come to the special ken of the physician, however, are those found with the chronic form, and here a more complex pathological condition is found to underlie it; the organization of the brain is altered, the vascular channels more or less diseased, and the vaso-motor mechanism continuously deranged. This disorder, as well as the apoplectiform states attributed to vascular stasis, and the active and passive hyperæmias associated with tumors, meningitic and other gross diseases of the brain, as well as with the status epilepticus, are usually included in the discussion of cerebral congestion, and serve to swell up the chapters devoted to it. They will be found discussed in more appropriate situations in this volume. In this place it is proposed to consider only those congestive states which present themselves to the physician, independently of conditions which, if associated, preponderate in clinical and therapeutic importance.5
1 Ziemssen's Cyclopædia, “Nervous System,” i. p. 39, 2d German ed.
2 It has repeatedly happened during the past decade that young persons competing for admission to higher institutions of learning in New York City through the channel of a competitive examination died with symptoms of cerebral irritation; the death certificates in several such cases assigned meningitis or cerebral congestion as the cause of death, and attributed the disorder to mental overstrain. It is not so much the intellectual effort that has proved hurtful to the pupils as the emotional excitement attending on all competitive work, the dread of failure, the fear of humiliation, and anxiety developed by the evident futility of the cramming process. Some years ago I recorded the results of some inquiries on this head in the following words: “The mental-hygiene sensationalists, who periodically enlighten the public through the columns of the press whenever an opportune moment for a crusade against our schools and colleges seems to have arrived, are evidently unaware of the existence of such a disease as delirium grave, and ignorant of the fact that the disorder which they attribute to excessive study is in truth due to a generally vitiated mental and physical state, perhaps inherited from a feeble ancestry. Our school system is responsible for a good deal of mischief, but not for meningitis” (Insanity, its Classification, Diagnosis, and Treatment). Since then I had an opportunity of obtaining an excellent description of such a case which had been attributed to the combined effects of malaria and educational overstrain, presenting opisthotonos, fulminating onset, and an eruption!
3 Virchow's Archiv, lxiv.
4 The observations of Gärntner (Medicinische Jahrbucher, 1884, 1) harmonize with this. He found that radiant heat contracts the blood-vessels of the frog's mesentery.
5 The same applies to conditions which are discussed under this head in textbooks, although they have either only a medico-legal bearing or are inconstant factors, such as the injection of the brain in death from strangulation. I need but instance the vascular condition of brains of criminals executed by hanging. In the case of one where the strangulation had been slow I found an engorgement of all the vessels and arachnoidal as well as endymal hemorrhages; in a second, where the criminal had been carried half fainting to the drop, and death ensued quickly and without signs of distress, the brain was decidedly anæmic.
It has been also considered best to omit treating of the collateral hyperæmia of the brain sometimes found with erysipelas of the face and scalp. This I regard as essentially of the same nature as the metastatic meningitis of erysipelas, if it be not in reality a first stage of the latter.
ETIOLOGY.—An individual predisposition to cerebral congestion was one of the unquestioned facts of the older medical writers. It undoubtedly exists, and to-day we attribute it to inherited vascular conditions either affecting the calibre and coats of the blood-vessels or the vigor of the vaso-motor apparatus. I have remarked the transmission of that weakness of the latter which underlies the congestive phenomena of later life much more frequently in the female than in the male sex.
It has been claimed that external refrigeration produces hyperæmia of the brain, as of other internal organs, and that this accounts for the greater frequency of the disorder in cold weather. Niemeyer indeed speaks of persons who, suffering from this condition, appear and act in such a way as to convince the laity that they are intoxicated; and Andral, Falret, and Hammond note the occurrence of a much larger number of cases in the winter than in the summer months. I apprehend that the condition described by Niemeyer must be extremely uncommon, both from individual experience and the rarity of its mention as an independently observed fact. With regard to the alleged greater frequency of the disorder in winter, it must be remembered that all the three observers cited include in their computation a number of cases in which congestion was a collateral feature; they did not limit themselves to the disorder as [p. 766] spoken of here. Certainly, the physician will see few if any persons who consult him because of the hyperæmia-producing effects of a cold day.
The suppression of habitual discharges, of the hemorrhoidal flux, and the cessation of menstruation are associated in many instances with the more formidable grades of cerebral hyperæmia. Many phenomena of so-called climacteric insanity depend on congestive states. The sudden closure of an old ulcer or the removal of hemorrhoids in advanced life has in some well-established instances provoked alarming seizures not unlike those noted with paretic dementia. The chain of proof establishing the direct influence of physiological and pathological discharges on the vascular controlling apparatus of the brain is most complete. Not alone cumulative clinical observation, but the occasional happy result of therapeutical procedure based on this supposed interdependence, support it. Thus, the congestive cerebral state is recovered from when the menstrual or hemorrhoidal flow is re-established, or an issue is formed in the nape of the neck, or an old ulcer is allowed to reopen.6
6 The treatment of paretic dementia, particularly of the congestive type, is also based on this relation. The irritating antimonial ointment and issues in the nape of the neck, etc. have been lauded by older observers, and in two of my own cases had the best results—in one, indeed, with established restitutio ad integrum of now nearly two years' duration. I am inclined to suppose that its abandonment is due to an improper selection of cases; in the ordinary premature senility and syphilitic types such treatment is altogether ineffective. It is applicable to but a minority of cases at best, and to them only at an early period. It is probably to a similar form of congestion that Bouchut refers when (“Les Nèvroses congestives de l'Encéphale,” Gazette des Hôpitaux, 1869) he speaks of a cerebral hyperæmia developing under the mask of a meningitis—an expression that may be allowed if understood in the same sense as the comparison between hydrocephaloid and hydrocephalus.
The origin of most cases that are brought to the physician's attention is more or less complicated. A business-man, lawyer, or student suffering from worry incident to his profession, living so irregularly as to provoke gastric disturbances, becomes afflicted with insomnia, and in addition is also constipated. Straining at stool, he finds a dull, heavy sensation affecting the upper part of his head; attempting to resume his work, this is aggravated, and after a series of temporary remissions the condition to be later described becomes continuous. In such a case the insomnia, usually due to neural irritability, if not aggravated by an existing dyspepsia, leads to such a one, and a circulus vitiosus familiar to all physicians is established. Each of the factors concerned involves strain of the cerebral vaso-motor apparatus, but none more so than the insomnia. It is not so much the intensity of the strain as its long duration and the exhaustion of the centre which in sleep is supposed to be at comparative rest. This rest is not obtained, and, in conformity to the laws of neural exhaustion, that centre becomes morbidly irritable. Now, gastric irritation is competent to produce a reflex influence on even the healthy cerebral organ; to do so it must be a severe one; but with the class of persons alluded to the slightest indiscretion in food or drink is sufficient to set up reflex vertigo or headache. The current theory regarding these symptoms is that they are due to stimulation of the vaso-constrictors and ensuing cerebral anæmia; but the subjects before us will usually be found to flush up instead of becoming pale, as in simple vertigo a stomacho læso, or if there be initial paleness, there is a [p. 767] secondary flush, as if the tired arterial muscle had become exhausted by the effort at obeying the reflex stimulus. In addition, a profuse perspiration sometimes breaks out on the upper part of the body.
The influence of traumatic causes and insolation in producing a tendency to repeated and severe cerebral congestion is recognized, particularly among alienists. It is supposed that an abnormal irritability of the vaso-motor apparatus is provoked by these causes. Abundant evidences are sometimes found in the brains of such persons of an altered state of nutrition of the brain and its membranes, and which point in the direction of congestion.
In the conditions thus far alluded to it can be fairly assumed that the determination of blood to the cerebral blood-vessels is more or less active. Passive congestion due to impeded return circulation is of secondary interest, as the primary disease, be it a pertussis or a laryngeal, cardiac, pulmonary, or surgical condition, will constitute the main object of recognition and management. Certain quasi-physiological acts, as coughing, hurried breathing, holding the breath while straining at stool, and placing the head in a dependent position while acting in the direction of passive hyperæmia, are to be considered in connection with the active forms of congestion which they may momentarily aggravate.
MORBID ANATOMY.—Owing to the non-fatality of the commoner forms of cerebral hyperæmia, no pathological observations of them are at our disposal, nor can we assume from analogy that the appearances would be well marked if they could be made. What little knowledge we have is derived from a study of more serious conditions of which cerebral hyperæmia is an initial, collateral, or episodial feature.
In pronounced cerebral hyperæmia the entire brain is, as it were, tumefied, so that the dura appears tensely stretched over its surface and the gyri are flattened; both the meningeal vessels proper and those of the pia are injected. According as the hyperæmia is active or passive the color of this injection varies, being of a brighter red in the former, of a purple or bluish color in the latter case. The purest instances of active cerebral hyperæmia which I have seen were found in patients dying in the apoplectiform phases of paretic dementia (progressive paralysis of the insane). Here the cortex on section exhibited a beautiful rosy tint, which was distributed in darker and lighter strata in correspondence with the distributional areas of the short and the long cortical arteries; there were numerous puncta vasculosa both in the cortex and in the white substance, and in some instances the arachnoid or the ventricular fluid was tinged with blood, albeit no vascular rupture could be discovered. The red blood-corpuscles undoubtedly escape by diapedesis from the surface as well as the endymal vessels; the same thing occurs in the intracerebral blood-vessels, whose adventitial spaces are often crowded with accumulations of red blood-discs, while groups or single ones are found scattered in the surrounding parenchyma, and even in the periganglionic spaces. Occasionally accumulations of pigment found near the vascular channels remain to attest the former existence of other hyperæmias, and indeed slight accumulations of this kind are found in the brains of most persons who have reached adult life. These are to be regarded as remnants of the physiological hyperæmias to which all active individuals are subject. It is only when the accumulations become considerable and numerous, as in the chronic insane, or are associated with those changes in the blood-vessels [p. 768] which are discussed in the articles on thrombotic and hemorrhagic cerebral disease, that they can be regarded as indications of a pathological condition.
Acute simple meningitis is ushered in by cerebral hyperæmia of the active form. This is not alone demonstrated by the early symptoms of this disease, but also by the fact, which I have observed in two cases, that where this form of meningitis originates on one side, as from extension of the middle-ear trouble, the opposite cerebral hemisphere exhibited intense congestion of the ideal type.
In that serious form of mental disease known variously as grave or acute delirium and typhomania (Luther Bell) a form of cerebral hyperæmia is observed which in its intensity approximates inflammatory congestion. The surface of the brain appears marbled and mottled; blood seems to exude from the gyri after the pia is removed; the cortical lamination is invisible, owing to the hyperæmic discoloration of the gray substance; and the parenchymatous elements themselves appear to be in a state of cloudy swelling. In one case I have observed transudation of a hyaline proteinaceous substance and an exudation of fibrin around the larger arterioles. In some cases of typhus fever a less intense but similar congestive hyperæmia is found. The hyperæmias of paretic dementia, of acute delirium, and of typhus fever agree in this one feature: that all districts of the brain, from the cortex and white substance of the cerebral hemispheres to the medulla oblongata, are involved nearly to the same degree. In the hyperæmia of simple meningitis of the convexity it is chiefly confined to the pia mater and the most superficial cortical strata.
Congestion of the brain from stagnation of the venous return circulation should not be confounded with active hyperæmia. With this condition, which may be due to thrombosis of the sinuses, morbid growths near the jugular foramen or in the neck around the internal jugular veins, or, finally, to certain cardiac and pulmonary disorders, there is rather a lesser than a greater amount of blood sent to the brain; and it is not infrequently found that while the surface of the brain appears congested, owing to the prominence of the cerebral veins, the deeper parts are quite anæmic; and if the injection be general, it will be found that the blood, whether in arteries or veins, has the venous character. An excellent example of this form of congestion is afforded by persons dying in the status epilepticus. In their brains the venous channels stand out, filled to their extreme capacity with blood almost black in color; and in prepared sections, particularly such as are taken from the pons and medulla oblongata, a beautiful natural injection of the vessels is found. But that rosy color which is so characteristic of active hyperæmia is absent, the tissues appearing purplish, bluish, or chocolate-colored.
SYMPTOMATOLOGY.—There are few symptoms attributable to the nervous system which have not been enumerated among the characteristics or the occasional manifestations of cerebral hyperæmia. Thus, Hammond not only follows Andral in enumerating apoplectic, convulsive, comatose, and maniacal symptoms as acute manifestations of active cerebral congestion, but assures us that aphasia may occur under the same circumstances. In the course of his work on the subject, “an absolute want of power to get correct ideas of even simple matters,” confusion of ideas, weakening of the judgment, vacillation of purpose, diminished logical power, [p. 769] illusions and hallucinations of every sense, delusions, morbid apprehension of impending evil, imperative, suicidal, and other impulses, suspicion, hypochondriasis, furious delirium, and the use of profane and obscene language, are enumerated among the characteristic or prominent symptoms of various forms and cases of cerebral hyperæmia.7 Not one but several of the recognized forms of insanity have yielded a fair quota of their symptoms to this long array. Among somatic signs he in like manner names neuralgic pains, numbness, spasms, paralysis, false impotence, hyperæmia of the tympanum, choked disc, abolition or perversion of the sense of smell, taste, and sight, fibrillary or fascicular twitches, various states of the urinary excretions, diplopia, and monoplegias. It is here equally evident that the initial symptoms of a considerable number of organic and clearly defined affections have been included. It is on account of the confusion engendered by this wide interpretation of the meaning of the term congestion of the brain that I have determined to limit the term as previously indicated, and to consider only the active form here.
7 A Treatise on the Diseases of the Nervous System, 7th ed., pp. 1-53. The natural inference following a perusal of this chapter, as well as the monographs to which their author refers, is that he has gathered together all states in which cerebral hyperæmia was an associated factor, as well as those in which he appears to assume its existence on theoretical grounds, and designated them as cerebral congestion. In some instances he uses the terms hypochondria and cerebral hyperæmia interchangeably (p. 50, loc. cit.).
A feeling of head-pressure, associated with a more or less severe dull pain, aggravated by mental exertion, by stooping down, by straining at stool, or when out of breath, and accompanied by a subjective sense of mental dulness, is the most constant feature of the ordinary cases. There is usually a vertiginous sensation, and an irritability of the eye and ear not unlike that described in the article on Cerebral Anæmia. Sleep is at first disturbed by vivid and sometimes frightful dreams; later, it becomes interrupted, and ultimately complete insomnia may develop. The action of the heart is accelerated and exaggerated in some cases; in that event increased pulsation of the carotids, flushing of the face, injection of the conjunctiva, and a subjective sense of heat in the head and face are experienced. Hammond, in accord with Hasse and Krishaber, believes that febrile symptoms may develop under these circumstances; most authorities, however, deny this for the uncomplicated form. I have never found an objective rise of the general temperature.
Such a condition as that described is usually slowly produced, several weeks, or even months, being occupied in its development. At first the unpleasant symptoms occur only at certain hours of the day, with temporary exacerbations and remissions. It may be arrested with comparative ease at any time; if neglected, the mental faculties become affected, not in the grave sense in which Hammond and the older authors describe it, so as to carry the patient into actual dementia or delusional insanity, but rather in the way of diminished working-power. It is more difficult to fix attention, to recollect words, names, and figures, or to keep up a protracted mental effort, than in health, but the formal judgment does not suffer. I have known patients to be in this condition for many months, and several for more than one year, without any grave deterioration. It is true that in the prodromal periods of some forms of insanity, such as acute mania, there is a condition very similar to that of these patients; [p. 770] and this has led to regarding mania as a possible phase of cerebral hyperæmia. But the very fact that, typically, mania is preceded by such a stage—which is always of brief duration—that maniacal excitement is a constant and unavoidable consequence upon it, while, as far as known, the condition here described may last for years without leading to a true psychosis, should prevent one regarding the two conditions as identical, however similar they may be for the time being.
In sufferers from cerebral hyperæmia who pass into the chronic state of this disorder the disturbance of sleep and of the digestive organs becomes very prominent, and continually reinforces the acting causes of the disorder. In a large number of cases the head-sensations become more or less localized; that is, while the general feeling of pressure or dull ache may continue, a special area, which can be covered by the palm of one hand, either in the middle part or to one side—usually the left—of that part of the vertex, is the seat of a more severe pain, complained of as a hot pressure. The patients frequently claim that the temperature is higher at this spot, and, contrary to what might be anticipated on a priori grounds, the statement will be confirmed, not alone by the coarse method of using the hand, but by the surface thermometer. The locality where this occasional rise of temperature and the more common sense of pressure are experienced corresponds to that part of the longitudinal sinus where the largest cerebral veins enter. It is a noteworthy fact that nearly all the important admunctories of this sinus empty into it within the short space of two inches at this point.
Not all sufferers from cerebral hyperæmia give a history of a gradual development of their symptoms. A few date their trouble from some single intellectual, physical, or emotional strain. In one case, complicated by marked evidences of cerebro-spinal exhaustion, the patient, a lady, had during an illness of her husband, being deserted by her servants, and the water-supply having been cut off, carried all the water required for the invalid and domestic as well as sanitary purposes up three flights of stairs for two unusually hot days in July. In two others, strikingly similar in many details of their cases, both being cornet-players, both attributing their illness to an extra call upon their instrument, it was brought on in the older patient within a few hours after playing on a hot day at the State Camp at Peekskill, and in the second at Narragansett Pier as he left the sultry concert-room and became exposed to a draught. In both these cases, as in a large number since examined, some stomach trouble could be positively determined to have antedated these symptoms. I mention this because it is only in such cases that I have found the nausea or vomiting which some writers regard as an occasional occurrence of, and due to, the lighter form of cerebral hyperæmia.
There are no ophthalmoscopic evidences of cerebral hyperæmia of this form. I have never found the optic disc presenting variations in tint beyond those found within normal limits, except in a case of saturnine encephalopathy with predominant signs of cerebral congestion. I believe that the statement of Hammond8 as to the existence of choked disc in cerebral hyperæmia is generally regarded as due to the interpretation of organic diseases as congestive states. It is not confirmed by authorities.
8 Loc. cit., p. 41, lines 29-36.
I have never found the tympanic membrane hyperæmic independently [p. 771] of ear disease, even when tinnitus was marked. It is claimed to exist by Hammond, and he adduces as analogous the observation of Roosa that quinine produces an injection around the handle of the malleus.9
9 It certainly is not necessary to look to the injection of the tympanum as an explanation for the tinnitus of cerebral hyperæmia, based on such an analogy. The tinnitus of cinchonism is more central in location, being producible in persons who have pathological or no tympanic membranes, just as the tinnitus of cerebral hyperæmia occurs indifferently under like circumstances.
The congestive states which follow traumatism and insolation are properly considered in connection with the traumatic neuroses and certain forms of insanity. But there are some milder cases in which the symptoms remain within such compass as is comprised in this section. The patient, after a fall or a blow on the head, suffers from insomnia, has a sensation of fulness and ache in the head, complains of a pulsating feeling in the occipital region and an inability to concentrate his thoughts on subjects which previously were parts of his routine. Under appropriate treatment recovery ensues, but there remains behind an intolerance of alcoholic beverages, and at times the patient experiences momentary fits of abstraction, which may be regarded as mild analogies of the more serious episodes of the full-blown traumatic neurosis. Thus, he may be walking along the street and suddenly lose his train of thought for an instant, to regain it on observing that he has inadvertently made a misstep. Or in the midst of an address a previously fluent orator in attempting to find a certain by-law in the rules of a society is unable to recollect which he was in search of, and is compelled to take his seat with a rambling apology. But for the fact that similar sequelæ are noted in cerebral hyperæmia from other causes, it would be questionable whether it be proper to attribute them to the congestive element engendered by the traumatic influence. They are usually noted when the hyperæmic phenomena proper have become latent or disappear, and, with other symptoms customarily treated of as mere results of circulatory trouble, may be regarded as signs of neural exhaustion or inadequacy rather than of insufficient ensanguination.
A more serious form of cerebral hyperæmia occurs in females in conjunction with the climacteric period, and in both sexes in consequences of the suppression of any habitual discharge in advanced, and exceptionally in middle and juvenile, life. The advent of the symptoms is rapid, a few hours or days sufficing for the development of the attack. The face is flushed, the carotids throb violently, the general cutaneous surface is congested, and the patient is incoherently talkative. The one side, usually the right, is heavy and tremulous, the fingers are devoid of their usual skill, and the speech is more or less thick. The sleep is disturbed or replaced by a stuporous condition, whose similitude to an apoplectiform seizure is sometimes heightened by stertorous breathing. After one or several days the patient emerges from this condition by degrees or suddenly with complete restitutio ad integrum. But the attack may recur, and ultimately it is noted in the event of repeated attacks that the return to the normal state is slower and less complete: the disorder then undergoes a transition into the congestive type of paretic dementia described in another portion of this volume.
DIFFERENTIAL DIAGNOSIS.—In some of its clinical aspects cerebral hyperæmia closely resembles cerebral anæmia. This is not surprising [p. 772] when we bear in mind that both constitute nutritive disturbances of the same organ, and that, notwithstanding the apparent difference in the surface injection of an anæmic and a hyperæmic brain, the state of affairs in the ultimate capillary districts may be much more alike than might be anticipated on theoretical grounds. In congestion we have wider vessels, and perhaps, though not necessarily, a better quality of blood; but at the same time the intracranial pressure may be such that the venous emunctories can labor but slowly: the result will be that although there is more blood in the brain, the lessened rate of flow places the nerve-elements under nearly the same nutritive disadvantage that they are placed under with the narrower and vitiated but more rapid blood-column of ordinary anæmia.10 It is particularly the symptoms dependent on those nerve-centres and tracts which are, so to speak, dynamically sensitive, which resemble each other so much that an intrinsic difference—both being placed side by side—is not always determinable. This is true of the aural and optic symptoms. Tinnitus, photophobia, scotomata, and blurring or darkening of the visual field occur in both, and in about the same varieties. In my experience the acuteness of hearing is more apt to be interfered with by the subjective sounds with hyperæmic than with anæmic tinnitus. The scotomata of hyperæmia are more distinct and coarser than those of anæmia; darkening of the visual field is more apt to occur with sudden rising in anæmia, while in hyperæmia it is provoked by coughing, straining at stool, or other cause operating directly or indirectly on the return circulation. It may be stated, as a general rule, that if any of these symptoms are aggravated on lying down or stooping, they are due to hyperæmia; while if the same procedures are resorted to in anæmia, amelioration ensues. But in many chronic cases these symptoms seem to continue as indications of a permanently altered activity of the nerve-elements themselves; that is, as a sort of pathological habit. In that case the position test may not be decisive. In one respect there is a decided difference between the anæmic and hyperæmic forms; there is never amaurosis in the latter, while it is approached, and occasionally fully developed, in the former. Much more importance attaches to the differentiation of tinnitus due to nutritive brain disorders and that due to aural disease. As a rule, the tinnitus from cerebral hyperæmia is symmetrical; if unilateral, it is of short duration. The procedure of Valsalva11 aggravates the tinnitus of hyperæmia, and relieves that which is due to the commoner forms of ear disease; the former is aggravated and the latter relieved by noise.
10 It is also admitted that the blood stagnating in the larger veins and accumulating in the arteries, the limits of compressibility of the other cerebral contents being passed, the capillaries will suffer, so that with injected and turgescent arterioles and venules there may be capillary anæmia.
11 I would caution against Politzer's method in cases of ear disease coexisting with cerebral congestion. In a patient now under my treatment each session at the aurist's was followed by a distinct exacerbation of the cerebral symptoms.
In the table on p. 773 I have attempted to formulate the principal differential relations of the protracted forms of cerebral anæmia and hyperæmia.
There are a number of so-called functional nervous states which, aside from the fact that they are unwarrantably confounded with cerebral congestion, do not require mention in a differential relation. Such are the [p. 773] masturbatory neurosis, certain hysterical states, and the asthenia resulting from nervous shock and overwork. These states have found a provisional resting-place under the comprehensive and non-committing title of neurasthenia or nervous exhaustion—a term which includes conditions fully recognized by Robert Whytt and Isenflamm in the last century.
| Symptomatic State. | In Cerebral Anæmia. | In Cerebral Hyperæmia. |
| Pupils. | Usually dilated and mobile. | Usually small or medium. |
| Respiration. | Often interrupted by sighing or by a deep breath, even when at rest. | Normal. |
| Headache. | Either sharp and agonizing, and then in a limited area, or a general dull ache, intensified in the temples and over or behind the eyes. | If localized, accompanied by a subjective and objective (always?) feeling of heat; if general, is compared to a bursting or steady pressure. |
| Activity. | There is lassitude. | There is indisposition to exertion, yet patient is restless. |
| Temperament. | Lethargic, with exceptions. | Choleric, with exceptions. |
| Intellect. | Inability to exert. | Rather confusion than inability of. |
| Sleep. | Insomnia, interrupted by trance-like conditions, in which the patient is comparatively comfortable. Dreams often pleasant. | Insomnia, with great restlessness, variegated by unpleasant and confused dreams. |
| Influence of upright position of body. | Aggravates all the symptoms. | Either without influence or beneficial. |
| Influence of recumbent position of body and dependent position of head. | Amelioration. | Aggravation. |
| Influence of acts involving deep inspiration, such as blowing, straining at stool, sneezing, etc. | If any, a sharp headache may ensue, but the other symptoms are not aggravated. | Aggravated. |
TREATMENT.—Ergot of rye with its preparations may be regarded as the cardinal drug in cerebral hyperæmia. There are few drugs in the domain of neurological therapeutics which are so directly antithetical to the pathological state as this one. There is scarcely a case of cerebral hyperæmia that is brought to the physician's attention but may be regarded as being in part due to an over-distension of the cerebral vascular tubes. This is directly overcome by ergot, and the quantity which such patients will sometimes bear without showing signs of ergotism is something remarkable, in notable contrast with the subjects of cerebral anæmia, who are usually very sensitive to it. About three grains of Bonjean's ergotin may be regarded as a safe trial-dose for an adult, and unless a distinct effect is produced within two or three days this dose may be raised to six grains twice or three times within twenty-four hours. It is not advisable to combine strychnia with the ergotin, as is often done; the effect of that alkaloid is to increase the psychical and sensorial irritability of the patient. Chloral hydrate or bromide, or both in combination, is as useful an adjuvant here as it would be hurtful in cerebral anæmia.
It is not usually necessary to employ special hypnotics in cerebral congestion. The same drug whose beneficial effect is so potently marked during the daytime that tinnitus, cerebral pressure, and subjective drowsiness will disappear before it, if not as rapidly, more enduringly, than the symptoms of cerebral anæmia disappear before nitrate of amyl, will also overcome the insomnia in the majority of cases. Where it fails, warm pediluvia or sitz-baths will prove more efficient than the majority of hypnotics. Their use, at all events, involves no hurtful effect on a—possible already—disordered stomach, and their certainty of action is [p. 774] much more even. Their temperature should be about 40-42° Centigrade, and the immersion continue from fifteen to twenty-five minutes.12
12 A number of experiments, the most recent of which were by Musso and Bergesio (Rivista sperimentale di Freniatria e di Medicina legale, 1885, xi. p. 124), have shown that in such baths the cerebral pulsations become less excursive and that the volume of the brain decreases. The same applies to general warm baths.
In those cases where the subject sensations accompanying hyperæmia, active or passive, are intensified in the posterior segment of the head or the nuchal region, leeches at the mastoid process, or cupping, wet or dry according to the severity of the symptoms, will often give immediate relief. Burning with the actual cautery, or, what is equivalent and a much neater application, the heated glass rod, has an equally happy effect in that class of cases where throbbing and pain are intensified low down. It should be done as near the spot indicated by the patient's complaints as possible.13
13 In a case of gliomatous hypertrophy of the pons oblongata transition marked by the development of numerous tortuous and enlarged blood-vessels the episodes of the disease were found to be of the congestive type, and yielded to no other treatment than that with the cautery.
The diet of patients who are suffering from or subject to cerebral hyperæmia should not be stimulating nor difficult of digestion. It is much more important to avoid distension or overstrain of the stomach than to reduce the nutritive value of the food in the majority of cases, for true plethora is much less common than is supposed. The bowels should be so regulated that the patient have at least one, and that an easy, movement a day. The saline cathartics, particularly the Carlsbad salt, are to be used to effect this if necessary. The clothing around the neck should be free and not compress the parts.
In those severe forms of cerebral congestion attending the climacteric period, or occurring in consequence of the suppression of discharges, and similar causes, the symptoms are often so alarming as to render energetic measures, such as bleeding, immediately necessary. This may be affected by applying leeches to the nose, the temples, or by bleeding at the arm. If due to the suppression of hemorrhoidal discharges or menstruation, the leeches should be applied to the anus and hot sitz-baths taken. In the milder forms a pill composed of aloes, podophyllin, and ox-gall, recommended by Schroeder van der Kolk, will be found effective.
The oft-confirmed observation of Treviranus, that the brain is paler in the sleeping than in the waking state, supplemented as it has been by more elaborate observations, which show that the difference between the intracranial blood-amounts, as estimated in these opposite states, is equivalent to one-twenty-fourth part of the total blood-amount of the body, has been made the basis of much dazzling theory and premature speculation. Hyperæmia of the central nervous apparatus or of certain of its provinces becomes regarded as synonymous with over-activity, and anæmia, general or provincial, as the expression of the opposite functional state. Elaborate directions may be found, even in recent treatises on the subject, how to diagnose, not alone hyperæmia and anæmia of the brain [p. 775] and spinal cord, but also of special lobes of the former and particular columns of the latter. These directions are in most instances based on assumptions which are not supported by direct or tangible evidence, and the consequence is that they have failed to stand the tests of experience, where this gauge is applicable, and necessarily failed to advance in any way either our theoretical or practical knowledge of those states of the brain mechanism which are due to alterations in its nutrition.
Much of the unsatisfactory state of our knowledge on this head is due to the grouping together of the physiological anæmia of sleep and the pathological anæmia with which the physician has to deal. The anæmia of the brain in a sleeping person is probably a secondary factor; it ensues after the person falls asleep, the first step in the latter process being probably an altered dynamic state of the brain which lessens the requirements of that organ for blood. This can be readily demonstrated in the case of infants whose anterior fontanelle has not yet closed. In deep sleep the fontanelle is deeply sunken in, but this sinking in does not occur simultaneously with the child's falling asleep, but shortly thereafter. On the other hand, the fontanelle does not rise simultaneously with the child's awakening, unless it cry, which adds a disturbing factor. There are a number of other facts which show that while a comparison between the sleeping state and cerebral anæmia may be made for the purposes of theoretical discussion, yet there are many important points in which they are at variance. To illustrate this I need but refer to the fact that in deep sleep the pupils are in a state of immobility and pinhole contraction,14 while in chronic cerebral anæmia of young persons a dilated and mobile pupil is the commoner condition. In acutely-produced cerebral anæmia an initial contraction has been noted, but it is not then persistent.
14 Inability to counterfeit this feature is one of the most reliable tests of simulation, and served to convince me that in the well-known case of a colored cadet, who was tried by a court-martial on charges involving simulation, the latter was proven. There are persons who can voluntarily contract the pupils, but as they are compelled to innervate all the muscles supplied by the third pair, in so doing they are compelled to converge the optic axes—an act which does not take place in sleep.
One of the main reasons of our imperfect knowledge of the nutritive disorders of the brain is the unsatisfactory state of their post-mortem evidence. Little has been learned in this field, except in those extreme cases where the suddenness and intensity of the circulatory catastrophe were sufficient to prove fatal. Even where all observations made during life justify us in supposing that the amount of blood sent to the brain is small, that the velocity of its current is reduced, and its quantity poor, the autopsy may reveal conditions apparently conflicting with the supposition based on ante-mortem observations. This is amply illustrated by the experience of alienists who have studied the relation between nutritive states of the brain and certain forms of insanity. It is generally held that in so far as the antithetical forms of mental disorder known as anæmia and melancholia can be connected with nutritive disorders, the former is indicative of hyperæmia and the latter of anæmia. A number of facts can be adduced in support of this view, particularly as regards the latter condition. It is found, however, in some examinations made of the brains of patients dying melancholic that the brain is apparently hyperæmic; the length of time elapsing before an autopsy is made, the form of somatic disease with which the patient dies, the position of the [p. 776] body after death,—all these may play a part in the production of cerebral injections which do not correctly indicate the condition of the brain as it existed prior to the moribund period, and when the symptoms of supposed anæmia or hyperæmia could be satisfactorily differentiated.
ETIOLOGY.—The best studied form of cerebral anæmia is that ensuing after extensive hemorrhages or from compression and ligature of either of the common carotid arteries.15 In the latter case symptoms are produced which are in harmony with the doctrine of localization, and permit us to form a conception of the mode in which a diminution of the cerebral blood-supply influences the functions of the brain. The chief symptoms are noted on the side of the body opposite to that on which the common carotid artery is tied. Thus if the left artery be tied, there is at first felt a tingling or pricking feeling on the right half of the body; this is followed by a warm, sometimes a cold, and ultimately by a numb, feeling. This sensory disturbance may become of what might be called the capsular type—that is, a complete hemianæsthesia; but at first it is distinctly like that which is found with cortical and subcortical disease, being limited to the muscular sense and the intelligent contact-perceptions of objects, the æsthesiometer showing but little or no impairment of the cutaneous space-sense. With the loss of muscular sense the movements become heavy, and later true paresis may appear with perhaps total anæsthesia. Aphasia is sometimes noted in such cases, and, in obedience to the predominant location of the speech-faculty in the left side of the brain, is rarely if ever found16 when the right common carotid artery is the one ligated.
15 As the conditions of the cerebral circulation resulting from surgical and other rare causes are not apt to be brought to the physician's attention separately from conditions of more immediate importance, their symptoms are discussed in the etiological portion of this section in order to avoid complicating the semeiological picture of cerebral anæmia of every-day experience. For similar reasons the anomalies of the cerebral circulation of an embolic and thrombotic nature, and those associated with eclampsia and epilepsy, are not mentioned in this connection, as their full discussion properly belongs to other portions of this work.
16 I am unaware of the record of any case where aphasia occurred with ligature of the right common carotid artery. There is a singular observation by Hagen-Torn of permanent paralysis of the right hypoglossal nerve after such an operation, but the report to which I have access does not state whether this may not have been due to some peripheral involvement of that nerve.
In this series of symptomatic sequelæ it is seen that the functional manifestations of the highest centres are the first to be involved, and this establishes that of all parts of the cerebrum the cortex and subcortical tracts are the more vulnerable to the influence of a deficient blood-supply.17 As we shall see, it is precisely to the insufficient nutrition of these parts that the more important symptoms of the cerebral anæmia of ordinary practice are attributable.
17 To this there is an apparent exception: when blindness occurs in consequence of ligature of one carotid artery, it is monocular and limited to the side of the ligation. The visual disturbance of cortical and subcortical disease is bilateral, being of the character known as hemianopsic. The blindness due to tying of the carotid is, however, not due to cerebral, but to retinal, anæmia, and its monocular character does not therefore invalidate the observation in the text. Litten and Hirschberg (Berliner klinische Wochenshrift, 1885, No. 20) found complete bilateral amaurosis in a chlorotic girl of fifteen, and on ophthalmoscopic examination the peripheral origin of the blindness was conclusively proven by the existence of an exquisite choked disc. Both the morbid ophthalmoscopic appearance and the amaurosis disappeared under tonic regimen. It is well to recollect that choked disc may occur in chlorosis, and thus be perhaps erroneously attributed to a coexisting hysteria, as was done in some cases at least by Rosenthal in his textbook.[p. 777]
With bilateral ligature18 of the primary carotids—and this applies in the main to cerebral anæmia from profuse hemorrhages or sudden changes in the blood-pressure, such as occur in enteric affections, ruptures of aneurisms, in obstetric practice, and after brusque tapping for ascites—the same phenomena noted with unilateral compression are observed on both sides of the body, and usually in slighter intensity. In addition, there is a profound and characteristic disturbance of respiration; a cold sweat breaks out; the senses of sight and hearing become greatly impaired or perverted; the mind becomes clouded, consciousness blurred; complete syncope may ensue, and pass to a fatal termination. In other cases vertigo preponderates or vomiting, and finally convulsions appear. It would seem that the respiratory centre exceeds even the cortex in susceptibility to the evil influence of anæmia. It differs from them in two features: firstly, it appears to require bilateral involvement of the brain for its production; secondly, although the respiratory disturbance precedes that of the higher cerebral functions, it does not become as intense, for at a time when the intellectual functions are abolished, as in anæmic coma and syncope, the respiratory function, however disturbed, is in most cases sufficiently well carried on to bear the organism safely through the crisis. The disturbance is marked by the following characters: The respiration is at first deep and sighing, perhaps frequent; it later becomes slow, and is associated with a subjective sense of oppression; the patient feels as if he could not fill his lungs properly; there is an unsatisfied sensation, as if a deeper breath should be taken, and when, in obedience to this subjective need, a full deep breath is taken, the patient feels as if he had stopped short of completing the act, and remains as unsatisfied as before.19 Yawning and moaning are often accompaniments of this symptom.20 As we shall see, these signs are often among the chief sources of complaint in the less grave forms of anæmia of every-day experience. In the serious condition before us the Cheyne-Stokes phenomena may follow.
18 I exclude the observations of Flemming, Hammond, and Corning on carotid compression by external pressure, owing to the difficulty of determining whether or no, and what, other important structures are compressed at the same time.
19 The occurrence of this functional respiratory trouble is a feature of toxic as well as of anæmic irritation of the respiratory centre; it is accordingly found in cases of profound alcoholic poisoning.
20 It is somewhat difficult to understand why in cases of anæmia induced in both carotid districts the symptoms of anæmia should be marked in the functions of that part of the brain-axis which through the basilar trunk derives its blood from the vertebral arteries. Here the blood-current must necessarily be increased. That the disturbance of breathing, the yawning, and the sighing belong to the group of irritative symptoms due to anæmia is in harmony with the general physiological law which is illustrated in the initial contraction of the pupil, which is found in experimental cerebral anæmia. Observations on anæmia of the brain-axis are too few, and, so far as noted, have been so rapidly fatal that it is not possible to derive from them any facts bearing on the physiological reactions of the respiratory centre to high-graded anæmia. One of the curiosities of medicine appertaining to this subject is the observation recorded in Virchow's Archiv, lxix. p. 93, of the case of a man who had fractured the base of the skull in its posterior fossa, and, the basilar artery becoming caught and pinched in the crack, death occurred rapidly with all the signs of cerebral anæmia, verified by the post-mortem appearances.
Anæmia of the brain may develop at any period of life, not excluding the intra-uterine period. Kundrat and Binswanger regard the deformity of the brain known as porencephaly as the result of an anæmic (non-embolic) necrosis of brain-substance, developed either in the fœtal or the [p. 778] infantile period. The occasional symmetry of the deformity is in favor of this view. That there are other conditions of cerebral malnutrition,21 masking themselves in defective development and imperfect isolation of the conducting tracts, and that the consequent differing rate of maturation of these tracts has some relation to the absence or presence of a predisposition to chorea and other disturbances of nervous equilibrium so common at this period of life, I regard as at least probable. But it is at the period of puberty that we encounter the most important discrepancies between the requirements of brain-nutrition and the furnished blood-supply. The disposition to uncomplicated cerebral anæmia is greatest at this period of life and in the female sex. Beneke22 has shown that as the human being grows the arteries, which in children are very large in proportion to the length of the body, get to be relatively smaller and smaller toward the period of puberty—that after this period they widen to again attain a large circumference at old age. There is thus added to the other and more obscure factors which may determine general anæmia at puberty a diminished calibre of the arteries in both sexes. To some extent the disadvantageous influence of (relatively) narrow vascular channels may be overcome by increased cardiac action, and the almost sudden increase in size of the heart about this period is probably the result of the demand made upon its compensatory power. But, as we learn from the same observer that the female heart remains relatively as well as absolutely smaller than that of the male, we can understand why the female should be less able to overcome the pubescent disposition to cerebral (and general) anæmia than the male. Menstruation, which in a certain proportion of girls scarcely maintains the semblance of a physiological process, acting rather as a drain than a functional discharge, is added to the anæmia-producing factors. It is among those who marry in the ensuing condition, who bring forth child after child in rapid succession, perhaps, in addition, flooding considerably at each confinement, that we find the classical symptoms of chronic cerebral anæmia developed.
21 I have found in three children under fourteen months of age, who died with symptoms not unlike those of slowly-developed tubercular meningitis, including convulsions, strabismus, temperature disturbance (slight), and terminal coma, without nuchal contracture or pupillary anomalies, a remarkably anæmic brain. The sulci gaped; there were few or no puncta vasculosa; the cortex extremely pale, and the white substance almost bluish-white. On attempting to harden the brain of the youngest of these children, using every precaution and a sufficient number of sets of hardening fluids, including the chromic salts and alcohol, I found that small cavities formed in the cortex, varying from the scarcely visible to two-thirds of a millimeter in diameter. Their existence were demonstrable the day after the death and almost immediate autopsy performed in this case. There had been no antecedent disease in any one of these cases; the children had been lethargic, inactive, and the oldest had made no attempt to walk or talk. There was no morphological or quantitative defect in cerebral or cranial development, and microscopic examination showed that the cavities were not perivascular. In all these cases the patients belonged to the tenement-house population.
22 An excellent abstract of Beneke's original monograph, by N. A. P. Bowditch, will be found in volume i. Transactions of the Massachusetts Medico-Legal Society.
In the male sex the period of adolescence has not the same profound influence in producing cerebral anæmia that it has in females. To some extent, however, habitual self-abuse and early sexual excess of the former produce results similar to those occurring in consequence of perverted physiological processes in the latter. Many of the symptoms presented by the inveterate masturbator are probably due to cerebral anæmia; there [p. 779] are, however, in his case and in that of the early libertine certain vaso-motor complications frequently present which render the clinical picture a mixed one.23 In addition, abuse of the sexual apparatus has a direct—probably dynamic and impalpable—exhausting effect on the central nervous apparatus.
23 Kiernan of Chicago has described peculiar trophic disturbances—dermato-neuroses, color-changes of the hair, etc.—in a case of masturbatory mental trouble associated with marked anæmia. The patient whenever he flushed up heard a noise as of a pistol snapped near the mastoid region. In the case of a young man of eighteen who—the pampered son of wealthy parents—became his own master at fifteen, and had at that age indulged in sexual orgies which were continued to an almost incredible extent, it was found that he gradually lost his memory, and on one occasion had a violent epileptiform attack. During his convalescence from the stuporous state which followed it was noted that the patient was quite bright in the morning, but that after he had been up a while he relapsed into a state of apathy, with amnesia, which, decreasing in intensity from week to week, was eventually only noted toward evening, and finally disappeared, the case terminating in complete recovery.
In the vast majority of cases anæmia of the brain is but a part of general anæmia, and all conditions which tend to impoverish the character of the blood and to reduce the rapidity of movement and fulness of the cerebral blood-column are apt to be associated with signs of cerebral malnutrition. As early an observer as Addison noticed the wandering of the mind in pernicious anæmia, in which disorder anæmia and wasting of the brain have been found post-mortem. In two cases of extreme chlorosis I heard the sound known as the cephalic soufflé with great distinctness;24 this sound, when the other morbid conditions that may lead to it can be excluded, indicates a high degree of anæmia. Both patients were somnolent and subject to fainting-spells. In leucocythæmia a rambling delirium is not infrequently noted toward the close of the patient's life, and the habitual sadness and depression of many leukæmic patients is due, as are also certain phases of melancholia, to cerebral malnutrition. In some stages of most, and in all stages of some, forms of renal disease the conditions of cerebral anæmia are present; and it is reasonable to attribute to it some share in the production of the head symptoms of Bright's disease; but here, as in cases of cardiac disease, symptoms due to other influences—uræmia in the former, and insufficient oxygenation of the blood in the latter instance—obscure or conceal those due to the anæmia strictly speaking.
24 When an anæmic murmur at the base of the heart coexists with the cephalic soufflé, the latter may be regarded as an evidence of anæmia; but where the former is absent—that is, when the cephalic soufflé is an isolated, independent symptom—there is reason to suspect the existence of a tumor or some other cause of compression of the carotid artery at or after its entry into the cranium. In one of the cases referred to in the text, pressing on one or the other carotid produced numbness and tingling in the opposite arm, leg, and cheek. Similar observations were made by Tripier (Revue de Médecine, March, 1881), who strenuously maintains the existence of the cephalic soufflé in the adult, against Henry Roger, and in consonance with the observations of Fisher and Whitney. In the last-mentioned case of mine the sound could be heard a distance from the head.
All exhausting diseases, many febrile affections, notably typhoid, starvation from any cause, and exhausting discharges, may produce cerebral anæmia. Under the latter head belong the diarrhœal affections of childhood, which not infrequently lead to an aggravated form of anæmia of the brain known as hydrocephaloid. In addition to the provoking causes of cerebral anæmia there are certain accessory ones: prominent among these is the upright position and sudden rising. The reason of this influence is self-evident, as is also the fact that it is most apt to manifest [p. 780] itself in cases of cardiac enfeeblement. Many a convalescent from an exhausting fever or other disease has on rising from bed fainted; some have fallen dead from cerebral anæmia already existing, but fatally intensified by this sudden change of position. A number of cases are on record by Abercrombie, Forbes Winslow, J. G. Kiernan, and others where persons manifested the symptoms of cerebral anæmia only when in the upright position and even in lying on one side or the other; these are, however, far rarer than is claimed by some later writers.
The purest form of acute cerebral anæmia, aside from that produced by surgical interference with the cerebral circulation or extensive hemorrhages, is that induced by mental influences, such as fright, a disagreeable odor, or a disgusting or harrowing spectacle. Some persons, not suffering from general anæmia or any diseased condition thus far mentioned, on experiencing the emotional influences named will be observed to turn pale, to breathe heavily, and either sink into a chair or fall on the floor partly or entirely unconscious. They are then suffering from a spasm of the cerebral arteries resulting in acute and high-graded cerebral anæmia or syncope. This condition is marked by some of the symptoms previously mentioned as occurring with bilateral ligature of the carotids: thus, the feeling of oppression on the chest, vertigo, heaviness of the limbs, nausea, and vomiting are characteristic; a cold sweat breaks out on the forehead; the visual field becomes darkened; and hearing is rendered difficult by the tinnitus.25 The pulse is small and of low tension, but regular.
25 Most authors claim that the sense of hearing is blunted, as that of vision is. This is so in some, but certainly not in a large number of other cases. I have now under observation a girl whose physical conformation—her neck is very long and her shoulders tapering—and extreme susceptibility combine to favor the occurrence of syncope. She faints in my office whenever an examination is made, even though it be entirely verbal; and after recovering frequently lies down to answer by deputy, as experience has shown her that she is less likely to faint in this position. I have repeatedly satisfied myself from her subsequent statements that she heard what was said, while she appeared to be quite unconscious and “saw everything black or through a cloud.” It is not improbable that the impressions which most writers on the subject convey were derived from the experience of novices in fainting; these, in the alarm and anxiety of their condition, and confused by the tinnitus, might well fail to hear what the bystanders said, particularly as on many such occasions the fainting person is apt to be surrounded by a confused Babel of tongues. While the auditory nerve is as sensitive to the irritative influence of anæmia as any, and there is a case of a boy on record (Abercrombie) who could only hear well when lying down, and was deaf when he stood up, yet the conclusions of other authorities who have studied the subject would lead one to think that there are individual differences in this respect. How often does not the dying person, after feeling for the hands of a relative whom he cannot see, converse with him responsively! And how much need is there not of the humane physician to remember that the sense of hearing is the last intellectual sense to die, lest he speak unguardedly at the bedside!
As a rule, the subjects of simple syncope recover, the horizontal position, which is assumed perforce in most cases, carrying with it the chief remedial influence—namely, the facilitating of the access of a fuller blood-supply to the brain. While, as stated, the tendency to syncope may exist in healthy non-anæmic individuals, it is far more common with those who suffer either from chronic cerebral anæmia or from many of its predisposing conditions. The arterial spasm which causes syncope is an exaggeration of what occurs within physiological limits26 in all persons [p. 781] when subjected to emotional or violent external impressions of any kind.
26 It has been experimentally determined by Istomanow (St. Petersburg Dissertation, 1885) in persons whose brain-surface had become partially accessible to observation through traumatic causes that pain, warmth, pleasant smells, and sweet tastes cause a contraction of the cerebral vessels and a sinking in of the brain-surface, while tickling, unpleasant odors, bitter and sour tastes, produce the reverse condition; that is, bulging of the brain-surface and increased injection of the vessels. Istomanow's results are verified by other observations, particularly by the fact that with the latter class of impressions there is an increase in the general blood-pressure, with sinking of the surface-temperature, and, as measured by Mosso's method, decrease in the volume of the extremities. While there is a general correspondence between these observations and clinical experience, there are a few unexplained discrepancies.
MORBID ANATOMY.—In those severe cases of cerebral anæmia which terminate fatally the entire brain appears bloodless. Since the color of this organ under ordinary circumstances is in great part due to the vascular injection, it appears very different when this admixture is lessened or removed. Then the gray substance, instead of presenting a reddish-gray tint, is of a pale buff color in infants, and a pale gray in adults who have died of acute or intense cerebral anæmia. The white substance exhibits few or no puncta vasculosa, and there is no indication of the faint rosy tinge which even the white substance has in the normal brain. All these appearances can be imitated in the brain of an animal that is bled to death; they are also met with in those who have died of inanition, particularly in cases of melancholia attonita, the subjects of which had long refused food. Most writers state that the ventricular and subarachnoid fluids are increased in amount,27 and that the sulci appear wider in anæmic than in normal brains. That these fluids must be increased to compensate for the diminished blood-amount is evident. But it is not unlikely that exaggerated estimates of the increase have been made; and for this reason: Since the meninges and choroid plexuses are comparatively bloodless, the cerebro-spinal fluids are more likely to present themselves free from that admixture of blood which renders the obtaining and measuring of their quantity so difficult under ordinary circumstances. The gaping of the sulci has not been verified by me either in animals that had been bled to death or in cases of cerebral anæmia in rapidly-fatal atonic and phthisical melancholia. In protracted cases of this nature I frequently found gaping of the sulci: here, from the nature of the cases, the patients dying either from self-starvation, imperfect assimilation, or wasting diseases, the occurrence of a certain amount of atrophy of the brain-substance proper could not be excluded.28
27 Hammond, on the other hand (Diseases of the Nervous System, p. 77), has the ventricles generally empty.
28 Up to within a very short time ago it would have appeared heretical to claim that any considerable amount of brain-wasting could ensue from starvation alone, as the oft-cited experiments of Chossat seemed to show that mammals, birds, reptiles, and amphibians lose in body-weight while being starved, but that the brain-weight is not disturbed to any appreciable extent. Six years ago I examined the brain of a tortoise (Cestudo Virginica) which had starved fully a year through ignorance of the keeper of an aquarium. The atrophy of the brain was so marked that it had undergone demonstrable changes of contour. Since then Rosenbach (Archiv für Psychiatrie, xvi. p. 276) has demonstrated that brain-wasting and other changes do occur in starved rabbits.
With protracted fevers accompanied by inanition—and this applies particularly to the later period of typhoid fever—a condition of cerebral anæmia is found which is of the greatest interest to the clinician. The brain as a whole is bloodless; there may or may not be apparently hyperæmic districts, but the injection is altogether on the surface; the consistency of the brain is considerably diminished, and this organ is often [p. 782] distinctly œdematous. In exceptional cases the œdema is so great that softening results, the white substance becoming fluidified at the cortical limit near the base of the sulci and at the ventricular walls. This is due perhaps as much to post-mortem maceration as to pre-mortem œdema, but that the latter condition exists is shown by the condition of the brain as a whole. The loss of memory, the difficulty of correlating the past and present, the rambling, incoherent conversation, and anenergic stupor observed in the decline of typhoid and other exhausting fevers, especially in older subjects, may be properly attributed to the injurious effects of post-febrile anæmia and anæmic œdema of the brain. Aside from fevers, œdema is apt to be associated with anæmia where venous stagnation is a complicating feature; consequently, it is not uncommon with certain uncompensated valvular lesions, emphysema, and other chronic pulmonic troubles.
Positive observations of tissue-changes from simple cerebral anæmia have not been recorded. Even in extreme cases the essential nervous structures, the ganglionic bodies, the nerve-fibres, their sheaths, and the neuroglia, appear healthy. The adventitial and pericellular spaces are sometimes enlarged, and variations in the number and distribution of the free nuclei of the neuroglia and the border bodies of the periadventitial districts have been observed by me, but not with such constancy as to justify more than this mere mention. In his researches on starvation Rosenbach found the brain œdematous and the ventricles dilated; there were also microscopical changes which indicated a profound disturbance of nutrition; the large cells of the anterior spinal horn and cerebellum had lost their transparency, being in a condition resembling cloudy swelling. The neuroglia appeared to be in a similar condition as that of nerve-cells. Singular as it may appear on first sight, the capillaries were found crowded with blood-corpuscles, and there were many evidences of diapedesis of such. This may indicate a passive accumulation due to deficient cardiac and vascular contractility. The changes, as a whole, were not unlike those found in myelitis,29 except in so far as no actual inflammatory signs were present.
29 Several distinguished neurologists, notably Westphal, who were present when Rosenbach presented his conclusions, were unable to recognize so profound a deviation from the normal structural conditions as he claimed (Archiv für Psychiatrie, xvi. p. 279).
SYMPTOMS.—The clinical phenomena of acute cerebral anæmia have been in the main related in connection with the etiology of this disorder. We shall now proceed to detail those which occur with cases more likely to engage the attention of the practitioner either on account of their gravity or protracted duration.
Uncomplicated Chronic Cerebral Anæmia of Adolescents and Adults.—This condition is one of the common manifestations of general anæmia. Most anæmic persons are languid, drowsy, suffer from insomnia, tinnitus aurium, and other signs of imperfect cerebral irrigation. In some these troubles become alarmingly prominent and may approach the confines of mental derangement. This is particularly apt to occur with women who have borne and nursed a large number of children. In addition to the typical signs of cerebral anæmia, they exhibit depression, may suffer from hallucinations, and even become afflicted with lachrymose or suicidal melancholia (insanity of lactation of the somato-etiological school). [p. 783] Depression of the mental functions is the most constant symptom of cerebral anæmia, and the one which most frequently directs the physician's attention to its existence; its subjects appear mentally blunted, the apperceptive powers are diminished, and it is difficult for the patient to interest himself in anything, or when interested to keep up a mental effort—that is, his attention—any length of time. In more severe grades of the trouble the patients become somnolent in the daytime. Contrary to what those who regard sleep as essentially due to cerebral anæmia might expect, sleep is disturbed, and the patient is wakeful or suffers from vivid and frightful dreams, or even deliria. Others pass a quiet night, but are rather in a trance-like condition than a healthy sleep. Lethargic as the cerebral anæmic person is on the whole, and unable as he feels himself to exert his will-power (aboulia), yet he is often irritable, perverse, and petulant in consequence of that morbid excitability which is a universal attribute of the overworked or imperfectly nourished nerve-element. The younger the patient the more likely is the condition apt to impress one as a stupor, while with older patients irritability is more prominent. In the former the obtuseness is often rapidly overcome when the patient assumes the horizontal position.
It was supposed by Abercrombie that an acute exacerbation of cerebral anæmia of this form in weakly and aged individuals might terminate in death. This condition corresponded to the so-called serous apoplexy of the old writers. With increasing accuracy in our autopsies this condition is more and more rarely recorded, although the possibility of its occurrence as a pathological rarity cannot be denied. As a rule, the chronic form of cerebral anæmia when it terminates fatally, which is exceptional, is marked by a deepening coma and gradual extinction of the vital processes, the Cheyne-Stokes phenomenon preceding this.
Patients suffering from chronic cerebral anæmia are afflicted with morbid irritability of the optic and auditory nerves. Loud sounds and bright lights are very annoying to them. Roaring, buzzing, and beating sounds in the ear are common, and scintillations, muscæ volitantes, and temporary darkening of the visual field—particularly noticed when the head is suddenly raised—are complained of in all cases. It is often found that the tinnitus disappears and the hearing power improves on assuming the horizontal position.
Headache of greater or less severity is found in the majority of cases: it is more severe in the rapidly-developed forms, and I have found it to be complained of in agonizing intensity by women who had risen from childbed and who had flooded considerably. As a rule, the headache, whether severe or mild, is symmetrical and verticalar, in some cases associated with an ache subjectively appearing as if it extended to the back of the orbit. It is remarkable for its constancy, and its exacerbations are often complicated with vertigo and nausea, so that it is not infrequently interpreted as a reflex evidence of gastric disorder. A stitch-like feeling, located in both temples, is often associated with it.
Occasionally sufferers from chronic cerebral anæmia experience seizures, or rather exacerbations, of their disorder which approach in character, while not equalling in degree, an attack of syncope. Whether in bed or in a chair, they then feel as if their limbs were of lead; they deem that they cannot stir hand or foot; the other symptoms related are [p. 784] aggravated; they yawn and breathe deeply, but hear all that is said by those near them, and do not lose consciousness. They express themselves as feeling as if everything around them were about to pass away. One of my patients would frequently find that if this condition overtook her while lying on one side, that side would remain numb for some time and be the seat of a tingling sensation which disappeared on the parts being rubbed. The same was noticed when she awoke in the morning in a similar position. To what extent these features were due to the general anæmia is doubtful. As previously stated, true syncope occurs in chronic cerebral anæmia, but much less frequently in those subjects of this disorder who have reached middle life than in adolescents.
The radial pulse in cerebral anæmia does not necessarily show the anæmic character; not infrequently the general blood-pressure is increased at the onset of the acute form, and if long continued this may be followed by a decrease of the same. The pulse-character may therefore vary greatly in frequency, resistance, and fulness. In protracted cases it is soft, easily compressible, and rapid.
It is not uncommon to find indications of a slight unilateral preponderance of the signs of cerebral anæmia. In one case which terminated in recovery, and was otherwise pure, vertigo was not produced on turning from the left to the right, but it was produced to a distressing degree on turning in the opposite direction; in a second, equally typical, there was for a long time a subjective sensation of falling over toward the right side.
There appears to be much less constancy in the relationship of the deficient blood-supply to the severity of the symptoms than is usually supposed. Much depends upon the time of life at which the disorder develops: a brain that has acquired stability through education and exercise is less vulnerable to the influence of general anæmia than one that has not. The nerve-centres appear, to some extent at least, to regulate their own blood-supply; and whether it be through a change in the blood-current rapidity or some other factor neutralizing the evil effects of the intrinsically inferior quality of the blood, we must attribute to the self-regulating nutrition power of the brain the not uncommon phenomena of an active mind in an anæmic body. And where the general anæmia reaches so high a degree as to involve the brain, under such circumstances we find that irritability to sensory impressions and fretfulness are more prominent than the lethargy and indifference which characterize the juvenile chlorotic form. Although this distinction is less marked between these two classes in regard to acutely-produced anæmia, yet it is observable even there. If in a youth or girl while undergoing phlebotomy cerebral anæmia were to reach such a degree as to cause subjective sounds, they would either approach or fall into a faint; but Leuret, the distinguished cerebral anatomist, while being subjected to the same procedure, hearing a hissing sound, did not lose consciousness, but complained that some one must have upset a bottle of acid on a marble table in the same room, as he supposed he was hearing the sound of effervescence thus produced.
Much, too, appears to depend on dynamic and other thus far undiscovered intrinsic conditions of the brain-tissue itself, irrespective of the mere amount and rapidity of the blood-current. If the subject be exposed to wasting diseases, to blood-poisons, or to vicissitudes of temperature and [p. 785] to physical exhaustion in addition to the causes producing cerebral malnutrition, deliria of a cortical nature are more apt to characterize the case than in simple anæmia. These are known as the deliria of inanition, and present themselves under two forms. The first has been frequently observed in sailors, travellers, and others who have undergone starvation in exposed situations, and is tinctured by the psychical influences incident to such a condition. Just as the Greeley survivors at Cape Sabine, when reduced to their miserable rations of seal-skin boot-leather and shrimps, entertained each other with the enumeration of imaginary culinary luxuries, so others who have suffered in the same way declaim about gorgeous banquets in the midst of a howling wilderness, or, as occurred to a miner who lost his way in Idaho a few winters ago, experienced hallucinatory visions of houses, kitchen utensils, and persons with baskets of provisions. In others the terror of the situation leads to the development of rambling and incoherent delusions of persecution.
The second form, regarded as a variety of starvation delirium, is found in the post-febrile periods of typhoid and other exhausting fevers. In aged persons it may even develop shortly after the onset of the disease. It is usually unsystematized, of a depressive cast, and may be associated with a condition resembling melancholia agitata. In a small proportion of cases insanity of the ordinary types, but more commonly of the special kinds comprised in the group of post-febrile insanity, develops from the anæmic fever delirium as its starting-point.
The spurious hydrocephalus (hydrocephaloid, hydrencephaloid) of Marshall Hall and Abercrombie, referred to in the section on Etiology, is an important condition for the diagnostician to recognize. A child suffering from this disorder presents many symptoms which are customarily regarded as characteristic of tubercular meningitis or of chronic hydrocephalus; thus the pupils are narrow—sometimes unequal;30 there is strabismus, and there may be even nuchal opisthotonos, while the somnolent state in which the little patient usually lies may deepen into a true coma, in which the pupils are dilated, do not react to light, nor do the eyelids close when the cornea is touched. Ominous as this state appears, it may be completely recovered from under stimulating and restorative treatment. On inquiry it is found that the symptoms above mentioned were preceded by cholera infantum or some other exhausting complaint, such as a dysentery or diarrhœa, and that the somnolent condition in which infants are often found toward the close of such complaints passed gradually into the more serious condition described.31 The infants thus affected do not, however, sleep as healthy children do, but moan and cry, while apparently unconscious of their surroundings. The surface of the body is cool and pale; the pulse and respiration are normal, except in the comatose period, but the former is easily compressible. The chief points distinguishing hydrocephaloid from true hydrocephalus and other diseases associated with similar symptoms are the following: 1st, There is no rise of temperature; 2d, the pupils are equal; 3d, the fontanelle is sunken in; 4th, the pulse and respiration, with the exception stated, are natural; 5th, there is an [p. 786] antecedent history of an exhausting abdominal disorder; 6th, also a facial appearance characteristic of the latter.
30 This is not admitted by most writers, but does occur exceptionally.
31 It should not be forgotten, however, that very similar symptoms occur after cholera infantum, with a much graver pathological condition—namely, marantic thrombosis of the sinuses.
One of the gravest and rarest forms of cerebral anæmia is one which occurs as a result of extreme general anæmia in very young infants. In a remarkable case which I have had an opportunity of studying, the abolition of certain cerebral functions reached such a degree that the opinion of a number of physicians was in favor of tubercular meningitis.32 There was at the time of my examination complete extremity hemiplegia, and there had been conjugated deviation, restlessness in sleep, and dulness in the waking hours: all these symptoms except the hemiplegia disappeared whenever a more assimilable and nutritious food was used than the one previously employed. On one occasion there were evidences of disturbed vaso-motor innervation; on several, convulsive movements. This history, associated with ordinary evidences of general anæmia, covered a period of eighteen months, without the slightest abnormality of temperature being noted or discoverable during that period. The mucous surfaces of this child were almost colorless, certainly without any indication of the normal tinge; the mother had nursed it, and her milk had been found to possess scarcely any nutritive value. The case terminated fatally at the age of twenty months.
32 It was stated by an experienced practitioner that death occurred with unmistakable symptoms of tubercular meningitis. Certainly, the absence of temperature disturbance at the time of the hemiplegic and other exacerbations, as well as other important features for a period exceeding a year, shows that whatever favorable soil the earlier condition may have furnished for the secondary development of such or other gross structural disease, tubercular meningitis did not exist at the time; while the absence of pupillary and optic-nerve symptoms, as well as the rapid changes from day to day or week to week under dietetic treatment, militate against the assumption of any other organic affection incident to childhood.
Partial Cerebral Anæmia.—Most writers on cerebral anæmia discuss a number of varieties of partial cerebral anæmia as distinguished from the acute and chronic general forms. Some of the conditions thus described properly appertain to the angio-spastic form of hemicrania, others to epilepsy, and the majority to circulatory disturbances dependent on arterial disease. Aside from the partial cerebral anæmia resulting from surgical causes, I am acquainted with but one evidence of limited cerebral anæmia which can be regarded as independent of the neuroses or of organic disease, and that is the scintillating scotoma. This symptom, in the only case in which I observed it, occurred in a medical student, accompanied by pallor and nausea in consequence of the disgust produced in him by the combined odors of a dissecting-room and of a neighboring varnish-factory. The totally blind area of the visual field was strictly hemianopsic in distribution and bounded by a colored zone scintillating, to use the sufferer's words, like an aurora borealis. The attack, probably protracted by his great alarm at being blind in one-half of the visual field, lasted three hours. As the cause in this case was a psychical impression and accompanied by the ordinary signs of that fainting which is not an uncommon occurrence in the dissecting-room; as, furthermore, the individual in question never had a headache except in connection with febrile affections, and then in the lightest form, and is neither neurotic himself nor has a neurotic ancestry or relatives,—I regard it as the result of a simple arterial spasm intensified in the visual field of [p. 787] one hemisphere, analogous to the more general spasm of ordinary syncope.33
33 It may be remembered that Wollaston had scintillating scotomata, and that after his death a small focus of softening was found in the one visual field. Ordinarily, this disturbance is associated with hemicrania.
DIAGNOSIS.—There is so little difficulty in recognizing the nature of those cases of acute cerebral anæmia which depend on recognizable anæmia-producing causes that it is unnecessary to point out their special diagnostic features. With regard to chronic cerebral anæmia, and its differentiation from other circulatory brain disorders, I refer to the last article. In this place it will be necessary only to point to some of the symptoms which, individually considered, are found in other disorders, and may therefore be misinterpreted. The chief of these is vertigo, which, as already stated, being associated with nausea, and even vomiting, is not infrequently confounded with stomachic vertigo, while the opposite error is also, though less frequently, fallen into. The chief differential points are—that stomachic vertigo is relieved by vomiting, and anæmic vertigo is not; that the former is rather episodical, the latter more continuous; that in the free intervals of the former, while there may be some dulness, there is not the lethargy found with anæmia; that the headache with the former is either over the eyes or occipital, and most intense after the passage of a vertiginous seizure, while anæmic headache is verticalar or general, and not subject to marked momentary changes. It is unnecessary to indicate here the positive evidences of gastric disorder which are always discoverable in persons suffering from stomachic vertigo; but it is also to be borne in mind that such disorder is frequently associated with the conditions underlying general and cerebral anæmia, particularly in the prodromal period of some pulmonary troubles.
There are a number of organic affections of the brain which are in their early periods associated with symptoms which are in a superficial way like those of cerebral anæmia. As a rule, focal or other pathognomonic signs are present which render the exclusion of a purely nutritive disorder easy; but with some tumors, as is generally admitted, these signs may be absent. It is not difficult to understand why a tumor not destructive to important brain-centres, nor growing sufficiently rapid to produce brain-pressure, yet rapidly enough to compress the blood-channels, may produce symptoms like those of simple cerebral anæmia. It is claimed that with such a tumor the symptoms are aggravated on the patient's lying down, while in simple anæmia they are ameliorated.34 The latter proposition holds good as a general rule; as to the former, I have some doubts. Not even the ophthalmoscope, although of unquestionable value in ascertaining the nature of so many organic conditions of the brain and its appendages, can be absolutely relied on in this field. Until quite recently, optic neuritis, if associated with cerebral symptoms, was regarded as satisfactory proof that the latter depended on organic disease; but within the year it has been shown by Juler35 that it may occur in simple [p. 788] cerebral anæmia, and both the latter and the associated condition of the optic nerve be recovered from.
34 The increased flow of blood to the brain in anæmia is not always momentarily remedial: if, for example, the patient stoop down, he flushes more easily than a normal person, and suffers more than the latter. The same is observed with regard to stimulants.
35 British Medical Journal, Jan. 30, 1886. In the case reported suppression of the catamenia is spoken of, as well as the fact that treatment was directed to the menstrual disturbance. It is not evident from the brief report at my disposal whether the suspension of the menstrual flow was symptomatic of general anæmia or of a local disturbance. Optic neuritis has been recorded as having been present in a large number of cases with no other assignable cause than a uterine disorder. As previously stated, Hirschberg and Litten found choked disc under like circumstances.
The claim of Hammond and Vance that ordinary anæmia of the brain may be recognized through the ophthalmoscope is almost unanimously disputed by experienced ophthalmoscopists, nor is it unreservedly endorsed by any authority of weight among neurologists. That there may be color-differences to indicate anæmia is, however, not impossible; and the fact that a concentric limitation of the visual field sometimes occurs should not be forgotten. It is distinguished from that found with organic diseases by its variability through the day and in different positions of the body.
TREATMENT.—Chronic as well as acute cerebral anæmia, dependent on general anæmia, usually requires no other medicinal treatment than that rendered necessary by the general anæmic state of which it is a part. This has been discussed at length in the third volume of this work: it remains to speak of certain special precautions and procedures rendered necessary by the nervous symptoms predominating in such cases. As the insufficiently nourished brain is not capable of exertion, mental as well as physical rest is naturally indicated. And this not only for the reason that it is necessary to avoid functional exhaustion, but also because the anæmic brain when overstrained furnishes a favorable soil for the development of morbid fears, imperative impulses, and imperative conceptions. This fact does not seem to have been noticed by most writers. The mind of the anæmic person is as peculiarly sensitive to psychical influences as the anæmic visual and auditory centres are to light and sound; and in a considerable proportion of cases of this kind the origin of the morbid idea has been traced to the period of convalescence from exhausting diseases. The prominent position which masturbation occupies among the causes of cerebral anæmia perhaps explains its frequent etiological relationship to imperative conceptions and impulsive insanity.
Although the radical and rational treatment of cerebral anæmia is covered by the treatment of the general anæmia, there are certain special symptoms which call for palliative measures. Most of these, such as the vertigo, the optic and aural phenomena, improve, as stated, on assuming the horizontal position. The headache if very intense will yield to one of three drugs: nitrite of amyl, cannabis indica, or morphine. I am not able to furnish other than approximative indications for the use of remedies differing so widely in their physiological action. Where the cerebral anæmia and facial pallor are disproportionately great in relation to the general anæmia, and we have reason to suppose the existence of irritative spasm of the cerebral blood-vessels—a condition with which the cephalalgia is often of great severity—nitrite of amyl acts as wonderfully as it does in the analogous condition of syncope.36 Where palpitations are complained of, and exist to such a degree as to produce or aggravate existing insomnia, small doses of morphine will act very well, due [p. 789] precautions being taken to reduce the disturbance of the visceral functions to a minimum, and to prevent the formation of a drug habit by keeping the patient in ignorance of the nature of the remedy. When trance-like conditions and melancholic depression are in the foreground, cannabis indica with or without morphia will have the best temporary effect: it is often directly remedial to the cephalalgia. Chloral and the bromides are positively contraindicated, and untold harm is done by their routine administration in nervous headache and insomnia, irrespective of their origin. Nor are hypnotics, aside from those previously mentioned, to be recommended; the disadvantages of their administration are not counterbalanced by the advantages.37 Frequently, in constitutional syphilis, insomnia resembling and probably identical with the insomnia of cerebral anæmia will call for special treatment. In such cases the iodides, if then being administered, should be suspended, and if the luetic manifestations urgently require active measures, they should be restricted to the use of mercury in small and frequent dosage, while the vegetable alteratives may be administered if the state of the stomach permit.
36 There are disturbances in the early phases of cerebral syphilis, whose exact pathological character is not yet ascertained, which so closely resemble the condition here described that without a knowledge of the syphilitic history, and misled by the frequently coexisting general anæmia, it is regarded as simple cerebral anæmia. Under such circumstances, as also with the cerebral anæmia of old age, amyl nitrite should not be employed.
37 Urethran and paraldehyde have failed in my hands with anæmic persons.
Among the measures applicable to the treatment of general anæmia there are three which require special consideration when the cerebral symptoms are in the foreground: these are alcoholic stimulants, the cold pack, and massage. It is a remarkable and characteristic feature of cerebral anæmia that alcoholic stimulants, although indicated, are not well borne38—at least not in such quantities as healthy persons can and do take without any appreciable effect. I therefore order them—usually in the shape of Hungarian extract wines,39 South Side madeira, or California angelica—to be given at first in such small quantities as cannot affect the cerebral circulation unpleasantly, and then gradually have the quantity increased as tolerated. In fact, both with regard to the solid nourishment and the stimulating or nourishing fluids and restorative drugs the division-of-labor principle is well worth following. The cerebral anæmic is not in a position to take much exercise, his somatic functions are more or less stagnant, and bulky meals are therefore not well borne. Small quantities of food, pleasingly varied in character and frequently administered, will accomplish the purpose of the physician much better.
38 Hammond, who classes many disorders under the head of cerebral anæmia which the majority of neurologists regard as of a different character, has offered a very happy explanation. He says, “Now, it must be recollected that the brains of anæmic persons are in very much the same condition as the eyes of those who have for a long time been shut out from their natural stimulus, light. When the full blaze of day is allowed to fall upon them retinal pain is produced, the pupils are contracted, and the lids close involuntarily. The light must be admitted in a diffused form, and gradually, till the eye becomes accustomed to the excitation. So it is with the use of alcohol in some cases of cerebral anæmia. The quantity must be small at first and administered in a highly diluted form, though it may be frequently repeated.”
39 Such as Meneszer Aszu; there is no genuine tokay wine imported to this country, as far as I am able to learn.
The cold pack, strongly recommended by some in general anæmia, is not, in my opinion, beneficial in cases where the nervous phenomena are in the foreground, particularly in elderly persons. Gentle massage, on the other hand, has the happiest effects in this very class of cases.
Of late years my attention has been repeatedly directed to cerebral anæmia of peculiar localization due to malarial poisoning. It has been [p. 790] noted by others that temporary aphasia and other evidences of spasm of the cortical arteries may occur as equivalents or sequelæ of a malarial attack. I have seen an analogous case in which hemianopsia and hemianæsthesia occurred under like circumstances, and were recovered from. Whether more permanent lesions, in the way of pigmentary embolism or progressing vascular disease, causing thrombotic or other forms of softening, may develop after such focal symptoms is a matter of conjecture, but I have observed two fatal cases in which the premonitory symptoms resembled those of one which recovered, and in which these were preceded by signs of a more general cerebral anæmia, and in one case had been mistaken for the uncomplicated form of that disorder. Where a type is observable in the exacerbation of the vertigo, headache, tinnitus, and lethargy of cerebral anæmia, particularly if numbness, tingling, or other signs of cortical malnutrition are noted in focal distribution, a careful search for evidences of malarial poisoning should be made; and if such be discovered the most energetic antimalarial treatment instituted. It is in such cases that arsenic is of special benefit.
The treatment of syncope properly belongs to this article. Where the signs of returning animation do not immediately follow the assumption of the recumbent position, the nitrite of amyl, ammonia, or small quantities of ether should be exhibited for inhalation. The action of the former is peculiarly rapid and gratifying, though the patient on recovery may suffer from fulness and pain in the head as after-effects of its administration. The customary giving of stimulants by the mouth is to be deprecated. Even when the patient is sufficiently conscious to be able to swallow, he is usually nauseated, and, as he is extremely susceptible to strong odors or tastes in his then condition, this nausea is aggravated by them. By far the greater number of fainting persons recover spontaneously or have their recovery accelerated by such simple measures as cold affusion, which, by causing a reflex inspiration, excites the circulatory forces to a more normal action. Rarely will the electric brush be necessary, but in all cases where surgical operations of such a nature as to render the development of a grave form of cerebral anæmia a possibility are to be performed, a powerful battery and clysters of hot vinegar, as well as the apparatus for transfusion, should be provided, so as to be within reach at a moment's notice.
Before the introduction of accurate methods of examining the diseased brain the term inflammatory softening was used in a much wider sense than it is to-day. Most of the disorders ascribed to inflammatory irritation by writers of the period of Andral and Rush are to-day recognized as regressive, and in great part passive, results of necrotic destruction through embolic or thrombic closure of afferent blood-channels. Two forms of inflammation are universally recognized. One manifests itself in slow vascular and connective-tissue changes and in an indurating inflammation. There are two varieties of it: the first of these, which is associated with furibund vaso-motor explosions and regressive metamorphosis of the functional brain-elements, is known from its typical [p. 791] association with grave motor and mental enfeeblement as paretic dementia or dementia paralytica. The second, which is focal in the distribution of the affected brain-areas, is known as sclerosis. The former is treated of in a separate article; the latter is considered in connection with the spinal affections which either resemble it in histological character or complicate its course. The second form of cerebral inflammation is marked by the formation of the ordinary fluid products of acute inflammation in other organs of the body; this is the suppurative form, usually spoken of as abscess of the brain.
In addition to these two generally recognized inflammatory affections there are a number of rare diseases which are regarded by excellent authority as also of that character. The vaguely-used term acute encephalitis has been recently reapplied with distinct limitations to an acute affection of children by Strümpell. This disease is usually of acute onset, infants under the sixth year of age being suddenly, and in the midst of apparently previous good health sometimes, attacked by fever, vomiting, and convulsions.40 Occasionally coma follows, which may last for several days, perhaps interrupted from time to time by recurring convulsions or delirium. The convalescence from this condition is rapid, and in some cases is complete; in others paralysis remains behind in the hemiplegic form. The paralysis is usually greater in the arm than in the leg; in extreme cases it involves the corresponding side of the face, and, as the paralyzed parts are arrested or perverted in growth, considerable deformity, even extending to asymmetry of the skull, may ensue. The deformity is aggravated by contractures. Usually there is some atrophy of the muscles, but in one case I found actual hypertrophy41 of some groups, probably in association with the hemiathetoid movements.
40 As in my case of infantile encephalitis followed by athetoid symptoms (Journal of Nervous and Mental Diseases).
41 This was followed by atrophy. There are never any qualitative electrical changes.
The sequelæ of acute infantile encephalitis present us with the most interesting forms of post-paralytic disturbances of muscular equilibrium. Hemichorea and hemiathetosis, as well as peculiar associated movements and hemicontracture, are found in their highest development with this class of cases. Occasionally epileptiform symptoms are noted,42 and in others true epilepsy is developed. It is under such circumstances that imbecility is apt to be a companion symptom or result; and this imbecility is prominently noted in the moral sphere.
42 Which in one case of my own disappeared spontaneously.
The grave set of symptoms briefly detailed here are attributed by Strümpell43 to an acute encephalitis, analogous, in his opinion, to the acute poliomyelitis of children. Its frequent occurrence after measles and scarlatina, as well as the fact that Ross44 in a carefully-studied case arrived at the opinion that the disease was an embolo-necrotic result of endocarditis, would lead to the conclusion that it is a focal affection, probably due to the transportation of infectious elements to the brain through the blood-vessels. Its occurrence in children in the midst of apparent health45 [p. 792] is consistent with the fact that rheumatism and an attendant slight endocarditis frequently pass unrecognized in infancy. It is supposed that a diffuse form of inflammatory non-suppurative softening exists by some of the Germans, but the proof advanced in favor of this view is not conclusive.
43 As a surmise, for up to his writing no reliable autopsies had been made.
44 Brain, October, 1883.
45 McNutt (American Journal of Medical Sciences, January, 1885) cites Strümpell as attributing the theory of an inflammatory affection, which is analogous to poliomyelitis in its suddenness and nature, to Benedict, and refers to p. 349 of Strümpell's textbook under the erroneous date of 1864. This work was published in 1883-84, and the theory is advanced by Strümpell as his own. It is only a synonym, hemiplegia spastica infantile, that is attributed to Benedict.
A number of rare forms of interstitial encephalitis have been described. In one, elaborately studied by Danillo, an inflammatory hypertrophy of the cortex, involving the parenchyma as well as the connective and vascular structures, was found in a limited area of the motor province of the right hemisphere. There had been crossed epileptiform convulsions during life.46
46 Bulletin de la Société de Biologie, 1883, p. 238.
There is some question among pathologists as to the recognition of Virchow's encephalitis of the new-born. Certainly a part of Virchow's material was derived from the imperfect study of a condition of infantile brain-development which, as Jastrowitz showed, is physiological, and on which Flechsig based his important researches of tract-development. More recent studies, however, demonstrate that there is a form of miliary encephalitis in new-born children due to septic causes, such as, for example, suppuration of the umbilical cord. The demonstration by Zenker of the occurrence of metastatic parasitic emboli in cases of aphthous stomatitis, and by Letzerich of a diphtheritic micrococcus invasion in the brain of his own child, show that the subject of early infantile encephalitis merits renewed consideration.47
47 The attempt of Jacusiel to revive Virchow's encephalitis of the new-born (Berliner klinische Wochenschrift, 1883, No. 7) under the title of interstitial encephalitis does not seem to have met with encouragement, for, besides Jastrowitz, Henoch and Hirschberg opposed this view in the discussion.
Strictly speaking, the reactive changes which occur in the brain-substance bordering on tumors, hemorrhagic and softened foci, belong to the domain of encephalitis; but as they are considered in conjunction with the graver lesions to which they are secondary both in occurrence and importance, it is not necessary to more than refer to them here.
As indicated in the last article, there formerly existed much confusion in the minds of pathologists regarding the terms softening and abscess of the brain. As long as softening was regarded as an inflammation, so long was abscess of the brain regarded as a suppurative form of softening. Aside from the fact that there is some resemblance in mechanical consistency between a spot of ordinary softening and one of inflammatory softening, there is no essential similarity of the two conditions. True softening is to-day regarded as the result of a death of brain-tissue produced by interference with the blood-supply; it is therefore a passive process. Inflammatory softening, of which abscess is a form, is due to an irritant, usually of an infectious nature. It is to the results of such irritation that the term suppurative encephalitis should be limited.
MORBID ANATOMY.—In all well-established inflammatory brain [p. 793] troubles the active part is taken by the blood-vessels and connective tissue; the ganglionic elements undergo secondary, usually regressive or necrotic, changes. The brain, considered as a parenchymatous organ, is not disposed to react readily in the way of suppurative inflammation unless some septic elements are added to the inflammatory irritant. Foreign bodies, such as knitting-needles, bullets, and slate-pencils, have been found encapsulated in this organ or projecting into it from the surrounding bony shell without encapsulation and without any evidences of inflammatory change. As a rule, a foreign body which enters the brain under aseptic conditions will, if the subject survive sufficiently long, be found to have made its way to the deepest part of the brain, in obedience to the law of gravity, and through an area of so-called inflammatory red softening which appears to precede it and facilitate the movement downward. This form of softening derives its color from the colored elements of the blood, which either escape from the vessels in consequence of the direct action of the traumatic agent; secondly, in consequence of vascular rupture from the reduced resistance of the perivascular tissue in consequence of inflammatory œdema and infiltration; or, thirdly, in obedience to the general laws governing simple inflammation.
A cerebral abscess may present itself to the pathological anatomist in one of three phases—the formative, the crude, and the encapsulated. In the first it is not dissimilar to a focus of yellow softening, being, like the latter, a diffuse softened area varying from almost microscopical dimensions to the size of a walnut, and of a distinctly yellow tinge. Microscopic examination, however, shows a profound difference. In pure yellow softening there are no pus-cells; in the suppurative encephalitic foci they are very numerous, and congregated around the vessels and in the parenchyma in groups. The crude abscess is the form usually found in cases rapidly running to a fatal termination. Here there is an irregular cavity in the brain, usually the white central substance of the cerebrum or cerebellum, formed by its eroded and pulpy tissue; it is filled with yellow, greenish, and more rarely brownish pus. In the most furibund cases broken-down brain-detritus may be found in the shape of whitish or reddish flocculi, but in slowly-formed abscesses the contents are free from such admixture, and thus the third phase is produced, known as the encapsulated abscess. The cavity of the abscess becomes more regular, usually spheroid or ovoid; the pus is less fluid, more tenacious, and slightly transparent; and the walls are formed by a pseudo-membrane48 which is contributed by the sclerosing brain-substance, which merges gradually into the outlying normal tissue. I have seen one acute cerebral abscess from ear disease which might be appropriately designated as hemorrhagic; the contents were almost chocolate-colored; on closer inspection it was found that they were true pus, mingled with a large number of red blood-discs and some small flocculi of softened brain-substance. This hemorrhagic admixture was not due to the erosion of any [p. 794] large vessel, for the abscess had ruptured into the lateral ventricle at that part where it was most purely purulent. In a case of tubercular meningitis, Mollenhauer in my laboratory found an abscess in the white axis of the precentral gyrus, with a distinct purulent infiltration following the line of one of the long cortical vessels. The abscess was not encapsulated, the surrounding white substance exhibited an injected halo, and the consistency of the contents was that of mucoid material.
48 There is considerable dispute as to the real nature of the tissue encapsulating cerebral abscesses. It is known, through the careful observations of R. Meyer, Goll, Lebert, Schott, and Huguenin, that the capsule may form in from seven to ten weeks in the majority of cases, about eight weeks being the presumable time, and that at first the so-called capsule of Lallemand does not deserve the name, being a mucoid lining of the wall. At about the fiftieth day, according to Huguenin, this lining becomes a delicate membrane composed of young cells and a layer of spindle-shaped connective elements.
In cases where the symptoms accompanying the abscess during life had been very severe it is not rare to find intense vascular injection of the parts near the abscess, and it is not unlikely that the reddish or chocolate color of the contents of some acutely developed abscesses is due to blood admixture derived from the rupture of vessels in this congested vicinity. Sometimes the entire segment of the brain in which the abscess is situated, or the whole brain, is congested or œdematous. In a few cases meningitis with lymphoid and purulent exudation has been found to accompany abscesses that had not ruptured. It is impossible to say whether in this case there was any relation between the focal and the meningeal inflammation, as both may have been due to a common primary cause.49 In such cases, usually secondary to ear disease, thrombosis of the lateral sinus may be found on the same side. Where rupture of an abscess occurs, if the patient have survived this accident long enough—for it is usually fatal in a few minutes or hours—meningitis will be found in its most malignant form. A rupture into the lateral and other ventricles has been noted in a few cases.50
49 Otitis media purulenta in the two cases of this kind I examined.
50 In one, observed together with E. G. Messemer, intense injection of the endymal lining, with capillary extravasations, demonstrated the irritant properties of the discharged contents.
Some rare forms of abscess have been related in the various journals and archives which have less interest as objects of clinical study than as curiosities of medical literature. Thus, Chiari51 found the cavity of a cerebral abscess filled with air, a communication with the nose having become established by its rupture and discharge.
51 Zeitschrift für Heilkunde, 1884, v. p. 383. In this remarkable rase the abscess, situated in the frontal lobe, had perforated in two directions—one outward into the ethmoidal cells, the other inward into the ventricles, so that the ventricles had also become filled with air. This event precipitated a fatal apoplectiform seizure.
The contents of a cerebral abscess usually develop a peculiarly fetid odor. It has been claimed that this odor is particularly marked in cases where the abscess was due to some necrotic process in the neighborhood of the brain-cavity. The only special odor developed by cerebral abscesses, as a rule, is identical with that of putrid brain-substance, and it must therefore depend upon the presence of brain-detritus in the contents of the abscess or upon the rapid post-mortem decomposition of the neighboring brain-substance.
In two cases of miliary abscess which, as far as an imperfect examination showed, depended on an invasion of micro-organisms, an odor was noticed by me which was of so specific a character that on cutting open the second brain it instantly suggested that of the first case, examined six years previous, although up to that moment I had not yet determined the nature of the lesion.52
52 Owing to the lack of proper methods of demonstrating micro-organisms, the first case whose clinical history was known was imperfectly studied; of the second case, accidentally found in a brain obtained for anatomical purposes, the examination is not yet completed.[p. 795]
That form of abscess which, from its situation in or immediately beneath the surface, has latterly aroused so much interest from its important relations to localizations is usually metastatic, and directly connected with disease of the overlying structures, notably the cranial walls. In this case the membranes are nearly always involved. The dura shows a necrotic perforation resembling that found with internal perforation of a mastoid or tympanic abscess. The pia is thickened and covered with a tough fibro-purulent exudation; occasionally the dura and leptomeninges are fused into a continuous mass of the consistency of leather through the agglutinating exudation. The abscess is usually found open, and it is not yet determined whether it begins as a surface erosion, and, bursting through the cortex, spreads rapidly on reaching the white substance, or not. The white substance is much more vulnerable to the assault of suppurative inflammation than the gray, and not infrequently the superficial part of the cortex may appear in its normal contiguity with the pia, but undermined by the cavity of the abscess, which has destroyed the subcortical tissue. Possibly the infecting agent, as in some cases of ear disease, makes its way to the brain-tissue through the vascular connections, which, however sparse at the convexity of the brain, still exist.
CLINICAL HISTORY.—The symptoms of a cerebral abscess depend on its location, size, and rapidity of formation. There are certain parts of the brain, particularly near the apex of the temporal lobe and in the centre of the cerebellar hemisphere, where a moderately large abscess may produce no special symptoms leading us to suspect its presence. There are other localities where the suppurative focus53 indicates its presence, and nearly its precise location and extent, by the irritative focal symptoms which mark its development and by the elimination of important functions which follows its maturation. It is also in accordance with the general law governing the influence of new formations on the cerebral functions that an acutely produced abscess will mark its presence by more pronounced symptoms than one of slow, insidious development. Indeed, there are found abscesses in the brain, even of fair dimensions, that are called latent because their existence could not have been suspected from any indication during life, while many others of equal size are latent at some time in their history.
53 Practically, our knowledge of localization of functions in the human brain begins with the observation by Hitzig of a traumatic abscess in a wounded French prisoner at Nancy named Joseph Masseau. The year of the publication of this interesting case constitutes an epoch in advancing biological knowledge, which will be remembered when even the mighty historical events in which Hitzig's patient played the part of an insignificant unit shall have become obsolete. This, the first case in the human subject where a reliable observation was made was an unusually pure one; the abscess involved the facial-hypoglossal cortical field (Archiv für Psychiatrie, iii. p. 231).
An acute cerebral abscess is ushered in by severe, deep, and dull headache, which is rarely piercing, but often of a pulsating character. The pain is sometimes localized, but the subjective localization does not correspond to the actual site of the morbid focus.54 It is often accompanied [p. 796] by vertigo or by a tendency to dig the head into the pillow or to grind it against the wall. With this there is more or less delirium, usually of the same character as that which accompanies acute simple meningitis. As the delirium increases the slight rise in temperature which often occurs in the beginning undergoes an increase; finally coma develops, and the patient dies either in this state or in violent convulsions. The case may run its course in this way in a few days, but usually one to three weeks intervene between the initial symptoms and death.
54 Although Ross seems to be of a contrary opinion, it is the exception for the pain to correspond in location to the abscess.
Between the rapid and violent course of acute cerebral abscess detailed, and the insidious course of those which as latent abscesses may exist for many years without producing any noticeable symptoms whatever, there is every connecting link as to suddenness and slowness of onset, severity and mildness of symptoms, and rapidity and slowness of development and progress. It is the encapsulated abscesses which are properly spoken of as chronic, and which may even constitute an exception to the almost uniform fatality of the suppurative affections of the brain. Thus, the symptoms marking their development may correspond to those of an acute abscess, but coma does not supervene, temporary recovery ensues, and the patient leaves the hospital or returns to his vocation. But all this time he appears cachectic, and there will be found, on accurate observation, pathological variations of the temperature and pulse. The appetite is poor; the bowels are usually constipated; there are frequent chilly sensations and horripilations, and a general malaise. This condition slowly passes away in the few cases which recover; in others relapses occur, usually of progressing severity, and terminate life. The period during which the symptoms of the abscess are latent may be regarded as corresponding to the latent period which sometimes intervenes between an injury and the development of the symptoms of acute abscess, and which, according to Lebert, may comprise several weeks or months. In other words, the morbid process may be regarded all this time as progressing under the mask of a remission. It is this latent period which it is of the highest importance for the diagnostician to recognize. There is usually headache, which is continuous and does not change in character, though it may be aggravated in paroxysms. Usually the temperature rises with these paroxysms, and if they continue increasing in severity they may culminate in epileptic convulsions.
Many of the symptoms of cerebral abscess—prominently those attending the rapidly-developed forms and the exacerbations of the chronic form—are due to cerebral compression. It is the pulse and pupils, above all, that are influenced by this factor.
In an affection having so many different modes of origin as cerebral abscess, and occupying such a wide range of possible relations to the cerebral mechanism, it is natural that there should exist many different clinical types. So far as the question of the diagnosis of localized cerebral abscesses is concerned, I would refer to the article dealing with cerebral localization, in order to avoid repetition. With regard to the etiological types, they will be discussed with the respective causal factors.
ETIOLOGY.—Abscess of the brain is so frequently found to be due to metastatic or other infectious causes that it is to be regarded as highly improbable that it is ever of idiopathic occurrence. The most frequent [p. 797] associated conditions are—suppurative inflammation in neighboring structures, such as the tympanic cavity, the mastoid cells, the nasal cavity, or inflammation or injury of any part of the cranium and scalp. The connection of these structures with the brain through lymphatic and vascular channels is so intimate that the transmission of a pyogenic inflammatory process from the former to the latter is not difficult to understand. But disease of far distant organs, such as gangrene of the lung, and general affections, such as typhoid fever, occasionally figure among the causes of cerebral abscess, particularly of the miliary variety.
Among the commonest causes of cerebral abscesses are those which the surgeon encounters. The injury may be apparently slight and limited to the soft parts, or the bone may be merely grazed. Gunshot wounds are particularly apt to be followed by a cerebral abscess; and it has been noted that those which granulate feebly, whose base is formed by a grayish, dirty, and fetid material, are most apt to lead to this ominous complication. The symptoms do not usually develop immediately, and after the surgeon is led to indulge in the hope that danger is past, proper reaction sets in, healthy granulations develop—nay, the wound may close and be undergoing cicatrization—then the patient complains of feeling faint or drowsy, and with or without this premonition he has convulsive movements of one side, sometimes involving both extremities and the corresponding side of the face. Consciousness is usually preserved, but the spells recur, and the patient is noted to be absent-minded during and after the convulsive seizure. On some later day he is noticed to become pale, as in the initial stage of a true epileptic seizure; total abolition of consciousness follows, and the clonic spasms, affecting the same limbs and muscles involved in the first seizures, now recur with redoubled violence. After such an attack more or less paresis is observed in the muscles previously convulsed. A number of such seizures may occur, or a fatal issue terminate any one of them. Not infrequently the field of the involved muscles increases with each fit. Thus the thumb or a few fingers may be the first to show clonic spasm; in the next fits, the entire arm; in succeeding ones, the leg and face may follow suit. In such a case the periphery first to be convulsed is the first to become paralyzed, thus showing that where the disease began as an irritative lesion the cortex is now destroyed, and that around the destructive focus as a centre the zone of irritation is spreading excentrically, first to irritate and then to destroy seriatim the functions of the various cortical fields in their order. According to the teachings laid down in the article on Localization, the order of invasion and extension, as well as the nature, of the focal symptoms will vary. Finally, the attacks become more severe and of longer duration; the patient does not recover in the intervals, but complains of nausea, pain, confusion, and head-pressure. He is noted to be dull, his temperature is slightly raised (100° F.), and the speech may be affected. Several attacks may occur in a day, each leaving the patient more and more crippled as to motility and mind. He is delirious and drowsy at intervals; his temperature may rise after an attack from one to four degrees, usually remaining near 103°–104° F. in the evening; and, coma developing, death occurs, the convulsion or paralytic phenomena continuing at intervals during the moribund period, and the temperature and pulse sometimes running up rapidly toward the last. On examining [p. 798] the parts, it is found that the bone is necrotic at the point of injury, usually only in its outer table, but sometimes in its entire thickness. In exceptional cases the normal continuity of the entire table is not interrupted to all appearances, and a small eroded spot on the inner table is found bathed in pus, or a detached necrotic fragment may be found in the latter. Corresponding to the purulent focus on the inner table the dura mater is detached, discolored, and perforated in one or more places with irregular rents or holes which have a greenish or blackish border. An abscess is found in that part of the brain which corresponds to this opening. There is no question that it was caused by direct infection from the necrotic spot.
Cases have been noted,55 apparently of idiopathic origin, in which a sudden paralysis of a few fingers was the first symptom produced by the development of a cerebral abscess. In a few days such a paralysis extends to the other fingers and to the forearm. Occasionally no convulsive phenomena are noted, or choreic movements indicate, in their place, that the cortical field is irritated. Such cases usually run a rapidly fatal course.
55 Arthur E. W. Fox, Brain, July, 1885.
The most frequent cause of cerebral abscess in civil practice is suppurative inflammation of the middle ear. It may be safely asserted that the person suffering from this affection is at no time free from the danger of a cerebral abscess, a purulent meningitis, or a phlebitic thrombosis of the sinuses. Cases are on record where the aural trouble had become chronic, and even quiescent, for a period of thirty years, and at that late date led to abscess with a fatal termination. Of 6 cases of this character in my experience, 4 of which were verified by anatomical examination, not one but had occurred at least four years after the commencement of the ear trouble, and 1 happened in a man aged fifty-four who had contracted the latter affection in childhood. In 2 there was in addition diffuse purulent meningitis, limited on the convexity to the side where the abscess was situated.56 In 4 the abscess was in the temporal lobe, 1 of them having in addition an abscess in the cerebellar hemisphere of the same side; in a fifth the abscess was in the deep white substance of the cerebral hemisphere, opening into the lateral ventricle, and in the sixth it was in one cerebellar hemisphere alone.
56 One of these was seen during life by J. R. Pooley; the other was a paretic dement at the New York City Pauper Asylum.
The course of this class of abscesses is usually obscure: focal symptoms are not commonly present, and the constitutional and local symptoms usually appear as a gradual outgrowth from the aural troubles. Thus there is at first usually little fever, vertigo, and chilliness, but considerable tinnitus, and sometimes pain in the ear. Occasionally local signs of a septic metastasis of the otitis, such as œdema over the mastoid or painful tumefaction of the cervical glands, are visible. The pain previously referred to the region of the ear now becomes general; commonly—even where the abscess is in the temporal lobe—it becomes progressively aggravated in the frontal and sometimes in the nuchal region, and under an increase of the febrile phenomena death may exceptionally occur without further complication. Even large abscesses in one half of the cerebellum occur without producing Ménière's symptom—a fact [p. 799] which leads to the suspicion that the purulent deposit must have been of slow and gradual development. In one case distinct symptoms indicating an affection of the subcortical auditory tract were observed. As a rule, this class of abscesses are accompanied toward the close by active general symptoms—convulsions, coma, narrowing and impaired light-reaction of the pupils. Delirium, when a prominent symptom from the beginning, indicates the probable association of meningitis with the abscess.57 Occasionally severe pain, rigor, high temperature, and paralysis may be absent even with rapidly-developed abscess from otitis.58
57 The same is probably true of oculo-motor paralysis, which Ross (loc. cit., vol. ii. p. 735) refers to uncomplicated abscess.
58 This was the case with an abscess containing five ounces of pus recorded by C. S. Kilham at the Sheffield Medical Society (British Medical Journal, February 13, 1886). As illustrating what was stated about the non-correspondence of the pain and the location of the abscess, it may be stated that notwithstanding this large abscess was in the temporal lobe, what pain was present was in the forehead.
Ulcerative endocarditis, infectious osteomyelitis, pulmonary gangrene, general pyæmia, and, as is claimed by a few authors, typhoid fever, are often accompanied by multiple abscesses in the brain-substance. Usually the foci are small, as may be readily inferred from the fact that they are of embolic origin, the emboli being usually so small as to lodge in very small vessels, and that the fatality of the primary disease is so great as to cut short life before the abscess can reach larger dimensions. For the same reasons the symptoms they produce are rarely distinctive. In chronic lung affections accompanied by putrescence in bronchiectatic or other cavities cerebral abscesses are not uncommon occurrences. Under these circumstances, although we must assume an embolic origin, the abscess is rarely multiple, and the symptoms are as marked as in the ordinary varieties. Thus a patient suffering from chronic phthisis, with or without prodromal malaise or somnolence, experiences formications and pain in his right leg; he then notices a slight halt in walking; twitches appear in the affected extremity; it becomes distinctly paretic. The arm then becomes affected in like manner; the pupils become unequal; a severe chill occurs, followed by delirium, convulsions, coma, and death.
DIAGNOSIS.—There is little difficulty in recognizing the existence of a cerebral abscess in which well-marked focal and constitutional symptoms coincide, or where a distinct abscess-producing cause, such as an ear trouble, a head injury, or a putrid bronchiectasis, coexists.59 But there are a number of cases, varying from the latent form to forms with obscure general symptoms, whose recognition is impossible or at best a matter of conjecture. Such cases may be readily confounded with certain tumors. The existence of febrile symptoms, although not excluding tumor, as some tumors are accompanied by such, is greatly in favor of abscess. On the other hand, choked disc, which is rare with abscess and found only with the very largest, is in favor of tumor.
59 Yet a leading and careful authority was misled into making the diagnosis of abscess in a case of ear disease complicated by a cerebral tumor.
PROGNOSIS AND TREATMENT.—The majority of cerebral abscesses must, from the nature of the case, be regarded as not influenceable by medicinal measures or surgical treatment. The miliary and other abscesses due to general septic causes or to mycotic invasion, being in the nature of [p. 800] the case but features of intrinsically dangerous or fatal primary diseases, do not call for special measures. It is different with those due to local trouble about the head and to surgical causes. Remarkable advances have been made in the operative treatment of cerebral abscesses, chiefly owing to the increasing accuracy of the localization of the affected areas through the disturbance of their function, and to the perfection of surgical methods. A number of cases by Gussenbauer, Wernicke, and others have shown that some abscesses may be accurately located during life by the focal symptoms produced by their presence. Wernicke's observation of a large abscess in the occipital lobe showed two facts. First, it permitted the study of the effect of large abscesses on the cerebral movements, as it was found after trephining that the pulsation movement of the brain was lost and the dura tensely bulging, thus indicating a high degree of cerebral pressure. Secondly, the operation showed that an abscess can be emptied of its contents, under moderate aseptic precautions, without provoking contiguous inflammatory reaction or infecting the meninges. Notwithstanding these favorable local conditions, the patient died. Gussenbauer60 was more fortunate. He surmised from the fluctuation of some symptoms and the predominance of others that his patient had an abscess in the frontal lobe. The suspicion was verified: an abscess of the size of an apple was found, opened, and emptied of its contents. The patient recovered without any immediate untoward symptom.61
60 Prager medizinische Wochenschrift, 1885, Nos. 1, 2, and 3.
61 Epileptic and focal spasms subsequently developed, which shows that a new inflammatory or other destructive process may have set in in the vicinity of the emptied sac.
The uncertainties of localization in some districts of the brain are so great that a number of attempts to repeat the explorations and aspiration of Wernicke and Gussenbauer have failed. In one case recently operated on in New York City the aspirating-needle was run into the brain-substance in several different directions without striking the pus. It is a question under such circumstances whether the chances of an abscess becoming latent, minimal though they be in cases with pronounced signs, are not to be preferred to those which an uncertain operation can give. The superficial encephalitic foci offer far better opportunities for surgical triumphs. Here not only the symptoms are much more constant, and point more unerringly to the site of the morbid spot, but there are often other signs, such as the evidences of impaction of a foreign body, local tenderness on percussion, or bone disease, which aid in determining the proper spot for the application of the trephine. Several operations where traumatic encephalitis existed with or without leptomeningitis of the convexity, followed by complete recovery, were performed by Macewen.62
62 The Lancet, 1885, vol. i. p. 881.
The medicinal treatment of abscess of the brain is limited to derivative methods, whose aim is the relief of pressure—an aim whose fulfilment is more frequently illusory than otherwise.
Benefit has been claimed from the energetic use of mercury, chiefly in the form of calomel, by older writers; and recently Handfield Jones has endorsed its administration, attributing to it a remission in a case in which it was employed. It must be remembered, however, that remissions occur spontaneously in this disease, and that the purgative action of calomel may act well for the time being in an affection so apt to be [p. 801] associated with hyperæmia and increased cerebral pressure as is an abscess of the brain.63 In the nature of the case, even this latter momentarily beneficial effect is at the best temporary.
63 Brain, October, 1884, p. 398.
The prophylaxis of cerebral abscess can be carried out only in cases due to cranial and aural affections. The importance of treating all scalp and cranial injuries under aseptic64 precautions is recognized by all surgeons. It is generally admitted that the trephining of a bone suspected to be the site of an ostitic or necrotic process involves fewer risks than the allowing it to remain. Similar principles govern the treatment of the inflammatory involvement of the mastoid cells often complicating otitis media. If trephined at all, these should be trephined at the earliest moment. It was a belief among the older aurists that the sudden cessation of an aural discharge was of evil augury, and that cerebral complications were more apt to follow under such circumstances than when the ear discharged freely. Von Tröltsch, Politzer, Gruber, and Toynbee have opposed the exclusive application of the old dogma. In so far as the older ear-surgeons regarded a profuse aural discharge as an encouraging sign, in this respect they were of course wrong. But their observation of the frequent concurrence of cerebral sequelæ with suppression of discharge is, I think, borne out by a large number of cases. It does not apply, however, to the suppression of discharge by the rational employment of aseptic injections.
64 This term is used in its widest sense here.
The spinal cord is found to vary considerably in color in different individuals. To some extent this difference is influenced by the position occupied by the body after death, but not as markedly as in the case of the brain. Thus it will be paler in a body which has been kept in the prone than in one which has been kept in the supine position.65 It is usually found more injected in persons who have died of febrile affection than in those who have died of exhausting diseases; notably is this the case with typhus fever and with subjects who die with congestive malarial chill. But the most intense congestion, where the gray substance instead of having the normal rosy hue appears like a blood-soaked sponge, and the white substance instead of the tint to which it owes its name has a pink shade, is found in subjects dying in convulsive disorders complicated by asphyxia, such as epileptic status, tetanus, and certain toxic disorders.
65 I have not seen it noticed anywhere, but it is a fact readily demonstrable in any autopsy made in a well-preserved body that when a short segment of cord is observed at the moment of section the section surface appears pale; but if it be again examined after a few moments, it will show a reddish tinge, marked as a faint injection would be; this tinge distinctly deepens under the eye. I have observed this in specimens which were not held in the hand, so that the influence of pressure can be excluded. Nor do I believe that the elasticity of the tissues is such as to account for the phenomenon.
In attempting to apply the fact that varying degrees of vascular injection are found on post-mortem examinations of the spinal cord to the elucidation of certain clinical phenomena, we encounter the same difficulties and sources of error that confronted us in the study of nutritive [p. 802] brain disorders. The majority of writers have therefore contented themselves with making a careful clinical study of the mostly subjective signs of disorders which, once designated as spinal anæmia and hyperæmia, are now classified under the non-committal titles of spinal irritation and exhaustion (neurasthenia), as in this volume. A number of these disorders, like the so-called anæmic paralysis of Bouchut, Leroy d'Etiolles, Beroliet, Baimer, and Brandis, would to-day be considered as hysterical or reflex; and a few of the instances cited by their contemporaries as cases of spinal hyperæmia have been since demonstrated to resemble the initial phases of organic diseases of the cord.
The causes of active spinal hyperæmia are either direct, as when the spinal centres are overtasked by muscular strain either through over-exertion or through toxic convulsions, surprised by violent shocks, such as concussion accidents, or collateral, as when a physiological discharge (menstruation) or a pathological one (hemorrhoidal flux) is suddenly checked. A few cases are reported where carbonic-oxide-gas poisoning provoked spinal hyperæmia. But, like the alleged cases of spinal hyperæmia after continued and exanthematic fevers, they were probably cases of incipient or established myelitis. Hammond claims that surface chilling exerts the same congesting influence on the cord which he claims for the brain; but no definite observations have been made in this direction.
Passive spinal hyperæmia has been attributed to obstructive cardiac and chronic pulmonary affections. In such cases, as with most causes acting on the circulation of blood in the nerve-centres, the coexisting cerebral congestion usually masks the spinal. It is a question how far the intense hyperæmia of the cord found in some cases of tetanus, strychnia-poisoning, and the condition called hydrophobia66 is primary and an indication of neural hyperexcitability, and how far it is secondary to the asphyxia attending the last phases of these convulsive states. The weight of opinion is in favor of an acceptation of the latter as the chief or only factor.
66 In a case of hydrophobia clinically as well marked as has been recorded, which I had the privilege of examining through the courtesy of Kretschmar, both brain and cord were found remarkably anæmic.
Over-exertion and sexual excesses are frequently followed by a sensation of fulness and tension in the sacral and lumbar regions, which may be relieved by lying prone, while it is aggravated while lying supine.67 From the location of this pain it is evident that it is not due to congestion of the cord or its membranes, but to fulness of the vertebral and spinal veins of the lower segment of the vertebral column. A similar sensation, which may be relieved by the same change in position or by a hemorrhoidal flux, is complained of by patients suffering from portal obstruction. The veritable symptoms of hyperæmia manifest themselves in the parts which receive their nervous supply from the affected districts. The reflexes are usually more active; paræsthesias of different kinds, such as formication, tingling, and creeping sensations, are common; and [p. 803] there is more or less motor weakness, the limbs feeling heavy and sometimes being the seat of an acute pain. As a rule, these symptoms are limited to the lower half of the body.
67 Although this fact has been questioned, I have no doubt whatever that it is true, from a large number of observations. In many subjects suffering from the results of excessive venery or masturbation, an intolerable, sometimes pulsating, feeling in the lumbo-sacral region is only relieved by raising the lower end of the trunk with the back up. This condition is influenced by a change of residence to a district having a different level above the sea, and consequently a different barometric condition.
There is very little question when these symptoms exist for any length of time, and become aggravated, that more subtle nutritive changes than are covered by the single term hyperæmia become responsible for them. In a pure hyperæmia the position-test of Brown-Séquard, which shows relief when the patient is upright or prone and aggravation when he is supine, particularly if the gravitation of blood to the cord be facilitated by raising the head and extremities, ought to yield constant results. But in some cases, particularly those of long-standing, the very opposite is noted: the patient's symptoms are aggravated by standing or sitting up, and relieved by lying down. Here there is probably exhaustion or malnutrition of the nerve-elements, rendering them abnormally sensitive to exertion. This view is supported by the fact that molecular disturbances, such as those which probably accompany simple concussion, predispose the patient to the development of the symptoms of spinal hyperæmia, and aggravate them if established previous to such accident.
Hammond,68 who in his chapter on Spinal Congestion and Anæmia follows rather the older authors, such as Ollivier, than the newer and either more cautious or more sceptical writers on the subject, describes the symptoms of congestion as comprising belt sensations, paraplegia, erections of the penis, muscular twitches, loss of expulsive power, and incontinence of the bladder, paralysis of the abdominal muscles, paralysis of the anal sphincter, loss or abolition of reflex excitability, diminution of electro-muscular contractility, and occasionally hyperæsthesia and shooting pains. It is not doubtful for a moment that if such a case were to occur in hospital experience it would be regarded as one of organic disease, and not incipient, but well-established organic disease of the cord. Those making the diagnosis would have their opinion strengthened if, as Hammond states, the process took place with great rapidity and had a tendency to extend itself and eventually involve the whole cord, or if, as Brown-Séquard is by him cited as stating, bed-sores occurred in addition. Although Hammond describes certain anatomical changes, such as increased development of blood-vessels and distension and injection of them, I am unable to find any cases recorded as spinal congestion during life, and carefully examined with a due regard to sources of error after death, in which such changes were found. It is true that after strychnine- and cocaine-poisoning an intense hyperæmia69 of the cord is found. In mammals it is of a far more pronounced character than in reptiles, and usually more marked in proportion to the existing asphyxia. That the characteristic toxic effects of these drugs is not to be sought for in their direct or indirect congesting influence is shown by the fact that exsanguinated frogs can be made to undergo strychnine tetanus when their blood is replaced by a saline solution according to the method of Salkowski. Little support, therefore, could be derived from a pretended analogy between toxic and [p. 804] pathological hyperæmias, even if the phenomena of both were similar; which is not the case.
68 Diseases of the Nervous System, 7th ed., p. 392.
69 It is true that in animals which are so organized that the congestion cannot be attributed to asphyxia, as I showed (Hammond Prize Essay of the American Neurological Association, 1878) in some experiments on strychnine, arterial congestion and small foci of hemorrhage were found in the upper cervical cord of frogs who had been kept in continuous strychnine tetanus for over seventy days.
The introduction of subaqueous caissons for workmen engaged in the building of bridges, in which those employed labor under abnormal atmospheric pressure, has led to the development of a previously-unknown cerebro-spinal affection known as the caisson disease, and in which, it is generally supposed, either congestion or hemorrhage of the spinal cord occurs in consequence of sudden changes of vascular pressure resulting from sudden diminution of the barometric pressure. Clinically, this affection has been studied in England, France, and above all in America in connection with the building of the East River Bridge and the one over the Mississippi at St. Louis.70 Experiments by Hoppe-Seyler, Bert, and I. Rosenthal have shown that a sudden diminution of pressure leads to hemorrhages in various tissues, and, according to the two first-named, a development of gas occurs in the vascular and other fluids of the body. A number of peculiar symptoms which do not specially interest us here occur in conjunction with the so-called caisson disease: these are—pain in the ear, with or without otitis sicca; peculiar pains in the joints, which occur on leaving the caisson, and are probably due to hyperæmia of the joint-surfaces and sudden increase of the intra-articular fluid; and retardation of the pulse-rate. In some cases cerebral hyperæmia is added, the patients tottering about as if drunk. The spinal symptoms consist of a paraplegiform affection. The paralysis is usually sudden; in some cases the patient a few minutes after stepping from the air-chamber falls down perfectly helpless as far as the lower half of the body is concerned. The expulsive power of the bladder is usually weakened, and there is anæsthesia to all forms of sensation in the affected limbs, as well as diminished electro-cutaneous sensibility. The patient often complains of a strange feeling, as if the lower half of his body were a foreign substance. With this the electro-muscular reactions are normal. In the majority of cases these symptoms disappear entirely in from three to ten days, but occasionally they remain longer; imperfect recovery of motion and sensation occurs, or, as happened in a few cases, one of which was carefully examined during life by Lehwess and after death by Leyden, death occurs as in myelitis. In the only case where an autopsy and careful microscopical examination were made under these circumstances71 peculiar fissures were found in the substance of the spinal cord, surrounded by areas of reactive myelitis and filled with granule-cells. The absence of any pigmentary relics of a hemorrhage induced Leyden to assume that the lacunæ were not of hemorrhagic origin. He inclines to the view that they were due to the escape of gas from the blood-plasma, and consequent multilocular inflation of the tissue. If his observation be confirmed, it constitutes a strong objection to the hyperæmia theory of the caisson disease. There is neither permanent hyperæmia nor congestive or hemorrhagic myelitis developed, as far as the limited material thus far studied permits a conclusion.
70 Clark, St. Louis Med. and Surg. Journ., cited from Hammond, loc. cit.
71 E. Leyden, Archiv für Psychiatrie, ix. p. 316.
Pure spinal hyperæmia rarely presents itself for treatment. The form due to over-exertion is recovered from by rest in a very short time; that due to suppressed discharges, by the re-establishment of the latter or by [p. 805] the application of leeches to the lumbo-sacral and iliac region. Ergotin is recommended by Hammond in very large doses. It is a question whether this drug may not exert a bad effect in protracted cases where its use has to be continued for a long time.72 In using it, it is well to bear in mind that imperfect nutrition of nerve-elements is perfectly compatible with an increased blood-amount.
72 A young physician, who for a long period took ergotin in twelve-grain doses for the relief of symptoms regarded as congestive, acquired a tolerance of the drug such as I have not seen recorded anywhere, and in addition presents some obscure signs of cerebellar disease and initial optic-nerve atrophy.
Strychnia has been given with benefit in the caisson disease—another evidence, as this drug is theoretically contraindicated in true hyperæmia, that this disease is not, as Hammond and the majority of authors with him regard it, essentially a congestive affection. The treatment of those numerous cases in which signs of venous fulness accompany spinal exhaustion and irritation is detailed in the articles dealing with those affections.
Anæmia of the cord-substance proper, like hyperæmia, is practically inseparable from the corresponding condition of the membranes. The influence of a reduced blood-amount on the functional activity of the spinal cord is more susceptible of exact demonstration than the corresponding nutritive disturbance of the brain. As the functions of this segment of the nervous axis are far simpler than those of the higher organ, there is more unanimity among observers as to the interpretation of their disordered states. In Stenon's experiment, and the more elaborate modifications made by those who have followed his method, it is found that interference with the supply of arterial blood to the spinal cord is followed by abolition of the function of the gray matter; if the supply be still further diminished, the functions of the white tracts become eliminated; next the peripheral nerves, and ultimately the muscles themselves, lose their normal excitability. On the re-establishment of the circulation these various parts regain their functional capacity in the inverse order of its suspension—the muscles first, next the nerves, then the white substance, and last the gray substance of the cord. The initial symptoms of some cases of myelitis from refrigeration correspond more nearly to such a result of artificial anæmia of the cord than they do to anything that is customarily regarded as hyperæmia.73
73 I have seen distinct pallor of the spinal meninges on dipping the posterior extremities of a dog, whose cord had been exposed, into water. It is to be remarked, however, that other observers, notably Hammond, have either obtained different results or interpreted the consequences of refrigeration differently.
No one has gone farther than Hammond in erecting a theoretical anatomical framework which elaborately provides for the accommodation of various symptoms of spinal anæmia. He describes anæmia of the posterior columns, and sharply discriminates between it and anæmia of the antero-lateral columns. It is a question whether the conducting tracts of these columns are seriously affected in their functions by anæmia as long as the centres of innervation are well nourished. Undoubtedly, it is the gray substance of the cord which is most vulnerable to the influence of [p. 806] disturbed circulation and nutrition, as Stenon's experiment has shown; and a glance at the distribution of the blood-vessels will show that a partial anæmia or hyperæmia, limited to special cornua in any considerable length of the cord, is an exceedingly improbable occurrence. With regard to isolated anæmia of the white columns, it is to be admitted that the posterior are most vulnerable to malnutrition. But it is doubtful whether this vulnerability is so great as to allow of an exclusively posterior anæmia, or whether a protracted anæmia of this kind could exist for years as a purely symptomatic—or, as some designate it, functional—disorder.
Hammond candidly states that in specifically locating the lesions in these affections he is aware that post-mortem examinations are wanting to support them, and admits that what he calls anæmia of special parts of the cord is the spinal irritation of most authors, and in part the reflex paraplegia of others.
The most clearly-established form of cerebral anæmia is the one which is indicated by the ischæmic paraplegia of Jaccoud and the paraplegia following profuse hemorrhages. The former is produced by all causes which, by obstructing the flow of arterial blood in the abdominal or thoracic aorta, cut off the proper blood-supply to the cord, which the latter receives through the intercostal and upper lumbar arteries. Aneurism, compression by tumors, and embolism of the aorta produce this result. The consequence is paraplegia corresponding in all features of its development to the phenomena observed in Stenon's experiment. These features, already detailed, suffice to show that it is not the anæmia of the peripheral nerves and muscles that is chiefly responsible for the paraplegia, but the insufficient irrigation of the gray and white substance of the cord itself. The same is true of the paraplegia following hemorrhage which has been noted after uterine, renal, and enteric hemorrhages. Both affections are exceedingly rare.
The influence of general anæmia on the functions of the spinal cord is not susceptible of accurate study. The cerebral enlargement of the nervous axis is so much more unfavorably situated than the cord that it suffers first and most when general anæmia is present. The consequence is that the signs of cerebral anæmia mask those of spinal anæmia. It is supposed, however, by many authorities that the effect of anæmia on the cord may be regarded as an auxiliary factor in the production of hysterical and neurasthenic symptoms.
How far the spinal cord is liable to suffer from arterial spasm is as yet a matter of conjecture. It is supposable that just as a powerful psychical impression provokes a sudden spasm of the cerebral arteries, so a peripheral irritation may provoke a spasm of the spinal arteries. In this way the reflex paralyses, motor and vaso-motor, are explained by many writers.
The subject of reflex palsy has been so much confused by improper cataloguing—if it can be so called—that some of the best authorities have become sceptical as to its occurrence. Among the chief sources of error has been the attributing to irritation of the genital organs various convulsive, psychical, and paralytic disorders. Adherence of the prepuce and its excessive length were charged with being responsible for idiocy, imbecility, epilepsy, and every form of paraplegia and panplegia. It was further claimed that instances of complete cure of each of these [p. 807] affections had followed the removal of the exuberant or adherent prepuce. I cannot find a single instance recorded where such a cure was effected in any of our large medical centres, so as to prove convincing to critical colleagues. On the contrary, L. C. Gray74 has shown that various surgical procedures have been needlessly resorted to on this erroneous theory in cases of organic diseases of the spinal cord. I have seen two unfortunate children suffering from the worst forms of anterior poliomyelitis, one afflicted with pseudo-hypertrophic paralysis, and several hydrocephalous and microcephalous idiots, whose prepuces had been sacrificed to the theory alluded to—it is needless to add without any result, good or bad.
74 Reflex Irritation from Genital Irritation. In this paper written communications from all or nearly all neurologists in the United States—certainly including all those of national fame and large experience—are cited, in which they testify to never having seen a case of this character cured by operations on the penis (Annals of Anatomy and Surgery, Jan. and Feb., 1882.)
The possibility of a reflex paralysis occurring from genital irritation in the male cannot be denied; among the lower animals a ligature around the spermatic cords sometimes produces paraparesis, and paraplegia is a common complication of renal and vesical troubles in others. But analogous observations in man are rare, and becoming rarer with our increasing acumen in diagnosis. In females peculiar reflex disturbances are found associated with uterine and ovarian derangements. In one case of retroflexion, with possible dislocation of the ovary, referred to me by H. J. Boldt, there is a remarkable vaso-motor paralysis of the right arm during each menstrual period: this member becomes greatly enlarged, of a purplish-blue color, and cold. Equally remarkable are the reflex disturbances resulting from the presence of worms in the intestinal canal. Every form of spinal and cerebral paralysis, even aphasia, has been observed in connection with helminthiasis. Such disorders yield as rapidly as they are developed to the exhibition of vermifuges.
Special interest has been aroused by the discovery laid down in the joint treatise of J. W. Mitchell, Morehouse, and Keen of reflex paralysis following injuries, observed in the War of the Rebellion. The cases cited by them appear singular on first sight. The paralysis is often observed in parts of the body which are not only remote from the seat of injury, but have no direct connection, physiologically or otherwise, with it. The hand may be injured and the opposite leg paralyzed.
Since Mitchell, Morehouse, and Keen first announced the existence of this peculiar form of reflex paralysis a careful search has been made by military surgeons engaged in other campaigns for like results. Notably was this done in the Franco-Prussian War. A number of confirmatory instances have been collected, some of which rival in singularity those related by the discoverers of the affection. In one case a unilateral paralysis agitans followed a punctured wound of the opposite shoulder, and in another reflex aphasia followed a gunshot wound of the lumbar region.75 A discrimination is to be made between such cases where the paralysis, anæsthesia, or neuralgia is an immediate result of the injury, and those where they follow after weeks or months. In the latter instance we have not true reflex disorders to deal with, an ascending [p. 808] neuritis having been found in the few cases which could be carefully followed up.76
75 Sanitäts Bericht über die deutschen Heere im Krieg gegen Frankreich, 1870-71, vol. vii.—abstracted in Neurologisches Centralblatt, 1886, p. 207.
76 In a case of Mollenhauer's, vesical paralysis and paresis of the right leg occurred six years ago (1880) in a veteran of our civil war who had a gunshot wound of the right hand, with signs, which are still present, of occasional exacerbation of brachial neuritis. Prodromal signs of paresis were noticed at intervals since his return from the campaign. The bladder trouble and paresis are now apparently stationary. Such a case can be accounted for only on the assumption of an organic cord-change secondary to a neuritis.
The theory that the reflex paralysis from utero-ovarian, intestinal, and surgical affections, when acutely produced, is due to central anæmia, is as acceptable as any other would be in the absence of decisive observations.
Spinal anæmia will but rarely present itself as a subject for special and separate treatment. When not associated with an intrinsically grave condition, such as aortic obstruction, dysentery, fatal hemorrhage, or typhoid fever, it is an exceedingly benign affection, rapidly yielding to tonic and restorative measures combined with rest.
Although the spinal cord is a segment of the same central organ as the brain, nourished in a similar way, and subject to the same physiological and pathological laws, lesions of the vascular apparatus, which play so important a part in brain pathology, play a comparatively insignificant one in that of the spinal cord. Embolic, thrombic, and primary hemorrhagic lesions of the cord are so rare that their possible existence has even been denied. A primary thrombosis of the cord has not yet been satisfactorily demonstrated to occur independently of syphilitic lesions; and when it occurs the ensuing tissue-changes, as described by Heubner, Julliard, and Greiff, are usually in the background as compared to the gummatous, sclerotic, or meningitic changes which coexist. The clinical as well as the anatomical picture is accordingly either one of a myelitis or meningitis, as the cases of Charcot-Gombault, Heubner, McDowell, Wilks, Wagner, Zambaco, Homolle, Winge, Moxon, Schultze, Westphal, Julliard, and Greiff show. (See Myelitis and Spinal Meningitis.)
With regard to the occurrence of hemorrhage into the substance of the spinal cord (hæmato-myelia), it is so rare an occurrence that I can recall but a single case in which I entertained the diagnosis of this lesion; and in that very case I am unable to declare that it was not a hemorrhagic myelitis. Aneurismal changes of the spinal arteries are comparatively of rare occurrence, and as other predisposing causes to primary vascular rupture are rare in the cord, the probability of its occurrence is very much diminished. Hebold,77 in a young girl who had developed severe cerebro-spinal symptoms during a period of nine months following an erysipelatous disorder, found the upper dorsal cord, on section, dotted with numerous reddish and round points. These points corresponded to [p. 809] aneurismal dilatations of the vessels. As there were other inflammatory and vascular lesions in the same subject, the author referred their causation to a general constitutional vice, the result either of the phlegmonous or of a tuberculous disorder.
77 Archiv für Psychiatrie, xvi. 3. Rupture of miliary and other aneurisms in the meninges has been reported by Astley Cooper, Traube, and others. It is remarkable that such cases are more and more rarely recorded from year to year in inverse ratio to the accuracy of our spinal autopsies. I have never found a miliary aneurism below the uppermost cervical level of the cord. On the other hand, I have found extensive spinal hemorrhage in cases where the vessels of the cord proper were fairly healthy.
It is claimed that suppression of the menses, over-exertion, lifting heavy weights, and concussion are causes of spinal hemorrhage. The same causes are also mentioned for acute hemorrhagic myelitis; and it is a question whether the supposed hemorrhage is an initial lesion or secondary to congestive or anæmic softening.78
78 I have never found vascular ruptures, although carefully searching for them, in the spinal cord of persons dying instantly after falls from a great height, or, as in one case which I was fortunately able to secure the cord of, where the subject had been violently thrown down. Where hemorrhages have been found under these circumstances they were, as far as I am able to learn from the cases recorded, meningeal.
The symptoms attributed to spinal hemorrhage are the same, taking the same locality of the cord, as those of a very rapidly-developed transverse myelitis. It is unnecessary to enumerate these here in anticipation of the next section. They are described as being much more sudden. This suddenness is the only diagnostic aid on which we can rely.79 The fate of the patient is said by Erb to be decided within a few days. If he survive the immediate consequences of the hemorrhage, he is apt to recover, as to life, altogether, with such permanent atrophies, paralyses, and anæsthesias as are entailed by the destruction of the tracts and gray substance involved in the hemorrhage. The treatment recommended for this condition consists of rest, either in the lateral or prone position, local depletion and derivation to the intestinal canal, as well as the internal use of ergotin. The local application of ice, which is also advised, is probably based on illusory views.80 After the immediate danger is past the case is to be treated as one of myelitis—a very safe recommendation in view of the probability that it was a case of myelitis from the beginning.
79 And even this sign is unavailable as a distinguishing feature in supposed hemorrhage from concussion, as sudden paraplegias of motion and sensation are found in some cases of railway spine, and, although a number of cases terminating fatally have been examined, there was not always hemorrhage even in the meninges.
80 Until authorities shall have agreed as to what effect the exposure of the bodily periphery to certain temperatures has on the circulation of the cord, it would be premature to make any special recommendations as to the temperature at which they should be kept. I am inclined to believe that while, as is universally accepted, a general cooling of the bodily surface tends to increase vascular fulness in the cord, as in all other internal organs, a partial cooling, as of the feet, produces local anæmia at the level of origin of the nerves supplying the cooled part. Certainly, the bilateral neural effects of unilateral cooling are in favor of this view.
The descriptions given of the hemorrhagic foci as observed after death strengthen the view that they were in the majority of cases of myelitic origin. Usually, they are stated to extend up and down the cord in the direction of least resistance—that is, in the gray substance—resembling an ordinary apoplectic clot. But in their neighborhood there was usually considerable softening, and, to judge by the descriptions given, this softening differed in no wise from that which is the characteristic feature of acute myelitis;81 and often the transition from a peripheral zone of white [p. 810] softening, through an intermediate zone of red softening, to a central compact clot, is so gradual as to leave it unquestionable that the softening pre-existed, and that a vessel had broken down in the midst of the myelitic detritus. Many ancient foci of myelitis betray the hemorrhagic complication of their initial period by the presence of pigmented residue of the absorbed clot.
81 In the latest treatise on nervous diseases published in our language (Ross, loc. cit., vol. ii. p. 325) the insufficient foundation on which a whole chapter has been built up is illustrated by the admission that the usual evidence of acute central myelitis may be observed far beyond the limits of the hemorrhagic infiltration. If a large area of softening in the brain were found to contain a central or peripheral clot of blood, and histologically resembling a typical embolic or thrombic softening, no one would be in doubt as to which of the two was the primary lesion.
Embolisms and embolic softenings of that part of the spinal cord which is supplied by the small spinal vessels are so rarely observed in the dead-house that our knowledge of their possible occurrence and character is almost entirely the result of experimental observations or based on analogy. The situation of these vessels, the angle at which their supply-tubes are given off from the aorta, all act as protectors of the cord against what is one of the chief dangers to which the brain is exposed. No definite symptoms have been attributed to the few doubtful cases of simple embolic occlusion of the spinal arteries found accidentally in human subjects. Even those emboli which, when once let loose in the circulation, are found distributed in nearly every organ of the body, those derived from ulcerative endocarditis and those due to the invasion of micrococci, are comparatively rare in the cord. Leyden found multiple capillary emboli in the spinal cord from the former cause. Small grayish white foci in a similar distribution were found to be due to an invasion of cocco-bacteria from a decubitus by Rovigli.82 In this latter case an increase of pain and muscular spasm in the history of the case of sclerosis which was thus complicated was attributed to the parasitic affection.
82 Rivista sperimentale di Freniatria, 1884, x. p. 227.
Just as simple and infectious embolic lesions are frequent in the brain and rare in the cord, so purulent inflammation or abscess is an exceptional occurrence in spinal as compared with cerebral pathology, and probably for the same reasons.
SYNONYMS.—Spontane (primäre) acute Rückenmarkserweichung, Softening of the spinal cord, Ramollissement blanc de la moelle, Myélite aiguë.
As Leyden, whose treatise83 may be regarded as the foundation of our knowledge on this subject, correctly avers, it is to Abercrombie and Ollivier that we owe the determination of the existence of that acute structural disease of the spinal cord, now termed myelitis, as an affection independent of meningeal changes. The anatomical descriptions given by these older writers may be accepted at the present day as models of accurate observation by the naked eye. Their statement that in acute myelitis the substance of the spinal cord is softened and changed into a puriform, yellowish, diffluent mass; that while the disorganization is sometimes more marked in the posterior, at others in the anterior, and occasionally in the lateral half, it is most pronounced in the axis of the cord, because the central gray substance is the favorite starting-point [p. 811] of the morbid process,—requires no modification to-day. Considerable doubt existed in the minds of the contemporaries of Ollivier and Abercrombie as to whether this change was the result of a true inflammation; and one of the clearest thinkers of the day, Recamier,84 regarded myelitic softening as a lesion peculiar to the nervous apparatus, and different from ordinary inflammation. I believe that the most profound investigators of the present day have not been able to rid themselves of a similar doubt. The discovery of Gluge's so-called inflammatory corpuscles, which was regarded as settling the question, only served to confuse the student by the confidence with which it was urged that they were infallible criteria of the inflammatory process. Under the non-committal designation of granule-cells these bodies still flourish in the annals of cerebro-spinal pathology. As we shall see, a number of products of real disease, of artifice, and of cadaverous change have passed and do pass muster under this name. The first substantial progress in our knowledge of the minute processes underlying inflammation of the spinal cord was made by Frommann and Mannkopf, but it applied altogether to the chronic inflammatory or cirrhotic affections of the cord. The difference between acute and chronic myelitis is greater than is the difference between acute and chronic inflammation in any other organ; and it must be admitted that if Recamier is to be regarded as having erred in asserting that acute myelitis is not a true inflammation, he is justified in so far as he asserted many features of the process to be altogether peculiar to the organ affected. Leyden himself attempted to throw light on the subject by provoking myelitis experimentally in dogs. He injected Fowler's solution into the spinal cords of three dogs, and in each instance produced changes which he interpreted as comparable to the myelitis of human pathology. But the inflammation thus provoked was not of the cord-substance alone; it also involved the membranes, and the inflammatory foci were in several instances purulent. Now, pus never85 forms in ordinary myelitis. An abscess of the cord never occurs where a septic agency can be excluded. In six dogs whose spinal cords I wounded in the dorsal and lumbar regions by aseptic methods, and who survived from two to seven days, I never found purulent or indeed any active inflammatory process, as that term is ordinarily understood, but exactly such passive and necrotic or reactive changes as occur in the acute myelitis of human pathology.
83 Klinik der Rückenmarkskrankheiten, ii. p. 115.
84 Cited by Leyden.
85 In the textbooks and encylopædias, without an exception, the statement that pus may be a product of myelitis is made. This is true of traumatic cases and of such depending on septic and zymotic causes alone. I am unable to find a single carefully observed case of the occurrence of pus in simple myelitis in the literature.
Owing to the advance of clinical and anatomical knowledge made within the past fifteen years many forms of spinal disease classed with the inflammations have been recognized as distinct pathological entities, no longer to be confounded with simple acute myelitis, ordinarily so called. Special forms of acute spinal paralysis, notably acute poliomyelitis anterior of children and the corresponding chronic affection among adults, have become separated in this way, and are accordingly treated of in separate parts of this volume.86
86 For other and practical reasons the traumatic and compression forms of myelitis are also assigned a separate place.[p. 812]
Some dispute exists as to the propriety of making a distinction between acute and chronic myelitis, since an acute myelitis, if the initial attack be recovered from with life, presents a similar condition clinically as chronic myelitis; and this quiescent or slowly-progressing condition may extend over many years. The term acute with reference to inflammation of the spinal cord refers only to the active period of the disease. Just as an embolic softening of the brain is an acute affection, but may be followed by a chronic paralysis or aphasia, so the acute myelitic process may be followed by a chronic paraplegia. It is improper to call the latter a chronic myelitis. It is merely a protracted symptomatic sequel of the acute process. The latter is distinguished from chronic myelitis both clinically (by the rapidity of its onset) and anatomically (by the early dissolution of nerve-elements in the focus of disease). Limited in this sense, acute myelitis, excluding the special clinical forms already adverted to, is rather a rare disease.
MORBID ANATOMY.—The most recognizable change noted in an acute myelitic focus is one of consistency: the spinal substance is softened. In some cases the softening is so slight that the observer may doubt whether he has a pathological or cadaveric softening to deal with, the dorsal cord, which is most apt to be the site of an acute transverse myelitis, being precisely the part which is most apt to show the latter change even in fairly well-preserved bodies. In extreme cases the softening may be so intense that the cord-substance, completely fluidified, runs out of the meningeal sac, leaving the latter a collapsed membranous cylinder to mark the place where the cord once was. Where the cord-substance is sufficiently firm to permit of sections being made through it, the normal outline of the gray and white substance is found obliterated, either presenting the appearance as if the gray and white matter had been stirred up together or of a more uniform color-change. The color may be either white, reddish, yellowish, or chocolate-like. It depends upon the participation of the blood-vessels in the change. If there be much hyperæmia, there will be developed what is known as red softening; if there be much extravasation and commingling of blood with the diffluent cord-tissue, a chocolate color will mark the diseased area; and similarly one and the same focus may present different tints in different parts according to the age and intensity of the process and the more or less advanced retrogressive metamorphosis of the extravasated fluid. As already stated, the purulent form of softening or abscess does not occur in ordinary myelitis.
There is considerable variation in the extent of the affected areas of acute myelitis. In the typical and severe transverse form the whole thickness of the cord may be disorganized, and the disorganization may extend in the length of the cord, so as to involve the level of exit of from two to five pairs of nerves. In less furibund cases the area of absolute softening is confined to the gray substance and its immediate neighborhood, the submeningeal white substance being but slightly affected or escaping. Sometimes several foci of intense softening are scattered through a short length of the cord and connected by less severely involved areas of softening or œdema. Leyden distinguishes three types of distribution—the transverse, the longitudinal, and the disseminated insular or multiple form. He includes under the [p. 813] longitudinal type the so-called central softening of Albert, but undoubtedly many cases of syringo-myelia have passed under this designation. The submeningeal form of softening which, with Ollivier, he states to occur in association with spinal meningitis, must be a very rare affection, as it is difficult to find a well-established case recorded. The longitudinal form shows the same predilection for the gray substance which the acute myelitic process generally does, but I have seen a finely demarcated fascicular myelitis limited to the lateral column in a paretic negro. In this case the pyramid tract and the contiguous area in front of it were so intensely softened that for a length of twelve centimeters a hollow canal ran through the cord in the place previously occupied by the diseased substance. In recent cases of myelitis the diseased area is usually found surrounded by a transition zone in which, the morbid change gradually becoming less intense, the consistency is firmer, and which merges into that of the normal cord. In cases where death occurs after a few weeks a more abrupt demarcation is usually found; this is due to the reactive changes occurring in the neighborhood. The connective tissue becomes firmer, and thus the softening centre becomes surrounded by a sclerosing capsule. Ultimately, the centre undergoes complete disintegration and absorption, and a cavity is left behind filled with a clear fluid; in short, a cyst surrounded by a firm capsule represents the residua of disease. In cases where the softening at the centre of the focus does not proceed so rapidly nor reach so high a degree as to result in liquefaction, the less vulnerable elements, the blood-vessels and supporting tissues, survive the death of the ganglionic and conducting substance; the connective elements hypertrophy, and thus a firm sclerotic patch is formed, indicating the location of the previously softened field.
It seems to be generally admitted, with Hayem, that the blood found exuded in the hemorrhagic form of myelitis does not necessarily indicate an active determination, but is rather, like some forms of so-called red softening of the brain, the result of capillary rupture or necrosis in the midst of the disintegrated tissue, now rendered incapable of supporting the vessels. The existence of a purely white form of myelitic softening shows that a textural change is the primary occurrence, and that the participation of hyperæmia or congestion is not an essential feature of myelitis. The assumption of an initial inflammatory congestion is made rather on theoretical grounds than on the basis of observation. It is simply incredible that, as Ross87 claims, white softening should be a third stage, preceded by red and yellow softening as a first and a second stage! How the extravasated blood, which pathologists generally allow to leave long-lasting traces, manages to disappear, and how blood-vessels in the midst of necrotic or œdematous surroundings suddenly acquire such contractile energy as to produce a total emptying of their contents while the perishable nerve-elements remain behind, are problems which should be solved before attempting to assign to a condition which is often found to be a primary phase of myelitis the position of a late and regressive stage. Erb admits that red softening, to which he also assigns the position of a first stage, is very rarely seen, only traumatic and rapidly fatal cases of central myelitis offering opportunities of examining it. None of the [p. 814] various forms of exudation claimed to occur at this period under the names of vitreous, colloid, or hyaline deposit have been confirmed in any recently well-studied case.88 The great mass of authorities, however, still agree in regarding the minute changes of the initial stage of myelitis to correspond to those of ordinary inflammation. The vessels are described as injected, the adventitial spaces as crowded with the formed elements of the blood, and the vascular walls and the neuroglia infiltrated with granule-cells and fatty granular matter. By some, inflammatory changes of the neuroglia are described, but I am unable to find a single case in which these were determined in early fatal cases. As far as our observation goes, the hypertrophy of the neuroglia is a later occurrence.
87 A Treatise on Diseases of the Nervous System, 1882, vol. ii. p. 280. The author states no authority, nor does he advance his own observations in support of this statement.
88 Baumgarten's case of hyaline exudation, Archiv der Heilkunde, vol. xvii. 276, was an infectious myelitis and associated with anthrax.
As to the nervous elements themselves, they are always found affected. The nerve-cells appear inflated, their processes fragile, sometimes suddenly swollen in their course, at others very thin and brittle. Multiplication of the nuclei of the large multipolar cells has been described. It must be an unusual occurrence, as it has been confirmed by but a few of the numerous observers who have examined into this question. The protoplasm of the nervous elements loses its normal striation and fine molecular granulation; it becomes either coarsely granular or hyaline. The axis-cylinders, both in their intracinereal and their intramyelinic course, show changes similar to those of the cell-processes in the gray matter. Particularly frequent are swellings in their course, the diameter of the cylinder being so much increased as to almost equal that of the myelin tube. This increase in diameter is regarded as an inflammatory swelling by some, as secondary to disturbed nutrition by others; it precedes disintegration: the substance becomes granular, fragile, and in the end dissolves. In the mean time the myelin loses its continuity, irregular segments of it fusing into round and oval masses.89
89 Many of the bodies represented as granule and colloidal cells are in reality round spheres of myelin, whose resemblance to a nucleated cell is sometimes heightened by their occasional inclusion of a fragment of an axis-cylinder which has not yet lost its power of imbibing carmine and other dyes. Where softening has proceeded farthest, there the spherical and other forms of myelin are found crowding the field, and mingled with them are blood-corpuscles, fragments of blood-pigment, granular detritus, and bodies known as fatty granular cells. A number of bodies of very different origin have received this name, some of them, like the fragments of myelin alluded to, not even meriting the name of cells. Others, however, are veritable formed histological elements, either leucocytes or cellular ingredients of the neuroglia, which, having fed on the products of myelin disintegration, have become enlarged and coarsely granular. The longer the duration of the process the more numerous are these bodies, showing that they are not the coarse and essential factor of the inflammation, but an accompaniment, subserving some conservative process, inasmuch as they either remove effete material or contribute to the permanent organization of the cicatricial or atrophic tissue.
The period now reached by the morbid process may be regarded as a sort of interregnum. The necrotic tissues have not yet disappeared on the one hand, the products of inflammation have not yet organized themselves on the other. It is in this period that the ganglionic elements are described as undergoing certain changes in outline and in appearance. Above all, one change has interested observers, which, consisting in the development of what appear to be spherical vacuoles in the interior of the cell, is termed vacuolization. I can compare it to nothing so nearly as to [p. 815] the appearance which is produced by the formation of gas-bubbles in a putrefying albumen or other semifluid substance.
This vacuolization of ganglion-cells is now regarded as a cadaveric change. It is not agreed, as yet, whether its occurrence in myelitis is so frequent as to suggest its ante-mortem occurrence as a veritable feature of the disease. I have been struck by this change in the neighborhood of wounds artificially produced in dogs, even in the fresh specimen. It must be remembered, however, that under these circumstances, the nutrition of the cell being destroyed and exposure to the macerating effect of the cerebro-spinal and pathologically exuded fluids occurring, a cadaveric change may take place intra vitam.
The influence of phosphorus and alkaloid as well as metallic poisons on the cord has been experimentally studied by a number of observers. Unfortunately, Popow, Tschisch, and Danillo—who described as characteristic a resulting change in the staining reaction of the cells, the development of vacuoli in them, and an atrophy of their processes—had not made a sufficient number of examinations of normal cords under like methods of preparation to recognize which of these deviations is without the physiological confines. Kreyssig90 demonstrated the existence of all these conditions in the cords of perfectly healthy animals preserved in chromic acid;91 and Schultze confirms him, and expresses a surprise, which must be shared by all reflecting investigators, that poisons of so widely different a character should have an identical effect on the cord-substance, as is claimed by the writers named.
90 Virchow's Archiv, cii.
91 He attributes the remarkable difference in staining of nerve-cells of the same ganglionic group and in the same section to the sudden transferral of the hardened specimens to strong alcohol, which seems to be the custom in some German laboratories. He claims that uniformity in staining is effected if the specimen be transferred from the chromic preparation to weak alcohol, then to stronger, and thus by gradual increase of the strength to strong spirit. Possibly, instead of approximating the real structural indications by this method, Kreyssig may obliterate them. In specimens which alcohol is not permitted to touch before staining is completed, very deeply and very lightly stained cells will be found almost side by side. The shorter the hardening process, the more perfect the staining method, the more likely are these differences to be found. It is reasonable to assume that the difference in dye-absorbing power indicates slight differences in the cell-protoplasm, marking the nutritive state of the latter and occurring within physiological limits.
If life be prolonged and the conservative processes assert themselves, the disintegrated material disappears, and as the white color of the greater area of the cord was due to the myelin, and the latter has now become destroyed within the diseased area, the latter presents a grayish color. This phase is often termed gray softening. The consistency is, however, much firmer than in the previous stage. Trabeculæ of connective tissue form, enclosing in their meshes a large number of neuroglia-nuclei and sometimes spaces filled with fluid. According as condensation and retraction or rarefication preponderate the process will terminate either in the formation of a sclerotic focus or of a cyst. Occasionally an irregular spongy tissue containing several small cysts results.
Charcot claims that a restitution of anatomical continuity, and therefore of physiological potentiality, may occur in a myelitic cicatrix. But the experiments of Kahler92 and Homén93 prove that when a nerve-tract [p. 816] is once destroyed within the spinal cord all hope of restoring that tract in structure, and thus to restore its functions, is at an end. Unlike the fibres of the peripheral nerves, those of the spinal cord and brain do not seem capable of regeneration.94 If a restoration of function is to occur at all, it must occur through other channels than those destroyed—in other words, by vicarious action.
92 Prager medizinische Wochenschrift, 1884, No. 31.
93 Contribution expérimentale à la Pathologie et à l'Anatomie pathologique de la moelle épinière, Helsingfors, 1885, abstracted in Centralblatt für die medizinisches Wochenschriften, 1886, No. 16.
94 According to the first observer, this is probably due to structural differences. The extramedullary fibres have a sheath and annular constrictions which are absent in the intramedullary.
In a large number of cases myelitis is a limited affection; that is, its ravages remain confined to the area originally involved. But occasionally the morbid process involves the next segments above or below, extending with specially great rapidity through the anterior gray horns. Exceptionally, the entire cord may thus become the site of a generalized myelitis. There is one segment of the cord which may be regarded as possessing an acquired vulnerability when a myelitic focus is in its neighborhood, and that is the lower end. It seems that while the results of a transverse myelitis in the middle dorsal cord may remain stationary for ten or more years, those of a transverse myelitis at the upper lumbar level do not; on the contrary, the entire cord below the lesion appears to be doomed to undergo the same degeneration by contiguity. This is the only occurrence which seems to deserve the name of a descending myelitis: an ascending extension is more frequently noted in other parts of the cord, but the frequency of both the so-called ascending and descending types has been unduly magnified by the inclusion of the secondary degenerations, which are constant sequelæ of all complete destructive transverse lesions of the cord, but which are rather passive phenomena, and probably influence the clinical progress of the case but little, except under such conditions as are potent in that chronic form of myelitis which underlies tabes dorsalis.
CLINICAL HISTORY.—The symptoms of acute myelitis usually correspond to those of any more or less completely transverse lesion of the cord, and accordingly vary with the altitude of the upper level of the lesion. In a general way, they may be stated as consisting of—
First, paralysis of movement in the parts supplied from the nerves given off below the level of the lesion. The reason for this can be easily recognized in those cases where the pyramid tract, which conveys voluntary impulses centrifugally, is interrupted by the softening.
Second, paralysis of sensation in the parts supplied by the same nerves. This is equally explained by the pathological interruption of the centripetal impressions normally conveyed brainward.
Third, alterations in the nutrition of the parts supplied by the nerves arising in the affected level.
Fourth, abolition of those reflexes which are translated in the level of the lesion.
Speaking crudely, then, the symptoms of a transverse myelitis fall into two natural groups. The one which includes the first and second categories enumerated are symptoms due to interruption of cerebral functions; the other, which comprises the last two categories, being due to abolition or perversion of spinal functions. There is a third group comprising certain constitutional symptoms.
[p. 817]Aside from those variations due to the distribution, extent, and intensity of the lesion there are others which depend on the rapidity of its invasion. There are three types in this respect—the apoplectiform, the ordinary acute, and the subacute. The term apoplectiform has been used in two different senses, one being clinical, and referring to the rapidity of onset of the symptoms; the other anatomical, and referring to the nature of the lesion. It is, however, doubtful if a distinction in the latter sense is practically valuable. The presence of a blood-clot in a myelitic focus is itself secondary to the softening, and the intensity and rapidity of the process must have shown itself in the development of the latter.95 The term ought, therefore, to be used in a clinical sense only.
95 I am able to recall but a single case in which, even clinically speaking, a primary hemorrhage into the cord-substance was plausible. In this instance a sudden arrest of menstruation had occurred nearly simultaneously with a combined strain and exposure in a young girl.
The constitutional symptoms of acute myelitis—which, however, are often absent—are its most distinctive features in one sense. Disorders of motion and sensation and perversions of nutrition are signs common to all destructive affections of the cord, whether of a traumatic, neoplastic, or a chronic inflammatory character. But fever, headache, and delirium,96 associated with gastric and visceral disturbances of acute development, are not found to be initial and intrinsic symptoms with them as with acute myelitis. In their absence the mode of onset is characteristic. A high degree of paralysis, motor or sensory, is developed with a rapidity unequalled in any chronic affection of the cord. Sometimes there is a prodromal period in which formication, numbness, and disorders of movement are observed in the same part of the body which are destined to become paralyzed at a later stage of the malady. Within a few hours, days, or at most weeks, complete paraplegia may become developed. The prodromal symptoms may include any form of disturbed sensation. Lancinating pains, tingling, a feeling of the limbs falling asleep, peculiar and indescribable sensations attending the acts of micturition and defecation or of placing the feet violently on the ground, are common. Occasionally they are found in one limb only, although motor and sensory paralysis may ultimately occupy the symmetrical member as completely as the one first involved. In some cases it has been noted that the patient is unable to lie down, or, if lying, to occupy the dorsal recumbent position. This feature has been utilized to support the theory of an initial congestion, which is supposed to be relieved or aggravated according as the cord is kept elevated or depressed.
96 These symptoms are to be regarded as actual parts of the myelitic symptoms only when they accompany the prodromal or initial periods. The later complications, uræmia and septicæmia, the latter arising from pyelitis, cystitis, or decubitus, often lead to constitutional disturbance which is not due to the myelitis as such.
In most cases of transverse myelitis, when the anterior cornua are destructively involved, we possess in the electrical tests valuable and unerring means of determining the altitude and extent of the lesion. Whenever we find the atrophy of a paralyzed muscle accompanied by qualitative electrical changes in myelitis, we must conclude that the cell-group from which that muscle receives its nerve-supply is destructively involved.97 These changes are particularly well demonstrable when the [p. 818] cervical or lumbar enlargements are affected. They are not as readily ascertainable in the case of a transverse myelitis in the upper dorsal region, on account of the situation of the muscles supplied by the upper dorsal nerves, and the consequent difficulty of application of the necessary tests.
97 The proposition, originally, I believe, made by myself, that there are distinct cell-groups in the spinal cord which are constant with certain animal species, and correspond in relative development to ventral, dorsal, and appendicular muscular groups (“Architecture and Mechanism of the Brain,” Journal of Nervous and Mental Diseases, April, 1880), appears to be confirmed in a general way by the researches and cases of Edinger, Kahler-Pick, Dejerine-Major, Genzmer, Von Monakow, Sahli, Prévost-David, F. Schultze, Remak, and Parrot-Joffroy; for the knowledge of the first and last of which I am indebted to the review of the subject by Starr (“Localization of the Functions of the Spinal Cord,” American Journal of Neurology and Psychiatry, August, 1883).
The disturbance of the deep reflexes with very few exceptions affects the same peripheries as are represented in the destroyed and impaired gray nuclei. Thus, if the lower part of the lumbar enlargement be affected, the reflexes of the Achilles tendon and the gluteal muscles will disappear; if the upper lumbar enlargement, the knee-jerk disappears.98 Disease of the lower part of the cervical enlargement is in like manner associated with absence of the wrist-tendon reflexes, while the disappearance of the elbow-tendon reflex suggests a higher involvement at the levels of the fifth and sixth cervical nerve-roots.
98 The disappearance of the knee-jerk and similar reflexes was originally supposed to be a phenomenon exclusively pertaining to spinal disease and to a destructive lesion anywhere in the track of the centripetal and centrifugal nerves connected with that segment of the cord in which the reflex is supposed to be translated. But aside from a number of physiological observations99 which prove that cerebral conditions may influence the intensity of the jerk, there are pathological ones which show that it may be permanently abolished in disease of the pons and cerebellum, and temporarily abolished or diminished immediately after capsular and ventricular hemorrhage. The associated symptoms in the former case, and the history of the onset and total hemiplegia in the latter, serve to distinguish them from destructive spinal lesions should the occasion for discriminating between them ever arise; which is not likely.
99 S. Weir Mitchell and M. J. Lewis found that voluntary effort increases the jerk at first, but if continued diminishes its excursiveness (The Medical News, 1886, Feb. 13th and 20th).
In complete transverse acute myelitis of the cervical region high fever is a constant symptom. In unilateral myelitis of this region flushing of the face and unilateral sweating are produced, together with iridoplegia, sometimes preceded by dilatation, owing to initial irritation and succeeding paralysis of the sympathetic branches originating at this level of the cord.
Just as the disturbed reflexes and the belt sensations enable us to distinguish at what levels of the cord the myelitis is situated, so the distribution of the motor and sensory paralysis affords corroborative evidence of such location and additional proof of its extent and intensity.
Transverse myelitis at and above the level of origin of the phrenic nerve is almost immediately fatal, through its interference with the innervations required in respiration. In the upper part of the cervical enlargement it produces complete paraplegia of motion and sensation in the trunk and all four extremities. In the lowest part of the cervical enlargement it produces paralysis of the same parts, but the serratus magnus and scapular muscles escape. The nuclei of origin of the muscles moving the upper extremity are situated so that those which are farthest removed from the axis of the body when the arms are extended are situated lowest in the cord. The sensory paralysis is distributed in harmony with the motor paralysis; that is, when there is paralysis of motion in the hand [p. 819] and forearm the anæsthesia or subjective numbness is also in the hand and forearm. The same correspondence is not found in affections of the lumbar enlargement, for anæsthesia of the gluteal region accompanies paralysis of the crural muscles when the lesion is low down at the level of the lower lumbar and upper sacral nerves. The distribution of the anæsthesia, in other words, is not by segments of the limb, but by surfaces. The gluteal, posterior femoral, gastrocnemial, and outer pedal surfaces are affected together with the muscles moving the foot, while the thigh and inner side of the leg and foot become anæsthetic, with lesion of the upper part of the lumbar enlargement accompanying paralysis of the quadriceps and deep muscles. It is not difficult to understand this discrepancy when we bear in mind the different plan of distribution followed by the brachial plexus as compared with the lumbar and sacral plexuses. It is not, in my experience, found that the anæsthesia affects that surface which covers the part moved by the paralyzed muscle; which is characteristic of associated paralysis and anæsthesia from cortical disease.
One of the most dreaded occurrences in acute myelitis is the malignant bed-sore. The ordinary decubitus which results from the protracted sojourn of the patient in bed, coupled with the prominence of his trochanters and sacrum resulting from general or atrophic emaciation, is also common, but is comparatively benign and easy to prevent or to manage when established. The malignant bed-sore, on the other hand, is a spontaneous occurrence, due to the same obscure but undeniable trophic influences exerted for good by the normal and for evil by the diseased nerve-centres, which play so large a part in the symptomatology of tabes dorsalis. It cannot be avoided; it is not due to pressure alone, or, as some have claimed, to the macerating influence of the dribbling and decomposing urine. The development of this lesion is exceedingly rapid, and it may be regarded as a sort of local gangrene. The skin shows a livid color; vesicles appear, then burst; the part becomes denuded; and within a few days a deep ulcer with a dark border and base appears, discharging a sanious fluid. The subsequent history is that of a rapid extension and destruction of the neighboring tissues, even down to the bone, and if situated over the sacrum opening into the spinal canal through the necrotic arches of the sacral vertebra, thus leading either to general septicæmia or to putrid infection of the spinal meningeal sac. Occasionally, gangrenous spots coexist on other parts of the body, notably the lower extremities, where neither pressure nor maceration can be accused of playing a part, proving that the process is primarily due to the spinal affection.
Acute central myelitis, as described by Dujardin-Beaumetz, Hayem, Hallopeau, and Erb, usually runs its course very rapidly. Indeed, all of these observers speak of it as the most violent and quickly fatal variety of spinal inflammation. I have, however, seen one case with T. A. McBride at the Presbyterian Hospital in which all the characteristic symptoms of acute central myelitis were markedly developed and present in their characteristic groupings, and yet the patient had been suffering from progressing symptoms of myelitis for one year and a half before that time.100 [p. 820] Usually, complete anæsthesia and paralysis of the lower half of the body occur in this form. But the most characteristic feature is a rapidly progressive atrophy not only of the paralyzed muscles, but also of some which are still partially under the dominion of the will. With this there is extreme vesical and rectal trouble, the sphincters being paralyzed. As a rule, the deep and superficial reflexes are destroyed—they are always diminished—and trophic disturbances of a malignant type, such as acute decubitus, joint-changes, and œdema, are common. The paraplegia is characterized by the flaccid condition of the limbs; the contractures and spastic symptoms found with other forms of myelitis are entirely absent, and qualitative electrical changes, beginning with disappearance of farado-muscular contractility, are found in the atrophying muscles. There are marked constitutional symptoms with this form; the tendency to an ascent of the process and successive involvement of one segment after another of the gray matter is great, and a fatal issue, as far as known, is inevitable.
100 At the time the patient had undergone such a profound change in appearance that I failed to remember him, and it was only by accident I learned that I had seen him in private consultation with his family attendent, F. A. McGuire, a year previous. On the latter occasion I had made the diagnosis of subacute myelitis chiefly limited to the posterior columns; there were ataxia, both static and locomotor, slight incontinence, belt sensation, and ocular symptoms, with abolition of the deep reflexes in the lower limbs.
DIAGNOSIS.—The principles governing the determination of the affected region of the cord in acute myelitis are exactly the same as those detailed in the later sections on Chronic Myelitis or Sclerosis, the acuteness of the onset, and the relapses which sometimes occur, and the predominance of irritative spasms—which, however, is an inconstant criterion—serving to distinguish between the acute and chronic form of spinal inflammation. In the present state of our knowledge it is impossible to always differentiate between acute central myelitis and syringo-myelus—a condition in which the formation of a periendymal neoplasm, and its subsequent breaking down in the axis of the cord, lead to the formation of a tubular cavity.101 The neoplasm in this instance is classified among the gliomatous new formations. The symptoms depend, exactly as do those of myelitis, on the distribution of the destructive lesion. In some cases the posterior cornua and columns are chiefly involved, and extreme anæsthesia is found; in others the anterior columns are affected, and the symptoms of a poliomyelitis or an imperfect transverse myelitis may be imitated.102
101 This cavity, unlike that of hydro-myelus, is not a dilatation of the central canal, but, lying to one side of it, is excavated in the cord-substance.
102 Repeated fractures have been noted in cases marked by profound analgesia. It is believed that they are not always due to trophic changes, but may be the result of muscular action, exaggerated on account of the patient's inability to gauge his efforts. Still, in the majority of cases the presence of positive trophic disturbances of the skin seems to indicate the probability of some textural change facilitating the fracture.
As a rule, the sensory disturbance in syringo-myelus is out of proportion to the muscular atrophy developed; that is, it involves a far more extensive province. It is usually of a peculiar character: some forms of sensation are involved but slightly, or even escape, and others may be nearly destroyed. Commonly, it is the pain and temperature-sense which suffer most, while the cutaneous space and pressure, as well as the muscular sense, are not materially disturbed. These peculiarities are not commonly found in cases of myelitis, and when present, and particularly when the paralytic or sensory affections involve all four extremities [p. 821] alike, they suggest the existence of syringo-myelus. As yet we are unable to make more than a probable diagnosis between the two diseases.
DURATION AND PROGNOSIS.—The duration of the disease varies. Cases of the apoplectiform variety are mentioned, in which the process reached its height in a few minutes, or where the patient, having retired in good health the night before, awoke finding himself paralyzed in the lower half of his body. Death may terminate such a case in a few days or weeks. In another class of cases, complicated by serious involvement of the bladder, the fatal termination is often precipitated by putrid cystitis, pyelitis, or uræmic poisoning, and even in cases which have passed the dangers of the early period in safety these ominous complications may develop with the usual result many years after the beginning of the illness. In a number of cases the first period, that in which the morbid process becomes developed, is followed by one of comparative quiescence, in which the paralyses of sensation and motion then established remain stationary for months and years. A number of authors, Erb, Leyden, Strümpell, and Ross, speak of such a case as one in which chronic myelitis has followed an acute myelitis. It seems improper to use the terms acute or chronic in this way. As it is generally understood that the term acute applies to myelitis in which disintegration of the nerve-elements predominates over interstitial proliferation, and in which the secondary sclerosis is rather like the cicatrix of an acute inflammation and necrosis, it should not be confounded at any period, no matter how similar the clinical signs may be, with a process which is essentially an interstitial one from the start. If chronic amaurosis results from an acute glaucoma, we do not change the latter designation to chronic glaucoma.
In cases where the symptoms at the acme indicate rather an involvement of the peripheral than the central paths of the cord, and in which an incomplete motor and sensory paralysis develops, the patients often regain a considerable amount of motor power and sensation, so that they may reach a good age, suffering at most from a paresis of some one muscle or muscular group, occasional bladder trouble, and pains. It has been laid down as a rule that where paraplegia and other signs remain stationary for years, there is no hope of even partial recovery. The following remarkable and well-attested case proves that this rule is not without exceptions:
Isidor K——, æt. forty-four years, worker in tobacco. After over-exertion in the fall of the year 1879 he had numbness, tingling, dorsal pain, and paresis rapidly developed, which induced him to consult the physicians at the clinic of the University of the City of New York. After some slight improvement a relapse occurred, and several others followed, usually provoked by over-exertion, till he became completely paraplegic. He was, according to his account, several times exhibited to a medical class by William A. Hammond, and remembers that this authority spoke of a possible ascent of the affection and ensuing involvement of the arms. His bladder was at no time seriously disturbed. For four years and three months he was totally paraplegic; his lower extremities were without life; and for the greater part of the time he could not move his toes. The limbs were cold and pale, but underwent little atrophy. The only exercise obtained during this time was in a roller carriage. His sexual power was abolished throughout the whole [p. 822] four years and over. Nothing can be learned as to his reflexes in this period.103 The paralysis of sensation was as complete as that of motion, and the lower limbs never perspired. The arms remained free. There was a dorsal belt sensation.
103 Hammond has no notes of the case, having discontinued the clinic, and Ludwig Weiss, the physician in charge, saw him only occasionally in behalf of a benefit society.
On July 23, 1884, shortly before mid-day, while lying on the bed, in which he had lain a helpless cripple for over four years, except when lifted into the roller carriage, he felt a sudden rush of warmth. Surprised at this first sensation he had felt for years in limbs which had been quasi-foreign appendages, he raised up the bed-clothes and saw that they changed color. There was some tingling for about three minutes, and a perspiration broke out in the affected members. With this he found he could move his feet: half alarmed, half exulting, he sent for his physician, L. Weiss, who found that the patient could stand and walk with considerable freedom. I was then consulted, and found the patient presenting a picture of incomplete transverse myelitis. He could walk, turn about, stand with closed eyes with slight swaying, and his knee-phenomenon was of short excursiveness, but exceedingly spasmodic, and this symmetrically so. He was carefully watched, and against the advice of his physician engaged in peddling cigars, and subsequently took a position as attendant at the pauper asylum on Ward's Island. Here he was on his feet fully twelve hours a day, and his motion, which had continued improving until it was to all practical intents and purposes normal, aside from a slight stiffness, again became impaired, and a joint trouble in the metacarpo-phalangeal articulation of the right little toe, which had troubled him a week after his partial recovery, recurred.104 On January 15th of the present year I again examined him. His knee-phenomenon was greatly exaggerated, cutaneous sensations scarcely impaired, gait paraparetic, but he could walk great distances, and claimed to suffer less from the exertion than from the tenderness accompanying the joint trouble referred to. There had, therefore, occurred, without any assignable cause—for the patient was not under treatment for a year or more before the event—an almost instantaneous restoration of sensation, locomotion, and sexual power; all of which faculties, notwithstanding the infraction of every medical direction given, remained established for two years, with prospects of so continuing a longer period.
104 This was a trophic joint trouble.
TREATMENT.—Most of the therapeutic propositions relating to the treatment of the acute myelitic process are based on the theory that it is of a congestive character or associated with congestion. Accordingly, the internal administration of such drugs as ergotin, which diminish the calibre of the blood-vessels, and local measures, such as depletion, wet cupping, and counter-irritation, intended to act in the same way by derivation, are unanimously recommended by authorities. The suggestion of Hammond, that the patient occupy a ventral or lateral, and not the dorsal, position, is based on, and entirely consistent with, this same view. It is difficult to say what effect is attributable to these measures. Remarkable spontaneous changes—retrogressions as well as advances of the morbid process—occur equally under expectant as under active treatment. I have never seen any improvement in the active phase of simple myelitis which [p. 823] I felt confident I could attribute to any special remedy employed with a view of acting directly on the morbid process. Indeed, improvement has been claimed by Jewell as a result of the use of strychnia—a drug which under the very dogmas governing the orthodox treatment of the disease might be expected to do positive damage.105
105 Jewell gives very large doses of this alkaloid. L. C. Gray, in a discussion held before the American Neurological Association, cited numerous observations directly conflicting with those of Jewell. I cannot, in view of a recent observation in a typical case of acute anterior poliomyelitis, in which by accident the toxic effects of strychnia were obtained, consider this dispute as at all settled. In direct connection with the toxic symptoms the abolished patellar jerk returned in an exaggerated form; motion also returned, and rapid improvement ensued.
In relapses of acute myelitis which had been brought on by chilling of the feet I have obtained good results by derivation to the lower extremities, and on many grounds think that the morbid process in the cord, if it can be affected at all, can be affected by treating the periphery where the symptoms are noted more readily than by applying the cautery or bleeding over the proven site of the disease. Exposure of the dorsal region to cold has not yet been noted as a cause of acute myelitis, whereas such exposure of the lower extremities is a frequent one. This seems to show that the spinal cord is more vulnerable to influences affecting its nervous distribution than to those which are topographically nearer. If this is true as regards morbid influences, it may be urged that it is plausible as regards remedial influences if these are to drive out the disease tendency by the same door it entered.
Rest is imperative during the active progress of the disease. It may be stated as a canon that the earlier the patient takes to his bed, and the more thoroughly he obeys the injunction to attempt no motion of the affected members, the better, cæteris paribus, will the result obtained be. Countless cases are on record where a relapse was directly traceable to a walk undertaken prematurely or carried farther than was wise. As convalescence or partial restitution advances, gradually increasing exercise is to be attempted, not waiting for the danger-signal of a tired feeling to discontinue it; for that feeling, developed, means positive harm already done. It is therefore necessary to allow the returning function to be utilized only within small limits at first, and extending them slowly.
In all cases of severe myelitis where the formation of bed-sores is to be apprehended the water-bed should be employed. Owing to the low temperature which the rubber sac constituting it has, it is necessary to cover it with some well-warmed and non-conducting material and to have the room well warmed. If bed-sores are already formed, they are to be treated according to ordinary surgical principles. Antiseptic means should be in the foreground in the case of the malignant bed-sore. It is to be remembered that the latter is a gangrenous process, and, in so far as the formation of a line of demarcation between the necrotic and the conserved tissue is concerned, the ordinary expectant rules of surgery govern the case: the water-bath appears to yield the best results. Ordinary bed-sores yield readily to mechanical protection and stimulating ointments or the balsam of Peru. Iodoform is recommended, but it produces granulations of an indolent character as compared with those obtained through the use of resinous ointments.
The warm bath is probably the most useful measure in acute myelitis. [p. 824] In cases due to exposure I do not believe it can be applied too soon. Its temperature should, in the beginning at least, not be higher than about 88° F., and the duration about seven minutes. The continued administration will depend on the immediate effect on the patient, and the sittings can be ultimately prolonged to half an hour or even longer. It should be administered once daily, and, when the patient is not disturbed by the manipulation connected with its use, even oftener. Cold baths are recommended by the Germans, but it seems rather in the passive period of the disease than during its active phase.
The management of the bladder trouble is one of the most critical points in the treatment of most cases. The results of retention of urine are more frequently the cause of a fatal issue than any other single complication. Where there is complete retention continuous catheterization is to be employed, as recommended by Strümpell.106 In other cases the bladder should be emptied thrice in the twenty-four hours. The catheter is to be thoroughly disinfected, and if the slightest sign of cystitis is noted the bladder should be washed out with astringent and disinfectant solutions. The continuous irrigation with a solution of corrosive sublimate, 1:2000, appears to give the best results.
106 A. Nelaton's catheter is introduced into the bladder, and kept in place by strips of adhesive plaster fixed to the inner aspect of the thighs. A perforated condom fixed to the catheter, and then fastened to the inguinal region, is in my opinion a better measure, especially in patients who have some motor power left. The catheter is connected with a rubber tube, which should run on a decline in order to effect complete drainage.
If there be a syphilitic taint present—and more particularly is this true of cases where no other cause can be assigned—large doses of iodide of potassium107 should be administered, and mercurial ointment energetically applied, even to the point of salivation.
107 Here, if anywhere, the so-called heroic doses are applicable.
I am unable to say anything with regard to the local use of electricity in the active period of the disease. Ascending currents are recommended by Erb, weak currents of about five minutes' duration being employed over the part supposed to be affected. In order to secure sufficiently deep deflection of the current large electrodes are applied. The use of galvanism and faradism on the affected periphery, the former being preferred where atrophic, the latter where anæsthetic conditions preponderate, is to be instituted early and continued through the duration of the disease. The rules stated in the section devoted to electro-therapeutics are to be followed. In cases where the bladder or rectum are paralytic, these organs should have galvanism applied to them by means of electrodes shaped like catheters or sounds.
After the acute phase of myelitis is passed, the secondary period is to be managed according to the principles laid down in the section on the Treatment of the Sclerotic Processes.
The intimate dovetailing of parenchymatous and connective substance in the spinal cord renders the determination of the precise origin of a morbid process often difficult if not impossible. Whatever the mode of origin, the typical termination of inflammatory and degenerative spinal disorders is sclerosis—a condition in which the essential nervous elements suffer diminution or destruction, while the connective substance is either absolutely or relatively in preponderance. The clinical result is nearly the same in all cases, and with few exceptions depends less upon the histological character than on the topographical distribution of the lesion. It is for this reason that we shall follow rather the topographical than the morbid histological principle in classification.
The chronic disorders of the spinal cord here considered have as a common character the slow and progressive displacement of the normal conducting nerve-tubes by a grayish, reddish, or otherwise discolored tissue, which is firmer in texture than normal nerve-substance. Minute examination shows that it is above all the myelin of the nerve-tubes that is wasted or destroyed, while the axis-cylinders may share in this dissolution, or, as in one form of sclerosis, they may persist and even continue in their conducting function. This increased consistency is found to be due to the increase of connective-tissue trabeculæ and of the neuroglia. In some cases this increase is active and absolute, like the increase in certain phases of hepatic cirrhosis; in others it is rather relative and passive, being merely a condensation of the connective framework after the intervening elements have wasted away, just as the texture of a compressed sponge is more compact than that of an expanded one.
Crudely, the affections of the cord characterized by this change may be divided into two great groups—the regular and the irregular. The former are characterized by their limitation to special nerve-tracts. Thus, in primary lateral sclerosis we find a special tract in the posterior part of the lateral columns occupied by the lesion. A number of spinal diseases with well-defined symptoms are due to active morbid processes which similarly follow the normal distribution of the great nerve-tracts of the cord, with the same, almost mathematical, regularity with which the medullary white develops in the fœtal and infantile cord. In another class of cases we find that the same tracts are involved in like manner—not in the way [p. 826] of primary disease, but through the interruption of the physiological continuity of the nerve-tract by some other disease, to which the sclerosis is therefore secondary. These are the so-called secondary degenerations.
The irregular affections of the cord comprise cases in which the sclerotic foci are either disseminated through the cerebro-spinal axis in numerous foci, or diffusely involve a greater or lesser length and thickness of the medullary cylinder, or, finally, extend in the transverse plane completely or nearly so across the section area of the cord at a definite level.
As the symptoms of the regular affections of the cord are by far the most readily recognizable, and a preliminary knowledge of them will facilitate the better understanding of the irregular forms, we shall consider the former first. They may be subdivided into two groups. The largest, longest known, and best studied consists of acquired, the other, containing less numerous cases and varieties, and rendered familiar to the profession only within the last decade, comprises the spinal disorders due to defective development of the cerebro-spinal and spinal-fibro systems.
SYNONYMS.—Locomotor ataxia and ataxy, Posterior spinal sclerosis; Graue degeneration der Hinterstränge (Leyden), Rückenmarksdarre (popular), Rückenmarksschwindsucht; Tabes dorsualis (Romberg); Ataxie locomotrice progressive (Duchenne).
HISTORY.—Undoubtedly, this disease must have been observed by the ancient masters of medicine, but their descriptions group together so many symptoms of other organic as well as functional diseases of the cord that it is impossible to obtain a clear idea as to what special form they had in view when they spoke of tabes dorsualis. This term was adopted by the German writers of the last and the earlier part of this century as designating all wasting affections of the cord; and it was not till Romberg in 1853 and Duchenne in 1858 differentiated the characteristic clinical signs, and Cruveilhier and Todd (1847) determined the distribution of the lesion in the posterior columns, that the medical profession began to recognize the distinctness of this the most common form of organic spinal ailment.
At this time, when tabes dorsalis became recognized as a clinical entity depending on sclerotic degeneration of the posterior segment of the cord, the inco-ordination or ataxia manifested in the peculiar gait of the patient was regarded as the most characteristic, essential, and constant symptom of the disease. It was regarded as an axiom in physiology that the posterior segment of the cord was subservient to centripetal and sensory conduction, and nothing appeared to follow more naturally than the conclusion that the patient exhibited inco-ordination because, his sensory conduction being interrupted or destroyed, he had lost the necessary gauge for judging of the required extent and force of a given movement. Since then both spinal physiology and pathology have undergone a profound revolution. So far are we to-day from regarding anterior and motor or posterior and sensory as convertible terms that we locate the [p. 827] most important centrifugal tract of the cord behind the plane which divides it into anterior and posterior halves, while the most recently differentiated centripetal tract is represented by Gowers as lying in front of it. It has been determined, through Türck, Bouchard, and Flechsig and his pupils, that the posterior white columns of the cord contain several systems of fibres, whose functions—where determinable—are of an exceedingly complex nature. The elaborate investigations of Charcot, Schultze, and Strümpell, made during the past decade, have shown that the distribution of the diseased field in the posterior segment is not uniform, but is most intense in special areas. These were found to be affected with a remarkable constancy and regularity. Almost coeval with this discovery came the recognition of symptoms found in the earliest phases of the disorder by Westphal, which, attributable as they were found to be to the involvement of the special reflex mechanisms of the cord, enable us to demonstrate the existence and extent of the disease at periods which previously were not within the ken of the clinician. The reproach which Leyden was justified in making, that most tabic patients pass through the pre-ataxic phase of their disorder under the diagnosis of rheumatism or some similar affection, can now no longer be made. Our ability to recognize the advent of this disease has reached such a degree of refinement that the question arises whether we are always justified in alarming a patient who has a prospect of remaining free from invalidating complications for many years with the announcement of a disease which, above all other spinal affections, is looked upon with dread as equally hopeless, insidious, and distressing.
CLINICAL HISTORY.—The development of tabes dorsalis is typically slow and its precise commencement usually not determinable. In some cases this or that one of the characteristic symptoms of the disease preponderates from the beginning, and continues throughout the illness as a prominent feature; in others distinct stages can be recognized, each marked by one or several symptoms which were absent or slight in the other stages. In some cases the progress of the affection is marked by episodes which are absent or rare in other cases. As a rule, however, it may be stated that tabes is a progressive affection, marked by pronounced temporary changes for better or worse, which are often developed with astonishing rapidity, and subside as quickly, terminating fatally unless its progress be arrested by treatment or interrupted by some other fatal affection. The latter is by far the more frequent termination in the well-to-do class of sufferers.
For purposes of convenience we may consider the symptoms of the earlier period of the illness as pre-ataxic, and those of the later as the ataxic. It is to be remembered, however, that in the strictest sense of the term there is usually some disturbance of co-ordination even in the early period, while the symptoms of the pre-ataxic period continue over the ataxic period, and may even become aggravated with it. Often the patient does not himself suspect a spinal, or indeed any nervous, disorder, and consults the physician either on account of rheumatic pains, double sciatic neuralgia, bladder disturbance, diminished sexual power, amaurosis, diplopia, or even gastric symptoms, which on closer examination are revealed to be evidences of tabes. The determination of the initial symptoms is retrospective as a rule.
[p. 828]Of the subjective signs, one of the commonest, if indeed it be ever entirely absent, is a tired feeling, particularly noted in the knees and ankles. This sensation is compared to ordinary muscle-tire, but is provoked by slight exertion, and not as easily remedied by rest. Often a numb feeling is associated with it, although no objective diminution of cutaneous sensation be determinable. This combined feeling of tire and numbness, described as a going-to-sleep feeling in the ankle, has indeed been claimed by one observer1 to be pathognomonic of early tabes. Next in frequency, and almost as universal, are peculiar pains: these are manifold in character and distribution, but so distinctive as to alone suggest the existence of the disease from the manner in which the patient describes them. One variety, the lightning-like, is compared to a sudden twinge of great intensity shooting through the limb. The sciatic and anterior crural branches are the lines usually followed by this pain, but there are cases where perineal and abdominal regions are affected. Often the pain is so severe that the patient cries out or the limb is violently contracted under its influence. It differs from rheumatic pain in the fact that it is distinctly paroxysmal and that the intermissions are complete; that it is not greatly aggravated by motion nor relieved by rest, while the rheumatic pain is; that tabic pain is usually relieved, and rheumatic pain aggravated, by pressure, while hyperæsthesia is present with the former, and either absent or barely indicated with the latter. The lightning-like pains are sometimes combined with another form, which is even more distinctive in character. This form does not affect the distribution of special nerves, but is found limited to a small area which the patient is able to localize definitely: it may not exceed a centimeter or two in diameter, and within this area the pain is excruciating. It is either of a burning character or compared to the firm pressure of a vise or heavy weight, or to the tearing, boring, and jumping of a violent toothache.
1 Canfield, Lancet, 1885, vol. ii. p. 110.
While some patients escape these pains almost entirely,2 others are tormented with them at intervals for years, their intensity usually diminishing when the ataxic period is reached. There is little question among those who have watched patients in this condition that their pains are probably the most agonizing which the human frame is ever compelled to endure. That some of the greatest sufferers survive their martyrdom appears almost miraculous to themselves. Thus, in one case the patient, who had experienced initial symptoms for a year, woke up at night with a fulminating pain in the heels which recurred with the intensity of a hot spear-thrust and the rapidity of a flash every seven minutes; then it jumped to other spots, none of which seemed larger than a pin's head, till the patient, driven to the verge of despair and utterly beside himself with agony, was in one continued convulsion of pain, and repeatedly—against his conviction—felt for the heated needles that were piercing him. In another case the patient, with the pathetic picturesqueness of invalid misery, compared his fulminating pains to strokes of lightning, [p. 829] “but not,” he added, “as they used to appear, like lightning out of a clear sky, but with the background of a general electrical storm flashing and playing through the limbs.”
2 I have at present under observation two intelligent patients (one of whom had been hypochondriacally observant of himself for years) who experienced not a single pain, as far as they could remember, and who have developed none while under observation. Seguin mentioned a case at a meeting of the Neurological Society with a record of but a single paroxysm of the fulgurating variety. Bramwell (Brit. Med. Journ., Jan. 2, 1886) relates another in which the pains were entirely absent.
Either while the pains are first noticed or somewhat later other signs of disturbed sensation are noted. Certain parts of the extremities feel numb or are the site of perverted feelings. The soles of the feet, the extremities of the toes, the region about the knee-pan, and the peroneal distribution, and, more rarely, the perineum and gluteal region, are the localities usually affected.3 In a considerable percentage of cases the numbness and tingling are noted in the little finger and the ulnar side of the ring finger; that is, in the digital distribution of the ulnar nerve. The early appearance of this symptom indicates an early involvement of the cord at a high level. Some parallelism is usually observable between the distribution of the lightning-like pains when present and the anæsthesia and paræsthesia if they follow them. With these signs there is almost invariably found a form of illusive sensation known as the belt sensation. The patient feels as if a tight band were drawn around his body or as if a pressure were exerted on it at a definite point. This sensation is found in various situations, according as the level of the diseased part of the cord be a low or high one. Thus, when the lower limbs are exclusively affected or nearly so the belt will be in the hypogastric or umbilical region; if the upper limbs be much involved, in the thoracic region; and if occipital pain, anæsthesia of the trigeminus, and laryngeal crises are present, it may even be in the neck. Correspondingly, it is found in the history of one and the same patient: if there be a marked ascent—that is, a successive involvement of higher levels in the cord—the belt will move up with the progressing disease. This occurrence, however, is less frequently witnessed than described. In the majority of cases of tabes disturbances of the bladder function occur very early in the disease. Hammond indeed claims that in the shape of incontinence it may be the only prodromal symptom for a long period.4
3 In the exceptional cases where the initial sensory disturbance is marked in the perineal and scrotal region I have found that the antecedent fulminating pains had been attributed to the penis, rectum, and anal region; and in one case the subjective sense of a large body being forcibly pressed through the rectum was a marked early sign.
4 New England Medical Monthly, 1883.
I have under observation a patient who has been compelled to use the catheter daily for years, who has gradual disappearance of the knee-jerk and reflex iridoplegia, but who has presented no other evidence of tabes during the year and a half he has been watched. Among the exact signs of tabes, reflex iridoplegia and abolition of the knee-jerk are probably the earliest to appear. It may be assumed with safety that in ninety-nine out of a hundred cases both the inability of the pupil to respond to light and the absence of the knee-jerk will be found long before ataxia is developed. Cases are recorded where no other positive signs were found, and no other signs of the disease developed for a number of years,5 and others where disappearance of the knee-jerk was the very first indication.
5 Westphal, also Tuczek, Archiv für Psychiatrie, xiii. p. 144.
The opinion of observers as to the frequency of double vision as an early symptom of tabes is far from being unanimous. The majority of writers speak of it as rare, but it is probable that this usually transient symptom is forgotten by the patient, or because of its apparent triviality [p. 830] escapes notice. The patient while looking at an object sees a double image of the latter. This may last for a few seconds, minutes, or hours, and rarely for a day or week.6 A distinct history of this symptom was given by 58 out of 81 patients in whom I recorded the oculo-motor signs. By far the most important of the exact prodromal signs of tabes are two symptoms—one involving a special faculty of co-ordination, the other the reflex movements of the pupil. One or both of these must be present to justify the diagnosis of incipient tabes.7 The disturbance of co-ordination consists in an inability of the patient to stand steadily when his eyes are closed. The majority of healthy persons when tested in this way may show a little swaying in the beginning, but eventually they stand as steadily as they do with open eyes, and there is no subjective feeling of uncertainty as to falling. But the tabic patient exhibits oscillations, and makes efforts to overcome them which, instead of neutralizing, usually aggravate them and betray the great disturbance of his equilibrium. It is not as if he swayed merely because he is uncertain of his upright position, but as if some perverted force were active in throwing him out of it. It is found to be a pronounced feature even in cases where the patient with open eyes is able to walk nearly as well as normal persons, and experiences no trouble in performing intricate evolutions, such as dancing, walking a line, or even walking in the dark—faculties which the patient is destined to lose as his disease progresses.8
6 It has been asserted that the severer and more persistent diplopias are found with tabes dependent on syphilis.
7 Not even the absence of the knee-jerk ranks as high as these two signs. Aside from the fact that this is a negative symptom, it is not even a constant feature in advanced tabes.
8 It does not seem as if the disturbance of static equilibrium were due merely to the removal of the guide afforded by the eyes, for it is noted not alone in patients who are able to carry out the average amount of locomotion in the dark, but also in those who have complete amaurosis. Leyden (loc. cit., p. 334) and Westphal (Archiv für Psychiatrie, xv. p. 733) describe such cases. The act of shutting the eyes alone, whether through a psychical or some occult automatic influence, seems to be the main factor.
In most cases of early tabes it is found that the pupil does not respond to light; it may be contracted or dilated, but it does not become wider in the dark nor narrower under the influence of light. At the same time, it does contract under the influence of the accommodative as well as the converging efforts controlled by the third pair, and in these respects acts like the normal pupil. It is paralyzed only in one sense—namely, in regard to the reflex to light; just as the muscles which extend the leg upon the thigh may be as powerful as in health, but fail to contract in response to the reflex stimulus applied when the ligamentum patellæ is struck. For this reason it is termed reflex iridoplegia.9 It is, when once established, the most permanent and unvarying evidence of the disease, and is of great differential diagnostic value, because it is found in comparatively few other conditions.
9 It is also known as the Argyll-Robertson pupil. Most of the important symptoms of tabes are known by the names of their discoverers and interpreters. Thus, the swaying with the eyes closed is the Romberg or Brach-Romberg symptom; the absence of the knee-phenomenon, Westphal's or the Westphal-Erb symptom; and the arthropathies are collectively spoken of as Charcot's joint disease.
In a number of cases ptosis of one or both eyelids is noted at an early stage of the disease. It is usually temporary, and coincides as to time with the diplopia, if present.
Patients presenting some or all of the subjective and objective [p. 831] manifestations of tabes mentioned may continue in a condition of otherwise comparative health, enabling them to attend to their vocation for from one to twenty years, and it is not improbable that the pre-ataxic period may extend over nearly a lifetime. In a less fortunate minority of cases some of the most distressing evidences usually marking the last stages of the disease are found developed at the onset. Thus, cases are known where optic nerve-atrophy preceded the true tabic period by ten or more years; others in which trophic disturbances, manifested in spontaneous fractures of bones10 or violent gastric crises, or even mental disturbance, inaugurated tabes dorsalis, instead of closing or accompanying the last chapter of its history, which is the rule.
10 Berger, Deutsche medizinische Wochenschrift, 1885, 1 and 2.
The disturbance of co-ordination above spoken of as manifested in the inability of the patient to stand well with his eyes closed is the first step in the development of the characteristic ataxia which marks the full-blown affection. The patient finds that he tires more and more on slight exertion—not because his muscles are weak, but because he has to make more voluntary effort than a person in health. He finds that he stumbles easily—is unable to ascend and descend at the curbstone or to walk over an irregular surface with ease. Going down stairs is peculiarly irksome. “I would rather,” aptly said one patient, “troubled as I am in walking, go a mile in the street than walk up three flights of stairs; but I would rather go up six flights of stairs than walk down one.” Soon the patient notices that walking in the dark becomes more a feat of relative skill than the easy, almost automatic, act it was in health. His vocation, if it was one involving the use of the feet, becomes irksome, difficult, and finally impossible, and in a number of cases the upper extremities are also involved.11 Delicate motions, such as those required in needlework, in writing, and by watchmakers, musicians, opticians, and lapidaries, are clumsily performed; even coarser movements, such as buttoning the clothes and carrying a glass filled with water to the mouth, are performed in an uncertain and clumsy manner. Meanwhile, the disturbance of motion in the lower limbs progresses. Difficult as it formerly was for the patient to stand on one foot or with both feet together while the eyes were closed, he is now unable to do either with the eyes open. He straddles in his walk, or, in order to overcome the element of uncertainty involved in moving the knee-joint, keeps this joint fixed and walks with short, stiff steps. If ordered to halt suddenly while thus walking, the patient sways violently, and makes movements with his hands or arms to recover his balance, in some cases staggering and even falling down. He shows a similar unsteadiness when told to rise suddenly from a chair or to mount one, and it becomes impossible for him to walk backward. Later on, it will be found that his feet interfere in walking. He has lost the power of gauging the extent and power of his motions to such a degree that he may actually trip himself up. To neutralize in some way this element of uncertainty of his steps, the patient is compelled to exaggerate all his ambulatory movements, and there results that peculiar gait which was the first symptom directing attention to the [p. 832] disease to which it is due. The feet are thrown outward, and violently strike the ground; the heel touches the latter first, and the patient appears as if he were punishing the ground and stamping along instead of walking. The reason for his adopting these tactics are twofold. In the first place, he has a subjective sense of walking in a yielding substance, as if on a feather bed, air-bladders, cushions, or innumerable layers of carpet, and he therefore makes efforts to touch firm bottom. In the second place, his motor inco-ordination, in so far as it is not the result of anæsthesias, is greatest in those segments of his limbs which are farthest removed from the trunk, and which, enjoying the greatest freedom of combined motion, are also most readily disturbed. His uncertainty is therefore greater in the toes than in the ankle, greater in the ankle than in the knee, and greater in the knee than in the thigh: he prefers to touch the ground with the heel to touching it with the toes, and to move his limb in the hip than in the knee-joint. As the patient advances in life even this limited and clumsy form of locomotion becomes impossible: he takes to his bed, and it is found that he loses all sense of the position of his lower and occasionally of his upper limbs. He is unable to tell which limb overlies the other when his leg is crossed—unable to bring one limb in parallel position with another without the aid of his eyes. If told to touch one knee or ankle with the toes of the other side, his limb oscillates around uncertainly, and makes repeated unskilful dashes at the wrong point, and ultimately all but the very coarsest muscular co-ordination appears to be lost, even when the supplementary aid of the eyes is invoked.
11 Cases in which the upper extremities are intensely involved in the beginning are uncommon, and those in which they are more intensely involved than the lower, or exclusively involved, may be regarded as pathological curiosities.
Together with this gradual impairment and abolition of co-ordination, which has given the name of locomotor ataxia to the disease, but not always in that strict parallelism with it on which Leyden12 based his theory of inco-ordination, the sensory functions proper become perverted and impaired. Usually the determinable anæsthesias are preceded by subjectively perverted sensations, such as the numbness already referred to, or even by hyperæsthesia. Usually, all categories of cutaneous sensation, whether special or pathic, are impaired in advanced tabes; the points of the æsthesiometer are not readily differentiated; the patient is unable to correctly designate the locality which is touched or pinched; the pain-sense is occasionally so much blunted that a needle may be run through the calf of the leg without producing pain, and in some cases without being appreciated in any form. Even if the pain-sense be preserved, it will be found that its appreciation by the patient is delayed as to time. Not infrequently bizarre misinterpretations are made of the impressions acting on the skin. One of these, the feeling as if the patient were standing on carpet, cushions, or furs, whereas he may be standing on stone flagging, has already been mentioned as a factor in the disturbed locomotion of the patient. In the later period, numerous perversions of this kind are noted: to one of these, already mentioned by Leyden, Obersteiner has called renewed attention. It consists in a confusion of sides; the patient when pricked or touched on one foot or leg correctly indicates the spot touched, but attributes it to the wrong side.13
12 Klinik der Rückenmarkskrankheiten, Band ii.
13 Allochiria is the term applied by Obersteiner. Hammond has offered an explanation, which, as it is based on the assumption of altogether hypothetical nerve-tracts, and not in any sense accords with positively established facts, is more properly a subject for consideration in a theoretical treatise.[p. 833]
While it may be affirmed, as a general proposition, that the tendency of the tabic process is to abolish sensation below the level of the disease, there are noteworthy exceptions, not only in individual cases, but with regard to certain kinds of sensation; nor do the different kinds of sensation always suffer together. Thus, the pain-sense may be blunted and the contact-sense preserved, or, more commonly, the latter blunted and the former exaggerated, so that the unfortunate patient, in addition to being debarred of the useful varieties of sensation, those of pressure and space, has the painful ones exaggerated, as a hyperalgesia. According to Donath,14 the temperature-sense is usually blunted in tabes, and a greater degree of heat or cold can be borne without discomfort than in health; but in about two-sevenths of the cases studied there was increased sensitiveness to heat, and in one-seventh to cold. One of the commonest manifestations is delayed conduction. This interesting phenomenon has been especially observed in that phase of the disease where tactile perception is beginning to be blunted. If the patient be pricked with a pin, he feels the contact of the latter at the proper moment as a tactile perception, and then after a distinct interval, varying from one to four seconds, his limb is suddenly drawn up and his face contorted under the influence of an exaggerated pain. This fact furnishes one of the chief grounds for the assumption that there are distinct channels for the transmission of pain and tactile perception in the cord, and that they may be involved separately or with different intensity in the disease under consideration. In some advanced cases it is found that not only the transmission of pain-appreciation is delayed, but that there are after-sensations recurring at nearly regular intervals of several seconds, and accurately imitating the first pain-impression.
14 Archiv für Psychiatrie, xv. p. 707.
To what extent the muscular sense is affected in tabes at various stages of the disorder is somewhat in doubt. Strümpell15 by implication, and other writers directly, attribute the inco-ordination observed on closing the eyes to the loss of the muscular sense. As this symptom is also observed in patients who when they lie on their backs are able to execute intricate movements notwithstanding the exclusion of the visual sense, and as their uncertainty in an early stage is not always with regard to the position of their limbs nor the innervation of individual or grouped muscles, it seems inadmissible to refer the Romberg symptom16 to the loss of muscular sense alone.
15 Lehrbuch der Speciellen Pathologie und Therapie, p. 193, vol. ii.
16 It should be designated as static ataxia, in distinction from locomotor or motor ataxia, which is manifested in unskilled movements.
The important part played by eye symptoms in the early stages of tabes has been already referred to. Reflex iridoplegia is one of these early and persisting features; it is sometimes complicated with mydriasis, and occasionally with paralysis of accommodation of one eye. In the majority of my cases there was spinal myosis, often of maximum intensity; in a large number there was in addition irregularity of the outline of the pupil; and where there was mydriasis I found it to be quite symmetrical, in this respect differing from the experience of Müller17 and Schmeichler.18
17 Centralblatt für die Gesammte Therapie.
18 Loc. cit.[p. 834]
Atrophy of the optic nerve is a common and sometimes, as stated, the initial symptom of tabes. It is rarely found in its incipient phase in advanced stages. The patient who escapes involvement of the optic nerve in the pre-ataxic stage is very apt to escape it altogether. It is more frequently found either to precede the pre-ataxic period by months and even years, or to develop during this period, leading to complete atrophy in the ataxic period, and sometimes before. Erb calculates that 12 per cent. of tabic patients have optic-nerve atrophy; he probably includes only such cases in which the atrophy was marked or led to amblyopia. Including the lesser degrees of atrophy, it is found in a larger number of patients. Schmeichler claims as high as 40 per cent.19 If we regard those cases in which there is noted progressing limitation of the color-field of the retina as beginning optic-nerve atrophy, the majority of tabic patients may be said to have some grade of this disorder. The ophthalmoscopic changes are quite distinctive: at first there is noted a discoloration of the papilla and apparent diminution of the number of arterial vessels; the veins then become dilated; and finally the papilla becomes atrophied, the vessels usually undergoing a narrowing after their previous dilatation. In the first stages of this process visual power is not gravely impaired, but as soon as shrinkage has set in visual power sinks rapidly to a minimum, decreasing till only quantitative light-perception remains. This limited function usually remains throughout, but in a few cases complete amaurosis ensues. As the field of vision becomes diminished, the concentric extinction of quantitative perception is preceded by concentric extinction of color-perception, the color-field for green being the first to suffer; red follows, and blue remains last.
19 Archives of Ophthalmology and Otology, 1883.
In a large number of cases the only symptoms attributable to a disturbance of the cerebral functions are those connected with the motor relations of the eyeball and pupil, and the function and appearance of the optic nerve. The special senses other than those of sight and touch are rarely affected. Sometimes there is obstinate tinnitus, exceptionaly followed by deafness, attributed to atrophy of the auditory nerve. The development of symptoms resembling those named after Ménière is not referable with certainty to a disturbance of the same nerve.
The sexual functions become involved in all cases of tabes sooner or later. In the majority of cases there is a slow, gradual extinction of virile power; in a large minority this extinction is preceded by irritative phenomena on the part of the genital apparatus. Some patients display increased sexual desire and corresponding performing powers, but mostly they suffer from erections of long duration which may be painful, and loss of the normal sensations attending the sexual orgasm. There is no constant relationship between the intensity of the general affection and the diminution of sexual power. It is retained to a limited degree by patients who are barely able to walk, and it may be entirely destroyed in those who have but entered the initial period.
The bladder disturbance,20 which in some forms is usually found among the initial symptoms, is always a marked feature in the ataxic period. [p. 835] Usually, there is a frequent desire for micturition, with more or less after-dribbling; sometimes there is retention, alternating with involuntary discharge; complete incontinence may close the scene through the channel of an ensuing cystitis and pyelitis. With the incontinence of urine there is usually found obstinate constipation, which may be varied by occasional spells of incontinence of feces. The crises of tabes often complicate these visceral symptoms.
20 Contrary to what might be anticipated from the topographical nearness of the vesical and genital centres in the cord, the disturbances of bladder function and virile power do not go hand in hand.
The reflex disturbances are among the most continuous evidences of the disease. Of two of these, the disappearance of the patellar jerk or knee-phenomenon and the inability of the pupil to react to light, we have already spoken when discussing the initial period. Practically, it may be claimed that both are always found in typical tabes. It has been claimed that the patellar jerk may be exaggerated, or even that its disappearance is preceded by exaggeration. As this disappearance usually occurs extremely early in the pre-ataxic period, it is difficult to follow the deductions of those who claim to have watched an alleged earlier phase of exaggeration. It is more than probable that cases of combined sclerosis, in which the lateral columns were affected together with or earlier than the anterior, have been mistaken for typical tabes. Here, it is true, the jerk is first exaggerated through the disease of the lateral column, and later abolished as the lesion in the posterior reflex arch progresses and becomes absolute.
Other tendinous reflexes21 suffer with the knee-jerk in the peripheries corresponding to and below the involved level of the cord. The cutaneous reflexes are usually abolished, but may be retained in advanced stages of the disease. The same is true of the cremaster reflex.
21 Whether the tendon phenomena are true reflexes or not is a question still agitating physiologists. Opinion inclines in favor of their reflex nature, and, pathologically considered, it is difficult to regard them in any other light.
Opinion is divided as to the electrical reactions in tabes dorsalis. That qualitative changes never occur in uncomplicated cases all authorities are agreed, but while Strümpell and other modern writers claim there is no change of any kind, a number of careful investigators have found an increased irritability in the initial period, particularly marked in the peroneal group of muscles (Erb). In my own experience this is frequently the case, where lightning-like pains are the only subjectively distressing symptoms complained of.
While the symptoms thus far considered as marking the origin and progress of tabes dorsalis are more or less constant, and although some of them show remarkable remissions and exacerbations, yet may in their entity be regarded as a continuous condition slowly and surely increasing in severity, there are others which constitute episodes of the disease, appearing only to disappear after a brief duration varying from a few hours to a few days: they have been termed the crises of tabes dorsalis. These crises consist in disturbances of the functions of one or several viscera, and are undoubtedly due to an error in innervation provoked by the progressing affection of the spinal marrow and oblongata. The most frequent and important are the gastric crises. In the midst of apparent somatic health, without any assignable cause, the patient is seized with a terrible distress in the epigastric region, accompanied by pain which may rival in severity the fulgurating pains of another phase [p. 836] of the disease, and by uncontrollable vomiting. Usually, these symptoms are accompanied by disturbances of some other of the organs under the influence of the pneumogastric and sympathetic nerves. The heart is agitated by violent palpitations, a cold sweat breaks out, and a vertigo may accompany it, which, but for the fact that it is not relieved by the vomiting and from its other associations, might mislead the physician into regarding it as a reflex symptom. In other cases the symptoms of disturbed cardiac innervation or those of respiration are in the foreground, constituting respectively the cardiac and bronchial crises. Laryngeal crises are marked by a tickling and strangling sensation in the throat, and in their severer form, which is associated with spasm of the glottis, a crowing cough is added.22 Enteric crises, which sometimes coexist with gastric crises, at others follow them, and occasionally occur independently, consist in sudden diarrhœal movements, with or without pain, and may continue for several days. Renal or nephritic crises are described23 as resembling an attack of renal colic. The sudden disturbances of bladder function have been described as vesical crises, and recent French observers have observed so-called crises clitoridiennes in female tabic patients which were characterized by voluptuous sensations. All of these symptoms have these in common: that they last but a short time, that their disappearance is as rapid as their advent, and that they depend for their distribution on the attitude of the disease in the cord. The vesical crises are more apt to occur early than late in the disease and where the belt sensation is in the hypogastric region. The gastric and enteric crises are usually found when the belt is in the epigastric level, and the bronchial, cardiac, and laryngeal crises when it is in the thorax and neck. Some connection has been observed between the occurrence of the lightning-like pains and these crises. Thus, a sudden cessation of the former is sometimes the forerunner of the latter. It is also found that one variety of these crises disappears to give way to another: this is particularly noticed with the bronchial crises, which often cease suddenly, to be followed by vomiting.
22 Krause, in a paper read before the Society of Neurologists at Berlin (Neurologisches Centralblatt, 1885, p. 543), found either laryngeal crises or other laryngeal symptoms, such as demonstrable ataxia of movement of the vocal cords, in 13 out of 38 cases. This proportion would be far too high for tabes in general; his cases were probably advanced ones. He established the interesting fact that the laryngeal crisis may sometimes be provoked by pressure with a probe on the superior laryngeal nerve at its laryngeal entry-point. Jastrowitz claims to have determined the existence of actual paralysis of the vocal cords with the crises, but Krause concludes from the experimental inductibility of the crisis that it cannot be due to a posticus paralysis. In a discussion on the subject Remak affirms that a unilateral paralysis of the crico-arytenoideus posticus may be an early or the earliest symptom of tabes. It seems, however, that in all cases where he determined such paralysis there had been disturbances of function of other cranial nerves in unusual severity at about the same time.
23 They must be extremely rare: they have not occurred in a single one of my 81 private cases, nor do I recall one in clinic or dispensary experience.
There is some analogy between the exceptionally-occurring mental disturbance of tabic patients and the crises. Like them, it resembles a disturbance of innervation, in this instance the centres regulating the cerebral circulation appearing to be at fault. It also seems as if in cases of this character the direction of the mental disturbance were determined in some sense by the emotional relations of the oblongata, for the insane outbreak usually consists in a brief but extreme outburst either of a [p. 837] depressed and melancholiac or an expansive maniacal or delirious outburst. It is a very rare occurrence, and usually limited to the latest stages. Much more common is the development of paretic dementia, but this is to be regarded rather as a complication than an integral feature of tabes. Most tabic patients retain their mental equilibrium to the last moment; some develop truly heroic resignation to their terrible sufferings and gloomy prospects; and a few, becoming irritable, petulant, and abnormally selfish, show the effect of invalidism manifested equally with other chronic diseases.
In addition to the visceral crises there are other disturbances of innervation of a nutritive or trophic character which are characteristic of tabes. There is scarcely one of the eruptions or other changes which are attributable to central nervous disease which may not occur at some one or other period of this disease. Thus, herpetic eruptions may occur independently or in conjunction with lancinating pains, in one case even corresponding to the area of the belt sensation. Discoloration of the skin or hair, the latter turning gray or white in circular24 or in irregular patches, spontaneous falling of the nails, spontaneous hemorrhages in the matrix of the nail, ichthyosis,25 purpura, diffuse œdemas, localized perspiration sometimes associated with sudamina and accompanied by ecchymoses, muscular atrophies, bullæ, and pemphigus-like eruptions, have been noted by various observers. As yet, they are to be regarded rather as clinical curiosities than as constant features, as diagnostic criteria, or as presenting special indications for treatment. The trophic disturbances affecting the bones and joints and a peculiar ulcerative process known as the perforating ulcer of the foot are better studied, and, ranking among the most formidable and striking manifestations of tabes, merit special consideration. The tabic joint affection, first described by Charcot as a trophic manifestation of tabes, is usually located in the hip or knee, but almost any joint, including the temporo-maxillary articulation, may be its seat. The earlier or lighter forms consist in serous exudations with or without active local manifestations resembling those of synovitis; but the commoner and graver form consists in actual deformity of the articular surfaces, such as enlargement or atrophy, sometimes supplemented by the formation of osteophytes. In addition, spontaneous dislocations occur in a manner which is often quite surprising.26 As a type of such an occurrence the following may serve: A tabic patient presented a synovial swelling of the left knee of truly enormous dimensions; as soon as this became reduced a distinct crepitus was elicited, and both the femoral and tibial articular surfaces found enlarged. The whole process occupied only a few days; the lateral ligaments were then found so relaxed that the leg could be freely moved in every direction.
24 Rossolymmo, Archiv für Psychiatrie, xv. p. 727. I have never observed this symptom as beautifully developed as in a case of spinal irritation, in which the possibility of the existence of any organic disease could be positively excluded. Bulkley has observed albinism.
25 In three cases by Ballet et Dutil, Progrès médicale, May 19, 1882.
26 Boyer (Revue de Médecine, 1884, p. 487) records a case where the hip became luxated spontaneously as an early symptom.
The connection between the morbid process in the spinal cord and these remarkable arthropathies is as yet unexplained; and as Charcot's original [p. 838] proposition, that they can be always referred to lesions in the anterior horns of the gray matter, has not been sustained, some of the German clinicians, notably Strümpell, are inclined to attribute them, in part at least, to ordinary results and accidents due to the anæsthesia and its disturbing effect on voluntary and automatic joint protection. A controversy arose which was participated in by the Clinical Society of London,27 and evoked opinions from nearly all the eminent neurologists of Europe. The result of this thorough discussion has been to establish the joint affection as a true tabic symptom due to the same morbid process which underlies the less enigmatical symptoms of the disease. One of the best reasons for regarding these joint lesions as of trophic origin is the fact that they are associated with textural bone-changes by which they become either unduly soft or brittle, and therefore exposed to apparently spontaneous fracture. Cases of fracture of almost every long and some of the short bones are recorded, among the most remarkable being one by Dutil,28 where fracture of the radius occurred without adequate cause in the initial period of tabes; and one by Krönig,29 in which the patient, who had been tabic for eight years, broke a lumbar vertebra while catching himself in the act of falling down stairs.
27 The question was formally raised by Morrant Baker at the December meeting in 1884, and the discussion participated in by Charcot himself. Among the opponents of Charcot's theory were Jonathan Hutchinson and Moxon, the latter of whom administered a sound and well-merited criticism regarding some of the premature, if not sensational, announcements of the distinguished French neurologist. He compared the joint lesions of tabes to decubitus: just as the latter can be avoided by a proper protection of the exposed parts, so the former would not occur if the joints could be kept in a, surgically speaking, normal state. Moxon seems to have forgotten, in suggesting this comparison, that there is a form of decubitus which will occur independently of the greatest care and in spite of every measure taken to arrest it, and which can be attributed only to an obscure but active perversion of nervous nutritive control. Barwell, Paget, Herbert Page, Broadbent, and McNamara agreed that the joint lesions are not of surgical or rheumatic origin, but essentially signs of the nervous affection. Although Barwell's claim, that the rheumatic and tabic joint diseases are essentially different, because the former is hyperplastic and the latter is atrophic, is not borne out by all cases of tabic joint disease, some of which are certainly hyperplastic, yet the other reasons advanced for regarding these affections as distinct, and considering the joint affection of Charcot as a trophic disorder, far outweighed those advanced by the opponents of this view. In fact, the only ground the latter had to stand on was the fact that Charcot's asserted anatomical foundation was found to be chimerical.
28 Gazette médicale de Paris, 1885, No. 25.
29 Zeitschrift für klinische Medizin, 1884, vii., Suppl. H.
Another reason for considering the arthropathies as of central origin is their chronological association with other signs whose trophic origin cannot be disputed, such as unilateral sweats and œdemas and visceral crises. They are also found to correspond in many cases to the lancinating pains both in location and time.
The feet of an advanced tabic patient usually appear deformed; the extremities of the bones, particularly at the metacarpo-phalangeal articulation, are thickened, and the axis of the foot as a whole is bent. It is a question how far this deformity may be due to persistent faulty innervation of the muscles going to the foot and to ensuing mechanical influences. A most pronounced deformity found in a few cases has been designated by Féré as the tabic foot.30 It consists in the thickening of the tissues on the inner side of the foot, obliterating its arch in such a manner that in standing the plantar surface is everywhere in contact with the floor. [p. 839] With this the tarso-metatarsal and the metacarpo-phalangeal joints of the great toes appear greatly swollen.
30 Pied tabétique—Revue de Médecine, 1884, p. 473.
There is less dispute concerning the nature of the so-called perforating ulcer of the foot. This lesion occurs only in cases where the central or peripheral nervous apparatus is diseased; thus, it may occur with neuritis, and it is therefore unanimously regarded as due to morbid nervous influences. In tabes it may follow an exacerbation of the fulminating pains. It consists in a swelling of the tissues of the foot; the skin becomes firm and thickened; deep sinuous ulcers are then developed, showing but slight if any tendency to granulate, and which extend down to the bone, the latter usually remaining unaffected.31 In a few cases more remarkable accidents due to disturbed nutrition have been noted. Thus, J. Hoffmann records a subcutaneous rupture of the Achilles tendon, and in another case the spontaneous discharge of all the teeth of the upper jaw within about a week's time.32
31 Like most of the manifestations of advanced tabes, the perforating ulcer may occur exceptionally as a pre-ataxic symptom. Thus, Suckling (British Medical Journal, 1885, April 4, p. 693) mentions its preceding the development of tabes proper by one year.
32 Berliner klinische Wochenschrift, 1885, No. 12. In this unique case the loosening and falling out of the teeth preceded the tabes by a year. Demange, who observed the same phenomenon in two cases, found that the ascending root of the fifth pair was involved. The only analogous observation in my experience relates, like the bleaching of the hair in circular patches, to a case of spinal irritation: here the gums and alveolar borders underwent atrophy, exposing the roots of the teeth to beyond the normal alveolar border: first the right upper row, then the right lower row, and finally the teeth on the left side in the same order, showed this condition; only the most posterior fell out.
COURSE.—Tabes dorsalis is to be regarded as an extremely chronic affection. Its development, as previously stated, is insidious,33 and the symptoms demonstrating the advent of the disease may be so slight for many years that the patient does not regard himself as ill or as likely to become so. In this condition he may remain for ten or more years; and there are cases recorded where the exact signs of the incipient stage were well marked, and yet no ascertainable progress was made in a period of such long duration that the inference naturally follows of a much longer prospective period in which the patient would not have become ataxic. There may be distinguished two forms of invasion: the more frequent is marked by the development of the terebrating, fulgurating, and fulminating pains, to which, sooner or later, the abolition of the pupillary and certain other deep reflexes is added. In the vast majority of cases they are found absent when the physician's attention is directed to the question of the existence of spinal disease. In about one-fifth of the cases pain is at no time a prominent feature of the disease, and may be, as is established by the cases cited, entirely absent. In these patients the first symptoms noted are muscle-tire on slight exertion. Usually, the evidences of disturbed sensation and innervation begin in one extremity or preponderate in it, but symmetry is soon established. The same is noticed in the extension of the morbid process: when the ulnar distribution is involved—which is the first danger-signal on the part of the cervical enlargement of the cord—usually one side is first involved, but the other soon follows, and becomes affected in equal or nearly equal degree. In the [p. 840] overwhelming majority of cases the disease manifests itself in the lower extremities first, remaining limited to them for a long period, and if extending to the upper extremities doing so in much slighter intensity than in the lower. Gull, Leyden, and others have observed cases where the arms were first and chiefly involved; but this is extremely rare. Cases of a simultaneous involvement of the upper and lower extremities are more frequently noted. The symptoms detailed above are developed in varying order in different patients, and the line has been already indicated which separates the progressive from the episodial features of the disease. Even in the ataxic period the patients may remain in a comparatively stationary period for many months and years.34 The general bodily nutrition is usually good, and the muscular strength, as such, rarely affected to any noteworthy extent until the extreme phase of the disease is reached. Even the formidable-appearing crises and trophic disturbances, though occasionally fatal, are not always so. The direct danger from the disease proper, so far as life is concerned, is in the possible development of cystitis and pyelitis, of the malignant bed-sore, and of delirium and coma, the latter of which is occasionally found to be due to cerebral hemorrhage—a lesion which some writers regard as possibly due to some impalpable influence of the spinal disease on the cerebral circulation.35
33 Cases of acute locomotor ataxia have been described. In no instance are they pure or typical, and the last case of the kind published in America, beginning, as it is evident from the account, with signs of general myelitis, illustrates the impropriety of utilizing one or a few symptoms as determining nomenclature.
34 Thirteen patients are now under my observation, or I have been able to obtain reliable medical information concerning their condition, who have been in the ataxic period since the date of my first examination, varying from a year to seven years ago. Not one of these patients is materially much worse than at that time. Two only died, both being bedridden at the time they came under observation. Of the first group, three have shown more or less lasting improvement in respect to special symptoms, as will be detailed in connection with the treatment.
35 In a case of sudden death, with an asthma-like seizure, of a tabic patient under the charge of T. A. McBride, I found an intense injection of one (the right) vagus nucleus, the color of the ala cinerea and of the nucleus on section being almost black.
MORBID ANATOMY AND PHYSIOLOGY.—Our knowledge of the structural disease underlying the symptoms which comprise the clinical picture of tabes dorsalis is perhaps the clearest in the domain of spinal pathology. Not alone the commencement of the morbid process and every stage of its subsequent encroachment on the spinal cord, but also its relations to special symptoms, have been demonstrated in numerous cases by some of the most careful German and French investigators.
In advanced cases of tabes the disease of the spinal cord is so evident that it was noted even by earlier observers, the region of the cord lying between the posterior nerve-roots being altered in color, consistency, and dimensions. It is gray instead of white, hard instead of soft, and considerably shrunken. The gray discoloration of the surface appears to be complete in the lumbar and lower dorsal region; it is less intense in the upper dorsal and cervical part of the cord; and often shows a division into three streaks, of which one, in the middle line, occupies both columns of Goll, while on either side another extends in the inner side of the posterior root-entry. The posterior roots themselves are frequently atrophied, and exhibit a firmer consistency and darker color than in health. On making cross-sections of the spinal cord it is found that the gray discoloration extends inward, involving more or less of the posterior columns in well-defined areas. Microscopic examination shows that the myelin of the nerve-tubes is either destroyed or atrophied, and the axis-cylinder is found to be affected in the same way, usually presenting alterations in its [p. 841] refraction and diameter where it is not entirely destroyed. In the maximum foci of disease the conducting elements of the cord are nearly destroyed, and their place is occupied by a firm connective substance made up of wavy bundles, enclosing here and there a few atrophied axis-cylinders with wasted myelin-sheaths. The blood-vessels participate in the morbid process, at least as far as the larger vessels are concerned: these are sclerotic, their lumen appears contracted, the adventitial sheath is hypertrophied and occupied by a nucleated, fibrillar connective substance. The capillaries are sometimes normal, or participate in the morbid process to the extent of a thickening of the extra-endothelial sheaths which is either hyaline or fibrillary, and may show inflammatory cell-proliferation. It is evident that the increase of connective tissue in the posterior columns is not merely a relative one, due to the condensation of the normal neuroglia after the disappearance of the normal nerve-tubes, but is the result of actual proliferation. Opinion is somewhat divided as to whether this is to be considered as an inflammatory interstitial proliferation or as a more passive development of tissue compensating for the destroyed conducting elements. My own observations incline me to the belief that in syphilitic tabes the morbid process is essentially interstitial, while in non-syphilitic tabes it is parenchymatous, the disease beginning in the nerve-tubes proper. Perhaps the controversies between pathologists as eminent as Schultze, Tuczek, Rumpf, Zacher, Kahler-Pick, Rosenstein, and Adamkiewicz—who are rather evenly divided into opposing camps, one maintaining the parenchymatous, the other the interstitial, origin of the disease—may be solved when we learn to distinguish between the non-syphilitic and syphilitic cases, which is clinically, as yet, impossible. The difficulty of deciding what is a parenchymatous and what is an interstitial disease of the cord is considerably enhanced by the fact that the neuroglia, which by some at least is regarded as an interstitial connective tissue, is derived, like the nerve-substance proper, from the upper or neuro-epidermic germ-layer of the embryo, and not from the mesoblast, which furnishes all other connective substances in the body.
It is regarded as well established that the sclerosis of the areas of the spinal cord which are affected is preceded by a stage of granular degeneration.36 This is supported by the facts that the sclerotic areas are surrounded by a zone in which sclerosis has not yet developed, but which is in a state of granular degeneration, and that in more advanced tabes this belt is also found sclerosed. In paretic dementia, a disease whose complicating cord affection closely resembles that of locomotor ataxia, a granular degeneration of the posterior columns is very common in earlier periods, while in later periods a sclerotic tissue is found in the same locality.
36 Westphal, Archiv für Psychiatrie, ix. p. 725.
I regard these observations as opposed to the assumption of Strümpell that tabes is a system-disease of the cord in the sense in which he employs that term. In his fascinating and suggestive thesis on the systemic affections he cites the observations of Tuczek made on the posterior sclerosis ensuing from ergotism as confirming his view that special systems of nerve-fibres are separately vulnerable to special morbid influences. The remarkable correspondence between the topographical distribution of the lesion of ergotin tabes described by Tuczek and the characteristic areas [p. 842] of sclerosis found in the column of Burdach in ordinary tabes, seems to justify a very different conclusion. Ergot exerts its morbid influence through a disturbance of nutrition. Just as it produces gangrene by constriction of the nutritive vessels of the fingers and of whole extremities, so it produces interference with nutrition of those nerve-elements in the cord which are most liable to suffer from general arterial constriction. These are presumably those portions which are supplied by the longest and narrowest arterial stems—a condition obtaining in precisely those parts of the cord which are affected both in ergotin tabes and in ordinary tabes.
It has also been supposed that the morbid process began in the posterior roots and crept in with these, thence extending upward.37 This view is opposed by the fact that there is no constant relationship between the root lesion and the cord lesion; the sclerosis of the root-zones within the columns of Burdach I found to be absolute in at least one case where the outer nerve-roots were not distinctly affected.38
37 Takacs is the most recent defender of this view.
38 The root lesion may, like that of the column of Goll, according to a minority of the interpreters, be a secondary process, for in ergotin tabes (Tuczek) both are usually intact.
In typical tabes the sclerotic process begins in a special triangular field of the posterior column in the lumbar enlargement of the cord. The innermost of the posterior rootlets run through this field, which has been designated by the French school as the posterior root-zones, and the rootlets become exposed to all the vicissitudes which the conducting tracts are destined to undergo in consequence. Throughout the remainder of the cord it is the involvement of the root-zone which indicates the advance of the affection upward. At a time when the lesion is comparatively slight in the cervical level, manifesting itself by a slight grayish or reddish streak to the naked eye, a faint, pale discoloration in chromic-acid specimens, a deeper stain in carminized, and a pallor in sections stained by Weigert's method, the affected part in the lumbar region has undergone great shrinkage; scarcely a single myelin-tube is preserved to receive Weigert's stain within the affected area; the latter involves nearly the entire field between the cornua, and absorbs carmine deeply, so that it is difficult to differentiate the gray and white substance in carminized sections. A small part of the posterior column which most closely adjoins the posterior (gray) commissure remains free in all cases; so also does a small laurel-leaf-shaped field bisected by the posterior median septum. Examination with higher magnifying powers, aided by the modern improved methods of preservation and staining, reveals that the gray substance of the posterior segment of the cord is usually more or less diseased. In advanced cases the gelatinous as well as the spongy part of the posterior gray horn, and even the posterior gray commissure, undergo such considerable atrophy that they may occupy but half the normal area. In some cases the columns of Clarke appear to be involved quite early in the disease.39
39 Leyden discovered the degeneration in the fibres which in part make up these columns and correctly traced its origin to the posterior rootlets. Lissaner and Zacher (Archiv für Psychiatrie, xv. p. 437) confirmed him, the latter finding, as Leyden was the first to discriminate, that the cells may escape while the fibres are materially diminished. Krause claims that the columns of Clarke are constantly affected, but not necessarily in their entire length, the higher levels appearing quite normal at a time when the lower are severely involved (Neurologisches Centralblatt, 1884, p. 50).[p. 843]
The triangular field in the lumbar part of the posterior column, which is one of the typical starting-points of the affection, contains those ascending nerve-bundles which in their cephalic course emancipate themselves from the column of Burdach and constitute the slender columns of Goll. The result is that the degenerative process creeps up these columns at the same time that it ascends in the root-zones and deep portions of Burdach's columns. Some authorities regard this as a mere extension by contiguity;40 others incline to consider it a secondary degeneration. It may extend to the medulla oblongata, becoming lost in the level where the nucleus of the column of Goll terminates, and is accompanied, at least in those advanced cases in which the upper extremities are involved, by a comma-shaped area of degeneration in the adjoining part of the column of Burdach, which similarly extends into the oblongata and terminates slightly more cephalad. In typical advanced tabes, therefore, the cross-section of the cord exhibits a characteristic distribution of the sclerosis in each level. As this distribution is associated with certain constant symptoms, it is permissible to attempt bringing certain features of the lesion in relation with special features of the disease symptoms. The posterior gray horns and the posterior white columns, together with other fibre-systems connected with them, are much more complicated in structural and physiological relations than the corresponding anterior structures. The relations of the anterior rootlets to the gray substance, and those of the motor ganglionic elements to their controlling tracts, are comparatively simple; those of the posterior roots are very intricate. They run up, in great part, at an angle to the longitudinal tracts; a few pass in directly, and still fewer dip to a lower level. The result is that a section of the cord made in the longitudinal direction through the root-zones, so as to pass from the root-entry to the anterior commissure, shows the column and root-fibres to be woven into each other like a plait. Trabeculæ of connective tissue, dragged in as it were with the posterior roots, fill up the interstices of this labyrinth. They are particularly dense in the lowest part of the lumbar enlargement of the cord, constituting the so-called posterior processi reticulares. It is reasonable to suppose that the overlapping of ascending and descending root-fibres, associated with the presence of an extra amount of connective tissue, imbedded as this fibre-maze is in that part of the cord which is most distant from its lymphatic emunctories, affords a favorable soil for slow inflammatory trouble. This is the primary field of tabic sclerosis, and in it the disease may remain most intense for years, extending but slowly and with diminishing intensity upward, hand over hand, as it were, on the natural ladder which the intertwined fasciculi and their matrix constitute. The longitudinal tracts which lie in and near the root-zones belong to the so-called short fibre systems, uniting the segments of higher and lower levels of [p. 844] the cord with each other. As the sclerotic process ascends it involves the caudal ends of these systems: they consequently undergo secondary degeneration, and, shrinking in their turn, affect the caudal part of the next system above in the same manner. The morbid process in the column of Burdach may therefore be considered as a combination of inflammatory and degenerative changes, the inflammatory products causing a series of short ascending degenerations, and the vulnerable path thus established being followed by a cirrhotic condition in which the connective and vascular structures participate actively. With regard to the reasons for regarding the degeneration of the column of Goll and that of the comma-shaped field near it as a secondary process due to the cutting off of its apparent nerve-supply at the caudal end, and of the posterior nerve-roots or their provisional terminations, they may be stated in this way: When the lesion of the primary field is limited to the lower lumbar or sacral part of the cord, the degeneration of the column of Goll is limited to its postero-internal part; when the upper lumbar and lower dorsal cord is involved, the entire tract is affected; and when the cervical portion is diseased, the supplementary comma-shaped area degenerates. In other words, the projection tract of the sciatic nerve, as far as it is represented in Goll's column, suffers in the first, that of the crural nerves in the second, and that of the brachial nerves in the third instance. In all advanced cases of tabes the affection of the column of Goll is in direct proportion to the altitude of the lesion in the primary field. Symptomatically, it bears an equally constant relation to the ataxia.41 No case is on record in which these columns were totally degenerated without some motor inco-ordination of the lower extremity having been observed during life; and no case is recorded in which brachial ataxia had been a marked and persistent feature in which the comma-shaped area—area of the column of Burdach—was healthy.
40 It is held by them that the histological character of the change of the columns of Goll is not different from that in the column of Burdach. Zacher (Archiv für Psychiatrie, xv. p. 435) urges that it does not resemble true secondary degeneration, beginning in the vessels and connective substance instead of the nerve-fibres. Schultze (ibid., xiv. p. 386), on the other hand, recognizes a primary involvement of the nerve-fibres in both of the areas of fascicular degeneration in tabes. The observation of intact axis-cylinders by Babinski in the sclerotic fields is in conflict with the latter's claim, and the various differences of observation and interpretation seem to be reconcilable only on the assumption that there are two different modes of origin, both leading to nearly the same results and occasionally combined in one and the same case.
41 Krause's case and others show that the ataxia of movement is not influenced by lesion of the column of Clarke; but we are not informed as to the static equilibrium of the patients in whose cords these columns were found intensely affected.
It is scarcely necessary to seriously consider the suggestion of Strümpell, that the lesion of the column of Goll is in relation with the bladder disturbance.42 Cases are on record by Wolff and others where this lesion was intense and there was little or no bladder disturbance.43
42 Archiv für Psychiatrie, xii.
43 The column of Goll is not present in those mammals which, like the porpoise, have no developed hind limbs, but these animals have urinary bladders.
If the disease of the column of Goll were a primary systemic affection independent of the disease of the root-field, it would be difficult to understand why it, as well as the likelihood of finding a corresponding degeneration of the direct cerebellar tract, increases with the extent to which this field is involved. This occurrence becomes quite clear when we remember that both the direct cerebellar tract and that of Goll, being centripetal, are under the trophic dominion of the posterior nerve-roots. The opinion is not distinctly expressed, but implied in some writings, that the column of Goll degenerates because of a general transverse cord lesion at a low level; this is not the case in the tabic cord. There is a difference in appearance between that part of the primary field which corresponds to the column of Goll in the lumbar cord and the surrounding sclerosis in early cases: it is more intensely degenerated, more [p. 845] homogeneous in appearance, and more evenly stained. The other part of the triangular field presents a more trabecular appearance. In the specimen represented in the accompanying figure this is easily recognized: the darker field corresponds exactly with the ascending degeneration, which follows compression of the cauda equina,44 and is the sciatic equivalent of the column of Goll.
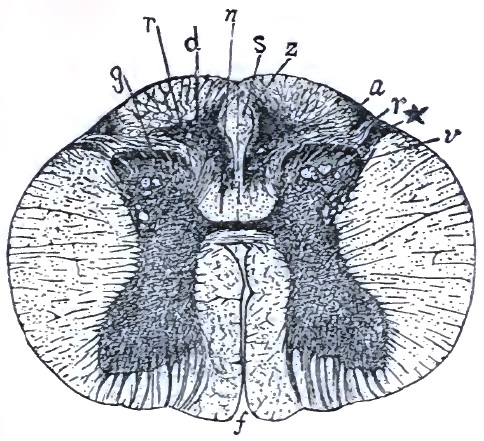
44 I have also found that this field corresponds to the column of Goll in its myelinic development: the lumbar part of this column—designated as such by Flechsig—is an entirely different tract, which enjoys a remarkable immunity from disease in tabes.
As illustrating the bearing of the lesion of the column of Goll on the motor ataxia I may refer to two cases which happen to be related side by side by Strümpell (Archiv für Psychiatrie, xii. p. 737, Cases 1 and 2). As far as the lumbar segment of the cord is concerned, the distribution of the lesion is similar; but in the one presenting marked motor ataxia the triangular field was slightly diseased, and there was no upward extension of the lesion in the column of Goll. In the other, with marked ataxia, the triangular field was intensely diseased, and ascending degeneration (?) occurred in the sciatic fields of the latter.
In support of the view that the comma-shaped area in Burdach's columns is homologous with the fibres of the column of Goll, it is to be advanced that degeneration of this field bears the same relation to symptoms in the distribution of the ulnar nerve that degeneration of the column of Goll bears to sciatic and crural symptoms. Where the initial pains and subsequent tactile and locomotor disturbance were severe, this field was found affected, and most so in the side where the symptoms had been most intense (Friedreich-Schultze's cured cases, Archiv für Psychiatrie, xii. p. 234). This area has no direct connection with the root-fields. Secondly, in a primary system disease of the column of Goll, associated with degeneration of the nucleus of the column of Goll, described by Scoli, an irregular encroachment of the column of Burdach was noted. Third, the innermost fibres of the column of Burdach (those belting the nucleus in the oblongata) have the same relation to the interolivary layer which the column of Goll has through its provisional nucleus of termination.
While the evidence of high lesion of the cerebral continuation of the column of Goll, and, what I regard as its homologue, the comma-shaped area of Burdach, together with the constant association of marked degeneration of these columns with motor ataxia, is strong positive proof of its relation to this symptom, there is equally strong evidence negativing its relation to any other of the prominent symptoms of tabes dorsalis. Thus Babesin (Virchow's Archiv, lxxvi. p. 74) found degeneration of the posterior columns limited to the column of Goll, and the patellar reflex was not destroyed; the root-fields at the upper lumbar levels were intact. That the columns of Goll have been found profoundly affected without bladder disturbance has been stated previously, and constitutes a stronger argument against Strümpell's view than the frequent observation of bladder trouble in spinal diseases, along with which these columns may be entirely free.
Among the various constituents of the posterior columns which appear [p. 846] to present a relative immunity to the disease, aside from the area near the posterior commissure and the laurel-leaf-shaped area of the posterior septum, Strümpell noted one which is situated at the periphery of the cord, bordering on the entry-line of the posterior roots and the inner contour of the posterior roots. In the few cases where it was found destroyed there was, what is a comparatively rare thing in moderately severe tabes, complete analgesia. It is not, however, certain that there is a necessary connection between the pathological and clinical fact here. The nerve-roots themselves are involved within the diseased area of the root-zones. The lesion is one of a kind which, affecting a nerve-trunk, would produce first irritation of, then impediment to, and ultimately destruction of, its function. The clinical parallel to this is the occurrence of the lightning-like pains in the earlier phases of the disease, which are followed by delayed pain-conduction, and finally by loss of sensation. Of the rootlets or fibres subservient to the various sensory and reflex functions mediated by the posterior roots, those which convey the centripetal impression normally evoking the patellar jerk appear to be the most vulnerable, or, because of their limited number, the earliest to be destroyed or compressed, with the result of total functional paralysis.45
45 It is now conceded that, as Westphal claimed, the patellar jerk is always abolished when the upper lumbar level of the root-zones (bandelettes externes of Charcot) is involved. Tshirijew has shown that the translation of the knee-jerk reflex occurs in a single segment of the rabbit's cord at the homologous level. In transverse sections a distinct fascicle may be seen coursing from the innermost root-fibres toward the antero-intermediate cell-group of the anterior horn; it furnishes a pictorial substratum, if not anatomical proof, for the patho-physiological observation, and harmonizes with the fact that it is the innermost rootlets which usually suffer first. Perhaps the delicacy of this tract accounts for the frequent disappearance of the jerk in old people as a result of senile sclerosis.
With regard to the interpretation of the various tactile sensory disturbances of tabes and the delayed pain-sense conduction little positive advance has been made. That the lesion of the root-zones and gray substance is responsible for them seems to be the general conclusion of French and German observers. Recent researches have shown that disease of the peripheral nerves (multiple neuritis) may produce sensory phenomena which it had previously been customary to regard as pathognomonic of disturbance of their intraspinal terminations and continuations. At the same time, we are confounded by the observation of Erb, that even retardation of conduction of the pain-sense, which the dictum of Schiff taught us to regard as a sign of disturbed function of the spinal gray matter, is also produced by peripheral neuritis.
Immediately adjoining the gelatinous apex of the posterior horn there is a column of vertical fibres which bear a relation to it resembling that [p. 847] of the ascending root of the fifth pair in the oblongata to the tuber cinereum of Rolando. Sclerosis of this column, as well as of the ascending root in question (Demange), has been found in tabes, and usually in association with pronounced trophic disturbances. In a number of cases (Oppenheim, Eisenlohr, and others) where spasmodic laryngeal crises had been a marked feature during life, lesion of the floor of the fourth ventricle, or atrophy of the pneumogastric nerve, or even of its nucleus, was found. In one case with marked gastric crises I found sclerotic changes of the arteries in the ala cinerea.
With regard to the involvement of the peripheral nerves proper, aside from the optic, opinion is somewhat divided. The discovery of multiple neuritis, and the recognition of the fact that it had been erroneously confounded with tabes, led Dejerine to claim that tabes might be of peripheral origin. He even proposed to account for the oculo-motor trouble on the basis of an affection of the oculo-motor nerves. This explanation has been repudiated by Westphal and sound authorities generally. That the peripheral nerves are occasionally involved in tabes was already known to Friedreich in 1863,46 and later Westphal found the cutaneous branches in an advanced tabic patient to present similar changes to those discovered by Friedreich: these findings are confirmed by his Japanese pupil, Sakaky. The nerve-tubes are atrophied, the axis-cylinder being often preserved, and the interneural connective substance is proliferated. But there is no constant relation between these changes and the symptoms of the disease; in one of Sakaky's cases the nerves of an extremity which had been the seat of severe sensory symptoms were entirely normal. The findings in the peripheral nerves of tabic subjects lose much of their value in view of their recent discovery in marantic persons47 advanced in life, but who had no nervous disease whatever.
46 Virchow's Archiv, vol. xxvi. pp. 399-452.
47 Krause, Neurologisches Centralblatt, 1885, p. 53.
It has been attempted to bring the tabic process in relation to a supposed primary meningitis. Tabes is a rather common nervous affection, and primary spinal meningitis is one of the very rarest. The leptomeninges are found considerably thickened in one out of ten tabic cords, and those who defend the meningitic origin of the disease base their theory on this inconstant finding, and allege that in the cases where it is absent the meningitis has disappeared while the cord lesion progressed. It is a fatal objection to this view that the part of the posterior columns immediately adjoining the pia is often quite free from disease. A meningitic affection, either as an etiological or a complicating factor, can be admitted in those cases only where there is a marginal sclerosis.
The changes in the optic nerve resemble those of the white columns of the cord in their naked-eye and minute character as well as in the controversial nature of the various interpretations made. When affected, the nerve is found to be firmer than normal, and discolored; later it becomes quite gray, and may eventually shrink to two-thirds, and even less, of its normal diameter. It is generally believed that, as in the cord, the myelin undergoes wasting before the axis-cylinder disappears, and that the latter may survive a long time, thus explaining why the patient may retain his visual power for a considerable period after the ophthalmoscope determines the existence of atrophy. No satisfactory explanation [p. 848] has as yet been offered for the optic-nerve affection of tabes. There is no direct continuity of the spinal and optic sclerosis. Two theoretical possibilities suggest themselves. The first is that the lesion of the cord exerts a remote effect upon the physiological, and through this the structural, condition of the optic nerve. That such an influence may be exerted is shown by cases of transverse myelitis low down in the cord, which, according to Erb and Seguin, were complicated by double optic-nerve atrophy. The second theory is that the involved part of the cord and the optic nerve present a similar vulnerability to the same morbid influences. This is illustrated in some cases of chronic alcoholic and nicotine poisoning, in ergotism, and in the spinal affections due to hereditary influences and developmental defects.
To discuss the nature of the disturbing influence which is responsible for the most characteristic evidence of the disease, the ataxia, would be equivalent to reviewing almost every mooted question in spinal physiology. It is to be borne in mind that ataxia is a collective term designating any inco-ordination of movement which is independent of motor paralysis. It may be due to abolition or impairment of tactile perception; it may be due to loss of the muscular sense; it may be due to hampered motor co-ordination; and, finally, it may be due to a disturbance of the space-sense. In my opinion it is only in exceptional cases that any one of these factors can be positively excluded. Occasionally, one has been noted when the ataxia was grave but the tactile sense was unimpaired, or where the muscular sense was perfect but ataxia was well developed. The difficulty with most such records is that no discrimination is made as to the kind of ataxia present. That loss of skill which the patient shows when he shuts his eyes and attempts to perform certain movements without their aid is undoubtedly due to diminished sensation, either tactile or muscular, and usually both. The inability to stand with the eyes closed is probably a cerebellar phenomenon, and in this respect we are on the way to return to Duchenne's opinion. It is true that the cerebellar organ is healthy in most tabic subjects, but its centripetal informer, the direct cerebellar tract, is either itself involved or affected in its origin in the columns of Clarke. But, besides the static ataxia and that motor ataxia which can be neutralized by the use of the eye, there is another disturbance, which, as Erb and his followers hold, cannot be accounted for on the strength of any sensory disturbance. It consists in an interference with the proper succession and rhythm of movement. It seems as if that automatic mechanism by which the individual or grouped muscular contractions engaged in locomotion follow each other with the smoothness of the action of perfectly-fitting cog-wheels were disturbed; the correct after-movement is hesitated over or skipped, or even takes place at the wrong moment, neutralizing some other step in the co-ordination required. The tendency of physiologists and pathologists is to attribute this form of ataxia to the disease of the intrinsic co-ordinating apparatus of the cord itself. The experiments of Tarchanoff on a headless duck, and the determination of the existence of cursorial co-ordinating tracts uniting the brachial and lumbar nuclei in mammals, as well as the observations made on automatic co-ordinate movement in decapitated criminals, demonstrate the existence in the cord of such an apparatus. The combination of the ganglionic centres which underlies this co-ordination [p. 849] is affected by the so-called short tracts of the cord,48 and it is precisely a portion of these which are involved in the lesion of the column of Burdach. A number of arguments have been advanced against regarding the lesion of this column, or indeed any of the lesions of the posterior column, as explaining the ataxia-producing effect of tabes. Westphal has interposed some potent objections. He holds that lesion of these columns will be found more frequently when examinations shall no longer be limited to those cases where disease is suspected because ataxia was observed during life. He found extensive disease of the posterior columns in sufferers from paretic dementia who did not exhibit the characteristic ataxic gait of tabes. I believe this objection can be met by the very cases cited by Westphal in its support. Where the spinal disorder preceded the cerebral—that is, where paretic dementia occurred as a complication of tabes dorsalis—true locomotor and static ataxia had been present before the insanity exploded. On the other hand, where the spinal disease followed the cerebral, typical ataxia did not ensue. This would seem to indicate that the destruction of cortical control is inimical to the development of typical tabes. Leyden has made a suggestion in the same direction when he attributes the lesser manifestness of locomotor ataxia in tabic females to their inferior cerebral organization.49 A more convincing proof of the correctness of this conclusion is furnished by the fact that if the pathological process, after destroying the posterior columns and producing ataxia, invades the voluntary motor tract, the ataxic symptom becomes less palpable.50 This antagonism between lateral-column and posterior-column lesion is frequently exemplified in the combined forms of sclerosis. It would seem, then, that where the brain is healthy and the controlling voluntary tracts are unimpaired, the ataxia is aggravated, supporting the beautiful theory of Adamkiewicz, which assumes that the locomotor ataxia is due to a disturbance of the balance normally existing between the psycho-motor centres and those controlling the muscular tone as well as those mediating reflex excitability.51
48 Intersegmental tracts.
49 In one out of three female eases I found the active disturbance of gait as severe as in males, but Leyden's observation is supported by all who have seen a sufficiently large number of female cases.
50 Not because of paresis altogether, for it diminishes materially out of proportion to the paresis.
51 Archiv für Psychiatrie, x. p. 545. There is another observation which bears in this direction: James of Boston observed that absolute deaf-mutes in a large percentage of cases are insusceptible to vertigo or to the allied phenomenon of sea-sickness. Certainly, the auditory nerve is a space-sense nerve; its physiological elimination is, however, accompanied by an immunity against a symptom which may be an evidence of disturbed space-sense transmission. In like manner, the destruction of the central perceptive and voluntary centres in the paretic dement inhibits the legitimate results of posterior spinal sclerosis.
The degeneration of the crossed-pyramid tracts in typical tabes seem to be strictly an atrophy from disuse, perhaps facilitated by the general malnutrition of the cord. It is limited to that part supplying the most or solely affected extremities. Thus, where the lower extremities are alone grossly involved it is totally degenerated in the lumbar area, and only in its outer parts in higher levels. As if to fortify this comparison by analogous observations from every great segment of the nervous axis, a similar inhibiting influence of pyramid lesion on co-ordinating disturbance (muscular sense) is noted in secondary degeneration of the interolivary layer; when uncomplicated with pyramid lesion (Meyer and my own case,) ataxia is present; when so complicated (Schrader, Homén) it is not observed, even if determinable.[p. 850]
Lissauer52 has recently determined the existence of a degeneration of certain fine nerve-fibres, apparently derived from the outermost of the radicles into which the posterior nerve-roots divide on entry. They are situated on that border of the apex of the posterior horn which is in contact with the lateral column, and were found degenerated in all cases except such as were in the initial period. No symptomatic relation has been claimed for this lesion.
52 Neurologisches Centralblatt, 1885, No. 11.
One of the most important questions which have grown out of the pathological studies of tabes is the relationship between the lesions and the not infrequently observed restoration of functions which had been more or less seriously impaired in an earlier period of the disease. Even those symptoms which ordinarily comprise the continuous and essential clinical background of tabes may exhibit remarkable changes in this direction. I have two well-established observations—one of tabes of eight years' standing, the other of more recent date—in which that symptom which, once established, is the most constant, the reflex iridoplegia, disappeared, to reappear in two months in one case where it had been associated with myosis, and to reappear in eight months in the other, repeating this oscillation the following year. I have now under observation a tabic patient in the sixth year of his illness who two years ago had a return of both knee-phenomena to a nearly normal extent, to lose them in two months, and to regain the reflex on the left side four months ago, retaining it up to the present. These three cases were of syphilitic subjects. In a fourth advanced non-syphilitic tabic patient, whose ataxia had reached a maximal degree, I found a return of both knee-phenomena for three days after its absence had been established by medical examiners for over a year, and had probably been a feature for a much longer period. Hammond the younger and Eulenburg have reported similar cases. Nothing is more surprising to those unfamiliar with the progress of this disease than to find gross ataxia or the electrical pains and anæsthesia to disappear or nearly so; and the alleged success of more than one remedial measure is based on the fallacious attributing to the remedy what was really due to the natural remittence of the disease-process or of its manifestations. The financial success of quacks and the temporary but rapidly evanescent popularity of static electricity, Wilsonia belts, and like contrivances are owing to the hopefulness inspired in the credulous patient by the mere coincidence of spontaneous improvement and the administration of a new remedy, supplemented, it may be, by the influence of mind on body in his sanguine condition. It is to be assumed that the influences which are at work in provoking the trophic and visceral episodes of tabes are of an impalpable character, and that all theorizing regarding the reason of their preponderance in one and their absence in another case are as premature as would be any speculation regarding their rapid development and subsidence in the history of one and the same case. But we have better grounds for explaining the remissions of the ataxia and anæsthesia.
It is only in the most advanced stages of tabes that the destruction of the axis-cylinder becomes absolute or nearly so. Contrary to the opinion of Leyden,53 who held that the tabic sclerosis differs from disseminated sclerosis in the fact that the axis-cylinder does not survive the myelin [p. 851] disappearance, it is now generally admitted that a certain number of exposed or practically denuded axis-cylinders may be preserved in the sclerotic fields.54 It is on the theory that these delicate channels may be oppressed at one time, perhaps by inflammatory or congestive pressure, and relieved at another by its subsidence, that we may assume them to be the channels through which the now limited, now liberated, functions are mediated. It is also reasonable to suppose that vicarious action may supplement the impaired function, and to some extent overcome the disturbing factors. This is illustrated by the controlling influence of the visual function—yea, even of the unconscious and ineffectual co-operation of completely amaurotic eyes—in neutralizing both locomotor and static ataxia. One patient who was well advanced in the initial period of tabes, and who had been encouraged to consider the medical opinion to that effect as the result of an exaggerated refinement of diagnosis, made repeated tests of the Romberg symptom in his own case, and deluded himself into the belief that the physician was mistaken because he succeeded in practically overcoming it with an effort that too plainly told its own story; but still he overcame it. Certain peripheral influences have the power of stimulating the dormant activity of potentially vicarious tracts, and perhaps also the blunted activity of those whose function is impaired. The outside temperature, certain barometric conditions, all may exert an influence in this direction for good or evil.
53 Op. cit., p. 328, vol. ii.
54 Babinski (Neurologisches Centralblatt, 1885, p. 324) notes this feature, and, consistently with the findings of most modern observers, discovers much more resemblance to disseminated sclerosis than to the systemic sclerosis with which Strümpell and Westphal (in part) incline to classify tabes. Similar objections to the system-disease theory are advanced by Zacher (Archiv für Psychiatrie, xv. p. 340). I may not pass over in silence the fact that Babinski considers his observations to militate also against regarding any phase of the tabic sclerosis as a secondary process. But while it may fairly be asked that a sclerosis to be regarded as systemic must be shown to be total, this is not necessary for a secondary process, unless the primary involvement be total also; and that is not the case in tabes.
ETIOLOGY.—Authorities are now agreed that no single cause can be regarded as the sole responsible factor in all cases of tabes, and that a number of etiological influences are combined in the provocation of this disease in most instances. When the distinctiveness of the affection was first recognized it was customary to attribute it to sexual excesses, and the unfortunate sufferer had frequently to bear the implied reproach of having brought his misery on himself, in addition to the hopeless prospect which those who followed Romberg and other authorities of the day held out to him.55
55 This opinion survives in a large portion of the German laity and in French novels. About the time that the poet Heine was dying from an organic spinal affection two other prominent literary characters of Paris were affected with tabes. It so happened that all three were popularly regarded as libidinous, and one of their leading contemporaries, whose name escapes me, took occasion to issue a manifesto addressed to the jeunesse dorée which closed with the apostrophe, “Gardons à nos moelles.”
Heredity plays a very slight part in the etiology of tabes. Writers of ten and fifteen years ago attributed a greater importance to it than is now done. But this was due to the incorporation with tabes of the so-called family form of locomotor ataxia—a disease which is now regarded as a distinct affection.56
56 There is but one record of direct heredity (the father and son being affected nearly at the same time), to my knowledge. It was observed at the Berlin Hospital by Remak (Berliner klinische Wochenschrift, 1885, No. 7). Both father and son were syphilitic.[p. 852]
More importance may be attached to individual predisposition, but thus far no distinct formulation of this factor has been attempted except by Schmeichler,57 who offers the suggestion that there are persons with a predisposition to the development of connective-tissue proliferation in various organs of the body, and that in them tabes and other sclerotic affections are consequently more frequent than in others. This suggestion appears plausible, but it is unconfirmed by positive observations.
57 Op. cit.
Sex appears on a superficial view to be one of the most important elements. It is generally admitted that at most one female becomes tabic for every ten males who do so. Of 81 cases in private practice, I observed but 3 females. Rockwell, Seguin, Birdsall, and Putnam give similar figures. This comparative immunity is probably due to the fact that the female is less exposed to over-exertion, to surface chilling of the feet, to the injurious consequences of sexual excess, and to syphilis58 than the male. As a rule, the affection in females is more insidiously developed, progresses more slowly, is less marked by crises and trophic disturbances, and not accompanied by as severe pains and profound disturbance of co-ordination as is the corresponding affection in males.
58 Whether the shorter vitality of the syphilitic female as compared with that of the male is a factor in diminishing the accumulation of chronic tertiary sequelæ in that sex, or whether it be the lesser vulnerability of the inferior nervous system, I am unable to decide from the facts at my disposal. In private and clinical experience I have been struck by the fact that women affected with syphilis in the same way and under similar circumstances with tabic syphilitic males develop symptoms of functional disorder of the brain and cord, such as spinal and cerebro-spinal irritation. My cases referred to had in no instance any indication of a syphilitic condition or history, and a distinct and different cause was found in all three.
The most important element in creating an acquired predisposition to tabes is undoubtedly the existence of constitutional syphilis. Some difference of opinion still exists regarding the proportion of syphilitic tabic patients, chiefly due to the neglect of Erb—when he first announced the prevailing view, and which is generally attributed to him—to differentiate between cases of demonstrated constitutional syphilis and the so-called spurious or soft chancre. But although there occurred a reaction against his view which went to as great an extreme in the opposite direction, the careful and critically registered statistics accumulated in the mean time strengthen the view that there are more syphilitic subjects among the tabic than among any class of sufferers from other nervous affections.59 Reumont, a physician at Aix-la-Chapelle, to which place syphilitic patients in general resort in large numbers, found that of 3400 cases of syphilis, 290 had nervous affections, 40 being afflicted with tabes. Bernhardt60 took occasion to examine a group of hospital patients who were free from tabes, and found that not fully 16 per cent. were syphilitic, while of 125 tabic patients, over 46 per cent. were determined to have had positive syphilitic manifestations. Several of those observers who have paid attention to the question of the syphilitic origin of tabes have admitted that the more searching their inquiry the larger the proportion of detected syphilitic antecedent histories. Thus, Rumpf's earlier table shows 66, and his later 80, per cent. of such antecedents. This latter figure exactly corresponds to the percentage of syphilis in my private [p. 853] cases. At a discussion held by members of the American Neurological Association in 1884, Webber gave 54, Putnam 49, Rockwell 40, Birdsall 43,61 and Seguin 22 per cent.62 as the proportion in their experiences.
59 Excepting always those having the distinctive and undisputed syphilitic character.
60 Archiv für Psychiatrie, xv. p. 862.
61 Derived from over five hundred cases which had presented themselves at the clinic of the College of Physicians and Surgeons.
62 In the Archives of Medicine he tabulates 54 (private) cases as follows:
| Chancre alone | 23 |
| Chancre followed by secondary symptoms | 16 |
| Total of those with history of chancre | 39 |
| No history of chancre in | 15 |
| Total | 54 |
Of European writers, aside from those already mentioned, Berger claims 43 per cent., and Bernhardt, in commenting on the increasing percentage obtained by accurate investigation, reports an additional series of 7 new cases in private practice, all of which were syphilitic. Fournier, Voigt, Œhnhausen, and George Fisher estimate the syphilitic tabic patients at respectively 93, 81, and 72 per cent. of the whole number. The almost monotonous recurrence of a clear syphilitic history in my more recent records is such that in private practice I have come to regard a non-syphilitic tabic patient as the exception. Among the poorer classes the percentage of discoverable syphilitic antecedents is undoubtedly much less. The direct exciting causes of tabes, exposure and over-exertion, are more common with them and more severe in their operation.
The proof of a relationship between syphilis and tabes dorsalis does not rest on statistical evidence alone. A number of observations show that the syphilitic virus is competent to produce individual symptoms which demonstrate its profound influence on the very centres and tracts which are affected in tabes. Thus, Finger63 showed that obliteration of the knee-jerk is a frequent symptom of the secondary fever of syphilis, and that the relation is so intimate between cause and effect that after the return of the reflex, if there be a relapse of the fever, the obliteration of the knee-jerk is repeated. Both the permanent loss of the knee-jerk (Remak) and the peculiar pupillary symptoms of tabes are sometimes found in syphilitic subjects who have no other sign of nervous disorder; and Rieger and Foster64 regard the syphilitic ocular disturbances, even when they exist independently, as due, like those of tabes, to the spinal, and not to a primarily cerebral, disturbance. Another argument in favor of the syphilitic origin of tabes is derived from the occasional remedial influence of antisyphilitic treatment. The force of this argument is somewhat impaired by the fact that the same measures occasionally appear to be beneficial in tabes where syphilis can be excluded. Still, the results of the mixed treatment in a few cases of undoubted syphilitic origin are sometimes unmistakable and brilliant.65 As some cases, even of long [p. 854] standing, yield to such measures, while others, apparently of lesser gravity and briefer duration, fail to respond to them, the question as to whether syphilis is a direct cause or merely a predisposing factor may be answered in this way: That in the former class it must have been more or less directly instrumental in provoking the disease, while in the latter class it is to be regarded as a remote and predisposing factor, to which other causes, not reached by antisyphilitic treatment, became added. The claim of Erb, that “tabes dorsalis is probably a syphilitic disease whose outbreak is determined by certain accessory provocations,” is not subscribed to unreservedly by a single writer of eminence.
63 “Ueber eine constante nervöse Störung bei florider Syphilis der Secundärperiode,” Vierteljahrschrift für Dermatologie und Syphilis, viii., 1882.
64 “Auge und Rückenmark,” Graefe's Archiv für Ophthalmologie, Bd. xxvii. iii.
65 In one case already referred to a return of both knee-phenomena and complete disappearance of locomotor and static ataxia were effected after a duration of four years. The treatment was neglected and the knee-jerks disappeared, and one has now returned under the resumed treatment, but accompanied by lightning-like pains. At a meeting of the Société médicale des Hôpitaux, held November 10, 1882, Desplats reported a case in which even better results were obtained. Reumont (Syphilis und Tabes nach eigenen Erfahrungen, Aachen, 1881) reports 2 out of 36 carefully observed syphilitic cases cured, and 13 as improved under antisyphilitic treatment.
The question has been raised whether the influence of syphilis is sufficiently great to justify a clinical demarcation between syphilitic and non-syphilitic cases. A number of observers, including Reumont, Leonard Weber, and Fournier, incline to the belief that there are more atypical forms of tabes in the syphilitic group. Others, including Rumpf, Krause, and Berger, are unable to confirm this, but the former admits, what seems to be a general impression among neurologists, that an early preponderance of ptosis, diplopia, and pupillary symptoms is more common with syphilitic than with non-syphilitic tabes. Fournier66 believes that syphilitic patients show more mental involvement in the pre-ataxic period; but it is evident that he has based this belief on a study of impure forms. The advent of tabes in syphilitic cases does not in this respect differ from the rule. The most protracted and severe diplopia I have yet encountered in a tabic patient is one, now under observation, in the initial period of the disease, syphilis being positively excluded as an etiological factor.
66 L'Éncephale, 1884, No. 6.
It seems to be a prevalent opinion that the cases of syphilis in which tabes is developed include a large proportion of instances in which the secondary manifestations were slight and unlike that florid syphilis with well-marked cutaneous and visceral lesions which is more apt to be followed by transitory or severe vascular affections of the cord and brain.
Excesses in alcohol, tobacco, and abuse of the sexual function are among the factors which frequently aggravate the tendency to tabes, and one or more of them will usually be found associated with the constitutional factor in syphilitic tabes. Both alcohol and nicotine have a deleterious effect on nervous nutrition and on the spinal functions, as is illustrated in the effect of the former in producing general neuritis, and of both in provoking optic-nerve atrophy and general paralysis of the insane, not to speak of the pupillary states which often follow their abuse, and the undeniable existence of a true alcoholic ataxia. Sexual excesses were, as stated, at one time regarded as the chief cause: the reaction that set in against this belief went to the extreme of questioning its influence altogether. It is to-day regarded as an important aggravating cause in a large number of cases, and this irrespective of whether it be the result of a satyriacal irritation of the initial period or a precedent factor. In a large number of my patients (18 out of 23 in whom this subject was inquired into) the habit of withdrawing had been indulged in,67 and, as the patients admitted, with distinct deleterious effects, such as fulness and throbbing in the lumbo-sacral region, tremor [p. 855] and rigidity, with tingling or numbness, in the limbs, blurred vision, and sometimes severe occipital headache; in one case lightning-like pains in the region of the anus ensued.68
67 Coitus reservatus, the real crime of the Onan of Scripture.
68 Leyden states that coitus in the upright position has been accused of producing tabes, without mentioning his authority. I have no observation on this subject touching tabes, but am prepared to credit its bad effect from the account of a masturbator, who during the orgasm produced while standing felt a distinct shock, like that from a battery, shooting from the lumbar region into his lower limbs, and causing him to fall as if knocked down. He consulted me in great alarm—was scarcely able to walk from motor weakness, and had no knee-phenomenon; in a few weeks it returned, and no further morbid sign appeared. Masturbators of the worst type occasionally manifest ataxia, and in three cases I have been able to establish the return of the knee-jerk, together with other improvements in the spinal exhaustion of these subjects. The loss and diminution of the patellar jerk, and the frequently associated urinary incontinence, as well as certain of the peripheral pains found in masturbators, certainly prove that undue repetition of the sexual act (be it natural or artificial) is competent to affect the cord in a way that cannot but be injurious in case of a predisposition to tabes, if not without the latter.
Of single causes, none exerts so direct and indisputable an influence on the production of tabes as the action of cold and wet upon the lower segment of the body. It is usually the case that such exposure is frequently repeated and combined with over-exertion before the disease is produced, but it is occasionally possible to trace the very first symptom of the disease directly to a single exposure. A soldier who stands up to his knees in a rifle-pit half full of water finds his limbs numb or tingling; develops slight motor weakness, then lightning-like pains, and ultimately a typical tabes. In the case of a peddler who presented an advanced form of the disease, the first symptoms had developed after a single wetting of his feet: while walking along one of our watering-places with his wares the swell of a steamer inundated the beach. He had been subject to perspiring feet before that, and the perspiration remained checked from that time on.69 The influence of surface chilling was remarkably manifest in all three of my female cases. In one of them it was due to frequent wetting of the feet; in the second, a midwife, the first symptoms began immediately after standing on a cold hearthstone while preparing some article needed in a lying-in case. In the third case, a lady who contracted and safely passed through a scarlatina in her twenty-eighth year was taken out driving while desquamation was going on. She became thoroughly chilled, experienced numbness in the fingers and toes, and from that day on developed a slowly progressing tabes involving all extremities alike.70
69 Checking of habitual perspiration by violent measures is mentioned by the German textbook writers as a frequent cause, but occurs quite rarely in the modern tables.
70 In view of the absence of spinal—or, in fact, any nervous—symptoms prior to the exposure referred to, it does not seem necessary to insist that this was not an instance of a true post-scarlatinal tabes; and possibly the case thus designated by Tuczek (Archiv für Psychiatrie, xiii. p. 147) may have been really due to chilling of the delicate body-surface after desquamation or during that process. The typical form of myelitis and sclerosis after exanthematous fevers is rather of the disseminated type.
Spinal concussion has been mentioned by a number of authorities as a possible cause for tabes, as for other forms of sclerotic spinal disease. In 1 of 81 cases in my own observation the development of the disorder could be distinctly traced to a railway injury; in 2 a sudden aggravation was as distinctly referable to a similar cause.71 To what extent railroad [p. 856] travelling, with its attendant continual jarring of the body, may predispose to the development of tabes or of other spinal diseases is as yet a matter of mere conjecture. That railroad travelling exerts a bad influence in some cases of the established disease is evident; but in others the patients rather like the motion, and claim to feel benefited by it.
71 A fall from a chair, striking on the back of the latter, while endeavoring to keep a row of books from coming down in one case, and the shock of the Ashtabula disaster in the other. The latter patient, the same one who is referred to as describing the electric-storm sensation in an earlier part of this article, had his foot amputated in consequence of that disaster; but, like one of the characters in Jacob Faithful, who felt his toes when the weather changed, though he left both legs at Aboukir, he felt the terrific pains of the disease in the absent foot as distinctly as in the other. Dumenil and Petit (Archives de Névrologie, ix. Nos. 25 and 26) relate cases in which a spinal concussion was the only ascertainable cause.
A number of toxic agents have been charged with producing tabes: thus, Bourdon maintains this of absinthe; Oppenheim attributes one case to poisoning by illuminating gas, the exposure to its influence being immediately followed by a gastric crisis, and this by a regulation tabes.72 It is supposed that most of the poisons acting on the cord in this or a similar way, such as arsenic, cyanogen,73 barium, and chloral,74 do not produce a spinal lesion directly, but through the medium of a secondary cachexia. Of no agent is the effect in producing tabes so well studied as ergot of rye. It had long been known that ergot-poisoning provoked certain co-ordinating, motor, and sensory disturbances, but it was left for Tuczek75 to show that this vegetable parasite produces a lesion of the spinal cord which in its character and distribution apes typical posterior sclerosis so closely as to justify the designation of a tabes ergotica. Possibly, pellagra, which is sometimes manifested in a similar way,76 may yet be shown to have a like influence.
72 Archiv für Psychiatrie, xv. p. 861.
73 Bunge, Archiv für experimentelle Pathologie, xii.
74 Transactions of the Clinical Society of London, xiii. p. 117, 1880.
75 Archiv für Psychiatrie, xiii. p. 148.
76 Bouchard, “Étude d'Anatomie pathologique sur un Cas de Péllagrie,” Gaz. méd. de Paris, 1864, No. 39.
Among the occasional and exceptional causes of tabes, Leyden and Jolly mention the puerperal state; Bouchut, diphtheria; and several instances are recorded in which psychical shock was responsible for the outbreak of the disease. In a small number of cases I found that mental worry and anxiety coincided with the period of presumable origin of the disease.
Age seems to have no special determining influence. It is true that most sufferers from this disease are men in the prime of life or in the period following it. But it is precisely at these periods that the exposure to the recognized causes of tabes is greatest. It seems as if there were very little liability to the development of tabes after the fiftieth and before the twenty-fifth year; still, some cases of infantile tabes have been recorded.77
77 Excluding the so-called family form of locomotor ataxia: 6 rather imperfectly described cases are cited by Remak (loc. cit.), and 3 additional ones related by himself. Of the latter, 2 had hereditary syphilis, and of 1 the father was both syphilitic and tabic.
In the majority of cases tabes is due to a combination of a number of the above-mentioned factors. The majority of tabic patients in the middle and wealthy classes have had syphilis, and of these, in turn, the majority have been guilty of sexual excesses or perverted sexual acts, while excesses in tobacco and of alcohol are often superadded. Among [p. 857] the poorer patients we find syphilis less frequently a factor, but still present, according to various estimates, in from 20 to 60 per cent. of the cases. Excesses in tobacco play a lesser, and excesses in alcohol a larger, part in the supplemental etiology than in the other class, while exposure to wet and cold and over-exertion are noted in the majority; indeed, in a fair proportion they are the only assignable causes.
DIAGNOSIS.—The recognition of advanced tabes dorsalis is one of the easiest problems of neurological differentiation. The single symptom which has given one of its names to the disease—locomotor ataxia—is so manifest in the gait that even the sufferers from the affection learn to recognize the disease in their fellow-sufferers by the peculiar walk.78
78 At present I have six tabic patients under treatment, who are acquainted with each other, and who have made each other's acquaintance in the singular way of addressing one another on the strength of mutual suffering at Saratoga, at the Hot Springs of Arkansas, and in New York City.
Although there are other chronic affections of the cord which manifest ataxia, such as myelitis predominating in the posterior columns, disseminated sclerosis in a similar distribution, and some partially recovered cases of acute myelitis, the gait is not exactly like that of tabes. The uncertainty may be as great, but the peculiarly stamping and throwing motions are rarely present in these affections. The clinical picture presented by the ataxic patient, aside from his gait, is equally characteristic in advanced cases. Absence of the knee-jerk and other deep reflexes, the bladder paralysis, sensory disturbance, delayed pain-conduction, trophic disturbances, and reflex iridoplegia are found in the same combination in no other chronic disorder of the cord. It is supposable that an imperfect transverse myelitis in the lumbar part of the cord might produce the reflex, ataxic, sensory, sexual, and vesical symptoms of ataxia, but the brachial symptoms found in typical tabes as well as gastric crises would be absent. The pupillary symptoms would also fail to be developed, in all probability. It is to be remembered that only fascicular cord affections can produce a clinical picture exactly like that of tabes in more than one important respect. In analyzing the individual symptoms of the early stage the more important differential features can be most practically surveyed.
The discovery of no single symptom of tabes dorsalis marks so important an epoch in its study as Westphal's observation that the knee-phenomenon is usually destroyed in it. Had this symptom not been detected, so Tuczek admits, ergotin tabes would have eluded recognition.79 It was claimed by a majority of neurologists at first that this jerk is always abolished in tabes, but it is now recognized that there are exceptions, as is shown by cases of Hirt,80 Westphal, and others, not to mention some well-established cases of its return during the progress of the disease.
79 It is not to be wondered that, like most new discoveries, that of the pathological changes of the patellar reflex should have been made the basis of premature generalizations. The attempt of Shaw (Archives of Medicine) to establish a relation between disturbances of the speech-faculty and an increased knee-jerk has not met with any encouragement or confirmation, and has been rebutted by Bettencourt, Rodrigues (L'Éncephale, 1885, 2), and others.
80 Berliner klinische Wochenschrift, 1886, 10.
The knee-phenomenon is supposed to be a constant attribute of physiological man. It is difficult to elicit it in children, and frequently impossible to obtain it in young infants. It also disappears in old age, [p. 858] without having any special signification, except that this occurrence seems to be in direct relation to senile involution. In 2403 boys between the ages of six and thirteen years, Pelizæus81 found it absent in one only. It is customarily elicited by having the patient while sitting in a chair throw one leg over the other; hereupon the ligamentum patellæ is struck a short, quick blow. Under physiological circumstances the leg is jerked outward involuntarily after an interval of about one-fifth of a second—one that is scarcely appreciated by the eye. But if it be found absent by this mode of examination, the case is not to be regarded as one of absence of the jerk without further ado. The patient is made to sit on a table, his legs dangling down and his body leaning back, while he clenches his fists. By this means the jerk will often be produced where it appears to be impossible to evolve it by the ordinary means. It is also well to try different parts of the ligament, and when comparing both sides to strike on the corresponding spot and in the same direction. Many subjects who appear to be irresponsive will respond very well when a point on the outer edge near the tibial insertion is percussed. The elbow reflex, which has the same signification for the upper extremity that the knee-jerk has for the lower, is elicited in the same manner.
81 Archiv für Psychiatrie, xv. p. 206.
The absence of the knee-jerk is usually regarded as a suspicious circumstance in persons of middle life; and where it can be demonstrated that it has been present years previously and subsequently disappeared, it is looked upon as of grave import. I, however, published three years ago an authentic case of disappearance of the knee-jerk in a physician now in active practice in New York City who to this day enjoys excellent health and has developed no other sign of spinal disease. The knee-jerk is also abolished in a number of conditions not belonging to the domain of strictly spinal diseases, such as diphtheria, diabetes, secondary syphilis, and severe cases of intermittent fever. Of these, diabetes alone can be possibly confounded with tabes dorsalis. The difficulty of differentiating early tabes and diabetes is enhanced by the fact that on the one hand there are often ataxic symptoms with diabetes, while on the other both glycosuria and diabetes insipidus may complicate tabes. Senator, Frerichs, Rosenstein, Leval-Piquechef, Charcot, Raymond, Demange, Féré, Bernard, and T. A. McBride all recognize the occasional presence of the ataxic gait, paræsthesia, belt sensation, and even fulgurating pains, besides the abolition of the jerk, in diabetes mellitus.82 In pure cases of diabetes, however, I am not aware that spinal myosis or the reflex paralytic pupil has been found.
82 I have now under observation a case of myelitis with predominating sclerosis of the posterior columns of five years' standing in a merchant who has been under antidiabetic treatment for eleven years.
Abolition of the knee-jerk is found in all organic diseases of the spinal cord which destroy any part of the neural arch at the upper lumbar level, where the translation of the reflex occurs, whether it be in the posterior root-zones or in the gray matter of the origin of the crural nerves. Thus, acute or chronic myelitis, disseminated sclerotic foci of this level, may cause obliteration of the reflex at any time of the disease; so may acute or chronic anterior poliomyelitis, neoplasms, and amyotrophic lateral sclerosis of the anterior cornua type if the destruction of the anterior cornua [p. 859] be complete enough. It is also found abolished with all diseases of the peripheral nerves—traumatic and neuritic—which produce absolute motor paralysis of such nerves.
Among the sources of error possibly incurred in examining for this important symptom the presence of rheumatism is one. There is sometimes a tetanic rigidity of the joints which prevents the reflex from becoming manifest. It is also sometimes found to be absent immediately after severe epileptic attacks, according to Moeli.83
83 In three examinations after severe attacks of epilepsy I found it normal.
The condition of the pupil is perhaps a more constant sign of early tabes than the loss of the knee-jerk; at least it has been found well marked in cases where the jerk had not yet disappeared. It may be regarded as a rule in neuro-pathology that wherever reflex iridoplegia is at any time accompanied by other oculo-motor disturbance, it is either of spinal origin or in exceptional cases due to disease of the pons varolii. The peculiar character of the pupillary disturbance of tabes furnishes us with a criterion for distinguishing it from one affection which in common with it exhibits loss of the knee-jerk—diphtheria. In diphtheria there is also a reflex disturbance of the pupil, but it is the reverse of that of early tabes. In the latter reaction to light is lost, but the accommodative contraction power is retained; in diphtheria accommodative contraction power is lost, but reaction to light is retained.
The bladder disturbance has already been described. It is found as a marked symptom so prominently in no other systemic affection of the cord, and in few of the non-systemic forms, of sclerosis. In none of these is it associated with absence of the patellar jerk, reflex iridoplegia, and fulminating pains, as in tabes, except there be also some motor paresis. It is the combination of any two of the important initial symptoms of tabes without paralysis or atrophy that is regarded as indicative of the disease by most authorities. Thus the swaying in closing the eyes, if associated with the Argyll-Robertson pupil, is considered as sufficient to justify the diagnosis of incipient tabes, even if the knee-jerk be present and fulminating pains and bladder trouble absent. Undoubtedly, the tabic symptoms must begin somewhere. But at what point it is justifiable to give a man the alarming information that he is tabic is a question. I have a number of neurasthenic subjects now under treatment who have had reflex iridoplegia for years; in one the knee-jerk is slowly becoming extinguished; in two it has been becoming more marked after becoming less; in all the three mentioned there is slight swaying in closing the eyes and some difficulty in expelling the last drops of urine while micturating. I do not believe that such a condition justifies a positive opinion, although the surmise that they are on the road to developing tabes may turn out correct for all these and for some of those who have merely reflex iridoplegia.
Incipient tabes cannot be readily confounded with any other chronic disease of the spinal cord. Some of the cases produced by sudden refrigeration resemble a beginning myelitis. But the absence of true paralysis seems to distinguish it from the latter. In all the cases of so-called acute locomotor ataxia of myelitic origin that I can find a record of, paralytic symptoms were marked, if not throughout the disease, at least in the initial period.
[p. 860]Other forms of sclerosis occasionally limited to the posterior columns imitate the symptoms of tabes. It is unusual, however, for such sclerosis to be distributed through so great an extent of the posterior columns as to produce symptoms consistent with tabes in both the upper and lower extremities. And even where this condition is complied with, the typical progress so characteristic of tabes is not adhered to. As previously stated, the progress is weakened by variations in certain symptoms. Such variations are found in other forms of sclerosis, but they are not as great, trophic disturbances not so common, and visceral crises not so violent, as a rule.
The discovery of ataxic phenomena as a symptom of peripheral neuritis has added another to the long list of pseudo-tabic affections. Indeed, Dejerine, who greatly advanced our knowledge of this affection, undertook on the strength of his discovery to place tabes among the peripheral affections complicated by secondary affection of the cord. In a large number of cases of peripheral neuritis, particularly the alcoholic form described by Fischer, the static ataxia, belt sensation, bladder trouble, and reflex iridoplegia are absent. In tabes the severe pains, if influenced by deep pressure at all, are affected favorably, but in peripheral neuritis pressure on the affected nerve-trunk greatly aggravates the trouble.
In addition, those severe forms of neuritis that lead to ataxia, abolition of deep and other reflexes, are accompanied by qualitative electrical changes and atrophic paralysis—features not found in tabes. Sometimes a disseminated neuritis will become so generalized as to cause diplopia and other evidences of ocular paralysis through the affection of the peripheral nerves, but, so far as my observations extend, not with the characteristic pupillary phenomena of tabes.
Cerebellar disease, alcoholic and hysterical neuroses, sometimes produce ataxia, and this may be associated with one or more of the other characteristic symptoms of tabes. Cerebellar ataxia is usually very different from that of tabes, as far as the locomotor element is concerned. In tabes it is the movements the patient makes which cause him to stagger; in cerebellar disease those movements made to prevent staggering are usually co-ordinated. The gait properly called cerebellar is therefore very different from that of tabes. There is, however, static ataxia in both cerebellar and posterior-column disease. In addition, the knee-jerk may be abolished in the former, heightening the resemblance: the history of the case is, however, decisive where these latter symptoms might lead to doubt. Bladder trouble in cerebellar disease is not an early feature, nor are paræsthesias and delayed pain-conduction intrinsic features, of cerebellar disease. Their presence is in favor of tabes.
Alcoholic ataxia is very rapid in its course, while tabic ataxia is exceedingly slow. In addition, the former is accompanied by atrophic paralyses as early features; if such occur in tabes, they occur late in the disease, and are not marked by degenerative electrical reactions as alcoholic ataxia is. This disorder is usually, too, accompanied by fever, which is an exceptional, and certainly never an intrinsic, feature in tabes. Discontinuing the alcoholic poison is usually followed by rapid amelioration of the ataxia. Hysterical ataxia exceptionally apes the ataxia of tabes; the presence of other hysterical phenomena, the rapid and bizarre change of the symptoms, are distinguishing features. There are cases of hysterical [p. 861] ataxia accompanied by concentric limitation of the field of vision.84 The outline of the limitation is strikingly like that accompanying atrophy, but repeated examination shows a variation of a kind not found in the latter. The blind field advances in one direction to recede in another on one day, and reoccupies the latter and recedes from the former on the next.
84 Landesberg, Journal of Nervous and Mental Diseases, vol. xiii. 2.
Ataxia after most acute diseases, such as scarlatina and typhoid, is not usually accompanied by loss of the knee-jerk, and never by reflex iridoplegia. The ataxia after diphtheria is complicated by the former, but, as already stated, the very opposite state of the pupil serves to distinguish it.
The hereditary form of tabes is frequently confounded to this day with true tabes dorsalis. The family history and age of the patient are collateral evidences of the nature of the case. In the hereditary form the sphincters, optic nerves, and the eye-muscles are not affected; in the acquired form the first and last are always involved; and this involvement occurs so early in the disease as to constitute a valuable discriminating feature. Although the locomotor ataxia is very similar in the two affections, static ataxia, the symptom manifested on closing the eyes, is not found in the hereditary form, while it is found more constantly than even the locomotor ataxia in the acquired form.
The electrical reactions in tabes are either normal or quantitatively slightly increased. This serves to distinguish it from all spinal affections accompanied by marked paralysis. In the later stages, when some atrophy results, there may be a quantitative decrease, but these are without qualitative changes. A change may occur in those exceptional cases where the anterior gray horns become involved, but we then have to deal with a true complication; and complications can be recognized only in their development and by the application of the diagnostic criteria characterizing the complicating disorder when of an independent occurrence.85
85 It is not impossible that many of the symptoms described as occurring in advanced tabes are due to independent focal disease. In the case of a female aged seventy years mentioned by Hirt (Berliner klinische Wochenschrift, 1885, No. 26), who developed hemiatrophy of the tongue, probably from a hemorrhage in the brain isthmus, there was no tabes, although this symptom when found with tabes is supposed to be part of the tabic symptom-group.
The TREATMENT of tabes dorsalis will be considered at the end of this article, together with that of the sclerotic processes generally. The duration and prospects of the disorder have been considered with the clinical history. In the vast majority of cases the course of the illness is progressive. A few cases have been reported, but in the only instance where an autopsy was made to test the matter it was found that the sclerosis had not been removed. It may be therefore stated that an arrest of the disease is possible, but that restitution of the nerve-elements, once destroyed, is impossible.
SYNONYMS.—Primary lateral sclerosis. Tetanoid pseudo-paraplegia, (Seguin), Tabes dorsal spasmodique. This symptom-group was first [p. 862] recognized by the American neurologist Seguin86 thirteen years ago; two years later Erb87 described it under the title at the head of this section, and about the same time Charcot88 attributed the well-marked clinical signs thus discovered on both sides of the Atlantic to a primary sclerosis of the lateral columns of the cord in that portion which is known as the crossed-pyramid tract, and whose isolated disease had been known to Türck,89 but not clearly brought into relation with what is now regarded as one of the most remarkable and recognizable of spinal symptom-groups. Our earlier knowledge of the disease has been much confused through the discovery by Charcot90 of the same lesion to which spastic paralysis is attributed by him, in a female who had been suffering from permanent contractures of all extremities, and which he persisted in regarding as hysterical. The only solution of the difficulty is to accept one of two alternatives—either believing that the sclerosis was in this case primary, in which case contracture cannot be regarded as hysterical, or that it was secondary to protracted disuse of the limbs, in which case it proves nothing. An additional source of confusion has been the discovery of an analogous affection, now regarded as clinically and pathologically distinct, known as amyotrophic lateral sclerosis, and of a corresponding affection of the lateral columns in a large number of cases of paretic dementia.
86 E. C. Seguin, “Description of a Peculiar Paraplegiform Affection (tetanoid pseudo-paraplegia),” Archives of Scientific and Practical Medicine, February, 1873. Erb's statement (Ziemssen's Cyclopædia, vol. xi. 2, p. 628) that Seguin's description includes symptoms which do not properly appertain here can no longer be sustained, in view of the similar and identical symptoms which have been since attributed to the same affection and to amyotrophic lateral sclerosis by later writers. There seems to be no question that the priority of recognition of the clinical form belongs to this side of the Atlantic.
That Seguin's title was not as badly chosen as Erb implies in his first reference to it may be inferred from the fact that Strümpell, without any reference to Seguin, and evidently independently of him, uses the following language ten years later: “As also in these cases, the movements are not immaterially influenced by the ever-occurring spasms, a motor disturbance may be simulated which we feel inclined to term spastic pseudo-paralysis, or, more correctly, pseudo-paresis” (Pathologie und Therapie).
87 “Ueber einem wenig bekannten spinalen Symptomencomplex,” Berliner klinische Wochenschrift, 1875, No. 26.
88 “Sclérose primitive de la partie postérieure des cordons antero-lateraux,” Gazette médicale de Paris, 1874, pp. 38, 39.
89 “Ueber primäre degeneration einzelner Rückenmarkstränge,” Sitzungsberichte der Kaiserlichen Akademie der Wissenschaften zu Wien, Mathematisch-Naturwissenschäftliche Klasse, Band xxi. Jahrgang 1856, p. 112.
90 Gazette hébdomadaire, 1865, 7.
CLINICAL HISTORY.—Spastic paralysis manifests itself chiefly in three symptoms: first and most noticeable, a condition of rigidity of the limbs; second, an increase of all the muscular reflexes; and third, a true motor paresis. It manifests itself in the adolescent or middle period of life, usually without any noticeable cause, beginning in the lower extremities, and, if progressive, involving the muscles of the trunk and arms. The invasion of the disease is first marked by an increase in the excursiveness of the muscular phenomena, such as the knee-jerk and the ankle-clonus. But while this reflex irritability is originally only manifested when the diagnostician applies his special tests, it soon becomes so great that the most trivial influence suffices to bring about exaggerated muscular reaction. The mere tension of a tendon in walking, the weight of the limb, the slightest change in position, suffice to produce reflex muscular tension. The muscles feel firm and stiff to the touch, as if permanently contracted, [p. 863] and the lower limbs, as a result of the combined contraction of special muscular groups, assume a characteristic position—namely, an extension contracture of the leg on the thigh and a flexion of the foot on the leg. In advanced cases the contracture is so extreme that it is almost or actually impossible to flex the leg and to extend (dorsiflect) the feet. This is particularly noticeable when it is attempted to overcome the strained position suddenly, while gradual traction will often succeed in relaxing the contracture. The latter procedure succeeds because sudden traction of the tendons and the reflex contraction thereby provoked are avoided by it. Gowers compares this symptom to the mechanism of a clasp-knife. When the leg is slowly extended it yields to the manipulator's influence, but as soon as it reaches full extension it remains like the blade of the knife fixed by a spring.
Although some degree of muscular weakness is experienced in the beginning of the affection—often more marked in one leg than the other—it is insufficient to account for the grave and characteristic disturbance of locomotion. This is due rather to the stiffness of the limb resulting from the morbid muscular spasm. As the limbs are rigid, the steps are short; the leg not being flexed, and consequently not being lifted from the ground, the gait consists in an awkward shuffle.91 The feet are in continuous contact with the ground, and it is observed that there is a tendency to walk on tiptoe, owing to the contracture of the gastrocnemius, in this respect resembling the pes-equinus position. In some cases it has been observed that the reflex excitability was so great that the mere need of urinating brought on a sudden tonic spasm, and there have been noted others in which the very first spasmodic phenomena occurring in the history of the case appeared while the patient emptied his bladder.92
91 It was Theodore Simon, I believe, who first suggested the registration of peculiarities in gait by using sand on the floor or compelling the patient to walk over large sheets of paper with black-leaded shoes. Among the varieties of gait noted in paretic dementia by him he accurately describes that of spastic paralysis (Die Gehirnerweichung der Irren, Hamburg, 1871).
92 Westphal, Archiv für Psychiatrie, xv. p. 224; ibid., p. 229.
When the upper extremities are involved, the same initial muscular weakness and exaggerated reflex excitability are noted, but the contracture at the elbow, unlike that at the knee, is usually in the flexed position.
If from any cause the spastic phenomena happen to be in the background temporarily, so as to admit testing the voluntary muscular power, it is always found to be grossly impaired.93
93 This statement is made by Westphal, but as he considers the only pure cases of pure primary lateral sclerosis to be those associated with paretic dementia, and it is in the latter form alone that there are marked exacerbations and remissions in the spastic symptoms, it probably does not apply to uncomplicated spastic paralysis.
As the disease progresses locomotion becomes impossible; the advancing rigidity of the trunk-muscles renders sitting impossible, and the patients become bedridden. But even in this advanced stage no sensory or vegetative disturbances were noted. The cutaneous reflexes sometimes appear exaggerated, but this is not an evidence of sensory hyperexcitability, but of the increased ease with which the motor response is elicited—a feature which is also illustrated by the spasm resulting from fulness of the bladder or even from the mere act of micturition. Ataxia has never been noted in pure cases, and the uncertainty in gait sometimes [p. 864] noted at the onset of the disease is secondary to the motor weakness and the interference with free mobility by the, as it were, frozen state of the muscles. Occasionally the paresis becomes a veritable paralysis, but this occurrence is limited to one or several muscular groups. Cases are related in which the spastic symptoms occurred on one side, involving one arm and leg for years before involving the other. It is not improbable that these were cases of some obscure cerebral affection. Other exceptional cases in which the spastic phenomena appeared first in the arms are better authenticated.
The early occurrence of ankle-clonus in this disease heralds the appearance of apparently spontaneous clonus when the toes are put on the ground, and later on of cramps of the gastrocnemius or other muscles, which produce an exacerbation of the existing stiffness. Occasionally sudden spasms occur while the patient is at rest, and which resemble the sudden shocks which healthy persons occasionally experience when about to fall asleep.
The electrical reactions show little that can be called characteristic, and there is little unanimity among observers on this point. The majority agree that there is a slight quantitative decrease of both faradic and galvanic excitability in parallelism with the degree of paresis. In the pure form of the disease there are no other symptoms than those mentioned. Should evidences of involvement of the gray substance of the cord or the cranial nerves be added, it is a certain indication that we have to do with the similar but far from identical affection, amyotrophic lateral sclerosis.
The course of the disease is extremely slow and its development insidious. It is considered incurable, and although a few cases have been described as terminating in recovery, the most recent and reliable annals fail to make mention of any cure in a well-established case of spastic paralysis. The disease is not in itself fatal, death usually occurring from intercurrent affections.
ETIOLOGY.—Our knowledge of the causes of this disease is practically nil. It has been, like tabes dorsalis, attributed to a family tendency. Excessive sexual indulgence, over-exertion, and syphilis have been recorded as possible causes in the few cases in which an etiological assignment could be attempted. Tuczek surmises that the spastic phenomena of lathyrism, a constitutional disease analogous to pellagra and ergotism which is observed in those who live on bread prepared from a legumen grown in Italy (lathyrus bean), and which manifests itself in spastic symptoms, may be due to an affection of the pyramid tract, just as tabes ergotica is due to an affection of the posterior columns. One case of spastic paralysis of a severe nature, associated with scanning speech, in consequence of a lightning-stroke, is reported by Demme.94 I have been able to assign a cause in but two cases of spastic paralysis. Both were in Quakers; in both there had been a history of almost incredible sexual excesses. The disease in both involved the muscles of the jaw and face. An autopsy in the one case revealed no lesion whatever.95
94 “Bericht über die Thätigkeit des Jennerischen Kinderspitals,” Wiener medizinischer Blätter, 1884, No. 23.
95 The contracture in the lower extremities, differing from the rule, was a flexion contracture.[p. 865]
MORBID ANATOMY AND PHYSIOLOGY.—Although Charcot's announcement that spastic paralysis is due to sclerosis of the crossed-pyramid tract was made with great positiveness, the more careful authorities have not committed themselves to his view without reservation. Their reserved position is the result of some observations which certainly show that there is no constancy between the distribution of the lesion and the distribution of the spastic paralysis;96 while, on the other hand, characteristic spastic symptoms have been noted with purely cerebral lesions.97 Morgan and Dreschfeld98 publish cases in which the lesion was stated to be characteristic, but as the cell-groups in the anterior horn were found by them to have been more or less affected, it is evident they had cases of amyotrophic lateral sclerosis to deal with. In view of similar revelations in a large number of the cases that had been considered as spastic paralyses during life, and in which similar findings were found after death, Westphal,99 one of the most critical students of the subject, concludes that thus far an anatomical basis has not been demonstrated with any constancy for the cases of spastic paralysis uncomplicated with paretic dementia. With this disease a sclerosis of the lateral column, apparently independent of the cerebral affection, is often found. It has no continuity, as a rule, with the cerebral lesion, and it may be limited to special districts of the cord. It is not usually intense enough to produce material destruction of the tract itself, and for this reason, probably, we do not find any other symptoms than a paretic weakness and an increase of the patellar and other muscular phenomena developed in the majority of paretics. In some, however, the characteristic spastic gait and muscular rigidity do develop. Westphal conjectures that if paretic dements lived as long as the sufferers from uncomplicated spastic paralysis, they would ultimately show the typical symptoms.100 Numerous observations, however, show that the presence and intensity of the spastic symptoms in paretic dementia are not related to the presence and intensity of lateral-column lesion. Thus, Zacher101 failed to find such lesion in a case where the spastic symptoms had been well marked. It must be remembered, in drawing conclusions regarding the pathogeny of simple spastic paralysis from the lateral-cord affection and associated symptoms of paretic dementia, that the possibility of the lesion of the pyramid tract in this affection being secondary to disuse102 cannot be excluded. On the other hand, the symptoms of most paretic dements presenting lateral-column [p. 866] lesion differ in some respects from those of a pure spastic paralytic. There is a precedent clumsiness and helplessness of movement; the patient stumbles and trips more than is the case with the pure spastic gait; he wavers after suddenly turning around, and there is considerable tremor with intended movement. There is also more exacerbation and remission of these symptoms than is the case with true spastic paralysis, and it is observed that the exacerbations usually follow apoplectiform and epileptiform attacks, thus showing that the cerebral condition, after all, may be the determining factor.
96 Fischer and Schultze (Archiv für Psychiatrie, xi. 3) report an impure case in which, with exquisite spastic symptoms in the neck and arms, the degeneration of the pyramid tract was limited to the dorsal part of the cord.
97 Schulz (Deutsches Archiv für klinische Medizin, Band xxiii.) and Strümpell (Archiv für Psychiatrie, x.).
98 Journal of Anatomy and Physiology, xv. p. 510.
99 Archiv für Psychiatrie, xv. p. 246.
100 Another feature which antagonizes the development of spastic phenomena in paretic dementia is the lesion of the posterior columns which often ensues. In proportion as this is developed it neutralizes the exaggerated knee-jerk, stiffness, and spastic gait.
101 Archiv für Psychiatrie, xiii. p. 155.
102 It has been claimed against this view that if this were so the degeneration of the pyramid tract should be accompanied by degeneration of the cells in the anterior horn. This claim assumes that the cells and the pyramid tract are directly continuous, but the most modern researches, those of Von Monakow, confirming an older observation of Homén's, show that a system of small cells in the lateral reticular processes is interpolated; which I can confirm. It is certainly compatible with an atrophy from disuse of the voluntary tract that the cells themselves, presiding over reflex and nutritive functions not necessarily disturbed in paretic dementia, should remain nearly intact.
There is another respect in which the two conditions differ. Spastic paralysis is usually an ascending affection, the lower extremities being involved first, the trunk next, and the upper extremities last. But in paretic dementia the spastic phenomena develop in both upper and lower extremities simultaneously, and there are universal tremors, probably of irritative origin. The lower extremities are not commonly in the extension contracture of spastic paralysis, but in the same flexed position as the arms, the adductors usually preceding the flexors in becoming rigid. If it be added to this that the lateral-column lesion in paretic dementia appears to answer all the requirements which could be made of the lesion on theoretical grounds were the case one of pure spastic paralysis—that is, that its area decreases upward—the inconsistency of the observed anatomical and clinical facts becomes strongly evident. Thus far, the attributing of spastic paralysis to a primary lesion of the pyramid tract rests in a few contested cases, on a number of doubtful analogies, and on the undoubted fact that sclerosis of this tract in the event of a myelitis is followed by pronounced spastic symptoms in all those muscles which derive their voluntary innervation from the part of the tract which lies below the level of the lesion.
The situation of this tract, which was not discovered by Türck and Flechsig, as is usually supposed, but accurately known to Burdach103 in 1819, may be roughly stated as follows: It lies in the dorsal half of the lateral column, making up the bulk and core of this part of the column. It is separated from the pia mater by the direct cerebellar tract, and from the posterior gray horn by a narrow zone of fibres differentiated by Lissauer (see Tabes). It is connected with the lateral reticular processes, and in its cephalo-caudal course becomes gradually attenuated, giving off its fibres to these processes, thus to be exhausted in the lower part of the lumbar enlargement of the cord, where it approaches, if it does not actually reach, the surface. The fibres controlling the voluntary motions of the lower limbs, and which have a longer course to run before they reach the brain than those which mediate the voluntary control of the arms, are situated nearest the lateral boundary of the cord. Where the spastic phenomena are mainly marked in the lower limbs the sclerotic process has been found most marked in the corresponding area.
103 Vom Bau und Leben des Gehirns. This gifted author says that the crossed-pyramid tract lies in the lateral column of the cord, behind a line corresponding to the attachment of the ligamenta denticulata and removed from the surface.
The progress of this affection has not been materially modified in any case by treatment. The same measures employed in sclerotic processes generally, particularly galvanism and warm baths, are recommended. It [p. 867] is difficult to understand what good effect ergotin, which is mentioned by a number of the German writers, can have in a disease of this nature.
Amyotrophic lateral sclerosis, so named by Charcot104 and Joffroy, who first described it, consists in a disease affecting both the conducting tracts and nuclear centres of the motor system of the spinal cord and medulla oblongata, manifesting itself in a combination of atrophic and irritative phenomena on the part of the muscles. The relations between the symptoms and lesions of this disease rival in constancy and preciseness those noted in typical tabes dorsalis. As the variations in the mode of invasion and distribution of the lesion account for the widely-differing clinical types of the disease, and the advanced state of our anatomical and physiological knowledge of the cord enables us to interpret the reason of this difference, we shall invert the usual order and discuss the morbid anatomy first.
104 In 1869 and 1874 (Leçons sur les Maladies de la Système nerveux) Charcot termed this, and one other form of disease associated with muscular atrophy, amyotrophic, to distinguish them from the myopathic forms. He considers amyotrophic lateral sclerosis as deuteropathic, the nuclear atrophy being secondary to the lesion of the white substance, and the progressive muscular atrophy of the type described by Duchenne and Aran as a protopathic form of the amyotrophies. Among the true myopathies he enumerates pseudo-hypertrophic paralysis, Erb's juvenile form, Duchenne's infantile form, certain mixed forms, and, without justification, Leyden's hereditary forms (report by Marie et Guivron, Progrès médicale, 1885, No. 10).
MORBID ANATOMY.—In advanced cases of amyotrophic lateral sclerosis there is found marked sclerotic degeneration of both the crossed and the uncrossed pyramid tracts; atrophy of the cells of the anterior horns; atrophy of some of the nuclei of the motor and mixed cranial nerve, particularly the hypoglossal and spinal accessory; atrophy of the anterior roots of the spinal and the roots of certain motor cranial nerves; and, finally, atrophy of the voluntary muscles. The greater part of the tract through which the voluntary impulse travels after leaving the voluntary motor-fields of the cortex is therefore continuously involved; and it would seem that there are cases (Kahler-Pick's) where the entire motor system is affected, the morbid process demarcating the course taken by the motor impulse through the cerebro-spinal fibre-labyrinth from the cortical motor-field down to the muscles.
The morbid process in the muscles consists of a narrowing of the fibres, which subsequently lose their transverse striation and undergo a granular disintegration. Sometimes a muscle disappears entirely; usually the connective-tissue elements, including the interstitial cellular and adipose tissue, undergo proliferation, so as to mask the wasting of the muscles to some extent.
The morbid process in the nervous system is also a simple degenerative process. The nerve-fibres and cells atrophy first, and the connective-tissue proliferation which marks the sclerotic change of the diseased area is a secondary process. There is still considerable dispute among authorities as to which segment of the motor-conduits the degeneration begins in. But from the great difference found in the individual cases which [p. 868] have become the subject of patho-anatomical studies there can be little doubt that there is no uniformity in this respect. In some cases the lesion is far advanced in the lateral columns, while the anterior horn is but slightly involved; in others the reverse is found. Sometimes the nuclei of the motor cranial nerves are the chief foci of disease; at others they are the least affected parts of the motor apparatus. As we shall see, there are differences in the clinical picture corresponding to the variations of the anatomical findings.
CLINICAL HISTORY.—In typical cases the first symptom is a tired feeling in one arm or leg, usually the former; in dextral persons the right arm, the one which is subject to the severest strain, is most frequently the first to be affected. With the increase in this tired feeling there develops actual loss of power; the muscles become wasted, and the other arm becomes involved. Often it is observed that the right leg suffers with the corresponding arm, but as a rule the lower extremities do not become involved to any marked degree within the first six months of the illness. It is then noted that a gait not unlike that of spastic paralysis is noted, but with more loss of motor power and less stiffness. There is, however, this noteworthy difference between the affection of the lower and that of the upper extremities: that atrophy and loss of power are more marked in the latter, and spastic phenomena in the former. The knee-jerk and other deep reflexes are greatly increased, and ankle-clonus is usually very well marked. As with spastic paralysis, there are no visceral or sensory disturbances. Unlike that affection, there are qualitative changes in the electrical reaction of the muscles105 in amyotrophic lateral sclerosis. The degeneration reaction is found in the atrophied divisions, and particularly in such groups as those of the thenar and hypothenar eminence, which undergo complete atrophy at a comparatively early period of the disease.
105 Moeli, Strümpell, Pick, and Mierzejewski describe cases in which only quantitative changes were found. They were such in which spastic phenomena preponderated at the time of the examination.
Soon after the spastic and atrophic involvements of the lower extremities, symptoms indicating the involvement of the cranial nerve-nuclei are developed, usually after the disease has lasted a year or so. Deglutition becomes difficult and speech indistinct, the general picture of a glosso-labio-laryngeal paralysis being imitated. The patient cannot pucker his lips, his lingual muscles undergo atrophy, and fibrillary and fascicular twitches are noted in the tongue and lips. But just as the atrophic affection of the muscles of the arms and legs differs from that of progressive muscular atrophy in the fact that the deep reflexes are exaggerated with amyotrophic sclerosis, so in the bulbar symptoms of the latter it is found, unlike the typical form of bulbar paralysis, that the jaw reflex is increased.
The duration of the disease may be stated at about three years, death usually occurring in consequence of the involvement of the cranial nerves. There are cases recorded where the disease was almost simultaneously developed in all four extremities and the tongue, reaching a high degree within a year (Mierzejewski). It is generally agreed that the reason contractures do not develop in typical cases of this kind, although the lateral column is sclerosed and spastic phenomena occur early in the disease, is the destruction of the cell-groups in the anterior horn. The reflex arch [p. 869] through which a reflex contracture would be mediated is broken, or rather weakened, in that part of its course which passes through these cells, and therefore a contracture is as efficiently antagonized as it would be if the posterior roots were divided. Still, in some cases a frozen attitude of the lower extremities is very well marked (Vierordt, Zacher). To reconcile these conflicting observations it has been suggested that it may be regarded as a question of speed between the progress of the pyramid-tract and the anterior-horn lesions. If the former be much in advance of the latter, spastic phenomena will preponderate and contractures be possible, to disappear with the subsequent anterior-horn lesion. But if the latter precede and preponderate, the spastic phenomena will be in the background and contractures impossible. Indeed, Zacher106 suggests that there may be an ascending form in which the lesion of the pyramid tract is secondary to the nuclear atrophy, corresponding to the typical class of cases on which Charcot based his first description of the disease, and a descending form in which the pyramid tract is first affected and the nuclear cell-groups follow. Vierordt107 and Kahler108 express similar opinions. The latter goes so far as to suggest that progressive muscular atrophy, progressive glosso-labio-laryngeal paralysis, and amyotrophic lateral sclerosis are really due to one and the same kind of degenerative process, merely differing in location. There is certainly, as he claims, a remarkably complete chain of cases, beginning with such (1) in which spastic paralysis preponderates, passing thence to (2) those in which some muscular atrophy preponderates, then (3) those in which muscular atrophy is in the foreground and the spastic phenomena are slight, and ending with (4) the pure atrophies. A similar transition may be established on the regional principle between pure glosso-labio-laryngeal paralysis and amyotrophic lateral sclerosis, for there are cases of this affection in which the oblongata symptoms preponderate throughout, and the focus of the disease is formed there, just enough lesion being demonstrable in the pyramid tract and the spinal gray matter to prove the family relationship of what clinically appears as a spastic bulbar paralysis.109
106 Archiv für Psychiatrie, xv. p. 416.
107 Ibid., xiv. p. 397.
108 Zeitschrift für Heilkunde, 1884, p. 109.
109 Such a case is described by Freund in Deutsches Archiv für klinische Medizin, xxxvii. p. 405.
PROGNOSIS.—As far as the typical cases of this disease have been studied, a fatal termination seems to be invariable. Seeligmüller reports a few cases in which the progress appeared to become arrested, but it is not clear that these were not in reality cases of some juvenile form of muscular atrophy. Not only is the affection in adults fatal, but it is so in a short period of time as compared with other spinal disorders, and particularly with the related disorder spastic paralysis. Few patients survive the third year of their illness; a number do not live to that length.
A number of cases of chronic sclerotic disease of the cord have been discovered and analyzed during the past decade, which, while they show the regularity of distribution noted in posterior and lateral scleroses, [p. 870] differ from them in involving at once more than one column of the spinal cord. Usually, it is the posterior column and the posterior part of the lateral column which are affected. The symptoms constitute a combination of those of tabes dorsalis and of spastic paralysis. But this combination does not represent a mere addition of symptoms; where the tendency of the two diseases conflicts, they neutralize each other. Thus the tendency of lateral sclerosis uncomplicated by posterior sclerosis is to increase the patellar jerk; when posterior sclerosis complicates it, the jerk is annihilated. The degeneration of the lateral column and the ensuing motor paresis in like manner neutralize the ataxic character of the gait by limiting its excursiveness.
The upper extremities are usually involved equally with the lower. In the cases of Kahler-Pick considerable atrophy of the muscles developed; in those of Prévost and Westphal this was not very noticeable. In a few cases, where the posterior sclerosis did not involve the lumbar part of the cord, spastic symptoms were noted in the lower extremity. In the only case of combined sclerosis now under my observation this peculiarity, noticed by Prévost, is well marked. In one of Westphal's cases there was evident mimic ataxia. The few cases of this affection observed show so many variations that it would be at present premature to attempt sketching a common clinical type. The majority of the subjects were affected between the twenty-fifth and forty-fifth years.
ETIOLOGY.—Little is known of the causes of this disease. Usually beginning insidiously, no special mode of origin can be determined. Surface chilling has been assigned in a case by Erlitzky and Rybalkin, and others are reported to have begun during pregnancy. One of Westphal's cases developed in a lithographer who had been subject to epileptoid fits.
DIAGNOSIS.—As yet we have no reliable criteria for distinguishing between a combined sclerosis and certain forms of diffused sclerosis during life. Ballet and Minor110 found such a sclerosis diffusely involving the posterior and lateral columns of the cord in a case where they were justified from the symptoms in expecting a combined fascicular sclerosis of these columns, and after a careful study of all similar cases collated by them in consequence of this experience, they came to the conclusion that a number of affections of different origin, but eventually involving both columns, may impose on the observer as combined fascicular sclerosis during life. Diffuse meningo-myelitis is one of these affections, and is far from uncommon, while true system or combined sclerosis is apparently a very rare disease.
110 Archives de Névrologie, vii. p. 44.
SYNONYMS.—Friedreich's disease, the Family form of locomotor ataxia, Hereditary ataxia, Hereditary tabes.
Friedreich discovered a peculiar form of co-ordinating disturbance in a number of children of the same family, which he brought into relation with a lesion of the posterior columns, and which has been since found by him and by subsequent observers to occur in other cases, always [p. 871] affecting several members of the same family, as in the first case observed by him. The clinical and pathological features, though resembling those of the tabes dorsalis of adults in many respects, are distinct in others, and for this reason it is generally assigned a separate place in classification.
ETIOLOGY.—The disorder is usually manifested in juvenile life, the age of the affected subjects varying from the seventh to the twenty-fifth year. The male sex preponderates in the statistics of the affection. Some neuropathic vice can always be found in the patient's immediate ancestry, and the limitation of the disease to families burdened by such a diathesis is exemplified in the fact that the ninety individual cases thus far accurately studied occurred in thirty-six families.111 The disease type of the ancestors of the patients is usually different from that of the latter. Alcoholism in the father is one of the commonest forms, but convulsions, hysteria, and insanity are also frequent features of the family history. In a few cases tabes dorsalis, properly so called, was present in the father. In others there was consanguinity of the father and mother. In Musso's group the parents had been brother and sister, and their mother had been a melancholic dement. Three other grandchildren and six grandchildren by the incestuous marriage developed the family form of tabes. In this family the frequent experience of hereditary transmission was verified—that the neurotic taint skipped the intermediate generations.
111 Raffaele Vizzioli, Giornale di Neuropatologia, 1885.
CLINICAL HISTORY.—Usually the first symptom is ataxia of the lower extremities; occasionally this is preceded by severe frontal headache or by vague rheumatoid pains. The inco-ordination is very similar to that of true tabes dorsalis, but swaying on closing the eyes is not noticed early in the disease, as in the latter affection. The arms soon become involved in the ataxia, but cutaneous sensibility and the muscular sense remain either intact or nearly so—a fact utilized with some success by Erb in polemicizing against the theory of Leyden that the ataxia of tabes is due to imperfect sensation. Later in the disease, usually after a few years, a peculiar speech-disturbance is noticed, which resembles the scanning of disseminated sclerosis. It depends on ataxia of the tongue and lips. This is usually associated with nystagmus. About this time the patient develops a different set of motor symptoms from those characterizing the onset of the disease; contractures, paralysis, and atrophy are found in the affected extremities; sometimes the patients cannot ascend a stair, owing to their inability to lift the feet high enough. Pes equino-varus, deformity of other joints and of the vertebral column, have been observed112 to result from the associated effects of paralysis and contracture. At this stage some sensory disturbance may be developed, formication having been observed toward the close of the history in a number of cases. But the distribution of this disturbance is usually different from that of tabes dorsalis, being more intense in the trunk than in the extremities or evenly marked in the entire periphery.
112 H. E. Smith, Boston Medical and Surgical Journal, 1885, vol. cxiii. p. 361.
COURSE AND PROGNOSIS.—The progress of this disease is slow. It has not yet been known to be arrested by any therapeutical procedure. Death rarely occurs directly from the disease by exhaustion; more commonly life is cut short by some intercurrent affection. Unless this occurs [p. 872] the patients may survive the commencement of the illness from eight to forty and more years.
MORBID ANATOMY.—The sclerosis which is found to be the constant lesion underlying this disease corresponds in every character to a combined sclerosis of the pyramid tracts and the posterior columns. Usually, the crossed-pyramid tract is degenerated in its spinal course, and the uncrossed in the cervical and dorsal part, which, in many subjects at least, is its whole extent. The cerebral part of the pyramid tract is not affected. The nerve-fibres found normally in the gray substance are materially reduced, probably in dependence upon the atrophy of the great nerve-tracts.
The lesion of the posterior columns resembles that of true tabes very closely, particularly in the lumbar part of the cord. It is, however, not probable that it commences in precisely the same distribution, and if cases dying early in the disease be autopsied it will be interesting to see whether the initial sclerosis occupies identical fields—a contingency which is unlikely, owing to the profound difference in the initial symptoms of true tabes and the family form. It is claimed by Schultze that in addition to the pyramid and posterior tracts the cerebellar tract—or, rather, a large part of the periphery of the lateral column—may be sclerosed in this disease. In this way, since the direct pyramid tract in the anterior, the greater part of the border of the lateral, and the entire posterior column are degenerated, the sclerosis resembles a marginal ring113 in shape.
113 Archiv für Psychiatrie, xiv. p. 384.
Anatomically, the sclerosis of the family form of tabes resembles that form of combined sclerosis in which the lateral and posterior columns are together affected. It is probably due to a defective development of these tracts, rendering them liable to premature decrepitude or increasing their vulnerability. The latter alternative is exemplified in those cases where some acute disease of childhood, such as scarlatina or measles, acted as an exciting cause.
DIAGNOSIS.—There are two affections some of whose leading symptoms are so closely imitated by those of this disease that they may be confounded with it on first sight. These are tabes dorsalis—of which the family form is still regarded a variety, as the name indicates—and disseminated sclerosis. In the gait the former, in the nystagmus and scanning speech the latter, disorder is approximated. The distinction from true tabes has already been dilated on. (See Tabes.) The fact that relatives—usually the sisters and brothers—of the patient are affected in the same way in their youth speaks in favor of the family form. The deep reflexes are not abolished early, as in tabes, nor are anæsthesias or paræsthesias early symptoms, as in the latter. The speech-disturbance and nystagmus, which in most cases develop later in the family form, serve to distinguish it from true tabes in the advanced stage. It is at this period that the disease may resemble a disseminated sclerosis. The hereditary or family character does not aid us in making a discrimination here, as there is also a family form of the latter disease. But the absence of intention tremor, which we would assume to be present in a case of disseminated sclerosis of the cerebral type, and of optic-nerve atrophy serves to distinguish the two. Musso claims that the speech-disturbance is also different in character. There certainly is more lingual ataxia in the [p. 873] family form of tabes, and less of typical scanning, but I am doubtful about our ability to differentiate these characters in all cases. The following table includes the main points of difference, clinically considered, between the acquired and the family form of tabes:
| Tabes Dorsalis. | The Family Form. | |
| Prodromata. | Marked and constant. | Absent or slight. |
| Static ataxia (Romberg symptom). | Early and constant. | Absent. |
| Involvement of upper extremities. | Usually late. | Early. |
| Ataxia of tongue, eyes, and trunk-muscles. | Absent or unnoticeable. | Always developed. |
| Paresis. | Rare. | Characteristic. |
| Anæsthesia. | Present in some form. | Absent or slight. |
| Paræsthesia. | Constant. | Rare. |
| Sexual desire. | Becomes extinguished. | Remains unaffected. |
| Deep reflexes. | Abolition usually initial. | Abolition in course of disease.114 |
| Sphincters. | Involvement is characteristic and early. | Involvement late, if at all. |
114 There are conflicting observations on this point.
SYNONYMS.—Multiple cerebro-spinal sclerosis (also spinal and cerebral form), Insular cerebro-spinal sclerosis, Focal sclerosis, Multilocular sclerosis; Herd-sklerose (Ger.); Sclerose en plaques disseminées, Sclerose en plaques generalisées (French).
The occurrence of disseminated patches of gray degeneration in the nervous axis was observed by Cruveilhier and Türck, but they regarded the affection rather from the anatomical than the clinical standpoint, and it was left for Frerichs to recognize its important position among the chronic affections of the brain and spinal cord. The earlier German investigators who followed him were cautious in generalization, and it was not until Vulpian, Charcot, and their followers announced the discovery of infallible diagnostic criteria that disseminated sclerosis received that attention at the hands of the profession which it merits. But the more thorough researches made during the last two decades have shown that this announcement was premature. The best authorities recognize the existence of a large number of cases in which the supposed pathognomonic signs of disseminated sclerosis are absent, notwithstanding the existence of characteristic lesions, and thus the more cautious earlier investigators are justified in the reserve they had maintained.
It is in perfect harmony with the irregular location of the disease and the lack of any constant rule governing the distribution of the sclerotic foci that there is no constant clinical picture by which its existence can be accurately determined in all cases. The diagnosis of tabes dorsalis, of spastic paralysis, of amyotrophic lateral sclerosis, and of transverse myelitis rests on exact and constant signs, but that of disseminated sclerosis does not. The dictum of Charcot, that there is always intention tremor and nystagmus in disseminated sclerosis, has long been overthrown. Well-determined cases are on record by De Fleury and Westphal, and a number have been observed by myself, where there was no [p. 874] tremor or no increased tremor with intended movement, and no nystagmus, nor any other of the pathognomonic symptoms so considered by Charcot and his followers.
The morbid process of disseminated sclerosis consists in the development of patches of sclerosed tissue, scattered apparently without any regularity or rule through the brain and spinal cord. They are the results of insidious inflammatory changes. The symptoms marking their presence may include nearly every known focal and general symptom studied by neurologists, varying with the number, size, and distribution of the foci. Usually there is some disturbance of motility, both ataxic and paretic; in the majority there is tremor, which in a large proportion of cases is of a distinctive character, and disturbance of the functions of the cranial nerves, amblyopia, color-blindness, mental enfeeblement; and, above all, apoplectiform seizures are frequent.
Some writers discriminate between cases in which the lesions are limited to, or most intense in, the spinal cord, and those in which the brain is chiefly or exclusively involved, and hence they speak of a spinal, a cerebral, and a cerebro-spinal form. This discrimination is not sufficiently supported by clinical evidence to be of any practical value. Each case is to be studied by itself during life and after death, and to be regarded as one of a series in which the lesion may be concentrated in any one segment of the cerebro-spinal axis. It seems that when the sclerotic foci are limited to or chiefly located in the spinal cord, the clinical signs are less pronounced than where the brain is seriously involved; those cases in which the symptoms are latent, or so vague that they cannot be distinguished from spinal irritation or spinal exhaustion, have been found to be of the spinal type. The cases of this character thus far observed are not sufficiently numerous to justify the creation of special subdivisions.115
115 According as the formation of the sclerotic foci preponderates in a given segment of the nervous axis, the early signs of the disease may consist in disturbances of the cerebral or the spinal functions, and we may speak accordingly of a cerebral or spinal invasion type. But the principle of classification adopted by several recent writers, which would rank the spinal type among the spinal diseases, the cerebral type among the cerebral diseases, and which is compelled to erect a third category for the reception of the cerebro-spinal type under the name of cerebro-spinal diseases, is a bad one. Modern pathology recognizes the existence of affections which involve whole fibre-systems, which are intracerebral in one and intraspinal in other parts of their course, such as tabes and amyotrophic sclerosis, which would therefore have to rank among the cerebro-spinal, and not among the spinal affections, with which the authors referred to classify them.
CLINICAL HISTORY.—Prodromal.—Disseminated sclerosis is usually inaugurated by a long initial period in which the symptoms are not characteristic, and in which, unless there be decisive pupillary or optic-nerve symptoms present, the nature of the disease is not recognized. The patients feel weak and tired; walking is difficult, and an element of unsteadiness suggests the development of a tabic disorder. In other cases ankle-clonus is found and tremor of the foot on extension (dorsiflexion); it is discovered that the unsteadiness is due to weakness or to rigidity of the muscles, and thus the impression of a developing spastic paralysis may be created. But symptoms on the part of the cranial nerves soon show that the case is one of disseminated sclerosis. Sometimes a marked belt sensation is developed, and other forms of paræsthesia are not uncommon; nay, the symptoms of spastic paralysis and tabes [p. 875] dorsalis may be mingled. Diplopia of the same transitory character as in tabes usually accompanies the gradually-developing speech trouble. The reflex and mechanical excitability of the muscles is increased in all cases where the lateral column is extensively involved and the gray substance of the cord is—as it usually is in the main—intact. In some cases a slight tap on the knee when held in the position required to demonstrate the knee-jerk produces oscillatory movements of the limb; as the patient endeavors to suppress these they become more violent, extend to the trunk and head, and may eventually involve the opposite side. In those cases which show the cerebral-invasion type headache, vertigo, and speech disturbance, temporary darkening of the visual field, and loss of memory are the earliest symptoms directing attention to the existence of serious disease.
Whether the spinal or the cerebral symptoms preponderate, they continue increasing slowly and with temporary variations, which are particularly marked in the cerebral-invasion type. As a rule, the sensory disturbances are not pronounced at this time, but later, after the initial symptoms have existed for a few years, they become intense, and often extremely distressing. Those most complained of by the patient are neuralgic, lancinating, and other pains. The lancinating pains are, as a rule, not as severe as those of tabes dorsalis, but they are apt to be associated with a dull heavy pain which is located in a whole extremity, referred to the deep structures, and very persistent. This diffuse pain sometimes occupies all of the lower half of the body. As in tabes, the pain may be regarded the forerunner of anæsthesia, which rarely, however, reaches a high degree or an extensive distribution. Its distribution, like that of the other peripheral symptoms of disseminated sclerosis, is commonly irregular. Like the motor disturbance, which at this period consists in a combination of paretic and spastic—occasionally of ataxic—symptoms, it is most marked in the lower extremities.
In the majority of cases there is a peculiar tremor, which usually presents the character to which Charcot directed attention—namely, that it increases when the patient attempts to carry out a voluntary movement, and disappears, or at least diminishes, when the muscles of the part in question are at rest. This is the important symptom known as the tremor on intended movement or intention tremor. One of the time-honored means of testing it is to order the patient to take a glass of water and pass it to his mouth. While he reaches out for it some oscillatory unsteadiness is observed, but on grasping, this is increased, and on raising the glass the oscillations increase till he spills the water; if he succeeds in carrying it to his mouth, there is a clattering against the teeth, and but for the steadying aid of his mouth he would throw it aside by the violence of the disturbing movements. In incipient cases this intention tremor is best shown with delicate movements, and the more distinctly the more slowly they are performed. It has been suggested that the peculiar character of the lesion of disseminated sclerosis has some relation to the intention tremor. It is a remarkable feature of the morbid process that it leaves the axis-cylinder comparatively intact, beyond any other form of myelitis or encephalitis. The myelin, however, is destroyed, and the consequence is that the naked axis-cylinders lie in a newly-formed connective tissue, which has not the same faculty the myelin has of [p. 876] isolating the nervous impulses conducted through the axis-cylinders. The result is, that when a nervous impulse, such as a voluntary movement, travels through a sclerotic focus, it may become deflected to neighboring fibres going to another muscle or muscular bundle than the one intended to be innervated. An unintended motion results; the patient makes a stronger effort, intended for the right channel, but again it slips off, to use a coarse simile, and thus a number of erroneous messages are transmitted, and an equal number of disturbing motions respond to these messages.
Whether this histological explanation be correct or not, the tremor is probably due to the lesion of the peduncular tracts of the brain. At least, this is rendered plausible for the tremor on intended movement, which indicates an interference with the transmission of voluntary impulses. Whether, as Pasternatzky116 claims, the extreme muscular oscillation seen in advanced cases is due to irritation of the cortical motor fields, it is impossible to decide. No strong evidence can be adduced in favor of his view. A few cases have been described (Schüle, Jolly, and Greiff); and, in my opinion, such are far more numerous than is usually supposed, where the tremor did not have the so-called characteristic feature of ceasing in conditions of rest, claimed by Charcot, but continued as in paralysis agitans.117 A collection of cases by Erb, Ordenstein, and Greiff shows clearly that with a typical dissemination of sclerotic foci in the cord the tremor on intended movement may be entirely absent, while no case is known where the crus and pons were involved to a similar extent in which it was absent. So it seems that a cerebral lesion is necessary to produce this symptom in its characteristic form.
116 Jahrbücher für Psychiatrie, iii. 3, 1882.
117 For several years I had been puzzled by the fact that Charcot's formula failed to correspond to the clinical picture in the majority of cases, and I registered such cases as incipient multiple sclerosis or as a connecting group between paralysis agitans and that disease.
In advanced cases of disseminated sclerosis the intention tremor becomes generalized; previously noticed, perhaps, only in one arm, it now affects all the limbs and the muscles which maintain the trunk and head in static equilibrium. The result is, that even when the patient is at rest sitting in a chair, his body, and particularly his head, are agitated by a violent and coarse tremor, which is increased on rising and walking, as well as on attempting to use the hands. Delicate mechanical occupations become impossible, and the handwriting shows a characteristic change, the forward strokes of the letters and the curvilinear back strokes, as well as the dots and crosses, registering the tremor of the hand in their peculiar irregularity.
The speech is usually rough and broken, and sometimes enunciation is impeded in a peculiar way, the patient appearing to scan his words. Krause118 has found relaxation of the vocal cords in a remarkable degree to underlie the change in phonation. The scanning of speech appears to be due to impeded innervation of the lips and tongue. When the patient is told to protrude his tongue, he does so either in spasmodic instalments of movement or with a sudden jerk after delay. The same delay and apparent halting are noticed in the mimic expressions that are observed [p. 877] in speech. The features sometimes express an emotion opposite to the one experienced by the patient.119
118 Neurologisches Centralblatt, 1885.
119 This symptom is found where there are other reasons for suspecting the existence of large foci in the pons. I have observed it in one case of tumor of this region, and one of a focal disease of undetermined anatomical nature in the same location, in a remarkable form. In the former case the patient not only exhibited the facial contortions of hearty laughter when she felt as if about to break out in tears, and broke out in tears when she felt amused, with perverse regularity, but both emotional manifestations occurred simultaneously. The other case is still under observation. There was complete anarthria in the first, and nearly complete anarthria in the second case—a fact not unrelated to the inferred site of the lesion, and which may be associated with the fact that where the perverse mimic expression occurs in disseminated sclerosis the speech-disturbance often has an anarthric character.
Whether diplopia occur as an early symptom or not, nystagmic oscillation of the eyeballs is commonly found in the developed affection. This nystagmus is usually universal, noted in associated movements in every direction, and aggravated by excitement, by constrained positions, and by any act of innervation of the eye-muscles. It may be looked upon as an intention tremor of the latter, and attributed to sclerotic foci in the cerebral axis, particularly in the tegmental part of the pons varolii.
The deep reflexes are in some cases but slightly affected. Where spastic phenomena preponderate, they are exaggerated, and where the posterior root-zones are involved in the lesion, they may be, as in tabes dorsalis, diminished or absent. The nutrition of the muscles is not impaired in the early stages, and indeed most functions which depend for their proper performance on the intact condition of the gray substance, such as the power of retaining the urine, micturition, and the functions of the rectum, are properly performed at this period. The cutaneous reflexes are not markedly abnormal in the majority of cases. They sometimes become diminished in the last stages.
In cases regarded as disseminated scleroses and similar disorders approximating the combined form of sclerosis, Westphal120 noticed a paradoxical muscular phenomenon which is the reverse in action of the tendon reflexes. It is best observed in the tibialis anticus: if the foot be extended (dorsiflected)—in other words, if the origin and insertion of this muscle be approximated—the muscle contracts firmly, keeping the foot in the enforced position, as if frozen into that attitude. The same occasionally occurs if the patient voluntarily extends his foot. Westphal observed the same phenomenon in the disease described by him in which the symptoms of disseminated sclerosis are present, but the corresponding lesion is not visible.121
120 Archiv für Psychiatrie, x. p. 243.
121 Ibid., xiv. p. 132. It is a noteworthy fact that this sign has been observed by its discoverer also in paralysis agitans.
In a number of cases the mind becomes involved. Simple dementia is the commoner condition, and some indication of passive mental enfeeblement is found sooner or later in the history of the disease in the majority of cases. In addition, there may be a morbid emotional condition, usually in the direction of depression. I have been struck by the frequent association of a melancholic state with large foci in the oblongata. When it is borne in mind that the patient exhibits tremor and speech-disturbance in addition to his mental trouble, it will be understood that with some modifications of the typical signs the case may simulate one of paretic dementia; and there are cases in which it is exceedingly difficult to decide [p. 878] whether they belong to an aberrant type of disseminated sclerosis or to the sclerotic type of paretic dementia. There are some which constitute veritable connecting-links between the two affections.122
122 Zacher, Archiv für Psychiatrie, xiii. p. 168; the writer, Journal of Nervous and Mental Diseases, April, 1877, and Insanity, its Classification, Diagnosis, and Treatment, p. 240.
Like tabes dorsalis, the progress of disseminated sclerosis is often marked by episodes. Some of these differ in no way from the visceral crises of posterior-column sclerosis; every form of these symptoms found with that affection may occur in the present one, while episodes involving the cerebral functions are much more common. The latter manifest themselves as apoplectiform or epileptiform seizures. They are preceded by headache and vertigo, or, if these be continuously present, by an aggravation of them; then unconsciousness develops, either accompanied by convulsions or not, and the face is flushed, the pulse full and frequent, and the temperature raised. Consciousness returns in a few hours or a day, the attack rarely lasting more than two days, and it is found that the patient is hemiplegic. But, unlike the hemiplegia found after vascular rupture, embolism, or structural cortical disease, it is rapidly recovered from.
In a case of Gnauck's an attack of scotoma scintillans, associated with a noise of thunder in the right ear and pricking pains on the right side of the face, preceded anæsthesia and the formation of a small defect of the visual field.
There is a close resemblance between these apoplectiform and epileptiform seizures and those of paretic dementia, not alone in clinical character, but also in the surprisingly complete and rapid recovery from the more serious symptoms. But just as in paretic dementia, especially in its advanced stage, each seizure leaves the patient somewhat more impaired in mind and body than he was before, so it is in disseminated sclerosis; each attack marks a step forward in the invasion of the morbid state.
Eye-trouble is much less frequently a premonitory sign of disseminated sclerosis than of tabes. A few such cases are on record. Magnan observed the development of the characteristic symptoms of disseminated sclerosis fourteen years after an amaurosis which followed typhoid; and Gnauck reports another in which first a right ptosis, and then a right amblyopia, preceded the ordinary symptoms. In exceptional cases this premonitory eye-trouble may, like that of tabes, rapidly lead to extreme amblyopia or even amaurosis. The visual disturbances are remarkable for their rapid changes. They appear within a short period, attain their maximum rapidly, and may occasionally retrograde as quickly. They develop under two forms—the central and the peripheral scotoma, or, rather, limitation of the visual or color field. The former, like the amblyopia of alcoholic and nicotine intoxication, consists in an inability to differentiate between red and green in the centre of the visual field. It never, in my experience, proceeds as far as the toxic amblyopias; that is, to the complete extinction of vision.123 The peripheral limitation of vision may be for both quantitative and qualitative light-perception, but it is not, as a rule,124 concentric as in tabes, but sector-like.
123 Gnauck says that the central color-blindness may become total, and the red-green blindness extend to the periphery.
124 Concentric limitation of ten to thirty degrees has been noted for color-perception.[p. 879]
The atrophy of the optic nerve in disseminated sclerosis is typically partial, in the majority of cases manifesting itself as a sharply-marked discoloration of the temporal half of the papilla. In others the nasal half of the papilla also becomes discolored, but so much less intensely that the difference between the earlier involved and later involved portions is quite easy. It is doubtful whether the subjective visual disturbance is always an indication of the extent to which the optic nerve is involved. There are good reasons for believing those amblyopias and limitations of the field of vision which show marked remissions and exacerbations to be due to some dynamic central condition involving the visual centres and tracts. Thus it has been observed that almost total amaurosis occurred after an apoplectiform attack, to disappear later on. Occasionally the amblyopia is bilateral and the optic-nerve lesion unilateral. The frequency of this affection is stated by Gnauck125 as follows: In one half the cases there is diminished vision, and in half this half optic-nerve atrophy with limitation of the visual field. It is only in exceptional cases that an optic neuritis can be determined to have preceded the atrophy.
125 Of 50 cases, 22 had no visual trouble, 8 showed simple diminution of perception, 5 added limitation, and 15 changes of the optic disc, a case of total atrophy and amaurosis being included in the latter.
The pupils are perfectly normal in some cases; in others myosis of the spinal type is observed; and this I found to be nearly constant in all advanced cases. Irregularity in outline and inequality exist in a small proportion, and reflex iridoplegia is found in about 10 per cent. of the cases.
Thus far, the symptoms which occur either in a majority or in a large percentage of cases have been enumerated. The typical course of disseminated sclerosis may be stated as consisting in their gradual development and intensification, covering a period of from four to twenty or more years. There are a number of cases in which so many of the symptoms regarded as typical are either absent or where some given symptom-group preponderates over the others to such an extent that they require special mention.
It is not difficult to understand that disseminated sclerosis may ape other forms of spinal disease. Its symptoms depend on the location of the sclerotic foci. If these are situated chiefly in the crossed-pyramid tract, spastic phenomena will predominate, and the case may resemble a spastic paralysis.126 If they be distributed in both the posterior and lateral columns, the symptoms will resemble those of a combined form of sclerosis in which the tabic and spastic signs are associated, as far as they do not, in the nature of the case, neutralize each other. This was well shown in a case of De Fleury's. Not infrequently an unusually large focus involves the entire transverse section of the cord, and the case becomes complicated by the symptoms of a transverse myelitis. In such a case, described by Rovigli,127 a large transverse focus in the cord had led to ascending secondary degeneration in the column of Goll and descending degeneration of the crossed pyramid tract. In a large series, instances of which are related by Kilian,128 Siemens,129 Schultze,130 Zacher,131 and Greiff,132 [p. 880] the disseminated foci were complicated by a diffuse lesion distributed like that of a diffuse or fascicular myelitis; and there seems to exist every connecting-link between ordinary chronic myelitis, strictly so called, and disseminated sclerosis.
126 Gnauck, Neurologisches Centralblatt, 1884, p. 315.
127 Rivista sperimentale di Freniatria e di Medicina leqale, x. p. 227.
128 Archiv für Psychiatrie, vii. p. 28. He designates this form sclerosis continua multiplex.
129 Ibid., x. p. 135.
130 Ibid., xi. p. 216.
131 Ibid., xiii. p. 168.
132 Ibid., xiv. p. 287.
Not only does disseminated sclerosis occasionally imitate or approximate the regular (fascicular) affections of the cord, as well as diffuse cerebro-spinal affections, but it may appear under the mask of a nuclear oblongata paralysis.133 And cases are on record where, in addition to the disseminated sclerosis, there occurred sclerotic atrophy of an entire hemisphere or of its capsular tracts, thus leading to a hemiplegic resemblance of the motor paralysis. In my experience the cases presenting the type of a nuclear oblongata paralysis run a more rapidly fatal course than others. The shortest history in my series, one of four years, was of such a case. A number of instances are on record by careful observers—and are probably much more numerous than is commonly suspected—where no decisive evidence of spinal or cerebral disease could be detected during life, and yet disseminated foci of sclerosis existed in the nerve-centres. In such cases the symptoms may be in the direction of simple nervous prostration, more commonly of spinal irritation. I have now under observation a case which for years had been regarded as one of spinal irritation, and which made that impression on me until I discovered the existence of optic-nerve atrophy, which was the only indication that the symptoms depended on gross structural disease.134
133 It is customary to speak of symptoms referable to the oblongata as bulbar. The designation bulbus rachidicus is now obsolete, and just as we speak of a capsular hemiplegia, a pons paralysis, or a spinal hemiplegia, so we should say an oblongata paralysis, discriminating between the nuclear, the neural, and the tract affections by means of a prefix.
134 At present the symptoms of disseminated sclerosis are unmistakable. Cases are mentioned by Strümpell and others in which they remained indecisive throughout.
Among the anomalous forms of disseminated sclerosis there is one which is characterized by the preponderance of paraplegia and contractures in a combination which is usually found in spinal diseases of a different type. The coexistence of dementia, however, usually enables the observer to determine that the lesion is both cerebral and spinal, although those signs which might enable him to decide the disseminated focal character may be absent.
MORBID ANATOMY.—In advanced cases of disseminated sclerosis the lesion is visible to the naked eye on the surface of the brain and spinal cord. Grayish maculas, sometimes elevated, more rarely a little sunken, and occasionally showing a buff or reddish tinge, are seen on the surface of the spinal cord, the oblongata, pons, and crura. On making sections across the region of the spots, it is found that the color-change is not superficial, but extends inward, involving large parts of the transverse area of the cord or the cerebral axis; and patches lying more deeply in their substance are revealed whose existence could not have been suspected from a mere surface inspection. Exceptionally, patches are found involving the entire transverse section of the spinal cord in a length of a half to two inches. And, similarly, in the brain nearly the entire area of the pons or one of the crura or an entire division of the internal capsule may be occupied by a sclerotic focus. Otherwise, they may vary from almost microscopic dimensions to the size of a chestnut or even larger. [p. 881] Bourneville135 has described cases in which the nerve-centres appeared normal to the naked eye, while the microscope revealed the existence of sclerotic foci. It is, however, unlikely that the fresh brain- and cord-tissue, when the site of disseminated sclerosis, will appear perfectly healthy to the naked eye under fairly good illumination. Much less intense lesions than those of disseminated sclerosis reveal their presence by changes in color and consistency.
135 Mouvement medicale, 1869, No. 27.
On examining the diseased spots more narrowly, they are found to be slightly diaphanous. Usually, they are rounded or elliptical, but they are often drawn out, as it were, in the most irregular shapes, and not infrequently appear to be the result of a confluence of originally remote and separate foci. In the cord they are sometimes wedge-shaped, extending inward from the periphery. To the touch they appear firm—sometimes not much more so than the normal tissue, contrasting with it as hard-boiled white of egg would contrast with soft-boiled; in advanced cases they become of almost leathery consistency, and there are instances recorded where they actually creaked under the knife. A clear fluid usually runs from their cut surface, and the latter does not jut up on section like normal nerve-tissue.
The distribution of the diseased areas follows no known law. They may be numerous and of large size in one segment of the nervous axis, and small, few in numbers, or even absent, in others. In some altitudes of the cord the lateral, in others the posterior, in still others the anterior, columns are chiefly involved. The cerebrum usually contains a larger number of foci irregularly scattered in the centrum ovale of Vieussens, the internal capsule and its surrounding ganglia, as well as in the corpus callosum. Throughout the nervous axis it seems that the lesion chiefly affects the white substances, and even the roots of the peripheral nerves, both cranial and spinal, are occasionally found to contain small foci, gray, firm in consistency, and as distinctly outlined as those of the central organs.
The morbid process consists in an atrophy and gradual disappearance of the myelin, which is preceded, if not caused, by an increase of the enveloping interstitial substance. This change is of the same character as that found in chronic myelitis. The septa and trabeculæ of connective tissue become thicker, formless connective substance and fibrillar tissue, which seems to arise in, if not in part from, it, constituting the new formation. The neuroglia-nuclei are increased, enlarged, and develop into spider-shaped cells, whose long processes contribute (according to some authors exclusively) to the newly-formed fibrillar network.
While the myelin undergoes wasting, the axis-cylinders remain intact for a long period, and even in intensely sclerosed regions they may be found in nearly their normal number, but naked and in direct contact with the pathological fibrillæ. Some of them become hypertrophied, increasing to twice, thrice, and, according to Leyden, even more, of their normal diameter. This change seems to inaugurate the last phase of the process: the axis-cylinders, becoming sclerosed and brittle, ultimately disappear, and no trace, or at best but doubtful traces, of the normal nerve-tissue are left behind. The blood-vessels, following the rule of [p. 882] the sclerotic process, take part in it. Their walls become thickened, richly nucleated, and the lumen becomes narrowed in consequence. In the smaller vessels complete obliteration of the lumen is sometimes observed.
The gray substance is not involved as frequently as the white, but it opposes no barrier to the extension of the morbid process when once established in its neighborhood. The nerve-cells show the same resistance which the axis-cylinder does; that is, they retain their outline and fibre-connections a long time in the midst of the diseased area. But eventually they become discolored, undergo hyaline or granular disintegration, their processes shrink, and finally they disappear.
Ribbert and Zacher consider the sclerosis of tabes and the disseminated affection to be much more similar than Leyden and Charcot supposed. They locate the starting-point of the morbid process in the vascular and connective tissues; and Greiff, in harmony with this view, finds that the foci occur most frequently in those parts of the cord where the connective-tissue trabeculæ are most numerous, as in the posterior columns and at the junction of the anterior and lateral columns.
Although the morbid foci appear to the naked eye to be uniform, and to be sharply demarcated in the normal tissue, closer examination shows that the areas of maximum lesion are surrounded by a narrow transition zone by which the lesion seems to mark its eccentric progress, and occasionally a focus of intense disease lies in a diffused area of slight changes, resembling those of diffuse myelitis. Sometimes the cord appears to be almost continuously involved by a lesion of moderate intensity, and a few disseminated foci in the brain alone prove that the case belongs to this form of sclerosis.
A few years ago Greiff described what he considered a new lesion in multiple sclerosis, under the name of disseminated vitreous degeneration of the cerebral cortex.136 I have been familiar with this lesion since 1876: it can be produced at will in perfectly healthy brains, and consists in a precipitation of leucine crystals extracted from the brain-substance by the action of alcohol. His accompanying figure137 represents this artificial lesion very accurately; and Greiff, if he fails to recognize that his vitreous degeneration is a spurious lesion, at least identifies it with the miliary sclerosis of Bucknill and Tuke and the spheres of Schüle, which are now generally recognized to be the results of post-mortem manipulations and not actual lesions.138
136 Archiv für Psychiatrie, xiv. p. 286.
137 Ibid., xiv., Plate ii. Fig. 5.
138 Attention was first called to the artificial nature of these bodies by the writer in the Journal of Nervous and Mental Diseases, October, 1877, and a more accurate description was given in the Chicago Medical Review of 1880, and in a demonstration before the New York Neurological Society in 1883. In commenting on the latter a German critic stated that the facts related had been long known in Germany (Neurologisches Centralblatt, 1883, p. 283). On inquiring of the critic what publication contained any reference to this discovery, he frankly stated that he knew of none, but had had in mind what he considered a tradition of the laboratory. It was in the same year that Greiff worked at the Heidelberg laboratory under the eminent supervision of Fürstner, and it was a few years previous that Schüle, one of the collaborators of Ziemssen's Cyclopædia, had made the same mistake. So it seems that the tradition is in some danger of expiring, and that it would do no harm to accept the caution, even though it travel across the Atlantic in the reverse of the usual direction. It has been amply confirmed by Savage and Plaxton (Journal of Mental Science, October, 1882, and April, 1883).
In judging as to the nature and intensity of the inflammatory process [p. 883] which leads to the development of the sclerotic foci, it must be remembered that we are acquainted thus far only with the terminal period of the disease, when, as is to be presumed, the active inflammatory changes have gone by or are in the background. It is very probable that the newly-formed tissue is more nucleated in early periods than is found in the cases which constitute the material of pathological laboratories. In a case of protracted nervous exhaustion accompanied by spinal irritation in an alcoholic subject who was murdered, and whose brain and cord I had an opportunity of examining, I found, both in the cord and brain, districts in which the white substance showed a slight grayish discoloration and increased consistency. Minute examination failed to show any qualitative change in the conducting elements, but the interstitial tissue was hypertrophied, richly nucleated, and showed Frommann's cells in abundance.
ETIOLOGY.—Heredity has been observed in a number of cases by Duchenne, Erb, and Frerichs. The latter two had each an opportunity of recording this inheritance in several members—sisters or brothers—of the same family. In these cases the transmitted affection developed in adult life. Dreschfeld, however, cites a case where two brothers developed its symptoms in a marked degree in infancy. As an associated feature it is found with some cases of congenital defect. Thus Pollak139 discovered disseminated sclerosis in an infant which had a defective corpus callosum and exhibited the characteristic signs of the focal affection side by side with the imbecility due to imperfect cerebral development. As a rule, the disease is developed after the twentieth year. But cases have been related (De Fleury) where the patient developed the disease and died with an apoplectiform onset in earlier life. One of the youngest on record is described by Hödemacker.140 The subject developed the disease at the seventh year, and died with it at the fourteenth, having shown the characteristic symptoms, besides more muscular atrophy than is common. The sclerosis in this case belonged to the type which has been referred to as a connecting-link between diffuse and disseminated sclerosis. Pelizæus141 reports five cases developing in the same family in early life, corresponding somewhat in their relation to multiple sclerosis of advanced life, as the family forms of tabes and spastic paralysis correspond to the typical adult forms of those diseases. All the cases were of males, and the ancestral taint had been present in male members of the family, passing through the females to their progeny without breaking out in the mothers. Each branch of this family appeared to develop its own peculiar type of the disorder.
139 Deutsches Archiv für klinische Medizin, Bd. xxiv. p. 404.
140 Ibid., vol. xxiii. p. 442.
141 Archiv für Psychiatrie, xvi. p. 698.
CAUSES.—Disseminated sclerosis may develop as a sequel of an acute myelitis. An excellent observation of Singer,142 in which a unilateral optic-nerve atrophy of central origin occurred after recovery from an acute inflammation of the cord, proves that sclerotic foci may develop secondarily to an acute process. Westphal believes that obstruction to the circulation, both of blood and lymph, in the cord may act as a predisposing factor in the production of multiple sclerosis. He rests this opinion on a case where the cord had been compressed by a tumor, and [p. 884] sclerotic foci of probably later date were found in the neighboring segments of the cord.
142 Prager medizinisch Wochenschrift, 1885, No. 8.
The myelitic affection discovered by the same observer143 to be an occasional sequel of typhus, smallpox, diphtheria, measles, and erysipelas is a true disseminated sclerosis. The foci are usually very small and very numerous. A focal sclerosis of the posterior columns of the disseminated type has been found by Brigidi-Bandi in a case of pellagra which presented ataxic symptoms.144
143 Archiv für Psychiatrie, iii. p. 376, iv.; Oertel, Deutsches Archiv für klinische Medizin, viii.; Damaschino, Gazette médicale de Paris, 1871, p. 505. In one case now under observation a typical disseminated sclerosis developed in a robust young man of thirty after typhoid fever.
144 Lo sperimentale, December, 1879.
Among the exciting causes, prolonged exposure to wet and cold are acknowledged to occupy an important position. The frequent combination of these factors with over-exertion and depressing emotions among the poorer classes probably account for its great frequency among them. In some cases excessive grief has been the only discoverable etiological factor: in three of my own cases this was so prominent and connected a feature that I could not doubt its influence, if not as a primary at least as an exciting cause.145 Fright has been distinctly connected with the outbreak of the disease in a number of cases.146 There is considerable unanimity among observers regarding the effects of shock and injury in producing disseminated sclerosis, usually of that anomalous type which approximates the diffuse or fascicular form. Railway spine is undoubtedly the mask of a disseminated inflammatory trouble in a number of cases; the only authority of weight who opposes this view is Charcot, and his opposition is abundantly neutralized by a number of carefully-studied American and European cases.
145 The coincidences among these three cases were remarkable. All three were Germans, all three musicians, two had lost an only son. In all, the emotional manifestations were pronounced from the initial to the advanced period of the disease.
146 A Bohemian cigar-maker was startled by the sudden firing of a pistol-shot in a dark hallway, and on arriving at the factory, and not fully recovered from the first fright, he was again startled by the sudden descent of an elevator and the fall of a heavy case from it close to where he stood. From the latter moment he trembled, and his tremor continued increasing till the last stage of his illness was reached. This was my shortest duration, four years, and of nuclear oblongata paralysis type.
Hysterical and other obscure neuroses have been claimed to act as predisposing causes. But, inasmuch as it is well established that sclerosis is not a legitimate sequel of even the most aggravated forms of true hysteria,147 and, on the other hand, that disseminated sclerosis, particularly in the early stages, may progress under the mask of spinal irritative or other neuroses, it is reasonable to suppose that cause and effect have been confounded by those who advanced this view. According to Charcot, the female sex shows a greater disposition to the disease than the male. Erb, who bases his remarks on the surprisingly small number of nine cases, is inclined to account for Charcot's statement on the ground that it was at a hospital for females that Charcot made his observations. On comparing the figures of numerous observers, it will be found that in the experience of one the females, and of the other the males, preponderate. [p. 885] In my own experience the males far exceed the females both in private and in dispensary practice. Of 22 cases with accessible records, only 7 were females.
147 Charcot's observation of lateral sclerosis in hysterical contracture, although made so long ago, has not been confirmed, and the most careful examinations in equally severe and protracted cases have proven altogether negative.
Syphilis has also been assigned as a cause. The connection is not as clear as in tabes. In the few cases where there appears to be a direct causal relation the lesion is not typical. There are sclerotic foci, but in addition there is a general lesion, particularly of the posterior columns of the cord, such as is found with paretic dementia. And it has been noted that periendymal and subendymal sclerosis is more frequent with the cases of alleged syphilitic origin than with those of the typical form.
DIFFERENTIAL DIAGNOSIS.—In view of what has been already stated regarding the numerous clinical types found in disseminated sclerosis, it is easily understood why the diagnosis of this disease is becoming more and more uncertain: every new set of researches removes some one or several of the old and cherished landmarks; and it may be safely asserted that only a minority of the cases show that symptom-group which was formerly claimed as characteristic of all. The discovery of a series of cases by Westphal,148 in which the typical symptom-group of Charcot was present, but no sclerosis deserving the name found after death, as well as the interesting experience of Seguin, who found well-marked disseminated sclerosis in a case regarded as hysterical intra vitam, illustrates the increasing uncertainly of our advancing knowledge. It was believed within a few years that the presence of cranial nerve-symptoms was a positive factor in determining a given case to be one of disseminated sclerosis, but in the very cases described by Westphal such symptoms were present notwithstanding the lesion was absent. Up to this time, however, no case has been discovered in which, optic-nerve atrophy being present in addition to the so-called characteristic symptoms of intention tremor, nystagmus, and scanning in speech, disseminated foci of sclerosis were not found at the autopsy. This sign may be therefore regarded as of the highest determining value when present; but as it is absent in the majority of cases, its absence cannot be regarded as decisive. The presence of pupillary symptoms also increases the certainty of the diagnosis when added to the ordinary and general symptoms of the disorder related above.
148 Archiv für Psychiatrie, xiv. p. 128.
Although the difference between the tremor of typical disseminated sclerosis and that of paralysis agitans is pathognomonic, yet the existence of a group of cases of disseminated sclerosis, as well as of one of cases of paralysis agitans without tremor, renders an exact discrimination in all cases impossible. It is a question, as yet, whether the form of paralysis agitans without tremor described by Charcot, and which is marked by pains in the extremities, rigidity, clumsiness, and slowness of movement, general motor weakness, a frozen countenance, impeded speech, and mental enfeeblement, is not in reality a diffuse or disseminated sclerosis.
The diagnosis of this disease, while readily made in a large number of cases on the strength of the characteristic symptoms detailed, may be regarded as impossible in a minority which some good authorities incline to regard as a large one.
SYNONYMS.—Chronic myelitis, Diffuse myelitis, Simple or Diffuse spinal sclerosis, Chronic transverse myelitis, Sclerosis stricte sic dicta (Leyden, in part), Gray degeneration.
The various forms of sclerosis thus far considered were at one time considered as varieties of chronic myelitis, and under different names, founded on leading symptoms, were considered to be merely local, and perhaps accidental, variations of one and the same morbid process. More accurate clinical and pathological analysis has separated from the general family of the scleroses one clearly demarcated form after another. Tabes dorsalis, disseminated sclerosis, amyotrophic lateral sclerosis, and the combined forms of sclerosis have been successively isolated. Still, a large number of cases are left which cannot be classified either with the regular affections of the cord, limited to special systems of fibres, or with the disseminated form last considered. They agree with the latter in that they are not uniform; they differ from it in that they are not multilocular. Not a few modern authors have neglected making any provisions for these cases, while others treat of them in conjunction with acute myelitis, of which disease it is sometimes regarded as a sequel. The term diffuse sclerosis is here applied to those forms of chronic myelitis which follow no special rule in their location, and to such as are atypical and do not correspond in their symptomatology or anatomy to the more regular forms of sclerosis. In regional distribution the foci of diffuse sclerosis imitate those of acute myelitis: they may be transverse, fascicular, or irregular.
MORBID ANATOMY.—In typical cases the lesion of diffuse sclerosis constitutes a connecting-link between that of the disseminated form and posterior sclerosis. Its naked-eye characters are the same. There is usually more rapid destruction of the axis-cylinders, more inflammatory vascularization, proliferation of the neuroglia-nuclei, and pigmentary and hyaline degeneration of the nerve-cells, than in the disseminated form.
Syphilitic inflammation of the cord extends along the lymphatic channels, including the adventitial spaces, and leads to a diffuse fibrous interstitial sclerosis. In one case in which I suspected syphilis, though a fellow-observer failed to detect it after a rigid search, I found a peculiar form of what would probably be best designated as vesicular degeneration, according to Leyden, though associated with a veritable sclerosis. The lymph-space in the posterior septum showed ectasis; the blood-vessels were sclerotic, and each was the centre of the mingled sclerotic and rarefying change. It appears that while the interstitial tissue hypertrophied, the myelin of adjoining nerve-tubes was pressed together till the intervening tissue underwent pressure atrophy. The result was, the myelin-tubes consolidated, some axis-cylinders perished, others atrophied, a few remained, and, the myelin undergoing liquefaction, long tubular cavities resulted, running parallel with the axis of the cord, and exposed as round cavities on cross-section (Fig. 32). The changes in the cells of the anterior horn in the same cord (Fig. 33) illustrate one of the common forms of disease to which they are subjected in the course of sclerotic disease.
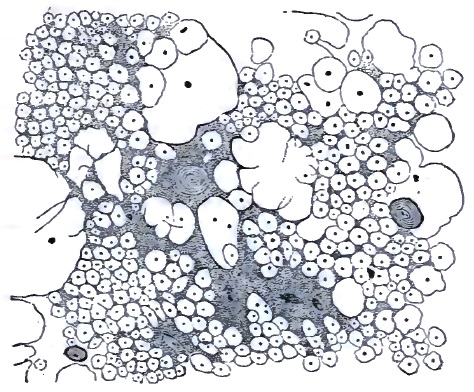
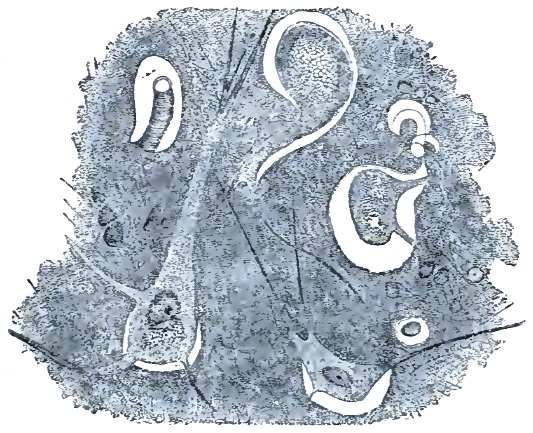
The so-called myelitis without softening, or hyperplastic myelitis of [p. 887] Dujardin-Beaumetz, which is ranked by Leyden and Erb among the acute processes, properly belongs here. It is characterized by a proliferation of the interstitial substance, both of its cellular and fibrillar elements. The nerve-elements proper play no part, or at best a very slight or secondary one. In the sense that this affection occurs after acute diseases and develops in a brief period it may be called an acute myelitis, but both in its histological products and its clinical features it approximates the sclerotic or chronic inflammatory affections of the cord. As far as the clinical features are concerned, this is particularly well shown in the disseminated myelitis found by Westphal after acute diseases, such as the exanthematous and continued fevers.
[p. 888]CLINICAL HISTORY.—Impairment of motion is the most constant early feature of chronic myelitis; in the transverse form it may be as absolute as in the severest forms of acute myelitis; as a rule, however, it is rather a paresis than a paralysis. The patient is usually able to walk, manifesting the paraparetic gait: he moves along slowly, does not lift his feet, drags them along, makes short steps; in short, acts as if his limbs were heavily weighted. This difficulty of locomotion is preceded and accompanied by a tired feeling before other sensory symptoms are developed. Rigidity of the muscles, like that found in disseminated sclerosis, is a common accompaniment, and may even preponderate over the paresis to such an extent as to modify the patient's walk, rendering it spastic in character. In such cases the muscles feel hard to the touch, and the same exaggerated reflex excitability may be present as was described to be characteristic of spastic paralysis.
If, while the leg is slightly flexed on the thigh, the foot be extended,149 so as to render the Achilles tendon and the muscles connected with it tense, and the hand while grasping the foot suddenly presses the latter to still further extension, a quick contraction occurs, which, if the pressure be renewed and kept up, recurs again and again, the succession of the involuntary movements resembling a clonic spasm. This action is termed the ankle-clonus or foot-phenomenon. Gowers has amplified this test of exaggerated reflex excitability by adding what he calls the front-tap contraction. The foot being held in the same way as stated above, the examiner strikes the muscles on the front of the leg; the calf-muscles contract and cause a brief extension movement of the foot. It is believed that the foot-clonus and the front-tap contraction are always pathological, but a few observers, notably Gnauck, leave it an open question whether it may not occur in neurotic subjects who have no organic disease. Gowers considers the foot-clonus found in hysterical women as spurious, and states that it differs from the true form in that it is not constant, being broken by voluntary contractions, and does not begin as soon as the observer applies pressure. But I have seen the form of clonus which Gowers regards as hysterical in cases of diffuse sclerosis. With regard to the front-tap contraction, its discoverer150 admits that it may be obtained in persons in whom there is no reason to suspect organic disease. It is significant only when unequal on the two sides.
149 By extension the approximation of the dorsal surface to the tibial aspect of the leg—what some German writers call dorsal flexion—is meant.
150 Gowers, The Diagnosis of the Diseases of the Spinal Cord, 3d ed., p. 33.
In severe cases contractures are developed in the affected muscular groups, being, as a rule, preceded by the rigidity, increased reflex excitability, and the thereon dependent phenomena above detailed. These contractures may be like those of spastic paralysis, but usually the adductors show the chief involvement, and sometimes the leg becomes flexed on the thigh and the thigh on the abdomen in such firm contraction that the patient, albeit his gross motor power is not sufficiently impaired, is unable to move about, and is confined to his bed, his heel firmly drawn up against his buttock. It is stated by Leyden that the contracted muscles occasionally become hypertrophied—an occurrence I have not been able to verify. As a rule, some muscular groups are atrophied, though [p. 889] the limbs as a whole, particularly in those patients who are able to walk about, are fairly well nourished.
Pain in the back is a frequent accompaniment of diffuse sclerosis. It is not pronounced, but constant.
The drift of opinion to-day is to regard pain in the spinal region as not pathognomonic of organic spinal affections. It is true that pain is a frequent concomitant of neuroses, and that it is more intense and characteristic in vertebral and meningeal disease; but in denying a significance to pain in the back as an evidence of diffuse disease of the cord itself, I think many modern observers have gone to an extreme. It is particularly in diffuse sclerosis that a dull heavy sensation is experienced in the lumbo-sacral region; and in a number of my cases of slowly ascending myelitis and of tabes dorsalis the involvement of the arms was accompanied by an extension of the same pain, in one case associated with intolerable itching, to the interscapular region. It cannot be maintained that the pain corresponds in situation to the sclerotic area. It is probably, like the pain in the extremities, a symptom of irradiation, and corresponds in distribution to that of the spinal rami of the nerves arising in the affected level.
As the posterior columns are usually involved in transverse myelitis, the same lancinating and terebrating pains may occur as in tabes dorsalis. As a rule, they are not as severe, and a dull, heavy feeling, comparable to a tired or a burning sensation, is more common. A belt sensation, like that of tabes, and as in tabes corresponding to the altitude of the lesion, is a much more constant symptom than acute pains.
Cutaneous sensibility is not usually impaired to anything like the extent found in advanced tabes. It is marked in proportion to the severity of the motor paralysis; where mobility is greatly impaired, profound anæsthesia and paræsthesia will be found; where it is not much disturbed, subjective numbness, slight hyperæsthesia, or tingling and formication may be the only symptoms indicating sensory disturbance; and there are cases where even these may be wanting.
The visceral functions are not usually disturbed. In intense transverse sclerosis of the upper dorsal region I observed gastric crises, and in a second, whose lesion is of slight intensity, but probably diffused over a considerable length of the cerebro-spinal axis, there is at present pathological glycosuria. The bladder commonly shows slight impairment of expulsive as well as retaining power, the patients micturating frequently and passing the last drops of urine with difficulty. Constipation is the rule. The sexual powers are usually diminished, though rarely abolished. As with sclerotic processes generally, the sexual functions of the female, both menstrual and reproductive, are rarely disturbed.
It is not necessary to recapitulate here the symptoms which mark diffuse sclerosis at different altitudes of the cord. With this modification, that they are less intense, not apt to be associated with much atrophic degeneration, nor, as a rule, quite as abruptly demarcated in regional distribution, what was said for acute myelitis may be transferred to this form of chronic myelitis. The progress of diffuse sclerosis is slow, its development insidious, and the history of the case may extend over as long a period as that of diffuse sclerosis. Sooner or later, higher levels of the cord are involved in those cases where the primary focus was low down. [p. 890] In this way the course of the disease may appear very rapid at one time, to become almost stationary at others. Of three deaths which occurred from the disease in my experience, one, in which there were distinct signs of involvement of the oblongata,151 occurred from sudden paralysis of respiration; a second from a cardiac complication, which, in view of some recent revelations concerning the influence of the tabic process on the organic condition of the valves of the heart, I should be inclined to regard as not unconnected with the sclerosis; and in a third, from bed-sores of the ordinary surgical variety. The malignant bed-sore is not of frequent occurrence in this disease.
151 On one occasion the patient had momentary anarthria, followed a day later by two successive periods of anarthria, lasting respectively about twenty seconds and one minute, one of which was accompanied by diplopia of equally brief duration.
PROGNOSIS.—The disease may, as in the instances cited, lead to a fatal termination, directly or indirectly, in from three to twenty years. The average duration of life is from six to fifteen years, being greater in cases where the sclerotic process is of slight intensity, even though it be of considerable extent, than where it is of maximum or destructive severity in one area, albeit limited. I am able to say, as in the case of tabes dorsalis, that a fair number of patients suffering from this disease whom I have observed for from two to six years have not made any material progress in an unfavorable sense in that time. One cure152 occurred in this series, of a patient manifesting extreme contractures, atrophies, bladder trouble, and ataxiform paresis, where the cause was plainly syphilis, and the histological character of the lesion is somewhat a matter of conjecture in consequence. Diffuse sclerosis of non-syphilitic origin—and this may apply also to established sclerosis in syphilitic subjects—is probably as unamenable to remedial treatment as any other sclerotic affection.
152 The patient went, under direction of Leonard Weber and R. H. Saunders, to Aix-la-Chapelle, where this happy result was obtained after mixed treatment had practically failed.
The same rules of DIAGNOSIS applicable to transverse myelitis of acute onset apply, level for level, to the diagnosis of transverse myelitis of insidious development, the history of the case often furnishing the only distinguishing point between the acute and the chronic form.
The main difference between the diffuse sclerosis and acute myelitis, clinically considered, consists in the gradual development of symptoms in the former as contrasted with their rapid development in the latter disease. Acute myelitis is established within a few hours, days, or at most, in the subacute forms, a few weeks; chronic myelitis requires months and years to become a clearly-manifested disorder. It is the essential correspondence of the symptoms of both conditions, intrinsically considered, which renders it impossible to distinguish clinically and in the absence of a history of the case between some cases of acute myelitis in the secondary period and the processes which are primarily of a sclerotic character.
It is unusual to find the degeneration reaction in myelitis of slow and gradual development. Sometimes there is diminished reaction to both the faradic and galvanic currents, or the so-called middle form of degeneration reaction is obtained from atrophied muscles, the nerve presenting normal or nearly normal irritability, and the muscle increased galvanic irritability and inversion of the formula.
[p. 891]Among the less reliable or accessible points of differentiation between the residua of acute myelitis and the chronic form is the history of the onset and the age of the patient at the time of the onset. Myelitis in young subjects is more likely to be of the acute kind; in older persons it is more apt to be chronic.
In the diagnosis of diffuse sclerosis the question of differentiation from neuroses not based on ascertainable structural disease, such as are called functional, will be most frequently raised. In differentiating between organic and functional spinal disorders all known exact signs of organic disease must be excluded before the case can be considered as appertaining to the latter group. Symptoms of hysteria, nervous exhaustion, and spinal irritation frequently coexist with diffuse sclerosis as well as with the disseminated form; and this is not surprising, for, instead, as seemed at one time to be believed, of the neurotic taint granting comparative immunity against organic disease, it is the reverse, and it is not at all uncommon to find a strongly-marked neurotic diathesis in the family history of sufferers from diffuse sclerosis. That ordinary hysteria, epilepsy, and what is vaguely called nervousness are common features in the ancestral record of the hereditary forms of spinal disease has already been stated in considering those affections.
One of the commoner forms of the grave phase of hysteria is paraplegia.153 Often muscular atrophy—which ensues from disuse—exaggeration of the deep reflexes, and retention of urine are added to the paraplegia and heighten the resemblance to an organic affection. Its development, though sometimes sudden, often occupies weeks or months, and may be preceded, exactly as in chronic myelitis, by weakness in the legs, and not infrequently by combined ataxia and weakness. It is much more difficult to discriminate here than is generally held or than is enunciated in textbooks. The sufferer from hysterical paraplegia does not always give other indications of the hysterical neurosis, and even if she did show a globus and tenderness at certain points, it is a question whether it could be called a scientific diagnosis which determined the case to be one of functional trouble on these signs alone. More than one error has been committed in this respect. In chronic myelitis retention of urine is less common than incontinence, which is the reverse of hysterical paraplegia. Pupillary symptoms do not occur with the latter affection. If there be sensory anæsthesias, they are bizarre in character or distribution, and do not usually harmonize with the distribution of the paralysis. In most cases moral influences can be exerted so as to increase the power of movement far beyond what would be possible in an organic disease; and while an electrical examination will not always yield positive results in chronic myelitis, yet no case of chronic myelitis with complete or nearly complete paraplegia but will show at least quantitative changes of such extent as to prove beyond doubt that the case is of an organic character.
153 I have observed for two years a stationary brachial diplegia, of undoubted hysterical origin, although the patient had never shown any ordinary hysterical manifestations, and had had no other hysterical symptom than chromatopsia, and that only for a short period. From its long duration, constancy, and the resulting atrophy of disuse it had been regarded as a case of peculiarly limited chronic myelitis.
There is one point in which spinal and cerebral disease involving the motor tract differs in the majority of cases, which may be utilized in [p. 892] distinguishing obscure affections of the former from those of the latter kind. In cerebral paralysis of any standing the superficial reflexes, such as the cremaster and abdominal reflexes, are usually diminished or abolished, while the deep or tendon reflexes are exaggerated. In spastic conditions due to spinal disease—say sclerosis of any kind affecting the lateral column and leaving the motor nuclei of the anterior cornua unaffected—the deep reflexes are similarly increased, but the cremaster reflex is increased also.154 This feature of the superficial reflexes is significant in the case of cerebral disease only when unilateral.
154 Attention has been called, I believe, by Westphal, to the fact that the cremaster reflex may not be demonstrable when reflex excitability is at its highest, because the cremaster muscle is already in extreme spastic contraction.
The initial period of diffuse sclerosis is sometimes confounded with rheumatism—an error less pardonable than in the case of tabes, inasmuch as in diffuse sclerosis the pains are not usually premonitory, but associated with motor paresis. It is erroneous to regard a pain as rheumatic because it is aggravated or relieved by changes in the weather. There are many subjects of myelitis who regard themselves as veritable barometers, and with more justice than most rheumatic patients.
In some cases of chronic alcoholism there are motor weakness and a gait much like that of diffuse sclerosis.155 It is to be remembered that the solar tickling reflex is very often abolished in alcoholic subjects, and profound diminution of the normal cutaneous sensibility of the leg and feet usually coexist. But unless there is peripheral neuritis—which is an exceptional and, when present, well-marked affection—the absence of profound nutritive changes of the muscle, the presence of the alcoholic tremor, the absence of sphincter and bladder trouble, and the great variation of the symptoms from week to week, and even from day to day, serve to distinguish the alcoholic spinal neurosis from myelitis.
155 Wilks' alcoholic paraplegia.
In studying the lesions underlying the symptoms of organic spinal disease, the occurrence of fascicular scleroses, secondary to such disease and due to the destructive involvement of nerve-tracts, was repeatedly noted. Türck may be regarded as the discoverer of these degenerations, and the reliability of this old observer may be inferred from the fact that one bundle of fibres liable to individual degeneration still goes by his name, and that, as far as he was able to discriminate between the various paths which secondary degenerations follow through the cerebro-spinal fibre-labyrinth, his statements have not been materially modified by more recent investigators, such as Bouchard, Vulpian, and Westphal.
The discovery by Meynert that the great cerebro-spinal tracts attain the white color which they owe to the development of myelin around their component axis-cylinders with advancing maturity, and that the tracts of noblest, and therefore most intelligent, function were the last to show this sign of maturity, was greatly extended by Flechsig, who found that each tract receives its myelin at a definite period of intra-uterine life, the lowest or the nerve-roots first; then the short or intersegmental or—as [p. 893] the physiologist may call them—the automatic tracts; then the long or controlling tracts; and last, the associating tracts of the cerebral hemispheres which mediate the complex relations underlying mental action. It was this discovery which gave a new impulse to the study of the secondary affections of the cord and brain. The accuracy with which secondary degeneration follows the lines marked out by the normal course of the tract is as great, diminishing when the tract diminishes, changing its position or direction and decussating where the latter changes its direction or position or decussates, that it constitutes not alone an interesting subject for pathological study, but has become one of the most reliable guides of the cerebral anatomist. It is of great importance to the pathologist to be able to differentiate between the primary disease and its secondary results, and, as the controversy concerning the so-called system diseases shows, even the most studious observers are uncertain in this direction in many cases.
MORBID ANATOMY.—Secondary degeneration manifests itself by a discoloration of the affected nerve-tract, which accurately corresponds in area to the normal area of that tract. The more recent the degeneration the less pronounced is this change. In advanced cases the color may be a dark gray, in moderately old ones a reddish or yellowish gray, and in those of very recent origin no change may be visible to the naked eye. It is claimed, however, that even here a loss of translucency of the white substance, giving it a sort of cheese-like opacity, may be detected. On hardening the specimen containing the degenerated tract in Müller's fluid or a simple bichromate salt solution, the affected area, instead of appearing dark on section in contrast with the gray substance—which in such preparations appears yellowish or a light brown—contrasts with the former by its lighter tinge. This contrast is observable even in cases where the naked eye was unable to detect the change in the fresh specimen. It can be sometimes found as early as the tenth day after the primary lesion, and is apparently simultaneously developed in the whole length of the nerve-tract affected.
The minute changes characterizing secondary degeneration begin in the essential conducting elements, the axis-cylinder, which exhibits a finely granular or molecular disintegration, and disappear. According to Homén, it shows an initial swelling and a failure to stain properly before this. The myelin then follows suit: it becomes fragile, forms variously-shaped globules, and also disappears, and together with this a nuclear proliferation is noticed in the interstitial substance; fatty granule-cells are observed in large numbers, and manifest a tendency to accumulate in the perivascular districts. These cells are not permanent; their gradual diminution is accompanied by a proliferation of the interstitial tissue, which ultimately appears as a pure connective substance composed of fine fibrillæ arranged in undulating bundles. The entire process may be not inaptly compared to an hypertrophy of the interstitial substance resulting from overfeeding of its cellular elements by the morbid pabulum furnished through the disintegration of the nervous substance proper.
The disappearance of the nerve-tubes, and the formation of a new tissue in their place, which, like all tissues of the same character, undergoes shrinkage, leads to considerable deformity in the shape of the part which is the site of secondary degeneration. This is seen in the [p. 894] accompanying figure, where in an old-standing secondary degeneration of one interolivary layer the corresponding half of the medulla is greatly reduced in diameter as compared with the other side (Fig. 34), and the entire raphé is distorted. When one side of the cord is the site of such a change a similar asymmetry results.
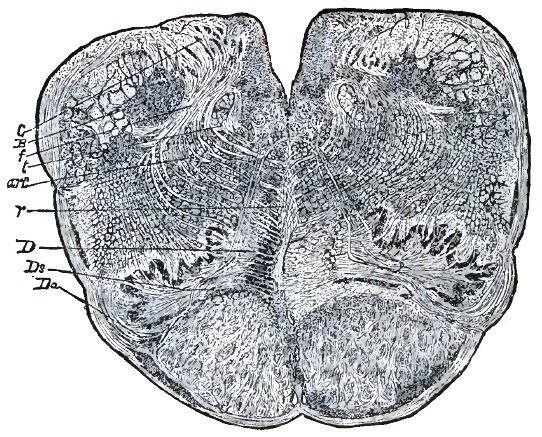
According as the original lesion is incompletely or completely destructive, a larger or fewer number of axis-cylinders may be found preserved in the sclerotic tissue. It is not yet determined whether in some instances these fibres may not represent an admixture from another source than are comprised in the mainly affected tract.
Secondary degenerations are classified as ascending and descending. An ascending degeneration is one which is found situated brainward of the primary lesion; a descending one is found caudad of the lesion. It was once maintained that the direction of the secondary degeneration was constant for each individual tract. This seems to be true for a few. Some tracts, particularly in the brain, degenerate on both sides of the lesion, as I showed with regard to the interolivary layer.
The best studied form of secondary degeneration is that of the voluntary motor conduit known as the pyramid tract. Beginning in the so-called motor area of each cerebral hemisphere, the Rolandic loop passes into the anterior part of the posterior half of the internal capsule, to be thence continued through the crus, pons, and the pyramids of the oblongata to the decussation or crossing-point of the pyramids. Here the greater part of the tract crosses into the opposite lateral column, occupying the position described in the section on Spastic Paralysis. A smaller part remains on the same side of the continuous interpyramidal and ventro-spinal fissure, constituting the direct fasciculus of Türck.
The crossed-pyramid tract diminishes as it passes caudad in the cord, giving off its fibres to the lateral reticular processes of the cord, [p. 895] whence—whether interrupted by cells (Von Monakow) or not—they probably reach the great cells in the gray substance from which the anterior rootlets spring. The direct fasciculus probably terminates in a similar way, and perhaps makes good, as it were, its failure to participate in the gross decussation at the level of the foramen magnum by decussating in detail along its entire length. It is usually exhausted before the lumbar cord is reached, whereas the crossed tract in the lateral column continues down as low as the origin of the sacral nerves. A destructive lesion anywhere in the course of the pyramid tract, whether it be in the motor area of the cortex, in the loop of Rolando, in the internal capsule, the pons, or the cord itself, will provoke descending degeneration; that is, sclerosis of so much of the tract as lies below the lesion. Thus such degeneration is found with porencephalic defect of the motor area. I found it in a paretic dement who had extensive cortical destruction following a submeningeal hemorrhage. It has been observed after focal lesion of the pons (Homén, Schrader), and after transverse lesions of the cord, either myelitic, traumatic, or as the result of compression by vertebral disease. As a rule, the cells in the anterior horn are not involved, and some observers question whether this ever occurs. I have never found such involvement, although in its gross dimensions the anterior horn as a whole appears atrophied. This atrophy I have been able to account for satisfactorily by the disappearance of many of the fibres which run into the gray substance from the reticular processes.
While the distribution of degeneration in the cord is rather uniform, varying only in harmony with the ascertained individual variations in the relative preponderance of the crossed and uncrossed parts of the pyramid tract, there is much more variation in the cerebral distribution of the degeneration according to the extent of the original lesion. Thus, if the entire capsule be destroyed, the greater part of the crus is involved. If only the posterior division in its anterior part be destroyed, the degeneration is in the crus, limited to that part which runs a subpial course on the crural demi-cylinder, occupying from a fifth to a third of its surface-area. Still more limited degenerations are described, but as yet are too few in number to base other than tentative conclusions on them. Among these is one occupying a thin strip on the inner side of the crus, which degenerates after lesions near the genu of the capsule, and probably represents the tract which governs the cranial nerve-nuclei. An excellent observation by Von Mannkopf shows that the course of the motor fasciculus is subject to some individual variation even within the capsule.
A number of forms of secondary degeneration are described, involving intracerebral tracts, such as those connecting the cerebrum and cerebellum. The degeneration of the visual tract, from the optic nerve to the occipital lobe, observed by Richter and Von Monakow, with some conflict of opinion between these observers, is often as perfectly demonstrative of the course of the optic fasciculi as degeneration of the pyramid tract is demonstrative of the course of the voluntary innervation of the muscles moving the limbs.
The secondary degenerations following lesion of the pons varolii are acquiring special interest in view of their relation to special nerve-tracts of the spinal cord of hitherto unknown function. The purest instance [p. 896] of an isolated degeneration of other than the pyramid tract is the case illustrated in the accompanying diagrams. It involved the interolivary layer, was both ascending and descending, being traced above into the subthalamic region, and below decussating into the opposite side of the oblongata, to terminate in the nuclei of the columns of Burdach and Goll. The leading symptom manifested by the patient was a hemiplegia of the muscular sense.156
156 Besides my case, others have been recorded by Homén, Meyer (Strassburg), and Schrader, which are impure. In the former and latter degeneration of the pyramid tract, in the second degeneration of the olivary fasciculus, coexisted. It is not generally known that Westphal, in one of the first volumes of the Archives now edited by him, found an ascending degeneration of the same tract for a short distance.
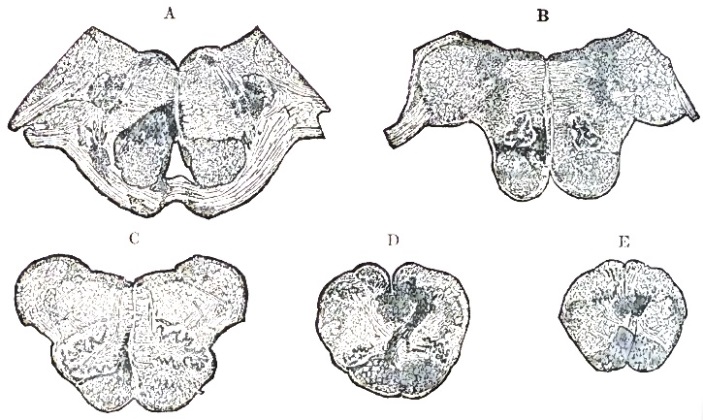
Ascending degeneration is found in a very distinct form after compression of the cauda equina. It is limited to the posterior columns, occupying nearly the entire area of the latter in the lumbar cord, particularly the triangular field of Burdach's column mentioned in the article on Tabes. In the dorsal and cervical cord it is limited to the columns of Goll, and terminates in the clava of the oblongata at the nuclei of those columns.
Higher lesions produce the same ascending degeneration of the column of Goll, and in addition involve other, probably centripetal, tracts which happen to be injured at their origin or in their course. For example, a transverse lesion of the dorsal cord would produce ascending degeneration for its whole length of the column of Goll and of the direct cerebellar tract. In addition, it would, in obedience to the law previously stated, produce descending degeneration of the pyramid tract. This combination is almost a typical sequence of compression myelitis of the cord, as [p. 897] well as of ordinary transverse sclerosis. Recently, Gowers157 has described a secondary degeneration in such a case of transverse lesion not previously noticed. It is found in cases showing gross disturbance of cutaneous sensibility, and occupies a narrow belt encircling the anterior quarter of the circumference of the crossed-pyramid tract. It is continuous, in my opinion, with a tract which in the upper cervical cord is situated in a corresponding situation, and which degenerated a short distance caudad in a case of secondary degeneration of the olivary fasciculus described by Meyer, and in which similar sensory symptoms were noted.
157 Diseases of the Spinal Cord, and Neurologisches Centralblatt, 1886.
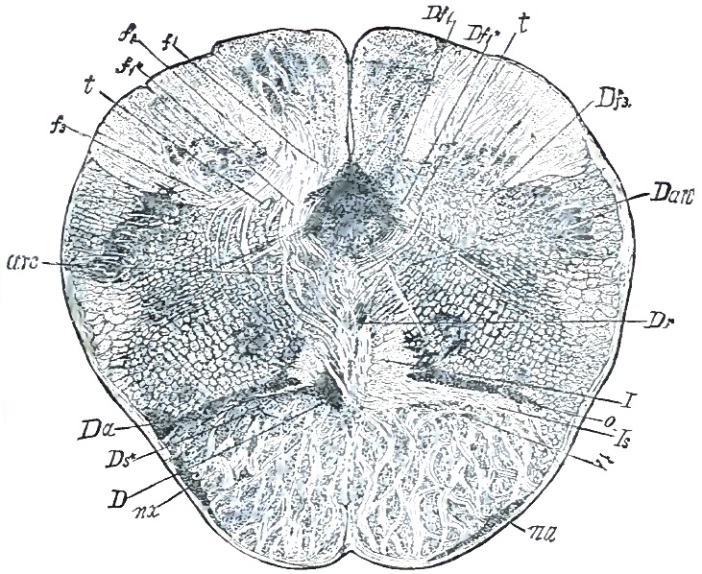
CLINICAL HISTORY.—Secondary degenerations are passive results of other more active processes, and few clinical signs are attributable to them. The most important of these is the contracture which is found in old hemiplegias, and attributed, like the secondary exaggeration of deep reflexes in such, to the descending degeneration of the pyramid tract. Bouchard believed that it was the retraction of the sclerotic strand which acted as an irritant on the neighboring fibres. The development of spastic symptoms in amyotrophic lateral sclerosis and in focal lesions of the crossed-pyramid tract is in favor of this view. On the other hand, the occurrence of flaccid hemiplegia, and its conservation for years after the most extensive lesions, is against it, as it is in these very cases that the secondary degeneration is most intense. That the retraction of a [p. 898] longitudinal strand exercises any serious effect on neighboring and parallel fasciculi is questionable, as the process is slow. There is, however, one situation where such influence is very likely to occur—the decussations of the oblongata. In the case already referred to, the retracting sclerosing bundles undoubtedly must have exercised a damaging effect on their fellows of the opposite side, which, interdigitating with them, were compelled to pass through the sclerosing tissue. It has occurred to me that the slight sclerosis which is sometimes observed in the crossed-pyramid tract of the same side of a cerebral lesion, even where that lesion is strictly unilateral, is due to a similar influence. I think it can be shown that such sclerosis cannot be traced to the primary lesion; it begins at the decussation, and it is more than probable that the firm constriction to which the healthy fibres are subjected in crossing through their shrinking fellows of the opposite side is not alone the cause of the symmetrical yet slighter lesion, but also accounts for the observation by Pitrés and Charcot of a slight motor weakness observed on the same side as the hemiplegia, producing lesion in ordinary cases of capsular hemorrhage.158
158 Some of the French observers claim that this occurs only in the early period, but a careful study of the matter by R. Friedländer shows that the weakness of the side not usually regarded as involved is found in the later periods, and well marked then (Neurologisches Centralblatt, June 1, 1886).
The PROGNOSIS and TREATMENT of secondary degenerations are practically involved in the primary lesion which gave rise to them. The contractures attributed to secondary sclerosis of the motor tracts is to be treated on the principles mentioned in the following section.
As the histological character of the different forms of sclerosis is similar—at least in the terminal period—the causes producing them identical even in name, and the indications furnished by leading symptoms analogous if not identical, the treatment of these various disorders is naturally based on the same leading principles. There are two objects to be aimed at in dealing with these chronic disorders: The first is the cure or arrest of the morbid process itself; the second is the amelioration of distressing and disabling symptoms.
It is generally recognized that a perfect cure of a sclerosis is a consummation never to be realized by any plan of treatment now at our disposal. The experiments of Kahler and others have shown that spinal tissue, once destroyed, is not regenerated. The post-mortem examination of cases of tabes which were considered as cured during life (Schultze) has shown that the sclerosis had not been removed; the process had merely become quiescent, and the apparent recovery had been due to the vicarization of other nerve-elements than those destroyed for the latter.
But if attempts at the regeneration of destroyed fibres and cells are to be regarded as futile, the arrest of the destructive process is to be considered as an object which offers better chances of realization, and which is worth attempting for other than merely conservative reasons. In a number of the forms of sclerosis described, notably in tabes and the disseminated form, it is remarked that the axis-cylinders lying within the [p. 899] morbid district are in part intact and in part but slightly affected. Here and there groups of nerve-tubes may be found which retain even their myelin. While subject to the vicissitudes inseparable from their position in the midst of active pathological changes, these channels of nerve-force, though anatomically patent, may have their function perverted or destroyed, just as a nerve outside of the cord may be paralyzed by pressure or anæmia though its structure be intact. Should the active phase of the sclerotic process be arrested, these intact or nearly intact fibres will resume their function, and thus an apparent improvement will be effected. The spontaneous ameliorations in the course of tabes dorsalis and the less marked ones of diffuse sclerosis, coupled with temporarily improved sensation in the former and improved motion in the latter disease, show that retrogressions of this character are possible and do occur. How is the physician to imitate the action of nature? how to intensify it so as to secure the permanent improvement which nature unaided does not grant? The first factor to be considered is the removal of the cause of the disease. A number of cases are due to exposure to wet and cold and to over-exertion. Such exposure and over-exertion, if not already rendered impossible by the disease, is to be discontinued. A large number of cases of tabes—according to many authors, a majority—a considerable number of cases of diffuse sclerosis, and not a few of other forms, are connected with the syphilitic dyscrasia. Here, at the very outset, we have a definite indication for treatment, and while we may be disappointed in the results of such treatment in a large proportion of cases, yet enough of well-assured and substantial success has been and is obtained to render it almost a matter of duty for the physician to try antisyphilitic measures in every such instance.
The mixed treatment in chronic spinal disorders should be followed out for long periods and faithfully. Most tabic and other sclerotic subjects affected with constitutional syphilis are in what is called the tertiary period of that disease, when iodide of potassium is less useful than mercury. I have never gained anything by pushing either drug to the extreme point in advanced cases, and it should be borne in mind that mercurialization carried too far may itself prove directly injurious to the nerve-centres.159 In cases where gastric crises, gross ataxia, muscular atrophy, and bladder disturbance have been of long duration this treatment is rarely successful.160 But in the initial and early periods of tabes and in diffuse sclerosis of slight intensity the effect is sometimes gratifying, and of such a nature that it cannot be attributed to a coincidence with spontaneous remissions of the disease. In one case both knee-jerks and the pupillary reflexes returned, to disappear on premature discontinuance of the treatment; and on resumption one knee-jerk again returned, and has remained demonstrable now over half a year. In a second case the fulminating pains and the bladder disturbance disappeared, a slight indication of the pupillary reflex developed, and the patient has remained stationary with this gain for a period of three [p. 900] years.161 In a third case, one of established ataxia, with which luetic osseous lesions occurred, the pupillary reflex has returned twice, disappearing after the first reappearance. In one case of combined sclerosis in which no syphilitic antecedents could be found the paresis of the arms has disappeared, and the ataxic paresis of the lower extremities has improved to such an extent that the patient can stand with his eyes closed and his feet together, and on one leg with the eyes open—feats which a year ago he was unable to perform. None of the changes in symptoms taking place in these cases occur spontaneously in sclerotic spinal disorders, and they must be attributed to the treatment. Such treatment is best carried out in conjunction with warm bathing. The Hot Springs of Arkansas, those at Las Vegas, New Mexico, and the baths of Aix-la-Chapelle in Europe enjoy a special reputation in this field. The springs of Arkansas, as regards the intrinsic character of the water, possess advantages which are probably not excelled by any European baths, but the therapeutical management162 is far from that ideal point of development attained, for example, at Aix-la-Chapelle.
159 Mendel thus found in his experiments made on dogs, developing cerebral disease from rotation with the head directed toward the axis of rotation, that dogs who had previously received subcutaneous injections of corrosive sublimate showed an increased vulnerability to the action of the rotary apparatus.
160 A remarkable exception is related in the section on Chronic Myelitis.
161 There was concentric limitation of all color-fields, and only central perception of green; to-day, if anything, the color-fields of this patient are a little greater than in the physiological average. The case was undoubtedly one of initial tabes.
162 Mercurial ointment is used by the hundredweight, to quote the expression of a patient, and in certain establishments the sufferers from the common taint plaster each other from head to foot, as with mud, with this panacea for most of those ills which flock to the springs. Still, there seems to be no doubt that enormous quantities of mercury are borne well by those who use the baths, and who under other circumstances are susceptible to its most undesirable effects.
Optic-nerve atrophy, according to the best authorities, constitutes a contraindication to the use of mercury in any form. It may be laid down as a general rule that the more rapidly the symptoms indicating a sclerotic process are developed, and the more recent its advent, the more energetically should the treatment be pushed. Mercurial inunctions and the so-called heroic doses of iodide are to be employed. But in cases progressing slowly and of long antecedent history what may be called a dilute plan is more apt to yield good results. Small doses of mercury,163 given steadily for years, and iodide of potassium, administered in well-tolerated doses for periods of ten days, alternating with corresponding periods of intermission, have, in my opinion, delayed or arrested the progress of tabes and other forms of sclerosis for the long periods referred to in the preceding sections.164 Although the antisyphilitic measures adopted in sclerosis of syphilitic origin are the most important, and the prognosis of no such case can be regarded as hopeless as to recovery or duration until they have been tried, other procedures, detailed under the head of Peripheral Treatment, should not be neglected. While some very severe cases improve rapidly on antisyphilitic treatment, other much less severe and more recent cases, in which the same cause is assigned with equal reason, are not affected by it in the slightest visible degree. The reason for this difference is unknown, but it necessitates the bearing in mind that by [p. 901] limiting the treatment to the etiological indication valuable time may be wasted in which the symptomatic indications could be profitably followed.
163 The tablet triturates of biniodide of mercury or corrosive sublimate furnished by Fraser & Co. of New York I have found peculiarly useful; one one-hundredth or more of a grain may be thus administered every two to four hours.
164 I am now employing the same treatment in some cases showing no syphilitic history. If any medicinal measures can act upon connective-tissue proliferation, it is these very ones.
In cases of sclerosis due to other causes than syphilis a number of medicinal agents have been recommended as calculated to affect the central disease directly. Ergot is recommended in sclerotic troubles, particularly tabes, by a large number of writers. It is admitted that this substance can produce tabes itself, so that its administration in the large doses recommended by some is not without its possible dangers. I have seen a patient well advanced in the disease who had received the drug for three weeks consecutively in such quantities165 that on estimates made I came to the conclusion that he had received more than some of the persons in whom Tuczek discovered the development of ergotin tabes. Favorable results are reported ensuing after its use in the early stages, particularly where signs of irritation preponderated, such as lightning-like pains, hyperæsthesia, and frequent erections; and it has been suggested that the beneficial action is due to an effect on the blood-vessels, which are supposed to be congested in the beginning of the disease. Proof of such congestion has not been furnished: the vessels are usually sclerosed and their lumen narrowed. In view of the undeniable danger which attends the administration of ergot in tabes, it may be properly insisted that its indications be more precisely formulated than has yet been done. It is commonly noticed in the natural progress of tabes that the lightning-like pains disappear, usually about the time the anæsthesia becomes greater. The anatomical parallel is supposed to be the destruction of the nerve-tubes whose previous irritation caused these pains. If, as is claimed—and it seems to be substantiated—ergotin does produce amelioration of the lightning-like pains, it would prove a damaging revelation which showed that it did so in imitation of the natural process; that is, by increasing the sclerosis.
165 An expert ophthalmoscopist found that the retinal vessels, which were somewhat dilated in this patient, were not influenced by the treatment.
The first drug to which an influence was assigned upon the sclerotic processes, and which has maintained its reputation longest, is nitrate of silver.166 Its claim to being regarded as a remedy may be best characterized by the fact that an author who is far from being prejudiced against it, and who recognizes the claims of Wunderlich, its advocate, speaks of it as a valuable placebo.167 I have never obtained any effects from this drug in the scleroses, or from the chloride of gold, which has been also recommended for these affections, nor have I seen any in cases where either or both had been faithfully tried by others for years. The same is to be said of the chloride of barium, which has been warmly extolled on the basis of a very limited trial in disseminated and diffuse sclerosis.
166 One of the first patients on whom Wunderlich tried this drug died while I studied at Leipzig. He had extensive argyria and sclerosis of the posterior columns.
167 Leyden, op. cit., vol. ii. p. 359.
The direct application of the galvanic current to the spine is recommended, more particularly by Erb and Neftel.168 I am unable to state [p. 902] anything regarding currents derived from as many as twenty of Siemens cells and applied in the ascending direction, as the latter recommends beyond an experience which occurred in the practice of a colleague, who, alarmed by the event to be related, referred the patient subjected to this treatment to me. The patient suffered from tabes dorsalis, the symptoms being limited to the lower extremities, the ulnar distribution, and the pupils. The belt was in the lower thoracic region; the ataxia and lightning-like pains were not great. After a single application of an ascending current from twenty-two cells, continued for ten minutes, the patient suddenly felt a severe dull pain in the occiput and terrible lancinating pains in the distribution of the occipital nerves. With this there occurred scintillation before the eyes, and at the subsequent examination I found that the belt sensation had moved into the neck. The coincidence was so close, and sudden changes in the distributional area of tabic symptoms are otherwise so uncommon, that I attributed the observed change to the treatment.
168 In describing a case in which this measure not only ameliorated lancinating pains and vesical symptoms, but also, applied to the head, relieved the diplopia—usually a spontaneous occurrence, according to both American and European writers—this writer takes occasion to state that in the year 1869 tabes dorsalis was practically unknown to American physicians (Archiv für Psychiatrie, xii. p. 619). Duchenne described progressive locomotor ataxia in that and the preceding year; the necessity of referring to the unfamiliarity of American physicians with a disease not at the time recognized on either side of the Atlantic is hence not apparent. Leyden (op. cit., vol. ii. p. 325) candidly admits that the German medical profession was at first averse to recognizing Duchenne's limitation: this reproach cannot be laid at the door of American physicians, as I can distinctly recollect the demonstration of several well-marked cases exhibiting the characteristic symptoms then known, in the year 1870. The disease obtained recognition in American textbooks and journals as early as in those of any other land.
Erb does not recommend such powerful applications. But the most sanguine electro-therapeutist must admit that the action of galvanic currents on the spinal cord is an exceedingly uncertain one. It is questionable whether weak ones deflect sufficient current-loops to reach the cord and to exert any material effect. As to currents powerful enough to produce an effect, it is not known, except in the loosest and most empirical way, what that effect is. The procedure followed by Erb is to use large electrodes, the cathodal one being a little smaller than the anodal, the former being placed stabile, over the upper cervical sympathetic ganglion of one side, the latter labile, on the opposite side of the vertebral spines, moving gradually downward, the session not exceeding three minutes. This is repeated daily or every alternate day.169 It would prove a strong proof that this treatment really affected the morbid process in a remedial direction if any of the exact signs of the disease were to be modified by it, be it ever so slightly. If, after galvanization of the cervical cord and the sympathetic nerve, the initial myosis of tabes were temporarily lessened or the reflex contraction to light restored for ever so short a time, a brighter future would dawn for electro-therapeutics than seems now to be in store for it.170
169 Why, if the procedure be really remedial or efficiently palliative and devoid of evil consequences, it is not recommended to be repeated oftener I am at a loss to explain or understand. There are some factors involved in practical electro-therapeutic which it is scarcely possible to discuss without encroaching on delicate ground.
170 In healthy persons the extent of the knee-jerk is increased by the spinal ascending galvanic current, and possibly this observation may lead to the establishment of a rational basis for its use in cases where the reflex is abolished or diminished.
Peripheral Treatment.—A number of therapeutical applications are made to the periphery where the symptoms of the sclerotic process are localized. The rationale of such applications is based on the assumption that peripheral conditions are capable of modifying the nutrition and functions of the cord. This is proven not alone by a host of observations made [p. 903] on the normal cord, but is also disastrously illustrated in the part played by surface chilling in the etiology of many acute and chronic diseases of the cord. Notwithstanding this latter, a large and influential body of German neurologists recommend cold baths and cold spinal douches in these affections. I have seen such excellent results from the use of warm baths that I am compelled to plead, in defence of my ignorance of the effect of cold ones, that I have never dared to use them. In numerous cases the beneficial effect of a warm bath is almost instantaneous. Warmth in any shape, whether atmospheric or in the shape of baths, is usually agreeable to patients suffering from the various forms of sclerosis. Cold, on the other hand, is disagreeable, aggravates the symptoms, and in many cases at least hastens the progress of the disease. A winter spent in the latitude of New York or Boston means so much ground lost by the patient, and a sojourn during the colder months in Southern California, New Mexico, Florida, or the West Indies enables the patient to avoid this loss. As regards the choice of climate and baths for sclerotic patients, I should be inclined to roughly formulate the indications as being identical with those of chronic rheumatism. The reaction against the use of warm baths in Germany, where they once were popular,171 is due to the employment of too high temperatures. Hot baths, in the strict sense of the term, including the various forms of vapor-bath, act badly. They increase instead of calming the irritative symptoms, as moderately warm baths do, and they entail too sudden a change in the bodily state. That, for the present, it is advisable not to adopt unreservedly either the extreme plan once in vogue or the equally extreme one which constitutes the reaction against it, is shown by the observations of Richter of Dalldorf, who records some discouraging results obtained by the use of cold baths in cases of tabes dorsalis. It is but necessary to refer to the fact that the lancinating pains of the latter disease, the rigidity of diffuse myelitis, and the spasms of lateral sclerosis are usually most severe in cold weather, and that the diseases mentioned appear to be rare in warm countries, to show the need of caution in using a therapeutical measure so similar in its action, even if it be but momentary and followed by a reaction, to those which provoke or aggravate the original disease. Eulenburg has seen five recoveries in tabes, and under such different plans of treatment that the latter is not credited by him with the good result. Three were treated with warm baths, one with cold baths, and one with nitrate of silver. It is seen here that the warm baths were used with good results more frequently than the cold.
171 The mud-baths of Cudowa in Gallicia had a very high reputation.
One of the most singular delusions of modern therapeusis—nerve-stretching—has, following the prediction made by several on both sides of the Atlantic, become obsolete. Introduced by Langenbuch, a surgeon, and attacking the disease at the sciatic nerve—a point where, as well-versed students knew, it was not located—the operation was looked upon with distrust from the beginning. The enthusiasm with which it was taken up by surgeons and by the interested portion of the laity—ever hopeful as tabic patients are of new drugs and methods of treatment—has led to a large number of trials, now numbering several hundred, and from which the useful lesson can be gathered that the good ripens slowly. Nerve-stretching in an organic disease of the spinal cord may take its [p. 904] place among the needless vivisections; it has not influenced the progress of a single case in any essential feature. On the contrary, it has more than once been directly responsible for acute myelitis, spinal hemorrhage,172 and pyæmia. In a number of cases reported by Langenbuch,173 Benedict, Erlenmeyer, Schweminger, Debove, and W. J. Morton, the ataxia of the patient has been reported as relieved; in one case, exhibited by the latter operator before the American Neurological Association, this appeared quite evident, but not because the disease proper had been influenced, but for the same reason that prevents the development of marked ataxia in combined sclerosis. Just as the lateral-column lesion inhibits the ataxia which is due to the posterior-column lesion, so the motor paresis produced by stretching the sciatic nerves neutralizes the manifest features of the ataxic gait. As soon as the paresis is recovered from, the ataxia returns in its original form, unless, happily, one of the common spontaneous changes for the better occur. As a therapeutic procedure nerve-stretching is to-day properly limited to affections of the peripheral nerves.
172 Zacher, Archiv für Psychiatrie, xv. p. 430.
173 Westphal showed after the autopsy of Langenbuch's first successful case that there had been no spinal lesion whatever.
One of the most useful peripheral remedies in the sclerotic processes is the faradic wire brush. It is both an anodyne and remedial for anæsthesia. A number of the tabic patients to whom I referred as not having deteriorated within long periods are provided with a portable faradic battery, and apply the brush to the spots affected by terebrating pains the moment these commence, obtaining instantaneous relief. As has been shown by Rumpf,174 the cutaneous space-sense becomes more delicate in healthy and improved in tabic patients under its continued use. And while the inco-ordination of tabes is in part independent of the disturbance of cutaneous sensibility, yet if the latter can be refined the ataxic disturbance may be mitigated—a result occasionally obtained through the methodical use of the wire brush.
174 Report of a discussion, Neurologisches Centralblatt, 1885, p. 526.
It is frequently found that sufferers from tabes dorsalis and other forms of sclerosis accompanied by ataxia walk much better in their stocking feet and in slippers than they do in the conventional street shoe or boot. The reason for this is obvious. The patient's gait is impaired by the disease, and, whether the ataxia be a pure co-ordinatory trouble or no, subjective uncertainty regarding contact with the ground which is experienced by most ataxic patients is an aggravating factor. Our modern foot-clothing, with its inflexible soles and raised heels, handicaps the patient as it were, depriving him of the use of what little tactile sensibility may be left him.175 The use of low-heeled shoes with thin and flexible soles is therefore advantageous.
175 The question whether tabes dorsalis is a disease of civilization has not been raised in any treatise I am acquainted with. Myelitis, both acute and chronic, occurs, however, rarely in the lower animals, as do also central dilatation of the cord and congenital defects of the latter. Posterior sclerosis I can find no record of in veterinary pathology. The influence of the repression of normal aids to locomotion by the foot-gear of civilized life as a possible predisposing factor in the etiology of ataxic troubles is a legitimate subject of inquiry. The lateness of the infant of civilized parents in acquiring the art of skilled locomotion may be in part, as philosophers claim, a penalty of exuberant development of the higher and inhibitive centres. But what part has the artificial obliteration of solar sensibility and pedal flexibility played in this inherited feature? What is its influence in establishing a pathological vulnerability?[p. 905]
The tremors of sclerotic affections, particularly those accompanying the disseminated forms, are from their distressing character prominent objects of special treatment. The bromides have been given with alleged good effect which I am unable to confirm. Curare has caused the tremor to disappear for two days in one of Erlenmeyer's patients. I have seen good results from the descending galvanic current applied in long sittings to the head and neck, sliding in to the point of tolerance, and sliding out before discontinuing. The mydriatics, atropine, and particularly hyoscyamin, often remove tremor radically for the time being; unfortunately, it is necessary to give them in almost toxic doses to obtain this effect. Recently, Feris recommended veratrum in doses of half a milligram repeated every four to five hours. It acted very well in every case in which I tried it, but, as it became necessary to increase the dose, the same objection was encountered as in the case of hyoscyamin. All these measures should be used as emergency remedies only; they cannot, in the nature of the case, prove curative, while their continued use produces a physiological indifference to their effect, and to that extent decreases their value as the case progresses.
MANAGEMENT OF SPECIAL SYMPTOMS AND COMPLICATIONS.—Among the most distressing features of many sclerotic affections is pain, which is usually associated with sleeplessness. The fulminating variety may be often relieved by the use of the actual cautery applied over the affected level of the cord and along the course of the nerve involved. But in the majority of cases morphine will have to be resorted to. Erb cautions against the use of this anodyne in cases where there is much reflex irritability of the cord, as morphine is said to increase this irritability when administered in small doses, and to reduce it again only when larger ones are administered. It is the latter alone which are serviceable with pain, and I have not yet seen any bad effects in the direction apprehended by Erb from such doses as it is necessary to give. That the physician administering it should be always on guard against the possible formation of a drug habit it is unnecessary to add. But it is also unnecessary to add what alternative he shall adopt when his choice lies between the lesser evil of the opium or morphine habit and the terrible martyrdom which some patients would be compelled to submit to if not allowed to indulge in it.176 The evil effect of opium and its preparations on the visceral functions is to be neutralized, as far as possible, by the administration of laxatives and bitter tonics.
176 Few sufferers from spinal disease use anodynes habitually; opium and its preparations are not fascinating to the majority of persons. On the other hand, there are two cases of tabes dorsalis now under my observation in which the patients have been compelled to use hypodermic injections of Magendie's solution for two and three years without any materially bad effect.
The deep-seated diffuse pains, such as are found in disseminated and diffuse sclerosis, are not as markedly relieved by opium as the terebrating and lightning-like variety. Frequently spastic or other signs of increased reflex excitability are associated with them; and as both are favorably influenced by the bromides, the latter are doubly indicated in such conditions.
With pains of a rheumatic character static electricity has been recommended. It undoubtedly relieves such pains, as skilfully-applied [p. 906] galvanism would. Its chief effects, it seemed to me from a six months' trial with it, are on the imagination and hopes of the patient.177
177 A large apparatus of the new and improved make was at my disposal at the nervous department of the Metropolitan Throat Hospital. It was very popular with sufferers from rheumatism, who had been allowed to accumulate in the class before I took charge, and with a paretic dement who suffered with the rheumatoid pains often found with diseases such as his.
The bromides and camphor178 are recommended for the obstinate priapism found in some cases of early tabes and transverse myelitis. I have seen better results from warm hip-baths and general baths in this condition than from any drug. As a general rule, the exercise of the sexual function, where not already forbidden by the results of the disease, should be limited as much as possible. The frequency of normal seminal emissions in a given case is a guide to the amount of indulgence in this direction which may be permitted. Where there is the slightest indication of irritative or destructive lesions in the upper lumbar cord sexual acts should be entirely prohibited, for under these circumstances no greater injury could be done the weakened centres than to permit them. This is particularly noticed in those cases of tabes dorsalis which are marked by satyriasis in the early period.
178 Particularly the monobromate of camphor.
The treatment of the bladder trouble and of bed-sores is carried out in the manner described in the section on Acute Myelitis. For bed-sores Hammond recommends the application of a stabile galvanic element consisting of a plate of silver and one of zinc, the two being united by a wire isolated in the usual way. The silver plate is laid on the bed-sore; the zinc plate, covered by a piece of moistened cloth, is laid on the unbroken skin somewhere in the neighborhood. The result is a weak current under whose stimulant effect the healing process takes place very rapidly. I have seen excellent results that had been obtained by this means in indolent ulcers of the leg. It does not, however, seem to have been tested with the malignant variety of bed-sore.
With regard to the management of muscular atrophies by electricity, massage, and strychnia, the same rules are to be followed which are laid down in the section on the Myopathic Atrophies. It is only to be specially remarked that few authorities encourage the administration of strychnia in sclerotic affections, and fewer still in such large doses as could be of any benefit in a wasting process.
Faradization of the affected eye-muscles is often useful in diplopia. The current may be applied by means of a cup-shaped eye-electrode, or, better, by using a finger as an electrode.
The moral management of sufferers from sclerotic spinal affections is very important. The popular notion about spinal disease generally is such that the announcement made to a patient that he is suffering from any form of it is as alarming as would be the discovery of a tumor in his brain or a cancer in his stomach, and exerts a depressing effect. This it should be sought to avoid. A large number of sufferers from sclerosis live longer and suffer less than a portion of those afflicted with rheumatic and gouty affections; and the physician is justified in obtaining the desirable effect which a hopeful or resigned state of the mind undoubtedly has on the body, by laying great stress on this undeniable fact.
The writer was asked to contribute a short article upon Concussion of the Brain and Spinal Cord for this work, as these injuries are apt at first to come under the notice, if not charge, of the general practitioner. The article will therefore not be an exhaustive one, and there will be little but the details of personal experience and less quoting of authorities. Much has been written recently upon the subject both in volume and in pamphlet.
Diverse views of equally competent judges of the matter have been put forth, and the brains and spinal cords of the partisans appear to have received as severe a shaking up as the real recipients of the lesions, if absolute lesions there be.
This, in fact, is the point of controversy, for there are those who seem to deny that there can be a jarring or shaking of the cerebro-spinal mass sufficient to cause positive symptoms without producing positive lesions, whilst others are as firm in their convictions that pronounced symptoms may follow a mere disturbing ripple of the nervous elements. How is the question to be settled? The slightly shocked or injured recover rapidly, whilst some who only appear to be as slightly injured or shocked at first, go on to death, during the progress to which event there is no doubt as to the existence of lesion and no difficulty in finding it at the autopsy. Hence, say the lesionists, the first ones had it, but got well, whilst the non-lesionists affirm that it never existed in them.
The logician would think that these differences in opinion were only differences in degree about the same thing, but, nevertheless, the question is one for serious discussion, and is of much greater importance than would appear to be the case to the average layman.
This importance lies in the medico-legal aspects of the suits arising out of the alleged injuries and their consequences. Judges, lawyers, and doctors know them well. In doubtful cases authorities of equal eminence are quoted, and the results of trials are equally as doubtful as to whether justice or injustice has been done. These remarks, as will be seen, are especially applicable to injuries of the spine, but they also may have place in the consideration of consequences arising from concussion of the brain.
Whatever doubts there may be as to concussion of the spine, there are none, I believe, who deny the appropriateness of the expression as to the brain, it being, by its anatomical relations, so much more exposed to shock than the spine.
We understand that pure concussion, uncomplicated with fracture, refers to a condition caused by external violence, direct or indirect, which communicates a jar or shock to the cerebral mass, and which expresses itself by certain well-defined symptoms. The nervous system and the circulation are most manifestly involved, but in a pure case it may be said that all of the symptoms arise from central nervous disturbance. Even could it be shown that they were dependent on temporary congestions, these congestions, I think it will be admitted, would be due to vaso-motor derangements.
The anatomical appearances after early death from concussion of the brain are often insufficient for us to comprehend the fatal result, for we know that the organ will bear, both from disease and other kinds of injury, vastly greater inroads upon its structure and surroundings without causing death. Often there is mere localized cerebral congestion, with no ruptures of vessels; then there are slight extravasations shown as points or dots of blood in the nerve-matter; and, again, there is what is called the bruised brain. Sometimes there is nothing abnormal whatever to be found. Most of these cases, under modern criticism, have been justly shut out from the record as having no value; for it has been shown that the post-mortem examinations of them have been very imperfect, the brain only having been inspected, whereas the chest, the abdomen, or the spine might readily have revealed the cause of death.
It is fair, however, to assume that there must be a capacity for serious results in the vibratory jar, as the discoverable lesions in many well-examined cases have been in themselves insufficient to kill. The rapidity of recovery of those who get well also bears weight on this point.
Of nineteen cases of recovery from concussion of the brain of which I have record, the average stay in hospital was eight days. The range of stay was from one to twenty-five days. Many of these were at first profoundly shocked, some of them apparently hopelessly so when we compared their symptoms with those who died. As they recovered, however, in so short a time, there surely could not have been any gross lesion to account for their symptoms. What else, then, can account for them than vibratory jar? and if this can produce such severe results within the line of recovery, why cannot the degree of it be so extended as to involve, for example, the respiratory centres, and so kill without leaving perceptible sign?
The SYMPTOMS of concussion of the brain range from a mere daze or stunning to those of deep unconsciousness. There is no paralysis of the extremities in pure cases. Often the patient is very restless, and throws his limbs about in all directions. When these are quiet there is response to irritation and electricity. Loud speaking to him may elicit some attention, but the answers are mostly incoherent. There is pallor, often extreme, coldness of surface, and sweating. Vomiting is usual, and may come on immediately or later, and it continues as long [p. 909] as there is anything to discharge; sometimes there is retching. In favorable cases the cessation of vomiting is accompanied by a slow return to consciousness, which may be preceded by delirium. This return is never sudden, and the method of it serves to distinguish the case from that of some forms of epilepsy. The pulse is generally frequent and feeble, often irregular; in extreme cases it may be slow and feeble, very rarely, if ever, strong or bounding. After reaction it becomes more natural, and if recovery follows it will not show much variation. The temperature is depressed at first. In one characteristic case it was 98° on the first day, reached 101° on the third day, and receded to 98½° on the eighth day, when the brain symptoms disappeared.
There may be retention of urine and sluggishness of the bowels, but in bad cases coincident with the vomiting there is sometimes involuntary discharge both of feces and urine. The respiration is irregular, sometimes almost ceasing, and then returning with great rapidity.
Much has been said and written about the condition of the pupils in concussion of the brain. I have made this matter a subject of observation, and am convinced that the state of the pupils is of no diagnostic value whatever as to determining the existence of concussion or compression. Their state is of great value in telling us that the functions of certain brain-centres are partially or wholly impaired. The progress of the case will tell us whether the impairment is due to clot or effusion, congestion or jar.
It is wrong, therefore, to say that the pupils are one way in compression and another in concussion. It is right to say that in either case they are sluggish or wholly irresponsive to light. In one person they may be dilated, in another contracted, and in the same person the eyes may present marked contrasts.
In the light of modern physiology this is what might be expected. The condition of the pupils is dependent on that part of their nerve-connections which is involved in the injury, and also upon the method of that involvement. Clinical experience, I think, amply sustains this view.
The reaction from what may be called pure concussion is generally slow. The patient is apt to be dazed for some time, although the pulse and temperature may be normal. When there is a rebound with fever, and florid complexion, and suddenly or gradually another but deeper unconsciousness supervenes, it is almost certain that positive lesion took place at the time of injury, and that the reaction has brought with it great congestion if not extravasation.
Now, really, compression to be followed by inflammation is the condition demanding attention.
DIAGNOSIS.—The history of the case and the symptoms as detailed will enable us to reach a conclusion in most cases as to the existence of concussion of the brain. There are some conditions, however, from which it is to be carefully distinguished. These are simple fracture, with or without depression, compression from any cause, drunkenness, and epilepsy.
There may be such profound shock with fracture that at first concussion symptoms mask those of the lesion, or even keep them for a time completely in abeyance. The head bruises are often very deceptive to the touch in the search for fracture.
[p. 910]I am in the habit of directing students to feel their own scalps, in order that they may appreciate the fact that the touch gives no sensation whatever of the natural thickness of the cranial covering. It seems as though something like a piece of thin parchment only intervenes between the fingers and the bone. The fact is, the scalp varies from an eighth to a quarter of an inch thick, differing in different places, and where muscles, as the temporal, for example, are beneath it, the bone is much deeper. The importance of this observation lies in the fact that a pulpefied bruised mass of scalp will cause the edges of its healthy surrounding part to feel almost precisely like bone around the borders of a depressed fracture. The accompanying general symptoms will mostly not be in accord with this condition, but in some cases the deception is so complete that it is very difficult to persuade those not familiar with the fact that a fracture does not exist, and to induce them to refrain from rash proceedings.
One case I can call to mind where the opinion of the attending physician was only changed by the ultimate favorable result, which left no sign of permanent injury of any kind. These cases are particularly apt to occur with children.
I remember also another source of deception. A boy was severely injured by a blow upon the forehead. Concussion was marked. There was a lacerated wound reaching to the edge of the orbit; fractured bone could be felt, and at first sight what appeared to be brain-matter was oozing from the wound. A hasty unfavorable prognosis was given to the parents. On closer examination it was found that the fracture was of the external wall of the frontal sinus, and the supposed brain-matter was the delicate fat-lobules of the orbit. The patient recovered rapidly.
There is a marked distinction between the ordinary symptoms of concussion and those of compression, whether from depressed fracture or effusion, as of blood in apoplexy. Here there are flushed, often swollen, countenance, stertorous breathing, slow and it may be strong pulse, deep or absolute insensibility, and fixed pupils. The injury, if there is one, is mostly palpable and explanatory. If it is concealed, the other symptoms point to the true nature of the case.
The diagnosis from drunkenness is not always easy, although deep intoxication is more apt to be accompanied with compression than with concussion signs. Drunkards often have bruises on their heads caused by falls, and some of them are pale and sick after debauch. The smell of liquor is not always reliable, for it is so common after accident for friends to administer stimulants before the patient is seen by a medical man that he might be easily misled into too hasty a judgment. The general appearance of the old stager is well known, but in cases where there is the least doubt the patient, whether in hospital or in private, should be kept a sufficient time under observation for the effects of drink to pass off. Then it will be seen whether this has masked a more serious condition. Too hasty conclusions in this matter have led to most unpleasant occurrences. These are well known in police administration and to hospital men.
The convulsions of the epileptic, the foaming mouth, and the quick return to partial or complete consciousness will generally serve to distinguish the case from one of concussion, but at times there are those who [p. 911] require also to be kept under observation for some hours, and even a day or more, in order to come to a correct conclusion.
The PROGNOSIS in concussion is generally favorable, but if complete unconsciousness is present it is doubtful as to the individual so long as this lasts, for, as before intimated, the cases which recover may present as marked symptoms at first as those which prove fatal.
Recovery is mostly complete, but not suddenly so. The after-effects in any case may prove serious.
There is, however, an unwarranted tendency to attribute any defect in character, and even criminal lapses, to a blow upon the head, especially should the history or marks of one be discovered as having occurred at any time, no matter how long, previous to the inquiry.
The blow may be the cause of subsequent epilepsy, chronic inflammations, and insanity or imbecility. These cases have, however, an almost continuous history of trouble from the date of the injury, the manifestations varying in severity from time to time as pathological changes go on or as exciting causes develop them.
TREATMENT.—Absolute simple rest in bed is all that is necessary in mild cases of concussion. The patient should be well watched for any symptoms which might supervene and show that the injury was more severe than at first supposed. On the other hand, serious symptoms may be present without indicating any great gravity in the case. Children, for example, often have convulsions from the slightest cause. I have attended them when these set in immediately after the injury, but in a day or two there was entire recovery.
The more serious cases equally require rest, but also something more. To bring about reaction from shock, sinapisms to the extremities, to the nape of the neck, and over the stomach should be used. Hot-water bags should be placed along the sides of the body and limbs. Alcoholic stimulants must be sparingly used, if at all: they are rarely necessary. The stomach will often reject them unless in minute doses. If too much is absorbed, unpleasant consequences to the brain may follow. In extreme cases hypodermic injections of brandy or ether may be administered. Ammonia, camphor, and other diffusible stimulants may be useful, either externally or internally.
If the reaction is regular, with gradual restoration to consciousness and no noticeable rise in temperature, nothing further is required but a continuance of the rest and the use of cooling drinks and spare diet. The bowels and bladder must be attended to; the catheter may have to be used.
Restlessness, with or without delirium, is not unusual, but it generally subsides under full doses of bromide of potassium.
When reaction is followed by high fever, and especially when there is with it a passing on into secondary unconsciousness independent of true sleep, we have almost surely internal compression from congestion, effusion of serum, or hemorrhage to deal with. Now, blood may be taken generally or locally with great benefit. Cups, both dry and wet, to the temples and back of the neck are very useful. Leeching also is an efficient method of depletion. Ice in bags or towels, or cold water, should be applied to the head. Hot water, say about 120° to 130°, to the head is often of great service and very soothing.
[p. 912]The choice between cold and hot water is to be determined by the effects produced. Sometimes surprisingly good results come from alternating their use. Hot mustard foot-baths may be given in bed while the patient is kept lying on his back with the limbs flexed.
The result only in these severe cases will determine whether the symptoms were due to great congestion or to extravasation, possibly with brain lesion. Complete recovery takes place in the first condition. In the latter a fatal termination is much more probable, and if there is recovery it is apt to be only partial, and the patient may be the victim of nervous troubles more or less pronounced throughout a long life.
John G. Johnson of New York is authority for the statement that English railways paid in five years two million two hundred thousand pounds, or eleven million of dollars, as damages awarded by juries in cases of concussion of the spine. The statement appears almost incredible, but the facts are ample to sustain it.
It also illustrates the powerful influence of one great authority (Erichsen) better than anything I know of in the history of the medical profession. After this celebrated surgeon's lectures and work on concussion of the spine, etc. were published, dating back to 1866, the great body of medical men received them as the standard and guide in all such cases. They were a godsend to plaintiffs and prosecuting attorneys, and the defendant had a poor chance with juries when the possible miseries of any one who claimed compensation for injury to the spine was pathetically pictured to them.
That the defendants have suffered injustice in a great number of cases I think there can be no doubt. Is it any wonder, therefore, that a reaction has occurred of late, and that the views formerly held by professional men have been subjected to sharp criticism founded upon a much more scientific and practical knowledge of the subject at issue?
As in all reactions, extreme views have been reached by certain observers, and there are those who seem to hold that concussion of the spine cannot occur. By spine here is meant the spinal cord or marrow.
It has been well remarked, I think by Page, that we do not speak of concussion of the skull. We always say concussion of the brain. The use of the term spine has given rise to much confusion, but the professional man will understand what is meant when so-called concussion of the spine is under discussion.
The advocates of the rarity or even impossibility of the injury call attention with much force to the anatomical facts. First, to the immense strength, pliability, and cushioning of the bony and ligamentous encasement or column; then to the ample calibre of the canal in which the nervous cord is suspended, and to the pliant structures intervening between its inner walls and the cord itself. From without inward, in the canal, we have fat, watery connective tissue, and the plexus of spinal vessels; then comes the dura mater, loosely investing the cord and unattached to the bone, not forming here, as in the skull, the internal periosteum. Within the dura mater is the arachnoid, its visceral layer [p. 913] separated by a wide interval from the viscus or cord, which interval contains the cerebro-spinal fluid; then the pia mater or vascular membrane, which closely invests the cord.
Besides these structures there is the ligamentum denticulatum passing from the dense pia mater to the parietes of the canal and supporting the cord and roots of the nerves in the most efficient way—pliable enough to yield and break the force of vibrations, and strong enough to sustain.
Thus we see that the cord is much more securely protected from the effects of external violence than the brain, and we can understand that there is reason for the doubt of the sceptics as to the frequency of the injury described as concussion of the spine.
Clinical observation is, I think, of far greater value in determining questions of the kind than any theory, however strongly supported by anatomical facts. Does transient concussion of the spine occur as transient concussion of the brain occurs? Page, if I understand him, says not. In his work on Injuries of the Spine and Spinal Cord (London, 1883), in criticising a well-known case as to the claim of persistent paraplegia without discoverable lesion, he says: “We italicize the word persistent, for simple concussion of the brain may give rise to a transient unconsciousness, and, if the analogy holds good, concussion of the spine should per se produce a transient paraplegia. We know of no case, nor can we discover the history of any case, where this has happened.”
I italicise the last sentence. In 1881 a boy came under my care who was shot in the back three inches to the right of the third or fourth dorsal vertebra. He at once had characteristic symptoms in the legs of being wounded in the spine in such a way as to affect the cord somehow. There was partial paraplegia, with pains in both limbs. Under rest these symptoms soon disappeared. In a few days I made a deep incision and removed some clothing and fragments of bone, and then from the depths of the spinal gutter I took a large conical ball which was resting against the bony bridge of a vertebra. The boy recovered rapidly. I saw him some months afterward perfectly well.
Surely, this was a case of spinal shock or concussion with transient paraplegia, and the cause of it could have been nothing else than the impact of the ball against the column, producing vibratory jar sufficient to affect the cord. The immediate symptoms and the rapid and complete recovery are, in my opinion, inconsistent with any theory of congestion or pronounced lesion of the medulla.
Here is another case of transient paraplegia also occurring in 1881, and, to my mind, still more significant: A man fell from a height of about twenty feet and landed directly on his feet. He was immediately paraplegic. On examination no injury to the spinal column could be detected, but there was fracture of both calcanea. The spinal symptoms were thoroughly marked. Besides the paralysis of the limbs there was loss of control of the bladder and bowels, and the other accessories in such cases. But all went on to recovery. Pari passu with the fractures the spinal symptoms improved. It is not necessary here to give further details, but simply to state that in four months, the time required being chiefly due to the fractures, the patient was discharged able to walk and well in every other respect.
If this is not a case of transient paraplegia owing to spinal shock or [p. 914] concussion, I am willing to admit that I do not know the requirements of the critics when they ask for such cases. I think that it is no matter how the blow or shock to the column is received, whether direct or indirect, so that it is shown that the medulla is influenced within the line of recovery, without having suffered fairly presumable lesion.
President Garfield surely suffered from transient spinal shock produced immediately by impact of the bullet upon the column. The symptoms soon passed off, and at the post-mortem the cord was healthy in every respect. The differences between his case and the others I have mentioned were those of degree only, his concussion not being severe enough to cause paraplegia.
Spinal concussion or shock from railway collisions does not differ from forms of the same injury received in other ways. It is absurd, therefore, to give a peculiar pathological history to so-called railway spine. That the injury occurs, I have no doubt; that the medulla is seriously affected in the vast majority of cases, I have very great doubt.
I cannot now, after thirty years of hospital and private practice, call to mind a single case of concussion of the spine arising from other accidents than on railways which has had the terrible after-history that is so often attributed to them; and I have seen in that time many cases of spinal injuries of all kinds.
There is another fact of personal experience. I have examined many cases of claimed irreparable or serious injury to the spine in private, both for plaintiff and defendant, in impending suits, but I cannot remember a single application of a patient for admission to the hospital to be treated for the after-effects of concussion of the spine, the original injury having been received in a railway collision.
As all sorts of people ride on railways, it is strange that the numerous recipients of concussions of the spine are pecuniarily independent of hospitals. One old fraud I do remember who fell from a street-car and claimed lasting injury to the upper part of the spine and the head, and adequate compensation for it in court. I was not called as a witness at the trial, and the plaintiff recovered very heavy damages. These were afterward reduced to a much smaller amount when it was discovered what I knew about the case.
Other structures of the spine besides the medulla are much more subjected to injury than it is, and their consequences often mislead both patient and doctor, especially the former.
The ligaments and muscles are exposed to contusions, strains, ruptures, and twists which are wrongly attributed to concussion. From these injuries and from so-called concussions the patient recovers rapidly or slowly according to their extent. If damages are looked for from a corporation, he is in a state of what may be called expectant pecuniosity, and shows no amendment until the question is settled. Otherwise, he gets well, as those do who are injured but have no expectations.
There is a striking want of confirmation by post-mortem examination of the terrible effects which are said to follow concussion of the spine.
In fact, the records of such examinations are so few, notwithstanding the immense number of those who have claimed to have the injury that the sceptics are somewhat justified in attributing the few cases which have shown great pathological changes in the cord and its membranes to the [p. 915] coincidence of disease, as myelitis or syphilis, or to much graver injuries than concussion.
I have reported a case in full in the Medical News and Abstract (Philada., Nov., 1881) which illustrates how coincidence might easily play its part in a supposed concussion. This feature of it is not alluded to in that paper. A gentleman began to complain of pain posteriorly at the root of the neck. Paralytic symptoms gradually developed. It is unnecessary to repeat the details here, but the history was a most dreadful one, and precisely that of the few serious ones described in the works on concussion. Within a year the patient died. The autopsy revealed a meningitis and softening and destruction of the cord to the extent of two and a half inches of its brachial enlargement. There was no other disease. Now, this patient frequently travelled on railways, and if he had been subjected to the slightest accidental shock it would have been received on all sides as the cause of the disease. There was, however, no such history, nor was anything ever known to account for the fact that a man in otherwise perfect health should have two and a half inches of his spinal cord as it were spontaneously destroyed.
I will state in passing that this case did not confirm the views of Johnson and others as to there not being any severe pain on pressure in myelitis. It showed also that clinical observation is not always in accord with plausible anatomical facts or reasoning.
Thus, Johnson says: “It is a mistake to suppose that meningitis or myelitis is accompanied by pain on pressure: the spinal cord is surrounded by a bony wall thicker than the bones of the skull, and you might as well press on the head to see if the brain is diseased.”
Now, in this case the pain was simply atrocious and greatly increased by pressure. To relieve both it and the disease the actual cautery was applied on both sides of the spinous processes; and some estimate may be made of the sufferings of the patient, who would not take ether, when he exclaimed as the hot irons were burning through his tissues, “Oh, that is better than the pain.”
To sum up, then, I think I have shown that concussion of the spinal cord proper occurs. I also believe it may occur in a railway collision just as it occurred in the man who fell twenty feet. Why should not a traveller sitting in a peculiar position—with his feet, for example, firmly against a partition or wall of the car—suffer it in a collision.
On the other hand, the great majority of those who after accidents claim injury to the spinal cord as the cause of their disabilities are wholly mistaken. The question is of great importance, for upon it depends the testimony as to whether the patient has sustained temporary or permanent injury.
Each case must be studied on its own merits. There is no class of injuries so full of opportunity for the exaggerator or malingerer. The history of many of them is by no means complimentary to human honesty. Those interested can study the special works on the subject: space is not given to detail them in this paper.
The SYMPTOMS and PROGNOSIS of concussion of the spine may be almost inferred from what has been written above. There are tinglings, pain, and sometimes cramps in the limbs; there may be partial or complete paraplegia which is transient in character. Complete paraplegia is [p. 916] very rare, and when it exists it almost always indicates a more serious injury than concussion. The case I have cited is an exceptional one.
The bladder is almost always affected; there is either suppression or incontinence. The bowels are sluggish for a time. The pulse is mostly quickened; the temperature does not vary much from the normal. Priapism, which is so frequently present in wounds involving the spinal column and cord, is not present in concussion.
I have in the Medical News (Nov., 1881) given my reasons for believing this symptom to be due to a coincident impression or laceration of the sympathetic nerve when there is a fracture or other injury of the vertebra. This view I have been able to sustain by a case reported in the Medical News (Philada., Feb. 25, 1882).
The PROGNOSIS of concussion of the spine is generally favorable. The recovery is slow in pronounced cases. Where such terrible consequences follow as are described in some of the cases which have been caused by railway collision, there is reason to believe that the original injury was either too severe to come under the head of concussion, or that some coincident deterioration was present at the time of the accident.
The DIAGNOSIS from fractures and dislocations is mostly easy. In these cases the local and general symptoms are nearly always so definite as to give no trouble in coming to a conclusion as to their nature. In obscure cases time will develop the truth.
In the TREATMENT of concussion of the spine the great remedy is rest. Under this alone the slight cases will rapidly recover. The more severe ones will require other aids, such as cupping, both wet and dry, to the spine over and about the chief seat of complaint. Sinapisms, blisters, and iodine are useful in the order named. Opium will be borne much better for the relief of pain and restlessness than in like injuries of the head. The natural functions must be looked after. Both the catheter and enemata may be required. Great care must be taken to provide against chafing of the skin and bed-sores. For this I know of nothing better than repeated sponging with alcohol, and drying the surface at once by a good rubbing. The points of pressure should be frequently changed by shifting the patient.
As soon as the acute symptoms pass away the patient should be encouraged to rise and use moderate exertion. This, if well borne, should be increased day by day, for it will be soon found whether the efforts are injurious or not. All the requirements are present in these cases to produce chronic hysterical invalids, both male and female. It is therefore incumbent upon the medical attendant to protect his patient from discouraging surroundings of any kind. It is also his duty to so act that while he will be careful to work no injustice, he will at the same time be on the watch for malingering, for this will often be practised, especially by those who are among the expectants already mentioned in this article.
The various subjects embraced in this article are so closely united to each other, both in a clinical and in a pathological point of view, that they must be considered to a certain extent in common. It is of course more systematic to group them entirely according to the obvious and final lesion, as hemorrhage, thrombosis, or embolism; but when it is considered how very closely the symptoms of one affection may counterfeit those of another—so closely, in fact, that a diagnosis with absolute certainty is not only difficult, but often impossible—and also that similar conditions of the vessels may give rise either to rupture or occlusion, so that not infrequently two sets of lesions may be found in the same brain, and, finally, that the basis of prognosis and of the later treatment is not unlike in different lesions,—we are surely justified in bringing them, at least in the beginning, under a common head.
Intracranial hemorrhage, and especially cerebral hemorrhage, is the lesion which more frequently than any other gives rise to the group of symptoms known as apoplexy, and from this fact has arisen the frequent incorrect application of the word apoplexy, in a pathological as well as a clinical sense, to indicate an extravasation of blood, as in the so-called pulmonary apoplexy, where the anatomical lesion, being an extensive effusion of blood into the tissues of the lung, bears an apparent resemblance to the state of the brain often found in apoplexy primarily and properly so called, the symptoms, however, being entirely different. This error receives additional support from the fact that in some injuries to the brain, especially to the base, pulmonary hemorrhage may secondarily take place. Apoplexy, however, is not always the result of hemorrhage, but occurs with many cases of embolism and of thrombosis, and is sometimes, so far as we can tell, dependent upon neither of these conditions, recovery in one set of cases taking place so rapidly as to preclude the supposition of a considerable organic lesion, and in others, which are fatal, nothing being found beyond an excess of serum or of vascularity, and sometimes not even that. The first of these conditions has been called simple apoplexy, but with our present knowledge its simplicity seems to border closely on ignorance, or at any rate is not of a character [p. 918] to satisfy the inquiring mind. It is therefore better to retain the term apoplexy strictly as a convenient term for a certain set of symptoms, but, whenever possible to substitute for it an anatomical description of the lesion found post-mortem or diagnosticated with reasonable probability during life.
The practitioner may very properly, and without laying himself open to criticism of his diagnostic accuracy, return the cause of death in a case of sudden death, or where his opportunity for observation has been limited, or where no post-mortem examination has been held, as being apoplexy; but in others, where the symptoms were decisive or a post-mortem has disclosed the exact lesion, the condition of the cranial contents should be stated. It is also a not uncommon mistake—or rather piece of carelessness—to speak of small hemorrhages in the brain as small apoplexies. A small extravasation may give rise to slight symptoms or next to none, but a real apoplexy can hardly be small, although it may be short.
The root from which the word apoplexy is derived seems to have been used by the classic writers in something like its present clinical signification (Απορληκτος, seized with (apoplexy or) stupor—Aristophanes; mad—Demosthenes; Αποπλησσομαι, to be struck with amazement—Sophocles). Morbus attonitus, another of its names, expresses a somewhat similar idea.
Morgagni was familiar with cerebral hemorrhage, and Bonetus in the Sepulchretum gives several cases. The allusions of Galen and Hippocrates supposed to refer to this lesion are not unequivocal, although the Father of medicine could hardly have helped being familiar with the symptoms of so striking a form of disease.
Cerebral softening has been recognized since the early part of the present century, and in some of the cases thirty years ago an efficient cause, in the form of arterial disease, assigned to it; but the complete theory of its causation forms a part of the general doctrine of embolism and thrombosis which was so largely developed and systematized by Virchow. Andral and Durand-Fardel had apparently no idea of the exact mechanism of its origin, the latter supposing it to depend upon inflammation, while Todd mentions a case where softening giving rise to paralysis depended upon a dissecting aneurism of the carotid. He seems to have generalized so far as to say that white softening is atrophic, but the precise way in which this localized atrophy was usually brought about evidently escaped him. According to him, the suddenness of the attack was owing to a gradual disorganization of the brain-substance with few or no symptoms, and then a sudden rupture of diseased fibres by some accidental cause or by their having reached the extreme limit of cohesion.
Intracranial hemorrhage may be situated outside of the dura mater, separating this membrane from the bones of the skull and producing more or less compression of the brain. It is usually the result of a blow, but not necessarily of a fracture of the skull. When a fracture is present, blood may pass through it from the interior and give rise to an external extravasation in addition to that which is likely to be the direct result of the blow upon the skin and subjacent soft parts. The middle meningeal artery is a frequent source of this hemorrhage. Hemorrhage in this position will naturally give rise to symptoms of compression, and, if the fact of the blow be not known or the fracture manifest, may be mistaken for some of the deeper-seated forms.
[p. 919]Blood may be effused upon the surface of the brain in the so-called cavity of the arachnoid—that is, outside of the pia mater—or in the meshes of this membrane, following its course along the sulci. This also is not infrequently the result of violence either with or without fracture of the bone. Its source is likely to be found in the veins which empty into the longitudinal sinus from the surface of the brain. Rupture of a lateral sinus from a not very severe blow has been the source of large and fatal hemorrhage.1 Blows upon the head, with or without fracture of the cranial bones, are likely to cause rupture of the cerebral substance with hemorrhage, and this may find its way to the outside and cover more or less of the surface. Such injuries to the brain, it is important to note, do not necessarily correspond immediately to the place of the blow or to the external ecchymoses. Meningeal hemorrhage in this region may, however, be observed when no injury has been received, or at least when there is neither history nor external traces of any.
1 Cincinnati Clinic, p. 135, 1874.
The conditions under which it occurs may not vary greatly from those of the more ordinary intracerebral effusion. In two instances under the observation of the writer the source of hemorrhage has been a vessel of small, but not the smallest, calibre (artery), situated near the fissure of Sylvius, in the lower parietal or temporo-occipital lobe. In children meningeal hemorrhage is, with only a few exceptions, the usual lesion of apoplexy. The blood is usually dark and coagulated in recent cases. Blood found under the membranes where no fracture has taken place is, however, more likely to have been derived from the brain-substance and to form part of a cerebral hemorrhage.
Hemorrhagic pachymeningitis, indicated by a layer of fibrin included between the dura on the one hand and a false membrane on the other, is met with in connection with meningeal and cerebral hemorrhages. It is supposed to depend on a small and thin hemorrhage upon the surface of the brain, which forms, by its irritant action, a false membrane about itself. It is found usually over the vertex.
Hemorrhage into the ventricles is nearly always the consequence of a hemorrhage in the brain-substance breaking through, although it may in rare cases originate in the vessels of the choroid plexus, velum interpositum, or meninges. Its source, however, is sometimes so near the surface as to cause but little laceration of the cerebral tissue. The blood breaking into any one of the ventricles may be found in one or all of them (except the fifth), and form quite an accurate cast of their shape.
The most common form of intracranial hemorrhage, however, which most nearly concerns us here, and which is generally meant when sanguineous apoplexy is spoken of, has its principal seat in the brain itself, which is, of course, more or less lacerated. Such hemorrhages may vary greatly in size, from a mere red point (punctate or capillary), of which many may be present at once, to one of many ounces, filling a large cavity of nearly the length of one hemisphere, and pushing the torn and compressed brain-substance before it in every direction. The amount of laceration produced of course varies greatly; sometimes it seems as if nothing more than a pushing aside of fibres without rupture had taken place, while at others large masses of tissue are torn away and mixed up with the blood into a pulp.
[p. 920]In a recent hemorrhage the clot itself, speaking of those of a size above the capillary, is usually homogeneous, the brain-substance surrounding it ragged, œdematous, yellowish or red, and frequently containing many minute secondary hemorrhages. The rest of the brain is frequently found anæmic from pressure, the convolutions flattened, the surface dry, and the section exhibiting a diminished quantity of blood. In older cases, however, and probably also in some where atrophy, senile or otherwise, has preceded the hemorrhage, this condition is not found, and we may have the convolutions shrunken and the meshes of the pia containing an excess of serum.
If death does not take place speedily, the clot undergoes degenerative changes. Its color becomes somewhat lighter, chocolate color, reddish-yellow, or yellowish-red. A portion is absorbed, and after a time the cerebral substance in the neighborhood forms about it a wall of some density, so that finally nothing is left but a cyst with fluid or semifluid contents, and often remains of connective tissue. Sometimes the absorption of a clot of moderate size is so complete that only a firm mass of a reddish or yellowish-brown color marks the seat of an old hemorrhage. The brain-substance in the neighborhood may be more or less atrophied, and a distinct depression may be noted over the position. The microscope shows in a fresh hemorrhage only broken-down nerve-tissue and blood and vessels more or less degenerated. In an older one the blood-corpuscles have disappeared, but masses of pigment of a dark yellow or a brownish-red remain to show the former presence of blood. This pigment occurs in the form of rounded granules or of small rhombic crystals, and has received the name of hæmatoidin. The light-yellow masses often found along the course of the cerebral vessels are not evidence of hemorrhage, but of congestion merely. The so-called inflammation or granulation corpuscles, which are simply the fattily degenerated cells of the organ in which they are found, and which usually possess no distinctive form, being simply round masses of fat-drops, are often met with in the brain in hemorrhage or softening. It is sometimes perfectly evident, however, from their form, triangular or pyramidal, that they are degenerated nerve-cells. The blood-vessels, those just above the size of capillaries, are usually in a condition of fatty degeneration, masses of dark granules occupying more or less densely the line of their walls. A mere deposit of fatty granules inside the perivascular sheath, but outside of and not involving the walls of the arteries, may present the appearance of a degeneration of the walls themselves. This condition may be a consequence of any lesion involving degeneration of brain-tissue, and in no way a cause.
The intermediate stages of transformation in a hemorrhage are less frequently found than the recent or old ones, since the patient, if he does not die within a few days, is likely to live for some weeks or months.
The changes taking place in the clot itself within the first few days are not very marked, but the walls of the cavity may become softer and more deeply colored, at first red and afterward yellow. Blood-crystals have been detected on the seventeenth day (Virchow). The following descriptions have been given of clots of different ages: Eleven days—reddish-yellow softening clot, with brain-tissue stained for half an inch in depth, and brain rather hard in vicinity. Eighteen days—cavity with its [p. 921] edges anteriorly and superiorly sharply defined, with the edges posteriorly ragged and yellowish, filled with a tolerably firm brick-red mass adherent to surrounding brain, and showing in the centre a softened clot about the size of a pea. Twenty-eight to thirty-five days—soft, brownish, and semifluid. Forty-one days—spot of softening filled with brownish material. One hundred days—somewhat darker, and a little more distinctly marked from surrounding tissues; by microscope granular corpuscles, groups of fatty granules along the swollen vessels, granules of pigment. Eighty-three years—old hemorrhagic focus in right optic thalamus, color yellowish, and areolar structure.
The thirtieth day is given as about the time at which the walls of the cyst become more firm and distinct. The following statement is prepared from a considerable number of cases given by Durand-Fardel: From four to six weeks, the clot is dark-colored, from black to ochrey or reddish-yellow. It varies in firmness. The capsule is tolerably firm. From two to four months, it seems to be generally softer, pultaceous, grumous, or the clot still remaining swimming in serum; in some cases lighter in color. In six months it has lost more in color, and the cavity may be smaller. In a year there is still considerable color left. In a few cases after some years the blood has been found in the form of a dried mass, not changed or darker in color.
Hemorrhages of several months' standing may be indicated either by a brownish-red patch somewhat firmer in texture than the surrounding brain-substance, or by a cavity with firm walls, which often has strings and septa of connective tissue running across it, so as to convert it into a kind of spongy mass filled with brownish fluid.
The most important changes which are found in most if not all cases of ordinary hemorrhages (i.e. such as do not depend upon violence or cachexia) are those of the blood-vessels. They are not, however, visible in the ordinary inspection of the brain at an autopsy, but require to be carefully sought for, either with the microscope or a somewhat tedious process of washing. For this reason there are no trustworthy statistics of large numbers to determine in how large a proportion of all the cases alterations in the blood-vessels are to be found, and in what form. There can be but little doubt, however, that those cases in which no form of arterial disease is present (if, with the reservation just noted as to violence or cachexia, such exist) are to be looked upon as rare exceptions.
The presence of miliary aneurisms in the brain had been noted in some cases, and even in cerebral hemorrhage, without the great importance of the observation having been perceived; but the extended and careful observations of Charcot and Bouchard first showed how extremely common their presence is, while in many instances they were found actually ruptured. These aneurisms are present in the largest numbers in the regions of the brain where hemorrhage is most frequent, and at the age when death from apoplexy is most likely to occur. They have been found at the age of twenty, but very rarely at early ages, while after forty they are not uncommon. It is of course not always that they have gone on to rupture, but may occasionally be found where no hemorrhages have taken place. It is not going far, however, to infer that in such cases the hemorrhage was not very distant.
These aneurisms are dependent upon a periarteritis which is diffused [p. 922] more or less widely over the cerebral arteries, but not over those of the rest of the body. The larger arteries get a thin and shining appearance, compared by Charcot and Bouchard to the skin of an onion, while the smaller ones present besides distinct aneurisms, bulgings and irregularities of outline. This condition may be—and, as would be at once suggested from the age at which both lesions are met with, is—very likely to be associated with atheroma, but it is not the same thing, since the development of the aneurisms depends upon a periarteritis, and that of atheroma upon an endarteritis. It may be remarked, also, that atheroma usually does not affect the very small arteries which bear the aneurisms and give rise to the hemorrhage.
These aneurisms are visible to the naked eye, being from two-tenths to one millimeter, or a little more, in diameter, while the artery to which they are attached can be seen by the naked eye or with a lens magnifying two or three diameters. They may be strung along a small artery like beads or be found in groups like a bunch of grapes. Charcot and Bouchard found them in every case of cerebral hemorrhage which they examined, and, although the possibility of other sources was admitted, concluded that in by far the greater number of cases, excluding those dependent upon traumatism or hemorrhagic diseases, the blood effused in the brain has its origin in one of these aneurisms. The presence of these aneurisms has been abundantly established by other observers, and the fact that they are not usually demonstrated proves nothing except the amount of care and time necessary to find them. One does, however, find occasionally noted that they were sought for and not found. The statements of Charcot and Bouchard relate, so far as their own observations are concerned, and as they themselves remark, chiefly to aged persons, but in their first series of 66 cases there is found 1 of twenty and 1 of forty years of age. The patient of twenty was a semi-imbecile and a drunkard. Extensive cerebral hemorrhage, with atheroma, in the circle of Willis has been found in an apparently healthy and well-nourished boy of fifteen.2
2 Baker, Annals of Anat. and Surg. Soc. Brooklyn, 1879, p. 40.
Larger aneurisms, often multiple, are not very infrequent upon the arteries at the base of the brain. They may before their rupture give rise to symptoms of pressure like any other tumor, and may also be the source of hemorrhage, which is usually meningeal. They are not infrequently symmetrical, and a place of election is one of the early bifurcations of the middle cerebral.
Coats3 states that aneurism of the larger arteries is the most frequent source of hemorrhage in persons under fifty. They may be due to embolism, producing, when the occlusion is not complete, mechanical injury to the walls of the vessels by the constant hammering upon them of the embolus under the impulse of the blood. If this etiology is a common one, it accounts for the frequent situation of these aneurisms in the middle cerebral arteries.
3 Glasgow Med. Journ., 1882, xvii. 109.
Small vessels in a condition of fatty degeneration are often found in the neighborhood of a cerebral hemorrhage. In some cases, undoubtedly, the degeneration is a consequence of the injury to which the cerebral substance has been subjected, but they have also been found too soon [p. 923] after the hemorrhage for this explanation to hold; and in cases where no aneurisms are present the older supposition, that hemorrhage results from this kind of degeneration, seems to have a certain foundation, even if only in a minimum of cases.
In several cases of cerebral hemorrhage in purpura, where the general character of the disease was shown by hemorrhages in other organs, fatty degeneration of the cerebral vessels has been found, together with extensive steatosis of the liver, kidneys, muscles, and heart.4 In a cerebral hemorrhage found in the brain of a girl of eleven the walls of the vessels were dotted with fat-globules and dark granules, and several of them studded with round and oval nuclei closely resembling the nuclei (small cells?) commonly found in tubercle. There was no trace of tubercle in any part of the body.5
4 Gazette hébdomadaire, May 12, 1876, p. 288.
5 Trans. Path. Soc., Cayley.
There is no possible means of determining in which way any given bleeding has arisen, except a very minute search, and this may fail to show the actual point of rupture. It seems highly probable, from the connection of some cases of hemorrhage with valvular disease of the heart, that embolism may give rise to effusions of blood, especially capillary and multiple ones. In such cases the emboli may be deposited in arteries far too small to be obvious in the ordinary process of dissection. (See Capillary Embolism.)
Hemorrhage arises in some rare cases from the backing up of blood in the veins when they are obstructed by thrombosis. A case has been described where meningeal and ventricular hemorrhage resulted from a rupture of the straight sinus at its juncture with the torcular Herophili.6
6 Mullar, Lancet, 1849, i. 607.
In many diseases like purpura, idiopathic anæmia, and leucocythæmia many hemorrhages may take place in the brain as well as elsewhere throughout the body. Their importance under these circumstances is usually not great.
The usual localities of cerebral hemorrhage are stated with much minuteness in the following table from Durand-Fardel, which, although not very recent (1854), is not the less accurate on that account. No subsequent statistics have essentially altered its most important conclusions. In 139 cases the hemorrhage was situated in the hemispheres 119 times; in the protuberance (pons), 21; in the cerebellum, 13; total, 153.
I have placed beside these a small number of cases from the records of the Boston City Hospital and my own practice, and, to avoid the multiplication of headings, have entered some multiple hemorrhages under two or more heads, so that from the whole number of cases (46) there are 81 entries:
| Durand-Fardel. | B. C. H. | |
| Corpus striatum and optic thalamus, together | 22 | 4 |
| Corpus striatum | 13 | 10 |
| Optic thalamus | 5 | 3 |
| Corpus striatum, optic thalamus, and middle lobe | 2 | 1 |
| Corpus striatum, optic thalamus, and a considerable portion, not well defined, of the hemisphere | 12 | 2 |
| Corpus striatum, optic thalamus, with posterior lobe | 1 | |
| Corpus striatum and middle lobe | 3 | 3 |
| Corpus striatum, with a considerable portion of hemisphere | 5 | 1 |
| Corpus striatum, with an extended portion of base of ventricle | 1 | |
| Optic thalamus with middle lobe | 2 | 1 |
| [p. 924] Optic thalamus with posterior lobe | 1 | |
| Middle (parietal) lobe | 19 | 1 |
| Sphenoidal horn of middle lobe (temporal) | 2 | 4 |
| Anterior (frontal) lobe | 11 | 3 |
| Posterior (occipital) lobe | 11 | 5 |
| A not well-determined extent of one hemisphere | 4 | 3 |
| The superficies of the convolutions (once with corpus callosum) | 3 | 1 |
| Insula | — | 2 |
| Cortex (not further defined) | — | 1 |
| Small multiple | — | 3 |
| Meninges (secondarily) | 31 | 6 |
| Ventricles | 66 | 8 |
| In the cerebellum, right lobe In the cerebellum, left lobe In the cerebellum, middle lobe |
6 5 2 |
4 |
| In the protuberance (pons) | 13 | 4 |
| Protuberance and brain | 8 | |
| Protuberance, crus cerebri, crus cerebelli, external capsule, fourth ventricle | — | 1 |
It would not have been very difficult to increase these figures from the large number of recorded cases, but there is nothing in later statistics to invalidate the statement that the corpus striatum, including both its nuclei, but especially the nucleus lentiformis, the optic thalamus, and the white substance in their neighborhood, are the portions of the brain by far the most frequently affected by hemorrhage, and especially by hemorrhages of considerable size.
There is no essential difference in the frequency of hemorrhage on the two sides. It may occur on both sides at once. Hughlings-Jackson says that he saw a patient who escaped with life from the effects of a clot which had paralyzed both sides of the face as well as all four limbs. Charcot and Bouchard give the following localities as containing in decreasing frequency the miliary aneurisms: optic thalami, corpora striata, the convolutions, the protuberance, the cerebellum, the centrum ovale, the middle peduncles of the cerebellum, the cerebral peduncles, and the bulb. The close correspondence of this list with the table of Durand-Fardel is in itself a strong argument in favor of the importance of the miliary aneurisms as the principal factors in determining cerebral hemorrhage.
The arteries supplying the nucleus lenticularis and external capsule are small branches arising chiefly from the middle cerebral a short distance from its origin, with some assistance from the anterior and posterior cerebral. One of the larger of them runs along the outer side of the nucleus lenticularis where it is covered by the external capsule—a disposition which may have something to do with the occurrence of the larger hemorrhages so likely to take place just outside this nucleus and into the substance of the hemispheres.
The arteries of the optic thalamus arise from the posterior communicating or the posterior cerebral. Why these two groups should furnish, as they do, so large a part of cerebral hemorrhages it is impossible to state, unless it be that from their origin so near to the larger trunks before their division they are exposed to more pressure, and hence a greater tendency to form aneurisms. The functional activity of these regions is another possible reason. The largest hemorrhages also seem to spring from these sources, and if a table of large effusions were compiled [p. 925] it would probably show a greater predilection for this locality than even the general one given above, which includes those of all sizes.7
7 A very careful study of the form and size of foci of bleeding arising from the various nutrient arteries of the brain will be found in the well-known elaborate papers of Duret (Archives de Physiologie, 1874).
Before proceeding to a minute account of the symptoms accompanying cerebral hemorrhage, a consideration of the relation between extensive lesions and the most fully-developed clinical phenomena will be of value—in other words, the pathology of hemorrhagic or sanguineous apoplexy. This will naturally demand a reference to the cases where the same symptoms are present with a different lesion.
The most marked symptom, one which is essential to the definition of apoplexy, is the sudden, or more frequently rapid, loss of consciousness, and next, in a great proportion of cases, a unilateral paralysis or paresis. The latter, in many cases, finds a sufficient explanation in the rupture of fibres connecting the motor centres in the brain with the spinal cord; but this does not cover all cases, for it is well known that we may have paralysis without any laceration. In fact, in many cases paralysis may disappear so rapidly as to put aside at once any such explanation. Sufficient pressure upon contracting fibres is entirely competent to arrest their conductivity, and this pressure may be diffused over a considerably wider area than that where total destruction of tissue has taken place. Meningeal hemorrhage, where, of course, no laceration takes place, may be attended by a well-marked hemiplegia when the effusion is wholly or chiefly on one side.
The writer recalls a case of a man, of whose history little or nothing was known, found unconscious with a very distinct difference in the amount of motion to be provoked by irritation of the two sides. The diagnosis naturally inclined to the more common causes of hemiplegia, but the autopsy showed a purulent meningitis of the vertex, with a layer of pus considerably thicker on the side opposed to the paralysis.
A very similar statement may be made in regard to the symptom of unconsciousness, which seldom occurs more rapidly and completely than in cases of meningeal hemorrhage (not from injury), where, of course, there is no question of laceration.
F. Pagenstecher8 succeeded in producing phenomena closely allied to apoplexy by injecting at a known pressure, between the skull and dura mater in dogs, masses of melted wax and tallow. In the first group of cases the result was somnolence, great depression of the psychical capacity, and general muscular weakness. The second group showed, besides the condition of sopor, unilateral paralysis; and the third contained cases in a part of which death followed in a few hours after the setting in of coma, and in another part partial recovery took place after scooping out the waxy mass. The symptoms in these cases are referred to the pressure upon the vessels; and it is stated that in order to destroy life the pressure had to be equal to that of the blood. Convulsions were present in some cases where the pressure was not steady. The temperature showed a notable peculiarity in that, after the initial fall, in which it resembles the course in human apoplexy, it kept on falling in the fatal cases, instead of rapidly rising, as in man. After injection into the brain of animals [p. 926] of sufficient quantities of water to produce great tension of the occipito-atlantoid membrane, Duret9 found the respiration to cease and the heart to be slowed. On tearing the membrane so as to allow the water to escape, respiration began again, and the animals gradually recovered consciousness. Similar effects could, however, be produced by blows on the head.
8 Centralblatt f. d. Med. Wiss., 1871, p. 706.
9 Centralblatt f. d. Med. Wiss., 1878, p. 454.
Several cases are reported by P. R. Hoy10 where pressure upon the brain produced an arrest of function, which was resumed when the pressure was removed. In the first of these a piece of bone had been removed, but the dura was intact. If the patient were asked a question and the finger immediately pressed upon the dura, no answer was made, but as soon as the finger was removed the reply came. In two other cases, which are not without their parallels, the patients resumed after trephining the mental attitude in which they had been surprised by the injury—in one case hours, and in the other years, before.
10 Journ. Nerv. and Ment. Dis., vol. iv. p. 288.
The natural generalization to be made from these cases and experiments is, that pressure upon the brain-tissue suspends, for the time, its function; but when we find exactly the same symptoms arising from either sudden or gradual occlusion of the vessels where we can hardly imagine increased pressure to exist, except perhaps over a very small area of collateral hyperæmia, we must go a step farther for a common factor; and it seems possible to find one which will not only explain the several conditions spoken of, but also others which closely resemble them. Simple anæmia will cover the cases of hemorrhage and embolism, but certainly not narcotic poisoning and certain other conditions where characteristic apoplectic symptoms exist without discoverable lesion. If, however, we say that a deprivation of a considerable portion of gray matter of its due supply of arterialized and healthy blood suspends for a time its functional activity, we can explain the similarity of results arising from very different causes.
In a case of cerebral hemorrhage of considerable size the pressure is distributed over a space much exceeding the area of the clot itself, and renders a large part of at least one hemisphere anæmic. If the blood finds its way into the ventricles, the conditions are most favorable for compressing nearly the whole brain. The anæmic appearance of the cerebral surface is often remarked at autopsies.
When an embolus lodges in an artery and produces complete occlusion, the portion of brain supplied thereby becomes at once entirely anæmic, since the arteries on the surface have so slight anastomoses that they are entirely unable to supply the deficiency, except to a slight extent around the edges of the vascular territory involved. The anæmia, however, does not extend beyond the territory originally affected, and consequently we may have extensive paralysis from embolism without a marked apoplectic attack. In extreme congestion of the brain the reverse may seem to be the case.
In reality, the hindrance to the proper functions is nearly the same, since blood which is not duly renovated and contains the products of metamorphosis of tissue in excess is worth as little for healthy nutrition as no blood at all. There is no reason to suppose that blood in [p. 927] circulation, no matter in how great quantity, gives rise to unconsciousness. It may cause over-action or disordered action, as in mania, but not arrest of action.
The narcotic poisons also deprive the nerve-tissue of its healthy food; whether by interference with oxygenation and depuration, or by a direct action of the substance itself on the nerve-cells, it is not easy to say. The fact that the completeness and duration of the unconsciousness are not in proportion to the paralysis or anæsthesia shows that they are to some extent independent of each other; and, although it is possible to locate with some precision the lesion which abolishes motor power and conscious sensation, yet we cannot say how much or what part of the brain must be deprived of its function in order to produce that cutting off of all conscious relation with the external world and reduction of a feeling, thinking, remembering, and acting organism to the level of a mere automatic breathing-machine, which we designate as loss of consciousness.
In fact, in the present state of our knowledge as to what consciousness is, any speculation as to its seat would be a waste of time, and we must content ourselves with recognizing that experience seems to show that a large part, rather than any particular part of the brain, must be involved, not necessarily in the primary lesion, but in the resulting pressure or anæmia.
Another theory of unconsciousness is simply that it is due to shock—that the sudden irruption of blood acts like a blow, as it were, and abolishes for a time the function of the nervous structure. This is substituting something indefinite for something comparatively definite; and it is certainly not true that the more sudden the shock the more complete the unconsciousness. It may come on after the paralysis is apparent, and in fact is more commonly gradual than sudden in its onset. The classical instantaneous shock is the rare exception. In the celebrated case where a tamping-iron was driven completely through a man's skull and brain, he himself was able to give a clear description of the accident to the surgeon who first attended him. Several other instances of severe and sudden injury to the brain without loss of consciousness have been recorded.
ETIOLOGY.—As regards the greater number of cases and the most common pathology, the existence of so specific and peculiar lesion as aneurism enables us to distinguish between predisposing and exciting causes, or, in other words, the conditions which lead to the localized periarteritis with its resulting aneurisms and those which cause their rupture. Unfortunately, the aneurisms are not usually looked for, and in the collection of statistics we are obliged to group together cases the pathology of which is not always the same, and which are usually collected under the name of apoplexy.
Age, however, is well known, both on clinical and anatomical grounds, to be the most important factor. Among the predisposing causes of apoplexy, all statistics, both of recent and older date, agree in assigning the period of life beyond forty-five or fifty as that in which the liability to apoplexy is greatly increased. There is no age, however, below this, even to infancy, in which true cerebral hemorrhage may not occur, although the intracranial hemorrhage of children is more usually [p. 928] meningeal. It is probable, however, that in many of these the rupture of the vessel does not depend upon a previous aneurism, but on other lesions. The youngest case in which aneurisms were found by Charcot and Bouchard was twenty.
If we speak of cerebral hemorrhage in general, without reference to the presence of aneurisms, as we unfortunately are obliged to do in the great majority of cases, we may often go much below this point. In youth and childhood, however, it is possible, and often almost proved, that other conditions must have been of greater importance in determining the hemorrhage than aneurism.
In our own small series we find cases of eighteen, twenty-three, twenty-five, twenty-six, twenty-seven years of age, and quite a number from thirty to forty-five. A little further examination shows many of them not to have been of the ordinary kind; thus the patient of eighteen had valvular disease of the heart and advanced parenchymatous nephritis; the one of twenty was, so far as could be seen, typical, but no search was made for aneurisms; that of twenty-five had many small hemorrhages and was a marked case of idiopathic anæmia; that of twenty-six had valvular disease of the heart, an embolus in the middle cerebral artery, which was not in the immediate neighborhood of any hemorrhage, several old hemorrhages, and hemorrhagic infarction in other organs. The case aged twenty-seven had a very large clot in one hemisphere and advanced interstitial nephritis.
Cayley11 describes the case of a girl of eleven with a large cavity in the left middle cerebral lobe, where nothing was discovered abnormal upon the left middle cerebral artery, but when the cerebral matter was washed away with a stream of water, the walls of the vessels were found to be dotted with oil-globules, and in several places studded with round and oval nuclei. This was before miliary aneurisms were known, but the process of preparation was exactly suited to bring them to light had they been present, and they could hardly have escaped observation and mention. Other cases of boys have been reported where the hemorrhage was of the typical kind.
11 Trans. Path. Soc., vol. xx.
Meigs and Pepper speak of nine cases of hemorrhage into the substance of the brain in children, but give none of their own. Of the two cases mentioned by West as coming within his own observation, in one the source of the blood was in the cerebral veins obstructed by the formation of clots in the longitudinal sinus.
C. W. Dulles12 describes a case occurring in his own practice in a child of six months, where a considerable amount of blood was found in the lateral, third, and fourth ventricles. Nothing is said of aneurisms in particular, but the brain was carefully examined without the source of the hemorrhage being found, although it seemed to be in some of the vessels of the velum interpositum. Dulles mentions further a case reported in the books of the Philadelphia Hospital by Joseph Berens, where in the brain of a child ten days old there were found, besides a large meningeal hemorrhage, many points of subarachnoid extravasation, a clot filling all the ventricles, and a clot the size of a pea in the anterior portion of both corpora striata. In addition to these there were scattered points of hemorrhage throughout the brain-substance.
12 Philada. Med. Times, vol. vi. p. 507.[p. 929]
Cerebellar hemorrhage seems to show a certain preference for younger ages than the more usual forms. In a list of 25 cases from various sources I find the ages given thirty-two, twenty, nineteen, sixteen, thirteen and a half, eight. In the seven cases detailed by Hillairet there were two aged fifteen and twenty-six respectively.
These exceptions, however, do not invalidate the rule that cerebral hemorrhage of the ordinary type is pre-eminently a disease of later middle or advanced life.
The male sex is more liable than the female. Durand-Fardel gives 54 cases of men, 37 of women (old persons); our own list, 31 men, 15 women. Falret, cited by Rochoux and Durand-Fardel, gives 1670 cases of apoplexy among men and 627 among women. This, however, is only a rough approximation as regards cerebral hemorrhage, as it undoubtedly includes many cases not dependent upon this lesion. The same remark applies to Lidell's statement that there died in New York during three years, of apoplexy, 598 males and 440 females. This moderate predominance is ascribable to greater muscular effort, and probably also to the greater prevalence of alcoholic intoxication. Greenhow, in a Parliamentary report,13 states that in England and Wales the number of deaths from apoplexy in 100,000 of population is 46 males to 44 females. From paralysis the figures are 42 and 44, so that the total from the diseases registered under these two heads is alike for the two sexes—viz. 88 to 88. In London alone the discrepancy is a little greater on the male side—108 to 101; but in certain districts of England the excess is on the other side. Race is of little influence. High altitudes (7000 feet) favor the prevalence of apoplexy in the population,14 as in Peru and Mexico. Warm climates are somewhat, but less markedly, opposed to it.
13 Results of Inquiries into Different Proportions of Deaths, etc.
14 Hirsch, Handbuch der Hist. Geoqr. Pathologie, vol. ii.
Heredity seems to play an important part in the same sense as in tuberculosis; that is, in the establishment of a tendency, which of course means, anatomically speaking, periarteritis. Many deaths from cerebral hemorrhage may sometimes be found among the members of a single family. Dieulafoy has been able to trace this disposition through several generations. Among several instances, Mme. G—— died in three hours of paraplegia with loss of consciousness. Her mother had hemiplegia at the age of fifty-two, and two uncles and an aunt were also paralyzed at ages not stated. A commercial traveller, aged thirty-nine, was in the hospital with left hemiplegia, second attack; his mother, aged sixty-six, had an attack a few weeks before, and his grandmother died at seventy-five of fulminating apoplexy. A woman aged forty-six was hemiplegic for two months. Her mother, her maternal aunt, and uncle are all hemiplegic, and her son had a left hemiplegia at the age of seventeen. According to the cases of Dieulafoy, it is especially through the female side that the hemorrhagic disease is transmitted. Of course, the tendency may remain, and usually does so, latent until the age at which in the average of cases it becomes manifest by an apoplectic or paralytic attack; but the last two series given above show that it may develop at an earlier period of life in the younger than in the older generation.
Alcohol is universally stated by authorities to be one of the most potent factors in different races in establishing the hemorrhagic tendency: [p. 930] but it is not easy to get exact facts on this point, as so large a share of hospital patients are more or less alcoholic, and in private practice observations of this kind accumulate so slowly as not to be readily available. The greater frequency of this affection among the male sex may point in this direction. Two of the usual effects produced by the long-continued use of alcoholic drinks in excess probably combine to produce this result: first, the degeneration of tissues and tendency to low forms of inflammation of the tissues in general and arteries in particular; and secondly, the repeated dilatations of vessels under its paralyzing influence on the vaso-motor nerves, resulting in chronic congestion. This preparatory influence is distinct from the effect an occasional debauch may have in precipitating the attack.
Another highly important cause of cerebral hemorrhage is Bright's disease of the kidneys, in the form known as chronic interstitial nephritis, contracted, granular, cirrhotic, or atrophied kidney; or, as it would be perhaps more correct to say, cerebral hemorrhage is one of the results of the arterial lesion which almost invariably accompanies interstitial nephritis. As to the supposed or possible identity or relation of the arterio-capillary fibrosis of Gull and Sutton with the periarteritis of Charcot and Bouchard, the writer does not feel competent to express an opinion.
The connection between cerebral hemorrhage and hypertrophy of the heart was noticed and commented on long before it was known that the great majority of cases of hypertrophy, where no lesion of valves or of the aorta was present, were really cases of Bright's disease. The influence which might be exerted by the high arterial tension in the rupture of an aneurism is obvious enough theoretically, but it is far from certain that the effect of the renal disease, or rather the common cause of renal and cerebral disease, is not a more subtile one than this, and prepares the way for, as well as hastens along, the impending catastrophe.
This result, however, is not an extremely common one. Among 43 fatal cases of interstitial nephritis, well-marked cerebral hemorrhage was found in 4; in another, cysts and brownish indurations of small size were found which might have been partly the results of embolism. This patient had had a distinct paralytic attack. In a fifth the symptoms pointed unequivocally to a large rapid hemorrhage, although it was not demonstrated by an autopsy.
Looking at it from the other side, it was found that (in another series) of 48 cases of cerebral hemorrhage with autopsy, contracted kidneys were present in 17; and the writer is of the opinion, although he has not at his command a sufficient number of facts to make such an opinion conclusive, that if a series of cases were taken of persons under forty or fifty, excluding those where a hemorrhagic disease or a valvular disease of the heart might be present, the proportion of interstitial nephritis to cerebral hemorrhage would be greatly increased; and especially so if large hemorrhages into the great ganglia or the interior of the cerebral lobes were alone considered.
The so-called apoplectic constitution should be mentioned here; that is, the stout, thick-set build with short neck and florid complexion. The popular notions as to the peculiar dangers of this condition seem to have arisen rather from suppositions as to what might be supposed to take place, from inferring a similar state of things to exist in the brain to [p. 931] what exists in the countenance, than from any observation as to what has actually occurred. Cerebral hemorrhage may take place with any sort of complexion or any figure, and there is no sufficient evidence that persons of the physique above described are specially liable to it. Many recent writers distinctly deny any such connection.
Intellectual pursuits have been considered a disposing cause—a theory which it would be difficult to substantiate. It is not, of course, the quality of the work, but its relation to the capacity of the individual brain, which makes any amount of thought a special strain. The cases of Dieulafoy, in which the hereditary tendency was so strongly marked, were mostly hospital cases, among which class the so-called intellectual occupations do not specially preponderate. A life of constant cerebral excitement, like that of a speculator or stockbroker, certainly seems more likely to give rise to overstrain of the vessels than the more quiet and regular, but certainly more intellectual, labor of the professional or literary man.
Thackrah15 speaks of affections of the head as frequent among professional men, but does not advert to cerebral hemorrhage in particular. He evidently considers a want of sufficient exercise in the open air a far more potent factor than mental excitement.
15 Health and Longevity, p. 183.
It is very difficult to get statistics which bear upon the influence of mental labor on the brain, since the recorded occupation of an individual furnishes but a very rough estimate of the amount of thought evolved from his brain, and a very much less accurate one of what is probably of far greater importance—the amount of friction and anxiety with which it is done.
Hemorrhagic diseases may, for the sake of completeness, be once more mentioned as among the predisposing causes.
The exciting causes of cerebral hemorrhage are those which give rise to rupture of the fragile walls either of the aneurisms or fattily degenerated arterioles. They are to be found chiefly among such conditions as increase the pressure in the cerebral vessels, chiefly, though not wholly, from the arterial side. The connection of an attack of apoplexy with hypertrophy of the heart means, as has already been shown, in a great many cases, their mutual dependence upon arterial disease, as in chronic interstitial nephritis, but it seems probable also that an unusually powerful action of such a heart might be the immediate cause of the rupture. An excited action of the heart, connected with a dilatation of the cerebral vessels, naturally increases the strain on the weak portions, and we have thus the explanation of those instances where sudden or great excitement brings on the attack.
Apoplexy is less frequent in summer than in the other seasons, and it is especially remarked that sudden changes of temperature are likely to be accompanied by an unusual number of cases. Changes in the arterial tension consequent upon the varying amount of blood circulating in the skin are the probable connecting link.
Obstruction to the venous outflow, either alone or in conjunction with the preceding condition, has undoubtedly a marked effect. In addition to the cases of hemorrhage from veins obstructed by thrombi, already mentioned, instances of this method of production are to be found in [p. 932] the effects of severe muscular effort, as in lifting, in straining at stool, or, as has occasionally happened, in coitu. It has been objected to the congestion theory of apoplexy that even in severe paroxysms of whooping cough, where the face becomes cyanosed and congested, nothing like unconsciousness or paralysis occurs; but cases have been reported where aphasia and cerebral hemorrhage into the optic thalamus and cortex have accompanied whooping cough. Violent convulsions may be the cause of cerebral hemorrhage, as in puerperal eclampsia.
Obstruction to the circulation in the neck by tight clothing may be a means of increasing the back pressure from the veins. It is said that deaths from apoplexy have been unusually frequent among soldiers who have been obliged to wear tight stocks for the sake of imparting what was supposed to be a more military bearing. Probably some of the hemorrhages found with valvular disease of the heart are to be explained by venous congestion, although others are due to embolism.
Blows and shocks to the head, not producing fractures, are occasional causes of cerebral and ventricular as well as of meningeal hemorrhage. Important medico-legal questions are likely to arise where both bruises externally and internal hemorrhage are found. It is important to recollect that ecchymoses of the pericranium16 have been found in cases of apoplexy where no violence has been used. These may occur with occlusion of the cerebral vessels, as well as with hemorrhage, and are most likely to be situated on the paralyzed side, being sometimes distinctly limited at the median line. They have been supposed to be due to the general tendency of the blood toward the head, and to be of the same pathological origin as the cerebral lesion they accompany; but the fact that they may not be associated with hemorrhage proves that this explanation is inadequate. Another explanation attributes their causation to vaso-motor paralysis, together with some unknown factor present in only a certain number of cases. They may be compared to the subconjunctival hemorrhages seen after violent convulsions.
16 Lepine, Archives de Physiologie, tome ii., 1869, p. 667.
Cerebral hemorrhage depending upon a blow is likely to be accompanied by meningeal bleeding; to be situated at some point of the cortex, and not in the regions more frequently affected; and to consist of the effusion of no great amount of blood, mixed with cerebral substance. There are also very often more than one. All the circumstances should be carefully weighed when, as not infrequently happens, there is doubt as to whether a blow was the cause of a hemorrhage, or whether a person found insensible, with a bruise upon his head, may have fallen down suddenly from an apoplectic attack. In the following case it would be difficult to be sure of the sequence: A negro man aged fifty fell backward from the first step of a ladder. He got up and went to work again, but soon became unconscious. He became partially conscious again in the accident-room of the hospital, but died in a few hours. There was no sign of injury to the head, but there was a rupture of an aneurism (not miliary) of the left middle cerebral artery, and hemorrhage into the meninges and all the ventricles. If the first fall had occurred in a scuffle, and the autopsy had been made in such way as not to disclose the aneurism, it might have been considered a case of homicide.
[p. 933]Alcohol, besides not infrequently counterfeiting apoplexy, and besides acting as one of the predisposing causes, is occasionally an exciting cause. The dilatation of cerebral vessels, perhaps present as an habitual condition, is added to by the effect of the temporary narcotism and produces the rupture. In many cases these factors have their activity much increased by heavy sleep, very likely in a constrained posture, causing pressure on the veins of the neck and consequent venous congestion, which is in its turn intensified by the confined air of a station-house or the cold of the weather. The man who has possibly a vessel ready to burst in his brain should have, even if demonstrably drunk, the advantage at least of good air and an unconstrained position.
Other poisons, less frequently taken, may perhaps have a similar influence. In one case under the observation of the writer a number of small hemorrhages were found in various parts of the brain of a man who was found in his room some forty-eight hours after taking a quantity of opium, and having had, of course, no treatment during that time. He was aroused in the hospital without great difficulty, but died after a day or two with his brain in the condition above described, and bronchitis with inhalation pneumonia. There had been no paralysis, and the hemorrhages were probably not the immediate cause of death.
Durand-Fardel gives a table of supposed causes in 21 cases of persons over fifty: 8 of these were connected with either habitual use of liquor or a debauch; 9 had an attack immediately after a meal.
After naming all these causes, it must be said that in many cases it is impossible to find any reason for the occurrence of the hemorrhage at the particular moment it comes. A person may go to bed in apparent health, and be found some hours afterward unconscious and comatose, or unable to stir hand or foot on one side, or to speak. Gendrin, as quoted by Aitken, states that of 176 cases, 97 were attacked during sleep. The attack may come on when the patient is making no special muscular effort and under no special excitement. It is simply the gradual progress of the lesion, which has reached its limit.
SYMPTOMATOLOGY.—If we take as a point of departure the fully-developed attack, such as most frequently is found with a large and rapid hemorrhage into the cerebral hemispheres, pons, or cerebellum, the symptoms are those usually spoken of as an apoplectic attack, shock, or stroke, or, as the Germans say, Hemorrhagische Insult. Trousseau quotes as a satisfactory definition the words of Boerhaave: “Apoplexia dicitur adesse, quando repente actio quinque sensuum externorum, tum internorum, omnesque motus voluntarii abolentur, superstite pulsu plerumque forti, et respiratione difficili, magna, stertente, una cum imagine profundi perpetuique somni.”
Loss of consciousness, abolition of voluntary motion and sensation, and usually stertor, the appearance of the patient being that of one in deep sleep, are found in the extreme cases. In others the loss of consciousness and sensation are not complete; the patient can be aroused enough to utter a grunt or raise a hand to his face in order to brush away a fly or the hand of the physician who is trying to raise his eyelids, or can make a grimace to show that he is hurt, the face returning to its indifferent expression as soon as the cause of irritation is removed. Although the grade of action, both sensitive and motor, seems to be a little above the [p. 934] purely reflex, it is but very slightly so, and probably is not sufficient to remain an instant in the memory.
The rapidity with which this condition comes on varies widely, from a very few minutes, or even seconds, to some hours. It may even diminish for a time and return. The cases in which unconsciousness is most rapidly produced are apt to be meningeal and ventricular, and presumably depend upon the rupture of vessels of considerable size, although the location among the deeper ganglia, where the conductors of a large number of nervous impulses are gathered into a small space, will, of course, make the presence of a smaller clot more widely felt. Even in these, however, the onset is not absolutely instantaneous, and the very sudden attack is rather among the exceptions. Trousseau denies having seen, during fifteen years of hospital and consulting practice, a single case in which a patient was suddenly attacked as if knocked down with a hammer, and that since he had been giving lectures at the Hotel Dieu he had seen but two men and one woman in whom cerebral hemorrhage presented itself from the beginning with apoplectiform phenomena. In each of these the hemorrhage had taken place largely into the ventricles.
Lidell gives the following case: A colored woman, aged forty-nine, was engaged in rinsing clothes, and while in a stooping posture suddenly fell down upon her left side as if she had been struck down by a powerful blow. She was picked up insensible, and died in ten or fifteen minutes. The hemorrhage was chiefly meningeal, and especially abundant about her pons and medulla oblongata. The fourth ventricle was full of blood, and there were clots in the lateral ventricles.
A woman, aged about forty, had been hanging out clothes in an August sun. She was observed to run out of the house screaming, and fell to the ground unconscious. This was at 1 P.M., and she died at 3.30 P.M. Her temperature just after death was 107.2°. The neighborhood of the posterior surface of the pons Varolii was occupied by a broken-down-looking mass, appearing like an aggregation of small apoplexies (hemorrhages), involving and breaking down the middle crura of the cerebellum. There was no fatty degeneration nor any miliary aneurism. (I do not know upon how thorough an examination this last statement rests.)
In a large number of cases it is difficult to say, in the absence of any observation, intelligent or otherwise, exactly how rapid the onset of the symptoms may have been, but in those which occur where the patient is watched or is in the company of observant persons it is almost invariable to meet with symptoms less than unconsciousness which denote the actual beginning of the hemorrhage. From the nature of the lesion it can rarely give rise to symptoms which justify the epithet of fulminating in the sense of struck with a thunderbolt. The unconsciousness, so far as can be known, does not depend on the injury of any one special small point of the brain in which consciousness resides, but upon the compression of a considerable portion, which must necessarily take place gradually, but with a rapidity proportioned to the size of the current which issues from the ruptured vessel and the ease with which pressure can diffuse itself over a large area. It is undoubtedly the greater facility offered to such diffusion by the communication of the hemorrhage with the so-called cavity of the arachnoid and the ventricles which gives to [p. 935] these forms a peculiar severity. The difference between a hemorrhage spreading through all the ventricles or over a large surface of the brain, and one which is limited to a focus in the substance of one hemisphere, being restrained by more or less firm tissue, may be illustrated by the gain in power in the hydraulic press from the transfer of the stream of water from a small cylinder to a larger one.
Vomiting is a symptom of some importance in diagnosis, being not very common in cerebral hemorrhage, but very frequent in cerebellar.
Whether of sudden, rapid, or slow development, the apoplectic attack is, in its main features, described in the aphorism of Boerhaave given above. The muscular relaxation of the face imparts to it an expressionless, mask-like character; the limbs lie motionless by the side, unless they can be excited to some slight movement by some painful irritation or are agitated by convulsions, or in a condition of rigid spasm; the face may be pale or flushed; the cheeks flap nervelessly—le malade fume la pipe.
Swallowing, in the deepest coma, is not attempted. The fluid poured into the mouth remains, and distributes itself according to the laws of gravity without exciting reflex movements of the pharynx. When the depression is less profound, it may excite coughing or be swallowed. An attempt to swallow when the spoon touches the lips indicates a considerably higher degree of nervous activity. Respiration may be slow, but when the case is to terminate fatally rises with the pulse and temperature. It is often stertorous and difficult, the obstruction consisting partly in the gravitation backward of the soft palate and tongue, and partly in the accumulation of fluids in the pharynx. Hence stertor is in some cases only an accidental phenomenon, depending upon the position of the patient on the back, and can be relieved by turning him on his side and wiping out the mouth as far back as can be reached. Cheyne-Stokes respiration occurs in severe cases, though not confined to necessarily fatal ones.
The general temperature in cerebral hemorrhage has been studied enough to make it of considerable value, especially in prognosis. In a case which extends over a sufficiently long time several stages can be distinguished which in shorter ones may be wanting. An initial period of depression is described by Bourneville17 as occurring immediately after an attack, in which the temperature falls a degree or two below the normal, and, according to his view, continues depressed if death takes place rapidly. He gives the case of a man who died very shortly after an attack (his second one), where the temperature, taken in the rectum at the moment of death, was 35.8°. In cases which survive longer this initial fall passes either into a stage where it oscillates within the neighborhood of the normal or immediately begins to rise; the latter occurrence indicates an impending fatal termination (unless, of course, something else can be found to account for it). In the former condition we find patients whose life may be indefinitely prolonged for days or weeks, when, if a fatal termination is to result, the thermometer again indicates a rise.
17 Études cliniques et thermométriques sur les Maladies du Système nerveux, 1872.
The initial fall of temperature is not so likely to be observed except in institutions like the Salpêtrière, where large numbers of old persons are collected and under close medical surveillance; and, indeed, it [p. 936] may be doubted, even from Bourneville's own table, whether the rule is one without exceptions. At any rate, the rise is a more important phenomenon than the fall. When the rise of temperature is interrupted by a fall, and then continues again, it is due, according to the author already quoted, to a renewal of the hemorrhage.
These changes of temperature may be noted with various locations of the lesion, but it seems probable that further study might make them useful in diagnosis as well as prognosis. Hale White reports the case of a boy aged six and a half years, who was found unconscious with right hemiplegia, and who afterward had many and various paralyses with hyperpyrexia, the highest temperature being 107°. He lived long enough for secondary degeneration to extend down the crura and into the anterior cornua. A small soft patch a quarter of an inch in diameter existed at the anterior part of each corpus striatum.18
18 Guy's Hosp. Rep., 1882.
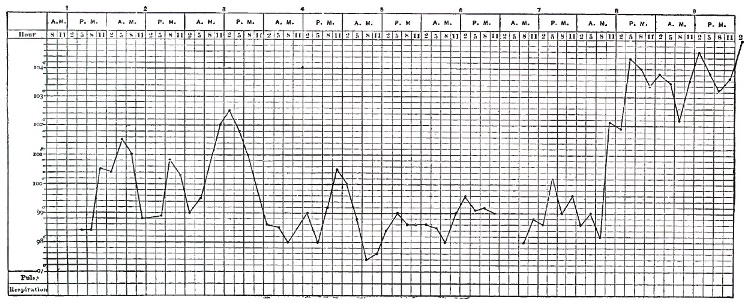
The chart W. H. (Fig. 37) is from a man aged fifty who fell in the street while returning from work at noon, and whose axillary temperature was taken at 5 P.M. and every two hours thereafter until death. The hemiplegia was not very marked, but the hemorrhage was extensive, involving the pons and left crus cerebri, the external capsule, left crus cerebelli, and medulla, bursting through into the fourth ventricle.
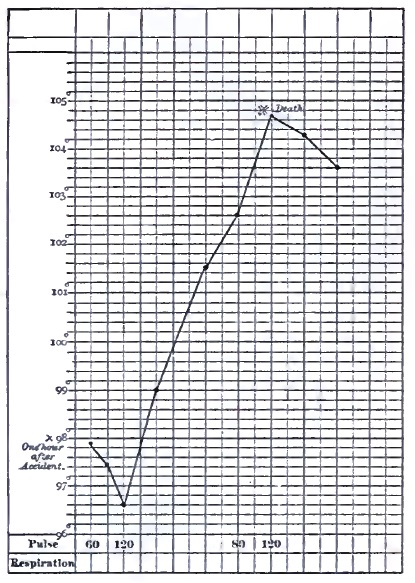
The chart M. M. (Fig. 38), as taken from Bourneville, represents the course of the temperature in a rapid case: each perpendicular line denotes an hour.
The difference in the temperature of the two sides has been variously stated, and probably depends on a number of factors besides the length of time that has elapsed since the first attack. There is probably, however, a tendency to excess of heat on the paralyzed side soon after the attack, owing to vaso-motor paralysis; and this difference will be more marked in the hands than in the axillæ. After a length of time which may be from days to months the temperature becomes equalized, or more frequently the relation is reversed, the paralyzed side being colder as atrophy takes place. Lepine19 gives a case where the axillary temperatures of the two sides continued the same within a small fraction of a degree for three days, and then separated very slowly, until at death the [p. 938] paralyzed side was six-tenths of a degree (Cent.) hotter than the other, in both being inferior to the rectal (107° Cent.).20
19 Mémoires de Société de Biol., 1867.
20 The chart in the original, and as reproduced by Bourneville, is wrongly lettered. The text says that the left side was the hotter.
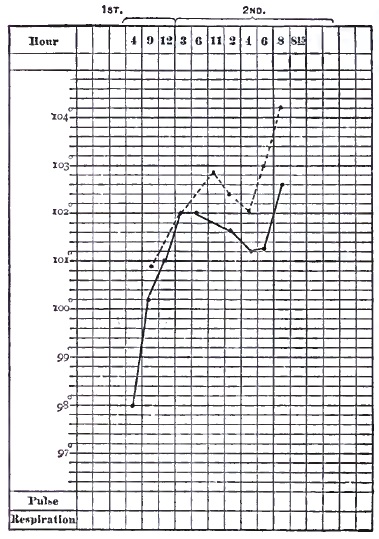
The chart C. M. (Fig. 39) shows the excess of temperature in a case of meningeal hemorrhage. The dotted line is from the paralyzed side. The first observation was made two and a half hours after the attack.
A very interesting case is reported by Johnson21 of crossed hemiplegia, where the temperature was about a degree higher on the paralyzed side of the body, and, corresponding to this, the sphygmograph showed a great diminution of tension; the lesion is supposed to have been a hemorrhage in the pons. Johnson, in commenting on the statement of Lorain that in all cases of hemiplegia the pulse is more full on the paralyzed side, says that it is incorrect for ordinary cases of hemorrhage into the corpus striatum, though true in his own case.
21 Brit. Med. Journ., Jan. 6, 1877.
The most marked differences of temperature have been observed where the lesion has been in the neighborhood of the pons, crus cerebri, or medulla oblongata. In a case reported by Allbutt there was a difference of 1.6°; the radial pulse was softer and fuller on the paralyzed side, and the cheek upon that side was flushed.22 The pulmonary hemorrhages which have been noticed by Brown-Séquard and others in animals after cerebral lesions, and the extravasation, congestion, subpleural ecchymoses noted by Ollivier23 in cerebral apoplexy, are probably to be referred to vaso-motor disturbances.
22 Med. Times and Gaz., Dec. 4, 1869.
23 Archives générales, 1873, 167.
Much more attention has been paid to the pulse than to the temperature, but it is less easy to lay down definite rules in regard to it. It may vary in either direction. When the case is approaching a fatal termination the pulse is apt to accompany the temperature in a general way in its rise, though not necessarily following exactly, as is seen in the chart in Fig. 38.
The throbbing or bounding of the arteries often described may indicate increased activity of heart, but means at the same time vaso-motor relaxation. The urine and feces are often passed involuntarily.
In some rare cases symptoms closely resembling those produced in animals by section of the sympathetic have been seen. These are false ptosis, narrowing of the palpebral opening and sinking of the globe of the eye [p. 939] into the orbit, diminution in the size of the pupil, higher temperature on the paralyzed side of the face and the corresponding ear, abnormal secretion of the eye, nose, and mouth on the same side.24 They are supposed to indicate a paralysis of the sympathetic.
24 Nothnagel, quoted by Grasset.
The condition of general relaxation may be so profound as to cover up everything else, but in many cases true paralytic symptoms may be discovered or provoked, which even at an early period give us information as to the locality and nature of the lesion.
A greater degree of muscular relaxation may be manifest on one side of the face than the other; the forehead may be a little smoother on one side, the corner of the mouth drooping, the downward line from the ala of the nose flattened, and the cheek flapping. There may be a little greater resistance to passive motion of the limbs on one side; one hand on being raised may drop helplessly back to the bed, while the other is laid slowly down; the right hand when pinched lies motionless and without power to escape the pain until the left comes to its assistance. Irregularity of the pupils, if present, is an important sign, but its absence signifies nothing.
One of the most significant signs is the conjugate deviation of the eyes, both eyes and the head being turned strongly to one side or the other. When the lesion is above the pons and is irritative, as in the early stage of hemorrhage, the deviation is toward the side of the body affected and away from the lesion; when paralysis is established, away from the paralysis and toward the lesion. Below the pons the rule is reversed. The spastic stage of conjugate deviation may coincide with stiffness (early rigidity) of the paralyzed limbs. This deviation must not be mistaken for an accidental position of the head. The patient should be addressed from the side away from which he is looking. Sometimes the eyes can be brought to the median line, and not beyond. An attempt to turn the head forcibly beyond the median line occasionally causes pain. The value of this symptom in diagnosis has been denied, but a part at least of the apparent contradictions have arisen from the neglect to notice whether it were of a paralytic or spastic character.
As the condition of unconsciousness gradually passes off, the face regaining, at least in part, its natural and more intelligent expression, the eyes trying to follow the movements of surrounding persons, an attempt being made, perhaps only by an unintelligible sound or by a nod, to answer questions, the tongue being protruded, or at least an attempt toward it made, and some motions being made with the limbs,—the exact extent and intensity of the paralysis become more apparent. Conjugate deviation, if it have existed, may disappear before the other symptoms, or, if it has been of the rigid form depending on an irritative lesion, it may become paralytic, and is then in the opposite direction. The patient is then usually found to be in a condition of hemiplegia, and at this point the history of hemorrhagic apoplexy becomes identical with that of paralysis from hemorrhage where no truly apoplectic condition has been present.
Lidell states that in more than one-third of all cases of cerebral hemorrhage hemiplegia is developed without loss of consciousness or coma. In some, the paralysis precedes unconsciousness, which then slowly supervenes.
[p. 940]Hemiplegia (ἥμι, half, πληγη blow) is a paralysis or paresis of a part of the voluntary muscles of one side of the body, and a few, in some cases, on the other, and is undoubtedly to be referred to a lesion interrupting the nervous communication between the cortical centres of motion and the nuclei of the motor nerves, cerebral and spinal; the conductors passing through the corpora striata, the internal capsule, the peduncles, and crossing in great part to the other side above or at the lower border of the medulla oblongata, and passing down the crossed pyramidal tracts of the cord, to be finally connected with the anterior gray columns of the cord. The portion which does not decussate passes down the inner border of the anterior columns under the name of columns of Türck. The amount of decussation which takes place varies somewhat, and the suggestion has been made, in order to explain certain cases of paralysis occurring on the same side with the lesion, that possibly in some rare cases there may be no decussation. It has never been shown, however, that this condition, highly exceptional if even it ever occurs, is present in such cases.
It may be said in a general way, although exceptions to the rule can be found, that it is those muscles trained to separate, specialized, or non-associated movements which are chiefly affected, while those which are habitually associated in function with those of the other side are less or not at all so. It would not, however, be in the least correct to say that specialized or educated movements of any set of muscles are alone paralyzed, since the fingers, which are trained to the most independent movements, are often just as incapable of making the slightest movement of simple flexion as of writing or sewing.
We have in ordinary hemiplegia more or less paralysis of the upper facial, the patient not being able to close his eye or to wink quite so well as on the paralyzed side. The forehead may be smoother on the paralyzed side. This condition is usually slight and of short duration, but varies in different cases. Paralysis of the lower facial angle of the mouth and cheek is usually better marked, but not absolute. The corner of the mouth droops, perhaps permits the saliva to escape; the naso-labial fold is less deep, and the glabella deviated away from the paralyzed side. The cheek flaps with respiration. The difference between this facial paralysis connected with hemiplegia and that dependent upon a lesion of the trunk or distribution of the nerve (Bell's), as in caries of the temporal bone or the so-called rheumatic paralysis, is very striking, the latter being so much more complete, and, by affecting the orbicularis palpebrarum so as to prevent closure of the eye, giving a very peculiar expression to the countenance. This distinction between the two portions of the facial seems to make an exception to the rule stated above, since in most persons the movements of the corner of the mouth and of the cheek are quite as closely bilaterally associated as those of the eyelids.
Paralyses of the third, fourth, and sixth pairs upon one side of the body are comparatively rare in hemiplegia, and when present are usually referable to localized lesions in the pons. They are to be looked upon as something superadded to the ordinary hemiplegia. These nerves, however, are affected in the peculiar way already spoken of as conjugate deviation, which phenomenon would seem to denote that muscles accomplishing combined movements in either lateral direction of both eyes, [p. 941] rather than all the muscles of each, are innervated from opposite sides—i.e. that the right rectus externus and the left rectus internus are innervated from the left motor centres, and vice versâ. Exactly the same remark will apply to the muscles of the neck which cause the rotation of the head seen together with the deviation of the eyes. The muscles controlling deviation to one side, although situated upon both sides of the median line, are apparently innervated from the side of the brain toward which the head is turned in paralysis.
The tongue is usually protruded with its point toward the paralyzed side; and this is simply for the reason that it is pushed out instead of pulled, and the stronger muscle thrusts the tongue away from it. The motor portion of the fifth is, according to Broadbent, affected to a certain extent, the bite upon the paralyzed side being less strong.
The hand and the foot are the parts most frequently and most completely affected, but one or the other may be partially or wholly spared, though the latter is rare. The muscles of the limbs nearer the trunk may be less affected, so that the patient may make shoulder or pelvis movements when asked to move hand or foot. In severe cases even the scapular movements may be paralyzed. The muscles of the trunk are but slightly affected, though Broadbent states that a difference in the abdominal muscles on the two sides may be perceived as the patient rises from a chair. The respiratory movements are alike on the two sides. A woman in the hospital service of the writer had a quite complete left hemiplegia at about the seventh month of pregnancy. There was some return of motion at the time of her confinement. None of the attendants could perceive any difference in the action of the abdominal muscles of the two sides, although, of course, the usual bracing of the hand and foot upon the left side was wanting. The pains were, however, generally inefficient, and she was delivered by turning. Muscular weakness often exists, and in some cases the non-paralyzed side shows a diminution of power.
The sphincters of the bladder and rectum frequently, and in severe cases almost invariably, lose their activity for a time. It is possible, however, that in some cases of alleged inability to retain urine and feces the defect is really mental, and akin to the dirty habits of the demented. The involuntary muscles probably take no part in hemiplegia, with the very important exception of the muscular coats of the arteries, which apparently share to a certain extent, and sometimes the iris.
Speech may be attempted, and the words be correct, so far as they can be understood, though the patient is apt to confine his remarks to the shortest possible answering of questions. It is, however, thick and indistinct, since the muscles of the tongue and lips are but imperfectly under the control of the will. This condition may be connected with paralysis of either side, and is to be sharply distinguished from aphasia or mental inability to select the proper word or to determine the necessary movements for its pronunciation. Aphasia is almost invariably connected with paralysis of the right side, and will be minutely spoken of hereafter. There is, of course, nothing to prevent the coexistence of the two conditions, but aphasia cannot well be shown to exist until we have reason to suppose, first, that the patient has ideas to express, and secondly, that the paralysis of the muscles of the lips and tongue has more or less completely disappeared. The patient may indistinctly mumble a word which, [p. 942] however, can be understood to be appropriate to the occasion (defective articulation, glosso-labial paralysis), or, on the other hand, pronounce with distinctness an entire wrong word or a number of sounds without meaning (aphasia).
Sensibility—that is, ordinary cutaneous sensation—and, so far as we can judge, the special senses, are not greatly affected after the deep coma has passed off, but exceptions to this rule will be noted later.
Having described this most typical but not most common form of cerebral hemorrhage—that is, the form in which both lesion and symptoms are most distinct and can be most clearly connected—we have a point of departure for conditions less clearly marked and less easily explained.
It is probable that cerebral hemorrhage is much less likely than cerebral embolism to take place without any disturbance of consciousness or abnormal sensations; but there can also be little doubt that a certain amount of paralysis is often accompanied by no other symptoms, and post-mortem appearances often show the remains of small hemorrhages which have passed unnoticed or are lightly estimated. It is highly probable that small hemorrhages may give rise to symptoms which pass for only a little accidental vertigo or a slight feeling of faintness, until a later and more serious attack gives a more definite explanation.
On the other hand, we have a set of cases in which all the symptoms of cerebral hemorrhage may be present without the lesion. Many of these are of course due to embolism, which will be considered later; but besides this condition, recognized as softening for many years, we find described under the head of simple, congestive, serous, and nervous apoplexy cases where sudden or rapid loss of consciousness occurs with general muscular relaxation, which, when fatal, show nothing beyond changes in the circulation—i.e. in the amount of blood in the cerebral vessels or of serum in the meshes of the pia or at the base of the brain.
Besides these, there are cases of temporary unconsciousness with complete recovery—the coup de sang of the French, or rush of blood to the head, which are attributed to congestion of the brain—a theory difficult to prove or disprove, but not in itself unreasonable. Trousseau, without denying the possibility, or even probability, of such a condition, says that which has been called apoplectiform cerebral congestion is in the greater number of cases an epileptic or eclamptic accident, sometimes a syncope. Simple epileptic vertigoes, vertigoes connected with a bad condition of the stomach or diseases of the ear, are wrongly considered as congestions of the brain. He speaks of various conditions, such as violent attacks of whooping cough, the expulsive efforts of women in labor, the congested faces of laborers under heavy burdens, to show that cerebral congestion does not give rise to an apoplectiform attack; and it is undoubtedly true that, as a rule, no long-continued attack is the result; but it must be within the personal experience of almost every one that decided cerebral disturbance is produced for a few moments by such efforts, as, for instance, blowing a fire with the head down. Besides this, a laborer under a heavy load is presumably healthy and accustomed to his work, so that his arteries may be supposed capable of maintaining a due balance between arterial and venous blood in the brain; and, again, although the ordinary efforts of women in labor do not cause unconsciousness, puerperal [p. 943] convulsions, involving a longer period of violent muscular action, may do so, and even give rise to hemiplegia.
Whatever name we may adopt for the temporary cases which recover, there are others, and fatal ones, which are not explained by any change in nomenclature. Epilepsy may, it is true, occur under such circumstances that no convulsion is observed, but, on the other hand, convulsions may accompany not only an attack of unconsciousness, but actual cerebral hemorrhage.
Cases of sudden death with no discoverable lesion furnish abundant opportunity and temptation for conjecture, and it is well known that too much dependence must not be placed upon the post-mortem appearances as to the amount of blood in the brain before death, and probably just as little upon the amount of serum, except as indicating a condition of atrophy.
Syncope, either from over-stimulation of the pneumogastric or from simple failure of the heart, may be put forward to explain some cases of sudden death, but seems to have no advantage as a universal theory over the older one, which meets with so little favor. Lidell gives no less than seventeen cases which he classifies as congestive or serous apoplexy. They are not all equally conclusive, and were almost all of alcoholics. In some of these there were absolutely no appearances which could account for death. The two most characteristic of congestive apoplexy were, first, a young negress who experienced a violent fit of passion, became unconscious, with stertorous breathing, and died, having had some tonic spasms. The brain contained a large amount of blood in the vessels, but no effusion. Second, a semi-intoxicated woman, aged thirty, became very angry, fell insensible, and expired almost immediately. The brain contained an excess of blood, with no effusion. In both these cases the patients were subject to fits under the influence of strong excitement, but in both the author took pains to inquire into and negative the probability of epilepsy of the ordinary kind; and a change of name does not go far toward clearing up the pathology.
Lidell's case (XXII.) was that of a man accustomed to alcohol, thin and pale, who had an apoplectic fit with coma and hemiplegia. He regained consciousness on the second day, and the hemiplegia disappeared in a fortnight. This rapid and complete recovery, exceptional to be sure, cannot be regarded as proof of the absence of hemorrhage or embolism. In fact, the latter is highly probable. It is possible that the clot may have been partially dislodged, so as to allow some blood to pass by it, or that an exceptionally favorable anastomosis allowed a better collateral circulation than usual to be established.
The following case occurred in the service of the writer: An elderly negress, who had extensive anasarca and signs of enfeebled action of the heart without any valvular lesion being detected, after washing her face was heard to groan, and found speechless and unable to swallow, with complete right hemiplegia. There was a slight improvement in a few hours, but she died two days later. The autopsy disclosed some hypertrophy and dilatation of the heart without valvular lesion. A careful search failed to discover any change in the brain or obstruction in its vessels, although there was chronic endarteritis.
The relations between epilepsy, apoplexy, and syncope are interesting [p. 944] and important, but are certainly far from clear. Little is gained by shifting obscure cases from one category to the other. If sudden deaths be synonymous with apoplexy, we shall certainly have to admit that apoplexy does not always demand for its cause cerebral changes sufficiently marked to be recognizable after death. If, on the other hand, we refer them to heart disease, we shall have to admit that a heart without valvular disease or extensive changes in its muscular substance may cease to beat under influences as yet not well understood.
Since the paralysis arising from hemorrhage resembles so closely in its progress that dependent upon occlusion of the cerebral vessels, a further description will be deferred until the latter lesion has been described; but this remark does not apply to the premonitory and initiative symptoms, which may be of great importance, and which are not always the same with the two or three sets of lesions. There are many of them, but, unfortunately, no one among them taken alone can be considered of high significance, unless we except what are sometimes called premonitory attacks, which are in all probability frequently genuine hemorrhages of so slight extent that they produce no unconsciousness, and but slight paralysis easily overlooked. A little indistinctness of speech or a forgetfulness of words, a droop of one angle of the mouth, or heaviness in the movement of a foot or hand, lasting but a few moments, may be real but slight attacks, which may be followed either by a much more severe one, by others of the same kind, or by nothing at all for a long time. They are sufficient to awaken apprehension, and to show in what direction danger lies, but they give little information as to the time of any future attack.
Retinal hemorrhage is admitted by all modern authors to be connected with disease of the vascular system, and hence also with renal inflammation and cerebral lesions. The writer is greatly indebted to Hasket Derby for the following facts: Out of 21 patients who had retinal hemorrhage, and of whose subsequent career he had information, 9 had some sort of apoplectic or paralytic attack; 1 had had such an attack before she was examined; 3 died of heart disease, 1 suddenly, the cause being variously assigned to heart disease or apoplexy; and 6 were alive when heard from, one of these, a man of forty-eight, being alive and well fourteen years after.
Bull25 describes four cases of his own where retinal hemorrhage was followed by cerebral hemorrhage, demonstrated or supposed in three, while in the fourth other symptoms rendered a similar termination by no means improbable. He quotes others of a similar character. The total number of cases which were kept under observation for some years is, unfortunately, not given. In a case under the observation of the writer a female patient, aged fifty-seven, who had irregularity of the pulse with some cardiac hypertrophy, was found to have a retinal hemorrhage two and a half years before an attack of hemiplegia. The hemorrhage was not accompanied by the white spots which often accompany retinitis albuminuria.
25 Am. Journ. Med. Sci., July, 1879.
In a case reported by Amidon26 retinal and cerebral hemorrhages seem to have been nearly simultaneous a few hours before death. There was diffuse neuro-retinitis and old hemorrhages besides the recent one.
26 N. Y. Med. Rec., 1878, xiv. 13.[p. 945]
The highly interesting observation has been made by Lionville27 that when miliary aneurisms are present in the brain, they may often be found in the retina also. In one case where they were very numerous in the cerebrum, cerebellum, pons, and meninges, aneurismal dilatations were found also in the pericardium, mesentery, cervical region, and carotids (the latter not being more minutely described). There was very general atheroma and numerous points of arteritis. The retinal aneurisms varied in size from those requiring a power of ten or twenty diameters to be examined up to the size of a pin's head or a millet-seed. He thinks they might have been recognized by the ophthalmoscope.
27 Comptes Rendus de l'Acad. des Sci., 1870.
The hemorrhages accompanying idiopathic anæmia and other diseases with a similar tendency are not to be taken into this account. Hemorrhage accompanying optic neuritis is likely to be due to some disease of the brain other than the one under consideration.
Mental disturbances of various kinds have been considered as significant, and Forbes Winslow gives a great many instances of different forms, but they are to be looked upon rather as indicating chronic cerebral changes which may result in various conditions, of which hemorrhage may be one, than as furnishing any definite indication of what is to be expected. Loss of memory should be regarded in this way. Some acute or temporary conditions of depression may affect the nutrition of the brain in such a way, without having anything to do with hemorrhage actual or anticipated.
Aberrations of the special senses are often observed, such as noises in the ears more or less definite, the sight of colors (red), or being unable to see more than a portion of an object. The fact to which these testify is probably a localized disturbance of the circulation which may not precede rupture of the vessels.
Distinct hallucinations of hearing, followed by those of smell and succeeding irritability, sleeplessness, were observed by Savage28 in a case which terminated soon after in apoplexy.
28 Journ. Ment. Sci., 1883, xxix. 90.
There are few symptoms which are more likely to excite alarm and apprehension of a stroke of paralysis than vertigo or attacks of dizziness, but it is too common under a great variety of circumstances to have much value, and is, as a matter of fact, rarely a distant precursor of intracranial hemorrhage, although it frequently appears among the almost initiatory symptoms, especially when the lesion is in the cerebellum, so that, if continuous, it is not likely to mean that anything worse is coming. It has been said to be strongly significant if occurring without the digestive derangements or circulatory disturbances likely to cause it, and be unconnected with disease of the ear. Unfortunately for diagnosis, but fortunately for the patients, the so-called vertigo a stomacho læso, may arise in cases where the stomach trouble is very difficult or impossible to detect, and it often continues for weeks or months after the most careful regulation of the diet, and yet is followed by no cerebral lesion. Although a vertigo for which every other cause can be excluded certainly justifies a suspicion of cerebral trouble, the tendency to exaggerate its prognostic importance should not be encouraged by the physician, as it may exist a long time, and disappear without another sign of the catastrophe which has been keeping the patient in dread.
[p. 946]Among the more significant and immediate symptoms are to be reckoned paræsthesiæ of the side about to be paralyzed, such as numbness or tickling. Headache of great severity is often, but not invariably, present. It has nothing characteristic about it, except that it may be different from those the patient has been in the habit of having, or may be of unusual severity, so that the patient says it is going to kill him. Such a headache in a person in whom there is good reason, from age, interstitial nephritis, or other symptoms, to suspect the existence of vascular lesions is likely to be an immediate precursor of a hemorrhage. Persistent early waking with a slight headache, which passes off soon after rising, is said by Thompson29 to be a somewhat frequent premonition. Vomiting is hardly a premonitory, but may be an initial, symptom, especially in hemorrhage of the cerebellum.
29 N. Y. Med. Record, 1878, ii. p. 381.
Reference is had in these statements chiefly to the ordinary form of cerebral hemorrhage. Of course if, during a leucocythæmia or purpura, large hemorrhages occur elsewhere, it may be taken as a hint that possibly the same thing may take place in the brain.
These signs of arterial disease must be considered as of the highest importance among the (possibly remoter) premonitory signs, not only of cerebral hemorrhage, but of the other lesions treated in this article. Atheroma and calcification of the tangible arteries place the existence of peri-endarteritis among the not remote possibilities. High arterial tension has already been spoken of in connection with etiology, and its presence should be sought for. An irregular and enfeebled cutaneous circulation has been spoken of as an indication of value.
OCCLUSION OF THE CEREBRAL ARTERIES may take place from several causes other than those which concern us here, as from the pressure of tumors or endarteritis, usually syphilitic. Thrombosis and embolism are grouped together from their great anatomical resemblance and their frequent coexistence, but the symptoms produced, although ultimately the same, are often different enough to make it necessary to bear in mind the fact that there is a distinction—that is, that embolism is rapid and thrombosis is slow.
A cerebral artery may be occluded from the presence of a plug of fibrin more or less intermixed with the other elements of the blood. This plug may have been formed in situ, and is then somewhat firmly attached to the walls of the vessel, and partly decolorized at its oldest portion, while on each side of it, but especially on the side away from the heart, it is prolonged by a looser and darker clot of more recent origin. This is a thrombus.
When the plug has been transported from elsewhere it is embolus.30 It may consist of various substances, as described in the article on General Pathology, but is usually of fibrin which has formed a thrombus or vegetation elsewhere, and, having been broken off, is carried by the blood until it comes to a place too narrow for it to pass, or where it lodges at the bifurcation of a vessel. The piece of fibrin thus lodged has a strong [p. 947] tendency to cause a still further deposition—that is, a secondary thrombus—which may progress until it comes to a place where the blood-current is too strong for the process to go on any farther. It may in such cases not be obvious at the first glance whether the whole process is thrombosis or whether it started from an embolus.
30 The Greek word εμβολος (εν, in, and βαλλω, to throw) signifies the beak or rostrum of a ship of war. Εμβολον signifies wedge or stopper, and would certainly seem the appropriate form to be adopted for anatomical purposes. As uniformity of nomenclature, however, seems more to be desired than etymological accuracy, the writer has conformed in this article to the general usage.
It is probable that a thrombus forming at one point in a cerebral vessel may break to pieces and its fragments be carried farther along, forming a number of small emboli. (See Capillary Embolism.) Embolism or thrombosis may take place anywhere in the brain or body generally, but has certain points of preference. Of these, the most usual in the brain is in the neighborhood where the internal carotid divides into the anterior and middle cerebral, or in either of these arteries, especially the middle, beyond this point. The plug may be situated in the carotid just before this point, or even as low down as its origin from the common trunk. Emboli lodge in this region, somewhat more often upon the left side. The brain is said to be third in the order of frequency with which the different organs are affected by embolism, the kidneys and spleen preceding it. It has been found that small emboli experimentally introduced into the carotids are found in much larger numbers in the middle cerebral than elsewhere. It is the largest branch, and most nearly in the direct line of the carotid. Position undoubtedly influences the point at which an embolus lodges, as it probably moves slowly along the vessels and along their lower side. It has been remarked that, on account of this course of the embolus, it is doubtful whether it can get into the carotid when the patient is standing, but it certainly can do so when he is sitting up; which, so far as the direction of the carotids is concerned, is the same thing. The frequency with which a hemiplegia is observed when a patient awakes in the morning may perhaps be accounted for by the position favoring the passage of an embolus into the carotid, which otherwise would reach organs more remote.
The vertebrals and basilar are not infrequently affected.
The sources whence cerebral emboli may spring are various, but cannot be found outside a certain range. They may, in the first place, be torn off from vegetations upon either the mitral or aortic valves; and this source is probably the most common. The appendix of the left auricle may furnish a plug from the thrombi formed among its trabeculæ, or the aorta from an aneurism or from parietal thrombi formed, upon spots roughened by atheroma. The pulmonary veins are occasionally the source of the embolus, though this is not very common.
It is rather doubtful whether an embolus can find its way from the systemic veins through the lungs to the brain, but it is possible that small emboli may do so, and increase in size from the addition of fresh fibrin when floating in the blood-current. The occurrence of pyæmic abscesses in the brain would suggest the possibility of this, though it is, on the other hand, possible that the brain abscesses are secondary to older ones in the lungs. In some cases, however, a careful examination does not disclose the source of the embolus.
In the blood-current the embolus may give rise to no symptoms whatever, and even after its arrival in the cerebral circulation it may lodge in such a way as not entirely to obstruct the current. In most instances, however, it does not stop until it plugs the vessel completely and arrests [p. 948] the current of blood beyond it for a moment. Whether it shall completely deprive the portion of brain to which it is distributed depends upon its situation as regards anastomoses and upon the formation of secondary thrombus. Hence the knowledge of the distribution of the arteries supplying the brain—that is, the two carotids and two vertebrals—is of more importance in reference to embolism and thrombosis than to cerebral hemorrhage, where the effusion takes place from quite small branches.
The anterior portion of the brain, including the anterior and posterior central convolutions and the first temporal, are supplied with blood by the two terminal branches of the internal carotid, the anterior and middle cerebral, the ganglia underlying these portions of the cortex being supplied, as already stated, by small branches arising near the origin of these two trunks, and principally the second. The anterior cerebrals of the two sides are connected by the anterior communicating, which is a short and usually wide vessel. Sometimes one anterior cerebral branches in the longitudinal fissure, and supplies a part of both sides. Hence in plugging of one internal carotid which does not reach its bifurcation a collateral supply may be received from the other side. If, however, an embolus or thrombus has penetrated beyond the origin of the middle cerebral, this vessel can no longer receive a supply from the anterior.
The posterior communicating arteries are two small vessels which connect on each side the posterior cerebrals and either the carotid, just as it gives off its two chief cerebral branches, or else the middle cerebral close to its origin. These arteries may be of quite unequal size, that upon the right usually being the larger, and sometimes so large as to give the appearance of being the principal origin of the posterior cerebral. When this happens the part of the posterior cerebral which arises from the basilar may be reduced to a minute arteriole, and the basilar, almost entire, goes to supply the left side of the brain. This condition of the posterior communicating may exist to some extent on both sides in the same brain. It is probable that in many cases these arteries are too small to be of great value in re-establishing the circulation in the anterior portion of the brain when it is suddenly interrupted by an embolus.
When the large trunks leave the circle of Willis to be distributed upon the surface of the brain, after giving off from the first centimeter or two of their course the nutrient arteries for the deep-seated ganglia, they break up into several branches which ramify upon the surface, but, as Duret has shown, undergo very few anastomoses. Instead of forming, as was once supposed, a richly inosculating network, small branches penetrate into the brain-substance perpendicularly from the superficial vessels, but these do not communicate freely with each other by vessels larger than capillaries.
From these anatomical conditions it happens that when a vascular territory is deprived of its normal supply by an embolus, it cannot be supplied with blood from surrounding districts. A certain limited amount of collateral supply is possible through the capillaries and the rare anastomoses, but it is only around the edges, and the centre of the territory becomes destitute of circulating blood. Thus an embolus does not in the brain produce, as it does in other organs with more abundant collateral supply, a large hemorrhagic infarction.
[p. 949]Small hemorrhages may, however, take place around the edges of the softening, and when a number of small emboli are present, so as to afford a number of overlapping areas with their borders of congestion, a red softening may be the result. When the emboli are very small, and at the same time not numerous enough to occlude all the ultimate ramifications of a trunk, the vascular compensation may be rapidly completed.
The change produced in the cerebral substance from cutting off its supply of blood is known as anæmic necrosis, and includes what has been known as white softening, with probably some yellow, and possibly a little red softening, the latter in case where simple softening has been complicated by hemorrhage.
When the circulation ceases the substance that should have been nourished loses its firmness and acquires a custard-like consistency. The gray and white substances are no longer so distinct in appearance, the latter losing its milky-white color, the whole surface of a section becoming of a dirty yellowish-white, somewhat shining, and looking as if it contained more moisture than normal. When a considerable portion of the interior of the hemisphere is thus affected, the brain outside, with its membranes, bags down, looks swollen, and feels to the fingers as if there were present a sacful of fluid. The boundaries of such an area of softening are marked off from the healthy substance with some distinctness, though less than that of a hemorrhage. There may be some hemorrhage around the edges or into the cavity, so that the presence of a little blood-pigment is no proof that the original lesion was not softening from occlusion. In the further progress the contents of the cavity become more fluid, and finally a somewhat distinct cyst is formed, not unlike that from a hemorrhage, with an internal areolar structure from the remains of connective tissue, and contents of a slightly yellowish or brownish color, or often of a chalky white. These cysts have little to distinguish them, when old, from similar ones left by hemorrhage, except the much greater amount of pigment in the latter. The smaller spots of softening may after a time lose their fluidity, and remain as yellowish patches as firm as, or firmer than, the surrounding brain. The region of the brain involved becomes atrophied, the convolutions shrink, and the membranes become filled with serous fluid, to compensate for the sinking of the surface.
The microscope shows gradually increasing fatty degeneration, disorganization of the nervous tissue, and degeneration of its elements. The pyramidal cells are sometimes distinctly recognizable by their form, and show gradual transition into the indeterminate round granulation-corpuscles. The vessels exhibit fatty degeneration of their coats, as well as accumulation of fatty granules between the vessel and the lymphatic sheath. The clot which blocks the artery becomes adherent to its walls, and the vessel with its contents forms a round solid cord.
In a few instances the thrombi have become perforated through the centre, so that a channel is formed for a renewal of the circulation. There is no reason to suppose that this takes place soon enough to be of any advantage in restoring the nutrition of the necrosed portions of brain.
The region involved in softening depends upon the artery which is plugged and the location of the obstructing body. The place of election seems to be the carotid near its separation into its large branches, or these [p. 950] branches after the separation, especially the middle cerebral, this being peculiarly liable because it is the largest branch and is the continuation in a direct line of the carotid. It is more frequent upon the left side. Cases have been observed where the whole of one hemisphere was softened from obstruction of the carotid at its bifurcation; which may be accounted for, as Charcot suggests, by an unusual distribution of the arteries, as described above, the posterior cerebral as well as the other two being derived almost entirely from the carotid. In a case recently observed by the writer the whole right cerebral hemisphere, with the exception of the tip of the frontal and tip of the occipital lobes, was softened to the consistency of custard, a thrombus extending from the bifurcation of the common carotid into all the ramifications of the middle cerebral. The most common form, however, is where more or less of the brain around the fissure of Rolando and fissure of Sylvius, with or without the underlying ganglia, is softened. This happens from a lodgment of the embolus in the middle cerebral. If the obstruction be close to the origin of the artery, the corpus striatum suffers, from the mouths of its small nutrient arteries arising in this part of its course being stopped, while if it have passed along a little farther, these remain open, and the cortex, to which the larger branches are distributed, alone is softened.
The anterior cerebral is not infrequently affected, either alone or with the middle, and in these arteries as well as the posterior the embolus, if of small size originally, may penetrate so far as to give rise only to quite a limited anæmia. The basilar is an artery not very rarely occluded, though more commonly by thrombus than embolus. This occlusion may be so limited as to affect only the nutrient arteries of the pons and cause a very limited softening, the parts before and behind it being supplied by the unobstructed portion or by collateral circulation from the carotids. Occlusion of the cerebellar arteries and softening of the cerebellum are among the rarer forms. The vertebrals themselves are sometimes plugged. A thrombosis has been observed in the only inferior cerebellar artery which existed, causing softening in both lobes. There was atheroma of the heart and arteries, and a thick calcareous plate in that which was occluded.31
31 Progrès méd., 1876, 373.
In a general way, it may be said, with many exceptions on both sides, that thrombosis and embolism tend to affect the cortex, and hemorrhage the central ganglia.
What has just been written applies to the simple mechanical action of emboli. If, however, they have a septic origin, as notably in cases of ulcerative endocarditis, the region in which they lodge becomes, instead of a simple spot of necrosis, a septic focus or abscess, with its results of compression or irritation. In such a case there are likely to be abscesses of similar origin in other organs, and the cerebral lesion is only a part of the general pyæmic condition.
ETIOLOGY.—So far as the lodgment of an embolus in an artery is concerned, it can hardly be said that there is any etiology, for the detachment of the plug from its place of origin is purely a matter of accident, and may take place at any time. As to its origin in the form of fibrinous deposit on the valves of the heart or a roughened spot on the aorta, we must refer to the article on General Pathology. The most important [p. 951] condition for embolism is disease of the valves of the heart, rheumatic or otherwise. Next comes arterial disease, producing roughening of the inner coat and subsequent deposition of fibrin. So far as we can tell, the causes leading to endarteritis or atheroma are essentially the same as those which produce the periarteritis described in connection with cerebral hemorrhage, and we may therefore put down old age, alcohol, and strain as among the causes of cerebral embolism. Injuries of the lungs leading to thrombosis of the veins may be considered as possible sources for the formation of an embolus, and we might suppose that phthisis and pneumonia would furnish plugs which would lodge in the brain, though as a matter of fact they seldom do so.
Experience shows that embolism, unlike hemorrhage, is not specially a disease of advanced life, but is distributed over different periods, with preference for old age less marked than with hemorrhage. Andral gives the ages of patients with softening—which, however, includes thrombosis as well as embolism—as follows: the average would undoubtedly be displaced in the direction of youth if thrombosis could be taken out of the list:
| Andral: Beginning of softening in 27 cases. |
Andral: Death with softening in 153 cases. |
Cases (with autopsies) of embolism, thrombosis, and softening—25 cases. |
| 17–20 4 27 2 30–37 2 43–45 2 53–59 4 63–69 7 76–78 6 |
15–20 10 20–30 18 30–40 11 40–50 19 50–60 27 60–70 34 70–80 30 80–89 4 |
20–30 4 30–40 3 40–50 3 50–60 1 60–70 5 70–80 2 Young 1 Middle-aged 1 Old 5 |
In the etiology of cerebral arterial thrombus there seem to be two factors of prime importance, although there are cases which seem to demand a third, and Charcot32 suggests the possibility of some hæmic dyscrasia favoring the formation of a thrombus, and relates a case of thrombosis of the middle cerebral, with three others of the same process in other arteries, occurring in patients with uterine cancer, where all the usual sources of emboli were explored with negative results. The first of the two is disease of the cerebral arteries, not necessarily extensive, but sufficient to form a starting-point on the inner wall for the deposit of fibrin. In this respect the etiology of thrombosis may be various. Syphilitic endarteritis, for instance, may very easily give rise to this lesion, but it is likely to be accompanied by others, and has a symptomatology more or less peculiar to itself. It is not, of course, to be included with the form we are considering.
32 Comptes Rendus Soc. de Biol., 1865, p. 24.
The second factor—one which is perhaps capable of giving rise to coagulation of the blood or deposit of fibrin without any arterial disease—is weakness of the heart, connected or not with anæmia. The causes of this condition may be manifold, and are likely to lead to many other consequences than cerebral thrombosis. A thrombus may form upon a very small basis of atheroma. Several of these points are illustrated in the [p. 952] following case: A lady, aged about sixty-five, had had for many months vague symptoms of want of strength, fatigue, want of appetite, and so on, with complaints of distress and fulness in the abdomen, for which no special cause could be found. On one occasion she was unusually long in dressing, and her expression was noticed to be changed and her voice altered for a few moments. The pulse was habitually 60 or less, and at times irregular, but nothing abnormal could be detected in the sounds or position of the heart. Fatty degeneration was suspected. One morning, after going to bed in her usual health, she was found on the floor of her room unconscious and with left hemiplegia. She lived about thirty-six hours. The autopsy showed nothing abnormal in the abdomen except a considerable accumulation of fat; and in the thorax the heart appeared normal, and was not fatty. There was very little atheroma. In the end of the internal carotid artery was a thrombus, of which the lower and firmest part was connected with a very small spot of roughening just at the point where the artery comes through the base of the skull. It extended just beyond the origin of the middle cerebral artery, which was of course occluded. The corresponding region of the brain was converted into a vast mass of softened tissue.
The SYMPTOMS of the lodgment of an embolus in the brain may closely resemble, or even be precisely the same as, those of hemorrhage. Unless, however, an embolus makes a pause on its journey, giving rise to a partial obstruction before there is a complete one, or unless the obstruction is not absolute until after the formation of a secondary thrombus, the attack may be absolutely sudden.
A thrombus, however, is slower in its formation, and may produce gradually increasing anæmia of the region of brain supplied before it is absolutely complete, with a gradually increasing paralysis and loss of consciousness slowly approaching. Thus we may have the early symptoms in the form of headache, vertigo, heaviness, and drowsiness, peculiar sensations in the limbs about to be paralyzed or in the head, delirium of various kinds, or hysterical manifestations. Prévost and Cotard33 lay special stress upon the importance of severe vertigo (étourdissement) as a prodrome or warning of softening, especially in the aged. It is dependent upon anæmia of the brain, and this, in its turn, upon atheroma of the arteries, and sometimes at least upon feebleness of the circulation, both of these being conditions likely to cause the deposit of a thrombus. As, however, the thrombus does not necessarily result from these conditions, and as the vertigo may arise from other sources, as stated under the head of Cerebral Hemorrhage, it is to be looked upon with special suspicion chiefly in those cases where other symptoms might lead in the same direction, and when other causes can be excluded.
33 Mémoires de la Soc. de Biol., 1865, p. 171.
The same authors also speak of less defined symptoms, like delirium and stupor, occurring among the inhabitants of the Salpêtrière (old women), with intervals of comparative health, as being premonitory.
It is possible, however, for the symptoms of thrombus to be developed rapidly when, as in the case last described, the thrombus begins to form in a place which does not entirely interrupt the current, but afterward reached the mouth of a large vessel, which it closes.
The loss of consciousness, coma, and all the phenomena of the [p. 953] apoplectic attack, with the possible exception of early rigidity, may be as fully developed from occlusion of the cerebral vessels as from their rupture; but it must be said that it is more common to meet with them in cases of large hemorrhage than with either embolism or thrombosis.
The general functions are even less disturbed than with a hemorrhage producing an equal extent of paralysis. The temperature follows nearly the same course as in hemorrhage, except that the initial fall, if present—which is not always the case—is said to be less than with cerebral hemorrhage. To this succeeds a rapid rise, which, even in cases which are to terminate fatally, gives place to a fall to the neighborhood of normal, and another rise before death. These are the statements of Bourneville. The rise is said not to be so high as with hemorrhage.
The annexed chart is from a man (W. I. W.) who was in the hospital with ill-defined nervous symptoms, and was suddenly attacked with convulsions, vomiting, and unconsciousness. He had a small tumor at the point of the right temporal lobe, and softening of the left corpus striatum. The apoplectic symptoms occurred on the 15th—that is, as will be seen by the chart, one day after the temperature began to rise. The pulse and respiration show no characteristic changes.
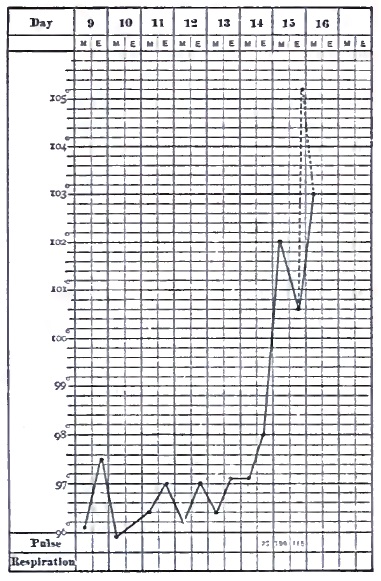
It is much more common for the embolus or thrombus to give rise to a set of symptoms less severe than a fully-developed apoplectic fit. During such a fit—or, more clearly, as it is passing off—we find more or less marked paralytic symptoms, but these are quite as frequently present without the loss of consciousness. The patient states that he waked up and found one side of his body helpless, or that he was reading the paper when it fell from his hand, and upon trying to walk found that he could not do so. Loss of speech may be an initial symptom. It has been spoken of as premonitory, but it is probable that it is in reality only the beginning, which, in some cases may go no farther, but is usually succeeded by more extensive paralysis, which makes its meaning unmistakable. These symptoms may be hours or even days in developing, with occlusion as well as with hemorrhage. Very slight attacks may occur which hardly excite attention, and lesions are found after death in many cases to which there is nothing in the history to correspond.
Improvement may begin very rapidly in some cases where the lesion is small, a sufficient amount of collateral circulation being developed to [p. 954] prevent the structure from being disorganized. In others a specially favorable anastomosis may preserve even a larger area, but in others still it is not easy to account on entirely anatomical grounds for the amount of improvement which takes place.
From this point onward the history of hemorrhagic and of embolic and thrombotic paralysis is essentially the same, and the description of the principal phenomena and progress of hemiplegia will apply to all.
SYMPTOMS AND PROGRESS OF HEMIPLEGIA DEPENDING ON CEREBRAL HEMORRHAGE OR OCCLUSION OF THE CEREBRAL VESSELS.—The cerebral cortex represents the centres for many of the higher nervous functions, spread out in such a way that they may be more or less separately affected, while the corpora striata and internal capsules are the regions where the various conductors are crowded together, so that embolism, when affecting small vessels and limited areas of the cortex, more frequently gives rise to narrowly-defined groups of symptoms than hemorrhage, which, taking place oftener in the central ganglia, is able to cut off the communication from large masses of cerebral tissue at once. This is a general remark, tending to explain why aphasia, for instance, is often spoken of as especially a symptom of embolism, while it is in reality common to all the lesions that affect the proper locality.
The motor paralysis, more or less complete, which has been described under the head of Hemorrhage continues indefinitely. It may disappear rapidly, so that motion begins to return in a day or two, and goes on to complete recovery in a short time. On the other hand, it may be months before the flexion of a finger or a toe gives the slightest token of the will resuming its control. The face often recovers its symmetry before the limbs are fully restored, but the leg may be used in locomotion before the complete recovery from paralysis, since the tone of the muscles is sufficient to keep the knee straight enough for support, as if the leg were all in one piece, while it is swung around at each step by the pelvic muscles. We may meet with all degrees of recovery—from that which is absolutely complete and comparatively rare, through the case where a little want of play upon one side of the face, a little thickness of speech, a feeble or awkward grasp of the hand, betrays what has happened, or that of the man so often seen in the streets with a mournful or stolid face, the arm in a sling or dangling straight down by the side, and swinging one leg awkwardly around, to the helpless paralytic lifted in and out of his chair or lying almost motionless in bed, and living only to be fed and be kept clean.
Involuntary movements may take place in limbs entirely incapable of voluntary ones, and may occur under conditions of excitement or with other involuntary movements, such as gaping. On the other hand, the patient often moves the well hand while making utterly ineffectual attempts on the paralyzed side. Involuntary twitching of the feet may be annoying. Reflex movements, especially of the feet, are often exaggerated, and in fact the twitching just spoken of is often excited by some trifling, perhaps unperceived, irritation. A touch with the point of a penknife upon the sole of the foot may call out a movement which the patient is utterly incapable of executing by the force of the will, and the appearance of volition is often increased by the grimace or exclamation of pain or annoyance.
[p. 955]Epileptiform attacks may be a sequence of hemiplegia, occurring at irregular intervals, and not of great severity. Sometimes the patient seems depressed or less talkative for a day or two previously, and relieved after the fit has occurred, as in true epilepsy.
Comparatively little attention has been given to the condition of sensation in hemiplegia. In the more complete apoplectic stupor it is apparently abolished, like nearly all the functions above those of respiration and circulation, but it often happens when the patient is unable or unwilling to make any voluntary response to the voice, and lies apparently perfectly indifferent, that any moderate irritation like a pinch will bring out evidence of sensation. It is often stated that in hemiplegia the sensation is not at all affected; and this is probably true of many cases, but a more attentive examination will often disclose a decided diminution on the affected side. Broadbent, who has tested with pricking, touch, the compasses, and hot substances, says that it is frequently diminished, and often greatly so, and not only in the limbs, but in the face, chest, and abdomen. Tripier34 says that a lesion of the larger part of the fronto-parietal region determines at the same time a paralysis of motion and a diminution of sensibility; and one may conclude that this region holds under its dependence sensitive as well as motor phenomena intimately connected with each other. The zone called motor, of which the limits are difficult to fix, may with more reason be called sensori-motor.
34 Revue mensuelle de Méd. et Chir., 1880, p. 18.
Anæsthesia probably in most instances disappears more rapidly than motor paralysis, which accounts for its being frequently overlooked. The more common location of lesions causing motor paralysis—i.e. the corpus striatum and the motor portion of the cortex—is one not likely, unless extensive, to concern sensation; but there are cases where a very complete hemianæsthesia, including the special senses, may be found; and when, in such cases, the motor paralysis is slight, a picture is presented almost identical with that of hysterical hemianæsthesia with great diminution or abolition of the special senses, hearing, taste, smell, with concentric diminution of the field of vision and of the color-field, or complete color-blindness on the affected side.
A man aged thirty-five while at work suddenly felt a prickling sensation upon his left side, and became unconscious. The bystanders say he was convulsed. On returning to consciousness after three hours he had lost his speech, which, however, was rapidly recovered, and his left side was not so strong as his right, though there was no distinct history of paralysis. Two or three days afterward it was noticed that sensation was much diminished upon the left side, two sharp points of the æsthesiometer being felt as one at two inches on the forearm and three-quarters of an inch on the tongue. He could feel the touch of a spoon, but could not tell whether it was cold or hot. Odors were not recognized upon the left side of the nose, except faintly ammonia and chloroform, and a watch was heard on that side only when in contact with the ear. The field of vision was much diminished and color-blindness was almost complete. A few days later the field of vision had increased, and there was color-sense, the field of perception for the different colors being arranged almost exactly as laid down by Charcot, vision for red being largest, but not so [p. 956] large as for simple perception of objects; those for blue, green, and yellow nearly the same and smaller; and that for violet limited to a small space in the centre of the field.
Less regular forms of anæsthesia may be met with, as well as hyperæsthesia. These are said to be especially connected with various lesions of the pons.35 A case is recorded36 of complete hemianæsthesia in a man, coming on like a blow. There was no loss of motor power; the face was symmetrical, sight and hearing unimpaired. Taste was lost and smell doubtful. There was aortic and mitral disease. Hughlings-Jackson speaks of a man who experienced a severe apoplectiform attack which it was thought would be fatal in a few hours. He recovered, however, with almost complete loss of hearing.
35 Conty, Centralblatt f. d. Med. Wiss., 1878, 571.
36 Med. Times and Gaz., 1871, i. 246.
Neuralgic pains of long continuance are not infrequent accompaniments of hemiplegia, and may be lasting even after nearly complete recovery from the paralysis. A peculiar restlessness, a constant desire for change of position, has been referred to derangement of the muscle-sense. It is sometimes very distressing, and causes much annoyance to attendants as well as to the sufferer, as the patient is no sooner placed in one position, no matter how comfortable, than he desires to change it.
The mental condition seldom fails to suffer more or less in cases of hemiplegia, but the limits are very wide between a slight emotional excitability on the one hand and almost dementia on the other. This is, of course, applicable to cases where the lesion is a single or limited one, and not where a hemorrhage or thrombus is merely a part of a general vascular degenerative change with chronic meningitis or atrophy of the brain, where the mental decay can hardly be called the result of any single lesion. In cases of aphasia the mental condition is harder to make out, from the peculiar inability to communicate ideas if present. It is very safe to say, however, that many such patients possess much greater intelligence than would appear to a casual observer, and yet the apathy with which they often bear the deprivation of speech and consequent isolation speaks more strongly in favor of some blunting of the perceptions than of Christian resignation. A patient whose general appearance is that of tolerable comfort is likely to cry when attention is called to the helpless condition of the hand. It is probable that memory suffers in such cases, if not the reasoning faculties.
Trousseau cites the case of Lordat, who became aphasic, and after recovery described his own case. The learned professor claims to have been in full possession of his faculties, and to have arranged a lecture with the divisions and subdivisions of the subject, and all this without the thought of a single word passing through his mind. Trousseau ventures to doubt the possibility of carrying on complicated mental processes without words, and thinks Lordat may have overestimated the precision of his mental processes. It appears in confirmation of this view that after his attack he always read his lectures, whereas before he had been distinguished as an extempore speaker.
McCready, in an excellent article in the New York Journal of Medicine (September, 1857), discusses this subject at length, and details a number of cases where it was evident that paralytics and aphasics (who, however, [p. 957] he did not know by that name, nor the special lesion connected with their condition) possessed not only ordinary intelligence, but excellent business judgment and ability. He says that the confusion of mind and difficulty in pursuing a train of thought of which apoplectics are apt to complain is, to a great extent, the mere result of diminished nervous energy—that they comprehend well and judge correctly. It is fair to say that while the mind is almost certainly impaired, it is not necessarily in exact proportion to the severity of other symptoms, aphasia included. The memory, either special or general, is most apt to be impaired.
The testamentary capacity of a person who has had an apoplectic fit or who is paralyzed at the time of making a will may be called in question. The only general remark to be made is that these facts alone are not sufficient to prove incapacity; neither should the presence of aphasia or agraphia do so without further evidence of want of comprehension of the meaning of language used by others; so that if, for instance, a person were seized with hemiplegia and aphasia between the drawing up of a will and its signature, it should not be invalidated unless there be further evidence to show that the testator was incapable of understanding it when read over to him. In cases of word-blindness, a patient, like one described by Magnan, may be able to draw up a will with full comprehension of what he is doing, and yet be unable to read it understandingly. Inability to signify intelligibly assent or dissent would, of course, entirely disqualify one from signing a will.
It is seldom that a paralytic attack fails to leave its mark, though perhaps slight, for years, if not for the remainder of life. An extreme ease of shedding tears is a very common symptom, and sometimes laughter comes on very slight provocation.
Among the most interesting groups of phenomena connected with hemiplegia, and sometimes the sole representative of this condition—that is, existing alone without any motor paralysis—is that embracing the means of communicating with the outer world by means of language spoken or written. Corresponding to, and usually but not always connected with, right motor paralysis we have the inability to use words in speaking, known as aphasia, aphemia, alalia, and others. The first of these names is the one most frequently used. Agraphia is the inability to use words in writing.
On the receptive side we have the inability to understand language as presented to the eye (word- or psychic blindness) or to the ear (word- or psychic deafness). A case of the former condition has already been spoken of. One still more singular was reported by Mdlle. Skwortzoff,37 where the patient, not being blind, could not understand letters presented to the eye, but could read with the fingers and understand raised letters like those used by the blind. In a case of the latter kind a man whose ears were normal, and who could distinguish different sounds, answered questions, but entirely at random, though he could read and understand what was written. All these defects are manifestly connected with a peculiar loss of memory, and hence the word amnesia is used sometimes to cover part of the group, and amnesic as an adjective to qualify aphasia.
37 Comptes Rendus de la Société de Biologie, 1883, p. 319.
It should, of course, be understood that the muscles are not paralyzed, so that glottis, lips, tongue, and fingers are capable of making the [p. 958] necessary movements to produce words, and, on the other hand, that the senses of sight and hearing are intact. Aphasia was confounded by some of the older writers with paralysis of these organs, and the whole grouped together under the name of alalia. Even now the distinction is not always clearly observed.
The act of speaking, according to Kussmaul,38 consists in three stages or processes: the preparation in the intelligence and feelings of the matter to be uttered; the diction, or the formation of the words internally, together with their syntax; the articulation, or formation of words outwardly, irrespective of their connection with one another in the matter spoken. Defects in the first condition have already been spoken of. In the entire absence of mind, as in the deepest apoplexy, aphasia can hardly be said to exist, and it is only later that it becomes manifest. If the second stage is defective, amnesic aphasia exists, and if the third, ataxic. In the great majority of cases of aphasia the loss of memory is the most important factor; and as this exists whatever be the mode in which it is desired to express the idea, amnesic aphasia is accompanied by agraphia. In those cases, however, in which the patient retains a few words, they are not always the same for speech and writing. Occasionally an instance is found where a person can write perfectly well and possesses complete intelligence, but is unable to speak a word. This is pure ataxic aphasia, and is certainly rare. An ataxic agraphia is less easy to detect, since the aphasic patient is likely to be paralyzed upon the right side, and thus unable to write, even if he remembers the words, until educated upon the left side.
38 Ziemssen's Cyclopædia.
There are many degrees and kinds of amnesic aphasia, and, in fact, every case is a study by itself. The slightest might be called physiological; at any rate, it is sufficiently common among people supposed to be well, and consists in the failure to recollect in time for use the name, most frequently of a person, but sometimes of a thing, which is really well known, is recognized at once if suggested, and perhaps returns spontaneously at a later period. Another person may forget only some words which are not recalled at any time, or parts of words. A man appeared among the out-patients at St. Bartholomew's Hospital who had his name written on a piece of paper, because he could not say it, but could carry on a long conversation. There were a few other words he could not say. The more complete cases have no vocabulary at all, or only a few words or syllables applied to all purposes, and perhaps an exclamation or two. In these cases the patient may know perfectly well that he is not expressing his ideas, and he may recognize perfectly well the word when it is told to him or reject a wrong one. If he be, as happens in nearly all cases, unable to pronounce the word after he has recognized it as the one he wished for, there is a combination of ataxic and amnesic aphasia. Incorrect or deficient words may be corrected or supplemented by gestures or intonation. “Yes” may do duty without confusion for “yes” or “no,” according to the tone.
Oaths may be retained, and sometimes an exclamation may be uttered with perfect propriety of application which cannot be repeated deliberately a moment afterward. This emotional use of words may be considered akin to the movement executed by paralyzed limbs under the [p. 959] stimulus of a movement taking place elsewhere, and may lead to an erroneous prognosis of recovery. This curious fact, that more or less automatic expressions are possible when deliberately-willed pronunciation is not, is a probable explanation for the observation which has occasionally been made that an aphasic patient is able to sing words which he cannot speak.
Paraphasia is the use of the wrong words, or of phrases which carry an entirely different meaning from that intended, as when Trousseau's patient receives a guest with politeness and invites her to be seated with the words “cochon, animal, fichue bête,” or an old paralytic, when a lady declines to drive with him, answers with great suavity, “It don't make any damnation to me whether you go or not.”
Word-blindness is more common than word-deafness, and is a frequent accompaniment of aphasia. Rostan, the well-known author of the work on softening of the brain, experienced an attack of aphasia lasting a few hours. The symptom which first attracted his attention was the inability to understand the book, by no means abstruse, which he was reading. He was, however, able carefully to observe his own symptoms, and made signs to be bled, which operation was followed by relief.
Gouty aphasia has been described in a man aged thirty-seven who on several occasions became aphasic, with recovery in a short time. This condition was connected with localized paralysis, and once with entire right hemiplegia. Afterward it was accompanied by convulsions. In the intervals the patient was in fair health.39 It is difficult to imagine the lesion in this case. The reporter speaks of “sudden blocking by a gouty thrombus,” but nothing is known of any thrombus which can disappear so rapidly. Ball40 describes twelve attacks of aphasia occurring within nine months, and accompanied by slight paresis and convulsive movements in the right hand. The patient suffered habitually from migraine. He supposes the cause to have been a temporary anæmia.
39 Brit. Med. Journ., Aug. 28, 1880.
40 L'Encephale, 1883, 2.
Aphasia may be entirely unconnected with motor paralysis, and is then likely to be of shorter duration, though just as complete. Most of these cases probably do not depend upon a lesion of the same kind as when aphasia is only one of several severe symptoms. It shows how delicate a function of the brain memory for words may be, and is possibly the result of a temporary malnutrition or a change in the vascular supply. It has been observed in various conditions of debility and after acute disease. Rostan was diabetic. It has been seen after chloroform narcosis, after santonin (5 cgr.), after fright, and is said to be one of the ordinary symptoms after the bite of venomous serpents. Aphasia and paraphasia may be met with in thorough bromization, and, naturally enough, may be part of the symptomatology of general paralysis. In other cases, even when it is the principal symptom, it depends upon an organic lesion, and is not infrequently the precursor of a more fully-developed attack. The diagnosis is of great importance, and other traces of paralysis should be carefully sought for. This symptom is far more common with occlusion of the vessels than with hemorrhage, though not unknown with the latter.41
41 Lancet, Oct. 11, 1884, p. 655.
By far the most common situation of the softening or hemorrhage which gives rise to aphasia is in the third left frontal convolution [p. 960] (convolution of Broca) or the white substance immediately underlying it. The island of Reil may be involved in some cases where but little damage is done to the third frontal.
In a respectable minority of cases aphasia may be associated with left hemiplegia. A case where a tumor in the third right frontal convolution was found in a case of aphasia is reported by Habershon.42 It is not stated whether the patient was left-handed. Some of these cases constitute those exceptions which prove the rule, inasmuch as the patient is left-handed, and Hughlings-Jackson has shown that the relationship of aphasia to the side which is congenitally pre-eminent, and which is in the vast majority of human beings the right side, is not destroyed by a partial education of the other side to such acts as writing or using a knife.
42 Med. Times and Gaz., 1881, i.
A lesion in the pons may give rise to aphasia or something closely resembling it, but it is probable that a careful distinction of true aphasia, both amnesic and aphasic, from paralysis or inco-ordination of the muscles of speech, would reduce the number of these cases, and bring the symptom into closer relations with the usual cortical lesions.
A case of congenital aphasia with right hemiplegia has been described.43 When six years old the boy was well developed, though less so on the paralyzed side; intelligent; heard well, but could say only a few words, and those badly. Whatever the lesion, which is thought by the author to have been in the speech-centre, but which may not improbably have been in the pons, it is interesting, as showing that the development of the speech-centre is certainly not accomplished by education.
43 Centralblatt f. d. Med. Wiss., 1873, p. 299.
Post-paralytic chorea is an affection the nature of which is indicated by its name. As the hemiplegia disappears, irregular movements are developed in the paralyzed limbs, sometimes closely resembling ordinary chorea, and at others consisting of irregular movements, as closing and spreading of the fingers, with curious and bizarre stiffenings, extensions, and contractions, sometimes known as athetosis, or in others still a tremor resembling paralysis agitans. These usually cease during sleep. It is very apt to be associated with hemianæsthesia more or less complete, though this may be represented by only a certain amount of numbness. A hemiathetosis has been observed to be gradually developed from a post-hemiplegic hemichorea of the more ordinary form.44
44 Archiv für Psychiatrie, xii. 516.
This affection is not a common one, and Weir Mitchell states that it is common in inverse proportion to the age. He thinks it possible that some of the congenital choreas may be the result of, or at least closely connected with, intra-uterine cerebral paralysis. It remains for years or for life. In the absence of history such a case might present difficulties of diagnosis from the more usual hemichorea, which is not infrequently accompanied by considerable weakness of the affected side.
The temperature in the early days of both hemorrhage and embolism has been described. At a later period of the hemiplegia it remains in the neighborhood of normal. The temperature of the affected side is often higher than that of the sound one for an indefinite period, but in many cases sinks below if atrophy takes place. The time at which the change occurs is extremely variable. Out of ten cases reported by Folet,45 in two of them for three years and one year after the attack the paralyzed [p. 961] side was eight-tenths and six-tenths of a degree respectively the warmer. In three others, of twenty months, four and six years, it was the same on both sides, and in the remaining five the paralyzed limb was a little the cooler. In the last eight there was more or less atrophy.
45 Gaz. hébd., 1867.
The coincidence of rise of temperature with vascular relaxation has already been noted under the head of Cerebral Hemorrhage. It is not difficult to explain why a vascular paralysis in a comparatively well-nourished limb, especially when the heart is vigorous, may, by allowing a larger amount of warm blood to circulate, raise the temperature, when the same paralysis with atrophied muscles, weak heart, and impaired general health, merely furnishes a larger reservoir in which the slowly-moving blood may be cooled. The accompanying charts represent the difference of temperature between the two sides in two cases of hemiplegia, the first, O. G. T. (Fig. 41), from embolism, and the second, J. B. (Fig. 42), from hemorrhage, the observation being made within two or three weeks of the attack. The dotted line is from the paralyzed side. A subjective feeling of coldness is not uncommon in paralyzed limbs.
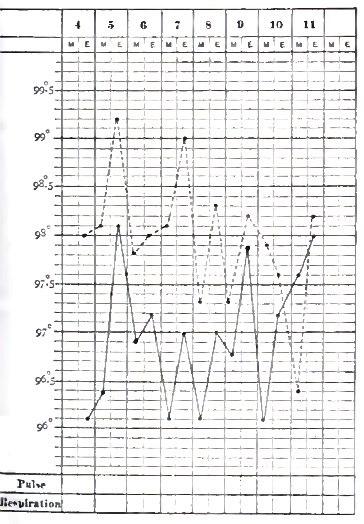
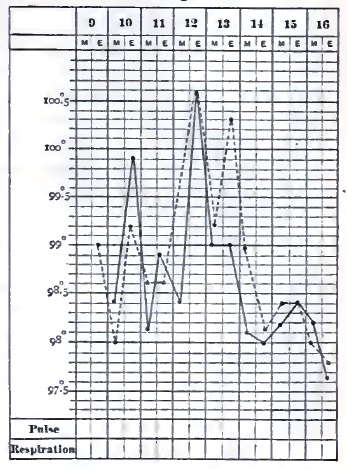
The modifications undergone by the urine in a case of cerebral hemorrhage are increase of quantity amounting to polyuria, the urine becoming limpid and afterward returning to the usual color; a diminution in the quantity of urea coinciding with the fall of temperature, and afterward a return to the normal or even above it. When this augmentation is considerable, it constitutes at the same time with a marked elevation of temperature an unfavorable prognostic sign.46 In a case under the observation of the writer, probably of thrombosis, the acid urine has been [p. 962] remarkable for the amount of mucus contained in it, so that it pours from one vessel to another like white of egg. There is a small amount of pus, but no vesical irritation whatever.
46 Ollivier, Archives de Physiol., 1876.
Since the trophic centres for the muscles are situated in the spinal cord, cerebral hemiplegia, which does not cut off their connection, does not produce the rapid wasting seen in some cases of spinal paralysis, unless descending degeneration involves the anterior gray columns. The limbs preserve their fulness for a time, although the muscular masses become flabby and slowly atrophy for want of use. This atrophy, however, seldom becomes extreme. The skin of the hands becomes dry, the folds at the knuckles disappear, and the hand loses its expression, looking more like a stuffed glove. The change, however, is not much greater than may be seen in a hand kept for a long time in a bandage. The growth of the nails is retarded, as may be seen by staining them with nitric acid.
If there is any tendency to œdema, as when nephritis is complicated with hemiplegia, the swelling is likely to be much greater upon the paralyzed side. In the adult, of course, there can be no question of the growth of limbs, but when a child becomes hemiplegic from cerebral disease, the limbs grow more slowly and remain smaller, as in a case of ordinary infantile palsy or anterior poliomyelitis.
Much importance has been attached to the fact that large sloughs form with great rapidity upon the nates of the paralyzed side, and Charcot says that this tendency is greater than can be accounted for in any mechanical way. He therefore thinks that a direct trophic influence of the brain upon nutrition is shown. At the very most, however, that can only be a contributory cause, and the freedom of other portions from a similar condition—and that, too, in regions farther removed from the centres of circulation—makes it highly improbable that anything more is necessary to account for it than the less sensitiveness of that side to irritation from urine, roughnesses in the bed, or pressure, and hence neglect. The writer, among a very considerable number of hemiplegias, fatal and otherwise, does not remember to have seen a well-marked case of the kind. Scrupulous cleanliness and changing the position sufficiently often make the preference for the paralyzed side a very slight one.
Arthropathies, consisting in a vegetating, and sometimes an exudative, synovitis, and accompanied by swelling, redness, and pain, are sometimes observed, especially in the upper extremity. They do not appear until fifteen days or a month after the attack.
The most significant change which occurs in the course of a hemiplegia is the development of increased reflexes and rigidity and contracture. After some weeks or months, during which the aspect of the case has not essentially changed, the limbs remaining in the same condition, it will be found on examination that the patellar reflex has become quite energetic, and ankle clonus developed upon the paralyzed side; the arm reflexes from the triceps, biceps, and supinator longus are much exaggerated. This has the same meaning as when similar phenomena are found with spinal disease, and signifies descending degeneration of the postero-lateral columns of the spinal cord, the crossed peduncular tracts. This degeneration may sometimes be traced completely down from the situation of the lesion in the cortical motor centres through the basal ganglia, crura, decussation, and cord. The fuller development of this condition is the [p. 963] contracture or rigidity, which was at one time referred to secondary changes taking place in the neighborhood of the original lesion, as well as to a purely reflex action having no relation to the degeneration of the cord.
The arms are usually flexed at the elbow, the wrists on the arm, and the fingers in the hand. Sometimes, however, the arm is straight. The leg, which is not always affected to the same extent, is generally in extension, though the toes are likely to be flexed. Attempts to move the limbs are resisted strongly, and in such a way as to show the reflex nature of the phenomenon. If an attempt be made to open the fingers of a contractured hand slowly and carefully, it can be often accomplished and the hand held open with but little pressure, but if it is twitched the fingers resist like a spring. The violent attempt to overcome rigidity is often painful.
In some rare cases rapid atrophy of the muscles of one limb may take place. This has been found to coincide with extension of degenerative changes in the cord to the anterior gray columns.
Late rigidity is an unfortunately clear symptom. There is little if any hope of complete recovery of the use of the limb after it has made its appearance, though it does not prevent walking. After long-continued contracture the activity of the muscles diminishes, but the increase of connective tissue and changes in the joints hold the limb in its fixed position, and the contracture is a more passive one. The electrical reactions of the muscles and their nerves in cerebral hemiplegia are not materially altered, but the neuro-muscular irritability may be somewhat increased for a time by the irritating influence of the cerebral lesion.
In most cases of flaccid cerebral hemiplegia the electrical irritability is somewhat decreased, though retaining the normal character with both currents. Since the muscles and their nerves retain their connection with the spinal nuclei which are their trophic centres, and these nuclei are uninjured, their nutrition does not undergo the changes which affect electric excitability.
When descending degeneration takes place there may be found, coinciding with increased reflex activity and contracture, increased sensitiveness to the electric currents. If the degeneration extend to the anterior columns, as happens in rare cases, the muscles waste rapidly and exhibit the reactions of anterior poliomyelitis—i.e. degenerative.
What has just been said applies to the muscles paralyzed by a central lesion. If, however, with or without a complete hemiplegia, a limited lesion, as in the pons, affects the nucleus of a nerve, the peripheral distribution of that nerve is cut off from its nutritive centre, and it undergoes the usual changes which lead to the reaction of degeneration, so that, in some unusual forms of paralysis, the two kinds of reaction, normal and degenerative, may be present in different sets of muscles.
DIAGNOSIS.—The apoplectiform attack due to hemorrhage or occlusion of the cerebral arteries is to be distinguished from narcotic poisoning, specially by opium or alcohol, or by coal gas; epilepsy with its succeeding coma; uræmia (so called) or cerebral symptoms connected with renal disease; comatose form of pernicious intermittent; diabetic coma; sunstroke; hysteria, and various other forms of intracranial disease, especially meningitis; concussion and compression of the brain, which often [p. 964] involve hemorrhage; the apoplectiform attacks of intracranial syphilis and of general paralysis, as well as the congestive attacks (coup de sang, rush of blood to the head).
The first of these distinctions is, in a practical point of view, among the most important and often the most difficult, so that distinguished authorities insist not only on the difficulty, but impossibility, of making a positive diagnosis in every case. The physician who is most familiar with all the different conditions which may cause coma is least likely to jump at a conclusion.
Persons are constantly being picked up in the street partially or wholly unconscious, or found alone in a room without history and away from friends. The physician must then form his opinion from the present condition, which without a history may be very obscure, though with one it might present no difficulty. An empty laudanum- or whiskey-bottle may be of assistance, the former of much, but the latter of less. The smell of the breath may give a hint, but even if the smell of alcohol be detected, considering the widespread belief in its virtues as a panacea, it may be as well the result of amateur therapeutic attempts as an indication of the cause of the attack. Neither does it follow that because a man has been or is drunk he has no organic disease in his brain. Alcohol should simply make us more careful to examine for possible injuries. In regard to both these poisons—and in fact in the diagnosis of these conditions generally—the first thing to be sought for, after assuring one's self that the patient can breathe and is likely to do so for a few minutes, is some evidence of hemiplegia. This is not so easy as it might appear at first sight, since the general muscular relaxation may be so complete as to cover up local manifestations. The face, however, may show inequality in its lines or one cheek flap more loosely than the other. The patient is not likely to undertake voluntary movements at the request of the physician, but he may make semi-voluntary ones if annoyed by the examination. The flaccidity of the arms may vary. Irregularity of the pupils is a piece of evidence to be received with some caution, as it may be habitual or the result of disease in the eye. Conjugate deviation of the eyes and head is a form of paralysis, or sometimes of unilateral spasm, which when present is of great significance. In opium-poisoning—and to a less extent in alcoholic coma—the pupils are much contracted, while they are not always so in apoplexy. Respiration is usually much more rapid in apoplexy than in opium-poisoning, and this, in the absence of distinct signs of hemiplegia, would be one of the most important means of distinction. The pulse is more nearly normal in frequency, while that of opium is either slow and hard or more often frequent and feeble.
After the time for the initial depression has passed, rapidly-rising temperature is very strong evidence in favor of apoplexy. If the patient be only partially unconscious and able to protest against being handled, to make some short answers, or even be inclined to be combative, this is not to be taken as evidence of alcohol. Hemiplegia may then be noticed. This condition of excitement may be observed in the early stage of an apoplectic attack before it deepens into coma. Unfortunately, when the lesion is situated in certain portions of the brain, as in the extremities of either the frontal or occipital lobes, there may be no paralysis, but then also there is less likelihood of the extreme symptoms we are supposing [p. 965] to be present. In the cerebellum, however, the symptoms may be very severe without hemiplegia, and the diagnosis correspondingly difficult. Vomiting, not caused by the presence of large quantities of food or liquor, and persisting after the stomach is once emptied, would be of some value in this case, but it would often be necessary to wait for a diagnosis. Cerebellar hemorrhage is, however, a very rare accident, and cerebellar embolism sufficiently large to cause apoplectiform symptoms still more so. A limited lesion in the pons may cause gradually-increasing stupor without distinct paralysis.
Chloroform, especially if swallowed, and chloral might possibly give rise to difficulties in the way of diagnosis, and would have to be distinguished on the same general principles as alcohol and opium.
The poisonous gases arising from burning coal, consisting chiefly of carbonic oxide and dioxide, or illuminating gas, consisting of carburetted hydrogen with a little carbonic oxide, cause unconsciousness, coma, and sometimes convulsions and vomiting. In case of a person found unconscious in bed the possibility of poisoning by one of these should not be lost sight of, nor, on the contrary, assumed to be a cause without investigation. A case has been reported where, after acute poisoning by coal gas, there occurred, presumably as the result of local anæmia, alternate paralysis, convulsions, and aphasia.47 The new water-gas process is said to furnish a product considerably richer in the poisonous carbonic oxide than that now most in use.
47 Boston Med. and Surg. Journal, Nov. 26, 1885.
The stupor succeeding an epileptic convulsion resembles apoplexy, and the fact that cerebral hemorrhage may be accompanied by some convulsions increases the possible similarity, but it requires only a short time for epilepsy to make itself manifest, either by a renewal of the convulsions or a rapid recovery without paralysis. According to Trousseau, however, many attacks of so-called congestion of the brain are really epilepsy. Puerperal eclampsia comes under the same head, but when convulsions are violent they may give rise to actual hemorrhage. Unilateral epileptiform convulsions are likely to be dependent on organic disease of the brain, usually not of the kind at present under consideration, but more frequently of a tumor.
Among the cerebral symptoms connected with renal disease, and not involving organic change in the brain, may be found unconsciousness, deep coma, and convulsions. It is obvious that the presence of a few hyaline casts and a little albumen will not decide the matter, since these may be present from many causes, and especially the changes in the circulation accompanying apoplexy. Neither will the most indubitable evidence of Bright's disease, such as dropsy, hypertrophy of the heart, rigid arteries, with fatty and waxy casts in the urine, do so, for, as we have already seen, not only is there nothing in the presence of nephritis to exclude apoplexy, but the very form, the interstitial, which, from the supervention of coma not preceded by other very severe symptoms, most nearly counterfeits apoplexy, is also the most likely to give rise to actual cerebral hemorrhage. The extreme and frequent cephalalgia which is so distressing a symptom in cases where there is no cerebral lesion may also be the precursors of hemorrhage.
If we have a history, the gradual onset of the symptoms, deepening [p. 966] unconsciousness without any paralytic or unilateral symptoms, especially if accompanied by a diminution in the amount of urine or contained urea or a marked change in the character of the casts, renders it probable that we are dealing with so-called uræmia alone. In the absence of history hemiplegia must be the chief dependence, but it would not be difficult to imagine a case of embolism of the basilar artery with softening of the pons which would defy a positive diagnosis.
Pernicious intermittent fever appears in a so-called comatose form, which, if it were to be accompanied, as in a case related by Bemiss in the second volume of this work, by paralysis of one arm, might present difficulties of diagnosis. If it were known that the attack had been only of short duration, the elevation of temperature would, as in the case of sunstroke, decide in favor of the fever, but if it had lasted some hours, this symptom would be of no value, as the temperature may rise to an equal height in apoplexy.
Diabetic coma is a much less common affection than apoplexy. The peculiar odor (aceton) of the breath, if present—which is not always the case—might be diagnostic. The peculiar long and deep respirations would awaken suspicion which would be confirmed by an examination of the urine.
Sunstroke, with its sudden onset, complete unconsciousness, and rapidly rising temperature, may present a very close resemblance for a while to apoplexy, and in fact has been known as heat apoplexy. Age, temperature, and surroundings would give strong probabilities one way or the other, and if the temperature of the patient were at first below the normal and did not rise for an hour or two, it would certainly not be sunstroke and would be apoplexy, while if the temperature were very high a few minutes after the patient had been observed to cease work or become unconscious, the evidence in favor of sunstroke would be equally strong.
It might appear that hysteria need hardly enter into our consideration, and could hardly be mistaken for apoplexy, but most experienced physicians could relate instances where serious organic disease has been made light of under the name of hysteria, and many inexperienced ones could tell of the opposite and safer mistake. An occasional case of deep coma presents itself where, although the age and sex of the patient awaken strong suspicion, we cannot at once be sure that no organic lesion is present; and if, in addition, the patient should be affected with hemiplegia—a combination which, although rare, is by no means beyond the limits attainable by this perplexing disease—an immediate positive diagnosis would be difficult. Absence of facial paralysis, which might be made manifest by some irritation like pinching or an attempt to raise the eyelids, would be of much value under these circumstances. The hysterical physiognomy might be well enough marked to be almost conclusive by itself. The urine and feces are not likely to be passed involuntarily in hysteria, as they are in apoplexy.
Injuries to the head should be carefully looked for in any case with unknown history. Actual fracture, which perhaps leads to no depression of bone, may give rise to hemorrhage, probably meningeal, which will cause the usual symptoms, and a shock which is not accompanied by fracture may cause considerable laceration of the brain with consequent hemorrhage. In the latter case, however, unless the brain be already [p. 967] predisposed by arterial disease, the laceration and hemorrhage will not be extreme and the symptoms will be those of concussion. The diagnosis can hardly be said to be between hemorrhage and concussion, but whether the hemorrhage be the result of concussion—a question which can hardly be answered without the history and observation of the further progress. Cuts and bruises may result from a fall caused by the shock, and pericranial ecchymoses may result from cerebral hemorrhage through the vaso-motor system without the intervention of accident.
Rapid meningitis of the vertex, with predominance of the effusion upon one side, may closely simulate compression from hemorrhage. At the base, by the time it has become severe enough to cause unconsciousness, it is likely to have affected the ocular muscles, and perhaps given rise to other paralyses less regular in their distribution than the ordinary hemiplegia. Ophthalmoscopic examination would be of value in these cases if—which is not very likely to happen—there is no history. The temperature in meningitis is more likely to be irregular and less rapidly and uniformly rising than in a severe hemorrhage or occlusion. In many cases emaciation, dry tongue, and constipation with sunken abdomen will testify to a previous illness, while after a few hours' observation the progress of the case will make the diagnosis more clear.
In differentiating cerebral hemorrhage or ordinary embolism from the apoplectiform attacks met with in syphilitic intracranial disease, it is rather a question of etiology than of diagnosis in the narrower sense, since unconsciousness and hemiplegia coming on with syphilis are often dependent upon a condition of the vessels closely resembling that which gives rise to the ordinary forms; that is, we are dealing in either case with an endarteritis which has furnished the basis for the deposit of a thrombus, and the question is, Of what nature is the endarteritis? It is obvious that this is only to be answered by a knowledge of the history, not necessarily of a primary or secondary lesion, but of previous disease. The syphilitic taint may often be suspected from the irregularity of the paralysis, the cranial nerves, for instance—especially the ocular—being much more frequently affected in syphilitic than in ordinary hemiplegia. After partial recovery or amendment the characteristics of irregularity and changeableness will be more strongly marked.
The pathology of hemiplegia and apoplectiform attacks, often transitory, in the course of general paralysis is not certain, but it is probable that they are due to sudden congestions of regions of some extent already in a condition of chronic periencephalitis or to cerebral œdema. The question of the existence of the previous disease can only be settled after the return of the patient to consciousness. Usually, these attacks are not of the severest kind, and are not necessarily attended with loss of consciousness, which, when it occurs, is usually not of long duration. An apoplectiform attack occurring in a young or middle-aged person who has neither cardiac nor renal disease, rapidly recovered from or changing its character, should awaken strong suspicions of either general paralysis or syphilis, or both.
The characteristic of the so-called congestion of the brain, or coup de sang, is a close resemblance to ordinary apoplexy, but without hemiplegia and usually with a rapid and complete recovery. A diagnosis from apoplexy cannot be made at once, except so far as hemiplegia can be shown to be either distinctly present or absent.
[p. 968]As has already been stated, the doctrine of the dependence of real apoplectiform attacks upon cerebral congestion alone has been vigorously combated by distinguished clinicians; and certainly the diagnosis of congestive (and the same may be stated even more strongly of so-called serous) apoplexy should never be made until after the rigorous exclusion of every other possibility.
After the severer apoplectic symptoms have passed off, and in cases where they have never been present, the diagnosis, so far as most of the conditions mentioned above is concerned, is divested of many of its difficulties when we are dealing with cases of well-marked hemiplegia. The chief points left are the distinctions from the apoplectiform attacks of general paralysis, cerebral syphilis, and cerebral tumor, which are to be made as already pointed out.
Slighter and more localized paralyses, such as may occur with limited lesion of the pons or where a hemorrhage having a large focus in the substance has escaped under the membranes and presses on some cranial nerve, would present more difficulties. Paralyses which are very limited, and at the same time complete, are not likely to arise from hemorrhage or embolism, though it is possible that they may do so, but the diagnosis is to be considered rather under the head of local palsies than of cerebral disease. General rules cannot be laid down for slighter cases, and each case must be diagnosticated for itself. In many of them the electrical diagnosis would be of great value and often decisive.
Hysteria remains, as always, ready to counterfeit anything, but the following case shows that the error is not always on that side: F. S——, a young woman, was brought to the hospital, apparently conscious and understanding what was going on, but unable or unwilling to speak or to protrude her tongue. There was no history except that she had probably been in the same condition for thirty-six hours. There was paralysis of the right side, including the face, and marked anæsthesia of the same side, quite distinctly limited at the median line; temperature 97.8°, pulse 60, respiration 20. The next day she seemed perfectly conscious, but did not speak. The faradic brush to her face caused loud outcries, and the facial paralysis was diminished. This condition remained nearly the same, the patient appearing half conscious, but passing urine in bed. Four days later there was marked diminution of sensation and motion on the left (previously sound) side, as well as the right. The note two days later was, “Shuts and opens her eyes when told, and moves eyeballs in every direction, but there is apparently no voluntary motion except slight of the head. Incontinence of urine and feces.” A week later the temperature rose to 100.4°, pulse 140, and she died. The autopsy showed red adherent thrombus in the left carotid, extending into the cerebrals, with extensive anæmic necrosis of the cortex and a part of the corpus striatum. On the right there was a grayish thrombus and softening of the cortex, while the great ganglia were not affected.
A woman of thirty-two had repeated attacks of loss of consciousness and somnolence lasting several hours, but leaving her apparently well. The case was considered hysteria, but the patient died in a similar attack. Degeneration of the cerebral arteries and hemorrhage were found.48
48 Christian, Centralblatt f. d. Med. Wiss., 1873, 864.
Post-paralytic chorea might present difficulties of diagnosis from [p. 969] hysteria or malingering, though the difficulty is quite as likely to be on the other side.
The diagnosis, however, is not complete until the lesion is located with some precision and its nature determined, although it must be confessed that when we have got as far as this the diagnosis in most cases is of more interest to the physician than to anybody else, except to a slight extent for prognosis, so that the event may be anticipated by a few hours. As to the localization of the lesion, recent experiments and observations, involving not only lesions of the kind we are here discussing, but tumors and injuries as well, permit this to be done with a reasonable degree of certainty. The general article on Cerebral Localization may be referred to by the reader for the minuter points, but certain groups of symptoms may be indicated here which are available to some extent before the complete return of the patient to consciousness.
In the vast majority of cases the lesion is situated upon the side of the brain opposite to the paralysis, except in some instances of cerebellar lesion, while in the peculiar form known as alternate paralysis due to lesion of the pons it is on the opposite side to the paralysis of the limbs and on the same side with the facial. It should be distinctly stated, however, that there are exceptions which are inexplicable on the present basis of cerebral anatomy. It is well known that only a part of the motor tracts cross to the other side of the cord at the decussation, and also that the proportion between the fibres which do and those which do not cross is a variable one. It has been suggested, in some cases of the kind mentioned, that all the motor fibres, instead of only a minority, as is usual, pass down on the same side of the cord as their origin. This has not been demonstrated. The number of such cases are so small that it need not be taken into account in diagnosis, and if the practitioner should make a mistake on this basis, he will have the recompense of knowing that he has assisted in a very rare case, in which it was next to impossible for him to be right. This condition is said to be found more frequently when the brain lesion and paralysis are on the right side.
Severe pain in the head, followed by gradually but rapidly deepening coma and paralysis of one side, becoming more and more complete, probably means a hemorrhage into or just outside of the great ganglia and involving a large extent of one of the hemispheres.
If there have been moderate loss of power or complete paralysis lasting some hours, with, afterward, sudden loss of consciousness and general muscular relaxation, with sudden fall, soon followed by rapid rise, of temperature, it is very probable that a hemorrhage has broken through into the ventricles or beneath the membranes, and is still going on.
Rapidly-deepening unconsciousness, with general muscular relaxation and gradual manifestations of more paralysis on one side than the other, may come from meningeal hemorrhage.
Very sudden and complete hemiplegia without prodromata, with deep unconsciousness coming on rapidly or suddenly, but a little after the paralysis, is likely to denote the occlusion of the middle (and perhaps anterior cerebral) artery of the opposite side at a point sufficiently low down to produce extensive anæmia of the motor centres along the fissure of Rolando as well as the underlying great ganglia.
[p. 970]Aphasia with hemiplegia, often without the slightest disturbance of consciousness, is in a considerable proportion of cases connected with a lesion of the third left frontal convolution, and in a somewhat larger proportion with the frontal lobes in general and the island of Reil. This lesion is in a great majority of cases occlusion of the artery. Difficulty of speech, connected with difficulty of swallowing and associated with a certain amount of amnesic aphasia, has been found with lesions of the pons. As aphasia, however, may occur without any fatal lesions at all, it is not certain in all these cases that the obvious lesion of the pons is a direct cause of all the symptoms.
Word-blindness is associated, according to a case reported by Skworzoff and a few others,49 with a lesion of the angular gyrus, pli courbe (P2 of Ecker), and word-deafness with a lesion of the first temporal (T1). These localizations agree with those experimentally determined.
49 West, Brit. Med. Journ., June 20, 1885.
Conjugate deviation is of importance as a localizing symptom, chiefly because it may be manifest when other signs of hemiplegia are difficult to elicit. I do not find it mentioned in twenty-seven cases of cerebellar hemorrhage not included in the table of Hillairet, but it is not infrequent with lesions of the pons; and when the lesion is in the lower third, it is in the opposite direction to that described as usual with lesions of the hemispheres.
Hemianæsthesia involving the organs of special sense, unilateral amblyopia, and color-blindness is supposed to be connected with a lesion of the posterior third of the internal capsule, or the thalamus in its immediate vicinity, sometimes also with a lesion of the pons. Bilateral hemiopia—blindness of the corresponding sides of both eyes—is apt to be connected with a lesion of the occipital lobe of the opposite side. Rendu and Gombault remark that hemianæsthesia of the limbs and face may be met with in certain lesions of the cerebral peduncles, but in this case the higher special senses (sight, smell) remain unaltered. Hemichorea points to the same localization as the more complete hemianæsthesia.
Alternate hemiplegia is due to a lesion of the pons upon the side of the facial paralysis, and opposed to the paralysis of the limbs and in the posterior or lower half. Care should be taken not to confound this with the accidental addition of a facial paralysis to a hemiplegia of the other side.
Irregular ocular paralyses are very likely to be due to lesion of the same region. In some of these forms an investigation of the electrical condition with reference to the presence of the degeneration reaction may be of great assistance.
With extensive lesions profound coma and relaxation without distinct hemiplegia are likely to be due to injury of the pons. A thrombus of the basilar artery may lead not only to rapid, but even to sudden, death. A phthisical patient died suddenly while eating his supper, and a thrombosis of the basilar artery, with softening of the pons, was found. Of course the lesion must have been of older date.50 Bright51 thought that when symptoms pointing to disease of the intracranial vessels were present the diagnosis was confirmed, and the location of the lesion in the vertebral arteries rendered highly probable, by a persistent occipital [p. 971] pain. In the upper part of one side of the pons the hemiplegia is not alternate, but of the ordinary form.
50 Bull. de Société anatomique, 1875.
51 Guy's Hospital Reports, 1836.
Any extensive lesion of the medulla must cause death so rapidly as almost to defy diagnosis, but such rarely occurs. The very rapid termination of certain cases of hemorrhage into the pons and cerebellum is due to the escape of blood into the fourth ventricle and consequent compression of the medulla.
Lesions of the lower and inner part of the crus are indicated by paralysis of the third nerve of the same, and hemiplegia of the opposite side of the body.
Obstinate vomiting, severe occipital headache, and vertigo, with or without a distinct paralysis, render a cerebellar hemorrhage probable, though no one of these symptoms is necessarily present or pathognomonic. Vomiting is very much more common with cerebellar hemorrhage than with cerebral. Ocular symptoms, like nystagmus and strabismus, accompany cerebellar lesions.
A difference in the temperature of the paralyzed and non-paralyzed sides, when amounting to one and a half to two degrees and lasting for a long time, is thought by Bastian to indicate a lesion of the optic thalamus.
The severe and rapid sloughing of the nates sometimes seen in rapidly-fatal cases is stated by Joffroy to be most frequently connected with a lesion of the occipital lobes.52
52 Arch. gén., Jan., 1876.
It is plain, from what has been said about the symptoms of the different kinds of lesion, that a distinction may be often very difficult, and at times impossible; and in this connection all observers are agreed, the apoplectiform shock, the hemiplegia, and the slighter attacks being common to two or three lesions. The diagnosis can be made, if at all, only by the consideration of more or less secondary symptoms and the careful weighing of the various probabilities against each other. Most of the statements of differences of symptoms are only relatively true.
A glance at the nature of the pathological processes involved may serve to systematize our observations.
Hemorrhage is a sudden accident, with a severity increasing as the amount of effusion increases. It has been prepared for by arterial disease, but this disease is one which may have no previous symptoms. It is at first an irritative lesion.
Embolism is a sudden attack which may be as severe at first as even a few minutes afterward. It is also prepared for by disease of other organs, which may or may not have symptoms according to the origin of the embolus. As embolism affects especially those regions where the motor centres are spread out, while hemorrhage attacks more frequently the conductors in their locality of concentration, the paralyses arising from the former affection may be more narrowly limited.
Thrombosis is a gradual affection, which may, however, manifest itself suddenly, from the obstruction reaching a certain point and suddenly cutting off the supply of blood. This also depends on previous disease which has more or less definite symptoms.
The severity of the attack is not conclusive, though the completely developed apoplectic attack is more frequent with hemorrhage. Rapidly [p. 972] increasing severity, especially if there have been prodromata, is in favor of hemorrhage. Convulsions, early rigidity, and conjugate deviation of the eyes of the spastic form, especially if afterward becoming paralytic, are strongly in favor of hemorrhage, and the latter possibly conclusive. Hughlings-Jackson states that he cannot call to mind a single case of hemiplegia from clot in a young person in which there were not convulsions.
Sudden paralysis without cerebral prodromata, unconsciousness, or pain can hardly be anything else than embolism; but, unfortunately for diagnosis, the initial paralysis from the embolus may be slight, and afterward added to by the secondary thrombus, so as to put on the appearance of more gradual approach.
Aphasia, and especially aphasia associated with but little or no paralysis, is very much more frequent with embolism than with hemorrhage.
The temperature, if we could always have it recorded from the very beginning, might be of value, as the initial depression is said to be less with embolism than with hemorrhage, but Bourneville,53 who lays down this rule, gives so many cases where no great depression occurred with hemorrhage that it cannot be considered decisive. Besides this, we are not likely to get the information at the time it is of the most value.
53 Op. cit.
Etiological information may have a very practical bearing on this part of the diagnosis. Age gives a slight amount of predominance to the chances of hemorrhage, and youth a considerably greater one to the chances of embolism. Interstitial nephritis with hypertrophy of the heart, after the exclusion of uræmia, gives a strong probability in favor of hemorrhage. Valvular disease of the heart, especially a more or less recent endocarditis, is strongly in favor of embolism. A feeble action of the heart, slow and irregular pulse, are more likely to be connected with thrombosis.
Atheroma and calcification, as detected by examination of the visible and tangible arteries like the radial and temporal, is a condition either connected with the periarteritis aneurysmatica which gives rise to hemorrhage, or one which furnishes a suitable spot for the deposition of a thrombus; hence it can be considered conclusive in neither direction.
Arcus senilis, even of the fatty variety, can only show some probability of arterial degeneration.
Retinal hemorrhage, if present, favors the presence of a similar cerebral lesion, but nothing can be argued from its absence. Landesberg54 has reported a case in which embolism of the central artery of the retina, easily diagnosticated by the ophthalmoscope, preceded by a few days a similar accident in the middle cerebral; and Gowers55 another in which the two arteries were occluded simultaneously.
54 Archiv für Ophthalmologie, xv. p. 214.
55 Lancet, Dec. 4, 1875.
If a sudden paralysis arises in connection with a septic process, we may diagnosticate an embolus with a good deal of confidence; but it is not unusual to meet with small abscesses of septic origin which have given rise to no special symptoms whatever, or only to such as are covered up by the more general constitutional ones.
PROGNOSIS.—The prognosis quoad vitam of cases of apoplexy still in the unconscious state is based upon the general severity of the symptoms [p. 973] as indicated by general muscular relaxation, or, at a later period, the extent of the paralysis, the amount of affection of the heart and respiration, and especially the progress during the first few hours. Too much weight should not be placed upon a very slight improvement at first, since this often takes place in cases soon to prove fatal.
Stertorous respiration with perfect tolerance of mucus in the throat, absolute loss of the reflexes, and immobility of the pupils signifies profound depression of the organic nervous centres, and is consequently of unfavorable augury.
The temperature is a valuable guide. In proportion as it moves steadily and rapidly upward is the prospect of an early fatal result. A person may die during the initial fall of temperature, but in such a case there would hardly be need of a prognosis.
In general, the prognosis from hemorrhage, supposing the symptoms to increase in severity for an hour or two, is worse than that from occlusion.
Age, aside from the fact that it makes hemorrhage more probable than occlusion, is not of great importance in prognosis, certainly not out of proportion to the general impairment of vigor in advanced years.
A renewal of the hemorrhage within a few hours cannot be predicted. It may be indicated by another fall of the temperature, which, if it have been previously on the rise, renders, of course, the prognosis more unfavorable.
After recovery, more or less complete, from the apoplectic condition the prognosis is favorable, for a time at least, except so far as one attack may be looked upon as the forerunner of another. After the temperature has reached a sort of standstill in the neighborhood of normal, its subsequent rise will furnish among the earliest indications of an approaching fatal termination.
Urinary trouble, retention, incontinence, or, much more, cystitis, is to be looked upon as a complication which materially increases the gravity of the situation. Bed-sores or abrasions may be placed in the same class, except that the early and extensive sloughing of the nates described by Charcot is of almost absolutely fatal significance.
After some days or weeks the progress of the paralysis either toward better or worse may be exceedingly slow, and as time goes on the danger to be apprehended from the latter becomes less and less.
When paralysis takes place in young persons and the primary attack is recovered from, it is doubtful if the chances of a long life are materially diminished. A case has already been referred to in this article where the consequences of a cerebral hemorrhage occurring in infancy were found in a woman of eighty-three in the form of atrophied limbs and an old pigmentary deposit in the brain.
Hemorrhage into the cerebellum would appear, from statistics, to be exceedingly fatal, but it is certain from old lesions occasionally found that it is not absolutely so, and its apparent severity is partly caused by the fact that it is very seldom diagnosticated except at the autopsy.
The prognosis quoad restitutionem ad integrum cannot be made to advantage at an early period. After the immediate danger to life has passed it is safe to say, if pressed for an answer, that it is highly probable that some recovery from paralysis may take place, but that it is [p. 974] highly improbable that it will be absolutely complete, and just how far improvement may go it is impossible to predict with accuracy at first. Time must be given, in the first place, for pressure to subside, compressed nerve-fibres to be restored, and for such collateral circulation as is possible to be established. How recovery takes place beyond this it is not easy to say. It is hardly supposable that any considerable portion of nerve-structure is renewed. A certain amount of substitution, by which one part of the brain takes up the functions of another part, is among the most plausible suppositions; but how this is accomplished it is hardly worth while in the present condition of cerebral physiology to speculate.
Practically, it may be said that physicians are apt to consider a paralysis absolute at too early a period, while the patient and his friends continue to hope for a complete restoration after it is evident that no really useful increase of power is to be looked for. Weeks, and even months, may elapse before any return of motion can be perceived in cases which are really susceptible of considerable improvement, and a year most certainly does not cover the limit of the time during which it may go on.
The most unfavorable symptom, one which probably precludes all hope of useful recovery in the limbs affected, is contracture, heralded for a time by increase of the deep reflexes, indicating degeneration of the motor tract in the white substance of the cord. Until this begins, certainly for many weeks, the patient may be fairly encouraged that some improvement is possible, though after a few weeks the chances diminish as time goes on. In the rare cases where the muscles undergo rapid wasting the prognosis is, if possible, worse still. The localization of the lesion after the early symptoms are passed does not greatly influence the prognosis.
A rapid recovery taking place in either hand or foot, and especially of the hand first, without corresponding improvement in the other limb, is of unfavorable import for the latter, and, in general, the prognosis is not exactly the same for both limbs involved. In the rare cases of hemiplegia from acute brain disease occurring in children the nutritive disturbances in the form of arrest of growth should be taken into the account in prognosis, since the result may be nearly or quite the same as is found after infantile paralysis from disease of the cord.
In regard to the slighter forms of paralysis, it may be said that the less extensive the original paralysis is, and the sooner improvement begins, the better is the chance of complete recovery.
TREATMENT, INCLUDING PROPHYLAXIS.—Cerebral Hemorrhage.—As the condition upon which the usual form of cerebral hemorrhage depends is so frequently aneurism, and probably nearly always some arterial disease, the prophylaxis must evidently consist in such a mode of life as will least tend to this degeneration, or at least put it off as long as possible. This, of course, means the avoidance of all the special causes described under the head of Etiology. It is a disease of old age, but in a pathological sense old age begins in different persons after a different number of years. Fortunately for rules of hygiene, there is little that is contradictory in those to be given for most chronic and degenerative diseases. Abstinence from alcohol, as an agent tending at once to paralysis and dilatation of the vessels, is one of the most important rules and insisted upon by nearly all writers. The avoidance of over-eating, and especially of [p. 975] nitrogenous food as tending to lithæmia—a generally recognized cause of arterial degeneration—is perhaps the next. Over-eating is of course to be understood as a relative term, and to be estimated with reference to the habits of exercise of each person. Practically, it will be decided by its effects; that is, if careful thought be given to the matter and the statements of the gourmand as to his immunity from all risk of trouble are not accepted as of scientific value. On the other hand, insufficient food, producing anæmia, may be a factor in arterial degeneration. Keeping one's self free from anxiety, and getting through the world with as little experience of its roughnesses as possible, might be, properly enough, added in a purely theoretical point of view if any one ever asked a physician's advice in youth as to avoidance of the diseases of age, or if any one could or would profit by this advice if it were given.
Intellectual pursuits have been credited with a special tendency to apoplexy, but there is no good reason to suppose that healthy exercise of the mind is otherwise than beneficial to its organ. Hurry, over-anxiety, and mental tension are undoubtedly potent factors in general breakdown, but do not necessarily lead to this form. They are certainly not to be found by preference in those persons who lead an intellectual life.
Syphilis, one of the most important of the causes of organic cerebral disease, and that too in the form of thrombosis, is not specially concerned in the etiology of the forms here under consideration.
If symptoms have occurred that justify the apprehension of apoplexy or paralysis, such as frequent headaches in an elderly person, hemiopia, temporary aphasia, or slight and temporary paralyses, or if one have reached a time of life at which the risk of cerebral hemorrhage becomes considerable, a stricter attention to the rules laid down above, and even to some to which but little heed would be given in health, is not out of place. A certain amount of limitation of diet, moderate and regular but not violent exercise, clothing suitable to the season, and especially warm enough in winter, and, most of all, rest if the patient be doing wearing and anxious work, should be enjoined. Finally, it should be said that the real prophylaxis of cerebral hemorrhage is to be begun in early life.
Among the exciting causes to be avoided are those which obstruct the flow of blood from the head, like tight clothing around the neck. Increase of the arterial pressure by severe or prolonged muscular effort, as in lifting or straining at stool, is to be avoided, as well as violent fits of passion. The condition of the bowels should be regulated by mild laxatives.
When the apoplectic attack has actually occurred, treatment, though apparently urgently demanded, is really of little avail. If a patient is about to die in an hour or two from rapidly increasing pressure, nothing within the reach of medical science can stop him.
There is one danger, however, easily avoided, but probably often overlooked. A patient may die from suffocation. The stertor is often a result of the paralysis of the tongue and palate and of the amount of fluids collecting in the pharynx from the almost invariable position of the patient on his back; that is, if he have been seen by some one who wished to do something for him, but did not know what. Insensibility and paralysis combine to favor this accumulation, which obstructs the respiration, and which may find its way to the lungs, together with brandy and milk, and set up an inhalation-pneumonia. The simple and obvious thing [p. 976] to do is to place the patient sufficiently on his side, with the face somewhat downward, for the tongue and palate and secretions to fall forward, instead of backward into the pharynx. Swabbing out the pharynx may be of some use, but cannot be so thorough. An easy position and proper ventilation should be secured in all cases of unconsciousness, even at the risk of treating a drunkard with undue consideration. Police-stations should be provided with rooms where these conditions can be secured, and the necessity avoided of placing persons picked up in the streets in the narrow, close, and perhaps distant cells provided for malefactors. The writer recalls the cases of two young men—one who had been drinking some time before, and the second roaring drunk—who were locked up in a suburban station-house in the evening, and found the next morning—one dying and the other dead.
Artificial respiration may be used to prolong life in some cases until the nervous centres have sufficiently recovered their functions to carry on the process without assistance. The condition of the bladder should be ascertained, and the urine drawn if necessary, though it is more frequently passed involuntarily.
Although it is manifestly impossible to remove the clot from the interior of the brain, it may appear that the further flow of blood may be stopped and the amount of damage done limited. For this purpose two remedies are proposed—namely, bleeding and purgatives. Both of these act to diminish arterial pressure, which is forcing the blood out of the rupture. Though the treatment seems reasonable, it would not be difficult to imagine a condition where sudden and premature diminution of pressure in the brain, which of course exists outside of the arteries as well as inside, would tend to set going again the flow which has ceased from the very force of the pressure it itself exerts, very much as if a tampon were prematurely removed from a bleeding cavity elsewhere. As the conditions are somewhat complicated, and at the same time only remotely to be estimated, it is safer to be guided by experience in the use of these remedies than by abstract reasoning. In some of the cases of temporary aphasia, as notably that of Rostan narrated by Trousseau, bleeding seems to have given immediate relief. Trousseau, however, is no advocate of that method of treatment. Most modern authors speak of venesection as to be used in cases where the pulse is strong and full and the face red, but not to be thought of in the opposite class. When a case presents the appearances of plethora and an attack has come on suddenly, the loss of a few ounces of blood can certainly do no harm. Other forms of bleeding, such as cups and leeches, are not rapid enough to be of great value, though a large number of leeches about the head might be useful. Some French writers recommend leeches to the anus as revulsives. Cathartics may be more freely used, although they should be given cautiously when there is any tendency to cardiac depression. It can be clearly shown that a brisk purgative lowers the arterial tension decidedly. In case of cerebral tumor or injury with occasional so-called congestive attacks, the relief afforded by cathartics is very great, and, although the conditions are not exactly parallel, it is fair to assume a similar action in the congestion accompanying cerebral hemorrhage. From one to three drops of croton oil may be placed far back on the tongue or it may be diluted with a neutral oil. Ail enema may be desirable for the unloading of the bowels, [p. 977] but has a much less marked effect on the tension of the cerebral circulation.
In most cases of apoplectiform cerebral hemorrhage, and probably in all of simple paralysis, no very active treatment is called for. Measures directed to the prevention of another hemorrhage, and to allay any irritation that may supervene during the changes taking place about the clot and the formation of its capsule, are of the simplest, and consist in keeping the head high and cool, the clothing sufficient for warmth, and offering no obstruction to respiration or circulation, laxatives sufficient to keep the bowels in good order, and a diet not highly nitrogenous, but sufficient and digestible.
That which will tax most severely, however, the care and patience of attendants is the scrupulous and minute attention to cleanliness and pressure over the bony prominences which is necessary when a patient is helpless and unable to control the discharges from the rectum and bladder. Frequent change of clothing, bathing, change of position, and avoidance of wrinkles and roughnesses in the bed may be successful in keeping the patient free from bed-sores. Bathing with alcohol hardens the skin and makes it less susceptible to pressure.
Surgical interference may perhaps be of value in cases where the portion of the clot outside the brain can be clearly demonstrated; and this would apply with special force where the hemorrhage arises from injury.
Trephining and removal of the clot has been done in a few cases of meningeal hemorrhage, though with indifferent success (3 cases—2 deaths, 1 unknown.)56 An intracerebral clot is obviously a step beyond, though possibly in some cases not absolutely without, the reach of the surgeon.
56 Med. Press and Circular, Oct. 14, 1885.
Treatment of Cerebral Embolism.—The prophylaxis is in the avoidance of such conditions as give rise to the formation of detachable vegetations or clots. Unfortunately, these are numerous, not completely known, and not always avoidable. Arterial disease is to be looked upon as of some importance, but cardiac valvular lesions of much greater, and the causes of these, like rheumatism, scarlet fever, and the puerperal condition, are not always to be escaped. The presence of a detachable piece of fibrin in the pulmonary veins, heart, or aorta being granted, nobody can possibly say what will prevent its being loosened and lodging in one of the cerebral arteries; so that, practically, the prophylaxis of embolism consists in the judicious treatment of acute rheumatism and the other conditions just mentioned. The treatment of the first attack must consist solely in the relief of respiration, bladder, and bowels, if they have not taken care of themselves. Stimulants may be of use for a short time, but there cannot be any call for even the slight amount of depletion suggested for some cases of hemorrhage. Bed-sores are to be looked out for, just as in hemorrhage, and the subsequent treatment conducted on the same principles. As regards the primary lesion, we can do nothing about it either in the way of removal of the embolus or restoration of the necrosed brain-tissue.
Treatment of Cerebral Thrombosis.—There being two factors in this affection, both of which are to a certain extent under control, something may be done toward diminishing the risk of its occurrence. Arterial disease and its prophylaxis have already been spoken of. The other [p. 978] condition which is necessary to the production of thrombosis—namely, an enfeebled circulation—is to some extent under the control of general hygienic rules: a nutritious, not too highly nitrogenous, diet, and especially sufficient exercise and the avoidance of completely sedentary habits. If there is a crasis which predisposes to the formation of coagula in the vessels, it is not known that there is any special treatment, medical or otherwise, which can prevent it. The attack is to be treated exactly on the principles already laid down. Bleeding is about the last thing to be thought of. Stimulants, though they cannot dislodge the clot, may be of use for a time to sustain the heart under the shock. The secretions and the condition of the skin are to be looked out for.
After a few weeks of waiting the patient and his friends not unnaturally feel as if something ought to be done to hasten recovery, and certain measures may be taken, in addition to careful hygiene, which have this object in view. It is very doubtful, however, whether anything really shortens the time necessary for such repair as is possible or diminishes the amount of damage which is to be permanent. As has already been said, improvement may go on slowly for months. In the first place, it is sometimes considered desirable to practise shampooing and massage of the affected muscles in order to keep them in as good a condition of nutrition as possible. This, as well as the regular use of the faradic battery if it be not begun too early, will prevent a certain moderate amount of atrophy, but could not have any influence in those rare cases where rapid wasting depends upon secondary degeneration of the anterior gray columns. It may be doubted, however, whether it is necessary to pay much attention to the condition of the muscles, as they do not ordinarily atrophy to the extent of becoming unsusceptible to the nervous stimulus from the brain so soon as it shall be transmitted to them. Faradism, like many other agencies, such as magnets, metals, pieces of wood, and so forth, is said to produce a transfer of sensibility in cases of hemianæsthesia.
There is no sufficient reason to suppose that any drug is of any value in the restoration of the nervous structure. Iodide of potassium may possibly prove to have some effect as a sorbefacient. Very favorable results have been claimed for ammonia salts in the restoration of aged persons to a nearly complete use of paralyzed limbs. Phosphorus has been spoken of as assisting in repair, but the writer is not aware upon how wide a basis of facts. Silver and gold have been said to counteract the sclerosing myelitis. Strychnia is certainly useless, and probably worse. It may make the paralyzed limbs twitch, but this does just as little good as the involuntary spasmodic movements, which have never been considered desirable, except as awakening in the patient false notions of immediate recovery, and which are frequently a very annoying symptom. The galvanic current has been applied with a view to a sorbefacient or restorative action directly to the brain, or rather to the pericranium.
Something can be done for the comfort of such patients: the rubbing and kneading of the paralyzed limbs, if they do not hasten the recovery of motion, relieve many of the painful and unpleasant feelings. Since we do not know how far one part of the brain may supplement another, attempts at motion after it has once appeared to ever so slight a degree should not be abandoned by the patient. He should walk [p. 979] with crutches frequently as soon as he can, though not to the point of fatigue.
There is one faculty which seems capable of re-education to some extent: that is of speech in cases of ataxic aphasia, and even in others the attempt should be made to teach the patient the names of things. A very interesting case has been reported by Bristowe57 of a man who came under his observation after an attack which may have been anterior poliomyelitis with extensive paralysis, able to write well and intelligently, but unable to say anything. By gradual education, first in the sound and formation of letters and afterward of words, he reacquired the use of language. It is obvious that in this case there could have been no loss of memory for the words themselves, but simply the loss of the knowledge of how to produce them. When his speech returned he spoke with his original American accent.
57 Clin. Soc. Trans., iii. p. 92.
In short, the therapeutics of hemiplegia from arterial disease in the brain is good nursing and attention to symptoms, with a moderate amount of care of the paralyzed muscles.
It may be remarked, in the first place, that the lesions known by this name are not necessarily strictly capillary, but are situated in the very small arteries. The microscope marks the transition from the larger to these smaller embolisms.
More is known about very small embolisms experimentally than clinically, since they have been produced by the injection of small seeds and insoluble particles of various kinds. Embolisms arising from natural causes and deposited in the minutest arteries may have very similar origin to the larger ones already described, but there are also other conditions which give rise to particles which pass through larger arteries without any disturbance, and are arrested in smaller ones. The softening of thrombi is undoubtedly one source. The same thrombus which, if detached en masse, would block the carotid artery, may, if broken up into a number of minute fragments of fibrin and fat, pass into the ultimate distribution of the cerebrals. The same thing may of course happen if the thrombus have already undergone one transportation.
Cases of localized softening are seen where no cause has been found, except perhaps a thrombus in the heart, which has discharged its softened and puriform contents; and it is probable that the connecting links exist in the form of embolisms so minute as to escape ordinary observation.
The consequences of capillary emboli if they block every minute ramification of an arterial branch must be essentially the same as if the branch itself were stopped; but if only a part are thus affected, the resulting anæmia is not so complete, since the zones of capillary congestion surrounding the part the supply of which is cut off may be sufficient entirely to cover it and make more or less complete compensation. The experimental emboli, in the form of tobacco-seed and other insoluble substances, which have been traced into the brain in considerable numbers, [p. 980] often give rise to no distinct lesions in the cases where the immediate effects are recovered from.
Among the other sources, ulcerative endocarditis may be mentioned as of special importance, not from the size but the character of detached emboli, which will give rise, not to simple anæmia, nor, on the other hand, to merely negative results, but to septic changes at the place of lodgment.
Aside from these conditions, which are almost the same on a small scale as we find with the large emboli, we have several peculiar substances formed in the body and floating in the blood which lodge in the capillaries of the brain. These are pigment, fat, lime salts, and white corpuscles. Every one of these, however, is much better known anatomically than clinically.
Pigment scales, flakes, granules, or cells containing them, are formed in the course of severe malarial fever, and deposits consisting of this pigment are found in the spleen, liver, kidneys, heart, lungs, and lymphatic glands, as well as the brain and spinal cord. The brain, when a deposit of pigment has taken place, is of a slaty-grayish or chocolate color, which is marked only in the cortical substance, the white being unaffected. The pigment is found in the capillaries, and, according to Frerichs, fibrinous coagula are often associated. Punctiform hemorrhages in the brain have been seen, as well as meningeal hemorrhages, in connection with this degeneration.
The point at which these masses are formed is still a matter of theory. If the liver, as has been supposed, is one of the places of formation, or if they originate in the blood, it is of course easy to see how they reach the brain. If in the spleen, they must pass through the wide portal capillaries before they are arrested in the narrower ones of the brain.
It is by no means certain, however, that pigment reaches the brain in the form of emboli. It is quite as probable that it is found in many organs which undergo repeated congestions from the local destruction of blood-corpuscles and changes in their pigment. The very general deposition seems to point to a process of this kind rather than to a local origin and a distribution through the blood. The punctiform extravasations which may be found with deposits of pigment are also found without it.
Minute particles of fat have been found in cerebral capillaries, but are much less common here than in the lungs. They may be derived from the decomposition of a thrombus, as described above, or they may come from a fractured bone, when, of course, only particles fine enough to pass through the pulmonary capillaries can reach the brain. This form of embolism has an interest in connection with diabetic coma.
Collections of white corpuscles in considerable number have been observed to form an embolus. These cannot be considered to differ very widely in character from the ordinary fibrinous embolus, which contains white corpuscles. It is, however, not certain that such emboli are deposited during life.
Calcareous masses formed from the decomposition of bone have been seen in cerebral arteries.
About the symptomatology of such emboli little is known. An array [p. 981] of minute emboli from the breaking up of a thrombus in the left auricle, carotid, or even aorta, might possibly so block up large numbers of arterial twigs as to give rise to the ordinary symptoms of embolism; but considering the possibility of the re-establishment of circulation, provided a certain proportion of the minutest vessels escape, complete anæmia of a large tract produced in this way must be rare. It is possible that some of the slighter and more transitory attacks of hemiplegia or of more or less vague cerebral symptoms may be referred to a lesion of this kind, the first action of a large number of emboli being to cause an anæmia, which is compensated for much more rapidly and thoroughly than would be the case if a single considerable vessel were obliterated.
Various attempts have been made to connect definite and peculiar diseases with capillary embolisms. Chorea in particular has been said to depend upon a lesion of this kind, but, although cases have been observed where the symptoms and lesion coexisted, yet they are very far from being the rule, or even from constituting a respectable minority of cases. The lesion of chorea in the great majority of cases is not known, although attention has been directed to this theory long enough to have established its truth.
The same may be said of the relationship between pernicious attacks of intermittent and pigment embolism. There is occasional coexistence, but far from invariable. Cerebral symptoms of the same kind and severity occur without as with the pigment deposit. If pigment embolism is the cause of coma, delirium, etc. in pernicious fever, it is difficult to see why such cases can recover so rapidly, and why no symptoms referable to a localized cerebral lesion are observed after the primary unconsciousness.
Even less proof can be adduced as to any connection between leukæmic embolisms and the cerebral symptoms occurring toward the end of severe acute disease.
Calcareous embolism is a pathological curiosity.
DIAGNOSIS.—In the case of multiple capillary embolism it would be impossible, if it were complete, to distinguish it from a blocking of the main branch.
Cerebral symptoms arising in the course of ulcerative endocarditis might be referred, with a high degree of probability, to an embolus, but if they were distinct enough to be referred to a localized lesion, the probability of a single embolus would be much greater than that of a multitude of capillary ones occluding the same vascular territory. The diagnosis of pigment embolism might be a probable, or at any rate a possible, one if in a long-continued case of paludal fever, where the liver and spleen were enlarged and the skin had the slaty hue marking the deposit of pigment, there were decisive cerebral symptoms. It could not, however, be a positive one.
Fatty embolism might be suspected in a case of diabetic coma, though even if the condition were found it would not establish the relation of causation.
PROGNOSIS AND TREATMENT can hardly have a definite basis in the absence of all ground for a satisfactory diagnosis, but do not differ essentially from those of the larger occlusions.
It has for centuries been known that coagulation of the blood might take place in the sinuses in a way different from the ordinary post-mortem clots, but this was looked upon rather as an anatomical curiosity than as a fact of practical importance and clinical significance, and it is chiefly among observers of the present century that we find a growing knowledge of the conditions under which it occurs and the symptoms to which it gives rise.
Thrombi in the cerebral sinuses are not essentially different from those formed elsewhere, and the reader is referred to the account given in the article on General Pathology for a history of their formation, growth, appearances, and transformations. For our purposes it is sufficient to recall that they may be white, red, or striated, either partly or wholly obstructing, and that they may become degenerated and partly or wholly washed away. The most important distinction of all, however, is that into two classes, of which the first consists of those which are simply depositions of fibrin in a comparatively healthy vessel, and the second of those which are dependent on a phlebitis.
In order that a thrombus may form it is necessary that there should be, in the first place, a special condition of the walls of the veins—not necessarily, however, inflammation, though this is one of the most frequent and probably the most active form; second, a slackening of the blood-current; and, third, perhaps a peculiar state of the blood, though this latter is not certain. A thrombus tends strongly to grow, and when already formed furnishes a most favorable point for the deposition of more fibrin.
The cerebral veins furnish a very suitable place for the coagulation of the blood for several reasons: they are roomy in proportion to the amount of blood they carry; they are tortuous and abundantly anastomosing, so that the current of blood is almost reversed at some points, and can easily stagnate; the veins of the diploë are held open by their bony walls, and the sinuses by their stiff membranous ones, so that they cannot collapse and thus limit the extension of a thrombus once formed.
The sinuses most frequently affected, though none are free from the liability, are the cavernous, superior longitudinal, and lateral.
The results of thrombosis of the sinuses and veins are not equivalent to those of a similar process in the arteries, and they may be said in a general way to be more diffused, as might be expected from the much greater freedom of anastomosis. Limited softening is rarely a consequence of occlusion even of a considerable number of veins, but it has been observed. A large area of softening of one hemisphere, not involving the temporal and occipital lobes, has been seen with thrombosis of the parietal veins58 (the internal capsule and ganglia were not affected).
58 Gaz. des Hôp., 1880, 1066.
Passive congestion in the brain, as elsewhere, although apparently entirely incompatible with the normal function, seems to be able to sustain a low form of structural integrity.
Bleeding may take place from the congested veins behind the obstruction, constituting a distinct form of cerebral hemorrhage which does not depend upon an arteritis, although if miliary aneurisms were present the [p. 983] occurrence of thrombosis would undoubtedly tend to their rupture. The writer, however, is not aware of such a coincidence having been actually observed. Hemorrhages are usually diffuse, composed of or accompanied by a number of small effusions, and situated on or near the surface of the brain or distinctly meningeal. Punctiform hemorrhages are exceedingly common.
Phlebitis of the cerebral veins is very likely to run into meningitis, and the two affections are often so closely united that it is difficult to say which was the first. Œdema is a consequence of venous obstruction in the brain as well as elsewhere, and is seen also around some of the peripheral veins connected with the sinuses.
ETIOLOGY.—Venous thrombosis in the brain depends chiefly on three sets of causes, though it must be admitted that there are a few cases where the origin cannot be distinctly traced and where no previous disease has existed. In the marantic form, occurring chiefly in the very old and in children, as well as in cases of wasting and depressing diseases in adults, a simple thrombosis without inflammation takes place. Two conditions, and sometimes three, are combined here to produce the result—feebleness of the blood-current from a corresponding state of the heart, diseased endothelium of the vessels from defective nutrition, and possibly, where profuse watery discharges have been going on for some time, an increased tendency to coagulation from the inspissation of the blood.
Rilliet and Barthez and Von Dusch59 give the following tables of ages at which this form of thrombosis has been observed. The observations of the former were made in a children's hospital, and hence do not affect the question of its frequency in later life. Perhaps the rules of admission may account for the absence of cases under one year of age, of which Von Dusch collected several:
| Rilliet and Barthez. |
Von Dusch. | |
| Under 1 year | ... | 5 |
| 2 years | 2 | 1 |
| 4 years | 4 | 1 |
| 5 years | 1 | 1 |
| 6 years | 1 | |
| 7 years | 1 | |
| 9 years | 2 | |
| 10 years | 1 | |
| 11 years | 1 | |
| 12 years | ... | 1 |
| 14 years | ... | 1 |
| Adults (20, 23, unknown) | ... | 3 |
| 53 years | ... | 1 |
| Aged women | ... | 2 |
59 Sydenham Society's translation.
The special diseases in which thrombosis is most likely to be met with are given by Bouchut as follows. The same remark is to be made about these as about those of Rilliet and Barthez. The table is given as convulsions from thrombosis of sinuses:60
| Chronic enteritis | 5 |
| Measles and catarrhal pneumonia | 2 |
| Chronic pneumonia | 5 |
| Phthisis | 8 |
| Anasarca without albuminuria | 1 |
| Chronic albuminuria | 2 |
| Whooping cough and pneumonia | 7 |
| Scrofula, tubercle of bones, etc. | 1 |
| Gangrene of mouth | 1 |
| Diphtheritis | 2 |
Von Dusch gives a number of cases of the same kind, as do many subsequent writers, but without tabulation. Virchow61 reports a case of congenital variola with thrombosis of the sinuses of the dura mater, the superior and inferior cava, and vessels of the cord.
60 Gazette des Hôpitaux, 1879.
61 Arch., 1859, 367.[p. 984]
It is probable that simple anæmia may, here as elsewhere, either alone or with other debilitating influences, lead to thrombosis. Von Dusch remarks that quickly operating and debilitating influences lead to thrombosis, and gives as an instance a case where a puerperal peritonitis, for the cure (?) of which repeated copious abstractions of blood were made during nine days, was supposed to be the cause. The puerperal condition seems to have a tendency in this direction in a way not always to be explained by the ordinary rules of the transmission of emboli or of phlebitis. Although in those reported by Ducrest62 phlebitis of the pelvic veins existed or was suspected, in the first of these five cases the lesion may have been, so far as the description goes, arterial instead of venous thrombosis; and in the second it is possible that the succession of events was uterine phlebitis (with the addition of a large sacral slough), lobular pneumonia surrounded and traversed by veins which were affected with phlebitis, emboli in the arteries of the cortex, and consequent venous thrombosis. In the third, fourth, and fifth the connection between the uterine phlebitis and the inflammation of the cerebral veins (in two cases meningitis) cannot easily be made out, except by the rather vague assumption of a general tendency to phlebitis, which was shown in one by a similar condition in the vein of the arm where the patient was bled. Empyema has been followed by hemiplegia, cerebral softening, and thrombosis of the lateral sinus. The venous thrombosis in such a case may be secondary.
62 Archives générales, 1847, p. 1.
Marantic thromboses are more likely to occur upon one side, and that the side upon which the patient habitually lies.
The second class of cases embraces those where a simple obstruction, partial or complete, of the current of the blood gives the starting-point for a thrombus in the veins. Such an obstruction may be formed by an embolus, but in the veins this cannot be considered an important factor, although a portion of a thrombus may be detached and become lodged in a narrower vessel or branch farther along. In this way the propagation of thrombosis for a short distance toward the heart may be accounted for.
A tumor or inflammatory exudation may press upon a vein or intrude into it, but most cases of obstruction-thrombosis are traumatic in origin. Thromboses arising in connection with tubercular meningitis may be looked upon as having both an obstructive and marantic cause. In many wounds of the vertex, gunshot and other, the walls of the superior longitudinal sinus are pressed upon by pieces of bone, and sometimes spiculæ have directly penetrated it. This class of injuries is also likely to cause phlebitis without any actual penetration or compression of the sinus, simply as a result of the inflammation of tissues in the neighborhood. The thrombi formed in these cases are not necessarily completely occluding. Where direct injury to the sinus or in its immediate neighborhood gives rise to phlebitis and consequent thrombosis, we have a condition closely resembling that of the third class, where disease of an inflammatory character in the tissues of the skull, neck, or face sets up a phlebitis and thrombosis which are transmitted to the intracranial veins and sinuses.
The most frequent source of this third form of inflammatory thrombosis [p. 985] is the chronic inflammation of the middle ear with the mastoid cells. The inflammation may be propagated through a carious or necrosed portion of the temporal bone to the petrosal and lateral sinuses, or may, without disease of the bone, be carried by the small veins which open into the sinuses from the petrous and mastoid portion of the temporal in this region. Abscesses in the neck may set up a phlebitis extending up the jugular to the lateral sinuses, to which a meningitis may possibly be added.
Carbuncles about the root of the nose, face, and so far down as the upper lip are very prone to give rise to thrombosis propagated through the ophthalmic vein to the cavernous sinus; and it is probably this risk which gives to carbuncles in this situation their well-known peculiar gravity. The divide or watershed between the regions which drain backward through the cranium and those which are connected with the facial vein below is apparently situated about the level of the mouth, so that a carbuncle of the lower lip is much less dangerous. Billroth, however, gives a case where a carbuncle in this situation was followed rapidly by cerebral symptoms and death, and where a thrombo-phlebitis was not improbable. He mentions another case where a carbuncle upon the side of the head set up an inflammation which travelled along a vein into the cellular tissue of the orbit, and thence through the optic foramen and superior orbital fissure into the skull.
Erysipelas of the scalp apparently causes phlebitis in some cases, and even eczema in the same situation seems to have done so. When the erysipelas is situated about the upper part of the face, the path of transmission is through the ophthalmic vein; but when upon the vertex, it may be propagated through the small veins that penetrate the bone. This result is certainly a rare one in facial erysipelas of the ordinary and superficial kind, which is a notoriously benign disease for one of such apparent severity. It may, however, be more frequent than ordinarily supposed, since cerebral symptoms occasionally appear at a date too late to be accounted for by the fever and too slight to be referred to extensive interference with the cerebral circulation; the lesion to account for which, as they do not cause death, can be only inferred, though it is not unreasonable to suppose it to be a limited thrombosis.
Dowse63 describes the case of a robust man who fell on the back of his head, but walked home. After a few days he had a severe headache, chill, and total loss of vision. His temperature rose; he had erysipelas and partial coma, but no convulsions. There was thickening of the scalp, but no fracture of the skull and no adhesions of the membranes. The superior longitudinal lateral sinuses were free from thrombi, though there was a roughness about the latter, as if there had been a fibrinous deposit. The cavernous sinuses were almost completely occluded with adherent fibroid masses, and there was hemorrhage in the anterior lobe. There was some degeneration of the brain-structure, but no disease of the arteries.
63 Trans. Clin. Soc., 1876.
Ulcerations in the nasal passages and ozæna have proved starting-points for thrombosis.64
64 Med. Times and Gaz., 1878, i. 614.
Thrombosis of the jugular veins and corresponding cavernous sinus, with paralytic symptoms, has been observed in the horse.
[p. 986]The symptoms produced by venous thrombosis, as might be supposed from their varying location and extent, and also from the fact of their being almost invariably connected with other diseases having marked and severe symptoms of their own, are not always easy to pick out from among many others, but they are sometimes very well marked and characteristic. A distinction must obviously be made between the symptoms of simple thrombosis depending on interruption of the cerebral circulation and those of phlebitis, which give rise in addition to febrile phenomena common to phlebitis in any of the large veins.
The symptoms which indicate venous obstruction, without reference to its inflammatory or non-inflammatory character, are of two kinds: first, those dependent upon the disturbance of the functions of the brain; and, secondly, those which depend upon congestion and compression of other structures.
According to the locality and completeness of the obstruction we meet with brain symptoms.
In the marantic thrombosis of children these may be very vague, and consist either in restlessness, followed by somnolence and coma, or, most especially, in convulsions. The convulsions may be partial and involve the face only; they may affect one side only, or, what is more usually the case, be general. There is almost always strabismus. There may be conjugate deviation. This latter phenomenon is said by Bouchut to be of no value in children, as it may take place in either direction, from or toward the lesion, but possibly the distinction between the spastic and paralytic forms was not duly observed by him. The condition of the fontanelles is spoken of as yielding and depressed, with the edges of the bones overlapping. They may, however, become again tense in the course of the disease from exudation or hemorrhage taking place. Paralysis is not so marked as in adults, but may be present.
In adults delirium takes the place of convulsions, due to a disturbance of circulation over a considerable area, rather than to a total suppression in a more limited one. Paralyses are not infrequently met with, either in the form of a hemiplegia or more localized. Hemorrhage will naturally be followed by its usual consequences, according to its location. Headache, often very severe, is among the early symptoms.
It is evident that none of these symptoms can be considered highly characteristic. They can only furnish a certain amount of probability in cases where the general course of the disease has made it likely that thrombosis may take place.
There is another set, however, which, when present, offer the strongest kind of confirmation: these are due to the pressure from the veins themselves.
Œdema about the points at which the intracranial circulation is connected with that of the face and neck may give rise to protrusion of the eyeball, conjunctival ecchymoses, swelling of the upper lip, and even of the upper part of the face, which sometimes becomes slightly cyanosed from the congestion. Epistaxis has been noted. Œdema may be noticed about the mastoid process when the thrombosis is situated in the lateral sinuses, but it would be important in many cases to distinguish this from inflammatory œdema directly due to disease of the bone.
Œdema of the optic disc, as shown by obscuration of its outlines, with large and pale vessels, has been observed by Bouchut.
[p. 987]Veins closely connected with those within the cranium may be thrombosed, and felt as hard cords by the finger. This may occur in the facial veins about the orbit, in those around the mastoid, or in the jugulars. On the other hand, if one cavernous sinus is filled with a coagulum which does not go down into the jugular, this vein will naturally be empty or receive only a small amount of blood from other veins.
When the cavernous sinuses are affected, we are likely to have a set of phenomena due to the pressure of the clot upon the nerves which pass through it—i.e. the third and fourth, part of the fifth and sixth—with filaments of the sympathetic accompanying the carotid artery. Hence dilatation of the pupil, strabismus, or ptosis, and other ocular paralyses may be the symptoms observed.
It is possible that a headache upon the side of the affected sinus may be due to vascular dilatation from paralysis of the sympathetic, or to a direct pressure upon the first branch of the fifth pair.
DIAGNOSIS.—The diagnosis of venous thrombosis may be almost entirely a conjectural one in those cases where the cerebral symptoms are vague or mixed with others peculiar to the causative disease. Where wasting disease has existed, the patient is much emaciated, and profuse discharges have diminished the fluidity of the blood, the rapid supervention of coma with slight spasms or general convulsions will render it highly probably that thrombosis is taking place. Unilateral symptoms would greatly increase this probability, and if any accessible veins about the head, neck, or face could be definitely distinguished as filled with firm coagula, the diagnosis would approach certainty.
In cases of this kind the only condition likely to put on the appearance of thrombosis is the simple inanition or so-called hydro-encephaloid disease, which comes on in exactly the same sort of cases. Localized phenomena must be the chief point of difference. Fortunately, the distinction is practically not an important one.
In wounds of the vertex affecting the longitudinal sinus the question likely to arise where cerebral symptoms supervene is that of thrombosis or abscess. Here the more definite localization is likely to be upon the side of the abscess, although, as is well known, this may remain latent or nearly so for a considerable time, and in general is much more chronic in its course than thrombosis.
The swelling of the external veins, epistaxis, œdema of the lid, protrusion of the eyeball, with œdema of the optic papilla, with only moderate fever, would favor the diagnosis of thrombosis, while optic neuritis, if present, with chills, would render the abscess more probable. Unless the wound were sufficiently severe to fracture a piece of bone into the sinus, or unless the subsequent inflammation were of an unhealthy character, the abscess in a person of middle age and previous good health may be considered the more probable of the two. In the case of Dowse, already mentioned, the diagnosis between abscess and thrombus must have been very difficult, and, as it seems to the writer, would have been more likely to rest upon abscess or meningitis than upon the condition afterward found to exist.
Where inflammatory diseases exist which are known to lead to thrombosis with phlebitis, the practitioner, if on the lookout, can often make a diagnosis with a high degree of probability in its favor. The cerebral [p. 988] symptoms with the venous swelling, collateral inflammatory œdema in the more immediate neighborhood of the lesion, and slight œdema and congestion at more distant points, and a febrile movement indicating a distinct inflammatory exacerbation, will point very strongly to thrombo-phlebitis.
An absolute distinction between such a condition of the veins and a meningitis arising under exactly the same circumstances may not always be possible, and is the less important since the two affections are likely to coexist and form a part of the same disease.
The localization of the thrombus is to be determined partly by the paralytic symptoms, if such exist, but principally by the situation of the secondary œdema and from the lesion which forms the starting-point. It has been said that the jugular vein of the side on which thrombosis exists is less full; and this point might be of value when the lateral sinus is affected.
PROGNOSIS.—From the character of the lesion itself, as well as from the diseases with which thrombosis is usually connected, it will readily be seen that the prognosis is in general a highly unfavorable one; but it is possibly regarded as too inevitably so, for the reason that a positive diagnosis may be in slighter cases a matter of considerable uncertainty, so that the practitioner, even if attempting to make an accurate anatomical explanation of obscure cerebral symptoms, is as likely to think that he has been mistaken as that his patient has recovered from so serious a disease.
Cases, however, have been reported where the diagnosis seems as clear as it can be made without an autopsy, and recovery has taken place.
A case is reported by Voorman65 of a child aged six months who had diarrhœa and vomiting, much prostration, sunken fontanelles, overlapping cranial bones, trembling of the tongue, slight spasm of the right arm and leg, head drawn back, and strabismus. The head afterward increased in size, the temporal vein was swollen and hard, with œdema of the skin in its neighborhood. There was gradual improvement and recovery, though when the patient was four and a half years old its mental development corresponded to that of a child two years younger.
65 Centralb. f. d. Med. Wis., 1883.
In another, by Kolb,66 a child of seventeen, well nourished, had a purulent discharge from the right ear. Besides headache, delirium, hyperæsthesia, convulsions, and then sleepiness and loss of consciousness, the following symptoms pointed toward thrombosis of the sinuses: Chills, inflammatory swelling over the right mastoid, with fulness of a cutaneous vein passing over it; a purely œdematous swelling in the neighborhood of the internal jugular or temporal fossa, forehead, and both upper eyelids, with exophthalmos on the right side; photophobia, blepharospasm, and cloudy vision; nose-bleed. There was no elevation of temperature, and recovery took place.
66 Berl. klin. Woch., Nov. 13, 1876.
A case of thrombo-phlebitis following otitis and terminating in recovery is reported at length by Wreden.67
67 Archives of Ophth. and Otol., 1874, lii. (translation).
The PROGNOSIS in any particular case can be based only on the severity of the symptoms and on the character of the preceding disease.
TREATMENT.—The prophylaxis of this affection evidently consists in [p. 989] the proper treatment of the diseases upon which it depends, and might therefore be made to embrace nearly the whole range of tonic, roborant, antiphlogistic, and antiseptic measures, to say nothing of surgery and obstetrics. The proper nourishment of infants and children, the cutting short, when possible, of their acute diseases, or preventing their debilitating effects, will reduce marantic thrombosis to a minimum. At a later period of life the proper surgical management of carbuncle, abscess in the neck, and of the puerperal condition will tend to avoid this risk.
The most important point of all, however, is undoubtedly the careful treatment of otitis media and early attention to inflammation in the mastoid cells, with incision or trephining as may be necessary.
After a thrombus has formed there is little to be done toward its removal.
It has been claimed68 that the preparations of ammonia are capable of diminishing considerably the coagulability of the blood when it is morbidly augmented. Though this cannot be considered proved, yet since the tendency of these salts is also to quicken the blood-current, a trial in a case where other indications are wanting is, to say the least, justifiable.
68 Lidell, Am. Journ. Med. Sci., July, 1874, p. 101.
In a case reported by O'Hara,69 where the symptoms pointed very strongly toward thrombosis of the cavernous sinuses, recovery took place under mercurials, iodide of potassium, and purgatives. The reporter was inclined to consider the cause of trouble specific.
69 N. Y. Med. Record, vol. xvii. p. 617.
Considering the fact that cases with such marked and decisive symptoms as those last recorded have recovered, it is certainly the duty of the physician to prolong the life of his patient to the utmost, that absorption and condensation may go on as long as possible and collateral circulation be developed. Probably most physicians can recall cases of obscure cerebral disease going on to recovery contrary to all expectation, in which thrombosis furnishes an explanation quite as plausible as any other.
is a name which it is yet too early to omit altogether from a systematic work, although in treating of it we have more to do with nomenclature and classification than with pathological anatomy. The phrase may be said to have both an anatomical and a clinical signification, which do not coincide at all points. Clinically and among the laity it is used to express various symptoms and groups of symptoms more or less referable to the brain, some of them connected with one and some with another lesion, and many purely functional—if the word may be used—or at any rate unconnected with any known or definite lesion.
Vertigo, dull headache, sleeplessness, or, on the other hand, drowsiness, failure of memory, failure of power of concentration, of steady application, mental depression, fatigue, and even slight aphasia or actual slight hemiplegia, may any of them be considered symptoms or forerunners of softening of the brain. As nearly as anything, the popular notion of this affection corresponds to general paralysis of the insane or senile dementia, or even mere exhaustion. Many of these symptoms may, of course, be connected with the real softening described as the result of embolism or [p. 990] thrombosis, but it is hardly necessary to say that a symptomatology based on these elements alone is either too vague or else too much like that of diseases already described to be considered useful as a separate clinical grouping.
On the anatomical side softening of the brain has had a definite meaning, and for many years a part of its pathology has been well known. A general softening of the whole brain, such as seems to be the condition supposed when the phrase is used, does not and cannot exist, since a vascular lesion sufficient to cause anæmic necrosis of the whole brain must cause death long before softening would have time to take place. Nearly all the works and reports on softening have been based upon cases such as are now referred to definite lesions of the blood-vessels; and a good idea of the change in nomenclature and pathological views may be obtained by noticing the dates given in the extensive literature of the subject in the Index Catalogue of the Surgeon-General's library, which are nearly all previous to 1860 or 1865.
Localized softening has already been described under the heads of hemorrhage, embolism, and thrombosis, venous and arterial. Whether it may occur from diseases of the cerebral vessels without actual occlusion is not certain, but, remembering the difficulty of detecting thrombi in minute vessels, and also the fact that it is not a great many years that occlusions have been systematically sought for at autopsies, it is better for the present to assume, in cases where softening is found in the usual form and the usual situations for the results of thrombosis and embolism, that one of these accidents is the cause, even if the actual point of occlusion is not found.
Softening may take place secondarily from tumors in the brain, and the name is also sometimes applied to a local encephalitis, which is an early stage of abscess. When, however, these various forms of disease are removed from the general heading of softening and referred to their proper pathological classes, there is a residuum in which the softening seems to be the primary affection, so far as the brain is concerned, though depending on other constitutional conditions.
In new-born infants softening of the brain, besides the rare cases in which it may be dependent on the same conditions which may cause it in the adult, is observed in two forms, as described by Parrot:70 A. White softening in multiple foci, dependent upon fatty degeneration, of which it constitutes the last stage, is found almost exclusively in the centres of the hemispheres. B. Red softening, which affects the same region, but more extensively, and is accompanied by hemorrhage into the lymphatic sheaths with rupture.
70 Arch. de Phys., 1873, p. 302.
These two forms may exist with each other, and with other intracranial lesions, such as thrombi of the sinuses and exudation under the arachnoid and around the veins.
Parrot compares this form of softening to that occurring in the other extreme of life, dependent on vascular lesions; but although he supposes the method of production to be unlike in the two cases, it is by no means so certain, either from his conclusions or his cases, that it is always so. In some of his cases the vessels are said not to be abnormal, but in others old thrombi are distinctly mentioned. As secondary consequences may [p. 991] be observed intracranial dropsy, with perhaps hydrocephalic cranium and degeneration of the pons, bulb, and medulla.
Two cases of red softening of the cerebellum have been reported.71 In one of them the pia was adherent, in the other thickened and covered with exudation. The microscopic details are not given nor the state of vessels mentioned. They are probably not strictly analogous to those described by Parrot.
71 Jahrbuch. f. Kinderheilkunde, 1877.
The occurrence of granular corpuscles in the brain of the new-born is described by Virchow, and it is thought by him to be pathological and of an irritative character (encephalitis congenita). It is somewhat doubtful if this process is characterized by any distinct symptoms.
The ETIOLOGY is impaired nutrition, deficient or improper feeding, and depressing diseases, frequently tubercle.
The SYMPTOMS and DIGNOSIS of this form of softening are even more obscure than those of venous thrombosis in the same class of cases. Vague cerebral symptoms arising in an infant poorly nourished and suffering from acute disease may be due to this condition, but a positive diagnosis is out of the question. In the two cases of softening of the cerebellum just mentioned, in one, aged five, there was dilatation of the pupil, difficulty of hearing, and vertigo; in the other, aged six, vertigo, inclination to vomit, and clonic spasm of the left facial muscles. Parrot says that in the greater number of patients the encephalopathic troubles observed during life cannot be referred to it (softening), and in no case can it be diagnosticated.
Under these circumstances it is obvious that remarks upon the PROGNOSIS and TREATMENT must be purely works of the imagination.
has already been spoken of as one of the most important factors in thrombosis, and perhaps of considerable consequence in embolism and hemorrhage. Its symptoms, when one of these accidents has taken place, are hardly to be separately considered; and if atheroma have produced complete occlusion, even without the assistance of a clot, the symptoms could not be distinguished from those of an ordinary thrombosis, and would follow the same course.
In some cases, however, the thickening of the artery may interfere with, without completely interrupting, the circulation in the part to which it is distributed, and the degree of the interference may vary from time to time. If, then, in a person whose age and general physical condition, as shown by the state of the tangible arteries, arcus senilis, complexion, and so forth, render the existence of atheromatous arteries in the brain probable, cerebral symptoms of an ill-defined character arise, it is very probable that they are the result of irregularities in the circulation dependent on atheroma.
This state of things is to be distinguished from the more clearly marked conditions which have already been described, partly by the incompleteness of the attack, and partly by its changes in severity and character from time to time—a paralysis undergoing alternations of [p. 992] improvement and the reverse from day to day, delirium appearing and disappearing in correspondence with the general health, the vigor of the heart, and the state of the digestive organs.
The diagnosis between these incomplete anæmias and an almost precisely similar result of syphilitic endarteritis is to be made chiefly by the history and age. In middle-aged persons general paralysis might present a not very different set of phenomena. A tolerably distinct, but not severe, hemiplegia in an old person, subsiding in a few hours under the influence of a cathartic, and perhaps returning more than once, may often be due to a local and temporary anæmia from atheroma, as well as to slight hemorrhage or a not completely occluding thrombus.
On the other hand, extensive atheroma may exist without serious impairment of the cerebral functions, provided it be evenly distributed and do not interfere with the passage of blood in any one vessel.
The prophylaxis of atheroma has already been considered. We do not know of any drug that can change the nature or extent of the processes going on in the arterial walls, but if any influence can be exerted it is through dietetic and hygienic means.
The consequences of rigidity of the arterial walls, as productive of resistance to the passage of blood, can be warded off to some extent by promoting the vigor of the heart. Treatment should therefore be directed to the improvement of the nutrition of the body in general and the heart in particular. Heart tonics and laxatives are the classes of medicaments most likely to be useful. Perhaps it is to its effect in increasing the force of the heart contractions, like digitalis, that coffee owes its reputation as a preservative from apoplexy.
INTRODUCTION AND DEFINITION.—Atrophy of the brain may originate during intra-uterine life or by defective development during the early periods of childhood, or it may occur during adult life, when the organ is fully developed. The atrophy is characterized by a diminution of the normal bulk of the brain-substance, in consequence of which the latter does not entirely fill the cavity of the cranium, but leaves a greater or less space to be occupied by a serous fluid. Generally, the atrophy affects, in a symmetrical or asymmetrical manner, larger or smaller portions of the brain; an atrophy symmetrically affecting all parts of the brain has never been observed, even in microcephalia. Nevertheless, when the atrophy affects both hemispheres of the cerebrum, it is generally called total, whilst it is designated partial when it is limited to only one hemisphere or to other individual parts of the brain, such as the cerebellum, the large cerebral ganglia, etc.
For the sake of convenience we shall treat the atrophy of the brain occurring during childhood, when the organ is still developing, separately from that of the fully-developed brain of the adult.
When congenital or originating during infancy the atrophy is either primarily due to certain pathological processes taking place in the substance of the brain, or secondary, being due to lesions of the skull, such as premature ossification of the sutures. Total atrophy of the brain at this period of life leads to an early death, while children affected with partial atrophy may continue to live, though almost always in a state of idiocy. The forms mostly observed in children are unilateral or bilateral atrophy of the cerebrum, partial or almost entire absence of the cerebellum, imperfect development of the large cerebral ganglia, and slight partial atrophy of the medulla oblongata. The large commissures as well as the crura cerebri are very seldom found atrophied.
The most frequent and, from a practical point of view, the most important of these forms is the unilateral atrophy of the cerebrum, for the reason that in a mild form it is to a certain degree consistent with the [p. 994] mental and physical development of the child. It is mostly found on the left side. In some cases the atrophy extends evenly throughout the hemisphere, while in others it affects more or less one or the other lobe. The loss in the bulk of the hemisphere may amount to only a slight diminution, or to as much as to one-half of the normal size. Its thickness above the ventricle may be reduced to a few millimeters; in some cases even the membranes of the brain may lie in contact with the ependyma. The ventricle of the atrophied hemisphere is almost always enlarged. The convolutions of the cerebrum are very narrow, sometimes quite indistinct. One or both of the corpora striata also are generally found atrophied. In many cases even the atrophy extends to one of the crura cerebri and to the pyramid of the same side, and to the anterior and lateral columns of the spinal cord on the opposite side. Frequently, one or the other lateral half of the cerebellum also is found affected. The condition of the substance of the cerebrum is nearly the same as in the senile atrophy of the brain to be described hereafter. The skull is mostly thickened on the side of the atrophy, and frequently asymmetrical.
SYMPTOMS.—In most cases the mental capacity is below the normal standard, and frequently borders on or represents a state of idiocy. The temperament of the patient is generally irritable and very excitable. The most prominent symptom is an incomplete paralysis on the side opposite to the atrophied hemisphere, which is the more pronounced the more the corpus striatum, thalamus opticus, and crus cerebri are involved. Frequently, there are contractures of the flexor and pronator muscles of both extremities, particularly of the upper; the muscles of the trunk remain free; sometimes one or the other half of the face is also paralyzed. Epileptic convulsions also are frequently present. Blindness and deafness, with a defective sense of smell and a blunted sensibility of the paralyzed limbs, as well as neuralgia of the latter, and headache, have also been observed.
CAUSES.—Besides the causes already mentioned, atrophy of the brain occurring in children after birth may be induced by injuries of the head, inflammation of the enveloping membranes, of the ependyma, or of the substance of the brain itself.
TREATMENT.—Atrophy of the brain in children is perhaps, in the majority of cases, incurable; it is therefore only in the milder cases that the patient may be benefited by treatment. Electricity and gymnastic exercises have been recommended. At any rate, it must be pursued in a very systematic manner, and based upon the principles established and practised by the late E. Seguin of New York in his Physiological School for Weak-minded Children, consisting in improving the mind, first by training the child to the use of his limbs by means of light mechanical work, etc.
In the brain of the adult the atrophy may be partial or total, symmetrical or asymmetrical, in the same sense as before used in connection with the atrophy of the brain of children. It may, further, be stationary, [p. 995] when the atrophying process remains limited to the part where it originated; or, progressive, when it extends to other parts of the brain. Generally, partial, asymmetrical, and stationary atrophy is due to certain accidental pathological processes, producing a destruction or loss of portions of the substance of the brain, such as apoplexy, softening, etc., by which the nutrition of the neighboring parts becomes disturbed. Total, symmetrical, and progressive atrophy, on the other hand, actually depends upon certain constitutional disturbances of the nutritive process in general, such as chronic alcoholic intoxication, etc.
CAUSES.—As already mentioned, the causes of atrophy of the brain in the adult may be direct or indirect. The former are generally represented by certain pathological processes which directly affect the substance of the brain, as, for instance, apoplectic hemorrhagic effusions into the brain-substance, thrombosis or embolism of the cerebral arteries, encephalitis, chronic serous effusions into the ventricles, inflammation and œdema of the pia mater, etc. To the latter or indirect causes, which affect the organ by disturbing or lowering the nutrition of its substance, belong the retrogressive processes of old age or of insanity; the introduction into the system of certain noxious substances, such as lead or alcohol; furthermore, certain wasting diseases, such as phthisis, Bright's disease, etc.
PATHOLOGICAL ANATOMY.—The cerebrum particularly is found diminished in volume. While the convolutions are thinner than normal, their intervening sulci are broader. The white substance presents a dirty-white color, and is abnormally dense and tough, especially near the ventricles. The latter are enlarged and filled with serum; their ependyma is thickened and frequently covered with granulations. The cortical layer appears of a dirty, rusty-brown or yellow color, is pale, soft, or hard, and frequently is found to adhere to the pia mater. In very pronounced cases the white substance is almost as tough as leather, and contracts upon section, especially in the convolutions; its cut surface is rendered concave. Sometimes the surface of the convolutions, after the removal of the pia mater, appears finely shrivelled. The dura mater is often found thickened and adhering to the skull. The space created in the cavity of the cranium by the atrophy of the brain is filled by serous effusions into the tissue of the pia mater, the subarachnoidal space, arachnoid sac, and ventricles.
The histological changes associated with atrophy of the brain differ in the different forms. In cases of partial atrophy caused by hemorrhages, etc. the destructive process generally embraces all the tissues at first, while the secondary degenerations particularly affect the nervous elements. In total atrophy the pathological process appears to commence in the connective tissue, and to involve the nervous elements subsequently; though in a number of cases, especially of senile atrophy, the nervous elements appear to be primarily affected. The blood-vessels also undergo certain changes, giving rise to the contraction of the brain-substance.
SYMPTOMS.—In partial atrophy of the brain the primary symptoms resemble those which characterize the particular destructive process to which the atrophy is due. The most prominent are the symptoms of motor disturbance, which are always semilateral and correspond to the extent and seat of the lesion; frequently they remain stationary. The [p. 996] sensibility of the paralyzed parts is but slightly diminished, and the mind generally undisturbed. But when the effects of the original lesion extend, in the form of a secondary degeneration of the nervous elements, to neighboring parts, or even to the other hemisphere, the cerebral functions may become secondarily disturbed.
In senile atrophy of the brain, which represents the most simple form of total atrophy of this organ, the first symptoms frequently appear toward the end of some intercurrent disease. They consist in a very slow and gradually increasing derangement of the cerebral functions, associated with a general loss of innervation, manifesting itself by talkative wanderings of the mind, restless sleep, hallucinations, foolish activity, attacks of tremor senilis, etc. The intellectual functions diminish and the memory is lost. The physical forces also gradually sink, the tremor senilis increases, and the patient, no more able to walk, becomes confined to bed. Finally, a relaxation of the sphincters takes place, and death is produced by the disturbance of the automatic functions of deglutition and respiration.
Total atrophy of the brain, when due to an extensive meningitis or to a general disturbance of the nutrition, as is met with in drunkards, may finally lead to a condition known as general paralysis of the insane. This disease, however, will be found treated elsewhere in this work.
TREATMENT.—There is no special treatment for atrophy of the brain; all that can be done is to palliate and combat the symptoms as they arise.
INTRODUCTION.—Notwithstanding the numerous measurings and weighings of human brains made in the course of time by different investigators, no absolute standard measure or weight has as yet been established by which we can accurately determine a pathological increase or decrease in the size and weight of this organ. The want of such a standard is principally due to the difference generally existing in the dimensions and weights of even a certain number of brains taken from individuals belonging to the same race or nation. The same difficulties are met with in the attempt at establishing a rule by which to measure the mental capacity of a certain brain, for the question has as yet not been solved whether this capacity depends upon the quantity or quality of the brain-substance. In speaking of hypertrophy of the brain, therefore, we must keep in mind that a large brain must not be considered hypertrophied unless there exists a disproportion between its size and that of the cavity from which it was removed; in other words, when its growth or hypertrophy meets a resistance at the inner walls of the cranial cavity. According to Virchow, a further distinction must be made between the increase (hyperplasia) of the nervous elements themselves and that of the supporting connective tissue, the neuroglia. To the latter condition particularly corresponds the peculiar doughy consistence of the white substance of hypertrophied brains.
[p. 997]ETIOLOGY.—Hypertrophy of the brain is sometimes congenital, and then associated with dwarfishness and a defective development of the cranium. Generally, however, it is an extra-uterine affection, originating mostly during infancy and childhood, though it is also met with at the age of puberty, and even in adult life. The male sex is more predisposed to the affection than the female. When hypertrophy of the brain occurs during infancy, it is almost always associated with an excessive development of the lymphatic glands, with a defective involution of the thymus gland, and with rachitis, but generally without cachexia. No special exciting cause can be assigned to the affection during youth or adult age, though it has been stated that during these periods of life the disease may supervene upon tubercle or carcinoma of the brain. Repeated active or passive congestion (Rokitanski, Andral), as well as the introduction of lead into the system, has also been supposed to incite the disease.
PATHOLOGICAL ANATOMY.—Directly after the removal of the vault of the cranium, and on cutting through the dura mater, the brain, as if liberated from pressure, is observed to swell out to such a degree as to render the replacement of the removed skull-cap impossible. The enveloping membranes are found closely adapted to one another and to the brain; they are very thin, bloodless, and dry, and their vessels are empty and pressed flat. The hemispheres of the cerebrum are large, and their convolutions, mutually pressing against one another, are flattened at their surfaces, so that the intervening sulci are hardly recognizable. After the removal of the brain from the skull the abnormal dimensions of the cerebrum present a remarkable contrast to the normal size of the cerebellum, pons, and medulla oblongata, which also appear flat and broad from pressure. When a horizontal section is made through the hemispheres of the cerebrum and a little above the corpus callosum, the centrum ovale appears unusually large. The cavities of the ventricles are very narrow, their walls touching one another. There is no serum in the pia mater or in the ventricles. The substance of the brain is pale, bloodless, and dry. The white substance, upon which the hypertrophy particularly depends, is of a doughy consistence, comparable to the boiled white of an egg or cheese, whilst the gray substance is so pale as to be hardly distinguishable from the former.
The condition of the skull is, according to Rokitanski,1 as follows: In cases in which the hypertrophy of the brain has advanced to a high degree, and in which the sutures of the skull are united, the bones of the cranium are found thinner and their inner table roughened by absorption. This is especially the case in the bones which form the vault of the cranium. The holes or other deficiencies found at the base of the cranium in the plates of the frontal, ethmoid, and sphenoid bones are not entirely due to the absorbing process, but rather to the thinness of these bones. In infants the cavity of the cranium enlarges in proportion to the hypertrophy of its contents; the head then resembles in form so much that of hydrocephalus that it may lead to errors in diagnosis. In some cases in which the disease rapidly develops to a high degree there is observed on the infant's skull a loosening and separation of the sutures of the cranial vault, with red coloration and suffusion of their cartilages.
1 Lehrbuch der Pathologischen Anatomie, 3d ed., 1855, vol. ii. p. 431.[p. 998]
SYMPTOMS.—There is a gradually increasing muscular weakness, manifesting itself especially in the lower extremities, and giving rise to an unsteady, stumbling gait and frequent falling, caused perhaps by the excessive weight of the head, and also an inability of securely grasping objects. Besides these disturbances of motion, epileptic spasms appear, at first light in degree and at long intervals, but becoming later on in the course of the disease more frequent and severe. Continuous or intermittent attacks of headache almost always accompany the disease, and, furthermore, vertigo, tinnitus aurium, photophobia, and dimness of sight with dilatation of the pupil; general sensation also becomes blunted, but without ever amounting to anæsthesia. In a number of cases there is no disturbance of the psychical functions, though in others symptoms of mental excitement amounting even to delirium have been observed. Most frequently the intelligence sinks from the beginning of the disease, to end in complete idiocy. The pulse also has been observed to fall considerably during the last stage.
The COURSE of the disease is, according to Andral and Hasse,2 almost always chronic, and if an acute development of the affection has been spoken of, it may be supposed that the latter has commenced a considerable time previous to the manifestation of the symptoms during the last stage. Andral divides the disease into two stages, of which the first is chronic and frequently latent, whilst the other is more acute and leads to a rapid fatal termination. In most cases death is caused by such intercurrent affections as give rise to irritation and hyperæmia of the brain, and thus increase the already abnormal pressure upon this organ.
2 “Krankheiten des Nervensystems,” 2d ed., 1869, in Handbuch der Speciellen Pathologie und Therapie, edited by R. Virchow, vol. iv. 1st div., p. 578.
DIAGNOSIS, PROGNOSIS, AND TREATMENT.—It has already been mentioned that errors in diagnosis may very easily be committed on account of the great resemblance in the form of the head in cases of hypertrophy of the brain and of hydrocephalus, though it has been stated that in the former affection convulsions, in the form of epileptic spasms, predominate, to be followed during the last stage by symptoms of depression; whilst in hydrocephalus the symptoms of depression manifest themselves from the beginning of the disease, and, moreover, the rachitic deformities are more prominently shown in the form of a chicken-breast. A positive diagnosis can only be made by the autopsy.
There are no remarks to be made on the prognosis and treatment of hypertrophy of the brain.
Syphilitic affections of the nerve-centres are best studied by separating those of the spinal cord from those of the cerebrum, and in the present article this natural division of the subject is adopted. Further, cerebral syphilis in its most characteristic or gummatous form usually attacks the brain-membranes, or perhaps in some cases the perivascular sheaths of the vessels, and only secondarily affects the tissue of the brain itself. The question of the occurrence of specific disease of the brain-cortex is so important that it shall have a separate discussion. It is perfectly well proven that with or without other brain lesion the vessels of the brain may undergo an atheromatous degeneration as the direct result of a syphilitic dyscrasia; but such disease links itself on the one hand with the subject of syphilitic disease of the general vascular system, and on the other hand with cerebral apoplexies, softenings, and other degenerations. Moreover, the space here allotted to brain syphilis is very insufficient. I, therefore, shall not enter upon the further discussion of syphilitic degeneration of the brain-vessels. The etiology of brain and spinal syphilis is best discussed under one heading.
GENERAL ETIOLOGY.—We do not know why in any individual case syphilis selects one portion of the nervous centres rather than another for attack; indeed, it is only rarely that any exciting cause can be discovered.
It is not unnatural to expect that any agency which is capable of exciting an inflammation of a nerve-centre may, when present in a syphilitic person, provoke a specific disease of such centre. Thus, thermic fever is a very common cause of chronic meningitis, and in the Journ. de Méd. et Chir. (Paris, 1879, p. 191) a case is reported in which cerebral syphilis followed a sunstroke; I have myself seen one similar instance, and in Roberts's case of precocious cerebral syphilis (see p. 804) the first convulsion came whilst the man was fishing on a very hot day, and may have been precipitated by the exposure.
Blows and other traumatisms would be expected to figure largely as exciting causes of nervous syphilis, but they, in fact, are only rarely present. I have seen one or two cases of specific brain disease attributed to violence by the patient, and several cases of possibly specific spinal [p. 1000] disease—one in which a poliomyelitis followed a fall on the ice; one in which, after a fall from a cart and marked spinal concussion, a local myelitis developed;1 and one of a general myelitis following an injury by a horse. The only records of such cases are those of Broadbent2 and those collected by Heubner.3
1 Univers. Hosp. Dispen. Service-Book, x., 1875, p. 58.
2 Lond. Lancet, 1876, ii. p. 741.
3 Ziemssen's Encyclopædia, xii. 301.
Various authorities attach much influence to over-study and other forms of cerebral strain in exciting brain syphilis. Engelstedt is stated to have reported cases having such etiological relations, and Fournier4 affirms that he has especially seen the disease in professional men and other persons habitually exercising their brains to excess. Neither in private nor public practice have I met with an instance where over-brainwork could be considered a distinct etiological factor, whilst I have seen some hundreds of cases from amongst the laboring classes, in whom the intellectual faculties are chiefly dormant.
4 La Syphilis du Cerveau.
The drift of the evidence in medical literature is so pronounced, and so in accord with my own experience, that I believe it may be positively affirmed that in the vast majority of cases of nervous syphilis no exciting cause can be found.
Inherited syphilis seems to be less prone than the acquired diathesis to attack the nervous system, but is certainly capable of so acting. As early as 1779, Joseph Glenck5 reported a case of a girl, six years old, cured by a mercurial course of an epilepsy of three years' standing and of other manifestations of hereditary syphilis. Graefe found gummatous tumors in the cerebrum of a child nearly two years old.6 O. Huebner7 details the occurrence of pachymeningitis hæmorrhagica in a syphilitic infant under a year old. Hans Chiari8 reports a case in which very pronounced syphilitic degeneration of the brain-vessels was found in a child fourteen months old. Both Barlow9 and T. S. Dowse10 report cases of nerve syphilis in male infants of fifteen months. For other similar cases the reader is referred to an article by J. Parrott,11 and to a paper by M. E. Troisier.12
5 Doctrina de Morbis Venereis, Vienna.
6 Arch. f. Ophthalm., Bd. i. Erst Abth.
7 Virchow's Archiv, Bd. lxxxiv. 269.
8 Wien. Med. Wochenschrift, xxxi. 1881, 17.
9 Lond. Patholog. Soc. Trans., 1877.
10 The Brain and its Diseases, vol. i. p. 76.
11 Archiv. de Physiologie, 1871-72, p. 319; also to his “Leçons sur le Syphilis hered.,” Progrès méd., 1877 and 1878.
12 Arch. de Tocologie, x. 411.
Recorded cases prove decisively that even after puberty specific nervous affections may primarily attack the unfortunate offspring. Thus, Nettleship reports13 the development of a cerebral gumma in a girl of ten years, and J. A.. Ormerod14 of a tumor of the median nerve (probably gummatous) in a woman of twenty-three, both the subjects of inherited syphilis. Thomas S. Dowse15 details a case of cerebral gumma at the age of ten years, and Samuel Wilks16 one of epilepsy, from inherited taint, in a boy of fourteen. J. Hughlings-Jackson reports17 paraplegia with epilepsy in a boy of eight, hemiplegia in a girl of eighteen, and hemiplegia in a woman of twenty-two;18 the nervous affection in each case being associated with or dependent upon inherited syphilis. E. Mendel reports19 a case of a child [p. 1001] who had inherited syphilis, and developed in her fifteenth year a maniacal attack with hallucinations. I have seen cerebral syphilis occur at twenty-one years of age as the first evident outbreak of the inherited disorder.
13 Trans. Lond. Path. Soc., xxxii. 13.
14 Ibid., p. 14.
15 Loc. cit., p. 71.
16 Lectures on Dis. of Nerv. Syst., Philada., 1878, p. 333.
17 Journ. Ment. and Nerv. Diseases, 1875, p. 516.
18 Brit. Med. Journal, May 18, 1872.
19 Archiv f. Psychiatrie, Bd. i. 313.
When a nervous affection develops first at a comparatively late period, and no very apparent evidences of the inherited taint are present, there is great danger of the case being misunderstood; indeed, in some instances an immediate diagnosis may be scarcely possible. It is probable that in most of the reported recoveries from alleged tubercular meningitis the disease has been syphilitic.
Some time since I saw, in an orphan of fourteen, a chronic basal meningitis, and in the absence of any history and of any evidences of syphilis gave the fatal prognosis of tubercular disease; but, to my astonishment, under the long-continued and free use of iodide of potassium complete recovery occurred. Another child, reported by a very good practitioner as cured of tubercular meningitis, and afterward for a long time under my own care, I believe suffered from hereditary syphilis. Cases of this character have also been reported by F. Dreyfous.20
20 Revue mensuelle des Malad. des Enfants, 1883, i. 497; see also Gaz. hébdom. Sci. méd. de Montpellier, 1883, v. 89.
It is of course very important to diagnose between a tubercular meningitis and one due to hereditary syphilis. Without a history certainty is not possible, but a general indefiniteness of symptoms and slowness of progression should arouse suspicion, especially if the absence of the pulse-retardation indicated that the vault rather than the base of the cranium was involved.
The relation of inherited syphilis to various nervous affections not distinctly specific cannot yet be determined. Arrested development, and the consequent epilepsy, idiocy,21 early brain sclerosis, are probably sometimes due to the inheritance; and the cases collected by E. Mendel22 show that chronic hydrocephalus is frequently of specific origin.23
21 See Brain, vol. vii. 409.
22 Archiv f. Psychiatrie, Bd. i. 309.
23 See, also, Virchow's Archiv, Bd. xxxviii. p. 129.
Another very important question connected with the etiology of these disorders is as to the time of their development. Nervous diseases following acquired syphilitic infection certainly belong to the advanced stages of the disorder. Huebner reports24 a case in which thirty years elapsed between the contraction of the chancre and the nervous explosion. I have seen a similar period of thirty years. Fournier reports intervals of twenty-five years, and thinks from the third to the tenth year is the period of maximum frequency of nervous accidents.
24 Ziemssen's Encyclopædia, xii. 298, New York ed.
The fact that nervous syphilis may occur many years after the cessation of all apparent evidences of the diathesis is of great practical importance, especially as the nervous system is more prone to be attacked when the secondaries have been very light than when the earlier manifestations have been severe. I have repeatedly seen nervous syphilis in persons whose secondaries have been so slight as to have been entirely overlooked or forgotten, and who honestly asserted that they never had had syphilis, although they acknowledged to gonorrhœa or to repeated exposure, and confessed that their asserted exemption was due to good fortune rather than to chastity.
[p. 1002]The following citations prove that this experience is not peculiar. Dowse25 says: “Often have I had patients totally ignorant of having at any time acquired or experienced the signs or symptoms of syphilis in its primary and secondary stages, yet the sequelæ have been made manifest in many ways, particularly in many of the obscure diseases of the nervous system.” Buzzard26 reports a case of nervous syphilis where the patient was unconscious of the previous existence of a chancre or of any secondaries. Rinecker also calls attention27 to the frequency of nervous syphilis in persons who afford no distinct history of secondary symptoms.
25 The Brain and its Diseases, London, 1879, vol. i. p. 7.
26 Syphilitic Nervous Affections, London, 1874, p. 80.
27 Archiv f. Psychiatrie, vii. p. 241.
Although syphilis is prone to attack the nervous system many years after infection, it would be a fatal mistake to suppose that nervous disease may not rapidly follow the chancre. What is the minimum possible intermediate period we do not know, but it is certainly very brief, as is shown by the following cases of this so-called precocious nervous syphilis. Alfrik Ljunggrén of Stockholm reports28 the case of H. R——, who had a rapidly-healed chancre in March, followed in May of the same year by a severe headache, mental confusion, and giddiness. Early in July H. R—— had an epileptic attack, but was finally cured by active antisyphilitic treatment. Although the history is not explicit, the nervous symptoms appear to have preceded the development of distinct secondaries other than rheumatic pains.
28 Archiv f. Dermatol. u. Syphilis, 1870, ii. p. 155.
Davaine is said29 to have seen paralysis of the portio dura “a month after the first symptoms of constitutional syphilis.” E. Leyden30 found advanced specific degeneration of the cerebral arteries in a man who had contracted syphilis one year previously. R. W. Taylor details a case in which epilepsy occurred five months after the infection.31 In the case of M. X——, reported by Ad. Schwarz,32 headache came on the fortieth day after the appearance of the primary sore, and a hemiplegia upon the forty-sixth day. S. L——33 had a paralytic stroke without prodromes six months after the chancre. A. P. L——34 had an apoplectic attack seven months after the chancre; A. S——, one five months after her chancre. In a case which recently occurred in the practice of A. Sydney Roberts of this city the chancre appeared after a period of incubation of twenty-six days, and two months and eight days subsequent to this came the first fit; eight days after the first the second convulsion occurred, with a distinct aura, which preceded by some minutes the unconsciousness. An interesting observation in this connection is that of Ern. Gaucher35 of a spinal syphilis occurring six months after the appearance of a chancre.
29 Buzzard, Syphilitic Nervous Affections, London, 1874.
30 Zeitschrift f. klin. Med., Bd. v. 165.
31 Journ. Nervous and Mental Dis., 1876, p. 38.
32 De l'Hémiplegia syphilitique Prêcoce, Inaug. Diss., Paris, 1880.
33 Ibid.
34 Ibid.
35 Revue de Méd., 1882, ii. 678.
This citation of cases might be much extended, but is sufficient to show that nervous syphilis occurs not very rarely within six months after infection, and may be present in two months.
CLINICAL HISTORY.—Brain syphilis of the type now under consideration may declare itself with great suddenness. An apoplectic attack, a convulsive paroxysm, a violent mania, or a paralytic stroke may be the first detected evidence of the disease. In most of these cases the coming storm ought to have been foreseen, and to a greater or less degree averted. The onset of cerebral syphilis is, however, generally more gradual, the symptoms coming on slowly and successively. Proper treatment, instituted at an early stage, is usually successful, so that a careful study of these prodromes is most important. They are generally such as denote cerebral disturbance, and, although they should excite suspicion, are not diagnostic, except as occurring in connection with a specific history or under suspicious circumstances.
Headache, slight failure of memory, unwonted slowness of speech, general lassitude, and especially lack of willingness to mental exertion, sleeplessness or excessive somnolence, attacks of momentary giddiness, vertiginous feelings when straining at stool, yelling or in any way disturbing the cerebral circulation, alteration of disposition,—any of these, and, a fortiori, several of them, occurring in a syphilitic subject, should be the immediate signal of alarm, and lead to the examination of the optic discs, for in some cases the eye-ground will be found altered even during the prodromic stage. Of course if choked disc be found the diagnosis becomes practically fixed, but the absence of choked disc is no proof that the patient is free from cerebral syphilis. In regard to the individual prodromic symptoms, my own experience does not lend especial importance to any one of them, although, perhaps, headache is the most common. There is one symptom which may occur during the prodromic stage of cerebral syphilis, but is more frequent at a later stage—a symptom which is not absolutely characteristic of the disease, but which, when it occurs in a person who is not hysterical, should give rise to the strongest suspicion. I refer to the occurrence of repeated, partial, passing palsies. A momentary weakness of one arm, a slight drawing of the face disappearing in a few hours, a temporary dragging of the toe, a partial aphasia which appears and disappears, a squint which to-morrow leaves no trace, may be due to a non-specific brain tumor, to miliary cerebral aneurisms, or to some other non-specific affection; but in the great majority of cases where such phenomena occur repeatedly the patient is suffering from syphilis or hysteria.
The first type or variety of the fully-formed syphilitic meningeal disease to which attention is here directed is that of an acute meningitis. I am much inclined to doubt whether an acute syphilitic meningitis can ever develop as a primary lesion—whether it must not always be preceded by a chronic meningitis or by the formation of a gummatous tumor; but it is very certain that acute meningitis may develop when there have been no apparent symptoms, and may therefore seem to be abrupt in its onset. Some years ago I saw, in consultation, a man who in the midst of apparent health was attacked by violent meningeal convulsions, with distinct evidences of acute meningitis. He was apparently saved from death by very heroic venesection, but after his return to consciousness developed very rapidly a partial specific hemiplegia, showing that a latent gumma had [p. 1004] probably preceded the acute attack. On the other hand, an acute attack is liable at any time to supervene upon a chronic syphilitic meningitis. At the University Hospital dispensary I once diagnosed chronic cerebral syphilis in a patient who the next day was seized with violent delirium, with convulsions and typical evidences of acute meningitis, and died four or five days afterward. At the autopsy an acute meningitis was found to have been engrafted on a chronic specific lesion of a similar character. In the case reported by Gamel,36 in which intense headache, fever, and delirium came on abruptly in an old syphilitic subject and ended in general palsy and death, the symptoms were found to depend upon an acute meningitis secondary to a large gumma.
36 Tumeurs gommeuses du Cerveau, Inaug. Diss., Montpellier, 1875.
In this connection may well be cited the observation of Molinier37 in which violent delirium, convulsions, and coma occurred suddenly. A very curious case is reported by D. A. Zambaco38 in which attacks simulating acute meningitis occurring in a man with a cerebral gummatous tumor appear to have been malarial. In such a case the diagnosis of a malarial paroxysm could only be made out by the presence of the cold stage, the transient nature of the attack, its going off with a sweat, its periodical recurrence, and the therapeutic effect on it of quinine.
37 Revue méd. de Toulouse, xiv. 1880, 341.
38 Des Affections nerveuses-syphilitiques, Paris, 1862, p. 485.
In the cases of chronic brain syphilis which have come under my observation, most usually after a greater or less continuance of prodromes such as have been mentioned, epileptic attacks have occurred with a hemiplegia, or a monoplegia, which is almost invariably incomplete and usually progressive; very frequently diplopia is manifested before the epilepsy, and on careful examination is found to be due to weakness of some of the ocular muscles. Not rarely oculo-motor palsy is an early and pronounced symptom, and a marked paralytic squint is very common. Along with the development of these symptoms there is almost always distinct failure of the general health and progressive intellectual deterioration, as shown by loss of memory, failure of the power to fix the attention, mental bewilderment, and perhaps aphasia. If the case convalesce under treatment, the amelioration is gradual, the patient travelling slowly up the road he has come down. If the case end fatally, it is usually by a gradual sinking into complete paralysis, or the patient is carried off by an acute inflammatory exacerbation, or, as in two of my cases, amelioration may be rapidly occurring and a very violent epileptic fit produce a sudden fatal asphyxia. Death from brain-softening around the tumor is not infrequent, but a fatal apoplectic hemorrhage is rare.
The clinical varieties of cerebral meningeal syphilis are so polymorphic and kaleidoscopic that it is almost impossible to reduce them to order for descriptive purposes. Fournier separates them into the cephalic, congestive, epileptic, aphasic, mental, and paralytic, but scarcely facilitates description by so doing. Heubner makes the following types:
"1. Psychical disturbances, with epilepsy, incomplete paralysis (seldom of the cranial nerves), and a final comatose condition, usually of short duration.
"2. Genuine apoplectic attacks with succeeding hemiplegia, in connection with peculiar somnolent conditions, occurring in often-repeated [p. 1005] episodes; frequently phenomena of unilateral irritation, and generally at the same time paralyses of the cerebral nerves.
"3. Course of the cerebral disease similar to paralytica dementia.”
In regard to these types, the latter seems to me clear and well defined, but contains those cases which I shall discuss under the head of Cortical Disease.
Meningeal syphilis as seen in this country does not conform rigidly with the other asserted types, although there is this much of agreement, that when the epilepsy is pronounced the basal cranial nerves are not usually paralyzed, the reason of this being that epilepsy is especially produced when the gummatous change is in the ventricles or on the upper cortex. In basal affections the epileptoid spells, if they occur at all, are usually of the form of petit mal; but this rule is general, not absolute. The apoplectic somnolent form of cerebral syphilis, for some reason, is rare in this city, and it seems necessary to add to those of Heubner's a fourth type to which a large proportion of our cases conform. This type I would characterize as follows:
4. Psychical disturbance without complete epileptic convulsions, associated with palsy of the basal nerves and often with partial hemiplegia.
The most satisfactory way of approaching this subject is, however, to study the important symptoms in severalty, rather than to attempt to group them into recognizable varieties of the disease; and this method I shall here adopt.
Headache is the most constant and usually the earliest symptom of meningeal syphilis; but it may be absent, especially when the lesion is located in the reflexions of the meninges which dip into the ventricles, or when the basal gumma is small and not surrounded with much inflammation. The length of time it may continue without the development of other distinct symptoms is remarkable. In one case39 at the University Dispensary the patient affirmed that he had had it for four years before other causes of complaint appeared. It sometimes disappears when other manifestations develop. It varies almost indefinitely in its type, but is, except in very rare cases, at least so far paroxysmal as to be subject to pronounced exacerbations. In most instances it is entirely paroxysmal; and a curious circumstance is, that very often these paroxysms may occur only at long intervals: such distant paroxysms are usually very severe, and are often accompanied by dizziness, sick stomach, partial unconsciousness, or even by more marked congestive symptoms. The pain may seem to fill the whole cranium, may be located in a cerebral region, or fixed in a very limited spot. Heubner asserts that when this headache can be localized it is generally made distinctly worse by pressure at certain points, but my own experience is hardly in accord with this. Any such soreness plainly cannot directly depend upon the cerebral lesion, but must be a reflex phenomenon or due to a neuritis. According to my own experience, localized soreness indicates an affection of the bone or of its periosteum. In many cases, especially when the headache is persistent, there are distinct nocturnal exacerbations.
39 Book Y., p. 88, 1879.
It will be seen that there is nothing absolutely characteristic in the headache of cerebral syphilis; but excessive persistency, apparent causelessness, and a tendency to nocturnal exacerbation should in any [p. 1006] cephalalgia excite suspicion of a specific origin—a suspicion which is always to be increased by the occurrence of slight spells of giddiness or by delirious mental wandering accompanying the paroxysms of pain. When an acute inflammatory attack supervenes upon a specific meningeal disease it is usually ushered in by a headache of intolerable severity.
When the headache in any case is habitually very constant and severe, the disease is probably in the dura mater or periosteum; and this probability is much increased if the pain be local and augmented by firm, hard pressure upon the skull over the seat of the pain.
Disorders of Sleep.—There are two antagonistic disorders of sleep, either of which may occur in cerebral syphilis, but which have only been present in a small proportion of the cases that I have seen. Insomnia is more apt to be troublesome in the prodromic than in the later stages, and is only of significance when combined with other more characteristic symptoms. A peculiar somnolence is of much more determinate import. It is not pathognomonic of cerebral syphilis, yet of all the single phenomena of this disease it is the most characteristic. Its absence is of no import in the theory of an individual case.
As I have seen it, it occurs in two forms: In the one variety the patient sits all day long or lies in bed in a state of semi-stupor, indifferent to everything, but capable of being aroused, answering questions slowly, imperfectly, and without complaint, but in an instant dropping off again into his quietude. In the other variety the sufferer may still be able to work, but often falls asleep while at his tasks, and especially toward evening has an irresistible desire to slumber, which leads him to pass, it may be, half of his time in sleep. This state of partial sleep may precede that of the more continuous stupor, or may pass off when an attack of hemiplegia seems to divert the symptoms. The mental phenomena in the more severe cases of somnolency are peculiar. The patient can be aroused—indeed in many instances he exists in a state of torpor rather than of sleep; when stirred up he thinks with extreme slowness, and may appear to have a form of aphasia; yet at intervals he may be endowed with a peculiar automatic activity, especially at night. Getting out of bed; wandering aimlessly and seemingly without knowledge of where he is, and unable to find his own bed; passing his excretions in a corner of the room or in other similar place, not because he is unable to control his bladder and bowels, but because he believes that he is in a proper place for such act,—he seems a restless nocturnal automaton rather than a man. In some cases the somnolent patient lies in a perpetual stupor.
An important fact in connection with the somnolence is that it may develop suddenly without marked premonition. Thus in a case reported by J. A. Ormerod40 a man who had been in good health, save only for headache, awoke one morning in a semi-delirious condition, and for three days slept steadily, only arousing for meals; after this there was impairment of memory and mental faculties, but no more marked symptoms.
40 Brain, vol. v. 260.
Apathy and indifference are the characteristics of the somnolent state, yet the patient will sometimes show excessive irritability when aroused, and will at other periods complain bitterly of pain in his head, or will groan as though suffering severely in the midst of his stupor—at a time, [p. 1007] too, when he is not able to recognize the seat of the pain. I have seen a man with a vacant, apathetic face, almost complete aphasia, persistent heaviness and stupor, arouse himself when the stir in the ward told him that the attending physician was present, and come forward in a dazed, highly pathetic manner, by signs and broken utterances begging for something to relieve his head. Heubner speaks of cases in which the irritability was such that the patient fought vigorously when aroused; this I have not seen.
This somnolent condition may last many weeks. T. Buzzard41 details the case of a man who after a specific hemiplegia lay silent and somnolent for a month, and yet finally recovered so completely as to win a rowing-match on the Thames. I have seen a fair degree of recovery after a somnolence of four months' duration.
41 Clinical Lectures on Dis. Nerv. Syst., London, 1882.
In its excessive development syphilitic stupor puts on the symptoms of advanced brain-softening, to which it is indeed often due. Of the two cases with fatal result of which I have notes, one at the autopsy was found to have symmetrical purulent breaking down of the anterior cerebral lobes; the other, softening of the right frontal and temporal lobes, due to the pressure of a gummatous tumor, and ending in a fatal apoplexy.
This close connection with cerebral softening explains the clinical fact that apoplectic hemorrhage is very apt to end the life in these cases of somnolent syphilis. But a prolonged deep stupor in persons suffering from cerebral syphilis does not prove the existence of extensive brain-softening, and is not incompatible with subsequent complete recovery. As an element of prognosis it is of serious but not of fatal import.
Paralysis.—When it is remembered that a syphilitic exudation may appear at almost any position in the brain, that spots of encephalic softening are a not rare result of the infection, that syphilitic disease is a common cause of cerebral hemorrhage, it is plain that a specific palsy may be of any conceivable variety, and affect either the sensory, motor, or intellectual sphere. The mode of onset is as various as the character of the palsy. The attack may be instantaneous, sudden, or gradual. The gradual development of the syphilitic gumma would lead us, a priori, to expect an equally gradual development of the palsy; but experience shows that in a large proportion of the cases the paralysis appears suddenly, with or without the occurrence of an apoplectic or epileptic fit. Under these circumstances it will be usually noted that the resulting palsy is incomplete; in rare instances it may be at its worst when the patient awakes from the apoplectic seizure, but usually it progressively increases for a few hours, and then becomes stationary. These sudden partial palsies probably result from an intense congestion around the seat of disease or from stoppage of the circulation in the same locality; whatever their mechanism may be, it is important to distinguish them from palsies which are due to hemorrhage. I believe this can usually be done by noting the degree of paralysis.
A suddenly-developed, complete hemiplegia or other paralysis may be considered as in all probability either hemorrhagic or produced by a thrombus so large that the results will be disorganization of the brain-substance, and a future no more hopeful than that of a clot. On the [p. 1008] other hand, an incomplete palsy may be rationally believed to be due to pressure or other removable cause; and this belief is much strengthened by a gradual development. The bearing of these facts upon prognosis it is scarcely necessary to point out.
Although the gummata may develop at almost any point, they especially affect the base of the brain, and are prone to involve the nerves which issue from it. Morbid exudations, not tubercular or syphilitic, are rare in this region. Hence a rapidly but not abruptly appearing strabismus, ptosis, dilated pupil, or any paralytic eye symptom in the adult is usually of syphilitic nature. Syphilitic facial palsy is not so frequent, whilst paralysis of the nerve from rheumatic and other inflammation within its bony canal is very common. Paralysis of the facial nerve may therefore be specific, but existing alone is of no diagnostic value. Since syphilitic palsies about the head are in most instances due to pressure upon the nerve-trunks, the electrical reactions of degeneration are present in the affected muscles.
There is one peculiarity about specific palsies which has already been alluded to as frequently present—namely, a temporary, transient, fugitive, varying character and seat. Thus an arm may be weak to-day, strong to-morrow, and the next day feeble again, or the recovered arm may retain its power and a leg fail in its stead. These transient palsies are much more apt to involve large than small brain territories. The explanation of their largeness, fugitiveness, and incompleteness is that they are not directly due to clots or other structural changes, but to congestions of the brain-tissues in the neighborhood of gummatous exudations. Squint due to direct pressure on a nerve will remain when the accompanying monoplegia due to congestion disappears.
Motor palsies are more frequent than sensory affections in syphilis, but hemianæsthesia, localized anæsthetic tracts, indeed any form of sensory paralysis, may occur. Numbness, formications, all varieties of paræsthesia, are frequently felt in the face, body, or extremities. Violent peripheral neuralgic pains are rare, and generally when present denote neuritis. Huguenin, however, reports42 a severe trigeminal anæsthesia dolorosa, which was found, after death from intercurrent disease, to have depended upon a small gumma pressing upon the Gasserian ganglion. A somewhat similar case has also been reported by Allen McLane Hamilton.43
42 Schwiez. Corr. Blät., 1875.
43 Alienist and Neurologist, iv. 58.
The special senses are liable to suffer from the invasion of their territories by cerebral syphilis, and the resulting palsies follow courses and have clinical histories parallel to those of the motor sphere. The onset may be sudden or gradual, the result temporary or permanent. Charles Mauriac44 reports a case in which the patient was frequently seized with sudden attacks of severe frontal pain and complete blindness lasting from a quarter to half an hour; at other times the same patient had spells of aphasia lasting only for one or two minutes. I have seen two cases of nearly complete deafness developing in a few hours in cerebral syphilis, and disappearing abruptly after some days. Like other syphilitic palsies, therefore, paralyses of special senses may come on suddenly or gradually, and may occur paroxysmally.
44 Loc. cit., p. 31.
Among the palsies of cerebral syphilis must be ranked aphasia. An [p. 1009] examination of recorded cases shows that syphilitic aphasia is subject to vagaries and laws similar to those connected with other specific cerebral palsies. It is usually a symptom of advanced disease, but may certainly develop as one of the first evidences of cerebral syphilis. Coming on after an apoplectic or epileptic fit, it may be complete or incomplete: owing to the smallness of the centre involved and the ease with which its function is held in abeyance, a total loss of word-thought is not so decisive as to the existence of cerebral hemorrhage as is a total motor palsy. Like hemiplegia or monoplegia, specific aphasia is sometimes transitory and paroxysmal. Buzzard45 records several such cases. Mauriac46 details a very curious case in which a patient, after long suffering from headache, was seized by sudden loss of power in the right hand and fingers, lasting about ten minutes only, but recurring many times a day. After this had continued some time the paroxysms became more completely paralytic, and were accompanyed by loss of the power of finding words, the height of the crises in the palsy and aphasia being simultaneously reached. For a whole month these attacks occurred five or six times a day, without other symptoms except headache, and then the patient became persistently paralytic and aphasic, but finally recovered. To describe the different forms of specific aphasia and their mechanism of production would be to enter upon a discussion of aphasia itself—a discussion out of place here. Suffice it to say that every conceivable form of the disorder may be induced by syphilis.
45 Loc. cit., p. 81.
46 Aphasie et Hemiplégia droite Syphilit., Paris, 1877.
Owing to the centres of speech being situated in the cortical portion of the brain, aphasia in cerebral syphilis is very frequently associated with epilepsy. Of course right-sided palsy and aphasia are united in syphilitic as in other disorders. If, however, the statistics given by Tanowsky47 be reliable, syphilitic aphasia is associated with left-sided hemiplegia in a most extraordinarily large proportion. Thus in 53 cases collected by Tanowsky, 18 times was there right-sided hemiplegia, and 14 times left-sided hemiplegia, the other cases being not at all hemiplegic. Judging from the autopsy on a case reported in Mauriac's brochure, this concurrence of left-sided paralysis and aphasia depends partly upon the great frequency of multiple brain lesions in syphilis, and partly upon the habitual involvement of large territories of the gray matter secondarily to diseased membrane. An important practical deduction is that the conjoint existence of left hemiplegia and aphasia is almost diagnostic of cerebral syphilis.
47 L'Aphasie syphilitique.
Probably amongst the palsies may be considered the disturbances of the renal functions, which are only rarely met with in cerebral syphilis, and which are probably usually dependent upon the specific exudation pressing upon the vaso-motor centres in the medulla. Fournier speaks of having notes of six cases in which polyuria with its accompaniment, polydipsia, was present, and details a case in which the specific growth was found in the floor of the fourth ventricle. Cases have been reported of true saccharine diabetes due to cerebral syphilis,48 and I can add to these an observation of my own. The symptoms, which occurred in a [p. 1010] man of middle age, with a distinct specific history, were headache, nearly complete hemiplegia, and mental failure, associated with the passage of comparatively small quantities of a urine so highly saccharine as to be really a syrup. Under the influence of the iodide of potassium the sugar in a few weeks disappeared from the urine.
48 Consult Servantié, Des Rapports du Diabète et de la Syphilis, Paris, Thèse, 1876; also, case reported by L. Putzel, New York Med. Record, xxv. 450.
Epilepsy.—Epileptic attacks are a very common symptom of meningeal syphilis, and are of great diagnostic value. The occurrence in an adult of an epileptic attack or of an apoplectic fit, or of a hemiplegia after a history of intense and protracted headache, should always excite grave suspicion.
Before I had read Fournier's work on Nervous Syphilis I taught that an epilepsy appearing after thirty years of age was very rarely, if ever, essential epilepsy, and unless alcoholism, uræmic poison, or other adequate cause could be found was in nine cases out of ten specific; and I therefore quote with satisfaction Fournier's words: “L'épilepsie vraie, ne fait jamais son premier dêbut à l'âge adulte, à l'âge mûr. Si un homme adulte, au dessus de 30, 35, à 40 ans, vient, à être pris pour la première fois d'une crise épileptique, et cela dans la cours d'une bonne santé apparente, il y a, je vous le répète, hui ou neuf chances sur dix pour que cette épilepsie soit d'origine syphilitique.”
Syphilitic epilepsy may occur either in the form of petit mal or of haut mal, and in either case may take on the exact characters and sequence of phenomena which belong to the so-called idiopathic or essential epilepsy. The momentary loss of consciousness of petit mal will usually, however, be found to be associated with attacks in which, although voluntary power is suspended, memory recalls what has happened during the paroxysm—attacks, therefore, which simulate those of hysteria, and which may lead to an error of diagnosis.
Even in the fully-developed type of the convulsions the aura is only rarely present. Its absence is not, however, of diagnostic value, because it is frequently not present in essential epilepsy, and it may be pronounced in the specific disease. It is said that when in an individual case the aura has once appeared the same type or form of approach of the convulsion is thereafter rigidly adhered to. The aura is sometimes bizarre: a severe pain in the foot, a localized cramp, a peculiar sensation, indescribable and unreal in its feeling, may be the first warning of the attack. An aura may affect a special sense. Thus, I have at present a patient whose attacks begin with blindness.
In many, perhaps most, cases of specific convulsions, instead of a paroxysm of essential epilepsy being closely simulated, the movements are in the onset, or more rarely throughout the paroxysm, unilateral; indeed, they may be confined to one extremity. This restriction of movement has been held to be almost characteristic of syphilitic epilepsy, but it is not so. Whatever diagnostic significance such restriction of the convulsion has is simply to indicate that the fit is due to a cortical organic lesion of some kind. Tumors, scleroses, and other organic lesions of the brain-cortex are as prone to cause unilateral or monoplegic epilepsy when they are not specific as when they are due to syphilis.
Sometimes an epilepsy dependent upon a specific lesion implicating the brain-cortex may be replaced by a spasm which is more or less local and is not attended with any loss of consciousness. Thus, in a case now [p. 1011] convalescent in the University Hospital, a man aged about thirty-five offered a history of repeated epileptic convulsions, but at the time of his entrance into the hospital, instead of epileptic attacks, there was a painless tic. The spasms, which were clonic and occurred very many times a day, sometimes every five minutes, were very violent, and mostly confined to the left facial nerve distribution. The trigeminus was never affected, but in the severer paroxysms the left hypoglossal and spinal accessory nerves were profoundly implicated in all of their branches. Once, fatal asphyxia from recurrent laryngeal spasm of the glottis was apparently averted only by the free inhalation of the nitrite of amyl. The sole other symptom was headache, but the specific history was clear and the effect of antisyphilitic remedies rapid and pronounced.
It is very plain that such attacks as those just detailed are closely allied to epilepsy; indeed, there are cases of cerebral syphilis in which widespread general spasms occur similar to those of a Jacksonian epilepsy, except that consciousness is not lost, because the nervous discharge does not overwhelm the centres which are connected with consciousness.49 On the other hand, these epileptoid spasmodic cases link themselves to those in which the local brain affection manifests itself in contractions or persistent irregular clonic spasms. Contractures may exist and may simulate those of descending degeneration,50 but in my own experience are very rare.51
49 Case, Canada Med. and Surg. Journ., xi. 487.
50 Case, Centralbl. Nerv. Heilk., 1883, p. 1.
51 A case of syphilitic athetosis may be found in Lancet, 1883, ii. 989.
The clonic spasms of cerebral syphilis may assume a distinctly choreic type, or may in their severity simulate those of hysteria, throwing the body about violently.52 It is, to my mind, misleading, and therefore improper, to call such cases syphilitic chorea, as there is no reason for believing that they have a direct relation with ordinary chorea. They are the expression of an organic irritation of the brain-cortex, and are sometimes followed by paralysis of the affected member; in other words, the disease, progressing inward from the brain-membrane, first irritates, and then so invades a cortical centre as to destroy its functional power.53
52 See Allison, Amer. Med. Journ., 1877, 74.
53 Case, Chicago Med. Journ. and Exam., xlvi. 21.
Psychical Symptoms.—As already stated, apathy, somnolence, loss of memory, and general mental failure are the most frequent and characteristic mental symptoms of meningeal syphilis; but, as will be shown in the next chapter, syphilis is able to produce almost any form of insanity, and therefore mania, melancholia, erotic mania, delirium of grandeur, etc. etc. may develop along with the ordinary manifestation of cerebral syphilis, or may come on during an attack which has hitherto produced only the usual symptoms. Without attempting any exhaustive citation of cases, the following may be alluded to.
A. Erlenmeyer reports54 a case in which an attack of violent headache and vomiting was followed by paralysis of the right arm and paresis of the left leg, with some mental depression; a little later the patient suddenly became very cheerful, and shortly afterward manifested very distinctly delirium of grandeur with failure of memory. Batty Tuke reports55 a case in which, with aphasia, muscular wasting, strabismus, [p. 1012] and various palsies, there were delusions and hallucinations. In the same journal56 S. D. Williams reports a case in which there were paroxysmal violent attacks of frontal headache. The woman was very dirty in her habits, only ate when fed, and existed in a state of hypochondriacal melancholy. Leiderdorf details a case with headache, partial hemiplegia, great psychical disturbance, irritability, change of character, marked delirium of grandeur, epileptic attacks, and finally dementia, eventually cured by iodide of potassium.57 Several cases illustrating different forms of insanity are reported by N. Manssurow.58
54 Die luëtischen Psychosen.
55 Journ. Ment. Sci., Jan., 1874, p. 560.
56 April, 1869.
57 Medicin Jahrbucher, xx. 1864, p. 114.
58 Die Tertiäre Syphilis, Wien, 1877.
That the attacks of syphilitic insanity, like the palsies of syphilis, may at times be temporary and fugitive, is shown by a curious case reported by H. Hayes Newington,59 in which, along with headache, failure of memory, and ptosis in a syphilitic person, there was a brief paroxysm of noisy insanity.
59 Journ. Ment. Sci., London, xix. 555.
DIAGNOSIS.—In a diagnosis of cerebral syphilis a correct history of the antecedents of the patients is of vital importance. Since very few of the first manifestations of the disorder are absolutely characteristic, whilst almost any conceivable cerebral symptoms may arise from syphilitic disease, treatment should be at once instituted on the appearance of any disturbance of the cerebral functions in an infected person.
Very frequently the history of the case is defective, and not rarely actually misleading. Patients often appear to have no suspicion of the nature of their complaint, and will deny the possibility of syphilis, although they confess to habitual unchastity. My own inquiries have been so often misleading in their results that I attach but little weight to the statements of the patient, and in private practice avoid asking questions which might recall unpleasant memories, depending upon the symptoms themselves for the diagnosis.
The general grounds of diagnosis have been sufficiently mapped out in the last section, but some reiteration may be allowable. After the exclusion of other non-specific disease, headache occurring with any form of ocular palsy or with a history of attack of partial monoplegia or hemiplegia, vertigo, petit mal, epileptoid convulsions, or disturbances of consciousness, or attacks of unilateral or localized spasms, should lead to the practical therapeutic test. Ocular palsies, epileptic forms of attacks occurring after thirty years of age, morbid somnolence, even when existing alone, are sufficient to put the practitioner upon his guard. It is sometimes of vital importance that the nature of the cephalalgia shall be recognized before the coming on of more serious symptoms; any apparent causelessness, severity, and persistency should arouse suspicion, to be much increased by a tendency to nocturnal exacerbations or by the occurrence of mental disturbance or of giddiness at the crises of the paroxysms. Not rarely there are very early in these cases curious, almost indefinable, disturbances of cerebral functions, which may be easily overlooked, such as temporary and partial failures of memory, word-stumbling, fleeting feelings of numbness or weakness, alterations of disposition. In the absence of hysteria an indefinite and apparently disconnected series of nerve accidents is of very urgent import. To use the words of Hughlings-Jackson, “A random association or a random succession of [p. 1013] nervous symptoms is very strong warrant for a diagnosis of a syphilitic disease of the nervous system.” Cerebral syphilis occurring in an hysterical subject may be readily overlooked until fatal mischief is done. When any paralysis occurs a study of the reflexes may sometimes lead to a correct diagnosis. Thus in a hemiplegia the reflex on the affected side in cerebral syphilis is very frequently exaggerated, whilst in hysteria the reflexes are usually alike on both sides. When both motion and sensation are disturbed in an organic hemiplegia, the anæsthesia and motor paralysis occur on the same side of the body, whilst in hysteria they are usually on opposite sides.
In all cases of doubtful diagnosis the so-called therapeutic test should be employed, and if sixty grains of iodide of potassium per day fail to produce iodism, for all practical purposes the person may be considered to be a syphilitic. No less an authority than Seguin has denied the validity of this, but I believe, myself, that some of his reported cases were suffering from unsuspected syphilis. I do not deny that there are rare individuals who, although untainted, can resist the action of iodide, but in ten years' practice in large hospitals, embracing probably some thousands of cases, I have not met with more than one or two instances which I believed to be of such character. Of course in making these statements I leave out of sight persons who have by long custom become accustomed to the use of the iodide, for although in most cases such use begets increase of susceptibility, the contrary sometimes occurs. Of course the physician who should publicly assert that a patient who did not respond to the iodide had syphilis would be a great fool, but in my opinion the physician who did not act upon such a basis would be even more culpable.
PROGNOSIS.—Cerebral meningeal syphilis varies so greatly and so unexpectedly in its course that it is very difficult to establish rules for predicting the future in any given case. The general laws of prognosis in brain disease hold to some extent, but may always be favorably modified, and patients apparently at the point of death will frequently recover under treatment. The prognosis is not, however, as absolutely favorable as is sometimes believed, and especially should patients be warned of the probable recurrence of the affection even when the symptoms have entirely disappeared. The only safety after the restoration of health consists in an immediate re-treatment upon the recurrence of the slightest symptom. The occurrence of a complete, sudden hemiplegia or monoplegia is sufficient to render probable the existence of a clot, which must be subject to the same laws as though not secondary to a specific lesion. If a rapid decided rise of temperature occur in an apoplectic or epileptic attack, the prognosis becomes very grave. An epileptic paroxysm very rarely ends fatally, although it has done so in two of my cases.
The prognosis in gummatous cerebral syphilis should always be guardedly favorable. In the great majority of cases a more or less incomplete recovery occurs under appropriate treatment, and I have seen repeatedly patients who were unconscious, with urinary and fecal incontinence, and apparently dying, recover. Nevertheless, so long as there is any particle of gummatous inflammation in the membrane the patient is liable to sudden congestions of the brain, which may prove rapidly fatal, or he may die in a brief epileptic fit. On the one hand there is an [p. 1014] element of uncertainty in the most favorable case, and on the other so long as there is life a positively hopeless prognosis is not justifiable.
PATHOLOGY.—Gummatous inflammation of the brain probably always has its starting-point in the brain-membranes, although it may be situated within the brain: thus, I have seen the gummatous tumors spring from the velum interpositum in the lateral ventricle. The disease most usually attacks the base of the brain, and is especially found in the neighborhood of the pons Varolii and the optic tract. It may, however, locate itself upon the vault of the cranium, and in my experience has seemed to prefer the anterior or motor regions. The mass may be well defined and roundish, but more usually it is spread out, irregular in shape, and more or less confluent with the substance of the brain beneath it. It varies in size from a line to several inches in length, and when small is prone to be multiple. The only lesion which it resembles in gross appearance is tubercle, from which it sometimes cannot be certainly distinguished without microscopic examination.
The large gummata have not rarely two distinct zones, the inner one of which is drier, somewhat yellowish in color, opaque, and resembles the region of caseous degeneration in the tubercle. The outer zone is more pinkish and more vascular, and is semi-translucent.
On microscopic examination the most characteristic structures are small cells, such as are found in gummatous tumors in other portions of the body. These cells are most abundant in the inner zone, which, indeed, may be entirely composed of them. In the centre of the tumor they are more or less granular and atrophied; in some cases the caseous degeneration has progressed so far that the centre of the gumma consists of minute acicular crystals of fat. In the external or peripheral zone of the tumor the mass may pass imperceptibly into the normal nerve tissue, and under these circumstances it is that it contains the spider-shaped cells or stellate bodies described by Jastrowitch, and especially commented upon by Charcot and Gombault and by Coyne. These are large cells containing an exaggerated nucleus and a granular protoplasm, which continues into multiple, branching, rigid, refracting prolongations, which prolongations are scarcely stained by carmine. Alongside of these cells other largish cells are often found without prolongations, but furnished with oval nuclei and granular protoplasm. Amongst these cells will be seen the true gummatous cells, as well as the more or less altered neuroglia and nerve-elements. In the perivascular lymphatic sheaths in the outer part of the gumma is usually a great abundance of small cells. The spider-shaped cells are probably hypertrophied normal cells of the neuroglia, and have been considered by Charcot and Gombault as characteristic of syphilitic gummata of the brain. In a solitary gumma, however, of considerable size from the neighborhood of the cerebellum, studied by Coyne and Peltier, there were no stellated cells. Coyne considers that their presence is due to their previous existence in the normal state of the regions affected by the gumma. Exactly what becomes of syphilitic gumma of the brain in cases of recovery it is difficult to determine. It is certain that they become softened and disappear more or less completely, and it is probable that the cicatrices or the small peripheral cysts which are not rarely found in the surfaces of the brain are sometimes remnants of gummatous tumors. In a number of cases collected by Gros and [p. 1015] Lancereaux there were small areas of softened tissue or small calcareous and caseous masses or cerebral lacunæ corresponding to the cicatrices of softening or imperfect cysts, coincident with evidences of syphilis elsewhere. V. Cornil also states that he has found small areas of softening with well-established syphilitic lesions of the dura mater and cranium, but believes that the lacunæ or cysts depend rather upon chronic syphilitic lesions of cerebral arteries than upon gummatous inflammation.
When a gummatous tumor comes in contact with an artery, the latter is usually compressed and its walls undergo degeneration. The specific arteritis may pass beyond the limit of the syphilome and extend along the arterial wall. Not rarely there is under these circumstances a thrombus, and if the artery be a large one secondary softening of its distributive brain-area occurs.
TREATMENT.—The treatment of cerebral syphilis is best studied under two heads: First, the treatment of the accidents which occur in the course of the disease; second, the general treatment of the disease itself.
It must be remembered that in the great majority of cases in which death occurs in properly-treated cerebral syphilis the fatal result is produced by an exacerbation—or, as I have termed it, an accident—of the disease. Under these circumstances the treatment should be that which is adapted to the relief of the same acute affection when dependent upon other than specific cause. In a large proportion of cases the acute outbreak takes the form either of a meningitis or else of a brain congestion. In either instance when the symptoms are severe free bleeding should be at once resorted to. The amount of blood taken is of course to be proportionate to the severity of the symptoms and the strength of the patient. I have seen life saved by the abstraction of about a quart of blood, whilst in other cases a few ounces suffice. Care must be, of course, taken not to mistake a simple epileptic fit for a severe cerebral attack; but when this fit has been preceded by severe headache and is accompanied by stupor, with marked disturbance of the respiration, measures for immediate relief are usually required; and if the convulsions be perpetually repeated or if there be violent delirious excitement, the symptoms may be considered as very urgent. In taking blood the orifice should be large, so as to favor a rapid flow, and the bleeding be continued until a distinct impression is made upon the pulse. In some cases which I have seen in which the action of the heart continued to be violent after as much blood as was deemed prudent had been taken, good results were obtained by the hypodermic injection of three drops of the tincture of aconite-root every half hour until the reduction of the pulse and the free sweating indicated that the system was coming under the influence of the cardiac sedative.
Of course, I do not mean to encourage the improper or too free use of the lancet in these cases, but in the few fatal cases which I have seen I have almost invariably regretted that blood had not been taken at once very freely at the beginning of the acute attack. In most of these cases the symptoms had progressed too far for good to be achieved before I reached the patient. After venesection, or in feeble cases as a substitute for it, the usual measures of relief in cerebral congestion should be instituted. I shall not occupy space with a discussion of these [p. 1016] measures, as they are in no way different from those to be employed in cases not syphilitic.
The most important part of the treatment of cerebral syphilis itself is antisyphilitic, and the practitioner is at once forced to select between the iodide of potassium and the mercurial preparations. In such choice it must be remembered that even a very small amount of syphilitic deposit in the brain may at any time cause a sudden congestion or other acute attack, and is therefore a very dangerous lesion. I have seen a cerebral syphilis which was manifested only by an epileptic attack occurring once in many months, and in which after death the affected membrane was found to be not larger than a quarter of a dollar, and the deposit not more than an eighth of an inch in thickness, suddenly produce a rapidly fatal congestion; and I have known a case fast progressing toward recovery suddenly ended by the too long continuance of the arrest of respiration during an epileptic fit. I have, myself, no doubt of the superiority of the mercurials over the iodide of potassium as a means of producing absorption of gummatous exudates; and as these exudates in the brain are so very dangerous, a mercurial course should in the majority of cases of cerebral syphilis be instituted so soon as the patient comes under the practitioner's care. When, however, there is a history of a recent prolonged free use of the mercurial, or when there is marked specific cachexia, the iodide should be chosen. Cachexia is, however, a distinctly rare condition in cerebral syphilis, the disease usually developing in those who have long had apparent immunity from the constitutional disorder. In my opinion the best preparation of the mercurial for internal use is calomel. It should be given in small doses, one-quarter of one grain every two hours, guarded with opium and astringents, so as to prevent as far as possible disturbance of the bowels, and should be continued until soreness of the teeth, sponginess of the gums, or other evidences of commencing ptyalism are induced. After this the dose of the mercurial should be so reduced as simply to maintain the slight impression which has been created, and the patient should be kept under the mercurial influence for some weeks.
A very effective method of using the mercury is by inunction, and where the surroundings of the patient are suitable the mercurial ointment may be substituted for the calomel. It should be applied regularly, according to the method laid down in my treatise on therapeutics. I have sometimes gained advantage by practising the mercurial unction and at the same time giving large doses of iodide of potassium internally.
After a mercurial course the iodide of potassium should always be exhibited freely, the object being not only to overcome the natural disease, but also to bring about the complete elimination of the mercury from the system. There is no use in giving the iodide in small doses; at least a drachm and a half should be administered in the twenty-four hours, and my own custom has been to increase this to three drachms unless evidences of iodism are produced. The compound syrup of sarsaparilla covers the disagreeable taste of the iodide of potassium better than any other substance of which I have knowledge. Moreover, I am well convinced that there is some truth in the old belief that the so-called “Woods” are of value in the treatment of chronic syphilis. [p. 1017] I have seen cases in which both the iodide of potassium and the mercurials had failed to bring about the desired relief, but in which the same alteratives, when given along with the “Woods,” rapidly produced favorable results. The old-fashioned Zittmann's decoction, made according to the formula of the United States Dispensatory, may be occasionally used with very excellent effect. But I have gradually come into the habit of substituting a mixture of the compound fluid extract and the compound syrup of sarsaparilla in equal proportions. The syrup itself is too feeble to have any influence upon the system, but is here employed on account of its flavor. A favorite method of administration is to furnish the patient with two bottles—one containing a watery solution of the iodide of potassium of such strength that two drops represent one grain of the drug, and the other the sarsaparilla mixture above mentioned. From one to two drachms of the solution of the iodide may be administered in a tablespoonful of the sarsaparilla well diluted after meals. When the patient has been previously mercurialized, or there is any doubt as to the propriety of using mercurials, corrosive sublimate in small doses may be added to the solution of the iodide, so that one-tenth to one-fifteenth of a grain shall be given in each dose. I have never seen especial advantage obtained by the use of the iodides of mercury. They are no doubt effective, but are not superior to the simpler forms of the drug.
The psychical symptoms which are produced by syphilis are often very pronounced in cases in which the paralysis, headache, epilepsy, and other palpable manifestations show the presence of gross brain lesions. In the study of syphilitic disease of the brain-membranes sufficient has been said in regard to these psychical disturbances, but the problem which now offers itself for solution is as to the existence or non-existence of syphilitic insanity—i.e. of an insanity produced by specific contagion without the obvious presence of gummatous disease of the brain-membranes. Very few alienists recognize the existence of a distinct affection entitled to be called syphilitic insanity, and there are some who deny that insanity is ever directly caused by syphilis. It is certain that insanity often occurs in the syphilitic, but syphilis is abundantly joined with alcoholism, poverty, mental distress, physical ruin, and various depressing emotions and conditions which are well known to be active exciting causes of mental disorder. It may well be that syphilis is in such way an indirect cause of an insanity which under the circumstances could not be properly styled syphilitic.
If there be disease of the brain-cortex produced directly by syphilis, of course such disease must give rise to mental disorders; and if the lesion be so situated as to affect the psychic and avoid the motor regions of the brain, it will produce mental disorder without paralysis—i.e. an insanity; again, if such brain disease be widespread, involving the whole cortex, it will cause a progressive mental disorder, accompanied by gradual loss of power in all parts of the body, and ending in dementia with general paralysis; or, in other words, it will produce an affection [p. 1018] more or less closely resembling the so-called general paralysis of the insane, or dementia paralytica.
As a man having syphilis may have a disease which is not directly due to the syphilis, when a syphilitic person has any disorder there is only one positive way of determining during life how far said disorder is specific—namely, by studying its amenability to antisyphilitic treatment. In approaching the question whether a lesion found after death is specific or not, of course such a therapeutic test as that just given is inapplicable. We can only study as to the coexistence of the lesion in consideration with other lesions known to be specific. Such coexistence of course does not absolutely prove the specific nature of a nutritive change, but renders such nature exceedingly probable.
What has just been said foreshadows the method in which the subject in hand is to be here examined, and the present article naturally divides itself into two sections—the first considering the coexistence of anatomical alterations occurring in the cerebral substance with syphilitic affections of the brain-membranes or blood-vessels, the second being a clinical study of syphilitic insanity.
In looking over the literature of the subject I have found the following cases in which a cerebral sclerotic affection coincided with a gummatous disease of the membrane. Gros and Lancereaux60 report a case having a clear syphilitic history in which the dura mater was adherent to the skull. The pia mater was not adherent. Beneath, upon the vault of the brain, was a gelatinous exudation. The upper cerebral substance was indurated, and pronounced by Robin after microscopic examination to be sclerosed. At the base of the brain there were atheromatous arteries and spots of marked softening.
60 Affec. Nerv. Syphilis, 1861, p. 245.
Jos. J. Brown61 reports a case in which the symptoms were melancholia, excessive irritability, violent outbursts of temper, very positive delusions, disordered gait, ending in dementia. At the autopsy, which was very exhaustive, extensive syphilitic disease of the vessels of the brain and spinal cord was found. The pia mater was not adherent to the brain. The convolutions, particularly of the frontal and parietal lobes, were atrophied, with very wide sulci filled with bloody serum. The neuroglia of these convolutions was much increased, and “appeared to be more molecular than normal, the cells were degenerated, and in many places had disappeared, their places being only occupied by some granules.” These changes were most marked in the frontal convolutions.
61 Journ. Ment. Sci., July, 1875, p. 271.
H. Schule reports62 a very carefully and meritoriously studied case. The symptoms during life exactly simulated those of dementia paralytica. The affection commenced with an entire change in the disposition of the patient; from being taciturn, quiet, and very parsimonious, he became very excited, restless, and desiring continuously to buy in the shops. Then failure of memory, marked sense of well-being, carelessness and indifference for the future, developed consentaneously with failure of the power of walking, trembling of the hands, inequality of the pupils, and hesitating speech. There was next a period of melancholy, which was in time followed by continuous failure of mental and motor powers, and [p. 1019] very pronounced delirium of grandeur, ending in complete dementia. Death finally occurred from universal palsy, with progressive increase of the motor symptoms. At the autopsy characteristic syphilitic lesions were found in the skull, dura mater, larynx, liver, intestines, and testicles. The brain presented the macroscopic and microscopic characters of sclerosis and atrophy; the neuroglia was much increased, full of numerous nuclei, the ganglion-cells destroyed. The vessels were very much diseased, some reduced to cords; their walls were greatly thickened, and full of long spindle-shaped cells, sometimes also containing fatty granules.
62 Allgem. Zeitschrift f. Psychiatrie, xxviii. 171, 172.
C. E. Stedman and Robt. T. Edes report63 a case in which the symptoms were failure of health, ptosis, trigeminal palsy with pain (anæsthesia dolorosa), finally mental failure with gradual loss of power of motion and sensation. At the autopsy the following conditions were noted: apex of the temporal lobe adherent to dura mater and softened; exuded lymph in neighborhood of optic chiasm; sclerosis of right Gasserian ganglion, as shown in a marked increase of the neuroglia; degeneration of the basal arteries of the brain.
63 American Journ. Med. Sciences, lxix. 433.
These cases are sufficient to demonstrate that sclerosis of the brain-substance not only may coexist with a brain lesion which is certainly specific in its character, but may also present the appearance of having developed pari passu with that lesion and from the same cause.
It has already been stated in this article that cerebral meningeal syphilis may coexist with various forms of insanity, and cases have been cited in proof thereof. It is of course very probable that in some of such cases there has been that double lesion of membrane and gray brain matter which has just been demonstrated by report of autopsies; but if we find that there is a syphilitic insanity, which exists without evidences of meningeal syphilis, and is capable of being cured by antispecific treatment, such insanity must be considered as representing the disease of the gray matter of the brain. Medical literature is so gigantic that it is impossible to exhaust it, but the following list of cases is amply sufficient to prove the point at issue—namely, that there is a syphilitic insanity which exists without obvious meningeal disease, and is capable of being cured by antisyphilitic treatment:
| No. | Reporter and Journal. | Symptoms. | Results.—Remarks. |
| 1 | Luis Streisand Die Lues als Ursache der Dementia, Inaug. Diss., Berlin, 1878. |
Epilepsy, delirium of exaltation, alteration of speech, headache, failure of memory. | Rapid cure with mercury. |
| 2 | Ibid. | Delusions, delirium, general mania, great muscular weakness. | Cure with mercury. |
| 3 | Müller of Leutkirch Journ. of Mental Dis., 1873–74, 561. |
Symptoms resembling general paralysis, and diagnosis of such made until a sternal node was discovered. | Cure by iodide of potassium. |
| 4 | Esmarch and W. Jersen Allgem. Zeitschrift f. Psychiatrie. |
Sleeplessness, great excitement, restlessness, great activity, incoherence, and violence. | Cure by mercury. |
| 5 | Leidesdorf Medizin. Jahrbucher, xx., 1864, 1. |
Complete mania; played with his excrement, and entirely irrational. | Complete cure by iodide of potassium. |
| 6 | Beauregard Gaz. hébdom. de Sci. méd. de Bordeaux, 1880, p. 64. |
Symptoms resembling those of general paralysis. | Cure by iodide of potassium. |
| 7 | M. Rendu Ibid. |
Loss of memory, headache, irregularity of pupils, ambitious delirium, periods of excitement, others of depression, embarrassment of speech, access of furious delirium, ending in stupor. | Mercurial treatment, cure. |
| 8 | M. Rendu Gaz. hébdom. de Sci. méd. de Bordeaux, 1880, p. 64. |
Hypochondria, irregularity of pupils, headache, [p. 1020] failure of memory, melancholy, stupor. | Mercurial treatment, cure. |
| 9 | Albrecht Erlenmeyer Die Luëtischen Psychosen, Neuwied, 1877. |
Melancholia with hypochondriasis, sleeplessness, fear of men, and belief they were all leagued against him. | Iodide of potassium, cure. |
| 10 | Ibid. | Religious melancholia, with two attempts at suicide, ending in mania. | Iodide of potassium, cure. |
| 11 | Ibid. | At times very violent, yelling, shrieking, destroying everything she could get hands on, at times erotomania; no distinct history of infection, but her habits known to be bad, and had bone ozæna and other physical syphilitic signs. | Iodide of potassium, cure. |
| 12 | Ibid. | Epileptic attack followed by a long soporose condition, ending in mental confusion, he not knowing his nearest friends, etc.; almost dementia. | Cured by mercurial inunction. |
| 13 | Ibid. | Great fear of gensd'armes, etc., mania, with hallucinations, loud crying, yelling, etc., then convulsion, followed by great difficulty of speech. | Cured by mercurial inunctions with iodide internally; subsequently return of convulsions, followed by hemiplegia and death. |
| 14 | Ibid. | Great unnatural vivacity and loquacity, wanted to buy everything, bragged of enormous gains at play, etc.; some trouble of speech. | Iodide of potassium, cure. Attended to business, and seems as well as before. Relapsed. (See Symptoms.) |
| Ibid. Relapse of Case 14. |
Fifteen months after discharge from asylum relapse; symptoms developing very rapidly, delirium of grandeur of the most aggravated type, with marked progressive dementia, failure of power of speech, and finally of locomotion. | Failure of various anti-specific treatment. | |
| 15 | A. Erlenmeyer Die Luëtischen, etc. |
Failure of mental powers, inequality of pupils, trembling of lip when speaking, uncertainty of gait, almost entire loss of memory, once temporary ptosis and strabismus. | Iodide of potassium in ascending doses failed. Recovery under mercurial inunctions. |
| 16 | Ibid. | Failure of mental powers, pronounced delirium of grandeur, hallucinations of hearing, failure of memory, strabismus and ptosis coming on late. | Iodide of potassium, corrosive-sublimate injections. Cure. |
| 17 | Ibid. | Failure of memory and mental powers, slight ideas of grandeur, disturbance of sensibility and motility, aphasia coming on late. | Cure with use of iodide and mercurial inunctions. |
| 18 | Ibid. | Melancholy, great excitability, ideas of grandeur; after a long time sudden ptosis and strabismus. | Iodide of potassium failed; mercurial course improved; joint use cured patient. |
| 19 | Ibid. | Various cerebral nerve palsies, great relief by use of mercurial inunctions, then development of great excitement, delirium of grandeur, failure of memory and mental powers, and finally death from apoplexy; no autopsy. | |
| 20 | J. B. Chapin Amer. Journ. Insanity, vol. xv. p. 249. |
Melancholia with attempted suicide, epilepsy, headache, somnolent spells. | Iodide of potassium, cure. |
| 21 | Ibid. | Acute mania, noisy, very destructive; syphilitic disease of tibia. | Iodide of potassium, cure. |
| 22 | Snel | Maniacal excitement. | Cured by specific treatment. |
| 23 | Wm. Smith Brit. Med. Journ., July, 1868, p. 30. |
Apathetic melancholy, indelicate, speaking only in monosyllables, and much of the time not at all, sullen and menacing. | Rapidly cured by conjoint use of iodide and mercurials. The symptoms first developed 3 months after chancre. |
A study of the brief analyses of the symptoms just given shows that syphilitic disease of the brain may cause any form of mania, but that the symptoms, however various they may be at first, end almost always in dementia unless relieved.
Of all the forms of insanity, general paralysis is most closely and frequently simulated by specific brain disease. The exact relation of the diathesis to true, incurable, general paralysis it is very difficult to [p. 1021] determine. It seems well established that amongst persons suffering from this disorder the proportion of syphilitics is not only much larger than normal, but also much larger than in other forms of insanity. Thus, E. Mendel64 found that in 146 cases of general paralysis, 109, or 75 per cent., had a distinct history of syphilis, whilst in 101 cases of various other forms of primary insanity only 18 per cent. had specific antecedents. H. Obersteiner has 1000 cases of mental disease,65 175 cases of dementia paralytica; of these, 21.6 per cent. had syphilis; moreover, of all the syphilitic patients 51.4 per cent. had dementia paralytica.
64 Progres. Paral. der Irren, Berlin, 1880.
65 Monatshefte f. prakt. Dermat., Dec., 1882.
Various opinions might be cited as to the nature of this relation between the two disorders, but for want of space the curious reader is referred to the work just quoted and to the thesis of C. Chauvet66 for an epitome of the most important recorded opinions.
66 Influence de la Syph. sur les Malad. du Syst. nerveux, Paris, 1880.
Those who suffer from syphilis are exposed in much greater proportion than are other persons to the ill effects of intemperance, sexual excesses, poverty, mental agony, and other well-established causes of general paralysis. It may be that in this is sufficient explanation of the frequency of general paralysis in syphilitics, but I incline to the belief that syphilis has some direct effect in producing the disease. However this may be, I think we must recognize as established the opinion of Voisin,67 that there is a syphilitic periencephalitis which presents symptoms closely resembling those of general paralysis. Such cases are examples of the pseudo-paralysie générale of Fournier.68
67 Paralysie générale des Alienés, 1879.
68 La Syphilis du Cerveau, Paris, 1879.
The question as to the diagnosis of these cases from the true incurable paresis is of course very important, and has been considered at great length by Voisin,69 Fournier,70 and Mickle.71
69 Loc. cit.
70 Loc. cit.
71 Brit. and For. Med.-Chir. Review, 1877.
The points which have been relied upon as diagnostic of syphilitic pseudo-general paralysis are—
The occurrence of headache, worse at night and present amongst the prodromes; an early persistent insomnia or somnolence; early epileptiform attacks; the exaltation being less marked, less persistent, and perhaps less associated with general maniacal restlessness and excitement; the articulation being paralytic rather than paretic; the absence of tremulousness, especially of the upper lip (Fournier); the effect of antispecific remedies.
When the conditions in any case correspond with the characters just paragraphed, or when any of the distinguishing characteristics of brain syphilis, as previously given, are present, the probability is that the disorder is specific and remediable. But the absence of these marks of specific disease is not proof that the patient is not suffering from syphilis. Headache may be absent in cerebral syphilis, as also may insomnia and somnolence. Epileptiform attacks are not always present in the pseudo-paralysis, and may be present in the genuine affection; a review of the cases previously tabulated shows that in several of them the megalomania was most pronounced; and a case with very pronounced delirium of grandeur, in which the autopsy revealed unquestionably specific brain lesions, may be found in Chauvet's Thesis, p. 31.
[p. 1022]I have myself seen symptoms of general paralysis occurring in persons with a specific history in which of these so-called diagnostic differences the therapeutic test was the only one that revealed the true nature of the disorder. In these cases a primary, immediate diagnosis was simply impossible.
Case 14 of the table is exceedingly interesting, because it seems to represent as successively occurring in one individual both pseudo and true general paralysis. The symptoms of general paralysis in a syphilitic subject disappeared under the use of mercury, to return some months afterward with increased violence and with a new obstinacy that resisted with complete success antisyphilitic treatment. Such a case is some evidence that syphilis has the power to produce true general paralysis.
In conclusion, I may state that it must be considered as at present proven that syphilis may produce a disorder whose symptoms and lesions do not differ from those of general paralysis; that true general paralysis is very frequent in the syphilitic; that the only constant difference between the two diseases is as to curability; that the curable sclerosis may change into or be followed by the incurable form of the disease. Whether under these circumstances it is philosophic to consider the so-called pseudo-general paralysis and general paralysis as essentially distinct affections, each physician can well judge for himself.
The subject of spinal syphilis is at present a difficult and unsatisfactory one. The recorded cases with well-observed autopsies are comparatively few, and when recovery occurs much uncertainty must rest upon the nature of the lesion. More than this, there is scarcely any chronic degeneration of the spinal cord which has not been attributed to syphilis, and my own experience as well as the records of medical literature lead to the very positive conclusion that all the various spinal scleroses are much more frequent in infected than in non-infected persons. Whether this is due to a direct or indirect influence of the disease is uncertain, but I shall not here discuss the relation of these chronic inflammations of the cord to syphilis.
It seems necessary to briefly consider at this place acute and subacute myelitis in their relations to syphilis. That these affections are not rare in syphilitics is certain. In the Revue de Médecine (Jan., 1884) Dejerine records the case of a person suffering from chronic syphilis in whom there were fulgurant pains with increasing weakness of the legs, and subsequently, after very severe exposure to the weather, a sudden development of complete paraplegia followed by trophic troubles, and death in twenty-eight days. At the autopsy there was found a central myelitis with pronounced lesion of the ganglionic cells, inflammatory changes of the pia mater, capillaries, and neuroglia, extreme alteration of the nerve-roots, and secondary degeneration of the columns of Goll and the lateral columns. In a second case recorded by Dejerine there appears to have been no exposure or apparent immediate exciting cause. The symptoms and lesions were similar to those just spoken of, but death occurred in eight days.
Whether such attacks as these occurring in syphilitic subjects are produced directly by the syphilis or not is at present doubtful. The same is [p. 1023] true of subacute myelitis, of which I have reported two rather peculiar fatal cases in syphilitic subjects. The general symptoms of this affection are progressive loss of power with grossly exaggerated reflexes, severe twitchings and jerkings of the legs, rigidity, usually more or less marked pain, and other sensory disturbances in the legs, and finally partial anæsthesia and complete paraplegia, paralysis of bladder, bed-sores, and death from exhaustion. At the autopsy the most important change in the cord has been the presence of great numbers of round neuroglia-cells in both gray and white matter. One of my cases died of a rapidly developed central myelitis supervening upon the subacute disease, and affording lesions similar to those described by Dejerine in addition to the changes of the subacute affection.
In another class of spinal cases occurring in syphilitics the symptoms resemble those of the so-called acute ascending paralysis (Landry's paralysis). The fourth variety of syphilitic diseases of the spinal cord of Huebner72 includes these cases. According to Huebner, they are without anatomical lesions, but in the majority of the recorded cases no proper microscopic study of the cord has been made. Huebner states, however, that Kussmaul failed in one case after such study to detect lesion. As some of these cases may really have been instances of peripheral neuritis, it is essential that in the future the peripheral nerves as well as the spinal cord be carefully studied. I have seen one case which might be placed in this category. The first symptom was some numbness in the legs, with a small deep sharp-cut ulcer on the plantar surface of the great toe; directly after this loss of motion and sensation in the legs and thighs, rapidly becoming almost complete and spreading quickly to the trunk and arms, so that in one week the patient was a flaccid, helpless mass, and the breathing so interfered with that he was believed to be dying. After almost losing the power of swallowing this patient began to get better, and finally so regained power of his hands and feet that he was able to partially dress himself and walk a distance of ten or twelve feet, when he was suddenly seized with a pleural effusion and died. During the first week of his disease his temperature was 100° F. At the autopsy the spinal membranes were found to be normal. But in the cord there were very distinct lesions found; the neuroglia seemed everywhere more granular than normal; the ganglionic cells were not distinctly diseased; the white matter in various places was much changed, the tissue appearing abnormally dense and opaque where most affected; the nerve-tubules appeared to gradually lose their myeline, and in places were reduced to simple axis-cylinders. Finally, the axis-cylinders became smaller and smaller until in the most altered portions of the cord they disappeared. As the autopsy was obtained with great difficulty, it was not possible to get the peripheral nerves for study.
72 Ziemssen's Encyclopædia, vol. xii.
In regard to these very acute cases, it seems to me uncertain whether the disease should be attributed to the syphilis. In my own case twenty years had elapsed since the chancre, alcohol was habitually used in great excess, and the attack was apparently precipitated by great exposure. On the other hand, the man bore well enormous doses of iodide of potassium, and lowly progressed under them.
Finally, there is a class of disease of the spinal cord in which the [p. 1024] lesion is undoubtedly the direct outcome of a syphilitic diathesis. In these cases the exudation commences primarily in the membranes of the cord, and may extend into the cord itself. In this class I would include the first two varieties of syphilitic spinal disease of Huebner. The number of recorded autopsies is not great; the only cases with which I am acquainted are those referred to in the note at the bottom of this page.73
73 Winge (Dublin Med. Press, 2d Series, vol. ix., 1863); Moxon (Dublin Quarterly Journ., li., 1870); Charcot and Gombault (Archiv. d. Physiologie, tome v., 143, 1873); Schultze (Archiv. Psychiat., xii. 567); Thos. Buzzard (Diseases of Nervous System, 1882, p. 407); Julliard (Étude Crit. sur les Localis. Spinal de la Syphilis, 1879); Westphal (Arch. Psychi., vol. xi.); Greif (Arch. Psychiat., xii. 579); Homolle (Progrès méd., 1876).
The lesions in these cases are entirely similar to those of brain syphilis. The disease very rarely or never begins in the interior of the cord. I know of no recorded case: Wagner's case, in which a yellow nodule was found within the cervical marrow, was probably not one of syphilis. If a gummatous inflammation does occur inside of the cord, it probably starts from the ependyma. The gummatous exudate may occur in the form of small multiple formations or of an extensive meningitis, with an infiltration of the membranes and their spaces with gummatous material. The membranes are usually agglutinated with one another and with the surface and with the cord. The exudation is usually made up of roundish cells, and in several cases spindle-shaped cells have been noticed, as have also the peculiar Deitres corpuscles already described as they occur in brain syphilis. The changes in the cord itself vary somewhat. In Winge's case the white matter seems to have undergone a rapid myelitis from pressure. It was of a grayish color, with numerous fine granular masses, corpora amylacea, pigment-masses, and fatty globules, the nerve-fibres being broken up. In other cases the change has been a sclerosis. The vessels of the cord have been noticed by various observers in the different stages of the degeneration seen in syphilis of the brain. They are often greatly dilated, their walls thickened, and, together with the lymph-spaces, infiltrated with small cells. Minute hemorrhages have been found.
The so-called syphilitic callus, as described by Heubner, is probably the remnant of a true gummatous inflammation. It consists of a circumscribed induration one to several lines in thickness, originating apparently from the dura mater, and causing sometimes adherence with the vertebræ, in others with the membranes of the spinal cord. In a case described by Virchow of this character the lesion was cervical, and the symptoms were stiffness in the nape of the neck, pains in the neck and arms, and finally paralysis in both arms. A second case is elaborately described by Heubner in his article in Ziemssen's Encyclopædia.
SYMPTOMS.—As the lesion of gummatous spinal syphilis affects primarily membranes of the cord, in the beginning of the attack the symptoms chiefly arise from the implication of the nerve-roots. Of course these symptoms vary with the seat of the lesion, for it must be remembered that the meningeal irritation is at first usually localized in a small region. As in a majority of cases this lesion affects a posterior portion of the cord, and as the posterior nerve-roots seem especially sensitive to irritations of this character, pain is usually a very marked and [p. 1025] precocious symptom of spinal syphilis. The seat of the pain varies with the seat of the lesion. At first the pain is slight, but in most cases it soon becomes severe. It is sometimes situated at a fixed spot on the spinal column, where, according to Heubner, it may be increased on pressure. I have seen two or three such cases, but have and still do believe that under these circumstances the patient was suffering not simply from a spinal syphilis, but also from an implication of the vertebral periosteum or of the vertebræ themselves. In one of my cases this diagnosis was confirmed at the autopsy. When the lesion is purely meningeal there is probably no marked local tenderness. The severe pains usually felt in the extremities or in the trunk are often fulgurant; sometimes they are described as resembling the thrust of a knife, and not rarely they closely resemble the pains of locomotor ataxia. In some instances the pains are comparatively slight and are aching in character. Paræsthesiæ are not rare phenomena: such are formications, tingling in the extremities, numbness and feeling as though the limb were asleep, intense sense of coldness on the surface, sensation of water running over the limb. Early in the disorder there is sometimes very marked hyperæsthesia, but later, even though the pain persists, blunting of sensibility is marked, and there may be a complete anæsthesia. This anæsthesia is sometimes localized in certain parts of the limb. Thus, in a case reported by Alfred Mathieu,74 although there was complete anæsthesia of the outer side of the left leg and foot, the inner side retained its normal sensibility. In some cases there is the abdominal cincture of ordinary myelitis. The records show that even in these early stages there may be diplopia, amblyopia, or other disorder of vision, and the pupil may be distinctly affected. In these cases it is probably the upper portion of the cord which is affected.
74 Ann. de Dermatol. et Syph., vol. iii., 1882.
Disturbances of motility in the majority of cases do not develop until some time after sensation has been affected, but may come on very early. Usually, the first symptoms are those of irritation, such as rigidity of the neck, back, and limbs or even of isolated groups of muscles. Tremors have been described as frequently present. These may be convulsive, and are often plainly reflex in their origin; indeed, I am inclined to believe that they are always reflex tremblings, and never true tremors. Heubner describes a case in which a paralyzed limb was thrown into violent tremblings whenever passive motion was attempted. The patella-reflex is usually grossly exaggerated, although it may be lost in the later stages of the disorder. Not rarely there is the condition which has received the misnomer of spinal epilepsy. This exaggeration of the reflexes may be limited to one leg, when it is almost pathognomonic. In some cases severe cramps are excited by movement. Usually there is no tenderness. These symptoms of the meningitic stage may continue for weeks or months without there being pronounced paralysis, although locomotion is not rarely interfered with by the stiffness of the legs. Finally, if the case progresses the patient notices a weakness in one or both legs, or (if the disease be situated high up in the spinal cord) in one arm, which rapidly increases until there is almost complete loss of power. This rapid increase of palsy following long-continued disturbance of sensation is almost pathognomonic. In most cases one side of the body is more [p. 1026] affected than the other. The sphincters are prone to be implicated, and in advanced stages of the disease there is usually complete loss of control over the bladder and rectum. The patient may live for months without very distinct change of this condition, or bed-sores and other trophic disturbances may rapidly develop and death ensue in a short time. I have seen under these circumstances marked elevation of temperature, rapid feeble pulse, mental weakness, and the general symptoms of septicæmia last for many weeks. Ammoniacal cystitis is of course prone to be developed during this stage. When motility fails, sensibility is usually blunted, although the pains may even increase. Heubner affirms that an incompleteness of the anæsthesia is characteristic of the disorder.
The typical course of spinal syphilis, such as has been described, may be variously departed from. Sometimes the power of co-ordination is early affected, and the symptoms may resemble those of locomotor ataxia. I doubt, however, whether under any circumstances there is a loss of the patella-reflex in the early stages of the gummatous disease of the spinal cord. In other cases the paralytic symptoms may be very prominent from the beginning: thus, in the case of R. P——, aged 27, which I believed to be gummatous disease of the spinal cord, the first disorder was a feeling of malaise lasting for about a week, followed by the sudden, rapidly-developed paralysis of the bladder, loss of power in the legs, and to a less extent in the arms, the only pain being a dull, steady ache in the arms. The bowels were obstinately costive. Double vision was soon very pronounced. When I first saw the patient, about three weeks after this, there was decided impairment of sensibility in the legs, but not in the arms; marked muscular weakness of both legs and arms; no loss of co-ordinating power; dropping of the right eyelid, with double vision; and only some slight aching pains in the arms. By the use of large doses of iodide of potassium and other appropriate measures a good recovery was secured.
A case illustrating the occasional difficulty of diagnosing spinal syphilis is reported by C. Eisenlohr.75 The first symptom was obstinate constipation, with very great discomfort after defecation; then appeared incontinence of urine with weakness of the legs: finally, a sudden complete palsy of the right leg occurred, with marked anæsthesia in both legs, partial loss of power in left leg, violent boring abdominal pains, and distress in the bladder. In the last stages there were severe neuralgic pains in both legs, with complete loss of sensation, bed-sores, atrophy of the leg-muscles, with reactions of degeneration, and death from exhaustion. At the autopsy an advanced meningitis was found which had apparently commenced in the regions of the cauda equina, and given rise to complete degeneration of the nerves. The only alteration of the cord was an ascending degeneration of the posterior columns.
75 Neurolog. Centralb., 1884, p. 73.
Again, owing to the diseased condition of the vessels, a spinal syphilis may be suddenly interrupted by an apoplectic accident.
In a patient of my own, who was believed to be suffering from gummatous spinal meningitis, there was an abrupt development of violent tearing pains, loss of power and sensibility, and all the other symptoms which are characteristic of meningeal spinal hemorrhage. A. Weber [p. 1027] reports a case in which, after doubtful premonitory symptoms, such as vertigo, loss of power on the right side, pressure on the top of the head, and tinnitus aurium, there was a sudden development of convulsions, and death. At the autopsy a syphilome of the right vertebral artery was found with a recent thrombosis of the basilar artery.76
76 American Journ. of Neur. and Psychiat., vol. ii.
DEFINITION.—Under the head of Tumors of the Brain and its Envelopes will be considered all forms of growths occurring within the skull, whether these involve the cranium itself, the membranes of the brain, the brain-substance, or several of these parts conjointly. A large majority of these growths spring from the brain-membranes.1
1 To this article will be appended a table of one hundred cases of brain tumor. Our researches included the investigation of many more cases, four to five hundred in all. Such a table, indeed, could be indefinitely extended. Our object, however, has been not so much to present a large number of cases, and these in great detail, but rather in the most condensed manner to give a definite number, carefully selected, from which to draw conclusions. The cases have not been chosen with the view of upholding any peculiar or preconceived views as to pathology, diagnosis, localization, etc., but because of the carefulness with which they have been recorded. They have been selected also, as will be seen, with the view of determining by clinico-pathological data the possibility of localizing such growths during life. Many of our general conclusions as to pathology, symptomatology, and diagnosis have been drawn from this table.
With the exception of such merely substitutional terms as cerebral or intracranial growths, neoplasms, or adventitious products, we have no general synonyms for brain tumors.
The literature of the subject of brain tumors is second only to that of such subjects as syphilis and hysteria. Vol. ii. of the Index Catalogue of the Library of the Surgeon-General's Office, U. S. A., contains no less than 632 references to this subject: number of books, 43; articles, 589. The books and papers occur in different languages, as follows: British, 142; French, 174; German, 133; American, 91; Italian, 30; Latin, 15; Swedish, 14; miscellaneous, 33.
ETIOLOGY.—Under predisposing or constitutional causes are first to be classed such special inheritances as tuberculosis or carcinoma and tendencies to vascular degeneration. The occurrence of syphilis of course predisposes its victims to cerebral or membranous growths, as it does to other so-called tertiary forms of this disorder.
Hereditary predisposition only enters in so far as the individual inherits a general tendency to the development of such affections as cancer and tubercle. Hereditary tendency to a brain tumor per se does not exist, but the individual who is of the tuberculous or cancerous diathesis under special causes may develop an intracranial growth. As to the comparative frequency with which diathetic tumors originate, a reference to the tabular statement which will be given under [p. 1029] Pathology will be sufficient. Gliomata are very common, but with them vie in frequency sarcomatous, tubercular, and gummatous growths. Any table, unless it includes a very large number of cases—at least a thousand or more—would be misleading as to the proportionate frequency of these different forms of intracranial constitutional diseases; but it is safe to say that syphilitic, tuberculous, and carcinomatous or sarcomatous tumors are of comparatively frequent occurrence.
Tumors of the brain occur oftener among men than women. This fact is dependent largely upon the difference between the habits and occupations of the two sexes. Men, in the first place, are much more addicted to alcoholic, venereal, and other abuses which give rise to special degenerations or constitutional infection; and secondly, they are more exposed to traumatisms. In 100 cases the tumors occurred among males in 58 cases, among females in 40 cases, and sex was not recorded in 2 cases.
Statistics show that intracranial growths are more likely to occur between puberty and middle age. Although gliomata may be found at any age, brain tumors in children are more likely to be of this character. This is what might be expected from the nature of these growths. Histologically, gliomata are most closely allied to the embryonal stage of the connective tissue, and, according to Cohnheim, tumors generally are the result of a surplusage of embryonal tissue—tissue which has remained over after the requirements of normal development have been met. Of 16 gliomata, 3 occurred in patients under ten years, 2 between the ages of ten and twenty, and 4 between twenty and thirty.
One hundred cases gave the following results as to age:
| Under 10 years | 10 | cases. |
| From 10 to 20 years | 12 | cases. |
| From 20 to 30 years | 18 | cases. |
| From 30 to 40 years | 24 | cases. |
| From 40 to 50 years | 12 | cases. |
| From 50 to 60 years | 13 | cases. |
| From 60 to 70 years | 3 | cases. |
| Over 70 years | 1 | cases. |
| Not recorded | 7 | cases. |
| 100 | cases. |
It is now generally admitted that injuries play a most important part as exciting causes of brain tumors. Frequently in our experience an apparently direct relation has existed between a head injury and the origin of the neoplasm. In 6 out of 12 cases reported by one of us,2 a history of traumatism was present, although in 5 of these a history of syphilis was also present. The great frequency with which injuries of all kinds occur must of course not be overlooked in this connection. It is said by those who oppose the idea of the direct causal relations of injury that almost every one could trace such disease to falls or blows which few escape. In some of the cases of brain tumor, however, the history of injury bears a direct relation in time to the initial symptoms of the tumor. Certain tumors, as the fibromata, osteomata, angiomata, would appear to be of more frequent occurrence as the direct result of traumatism. The part played by injuries in the production of carcinomata and sarcomata, whether in the brain or elsewhere, has not [p. 1030] infrequently been the subject of dispute. We have no doubt that, a constitutional predisposition existing, an injury frequently leads directly to the development of some form of malignant growth. In not a few of the syphilitic cases the history would appear to show that an injury to the skull had localized the constitutional poison.
2 Archives of Medicine, vol. viii. No. 1, August, 1882.
Echinococci and cysticerci are found within the cranium, and sometimes give rise to tumors, but the statement of Obernier can hardly be regarded as true, that they play an important part in the production of cerebral tumors. Our table shows only two cases of this kind.
SYMPTOMATOLOGY.—The symptoms of intracranial tumors from the standpoint of the course or progress of the affection can be divided into an early or beginning, a middle or developed, and a late or terminal stage.
Headache, vertigo, and vomiting are early symptoms, varying in severity from slight to very serious manifestations, and slight and changing mental phenomena are present. Eye symptoms, such as slight diminution or blurring of vision, may or may not show themselves; the ophthalmoscope may reveal the earliest appearances of choked disc or neuro-retinitis.
In the second or middle stage, the period of the fully-developed disease, we have an intensification and greatly increased constancy of all the general symptoms, with some additional manifestations. Mental disorder increases; headache becomes more violent, and sometimes more localized; amblyopia tends to advance to complete blindness, with marked swelling of the papilla, or special disorders of vision, such as hemianopsia, occur; palsies, ataxia, convulsions, contractures, rigidity of limbs, altered reflexes, local spasms, anæsthesia, hyperæsthesia, paræsthesiæ, neuralgias, appear according to the extent and location of the growth. Certain special phenomena, according largely to the seat of the tumor, may also appear, such as disorders of hearing, taste, or smell, polyuria, diabetes, albuminuria, polyphagia, or dysphagia.
In the third or terminal stage paralysis, anæsthesia, convulsions, etc. become more profound; mentality sometimes decreases to nearly complete imbecility, although in many cases a fair amount of mental power is preserved almost to dissolution. Involvement of the bowels and bladder becomes a distressing symptom, involuntary evacuations adding to the torments of the patient. Bed-sores, acquired or trophic, appear; the patient's limbs are painfully contractured; great emaciation is usually present. With agonized head, often blind or deaf, with torturing pains in anæsthetic, paralyzed, and wasted limbs, covered with painful sores, filthy involuntarily, imbecile or demented, death comes as a thrice-happy relief.
Cases have been reported in which intracranial tumors of considerable size were discovered on autopsy, and had evidently been present for years without their presence having been discovered or even suspected; but these are extremely rare. In general terms, however, it may be said that every case of brain tumor must give rise to symptoms. These symptoms may be few or many, slight or severe, brief or protracted, constant or paroxysmal, according to circumstances. Our experience and study of the literature of the subject lead us to the conclusion that the pathological character of the growth would have some influence as to the severity and prominence of symptoms. Gliomata—which are [p. 1031] sometimes hard to distinguish from the brain-substance, particularly the soft gliomata, producing comparatively little pressure—when located in certain so-called latent areas of the brain might escape detection during life; so might also very small tumors of any kind situated deeply in the substance of the brain.
The position taken by Obernier, that individuality has much to do with the activity of symptoms of brain tumor, has some strength. He refers particularly to the psychical response to the irritation caused by brain tumors, which differs very much in different individuals. The fact, which has been pointed out in the article on Hysteria, that hysterical symptoms are often present in cases of brain tumor as well as in other forms of organic disease, is also sometimes the cause of mistake by the diagnostician. The cases of Hughes Bennett and Eskridge will be referred to in this connection under Diagnosis.
When the subject of local diagnosis is considered farther on, those regions which are most active and those which hold an intermediate position in the production of particular and distinctive symptoms will be more particularly discussed.
The possibility of the existence of multiple tumors should never be overlooked. These are of comparatively frequent occurrence, and sometimes give rise to a puzzling symptomatology. In our search through the literature of the subject for cases we met with many examples of multiple tumors. In preparing our table multiple tumors were usually omitted. They give sometimes symptoms and signs so conflicting as to make a local diagnosis impossible, and even to confuse the expert as to general diagnosis. In other cases, however, one growth of larger size or in an active region takes command of the situation, and leads clearly to its diagnosis in spite of other less significant tumors. This was shown, for example, in one of our cases (Case 14). From the symptoms not only was the presence of the larger tumor diagnosticated, but its exact location was indicated during life. Post-mortem examination, however, showed a smaller tumor at the inferior angle of the right lobe of the cerebellum, and also some basal meningitis with effusion which had not been suspected. The first tumor was one of the ascending frontal convolution, extending into the fissure of Rolando. Its presence and location had been diagnosticated by the right brachial monoplegia and paresis of the leg, which later increased to paralysis of the limb, with right facial paresis, ptosis, partial anæsthesia of right side of face, and slight clonic spasms of the right arm. At the present time, when the question of operating for the removal of brain tumors is so prominently before the profession, and is now generally regarded as justifiable for growths in this one location, the cortical motor area, the possibility of the coexistence of another tumor should be carefully weighed. In this case, owing to the clear diagnostic indications, the question of operation was considered at the time of consultation, but fortunately—in large part because the patient was almost in extremis—it was decided not to operate. The operation would have been futile, the autopsy showing that the probable immediate cause of death was the basilar effusion which accompanied the cerebellar growth.
In another case reported by one of us3 three gummata were found in [p. 1032] three different locations: one in the prefrontal region, another in the retro-central fissure, and a third in the supramarginal convolution. The general symptoms of brain tumor were present in this case, but no localization was possible.
3 Arch. Med., viii. No. 1, August, 1882.
The following are other illustrations of multiple tumors and of tumors with other lesions out of a large number which we have collected:
M. 44.—Several severe falls on the head. Recent chancre with secondary symptoms. Six months before death headache which grew worse; most severe in right supraorbital region, and also obstinate vomiting, vertigo, hiccough, insomnia. Some loss of power on both sides. Slow in answering and indisposed to talk. Choked discs. Involuntary evacuations. Some improvement under treatment, and then relapse. Complete blindness. Polyuria. Specific gravity of urine as low as 1003 and 1005. Appetite at times ravenous. During last few weeks of illness head inclined to the right side, probably from spasm. Intense thirst throughout the illness.
(1) Large sarcoma in the white substance of the right parietal and frontal lobes, involving ascending parietal convolutions. (2) Softening and abscess of the right temporo-sphenoidal lobe and posterior base of the right anterior lobe. Softened mass size of a hickory-nut in the upper portion of the right ascending frontal convolution. (3) Small cystic tumors of the choroid plexuses.4
4 J. T. Eskridge, Trans. of Philada. Path. Society, for 1878-79, vol. ix. p. 119.
M. 5.—Convulsions, beginning either in right foot or in right face; not unconscious during fits. Right-sided hemiplegia. Double optic neuritis, followed by atrophy. Gradual increase in size of head, with gaping sutures. Later, rigidity of right arm and leg. Shortly before death the following symptoms suddenly set in: headache, convulsions of right side with unconsciousness and retraction of head, rigidity of right arm, and tremor of right leg. Later, both arms flexed, with constant tremors of left arm, spreading over whole body. Right sterno-cleido-mastoid was stiff; almost opisthotonos.
(1) Enormous tubercular tumor of left cerebral hemisphere, extending from depth of Sylvian fissure and eroding skull. Corpus striatum soft and diffluent. Weight, over eleven ounces. (2) Tumor, double size of pea, in lower part of middle lobe of cerebellum.5 This case was especially interesting for the onset of the cerebellar symptoms late in the case, caused probably by a late appearance of the cerebellar tumor.
5 Hughlings-Jackson, Med. Times and Gaz., London, 1872-73 (2), p. 34.
M. 2.—Screaming fits. Vomiting. Paralysis of left side of face, including corrugator and orbicularis palpebrarum. Winking in both eyes suspended. Paralysis of external rectus muscle. Agitation and contractures of right arm and leg. Later, unsteady movement of head and right arm and jerking of right leg.
(1) Small glioma in left hemisphere of cerebellum, and (2) a similar tumor projecting from left lateral half of floor of fourth ventricle at common nucleus of the abducens and facial nerves.6
6 W. H. Broadbent, Proc. Clin. Soc. Lond., v. 66-68.
F. 45.—Epileptiform attacks for fourteen years. Vertigo, occipital headache, disordered vision, intolerance of light, sleeplessness, excitability, constipation, with paræsthesia of left side. Retraction of head, [p. 1033] vomiting. Very late, convulsive movements of right eye and right side of mouth; then general clonic spasms, coma, and death. No paralysis. For twenty-six years there had been an induration of one breast, which toward end of life had a somewhat scirrhous appearance.
(1) Glioma in right hemisphere of cerebellum 1¾ inches in diameter. (2) Glioma in centre of middle lobe of left hemisphere of the cerebrum ¾ inch in diameter. Surrounding nervous tissue softened and broken down.7
7 William L. Bradley, Tr. Conn. Med. Soc., 1880, p. 39.
M. 65.—Sudden attack of spasm of left arm, with paresis and coldness and numbness. Headache and staggering. Wandering in mind. Not unconscious. Twitching in eye. Two days later violent convulsion in entire left half of body, with vomiting; not unconscious. After convulsion left hemiplegia, with left deviation of tongue. Head and eyes turned to right; vertigo. Partial anæsthesia of left face, body, and limbs. Paræsthesia; painful nervous shocks through affected limbs. Sounds in back of head. Later, mind cleared up and many symptoms ameliorated. Very late, convulsion and coma. Cheyne-Stokes respiration, involuntary evacuations. Duration, seven weeks.
(1) Tumor in ascending parietal convolution at junction of upper and middle thirds. (2) Large tumor occupied entire occipital lobe, but did not present on surface, reaching to convexity of descending cornu of lateral ventricle.8
8 W. H. Broadbent, Tr. Clin. Soc. Lond., v. 233-236.
Headache is the most frequent and positive symptom of brain tumor. It is rarely absent; in most cases it has peculiar characteristics. Its usual type might be described as continuous pain, sometimes of persistent severity, but generally with exacerbations or paroxysms of great violence. No suffering can surpass that which some of the victims of intracranial neoplasms are compelled for months or years to endure. It is only equalled by the torture produced by malignant growths in the vertebral axis, the throat, or the bones of the pelvis. The pain is not, however, always of this character. In a comparatively few cases it is described by the patient as dull or moderate, or he simply complains of distressing sensations of weight, pressure, or constriction. Usually in these cases, however, the pain increases and becomes less and less endurable. In 100 cases the headache is described as agonizing, violent, severe, or torturing 20 times; as moderate or dull, 26 times. It is simply mentioned 20 times, but here presumably it was of the ordinary severe type. Thus in 66 cases, or 66 per cent., headache of some type was recorded. No mention was made of headache at all in 29 cases, in some of which, however, it was doubtless present. In only 5 cases was it stated not to have been present: 3 out of these 5 were said to be gliomata, and of the other 2, one was probably gliomatous, and the other a cyst in the brain-substance. Tumors of this kind, which exert comparatively little pressure and which are not connected with the membranes, are probably those which are least likely to cause pain. In several instances the patients complained spontaneously of the pain being greatest in the region of the head nearest the seat of growth. With reference to cerebellar tumors, it somewhat generally supposed that occipital pain is usually present. It [p. 1034] sometimes is and sometimes is not. In 15 cases of tumor of the cerebellum and of the fourth ventricle the pain was described as occipital twice, as fronto-occipital three times, and as cervico-occipital once. Callender has noticed that cortical lesions are more frequently accompanied by localized pains than lesions of deeper parts.9 Some of our cases would seem to bear out this view, although the data are not numerous or complete.
9 St. Bartholomew's Hospital Reports, 1869, and Ferrier's Localization of Cerebral Disease, p. 99.
In a few cases percussion of the head elicited or intensified pain in the region corresponding to the location of the tumors. We believe that percussion of the skull may afford valuable aid in localizing encephalic tumors, particularly when they are meningeal or cortical. Ferrier10 holds that percussion often elicits pain over the cranial region beneath which a lesion is localized, and Alex. Robertson of Glasgow11 has also directed attention to the value of percussion of the skull in the localization of disease on the surface of the brain.
10 Brain, January, 1879.
11 Abstr. Internat. Med. Congress, 1881, p. 85, and Journal of Nervous and Mental Disease, April, 1882.
Vomiting is of frequent occurrence, although it does not usually come on as early or remain as persistently as headache. It is more likely to be paroxysmal, with longer or shorter intervals of relief. It frequently occurs at the time of the exacerbations of the headache, and between the paroxysms of vomiting, nausea, slight or great, is often present. It probably occurs in about 50 per cent. of all cases of brain tumor. It is recorded as having been present in 34 out of 100 cases. It was comparatively infrequent in antero-frontal growths, occurring only twice out of 10 cases.
A case reported by one of us (Case 70) was a remarkable example of persistent cerebral vomiting. For four weeks before her death the patient vomited almost incessantly. The tumor in this case involved the middle cerebellar peduncle and the adjacent region of the right cerebellar hemisphere, and had grazed and superficially softened the floor of the fourth ventricle.
We incline to agree with Ferrier12 that the majority of cases of cerebral vomiting can be ascribed to irradiation of irritation by the nerves of the cerebral membranes or to the physical effects of acute pain. The nuclei of the trigeminus and of the vagus are in close anatomical relationship in the medulla oblongata. Irritative impressions conveyed from the cerebral membranes, and particularly from the dura mater, to the trigeminal nuclei in the medulla are transferred to the vagus and give rise to vomiting. In tumors of the cerebellum the vomiting may be brought about through the affection of the centres of equilibration and the concurrent vertiginous sensations (Ferrier), or it may be due to direct irritation by contiguity of the floor of the fourth ventricle. In general, the tumors situated farthest forward in the brain appeared to be the least likely to give rise to vomiting.
12 Brain, July, 1879.
Vertigo was noted in 31 out of 100 cases. Under this general designation dizziness, giddiness, reeling, insecurity in the erect posture, etc. have been included. The vertigo can be explained in several ways [p. 1035] besides by the view which refers it to an affection of centres of equilibration in the cerebellum. Like headache and vomiting, it seems sometimes to be the outcome of pure irritation of the cerebral membranes. Alterations in the intracranial circulation produced by the growth of the tumor is another probable cause. Experiments have demonstrated the existence of a communication between the arachnoid cavity and the labyrinth, and consequently the increased intracranial tension present may result in pressure on the labyrinthine fibres of the auditory nerve, and thus occasion vertigo.
The importance of ophthalmoscopic examinations in suspected cases of brain tumor can scarcely be overestimated. They will often serve to clinch the diagnosis in favor of tumor. Of the 100 tabulated cases, choked discs were recorded in 8; optic neuritis or neuro-retinitis in 18. These results serve to show the importance of the examination of the eyes. It will be seen that with Allbutt, Norris, and others we make a distinction between choked disc, papillitis, congestion papilla, or ischæmia of the discs, and descending or interstitial neuritis. The differences between these two varieties of inflammation of the interocular ends of the optic nerve are well presented by Norris in a previous volume of this work,13 which will make it unnecessary for us to describe the conditions present in these cases. An examination of the tabulated cases will show that true choked discs were present in tumors situated in all portions of the encephalon. They were not infrequently present in tumors of the convexity. Descending neuritis would seem most likely to occur when the tumors are so situated that inflammation set up by them can readily extend by anatomical continuity along the membranes to the optic nerves. The lymph-space theory best accounts for the occurrence of choked discs in cases of tumor situated remotely from the base. In choked disc the appearance is one of intense swelling and engorgement of the optic papilla. In descending neuritis, as described by Graefe and Norris, there is rather a dull-red suffusion of the disc. Some of the cases reported as neuritis may have been choked discs, and the reverse, as physicians often do not make any distinction.
13 Vol. IV. p. 771 et seq.
Several practical matters should be borne in mind in connection with this subject of the condition of the eye-ground. In the first place, sight is not always impaired in cases of even somewhat advanced choking of the disc, so that when other symptoms and indications lead to the suspicion of a brain tumor, unexpected confirmation may be obtained by ophthalmoscopic examination. Some remarkable cases of this kind have been reported, and doubtless have been observed by all ophthalmologists and neurologists of large practice. In some cases of growths of large dimensions also careful ophthalmoscopic examination has shown neither choked disc nor neuro-retinitis to be present. In two of Seguin's cases, for instance (Cases 28 and 29), these appearances were absent. In one he reports no neuro-retinitis, but only some fulness of the veins. In the other, a large sarcoma of the centrum ovale, ophthalmoscopic changes were absent. The absence of disturbance of vision, therefore, should not lead the physician to overlook making a thorough ophthalmoscopic examination; nor should the absence of ophthalmoscopic appearances lead him to make up his mind that serious intracranial disease was not present. [p. 1036] The presence of double choked discs is in the highest degree significant of a brain tumor.
Observations on the temperature of the head have been made in a few cases of tumor of the brain. Full accounts of such observations in two cases (1 and 3 of Table) have been published by one of us.14 It is not within the scope of the present paper to review the general subject of cranial or cerebral thermometry. We will simply, in passing, recall the labors of E. Seguin,15 Broca,16 Gray,17 Lombard,18 Maragliano and Seppilli,19 and Amidon.20
14 Philadelphia Medical Times, Jan. 18, 1879, and New York Medical Record, Aug. 9, 1879.
15 Medical Thermometry and Human Temperature, by E. Seguin, M.D., New York, 1876.
16 Progrès médical, 1877.
17 New York Medical Journal, Aug., 1878.
18 Experimental Researches on the Temperature of the Head, London, 1881.
19 Quoted in Archives of Medicine, 1879.
20 Archives of Medicine, April, 1880.
L. C. Gray21 has recorded some observations in cerebral thermometry in one case of tumor of the brain. The tumor, a soft jelly-like mass the size of a hazelnut, was found between the horizontal branch of the Sylvian fissure and the first temporal fissure, while the whole of the right occipital lobe was converted into a colloid, extremely vascular mass, which gave way under examination, this degeneration also extending anteriorly to the tumor as far as the fissure of Sylvius. Microscopical examination showed it to be a typical glioma.
21 N. Y. Medical Journal, August, 1878.
The temperatures at different stations were as follows:
| Left. | Right. | |
| Frontal | 96.75° | 98.33° |
| Parietal | 95° | 99.75° |
| Occipital | 96.75° | 100.50° |
The average of the left side was 96.16°; of the right, 99.52°; of the whole head, 97.84°.
In a case of frontal tumor (Case 1 of Table) the average temperatures of the different stations taken were as follows:
| Middle frontal station | 96.5° |
| Middle occipital station | 95.5° |
| Right frontal station | 95° |
| Left frontal station | 94.7° |
| Right parietal station | 94.7° |
| Left parietal station | 94.4° |
In another case, reported in full by one of us22 (Case 94), a gumma involved the basal termination of the corpus callosum, the peduncles of the corpus callosum, the lamina cinerea, and anterior perforated spaces; and the average temperatures at the different stations were as follows:
| Right frontal station | 97.1° |
| Left frontal station | 97.4° |
| Right parietal station | 97.6° |
| Left parietal station | 94° |
| Right occipital station | 97° |
| Left occipital station | 94.5° |
| Right anterior vertical station | 97° |
| Left anterior vertical station | 94° |
| Right posterior vertical station | 96.6° |
| Left posterior vertical station | 94.3° |
22 New York Medical Record, Aug. 9, 1879.[p. 1037]
In a gumma in the cortical motor zone of the right side the head-temperatures, taken once, were found to be for the right parietal region, 97.2°; for the left, 96°. In another tumor of the right motor zone the right frontal region gave a temperature of 98°; the left, of 96°. In a tumor of the left occipito-parietal region the temperatures were for the right parietal region, 98°; for the left, 97.8°. Although the temperature of the head was only taken once in each of these three cases, the observations were carefully made with tested thermometers.
J. T. Eskridge, in a case of a tumor of the cerebellum with monocular hemianopia (Case 76), made the following temperature observations:
| Axillary | R. 98.6°; | L. 98.6° |
| Head: | ||
| Anterior frontal station | R. 98.4°; | L. 98.4° |
| Posterior frontal station | R. 98.5°; | L. 98.6° |
| Superior frontal station | R. 98.4°; | L. 98.4° |
| Parietal frontal station | R. 99.2°; | L. 98.6° |
| Rolandic frontal station | R. 98.8°; | L. 99.1° |
| Occipital frontal station | R. 99.4°; | L. 99.1° |
| Posterior central station | 99°. | |
| Anterior central station | 99°. | |
The normal average temperatures, as determined by Gray, were as follows:
| Left frontal station | 94.36° |
| Right frontal station | 93.71° |
| Left parietal station | 94.44° |
| Right parietal station | 93.59° |
| Left occipital station | 92.66° |
| Right occipital station | 91.94° |
| Left side of the head | 93.83° |
| Right side of the head | 92.92° |
| The whole head, exclusive of the vertex | 93.51° |
| Motor region of the vertex | 91.67° |
| The whole head, inclusive of the vertex | 92.66° |
We conclude that in brain tumors the average temperature of the whole head is elevated several degrees above the normal, and that the elevation of temperature is usually greatest at the station nearest the seat of the growth.
Mental disturbance of some description was present in about one-third of all the cases studied. Doubtless they were not recorded in a large number of cases. Obernier says: “If the psychical qualities of a patient suffering from cerebral tumor be analyzed, and a careful comparison made of the former with the existing mental condition, certain symptoms of mental disturbance will be discovered in most cases where the tumor is a growing one.” The disturbances may be in any sphere of the mind—in intellection, volition, emotion, or perception. Mental slowness and uncertainty, inability to fix the attention, impossibility of continuous mental action, apathy, or stupidity, with hesitation or slowness of speech, were strikingly exhibited in cases of tumor of the antero-frontal region. In Case 1 the patient's mental condition was studied with great care, and in the detailed report of the case23 the following facts were noted: The psychical manifestations were among the most important features of the case. Although comparatively uneducated, he had been when [p. 1038] in health intelligent and energetic. He had never during his illness had the gay humor or delirium of grandeur seen in the general paralysis of the insane. His condition, on the whole, was one of intellectual slowness and uncertainty. He seemed to have great difficulty in receiving mental impressions and in directing the movements of his body. His faculty of attention was, in great measure, destroyed. It could only be fixed, and then but partially, by distinctly and vehemently repeating a question or command. He could hear, but it was necessary to make a tremendous external impression on his sense of hearing in order to call out a mental response. He sometimes appeared to me like a man dazed by a great catastrophe which he could not understand. He was not aphasic, although he manifested certain striking peculiarities of speech, or, rather, of the manner of speaking. What he said, either spontaneously or in answer to questions, was spoken clearly and distinctly and in a firm, loud voice. His sentences were short, but complete; neither words nor syllables were omitted; and he made no mistakes in articulation, enunciation, or pronunciation. In answering he did not seem to be able to retain for any length of time a hold upon the same idea or to follow a particular train of thought. He did not wander from one subject to another, but he would suddenly stop speaking, as if unable to go farther. Often on being questioned he would try to reply, and after a sentence or two would sob and burst into tears like a violently hysterical woman. He would at times have what might be termed volcanic outbursts of speech. When all was perfectly quiet in the ward he would suddenly explode with a sentence or two, and then again subside into stillness. Exclamations of this kind might be repeated at intervals of a few minutes for hours together, or they might recur only at intervals of hours. Sometimes what he said would be connected with some past events of which he seemed to have a vague recollection; often it would be a demand for something to eat or drink; and often, again, it would be a paroxysm of profanity.
23 Philadelphia Medical Times, Jan. 18, 1879.
Impairment of will is not uncommon in antero-frontal and other cerebral tumors, and failure of memory, depression of spirits, and even acute mania, occur. Many of the patients are emotional, excitable, and irritable; they often sob and cry, apparently from the great pain. In some cases, however, emotional conditions are present which seem to be dependent on some special localization of the tumor. Hallucinations were noted in two of our tabulated cases. In one case, a tumor of the motor zone, the patient had delusions that some one was about to take him away. There were also illusions of fear or persecution. In another the patient had visual hallucinations.
Speech-defects of various kinds occur in connection with intracranial growths. Ladame, quoted by Rosenthal, has cited forty-five cases of disturbances of speech in which the tumor occupied the most varied regions of the brain. Peculiar disorders of speech from special localizations will be treated of under Local Diagnosis.
Local spasms, which go under various names, as cramps, twitchings, epileptoid attacks, athetosis or athetoid movements, are common symptoms, particularly of growths which involve the cortical motor area. They are of great diagnostic value. They are commonly, although not invariably, accompanied by paresis, which is usually most marked in the [p. 1039] part most affected by the spasm. These local spasms, beginning in one extremity, in a finger or toe it may be, often spread toward the centre, until they involve to a greater or less extent the whole limb, the side of the face, or one-half of the body. Sometimes instead of this they recur with the same definite movements over a long period. They are the expression of irritation of cerebral centres or tracts connected with the muscles or groups of muscles affected by the abnormal movement. They should always lead the physician to carefully consider the great probability of a lesion in some way involving the motor area.
Tumors of the cerebellum, pons, and medulla oblongata sometimes give rise to general convulsions which closely simulate attacks of grave epilepsy. These convulsions or general spasms are among the most important symptoms of intracranial neoplasms. More than paralysis, they may be regarded as general symptoms, as they are more likely to occur from tumors situated in different and distant regions of the brain than paralysis. They are by no means confined to cases in which the lesion is situated in the so-called motor area of the brain or in the cerebellum or pons-medulla region. Both physiological and pathological experiments have shown that convulsions violent in character, but having certain special characteristics, may originate from severe irritation of the dura mater. According to Duret,24 irritation of the sensory nerves of the dura mater cause reflex spasms or contractures of the muscles of organic life. These spasms or contractures may occur in the face, eyeballs, neck, trunk, or limbs, and sometimes on one side and sometimes on the other. They tend to diffuse and invade neighboring groups of muscles. “They have never the localization, the measured and purposed character, of the contractions which belong to the lesions of the cortex. They frequently become transformed into permanent contractures.” The application of these facts and conclusions to brain tumors is evident. As neoplasms are so frequently connected, either directly with the dura mater or with the fused membranes, it is evident that the convulsive attacks from which the patient suffers may occur from tumors located anywhere within the cavity of the skull.
24 Sur les Traumatismes cérébraux, par H. Duret, chapter iii., summarized in Brain. vol. i., 1878, p. 47.
General convulsions, as well as local or unilateral spasms, are present in many tumors of the motor cortex; but if their method of origin and their progress are closely watched they will usually be seen to begin with local twitchings.
A glance at the table will show examples of convulsion in almost every region of the brain.
Contractures—conditions of tonic spasm which continue more or less persistently—may be either early or late symptoms. They may occur in one or several limbs, in the face, or rarely in the neck. They are probably due in some cases to persistent irritation of the dura mater, in others to comparatively slight but continuous irritation of motor centres, and in still others to advanced degeneration of the motor tracts.
Choreas and choreic movements are not frequent, unless some of the forms of local spasm are regarded as local choreas. In one of Petrina's cases, a glioma involving the substance of both frontal lobes, choreic movements of the right arm were present, and in this same case tremor [p. 1040] in both arms was also a symptom. Tremor simulating that of paralysis agitans or multiple cerebral sclerosis is occasionally observed, and sometimes a tremor which is nervous or hysteroidal in character is one of the results of the great suffering of the patient.
Paralysis or paresis is of course one of the most frequent evidences of the existence of an intracranial tumor. The palsies of cerebral tumors are chiefly unilateral, but the loss of power may be in one or both limbs, in one side of the face, or in the entire one-half of the body, according to location and extent. Tumors of the cortical motor zone usually begin their paralytic manifestations with paresis of one member or one side of the face, which goes on, as the growth increases in size, to more or less complete hemiplegia.
The paralysis which results from brain tumor is due either to pressure or to absolute destruction of tissue. In the latter case the destruction is brought about not only by the simple displacement of brain-substance, but also through the obliteration of blood-vessels and the consequent softening.
Peculiar forms of paralysis occur as the result of neoplasm growing in special locations, as will be more clearly shown under Local Diagnosis. Thus we have the alternating paralyses from tumors of the crus cerebri or of the lower part of the pons, and paraplegia, or perhaps what might be better called double hemiplegia, from multiple tumors which affect both sides of the brain. In rare cases paralysis of all four extremities has resulted from a growth in the middle line of the base of the brain. Some form of paralysis is recorded to have been present in 20 cases out of 100.
Apoplectiform attacks sometimes take place suddenly during the progress of cases of brain tumor. A patient who has been suffering for months with the general symptoms of tumor, and who may or may not have had some paresis of the limbs or face, has an attack of unconsciousness, from which he arouses after a time, and is then found to be almost completely hemiplegic. After such attacks, in some cases, the symptoms of brain-irritation, particularly the headache and vomiting, subside or greatly improve. Such attacks may be explained in several ways—from the occurrence of congestion with œdema, of intercurrent hemorrhage, or of softening from obliteration of blood-vessels by the advancing growth; and the temporary subsidence or more permanent disappearance of the headache and other symptoms is probably, in some cases at least, owing to the diminution of tension because of the breakdown of tissue in the neighborhood of the growth. Sometimes the seizures which occur during the progress of the case are both epileptiform and apoplectiform in character.
Sometimes in cases of intracranial tumor there are present in the cranial nerve-trunks and the muscles supplied by them the changes known as the reactions of degeneration. These changes are characteristic of the peripheral palsies, and indeed sharply distinguish them from paralyses of central origin. The exception to this rule in cases of intracranial growths is, of course, only apparent and not real, because these palsies, when caused by the pressure of a tumor on a nerve-trunk, even within the cavity of the skull, and not upon their proper centres or intracerebral tracts, are as much peripheral as though the injury was caused by compression of these [p. 1041] nerve-trunks outside of the skull. These reactions of degeneration are briefly as follows: The nerve-trunk gradually, sometimes rapidly, loses its response to both the galvanic and faradic currents. The muscle loses its response to faradism coincidently with the nerve-trunk, but to galvanism it is apt to exhibit first increased excitability, then gradually lessening excitability: and with this lessening response it puts on the so-called qualitative changes. These consist of the serial alterations—i.e. the negative pole, instead of exciting the more active reaction at closure, gives a less response than the positive pole at closure, and also calls forth a response at opening which may be greater than the opening contraction of the positive pole, which may be abolished. In health the positive pole causes often an active response, and the negative pole none, or almost none, at opening. Finally, occur modal alterations in the affected muscles, which consist of a slow, lazy contraction instead of a quick, lively one as in health, and a tendency in the muscle to remain contracted (tetany) while the current is passing. The many modifications—or, better, the partial exhibitions of these changes and the conditions underlying them—are to be sought in detail in special treatises. It is sufficient to say that they have been reported in a number of cases of brain tumor, and that the nerves in whose distributions they would be especially seen are the motor oculi, or third, the abducens, or sixth, and the facial, or seventh. It is doubtful if a very exact electrical examination could be made of many muscles supplied by these nerves, except in the case of the facial, and possibly the elevator of the upper eyelid. It is in the case of the seventh nerve that the recorded observations have been made. It will be noticed, by reference to the table, that the third, sixth, and seventh nerves are frequently involved in tumors of the crus and pons-medulla region, and that the paralysis is usually on the side of the lesion. These are the cases which would exhibit the reactions of degeneration. It has been said that in ordinary hemiplegia, and also in paralyses from tumors of the brain high in the motor region, the affected side exhibits simply a qualitative increase to electrical excitation; and this may be explained by the increased excitability to all stimuli of the lower or spinal-cord centres when cut off from the brain. The statement, however, which has been made, that in tumors of the cerebellum the sound side exhibits a quantitative decrease, sounds like a paradox, and requires further tests before being accepted as a fact in electro-diagnosis.
Ataxia has been observed in cases of brain tumor situated in various locations. The symptom described as ataxia, staggering, or staggering backward, is more particularly observed in cases of tumor of the cerebellum, pons, and corpora quadrigemina.
Changes in the state of the reflexes are somewhat frequent. Usually the skin and tendon reflexes will be increased on the side opposite the lesion, although some striking exceptions, probably due to the positions of the growth, occur.
Atrophy of the limbs is sometimes present, but usually in brain tumor, as the lesions are above the nutritive connection of the nerve, true atrophies do not occur.
True neuralgias are frequent, particularly in the distribution of the trigeminal. Trigeminal neuritis also undoubtedly occurs in lesions [p. 1042] involving this nerve at its origin, in its course, or in the Gasserian ganglion.
Anæsthesia, either in the form of local or hemianæsthesia, was observed in about 20 per cent. of the cases. It is rarely present as an isolated symptom, but frequently accompanies unilateral paresis. In a partial or variable form it most frequently is seen in connection with tumors of the Rolandic region. It is a marked symptom in postero-parietal growths and those involving the posterior part of the internal capsule. It may take the form of loss of sensation to pain, touch, pressure, temperature, etc.
Hyperæsthesia occurs so commonly as to be almost regarded as a general symptom of brain tumor. Sometimes it is confined to the head; sometimes it is generally diffused; more frequently it is present in the limb or limbs affected with the paralysis. With hyperæsthesia the patients often complain of spontaneous pain in the limbs.
Diplopia or double vision is a somewhat frequent symptom, occurring most commonly, of course, when the ocular nerves are involved directly or indirectly by the tumor; hence tumors of the floor of the skull, of the crus cerebri, of the pons, or of the cerebellum are most likely to give rise to this symptom. A close study of the character of diplopia and of other symptoms which go with it will usually enable a local diagnosis to be made. Diplopia, however, does sometimes occur in tumors situated remotely from the base, either because of pressure, because of general nervous weakness, or possibly because of involvement of cortical oculo-motor centres.
Ptosis is another symptom, generally unilateral, and most frequently present in connection with strabismus, diplopia, and dilatation of the pupil from involvement of the third nerve. Dilatation of the pupil and contraction of the pupil may be present as general symptoms of tumors. The latter is most probably due to meningeal irritation.
Hemianopsia is another ocular symptom sometimes present in cases of brain tumor, as it may also be in other forms of encephalic lesion. It was present in 5 of 100 cases. Norris25 gives a full description, brought well up to the present time, of this symptom, and a discussion of the lesions upon which it depends. Seguin26 also discusses this subject. Starr27 has collected a large number of cases of lesion causing this symptom, some of which have been reproduced in our table. We will not go into any details as to the character of this symptom, referring the reader to the sources indicated. In the first case given in our table (Case 10) the hemianopsia was produced by a tumor in front of, and impinging upon, the optic chiasm; in the other four cases (Cases 40, 41, 42, and 43) the tumor was situated in the occipital lobe, and was surrounded by an area of destroyed tissue. Hemianopsia is not, strictly speaking, a symptom of brain tumor, but is likely to be present in cases occurring in certain regions of the brain. Starr's conclusions with reference to lateral homonymous hemianopsia when it is not produced by a lesion of one optic tract are that it may result from a lesion situated either (1) in the pulvinar of one optic thalamus; (2) in the posterior part of one interior capsule or its radiation backward toward the occipital lobe; (3) in the medullary portion of the occipital lobe; or [p. 1043] (4) in the cortex of one occipital lobe. The conclusions of Seguin are only different in so far as they more closely limit the position of the lesion.
25 Vol. IV.
26 Pp. 84, 85 of present Volume.
27 Amer. Journ. Med. Sci., N. S., vol. lxxxvii., January, 1884, p. 65.
Phosphenes, or subjective sensations of light, occur in various forms—simply flashes or sheets of light, scintillations, balls of fire, etc. They are not very common as isolated phenomena, and probably are dependent in most cases upon irritation of the nerve and retina in some of the stages of neuro-retinitis. Even visual hallucinations are occasionally present, as in one of Bennett's cases of tumor of the Rolandic region.
Conjugate deviation of the eyes, with rotation of the head, a symptom of the early stages of apoplectic attacks, is also sometimes observed in brain tumor. The patient is found with both eyes turned to one side and slightly upward, as if looking over one or the other shoulder, the head and neck being usually rotated in the same direction. Sometimes the deviation is slight, sometimes it is marked. Frequently the muscles of the neck on one side are rigid. The eyes are commonly motionless, but occasionally exhibit oscillations. This sign, well known to neurologists, usually disappears in cases of apoplexy in a few hours or days, although it occasionally persists for a long time. It will be more fully considered under Local Diagnosis.
Diminution or loss of hearing, tinnitus, and hyperæsthesia of hearing are all occasionally observed. The most decided disturbances of this sense are those which are found in connection with tumors of the base or of the cerebellum in such a position as to involve the auditory nerve or auditory tracts. Tinnitus, acoustic hyperæsthesia, with complete or partial deafness, accompanying facial paralysis, with or without paresis of the limbs of the opposite side, indicate clearly a tumor of the base so situated as to involve the superficial origin or intracranial course of the auditory and facial nerves.
The sense of smell is affected, of course, when the olfactory bulbs are involved in the growth, either directly or by pressure, as in certain tumors of the antero-frontal region (Cases 4 and 8). Disturbances in the power of consciously perceiving odors, or abnormal perceptions of odors or hallucinations of smell, are sometimes present in cerebral tumors involving certain convolutions. The lower postero-parietal region or the temporo-sphenoidal region of the base would seem, from the few reported cases, to be implicated when this sense is centrally affected. Smell was lost or impaired in two cases of tumors of the postero-parietal region, in one limited to the supramarginal convolutions. In a case reported by Allan McLane Hamilton (Case 47), an induration of the lower part of the right temporo-sphenoidal lobe involving the uncinate gyrus, the patient, preceding light epileptic attacks, always had an olfactory aura of a peculiar character—a disagreeable odor, sometimes of smoke and sometimes of a fetid character. In this case the olfactory nerves were examined and found to be healthy.
Taste may be involved in several ways. In the first place, subjective sensations of taste, particularly the so-called metallic taste, may be present when the growths involve the cranial nerves in such a way as to cause irritation to be conveyed to the nucleus of the hypoglossal. When it is remembered that a mild galvanic current applied to the nape of the neck or face will often cause this metallic taste, it can be seen [p. 1044] that the irritation of a tumor situated at almost any point of the base might lead to abnormal taste-phenomena. Neoplasms involving the trunk of the portio dura may of course cause diminution or loss of taste on the anterior extremity of the tongue by the involvement of the chorda tympani nerve. In the very few cases in which the hypoglossal trunk may be involved disturbances of taste posteriorly may occur. In two cases (Cases 33 and 36) some possible indications as to the cortical areas of taste are given. One was a tumor so situated as to cause pressure on the orbital, and possibly anterior, portion of the temporo-sphenoidal lobe; the other was a lesion closely localized to the supramarginal lobule.
Trophic disturbances of decided character are sometimes present in cases of brain tumor. Their presence, character, and extent depend upon the position of the tumor and the cranial nerves involved. Trophic disorders of the eye have been noted in cases of tumor of the antero-frontal region, and also of various positions at the base, especially those so situated as to involve the trigeminal nerve. In a fibroma of the superior antero-frontal region (Case 1) conjunctivitis and corneitis of the left eye, with anæsthesia of the conjunctiva, were present, and were very marked symptoms. This patient, who was under the care of one of us at the Philadelphia Hospital, was examined by O. E. Shakespeare, ophthalmologist to the hospital. At his first examination the bulbar conjunctivæ were slightly injected and the cornea clear. The sensibility of the cornea was possibly a little lowered. Ten days later, at a second examination, the central corneal epithelium of the left eye was found to be hazy and the whole bulbar conjuntivæ much congested. “This condition soon developed into a severe superficial corneitis, which was mainly limited to a central area of an extent about equal to three-fourths of the diameter of the cornea, which threatened to slough, a narrow peripheral ring of the cornea being comparative unaffected. At the same time the engorgement of the bulbar conjunctiva increased. The sclera, the iris, and the deeper parts were apparently not involved in the inflammatory process.”
Disturbances of respiration were observed in a number of cases in various stages. Cheyne-Stokes breathing was usually a late symptom. In a case of tubercular meningitis with a tubercular granulation springing from the left side of the fourth ventricle (Case 82) it was present. Extraordinary slowing of respiration occurred in a tumor of the right middle cerebellar peduncle and cerebellar hemisphere which caused irritation and softening of the floor of the fourth ventricle. The respirations ran as low as four and five per minute two weeks before death.
Persistent epistaxis and a tendency to hemorrhage from the mucous membranes were interesting vaso-motor phenomena in a case situated in the upper left quarter of the pons (Case 84). Profuse perspiration, more marked on one side, was observed in a case of tumor in front of the optic chiasm. Polyphagia was observed in two cases, one a growth of the cerebellum and the other on the floor of the skull. Polyuria was a very marked symptom in Case 95, a tumor at the base of the brain at a spot corresponding to the sella turcica, and diabetes was present in a case of frontal tumor. Albuminuria was recorded twice—once in the same case in which diabetes was present, and again in a case of [p. 1045] multiple tumor of the supramarginal convolution of one side and the angular gyrus of the other. Somnolence was occasionally observed.
Constipation or torpor of the bowels occurs somewhat frequently in the early stages of the brain tumor, giving place in the terminal periods to involuntary evacuations. The conditions of the bladder are practically the same. It is either not involved or suffers from torpor or paresis of the muscular walls early in the disorder, and later, and especially very late, incontinence from paralysis of the sphincter results.
DURATION, COURSE, AND TERMINATION.—The duration of cases of intracranial tumor is very uncertain. In many of the reported cases no definite information is given as to the exact length of time from the initial symptoms until the fatal termination. The few cases in which the time was recorded showed a duration of from three months to as many years.
In a few cases, even in some which are not syphilitic in character, a remission of all the symptoms and what appears to be an approximate cure sometimes take place, the general symptoms, such as headache, vertigo, vomiting, spasms, etc., disappearing for a time. Even the condition of the eyes and the paralysis in rare instances make marked improvement. In these cases, in all probability, the progress of the growth of the tumor is arrested either by the remedies employed or spontaneously, and the acute or subacute phenomena of congestion, œdema, etc. around the tumor subside. These patients may remain for a long period or until cut off by some other disease without any change for the worse; but the sword constantly hangs above their heads, and any excitement, traumatism, the abuse of alcohol or other narcotics, an attack of fever, or some other special exciting cause, may again light up the intracranial disorder, to then progress more or less rapidly to a fatal termination.
This fatal termination may occur in various ways. Sometimes a sudden apoplectic attack occurs. This may be an intercurrent hemorrhagic apoplexy, although our personal experience would not lead us to believe this mode of termination is common. In a few cases the enormous irritation of the cerebral growth suddenly or gradually inhibits the heart's action through the impression made on the pneumogastric. Apoplectic attacks which may or may not terminate fatally sometimes are the result of a sudden giving way of necrosed brain-tissue, the necrosis having resulted from the obliteration of numerous blood-vessels by the advancing growth. Blood-poisoning occasionally takes place from abscesses in proximity to the tumor. In some cases the patients slowly but surely emaciate, or are exhausted and worn out by the agonizing pain and incessant vomiting which they are called upon to endure. Occasionally a more or less diffused and violent meningitis hastens the fatal issue.
COMPLICATIONS AND SEQUELÆ.—Tumors of the brain may be complicated with other affections due to the same cause. Thus, for example, in a case of gumma other evidences of syphilis may be present in the form of nodes, eruptions, etc. A sarcoma or carcinoma of the brain may be associated with similar disease in other organs. Such affections as cystitis, pyelitis, keratitis, etc., which have been discussed under Symptomatology, are secondary complications of cases of tumor. As [p. 1046] intracranial tumors almost invariably terminate fatally, strictly speaking we have no sequelæ.
PATHOLOGY.—We present in tabular form the various classes of tumors found in the one hundred cases of brain tumor in the table appended to this article:
| Carcinoma | 7 | Glio-sarcoma | 1 |
| Cholesteotoma | 1 | Gumma | 13 |
| Cyst | 2 | Lipoma | 1 |
| Echinococcus | 2 | Myxo-sarcoma | 1 |
| Enchondroma | 1 | Myxo-glioma | 2 |
| Endothelioma | 1 | Osteoma | 2 |
| Fibro-glioma | 2 | Sarcoma | 15 |
| Fibroma | 4 | Tubercle | 13 |
| Glioma | 16 | Unclassified | 16 |
The histology of tumors of the brain does not in the main differ from that of the same growths as found in other parts of the body, so that a detailed description of their structures, even though founded upon original research, could not offer many novel facts in a field which has been so thoroughly cultivated. Such a description would probably repeat facts which have already been presented in other parts of this work, and which are better and more appropriately put forth in special treatises devoted to the science of pathology. It is proper, however, for the sake of convenience and thoroughness, to make brief mention of the structure of brain tumors, and especially to dwell upon certain features of these morbid growths which may be considered characteristic of their encephalic location, and hence have not only pathological but also clinical interest. It is hardly worth while to refer to speculations which aim to elucidate the very foundations of the science, except that in a few of these theories we gain an additional insight into both the structure and conduct of some very characteristic brain tumors.
Cohnheim's theory was that tumors are formed from foci of embryonal tissue which had been non-utilized or left over in the intra-uterine development of the body. Many have not accepted this idea, but have rather considered that in tumors we witness a reversion of tissue to lower or embryonic types.28 Whether we accept either or neither of these propositions, the idea sought to be conveyed is that in all these morbid structures we have a tissue of low or degraded character, springing in most instances from a connective or non-differentiated tissue. This fact is brought out very clearly in many of these intracranial growths. Virchow29 has said that tumors originate in the cells of the connective tissue, although his law has been condemned as not of sufficient breadth, since it seems to ignore the epithelial and myomatous tumors. Dermoid cysts, of which an example is given in the table of spinal tumors,30 are said to illustrate the embryonic function revived—i.e. the tendency of lower tissues to spontaneously differentiate into higher and more complex ones.
28 Article “Pathology” in Brit. Encyc., by C. Creighton.
29 Quoted by Cornil and Ranvier.
30 Page 1107.
The gliomata are among the most common and characteristic tumors of the cerebro-spinal axis, to which system and its prolongation into the retina they are confined. They invariably spring from the neuroglia or connective tissue of the nerve-centres, and reproduce this tissue in an embryonal state. They greatly resemble the brain-substance to naked-eye inspection, but have, histologically, several varieties of structure. [p. 1047] These variations depend upon the relations of the cell-elements to the fibres or felted matrix of the neoplasm. In the hard variety the well-packed fibrous tissue preponderates over the cell-elements, and we have a tumor resembling not a little the fibromata (Obernier). The second variety, or soft gliomata, show a marked increase of cells of varied shapes and sizes, with a rich vascular supply which allies these growths to the sarcomata. The elements of gliomata sometimes assume a mucoid character, which allies them, again, to the myxomata.
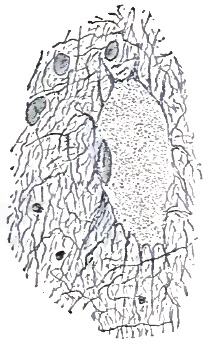
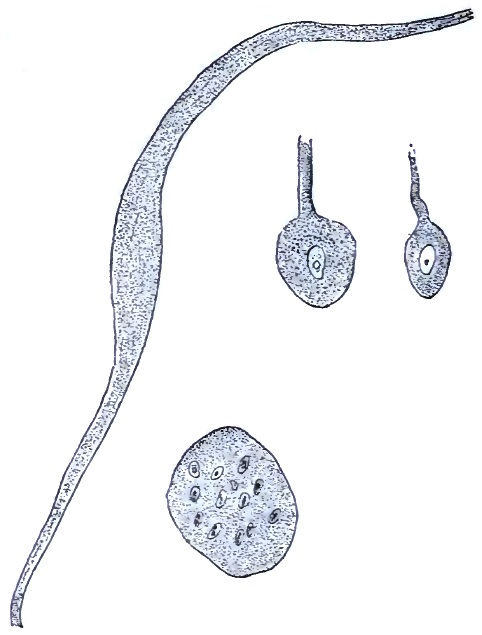
W. Osler has recently described31 to the Philadelphia Neurological Society the structure of certain of these tumors, from which we abstract the following facts: One point referred to is that gliomata sometimes contain larger cells and coarser fibres than are usually shown. The structures are (1) The “spinnen” or spider-cells (characteristic of glioma), which present variations in size; (2) large spindle-shaped cells with single large nuclei (some of the largest cells met with in tumors); (3) cells like the ganglion-cells of nerve-centres, with large nuclei and one or more processes: some are balloon-shaped with single processes; they are larger than the spider-cells; (4) translucent band-like fibres, tapering at each end, without nucleus or granular protoplasm, regarded as a vitreous or hyaline transformation of the large spindle-cells. Klebs (quoted by Osler) holds that the ganglion-like cells are derived from the nerve-cells of the gray matter, “and that in the development of this variety all elements of the nerve-tissue participate.” Osler examined the advancing region of [p. 1048] the tumor, and was not able to satisfy himself that the nerve-cells were in process of proliferation. He thinks they are connective-tissue elements. He has seen but two out of five cerebral gliomata which were of small-celled type.
31 “Structure of Certain Gliomas,” Philada. Med. News, Feb. 20, 1886.
The gliomata are subject to fatty degeneration, which usually occurs in the central (older) portions of the mass. The more vascular forms are also peculiarly liable to hemorrhage, which is probably caused in some instances by this process of retrograde metamorphosis. These hemorrhages resemble apoplexies, not only in their clinical features, but also on gross examination. Great care is therefore often necessary at the autopsy to distinguish such a hemorrhage, occurring as it does in a brain-like neoplasm, from one caused by the rupture of a diseased artery. The hypertrophy of the pineal gland, sometimes noted, is caused by the formation of gliomatous tissue. Under the microscope it is necessary carefully to distinguish some forms of inflammatory new formations from the gliomata. We have recently seen, by the courtesy of E. N. Brush of the Pennsylvania Hospital for the Insane, photographs of microscopic sections from the ependyma of the lateral ventricles in a case of general paresis, which showed the structure of this degenerated tissue to be a compound of fibres and cells of marked resemblance to gliomatous tissue.32
32 These micro-photographs were prepared in the laboratory of the State Lunatic Asylum, Utica, New York, by Theodore Deecke.
Sarcomata of the brain are common, as our table shows. In them the cell-elements predominate, both in the large- and small-celled variety. They are malignant and grow rapidly. The form known as alveolar sarcoma, which has a distinct stroma, is to be distinguished from the cancers; which has probably not always been done.
Tubercle, according to Ross, is the most common of all forms of brain tumor. Our table shows 13 cases out of 100, the gliomata and sarcomata being in larger number. Its favorite seat is in the cortex of both the cerebrum and cerebellum: some observations appear to show that it is more common in the cerebellum and mid-brain region than in the fore-brain, and in children than in adults; some of which points distinguish it from the gummata, which are more common in adults and occur anywhere. Tubercle is another form of development from the connective tissues, usually dependent upon a constitutional taint or predisposition: in it the cell-elements have generally undergone a degeneration into an amorphous cheesy mass. It is apt to be multiple and accompanied by a similar deposit in other organs of the body.
True neuromata are probably very rare growths, and it is likely that some tumors which have been described as such are really connective-tissue tumors of a gliomatous nature, in which some of the cell-elements have been mistaken for the ganglion-cells. Obernier33 says that these tumors are small and grow from the gray matter on the surface, also on the ventricular surfaces. They are also found in the white matter. He says they are only found in persons having some congenital or acquired aberration; by which is probably meant some other well-marked neurosis or psychosis. The one hundred tabulated cases afforded no examples of neuromata.
33 Op. cit.
Myxomata are not, histologically, to be distinguished from the [p. 1049] gliomatous tissues by anything but the peculiar mucoid changes which their structures have undergone. They are more rare in the brain, as our tables show, than in the spinal cord.
Lipomata are very rare in the brain, according to most observers. The table shows but one example. These tumors, as their name signifies, are made of fat-bearing tissues—another of the connective-tissue class.
The angiomata, somewhat rarely found within the skull, are noted for their abnormal development of the vascular tissues: they are composed mainly of blood-vessels and the connective tissue, which supports them in closely-packed masses. They also present cavernous enlargements. They are of especial interest in cerebral pathology, because the lesion known as pachymeningitis hæmorrhagica, often found in dementia paralytica, is considered by some to be angiomatous; although by far the most generally accepted view of this latter condition is that it is due to arterial degeneration, and in part is an inflammatory exudate.
Syphilitic tumors, or gummata, are, like tubercle, a special development with degeneration from the connective tissue, due to a constitutional taint. This new growth is sometimes single, sometimes multiple. The corpuscles of the neuroglia are the apparent points of origin of the tumor, the substance of which is the firm, peculiarly gummy, and non-juicy material from which the name is derived. It would be impossible in our allowed space to trace this neoplasm through the successive stages of its development. It has especial clinical interest, inasmuch as it and its damage are probably amenable to specific treatment when it has not progressed to too great a destruction of brain-tissue.
The true cancers, or epithelial neoplasms, are not a common form of tumor of either the brain or spinal cord. They present, as in other parts of the body, a stroma forming alveolar spaces in which are contained the nests of epithelial cells. These tumors thus present characteristic differences in their histology from the connective-tissue or mesoblastic groups, but clinically no very special interest attaches to them. Their location, the rapidity of their growth, and their fatal import are points which they share with most other new growths of the cranial cavity.
The cholesteotomata, or pearl cancers, consist of hardened epithelial cells which have undergone a sort of fatty degeneration.
The psammomata are loosely described as tumors containing sand-like bodies, which bodies are normal about the pineal gland. These sand-like bodies are found in tumors of some histological diversity, and do not appear to have much identity of their own. They occur in sarcomata and carcinomata, and are probably not to be distinguished from mere calcareous infiltration and degeneration. They are most common in sarcomata, as this is one of the most common of cerebral tumors.
True osteomata—i.e. tumors with the structure of true bone—are probably rare in the brain, although more common on the inner table of the cranium; but the deposition of calcareous salts has been recorded in a variety of conditions. F. X. Dercum, in a recent paper read before the Philadelphia Pathological Society,34 has recorded the autopsy of a paretic dement in which case calcareous deposits were scattered throughout both hemispheres and the cerebellum. He believes that “the areas in [p. 1050] which the concretions were found were probably foci of encephalitis of greater intensity than elsewhere. In these foci inflammatory changes in the walls of the vessels became pronounced; besides which the vessels increased enormously in size and number; so marked is this increase that these foci could, with perfect propriety, be called angiomata.” This is followed by proliferation of the neuroglia, compression and destruction of nerve-tissue, and deposit of the calcareous salts especially about and upon the coats of the vessels. This case illustrates in the simplest manner the formation of both vascular and sand tumors.
34 The Medical News, April 24, 1886, p. 460.
Pacchionian bodies are very common in the brain, and are really small fibromata. They may form true tumors (Cornil and Ranvier) capable of wearing away the bones of the cranium. In fact, even when small they may have corresponding indentations in the skull. They are not to be mistaken for tubercle. Clouston35 has described excrescences from the white matter of the brain, growing through the convolutions, projecting through the dura mater, and indenting the inner table of the skull; which new growths he calls hernia of the brain through the dura. We have not seen such a condition described elsewhere, and think that we have here probably Pacchionian bodies growing from the pia mater. They were found in a case of tumor of the cerebellum.
35 Journ. Ment. Sci., xviii. p. 153.
A cystic formation, constituting a veritable tumor, not unfrequently occurs in the pituitary body and mounts into the third and lateral ventricles. Echinococci and hydatids also occur, and have the same natural history as these parasitic offspring have when found in other parts of the human body.
Obernier refers to an enchondrosis of the basilar process. Our table presents one case of enchondroma.
Some of the gross appearances found on autopsies of tumors of the brain are worthy of note. Often an area of congestion or inflammation, especially of the membranes, is seen about the new growth, and the brain-substance in its immediate vicinity is much more frequently softened. The cerebro-spinal fluid is increased, and, especially when direct pressure has been exerted upon the veins of Galen, are found distended lateral ventricles. When a tumor does not approach the surface, but has attained some size, the hemisphere in which it is located often has a bulging appearance, crowding over upon its neighbor, and the convolutions are flattened by the pressure. The cranial nerve-trunks are occasionally involved in or stretched by the tumor, and also occasionally the bones of the vault or base of the cranium are extensively eroded. This happens especially in cancer and osteo-sarcoma.
A few remarks should be made about the methods of making post-mortem examinations and the gross appearances and conditions likely to be found in brain-tumor cases. As not a few intracranial tumors are connected with the bone or with the dura mater, the latter being adherent to the skull-cap in some positions because of inflammation arising from the seat of the growth, especial care should be taken in removing the calvarium. Examination of the external surface of the dura mater will sometimes reveal the presence of a growth beneath or incorporated with this membrane. The dura mater should not be roughly dragged from the surface of the brain, but should be carefully removed by a [p. 1051] process of partial dissection. During this process a meningeal growth will sometimes be found growing apparently from the fused membrane. In such cases it is usually better to so proceed as not to entirely separate the outer membrane from the growth. Indeed, this cannot be done sometimes without injury directly to the specimen, and especially to its cerebral surroundings. The dura mater having been removed, a marked opacity, sometimes a dirty-brown hue shading off into a lighter color, will indicate to the eye the probable presence of a tumor beneath and growing from the pia mater of the cortex. In such a case, and even when no such appearance is present, but a tumor is suspected, the fingers passed carefully over the cerebral surface will feel a hard, and it may be nodulated, mass at some position. A growth, having been located in this way, should not be roughly handled or at once examined by section. An effort should be made to accurately localize it, not only with reference to lobes, but also with reference to convolutions and fissures, and even special portions of these. This is best done, after a thorough examination has been made of the pia mater, by carefully stripping the pia mater from the brain, beginning at points some distance from the growth and gradually approaching it, and leaving the pia mater for a short distance around the growth connected with it. The location having been fixed and other portions of the brain having been examined, if it is not possible or desirable to retain the entire brain as a specimen, a block should be removed embracing a considerable portion of healthy brain-tissue on all sides of the tumor. In order to study the gross internal appearance of the tumor, it is a good plan to make a clean section through the middle of the tumor. From each side of this cut fragments can be taken for microscopical examination without deranging appreciably the size and appearance of the tumor.
When the tumor is not meningeal or cortical, or not situated at the base or floor of the skull, its presence may be revealed, when it is in centrum ovale and of considerable size, by either hardness or fluctuation of the hemisphere in which it is located, this fluctuation not being due to the tumor itself so much as to the breakdown of tissue around it. Large sections in known positions with reference to convolutions and ganglia should be made when examined for tumors deeply situated. If possible, sections close to and just before and behind the growth should be made, so as to assist in the accurate localization.
Small tumors are not infrequently overlooked by careless observers, and even growths of considerable size have escaped discovery by one examiner to be found by another. Tumors in certain special localities, as between the temporo-occipital lobe and the superior surface of the cerebellum in the great longitudinal fissure, or small growths in the substance of the cerebellum or deep in the Sylvian fissure, are more likely than others to be passed by, although this, of course, is not likely to occur when the examination is made by a competent or careful physician.
DIAGNOSIS.—The diagnosis of the existence of an intracranial tumor, as a rule, is not difficult. It can be made with greater certainty than that of almost any other serious encephalic disease.
It is sometimes important to decide as to the nature of an intracranial neoplasm, particularly whether or not it is syphilitic. Little is to be gained by following the plan adopted by some physicians, of treating all cases as if they were due to syphilis, on the principle that these [p. 1052] are the only forms of tumor which can be reached by treatment. The pitiable condition of such patients is sometimes thus made worse. In every case careful and persistent efforts should be made to obtain an authentic previous history from the patient. Whenever possible the physician should search directly for the physical evidences of the former existence of syphilis—for cicatrices on the genitals and elsewhere, for nodes and depressions, for post-cervical and other swellings, etc. A history of previous disease of the throat and of pains in bones and nerves, of epileptiform attacks, of headache, and eye symptoms which have disappeared under treatment, should be sought out. It is not well to give too much credence to the stories of patients, who are not always willing to admit their past lapses from virtue; but, on the other hand, the plan of suspecting everybody who presents advanced cerebral symptoms is often a grievous wrong. Not infrequently external cranial nodes are present in cases of intracranial syphilis.
Carcinomata and sarcomata, particularly the former, are comparatively rapid in their progress. They sometimes involve the bones of the skull, even to the extent of perforation.
The existence of an inherited tendency and of tuberculosis in other organs, with the special phenomena of general tuberculosis, assists in the diagnosis of tubercular tumors.
The frequent occurrence of gliomata in early life, and the comparatively frequent absence of severe irritative symptoms, with the well-preserved general nutrition of the patient, speak for these growths.
Cerebral abscess is, on the whole, more difficult to diagnosticate from intracranial tumor than any other affection. Abscess, however, more frequently than tumor, can be traced directly to a traumatism. It is often associated with disease of the internal ear. Obernier speaks of the headache of cerebral abscess as slight, but this does not correspond with usual experience. Headache, on the whole, may be oftener absent or less agonizing in abscess than in tumor, but it is frequently present, and sometimes of great severity. Its greater mildness in a few cases is to be explained by the fact that abscess does not produce so much pressure within the intracranial cavity, and does not so frequently cause irritation of the branches of the trigeminus in the dura. Undoubtedly, the symptoms of abscess often remain for a long time comparatively latent, with then a sudden outburst of violent symptoms. The course of brain tumor is more uniformly and steadily progressive, and febrile phenomena, the results of pyæmia, are of more frequent occurrence in abscess than in tumor.
In old cases of tumor it is sometimes necessary to differentiate between it and the results of various forms of apoplexy, such as hemorrhage, thrombosis, and embolism. Cerebral hemorrhage, embolism, or thrombosis leaves a condition of paralysis, sometimes with, but usually without, accompanying spasm or convulsion, which simulates closely the paralysis and other permanent conditions of cases of tumor occurring in the same cerebral locality. In these cases, in the first place, the history of the disease will throw considerable light upon the diagnosis. In both hemorrhage and embolism the history is usually one of a sudden attack without special premonitory symptoms. Hemorrhage gives usually a precedent history of diseased kidneys, hypertrophied heart, or [p. 1053] atheromatous blood-vessels, and occurs generally in advanced life; embolism, a history of rheumatism and valvular disease of the heart, occurring at any period of life, early or late. In brain tumor the previous history is usually one of traumatism, of constitutional infection, or of a special predisposing diathesis. Blows and falls upon the head are common antecedents, or a history of syphilis, tuberculosis, scrofula, or cancer is present. Tumor, like embolism and unlike hemorrhage, may occur at any time of life. While slight or dull headache, with more or less vertigo, may be present in cases of hemorrhage and thrombosis, the severe and often agonizing headache, with vomiting and serious vertiginous attacks, which precedes the paralytic or other phenomena of tumor, is a much more conclusive symptom in the latter cases than in the former. Choked discs and optic neuritis are much more likely to occur in tumor than in the other affections.
Brain tumor must sometimes be diagnosticated from the head symptoms of some form of Bright's disease. A case not long since presented itself to one of us with a history of having suffered at frequent intervals for two years with headache of gradually increasing severity. Dimness of vision and slight temporary œdema of the feet, circumscribed and painful swellings along the lymphatics of the thighs and legs, with some mental irritability, were other marked symptoms. The patient had been attended by several physicians of prominence, one of whom had diagnosticated tumor of the brain. The violent, apparently agonizing headache, with the diminution of vision, and the absence of marked symptoms indicating other organic disease, made the diagnosis of a growth in some non-excitable region of the cerebrum most probable. Examination of the urine showed no albumen. Careful examination of the eye-ground with the ophthalmoscope, however, revealed the appearances of retinitis albuminurica. Under a treatment directed to the relief of chronic nephritis the patient's headache and other symptoms improved.
It must not be forgotten just here, however, that, on the one hand, ophthalmoscopic appearances very similar to those of albuminuric retinitis are sometimes present in rare cases of brain tumor, and also in other constitutional disorders, such as leukæmia; and, on the other hand, that, as stated by Norris,36 exceptional forms of albuminuric retinitis have been reported where the only change seen in the fundus oculi was pronounced choking of the disc.
36 Op. cit.
Intracranial tumors must be diagnosticated from meningitis in its various forms. In children tubercular meningitis sometimes closely simulates brain tumor. Tumors of the brain are comparatively rare in children, but, as has already been shown, gliomata and other tumors do sometimes occur in early life. The course of tubercular meningitis, whether in children or in adults, differs from that of brain tumor. It is more irregular in its method of advance, or if it shows the regularity which is sometimes present, and which has led authors to subdivide it into three more or less completely separable stages, the symptoms of these stages do not correspond with any closeness to those of the initial, middle, and terminal periods of brain tumor, as already given. Headache is usually present in both affections, although the absence of headache in some cases of gliomata in children must be here borne in [p. 1054] mind. When headache is present in tubercular meningitis, it is less likely to be localized, and, on the whole, it is not so severe as the terrible torture of the neoplasm. Irregular but very decided febrile phenomena are more likely to be present in meningitis than in tumor. Like brain tumor, tubercular meningitis of the convexity may give psychical disturbances, palsies, local spasms, general convulsions, sensory disturbances, peculiar disorders of the special senses, etc.; but these symptoms in the former usually come on more irregularly and are accompanied less frequently with paroxysmal exacerbations of headache, vomiting, vertigo, etc. Tubercular meningitis of the base can be more readily distinguished from cases of tumor by the fact that one cranial nerve after another is likely to become involved in the diffusing inflammatory process. Tubercular meningitis is of shorter duration than the majority of cases of brain tumor, and in it delirium and mental confusion come on more frequently and earlier. A history and physical evidences of more or less generalized tuberculosis favor the diagnosis of tubercular meningitis. In both affections the ophthalmoscope may reveal choked disc or descending neuritis. It will be seen that the differentiation between the affections is not always very clear, although in some cases the decision may be quickly reached from a study of the points here suggested.
Some of the forms of chronic hydrocephalus are difficult to distinguish from tumors, especially gliomata. In hydrocephalus, when not the result of, or not accompanied by, tubercular meningitis, the disease advances more slowly and with less irritative symptoms than in cases of tumor. Headache, vertigo, vomiting, and the other symptoms of meningeal irritation are not so frequently present, although the ophthalmoscopic appearances are often the same.
Rosenthal speaks of the necessity of diagnosticating brain tumor from the chronic cerebral softening of Durand-Fardel, from acquired cerebral atrophy, and the cerebral hypertrophy of children. An elementary knowledge of the general symptomatology of intracranial tumors will, however, be sufficient to prevent mistakes of differentiation in these cases. Neither of these affections presents the violent paroxysmal symptoms, the affections of the special senses, or the severe motor and sensory phenomena of intracranial growths.
Acute mania and paretic dementia are sometimes confounded with intracranial growths. A case of brain tumor is more likely to be regarded as one of acute mania than the reverse. In some comparatively rare instances in the course of their sufferings the cases of tumor become maniacal, but even a superficial study of general symptomatology in such a case will be sufficient to clear up the doubt.
Paretic dements are occasionally supposed to be cases of brain tumor, because of the epileptiform attacks and isolated pareses which occur as the disorder progresses. It is only necessary to refer to this matter, as the mistake would not be likely to be made by one having any familiarity with dementia paralytica.
L. J. Lautenbach, in a recent communication to the Philadelphia Neurological Society, which embodied a large number of ophthalmoscopic examinations of the insane at the State Insane Hospital, Norristown, Pennsylvania, and the Insane Department of the Philadelphia Hospital, and also the results of the investigations of the fundus of the eye in [p. 1055] cases of insanity by other observers, showed that about 16 per cent. of cases of acute mania presented well-defined papillitis—a condition which he described as one of swelling and suffusion of the disc, corresponding to cases reported as choked disc, descending neuritis, and severe congestion of the optic nerve. No reports of post-mortem examinations were made of these cases, but they did not present the clinical history of meningitis or brain tumor. It therefore follows that the existence of papillitis in a case of acute mania does not necessarily point to a gross lesion, such as tumor or meningitis.
In the early stage of posterior spinal sclerosis some of the symptoms of the initial or middle stage of intracranial growths in certain positions are likely to be present; more particularly, such eye symptoms as diplopia from deficiency or paresis of the ocular muscles and disorders of the bladder may mislead. In posterior spinal sclerosis, however, some at least of the pathognomonic symptoms of locomotor ataxia, such as lancinating pains, absent knee-jerk, or Argyle-Robertson pupil, will almost invariably be present. Those tumors of the cerebellum, pons, tubercular quadrigemina, etc. which give rise to ataxic manifestations are usually readily discriminated from posterior spinal sclerosis by the headache, vomiting, and other general symptoms of brain tumor, which rarely occur in ataxia. It is far more difficult to separate non-irritative lesions of certain cerebellar and adjoining regions from the spinal disorder.
Strange to say, one of the most frequent mistakes of diagnosis is that which arises from confounding brain tumor with grave hysteria. In several of our tabulated cases the patients at different periods of the disease and by various physicians had been set down as suffering from hysteria. One of Hughes-Bennett's cases (Case 30), a wayward, hysterical girl of neurotic family, had had her case diagnosticated as hysteria by one of the highest medical authorities of Europe, and yet after death a tumor the size of a hen's egg was found in the cerebrum. In a case reported by Eskridge (Case 76) hysterical excitement and special hysterical manifestations were of frequent occurrence, and misled her physicians for a time. Eskridge remarks, in the detailed report of this case, that to such a degree was the emotional faculty manifest that had no ocular lesion been present there would have been great danger of mistaking the case for one of pure hysteria; and, indeed, a careful physician of many years' experience, not knowing the condition of the eyes, pronounced the woman's condition to be pregnancy complicated by hysteria. A close study of such objective phenomena as choked discs and paralysis will usually be of the most value.
Even malaria has been confounded in diagnosis with brain tumor. Holt37 reports a case which presented the history of a fever, at first periodical, with marked splenic enlargement, great muscular soreness, and incomplete paralysis, which was diagnosticated to be chronic malarial poison. The patient for a time improved under quinine, but eventually grew worse, and on an autopsy a glioma-sarcoma was found on the inferior surface of the cerebellum. Several years since a physician about fifty years of age was brought to one of us for consultation, and in his case a similar mistake had been made. The case was a clear one of [p. 1056] tumor, probably cerebellar, with headache, neuritis, vertigo, and other general symptoms, which pointed to an organic lesion. This patient, who came from a malarial district in the West, had doctored himself, and had been treated by others with enormous doses of quinine and arsenic.
37 Med. Record, March 1, 1883.
LOCAL DIAGNOSIS.—Niemeyer would hardly say to-day that the brilliant diagnoses where the precise location of a tumor is fully confirmed by autopsy are not usually due to the acumen of the observer, but are cases of lucky diagnosis. It can be asserted with confidence that the exact situation of a tumor can be indicated during life in at least two or three locations. Great caution should be exercised, as insisted upon by Nothnagel,38 in the localization of tumors of the brain, because, among other reasons, of the frequent polypus-like extension of such tumors.
38 Wien. Med. Bl., 1, 1882.
The subject of local diagnosis can be approached in several ways, according to the method of subdividing the brain into regions. Thus, Rosenthal discusses, in the first place, tumors of the convexity of the brain, but as this is a very general term, covering portions of several lobes, we can see no advantage in making such a subdivision.
A few general remarks might be made in the first place, however, with regard to the general symptoms presented by surface or cortical growths as compared with those which are produced by deep-seated neoplasms. The direct or indirect involvement of the membranes in nearly all cortical tumors makes the symptoms of irritation referable to these envelopes very numerous and important.
The various centres so called, motor, sensory, and of the special senses, which have their highest differentiation in the cerebral cortex, are each and all represented by well-defined tracts of white matter in the centrum ovale and capsules which connect these centres with the lower brain, the spinal cord, and the periphery of the organism. It therefore follows that symptoms produced by localized lesions of the cortex will be reproduced in other cases by those of the tracts which go to or come from these centres. We may thus have a monoplegia or a hemiplegia, a partial anæsthesia or a hemianæsthesia, a hemianopsia, a word-blindness or word-deafness, a loss of power to perceive odors or to appreciate gustatory sensations, from a peculiarly limited tumor or other lesions of either the gray centres of the cortex or of the white matter of the central area of the brain; but these specialized symptoms are more likely to arise from cortical lesions in the case of intracranial neoplasms, because of the much greater frequency with which these adventitious products arise from membranes and therefore involve the cortex.
Peculiar symptoms arise in the case of lesions of the centrum ovale from the fact that it contains not only projection-fibres which more or less directly connect cerebral centres with the outer world; but also a system of commissural fibres which unite corresponding regions of the two cerebral hemispheres by way of the corpus callosum and commissures, and a system of association-fibres which connect different convolutions together, in special cases even those which are situated remotely from each other, but are associated in function.
It is evident, therefore, as asserted by Starr,39 that a peculiar set of additional symptoms will be referable to the destruction or irritation of these commissural and association fibres. For example, failure to [p. 1057] perform easily corresponding bilateral motions in face, hands, or feet would indicate some obstruction to conduction in the commissural fibres joining the motor convolutions. “Integrity of both occipital lobes, and simultaneous, connected, and harmonious action in both, are necessary to the perfect perception of the whole of any object when the eyes are fixed upon one point of that object.” Starr gives the following examples of the methods of detecting a lesion of such fibres: “In the case of the fibres associating the auditory with the motor speech-area the symptoms to be elicited seem to be very simple. Can the patient talk correctly? Can he repeat at once a word spoken to him? These are the questions which any one will ask who examines a case of aphasia. But this is not all. The patient must be further questioned. Can he read understandingly to himself, and tell what he has read? This will test the occipito-temporal tract. Can he read aloud? This will test the occipito-temporo-frontal tract. Can he write what he sees? This will test his occipito-central tract. Can he write what he hears? This will test the temporo-central tract. Can he write what he says, speaking to himself in a whisper? This will test his fronto-central tract. Can he name an odor or a color? Brill has recorded40 a case of lesion of the cuneus associated with color-blindness to green, and he states that the patient had difficulty in naming various colors on account of the presence of a slight degree of amnesic aphasia.... Can the patient write the name of an odor? Can he tell how a surface feels—smooth, or warm, or heavy? Such questions as these will suggest themselves at once to any one who studies the association of ideas subjectively.
“Take as an example a lesion in the centrum ovale of the occipito-temporal region. Such a lesion will produce hemianopsia, because it involves the visual tract of the projection system. It may also produce a peculiar mental condition known as word-blindness, in which the patient is no longer able to associate a word or letter seen with its corresponding sound or with the motion necessary to write it. Charcot has reported a case of this kind.... The man, who was a very intelligent merchant, was suddenly seized with right hemianopsia while playing billiards, and was surprised to find that he saw but one-half of the ball and of the table. Soon after he had occasion to write a letter, and after writing it was surprised to find that he could not read what he had just written. He found, however, that on tracing individual letters with the pen or fingers he became conscious of the letters—a few letters (r, s, t, x, y, z), however, being an exception to this rule. When a book was given him to read he would trace out the forms of the letters with some rapidity, and thus manage to make out the words. If his hands were put behind him and he was asked to read, he would still be observed to put his fingers in motion and trace the letters in the air. Speech was in no way interfered with, but reading aloud was only accomplished, like reading to himself, by the aid of muscular sense. Here, then, was an example of a lesion which had separated entirely the tract associating sight with speech—viz. the occipito-temporal tract—but had left intact the tract associating sight with muscular sense—viz. the occipito-central tract.”
39 Med. Record, vol. xxix. No. 7, Feb. 13, 1886.
40 Amer. Journ. of Neurology, Feb., 1883.
Our tabulated cases, although collected for the purpose of studying inductively the phenomena of intracranial tumors from all points of view, [p. 1058] have been arranged to indicate, so far as is possible, the special symptoms which are produced by growths in special localities. Thus we have made thirteen subdivisions:
I. Superior antero-frontal region (5 cases).—The lateral and median aspects of the hemisphere from the anterior tip backward to the posterior thirds of the first three frontal convolutions, the region roughly bounded by the coronal suture.
II. Inferior antero-frontal or orbital region (5 cases).—From the anterior tip of hemisphere at the base backward to the optic chiasm and Sylvian fissures.
III. Rolandic region or motor cortex (15 cases).—From antero-frontal region backward nearly to mid-parietal lobe, including posterior thirds of superior middle and inferior frontal convolutions, ascending frontal and ascending parietal convolutions, and anterior extremities of superior and inferior parietal convolutions—lateral and median aspects.
IV. Centrum ovale, fronto-parietal region (5 cases).
V. Postero-parietal region (5 cases).—From Rolandic region to parieto-occipital fissure, including posterior two-thirds of the superior and inferior parietal convolutions and the præcuneus.
VI. Occipital region (9 cases).—Occipital lobe—cortex and centrum ovale.
VII. Temporo-sphenoidal region (4 cases).—Temporo-sphenoidal lobe.
VIII. Basal ganglia and adjoining regions (19 cases).—Caudate nucleus, lenticular nucleus, optic thalamus, internal capsule, corpora quadrigemina, and ventricles except the fourth.
IX. Cerebellum (9 cases).
X. Floor of fourth ventricle (6 cases).—(Directly or indirectly involved.)
XI. Pons varolii and medulla oblongata (8 cases).
XII. Crura cerebri (3 cases).
XIII. Middle region of base of brain and floor of skull (7 cases).—In the main, from optic chiasm backward to pons, in the middle basilar region, in some instances extending beyond this area in special directions.
Tumors of the antero-frontal regions can be diagnosticated with considerable certainty, partly by a study of the actual symptoms observed and partly by a process of exclusion. Headache of the usual type, vertigo, choked discs, inflammatory and trophic affections of the eyes, widely varying body-temperature, and high head-temperature are among the most positive manifestations. Mental slowness and uncertainty seem to be greater in these cases than in others. Mental disturbance of a peculiar character unquestionably occurs in cases of tumor, as of other lesions, in this region. This disturbance is exhibited chiefly in some peculiarity of character, showing want of control or want of attention. The speech-defects present in a number of cases were rather due to the change in mental condition than to any involvement of speech-centres. Under Symptomatology has been given in some detail a study of the psychical condition in one case of antero-frontal tumor. The absence of true paralysis and of anæsthesia is characteristic. Nystagmus and spasm in the muscles of the neck and forearm were present in one instance, but usually marked spasm is not to be expected. Vomiting is less frequent than in tumors situated farther back. Facial and other forms of paresis occasionally are present, but are not marked, and are probably due to involvement [p. 1059] by pressure or destruction of surrounding tissue of neighboring motor areas. Hemianopsia, such as was observed in Case 10, showed involvement of the orbital region. Tumors of the inferior antero-frontal lobe give the same positive and negative characteristics as those of the superior frontal region, with the involvement in addition of smell and certain special ocular symptoms, such as hemianopsia.
Tumors of the motor zone of the cerebral cortex, the region surrounding and extending for some distance on each side of the fissure of Rolando, can be diagnosticated with great positiveness: 15 of the 100 cases are examples of tumors of this region, and in many of these the diagnosis of the location of the growth was accurately made during life. Localized spasm in peripheral muscles; localized peripheral paralysis; neuro-retinitis or choked discs; headache; pain elicited or increased by percussion of the head near the seat of the tumor; and elevated temperature of the head, particularly in the region corresponding to the position of the growth,—are the prominent indications. The spasmodic symptoms usually precede the paralysis in these cases. The spasm is often local, and generally begins in the same part in different attacks—in the fingers or toes or face of one side.
A study of cases of tumor localized to the cortical motor area will show that in almost any case a local twitching convulsion preceded the development of paresis or paralysis. Hughlings-Jackson41 reports a case of sarcoma, a hard osseous mass on the right side of the head, of eighteen years' standing, subjacent to which was a tumor the size of a small orange growing from the dura mater. The patient was a woman aged forty-nine, whose symptoms were very severe headache and double optic neuritis, with paresis in left leg, followed by slighter paresis in left arm and left face. A very slow, gradual hemiplegia came on by pressure on the cortex without any fit. Jackson says this is the only case which he has seen in which the hemiplegia has not followed a convulsion where the lesion has been on the surface. In all very slowly oncoming hemiplegias which he has seen, except this one, the tumor was in the motor tract.
41 Medical Times and Gazette, London, 1874, vol. i. 152.
As the white matter of the centrum ovale and capsules represents simply tracts connecting cerebral centres with lower levels of the nervous system, with each other, or with the opposite hemisphere, lesions of this portion of the cerebrum will closely resemble those cortical lesions to which the tracts are related. We have already referred to the peculiar symptoms referable to involvement of commissural and association fibres. Tumors of the centrum ovale of the fronto-parietal region, of which five examples are reported in the table, vary in symptomatology according to their exact location. Those situated in the white matter in close proximity to the ascending convolutions give symptoms closely resembling those which result from lesions of the adjoining cortical motor centres. In the cases of Osler, Seguin, and Pick (Cases 26, 27, 28, 29) spastic symptoms in the limbs of one side of the body, with or without loss of consciousness, were marked symptoms. In two of these cases some paresis preceded the occurrence of the spasms. They did not, however, fully bear out the idea of Jackson that the hemiparesis or hemiplegia in tumors of the motor tract comes on slowly before the appearance of spasm.
[p. 1060]Tumors of the postero-parietal region present some characteristic peculiarities. In several cases tumors were located in this region, and in several others the white matter of the parietal lobe was softened as the result of the obliteration of blood-vessels by the tumors. In general terms, we might say that hemianæsthesia, partial or complete, and impairment of sight and hearing on the side opposite to the lesions, seemed to be the most constant peculiarities.
Tumors and other lesions of the occipital lobes have in the last few years received extended attention, and, where possible, exact study, because of the opportunities which they furnish for corroborating the work of the experimental physiologists. It is unfortunate that the records of older cases do not furnish the exact detail which would render these tumors among the most important and interesting to be met with in the brain: some cases have, however, been observed with great care, and a few such are included in the table. To understand the special significance of the symptoms of such tumors, it will be well briefly to state some of the well-established facts about the function of the occipital cortex. The investigations of Gratiolet and Wernicke especially have proved that this surface of the brain is in direct connection with the fibres (1) which are continued upward from the posterior or sensory columns of the cord through the posterior portion of the internal capsule, and (2) with the expansion of the optic nerve, or the tract which passes, according to Wernicke, from the thalamus to the occipital lobe. There is but a partial decussation of the optic nerves at the chiasm, so that each half of the brain receives fibres from both eyes. This arrangement is best stated by Munk (quoted by Starr) as follows: “Each occipital lobe is in functional relation with both eyes in such a manner that corresponding halves of both retinal areas are projected upon the cortex of the lobe of the like-named side; e.g. destruction of the left lobe produces loss of function of the left halves of both retinæ.” This, of course, causes the right halves of both fields of vision to appear black. This condition is known as lateral homonymous hemianopsia, and was exhibited in several of the tabulated cases (Cases 40, 41, 42, and 43). It is probable that the dimness of the right eye recorded in Case 38 was really right lateral hemianopsia, as patients mistake this condition for blindness of that eye alone which is on the side upon which the visual fields are blank. It follows that this condition of the eyes will be caused by a destructive unilateral lesion at any point upon the optic tract behind the chiasm; and its exact nature and location are to be inferred from other corroborating symptoms. Among these corroborating symptoms, as will be inferred from the other functions of the occipital cortex, is especially to be considered partial hemiplegia and partial hemianæsthesia. This was observed in Cases 38, 40. These most characteristic localizing symptoms of occipital tumor have usually others, which, if not of such special importance, yet help to form a special complexus. Among these diffused headache is referred to by some writers as characteristic, but it seems to us that a localized headache, with pain on percussion over the affected region, is the only kind in this as in other regions which could have special diagnostic importance. Affections of hearing are recorded by some. It is not at all uncommon to have an incomplete hemiplegia and local paralysis. In Case 41 complete hemiplegia with facial paralysis is recorded. Local palsies, ocular and facial, [p. 1061] are recorded in Cases 36, 37, 38, and 39. It is doubtless by transmitted pressure, or by extension of the tumor, or the softening caused by it, toward the motor fibres, that these more or less incomplete paralyses are caused. The general symptoms, such as vertigo, vomiting, and convulsions, are frequently present with tumors of the occipital lobes. We are at a loss to know upon what data of theory or experience Rosenthal bases his statement that psychic disorders are more common in occipital tumors than in those of the anterior and middle lobes, unless he refers simply to the hebetude and late coma which seem to come generally in these cases.
Tumors of the temporo-sphenoidal region, so far as we have been able to study them, present few characteristic features. Physiology seems to point to the upper temporal convolutions as the cerebral centres for hearing; thus, according to Starr,42 “disturbances of hearing, either actual deafness in one ear or hallucinations of sound on one side (voices, music, etc.), may indicate disease in the first temporal convolution of the opposite side. Failure to recognize or remember spoken language is characteristic of disease in the first temporal convolution of the left side in right-handed persons, and of the right side in left-handed persons. Failure to recognize written or printed language has accompanied the disease of the angular gyrus at the junction of the temporal and occipital regions of the left side in three foreign and one American case.” In two of our four cases of tumor in the temporo-sphenoidal region disturbances of hearing were noted, but in none was the sense studied with sufficient care to throw any light upon the actual character of the disorder. The case of Allan McLane Hamilton (Case 47), already referred to under Symptomatology, was interesting because of the presence of a peculiar aura connected with the sense of smell. Stupidity, want of energy, drowsiness, and general mental failure were marked in tumors of this region.
42 American Med. Sci., N. S. vol. lxxxviii., July, 1884.
Tumors of the motor ganglia of the brain are seldom strictly localized to one or the other of these bodies. Growths occurring in this region usually involve one or more of the ganglia and adjacent tracts, and can only be localized by a process of careful exclusion, assisted perhaps by a few special symptoms. Paralysis or paresis on the side opposite to the lesion usually occurs in cases of tumor of either the caudate nucleus or lenticular nucleus; but whether this symptom is due to the destruction of the ganglia themselves, or to destruction of or pressure upon the adjoining capsule, has not yet been clearly determined. In a case of long-standing osteoma of the left corpus striatum (Case 49) the patient exhibited the appearance of an atrophic hemiplegia: his arm and leg, which had been contractured since childhood, were atrophied and shortened, marked bone-changes having occurred. Another case showed only paresis of the face of the opposite side. Clonic spasms were present in two cases, in one being chiefly confined to the upper extremities of the face. In this case paralysis was absent. Disturbances of intellect and speech have been observed in tumors of this region. According to Rosenthal, aphasic disturbances of speech must be due to lesions of those fibres which enter the lenticular nucleus from the cortex of the island of Reil.
Tumors of the optic thalamus usually cause anæsthesia or other [p. 1062] disturbances of sensation in the extremities of the opposite side. They sometimes show third-nerve palsies of the same side in association with hemiplegia on the opposite side, these symptoms being probably due to pressure owing to the proximity of the neighboring cerebral crus. Speech and gait in such tumors are also often affected.
Tumors of the corpora quadrigemina give rise to disturbances of sight and special ocular symptoms, such as difficulty in the lateral movement of the eyes. Spasms were usually present. Automatic repetition of words was observed in one case, nystagmus in another, and diminished sexual inclinations in a third. In other cases peculiar ataxic movements or a tendency to move backward were noted; other symptoms, such as spasm, vomiting, headache, were general phenomena of intracranial tumors; still others, such as hemiplegia, hemiparesis, or anæsthesia, were probably simply due to the position of the growth in the neighborhood of motor ganglia and tracts.
Tumors of the cerebellum have some special symptoms, which also derive importance from their characteristic grouping. The symptoms which depend upon the lesion in the organ must be distinguished from those which are caused by pressure upon adjacent parts, although these latter symptoms are very important as corroborative evidence of the location. Among the special symptoms is occipital headache (often not present), especially when the pain is increased by percussion about the occiput or by pressure upon the upper part of the neck. In these cases weakness of the gait (Case 75) and other motor phenomena, which are usually described as inco-ordination, are of comparatively frequent occurrence. They are not so much true inco-ordination as tremor of the limbs, rotation (which is usually only partial), and the so-called movements of manége. These movements were present in one-third of the cases collected by Leven and Oliver (quoted by Rosenthal). Staggering gait is also present, and may be dependent upon the vertigo, which is apt to be unusually intense in this kind of intracranial tumor (Cases 69 and 71). The symptoms caused by pressure of cerebellar tumors upon adjacent organs are of importance, because in conjunction with the special symptoms they acquire unusual significance. Sight and hearing are the two special senses apt to be affected, because of pressure upon the geniculate bodies and upon the auditory nerve or its nucleus. Descending optic neuritis, progressing to total blindness, and varied forms of oculo-motor paralysis may be present. Strabismus convergens has been said to be a symptom, caused by the paralysis of the sixth nerve. A hemiplegia and hemianæsthesia result sometimes from pressure upon the tracts in the pons or medulla. Continued pressure upon the medulla may eventually, toward the termination of the case, according to Rosenthal, cause disorders of the pulse and of respiration and deglutition. This author gives absence of psychical symptoms as negative evidence which counts for tumors of the cerebellum, but our table shows several instances (Cases 70, 71, 74, and 76) in which were present hebetude, incoherence, or hysteroidal symptoms. It is probable, however, that such symptoms are not as common and distinct as in tumors of the cerebrum.
Certain symptoms—or, better, groups of symptoms—characterize tumors of the pons varolii, and serve to render the local diagnosis comparatively certain. These depend upon the fact that the pons combines in itself, or [p. 1063] has on its immediate borders, nerve-tracts, both motor and sensory, in great complexity, from or to almost every special or general region of the body. Among these symptoms may especially be mentioned alternating and crossed hemiplegia, paralysis of eye-muscles (strabismus), paresis of tongue, dysphagia, anæsthesia (sometimes of the crossed type), and painful affections of the trigeminus. Vaso-motor disturbances have also been noted. In one case persistent and uncontrollable epistaxis hastened the fatal termination of the case.
Conjugate deviation of the eyes, with rotation of the head, as stated under Symptomatology, is a condition often present in tumors of the pons varolii as well as in the early stages of apoplectic attacks. A paper43 has been published by one of us on a case of tumor of the pons, and from it we will give some discussion of this subject.
43 Journal of Nervous and Mental Disease, July, 1881; Case 84 of Table.
Vulpian was probably the first to study thoroughly conjugate deviation. The sign, when associated with disease of the pons, was supposed by him and by others to be connected in some way with the rotatory manifestations exhibited by animals after certain injuries to the pons. Transverse section across the longitudinal fibres of the anterior portions of the pons produces, according to Schiff, deviation of the anterior limbs (as in section of a cerebral peduncle), with extreme flexion of the body in a horizontal plane toward the opposite side, and very imperfect movements of the posterior limbs on the other side. Rotation in a very small circle develops in consequence of this paralysis.44 The movements of partial rotation are caused, according to Schiff, by a partial lesion of the most posterior of the transverse fibres of the pons, which is followed in animals by rotation of the cervical vertebræ (with the lateral part of the head directed downward, the snout directed obliquely upward and to the side).
44 Rosenthal's Diseases of the Nervous System, vol. i. p. 125.
This deviation, both of head and eyes, occurs, however, not only from lesions of the pons and cerebellar peduncles, but also from disease or injury of various parts of the cerebrum—of the cortex, centrum ovale, ganglia, capsules, and cerebral peduncles. It is always a matter of interest, and sometimes of importance, with reference especially to prognosis, to determine what is the probable seat of lesion as indicated by the deviation and rotation.
Lockhart Clarke, Prevost, Brown-Séquard, and Bastian, among others, have devoted considerable attention to this subject. To Prevost we owe an interesting memoir. Bastian, in his work on Paralysis from Brain Disease, summarizes the subject up to the date of publication (1875). Ferrier, Priestly Smith, and Hughlings-Jackson have investigated the relations which cortical lesions bear to the deviation of the eyes and head.
It has been pointed out by several of the observers alluded to that when the lesion is of the cerebrum the deviation is usually toward the side of the brain affected, and therefore away from the side of the body which is paralyzed. In a case of ordinary left hemiplegia it is toward the right; in one of right hemiplegia, toward the left. In several cases of limited disease of the pons, however, it has been observed that the deviation has been away from the side of the lesion. In our case (Case 84) the conjugate deviation was to the right, while the tumor was entirely [p. 1064] to the left of the median line, thus carrying out what appears to be the usual rule with reference to lesions of the pons.
During the life of the patient it was a question whether the case was not one of oculo-motor monoplegia or monospasm from lesion of cortical centres. It is probable, as Hughlings-Jackson believes, that ocular and indeed all other movements are in some way represented in the cerebral convolutions. In the British Medical Journal for June 2, 1877, Jackson discusses the subject of disorders of ocular movements from disease of nerve-centres. The right corpus striatum is damaged, left hemiplegia results, and the eyes and head often turn to the right for some hours or days. The healthy nervous arrangement for this lateral movement has been likened by Foville to the arrangement of reins for driving two horses. What occurs in lateral deviation is analogous to dropping one rein; the other pulls the heads of both horses to one side. The lateral deviation shows, according to Jackson, that after the nerve-fibres of the ocular nerve-trunks have entered the central nervous system they are probably redistributed into several centres. The nerve-fibres of the ocular muscles are rearranged in each cerebral hemisphere in complete ways for particular movements of both eyeballs. There is no such thing as paralysis of the muscles supplied by the third nerve or sixth nerve from disease above the crus cerebri, but the movement for turning the two eyes is represented still higher than the corpus striatum.
It would seem a plausible theory that we have in this conjugate deviation of the eyes and head a distinct motor analogue to the hemianopsia which results from certain lesions high in the optic tracts. The fact that we never have a distinct oculo-motor monoplegia from high lesions, but always a lateral deviation of both eyes in the same direction, suggests that only a partial decussation of the fibres of the motor nerves of the eyes occurs, and that each hemisphere does not control the whole motor apparatus of the opposite eye, but half of this apparatus in each eye.
Alternating hemiplegia, or paralysis of one side of the body followed by a paralysis of the other side, is observed in tumors of the pons, and is readily accounted for by the close proximity of the motor tracts, a lesion which affects one tract first being very likely, sooner or later, to involve, partially at least, the other, as in Case 84. Cross-paralysis of the face and body may be seen, and like crossed anæsthesia (seen also in Case 84) depends upon the fact that both motor and sensory fibres to the limbs do not decussate at the same level as these fibres to the face. Trigeminal neuralgia, from involvement of the nerve by pressure or otherwise, is recorded in this characteristic group of symptoms. The association of the general with the local paralytic symptoms in the manner stated, the involvement of sensory functions, and the deviation of the eyes and head serve to distinguish tumors of the pons from cortical or high cerebral local lesions. Cases 81, 84, 89, and 90 illustrate these facts in various ways. Case 82, involving the floor of the fourth ventricle, appears to be an exception, as the deviation is toward the side of the lesion.
The special localizing symptoms which indicate a tumor of the crus cerebri are paralysis of the oculo-motor nerve upon the same side as the tumor, and especially the tendency of this paralysis to pass to [p. 1065] the other side later in the case; disturbance of the innervation of the bladder; and involvement of the vaso-motor functions. In considering these symptoms in detail it becomes very evident why we have the alternating paralysis of the two oculo-motor nerves. As this trunk arises from the crus, it is in direct risk of injury by the neoplasm, and the extension of the new growth even slightly must later in the case involve its fellow. Therefore a ptosis, followed by a similar symptom on the other side, or other third-nerve symptoms passing from one side to the other, with other characteristic and corroborating symptoms, furnish strong evidence of this lesion, as in Case 93. Rosenthal refers especially to involvement of the bladder, as difficulty of micturition, but the three cases in the table do not present such a symptom. He says that experiments prove that irritation of the peduncle is followed by contraction of the bladder, and that it has been shown that lesions of the crus abolish the influence of the will upon micturition. As this occurs at all levels of the cord, its occurrence with lesions of the crus is not to be considered a very distinctive symptom. The involvement of the vaso-motor functions is one of much interest. Its occurrence is not recorded in the cases of tumors of the crus included in the table, but in Case 94 of twin tumors in front of the optic chiasm it is recorded that profuse perspiration occurred. We believe that the centres for the vaso-motors are not well determined: they seem to be affected by various lesions, especially about the base of the brain. Among other corroborating symptoms may be mentioned rotatory movements and deviation of the head: these rotatory movements are probably caused by the action of the sound side not antagonized by the muscles of the paralyzed side. Lateral deviation of the head is referred to by some. Partial or complete hemiplegia, with facial paralysis on the side opposite to the lesion, may occur; whereas the oculo-motor palsy is seen on the same side as the lesion. Diminution of sensibility happens on the opposite side, or occasionally pain in the legs, as recorded in Case 92. It is of interest to note, with Rosenthal, that the reactions of degeneration are not likely to appear in the facial muscles in this lesion, as it occurs above the nucleus of that nerve, and thus causes a true centric paralysis. The absence of psychic symptoms is usually to be noted.
Tumors anywhere in the middle portion of the base of the brain and floor of the skull, the region of the origin of the various cranial nerves, can of course be diagnosticated with comparative ease by a study of the various forms of paralysis and spasms in the distribution of these nerves, in connection with other special and general symptoms. Varieties of alternate hemiplegia are to be looked for, and also isolated or associated palsies of the oculo-motor, pathetic, facial, trigeminal, and other cranial nerves. In studying these palsies it must be borne in mind that although the lesions producing them are intracranial, the paralyses themselves are peripheral.
In most cases apparent exceptions to the ordinary rules as to localization are capable of easy explanation; thus, for instance, in a case of tumor of the occipital lobe (Case 44) numbness and pain were present in the right arm, although the tumor was situated in the right hemisphere. The tumor was of considerable size, and may have affected by pressure the adjoining sensory tracts.
[p. 1066]Hughlings-Jackson45 reports a case of tubercular tumor, half the size of a filbert, in the pons under the floor of the fourth ventricle, in the upper third of the left side. A much smaller nodule was found in the right half of the pons. This patient, a man thirty-three years old, had inconstant headache, a gradual incomplete hemiplegia of the right side, with also paresis of the left masseter and right lower face. Sensation was diminished in the right arm, leg, and trunk. The optic discs were normal; the left pupil was smaller than the right. There was lateral deviation of the eyes to the right. Diplopia was present in some positions, and one image was always above the other. Aphasic symptoms were also present. Especial interest attaches to the fact that the facial paralysis in this case was on the same side as the hemiplegia, opposite that of the lesion; whereas usually in lesions of the pons facial paralysis is on the side opposite the hemiplegia. This is explained by the fact that the tracts of the facial nerve decussate in the pons below its upper third, and therefore in this case the lesion caught the nerve-tracts above their decussation.
45 Med. Times and Gazette, London, 1874, p. 6.
PROGNOSIS.—The prognosis in intracranial tumors is of course usually in the highest degree unfavorable. The early recognition of the existence of a tumor syphilitic in origin will enable a comparatively favorable prognosis to be made. It is far from correct, however, to suppose that all or a majority of the cases of known syphilitic origin are likely to have a favorable termination. Amidon46 puts this matter very correctly as follows: “Has a destructive lesion occurred? and if so, where is it located, and what is its extent? Indications of a destructive lesion should lead one to a cautious prognosis as regards perfect recovery, while the prognosis for life and a moderate amount of health may be good. A gummy intracranial or spinal growth, giving rise to alarming symptoms, may vanish as by magic upon prompt treatment. The symptoms of these frank, specific growths are, as a general thing, characteristic and widely different from those of the more insidious destructive lesions.
“An intracranial gumma often heralds itself by sharp, localized headache, gradually deepening paralysis, aphasia, epilepsy, and optic neuritis, while destructive lesions are more apt to have diffuse, dull headache, stationary or lessening paralysis or aphasia, rarely epilepsy or optic neuritis. Intraspinal gummata give rise to a painful paraplegia, while an inflammatory or destructive change gives rise to various and atypical sensory and motor manifestations.
“As to the pathology of these cases, I can say but little, as such discussion opens the whole subject of the pathology of syphilis. This I will say, that, so far as can be told without autopsies, no permanent pathological condition was present in these cases which might not have been brought about by other etiological factors which were often present. The periencephalitis might be caused by alcohol, mental strain, or excesses; the arterial occlusion might be due to previous disease not specific.”
46 Medical News, vol. xlviii. No. 3, Jan. 16, 1886, p. 64.
TREATMENT.—The surgical treatment of tumors of the brain has recently received a great stimulus from the report of a case which [p. 1067] occurred in the practice of A. Hughes-Bennett of London, and which was operated on by Rickman J. Godlee. The case has been included in the table (Case 24), where the symptoms and details of treatment may be read. This case has served to bring into sharp outline many of the difficulties and dangers of such an operation on the one hand, and the few possible and exceptional advantages of it on the other. It must be apparent, in the present state of knowledge and with the additional light of this interesting case, that success must largely depend upon the following conditions: The tumor must be exceptionally localized—i.e. not very large—and non-multiple; it must be cortical, or at least not very deep-seated; it is also quite essential that it be in the motor zone, in order to admit of accurate diagnosis. It would seriously impair the usefulness of the operation and the prognosis if the case were of long standing with much necrosis of brain-tissue, or if the growth were malignant and recurring. The secondary complications, as inflammation and sepsis, are of course possible in all surgical cases, and may be guarded against, as well in cerebral as in other surgery. If such a criticism narrows the field for the operation into almost hopeless limits, it may be reflected that one or two successful cases are better than a hundred experimental failures; that cases do occur in which the tumor is just so localized, single, and superficial; that the urgency of distressing symptoms, as pain and convulsions, urge the operation for palliation as well as cure; and that these cases, without relief, are necessarily fatal, and hence justify large risks.
By exclusion and a careful study of the symptoms we believe it may become possible hereafter in some cases to localize in two other accessible regions brain tumors with sufficient accuracy for purposes of operation: these are the antero-frontal region and the postero-parietal region.
The case of Bennett and Godlee was a most successful test of diagnosis, and as a surgical endeavor might have been more successful, as the operator himself suggests, if more careful antiseptic precautions had been used. In the discussion of this case before the Royal Medical and Chirurgical Society47 it was stated by Hughlings-Jackson that three indications were of special importance for this diagnosis: (1) local persisting paralysis; (2) epileptiform convulsions, those beginning locally; (3) double optic neuritis, which is diagnostic of tumor as distinguished from a sclerotic patch. It is probable that permanent palsy would be left after a successful operation in which the cortical tissue were destroyed, but as this is compatible with life and comfort, it is not likely that, as an alternative, it would be rejected by the patient. McEwen's case, also given in the table (Case 25), is not as accurately reported48 as Bennett's, but was partially successful. At the opening over the Rolandic region false membrane was removed, and an incision made which let out grumous red-colored fluid: this was followed by a decrease in the paralysis and improvement in other brain symptoms. It is difficult to understand why the opening was made in the occipital region. The necessity for antiseptic measures is to be especially considered in cerebral surgery. In a recent operation for a case of traumatic epilepsy, under the care of Mills and White, in the Philadelphia Hospital, in which quite extensive injury was done to the membranes in removing fragments of bone, rigid [p. 1068] antisepsis was employed; and it is not too much to assume that the risks of the operation were much diminished by it and its success ensured in an old and crowded hospital building.
47 Brit. Med. Journ., May 16, 1885, p. 988.
48 Glasg. Med. Journ., xxi., 1884, p. 142.
In the medication of tumors of the brain we can unfortunately do but little more than treat the symptoms and ameliorate the various conditions as they arise. There is no specific for these growths, unless the syphilomata be an exception; and experience shows that specific treatment is usually disappointing even when applied to a syphilitic brain tumor. The dietetic and hygienic rules laid down by some are only such as are invariably recommended as routine practice in all kinds of disease; and it almost seems a mockery to offer them to a patient with an intracranial tumor with the same gravity and detail as we suggest them in a curable fever or a hopeful surgical case. It is possible that local depletion and revulsives, by controlling irritation and hyperæmia, may be beneficial, though we should hesitate to add to the sorrows of the patient the action of tartarized antimony, even, with Obernier, in special cases. Hot or cold effusions and the ether spray are worthy of mention. Local applications of the galvanic current might be tried for its catalytic action, but the observations are too few and the theory too inapplicable to allow us to attach much importance to the suggestion. The use of electricity to the limbs for paralytic symptoms certainly does not promise much in the case of an obstinate neoplasm in the brain.
Morphia and bromide of potassium are the two drugs which offer the most promise in these fatal cases. They can often control the most urgent and frightful symptoms. The headache, the obstinate vomiting, the epileptic seizures, are all more or less amenable to one or other of these remedies or a combination of them. Although the vomiting is of centric origin, it is possible that remedies addressed to the stomach might occasionally afford relief, just as we apply medicines to that viscus in reflex irritation, in pregnancy, and in debilitating diseases. The remedies which suggest themselves are the salts of bismuth and cerium, the more stimulating wines, as champagne, in small frequent doses, and cracked ice.
While morphia and bromide of potassium are, on the whole, the most useful remedies for the relief of pain and irritating symptoms of brain tumor, other remedies can often be used with great advantage as adjuvants. Ergot in the form of the solid or fluid extract has a beneficial influence in relieving the congestive symptoms. Cannabis indica in the form of the fluid extract in doses of five to ten minims, or the tincture in doses of fifteen to thirty minims, may be advantageously combined with morphia and a bromide, or sometimes may be tried alone. Hyoscyamus, either the fluid extract or tincture, in somewhat larger doses may also be tried. The great severity of the headache and the imperative demand, however, will usually compel the physician to fall back at last upon morphia in large dose by the mouth or hypodermically.
Leeches to the temples or behind the ears or to the mucous membrane of the nose, either wet or dry cupping to the back of the neck, and bladders or compresses of ice, or very hot water, may be used to the head.
The various serious complications which so often accompany intracranial tumors should be most carefully managed. Among the most important of these are such affections as the conjunctivitis and trophic [p. 1069] corneitis, with anæsthesia, present in a few cases, usually when the trigeminal is directly or indirectly involved. Cystitis and pyelitis must be appropriately treated, and patients must be carefully watched in order to prevent injurious consequences of over-distension of the bladder or enormous fecal accumulations.
| No. | Sex and Age. | Clinical History. | Pathology and Location. | Remarks. |
| Superior Antero-frontal Region. | ||||
| 1 | M. 35. | Syphilis and traumatism. Headache; vertigo; mental slowness; loss of attention; hysterical. Nystagmus. Tonic spasm of neck and forearm. Movements weak and uncertain. Explosive speech. Gradual blindness; choked discs. Conjunctivitis and corneitis of left eye. Anæsthesia of conjunctiva. Polyphagia. Constipation alternating with involuntary evacuations and urination. Temperature 97°-101°. Head-temperature above normal; highest at frontal station; average, 96.5. |
Fibroma. Anterior superior half of second frontal and anterior superior and inner half of first frontal; anterior segment of gyrus fornicatus, and anterior half inch of corp. callosum. |
C. K. Mills, Philada. Med. Times, Jan. 18, 1879 and Arch. of Med., vol. viii. No. 1, Aug., 1882. |
| 2 | M. 50. | Headache, dizziness, and slight right facial paralysis. Dimness of vision. Day before death had an attack of unconsciousness, from which he emerged in half an hour. In two hours had another attack; became comatose; Cheyne-Stokes respiration; temperature 102.3°; pulse 150. Reflexes completely abolished. | Fibroma. One and a half inches in diameter in the left antero-frontal lobe, located so as to involve the middle portions of the first and second frontal convolutions and white substance beneath them almost to the orbital surfaces. White matter softened posterior to tumor. Adherent to pia mater. |
C. K. Mills. Not before published. |
| 3 | M. 16. | Frontal headache, vertigo, staggering gait toward right. Later, paresis of sphincter of bladder. Some muscles of right face paretic. Some weakness of mind: emotional. Choreic movements of right arm, increased with mental excitement. No deafness, loss of taste, or of tactile or heat sense. Slight traces of sugar. Blurring of papilla and hyperæmia of retina. Later, vomiting. Urine sp. gr. 1031. Irritability of mind, with erotic conduct. Reduction of pulse—54. Progressive emaciation and mental failure. Tremor in both arms, and in right arm automatic movement. Boil on left hand. Scaphoid abdomen. Later, temperature below normal; also pulse and respiration. Right facial paralysis unchanged. Still later, contracture of both elbows. Pupils react tardily. Apathetic. Very late, small quantity albumen, no sugar. | Glioma. Frontal convolutions flattened; brain-substance doughy; cortex gray-red; medullary substance reddish-white. Corpus callosum arched upward; lateral ventricles enlarged in posterior horns. Tumor in medullary substance of both frontal lobes, springing from septum and radiating toward parietal lobes, almost filling both anterior lobes, and also adhering to walls (apparently) of ventricles. At base extended backward full extent of frontal lobe. |
Petrina. Vierteljahrschr. f. die Prakt. Heilk., 1 Bd., 1877, p. 126. |
| 4 | M. 36. | History of injury to the head. Frontal and occipital headache. Vomiting and giddiness. Memory much affected. Double internal strabismus with unequal pupils. Double optic neuritis. Hearing unaffected; sense of smell lost. Lies on back. Stumbles on trying to walk. Answers questions with difficulty; speech slow and hesitating. Pain in head, apparently increased by percussion to right frontal region. | Endothelioma. In right frontal lobe anterior portion. Three inches in diameter. Surrounded by soft diffluent cerebral tissue. Right frontal bone had on its internal surface a much greater concavity than the left, and at its upper and outer part was rough, deeper in color, and thin. Dura mater adherent. |
Philipson, Medical Times and Gazette, vol. ii., for 1882, Sept. 16, 1882, p. 355. |
| 5 | F. 32. | History of chancre with secondary and tertiary [p. 1070] lesions of syphilis. Frontal node. Constant headache. Epileptiform convulsions. Marked exophthalmus, with impairment of sight in both eyes. Improved under iodide of potassium. Grew worse again. Dimness of vision; pain in head constant, and worse at night. Ophthalmoscope revealed neuro-retinitis with commencing atrophy of optic nerves. | Gumma. From dura mater into the brain-substance at the anterior portion of the anterior lobe of the left hemisphere. Brain-substance softened around tumor. Left ventricle dilated, and filled with fluid. |
H. Knapp, Arch. of Ophthalmology and Otology, vol. iv. p. 245. |
| Inferior Antero-frontal or Orbital Region. | ||||
| 6 | M. 27. | Loss of sight, increasing to total blindness. Gradually increasing loss of hearing, of smell, and of taste, in order named. No anæsthesia. No paralysis mentioned. | Fibro-sarcoma. Involving inferior portion of right anterior lobe. The first and second pair of nerves were involved, but no other nerves. |
L. Howe, Buffalo Med. and Surg. Journ., xxi. p. 299. |
| 7 | F. 33. | Paralysis and wasting of right leg since childhood. Sudden severe general convulsions with loss of consciousness, followed by paresis of right upper extremity. No facial or ocular paralysis. Special and general sensibility normal. Recurrent convulsions, both tonic and clonic. Severe frontal headache; continued paresis of right arm. Apathetic. Right face partially paretic, and right oculo-motor weakened. | Cholesteatoma. Growing from pia mater at the base between both frontal lobes, extending to anterior margin of corpus callosum and to optic chiasm. |
Petrina, op. cit., p. 126. |
| 8 | F. 20. | Vomiting. Loss of sight and hearing; inability to speak. Somnolence. Pupils widely dilated. Later, all special senses involved. Tongue protrudes to right. Pulse irregular. Right face anæsthetic. Neuro-retinitis in both eyes, worse in right; left eye retained some vision. Hearing and taste perfect; smell impaired. No paralysis. Pain constant over eyes. No convulsions. | Under left anterior lobe and extending from falx cerebri, to which it was adherent, over the cribriform plate of the ethmoid, involving left olfactory nerve, backward and diagonally across the sella turcica to right petrous bone, where the end of it pressed on fifth nerve of right side at its point of exit. Pressed upon optic chiasm. | E. Williams, Med. Record, 1868, pp. 29-31. |
| 9 | M. 49. | Vertigo. Always excessively stupid, allowing himself to be made a fool of. Violent bleeding from the mouth and nose ten years before death, followed by nasal discharge. Frontal headache, especially on left side. Failure of sight. Small tumor in inner upper angle of left orbit, which dislocates left eye outward; right eye also deviated outward without any apparent mechanical reason. Pupils dilated and sluggish. Sight much diminished. Mouth slightly drawn to one side. Speech slow, but not hesitating. Gave replies to questions slowly, and did not usually keep to the point, but clothed his answers in general remarks. A certain amount of self-esteem pervaded his conversation. Continuous headache. Very late, had convulsions which began on the left side and extended to the right. | Tumor the size of a large walnut to the right of the middle line, external to the dura mater at a point corresponding to position of right olfactory bulb. Vitreous table of the frontal bone and crista galli of the ethmoid completely destroyed. On the inner side of dura mater another tumor fills the right anterior fossa and a large portion of the left. | Obernier, Virch. Arch., vol. xxxvi. p. 155, and Ziemssen's Cycl. Pract. of Medicine, Am. ed., vol. xii. p. 268. |
| 10 | M. —. | Diminution of vision. At first much reduced, without
any ophthalmoscopic changes. Slight headache; loss of appetite;
restless sleep; rapid pulse. Vision sank rapidly until completely
extinguished. Remained thus for nineteen days; then sight began to
return, first in the right eye, and then in the left. Increased, so
that an examination of the eccentric fields could be undertaken; this
showed absence of the external halves of the fields of
[p. 1071]
vision—hemianopsia. “The transition of the existing portions of the
fields of vision to the lost portions was effected by a region which,
by a low light, should be reckoned to the latter, so that then the
boundary-line of the defect fell somewhat to the outside of the
fixation-point running in the right eye in a vertical direction, and
in the left diagonally from the inside and above downward and outward.
Within the next four weeks the central vision increased in the right
to V = 1/2, and in the left to
V = 1/20, while the defect in the
eccentric vision continued in the way described.” Patient died of symptoms of acute meningitis. |
Sarcomata. Two tumors: one about the size of a pigeon's egg between the optic trunks in front of the chiasm, surrounded by the optic nerve in a forked manner, the nerve-fibres being parted by it. A second tumor situated beneath the pons, raising the dura mater. It had probably originated in cavernous sinus. |
Saemisch, Klin. Monatsblätter, 1865, p. 51, quoted by Obernier, Ziemssen's Cycl. of the Pract. of Medicine, Am. tr., vol. xii. p. 269. |
| Rolandic Region—Motor Cortex. | ||||
| 11 | F. 38. | History of syphilis. Blows on the head. Headache, with agonizing paroxysms. Top and right side of head sensitive to percussion and headache severest in these regions. Vomiting; vertigo. Great mental irritability. Severe left-sided spasms, beginning with twitchings in left toes and foot. Partial paralysis of right leg and arm, most marked in leg. Hyperæsthesia. Impaired sight. Choked discs. Head-temperature taken once: right parietal region, 97.2° F.; left parietal region, 96° F. | Gumma. Attached to the fused membranes of the right convexity. Involved the upper fourth of the ascending frontal and a smaller segment of the ascending parietal convolution, crossing Rolandic fissure at its upper extremity. A good example of strictly cortical lesion. |
C. K. Mills, Arch. Med., vol. viii. No. 1, August, 1882. |
| 12 | F. 30. | No history of causation. Headache continuous, sometimes agonizing. Percussion of head caused most pain in right parietal region. Vomiting when headache was most severe. Vertigo. Mind clear, but acted slowly: emotional. Spasm, beginning with twitching of fingers of left hand: most severe on left side, and especially in left arm. Upper as well as lower fibres of left facial nerve partially paralyzed; nearly complete paralysis of left arm; slight paralysis of left leg. Bowels and bladder partially paralyzed. Impaired sensibility in limbs of left side. Left patellar reflex diminished. Sight very imperfect. Choked discs. Hearing defective in right ear. | Carcinoma. The tumor involved the middle portion of the ascending parietal convolution and the upper part of the inferior parietal lobule, pushing aside the interparietal fissure. The anterior extremity of the tumor was about one-fifth of an inch back of the centre of the fissure of Rolando. On the inner side of the tumor the white matter of the brain was broken down. Adherent to the pia mater; the pia and dura mater were united by strong adhesions. |
C. K. Mills, reported at the meeting of the American Neurological Association, June, 1881, Arch. Med., vol. viii. No. 1, Aug., 1882. |
| 13 | M. 31. | Evidences of tuberculosis. Headache continuous, with severe exacerbations; most severe at vertex. Vertigo. Some irritability and emotionality; hallucination that some one was going to come and take him away. Spasm confined to left arm. Partial paralysis of left arm and leg, and, late in his illness, of left side of face. Left hemianæsthesia, at first partial, but later complete and persistent. Sight impaired; right pupil dilated and left contracted before death. No ophthalmoscopic examination. Hearing defective in left ear; tinnitus aurium. Head-temperature taken once: right frontal region, 98° F.; left frontal region, 96.3° F. Cheyne-Stokes breathing on day of death. | Tubercular tumor. Dura and pia mater adherent over the tumor, which involved the posterior extremities of first and second frontal and upper thirds of both ascending convolutions of right hemisphere. Interior of hemisphere broken down; the parts destroyed included white matter of the parietal lobe, the posterior third of lenticular nucleus, and the adjacent portion of internal capsule. Miliary tubercles in pia mater around and near the tumor. |
C. K. Mills, Arch. Med., vol. viii. No. 1, Aug., 1882. |
| 14 | M. 19. | First symptom, headache; then vertigo. Sudden right [p. 1072] brachial monoplegia; possibly some paresis of leg. Recovered use of arm; went to work; was kicked by a mule, and became worse. Headache and right-sided paresis returned. Increasing stupor; paralysis of right arm complete; of leg almost; right facial paresis; ptosis of right side. Partial anæsthesia on right side of face; pain on right side. Slight clonic spasms of right arm. Paralysis of bowels and bladder in last week. Tendency to Cheyne-Stokes respiration. No vomiting. Eyes not examined. | Gumma. A large tumor in the ascending frontal convolution, at junction of middle and upper thirds: one-third of mass on convexity of convolution, the remainder in fissure of Rolando. Smaller tumor at inferior angle of right lobe of cerebellum. Some basal meningitis with effusion. |
C. K. Mills, Med. and Surg. Rep., vol. li., Aug. 2, 1884, p. 119. |
| 15 | M. 56. | Sickness began with an epileptiform seizure lasting about ten minutes; flexing movements of right arm. Next day dragged his right leg slightly. Partial convulsions, without loss of consciousness, followed, and became very frequent. Two months before death convulsions ceased, but absolute paralysis of the arm and paresis of the leg remained. One month later complete palsy of right half of face occurred. Mind became impaired. Complete aphasia. Right-sided anæsthesia. Reflexes of right foot less marked than those of the left. Rectal temperature, 100.4° F. At times deviation of the head and eyes to the left. Left frontal and temporal regions tender to pressure. Very late nystagmus. No headache. | Glioma. In the left ascending frontal convolution, occupying the upper third of this convolution. The tumor extended backward to the fissure of Rolando, and in front was bounded by a vertical line which would meet the upper extremity of the vertical frontal fissure. The inferior boundary was distant about one and three-quarter inches from the longitudinal fissure. Surrounding convolutions flattened and widened. |
Samt, Arch. gén. de Méd., Jan., 1876, from Berlin. klin. Wochenschr., Nos. 40, 87. |
| 16 | M. 49. | Irritability and loss of memory. Paresis, passing to paralysis, of left arm; paresis of left leg. Slight left-sided paralysis of tongue. No facial paralysis; no optic neuritis. Ankle-clonus and exaggerated knee-jerk on left side. No wasting of muscles or abnormal electrical reactions. Toward end paroxysmal twitchings of left side, including side of face, with left-sided paresis of face. Hebetude. Visual hallucinations. Complete left hemiplegia. Paralysis of sphincter. Vomiting. Strong contraction of pupils. Duration about two months. | Glioma. Involving the middle portion of the right ascending frontal convolution and posterior end of middle frontal convolution, extending as a spheroidal mass downward to roof of lateral ventricle. |
A. Hughes Bennett, Brain, vol. v., 1882, p. 550. |
| 17 | M. 30. | Convulsions for twelve years prior to death. Character of fit: first, cramping of right big toe, then twitching of calf-muscles and drawing up of leg and knee. Most of the fits stop here, without loss of consciousness. In some fits the arm is convulsed after the leg, beginning in fingers, and consciousness is lost. Paralysis of right leg. Slight convulsive action of left leg. Sensation of right leg unimpaired. Temporary aphasia at beginning of attack; on one occasion the aphasia was present without fit. The right arm probably paretic after each seizure. No facial palsy. Has as many as thirty fits daily. Marked cessation of seizures at one time. Three days before death became hemiplegic, with exaggerated deep reflexes on paralyzed side; also ankle-clonus. During later years fit sometimes began in hand. No optic neuritis while under observation. | Glioma. Left hemisphere, including posterior half of superior frontal convolution and upper half of ascending frontal convolution, except the extreme end. The superficial area was defined by fissure of Rolando posteriorly, superior frontal fissure externally, and longitudinal fissure internally. Anteriorly, the tumor gradually merged into normal brain. In the longitudinal fissure the growth extended to calloso-marginal fissure. |
J. Hughlings-Jackson, Brain, vol. v., 1882, p. 364. |
| 18 | F. 58. | General headache, most marked in the occipital region, and always worse at night. Sore, stiff feeling in neck; at times nausea and vomiting. Trembling [p. 1073] of left hand; later, paresis. Two sorts of movements of left arm—one, a fine tremor; the other, attacks of jerking. Paresis of left arm increasing, with some contracture; slight paresis of left leg. Sight failing; later, semi-stupor; pupils small and fixed, the right larger. Right internal rectus weak. Left lower face paretic. Strong contractures of left arm and hand. Good knee-jerk. Choked discs. Some days bright, others almost moribund. Case advanced to complete paralysis of left arm and leg; involuntary evacuations; divergent strabismus and ptosis; indistinct speech; delirium and coma. | Alveolar carcinoma. An ovoid tumor in the upper part of the ascending frontal convolution and in its subjacent white matter. It extended well across the fissure of Rolando. |
E. C. Seguin, Opera Minora, p. 495, and Journal of Nervous and Mental Disease, vol. viii. No. 3, July, 1881. |
| 19 | M. 50. | History of syphilis and severe fall on the head. Vertigo. Prickling sensation in left foot, extending to thigh, finally to arm and head, followed by unconsciousness and convulsion. Stupor after convulsion. After this, convulsive attacks at intervals. Eighteen months before death an apoplectic attack, in which was unconscious for several hours. Spasmodic attacks, preceded by a peculiar twisting of the fingers of the left hand. Paresis of the right hand and arm. Some diminution of sensation, not well made out. Slight want of use of the left leg. | Gumma. One-third of an inch in thickness at the middle of the ascending frontal convolution. Membranes fused; tumor adherent to them. Œdema of the brain. Gumma in the lungs. |
H. C. Wood, “Proceedings of the Philada. Neurological Society,” Medical News, vol. xlviii. No. 9, Feb. 27, 1886, p. 248. |
| 20 | M. 59. | Gradual loss of speech—aphasia. Gradual paralysis of right side. No headache prior to this. No anæsthesia. Taste, smell, hearing, and sight intact. Apathetic face. Middle branch of facial nerve paralyzed, especially the muscles of the right corner of the mouth. Wrinkles of forehead less strongly marked. Right upper and right lower extremity in strong contracture. Leg swollen. Increasing torpor of bladder. Normal electrical reactions, except speedier and increased reaction of the right facial nerve. Reactions of convulsibility in the right arm with ten to twenty cells. Very late, unconsciousness and paralysis of bowels and bladder. | Myxo-glioma. In front of the left ascending frontal convolution, bounded below by the Sylvian fissure and the upper convolution of the island of Reil; seems to immediately enter into the structure of the island. Left optic thalamus and corpus striatum moist, but completely separated from the tumor. Convolutions flattened. |
Petrina, op. cit. |
| 21 | M. 35. | Had epileptic fits for two years before his death. Occasionally the spasms began in the left half of the face and extended to the arm and leg, but did not become general. After such attacks sensation was lost in the left arm, and the arm was paretic for some hours. Toward the close of life the paresis became permanent, and extended from the arm to the leg, and sensibility was somewhat impaired in these limbs. The temperature was 2.5° F. higher over the right parietal eminence than over the left. | Gumma. Arising from the membranes, two inches in diameter, but very thin, involved the gray matter of the posterior extremities of the first and second frontal convolutions, the upper and middle thirds of the ascending frontal convolution, and the adjacent border of the ascending parietal convolution of right hemisphere. |
F. H. Martin, Chicago Med. Journ. and Exam., vol. xlvi. 21. |
| 22 | F. 57. | After excitement lost consciousness. Paresis and heaviness of the right upper extremity. Aphasia; used words inaccurately; short of words and enunciation impaired. Second attack of loss of consciousness. Twitching in right half of body and face. Paralysis of right upper extremity. Severe pains in right arm and leg. Another attack of loss of consciousness, with spasms of right half of body. Right lower extremity and right lower face paretic. Slight trismus; right masseter contracted. Dull headache. Organs of sense not affected. Understands all that is said to her, although aphasic. [p. 1074] Sensibility good. Right-sided pneumonia; œdema of lung. | Fibro-glioma. Tumor size of fist occupied the whole of the lower and middle portion of the parietal lobe, imbedded in both ascending convolutions. Ascending frontal convolution pushed aside; the annectant gyrus and island of Reil compressed and flattened. Fissure of Sylvius arched over by tumor. White substance also pushed toward the corpus striatum. Meninges congested. Left parietal bone somewhat excavated. |
Petrina, op. cit. |
| 23 | F. 39. | Began to suffer with epilepsy two weeks after a blow on the left parietal region. The fits were preceded by formication in the right hand and tongue, and began with spasm in the right hand, which was weak for some hours afterward. A permanent right facial paresis developed one month after the blow, and two months later the tongue, arm, and hand were also paretic on the right side. Disturbance of vision due to choked discs had developed, and temporary attacks of aphasia occurred after the frequent convulsions. She sank into a condition of stupor and aphasia four months after the first symptoms. The skull was then trephined at the seat of the old injury in hopes of evacuating a chronic abscess, but no pus was found. One week after this she died. | Gumma. A gumma one inch in diameter was found on the surface of the left hemisphere, at the junction of the middle and lower thirds of the ascending parietal convolution, and involving also the convolution posterior to this. The membranes were adherent to the gumma. |
H. B. Sands, Med. News, April 28, 1883. |
| 24 | M. 25. | Four years previous to death had received a blow on
the left side of the head. A year later, twitching in the tongue and
the left side of the face. Twitching of the left arm. Twitching
increased. Paroxysmal spasm and general convulsions, with loss of
consciousness. Paresis, and then slowly-developed paralysis, of the
forearm and hand. Some paresis of left leg. Double optic neuritis.
Violent headache. This patient was in charge of Hughes-Bennett at the Hospital for Epilepsy and Paralysis, London. He diagnosticated brain tumor, and suggested its removal. Rickman Godlee trephined over suspected region, and removed a glioma of the size of a walnut. The operation was performed November 25th. The patient did well until December 16th, when he was seized with a rigor, followed by fever, sickness, and pain in the head. A hernia cerebri of large dimensions supervening, he died December 23d. |
Glioma. Meningitis was found at the lower border of the wound, spreading downward toward the base of the brain. |
Hughes-Bennett and Rickman Godlee, British Medical Journal, Nov. 29, 1885. |
| 25 | F. —. | Syphilitic history. Tingling sensation and numbness of the left arm and leg, which increased until it ended within six weeks from its commencement in complete motor paralysis, with a deficiency in the perception of touch. Left side of the face also slightly paretic. Mental confusion and loss of memory. | After antisyphilitic treatment and
counter-irritation, trephining was performed over the middle of the
ascending parietal and frontal convolutions. Internal table of the
disc removed was found softened and thicker than usual, having on its
internal surface projections or roughnesses. A second opening was made
over the occipital region, and a similar thickening was found.
Opposite first opening the dura mater pale and thickened. It was
elevated, and a false membrane of yellow color was removed. An
incision was made in the direction of the
[p. 1075] paracentral lobule,
when a gush of grumous, red-colored fluid escaped. Day after the operation much better; on third day moved her toes; within a week lifted her leg; fingers moved within a week. Mind greatly changed for the better. |
Macewen, “Proceedings of Path. and Clin. Soc. of Glasgow,” Glasgow Med. Journ., vol. xxi., 1884, p. 142. |
| Centrum Ovale—Fronto-parietal Region. | ||||
| 26 | F. 16. | Fell when sixteen months old from the table on her head. Left hand, five months later, noticed at times to be stiff and firmly closed. Three months later the leg became similarly affected, and two months later general paroxysms. Many seizures for periods of weeks or months, then intervals of freedom. Spasm began by contraction of the left hand: she would lie down and jerk for a half minute or minute, laughing or talking all through it, never losing consciousness. In about six years left leg became paretic. Seizures became much worse and more frequent; unconscious for six weeks, and fifty to eighty spasms in twenty-four hours. Ten months without spasms until a week before death, when they returned with great violence. Spasms always began in the left hand; appeared to extend to the leg first, and then to the face. Intellect clear. | Fibro-glioma. In the white matter, but touching upon the gray at several spots at the position of the upper end of the ascending frontal convolution of the right hemisphere. The tumor occupied largely the anterior portion of the paracentral lobule. |
Osler, Medical News, vol. xliii., Jan. 19, 1884, in “Proceedings of Medico-Chirurgical Society of Montreal;” also, Am. Journ. Med. Sci., N. S. vol. lxxxix., Jan., 1883, p. 31. |
| 27 | M. —. | Severe fall, followed by insensibility. Paralysis of the left side followed injury, but improved. Three years later, epileptic convulsions: sudden fall, general spasm, biting tongue. These attacks replaced by partial or localized epilepsy without loss of consciousness: tonico-clonic spasm of muscles of left side of face and neck and of left upper extremity, especially of the thumb and index finger. Left pupil a trifle larger than right; left cheek paretic, left arm and forearm absolutely paralyzed; left leg weak. Marked tactile anæsthesia on left side. Ophthalmoscope showed fulness of veins, but no neuro-retinitis. Late, some opisthotonos. Deafness in right ear; axillary temperature, 36.4° C. Pain in right arm and leg and in posterior part of head on right side. Conjugate deviation of head and eyes from palsied side. No neuro-retinitis. Localized and general convulsions recurred from time to time. | Sarcoma. Larger than a hen's egg in white substance of right hemisphere, occupying the whole thickness of the hemisphere above the opto-striate bodies. Exerted much pressure upon these bodies, on convolutions near, and even upon the inner surface of the left hemisphere. Adherent to the dura mater. Right half of the brain much enlarged, and lateral ventricle and septum lucidum forced over to the left. Two depressions on the top of the skull; dura mater depressed and adherent to convolutions. Some pachymeningitis. |
E. C. Seguin, Opera Minora, p. 215; reprinted from the Transactions of the Amer. Neurol. Ass., vol. ii., 1877. |
| 28 | M. 34. | Attacks of right-sided epilepsy every four or six weeks; later, every week or oftener. Spasms wholly restricted to the right arm or leg; the slightest attacks only momentary shocks on the right side of the body. No spasm in the face. Only very rarely lost consciousness. Never frothed at the mouth, bit his tongue, or micturated in the attacks. In intervals had good use of his right hand and leg up to a late period. Paresis of right limbs came on with indefinite numbness of right leg. Diffused headache, mostly frontal. No facial palsy; no anæsthesia. Knee-jerk absent on left side and strong on right. [p. 1076] Later, complete paralysis of right arm and leg, with œdema. Violent headaches, more to the left of the median line at the vertex; photophobia, nausea, and vomiting. No neuro-retinitis. Still later, paresis, and then paralysis of right face. Atrophy; contractures; bed-sores; semi-coma; profuse sweating; high temperature; conjugate deviation of the eyes to the right; head straight. | Sarcoma. In centrum ovale, underneath the left cortical motor area, and completely undermining it, was a large cavity which contained a large amount of coffee-red serum, and also a tumor lying on its inner side near the paracentral lobule. The tumor was connected behind with the falx cerebri in the region of the paracentral lobule. |
E. C. Seguin, Opera Minora, p. 499, and Journ. of Nerv. and Mental Dis., July, 1881. |
| 29 | M. 22. | First symptom was a fit, which was followed by a
rigor. After this fit paresis of right arm and leg, with inability to
articulate properly. Could not raise the affected arm, but could grip
objects weakly. Paralysis of right side of face and tongue. Was quite
rational. No loss of sensation. Later, violent headache, followed by
vomiting. Slight amelioration of many symptoms, soon followed by
second attack of violent headache, which could not be localized;
complete right hemiplegia and aphasia. Later, dysphagia. Death rather
sudden. Patient had had amputation of thigh about six months before for sarcomatous enchondroma of head of the tibia. Had also had chancre four years before. |
Enchondroma. In left hemisphere, between anterior part of corpus striatum and “surface of frontal lobe.” The cortex over tumor and the outer and anterior portion of corpus striatum were softened and broken down. |
T. P. Pick, St. George Hosp. Rep., vol. ix. p. 663. |
| 30 | F. 16. | Patient was a wayward, hysterical girl of neurotic
family, precocious, and with abnormal sexual instincts and
indulgences. Had a sudden attack of total blindness, then sudden
recovery; sudden blindness again, and deafness; then restoration of
hearing; loss of power in lower limbs, ending with total blindness,
deafness, and paraplegia. Had dilated pupils and some hyperæsthesia;
also marked hysteroidal attacks, becoming at last maniacal. Negatively, no constant headache or affection of ocular, facial, or lingual muscles, no convulsions or vomiting; no abnormal ophthalmoscopic appearances (except slight choked disc). The case had been diagnosticated by many doctors and one of the “first authorities in Europe” to be hysteria. |
Tumor in right hemisphere, size of hen's egg, translucent, and nodulated, soft, highly vascular, with small extravasations of blood on its surface, occupied medullary substance of middle lobe superior to lateral ventricle causing bulging of roof of ventricle. | A. Hughes-Bennett, Brain, 1878, vol. i. p. 114. |
| Postero-parietal Region. | ||||
| 31 | M. 25. | Kicked on the head. Headache, nearly continuous, with violent paroxysms. Vomiting at intervals, most when headache was most violent. Vertigo. Mental confusion; sometimes maniacal. Left convergent strabismus. Partial right hemianæsthesia. Patellar reflexes slightly exaggerated; slight ankle-clonus on the right side. Blind in both eyes; sight of right eye lost first. Choked discs, and eventually optic atrophy. Hearing defective in right ear. Constipation. Head-temperatures taken once; right parietal region, 98° F.; left parietal, 97.8° F. | Fibroma. Adherent to membranes, and involving the left postero-parietal and occipital region to within half an inch of longitudinal fissure. The brain-tissue around softened and broken down, the parts disintegrated being chiefly the white matter of the postero-parietal and occipital lobes. |
C. K. Mills, Arch. Med., vol. viii. No. 1, August, 1882. |
| 32 | M. 49. | Dropping of left hand at intervals, with power regained in about an hour. Brief attacks of loss of speech, and numbness in lips and tongue on both sides. Numbness in tips of his fingers and the left hand. Slight paroxysms of general rigidity. Severe frontal headache. No vomiting. Loss of sight, gradually increasing to total blindness. Involuntary micturition. Increasing hebetude. Slow but probably correct intellection. Left upper extremity, toward last, paretic. Was able to stand, but could scarcely walk. Hearing and taste preserved. [p. 1077] Some doubt as to smell. Later, imbecile. After a severe fit of general convulsions he died. Duration, about four months. | Carcinoma. It occupied nearly exactly the site of the right “poster-parietal lobule” (superior parietal). It was clear of the ascending parietal convolution in front, and behind did not quite touch the external parieto-occipital fissure; below it extended just short of the intraparietal fissure, and on inner face of hemisphere reached for half an inch into quadrilateral lobe. Below tumor toward ventricle brain-substance softened. |
James Russell, Brit. Med. Journ., 1876, ii. p. 709. |
| 33 | F. 36. | Right-sided temporal and orbital neuralgia. Anæsthesia of left arm. Epileptic attacks. Slighter attacks of spasm, without unconsciousness, in left face, left arm, and hand. Paresis of left arm. Blindness. Optic neuritis. Pupils dilated and immobile. Later, loss of smell and taste. Mental depression. | Gummata. In right supramarginal lobule two tumors size of pea, lying superficially. |
Broadbent, Lancet, Jan., Feb., 1874, quoted by Bernhardt,
p. 68. Beitrage zur Symptomatologie und Diagnostik der Herngeschwülste, von Dr. M. Bernhardt, Berlin, 1881. |
| 34 | —— | Left hemiplegia with some anæsthesia. Deafness developed in the left ear, with a total inability to localize the origin of sounds. | Tumor size of an apple in middle of ascending parietal convolution and backward. Around the tumor white softening, which extended forward as far as the fissure of Rolando, and backward throughout the right parietal lobe, and beneath almost into the central ganglia. | Strümpell, Neurolog. Centralb., Aug. 15, 1882. |
| 35 | M. 54. | Middle finger of the right hand began to jerk violently, also some of the flexor tendons. Twenty minutes after this he had a fit, in which he became unconscious and beat himself violently on the chest with the right arm. Had three of these fits. Aphasic after this for two weeks. Had high fever at the time of the seizures; was rubbed all over the body with ice. The fingers became paretic, not the forearm or arm. Arm became numb at times, especially after exertion. With dynamometer, left hand, 75; right hand, 55. Headache, which ceased after some months. Right optic disc abnormally red, but not choked; left disc normal. Had a convulsive attack in the Philadelphia Hospital, in which the four fingers of the right hand rapidly vibrated, contracting and extending without pain; no loss of consciousness or other disturbance. The tongue was also affected, so that speech was impossible. Later, the patient had a general convulsion, preceded by a drawing sensation in the face; convulsive movements began in right hand. Tongue bitten. Attack preceded by severe headache. Had another attack without loss of consciousness or convulsion, preceded by a sensation as of a knife cutting through the flesh, which travelled up from the left hand to the shoulder, and then to the head. Increasing loss of sensation in the fingers of the right hand. Increasing difficulty of speech, with spells of melancholia and crying. Right side of face markedly paralyzed. Right arm almost entirely paralyzed and much swollen. Speech much affected; difficulty in swallowing. Paralysis involves the right leg. | Gliomata. A small tumor occupies the lower end of the left supramarginal convolution, just where it joins the foot of the ascending parietal convolution. The latter convolution was not involved in the tumor, but was distinctly pressed upon in its lower third. The ascending frontal convolution was entirely healthy. In right hemisphere a similar gliomatous growth in the foot of the angular convolution where it runs into the middle temporo-sphenoidal convolution, involving also the upper part of this convolution, and to a slight extent the deepest portions of the superior temporo-sphenoidal convolution. |
H. C. Wood. Not before published. |
| Occipital Region.
[p. 1078] Occipital lobe—cortex and centrum ovale. |
||||
| 36 | M. 57. | Headache. Vertigo. Paresis of left side. Left facial paralysis, especially middle branch. Vomiting. Right pupil dilated. Tongue not involved. Uvula directed to left. Left velum palati relaxed. Taste, smell, sight, and hearing normal; sensibility of whole body normal. Reaction of degeneration on left side of face. Left side of body shows reaction of convulsibility. Slight quantity of albumen. Paresis declined with exception of facial nerve. Apathetic. Œdema of lung. | Glioma. In middle of right occipital lobe; lobe softened. Right lateral ventricle narrowed and left dilated. Right posterior horn and right thalamus opticus compressed. |
Petrina, op. cit. |
| 37 | M. 27. | Dysphagia, most marked with liquids, caused by paresis of pharynx, more marked on left. Left hemiparesis for three years. Headache (frontal and temporal), which is of a boring, tearing character. Failure of memory. Speech guttural and monotonous. Puriform expectoration. Later, feeble voice, hiccough, yawning, somnolence. | Fibroma. On posterior face of left petrous bone and inferior occipital fossa, extending behind occipital foramen and to right of cerebellar falx. A prolongation involving the pneumogastric and glosso-pharyngeal, and spinal accessory. Also cerebellar abscess. |
Cruveilhier, Bull. de la Soc. Anat., 1855, xxx. 475-479. |
| 38 | F. 20. | Headache. Dimness in right eye, then in left;
finally, blindness in both. Convulsions. External strabismus; right
pupil dilated, left contracted. Coma, alternating with consciousness.
Vertigo. Optic discs congested, presenting small hemorrhages;
exophthalmus. Paresis of right arm and leg; partial anæsthesiæ on same
side. Earache. Vomiting, not frequent. Coma and death. Duration, about three months. |
Sarcoma? Occupied all the posterior part of right hemisphere of cerebrum, pressing upon and indenting opposite hemisphere and right half of the cerebellum. |
S. O. Habershon, Guy's Hosp. Rep., 3d S., xx. 330-334. |
| 39 | M. 18. | Periodical headaches. Pains in the neck and vertebral column. Points of exit of trigeminal nerve sensitive. Staggering gait. Diplopia. Confused sounds in right ear. Tetanoid contractions of neck. | Echinococcus. In right occipital lobe. |
Visconti, Annal. Univer., Oct., 1869, quoted by Bernhardt, p. 98. |
| 40 | F. 21. | Right hemianopsia. Central vision good. Other
symptoms: headache, dysarthria, anæsthesia of the right half of the
face. No paralysis, no mental symptoms. Choked discs. Duration seven months. |
Cystic glioma. In the left occipital lobe; had reached and destroyed the cortex of the lobe at its apex, and had extended inward, nearly reaching the inferior cornu of the lateral ventricle. The entire inner half of the occipital lobe was thus destroyed. |
Jany, Knapp's Archiv f. Augenheilk., vol. xi. p. 190, quoted by Starr, Am. Journ. Med. Sci., N. S., lxxxvii., Jan., 1884, p. 72. |
| 41 | M. 42. | Right hemianopsia. Central vision good. Other symptoms: aphasia, right complete hemiplegia, with facial paralysis. | In left occipital lobe, surrounded by a zone of softening, reaching inward to and involving the pulvinar of the left optic thalamus. Optic tracts normal. | Hirschberg, Deut. Zeitsch. f. Prakt. Med., 1878, No. 4, quoted by M. Allen Starr, Am. Journ. Med. Sci., N. S., lxxxvii., Jan., 1884, p. 69. |
| 42 | M. 42. | Right hemianopsia, not quite reaching the point of fixation. Central vision good in both eyes. Ophthalmoscopic examination negative. Other symptoms: vertigo, loss of memory, aphasia, and partial agraphia, with temporary right hemiplegia. | Gelatinous sarcoma. In the left occipital lobe, involving all three of its convolutions, as well as the præcuncus. Softening extended inward through the white substance to the posterior cornu of the lateral ventricle. Thalamus and optic tracts normal. |
Jastrowitz, Arch. f. Augenheilk., 1877, p. 254, quoted by Starr, Am. Journ. Med. Sci., N. S., lxxxvii., Jan., 1884, p. 71. |
| 43 | M. 40. | For seven years epileptic seizure, beginning with [p. 1079] spasm of left leg and going on to general convulsions; motions more violent on left side. An aura consisting of a darkness, coming gradually over the field of vision from the left side, always preceded the attack. During the intervals left-sided headache was the chief symptom. It seems probable that a temporary left hemianopsia preceded the attack. | Cyst filled with serum. In white matter of the right occipital lobe, surrounded by a zone of softening which did not involve either the cortex or the wall of the lateral ventricle. |
Traube, Gesammt Beitrage zu Pathologie, ii. 1083, quoted by Starr, Am. Journ. Med. Sci., N. S., vol. lxxxvii., Jan., 1884, p. 73. |
| 44 | M. 52. | Headache. Numbness down right arm. Later, paroxysms
of headache lasting twenty to forty minutes, generally preceded by
pain and numbness in right hand and arm, ascending to head, and so
intense as to produce profuse perspiration. Delirium (lasting two
days) during these attacks. No paralysis or previous fit, nor
vomiting. Few hours before death had convulsions. The pain and numbness were in right arm, although tumor was in right hemisphere. |
Malignant tumor. Size of pullet's egg at inferior portion of posterior lobe on right side in substance of cerebrum, approaching within a few lines of surface. |
J. C. Langmore, Trans. Path. Soc. Lond., iii. pp. 246-248. |
| Temporo-sphenoidal Region.
Temporo-sphenoidal lobe. |
||||
| 45 | M. 33. | History of syphilis. Blows on the head. Headache, continuous, usually dull, occasionally severe. Occasional vomiting. Stupidity, want of energy, drowsiness. One general convulsion a few hours before death. Partial anæsthesia on the right side. Hyperæsthesia of left side. Sight impaired. No ophthalmoscopic examination. Hearing defective in right ear. Constipation. | Gumma. One and a quarter inches in diameter, attached to adherent membranes, and involved the middle portions of the first and second temporal convolutions of left hemisphere. A layer of brain-substance both anterior and posterior to the tumor was softened. The tumor grazed the ascending parietal and inferior parietal convolutions. A large foyer of greenish-yellow pus was found to the inner side of the tumor. |
C. K. Mills, Arch. Med., vol. viii. No. 1, August, 1882. |
| 46 | M. 42. | At first an attack of vertigo which lasted over twenty-four hours: some unconsciousness for a time. Continued headache; loss of memory; giddiness and vomiting, the latter occurring without connection with the state of the stomach as to food. Partial bilateral deafness, which the patient stated was of long duration. No paralysis, but right hand a little weaker than left. Distinct mental failure during last two weeks of life; incoherence and faulty memory. | Epithelioma. Ovoid tumor about one and a half inches in diameter in the central portion of the temporo-occipital region. Hippocampal convolution grazed. Some surrounding softening and meningitis. One corner of tumor had produced a small spot of softening in the cerebellum. |
H. C. Wood, “Trans. of Path. Soc. of Philada.,” 1880, Med. Times, vol. xi., Jan. 29, 1881. |
| 47 | F. 40. | Suffered from a light form of epilepsy dating from tenth year, which resulted, it was believed, from a fall. Rarely bit her tongue, but usually frothed at the mouth. No history of one-sided spasms. Always had an aura of a peculiar character. She suddenly perceived a disagreeable odor, sometimes of smoke, sometimes of a fetid character, and quite uncomplicated by other sensory warning. Developed phthisis, her attacks occurring from time to time until her death. | At lower part of right temporo-sphenoidal lobe a shrinking and induration involving the uncinate gyrus and parts of the adjacent convolution. The olfactory nerves were not involved. A form of low-grade hemorrhagic pachymeningitis present. | Allan McLane Hamilton, New York Med. Journ. and Obstet. Review, vol. xxxv., June, 1882, p. 575. |
| 48 | F. 39. | Attacks of convulsion seven weeks before her death. [p. 1080] In two weeks mind affected; drowsy and stupid; condition of dementia. Passed into a state of semi-consciousness. No eye symptoms. No paralysis. Percussion on left side of head painful. | Sarcoma. Occupied the posterior part of the fourth and fifth temporal convolutions, and the third convolution was atrophied. Did not involve the lateral ventricle. Under surface flattened and resting partly upon the left lobe of the cerebellum. |
W. H. Draper, New York Hosp. Histories, N. S. vol. x. p. 445, quoted by M. Allen Starr, Am. Journ. Med. Sci., N. S. vol. lxxxvii., April, 1884, p. 383. |
| Basal Ganglia and Adjoining Regions. | ||||
| 49 | M. 59. | Contractures of right arm and leg since childhood. Death from accident. The arm was atrophied and shortened, flexed at elbow and wrist; disappearance of some cartilages at wrist and wasting of joint-surface of radius. Femur flexed at hip; knee-joint flexed; ankle-joint in position of equinus. Other bone-changes. Right leg shortened. | Osteoma. Tumor in left corpus striatum on “surface of anterior thick half,” projecting outward into white substance of brain, and inward into anterior portion of optic thalamus. |
A. Bidder, Arch. f. Path. Anat. und Physiologie, und f. Klinische Med. Virchow, 1882, p. 91. |
| 50 | M. 30. | Right frontal and occipital headache. Vertigo. Paræsthesia of the toes, particularly the right. Face drawn to the right. Left face paretic. Right eye smaller than left. Weakness and fatigue of limbs. Convulsions. Vomiting. Slow pulse. | Myxo-sarcoma. In right corpus striatum protruding into right lateral ventricle and cortex. |
Schüppel, Arch. d. Heilk., p. 357, 1867. |
| 51 | M. 34. | Walked a mile to an infirmary, and in less than one hour went into a series of severe epileptic attacks, which continued for four hours. The spasms were clonic, and chiefly in upper extremities, with violent contortions of face; the latter most marked on left side and in zygomatici. Between the fits there was deep coma, especially three hours before death, when, after another violent fit, he died, seven hours after first seizure. No paralysis, and report says nothing about any previous fits. | Myxomatous glioma. It exactly occupied the place of right nucleus caudatus, extending outward as far as white fibres, but not involving them. Brain-tissue in proximity normal. |
Dowson, Med. S. and Gaz., London, 1878, p. 333. |
| 52 | —— | Partial anæsthesia of right half of trunk. Hyperæmia of retina, and capillary hyperæmia of left optic disc. Left pupil dilated; left ptosis; left diverging strabismus. Paralysis of right side and extremities. Paralysis of muscles around right corner of mouth. Incontinence of feces and urine. Redness of face. Variations in temperature. | Tubercle. In left optic thalamus. Partial destruction of left peduncle of cerebrum. |
Fleischmann, Wien. med. Wochenschrift, 6, 7, 8, 9, 1871, quoted by Petrina. |
| 53 | F. 44. | Severe headache on left side. Sensibility lessened in left extremities, at same time frequent pain. Intelligence diminished. Speech retarded. Strabismus of left eye. Amblyopia. Left pupil alternately dilated and contracted. Left lagophthalmos. Chattering of the teeth. Twitchings on the left paralyzed half of the face. Tongue and uvula tending toward the left. | Sarcoma. Right optic thalamus. Corpora quadrigemina compressed. |
Friedreich, quoted by Petrina, op. cit. |
| 54 | F. 38. | Headache. Creeping sensations in right arm and leg. Right facial paresis. Paresis of left extremities. Convulsions. Dimness and confusion of sight. Diplopia. Hardness of hearing. Failure of memory. Difficulty in speaking and swallowing. Improvement under iodide of potassium. | Glioma. Left optic thalamus. |
Bruzelius and Blix, 1870, quoted by Bernhardt, 153. |
| 55 | F. 14. | Headache, vertigo. Epileptic attack. Right hemiplegia. No anæsthesia. Slight dilatation of pupils. | Sarcoma. In left optic thalamus. The right optic thalamus also affected. Corpora quadrigemina enlarged and pushed backward. |
Rusconi, Gaz. Med. Ital., 1874, No. 11. |
| 56 | M. 30. | Headache. Left ptosis; fixation of left eyeball. [p. 1081] Drowsiness. Retarded speech. Gait unsteady. Paresis of right hand and foot. Emaciation; incontinence of urine. | Serous tumor. Large as a nut, in posterior half of right optic thalamus. |
Troschel, Med. das ver. für Heilk. in Preussen, xliii., 1839, quoted by Petrina. |
| 57 | F. 36. | Imbecile. Speech inarticulate. Pupils contracted. Spasms in arms, but light in limbs. | Cancer. Left optic thalamus and corpus striatum without definite boundary, extending into brain-mass. |
Brenner, quoted by Petrina, op. cit. |
| 58 | F. 33. | Headache and vomiting for three weeks: for one week had been maniacal. Convulsions. Apoplectiform attack, marked by unconsciousness, general muscular flaccidity, and stertorous breathing. Paralysis of left face; twitching of right face. | Glioma. Between left optic thalamus and hippocampus minor, extending from the ventricle to the under surface of the brain. Corpus striatum and optic thalamus unaffected. Hemorrhage on under surface. |
Owen, St. George's Hosp. Rep., ix., 1877-78, p. 150. |
| 59 | M. 45. | Vertigo, headache, and tinnitus. Five years before attack had fallen and struck the back of his head. Much exposed to the sun. One day in August a general feeling of numbness came over him. This was followed by vertigo, etc., as above. Staggered and stumbled in walking as if intoxicated. Unable to maintain his balance in the dark or with his eyes closed. Some numbness in legs and arms, but no actual loss of sensibility. No neuro-retinitis; no paralysis. When erect had a constantly increasing tendency to stagger backward. Divergent squint and diplopia appeared. Potassium, iodide blisters, and seton were used. Noises and headaches disappeared. During last two or three weeks some difficulty in swallowing. Involuntary evacuations. Occasional hallucinations. | Glio-sarcoma. Tumor size of walnut in third ventricle, moulded to the interior. Extending to base of brain just above corpora albicantia, and forward as far as anterior commissure. A caudate prolongation completely blocked up the Sylvian aqueduct. Owing to this obstruction, a large quantity of serum had been imprisoned, enormously distending the fourth and lateral ventricle. The growth invaded left optic thalamus. Superior surface of cerebellum softened from median line to middle of right hemisphere. |
F. Woodbury, Am. Journ. of the Med. Sci., N. S. lxxvi., July 1, 1878. |
| 60 | M. 15. | Epileptic from childhood: had had no fits for last three years. Had tremors and was dull. Short-sighted, and had a habit of absurdly frequent winking. Nothing else wrong with eyes. Suddenly, after a mental disturbance, had intermitting pulse. Cold surface, dulness, head and face swollen and flushed. Then tonic spasms, loss of consciousness, involuntary micturition. General tremors, dilated pupils, stupor. Next diffused dusky-red flush of both cheeks, also over back of hands and forearms. Temperature depressed to 92° in axilla. Automatic repetition of words. Taste and smell normal. He recognized himself in looking-glass on the day he died. | Sarcoma. In third ventricle, lying between corpora striata and optic thalami of opposite sides. It completely enveloped optic commissure, and partially involved track of optic nerves issuing from front. The sole organic connection of tumor was with the commissure. The tuber cinereum was distinct from its tissue. |
Russell, Med. Times and Gaz., 1873 (1), p. 522. |
| 61 | M. 19. | Periodical headaches. Unsteady gait. Left hemiparesis. Peculiar swelling of face. Delirium. Convulsions and sudden death. Bad-smelling discharge of the nose. | Echinococcus. In left lateral ventricle; the whole of the ventricle a sac. |
Yates, Med. Times and Gazette, Aug., 1870. |
| 62 | M. 14. | Convulsions; vomiting; internal strabismus of right eye; gradually increasing paresis of left leg and arm. Reeling toward left side. Occipital headache. Pain and numbness in left arm. [p. 1082] Lateral movements of eyes lost; paralysis of accommodation; nystagmus. Oscillation of left hand. Left leg ataxic. Patellar reflex exaggerated, and ankle-clonus present on left side. Superficial reflexes increased on right side. Partial anæsthesia on left side. Sight good; double optic neuritis. Left-sided hearing impaired. Taste and smell normal. Toward end, increasing torpor; left hemiplegia, except slight power retained in face, with anæsthesia and analgesia. Tonic fits. Right pupil dilated, and external strabismus in right eye. Slow respiration. Ankle-clonus and increased knee-jerk in right. | Glioma. Involved right anterior tubercle of corpora quadrigemina; also right optic thalamus, posterior part of internal capsule, and tegmentum of crus cerebri. The enlarged optic thalamus pressed back upon right anterior portion of cerebellum and middle peduncle, and exerted some transmitted pressure upon medulla oblongata. |
David Ferrier, Brain, vol. v. p. 123. |
| 63 | F. 29. | Cervico-occipital headache. Vertigo. Convulsions. Right facial paresis. Tendency to fall backward. Uncertain gait. Optic neuritis. Double amblyopia. Difficulty in moving both eyes toward the left. Diminished intelligence. Vomiting. | Glioma. In corpora quadrigemina. Cerebellum not involved. Tumor lay upward and outward from the left cerebellar crus ad pontem. |
Annuske, Von Graefe's Arch., 1873, Bd. xix., quoted by Bernhardt, 167. |
| 64 | M. 21. | Right temporo-frontal headache. Vertigo. Pains in right leg. No anæsthesia. Right leg paretic. Tinnitus. Atrophy of the right optic nerve. Abnormal somnolence. Sexual inclination diminished. Vomiting. Blindness, first of the right and then of the left. Right divergent strabismus. Pupils dilated. | Lipoma. Tumor compressed corpora quadrigemina and geniculate bodies. |
Hirtz, Bull. de Société Anat., Mars and April, 1875, quoted by Bernhardt, 168. |
| 65 | F. 3. | Right hemiparesis. Right-sided tremor. Contraction of the right elbow. Late, loss of sight in left eye. Ptosis, dilatation of the left pupil. Stupidity. Peculiar movements when seated from right backward to the left. | Tubercle. At site of corpora quadrigemina, springing into the third ventricle. Left cerebral peduncle compressed. |
Pilz, Jahrbuch. für Kinderkrankh., iii., 1870, 2, 133, quoted by Bernhardt, 168. |
| 66 | M. 25. | Cervico-cephalic pains. Vertigo. Uncertain gait. No paralysis. Tension of muscles of neck. Optic neuritis. Double amaurosis. Tinnitus. Diminution of hearing. Intelligence clear until within fourteen days of death. Insensibility, delirium, coma. Small irregular pulse. | Glioma. Tumor displaced corpora quadrigemina and pineal gland. Projected into the third ventricle through aqueduct of Sylvius and into fourth ventricle. |
Duffin, Lancet, June 17, 1876. |
| 67 | M. 7. | Occipital pains. Staggering gait toward right and backward. Hydrocephalic cries. Tendency of head forward. Alternating diverging strabismus. Double optic neuritis. Sudden death in paroxysm of pain. Paresis of bladder. Vomiting. | Tumor took the place of posterior part of corpora quadrigemina and velum. Cyst in the midst of the cerebellum, reaching the fourth ventricle. | Kohts, Virch. Arch., Bd. lxvii., 1876, quoted by Bernhardt, 168. |
| Cerebellum. | ||||
| 68 | M. 1. | Frontal headache. Slight control over arms and legs. Stiff neck. Dilated pupils. Sopor. Vomiting. Duration, one year. | Glioma. Size of an orange in the middle of cerebellum. Chronic hydrocephalus. |
H. Green, Trans. Path. Soc., vol. xx., 1870. |
| 69 | F. 21. | Fall from a swing upon the head, followed by loss of consciousness for a few minutes. Occasional headache during eleven years, always located at the occipital region. Eight months before death severe paroxysmal headaches, increased to one every five or six days, and lasting three to four days. Great hyperæsthesia of the head. Choked discs in both eyes. Complete blindness. Slight paresis of left side of body; twitching of muscles of left side of face. Staggering gait; sometimes complained of a momentary swinging or rotary sensation. Intellect clear. During last few days of life loss of power of deglutition, and also of taste, smell, and hearing. | Tubercle. In left and middle lobe of cerebellum, involving the pia mater. Over the tumefaction leptomeningitis. |
H. F. Formad, Tr. of Philada. Path. Soc., 1879-81, vol. x. p. 178. |
| 70 | F. 27. | History of syphilis. Headache, with paroxysmal [p. 1083] exacerbations. Vomiting, frequently recurring; for four weeks before death vomited almost incessantly. Vertigo; impossible to sit or stand because of vertigo late in illness. Slowness of mind and hebetude. General muscular weakness. Right partial hemiplegia and hemianæsthesia. Trigeminal neuralgia. No ophthalmoscopic examination, but sight impaired. Marked slowness of respiration; respirations ran down as low as four and five per minute two weeks before death. | A nodulated mass involved the right middle cerebellar peduncle and the adjacent region of the right cerebellar hemisphere. The right upper half of the floor of the fourth ventricle superficially softened. A small area of softening was also found involving the under outer surface of the left optic thalamus, the breadth of the internal capsule, and a small segment of the lenticular nucleus. | C. K. Mills, Arch. Med., vol. viii. No. 1, August, 1882. |
| 71 | F. 13. | Tubercular history. Headache, with severe paroxysms; most marked in frontal and occipital regions. Vomiting; vertigo; attacks of reeling and falling. Mental dulness. Weakness of limbs, but no distinct paralysis. Hyperæsthesia; severe pains in limbs. Gradually went blind, first in left eye, and then in right. Descending neuritis determined nearly a year before death; marked optic atrophy observed a month before death. Constipation. | Tubercle. A large nodulated mass occupied the lower two-thirds of the right cerebellar hemisphere; one small nodule extended across the posterior extremity of the superior vermiform process, destroying altogether about one-third to one-half of a cubic inch of its substance. Internal hydrocephalus. |
C. K. Mills, Arch. Med., vol. viii. No. 1, Aug., 1882. |
| 72 | F. 20. | Headache. Occasional vomiting, but only upon a full stomach and at the beginning of a paroxysm of headache. No impairment of intellect; no paralysis; no convulsion; no inco-ordination. During last few days, when in paroxysms of headache, her face would be drawn toward left side, accompanied by a rigid drawing backward of the head, by pain in left shoulder and arm, and by a marked diminution of sensation in the same shoulder and arm. Head-pain excruciating, at first involving the whole cranium, afterward only the forehead and temples, but finally only the back of the head and nape of the neck. Died of sheer exhaustion. Symptoms and physical signs of phthisis. | Tubercle. In right lobe of cerebellum. Tubercular disease of both lungs with pleuritic adhesion. Fatty liver. |
L. S. Clark for A. S. Gerhardt, Tr. of Philada. Path. Soc., 1878-79, vol. ix. p. 144. |
| 73 | M. 45. | Occipital headache. Movements weak; gait staggering. Inability to fix eyes; sight retained. Pupils unequal. Partial deafness in both ears. Vomiting. Sopor. Sudden death. History of fall upon head at twenty years of age, since which time much headache. | Tumor size of nut, compressing cerebellum and pons, situated between pons, middle peduncle of cerebellum, the cerebellum, and brain. Corpora quadrigemina atrophied. | Luys, Gaz. des Hôp., 1867, 105, quoted by Bernhardt, p. 225. |
| 74 | F. 52. | Violent and continuous headache. Gradual loss of sight. Very irritable. Psychic pain and complaints. Incoherence of ideas. In three to four years some anæsthesia of left leg; the left hand became rebellious to the will. Paralysis progressed; symptoms increased very slowly. Intense coryza, with running from the nose, accompanied with a feeling as if a strange body filled up this cavity. Great appetite. Had an attack of unconsciousness, preceded by violent pains and creepings in the left hand, and presenting the following conditions: Dorsal decubitus; flushed face; head strongly retracted; [p. 1084] frowning; respiration difficult, but not stertorous; pupils large and insensible to light; the left eye widely opened, the right shut; very marked contraction in the orbicular muscle; stringy mucus in large quantities from right nostril; the left commissure of the lip strongly carried downward and backward. Tongue white, not deviated. Limbs of the right side not anæsthetic or paralyzed; the hand strongly shut. On the left arm painful pricking; the elbow flexed at a right angle, hand completely paralyzed. Motion diminished in left leg; sensibility not altered; intelligence obtuse, but the patient responds to questions. Nausea; hiccough. Finally, diaphragmatic breathing; asphyxia by strangulation. | Tumor size of hen's egg lodged between the superior surface of the cerebellum and cerebrum. | M. Boullet, Gaz. méd. de Par., 1834, 2d S., vol. ii. p. 264. |
| 75 | F. 64. | History of a fall down stairs. Headache. Frequent vomiting. Stupor, and when admitted to the hospital three weeks before death could not give any account of herself or of her complaint. Semi-comatose. No definite paralysis. She could move both arms and legs, but could not stand. Involuntary evacuations. No deviations of the eyes; apparently saw well. Pupils equal and moderately contracted; right disc a little redder than the left, but no swelling of the disc. Died in a convulsion, the right side being most affected. | Tumor size of a greengage plum, sprang from the dura mater just under the tentorium cerebelli on the left side. It had caused the deep depression of the left lobe of the cerebellum. Also a small clot, partly decolorized, just outside the right corpus striatum. | B. Bramwell, quoted in Med. and Surg. Rep., vol. xxxiv., Mar. 11, 1876. |
| 76 | F. 32. | Headache first. Then pain in right eye and numbness in right arm and leg; vision poor in right eye, with improvement. The left soon similarly affected, without improvement. Vomiting (patient was pregnant); vertigo. Ataxia marked. Patellar reflexes diminished. Tongue protruded to left. Right pupil dilated. Taste abolished on right side. The left field of vision showed hemianopia of the temporal side. Both eyes showed optic neuritis. Later, shooting pains in legs and left arm. Mind clear, but hysteroidal excitement frequent. Surface-temperature of head elevated. Toward end mental aberration, then unconsciousness. Died during labor. | Sarcoma. A nodular tumor, size large horse-chestnut, on upper surface of right lateral hemisphere of cerebellum. |
J. T. Eskridge, M.D., Journ. of Nerv. and Ment. Dis., vol. xii. No. 1, Jan., 1885. |
| Floor of Fourth Ventricle.
Directly or indirectly involved. |
||||
| 77 | F. —. | Vertigo only on standing. Sensibility normal. Walking and standing impossible. Ataxia of legs. No paralysis. Facial and trigeminus intact. Dysphagia. Double amaurosis. Eyeballs fixed, directed forward. Symmetrically dilated pupils. Hearing, smell, and taste normal. Consciousness clear. | Tumor of whole anterior part of vermiform process of the cerebellum, lying on floor of fourth ventricle. Corpora quadrigemina compressed to thinness of paper. | Curschmann, Berlin. klin. Wochenschrift, 1877, p. 237, quoted by Bernhardt, 227. |
| 78 | M. 6½. | Fell from a bench, striking the occiput. Headache for a day or two afterward. Slight irregularity in gait. For weeks restlessness, headache, and motor ataxia the chief symptoms. In three months speech became indistinct. “He screamed his words.” Defective memory. Apparent exophthalmus; ataxic movements of the head, and a look of profound stupidity; epistaxis; bulbar conjunctiva anæsthetic; left pupil dilated; vomiting. Ophthalmoscopic examination showed congestion of right optic nerve and left descending neuritis, going on to progressive atrophy. | Glioma. Anterior portion of the fourth ventricle occupied by a rounded swelling of the pons; from under surface of the pons enlargement about equal on both sides. The anterior pyramids at entrance of pons seemed abnormally elevated, with the point of entrance also deeper than normal. Corpora quadrigemina much smaller than usual, and seemed pushed upward and flattened. |
V. P. Gibney, Am. Journ. of the Med. Sci., N. S. vol. lxx., July, 1875, p. 142. |
| 79 | M. 11. | Fronto-occipital headache. Vertigo. Staggering gait. [p. 1085] Falls often, and to right. No paralysis. Diminution of sight. Irregularity of movements of eyes. Right strabismus (?). Vomiting. | Tubercle. Size of hazelnut, in middle of vermiform process, above fourth ventricle. Some softening of surrounding tissue. |
Capozzi, quoted by Bernhardt, p. 224. |
| 80 | M. 25. | Fronto-occipital headache. No anæsthesia. No paralysis; staggering gait. Loss of consciousness, with trembling of upper extremities. Vertigo. Falls to right. Double optic neuritis; amaurosis; nystagmus. Dementia; moroseness. Vomiting. Sudden death. | Between the amygdalæ of cerebellum; in front of cerebellum, bulging into fourth ventricle, merging with floor of fourth ventricle. Medulla oblongata pushed forward to right. | Annusk, V. Graefe's Arch., Bd. xix., 1873, quoted by Bernhardt, 223. |
| 81 | M. 58. | Headache, vertigo, diplopia; vomiting. Left facial paralysis. Ptosis of both eyes, worse in left. Contracture of left masseter. Speech nasal. Sense of pharyngeal obstruction. Both eyes diverted to right; on looking toward left the right eye turns to middle line, and left eye does not follow. Pupils contracted, left more than right. Anæsthesia of right face. Left ear slightly deaf. Smell and taste normal. Head movable, with deviation. Trunk and extremities not anæsthetic or paralytic. Later, smell of left side diminished. Reactions of degeneration in left face. | Floor of fourth ventricle to left of median line, involving motor root of fifth and nuclei of sixth, seventh, eighth, and ninth nerves on that side. | C. Wernicke, Arch. für Psychiatrie und Nervenkrankh., vii. Bd. 5, iii. Heft., 1877, p. 513. |
| 82 | F. 6½. | Symptoms of tubercular meningitis with a few irregular symptoms; conjugate deviation of the eyes to the left and upward. Cheyne-Stokes breathing. | Tubercular granulation about the size of a large pea springing from the left side of the fourth ventricle, just inside the posterior pyramid, midway between the cerebellar peduncle and calamus scriptorius; touched the under surface of the middle lobe of cerebellum. Head hydrocephalic. Miliary tubercles along Sylvian fissure, and a few elsewhere. | Morris J. Lewis, Trans. of Phil. Path. Soc., 1879-81, vol. x. p. 172. |
| Pons Varolii and Medulla Oblongata. | ||||
| 83 | F. 8. | Right external strabismus, with contraction of the right corner of the mouth; contraction disappeared, but squint remained. Persistent cough, with stringy mucous expectoration. Staggering. Left hemiparesis, with left partial hemianæsthesia. Severe constipation. Bowels opened only about once in five days. Water passed voluntarily once every two days. Difficulty of articulation. Squint had almost disappeared, but later returned for a few days, and then disappeared entirely. Became unable to walk, or even to sit, unsupported. Also became unable to speak, but produced strange inarticulate sounds. Difficulty in swallowing. A marked feature in this case was the absence of headache. The only pain suffered was the pain of dull character referred to the left ear, but which lasted only two days. | Occupied the lower half of the pons and the upper half of the medulla oblongata, bulging most at the lower border of the pons at the right side, and extending a little lower and higher at the right side than on the left. Floor of fourth ventricle bulged slightly, and appeared to be expanded in all directions, so that the median fissure was pushed decidedly to the left. Incision revealed the tumor to be a large cyst filled with bloody fluid and detritus. The lower part of the ventricular floor not involved. | C. K. Mills, not before published. |
| 84 | M. 32. | Thrown from a horse and kicked on the head. History of syphilis; headache, severe at first, always came on at night; became less severe later. Vertigo. [p. 1086] Defective memory; apathy. Right hemiparesis; helplessness of all the limbs before death; partial ptosis of the right side. Sensation diminished in the left side of the face and in the right limbs. Pupils small before death. Descending optic neuritis. Conjugate deviations of the eyes and rotation of the head to the right. Persistent epistaxis; tendency to hemorrhage from mucous membranes. Constipation. | Gumma and fibroma. (1) Gumma, half an inch in diameter, distinctly limited to the left upper quarter of the pons. (2) Fibroma, no larger than a pea, between the dura and pia mater, causing a slight depression in the first temporal convolution about the junction of its middle and posterior thirds, and halfway between the parallel fissure and the horizontal branch of the Sylvian fissure. Microscopical examination of the optic nerves showed a descending neuritis of subacute character. |
C. K. Mills, reported at the meeting of the Amer. Neurol. Assoc., June, 1881, and published in the Journ. of Nerv. and Mental Dis., July, 1881; and Arch. Med., vol. viii. No. 1, Aug., 1882. |
| 85 | M. 35. | History of syphilis. Wounded in head by glancing bullet. Headache of great severity at intervals. Vomiting at time of headache. Vertigo. Failure of memory and depressed spirits. Epileptiform attacks. In the spasms lifted up the right side of his body and worked over toward the left. Occasional cramps in stomach and legs. Temporal and orbital neuralgias. Descending neuritis, and eventual atrophy of both optic nerves. Constipation. Died at the close of a series of convulsions, death being preceded by general paralysis. | Gumma. A rounded mass, quarter of an inch in diameter, attached to the pia mater, just to the left of the centre of the anterior surface of the pons. The entire anterior central portion of the pons was softer and more doughy than usual. At the junction of the pons with the medulla oblongata was a recent hemorrhage, which had spread downward to about the middle of the latter. |
C. K. Mills, Brain, Jan., 1880, and Arch. Med., vol. viii. No. 1, Aug., 1882. |
| 86 | M. 5. | At first left internal squint and nightly paroxysms of excessively silly laughter. Slight paralysis of right arm, with rigidity. Paresis of right leg, increasing to paralysis, with rigidity. During sleep arm and leg became relaxed. Difficulty in swallowing. Paralysis of left orbicularis palpebrarum and left external rectus muscles. Sensibility not impaired. Electro-muscular contractility present in all the paralyzed muscles (?). Speech lost, apparently from difficulty in articulation. Intelligence preserved till near the close. Sight, smell, and taste good. Later, suffered from intense headaches and frequent attacks of palpitation of the heart, with flushing of face and injection of left conjunctiva, and with increased rigidity of right arm and leg. Death from paralysis of the pneumogastric. | Glioma. Gliomatous transformation of the pons, but no distinct separable neoplasm. Had encroached somewhat on cerebellum, particularly in region of left pneumogastric lobule. |
W. Pepper, Trans. Phila. Path. Soc., 1878-79, vol. ix. p. 136. |
| 87 | M. 2. | Dysphagia; paresis of left arm and ptosis of left eye, which improved, followed by same symptoms on right side. “Legs affected.” Head very large. Dribbling. Paralysis of articulation. Contraction of orbicular muscle, causing ptosis (?). Clonic spasm of right side of mouth, and rhythmical jactitation of right arm on attempted movement. Unable to stand or sit. Optic discs normal. Evacuations involuntary. Left side of face paralyzed. Tonic spasms of right sterno-mastoid. Later, left arm jerked like right, and rigid contractions of legs. Retraction of head and occasional spasm of left sterno-mastoid. Impossible to gauge sensation. | Tubercle. Tumor of left side of lower part of pons and central and posterior part of upper half of medulla. Cerebral fluid increased. Medulla oblongata was twice the normal size. |
J. M. Hobson, M.D., Brain, vol. iv. p. 531. |
| 88 | M. 12. | Slight paresis of right side (arm and leg). He spoke thickly and swallowed badly. Slight headache. Was depressed. Delirious at night. Slight paresis of left face. [p. 1087] Irregularity of pulse. Choked discs. Later, paralysis of sixth nerve. Sudden death, probably in a fit. | Glioma. Membranes of base congested. Tumor, which appeared to occupy the whole left half of pons varolii. No trace of fifth nerve on left side. |
Hughlings-Jackson, Med. Times and Gaz., Lond., 1874, i. 151. |
| 89 | F. 60. | Headache frontal, severe and almost constant. Paresis of right arm and leg. Painful spasm of right arm. Paresis gradually extended to left half of body. Persistent pain in right arm, with tremor; later, same symptom, less marked, in left arm, simulating paralysis agitans. Atheromatous arteries. Melancholic; talks to herself; very hard of hearing. Head directed constantly to right. Tremor increased on voluntary motion. Atrophy of muscles of arms. Flexors of legs contractured. Electro-muscular contractility reduced, especially on right side. Later, pain on touch in right arm. Febrile intermitting symptoms, simulating malaria. Still later, distinct contracture of neck. Conjunctivitis of left eye, with corneal dulness, followed by kerato-iritis, with ulceration of cornea. Dysphagia; swelling of submaxillary glands. Œdema of lungs. | Sarcoma. Tumor of left side of pons and left cerebellar crus, extending toward transverse sinus. |
Petrina, op. cit. |
| 90 | M. 54. | Severe continuous headache. Eyes constantly turned
to the right. No diplopia. Eyes, moved together, could not turn beyond
the median line of the left, though the right eye alone could be
turned for some distance to the left beyond the median line. Pupils
equal and mobile. No paralysis or loss of sensation. Some dizziness
and stagger in walking. Died of pneumonia. After the autopsy the position of the head was regarded not as compensatory for the position of the eyes, but as due to a severing of fibres joining the rotatory muscles of the head with their reflex centres. |
In the pons at a level one centimeter below the apparent origin of the fifth nerve on the left side. It was so situated in front of the eminentia teres that it involved the course of the fibres of the left abducens, and by a little prolongation across the raphé toward the right side interrupted the fibres of communication between the centres for the sixth and third nerves. It did not involve the common nucleus of the sixth and seventh. It interrupted the posterior-interior longitudinal bundle and the adjacent part of the raphé. No other lesion was found. The tumor was the size of a small nut. | Quioc, Lyon Méd., 1881, July, Nos. 19 and 20, quoted by M. Allen Starr, Journ. of Nerv. and Mental Dis., vol. xi., July, 1884, p. 377. |
| Crura Cerebri. | ||||
| 91 | M. 25. | No headache. Staggering some days before death. Apoplectic seizure, with right-sided hemiplegia. Ptosis of left side (some days before death). Loss of consciousness for three or four days. No vomiting. | Glioma. In left crus cerebri, including also portion of right. |
Sutton, Brit. Med. Journ., Feb., 1870, quoted by Bernhardt, p. 163. |
| 92 | M. 9. | Awkwardness in using right hand; soon almost complete paralysis in the right arm. Headache; nausea; vomiting; double vision, followed by strabismus, due to paralysis of the left abducens. Occasional twitchings in right hand, but no convulsions. Paralysis extended to the right leg; staggering gait. Ataxia and rigidity in the fingers of the paralyzed hand. Pain in the legs. Optic neuritis. | Sarcoma. Pressing upon the left crus cerebri and the pons. |
E. C. Seguin, Journ. of Nerv. and Ment. Dis., Jan, 1882. |
| 93 | M. 3. | Headache; unnatural drowsiness. Ptosis of right eye, with very marked divergent strabismus and fully-dilated pupil; similar paralysis in left eye, not quite so [p. 1088] marked. Paresis of left leg. Very late, unconsciousness, constant motion of tongue and lips, and clonic spasms of left arm and leg. Twitching of right face. Convulsions, death. Duration, about one year. | Tubercle. Size of a walnut in right crus, almost destroying the crus just at its junction with pons; making pressure on left crus. Third pair of nerves diminished in size and softened. Recent inflammatory changes at base. Increased cerebral fluid. |
S. Browne, Dublin Q. J. Med. Sci., 1849, vii. 496-499. |
| Middle Region of Base of Brain and Floor of Skull. | ||||
| 94 | F. 35. | History of syphilis. Headache severe, at first with long intermissions; later, continuous, and often agonizing. Vomiting with paroxysmal headache, coming on late in illness. Vertigo, usually with headache. Excitable and irritable. Slight twitching of mouth, hands, and forearms. Left hemiplegia; upper as well as lower fibres of facial nerve paralyzed. Left internal strabismus. Electro-contractility diminished. Difficulty in enunciation. Sensibility diminished in left leg. Later, hyperæsthesia and great pain in paralyzed limbs. Conjunctivitis and necrosis of cornea of left eye; conjunctiva and cornea insensitive. Sight impaired. Descending optic neuritis. Hearing impaired on left side. Smell defective. Profuse perspiration, more marked on right side than on left. Constipation. Temperature, taken in right and left axilla for eleven weeks before death, gave the following averages: Right axilla, 99.1°, M.; 100°, E. Left axilla, 99.4°, M.; 101.4°, E. On some days remarkable falls in temperature to 96°, 95°, and even 94° and 93°. Average head-temperatures above the normal: for stations on right side of head averaging about 97°; on left side, about 94.3° F. | Gumma. A twin-tumor, each mass about two-thirds of an inch in diameter, in front of the optic chiasm. The growths involved the basal termination of the corpus callosum, the peduncles of the corpus callosum, the lamina cinerea, and anterior perforated spaces. They also probably encroached upon the roots of the olfactory nerves, the optic nerves and commissure, and the anterior portions of the circle of Willis, which seemed to have been broken in front. The base of the brain, from the posterior line of the tumor backward to the pons, was markedly softened. Microscopical sections of optic nerves showed the appearances peculiar to descending neuritis in a somewhat advanced stage. |
C. K. Mills, Philadelphia Medical Times, March 23, 1879, in “Proceedings of the Pathological Society of Philadelphia;” also, New York Medical Record, Aug. 9, 1879, and Arch. Med., vol. viii. No. 1, Aug., 1882. |
| 95 | F. 21. | Suffered for three years from excessive thirst and polyuria, with occasional vague pains in the head. A constant relation existed between the amount of fluid imbibed and of urine passed. Specific gravity of urine, 1002. No albumen nor sugar. Eight liters of urine passed in the twenty-four hours on an average. Slight headache and dimness of vision shortly before death; no other nervous symptoms. No ophthalmoscopic examination was made. | Sarcoma. About the size of a chestnut at the base of the brain, at a spot corresponding to the sella turcica. It had caused complete degeneration of the optic chiasm, and had encroached considerably on the circle of Willis. |
F. Fazio, Il Morgagni, quoted in Med. and Surg. Rep., vol. xlii., May 8, 1880, p. 415. |
| 96 | F. 73. | Suffered for several years from post-nasal catarrh, with enlargement of tonsils and granular pharyngitis. Fulness in right side of throat; muco-sanguinolent discharge from post-nasal space; bulging of soft palate. Severe pain through the right side of the head. Deafness of right ear and dimness of right eye. Mental failure. Paresis of levator palpebræ superioris and orbicularis; complete paralysis of external rectus; possibly slight paresis of the muscles supplied by the third nerve of the right side. Diminished sensibility of right half of face and cornea, and conjunctiva of right eye. Cornea opaque; conjunctival catarrh; vision almost nothing; ophthalmoscopic examination could not be made. Left [p. 1089] eye showed some diminution in acuity of vision, with concentric narrowing of visual field; pigmentation. | Lobulated epithelioma. Involved the cribriform plate of the ethmoid bone, the whole of the body of the sphenoid, and the anterior part of the basilar process of the occipital bone. These were softened to the consistency of cheese. Membranes and cerebral substance firmly adherent to the base of the skull at the inner portion of the bottom of the right cerebral fossa. Blood-clot in one of the large arteries of the optic papilla. Sclerosed blood-vessels. Atrophy of optic nerve and retina. |
W. Pepper, Trans. of Philada. Path. Soc. for 1878-79, vol. ix. p. 138. |
| 97 | F. 25. | Headache (for six years), with vomiting. For three years had dimness of vision. For a year had blindness. Exophthalmus, with dilated pupils and fixation of eyeballs. Painful spasm of right face occasionally. Occasional paresis of left arm and leg, with pain. Severe vertical headache. Anosmia. Involuntary discharge of urine and feces. Convulsions. Stupor. No local paralysis of face or extremities. Death happened unexpectedly. | Cancer. Tumor apparently springing from pituitary body, passing through infundibulum into right lateral ventricle. Tumor was “almost the shape and size of goose-egg.” It occupied anterior half of ventricle, and flattened out thalamus and corpus striatum. By pressure it had flattened the olfactory and optic nerves. The growth extended into the sphenoidal fissure, causing absorption of bone. |
Habershon, Med. Times and Gaz., 1864 (2), pp. 463, 464. |
| 98 | M. 44. | No symptoms during life indicating any brain disease. The patient had died of phthisis. | Osteoma. Consisting of true bone with Haversian canals, occupying position of infundibulum and corpora albicantia, which were totally absent. Not connected at all with dura mater. The pituitary body was apparently healthy. |
Bristowe, Tr. Path. Soc. Lond., vi. 25. |
| 99 | F. —. | Intense supraorbital neuralgia. Paralysis of the parts supplied by the third, fourth, fifth, sixth, seventh, and eighth nerves of the left side. The muscles moving the tongue not affected. No interference with respiration or the action of the heart; no choked discs. External tumors on each side of the neck, with a protuberance of the left eye. | Involved the petrous portion of the temporal bone, with a portion of the sphenoid bone of the left side, size of walnut. | James H. Hutchinson, Philada. Med. Times, vol. xiii., Sept. 22, 1883. |
| 100 | F. 66. | One-sided convulsions; first left leg, next left arm. Slow, syllabic speech, not aphasic. Abnormal, prolonged somnolence, followed by voracious appetite. Later, incontinence of urine. Apathetic. Muscles of left half of body, especially arm and leg, contractured. Pupils contracted. No facial paralysis. Slight ptosis upon right side. Conjugate deviation of eyes to right; fixed and immovable. Head drawn to right and backward. Extremities cyanotic and cold. Accentuated aortic sound; abdominal tympanitis. Taste, smell, hearing doubtful. Sensibility retained. Electric irritability rapidly exhausted; reflexes diminished. Unable to stand; constant tendency to turn to right. No albumen or sugar. All symptoms intensified; exhaustion; temperature below normal; death. | Sarcoma. Growing from right half of fossa of body of sphenoid bone, and extending outward and backward along petrous bone, only closely adherent at basilar portion of sphenoid. Slight depression of middle peduncle of cerebellum near entrance to pons. Basilar artery pushed to left. Vessels thick and rigid. Gyrus fornicatus of right side, temporal aspect, compressed. Right peduncle of cerebrum compressed. Brain-substance dense; numerous serous cysts in brain and ganglia. |
Petrina, op. cit. |
DEFINITION.—Under Spinal Tumors will be included the growths or adventitious products which arise in the substance of the spinal cord or spring from its envelopes, membranous or bony, in such manner as to directly or by pressure involve the spinal cord. Tumors strictly confined to the cord are extremely rare. First in order of frequency are the new growths which develop from the spinal membranes, either the dura mater or pia mater, most frequently the former. Tumors originating in the bony spine, like those of the substance of the cord, are comparatively rare.1
1 A “Table of Fifty Cases of Spinal Tumor” (which will be frequently referred to) is appended to this article.
ETIOLOGY.—Under the predisposing causes of spinal as of intracranial growths are such diatheses or constitutional affections as cancer, tuberculosis, and syphilis. Under Pathology a table will be given from which it appears that of 50 tabulated cases, 3 were cancerous, 5 syphilitic, and 4 tubercular.
Traumatisms, such as a fall from a height, a blow on the back, a wrench or twist of the spine, or a sudden concussion as in a railway accident, sometimes serve as exciting causes of spinal tumors. Even when a diathetic or infectious predisposition exists, the patient might frequently escape from the special intraspinal localization of the disease were it not for the accidental infliction of direct injury to the axis. When no special predisposition is present, an injury is more likely to produce an osteoma, fibroma, or sarcoma than some of the other forms which will be mentioned, such as a glioma, myxoma, neuroma, or psammoma.
Spinal tumors are said by most authors to occur much more frequently in the male than in the female sex. Our tabulated cases, however, gave 22 cases among males, 21 among females, and 7 in which the sex was not given.
Fifty cases of spinal tumor gave the following result as to age:
| Under 10 years | 4 | cases. |
| From 10 to 20 years | 3 | cases. |
| From 20 to 30 years | 7 | cases. |
| From 30 to 40 years | 12 | cases. |
| From 40 to 50 years | 10 | cases. |
| From 50 to 60 years | 6 | cases. |
| From 60 to 70 years | 1 | case. |
| Age not given | 7 | cases. |
| 50 | cases. |
SYMPTOMATOLOGY.—Can tumors of the spinal membrane be separated by a study of symptoms from intramedullary tumors? While this may be theoretically possible, in practice it will be found difficult, and of little value even when it can be done. The spinal canal is of such narrow calibre that a growth of any size either in the membranes or the cord itself will soon directly or indirectly involve both. On this subject Erb2 speaks as follows: “The attempt has thus far been made in vain to secure, from amongst the individual symptoms, at least a few fixed points on which to base the diagnosis of intramedullary tumors. The following have been claimed as such: A somewhat long antecedent history of active local manifestations of irritation, belt-like pains, eccentric pains, definite paræsthesiæ, local paralysis, as in meningeal tumors; early and well-marked atrophy, which points to a larger involvement of the gray substance; striking fluctuations in the course of the disease, spontaneous improvement, and equally spontaneous growing worse again (Schueppel); and, finally, Schueppel has also tried to connect the occurrence of scoliosis (curvature of the spinal column to the side on which the tumor is situated) with the presence of a tumor. In this he is doubtless wrong, as this manifestation merely depends on unilateral paralysis of the muscles of the back, which may depend on all sorts of causes.”
2 Ziemssen's Cycl. Prac. Med., Am. trans., p. 754.
In the discussion of symptomatology and diagnosis which follows therefore no effort will be made to separate the phenomena of meningeal and intramedullary growth. In most cases the symptoms indicate involvement early of the membranes, and later compression of the cord.
The symptomatology will differ according to the stage of the affection. The symptoms can be arranged into those of a first or early, a middle, and a late stage. As a rule, but not invariably, the symptoms of the early stage are those of beginning irritation—such sensory phenomena, for instance, as pain in the parts supplied by certain nerves in the neck, arms, hands, abdomen, legs, or feet. This pain is sometimes associated at an early period with more or less stiffness, which later may become well-marked contracture. Pain in the back is occasionally an early symptom. Paræsthesiæ, as numbness, formication, constriction or girdle sensations, coldness or heat or alternations of hot and cold feelings, are sometimes early symptoms, but occur in a more positive manner in the middle stages of the progress of the spinal growth. Hyperæsthesia is more likely to be pronounced in the middle stage of the disease. A slight paresis, which may vary a little from day to day for a time, slight twitchings or spasms, usually localized to certain muscles or groups of muscles, are also present, in some cases as an incipient manifestation. The presence of these motor symptoms will depend largely upon the location of the incipient growth with reference to the columns of the cord.
One general point of differentiation between intramedullary and membranous tumors is the fact that irritative phenomena, such as pain in the back and along nerve-tracts, spasmodic twitchings, etc., are not likely to appear as early in the intramedullary cases as in the meningeal or mixed forms.
In the middle period of the progress of a spinal tumor the irritative phenomena, such as pain, paræsthesiæ, hyperæsthesia, twitchings, cramps, stiffness, and paresis, will be found to persist and increase, and in [p. 1092] addition other manifestations will appear, chiefly those of compression of the cord. Anæsthesia frequently develops, and, when the posterior segment of the cord is the one chiefly implicated, soon becomes profound; it is, however, often variable in distribution for a time, and sometimes shows peculiar areas. One leg or one arm may be partially involved, or both lower or both upper extremities, or certain portions of any one of the limbs. Anæsthesia dolorosa—that is, absence of sensation to objective tests, although the patient suffers pain or distress in the affected part—is common. Hyperæsthesia, best observed in this middle period, is sometimes cutaneous, but in other cases follows certain nerve-trunks, probably indicating a neuritis descending from the seat of the spinal growth. In this and in the last stage the paresis advances to more or less complete paralysis, which is also variable in distribution according to the localization of the growth. Contractures and rigidity come on and changes in the reflexes now become important symptoms. These may be increase of knee-jerk with ankle-clonus, or diminished or abolished knee-jerk, according to the position and the extent of the lesion.
The late symptoms of spinal tumors, especially of those which are slowly developed, are—usually profound anæsthesia and paralysis of the limbs, with rigidity and contractures, atrophy, marked changes in the spinal reflexes, bed-sores, paralysis of bowels or bladders or their sphincters, impotence, œdema, dyspnœa, vomiting, cardiac palpitation, cystitis, and pyelitis, and, when the lesion is near the medulla oblongata, dysphagia and certain intracranial symptoms, as amblyopia, diplopia, deafness, contracted pupils, affections of speech, etc.
The size of the growth and the rapidity of its development will of course influence the character and the time of appearance of certain symptoms. According to the position of the growth, either as to its level in the spinal axis or as to its relative position to the various longitudinal segments of the spinal cord, the symptoms will also differ at special stages. These differences will appear as symptomatology and diagnosis are now further considered.
Pain in the back occurs, but is not as frequent a symptom as eccentric pain. Unlike headache in intracranial tumors, it is not a constant symptom. The headache of brain tumors is due in part at least to the conditions of tension which are produced by the growth interfering with the balance of pressure within the skull. Headache is also, as has been pointed out in the article on Brain Tumors, frequently due to the irritation of the membranes; but in this case the one great nerve through which pain expresses itself is the trigeminal, which has its distribution both within the skull and outside of it to all parts of the head. In spinal tumors the pains are more likely to be eccentric, because of the limited character of the lesion and the almost exclusively peripheral distribution of the nerves. Twisting the trunk or jarring the spinal column by blows on the head will sometimes cause pain along the spine, most frequently when the bone is involved. It sometimes cannot be elicited.
Leyden3 pointed out the fact that the movement of the spinal column is often difficult and painful in a certain direction, because this motion brings a greater pressure upon the tumor.
3 Quoted by Erb.[p. 1093]
Pain on percussion over the spinal column might be expected from the character of the affection, but has not been frequently reported. Like spinal hypersensitiveness and inflexibility with muscular rigidity, it is much more to be expected in those cases in which the vertebral bones and cartilages are implicated.
Constriction or girdle sensations are of comparatively frequently occurrence. When the cervical cord is involved, choking sensations or a sense of constriction about the neck are common. Tumors located in the lower cervical and dorsal region give girdle sensations most frequently in the chest or abdomen. So far as the assistance afforded by such sensations toward localizing the exact level of the growth is concerned, however, it must not be forgotten that curious and unexpected conditions sometimes occur. Thus, in one case (Case 16) a myxoma at the level of the sixth and seventh cervical vertebræ caused constriction sense about the legs and abdomen, and in another (Case 44), a glioma of the filum terminale, constriction of the chest.
The paralytic phenomena of spinal tumors have certain peculiarities which are not exhibited by any other spinal or by cerebral affections. A glance at the clinical history of a number of cases shows that many of them began with paresis of a single limb or part of a limb, in addition to the irritative phenomena. This paresis deepens after a time into complete paralysis, or before this occurs one or more of the other extremities become paretic. The progress toward bilateral paralysis may be comparatively rapid. The appearance and progress of the paresis or paralysis vary somewhat according to the level of the cord at which the tumor is located. In tumors of the cervical cord the paresis usually, but by no means invariably, first attacks the upper extremity. The fact that the arms are first the seat of irritative phenomena and paresis is in a case of spinal tumor indicative of a cervical location or a location in the upper dorsal region; but, on the other hand, not a few cases are recorded in which in tumors in these locations the loss of power first exhibited itself in one or both of the lower extremities. These cases are to be explained by the manner in which the descending motor tracts are affected directly or by pressure. In mid-dorsal tumors and those below this level the paresis shows itself first in the legs, and generally becomes before long a complete paraplegia.
To Brown-Séquard, more than to any other observer, we owe our accurate practical knowledge of unilateral lesions of the spinal cord, both in the cervical and other regions. When the lesion is localized in one lateral half of the cord and is situated in the cervical region, we have the affection known as spinal hemiplegia. The main symptoms of this affection are motor paralysis of the arm and leg on the side of the lesion and anæsthesia of the opposite limbs. Sensory fibres decussate in the cord soon after entering it, while the motor tracts cross at the anterior pyramids of the medulla oblongata; in which physiological facts we have a simple explanation of the peculiar motor and sensory phenomena presented by such a case. When the lesion is below the cervical portion of the cord, instead of spinal hemiplegia we have the affection known as spinal hemiparaplegia, in which the paralysis and hyperæsthesia in one lower extremity stand out in strong contrast to the anæsthesia and retained muscular power in the other. With a lesion so strictly localized as a spinal [p. 1094] tumor it might be expected that these crossed phenomena would present themselves in some cases. They are recorded, more or less distinctly, in Cases 4, 16, and 38, and it is probable that they would have been more frequently observed if they had been anticipated and looked for carefully.
Ataxia does not seem to have been a frequent symptom in reported cases. It has probably been sometimes overlooked or confounded with paresis. In a case of myxoma of the dura mater in the left dorsal region ataxia of both leg and arms was present; but in this case, however, the dura mater of the brain contained fluid and lymph. In the light of the commonly accepted views as to the physiology of the spinal cord regarding the posterior columns, as related in function both to co-ordination and sensation, ataxic manifestations might be frequently expected. Owing, however, to the narrowness of the spinal canal, compression of the entire cord takes place so early as to make paretic symptoms displace those of ataxia.
Atrophy which varies in distribution according to the extent of the destructive involvement of the cord is frequently present. In a few instances the atrophy will be of certain muscles or muscular groups. When true atrophy is present the anterior horn will be involved directly or indirectly, and accompanying changes in the electrical reactions will also be found.
The electrical condition of the atrophy of the paralyzed parts will vary with the extent of the trouble produced by the tumor. In a case of tumor of the cervical enlargement, for instance, producing more or less paralysis both of the upper and lower extremities, reactions of degeneration will be present only in the muscles supplied by the nerves which spring directly from the seat of lesion.
Spontaneous twitchings or spasms due to irritation of motor-centres or tracts are comparatively frequent. More or less permanent contracture in a limb or part is of frequent occurrence, particularly after the growth has advanced. Forms of torticollis or retraction of the head, strong flexures of the arms or legs, and, late in the history of many cases, complete and extremely painful drawing up of the limbs upon the body, may occur. Persistent subsultus was observed in one case, a glio-myxoma involving the gray columns from the medulla oblongata to the cauda equina. Fibrillary twitching is rare, and in our tabulated cases was observed only in one instance, a glioma of the filum terminale. General convulsions with unconsciousness are exceedingly uncommon. In one case, however, a round-celled sarcoma at the level of the seventh, eighth, ninth, and tenth cervical vertebræ, the patient is recorded as having died in a fit. Nystagmus was observed once, but probably had no significance so far as the spinal affection was concerned, as the cerebral dura mater exhibited evidences of inflammation.
The condition of the reflexes, both cutaneous and tendinous, is often peculiar and almost diagnostic, but varies greatly according to the position and extent of the lesion. Increase of reflex action is sometimes a marked symptom. The slightest irritation of the soles of the feet, the calves of the legs, palms of the hands, or other special regions will often produce decided contractions, and sometimes that symptom which has been designated by Brown-Séquard as spinal epilepsy, in which both lower extremities are thrown into violent clonic spasms, which may last [p. 1095] for many seconds or even minutes. In tumors of the dorsal region causing marked compression and preventing cerebral inhibition, clonus and knee-jerk are also markedly exaggerated. The so-called diplegic contractions—that is, contractions in one extremity from irritation of the other—are observed, especially when a transverse area of the cord, large or small, is involved in an irritative or inflammatory process. They probably result from the abnormal facility of transmitting impressions which has been acquired by the cord. When the cervical or the lumbar enlargement of the cord is completely compressed or destroyed by a tumor, reflex activity is diminished or abolished in the region supplied by nerves originating at the seat of lesion.
Alterations in the body-temperatures have been frequently noted in lesions of the spinal cord, such as fractures of the vertebræ and inflammatory changes in the cord and its membranes. Some of the observations are almost incredible, as that of J. W. Teale,4 who records an axillary temperature of 122° F. The subject has been somewhat obscured by physiological speculations. Thus, it has been asserted that paralysis of motor centres and strands causes an increase of temperature, while paralysis of sensory tracts produces a diminution. The accepted clinical facts apparently are as follows: after crushing the cervical cord a uniform rise in temperature occurs if peripheral cooling is prevented. This rise is caused by a paralysis of the vaso-motor nerves, which permits a paralysis of the vessels and floods the parts with blood. This assumes, of course, that mere increase of blood in a part means increase of heat. After a variable period this increase is followed by a decrease which is permanent. Hutchinson records5 a case of fracture of the cervical spine at the fifth vertebra in which the patient's body felt almost as cold as a corpse and the rectal temperature was only 95° F. In Cases 4 and 16 the affected parts are recorded as cold, just as in atrophic and other lesions of the cord. The tabulated cases do not show many exact thermometric observations, but in Case 8 the average temperature for two weeks before death is given as slightly below normal, while Case 7 shows a sudden rise on the day preceding death. It is probable that the permanent decrease following crushing and compressing lesions would also be found in cases of spinal tumors. The following exact observations, made by one of us6 upon a case of injury to the cervical cord, are directly illustrative of this subject. The case was of several months' standing. The patient could walk imperfectly, and the right arm was more paretic than the left. The observations were made at 10 o'clock A.M. on six successive days:
| Right Axilla. | Left Axilla. | |
| First observation | 98.2° | 97.3° |
| Second observation | 99.8° | 98.2° |
| Third observation | 96.4° | 96.2° |
| Fourth observation | 95.6° | 96.4° |
| Fifth observation | 97.2° | 96.8° |
| Sixth observation | 95.2° | 93.8° |
It will be seen that the temperatures range higher in this series on the more paretic side; but this did not hold in a series taken a few weeks [p. 1096] later. The fact is to be noted that all these temperatures, with one exception, are below the normal.
4 Lancet, March 6, 1875.
5 Ibid., August, 1875.
6 Hospital Gazette, Nov. 7, 1879.
Cystitis, pyelitis, and pyelo-nephritis are usually secondary symptoms, due to retention of urine, distension of the bladder, etc. in consequence of paralysis of this viscus. Bed-sores result in two ways: in the first place, they may be due to emaciation and immobility and the uncleanliness which it is almost impossible to prevent; or, in the second, trophic eschars may arise because of the involvement of nutritive regions of the cord. The so-called sacro-ischiatic eschars are of this character. Febrile phenomena, such as chills, increased temperature, increased respiratory action, are frequently secondary phenomena due to bed-sores, cystitis, continued pain, exhaustion, or septic infection.
Priapism was recorded in two of the fifty cases, both tumors of the cervical cord. Impotence was only recorded once, a dorsal myxoma. It is probable that both priapism and impotence, particularly the latter, were present, but overlooked in other reports.
Headache was present in three of fifty cases. One of these was a fibro-sarcoma at the level of the fourth cervical nerve; the other two were low down in the spinal axis, one in the lumbar enlargement, and the third, strange to say, in the filum terminale. Vertigo is a rare symptom in the spinal tumors. In one case in which the growth was located at the position of the third cervical vertebra its presence was recorded.
Out of five cases in which vomiting was present, two were in the cervical regions, one in the dorsal, one in the lumbar, one in the filum terminale.
Tumors involving the upper cervical and bulbar region of course will give rise to special symptoms indicating more or less involvement of cranial nerves.
Unfortunately, very few ophthalmoscopic observations have been made in cases of spinal tumor. Optic neuritis has been found in a few cervico-dorsal cases, and in other cases located in the same region no ophthalmoscopic alterations have been discoverable.
Mental disturbances were only especially recorded in four of the fifty cases. Such symptoms were certainly not of frequent occurrence, except those emotional manifestations which were due to the great suffering which the unfortunate patient was called upon to endure. These emotional disturbances, as in all forms of painful disease, varied according to the mental stamina of the patient. In one case the mental symptoms, in association with other phenomena and a probability of dog-bite, led to the suspicion of hydrophobia.
In one case (31) an interesting observation was made of an anal sphincter reflex, with frequent stools. The tumor in this case is reported at the level of the tenth dorsal vertebra, which would be at the level of the eleventh dorsal segment. The tumor was tubercular, and therefore probably meningeal, so that the irritation to the anal centre, which is in the lumbo-sacral segment, may have been caused by extension of inflammation along the meninges.
PATHOLOGY.—We present in tabulated form the various kinds of tumors as found in the fifty cases which have been collected:
[p. 1097]| Aneurism | 1 | Myxoma | 2 |
| Cancer (?) | 2 | Neuroma | 1 |
| Carcinoma | 1 | Organized blood-clot | 1 |
| Cysticercus and hydatids | 3 | Osteoma | 1 |
| Cyst (Dermoid?) | 1 | Phlegmon | 1 |
| Fibroma | 5 | Psammoma | 2 |
| Glioma | 5 | Sarcoma | 7 |
| Gumma | 5 | Tubercle | 4 |
| Myo-lipoma | 2 | Unclassified | 6 |
It will be observed that the predominance in this list is decidedly in favor of the sarcomata and structures which are likely to be associated with or to graduate into them, such as the gliomata, myxomata, and the psammoma. In one instance the resemblance (Case 15) to psammoma is referred to by the reporter. The comparatively large number of unclassified, and the two cases referred to vaguely as cancer, would probably, on more exact report, have added several more to the group of the sarcomata. The table shows that next in frequency come the fibromata and gummata, while the carcinomata have but a single representative in the group. Tubercular tumors occurred with comparative frequency, no less than 8 per cent. being recorded. Although the exact origin of only somewhat more than one-half (29) of all the tumors is given, it is stated of this fraction that 17 sprang from the membranes, while of the remainder 8 were located in the cord itself and 4 in the vertebræ. Of the 3 oases of parasitic invasion, it is recorded of one (Case 43) that a hydatid cyst was also found in the liver; and it is probable that in any given case the spinal cord would not be the only part to suffer. Cobbold's work refers to one case of hydatid of the spinal cord. Erb refers to 13 cases, all but 2 external to the dura mater. In Case 43 of the table pains in the back and hip, simulating rheumatism, were present early.
The dimensions of the spinal tumors of whatever character are never very great, for the reason that they have but little space in which to enlarge, and that their presence soon causes such grave changes as to be incompatible with life. They rarely exceed an inch in their longest diameter, and not unfrequently are smaller than this. There is usually about them a more or less marked meningitis and an area of vascular fulness. Œdema of the membranes is sometimes noted. The substance of the cord beneath is compressed, atrophied, or softened, and this softening sometimes extends for a considerable distance both above and below the neoplasm. These changes were reported in Case 8, in which there was the addition of an abscess. Secondary degenerations would probably be found in all cases, unless very recent; and these changes, following the Wallerian law, would ascend the posterior and descend the lateral columns. Such degenerations are reported in some of the cases. The spinal nerves are sometimes compressed and atrophied. Old or recent hemorrhages are found, as in Case 18. Among the changes which occur, probably at a late stage, are the formation of cysts, either large or small, either in the substance of the cord or consisting simply of a dilatation of the central canal of the cord. This condition is known as syringo-myelia, and is of exclusive pathological interest. In Case 1 is recorded, apparently, a well-marked dilatation of the central canal (hydromyelus), and cyst-formation is recorded with gliomata, sarcomata, and gummata in other cases. Caries of the vertebræ is recorded in a number of cases, and occurred both in cases of gumma (Case 8) and carcinoma (Case 14). These cases were, however, exceptions to the general rule that the bony envelope of the cord does not furnish external [p. 1098] evidence of the location of the tumor. It is worthy of note that the one instance of phlegmon or inflammatory exudate (Case 20) also presented infiltration of the tissues of the throat and mediastinal space. A case of organized blood-clot (Case 39) has been included in the list, although, properly, a spinal hemorrhage, because it became and acted as a tumor. The location of the single case of aneurism (Case 48) is not given. The symptoms were those of tumor in the dorsal spine.
As sequelæ of tumors of the cord may be mentioned especially bed-sores, which sometimes commit frightful ravages, as in a case (37) in which the spinal canal was laid open. The bronzing of the skin and diseased condition of the suprarenal capsules, as recorded in Case 41, were mere coincidences, and not probably at all connected in pathological sequence with the spinal lesion. Cystitis, pyelitis, and pyonephritis are not uncommon in cases of tumor of the cord, just as they are observed in other compressing and destructive lesions of that organ. In those cases in which the tumor is the result of a general taint, as in gummy and tubercular growths, the evidence of this taint is not usually wanting in other organs; thus in Case 37, of tubercle of the cord, tubercles were also found in the lungs, bowels, and uterus. In gummata of the cord it would not be likely to escape careful inquiry that the patient's history or his body presented evidence of the disease.
In a case (47) of congenital sacral neuroma amyilinicum the infant was also hydrocephalic and had a bifid spine—conditions of faulty development with which the patient cannot long survive.
In one case of psammoma (Case 5) a resemblance to endothelioma is noted, while in another (Case 15), already referred to, a sarcoma is said to have resembled a psammoma.
Vascular changes are usually notable. In addition to the congestion already spoken of, it is recorded in one case (No. 14) that the right vertebral artery was obliterated. This was a carcinoma which had partly destroyed one vertebra.
Virchow's case (No. 50) of a stillborn child with a large tumor of the size of the head of a child of two years, and containing bone, has some analogies in three cases, referred to by that author, in which both hair and bone were found.
In several cases a brown or yellow exudate (plastic lymph?) is mentioned as extending along the cord far beyond the immediate neighborhood of the tumor.
The histology of tumors of the whole cerebro-spinal axis will be found described in the article on Tumors of the Brain.
DIAGNOSIS.—The diagnosis of tumors of the spinal cord presents itself naturally under two heads—the differential, or general, and the local diagnosis. The conclusions reached in this paper are based on a careful study of the cases appended, two of which were personal observations, and the remainder were collected from American, English, French, and German literature. It cannot be denied that much obscurity rests upon the diagnosis of tumors of the spinal cord, and that the doubts expressed by Erb and other writers have much to support them. It is hoped that the systematized study presented in this table will do something to dispel this obscurity.
(1) General Diagnosis.—The differential diagnosis has regard first to [p. 1099] certain general phenomena which are broadly indicative of a spinal disorder as distinct from a cerebral or peripheral one. Thus, mental symptoms are absent, or if present are an accompaniment of tumors high up in the spinal axis, are the results of suffering, or appear very late in the disease because of progressive weakness. Briefly stated, the phenomena which point with comparative certainty to the existence of spinal tumors are symptoms of meningeal irritation gradually increasing, and symptoms of slow compression of the cord. These have been sketched at the beginning of Symptomatology. As to duration, the data in the cases studied were somewhat meagre. The usual duration is from six months to three years.
The differential diagnosis of spinal tumors will be considered in reference to the following affections: congestion, hemorrhage, meningitis (simple and specific), caries, traumatisms, sclerosis, aneurisms, neuritis, metallic and infectious disorders, and hysteria. Spinal tumors, it will be recalled, are from constitutional or special causes, as syphilis, cancer, and tuberculosis. The onset is gradual and irregular. The duration is comparatively long. The progress is by irregular advances toward a fatal termination. The symptoms are inclined to be at first unilateral or local; later, bilateral. Special symptoms, as paralysis, spasm, sensory and visceral disorders, occur irregularly as to time. Decubitus and trophic changes are common late in the history. Reactions of degeneration are often present. Gowers refers to the fact that two morbid processes often occur, one consecutive upon the other, as a secondary degeneration or a hemorrhage, after the establishment of the morbid growth, with characteristic increase of symptoms.
In spinal congestion a constitutional cause is not likely to be present. The onset is usually sudden and after exposure. The duration is shorter than in tumors, and is from a few days to four months. The disease is stationary for a while; then retrogression of symptoms toward recovery occurs. The symptoms are more uniformly bilateral, and motor and other symptoms develop about the same time. Decubitus is rare. Reactions of degeneration are rare (?). It is desirable that cases of so-called spinal congestion should be differentiated from the forms of peripheral neuritis above referred to, the most characteristic symptom of which appears to be tenderness of nerve-trunks.
In spinal hemorrhage there is no special history, or a history and signs of cardiac and vascular degeneration may be present. The onset is quite sudden and the progress of the case regular. The first symptoms persist, and secondary degenerations follow, and differ according to the extent and location of the lesion, but are most likely to be uniformly bilateral.
In meningitis the symptoms of localized compression are absent. The girdle symptom is absent. The affection is sometimes curable, and especially so if it has been of syphilitic origin. The reactions of degeneration are not marked.
In caries of the spinal vertebræ deformity is rarely absent, especially if the case has continued a few months. Rigidity of the muscles of the back is an important symptom, which, however, is occasionally found with tumor. Jarring of the spinal column by tapping upon the head or jumping from a chair or stool is more likely to elicit pain in caries than [p. 1100] in tumors. Strumous symptoms and evidence of tubercles in the lungs or other organs are often present.
In traumatisms usually a history of the injury can be obtained. The symptoms are those of caries, myelitis, meningitis, or of combinations of these, according to the character of the case.
In sclerosis the symptoms are usually those of progressive systemic affections, with absence of compression symptoms. The duration is longer. The progress is gradual and more regular.
Aneurisms are only to be distinguished when extra-spinal, causing erosion and compression.
In neuritis there is the soreness of the nerve-trunk already referred to, while compression symptoms and visceral disorders are absent. The motor and sensory symptoms are confined to the area of distribution of the affected nerve. It is amenable to treatment. In advanced stages the reactions of degeneration are marked. In the form of general peripheral neuritis, the existence of which, as a distinct disease, is being at present claimed, the characteristic symptoms are as yet not sufficiently determined or the pathology demonstrated by post-mortem research to admit of much discussion.
In metallic and infectious disorders a history of definite causation is present. Metallic disorders may present special distinctive signs, such as lead-line, wrist-drop, etc.
In hysteria a precedent characteristic history is usual. The onset is often sudden and an emotional element is present. The symptoms are bilateral and protean. Trophic changes are absent. No reactions of degeneration are present.
(2) Local Diagnosis.—It may be said of spinal tumors in a modified sense, as it can be said of brain tumors, that they are not good pathological experiments for illustrating the functions of the exact areas which they occupy. The spinal canal has such narrow limits, the tumor itself soon attains such a relatively large size and causes such wide vascular engorgement, and the different tracts and systems of the cord are so closely packed together, that the tumor does not often invade only one functional area and escape another. Hence the regional diagnosis presents special and greater difficulties than the diagnosis of the level of the cord at which the tumor presents itself. A tumor which destroys the trophic centres for the arm in the anterior cornua might exert sufficient backward pressure to paralyze the motor tracts running to the leg; or a cervical tumor, as in Case 5, might produce symptoms which are almost wholly observed in the legs. It will be seen, however, by reference to the table, that in Case 3, reported by Wilks, we have a tumor whose exact anatomical seat could have been predicted, and which seems to have reproduced almost the upper-arm paralysis of Remak. When we compare these two cases, in which the pathological conditions are so similar, it will be observed that the paralyzed arm is much wasted, which indicates a lesion of its trophic centre, whereas the affected legs in the other case are irritated by pressure and by isolation, but are not wasted, because their trophic centres are far below the point of lesion. The invasion of the trophic centres, and the accompanying wasting of particular groups of muscles, especially when this occurs early in the case, with the consequent reactions of degeneration in these muscles, would furnish very valuable indications [p. 1101] both as to the region and the level of the cord involved (Case 29). Unfortunately, the exact observations are wanting in most of the cases as reported.
M. Allen Starr, in a recent paper,7 has devoted much labor to the elucidation of the functions of different segments and regions of the cord. He demonstrates the existence of groups of cells in the gray matter, especially in the anterior horns, each of which he believes constitutes a physiological unit. He affirms that these cell-groups preside over certain associated movements or combinations of certain muscles, and, quoting from Spitzka, says that “the nearer a muscle is to the ventral aspect of an animal the nearer will its nucleus be to the median line of the cord; and the nearer the muscle is to the dorsal aspect of the animal the nearer will its nucleus be to the lateral cornua of the cord. Flexor nuclei are therefore in internal, extensor nuclei in external and posterior, cell-groups.” The only light that such a theory throws upon the subject of diagnosis is by affording a possible explanation of the fact that spastic flexion is much more common than spastic extension, and may be due to the fact that the cell-groups for flexion lie deeper and are more protected than those for extension; and the additional fact above referred to, that a paralysis of associated muscles or groups of muscles, with degeneration, as in the types of Remak, would indicate with great clearness the destruction of the cell-group which presides over them. Starr, in his article, also tabulates the various reflexes and their seats in the cord. As this subject is of much importance in any exact study of spinal-cord diseases, we will state here some of the facts as given in that article: The neck-pupil reflex (dilatation of the pupil on irritation of the neck) has its seat from the fourth to the seventh cervical segment; the elbow-tendon reflex in the fifth and sixth cervical; the wrist tendons from the sixth to the eighth cervical; the palmar in the seventh and eighth cervical; the epigastric and abdominal skin reflexes in the fourth to the eleventh dorsal segments; the cremasteric reflex in the first to the third lumbar; the patellar tendon in the second to the fourth lumbar, and bladder and sexual centres in same; the rectal centre in the fourth lumbar to the third sacral; the foot-clonus and Achilles-tendon reflex in the first sacral. A destructive lesion, such as a tumor, at any one of these points would cause abolition of that particular reflex, and this would probably occur early in the case. Our table of cases does not present any such observation, whereas exaggerated reflexes, such as occur from a compressing lesion above the seat of the excited centre, are recorded in abundance. Many of these deductions are of course only possible early in the history of the case, as at a late stage the secondary degenerations have caused too widespread havoc to admit of any exact localization. The distinction must also be sought for between a destructive lesion and the symptoms of irritation which it may project to distant parts. Fürstner's cases of syringo-myelia,8 in which were marked vaso-motor changes, such as pallor, flushings, copious sweat, and trophic disorders in the integument and its appendages, seem to show that a lesion in the gray matter just posterior and external to the central canal is necessary for such phenomena. Similar vaso-motor changes may be observed in some of the tabulated cases, as in No. 4, in [p. 1102] which there were islands of heat and cold in the leg, with a hydromyelia in the cord. Sensory symptoms are very common in cases of spinal tumor, but they furnish indications rather of the exact level of the lesion than of its region.
7 “Localization of the Functions of Spinal Cord,” Am. Journ. Neur. and Psych., 2-3, p. 443.
8 Quoted by Starr.
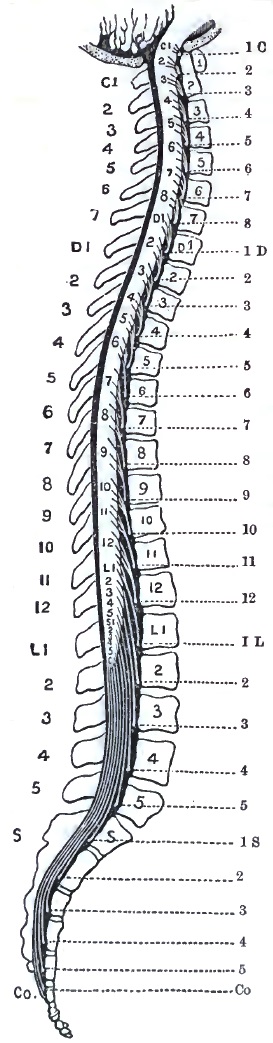

Before considering briefly the indications which point to the various levels of the cord as a possible seat of spinal tumor, it will be necessary also to make plain a few anatomical facts. It must be borne in mind, first, that the nerve-origins in the cord are never at the same level as their exits from the spinal canal, or, in other words, that the spinal segments do not correspond with the bodies of the same numerical vertebræ, and that there is, in fact, one more cervical segment than there are cervical vertebræ. The tendency is for the nerve-trunks to run downward before passing out of the canal, so that in every instance, without exception, from the medulla oblongata to the filum terminale the segments of the cord are above the corresponding vertebral body. This discrepancy increases as we descend the cord; whereas it is approximately correct to say of the cervical and dorsal regions that every segment is opposite the vertebral body which is numerically just above it, this difference becomes much greater in the lumbar and sacral regions. The cord itself terminates in the lumbar enlargement which ends opposite the interval between [p. 1103] the first and second lumbar vertebræ. All the remainder of the canal is occupied by the descending trunks of the lumbar, sacral, and coccygeal nerves as they pass to their respective foramina, constituting the cauda equina. It must be recalled, however, that the vertebral bodies, lying very deep, cannot serve as guides, but that we are dependent upon the spinous processes as landmarks in diagnosis. These again differ in their levels from their respective vertebral bodies, as they are deflected at somewhat different angles at different regions of the spine. Gowers has illustrated these facts by a very graphic wood-cut9 (Fig. 45), from which the general rule may be drawn that each vertebral spine is about opposite the spinal segment which is numerically two places below it; thus the eighth dorsal spine is opposite the tenth dorsal segment, etc. The indications afforded by this exact anatomical knowledge have reference largely to the existence of pain on pressure and to any deformity of the bony structures. The cases as reported do not indicate that this method of research has been utilized, and it may possibly be of only theoretical importance; but it has been considered worthy of reference as an indication in diagnosis.
9 Diagnosis of Diseases of Spinal Cord, p. 6.
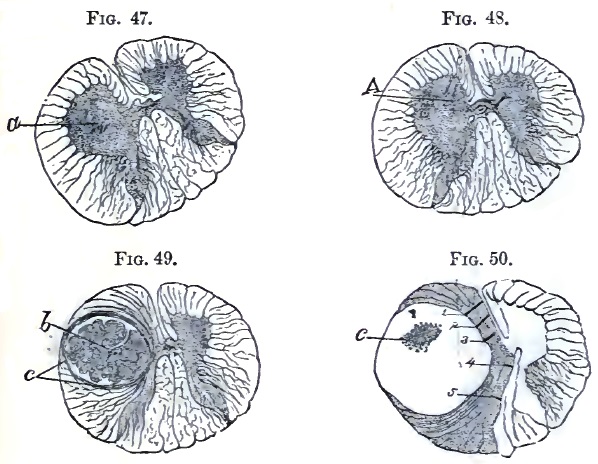
It will be seen by reference to the table that usually certain general features in the symptomatology indicate the seat of the lesion. Thus in tumors of the cervical region pain and stiffness of the neck occur, while the first appearances of paresis and sensory disturbances are usually observed in the arms and about the chest. The centres for the forearm and hand lie in the lower portion of the cervical enlargement; that for the upper arm, including the supinator longus, in the upper portion. Mental symptoms are more marked, and in Case 4 several of the cranial nerves were implicated. In the lower cervical and upper dorsal region there are symptoms of dyspnœa, fixation of the chest (Nos. 20, 22, 24), and cough. The girdle symptom is an important indication at any level, [p. 1104] as it is due to irritation of the nerves at the lowest level of healthy cord just above the transverse lesion. It has already been discussed under Symptomatology. In many of the dorsal cases (Nos. 32, 37, 38, 39, and 45) the symptoms are almost entirely confined to the legs and lower trunk, the arms escaping entirely. The condition of the bladder is usually given in the table as one of paralysis; this does not indicate whether automatic evacuation existed at the beginning of the case; which condition would indicate that the centre for micturition was below the lesion, and intact. It is probable that later in these cases the bladder is actually paralyzed by destruction of its centre in the cord, and this even when the tumor has been situated some distance above.

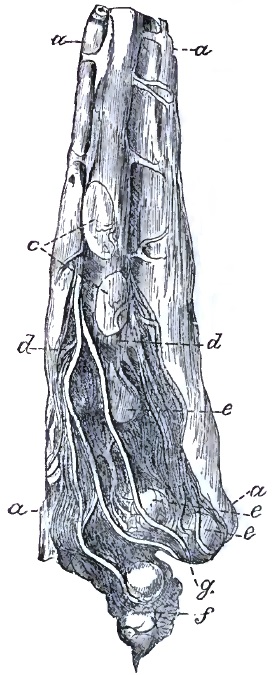
With reference to tumors of the cauda equina, Erb10 says that they have in every respect a great resemblance to those which are situated higher and affect the cord proper. “They are hard to distinguish from the latter, but may be in many cases perhaps, if it is borne in mind that tumors of the cauda produce exclusively nerve-root symptoms, and that the signs of compression of the cord, of secondary myelitis, etc. are absent. The higher the tumor, the nearer it approaches the lumbar [p. 1105] portion of the cord, the harder will it be to draw the distinction. In respect to tumors seated lower the following points may be attended to: the seat of the pains (which in such cases often attain enormous violence) is strictly localized in certain nerve-districts; all nerves leaving the spinal canal above the tumor are free; thus in myxo-sarcoma telangiectodes of the cauda I observed the pain strictly limited to the district of the sciatica, while the crural and the dorsal nerves were perfectly free; constant violent pain in the sacrum. If palsy occurs the reflex actions necessarily cease at once. Spasms are seldom observed, more frequently contractures. Atrophy of the muscles occurs rather frequently. The palsy and anæsthesia by their localization often give us the opportunity of fixing the upper limit of the lesion. Increase of the reflex acts and marked tendinous reflexions do not occur. Paraplegia, palsy of the bladder, bed-sores, etc. may develop exactly as in tumors occupying a higher seat, [p. 1106] but the symptoms of paralysis do not seem to belong necessarily to the disease, as is shown in my case (just mentioned), which terminated fatally before paralysis or anæsthesia occurred.”
10 Op. cit.
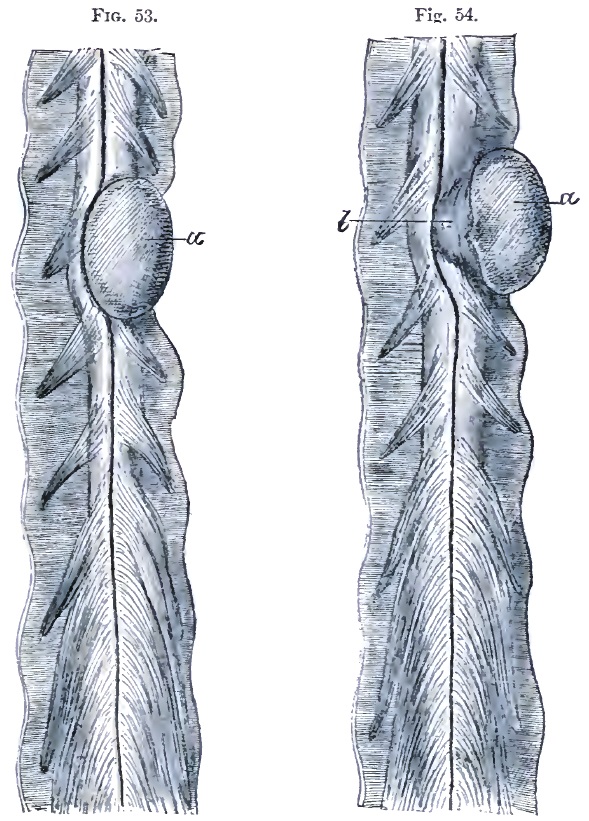
PROGNOSIS.—The prognosis of spinal tumors is generally very unfavorable. Syphilitic cases are of course the most hopeful, but even in these cases it is only when they are recognized early that much can be expected. A gumma that has grown to any dimensions will have so compressed the cord that even when the tumor is melted away by specific treatment its effects will remain.
DURATION AND TERMINATION.—Most cases of spinal tumor last from about six months to three years. Occasionally death may result, as from a rapidly-developing sarcoma, in less than six months, and somewhat more frequently in slowly-developing tumors, or in those which are held more or less in abeyance by treatment the sufferings of the patient are prolonged to four or five years or more. Hemorrhages into or around the growths sometimes take place, and are the cause of death, or more frequently of a sudden aggravation and multiplication of severe symptoms. Death sometimes takes place from the complete exhaustion which results from the disease and its accompanying secondary disorders, such as bed-sores, pyelitis, etc. Occasionally death results from intercurrent diseases, such as pneumonia, infectious fevers, etc., whose violence the weakened patient cannot well withstand. Sometimes the symptoms of a rapidly-ascending paralysis appear, probably due to an ascending myelitis or meningo-myelitis.
COMPLICATIONS AND SEQUELÆ.—Spinal tumors are sometimes complicated with other similar growths in the brain or the evidences of the same constitutional infection in other parts of the body. In one case of cysticercus of the cord sclerosis of the posterior columns was also present.
TREATMENT.—The treatment of spinal tumors can be compressed into very small compass. In cases with syphilitic history, or when such history is suspected, although not admitted, antisyphilitic remedies should be applied with great vigor. It should be borne in mind, however, that even in syphilitic cases after destruction of the cord by compression or softening specific remedies will be of no avail. In tubercular cases and in those in which the system is much run down tonics and nutritives are indicated. Bramwell11 advises an operation in any case in which the symptoms are urgent, in which the diagnosis clearly indicates the presence of a tumor, when there is no evidence of malignant disease, when the exact position of the growth can be determined, and when a vigorous antisyphilitic treatment has failed to produce beneficial results. As some meningitis, meningo-myelitis, or myelitis is usually present in cases of spinal tumor, treatment for the complication will assist in relieving the torments of the patient. Anodynes, particularly opium and its preparations, should be used freely in the later stages of the affection. Bromides and chloral are of little value except in association with opiates. Operation offers even less hope than in brain tumor, but in very rare cases should be taken into consideration.
11 Diseases of the Spinal Cord, Edinburgh, 1884.[p. 1107]
| No. | Sex and Age. | Clinical History. | Path. Anat. and Location. | Remarks. |
| 1 | M. 33. | Paresis of forearms, left worse. Paraplegia, then paralysis of all limbs; paralysis of intercostals. Contractures of hands, then of feet. Pain and stiffness of neck on motion. Wasting of interossei. Diplegic contractions of legs. Only partial paralysis of sphincters. Sensation perfect. Bed-sores. Duration, thirteen months. | Glioma; syringo-myelus. Dilated lymphatics. Entire length of cord, and involving medulla oblongata. Upper four inches of cord greatly enlarged. |
T. Whipham, Trans. Path. Soc. London, 1881, xxxii. 8-12. |
| 2 | F. —. | Constricting pains about abdomen. Paresis of legs. Persistent subsultus. Temporary improvement after labor. General paralysis. Scoliosis. | Glio-myxoma. In gray columns from medulla oblongata to cauda equina. |
Schueppel, Arch. d. Heilk., viii. Bd., 1867 (quoted by Rosenthal). |
| 3 | M. 15. | Paresis of left arm. Pain back of neck. Later, paralysis of left arm, and wasting of arm, shoulder, and neck muscles. Slight paresis of right arm. Prolonged vomiting. Constriction of neck; dysphagia; paralysis of chest. | Gelatinous tumor left side of cord, and
involving in some parts the gray matter. From medulla to sixth cervical vertebra. |
S. Wilks, Lectures on Dis. of Nervous System, p. 266. |
| 4 | M. 18. | Paresis of left leg, increasing; some atrophy. Weakness in left arm. Later, numbness in both legs. Contracture of fingers. Some mental confusion. Left hand and leg livid and cold. Hyperæsthesia of left leg; anæsthesia of right leg, perineum, penis, scrotum, rectum, and inguinal region, and of left arm. Right arm normal. Islands of heat and cold in leg, and of cold in arms. Left ankle clonus. Left pupil contracted. Vomiting. Dysphagia. Occipito-cervical pain and contracture of cervical muscles. Leg contractures and tremor. Later, hyperæsthesia disappeared. Incontinence of urine. Patellar and skin reflexes increased. Facial spasm. Amblyopia, optic neuritis, diplopia, deafness, paralysis of left abducens; pupils contracted. Sacral bed-sores. Thick speech. | Round-celled sarcoma or glio-sarcoma,
growing from ependyma of central canal, causing hydromyelia,
softening, and secondary degeneration. Dura mater thickened. Brown
exudate in cord and base of brain. From medulla oblongata to dorsal cord. |
Schultze (F.), Arch. f. Psychiat., Berlin, 1878, viii. 367-393, 1 pl. |
| 5 | F. 48. | Pain in abdomen and down legs, worse on left side. Tonic spasm in flexors and adductors of thighs. No anæsthesia. Two months before death paralysis of sphincters. Great emaciation. | Tumor (psammoma), growing from dura mater on
right side in cervical region. Upper part of cervical region. |
J. Hutchinson, Jr., Tr. Path. Soc. Lond., 1881-82, xxxiii. 23, 24. |
| 6 | —— | Pain in arms. Contracture of fingers of right, then left side. Numbness in right foot, then upward, then left foot. Girdle feeling. Priapism and dysuria. Complete anæsthesia, later, up to third rib, with paralysis of legs and paresis of fingers. Respiration diaphragmatic. Legs very jerky. Later, arms paralyzed. | Sarcoma of left post. aspect of cord;
adjacent cord compressed and soft. Belt of yellow substance enveloped
cord to cauda equina. Between cervical bulb and second cervical vertebra. |
E. Long Fox, Bris. Med.-Chir. Journ., 1883, i. 100-106, 2 pl. |
| 7 | F. 31. | Pain, stiffness in neck; pain radiating, aggravated by jarring. Sudden paralysis of both arms; next day paralysis of legs, incomplete. Partial anæsthesia. Marked skin reflexes in legs. Patellar reflexes retained, weaker on right than left. Dyspnœa. Profuse perspiration. Cardiac irregularity. Day before death temperature in right axilla 100°; left, 102.2°. | Gumma of dura mater two inches long, with
intercurrent hemorrhage; flattening and softening of cord, with
secondary sclerosis. From first to fifth cervical vertebra. |
Charles K. Mills, Philada. Med. Times, Nov. 8, 1879, p. 58. |
| 8 | M. 34. | Pain in back of neck, with stiffness and torticollis. Paresis of arms; later, of legs. Anæsthesia of arms, then of legs; also paræsthesia of legs. Late symptoms: shortening and great rigidity of neck, with choking sensation (girdle sensation at neck). Dimness of vision. Atrophy of arms and less of legs. Complete paralysis of arms, almost complete of legs. Electro-contractility preserved. Violent skin reflexes in legs. Involuntary evacuations and incomplete priapism. Severe pains in knees and ankles. No acute bed-sores. [p. 1108] Paroxysms of dyspnœa. Average temp. for two weeks before death, M. 97.9°, E. 98.3°. | Gumma of dura mater; caries, probably
syphilitic, of vertebræ. Abscess. Total (almost) transverse sclerosis
of cord. Secondary degeneration. Some softening above and below tumor.
Cervical nerves compressed and atrophied. From second to fifth cervical vertebra; most in front. |
Charles K. Mills, Philada. Med. Times, Nov. 8, 1879, p. 58. |
| 9 | M. 43. | Pain between shoulders. Numbness in right hand and arm, with weakness and swelling. Numbness in left arm, which spread over chest and abdomen. Unable at first to lie down. Felt as though encased in armor. Pain in back of neck. Tongue protruded to right. Exaggerated reflexes in legs. Right arm and leg weaker than left. Vertigo. Dysphagia. Sense of constriction about neck. Breathing impaired. | At third cervical vertebra, to right of front of cord. Destruction of opposite vertebra. | E. H. Clark, Bost. Med. and Surg. Journal, 1859-60, lxi. 209-212. |
| 10 | —— | No record of symptoms especially referable to the cysticercus. Symptoms of tabes dorsalis. | Cysticercus in substance of cord. Lesions of
tabes dorsalis. On level with third cervical nerve. |
Geo. L. Walton, ibid., vol. cv. p. 511. |
| 11 | M. 25. | Pain in back of neck; stiffness. Numbness of left hand. Gradual loss of power of left arm. Jerking of arm. Paresis of left leg. Constriction of upper chest. Right limbs involved, and eventual complete paralysis of trunk and extremities. Severe headache. Last three days absolute anæsthesia of arms and legs. No ophthalmoscopic changes. Constipation and dysuria. | Fibro-sarcoma at level of fourth cervical nerves. Cord compressed. | H. A. Lediard, Tr. Path. Soc. Lond., 1881-82, xxxiii. 25-27. |
| 12 | F. 25. | Œdema of ankles; pain in legs; afterward numbness, formication, and stiffness of legs. Painful contractures in upper extremities. Slight left scoliosis. Abdominal pains. Paresis of arms. Fingers flexed. Fever. Respiration became involved, and bowels and bladder paralyzed. Mind clear. Died in attack of suffocation. Duration, two years and three months. | Fibroma, size hazelnut, under pia mater. Between fourth and fifth cervical vertebræ. |
Bernhuber, Deutsch. Klin., Berlin, 1853, v. 406. |
| 13 | M. 16. | Restlessness. Cramps in pharynx on swallowing. Excitability. Delirium. Hallucination. Pain in the neck. On touching neck general cramps. Grimaces. Salivation. In three days complete paraplegia. No fever. Sudden change. Pulse 120. Pupils alternating. Blepharospasm. Irregular respiration. Pulmonary œdema. Suspicion of hydrophobia, because patient had been with hydrophobic dog; when offered coffee had symptoms simulating rabies. | Sarcoma. Extending from fifth to seventh cervical nerve on antero-lateral face of cord, compressing left half and penetrating into right half, so that anterior longitudinal fissure described arc of circle around it. |
Adamkiewicz, Arch. de Neurol., Paris, 1882, iv. 323-336, 1 pl. |
| 14 | F. | Paresis and partial anæsthesia in all limbs for many months, most marked on left side. Brain and special senses unaffected. Had a tumor at bottom of right side of neck. Extensive bed-sore. | Carcinoma. Tumor caused partial absorption of sixth cervical vertebra. Cord compressed and twisted. Right lateral aspect especially affected. Cord atrophied. At level of sixth cervical vertebra. |
J. W. Ogle, Tr. Path. Soc. Lond., 1885, 6, vii. 40, 41. |
| 15 | F. 34. | Pain in right foot, and paresis increasing to paraplegia. Paresis of arms. Contractures of legs. Hyperæsthesia in both legs up to crest of ilia. Later, great pain; paralysis of sphincters. Bed-sores. | Sarcoma, growing from dura mater; nerves
passing through and over tumor. Cord congested and pushed to one side.
Thin, but not softened. Growth resembled psammoma. Between sixth and seventh cervical nerves of left side. |
T. Whipham, Tr. Path. Soc. Lond., 1873, xxiv. 15-19. |
| 16 | M. 57. | Pain in right arm. Numbness in hand, and paresis. [p. 1109] Paresis and coldness of left leg. Some anæsthesia and wasting of right leg. Later, paraplegia. Diminished reflexes. Contractures. Constriction sense about legs and abdomen. Triceps, deltoid, and serratus magnus of right side paralyzed. Incontinence of urine, difficult defecation, decubitus, fever. Abdominal muscles paralyzed. Later, other muscles of arms paralyzed. Complete anæsthesia of legs. Dyspnœa, œdema of lungs. | Myxoma from arachnoid. Cord compressed and
softened on right postero-lateral side. Secondary degeneration. Some
œdema of brain. At sixth and seventh cervical vertebra on postero-lateral surface of cord. |
Pel (P. K.), Berlin. Klin. Wochensch., 1876, xiii. 461-463. |
| 17 | F. 35. | First, pain in right arm, weakness in right hand. Then paralysis almost complete in arms, and impaired sensation. In legs paralysis complete, sensation impaired. Alternate incontinence and dysuria. Ankle clonus and increased knee-jerks and plantar reflex. Tapping biceps causes reflex in little and ring fingers. No atrophy or bed-sores. Cold on one side, hot on other. Pain and little swelling over sixth cervical vertebra. No eye symptoms. Brain clear. Inability to turn head. Before death respiratory paralysis and bed-sores. Duration, fifteen months. | Spindle-cell sarcoma, springing from
arachnoid and destroying cord by pressure, except posterior columns.
Cord below tumor soft. At sixth cervical vertebra. |
E. Long Fox, Bris. Med.-Chir. Journ., 1883, i. 100-106, 2 pl. |
| 18 | M. 50. | Paresis in right arm. Stiffness in neck and back. Paralysis of all extremities gradually developed. | Glioma in right half of cord. Old
hemorrhages in adjacent parts and in medulla oblongata. A more recent
hemorrhage in dorsal cord. In lower cervical region. |
Schueppel, Arch. d. Heilk., viii. Bd., 1867 (quoted by Rosenthal). |
| 19 | —— | Coldness, numbness, violent pains, first in left arm, later in both legs. Paralysis of all limbs and muscles of trunk. Atrophy. Reactions of degeneration. Violent leg reflexes. | Tubercle, large as hazelnut. Consecutive
myelitis of adjacent parts and left anterior horn. In lower cervical region. |
Chvostek, Med. Press, 33-39, 1873 (quoted by Rosenthal). |
| 20 | M. 45. | Interscapular pain. Chest-pressure and dyspnœa. Paræsthesia and pain in legs. Spastic paralysis. Difficulty in stools; bloody urine and dysuria. Œdema of legs. Bed-sores. Kypho-scoliosis. Pain on pressure over spine. Paralysis of left leg, paresis of right, some anæsthesia of both. Broncho-pneumonia, fever. | Phlegmon of dura mater, compressing cord.
Some infiltration of tissues of throat and mediastinal space. From seventh cervical to second dorsal vertebra. |
Mankopff (E.), Berl. Klin. Wochensch., 1864, i. 33-46, 58, 65, 78. |
| 21 | M. 22. | Pain in back and side of neck and in limbs. Marked pain in sternal region on coughing. Pressure and jarring cause pain. Rapid loss of power in both arms. Feeble and slow movements of thighs, legs, and feet. Right deltoid and flexors of fingers much wasted. No paralysis of face. Knee-jerks exaggerated. Later, complete paralysis, including bladder and rectum. | Tumor of membrane. Cord beneath compressed
and degenerated. Lower cervical and upper dorsal region. |
H. C. Wood, “Proceedings of Philadelphia Neurological Society,” Medical News, vol. xlviii. No. 9, Feb. 27, 1886. |
| 22 | F. 50. | Pain in neck, shoulders, and chest. Stiffness of neck, back, and arms. Chest fixed; breathing diaphragmatic. No paralysis or altered sensation. | Secondary cancer of vertebræ. Cervical region. |
Gull, by Wilks, in Lect. on Dis. of Nerv. System. |
| 23 | F. 40. | Severe pain in back. At height complete paralysis in legs, some paresis in arms. Variable anæsthesia. Girdle sensation and mammary pain. Lively and distressing reflexes. Contractures in legs. Bed-sores and paralysis of sphincter of bladder. Toward close rigors (pyæmia?). | Fibro-cyst on right side, between cord and
dura, and between anterior and posterior nerves. Top of dorsal region. |
Risdon Bennett, Tr. Path. Soc. Lond., 1855-56, vii. 41-45. |
| 24 | M. 30. | Cough, dyspnœa, wasting, simulating phthisis. Pain in back of neck and shoulders. Pain in joints; paresis of legs and bladder. Pain in chest. Paresis of arms. Later, increased paralysis, bed-sores, sweating. | Tumor, size of hazelnut, inner anterior
surface of dura mater. Flattening and softening of cord. Top of dorsal region. |
Gull, in Guy's Hosp. Rep., (quoted by Wilks in Lectures on Dis. Nerv. Syst., p. 264). |
| 25 | F. 43. | Pain in shoulders, chest, and sides. Contractures of [p. 1110] legs; heels to nates. No anæsthesia. Later, retention of urine and bed-sores. Incessant pain in back and abdomen. | Fibro-nucleated tumor from inner surface of
dura mater. Opposite third dorsal vertebra. |
Gull, by Wilks, ibid. |
| 26 | F. 43. | Pain in chest and shoulder, then in legs. Paresis of legs. Contractures and jerking of legs. Spasm of abdominal muscles. No anæsthesia. Paresis of bladder and rectum. Wasting and bed-sores. Finally, paresis increased, but never complete paralysis. Duration, nine months. | Fibro-nucleated tumor, size of a bean, from
dura mater. Cord compressed backward, and softened. Opposite third dorsal vertebra. |
Wilks, Trans. Path. Soc. Lond., 1855-56, vii. 37-40. |
| 27 | M. 24. | Paraplegia. Depressed reflexes; girdle symptom. Partial anæsthesia. Dysuria. Vomiting. Pulse weak and intermittent. Partial recovery from paralysis, and anæsthesia in left leg, and reflexes in right foot regained. Later, complete paraplegia, anæsthesia, and bed-sores. Duration, five months. | Probable gumma. Middle dorsal region. |
B. G. McDowell, M.D., Dubl. Q. J. Med. Sci., 1861, xxxii. 299-303. |
| 28 | F. 44. | Paresis in legs. Spine hypersensitive and inflexible; least attempt at bending causes great cervico-brachial pain. Paræsthesia; sense of falling out of abdominal viscera through abdominal walls. Pains in extremities increasing, and involving right shoulder, intercostals on both sides, and lumbar region. Paralysis of right arm (first); complete paralysis of leg. Excessive spinal tenderness. Loss of sensation (partial) in legs, body, and right arm. Later, dyspnœa, then dysuria, then complete inability to empty bowels or bladder. Great tympanites. Girdle sense above umbilicus, and finally complete paralysis and anæsthesia below this band. Sense of twisting of legs and feet, so that latter seemed close to face. Œdema. Later, paresis of left arm. One small bed-sore. | Alveolar sarcoma. Eighth and ninth dorsal vertebræ. |
G. W. H. Kemper, Journ. Nerv. and Ment. Dis., xii. No. 1, Jan., 1885. |
| 29 | F. 42. | Projection of seventh, eighth, ninth, tenth, and eleventh dorsal vertebræ. Numbness below ankles, and early girdle sensation. Peronei and anterior tibial muscles first involved; then all leg-muscles, then sphincters, then arms. Died in a fit. | Round-celled sarcoma. The anterior columns
soft opposite tumor. Bodies of seventh, eighth, ninth, and tenth
vertebræ soft. Opposite seventh, eighth, ninth, and tenth dorsal vertebræ. |
E. Long Fox, Brit. Med. Journ., 1871, p. 566. |
| 30 | F. —. | Ill-defined hemiplegia; later, paraplegia, with contractures and rigidity. | Gumma and syringo-myelus. Small cavities in
anterior cornua. At ninth dorsal vertebra anterior aspect. |
Taylor, Lancet, 1883, p. 685. |
| 31 | M. 7. | Paraplegia, except adductors and rotators of thigh. Reflex contractures; most intense from irritation of penis and scrotum. Rigidity of legs. Complete anæsthesia of lower half of body. Later, anuria, incontinence of feces. Anal sphincter reflex; figured stools. Cystitis. Pain on percussion in dorsal region. Pain in back. Complete paraplegia. Very late, brain symptoms. Duration, nine months. | Tubercle (?). Cord soft for two inches. Tenth dorsal vertebra. |
Geoghegan, Dublin Med. Press, 1848, xix. 148-151. |
| 32 | F. 46. | Fixed pain in left iliac region. Paresis in left leg, increasing to paraplegia. Formication. Girdle sensation. Incomplete, increasing to complete, anæsthesia of legs. Spontaneous twitchings. Bladder and sphincter ani paralyzed. Bed-sores. Duration, one year. | Fibroma (?) from inner surface of dura. Cord
hollowed out and softened. Interval between tenth and eleventh dorsal vertebræ. |
William Cayley, Tr. Path. Soc. Lond., 1864-65, vol. xvi. 21-23. |
| 33 | M. 30. | Hyperæsthesia; later, anæsthesia in legs; then complete paraplegia. | Tubercle size of pea. Adjacent myelitis. In lower dorsal region. | Chvostek, Med. Presse, 33-39, 1873 (quoted by Rosenthal). |
| 34 | M. 31. | Ataxia; stiffness of legs and cramps in abdomen and [p. 1111] legs. Slight nystagmus. Difficulty in forming words. Ataxia of arms. Slight wasting of legs, especially of left. Lumbar pains; abdominal cramps. Dysuria. Impotence. Later, increased spastic state of legs. Mind depressed and emotional; attempts at suicide. Anuria. Bed-sores. Urine albuminous. Duration, one year. | Myxoma of dura mater 3 inches long. Dura
mater of brain contained fluid and lymph. Dorsal region, left side. |
Shearman, Lond. Lancet, vol. ii. 1877, p. 161. |
| 35 | F. 50. | Pains in limbs (thought to be rheumatic). Paresis in legs. Hyperæsthesia in right leg; burning pains alternating with sense or coldness. | Cancer of vertebræ (sarcoma?). Dorsal region. |
Gull, by Wilks, Dis. Nerv. Syst. |
| 36 | F. 35. | Paresis of left leg; soon of right leg. Pain in back and left side. Tonic spasms of legs. Darting pains in knees. Partial anæsthesia. Exalted plantar reflexes. Dysuria. Later, complete paraplegia and anæsthesia; violent reflexes; severe pain in back. Bed-sores. Duration, seven and a half years. | Tumor, osseous or fibrous, three-fourths of
an inch long, growing from dura mater. Cord flattened, and softened
below tumor. Lower part of dorsal cord. |
H. Ewen, Tr. Path. Soc. Lond., 1848-50, i. 179. |
| 37 | F. 28. | Weakness in legs. Aching and shooting pains in legs. Numbness and formication. Slight spasm in legs. “Felt as if ground was some distance below feet.” Œdema of ankles. Later, numbness extended to abdomen. Paralysis of bladder. Hyperæsthesia in right leg. Obstinate constipation. Bed-sores. Some paralysis of respiratory muscles. Duration, fourteen months. | Tubercle the size of cherry, which had
almost obliterated cord. Tubercles in lungs, bowels, and uterus.
Bed-sore had opened spinal canal. Lower part of dorsal cord. |
S. O. Habershon, M.D., Guy's Hosp. Rep., London, 1872, 3d S., xvii. 428-436. |
| 38 | M. 63. | Progressive paresis of left leg for five years. Right leg then paretic. Paralysis then in left leg. Rigidity on extension of right leg. Paroxysms of clonic spasms in right leg. Joint pains, sciatic pains. In left leg, hyperæsthesia, in right leg, anæsthesia. Plantar reflex retained; other reflexes exaggerated. Diplegic contractions in right leg from irritation in left. Late symptoms: purulent urine, with retention; chest and lumbar pains like bone pain; extension changed to flexion; swelling of legs and ecchymosis; sacral and other eschars. | Psammoma adherent to dura mater. Cord
softened. Ascending degeneration in posterior columns, and descending
degeneration of lateral columns. In dorsal region just above lumbar enlargement, anterior left side. |
Charcot, Arch. de Physiol., Paris, 1869, ii. 291-296. |
| 39 | M. 20. | Paralysis of lower extremities; tremor; exaggerated reflexes, hyperæsthesia of trunk; bed-sores. Œdema of feet. Fever. Pus in urine. | Organized blood-clot exterior to dura mater.
Cord compressed and softened. Opposite lower dorsal and upper lumbar. |
C. B. Nancrede, Am. Journ. Med. Sci., O. S., lxi. 156. |
| 40 | F. 38. | Pain around abdomen, in back, and legs. Paraplegia. Anæsthesia and tingling of feet and legs. Paralysis of bladder. | Hydatid cysts of vertebræ (?) and spin.
canal. Lower part of spinal canal (probably lumbar region). |
S. Wilks, Dis. Nerv. Syst., p. 265. |
| 41 | F. 23. | Bronzing of skin for two years; then headache, giddiness, fever. Choreic movements in left arm, then in leg, then general. Bronzing increased. Vomiting after meals. Duration, two years and two months. | Tumor, consisting of granular matter, with a
few nerve-fibres and cells, springing from centre of cord backward to
posterior fissure. Cord slightly widened. Suprarenal capsules large
and nodulated. Lumbar enlargement. |
W. H. Broadbent, Trans. Path. Soc. Lond., 1861-62, viii. 246. |
| 42 | 10 ms. | Twitching and convulsive movements of right leg. After removal of exterior tumor the movements ceased. Child died of peritonitis. | Tumor outside of sacrum, and also protruding through sacral opening. Reported to have been behind and pressing upon cord (?). Fatty growth within membranes. | Arthur Johnson, ibid., 1856-57, viii. 28, 29. |
| 43 | F. 54. | Paresis, first of left arm and leg; then paralysis [p. 1112] of these and of right arm and leg. Pain in back and hips early; then, suddenly, darting pains and incontinence of urine. Paræsthesia of left arm and leg; no anæsthesia. Coma. | Hydatid cyst. Cyst also in liver. Fluid
beneath membranes of cord and brain. At first and second left sacral foramen, opposite last lumbar and upper three sacral vertebræ. |
H. S. Wood, Australian Med. Journ., 1879, N. S. i. 222. |
| 44 | M. 46. | Fibrillary twitching. Increased patellar reflexes. Paræsthesia and hyperæsthesia in legs, disappearing. Constriction of chest (?). Headache. Dysuria for two years. Straining at stool. Indigestion. Bloody vomiting. Cardiac palpitation; intracardial murmurs; slow pulse. Swollen inguinal glands. Variations in temperature. Bed-sores. | Glioma. At filum terminale, upper part. |
Lachman, Arch. f. Psychiat., Berl., 1882, xiii. 50-62, 1 pl. |
| 45 | M. 38. | Pain in legs. Œdema. After two years could not lie down: rested on hands and knees. Paralyzed in legs; pain in seat. Anæsthesia in legs, not complete in right. Paræsthesia in left. Dysuria and constipation. Before death had incontinence with hæmaturia, and was able to lie down. | A lobulated tumor from pia mater at lower
end of spinal canal, surrounded by nerves of cauda equina. Structure
not made out. At cauda equina. |
W. W. Fisher, Tr. Prov. M. and S. Ass., 1882, x. 203-208. |
| 46 | —— | This case had symptoms of posterior spinal sclerosis, which possibly had no relation to growth, according to reporter. | Myo-lipoma attached to conus medullaris. Crescentic, clasping cord from anterior to posterior fissure. Nerve-roots of cauda equina imbedded in it. Contained striated muscular fibres. | W. R. Gowers, Tr. Path. Soc. Lond., 1875-76, xxvii. 19-22. |
| 47 | Und. 1 yr. |
Spina bifida (?); hydrocephalus; convulsions, bloody stools; partial paraplegia. (Above symptoms came on after closing of sacral opening by surgical operation.) | Congenital sacral neuroma amyilinicum. | W. F. Jenks, M.D., Trans. Path. Soc. Philada. (1871-73), 1874, iv. 190-192. |
| 48 | M. 30. | Pain in back; abdominal girdle sensation. Pain in legs; paraplegia; nearly complete anæsthesia; paralysis of bladder; bed-sores. | Aneurism, eroding vert. and compressing cord. Location not given. | Wilks, Dis. Nerv. Syst. |
| 49 | M. 54. | Paralysis of both legs, of sphincter ani, and of bladder; urine alkaline, with pus and blood. Partial anæsthesia. Pyonephritis. | Gumma from inner layer of dura mater and involving pia mater. Location not given. | Delafield, N. Y. Med. Rec., 1875, x. 131. |
| 50 | Still- born. |
—— | Tumor, size of head of child two years old, projected between legs from spinal column. Nerves of cauda equina over anterior part. Some bone in tumor (dermoid cyst?). | Virchow, Monatschr. f. Geburtsk., Berl., 1857, ix. 259-262. |
SYNONYMS.—Essential paralysis of childhood (Rilliet and Barthez); Myogenic paralysis (Bouchut); Acute fatty atrophic paralysis (Duchenne); Atrophic paralysis (Ferrier); Acute anterior poliomyelitis (Kussmaul, Erb, Seguin); Regressive paralysis (Barlow); Tephromyelitis (Charcot).
DEFINITION.—Of all the titles which have been given to the disease it is our purpose to describe, two alone may be considered irreproachable. In the present state of our knowledge it is unnecessary to argue that this disease is not essential—i.e. destitute of characteristic anatomical lesions. Neither can the theory of its myogenic origin be maintained; nor even is fatty degeneration invariably present in the paralyzed muscles. Finally, the disease cannot longer be regarded as peculiar to childhood,1 since cases in adults have been in these last years quite numerously reported2—four with autopsies demonstrating the identity of the lesion. But there are two definitions in our list of synonyms which embrace between them the most striking characteristics of the disease, yet contain no error of fact. Atrophic paralysis describes at once the two most salient symptoms; acute anterior poliomyelitis defines at once the seat and nature [p. 1114] of the lesion, classes it with the systematic diseases3 of the spinal cord, and notes the peculiarity in the mode of invasion by which it is so remarkably distinguished from nearly all the organic diseases of this centre.
1 W. H. Barlow, On Regressive Paralysis, 1828. See Brain, April, 1879.
2 In Dec., 1873, I quoted 14 cases of adult spinal paralysis, as follows: Duchenne, 4 cases; Charcot and Petitfils, 3; Moritz Meyer, 2; Bernhardt (Archiv Psych., 1873), 1; Cumming (Dublin Quart. Journ., 1869), 1; Lucas Championnière (by Hallopeau, Archives gén., 1861), autopsy, 1; Gombault (Archives de Psych., 1873), 1; personal, 1.
In 1874, Seguin published a summary of all the foregoing cases except the last, and added 6 personal observations, also 3 from Duchenne and 1 from Hammond. In the enlarged edition of his essay in 1877, Séguin increased the list to 45—by new personal cases, 3; cases related by Frey (Berlin. Wochens., 1874), 4; cases by Erb (Arch. f. Psych. u. Nervenkrank., v.), 4; case by Cornil and Lépine (Gaz. méd., 1875), autopsy, 1; case by Soulier (Lyon méd., 1875), 1; case by D. H. Lincoln (Boston Med. and Surg. Journ., 1875), 1; case by Lemoine (Lyon méd., 1875), 1; case by George M. Beard, 1; case by Leyden (Klinik Ruckenmarks Krankheiten) Bd. iv. 1; case by Hammond (6th ed. Treatise), 4; case by Courty (Gaz. méd., 1876), 1; case by Dejerine (Arch. de Phys., 1876), 1.
To these may be added—case by Goltdammer (Berl. klin. Wochen., 1876), 1; case by Webber (Trans. Amer. Neurol. Ass. for 1875, vol. i.), autopsy, 1; case by Klose (Diss. Breslau, 1876), 1; case by Schultze (Virchow's Archiv, Bd. lxviii.; also Bd. lxxiii.), autopsy, 1; case by Bernhardt (Archiv für Psych., Bd. ix., 1879); case by Sinkler (Amer. Journ. Med. Sci., Oct., 1878), 5; case by Althaus (ibid., April, 1878), 2; case by Ross (Dis. Nerv. Syst., vol. ii. p. 139), 1—total, 57 cases.
Morton (St. Bartholomew's Hospital Reports).
Others have doubtless been published since this date, but, as they do not immediately concern our subject, need no further citation.
3 Vulpian, Leçons sur les Myelitis, 1880.
SUMMARY OF CLINICAL HISTORY.—The clinical features of an acute attack of infantile paralysis are well known. The children affected are usually between eighteen months and four years of age (Henoch). The attack is more likely to occur in summer than in winter, as Sinkler4 found that 47 out of 57 cases began between May and September, and Barlow noted 27 out of 53 in July and August.5
4 Amer. Journ. Med. Sci., April, 1875.
5 Loc. cit., p. 75. Among Sinkler's 57 cases, only 6 furnish autopsies, thus:
Case by Cornil and Lepine and case by Webber (quoted and accepted by Erb in Ziemssen's Handbuch, Bd. xi.); case by Gombault (rejected by Erb and Westphal); case by Schultze; cases by Dejerine and Lucas Championnière (quoted by Hallopeau).
The influence of heat is perhaps shown in the case related by Dyce-Duckworth in the Lancet of 1877: a child two and a half years, after exposure to great heat on a steamboat-landing, became paralyzed in all four limbs, but the paralysis was subsequently confined to the lower extremities. Coincidently, the patient became delirious; suffered from anæsthesia and temporary paralysis of the sphincters. The paralyzed muscles wasted rapidly and lost faradic contractility. Treatment by faradization was begun in a month from the date of the attack, and recovery was complete three months later.
The onset of the paralysis is either really sudden, occurring in the daytime, while the child is under competent observation, or apparently sudden, being discovered in the morning after a quiet night, the child having gone to bed in health (West); or is preceded by some hours or days of fever or of nervous symptoms, especially convulsions, or both. The paralysis is almost always at its maximum of extent and intensity when first discovered, and from this maximum begins, within a few hours or days, to retrocede. The improvement may, however, be delayed much longer. A variable number of muscles remain permanently paralyzed, and in these, within a week (thirty-six hours, according to some observers), faradic contractility is first diminished, then abolished; galvanic reaction is exaggerated, ultimately is characterized by the degeneration signs (entartungs reaction). The temperature of the paralyzed limbs falls; the muscles waste; the atrophy may rapidly become extreme. The paralysis and loss of faradic contractility are complete, however, while the atrophy is only incipient and progressing. The absence of lesions of sensibility, of visceral disturbance, of trophic lesions of the skin, or of sphincter paralysis is as characteristic of the disease as are the positive symptoms above enumerated.
In the third or chronic stage the paralyzed limbs often become contracted and deformed. At other times, and with more complete paralysis, the growth of the bones is arrested, the muscles remain flaccid, the entire limb shrivels, and dangles so loosely from its articulations that it may be dislocated by slight effort (membre de Polichinelle). The general health of the patient remains remarkably good, the intelligence clear, the disposition lively. The duration of life seems to be in nowise shortened by the paralysis. Thus, suddenness of development, intimate association of trophic, motor, and electrical disturbance, absence of cerebral or sensory lesion, peculiar localization and grouping of the permanent paralyses,—such are the salient characteristics of this remarkable disease.
SYMPTOMS IN DETAIL.—Three well-defined stages exist—the initial, the paralytic, and the chronic.
[p. 1115]Initial Stage.—Seeligmüller6 signalizes three principal varieties in this stage. The first is characterized by fever; the second by nervous symptoms, principally convulsions, sometimes delirium or coma; in the third no symptoms either precede or accompany the local disease—"la paralysie est toute la maladie.”7
6 Gerhardt's Handbuch der Kinderkrankheiten, 1880 (separat Abdruck).
7 Rilliet et Barthez, Traité des Maladies des Enfants, ii. p. 551.
Mode of Invasion.—I have elsewhere8 described eight different modes of invasion: absolutely sudden, coming on in the daytime; morning paralysis (West), discovered after a quiet night, preceded by fever or by vomiting alone (?), or by another typical disease, especially one of the exanthemata, or, finally, by a traumatism, generally slight. An interval of time almost always elapses between the occurrence of the traumatism and the development of the paralysis—a fact which already indicates that a definitely-evolved morbid process must intervene between the two occurrences. An exception is related by Duchenne fils;9 and some apparent exceptions, in which recovery occurred rapidly, seem to belong to the temporary paralysis of Kennedy,10 more recently described again by Frey.11
8 Am. Journ. Obstet., May, 1874.
9 Archives gén., 1864. A father pulled his child from a table by the right arm, and set it rather roughly on the ground. Immediate pain, almost immediate paralysis of arm, which persisted, and was followed by atrophy of its muscles.
10 Dublin Quarterly, 1850.
11 Berlin. klin. Wochens., 1874. Frey considers these cases to be identical in nature with, though differing in severity from, anterior poliomyelitis.
PRODROMATA.—There is rarely any lengthened period of prodromata. Seeligmüller has noticed in some cases an indisposition on the part of the child to stand or walk during several weeks before the occurrence of the paralysis. He does not say whether such children were rachitical. In marked contrast with cases of cerebral paralysis is the habitual absence of generalized nervous symptoms. Thus in only 1 case of Seeligmüller's (total of 75) did the child suffer, and that during six months preceding the paralysis, from intermittent muscular contractions, and also from attacks of laryngismus stridulus.
The fever is usually of moderate severity (Seeligmüller), but sometimes extremely high (Erb)12—as much as 41° C. (Henoch),13 or 104° F. (Barlow).14 Duchenne fils observed 7 cases alleged to be entirely without fever, and Laborde counts 10 cases out of 50 as apyretic.15
12 Ziemssen's Handbuch, Bd. xi. Abh. 12.
13 Vorlesung. über Kinderkrank., 2d Aufl., 1881. Seeligmüller (Jahrb. für Kinderheilk., 1878, p. 345) quotes another case from Henoch's clinic where the fever lasted thirty-six hours, the temperature on the first evening being 39.2°, the following morning 39.0°, the second evening 39.5°; the second morning, at which date the paralysis was discovered, it was normal. The author states this to be the only case known to him in which thermometric measurements were taken.
14 Loc. cit.
15 De la Paralysie de l'Enfance.
The duration of the fever usually varies from a single night to forty-eight hours; much more rarely does it last six, eight, twelve, or fourteen days, or even, but quite exceptionally, three or four weeks. According to Duchenne, its intensity and duration increase with the age of the child, perhaps indicating greater resistance on the part of the nerve-tissues which are the seat of the morbid process of which it is symptomatic. Rarely does it last after the paralysis has once occurred, [p. 1116] but ceases then with an abruptness which recalls the defervescence of pneumonia when the exudation process is once completed.16
16 See p. 1144 for pathogenic inferences to be drawn from this fact. Seguin (New York Med. Record, Jan. 15, 1874) seems to throw some doubt on the existence of apyretic cases; but, as Seeligmüller remarks, there is too much testimony to this possibility to render it really doubtful.
There is no proportion between the intensity of the fever and the extent of the subsequent paralysis; nor is there any marked contrast between the fever in children and that in adults in those rare cases in which the disease, instead of being subacute, is sudden as in children.
Erb considers the fever to be purely symptomatic of an inflammatory process in the spinal cord.17 But Vogt regards it rather as an essential factor in the development of a spinal lesion, and thus explains the occurrence of this in the course of febrile diseases which at the outset have no special relation to the cord.
17 Loc. cit., p. 279.
Convulsions, usually accompanied by fever, were observed in 11 of Seeligmüller's cases out of 67; Duchenne had 13 out of 70; Heine, 9 out of 86;18 thus a total of 33 cases of convulsions in 223 cases of infantile paralysis—nearly 15 per cent. The paralysis may set in after a single brief convulsion, or this may be repeated several times at variable intervals before the paralysis is definitely declared (Ross).19 The convulsive movements are apt to be particularly intense in the limbs destined to become paralyzed (Vogt).
18 Die Spinale Kinderlahmung.
19 Loc. cit., p. 107. The author is quoting Laborde.
The convulsion may be very slight—an isolated spasm of a limb or even a single group of muscles. Whether, on the other hand, it can ever be so intense that the child succumbs to it before the development of paralysis, is a question which could only be decided by repeatedly examining the cord in the cases of convulsion which have terminated fatally. In a case of Seeligmüller's the child was affected for eight days preceding the paralysis by tremblings generalized through all his muscles.
The convulsion is usually followed by a soporous or even comatose condition, or this may replace the convulsion. Delirium may take the place of either.
Special interest attaches to those cases where the paralysis develops in the course of an acute specific disease; for then becomes most plausible the suggestion of Vogt, that a fever excited by some cause remote from the spinal cord may itself become a cause of lesion in this centre. In Roger's first and most celebrated case, paraplegia developed suddenly during the course of a fatal scarlatina in a child already suffering from paralysis of the left deltoid of two months' standing.20 The scarlatina was hemorrhagic, and, as will be shown farther on, the autopsy showed traces of a hemorrhagic extravasation in the cord. Thus a double influence was presumably exerted by the scarlatina, while, moreover, the previous and recent occurrence of a deltoid paralysis indicated a morbid predisposition in the spinal cord. Of Seeligmüller's 75 cases, 1 occurred during scarlet fever, 1 with measles, 1 in the course of an erysipelas, and 1 of pneumonia.
20 Gaz. méd., 1871.
Apyretic diseases, especially of the gastro-intestinal tract (Brown-Séquard), also seem to have an influence on the development of infantile paralysis. Two of my own cases occurred during an attack of [p. 1117] cholera infantum; another in a child who had been for several weeks in bed with a purulent conjunctivitis. Study of these varied antecedents is of interest in connection with the obscure question of the etiology of infantile paralysis. In this latter connection we will refer to them again.
Vomiting, or even the entire symptom-complex of gastric fever, not infrequently ushers in the paralysis. Fever is then usually present, but I have recorded one case of vomiting where, according to the mother's assurance, no fever at all existed.
At the moment that the symptoms of the invasion subside, and the child seems to enter upon convalescence, the terrifying discovery is made that an arm or a leg or all four limbs, or even they and the muscles of the trunk, are paralyzed.
In the severest form the child lies motionless, unable to stir hand or foot, or even a finger or toe. Yet, singularly enough, this extensive paralysis is sometimes overlooked, especially in very young children, as the immobility of the patient is attributed merely to weakness caused by previous illness. General paralysis, during at least the first few hours of the paralytic stage, is probably more common than appears from our present statistics. Not only, as has just been noted, may this condition be overlooked, but it may exist during the hours of sleep which precede the cases of morning paralysis. Seguin21 speaks as if the paralysis were at first always generalized, but this statement seems to me somewhat exaggerated. Referring merely to the statements of the parents, a considerable number of paralyses would be found limited from the beginning. Heine's third table of partial paralysis is entirely composed of cases so limited. In 16 out of the 19 cases of hemiplegia (monoplegia) the original limitation of the paralysis is also specified; similarly with 7 out of the 20 cases of paraplegia contained in the first table.
21 Loc. cit.
Paralysis of one or both lower extremities is often first detected when the child gets out of bed and attempts to walk; or in children too young to walk the flaccid immobility of the limb attracts attention as soon as they are again carried on the mother's arm. Paralysis of the upper extremities is discovered early in proportion to the liveliness recovered by the child, leading him to occupy himself with his toys as usual. In unilateral paralysis of the trunk the child will fall over to one side when placed in the sitting position; in bilateral paralysis it cannot be made to sit up at all.
From lack of competent observation during the initial stage it is really not quite certain whether any degree of paresis precedes the paralysis; but from the testimony at present accumulated the paralysis is nearly always complete when first observed. This is in striking contrast with adult spinal paralysis. In some few cases the paralysis has been observed to creep on slowly, and not reach its maximum for several days (Ross). Laborde relates a case where recovery from a first attack of paralysis was followed by two relapses in the same limbs at intervals, each ushered in by fever. After the second relapse the paralysis remained permanent.
Significance of Original Extent of Paralysis.—The question of the [p. 1118] original distribution of the paralysis is of special interest in connection with that of the original distribution of the morbid process in the spinal cord. The real effect of the latter cannot be adequately measured by the permanent paralyses; for, as will be seen, it is not unusual to find traces of an extensively diffused process in the cord in cases of quite partial paralysis.
It is interesting to notice that certain muscles are always exempt from paralysis. With the exception of a single case of paralysis of one temporal muscle, cited by Seguin,22 the muscles of the head, eyeballs, ears, larynx, and pharynx are always exempt, as are also the diaphragm and intercostals. The arrest of the spinal lesion below the medulla explains the immunity of muscles supplied by the vagus and spinal accessory nerves. But since the cervical plexus is often involved, the constant escape of the diaphragm, innervated by the phrenic nerve which comes from this plexus, is remarkable. Still more so the immunity of the intercostal muscles, whose nerves arise in the dorsal region—a position of the cord frequently affected. This fact tends to confirm Ross's hypothesis, that the nuclei of the intercostal nerves lie in the vesicular columns of Clarke—columns confined to the dorsal region of the cord, and which are invariably found intact at autopsies of atrophic paralysis.
22 Loc. cit.
The immunity of these respiratory nerves explains the absence of the dyspnœa which is so marked in Landry's ascending paralysis. In the adult case described by Schultze and Erb23 dyspnœa was present for a short time. The disease terminated fatally twenty months from the time of invasion. In this case traces of myelitis were found extending through the dorsal region of the cord, and including not only the anterior nerves, but, to a less degree, the columns of Clarke.
23 Arch. Virch., Bd. lxviii.
The facial nerve (itself a respiratory nerve) shares the immunity of the phrenic and intercostals. In the cases in which facial paralysis has been noted the limb paralysis has been hemiplegic, as in Seeligmüller's twentieth case. A cerebral origin is then always to be at least suspected.
Barlow24 has seen 6 cases of paralysis of the facial, but the histories render a cerebral paralysis more probable in 4 out of those 6. Henoch25 gives a case of paralysis of left arm, accompanied by paralysis of corresponding facial nerve. The latter rapidly recovered, but the paralysis of the arm persisted and was followed by atrophy. Ross26 implies that the sides of the neck, face, and tongue are always at first implicated in spinal hemiplegic paralysis, but do not remain permanently affected.
24 Loc. cit.
25 Loc. cit., p. 205.
26 Loc. cit., p. 108.
That the facial should be affected while the other medullary nerves escape probably depends on the more anterior position of its nucleus.
The regression of the original paralysis is characteristic, indeed almost pathognomonic, of the disease. It is on this account that Barlow has proposed the name regressive paralysis.27 This author quotes the case of a boy who at five months was affected with a universal paralysis, even affecting the neck, but entirely recovered except in the extensor longus digitorum of the foot. This improvement constitutes a second apparent convalescence, as deceptive as that which immediately succeeds the pyrexia. Only in rare cases do all the [p. 1119] muscles at first paralyzed remain so permanently (Seeligmüller); nor, on the other hand, do all entirely recover (temporary paralysis of Kennedy and Frey). Even when an entire limb appears to be paralyzed, careful examination will usually detect certain muscles that retain their faradic contractility. Thus the order of frequency of paralysis in the different limbs must be distinguished from that observed for different muscles.
27 Brit. Med. Journ., 1882.
Duchenne fils28 and Seeligmüller29 have tabulated, for lists of 62 and 75 cases respectively, the general locality of the permanent paralyses in their order of frequency. The cases of monoplegia are by far the most numerous. Thus in the table quoted below there are 97; in Heine's tables (86 cases), 47; in Sinkler's tables (86 cases), 29—total, 173 from a total of 309, or nearly one-half:
| Duchenne. | Seeligmüller. | Total. | ||
| Left lower extremity | 7 | 27 | 34 | |
| Right lower extremity | 25 | 15 | 40 | |
| Right upper extremity Left upper extremity |
10 | 13 | 9 4 |
23 |
| All four extremities | 5 | 2 | 7 | |
| Both upper extremities | 2 | 1 | 3 | |
| Both lower extremities | 9 | 14 | 23 | |
| Left over and under extremity | 1 | 1 | 2 | |
| Right over and under extremity | 0 | 1 | 1 | |
| Right over and left under extremity | 2 | 1 | 3 | |
| Muscles of trunk and abdomen | 1 | 0 | 1 | |
| 62 | 75 | 137 | ||
This limitation is all the more noteworthy when compared with the frequency of general paralysis at the outset.
28 Archives gén., 1864.
29 Jahrbuch der Kinderheilkunde, N. H. xii. pp. 338-343.
The next peculiarity is the great preponderance of paralysis of the lower over that of the upper extremities. This is noticeable even in the monoplegias. In Sinkler's cases only two of these affected an arm. But in bilateral paralysis the predilection is still more remarkable, paraplegia of the lower extremities being among the most frequent, paraplegia cervicalis the rarest, form of paralysis. This is not because a lesion situated in the cervical spinal cord must interfere with the motor tract going toward the lumbar, and hence nearly always paralyze all four extremities, if any. Because when this does happen the upper extremities alone exhibit the atrophic changes characteristic of anterior poliomyelitis: the lower, though paralyzed, do not atrophy and retain their faradic contractility. Heine denied the existence of paraplegia cervicalis. But in the table of Duchenne-Seeligmüller 3 cases are recorded; Rosenthal30 relates 1; Lockhart Clarke, 1.31 This is the somewhat famous case, described by Clarke as a progressive muscular atrophy, which contributed one of the earlier autopsies.
30 Klinik der Nervenkrankheiten, 2 Aufl. p. 413.
31 Med.-Chir. Trans., li. p. 219.
Seeligmüller's case32 is remarkable in several respects. The paralysis, occurring after a brief fever in a child seventeen months old, exclusively attacked the two arms at the moment of invasion, and never retreated from them, thus offering a double exception to the usual rule. At four rears of age the arms were much atrophied, and faradic contractility was lost in their muscles, the legs being sturdily developed. Nevertheless, [p. 1120] the child constantly fell in walking, because, observes Seeligmüller, he was unable to balance himself with his arms, as is habitual with little children learning to walk.
32 Jahrbuch, loc. cit., p. 349.
The hemiplegic variety of paralysis is again very rare. The Duchenne-Seeligmüller table contains (out of 137) 3 cases; Sinkler records (out of 86) 4; West, 5; Heine (out of 86), 1; Leyden, 1; Duchenne, 1. West's 5 cases all present certain peculiarities, at least unusual in spinal paralysis. In 2 the paralysis came out gradually; in 1 succeeded to remittent fever (pigmentary embolism?); in 1 was preceded by heaviness of the head for several days; and in 1 the leg was paralyzed fourteen days after the arm.33 It is probable that in almost all, if not in all cases, hemiplegic spinal paralysis is the residue of a paralysis originally generalized to all four limbs, if only for a few hours.34
33 In three cases of hemiplegia observed by myself, and previously diagnosed as spinal paralysis by other physicians, I doubted the diagnosis from the coincidence of unusual cerebral symptoms. In the first case the hemiplegia appeared after coma, during cerebro-spinal meningitis; in the second, after a violent convulsion the face was drawn to the opposite side, and the patient, a child of seven, remained for a month in a state of intense maniacal excitement. In a third case, developed during convalescence from scarlet fever, the hemiplegia was preceded during two days by hemiparesis, and accompanied for a year by complete aphasia. Finally, in these cases faradic contractility persisted in the paralyzed limbs (Am. Journ. Obstet., May, 1874).
34 Seeligmüller relates one case where hemiplegia, including the facial nerve, was observed in two days from the beginning of the fever.
The question of hemiplegia is closely connected with that of paralysis of the facial nerve, inasmuch as the existence of the latter often serves to suggest a cerebral paralysis—a suggestion confirmed later by the absence of atrophy and of characteristic electrical reactions. However, in some cases of undoubted spinal paralysis the facial does really seem to have become involved. Thus in the case just quoted from Seeligmüller (Case 20 of his table) Henoch35 relates a case of paralysis of the left facial coinciding with paralysis of the left arm. Rapid recovery from facial paralysis: arm atrophied. Barlow36 records temporary facial paralysis in six cases, but only two of these seem to be really spinal. Such temporary paralysis is not altogether infrequent in the poliomyelitis anterior of adults (Sinkler, Seguin). Ross37 implies that the sides of the neck, face, and tongue are always implicated at first in hemiplegic spinal paralysis, but do not remain so.
35 Loc. cit., p. 203.
36 Loc. cit., p. 76.
37 Loc. cit., p. 108.
Crossed paralysis is extremely rare. There are 3 cases in the Duchenne-Seeligmüller table; Leyden38 has one. But paraplegia of the lower extremities, coinciding with paralysis of one upper extremity, is by no means so rare, especially as a residual paralysis.
38 Archiv Psychiatrie, Bd. vi.
Finally, as in cerebral paralysis, the muscles of the trunk, though often paralyzed at the outset, rarely remain so in children—much more often in adults. Eulenburg39 relates one interesting case of complete paralysis and atrophy of the extensors of the back. Even the interspinous muscles were involved, as shown by the divergence of the spinous processes. The paralysis was observed in a girl of fifteen affected since the age of three, and was completely cured in five months by daily faradizations of ten minutes each, and two gymnastic séances, each lasting two hours.
39 Arch. Virch., Bd. xvii., 1859.[p. 1121]
Birdsall40 has described one case of unilateral paralysis of the abdominal muscles.
40 Journal of Nervous Diseases.
Study of the precise combinations of the muscles paralyzed has recently acquired peculiar interest in connection with the localization in the spinal cord of the motor or trophic nuclei of their nerves.41 Several facts have been ascertained: 1st, that, in notable contrast with progressive muscular atrophy, atrophic paralysis tends to involve definite groups of muscles; 2d, that this grouping is not effected in accordance with the proximity to each other of the muscles on the limb, but with their functional association. Remak affirms that Charles Bell had already called attention to the fact that in cases of local muscular paralysis of the extremities the paralysis does not spread by muscular continuity, but in accordance with the functional association of muscles. Thus, paralysis of the thumb is more often associated with that of the forearm than with paralysis of the other muscles of the hand. 3d. From such grouping may often be inferred a different localization of certain nerve-nuclei than would be supposed from the position of the muscles alone. 4th. That the fibres contained in a single nerve-trunk, but distributed to different muscles, probably separate from each other within the cord, to be there distributed to variously-situated nuclei.42
41 Ernst Remak, “Localis. der Atroph. lahmung,” Archiv f. Psych., ix., 1879; Ferrier, Brain, vol. iv. No. 3; also, Proceedings Royal Society, No. 212, p. 12.
42 The theory of course assumes the truth of the demonstration by which atrophic paralysis is rendered symptomatic of disease of the spinal cord, and the nutrition of a muscle dependent on the integrity of the muscles of origin of its nerves.
In the arm two mutually correlative cases are observed: (a) Immunity of the supinator longus during paralysis of the forearm muscles; (b) paralysis of the supinator in association with paralysis of the deltoid, biceps, and brachialis anticus. The latter constitutes Remak's upper-arm type of localization, and is exhibited in his first case.43
43 Loc. cit.; also, cases 1st and 2d by Ferrier, in which, however, other shoulder-muscles were involved.
Ferrier has experimentally confirmed this muscular association by means of isolated irritation of the fourth cervical nerve, which threw into contraction the supinator longus, together with the deltoid, biceps, and brachialis internus. At the same time, in the experiment the flexors and extensors of the wrist were excited, while in the special form of paralysis noted they were exempt. This electrical method is a less precise mode of analysis than the pathological, for the double reason that (a) fibres whose nuclei are dissociated may pass together in the same root; (b) because the same muscles receive fibres from more than one root: thus the flexors and extensors of the wrist from the fifth as well as the fourth cervical. Thus when the nucleus of the latter was destroyed paralysis would be averted by means of the fibres coming from the fifth root.
The experiment and the pathological observation, however, concur in indicating that the fibres innervating the supinator longus, though passing to it in the path afforded by the radial nerve, afterward ascend in the cord to a ganglionic nucleus in close proximity to those of the upper-arm muscles specified—liable, therefore, to be affected with them. The purpose effected by such association is the supination of the arm.
It is excitation of the fourth root in Ferrier's experiment which gives [p. 1122] results most closely corresponding to Remak's observations. Excitations of the fifth and sixth root reveal other combinations, which Ferrier has found realized in adult's spinal paralysis. Thus in his second case, in addition to the group of muscles already mentioned, the rhomboid, infraspinatus, and serratus magnus were paralyzed, the last muscle indicating complication with the fifth root. In the third and fourth cases muscles supplied from the sixth root were joined to those innervated by the fourth and fifth—namely, the pectoralis major and latissimus dorsi.
In this upper-arm type the muscles affected are supplied by three different nerve-stems—the axillary, musculo-cutaneous, and the radial. In the forearm type the most common variety consists in paralysis of the extensors of the wrist, thus exactly imitating lead palsy.44 The supinator remains intact, the intrinsic muscles of the hand are sometimes intact, sometimes paralyzed. Sometimes, however, the extensors are relatively intact; the interossei are atrophied, and a clawed hand, resembling that characteristic of cervical hypertrophic pachymeningitis, is developed.45
44 It is on this fact, indeed, that Remak has been led to argue the spinal nature of saturnine paralysis (“Zur Pathogenie der Blei lahmung,” Archiv für Psych., Bd. vi., 1876).
45 The march of this disease, together with that of tabes dorsalis, furnishes data for localizing the nervous nucleus for the wrist extensors. In both diseases the lesion is ascending: in tabes disturbance of sensibility occurs first in the distribution of the sensory fibres of the ulnar nerve; in cervical pachymeningitis the flexors and intrinsic muscles of the hand are first paralyzed. Hence it is to be inferred that the central nucleus for the latter muscles lies in the lower, that for the extensor muscles in the middle, segment of the cervical enlargement of the cord.
The much greater frequency of extensor paralysis in the forearm type of anterior poliomyelitis indicates that the lesion of this disease begins about the middle of the cervical enlargement (see note).
The foregoing groupings have been made out almost entirely from cases of adult spinal paralysis or else of lead palsy. In the lower extremity it is much more difficult to establish such definite muscular association. Certain laws, however, can be made out: 1st. The liability to paralysis increases from the thigh toward the foot; thus, the muscles moving the thigh on the pelvis are the least liable to paralysis, then those moving the leg on the thigh, while the muscles moving the foot and leg and thigh are the most frequently paralyzed of any in the body. 2d. Of the upper thigh-muscles, the glutæi are not infrequently paralyzed, the ilio-psoas hardly ever, the adductors rarely except in total paralysis. 3d. Of the muscles moving the leg on the thigh, the quadriceps extensor is very frequently paralyzed—the most often, indeed, after the foot-muscles: the sartorius is almost always exempt; the liability of the hamstring muscles corresponds to that of the thigh adductors. 4th. At the foot the tibialis anticus often suffers from isolated paralysis, sharing in this respect the fate of the deltoid in the upper extremity—a fact already noticed by Duchenne. On the other hand, (5th) the tibialis anticus often remains intact while the other muscles supplied by the perineal nerve, the perineus longus and brevis, are completely paralyzed.46
46 Thus Buzzard relates a case of paralysis involving the quadriceps extensor and peroneal muscles, while the anterior tibial were intact.
The remarkable contrast in the morbid susceptibility of the quadriceps on the one hand, and the sartorius on the other, suggests dissociations of their nuclei. Remak relates one interesting case (Obs. 13) where the [p. 1123] sartorius was paralyzed—coincidently with the quadriceps, it is true, but also with partial paralysis of the ilio-psoas muscle, which is as rarely attacked as the sartorius itself. The two facts, taken together, would indicate that the nucleus of the sartorius lies high in the lumbar enlargement, in proximity to that of the ileo-psoas. The inference, continues Remak, is reinforced by functional considerations, since the sartorius, obliquely flexing the leg on the thigh, is generally in action at the moment that the psoas flexes the thigh on the pelvis.
Again: according to Remak the tibialis anticus is generally paralyzed together with the quadriceps extensor, although supplied by a different nerve.47 And this should be expected from the necessity of exciting dorsal flexion of the foot by means of the tibialis anticus at the moment of extending the leg for the act of walking.48
47 Obs. 14, 15, 16, 17, from Remak's essay.
48 At the moment that the foot is thus flexed, however, to allow the leg to be swung forward, the thigh and leg are both slightly flexed.
Ferrier, from his experiments on the roots of the lumbar plexus, is inclined to doubt this association of the tibialis anticus with the quadriceps, and he adduces Buzzard's case, already quoted, to show coincident paralysis of the quadriceps and peroneal muscles. It is not improbable, however, that fibres associated together in nerve-roots may again diverge in the cord, and thus the discrepancy would be explained.
DIAGNOSIS OF SPECIAL PARALYSIS.—Paralysis of isolated muscles may sometimes be concealed by the vicarious action of their synergists: thus of the extensor communis for the tibialis anticus. Paralysis of both legs and feet may even be partly concealed by the energy of the thigh-muscles, which, using the paralyzed segments of the limbs as inert supports, succeeds in effecting locomotion.49 On the other hand, in limbs apparently abandoned to total paralysis persevering search will often discover some muscles or parts of muscles which respond to faradic electricity: these must be considered as susceptible of ultimate recovery.
49 Thus in Cornil's famous case, Soc Biol., 1863.
The following table sums up some special diagnostic marks for the different paralyses50 afforded by the position of the limb and loss of movements:
Upper Extremity. Deltoid. Absence of deformity, which is averted by weight of arm. Inability to raise arm. Sometimes subluxation. Frequent association with paralysis, biceps, brachialis anticus, and supinator longus.
Lower Extremity. Ilio-psoas. Rare except with total paralysis. Associated with paralysis, sartorius. Loss of flexion of thigh. Limb extended (if glutæi intact).
Glutæi. Thigh adducted. Outward rotation lost. Lordosis on standing. Frequent association with paralysis of extensors of back.
Quadriceps extensor. Flexion and adducting of leg (if hamstrings intact). Loss of extension of leg. Frequent association with paralysis of tibialis anticus.
Tibialis anticus. Often concealed if extensor communis intact. If both paralyzed, then fall of point of foot in equinus. Dragging point of foot on ground in walking. Big toe in dorsal flexion (if extensor pollicis intact). The tendons prominent. Hollow sole of foot (if perineus longus intact).
Extensor communis. Nearly always associated with that of tibialis anticus. Toes in forced flexion.
Peroneus longus. Sole of foot flattened. Point turned inward. Internal border elevated.[p. 1124]
Sural muscles. Heel depressed. Foot in dorsal flexion (calcaneus). Sole hollowed if perineus longus intact; flattened if paralyzed. Point turned outward (calcaneo-valgus).
Extensors of back. Lordosis on standing. Projection backward of shoulders. Plumb-line falls behind sacrum (unilateral). Trunk curved to side. Trunk cannot be moved toward paralyzed side.
Abdominal muscles. Lordosis, without projection backward of shoulders.
50 See Duchenne, loc. cit., and also Roth, On Paralysis in Infancy, London, 1869.
After the paralysis the most remarkable symptom of anterior poliomyelitis is the rapid wasting of the paralyzed muscles. The atrophy begins within a week after the paralysis, and its progress is even more rapid than that following the section of a nerve. Sometimes all the flesh on a limb is shrivelled down to the bone; at other times the muscular atrophy is concealed by an abnormal development of fat, constituting a pseudo-hypertrophy. When all the muscles surrounding a joint are equally paralyzed and atrophied, no deformity develops,51 unless, indeed, the segment of a limb is used by means of the non-paralyzed proximate segment. In this case deformities may be produced by the effect of weight quite irrespective of muscular action, or in directions opposed to what we should expect from that.
51 Except talipes equinus.
The weight of the limb or a portion of it, by stretching paralyzed muscles, often aggravates their atrophy. This is most likely to occur with the paralyzed deltoid when the arm is unsupported, and with the anterior tibial muscles when the foot is allowed to drop.
Muscular atrophy occurs in the spinal paralysis of adults as well as in children; but in the latter alone does the atrophy extend to the bones and cartilages, tendons, fascia, ligaments, and blood-vessels. The osseous projections to which the muscles are attached waste; so do the epiphyses.52 The long bones are thinner and shorter, the foot is shorter, and the hand is shortened in paralysis of the upper extremity, even where this is limited to the upper arm, and the forearm is scarcely affected (Seeligmüller).
52 Seeligmüller, Centralbl. f. Chirug., No. 29, 1879.
In exceptional cases the limb may become even elongated from passive extension of the ligaments of the articulation. The bones may become soft and flexible, and break if pressure be applied.53
53 Ch. Salomon, “Des Lesions osseuses et articulaires lieés aux Maladies du Système nerveux,” Revue mensuelle, No. 8, 1878.
Atrophy of the bones stands in no fixed relation to that of the muscles, now exceeding, now falling short of that in intensity. This naturally progresses more slowly; still, within seven or eight months there may be a centimeter of difference between two limbs.
In marked contrast with this profound trophic disturbance of the bones is the intact nutrition of the skin. The absence of decubitus is indeed an important diagnostic mark from ordinary myelitis. The subcutaneous fat, however, wastes so completely that the skin seems to be closely adherent to the subjacent tissues, and cannot be pinched up into folds.
The temperature of the skin always falls; the limb is perceptibly colder to the touch than its fellow, and is often bluish and cyanotic. Heine has observed that the temperature diminishes gradually from the centre to the periphery, and at the coldest point may sink to 14° R.54 Hammond relates a case where the local temperature was 75° in an [p. 1125] atmosphere of 72°. The author says that exact measurements of surface temperature should be taken with Lombard's differential calorimeter, especially when convalescence is expected, as then a rise of temperature, however slight, is of most favorable augury.
54 Loc. cit., p. 16. This is not a difference of 14 degrees between the sound and paralyzed limbs, as is erroneously quoted by Seeligmüller (loc. cit., p. 67).
General factors contribute to the fall of temperature: diminished blood-supply from shrinkage of blood-vessels, or even atrophy of a certain number among these; loss of nerve-influence upon the oxidation processes; loss of muscular contractions, which should attract an afflux of blood. Among these factors the loss of nerve-supply is probably the most important, since the others exist in cerebral paralysis without causing the remarkable coldness characteristic of anterior poliomyelitis.
The atrophy of the blood-vessels is not always confined to the terminal twigs. The entire iliac artery, and even the lower part of the aorta, have been found markedly diminished in calibre.55 This shrinkage is unaccompanied by any change in the walls of the blood-vessels: it is a simple arrest of development. It strikingly illustrates the dependence of the blood-vessels on the vascular demands of the tissues they are destined to supply.
55 Charcot and Joffroy, Archives de Phys., 1870, case by Séguin, loc. cit., p. 9.
The changes which take place in the electrical reactions of the paralyzed limbs rank in importance with their paralysis and their atrophy. They serve to establish the diagnosis, to decide, to a large extent, the prognosis, and to measure the degree of nervo-muscular degeneration.
It is well known that the early diminution, and even entire loss, of faradic contractility was first emphasized by Duchenne as pathognomonic of infantile spinal paralysis. Contractility is diminished in from three to five days after the occurrence of the paralysis, and by the end of a week is completely lost in those muscles in which the paralysis is to be permanent. The muscles which recover spontaneously during the period of early regression recover their faradic with their voluntary contractility. In others, persistently but less profoundly paralyzed and susceptible of cure, the faradic contractility remains simply diminished and in unequal degrees. Progress to recovery under treatment is usually marked by progressive increase in the faradic response; but sometimes the power of voluntary contraction is fully regained, while the faradic response is still permanently lessened. The loss of faradic contractility is more complete and permanent in muscles irretrievably paralyzed by anterior poliomyelitis than in any other disease. These laws have been generally accepted by late observers.56
56 Simon disputes their validity, and declares that the importance of electricity in the diagnosis of spinal paralysis may easily be exaggerated (Union médicale, 7, 28, p. 942, 1879).
In 1868, Salomon discovered that muscles in which faradic contractility had been completely lost were nevertheless capable of contracting under the stimulus of galvanism—that this contraction is exaggerated, and sometimes occurs at the opening as well as at the closing of the circuit.57 The author remarks that the persistence of galvanic reaction after the complete loss of faradic contractility is completely analogous to an [p. 1126] observation of Brucke's on muscles poisoned by woorara,58 where the intramuscular termination of the nerve is paralyzed. It is to be inferred, therefore, in both cases that the muscular contraction results from direct irritation of the muscle, and implies the entire loss of influence from the nerve.
57 Jahrb. f. Kinderheilkunde, N. F. i., 1868. According to Erb (loc. cit., p. 984) and to Ross (loc. cit., p. 111), Salomon was the first to make this observation. Seguin, however, attributes priority to Lobb (Lond. Med. Times and Gaz., 1863), to Hammond (New York Med. Journal, 1865), and to J. Netten Radcliffe between 1863 and 1865. These dates precede that of the publication of Salomon's paper, but the latter seems to have been written without knowledge of earlier observations. (See also Onimus, Soc. de Biol., 1878, who argues that muscle-termination of nerve is partly destroyed.)
58 “Ueber den Einfluss der Stromes dauer auf die Elektrische Bewegung der Muskeln,” Sitzber. d. k. Akad. d. Wissensch. in Wien, 1867, Bd. lxi., quoted by Salomon, loc. cit., p. 388.
Erb has greatly extended these observations, and shown that the galvanic reactions of paralyzed muscles indicate their structural degeneration, and are identical with those observed after section of a peripheric nerve. There are three characteristic peculiarities in the contractions thus obtained: 1st, they are slow, tonic, long drawn out; 2d, they are more painful than in normal muscles submitted to an equal amount of electricity; 3d, in complete degeneration the contraction obtained at anode closure equals or exceeds in intensity that excited by cathode closure [AnSZ = or > KSZ]. The excitability of the muscle to the galvanic current remains increased for several months, then gradually diminishes, and finally falls below normal. The qualitative alterations persist somewhat longer: finally, the muscle fails altogether to contract.
Spinal paralysis differs markedly from progressive muscular atrophy in the absence of constant correlation between the degree of paralysis or atrophy and of electrical changes.
The last positive symptom to be noted in the paralytic stage of infantile paralysis is the diminution and ultimate loss of reflex excitability. This is correlative in time and extent with the loss of faradic contractility. This seems to be an exception to the usual rule, which associates loss of tendon reflex with lesion of the posterior columns or nerve-roots. This is a proof that interruption of the reflex arc at any point suffices to abolish the tendon phenomena.59
59 Buzzard tested the tendon reflex in the zygomaticus major in a patient in whom the sensory branch of the fifth nerve had been stretched, and therefore, to a certain extent insulted. The reflex response was decidedly lower than on the opposite side (Lancet, Nov. 27, 1880).
Negative Symptoms.—The negative symptoms of atrophic paralysis are as important for the diagnosis and pathogeny as are the positive characters, which have now been sufficiently detailed. The absence of decubitus or other nutritive lesions of the skin has been already mentioned. The absence of anæsthesia, or, as a rule, of any marked degree of hyperæsthesia, is most important as indicating immunity of the sensory tracts in the cord. Some diffused hyperæsthesia is sometimes noted during the febrile stage: pain is by no means rare in adults. But in children this is altogether absent, or else slight and transitory. On the other hand, the complete preservation of sensibility constitutes, in children, a serious obstacle to electrical investigation.
After subsidence of the cerebral symptoms, if any, of the initial stage, the functions of the brain are always intact60 and the disposition of the children apt to be remarkably lively. The general health is often remarkable for its vigor. The worst, because the most neglected, cases are naturally most often seen among the poor: the ranks of professional beggars are largely recruited from among the victims of infantile paralysis.
60 Practically, it may often be of importance for the physician to ascertain that an intellectual enfeeblement, or even idiocy, existing at the time of examination had preceded the onset of the paralysis by months or years.[p. 1127]
The chronic stage is marked by the development of a new set of symptoms—contractions of certain muscles surrounding one or more joints and deformed positions of the limbs. These symptoms do not always appear. If all the muscles surrounding a joint are completely paralyzed and extensively atrophied, and if no weight is imposed on the limb by the action of a non-paralyzed upper segment, and if the paralyzed segment be so supported that its own weight does not approximate the insertion-points of muscles, and thus cause their passive retraction, then there is no deformity, but a dangling limb, a membre de Polichinelle.
Laborde states that contractions appeared at the earliest about two months after the paralysis. Seeligmüller, however, has seen pes equinus and pes calcaneus develop in four weeks. The date is partly, at least, determined by the time at which the children try to walk or otherwise to use the paralyzed limbs; and the deformities are very much more marked in the lower extremities, proportioned to the much greater weight which they are obliged to sustain.
All varieties of club-foot, and most frequently equino-varus, knock-knees, rigid flexions at the knee and hip, cyphosis, lordosis, and colossal scoliosis may develop as manifold consequences of atrophic paralysis. That subluxation of the humerus and the claw-hand may occur in the upper extremities has already been mentioned.
In Seeligmüller's 75 cases, 53, or 71 per cent., exhibited some kind of deformity. Among these, 43, or 56 per cent., were of the foot; 6 were cases of subluxated humeri; 5, easily-reducible luxation of the fingers.
The following table contains a summary of the deformities observed as a consequence of atrophic paralysis. They are distinguishable from congenital deformities dependent on altered relations of articular surfaces through defective development61 by being easily reducible. This remark especially applies to paralytic club-foot:
| Foot. | Equinus. Equino-varus (varus hardly ever alone). Calcaneus. Calcaneo-valgus. Valgus. |
| Knee. | Genu-recurvation. Genu-incurvation. Permanent flexion. |
| Hip. | Luxation. Permanent flexion. Permanent adduction. |
| Hand. | Flexion fingers or wrist (rare). Extension of wrist. Claw-hand. |
| Elbow. | No deformity (Seeligmüller). |
| Shoulder. | Subluxation humeri. |
| Trunk. | Dorsal scoliosis. Lateral incurvation lumbar region. Cyphosis. Lordosis with backward projection of shoulders. Lordosis without backward projection of shoulders. |
61 Volkmann's Handbuch, Billroth und Pitha.[p. 1128]
Mechanism of Deformities.—From what has been said on the cases in which deformities are absent it is evident that one at least of three conditions are required for their production: the paralysis must be unequally distributed in the muscles surrounding a joint; pressure must be exerted by the weight of the body or traction by the weight of the limb; effort must be made to utilize the maimed part of the limb by means of other parts, or even by the muscles of the trunk.
The share taken by these different factors in the production of deformities has been differently estimated by different observers. The French surgeon Delpech was the first to explain the phenomenon on the theory of muscular antagonism. The same theory has been most minutely elaborated by Duchenne.62 According to it, the intact or less paralyzed muscles, in virtue of their tonus, constantly tend to draw the segment of the limb on which they act in a direction opposed to that in which it should be drawn by the paralyzed muscles. Since this action is unantagonized, its influence persists; the insertion-points of the contracting muscle being permanently approximated, the nutrition of the muscle is modified: it grows shorter (adapted atrophy). There results finally shortening and retraction of the muscles on one side of the joint, over-stretching of those on the other.
62 De l'Électrisation localisée, 1861.
Duchenne used to illustrate this theory by means of a skeleton supplied with artificial muscles, whose successive section would cause the appearance of the corresponding deformity. Werner63 first protested against this theory, and the protest has been further developed and a different theory built up through the efforts of Hueter64 and Volkmann.65 The latter observes that the muscles and ligaments surrounding a joint normally receive a large amount of the weight falling upon its articular surfaces. Removal of this elastic resistance exposes these surfaces to the full force of the pressure, and thence to almost certain danger of deformity—a danger, therefore, always incurred after paralysis of the muscles. Thus, the weight of the body, pressing, unresisted, on the arch of the foot, is able to displace the bones of the arch from their normal relations and completely flatten the arch.
63 Reform der Orthopædie, 1845.
64 Gelenkkrankheiten.
65 Sammlung klin. Vort., No. 1.
A position of ease is that in which the movement of the joint has been pushed as far as possible until limited by the passive resistance of the ligaments or the conformation of the articular surfaces. The weight of the body must then be so placed that the line of gravity falls on the side of the open angle, while the limiting bands stretch across the base. Thus, a tired man sits with a curved back; the muscles which may extend the spinal column in a straight line are relaxed; the column falls forward until arrested by the anterior vertebral ligaments. Thus, in standing at ease the thigh presses against the leg, so as to form a wide angle open anteriorly. When the quadriceps extensor is paralyzed, this position is inevitable and exaggerated, since the force which might counteract it, contraction of the thigh extensor, has been removed.
Formerly, the rôle of muscles in this elastic resistance was under-estimated and that of ligaments exaggerated.
CRITICISM OF THE THEORY OF MUSCULAR ANTAGONISM.—Three considerations have been urged in objection to the theory of muscular [p. 1129] antagonism: First, deformities may develop even in limbs totally paralyzed, provided these limbs be subjected to weight and pressure. Pes equinus, the most common form of paralytic club-foot, develops with total paralysis of the muscles of the leg where the child does not walk, but is carried on the arms of a nurse with its foot dangling. The part of the foot anterior to the ankle-joint being longer and heavier than that behind, the point falls; the tendo Achillis is passively shortened, and by nutritive adaptation to this position may become permanently retracted. Long persistence in this position accustoms the dorsal surface of the bones to a less degree of pressure than the plantar surface: as a consequence, the growth of the bone becomes more active above, while it is arrested below; the arch of the foot is increased until the sole is curved into a deep hollow; and the plantar aponeurosis is correspondingly shortened.
Volkmann relates a case where this same deformity appeared without the least paralysis, but simply from prolonged passive extension of the feet in bed. The patient was an adult, and suffered from a severe typhoid with a double relapse. After recovering from the fever a year of orthopædic treatment was required to restore the feet to their normal position.
The second objection is the absence of any proof of such constant tonus in the muscles as may be sufficiently powerful to determine the position of a limb. Such tonus exists in the involuntary muscles, especially in those of the blood-vessels, but there is no evidence that it exists in the voluntary muscles. To this Seeligmüller has replied by admitting the objection to the theory as thus proposed, but substituting the more plausible influence of repeated contractions on the part of the non-paralyzed muscles. Each contraction draws the limb in a certain direction, and there it tends to remain, because there is nothing to antagonize the force which it has obeyed.
The third objection is that examination of individual cases not infrequently shows displacements in directions opposed to that which should be determined by muscular antagonism. Volkmann has especially illustrated the latter assertion by the mechanism of genu-recurvation. In paralysis of the quadriceps extensor of the tibia the weight of the body is exercised, not merely from above downward, but from without inward, falling, therefore, on the inner malleolus. It thus tends to press the anterior part of the foot outward,66 and a valgus finally complicates the calcaneus. Seeligmüller, however, quotes two cases of pes calcaneus developed in children who had never walked: in one paralysis of the sural muscles had occurred at the age of four weeks, and the other case was observed at the age of fourteen weeks. Seeligmüller remarks that only early examination of the faradic contractility of a group of paralyzed muscles can decide whether any among them preponderate during a time sufficient to fix the limb in a vicious position. Thus in one case of pes calcaneus he found two years after the occurrence of the paralysis that some contractility still persisted in the dorsal flexors, but six months later this had quite disappeared. Had the examination then been made for the first time when all the muscles were equally paralyzed, it would have seemed impossible to explain the deformity by muscular antagonism.
66 Sayre asserts that lateral rotation cannot take place at the ankle-joint, but at the medio-tarsal articulation. Hueter also refers pes varus and pes valgus to the talo-tarsal articulation.[p. 1130]
RELATION OF WEIGHT AND MUSCULAR FORCES.—The influences of weight and of muscular action sometimes concur, sometimes are opposed to each other. Thus, the weight of the foot alone always tends to produce equino-varus; it acts therefore to intensify the action of the sural muscles when the anterior tibial are paralyzed, but to diminish the influence of paralysis of the gastrocnemius when the foot is being drawn into dorsal flexion. Hence one reason for the comparative rarity of pes calcaneus.
Paralytic deformities at the hip and knee are much rarer than those of the foot. At the hip this immunity is partly due to the relative rarity of paralysis in the muscles surrounding the joint—still more to the fact that the weight of the limb tends to correct excessive flexions. These are therefore more likely to occur in children allowed to remain in bed than in those who are encouraged to walk by means of suitable apparatus. The use of crutches, however, favors the development of deformity, because, since with paralysis of the thigh- or leg-muscles pes equinus nearly always exists, the thigh is unduly lengthened. To palliate this inconvenience the patient instinctively flexes the knee or hip, or both, and the position tends to become permanent.
When the flexion is rigid and extension becomes impossible, the gastrocnemii are relaxed until they lose their power of tension, and thence of fixing or raising the heel. Further, as by the flexion the limb is moved in front of the body, it is necessary to project the body forward again over the support. Hence a lordosis is developed, to be distinguished from that caused by paralysis of the vertebral extensors (a) by the rigid flexion of the thigh; (b) by the facility with which the patient can extend the back as soon as he is placed in a sitting position.
Although the quadriceps extensor is so frequently paralyzed, rigid flexion at the knee—such as on the theory of muscular antagonism might be expected from the action of the hamstring muscles—is very rare. As already observed, it occurs, if at all, in neglected children allowed to lie or sit with the leg partly flexed. In those who attempt to walk the leg is not flexed, but forced into hyper-extension by the following mechanism: The muscles inserted on the upper part of the thigh swing the leg forward like a passive support. Afterward the body bends forward over the support, and its weight, pressing from above downward and from before backward, and pressing the articular surfaces of the joint together, forces the head of the tibia backward until the movement is checked by the posterior ligaments. The deformity is the same whether the quadriceps or one or all the muscles surrounding a joint are paralyzed (Volkmann).
DISLOCATIONS.—Dangling limbs are, however, much more frequently the consequence of total paralysis, with extraordinary relaxation of the ligaments of the joint permitting dislocation. Reclus67 has published several such cases. Verneuil has even suggested that congenital luxation of the hip-joint always depends on an intra-uterine spinal paralysis.68<
67 Revue mensuelle de Méd. et de Chir., Mars, 1878.
68 Quoted from Seeligmüller.
In the upper extremities rigid contractions are much less frequent, even in proportion to the number of paralyses. Seeligmüller has seen five cases of reducible flexion of the fingers, and one of permanent extension of the wrist and fingers, associated with paralysis [p. 1131] of all the flexors. In this case, if the arms were so suspended that the hand hung freely, its weight gradually overcame the action of the extensors and the fingers fell into flexion. Upon any attempt at exertion the hyperextension was reproduced.
DEFORMITIES OF THE TRUNK.—Scoliosis will be caused when, with unilateral paralysis of the extensors of the vertical column, the lower part of the trunk is drawn to the non-paralyzed side, and the upper half is bent over the paralyzed side in order to restore the balance. In bilateral paralysis of the extensors both shoulders are projected backward, so that a plumb-line dropped from between them falls behind the sacrum, and lordosis is developed, although the lumbar column is not projected forward. The same form of lordosis occurs when the glutæi are paralyzed. When, however, the abdominal muscles are paralyzed, the lumbar column is really projected forward, and then a plumb-line dropped from the shoulders passes over the sacrum.69
69 Duchenne, loc. cit., 1861.
PARALYSIS OF THE ABDOMINAL MUSCLES.—Unilateral paralysis of the extensors of the back is often difficult to detect in young children. Seeligmüller recommends that the child be laid across the mother's knees and told to move the trunk from one side to the other while the pelvis is held firm. If too young to obey the direction, the movement can be excited by pricking or by electric irritation. It will be seen that the trunk can be turned only to one side.
In these paralyses of the trunk it is clear that the deformity does not develop under the influence of muscular antagonism alone, but only when the non-paralyzed muscles attempt to sustain the superincumbent weight of the body or a portion of it.
SUMMARY OF MECHANISMS OF THE DEFORMITIES.—We may indeed conclude, as stated at the beginning, that this complex etiology exists in almost all cases. When the limb is at rest in bed or the weight of the body is transferred to crutches, then repeated contraction of the flexus will suffice to bring the limb into a vicious position (contraction at knee- and hip-joint). When the foot or hand hangs unsupported, its weight is sufficient to cause deformity, even when all the muscles are paralyzed, and sometimes in opposition to the direction of intact muscles. Thus the weight which is passively borne by the limb, and the efforts of intact muscles to effect the function of the limb in spite of the paralysis, both concur in the production of the deformity.
ANATOMICAL LESIONS.—The theory of the anatomical basis of infantile paralysis constitutes one of the most interesting portions of its history. It is indeed one of the most instructive chapters of modern pathology from the rapidity with which in a short time precise knowledge has accumulated, and for the degree in which this has revolutionized previous ideas.
Autopsies.—Until 1863 only five autopsies had been made upon persons affected with infantile paralysis.70 As the disease was never, of itself, [p. 1132] fatal, opportunity for pathological investigation did not present itself, while attention was still vividly attracted to the paralysis. When this had become a chronic infirmity, and patients had succumbed to intercurrent disease, the opportunity must have occurred, but was not then utilized.
70 I believe the first list of modern autopsies was made by myself in a paper read before the New York County Medical Society, Dec. 22, 1873. The paper was not published until May, 1874, and in the mean time Seguin's lecture on “Infantile Paralysis” was published in the N. Y. Med. Record, Jan. 15, 1874, with a tabulated list of 25 autopsies, necessarily almost identical with mv own—cases 9 and 10 are really identical. A case by Roth is included; 4 negative autopsies are omitted. In 1880, Seeligmüller, in his elaborate essay in Gerhardt's Handbuch, published a list of 32 cases, including the above, and adding to them the following: Case by Müller, 1871; 4 cases by Leyden, 1875 (Arch. de Psych.); 1 case by Raymond, 1874 (Gaz. méd. de Paris); 1 case by Demme, 1876 (B. med. Bericht über das Jennerischt Kinderspital zu Bern); 1 case by Eisenlohr, 1876 (Tageblatt des Hamburger Naturforscher Versammlung); 1 case by Schultze, 1877 (Virch. Arch., Bd. lviii.).
To this list we may now add 3 cases by Turner, Humphrey, Taylor, 1881 (Path. Trans. London); 2 cases by Dejerine, 1878 (Progrès méd.), giving a total of 37 cases with detailed histories and autopsies.
The first cases affording autopsies in which the spinal cord was thoroughly investigated, belonged, however, precisely to this class of extremely chronic lesions, which should be regarded as showing rather the results of the morbid process than that process itself. Omission to observe this distinction has been the occasion of several misinterpretations of the pathological appearances.
Premature Theories.—In the entire absence of evidence it is a little remarkable that such high authorities as Rilliet and Barthez,71 West,72 Vogel,73 Eulenburg,74 should have pronounced dogmatically that the disease was essential—i.e. unaccompanied by any structural lesion whatever; and that Bouchut,75 on the strength of most incomplete examination, should have built up a theory of myogenic paralysis. It is still more remarkable, after the published autopsies of Rinecker,76 Laborde,77 Cornil,78 Prévost,79 Charcot and Joffroy,80 Parrot and Joffroy,81 Vulpian,82 Roger and Damaschino,83 that Politzer in 1866,84 Brown in 1871,85 Barwell in 1872,86 Kétli,87 Adams in 1873,88 should still adhere to this doctrine. They are, however, entirely in the minority, and all recent monographs and works published with a view to presenting the state of science assume the spinal nature of infantile paralysis to be established beyond possibility of controversy.89
71 Traité des Maladies des Enfants.
72 Diseases of Children, Am. ed., 1860.
73 Diseases of Children, trans. from 4th ed., 1870.
74 Arch. Virchow, Bd. xvii. 1859.
75 Deutsche Klinik, 1863.
76 Gaz. méd., 1864, Soc. de Biol., 1864.
77 De la Paralysie de l'Enfance.
78 Gaz. méd., 1866, Soc. de Biol., 1866.
79 Arch. de Phys., 1870, p. 134.
80 Ibid., p. 310.
81 Ibid., p. 316.
82 Bouchut is said by Simon (loc. cit.) to be alone in his theory; Kétli, however, agrees with him. Eulenburg, in 1872, in his systematic treatise, assigns a central origin to infantile paralysis, but offers no opinion in regard to its nature.
83 Gaz. méd., 1871.
84 Jahrbuch für Kinderkrankheiten, 1866.
85 Compend. für Kinderkrank., p. 161.
86 Lancet, 1872.
87 Jahrbuch für Kinderkrank., 1873.
88 Treatise on Club-foot.
89 See Seguin, loc. cit., 1874; Erb, Ziemssen's Handbuch, Bd. xi.; Seeligmüller, Gerhardt's Handbuch der Kinderkrankheiten; Ross, Treatise on Diseases of Nervous System, vol. ii.; Hammond, Diseases of Nervous System, 6th ed., 1881, etc. etc.
The following table contains a summary of the seven autopsies in which the spinal cord is said to have been examined with negative results. Of these, the only really important case is the third, in which a microscopic examination, made by so competent an histologist as Robin, was said to have discovered no lesion of the cord.
[p. 1133]The foregoing autopsies may be tabulated as follows:
| No. | Year. | Name of Author and Patient. | Age at time of Paralysis. | Age at time of Autopsy. | Nature of Symptoms. | Limbs Paralyzed. | Electric Reaction. | Appearances at Autopsy. | Reference in Literature. |
| 1 | 1850 or '51? | Rilliet and Barthez. | ? | ? | ? | l. o. | ? | Negative. | Gaz. méd. de Paris, 1850 (or '51?) p. 681. |
| 2 | 1850 or '51? | Rilliet and Barthez. | ? | ? | ? | b. u. | ? | Negative. | Ibid. |
| 3 | 1867 | Bouchut and Robin. (Angélique Lermain). | 1½ | 3 | Suddenly after 3 days' fever. | both u. | Negative micro- scopically. |
Union méd., 1867, No. 130, p. 187. | |
| 4 | 1873 | Adams. | — | — | — | — | — | Negative. | Treatise on Club-foot, p. —. |
| 5 | 1873 | Elischer and Kétli. | — | — | — | — | — | Negative. | Jahrb. Kinderheilk., 1873. |
| 6 | 1873 | Elischer and Kétli. | — | — | — | — | — | Negative. | Ibid. |
Heine, in the absence of autopsies, but arguing from clinical symptoms alone, already inferred the existence of a spinal lesion as cause of the paralysis, and believed that it consisted in congestion, or even in hemorrhagic exudation, capillary or massive, which should compress the cord and result in partial atrophy. The same opinion is advanced in 1844 by Brunnière,90 also by Vogt,91 in 1868 by Salomon92 and Radcliffe.93 The autopsies contained in the following table, in all of which vascular lesions are prominent, might be invoked in support of this view:
| No. | Year. | Name of Author and Patient. | Age at time of Paralysis. | Age at time of Autopsy. | Nature of Symptoms. | Limbs Paralyzed. | Electric Reaction. | Appearances at Autopsy. | Reference in Literature. |
| 7 | 1829 | Klein. | 5 | 5 | Persistent cerebral symptoms. | l. o. | ? | Congestion of pia around roots of left brachial plexus. | Quoted by Heine. |
| 8 | 1855 | Brund. | 1 | 5 | Meningitis? | r. u. | ? | Chronic spinal klepto-meningitis. | |
| 9 | — | Hammond. | 4 yrs. stand. | — | l. u. | ? | Encysted clot in left ant. column, lower dorsal cord. | Journ. Psych. Medicine, 1867. | |
90 Krankheiten des Gehirns und Ruckenmarkes.
91 Lahmung der Kinder, p. —.
92 Jahrb. f. Kinderheilk., 1865.
93 Reynolds's Syst. of Medicine.
The first really modern autopsy, that made by Cornil in 1863, agrees with the two earliest on record in disclosing only an atrophy of the cord. Some of the other cases, contained in Table III., note in addition sclerosis of the lateral columns.
In all the remaining autopsies on record are noted atrophy of the anterior gray cornua and more or less extensive destruction of the ganglionic cells.
In a certain number of cases the atrophy seemed to be the unique lesion. But it never was confined to the ganglionic cells, but included the reticulum of gray fibres in which these were imbedded, and which [p. 1134] was replaced by a reticulum of connective tissue. These cases were all examined many years after the occurrence of the paralysis.
| No. | Year. | Name of Author and Patient. | Age at time of Paralysis. | Age at time of Autopsy. | Nature of Symptoms. | Limbs Paralyzed. | Electric Reaction. | Appearance at Autopsy. | Reference in Literature. |
| 10 | 1825 | Hutin. | 7 | 49 | Convulsions. | b. u. | ? | Atrophy of cord from below 8th dorsal nerve to thickness pencil, and of nerves. | Quoted by Heine, p. 151. |
| 11 | 1842 | Lunget. | ? | 8 | ? | r. u. | ? | Atrophy and brown discol. of ant. roots of lumbar and sacral nerves going to sciatic. | Anat. et Phys. du Syst. nerveux, i. p. 358. |
| 12 | 1863 | Reckling- hausen. |
? | ? | ? | b. u. | ? | Atrophy of ant.-lateral columns. | Deutsche Klinik, 1863, Jan. 3. Seel. says also atrophy of cells; Seguin and J., tubercles. |
| 13 | 1863 | Cornil. | 2 | 49 | ? | b. u. | ? | Atrophy antero-lateral columns. Seeligmüller says also atrophy of ganglion-cells, as if quoting Charcot. |
Soc. de Biol., Comptes Rendus, 1863. Infiltration of gray and white corpuscles, with abundant amyloid corpuscles, especially in anterior gray cornua. These through entire extent of cord—cells—intact. Paraplegia, but walks by muscles of thigh and pelvis; leg and foot atrophied. |
| 14 | 1864 | Laborde and Bouvier. | 1 | 2 | ? | all four. | noted. | Atrophy antero-lateral columns; nerve-fibres atrophied and varicose. | Laborde, De la Paralysie de l'Enfance, pp. 109-119. |
| 15 | 1864 | Laborde and Cornil. | ⅔ | 2 | ? | b. u. | ? | Sclerosis of ant.-lateral columns. Ganglion-cells normal; sciatic neuritis. |
Laborde, loc. cit., p. 104. |
The first group is contained in the following table:
| No. | Year. | Name of Author and Patient. | Age at time of Paralysis. | Age at time of Autopsy. | Nature of Symptoms. | Limbs Paralyzed. | Result of Autopsy. | Reference in Literature. |
| 16 | 1866 | Prévost. | ? | 78 | ? | L. u. | Atrophy of left anterior cornu, especially of ganglion-cells. | Comptes Rendus, Soc. Biol., Gaz. méd., 1866. |
| 17 | 1870 | Charcot and Joffroy. | 7 | 32 | Sudden. | All esp. l. u. | Atrophy of cells ant. horns and ant. lateral columns. | Archives de Phys., 1870. |
| 18 | 1870 | Parrot and Joffroy. | — | 3 | Unknown. | B. l. | Atrophy and partial sclerosis of anterior cornua and ant. lat. columns. | |
| 19 | 1870 | Vulpian. | ? | 66 | ? | L. l. | Atrophy of ganglion-cells, sclerosis of [p. 1135] antero-lateral columns. | Archives Physiol., 1870. |
| 20 | 1871 | Müller. | 4 | 34 | Fall from bed. | L. lower. | Atrophy of ganglion-cells ant. cornua; sclerosis of anterior roots. | Quoted by Seeligmüller, Gerhardt's Handbuch, Tabeln. |
| 21 | 1873 | Lancereaux and Pierret. | 2 | 18 | ? | L. upper. | Atrophy of external group cells in ant. cornua; general atrophy of left half of lumbar cord. | Petitfils, Thesis on Atrophie aigue des Cellules motrices, 1873, p. 33. |
| 22 | 1875 | Raymond. | ? | 75 | ? | R. arm. | Atrophy of ganglion-cells in right ant. horn cerv. region. | Gaz. méd de Paris, No. 19, 1875. |
| 23 | 1879 | Taylor. | 1½ | 3 | 3 days' fever. | L. leg. | Atrophy of left ant. cornua; disappearance of ganglion-cells; no lesion in white column. | Trans. Path. Soc. London, 1879. |
| 24 | 1875 | Dejerine. | — | — | — | R. foot (congenital equinus). | Atrophy of ant. horn right side; atrophy external group of motor-cells. | Arch. Phys., 1874. |
| 25 | 1879 | Humphreys. | 1½ | 3½ | ? | L. leg. | Atrophy of left half lumbar cord; disappearance of medial group cells both sides; antero-lateral on left side. | Trans. Path. Soc. London, 1879. |
In the remaining cases the ganglion-cells of the anterior cornua had also disappeared; but in addition to this atrophy excited distinct evidence of more or less extensive inflammation. This table includes one case of autopsy at two months (Roger's); one at six weeks after paralysis (Turner's).
| No. | Year. | Name of Author and Patient. | Age at time of Paralysis. | Age at time of Autopsy. | Nature of Symptoms. | Limbs Paralyzed. | Appearance at Autopsy. | Reference in Literature. |
| 26 | 1866 | Echeverria. | 3 | 10 | Fever. | R. arm, R. leg. | Granular pigmentation anterior cornua, diffuse myelitis. | Quoted by Seguin, loc. cit. |
| 27 | 1866 | Echeverria. | 2 | 2½ | Febrile diarrhœa. | Both legs. | Ibid. | Ibid. |
| 28 | 1871 | Roger and Damaschino. | 15/6 | 2 | Scarlatina with second attack. | L. arm, then both legs. | Foci of softening throughout cord. Atrophy ganglion-cells and nerve-fibres. Dilatation, fatty degen. vessels. Sclerosis ant. columns. Atrophy ant. roots. | Gaz. méd. de Paris, 1871. |
| 29 | 1871 | Roger and Damaschino. | 2 | 2½ | Variola. | Both legs. | Foci of softening in ant. cornua. Fatty degen. blood-vessels, circumscribed myelitis. | Ibid. |
| 30 | 1871 | Roger and Damaschino. | 2 | 3 | Fever. | Ibid. | Foci of softening, as above. | Ibid. |
| 31 | 1873 | Roth. | 1 | 2 | Ibid. | Ibid. | Focus myelitis on both sides. Disappearance ganglion-cells, abundant exudation corpuscles. | Virch. Arch., 1873, Bd. lviii. |
| 32 | 1868 | L. Clarke. | 1 | 32 | After inoculation. | Both arms. | Extensive myelitis ant. and central part gray [p. 1136] matter. Disappearance ganglion-cells. | Med.-Chir. Trans., li. p. 219. |
| 33 | 1876 | Schultze. | 3 | 22 | Acute disease. | Both legs. | Atrophy lumbar cord ant. lat. columns. Atrophy ganglion-cells. Abundant exud. corpuscles. Proliferation neuroglia. | Virch. Archiv, Bd. lxviii., 1876. |
| 34 | 1876 | Leyden. | 2 | 60 | Fall from table. | L. leg. | Circumscribed cicatrix with complete destruction gray substance. Amyloid degeneration. Atrophy ant. roots. | Archiv f. Psych., 1876, Bd. vi. |
| 35 | 1876 | Leyden. | ¾ | 1¾ | Suddenly. | L. leg. | Atrophy ganglion-cells. Cellular diffused infilt. (myelitis) gray subst'ce. | Ibid. |
| 36 | 1876 | Leyden. | 4 | 58 | Sudden over night. | L. leg. | Amyloid infiltration ant. horns, atrophy ganglion-cells left lumbar horn. Diffuse atrophy gray substance. | Ibid. |
| 37 | 1876 | Leyden. | 3 | 20 | Ibid. | R. leg, L. arm. | Sclerotic focus in right lumbar and in left cerv. region. Diffuse meningo-myelitis. Atrophy ant. lat. columns. Encapsulated myelitis. | Ibid. |
| 38 | 1876 | Demme. | ? | 3½ | ? | — | Purulent focus in ant. cornua lumbar region. Atrophy ganglion-cells. | Quoted by Seeligmüller, loc. cit., p. 18. |
| 39 | 1876 | Eisenlohr. | ? | ¾ | ? | B. legs. | Diffuse inflammation anterior horns and ant. lat. columns. | Ibid. |
| 40 | 1879 | Turner. | 2½ | 2¾ | ? | Myelitic disorganization gray substance ant. cornua lumbar cord. | Trans. Path. Soc. Lond., 1879. | |
| 41 | 1883 | Archambault et Damaschino. | 30 m's | 31 m's, or 26 d'ys fr. début. | Malaise and prostration one day. | Left leg and right arm. | Focus red softening ant. horns left lumbar; right cervical region. Enormous enlargement vascular network, and distension blood-vessels; granular corpuscles in lymphatic sheaths; marked atrophy cells and of myeline sheaths of fibres in ant. roots; myeline balls in sheath; axis-cylinders disappeared. Lesions more or less marked throughout cord. Nerves not examined. | Le Union médicale, 1883. |
| 42 | 1884 | Money. | 2 yrs. | 28 m's. | Fever and vomiting for a week. | Paraplegia. | Red area both anterior cornua lumbar region. Here distension and thrombosis vessels; infiltration leucocytes; absence multipolar cells. | Trans. Path. Soc. Lond., 1884. |
| 1884 | Money. | Unknown | 7 yrs. | Unknown. | Right leg. | Wasting anterior horn almost throughout lumbar region. Atrophy cells chiefly in ant., ant.-lat., post.-lateral, and central groups, replaced by dense nucleated tissue. |
It will be useful to add another table, which will group together the cases in which the autopsies were made within two years after the occurrence of the paralysis. Of these, all but the two made by Laborde, in which the cornua are declared to be healthy and the lesion limited to the [p. 1137] white columns, show traces of destructive morbid processes in the gray substance of the cord, greatly predominating in the anterior cornua, but not absolutely limited to them, nor even to the part of the cord which corresponds to the paralyzed limb:
| Case No. | Name of Author. | Date of Autopsy after Paralysis. |
Year of Publication. |
|
| 41 | Damaschino. | 6 | weeks. | 1883 |
| 40 | Turner. | 26 | days. | 1879 |
| 28 | Roger and Damaschino. | 2 | mos. | 1871 |
| 42 | Money. | 4 | mos. | 1884 |
| 27 | Echeverria. | 6 | mos. | |
| 39 | Eisenlohr. | 6 | mos. | |
| 29 | Roger. | 6 | mos. | 1871 |
| 31 | Roth. | 9 | mos. | 1873 |
| 35 | Leyden. | 11 | mos. | 1876 |
| 14 | Bouvier and Laborde. | 12 | mos. | 1864 |
| 30 | Roger. | 13 | mos. | 1871 |
| 15 | Cornil and Laborde. | 16 | mos. | 1864 |
| 12 | Recklinghausen. | 24 | mos. | 1863 |
| 38 | Demme. | 24 | mos. | 1876 |
| 23 | Taylor. | 18 | mos. | 1879 |
| 25 | Humphrey. | 24 | mos. | 1879 |
AUTOPSIES OF RELATIVELY RECENT CASES.—In cases relatively recent all macroscopic changes in the cord may be entirely wanting. There may be some degree of asymmetry in the surface of section, patches of white coloration in the anterior gray substance, or of gray or yellow color in the white columns; the anterior roots may be congested or even already atrophied.94 On the other hand, there have several times been found foci of visible red softening, much more frequently at a point corresponding to the origin of the paralyzed nerves, but not absolutely confined to them, and sometimes existing at points where they have given rise to no symptoms whatever.95
94 Roger's first case, No. 28 of Table V.
95 Case 1st of Roger, Tab. V.
Microscopic Lesions.—In striking contrast with this paucity of macroscopic lesions are the interesting structural changes revealed under the microscope. These lesions are usually comprised within circumscribed foci whose size may vary from a long diameter of 2 mm.96 to one of from 10 to 30 mm.97 Sometimes bilateral foci are found with monoplegic paralysis; thus one side or the other preponderates in the morbid process.
96 Case Roth, Tab. V.
97 Case Schulze, Tab. V.
In recent cases (Damaschino's, at twenty-six days; Roger's, at two months; Turner's, at six weeks) patches of red softening existed at the portions of the cord containing the nuclei of origin of the paralyzed nerves. In Turner's case the focus contained hemorrhagic extravasation, and the traces of this were clearly perceptible in Roger's first case. The blood-vessels are dilated; their lymphatic sheaths infiltrated with leucocytes and with granular corpuscles; their walls are thickened, pigmented, or fatty.
[p. 1138]Leucocytes are often disseminated through the diseased area, and in one case (Demme) were accumulated into a focus of pus. Besides the leucocytes, the foci are often infiltrated with large round granular cells that seem to be transformed neuroglia-cells (Leyden). In one case neuroglia nuclei were accumulated in a ring around the focus, seeming to indicate the beginning of encapsulation.
The most striking lesion, however, and the one which is common to the most recent as well as to old cases, is the deformation, atrophy, and final disappearance of the large ganglionic cells of the anterior cornua. The first change consists in granular pigmentation;98 then the prolongations disappear, leaving the body of the cell shrunken and deformed; at last the whole cell disappears. Sometimes all the cells of an anterior horn have disappeared throughout the entire depth of the focus; quite as often, in certain sections at least, the atrophy is limited to certain groups, as the external,99 or the external in one focus, the antero-lateral in another, situated on the opposite side of the cord.100
98 Case of Echeverria, Tab. V.
99 Case by Schultze (this is a case of ancient lesion), Tab. V. (Virch. Arch., Bd. lviii.).
100 Case by Taylor, Tab. IV. (Path. Trans., London, 1879.)
In a case rendered celebrated by Charcot it is stated that in many sections of the cord atrophy of ganglionic cells constituted the unique alteration, the tissue immediately surrounding the place whence they had disappeared being perfectly healthy. It is on this appearance that has been built up the theory of a primary idiopathic atrophy of the ganglionic cells as the characteristic lesion of infantile paralysis. But in other portions of the same cord Charcot himself describes destruction of the gray reticulum imbedding the cells; and this destruction is insisted upon in many other observations. In other words, there is a general disintegration of the gray nervous tissue of the anterior cornua which contain the focal lesion. The normal tissue is then replaced by a reticulum of conjunctive fibres, more or less dense according to the age of the case.
These focal lesions of the cord explain admirably, as will be seen, the permanent symptoms of the disease. But of great importance for understanding its initial period is the fact that structural changes—similar to, but less severe than, those just described—have beer found diffused throughout the cord. In several cases hyperæmia, partial atrophy of ganglionic cells and nerve-fibres, infiltration with exudation corpuscles, in the anterior cornua and even central gray canal from the lumbar to the cervical region.101 In Damaschino's case, besides the focal lesions which corresponded to the paralyses of the right arm and left leg, were others corresponding to the left arm and right leg where no paralysis existed.
101 See cases by Leyden, Roth, Schultze, Clarke, Damaschino.
This case (1883) is also interesting in bringing out another lesion not usually noticed. This is the breaking up into balls of the myeline in the medullated tubes, both of the anterior intraspinal nerve-roots and of such fibres as traversed the anterior nerves. In balsam preparations these myeline drops are dissolved; but in osmic acid and glycerin preparations they appear as black balls all over the field. The lesion is identical with that already described by Dejerine (1875) in both nerves, roots, and white columns. The columns of Clarke have always been found intact.
[p. 1139]In the recent cases no lesions of the white columns have been observed—a fact upon which reposes the doctrine that such lesions, when existing, are secondary to those of the cornua.
SECOND GROUP OF CASES.—The next group of cases contains 16, where the autopsy was made more than two years after the début of the paralysis.
| Case No. | Name of Author. | Date of Lesion. | Year of Publication. |
|
| 11 | Longet. | 7 | yrs. | 1842 |
| 27 | Echeverria. | 7 | yrs. | 1866 |
| 43 | Money. | 7 | yrs. | 1884 |
| 16 | Lancereaux. | 16 | yrs. | 1873 |
| 38 | Leyden. | 17 | yrs. | 1876 |
| 33 | Schultze. | 19 | yrs. | 1876 |
| 17 | Charcot and Joffroy. | 25 | yrs. | 1870 |
| 20 | Müller. | 30 | yrs. | 1871 |
| 22 | Clarke. | 31 | yrs. | 1868 |
| 10 | Hutin. | 42 | yrs. | 1825 |
| 13 | Cornil. | 47 | yrs. | 1863 |
| 36 | Leyden. | 54 | yrs. | |
| 34 | Leyden. | 58 | yrs. | 1876 |
| 19 | Vulpian. | 64 | yrs. | 1870 |
| 22 | Raymond. | 70 | yrs. | 1875 |
| 16 | Prévost. | 76 | yrs. | 1866 |
The date of these lesions varies from seven to seventy-six years. In two or three cases, where the autopsy was made on very old people, the early history of the disease was unknown, but the probable date of the paralysis was calculated.
In this group of cases patches of atrophy, semi-transparent and grayish in color, focal or diffused, are clearly perceptible to the naked eye. As a rule, the atrophy is unilateral, and sensibly affects the entire half of the cord. In some cases of paraplegia, however, there is a bilateral, symmetrical shrinkage of the entire lumbar cord, which has been reduced to the size of a quill.
The atrophy involves, first and most markedly, one or both anterior cornua; second, the anterior nerve-roots arising from them; third, the antero-lateral columns.
In both the latter localities the microscope will often find individual nerve-tubes wasted and deprived of their myeline. The atrophied patches are generally sclerosed as the seat of a proliferated neuroglia, coloring deeply with carmine. In Laborde's cases, published at the very beginning of what may be called the anatomical period, the atrophy and sclerosis were said to be limited to the antero-lateral columns and the nerve-roots, while the cornua remained intact. In all more recent observations, however, the lesion of the white columns and roots has been found strictly proportioned to that of the gray horns. The sclerosis extended into the latter, constituted by a reticulum of connective-tissue fibres, sometimes fine, sometimes so matted together as to form a dense felt-like substance, sometimes offering the ordinary aspect of sclerosis.
Amyloid corpuscles have been found infiltrated in great numbers [p. 1140] through both the gray and white substance in these old cases (case by Cornil),102 seeming to replace the infiltration with exudation corpuscles observed in the more recent ones.103 When the lesion is distinctly circumscribed the focus is often surrounded by a zone of embryonic cells, seeming to indicate a reactive proliferation on the periphery.104
102 Loc. cit., Soc. Biol.,1863.
103 Seguin (loc. cit.) observes that the opinion is gaining ground which ascribes these to a transformation of the neuroglia corpuscles.
104 Case by Schultze, loc. cit.
As in the relatively fresh cases, the circumstance which has attracted the most attention is the atrophy of the ganglionic cells from the sclerosed patches of the anterior cornua. The completeness with which these have disappeared in any focus seems to be proportioned to the completeness of the paralysis in the corresponding limb. Partial atrophy or disappearance of spinal groups of cells from the cornua may sometimes be correlated with paralysis of special muscles.105
105 Thus in Schultze's case, already quoted, the external group of cells had disappeared from the focus in one gray horn, and the extensors of the foot were alone paralyzed. This seems to confirm the opinion advanced by Spitzka, that this external group of motor-cells corresponds to the extensor, the internal groups to the flexor muscles.
Study of the pathology of infantile paralysis is not completed when the above series of spinal lesions has been enumerated. Most various interpretations have been made of these lesions as they have been successively discovered. Thus, after the theory of congestion came the theory of primary sclerosis, built upon Laborde's two autopsies;106 then the theory of primary atrophy of ganglionic cells;107 then the theory of myelitis;108 finally, a theory of complex and variable lesion.109
106 Laborde, loc. cit.; Cornil, loc. cit.
107 Charcot, Leçons sur les Maladies du Syst. nerveux; Prévost, Soc. Biol., 1864; Joffroy, Arch. de Physiol., 1870; Petitfils, “De l'Atrophie aigue des Cellules matrices,” Thèse de Paris, 1873.
108 Schultze, Virch. Arch., Bd. lxviii.; Roth, Ibid., Bd. lviii.; Henoch, loc. cit., p. 208; Ross, loc. cit., p. 125; Seguin, loc. cit., 1877; Erb, Ziemssen's Handbuch; Seeligmüller, Gerhardt's Handbuch; Roger and Damaschino, Gaz. méd., 1871; Turner, Path. Trans. Lond., 1879; Hammond, loc. cit.
109 Leyden, Archiv für Psych., Bd. vi., 1876.
It was Prévost who first ascribed a predominant importance to the atrophy of the ganglionic cells of the anterior cornua; but it was in the hands of Vulpian, Joffroy, and more especially Charcot and his pupils, that the theory was fully developed. Infantile paralysis was ranked in a newly-formed group of diseases, all characterized by atrophy of these same cells, and differing from each other principally in the acuteness of the process and in its complications.110 Seguin, in his original lecture in 1874, supported the same views, but in 1877 fully adopted that of myelitis. The objections to this theory are: 1st, that by it two diseases so different in their course, localization, electrical reactions, and form of paralysis as atrophic paralysis and progressive muscular atrophy are essentially identified on account of the identity of one lesion, the atrophy of the anterior ganglionic cells;111 2d, the presence of other lesions or of traces of them peremptorily proves the pre-existence of a complex [p. 1141] morbid process which involves the ganglionic cells, but is neither limited to them, nor, necessarily, originates in them.
110 Thus, acute anterior poliomyelitis, subacute anterior poliomyelitis, progressive muscular atrophy, amyotrophic lateral sclerosis, bulbar paralysis.
111 When this objection is accepted, Barlow's remark falls to the ground, that “the similarity of lesion found in two such different diseases as infantile paralysis and progressive muscular atrophy proves the failure of anatomical characters, taken alone, to serve as a basis of nosology” (Brain, April, 1879, p. 74).
This inference was drawn by Roger from the hemorrhagic softening, dilatation, and degeneration of blood-vessels, infiltrations with exudation-corpuscles, and hyperplasia of conjunctive nuclei present in his case. Similarily, Schultze, in a case examined nineteen years after the occurrence of the paralysis, found traces of an extensive myelitis in the diffusion of the lesions,112 in the exquisite cellular infiltration, the proliferation of the neuroglia, and the atrophy of axis-cylinders of nerve-fibres together with the cells; and inferred an anterior myelitis, diffused in the long axis of the cord, but limited to the antero-posterior region. Schultze defines Charcot's theory to be an hypothesis of such an acute atrophy of ganglionic cells as leads to a rapid melting down of these bodies, whereby reactionary inflammation is excited in the surrounding tissue. This implies that the dying cells are able to act like a virulent substance on the imbedding tissue, and of this, declares Schultze, “Charcot has offered no proof.”113
112 In this case of paraplegia without lesion of the upper extremity, to which we have several times alluded, there was bilateral atrophy of the lumbar cord, atrophy of the right anterior nerve in the dorsal and lower cervical region, also in the cervical enlargement.
113 It might be said that the fall of the fever as soon as the paralysis is declared and the motor cells presumably melted down should contradict the idea that their dying substance acts as an irritant upon surrounding tissues.
A third objection has been brought forward by Leyden, and is really an enlargement on the second. It is, that various lesions or morbid processes may underlie the same clinical history. In four autopsies of cases presenting all the clinical history of acute anterior poliomyelitis this author has found three different lesions. In one an extensive lepto-meningitis, together with irregular focal sclerosis of the white columns, evidently depended upon the latter, and in turn caused sclerosis of the anterior cornua with consequent destruction of their cells.114 In two other cases an anterior poliomyelitis was accompanied by diffused lesions of the central canal. Finally, in a fourth case the lesions were limited to the anterior cornua, as is most usual.
114 This case of Leyden's throws light on the two autopsies by Laborde with sclerosis of the white columns and intact cornua. It seems probable that a process originating in the cornua had then been arrested or had receded, while continuing its evolution in the white columns.
The theory of acute atrophy of ganglionic cells is not sensibly different from that of a parenchymatous myelitis.115 But all the objections which can be urged against the former theory apply to the latter also, with the exception that the hypothesis of inflammation suggests a cause for the otherwise inexplicable atrophy. Observation of the pathological appearances alone could not decide whether the irritation started in the parenchymatous or interstitial tissues. Reference to the etiology of the disease shows that of the two most frequent apparent causes, [p. 1142] blood-poisoning and traumatisms, the first would indicate that the inflammation started in the connective tissue supporting the blood-vessels; the second suggests that the irritation began in the spinal elements constituting the origin of the nerves.
115 Hammond assumes such a form of myelitis in his classification of inflammations limited to the anterior part of the gray matter of the spinal cord:
1. Inflammation of motor and trophic nerve-cells: (a) Infantile spinal paralysis; (b) Spinal paralysis of adults; (c) Pseudo-hypertrophic spinal paralysis.
2. Inflammation of motor cells: (a) Glosso-labia-laryngeal paralysis.
3. Inflammation of trophic cells: (a) Progressive muscular atrophy; (b) Progressive facial atrophy (Dis. Nerv. Syst., 6th ed., p. 464).
We think this classification open to several fundamental criticisms.
Whatever be the starting-point, however, it is very evident that the morbid process soon involves all the tissues contained in the gray matter of the anterior horns, and constitutes, therefore, a real anterior poliomyelitis.
A question of much interest is the relation to this of the lesions of the anterior roots and of the white columns. Is the atrophy of nerve-tubes a passive consequence of their separation from the ganglionic cells, the sclerosis a secondary consequence of this? or is the sclerosis the cause of the atrophy, itself the result of an irritation propagated downward from the myelitic focus, according to the usual law for secondary degenerations in motor tracts? or, finally, is it a residuum of a leucomyelitis (or of the white substance), complicating by simple extension the inflammation of the gray substance?
Review of the autopsies recorded would indicate that the lesions in question are brought about sometimes in one, sometimes in another, of these ways—sometimes even, as in Leyden's case, by extension from a meningitis. That sclerosis of the white columns is most frequently a secondary degeneration is indicated by the frequency with which it appears below the lesion of the cornua, by the rarity with which it is found above, and also by the general proportion between its intensity and that of the disease of the gray matter.
We have devoted so much space to consideration of spinal-cord lesions, because they are by far the most constant and the most important; after these rank the structural alterations of the muscles, which received for a while such a preponderance of attention.
Hammond has studied the progress of these changes on the living subject by fragments of fibre successively removed with Duchenne's harpoon. In an incipient stage of degeneration the fibrillæ are found to be irregular and torn,116 the transverse striæ dim; oil-globules are seen arranged according to the long axis of the fibre. In a more advanced stage the transverse striæ nearly disappear, the oil-globules are in large numbers, and fat-corpuscles are also abundant. Finally, the whole specimen is seen as a mass of air-globules. Six weeks later, however, these had in turn disappeared, and there remained a mass of connective tissue.
116 Though, from the method of removal, this appearance cannot be considered as certainly pathological.
This series of changes, however, does not always take place, as Hammond himself recognizes. Laborde117 first described a granular form of muscle atrophy, where the muscular substance gradually wastes away without ever becoming fatty, and leaving a transparent and hyaline sheath. The two forms of fatty and of simple atrophy can be distinguished by the naked eye. In the latter the muscle begins by being thinner or lighter and softer than usual, ultimately turning light brown. The fatty muscle becomes a homogeneous yellowish-white, diversified by occasional remnants of reddish fibres.
117 Loc. cit., p. 131.[p. 1143]
Proliferation of the interstitial connective tissue may be combined with either simple or fatty atrophy. A combination of abundant sclerosis and abundant fatty infiltration may lead to a pseudo-hypertrophy of the muscles.
“There cannot be the slightest doubt,” observes Erb, “that the lesions described constitute a degenerative atrophy similar to what may be caused by section or sense traumatism of a peripheric nerve.”
The peripheric nerves have been much less thoroughly studied than the spinal cord. Leyden first directed special attention to the nerves. He found the sciatic altered in two cases,118 in the first by an interstitial neuritis; in the second by partial atrophy. In 1880 the same writer, in an extensive article on poliomyelitis and neuritis,119 greatly extends his views as earlier expressed. Not only does he claim the coexistence of neuritis with spinal-cord disease in atrophic paralysis, but thinks that many cases of this, and also of other forms of paralysis, “lately supposed to originate in the spinal cord, may really begin in any part of the motor apparatus,” thence sometimes generalize throughout the whole apparatus, sometimes remain limited to the original portion affected. Thus, progressive muscular atrophy may sometimes begin in the nerves, sometimes in the muscles, and sometimes in the ganglionic cells of the cord; and this variety of origin explains the discrepancies of opinion which have been held upon the nature of this disease. Similarly, all forms of acute or chronic atrophic paralysis in either children or adults may begin in either the nerves or cord, thence become generalized to both, or remain limited to one part of the spinal motor system. Cases of atrophic paralysis which recover are probably not cases of poliomyelitis at all, but of multiple neuritis, rheumatic, traumatic, or infectious in nature. The regeneration of peripheric nerves is a well-demonstrated possibility, but not that of the cells of the cord. Lead-paralysis is usually confined to the nerves, but sometimes extends to the cord. In diphtheritic paralysis Buhl has found injection, thickening, and granular infiltration of nerves at the union of their anterior and posterior roots;120 and as long ago as 1876, Dejerine, in a case of atrophic paralysis in a syphilitic woman, found varicose swelling of the medullary sheath in the nerves of the paralyzed lower extremities, together with heaping up of the myeline into large drops, colored black in glycerin and osmic-acid preparations. Coincidently, in the cord, at the origin of the same nerves, the number of motor-cells was diminished, and of those that remained the prolongations, and even the body, of the cell were atrophied.121
118 Cases 34 and 35 of Table V., quoted from Arch. de Psychiatrie, Bd. vi., 1876.
119 Zeitschrift für Klin. Med., 1880.
120 Zeitschrift für Biol., 1867.
121 Arch. de Phys., 1876.
These views of Leyden's are extremely interesting, and should stimulate future research into the condition of nerves in all cases of atrophic paralysis. It is quite incorrect to say, as Archambault and Damaschino have recently done,122 that Leyden denies the existence of anterior poliomyelitis in such cases, especially in such as prove permanent. He only insists on the frequent coincidence of neuritis, on a varying point of departure for the morbid process, and on the probability that in cases of recovery this process has always remained peripheric.
122 Le Union méd., 1883, 7, 35, case quoted in Table V. It is much to be regretted that Damaschino, who strongly controverts Leyden's views, did not examine the nerves in his own most interesting case.[p. 1144]
The strongest objection to Leyden's theory is the absence in most recorded cases, either infantile or adult, of the usual signs of nerve inflammation, local pain, or tenderness. Autopsies of old cases are not able to differentiate an inflammation from an atrophic process in the nerves, followed by a secondary thickening of the endoneurium. This thickening was found in three cases examined by Edmonds in 1882, whose subjects had suffered from infantile paralysis in early life, and had had the paralyzed limb amputated at the age of fifteen or sixteen. Transverse sections were made from the internal popliteal nerves. The specimens showed some healthy nerve-fibres, presumed to be sensory; others much smaller, with the axis-cylinders wasted or degenerated; while strands of connective tissue traversed the nerve-bundles, resulting from hypertrophy of the endoneurium. The vessels showed inflammation of their coats, with proliferation of the endothelium.123
123 Trans. Path. Soc. London, 1883.
The brain is usually normal, unless indeed the paralysis has affected children previously rendered idiotic by congenital atrophia cerebri. Sandie, however, examined one brain with an interesting positive result.124 The brain was taken from a boy of fifteen paralyzed since the age of three in almost all his muscles, with even paresis of the muscles of the trunk and neck. The paralysis was more marked upon the right than on the left side. At the autopsy, in addition to atrophy of the muscles and of the motor nerves, with exquisite atrophy of the anterior columns and anterior cornua, was found a decided atrophy of the left central convolution, and, less marked, of the paracentral lobule. This was shown by comparative measurements with the opposite side of the same brain, and also with the corresponding convolution and lobule in two other brains. The child's intelligence had not been affected.
124 Centralblatt f. d. Med. Wissensch., No. 15, 1875.
The arrest of development of the bones has been already mentioned, as well as that of their epiphyses and apophyses. The compact osseous tissue is atrophied: the medullary, on the contrary, abundantly developed and rich in fat.
PATHOGENY OF INFANTILE PARALYSIS.—In the pathological anatomy of infantile paralysis there are two principal facts to be correlated with its clinical phenomena—namely, the limitation of the myelitis to the anterior gray horns of the spinal cord; the destruction of the ganglionic nerve-cells in these gray horns. That the other lesions observed are subordinate to these is shown by their variableness as compared with the constancy of the anterior poliomyelitis. These lesions are, in the cord, the atrophy and sclerosis of the anterior nerve-roots and white columns; in the muscle, the fatty degeneration or simple atrophy of the fibre; in the nerve, breaking down, and finally atrophy of the myeline sheath, sometimes of the axis-cylinder; proliferation of the endoneurium.
Consequence of Limitation of Myelitis.—Limitation of the morbid process to a portion of the motor tract, the anterior cornua, and exclusion of the posterior horns and roots, readily explain the predominant positive symptom of motor paralysis, together with the absence of sensory disturbance. The absence of muscular rigidity, spasm, active contraction, and of exaggerated reflexes is similarly explained by the immunity from the morbid process of the posterior white columns and the portion of the [p. 1145] lateral columns immediately adjacent to them. The motor paralysis resulting from destruction of the anterior ganglionic cells of the cord is much more complete than that which depends on simple interruption of the motor tracts passing from the brain. The manner in which the motor tracts are connected by a succession of arching fibres with these cells already indicates that the latter are dépôts for the reinforcement of the motor impulses. We must believe, indeed, that the centrifugal impulses reaching the anterior cornua are not yet motor in character, but to become so must sustain a new elaboration in the ganglionic cells of this region. Evidently, the network of gray fibres connecting the arcuate strands of the antero-lateral columns with the cells become, in virtue of that fact alone, essential to the process. But it is also probable that the multiplied transmission of impressions, which lies perhaps at the basis of the process of their higher elaboration in ganglionic centres, is carried on in the larger network of gray fibres as well as in the smaller network contained in the ganglionic cells. Destruction of a portion of this network would therefore interfere with the elaboration of the motor impulse, in the same manner, though to a relatively less extent, as destruction of the ganglionic cells themselves.
Trophic Lesions.—The rapid wasting of the paralyzed muscles, with their degenerative electrical reactions, seems, however, to be an effect altogether peculiar to lesions of the ganglionic bodies.125 According to Charcot, who has so especially formulated the laws of amyotrophic paralysis, all the ganglionic cells essential to the elaboration of motor impulses exercise a trophic influence upon muscles. The spinal cell, nerve-fibre, and muscle-fibre combine into a complex indissoluble unity or element. One part of this lesion of complex elements is necessarily followed by proportionate lesion of all its other parts.
125 The amyotrophic lateral sclerosis of Charcot exhibits in an exquisite manner the difference between paralysis without atrophy, caused by sclerosis of the antero-lateral columns, and paralysis with atrophy when the morbid process has extended to the anterior cornua.
According to Erb, however, who extends Samuel's doctrine of special trophic nerves, it is not the motor cells which influence the nutrition of the muscle-fibres with which they are connected, but special trophic cells lying among the others in the anterior cornua. This theory is principally based on the existence of muscular atrophies of central origin (progressive muscular atrophy, bulbar paralysis), unaccompanied for a long time by paralysis.126 Hammond cites as a converse example the anterior poliomyelitis “where the peripheric disturbance is, in the first place, solely one of motility; this is paralysis without atrophy. After a time, which may be as much as six months or even more, the trophic changes begin.”127
126 Ziemssen's Handbuch.
127 Loc. cit., p. 429.
But surely this is an exaggerated emphasis on the exception, rather than the true inference from the rule of rapid wasting in anterior poliomyelitis—a rule so general as to have originated the title atrophic paralysis. Erb gives an ingenious scheme (Fig. 55) of the mental relations of motor and trophic cells with cerebral and spinal nerve-fibres. It will be seen that isolated lesions of one or the other trophic apparatus might occur without paralysis of motor tracts, while simultaneous lesion of the trophic [p. 1146] apparatus and of the ganglion-cells, or of the latter, involving the tracts coming from the trophic cells, would cause, as in anterior poliomyelitis, motor paralysis, muscular atrophy, loss of the reflexes, degenerative reaction in nerves and muscles.
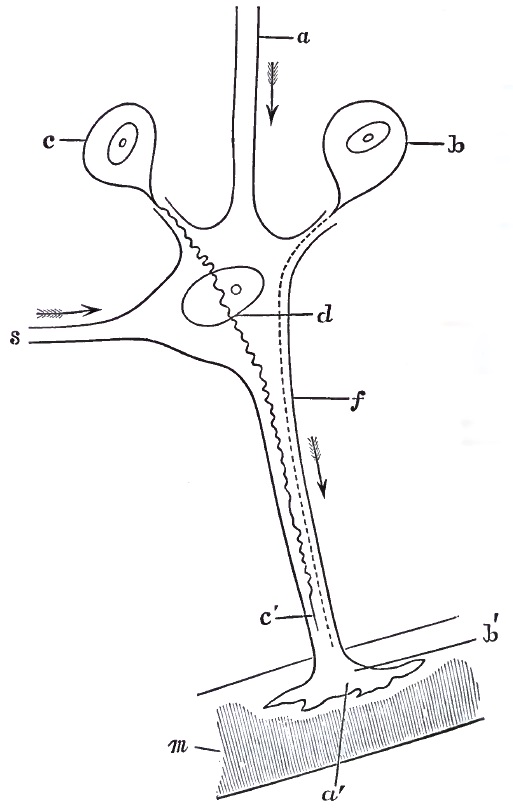
Duchenne and Joffroy128 also argue the existence of special trophic nerve-cells. The absence129 of the nutritive lesions of the skin and cellular tissue which are so conspicuous when the gray matter around the [p. 1147] central canal or posterior to it is involved,130 the dependence of the nutrition of the motor apparatus, nerves, muscles, bones on the integrity of the anterior horns, are facts which, taken together, seem to indicate that the maintenance of nutrition depends on the unbroken continuity of the motor or sensory apparatus from the periphery to the ultimate central element, rather than on any special central cells endowed with trophic functions.131 Erb's hypothesis, as his own scheme moreover denotes, demands not only trophic cells distinct from motor cells, but separate trophic cells for the muscles, for the motor, and for the sensory nerves.
128 “De l'Atrophie aigue et chronique des Cellules nerveuses,” Arch. de Phys., No. 4, 1870.
129 Money, and also Gowers, have signalized a condition of the skin resembling myxœdema (Tr. Path. Soc. London, 1884, and Brit. Med. Journ., 1879).
130 Mayer (Herman's Handbuch Physiol.) sums up the great mass of evidence now accumulated, which demonstrates the trophic influence of the central gray mass of the cord upon the tissue.
131 Nepveu (La France médicale, 1879) mentions some cases of infantile paralysis complicated with trophic lesions of the skin. The facts, if accepted, could only indicate an extension of the myelitis to the central and posterior regions of the gray columns. The relations between non-atrophic paralysis caused by interruptions of the motor tracts and muscular atrophy dependent on lesion of the anterior cornua are exquisitely shown in a case reported by Sander. An adult suffered from chronic motor paralysis, gradually increasing, in the right arm, with paresis of the lower extremities. In the hand, arm, and shoulder the paralysis was followed by gradual atrophy and diminution of the faradic contractility; in the lower extremities no atrophy occurred. At the autopsy was found a gliomatous tumor seated in the anterior cornua predominating on the right side, extending from the level of the sixth dorsal to that of the eighth cervical vertebra. The ganglion-cells were pigmented and compressed, not altogether destroyed. The lumbar cord was intact, and the non-atrophic paresis of the lower extremities evidently resulted from the interruption of the motor tract above.
The peculiar grouping of nerve-centres within the cord that seems to be indicated by some of the groupings of infantile paralysis shows, as has been said, a probable divergence within the cord of nerve-fibres which run together in the same nerve-stem. The associations to be expected from the data of functional association and of clinical history are by no means fully decided. It is even a matter of dispute whether the tibialis anticus is functionally more associated with the flexors or with the extensors of the thigh, and whether its experimental irritation or clinical paralysis really coincides with that of the first or of the second group. This entire field of observation is new and promises fertile results.132
132 It is from this field that has come a new argument for the spinal nature of lead-paralysis, from its peculiar grouping, and from analogy with that of anterior poliomyelitis of the upper extremities (Remak, “Ueber die Local. Atropa. Spinal Lahm.,” Archiv für Psych., Bd. ix.; also, Ferrier, loc. cit.).
Relation between Limitation of Myelitis and Age.—From the relative frequency of anterior poliomyelitis in childhood, as compared with its much greater rarity in adult life, we must infer the existence of some special conditions in childhood which tend to limit the morbid process to such a portion of the cord. The theory of a primitive spontaneous atrophy of the motor cells would serve, indeed, to explain this limitation. The reasons already alleged for regarding the morbid process as a systematic myelitis decisively hinder the acceptance of such an explanation as it stands. On the assumption, however, that the myelitis is usually of functional origin, and starts, therefore, in the elements of the anterior cornua essentially involved in the motor functions, the morbid susceptibility of these elements may be ranked with the liability to disease of the entire locomotor system which is known to be so predominant in children. From pathological evidence, even without anatomical proof, we may reasonably infer an incompleteness of development in the anterior [p. 1148] cornua of the cord correlative with that well demonstrated in the bones and functionally inexperienced muscles. If the antero-posterior fibres which connect the anterior cornua with the central and posterior gray masses be also incomplete, the radiation of irritations, and consequent vascular irritation, would also be arrested within the boundaries of the original lesion. Thus a peculiarly circumscribed, instead of the common diffused, myelitis of adults.
Money133 points out that for the gray matter of the cord, as of the brain, the centre or maximum force of the circulation is on the periphery, and the nutritive supply of the centre is thus easily cut off. Moreover, while the blood-vessels of the cervical and dorsal regions of the cord pass to it transversely, the vessels of the lumbar region are compelled to describe a somewhat prolonged vertical course before reaching their point of distribution. From these circumstances, even transitory congestions in the circulation of the cord are easily followed by irreparable injury of its delicate elements.
133 Loc. cit., Path. Trans., 1884.
Finally, in all discussions on pathogeny must not be forgotten the doctrine of Leyden134 that infantile paralysis, also progressive muscular atrophy, is a disease which may begin at the periphery and extend to the centres, as well as the reverse. It must also be remembered that, as yet, only very scanty evidence exists to support this, in itself, plausible theory.
134 See loc. cit., ut supra.
COURSE OF INFANTILE PARALYSIS.—The most ordinary course of infantile paralysis is that already described as typical—namely, extremely rapid development to a maximum degree of intensity, then apparent convalescence, retrocession of paralysis, atrophy, and ultimate deformities in limbs in which paralysis persists.
Several variations from this typical course are observed. Complete recovery may take place, as in the so-called temporary paralysis of Kennedy135 and of Frey.136 These cases are very rare. But their possibility seriously complicates the estimate we may make of the efficacy of therapeutic measures.137
135 Dublin Quarterly Journal, 1840.
136 Berlin. Klin. Wochensch., 1874. I have described one such temporary case in the article already quoted. These cases seem about as frequent in adults. (See Frey, loc. cit.; also case of Miles, etc. etc.)
137 As of the case of complete recovery, the only one the author had seen, related by Dally, Journal de Thérap., 1880, 1, vii.
On the other hand, there may be a complete absence of regression; and this is observed sometimes in cases where the paralysis is originally limited; sometimes where it is extremely extensive, involving nearly all the muscles of the trunk or limbs;138 or muscles or limbs originally spared may become involved in a fresh attack. Laborde relates cases of this kind. In Roger's first case paraplegia occurred under the influence of scarlatina two months after paralysis of one arm.
138 Thus in Eulenburg's case, quoted ut supra.
The form of anterior poliomyelitis most frequent in adults is the subacute, and after that the chronic. Both are extremely rare in children, the latter excessively so. Seeligmüller and Seguin139 both admit the possibility of a chronic form in children, and the latter has kindly communicated to me one case from his private practice:
[p. 1149]Miss N. D——, æt. 15, paresis in both legs, first at age of nine, increased at age of twelve, when weakness of vision first noted. At fourteen both feet in rigid pes equinus, and both tendons achilleis cut, without benefit. Hands became tremulous, without paresis. On examination at age of fifteen found moderate atrophy of muscles of both legs. Tendo Achillis united on both sides, and equinus persists. Voluntary movement exists, both in anterior tibial and in gastrocnemius muscles, but diminished in anterior tibial. Faradic contractility diminished in both sets of muscles; examination difficult from extreme sensibility of patient. In both hands interossei, muscles of thumb, and little finger show tremors and fibrillary contractions. Thenar eminences small, abductor pollicis nearly absent, not reacting to faradic current. Optic nerves slightly atrophied. Mind enfeebled, memory poor; articulation not affected. Five years later the motor paralysis and mental enfeeblement had still further progressed, but no exact notes exist of this period.
139 Loc. cit. (ed. 1877).
Erb140 relates a case that he considers unique at the time in a girl of six. The paralysis began insidiously in the right foot in July; a fortnight later had extended to the left foot; complete motor paralysis existed in August, without any lesion of sensibility: after electrical treatment, then instituted, first return to motility to peroneal muscles in November; by January child able to walk again and electrical reactions nearly normal.141
140 Brain, 1883.
141 In the same number of Brain, A. Hughes Bennett quotes cases of so-called chronic paralysis in very young children which are evidently cases of general paresis from congenital cerebral atrophy. The children were defective in intelligence, could not sit up nor hold up the head; the electrical reactions were preserved. I have seen a great many such cases: they are indeed not at all uncommon. Much more so is Bennett's diagnosis.
COMPLICATION WITH PROGRESSIVE MUSCULAR ATROPHY.—Raymond142 and Seeligmüller describe some rare cases where progressive muscular atrophy declared itself in persons previously affected with infantile paralysis in other limbs. Both observers infer a gradual and chronic extension along the cord of the originally acute anterior poliomyelitis.143 Similar cases have much more recently (1884) been quoted by Ballet as tending to modify the prognosis which has usually been pronounced favorable quoad life and further spinal accidents. (See infra.)
142 Gaz. méd., 1875. No. 17.
143 It seems to me that Seguin's case, above quoted, might be an example of such complication(?). But I have not seen the patient myself, and describe the case according to the views of the author.
PROGNOSIS.—The prognosis of atrophic paralysis, quoad vitam, is, as is well known, extremely good. The prospect of recovery from the paralysis is variable. It cannot be estimated either by the extent of the initial paralysis or by the severity of the fever or attendant nervous symptoms. The electrical reactions alone are of value in the prognosis, and their value is very great. Duchenne first formulated their law: “All the cases of infantile paralysis which I have seen where the faradic contractility was diminished but not lost, and which could be treated by faradic electricity within two years after the onset of the paralysis, have completely recovered.”144 This encouraging statement must be read as applying rather to individual muscles than to cases as a whole. Few [p. 1150] complete recoveries of patients are claimed even by so enthusiastic an electrician as Duchenne; who nevertheless affirms his not unfrequent success in re-creating entire muscles out of a few fibres saved from degeneration.
144 Loc. cit.
The persistence of galvanic irritability in muscles which fail to contract to the faradic current has been shown by Erb to belong to the degenerative reactions. Hammond, however, without alluding to the qualitative changes in the galvanic contractions, sees in them the elements of a relatively favorable prognosis, even when faradic contractility is lost. Thus, out of 87 cases, in 39 of which the paralyzed muscles contracted to the galvanic but not the faradic current, 14 were entirely cured, 28 greatly improved, 30 slightly improved, 15 discontinued treatment very early.145
145 Loc. cit., p. 482.
Examination of fragments of living muscle obtained by Duchenne's harpoon, though useful, should not be allowed to exaggerate an unfavorable prognosis. Much fat may be found in such fragments when the muscle is as yet by no means completely degenerated and can be made to contract to one or the other current. Erb, however, admits that the results of treatment have not, in his hands, been brilliant; but adds that he has had no opportunity to treat any cases which were not of long standing.146
146 Loc. cit.
Volkmann147 considers the paralysis entirely hopeless, and advises the concentration of all effort upon the prevention or palliation of deformities.
147 Loc. cit.
It seems probable that at the present moment sufficient data do not exist for formulating a fair prognosis; nor will they until a much larger number of cases than hitherto have been submitted to all the resources of a complex and persevering system of therapeutics from the earliest period of the disease.
SPECIAL PARALYSES.—Among the paralyses, some exercise a more unfavorable influence on locomotion than others. Thus, paralysis of the muscles of the trunk is more difficult to palliate, either by apparatus or by the efforts of the patient, than any paralysis of the limbs. Similarly, paralysis of the upper segments of a limb is more crippling than when confined to the lower. Partial paralysis of the muscles surrounding a joint is often (but not always) more liable to lead to deformity than total paralysis.
Influence of Neglect.—Apart from the influence of treatment in curing the paralysis, must be estimated in the prognosis the effect of care and watchfulness in limiting the disease and in averting many consequences, even of those which are incurable. The rescue of muscles only partially degenerated may often serve to compensate the inaction of those which are irretrievably ruined.
Ballet148 has recently called attention to the fact that in certain cases persons who had been attacked with an anterior poliomyelitis in childhood became predisposed to different forms of spinal disease. Four have been observed: (1) transitory congestion of the cord, causing paralysis of a day or two's duration; (2) an acute spinal paralysis of the form usually seen in adults; (3) subacute spinal paralysis; (4) progressive muscular atrophy. The author relates cases under each of these heads, and further quotes one [p. 1151] related by Dejerine in 1882.149 The patient, a carpenter aged fifty-five and with an atrophic deformity of the foot, became suddenly paralyzed in the four limbs, trunk, and abdomen. The paralysis was complete in a month, was stationary for three months, then began to improve, and at the end of six months from the onset of the disease recovery was complete.
148 Revue de Médecine, 1884.
149 Revue de Médecine, 1882.
The observations of progressive muscular atrophy in persons bearing the stigmata of an infantile paralysis are quite numerous.150
150 Charcot, Soc. Biol., 1875, and Gaz. méd.; Seeligmüller (4 cases), in Gerhardt's Handbuch, 1880; Hayem, Bull. Soc. de Biol., 1879; Vulpian, Clinique méd. de la Charité, 1879; Pitres, new observation, quoted by Ballet in 1884.
The prognosis cannot be the same for cases where everything is done to avert malpositions and for those where all precautions are neglected. Thus, prolonged rest in bed favors pes equinus; the use of crutches necessitates flexion of the thigh and forced extension of the foot; locomotion without support tends to displace articulations by superincumbent weight, causing pes calcaneus, genu-recurvatum. Finally, compensatory deformities must be averted from sound parts, as scoliosis from shortening of the atrophied leg, equinus from passive shortening of the gastrocnemii through flexion of the leg, etc.
ETIOLOGY.—Concerning the etiology proper of infantile paralysis little definite is known. It is probable, as has been already noticed, that traumatisms have a much more decided influence than is generally assigned to them. Leyden particularly insists on this influence, and on the facility with which a traumatism relatively severe for a young child may be overlooked, because it would not be recognized as such for an adult. It must be noticed, however, that children are much more liable to have the arms wrenched and pulled violently than the lower extremities; yet in a great majority of cases the lesion is situated in the lumbar cord.
It has been shown that the myelitis, though so limited transversely, is often far more diffused in the longitudinal axis of the cord than might be supposed from the permanent paralyses. This fact corresponds to the initial generalization of the motor disturbance. It seems possible that the traumatic irritation, starting from the central extremity of the insulted nerve, diffuses itself through the cord until it meets with its point of least resistance, and here excites a focal myelitis. That this point should most frequently be found in the lumbar cord would be explained by its relatively less elaborate development, corresponding to the imperfect growth and function of the lower extremities.
A second cause of anterior poliomyelitis is, almost certainly, the presence of some poison circulating in the blood. The frequent occurrence of the accident in the course of one of the exanthemata is one indication of this; other indications are found in such cases as that related by Simon, where three children in one family were suddenly attacked—two on one day, one, twenty-four hours later.151 The same author relates a case of motor paralysis in an adult, followed by atrophy of left lower extremity, and which occurred during a fit of indigestion caused by eating mussels.152 The acute ascending paralysis of Landry, [p. 1152] with its absence of visible lesion, has been said to strikingly resemble the effects of poison. Hydrophobia and tetanus are again examples of the predilection exhibited by certain poisons for the motor regions of the cord.
151 Journal de Thérap., 7, vii., 1880, p. 16. These children belonged to an American family, but were seen by several distinguished French physicians.
152 P. 357.
The evidence that infectious diseases may constitute the immediate (apparent) causal antecedent of acute poliomyelitis has led, not unnaturally, to the theory that all cases of acute infantile paralysis are due to a specific infecting agent, some as yet unknown member of the great class of pathogenic bacteria. It may be noticed, however, that the occurrence of the spinal accidents after the ordinary infectious diseases, as scarlatina and measles, should as well indicate that a specific agent proper to itself was at least not essential to its development.153
153 Perhaps the occurrence of diphtheria in the course of scarlatina and typhoid should indicate a similar lack of real specificity in the morbid agent of the former disease.
The influence of exposure to cold, which seems to have been sometimes demonstrated, must probably be interpreted, as in the case of rheumatism and pneumonia, as effective by means of some poison generated in the organism when cutaneous secretion, exhalation, or circulation has been suddenly checked.
DIAGNOSIS.—The diagnosis of the acute anterior poliomyelitis of childhood is usually easy, but unexpected difficulties occasionally arise.
Typical cases are markedly different from typical cases of cerebral paralysis, but in exceptional cases these differences disappear. This is shown in the following table:
| SPINAL PARALYSIS. | CEREBRAL PARALYSIS. |
| Paraplegic or monoplegic (rule). | Hemiplegic, (rule). Monoplegic as residuum of hemiplegia or as consequence of solitary tubercle (exception). |
| Hemiplegic as residuum from paraplegia, or original and involving facial nerve (very exceptional). | |
| Intelligence free (rule). | Intelligence depressed (rule). |
| Intelligence depressed (when spinal paralysis has affected imbecile children). | Intelligence free (exception, especially with solitary tubercle). |
| Disposition lively. | Disposition apathetic or cross. |
| Initial convulsion unique; general symptoms of a few hours' duration (rule). | Convulsions repeated; pyrexia prolonged several days or weeks (rule). |
| Convulsion repeated during two to three weeks before paralysis; fever a month (rare exceptions). | |
| Sensibility intact (rule). | Sensibility intact after initial period. |
| Occasional hyperæsthesia (exception). | |
| Reflexes cutaneous, and tenderness lowered or lost (rule). | Reflexes intact. |
| Reflexes preserved when only single muscles in groups paralyzed. | |
| Associated movements of hand absent (Seeligmüller). | Associated movements frequently observed in hand. |
| No rigid contractions of upper extremity. | Extensive and rigid contractions of upper extremity very frequent. |
| Atrophy of paralyzed muscles and arrested development of limb, very marked. | Atrophy very slight. |
| Faradic contractility diminished or lost; degenerative galvanic reaction. | Electrical reactions normal. |
Rather singularly, the diagnosis from transverse myelitis is less liable to error than that from cerebral paralysis:
[p. 1153]| ANTERIOR POLIOMYELITIS. | TRANSVERSE MYELITIS. |
| Fever brief or absent. | Persistent fever. |
| Sensibility intact. | Hyperæsthesia, then anæsthesia. |
| Decubitus absent. | Presence decubitus. |
| Reflexes lost. | Reflexes increased. |
| Atrophy of muscles. | Atrophy of muscles sometimes as intense. |
| Electrical muscular contractility lost. | Loss of electrical contractility, but not proportioned to sensory and motor disturbance; less rapidly completed. |
The diagnosis from hæmatomyelitis is almost impossible, and practically useless. For if the hemorrhage be severe, the child dies at once, as in Clifford Albutt's case. If less severe, it excites a myelitis, and the history becomes identical with that of the disease we are considering; or if the clot beyond the anterior cornua, it is identified with a vulgar myelitis of traumatic origin.
Progressive muscular atrophy is extremely rare in childhood, but is occasionally seen under hereditary influence (Friedreich's disease). In adult cases confusion is not only easy to make, but often difficult to avoid, especially with the rare, chronic form of poliomyelitis. The basis of distinction is as follows:
| ANTERIOR POLIOMYELITIS. | PROGRESSIVE MUSCULAR ATROPHY. |
| Onset sudden; maximum of paralysis at the beginning. | March very gradual; maximum of disease not attained for years. |
| Faradic contractility lost almost at once. | Faradic contractility not lost until atrophy complete. |
| Shortening of limbs and atrophy of limbs (in infantile cases). | No arrest of development of limbs. |
| Functionally associated muscles frequently associated in paralysis: hand rarely affected. | Capricious selection of muscles, but frequent wasting of these at eminences. |
Paralysis from lesion of a peripheric nerve closely imitates anterior spinal paralysis.154 It is distinguished by closely following the distribution of the injured nerve, and, usually, by concomitant lesions of the sensibility and of cutaneous nutrition.
154 The importance of this fact has been shown in the section on Pathogeny. (See also quotations from Leyden and remarks on lesions of peripheric nerves.)
The pseudo-paralysis sometimes observed in syphilitic children as a consequence of a gummatous infiltration of the bones at the junction of the epiphysis and diaphysis155 might easily be mistaken for a spinal paralysis. But it is an affection peculiar to the new-born; the electrical reactions of the paralyzed muscles are intact; careful examination will show that the movements of the muscles are not impossible, but restrained by pain; often other syphilitic affections are present.
155 Parrot, Wagner.
The diagnosis from diphtheritic paralysis is embarrassed, from the fact that true anterior poliomyelitis may develop in the course of diphtheria as of other infectious diseases. The paralysis of the soft palate, preservation of faradic reaction, absence of atrophy, and the usually rapid recovery must establish the differentiation.
In spinal paralysis there is loss of the reflexes,156 and also of faradic [p. 1154] contractility, both of which are preserved in hysteria. In hysterical paralysis, also, there is no wasting of the affected muscles.
156 See Gowers's monograph on “Spinal-Cord Diseases” for an excellent summary of the spinal reflexes.
Various diseases of the bony skeleton or articulations may simulate spinal paralysis. Congenital club-foot, caused by unequal development of the bones and cuticular surfaces, is to be distinguished from the paralytic variety by the date of its appearance,157 by the deformity of the tarsal bones, and by the extreme difficulty of reduction.
157 Though in some cases paralysis of the muscles of the foot seems to take place during fœtal life, and a club-foot result which is both congenital and paralytic.
Caries of the calcaneum, leading the child to walk on the anterior part of the foot to avoid pressure on the heel, may leave after recovery such a retraction of the plantar fascia as to cause a degree of equinus and varus, with apparent paralysis of the peroneal muscles. I have seen one such case.
Congenital luxation of the hip may simulate paralysis; indeed, by Verneuil, it has been attributed to an intra-uterine spinal paralysis. There is, however, no change in the electrical reactions of the muscles surrounding the joint.
In coxitis, however, Newton Shaffer158 has demonstrated a moderate diminution of faradic contractility in such muscles, and a corresponding degree of atrophy; and this fact might complicate the diagnosis of paralysis from arthritis of the hip-joint. Gibney159 has called attention to the facility with which this confusion may arise, and Sayre160 relates cases of infantile paralysis mistaken for coxitis.
158 Archives of Medicine.
159 Am. Journ. Med. Sci., Oct., 1878.
160 Orthopædic Surgery.
In a case observed by myself, which had been previously diagnosed as coxitis, the mistake was all the more interesting as the paralysis which really existed seemed to have been caused by a meningitis rather than primary myelitis of the cornua.161 It thus corresponded to the meningo-myelitic case related by Leyden.
161 The details of this case are as follows: C. P——, aged 11, ten months previous to consultation suffered from febrile attack, accompanied by retraction of head, severe pains diffused through body and intense at nape of neck; unconsciousness for thirty-six hours; vomiting; no convulsions. Case diagnosed as cerebro-spinal meningitis by attendant physician. Convalescence in a week, but with pain in lumbar region of back, predominating on right side, so aggravated by standing or walking that both acts impossible. Coincidently, pain in right calf; exquisite tenderness to pressure even from stocking. No complaint in recumbent position. Child could not get from floor to bed, nor raise right leg from ground. As pain subsided walking became possible, but right leg dragged. Chronic twitchings on left side, face, arm, leg. These symptoms lasted ten or twelve weeks, but at end of nine weeks patient could walk up stairs. In ten months power of walking almost recovered, but there remained a certain amount of lordosis and oscillation of pelvis, which is jarred on the left side while the right leg is swung forward. Recumbent, all movements executed equally well on both sides and passive motion of the hip-joint perfectly free. Circumference of right thigh and leg diminished from one-half to one inch as compared with the left. Faradic contractility diminished on the right side in the gluteal muscles, vastus externus, and rectus, and in the gastrocnemii. The sacro-lumbalis muscle was, unfortunately, not examined, but from the lordosis was probably affected. The remaining muscles were intact. Pain on pressure persisted over right side of second, third, and fourth lumbar vertebræ. Diagnosis was made of a limited meningeal exudation, with compression of anterior part of cord or of a portion of the lumbar and of the sacral plexus.
Scoliosis, which may be caused by the relatively rare unilateral paralysis of some of the muscles of the trunk, may also be simulated by paralysis with shortening of one lower extremity. To compensate the [p. 1155] shortening, the trunk is bent over on the paralyzed side; hence a lateral curvature, easily reducible, but easily leading into error.
It would seem easy to distinguish traumatic cases of subluxation of the humerus from those due to paralysis of the deltoid. Yet sometimes only the history will serve to establish, and that somewhat doubtfully, the diagnosis.162
162 A child of four was brought to me with a stiffness and rigidity of the shoulder-joint which could only very partially be overcome by passive motion, and not at all by voluntary effort. The mother stated that several months previously the child had, without apparent cause, become suddenly unable to move the arm. After two months' delay it was taken to a dispensary, and told that the arm was out of joint, and had it reset under ether. From this date the stiffness had gradually developed. The deltoid was atrophied, with marked diminution of the faradic contractility. Question: Were these signs merely symptomatic of an arthritis consequent on a dislocation, or was the latter the result of a spinal paralysis of the deltoid?
THERAPEUTICS.—The treatment of anterior poliomyelitis embraces two stages. In the first it is directed against inflammation of the spinal cord and the paralysis of the muscles; in the second period the spinal lesion has run its course and the paralysis is considered incurable. Treatment is then directed to the prevention or palliation of deformities or toward facilitating the functions of the limb in spite of them.
These two periods are not, however, rigidly separated from each other in chronological order. From the very outset it is important to take certain precautions to prevent deformities, and while palliating these with orthopædic apparatus it is important for years to continue treatment of the paralyzed muscles in the hope that at least a remnant of them may be saved. To abandon the case to the orthopædic instrument-maker, or to neglect the problem of dynamic mechanics while applying electricity and studying the progress of fatty degeneration, are errors greatly to be condemned.
The treatment of the initial stage is necessarily purely symptomatic for the fever and convulsions, since the diagnosis cannot be made out until these have subsided.
As soon as the diagnosis is clear, however, certain measures should be adopted to diminish the hyperæmia of the spinal cord. Dally163 recommends the ventral decubitus; almost all modern authorities advise ice to the spine and ergot internally or subcutaneously. Thus, Althaus164 makes hypodermic injections of ergotin in doses of one-fourth of a grain for a child between one and two years old; one-third of a grain between three and five; and one half grain from five to ten; and these doses repeated once or twice daily. The only objection to this treatment is the degree of local irritation it can hardly fail to occasion. Hammond, who “affirms ergot to be of great service, the only medicine capable of cutting short the disease or of limiting its lesions,” recommends the internal administration of the fluid extract—ten drops three times a day for infants of six months, half a drachm for children between one and two years.165
163 Journ. Thérap., t. viii., 1880.
164 On Infantile Paralysis.
165 I have elsewhere quoted one case of early recovery under the use of ice and ergot; or was this a case of temporary paralysis?
The belladonna treatment, at one time so warmly praised by Brown-Séquard, retains to-day few adherents.
Simon advises cutaneous revulsives to divert the circulation to the [p. 1156] surface; thus, hot-air baths, mustard powder sprinkled on cotton enveloping the limbs. Ross advises mercurial inunction along the spine, followed by iodine and blisters. At the same time, iodide of potassium should be given internally in large doses. The action of this drug upon inflammations of the nerve-centres seems, within certain limits, to be indisputable, but its mode of action is certainly very obscure. Where the lesion can be attributed to a meningo-myelitis,166 the iodide may be expected to facilitate the absorption of the exudation. In these cases it should be continued for a long time.167
166 As in Leyden's first case, and my own.
167 Binz explains the local action of iodine by an exudation of leucocytes which follows the dilatation of blood-vessels. These elements break down the exudation into which they are poured, and thus facilitate its absorption.
Electrical treatment may be begun by the end of the first week after the paralysis. At this stage Erb recommends central galvanization as an antiphlogistic remedy for the myelitis. For this purpose a large anode must be placed over the spine at the presumed seat of the lesion, while the cathode is applied over the abdomen. By a slight modification of the method the cathode is placed over the paralyzed muscles. The application is stabile, and, according to Erb, should last from three to ten minutes; according to Bouchut, several hours daily. Erb's method is intended exclusively as a sedative to the local inflammation. When the cathode is placed on the muscles it is hoped that the descending current, replacing the lost nervous impulses, may avert the threatening degeneration of the muscle and nerve.
Faradization cannot modify the inflammatory lesions of the cord. As a means of averting degeneration in completely paralyzed muscles it is inferior to galvanism, and should not therefore be used in those muscles which refuse to contract under its stimulus. Its immense utility, however, is as a stimulus to muscles imperfectly paralyzed, but liable to degenerate from inaction and to be overborne by their antagonists. The excitation of contractions in such muscles is a powerful local gymnastic, helping to maintain nutrition by artificially-excited function.
For the same purpose, muscles inexcitable to the faradic current should be, when this is possible, made to contract by the interrupted galvanic current. After this treatment has been prolonged during several months, the faradic contractility often returns, and the current then should be changed (Seguin).
The value of electrical treatment has been very differently estimated. Erb remarks that “its results are not precisely brilliant.” Roth, whose testimony perhaps is not above suspicion, since evidently prejudiced, insists that numerous cases fall into his hands which have submitted for months to electrical treatment without the slightest benefit. On the other hand, Duchenne, as is well known, has expressed almost unbounded confidence in the therapeutic efficacy of faradization, declaring that it was capable of “creating entire muscles out of a few fibres.”
The sensitiveness of children to the electrical current, and their terror at its application, seriously interfere with its persistent use; as, if the patience of the physician is maintained, that of the parents is very likely to fail in the presence of the cries and resistance of the child.
It is very probable that some of the failures of electrical treatment are [p. 1157] due to the attempt to rely upon it exclusively, instead of suitably combining both electrical methods with each other and with other remedial measures. With our present knowledge it is safe to assert the desirability of persistent electrical treatment during at least the first two years following the paralysis. The currents must never be too strong—the faradic, at least, never applied for longer than ten minutes at a time. The muscles should be relaxed by the position of the limbs (Sayre). If the muscles continue to waste, and especially if they become fatty, the electrical response will grow less and less, and finally cease altogether.168 In the contrary case the galvanic contraction will become normal in quality, and the faradic contractility will return and increase, while the atrophy is arrested and the muscle regains its bulk and voluntary powers. Sometimes, as already stated, the latter is regained, while faradic contractility remains greatly diminished.169
168 Passing through three stages: faradic contractility diminished, galvanic contraction increased; faradic response lost, galvanic degenerative; absence of contraction to either current.
169 Sayre (loc. cit.) has noticed cases in which the muscle would contract several times under faradism, then refuse to do so for a day or two. This observation, if valid and not due to unequal working of the battery, is a most curious one.
A succedaneum to electricity that is highly prized by some authorities is strychnia, especially when subcutaneously administered. Pelione170 relates the cure of two cases in children of four and five years, after three and four years' duration of the paralysis, by strychnia—one-half milligramme daily. None should be given to children under six months, but over that age one-ninety-sixth of a grain may be given (Hammond). It should not be given subcutaneously more than two or three times a week (Seeligmüller).171
170 L'Union médicale, 1883.
171 Duchenne relates a case of a paralysis general at the outset and remaining so for six months. It was then treated by strychnine for five or six months, and at the end of that time had become limited to the lower extremities (Elect. local., ed. 1861, p. 278).
The incidental action of electricity in attracting blood to the paralyzed muscles may be sustained by several other methods.
Among these the external application of heat, either dry or in the form of hot douches, alternating with cold, is an adjuvant remedy of real importance. Beard has suggested tubing, malleable to the limbs, for the conduction of hot water. It is desirable to employ massage immediately after cessation of the hot applications.
On the value of massage and passive gymnastics opinion is even more variable than in regard to electricity. Roth, a specialist in orthopædics, places it at the head of all remedial measures, and denounces electricity in comparison. Many professional manipulators, ignorant of medical science, continually claim wonderful triumphs over regular physicians obtained by means of systematized massage. Volkmann, on the other hand, dismisses the pretensions of the Heilgymnastik with considerable contempt, declaring that faradization is the only method which can really secure exercise to paralyzed muscles.
The Swedish movement cure consists in passive movements imparted to a limb by the manipulator, at the same time that they are strenuously resisted by the patient. From the nature of this method, and its aim in stimulating the voluntary innervation of the muscles, it [p. 1158] is admirably adapted to hysterical paralysis. Theoretically, it is difficult to perceive the applicability of this method in organic atrophic paralysis, especially in young children, whose voluntary efforts cannot be commanded. There are, however, several real indications for passive gymnastics in the treatment of infantile paralysis. Surface friction and deep massage have some influence in dilating the blood-vessels and causing an afflux of blood to the cold and wasting muscles. A probably more important effect may be produced upon the contraction caused by malposition and adapted atrophy of certain groups of muscles. It is these contractions which formerly constituted the special objection of the orthopædist, and were treated almost universally by tenotomy. They are in any case the proximate cause of deformities; and, generally existing on the side of the joint opposite to the most severely paralyzed muscles, they keep these over-stretched and prevent them from receiving the benefit of the electrical treatment. Muscles which will not contract to the faradic current while thus stretched will often begin at once to do so when the rigidity of their antagonists has been overcome.
Persevering stretching by the hands will often overcome this rigidity as completely, and even more permanently, than will the tenotomy-knife. It is in this part of the treatment that entirely ignorant and even charlatan manipulations do, not unfrequently, achieve remarkable results.172
172 Of course many of those on record, and to some of which I have been a witness, relate to hysterical contractions, hysterical scoliosis, etc.
It is the retracted tendo Achillis and plantar fascia which most frequently require this manipulation. In the paralytic club-foot of young children all authorities agree in the value of repeated manipulations and restorations of the foot as nearly as possible to a position where it may be retained by simple bandaging. While turning the foot out it becomes perfectly white, but on releasing hold of it the circulation is restored, after which the manœuvre may be repeated (Sayre).
This principle of intermittent stretching by seizure of the segments of the limb above and below the joint applies to all forms of paralytic contraction. In the trunk the pelvis should be held by the mother, while the manipulator, seizing the thorax of the child between both hands, moves it gently but forcibly to and fro in the required direction. Great care is required in these manipulations—not merely to avoid exhausting the muscles, but even to avoid fracturing atrophied bones.
It may be laid down as a positive rule that tenotomy should never be performed in the contractions of spinal paralysis until the resources of manipulation have been exhausted. It is to be remembered that the rigidity depends on no active contraction of the muscle, but on its elastic retraction. The manœuvre of stretching does not appeal to the force of contractility, which may have been lost, but to the force of elasticity, which remains and can be made to act in a reverse direction. Finally, in the cases where the retracted muscles have not been originally paralyzed, but have lost the power of contracting during the process of shortening, this power may be restored if the muscle regain its normal length.
The operation of tenotomy, apparently a far more heroic measure, is often a less efficacious means of arriving at the results. Unless followed by the application of apparatus which permits motion in the joint, section of contracted tendons is only of brief utility.
[p. 1159]Though the edges of the cut tendon have been kept apart until the intervening space is filled by new tissue, union is finally effected by the latter, and retraction through elasticity is again imminent. Often, therefore, the deformity is repeated in spite of repeated operations; when it is not, the happy issue is due to the fact that, with increased freedom of locomotion immediately after the tenotomy, the patient has been enabled to bring the influence of weight to bear in such a manner as to fix the limb in a new and more convenient position. Thus, after section of the tendo Achillis for pes equinus, if the patient begins at once to walk on the paralyzed foot, the weight of the body, pressing down the heel, may keep the tendon stretched. So walking immediately after section of the hamstring muscles will have a tendency to produce genu-recurvation by the same mechanism which produces it in total paralysis, and the original deformity will not recur.
Besides the tendo Achillis, the parts which may be occasionally submitted to tenotomy are the plantar fascia, the peroneal muscles, very rarely the anterior tibial and extensors, the hamstrings, the thigh adductors. Section of the external rotators of the thigh or of the tensors of the fascia lata could hardly ever be required, and among these operations Hueter173 rejects that on the plantar aponeurosis as inadequate. The excavation in the foot it is designed to remedy depends upon alteration in the form of the tarsal bones, and can only be cured by means of forcible pressure exerted on their dorsal surface. Section of the peroneal muscles, often recommended by Sayre, is considered by Hueter to be superfluous after section of the tendon achilleis. Paralytic contraction of the hamstrings or of the hip flexors is rarely sufficiently severe to demand tenotomy.
173 Loc. cit., p. 416.
From what has preceded it is evident that maintenance of locomotion is of great importance, in order to avoid the deformities which are threatened by prolonged repose. Locomotion, however, can only be safely permitted with the assistance of apparatus capable of restraining the movements liable to be produced by the weight of the body. The supporting instrument which restrains movement in certain directions must, however, facilitate it in others: immovable apparatus, such as is not infrequently applied after tenotomy, is always injurious.
In young children unable to walk, the development of pes equinus may often be prevented by drawing down the foot to a sole splint made of thin wood, gutta-percha, or felt, and fastening it with a flannel bandage. The point of the foot may be drawn up toward the tibia by a strip of diachylon plaster. If the equinus has already developed, a splint of gutta-percha or of felt (Sayre) may be modelled to the leg and foot while the latter is held forcibly in dorsal flexion. The splint is attached by means of strips of adhesive plaster. It should extend as far as the knee, and be suitably padded (Seeligmüller).
In children able to walk a sole splint of thin metal, to which the foot had been previously attached by a flannel band, should be inserted in a stout leather boot. On the outer side of this boot should run a metallic splint, jointed at the ankle and extending to a leather band surrounding the leg just below the knee. A broad leather band, attached to the outer edge of the sole anterior to the talo-tarsal articulation, also passes up on [p. 1160] the outside of the foot, gradually narrowing until, opposite the ankle, it passes through a slit in the side of the shoe, to be attached to the leg-splint. This band tends to draw the point of the foot outward, and thus correct the varus (Volkmann). Sayre174 has improved on this shoe by dividing the sole at the medio-tarsal articulation, in which lateral deviation takes place, and uniting the anterior and posterior parts by a ball-and-socket joint, permitting movement in every direction.
174 Loc. cit., p. 88.
The orthopædic boot for the treatment of calcaneo-valgus is constructed on the same principle. But the splint runs up the inner side of the leg, and the leather strap passing to it from the edge of the sole draws the point of the foot inward and raises its depressed inner border (Volkmann). Essential to the treatment of this deformity, however, is the elevation of the heel. This is effected by means of a gutta-percha strap which is attached below to a spur projecting from the heel of the shoe, and above to a band encircling the leg. If, by rare exception, a paralytic calcaneus exists in a child unable to walk, a simple substitute may be found for the shoe in a board sole-splint projecting behind the heel, attached to the foot by a strip of adhesive plaster, which finally passes from the posterior extremity of the board up the back of the leg, and is there secured by a roller bandage.
The device of the gutta-percha elastic band to replace the gastrocnemius muscle illustrates a principle of wide application in orthopædic apparatus. The suggestion to replace paralyzed muscles by artificial ones was first made by Delacroix175 in an apparatus designed for the hand. The suggestion was repeated by Gerdy;176 and in 1840, Rigal de Gaillac proposed to exchange the metallic springs hitherto used for India-rubber straps. Duchenne elaborated the suggestion in a remarkable manner,177 using delicate spiral springs as a substitute for the lost muscles, and taking the greatest pains to make the insertion-points of these to exactly correspond with the insertions of the natural muscles. This was effected by means of sheaths, imitating natural tendinous sheaths, sewed to a glove or gaiter in which the hand or foot was encased.
175 Article “Orthopédie,” Dict. des Sciences médicales, quoted by Duchenne.
176 Traité des Bandages, 2d ed., Paris, 1837, quoted by Duchenne.
177 See chapter on “Prothetic Apparatus” in his treatise De l'Électrisation localisée.
At the present day the prothetic apparatus the most employed is that contrived by Barwell.178 The principle is the same as Duchenne's, but the artificial muscles are made of India-rubber, to which a small metallic chain is adjusted, and they are attached to the limb by means of specially-devised bands of adhesive plaster and pieces of tin bearing loops for the insertion of the muscle. In this apparatus the artificial muscles do not attempt to imitate the situation of the natural muscles with the precision which Duchenne claimed for his. Barwell's own dressing for talipes valgus consists of two rubber muscles which pass from the inner border of the foot, one to the inner, the other to the anterior, part of a band which encircles the leg just below the knee. For talipes calcaneus another band is required behind the leg, passing to the heel, as in Volkmann's apparatus, already mentioned. For talipes varus a rubber band [p. 1161] should pass on the outside of the foot; for equinus, one or more from the anterior part of the leg to the sides of the anterior part of the foot.
178 A tolerably minute account of the Barwell dressing is given by Sayre, loc. cit., p. 84.
Sayre endorses Barwell's dressing as entirely adequate for the treatment of any form of club-foot, but modifies it by substituting a ball-and-socket shoe for the adhesive plaster which should encircle the foot. The artificial muscles are then passed from the sides of the shoe to a padded leather girdle encircling the leg. A straight splint, jointed opposite the ankle, runs up from each side of the foot to this girdle, and from it two lateral upright bars, jointed at the ankle, pass to the heel of the shoe; and from below the joint passes forward on each side a horizontal bar reaching the point of origin of the artificial muscles and giving attachment to them.
In equinus it is necessary to bind the heel of the foot down firmly in the heel of the shoe; and this is accomplished by means of two chamois-leather flaps which are attached to the inside walls of the shoe and lace firmly across the foot.179
179 “The aim of the dressing or instrument is simply to imitate the action of the surgeon's hand; accordingly, any apparatus combining elastic force is far superior to any fixed appliance; and, moreover, that is to be preferred which is the most readily removable. Shoes, therefore, are better than bandages or splints. A proper shoe must have joints opposite the ankle and the medio-tarsal articulation; it must permit the ready application of elastic power; and it must not so girdle the limb as to interfere with the circulation” (Sayre, loc. cit., p. 91).
Sayre places so much confidence in the power of this elastic tension to overcome contractions that he rarely resorts to tenotomy in the treatment of paralytic talipes. Hueter, however,180 considers tenotomy much the speediest, and therefore the most desirable, way of removing contractions.181
180 Loc. cit.
181 Loc. cit.
Seeligmüller quotes with approval Böttger's method for the treatment of deformities, where the weight of the body is utilized to stretch the retracted tendons. Thus, for talipes equino-varus an over-reduction is effected under ether, and the foot forced into a position of moderate calcaneo-valgus. In this position it is retained by the immediate application of a plaster or silica bandage. After this has hardened the child should be encouraged to walk in the mould, with the addition of felt shoes having a slanting sole that is thickened like a wedge at the inner side of the foot and strapped on like a skate. Then, during the act of walking the body tends to constantly force down the heel and thus stretch the retracted tendo Achillis, while the bandage and felt sole (acting like a splint) prevent the inner side of the foot from slipping up.
For talipes valgus the method is analogous, but the foot is forced into an equino-varus position, so that the tendo Achillis is artificially shortened, and ultimately becomes a rigid band, capable, in spite of the sural paralysis, of sustaining the heel.
A cause of relapse in talipes not unfrequently overlooked is the presence of even slight contractions of the hip- and knee-joints. These by shortening the limb tend to the production of equinus, since the foot points itself in order to reach the ground. These contractions, whose rigidity is far inferior to that induced by chronic arthritis, may be overcome by forced extension under ether or gradually by manipulations, or by the weight-and-pulley apparatus, applied in the recumbent position, as in morbus [p. 1162] coxarius. The obvious objection to the latter method is the confinement in bed which it necessitates in a child enjoying at the time perhaps robust general health.
The contraction once overcome, the limb must be placed in apparatus which shall both maintain suitable extension and assist in supporting the trunk during station and locomotion. The latter purpose is effected, as in apparatus for chronic joint diseases, by transferring the weight of the body to steel splints running up each side of the limb, the outer one as far as a girdle which encircles the hips; the inner to a band surrounding the upper part of the thigh. Thus is extended the support which in paralysis limited to the leg-muscles is given by the steel splints inserted in the side of the club-foot shoes.
In the simplest form of apparatus locomotion is expected to be accomplished by the action of muscles inserted above the seat of the paralysis. Thus, when the muscles passing over the ankle-joint are paralyzed, the foot is moved as a dead weight by means of the quadriceps extensor, popliteus, and hamstring muscles inserted at the upper extremity of the leg. If the quadriceps cruris is paralyzed, the rotators of the thigh, ilio-psoas, sartorius, and adductor muscles, passing from the pelvis to the thigh, and which are so frequently intact in atrophic paralysis, are enabled to move the limb if the weight of the body is borne by steel splints, if these be light and properly jointed at the hip, knees, and ankle.182
182 Or the joint of the knee may be kept locked while the patient walks, when extension of the limb is mainly required, during both the active and passive movements of locomotion, the necessary flexion being supplied at the hip and ankle. By means of a key the knee-joint can be flexed during the sitting positions.
But an important aid to locomotion may be obtained from the artificial muscles, whose elastic tension is of such value in overcoming contractions. The quadriceps extensor, the most frequently paralyzed, may be supplemented by an India-rubber band and chain passing down the front of the thigh from a point on the pelvic girdle corresponding to the anterior iliac spine to a point on a leg-band, imitating the tibial insertion of the quadriceps tendon. Analogous bands stretched on the posterior aspect of the thigh simulate the hamstring muscles. When the external rotators are paralyzed, the artificial muscle must stretch from the pelvic girdle to a band encircling the upper part of the thigh.
The action of these muscles, apart from their elastic tension of repose, is thus explained by Duchenne: When any effort is made to move a paralyzed limb, the intact antagonists to the paralyzed muscles contract; thus, the flexors of the leg. But this contraction, being constantly opposed by the elastic tension of the artificial quadriceps, is restrained and gradual, instead of being brusque, jerking, and excessive, as it otherwise would be. This is the first result obtained. In the second place, contraction of the antagonist having ceased, the artificial muscle which has been stretched returns upon itself in virtue of its elasticity, and restores the limb to the position of normal equilibrium.
For the act of walking, however, the artificial quadriceps would require to be made tense enough to resist flexion, and thus keep the limb in extension. An artificial anterior tibial muscle, however, would require to yield to the intact gastrocnemius while the heel was being raised from the floor; then its elastic force should be sufficient to retract the point of [p. 1163] the foot in dorsal flexion during the pendulum movement which passively swings the leg forward. The tension of the artificial muscle should therefore be so adjusted that it can only be overcome by the active contraction of the gastrocnemius, and at the moment of greatest tension, immediately after stretching, it should be able to quite overcome the gastrocnemius, then relatively183 relaxed.
183 We say relatively, believing that the simultaneous contraction of antagonist muscles has been well established as a constant normal phenomenon.
The anterior tibial, gastrocnemius, and many other of the artificial muscles devised by Duchenne are still in use in the modified form given to them by Barwell. On the other hand, the action of the long peroneus in pronating the foot, and which Duchenne imitated by an elaborate artificial tendon following the exact course of the natural one, is to-day generally supplemented by the jointed shoe and laced bandage.
In paralysis of all the muscles surrounding a joint, when the limb is placid and no retractions by adapted atrophy have taken place, the artificial muscles can only serve to oppose the malpositions which are threatened from mechanical influences.
In the upper extremities prothetic apparatus has been principally used for progressive muscular atrophy. Paralysis of the wrist extensors is perhaps the only case in which the artificial muscle is required in anterior poliomyelitis. A string may be necessary to support the arm in paralysis of the deltoid, to avert luxation of the humerus.
Duchenne's ingenuity did not shrink from the difficult task of supplementing the muscles of the trunk. This he did by inserting the elastic spirals in corsets in a direction following that of the muscles paralyzed. Thus, a unilateral paralysis of the sacro-lumbalis may be met by a spiral splint running up one side of the spine; below, to the lateral posterior portion of a pelvic girdle. In bilateral paralysis two springs are used to antagonize the action of the abdominal muscles.
In Barwell's apparatus for the trunk184 India-rubber bands are again substituted for spiral springs. No attempt is made to imitate the direction of muscles, but the force is applied in any direction required to antagonize the pressure producing the deformity.185
184 Especially designed for habitual scoliosis, but applicable also to the paralytic deformity.
185 Volkmann (loc. cit., p. 778) thinks that the force of Barwell's India-rubber straps, whether for scoliosis or club-foot apparatus, is inadequate, and much inferior to metallic springs.
It is always important to remember the rarity of scoliosis caused by spinal paralysis of the trunk-muscles, and the much greater frequency with which this deformity occurs as a consequence of the paralytic shortening of a leg. A high shoe, equalizing the length of the lower extremities, is then the simple and efficient remedy.
In cases of long standing, even when the scoliosis is due to this cause, certain muscles on the concave side of the curve may become so retracted and rigid as to require tenotomy. Before this operation it is necessary to put the rigid muscles on the stretch as much as possible; and this may be done, if necessary, by means of Sayre's hanging apparatus. After this operation the spine may be straightened out with ease—an important distinction from advanced habitual scoliosis, where the alteration in the shape of the vertebræ defeats all attempts at rectification. The position [p. 1164] may be maintained by elastic straps or corsets and by removing the condition which has led to the deformity.
Seeligmüller criticises too unfavorably the entire system of elastic tension in the prophylaxis and treatment of paralytic deformities. He quotes Duchenne's admission, that in certain cases traction upon rigidly-retracted tissues becomes insupportably painful, and must be abandoned. It is in these cases that tenotomy becomes an indispensable preliminary to the use of apparatus. Sayre insists that the necessity for tenotomy is indicated when pressure on the rigid muscle is followed by instantaneous spasmodic contraction in the affected or neighboring muscles. He declares that such contractions indicate reflex irritations, show that the muscle has undergone structural change, and that any attempt to stretch or lengthen it would be followed by an excess of irritation and pain.
This explanation can hardly be accepted, since muscles, whether imperfectly or not at all paralyzed, which from position and adapted atrophy have become retracted, have necessarily undergone structural changes. The greater these changes, the greater the diminution of reflex excitability; and in any muscle completely paralyzed and degenerated this is entirely lost. If, however, the afferent nerves retain enough vitality, if the muscle be slightly paralyzed or altogether intact, then irritation of its tendon by stretching may serve to excite contractions in the belly of the muscle. The possibility of such spinal reflexes is demonstrated by the now familiar phenomenon of the tendon reflex in various spinal diseases.186 The contractions must be painful from the impediments offered to the progress of the contracting nerve, and from the exaggeratedly vicious position into which they tend to force the limb. Under these circumstances prothetic apparatus must be deferred until section of the tendons has been made.
186 “Passive muscular tension excites tonic contraction in a muscle, and this action may, in abnormal conditions, be excessive, as in the myelitic contractions (so-called tendon reflexes).... The afferent nerves commence in the fibrous tissues of the muscle, and seem to be especially stimulated by extension” (Gowers, On Epilepsy, 1881, p. 97).
SYNONYMS.—Unilateral lesion of the spinal cord; Spinal hemiplegia and hemiparaplegia; Unilateral spinal paralysis.
INTRODUCTION.—This disease remained unnoticed until twenty years ago, when Brown-Séquard, observing that certain lesions of the spinal cord were accompanied by symptoms resembling those which he witnessed in animals after section of one lateral half of the cord, recognized it as a special affection. Although some of the accompanying phenomena of such a section had likewise been observed by Stilling, Budge, Eigenbrodt, Tuerk, Schiff, Von Bezold, and Van Kempen,1 nevertheless this whole group of symptoms, as belonging to the same disease, was first clearly recognized and anatomically demonstrated by Brown-Séquard.2 According to this physiologist, a section or a destruction of a small portion of a lateral half of the spinal cord in its cervical region gives rise to the following phenomena: namely, on the injured side is observed a paralysis of voluntary motion, of the muscular sense, and of the blood-vessels; the latter, manifesting itself by a greater supply of blood and a higher temperature of the parts, may continue to exist for some years. There is, furthermore, an increased sensibility of the trunk and extremity to touch, prick, heat, cold, electricity, etc., owing to vaso-motor paralysis, though in some cases a slight anæsthesia may exist in a limited zone above the hyperæsthetic part, and also in certain parts of the arm, breast, and neck. Besides these symptoms, vaso-motor paralysis of the corresponding side of the face and of the eye, manifested by an elevated temperature and sensibility, partial closure of the eyelid, contracted pupil, slight contraction of some of the muscles of the face, etc., may also be present. On the opposite side of the injury an anæsthesia of all kinds of sensation, excepting the muscular sense, is observed in both extremities; there is also an absence of motor paralysis. The anæsthesia on this side is owing to the decussation of the sensory nerves in the spinal cord.
1 Eckhard, “Physiologie des Nervensystems,” in Handbuch der Physiologie, edited by L. Hermann, 2d part of vol. ii. p. 165.
2 “On Spinal Hemiplegia,” Lancet, Nov. 7, 21, and Dec. 12, 26, 1868, reported in Virchow and Hirsch's Jahresbericht for the year 1868, vol. ii. p. 37.
If the hemisection of the cord is made in the dorsal region, the functional disturbances are limited to that part of the body below the point [p. 1166] of division, and a hemiparaplegia, or paralysis of the corresponding lower extremity, will be the result.
From these facts it will be readily understood that a lesion occurring in any portion of one lateral half of the spinal cord of man must be followed by some or all of the above-mentioned symptoms, and that the phenomena produced by physiological experiments on animals constitute, in reality, the pathological basis of unilateral spinal paralysis in man. They will be more clearly understood by calling to mind the course of the musculo-motor, vaso-motor, and sensitive tracts in the spinal cord. Thus, the musculo-motor tracts, after having descended to the crura cerebri, cross one another in the pyramids of the medulla oblongata and adjoining upper portion of the spinal cord, forming the so-called decussation of the pyramids; they then descend through the spinal cord to supply the muscles of the same side of the body.3 A section of one lateral half of the cord therefore causes motor paralysis on the same side. The vaso-motor tracts remain uncrossed, and pass, each, through one lateral half of the cord to supply the vessels on the same side; some regions of the body are stated to make an exception to this rule. According to Brown-Séquard, the sensitive tracts conducting the different kinds of sensation, with the exception of the muscular sense, on the contrary, cross over to the opposite half of the spinal cord soon after their entrance into it, and thence pursue their further course to the brain. A section of one lateral half of the cord, therefore, will be followed by a loss of sensation of touch, pain, heat, tickling, etc. on the other side of the body.
3 Though, in the majority of cases, a complete decussation of the motor tracts probably takes place in the pyramids, the researches of Flechsig have shown (Die Leitungsbahnen im Gehirn und Rückenmark des Menschen, p. 273) that there are a number of others in which the decussation is not complete, but where a part of these tracts passes to the spinal marrow uncrossed on the inner surface of the anterior white columns.
The symptoms above mentioned must of course vary according to the extent, the intensity, and the particular nature of the lesion, as well as the height at which it is located in the spinal cord.
DEFINITION.—The chief characters of unilateral spinal disease are motor paralysis, hemiplegia, or hemiparaplegia, paralysis of the muscular sense and of the blood-vessels on the side of the lesion, and paralysis of sensation with preservation of the muscular sense on the other side of the body. These symptoms may vary, and be accompanied by other phenomena according to the particular seat, extent, and depth of the lesion.
SYMPTOMS.—According to the nature of the lesion, the symptoms of unilateral disease of the spinal cord may be developed suddenly, as, for instance, when caused by traumatic injuries; or in a gradual and slow manner, when they may be preceded by premonitory symptoms, such as vertigo, pain on the side of the lesion, etc. The most prominent clinical phenomena, as before mentioned, are motor paralysis on the side of the lesion, and anæsthesia on the opposite side of the body. The motor paralysis on the side of the lesion may, according to the seat of the latter, manifest itself in either the form of a hemiplegia or hemiparaplegia, and even extend in a light form to the opposite side of the body. In typical cases, however, in which the injury or disease is strictly confined to one lateral half of the cord, the motor power on the other side [p. 1167] of the body remains entirely undisturbed. At the same time, the muscular sense on the injured side is paralyzed or considerably diminished, and in some cases (Fieber, Lanzoni, Allessandrini) the electro-muscular excitability also has been found lowered, while in others it has remained normal. There is furthermore observed, on the side of the lesion, a vaso-motor paralysis, manifesting itself by a greater supply of blood to, and a higher temperature of, the paralyzed trunk and limbs, giving rise to an increase of sensibility (hyperæsthesia) of touch, prick, heat, cold, electricity, etc. in these parts. If the seat of the lesion is sufficiently high up in the cord, this paralysis extends, moreover, to the corresponding side of the face and eye, where it also causes an elevation of temperature, increase of sensibility, partial closure of the eyelid, contracted pupil, slight contraction of some of the muscles of the face, etc. In a number of cases at the boundary of the hyperæsthetic region a narrow anæsthetic zone is observed to exist on the breast, neck, or arm. This anæsthesia is owing to the division, at the level of the section, of some nerves of sensation on their way to the other half of the spinal cord. An increase of the reflex irritability of the tendons has in some cases (Erb, Schulz, Revillons) been observed, while in one case (Glaeser) the reflex was found to be absent. Swelling and œdema of the paralyzed limbs have also been met with (Glaeser), and in one case (Allessandrini) even swelling and pain in all the joints of the injured side were observed before death, while masses of coagulated blood in these joints, particularly in the knee, were revealed by the autopsy. The inflammatory affection of the knee-joint of the paralyzed leg has, moreover, been observed by Viguès, Joffroy, and Solomon.4 Frequently, atrophy of the paralyzed muscles takes place, especially in chronic cases. In one case (Fieber) even atrophy of the upper extremity of the uninjured side of the body was observed.
4 Erb, “Diseases of the Spinal Cord, etc.,” Cyclopædia of the Practice of Medicine, edited by H. v. Ziemssen, Amer. ed.
The most prominent symptoms observed on the side of the body opposite to the seat of the lesion are anæsthesia of every kind of sensation, preservation of the muscular sense, and absence of motor paralysis. Reflex action and electro-muscular contractility generally remain normal, though in one case (Fieber) the latter was found increased. Although the anæsthesia of the skin generally comprises every kind of sensation, three cases were observed (Fieber) in which the sensation of heat remained unimpaired, while the electro-cutaneous sensibility appeared to be lost. As a general rule, there is no vaso-motor paralysis on the uninjured side, though in some cases (Erb, Allessandrini) an elevation of temperature has been observed.
Besides the above symptoms, some others, less characteristic in nature, are now and then observed in individual cases. They are painful sensations on one or the other side, or even simultaneously on both sides of the body, and also a feeling of constriction at the level of the lesion (Erb). Disturbances of the functions of the bowels or bladder are also met with, though in other cases they are absent.
PATHOLOGICAL ANATOMY.—The pathological changes taking place in the spinal cord of patients affected with unilateral spinal paralysis must vary in different cases according to the particular nature of the lesion giving rise to the characteristic symptoms. In those cases reported to [p. 1168] have terminated by a gradual disappearance of the symptoms with or without therapeutic interference it is very probable that the exciting cause was a hyperæmia or a myelitis of a small portion of one lateral half of the spinal cord, sufficiently high in degree to impair the conducting power of the nerve-fibres passing through it. In some cases the myelitis may lead to a degeneration of the nerve-fibres, or even extend to the other half of the cord, and by calling forth additional symptoms render the case more complicated. In syphilitic cases the disease depends upon syphilitic deposits or neoplasms in the affected portion of the spinal cord; these cases, however, generally yield to treatment. In the same manner may circumscribed sclerosis give rise to the disease. Another cause may be found in the compression of the cord caused by meningeal tumors or by the fractured portions of some of the vertebræ. Chronic disease of the vertebral bones themselves (Pott's disease) may also, by encroaching upon the spinal cord, become an exciting cause.
The most typical cases, however, are those depending upon traumatic injuries, by which one lateral half of the spinal cord is forcibly divided. These lesions resemble in nature the division of the cord in the physiological experiments on animals, and are most frequently caused by a stab from a knife penetrating to the cord through the intervertebral spaces.
DIAGNOSIS.—In those cases in which the symptoms of unilateral spinal paralysis appear soon after an external injury to the spine, it becomes obvious that the latter is the exciting cause. In cases of a more chronic character, in which the symptoms appear gradually, the nature of the exciting cause can only be correctly determined by the observation of certain collateral symptoms characteristic of such causes as might give rise to the symptoms of the disease in question. As regards the diagnostic symptoms of unilateral spinal paralysis themselves, they are sufficiently characteristic to be easily distinguished from those of other forms of hemiplegia or hemiparaplegia. Thus, cerebral hemiplegia may be distinguished from the disease under discussion by the sensory disturbances being either absent or on the same side as the paralysis; furthermore, by the one-sided paralysis of the face and of the tongue and by the affection of various cranial nerves. The hemiplegic form of spasmodic spinal paralysis is distinguished by the absence of sensory disturbance, etc. Lastly, hemiplegia depending upon lesion of one side of the cauda equina is distinguished from unilateral spinal disease by the paralysis and anæsthesia being confined to the same side, and by generally affecting certain nervous districts of the lower extremities.
PROGNOSIS.—In unilateral spinal lesions the prognosis depends obviously on the particular nature and intensity of the exciting cause. On the whole, there are quite a number of cases reported, even of traumatic origin, which have terminated favorably.
TREATMENT.—The treatment of unilateral spinal paralysis depends, like the prognosis, upon the nature of the exciting cause. The principles upon which it is to be pursued of course are the same as those upon which the treatment of the various lesions causing the disease—such as hyperæmia, myelitis, sclerosis, wound of the spinal cord, etc.—is based.
SYNONYMS.—Chronic progressive bulbar paralysis; Progressive muscular paralysis of the tongue, soft palate, and lips.
HISTORY.—Although the particular group of symptoms constituting this disease must have been met with and known to the older medical observers, they were nevertheless first recognized as a special variety of paralysis in 1841 by Trousseau,1 who named the affection labio-glosso-laryngeal paralysis. But as the memorandum prepared by this distinguished physician at the time when, in consultation with a medical colleague, he had observed the particular symptoms of this affection, unfortunately remained unpublished, twenty years more elapsed before the first accurate and detailed description of the symptoms and progressive nature of this disease under the name of progressive muscular paralysis of the tongue, soft palate, and lips was rendered by Duchenne. The writings of this author directed at once the attention of other medical men to this disease, and since that time a large number of cases have been reported and discussed,2 while the microscopical examination accompanying the autopsies of many of them finally revealed that the seat of the lesion giving rise to the phenomena of this disease was to be sought in the nervous nuclei of the medulla oblongata. Hence at the present time the pathology of this disease is thoroughly understood.
1 Clinique médicale de l'Hôtel Dieu de Paris, vol. ii. p. 334.
2 A very considerable number of cases of this disease, and discussions thereon, will be found reported in Virchow and Hirsch's Jahresbericht über die Leistungen und Fortschritte der Gesammten Medizin, for the years 1866-80, vol. ii., section “Krankheiten des Nervensystems.”
DEFINITION.—That form of labio-glosso-laryngeal paralysis to be treated in the following pages is characterized by a progressive paralysis and atrophy of the muscles of the tongue, lips, palate, pharynx, and larynx, interfering in a greater or lesser degree with the articulation of words and sounds and with the functions of mastication and deglutition—affecting, furthermore, in the later stages of the disease, the voice and the function of respiration. The paralysis is caused by a progressive degeneration and atrophy of the ganglion-cells of those nerve-centres in the medulla oblongata from which the muscles of the above-named organs receive their supply of nervous energy, though in most cases the pathological process extends to, or even beyond, the roots of those nerves [p. 1170] which originate in these centres and terminate in the respective muscles. In many cases the pathological process extends to the spinal marrow, and there causes paralysis and atrophy of the muscles of the trunk, and, generally, of the upper extremities. Almost in every case the disease, as its name indicates, slowly progresses until it terminates in death.
There are, however, a number of cases observed which, though exhibiting the same or similar symptoms, do not, in reality, depend upon a progressive degeneration and atrophy of the centres and nerve-roots of the medulla, but, on the contrary, owe their symptoms to other causes; as, for instance, to tumors, hemorrhages, syphilitic neoplasms, etc., which, either by pressing upon the medulla from without, or, if situated within, by deranging in various manners the individual nervous elements of that part, may give rise to some or even all of the symptoms of true labio-glosso-laryngeal paralysis. These symptoms, however, according to the character of the lesion, may, after remaining stationary for some time, retrograde, and even disappear, as has been observed in syphilitic cases; or they may progress, and finally end in death. In order to distinguish these cases from the chronic or progressive bulbar paralysis some authors have attached the term retrogressive to this form of the disease.
SYMPTOMS.—As the degeneration of the nerve-centres in the medulla oblongata, upon which the disease depends, does not proceed in a regular fixed order, the order in which the clinical symptoms successively appear also varies in different cases. In the majority of cases, however, the symptoms appear gradually, manifesting themselves generally in the form of a greater or lesser impediment in the articulation of certain sounds or letters depending upon the movements of the tongue, such as e, i, k, l, s, and c, while at the same time a difficulty of mastication and deglutition may be experienced by the patient, due to the progressive development of the paralysis, which deprives the tongue of its lateral and forward movements. To this cause also, at this period, the apparently increased secretion of saliva, running from the corners of the mouth, must be attributed. With intelligent patients these symptoms are rendered less prominent by the special effort which they make to pronounce slowly for the purpose of hiding the deficiency in their speech. But as the disease advances the difficulty of articulation increases on account of the paralysis extending to the orbicularis oris, thus affecting the mobility of the lips and interfering with the pronunciation of the labial sounds p, b, f, m, and w. With the loss of power of articulation the patient's speech becomes gradually reduced to monosyllables, or even, finally, to incomprehensible and inarticulated grunts, by which he expresses his wants to his friends. In consequence of the paralysis of the lips the patient becomes unable to whistle or blow or to perform any movement depending upon these organs, while at the same time, through the disturbance created in the co-ordination of the facial muscles by the paralysis of the orbicularis oris, the mouth becomes transversely elongated and drawn downward by the action of the remaining unparalyzed muscles upon its angles. With the mouth partially open and the lower lip hanging down, the face of the patient has a peculiar sad and painful expression, while the voice assumes a nasal sound on account of the paralysis of the palate.
After a while the difficulty of deglutition, caused by the inability of the [p. 1171] tongue to properly assist in the formation of the bolus of food and its propulsion into the pharynx, increases on account of the paralysis extending to the muscles of the pharynx. The failure of these muscles in the performance of their special function of grasping the food and carrying it to the œsophagus obliges the patient to push it down the pharynx with his fingers. In some cases the difficulty of swallowing rests with solids, in others with fluids. The defective deglutition furthermore gives rise to spells of coughing and suffocation by portions of food getting between the epiglottis and larynx, while the paralyzed muscles of the palate allow the fluids to pass through the nose and enter the posterior nares.
As the case slowly proceeds the symptoms grow worse. The paralysis of the orbicularis oris reaches a point when this muscle is no more able to close the oral cavity; the mouth of the patient therefore remains open. The tongue, having now entirely lost its lateral, forward, or upward movements, rests motionless upon the floor of the mouth, evincing no other signs of life but occasional slight muscular twitchings. In some cases a diminution of the sense of taste, and also of that of touch in the tongue, pharynx, and larynx, has been observed. Atrophy of the tongue and lips now sets in, and the function of speech is almost entirely lost. The only letter which the patient is still able to pronounce is a (broad); all other sounds are indistinct and can hardly be understood. The paralysis of the tongue and other muscles of deglutition gives rise, furthermore, to an accumulation of the now excessively secreted saliva, which, being retained in the oral cavity, assumes the form of a viscid mucous liquid dripping from the mouth, extending, in the form of strings or ribbons, between the surfaces of the lips. Finally, when, through the progressive paralysis of the orbicularis oris, the patient can no more close the lips, the flow of saliva from the mouth becomes continuous; he is then seen engaged in the constant use of his handkerchief for removing the secretion.
In the latter stages of the disease the pathological process extends to the centres of respiration, paralyzing not only the muscles of respiration, but diminishing at the same time the contractile power of the lungs. A great difficulty of breathing—consisting not only in the want of depth of the inspirations, but, moreover, in a feebleness of expiration (manifested by weak, powerless coughing)—then ensues, and the patient is no further able to blow his nose or clear his bronchial tubes from the accumulating mucus. The paralysis of the muscles of the larynx, also occurring at this stage, not only increases the difficulties of deglutition, but most seriously affects the voice of the patient by decreasing the innervation of the vocal cords; the voice then becomes hoarse and weak, to be finally entirely lost.
The decrease in the innervation of the heart—which, lastly, also occurs—gives rise to irregularities in the action of this organ, followed by irregularity of the pulse, attacks of syncope, feelings of extreme weakness, and fears of death; whilst simultaneously the insufficient performance of the respiratory function renders the breathing of the patient weaker and weaker. Feelings of great oppression in the chest then arise, and the patient may die during one of the now frequent attacks of dyspnœa and suffocation.
No fever or pain is observed during the course of this disease; sensation [p. 1172] remains unaffected and the mind is perfectly clear. It is owing to these circumstances that frequently the patient walks about and attends to the duties of life, until shortly before death he becomes confined to bed by the great weakness caused by the want of nutrition. The appetite also remains good, but, unfortunately, in consequence of the difficulties attending the act of deglutition, the patient cannot satisfy the demands of his stomach. In the latter stages of the disease, therefore, when feeding can only be accomplished by the aid of the stomach-tube, every attempt to relieve the terrible gnawings and pains of hunger ends in a failure. With starvation staring in his face, the unhappy victim of the disease finally sinks into a state of extreme inanition, which, if life is not suddenly extinguished by an attack of suffocation, slowly leads to final dissolution.
The symptoms above described are those generally observed in uncomplicated cases of labio-glosso-laryngeal paralysis. There are, however, a number of cases reported in which the degenerative process has passed from the medulla oblongata to the spinal cord, and given rise to paralysis of the muscles of the neck, especially of the trapezius, and to those of the shoulders, and even to those of the upper extremities. Atrophy of the interosseus muscles of the hand, with those of the ball of the thumb, is not unfrequently observed. In other cases the disease has been found associated with progressive muscular atrophy, and in others, again, with paralysis of the lower extremities, accompanied by contractures and depending upon amyotrophic lateral sclerosis.
Labio-glosso-laryngeal paralysis is, as before mentioned, slow but progressive in its course, the duration of which is from one to three, or even five, years. It always terminates in death within the limits of this time, either from suffocation, inanition, paralysis of the heart, or some other intercurrent disease.
PATHOLOGICAL ANATOMY.—The macroscopical and microscopical examinations made during the last fifteen years of the cerebro-spinal axis in quite a number of cases of progressive labio-glosso-laryngeal paralysis show that this disease depends upon a degeneration of the nervous elements of the nuclei or nerve-centres in the medulla oblongata, involving also the roots of the nerves arising from the latter, and supplying with nervous energy the muscles of the different organs paralyzed in this disease. The exact nature of this degeneration—that is, whether it represents the sequel of a previously existing myelitis or originates in a so-called parenchymatous inflammation—appears to be as yet not definitely settled, though a number of pathologists entertain the view that it is preceded by a chronic myelitis. This view appears to be corroborated by the fact that frequently portions of the medulla oblongata and cervical portion of the spinal cord are found in a state of sclerosis. The uncertainty in the determination of the exact nature of the pathological process here concerned chiefly depends upon the diverse conditions in which the blood-vessels of the medulla are found. For while, in some cases, perhaps the majority, they have been found empty and in a normal condition, they have in others been met with congested with blood—a condition pointing to a chronic inflammatory process. In other cases, again, their walls have been found thickened or undergoing fatty degeneration.
At any rate, whether inflammatory or not, the now numerous microscopical examinations have revealed that the main features of the [p. 1173] process are a degeneration and atrophy, not only of the ganglion-cells of the respective nervous nuclei with their plexuses, but also of the fibres of the roots of the peripheral nerves arising from these centres; frequently the degeneration extends to some distance upon the nerves themselves. The microscopical changes in the ganglion-cells consist of an increase of yellow pigment, a gradual disappearance of their nuclei, terminating in an atrophy of the ganglionic bodies themselves, the pathological process leaving, finally, nothing but irregularly-shaped masses of pigment in the places of these bodies. The degeneration of the nerve-fibres appears to consist, as elsewhere, in a swelling of the axis-cylinder, accompanied by atrophy of the medullary sheath—a condition which finally leads to the complete destruction of these elements of the nerve-fibres, so that, at last, the whole nerve is only represented by the connective tissue of its neurolemma. Besides these changes, certain pathological products, such as conglomerations of fatty granules or globules, amylaceous bodies, etc., are also found in the degenerated nerve-centres and nerve-fibres.
Although in different cases the route which the degenerative process pursues is not the same, a certain general order, in which the nerves and nerve-centres are successively affected, and corresponding to the clinical symptoms, appears, nevertheless, to exist. It is thus that the nucleus of the hypoglossus has been observed to degenerate before the other nerve-centres. The nuclei of the spinal accessory and pneumogastric nerves, and also that part of the facial nucleus from which the inferior division of the facial nerve arises, appear to be affected next. The glosso-pharyngeal nucleus appears not to be affected in all cases, and still less frequently the nuclei and roots of the abducens, auditory, and trifacial nerves. The fibres forming the anterior pyramids have frequently been found degenerated throughout the medulla oblongata and pons; sclerosis also has been met with in this locality. In many cases, as has been remarked before, the pathological process descends into the spinal cord. Here, as in the medulla oblongata, the degeneration is principally confined to the motor centres located in the anterior horns, while the posterior horns, together with the lateral and posterior white columns, remain free from disease. The degree of degeneration taking place in the fibres of the respectively paralyzed muscles also corresponds to that of the elements of the nerve-centres from which they are supplied. The microscopical changes observed in the muscular fibres consist in a decrease of their diameter, accompanied by an increase in the number of their nuclei, as well as in the quantity of the connective tissue surrounding the primary bundles; some authors have observed amyloid degeneration of the muscular fibres.
ETIOLOGY.—The causes which give rise to the pathological process above described are but little known. Nevertheless, in a number of cases the disease has been traced back to taking cold, to physical as well as cerebral over-exertion, mental excitement, sorrow caused by misfortunes, poverty of nutrition, excessive use of tobacco, etc. In some cases the disease commences in the spinal cord in the form of progressive muscular atrophy or amyotrophic lateral sclerosis, and gradually extends to the medulla oblongata; in many other cases no particular cause can be found. The disease is rarely if ever met with in persons under twenty years of age, but is confined to adult life and old age. It occurs in [p. 1174] both high and low walks of life, attacking more frequently men than women.
DIAGNOSIS.—The symptoms of progressive labio-glosso-laryngeal paralysis are so characteristic in themselves as to exclude any mistake in the formation of a diagnosis. There are, nevertheless, some pathological conditions, such as hemorrhages in the medulla oblongata or thrombosis and embolism of the arteries supplying the latter with blood, which may give rise to the same or very similar phenomena, and thus render a correct diagnosis difficult. In such cases it must be remembered that the cause of true labio-glosso-laryngeal paralysis, depending upon degeneration and atrophy of the nervous nuclei along the floor of the fourth ventricle, is very gradual, while the symptoms produced by the causes before mentioned generally make their appearance in a more acute and sudden manner. The latter also, if not remaining stationary for some time, have rather a tendency to improvement, wanting, therefore, the progressive character of the former.
Tumors at the base of the brain also, by pressing upon the roots of the cerebral nerves or upon the medulla oblongata itself, may produce similar symptoms, which, on account of their comparatively slow and gradual development, may prove more difficult to distinguish from those characterizing genuine, progressive labio-glosso-laryngeal paralysis. Errors of diagnosis, however, may here be avoided by taking into consideration the special symptoms which generally accompany the presence of tumors of the brain, such as vertigo, headache, vomiting or even hemiplegia, and local paralysis. The sensory nerves also may become affected by the pressure of the tumor upon them. Thus, pressure upon the trifacial nerve may give rise to neuralgic pains, feelings of tingling and numbness, or even anæsthesia; while pressure upon the optic nerves or their tracts, or upon the olfactory and lingual nerves, will be followed by derangements of vision, smell, and taste. The symptoms produced by the pressure of a tumor at the base of the brain, moreover, are not strictly progressive, but may for some time appear, and disappear again before becoming permanent.
Facial diplegia, in which the expression of the face somewhat resembles that of a patient affected with labio-glosso-laryngeal paralysis, is distinguished from the latter disease by the paralysis affecting both divisions of the facial nerve, while the tongue remains free and deglutition is undisturbed.
There are still other affections of the cerebro-spinal axis, such as paralysis of the insane, disseminated sclerosis, etc., which in their course present some or perhaps all of the symptoms characterizing labio-glosso-laryngeal paralysis; these may be distinguished from the latter disease by taking their own special symptoms into consideration.
TREATMENT.—Although almost all cases of progressive labio-glosso-laryngeal paralysis terminate fatally, some cases have been reported by several observers in which a temporary improvement in the symptoms of the disease, or even a total cure, had been obtained by treatment. Of course such favorable results can only be obtained in the initial or earlier stages of the disease. Thus, Kussmaul recommends in the initial stage, when pains in the head and neck are present, wet cupping of the nape of the neck in strong persons, also the use of the shower-bath, while [p. 1175] nitrate of silver may be given internally. The application of galvanism in an alternate direction he also recommends—first, through the neck, and later on through the whole spinal column—and at the same time currents in an alternating direction from the neck and hypoglossus nerve to the tongue. Dowse reported a case of bulbar paralysis which he cured by the application of the constant current upon the paralyzed parts, subcutaneous injections of atropine and strychnine, with the internal administration of cod-liver oil, quinine, and phosphorus. He attaches great importance to the careful feeding of the patient through a tube passed through the nose, and to the strict application of the galvanic current; for excessive salivation he recommends atropine. Erb recommends to regulate the diet and the habits of life of the patient in such a manner as to avoid every irritation of the nervous system; furthermore, to generally stimulate the nutrition in order to produce a tonic effect upon the nervous system. For this purpose he principally relies upon a cautious hydropathic treatment, to be continued for a long time and with great regularity. The greatest importance, however, he attaches to electricity, considering the best method of galvanism as follows: “Galvanize with stabile application transversely through the mastoid processes and longitudinally through the skull, the so-called galvanism of the cervical sympathetic (anode on the nuchus, and cathode at the angle of the lower jaw), and then induce movements of deglutition (twelve to twenty at each sitting); besides this, apply, according to circumstances, direct galvanic or faradic currents to the tongue, lips, and palate.” The electric treatment must be continued for some time, with from four to seven sittings a week. Of the medicines taken internally, Erb recommends nitrate of silver, iodide of potassium, iodide of iron, chloride of gold and sodium, ergotin, belladonna, and preparation of iron and quinine.
[p. 1176]The nervous system of the higher animals is the apparatus by which stimuli coming from the external world or originating in the interior of their own bodies are perceived (its sensitive functions), or cause muscular contraction (its motor functions), or, lastly, cause molecular changes in tissues (its trophic functions).
Besides this power which the nervous system possesses of receiving impressions originating outside of itself and actively replying to them, it appears also to possess the power of originating within itself changes the result of which are sensations, movements, and trophic alterations. In other words, it can act automatically.
The apparatus for the performance of these various functions consists of the end-organs, the nervous centres, and the nerves.
The end-organs are peripheral mechanisms for the reception of impressions. The structure and mode of action of some of them, as the eye and the ear, are pretty well understood, while others, as those connected with the sense of touch, temperature, etc., are but imperfectly known. It is probable that there are also peripheral mechanisms which facilitate the delivery of the impulses coming from the nerve-centres to the organs, tissues, muscles, glands, etc.
The nervous centres are made up of nerve-cells variously connected with each other. They are immediately concerned in receiving impressions conveyed to them by the nerves and transforming them into sensations, or transmitting them to other organs, causing reflex actions, or in originating sensations and impulses.
The nerves are organs which, connected at one extremity with the end-organs and at the other with the nervous centres, convey peripheral impressions to the centres, and impulses and influences from the centres to the various organs of the body.
As it is with diseases of the peripheral nerves that we are now concerned, let us begin by looking more closely into their structure and functions.
The nerves appear to the naked eye as white strands of variable size, which a close inspection shows to be made up of threads or fibrils (best seen when the cut end of a nerve is examined) bound together by fine connective tissue and scantily supplied with blood-vessels. A microscopic examination shows that each of the fibrils visible to the naked eye is made up of a great number of fibres. These are the medullated [p. 1178] nerve-fibres, and they extend unbroken between the nerve-centres, with the cells of which they are connected, to the various organs and tissues, with which they also enter into organic union.
If we examine the structure of a medullated nerve-fibre, we find it to consist of a central thread called the central axis or axis-cylinder, in which close microscopic investigation shows a longitudinal striation, indicating that it is made up of fibrillæ. Surrounding the central axis like a sheath is the white substance of Schwann, composed of an oleo-albuminous substance, myeline, to which the nerves owe their white appearance. According to some observers, the white substance of Schwann is pervaded by a meshwork of fibres. Surrounding the white substance of Schwann is the sheath of Schwann, a structureless membrane having at intervals upon its inner surface nuclei, around which is a small amount of protoplasm.
At intervals along the course of the nerve-fibres are seen constrictions which involve the sheath and white substance of Schwann, but which do not affect the central axis, which passes unbroken the points of constriction. These are the nodes of Ranvier. Each space on the fibre beneath the nodes of Ranvier contains one of the nuclei of the sheath of Schwann, and probably, together with the white substance of Schwann, represents a cellular element. Diseased conditions sometimes respect the limits of these cellular elements.
The central axis is the true conducting part of the nerve-fibre, and it is probable that each of the fibrillæ of which it is composed has a separate peripheral termination and possesses the power of isolated conduction. The white substance of Schwann and the sheath of Schwann protect the central axis and seem to be connected with its nutrition.
The fibres in a nerve are bound together by loose connective tissue, the endoneurium, into the primitive bundles, which are again united by the perineurium, a membrane of laminated connective tissue, into more definite funiculi seen by the naked eye, the secondary bundles.
The secondary bundles are tied together by connective tissue, in which are found fat-cells and in which run the fine blood-vessels supplying the nerves. This connective tissue has been named the epineurium, and its condensed outer layers constitute the sheath of the nerve. It is important to observe that the connective tissue of the nerves is permeated by lymphatics which penetrate to the nerve-fibres, so that these are brought in contact with, and as it were, bathed in, the lymph.
Each nerve-fibre runs an isolated course from end to end, without anastomosing with other fibres, and near its peripheral termination it usually divides into two or more branches.
The fibres of the peripheral nerves depend for their integrity and nutrition upon their connection with central organs. The large multipolar cells of the anterior horns of gray matter of the spinal cord preside over the nutrition of the motor fibres; the ganglia on the posterior roots of the spinal nerves over the nutrition of the sensitive fibres.
If a nerve be severed from its connection with these centres of nutrition, it in a short while undergoes degenerative changes which result in complete destruction of its fibres.
The nerve-fibres when in a state of functional activity conduct impressions along their length to the end-organs or to the nerve-centres with [p. 1179] which they are in connection. This property of the fibres we call their conductivity. Each fibre conducts impressions in an isolated manner, not communicating them to other fibres with which it may be in contact. The rapidity of this conduction in human nerve-fibres is estimated at 33.9 meters (about 38 yds.) per second. This rate may be diminished by cold or by the anelectrotonic condition which is induced in the nerve by the passage through it of an electric current.
The nerve-fibres are irritable; that is, the application to them of stimuli excites their functional activity, and the impression made by the stimulus is transmitted to their extremities.1
1 The nerve-fibres in man do not appear to attain their full irritability until the fifth or tenth month after birth (Soltman).
The natural or physiological stimuli of the nerves act upon their extremities. Either they act through the peripheral mechanisms, giving rise to impressions which are conducted centripetally to the cells of the nerve-centres and there cause sensations or reflex actions, or they act upon the nerve-centres, giving rise to impulses which are conducted centrifugally and cause the various phenomena of contraction of muscles, inhibition of contraction, secretion, etc. Besides the physiological, there are other stimuli which excite the functional activity of nerve-fibres when applied at any point along their course.
Mechanical stimuli, blows, concussions, pressure, traction, etc., excite the nerves, causing sensations when applied to sensitive nerves, or contraction of muscles when applied to motor nerves. When mechanical stimuli are pushed farther, the irritability of the nerves may be destroyed. The gradual application of mechanical stimuli may destroy the irritability of nerve-fibres without any exhibition of excitation, as in paralysis from pressure. In nerve-stretching it is probable that many of the results depend upon the mechanical stimulation of the nerve-fibres by the traction. With a certain amount of force used the irritability of the nerve may be increased; carried farther, both the irritability and the conductivity may be diminished, and finally destroyed. As the centripetal fibres are soonest affected in the stretching, we can see how this proceeding is most beneficial in neuralgias, where a potent factor, if not the cause of the disease, is an abnormal excitability of the nerve-fibres. It is to be observed, nevertheless, that in cases of continued pressure upon mixed nerves the motor fibres are the first to suffer loss of their conductivity.
Sudden alterations of temperature act as stimuli to nerves. Heat increases their irritability, but its prolonged application diminishes it. Cold in general diminishes the nervous irritability, and may be carried to the point of completely destroying it temporarily.2
2 But at a certain age in freezing the ulnar nerve Mitchell found its irritability notably increased.
Many substances of widely-different chemical constitution, as acids, alkalies, salts, alcohol, chloroform, strychnine, etc., act as stimuli when applied directly to the nerves, apparently by causing in them rapid molecular changes. Also may be enumerated as chemical stimuli to the nerves substances found naturally in the body, as bile, bile salts, urea. The rapid withdrawal of water from nerve-tissue first increases, and then diminishes, its irritability. The imbibition of water decreases nervous irritability.
[p. 1180]An electric current of less duration than the 0.0015 of a second does not stimulate the nerve-fibres. It would appear that more time is required for the electric current to excite in nerve-tissue the state of electrotonus which is necessary to the exhibition of its functional activity. The electric current stimulates a nerve most powerfully at the moments of entrance into and exit from the nerve, and the more abruptly this takes place the greater the stimulation. Thus the weak interrupted currents of the faradic or induced electricity owe their powerfully stimulating effects to the abruptness of their generation and entrance into and exit from the nerves. At the moment of the entrance of the electric current into the nerve—that is, upon closing the circuit—the stimulating effect is at the negative pole or cathode; when the current is broken—i.e. leaves the nerve—the stimulating effect is at the positive pole or anode. A current of electricity very gradually introduced into or withdrawn from a nerve does not stimulate it. But if while a current is passing through a nerve its density or strength be increased or diminished with some degree of rapidity, the nerve is stimulated, and the degree of stimulation is in proportion to the suddenness and amount of change in the density or strength of the current. Although with moderate currents the stimulation of the nerve takes place only upon their entrance and exit, or upon variations of their density, nevertheless, with a very strong current the stimulation continues during the passage of the current through the nerve. This is shown by the pain elicited in sensitive nerves, and the tetanic contraction of the muscles to which motor nerves are distributed.
An important factor in electrical stimulation is the direction of the current through the nerve. A current passed through a nerve at right angles with its length does not stimulate it. Currents passing through a nerve stimulate in proportion to the obliquity of their direction, the most stimulating being those passing along the length of the nerve. Motor nerves are more readily stimulated by the electric current the nearer it is applied to their central connection. Experiments on the lower animals would seem to indicate that the motor fibres in a nerve-trunk do not all show the same degree of irritability when stimulated by the electric current.
The irritability of the nerve-fibres may be modified or destroyed in various ways. Separation of nerves from their nutritive centres causes at first an increase of their irritability, which is succeeded by a diminution and total loss, these effects taking place more rapidly in the portions nearer the nerve-centres. It is important to observe that an increase of irritability preceding its diminution is generally observed in connection with the impaired nutrition of nerves, and is the first phase of their exhaustion.
Prolonged and excessive activity or disuse of nerves causes diminution of their irritability, which may go to the extent that neither rest in the one case nor stimulation in the other can restore it. If a galvanic current is passed through a nerve in its length, the irritability of the fibres is increased in the region of catelectrotonus—viz. in the part near the cathode—and diminished in the region of anelectrotonus—viz. in the part near the anode. Certain substances, as veratria, first increase and then destroy the irritability of the nerves; others, as woorara, rapidly destroy it.
[p. 1181]The fibres of the peripheral nerves are divided into two classes: first, those which conduct impressions or stimuli to the nerve-centres, the afferent or centripetal fibres; and, secondly, those which conduct impulses from the centres to peripheral organs, the efferent or centrifugal fibres. Belonging to the first class are (1) sensitive fibres, whose stimulation sets up changes in the nerve-centres which give rise to a sensation; (2) excito-motor fibres, whose stimulation sets up in the nerve-centres changes by which impulses are sent along certain of the centrifugal fibres to peripheral end-organs, causing muscular contraction, secretion, etc. Belonging to the second class are (1) motor fibres, through which impulses are sent from the nerve-centres to muscles, causing their contraction; (2) secretory fibres, through which impulses from nerve-centres stimulate glands to secretion; (3) trophic fibres, through which are conveyed influences from the centres, affecting the nutritive changes in the tissues; (4) inhibitory fibres, through which central influences diminish or arrest muscular contraction or glandular activity. No microscopic or other examination reveals any distinction between these various fibres.
Every nerve-fibre has the power of conducting both centripetally and centrifugally, but the organs with which they are connected at their extremities permit the exhibition of their conductivity only in one direction. Thus, if a nerve-fibre in connection with a muscle at one end and a motor nerve-cell at the other be stimulated, although the stimulus is conducted to both ends of the fibre, the effect of the stimulus can only be exhibited at the end in connection with the muscle, causing the muscle to contract. Or if a fibre in connection with a peripheral organ of touch be stimulated, we can only recognize the effects of such stimulation by changes in the nerve-cells at its central end which give rise to a sensation.
When we consider the extensive distribution and exposed position of the peripheral nerves, their liability to mechanical injury and to the vicissitudes of heat and cold, we cannot but anticipate that they will be the frequent seat of lesions and morbid disturbances. It may be that not a few of their diseased conditions have escaped observation from a too exclusive looking to the central nervous system as the starting-point of morbid nervous symptoms. This occurs the more readily as many of the symptoms of disease of the peripheral nerves, as paralysis of muscles, anæsthesia, hyperæsthesia, etc., may equally result from morbid conditions of the brain or spinal cord, and not unfrequently the peripheral and central systems are conjointly affected in a way which leaves it doubtful in which the disease began or whether both systems were simultaneously affected.
The elucidation of such cases involves some of the most difficult problems in diagnosis, and requires not only a thorough acquaintance with the normal functions of the peripheral nerves, but also the knowledge of how those functions are modified and distorted in disease.
The symptoms arising from injuries and diseases of the peripheral nerves are referable to a loss, exaggeration, or perversion of their functions, and we often see several of these results combined in a single disease or as the result of an injury.
The fibres may lose their conductivity or have it impaired, causing feebleness or loss of motion (paralysis), or diminution or loss of sensation [p. 1182] (anæsthesia). Or there may be induced a condition of over-excitability, giving rise to spasm of muscles and sensations of pain upon the slightest excitation, not only from external agents, but from the subtler stimulation of molecular changes within themselves (hyperæsthesia). Or diseased conditions may induce a state of irritation of the nerve-fibres, which shows itself in apparently spontaneous muscular contraction or in sensations abnormal in their character, and not corresponding to those ordinarily elicited by the particular excitation applied, as formication or tingling from simple contact, etc. (paræsthesiæ), or in morbid alterations of nutrition in the tissues to which the fibres are distributed (trophic changes).
If we could recognize the causes of all these varied symptoms and discover the histological changes invariably connected with them, it would enable us to separate and classify the diseases of the peripheral nerves, and give us a sound basis for accurate observation and rational therapeutics. But, although the progress of investigation is continually toward the discovery of an anatomical lesion for every functional aberration, we are still so far from a complete pathological anatomy of the peripheral nerves that of many of their diseases we know nothing but their clinical history. We are therefore compelled in treating of the diseases of the peripheral nerves to hold still to their classification into anatomical and functional, as being most useful and convenient, remembering, however, that the two classes merge into each other, so that a rigid line cannot be drawn between them, and that such a classification can only be considered as provisional, and for the purpose of more clearly presenting symptoms which we group together, not as entities, but as pictures of diseased conditions which may thus be more readily observed and studied.
It is well to begin the study of the diseases of the peripheral nerves by a consideration of nerve-injuries, because in such cases we are enabled to connect the symptoms which present themselves with known anatomical alterations, and thus obtain important data for the elucidation of those cases of disease in which, although their symptomatology is similar, their pathological anatomy is imperfectly or not at all known.
If the continuity of the fibres of a mixed nerve be destroyed at some point in its course by cutting, bruising, pressure, traction, the application of cold, the invasion of neighboring disease, etc., there will be an immediate loss of the functions dependent on the nerve in the parts to which it is distributed. The muscles which are supplied by its motor fibres are paralyzed; they no longer respond by contraction to the impulse of the will. No reflex movements can be excited in them either from the skin or the tendons. They lose their tonicity, which they derive from the spinal cord, and are relaxed, soft, and flabby. As the interrupted sensory fibres can no longer convey impressions to the brain, we might naturally look for an anæsthesia, a paralysis of sensation, in the parts to which they are distributed, as complete as is the loss of function in the muscles. Such, however, is not the fact. Long ago cases were observed in which, although sensitive nerves were divided, the region of their distribution retained more or less sensation, or seemed to recover it so [p. 1183] quickly that an explanation was sought in a supposed rapid reunion of the cut fibres. Recent investigations, moreover, show that in a large number of cases where there is complete interruption of continuity in a mixed nerve the region to which its sensitive fibres are distributed retains, or rapidly regains, a certain amount of sensation, and that absolute anæsthesia is confined to a comparatively small area, while around this area there is a zone in which the sensations of pain, touch, and heat are retained, though in a degree far below the normal condition; in short, that there is not an accurate correspondence between the area of anæsthesia consequent upon cutting a sensitive nerve and the recognized anatomical distribution of its fibres. We find the explanation of this partly in the abnormal distribution of nerves, but principally in the fact of the frequent anastomoses of sensitive nerves, especially toward their peripheral distribution, thus securing for the parts to which the cut nerve is distributed a limited supply of sensitive fibres from neighboring nerves which have joined the trunk below the point of section. This seems proved not only by direct anatomical investigation, but also from the fact that the peripheral portion of the divided nerve may be sensitive upon pressure, and that the microscope shows normal fibres in it after a time has elapsed sufficiently long to allow all the divided fibres to degenerate, in accordance with the Wallerian law. Some of the sensation apparently retained in parts the sensitive nerve of which has been divided may be due to the excitation of the nerves in the adjacent uninjured parts, caused by the vibration or jar propagated to them by the mechanical means used to test sensation, as tapping, rubbing, stroking, etc.3 It is to be observed that this retained sensation after the division of nerves exists in different degrees in different regions of the body; thus it is greatest in the hands, least in the face.
3 Létiévant, Traité des Sections nerveuses.
As the vaso-motor and trophic nerve-fibres run in the trunks of the cerebro-spinal nerves, destructive lesions of these trunks cut off the influence of the centres with which those fibres are connected, and hence they are followed by changes in the circulation, calorification, and nutrition of the parts to which they are distributed. Thus, the loss of the vaso-motor influence is at first shown in the dilation of the vessels and the unvarying warmth and4 congestion of the part.5 This gives way in time to coldness, due to sluggish circulation and diminished nutritive activity. Marked trophic changes occur in the paralyzed muscles. They atrophy, their fibres becoming smaller and losing the striations, while the interstitial areolar tissues proliferates, and finally contracts cicatricially. The skin is sometimes affected in its nutrition, becoming rough and scaly. Other trophic changes of the skin resembling those produced by irritation of a nerve are very rarely seen, and they may probably be referred to irritation of fibres with which the part is supplied from neighboring trunks.
4 A remarkable exception is seen, however, in the effect of gradual pressure experimentally applied to nerve-trunks until there is complete interruption of sensation and motion, in which case the temperature invariably falls.
5 In a case of gunshot wound that came under the writer's care in 1862, the leg and foot, which were paralyzed from lesion of the popliteal nerve, remained warm and natural in color during repeated malarial chills, which caused coldness and pallor of the rest of the body.[p. 1184]
Anatomical Changes in the Divided Nerve and Muscles.—The peripheral portion of a divided nerve separated from its nutritive centres degenerates and loses its characteristic appearance, looking to the naked eye like a grayish cord, and being shrunken to one-fourth of its natural size. The changes which take place in the degeneration of the nerve-fibres, and which proceed from the point of lesion toward the periphery, are, first, an alteration of the white substance of Schwann, which breaks into fragments, these melting into drops of myeline, and finally becoming reduced to a granular mass. The central axis at a later period likewise breaks up, and is lost in the granular contents of the sheath of Schwann. Meanwhile, absorption of the débris of the fibres goes on, until, finally, there remains but the empty and collapsed sheath of Schwann with its nuclei, the whole presenting a fibrous appearance. When this has taken place the degenerated motor nerve-fibres can no longer be excited, and no stimulation applied to them can cause the muscles to contract. At the same time, the muscles atrophy and undergo degenerative changes in their tissue. The fibres become smaller and their transverse striæ indistinct, with the appearance of fatty degeneration, and finally there is proliferation of the interstitial cellular tissue. They do not, however, lose their contractility, and upon a mechanical stimulus being applied directly to them they contract in a degree that is even exaggerated, but with a slowness that is abnormal. If, now, we apply the stimulus of electricity to the muscles themselves, we encounter phenomena of the greatest interest and importance. The application of the faradic current, however strong, elicits no contraction; there is loss of faradic excitability. But if the galvanic current be applied the muscles contract, and that, too, in reply to a current too weak to excite healthy muscles to action; there is increased galvanic excitability. The kind of contraction thus induced is peculiar, differing from that ordinarily seen in muscles. Instead of its being short, and immediately followed by relaxation, as when we make or break the galvanic current in healthy muscles, it is sluggish, long-drawn out, and almost peristaltic in appearance. This is characteristic of degenerated muscles, and is the degenerative reaction. But there is also a change in the manner in which the degenerated muscles reply to the two poles of the galvanic current. Instead of the strongest contraction being elicited, as in the normal condition, by the application of the negative pole to the muscle (C. C. C., cathode closing contraction), an equally strong or stronger is obtained by the application of the positive pole (A. C. C., anode closing contraction), while the contraction normally caused on opening the circuit by removal of the positive pole (A. O. C., anode opening contraction) becomes weaker and weaker, until it is at last exceeded by the contraction upon opening the current by the removal of the negative pole (C. O. C., cathode opening contractions). In short, the formula for the reply of the healthy muscles to galvanic excitation is reversed; there is a qualitative galvanic change in the paralyzed and degenerated muscles.
If no regeneration of the nerve takes place, the reaction of the muscles to the galvanic current is finally lost, and they exhibit those rigid contractions which probably result from a sclerotic condition of the intramuscular areolar tissue.
After complete destruction of the fibres of a nerve at some point of its [p. 1185] course, even when a considerable length of it is involved, and after the consequent degeneration of the peripheral portion has taken place, we have, with lapse of time, restoration of its function, consequent upon its regeneration and the re-establishment of its continuity. The histological changes by which the degenerated fibres are restored and the divided ends reunited have not been made out with such certainty as to preclude difference of opinion as to the details. But the process in general seems to be a proliferation of the nuclei in the sheath of Schwann, with increase of the protoplasm which surrounds them, filling the sheath of Schwann with the material from which the new fibre originates. In this mass within the sheath is formed first the central axis of the new fibre, which is later surrounded by the white substance of Schwann. With the regeneration of the nerve-fibres the functions of the nerve return, but in the order of sensation first, and afterward the power of transmitting the volitional impulse to the muscles. Even after regeneration has so far advanced that the muscles may be made to contract by an exercise of the will, the newly-formed fibres fail to respond to other stimuli; thus, the faradic current applied to the nerve does not cause the muscles to contract; the stimulation is not transmitted along the imperfectly restored fibres.
It may be here remarked that after regeneration has restored the functions of a divided nerve the muscles to which it is distributed may still exhibit for a time the degenerative reaction in consequence of unrepaired changes in themselves. In the end we may look for complete restoration in both nerve and muscles.
The time required for the regeneration and reunion of a divided nerve depends somewhat upon the manner in which the destruction has been caused. Thus, a nerve which has been divided by a clean cut, and where the cut ends remain in apposition or close proximity, unites much more readily than one in which bruising, tearing, or pressure has destroyed an appreciable length of its fibres or the divided ends have been thrust apart.
In complete division of a nerve we must not look for regeneration and restoration of its functions, even in favorable circumstances, before the lapse of several months, although cases have been recorded where the process has been much more rapid.
Injuries of mixed nerves, with incomplete destruction of the fibres, give rise to many and varied symptoms, some of which are the direct result of the injury—many others of subsequent changes of an inflammatory character (neuritis) in the nerves or in the parts to which they are distributed. Pain is one of the most prominent symptoms immediately resulting from nerve-injury, although as a rule it soon subsides. There is sometimes merely numbness or tingling, or there may be no disturbance of sensation at the moment of injury. Rarely is spasm of muscles an immediate effect. Generally, motion is at first very much impaired, but if the injury is not grave enough to cause a lasting paralysis, the muscles may rapidly regain their activity. In observing the effects of injuries of mixed nerves one remarkable fact strikes us: it is the very much greater liability of the motor fibres to suffer loss or impairment of function. Thus, it is common to see sensation but little or only transiently affected by injuries which cause marked paralysis of muscles. [p. 1186] So in the progress of recovery the sensory disturbances usually disappear long before restoration of the motor function; indeed, sensation may be entirely restored while the muscular paralysis remains permanent. Direct experimental lesions of the mixed nerve-trunks of animals give the same result.6 For this immunity of the sensitive nerve-fibres no explanation can be given other than an assumed difference in their inherent endowments.
6 Luderitz, Zeitschrift für klin. Med., 1881.
According to the amount of damage the nerve has sustained will there remain after the immediate effects of the injury have passed off more or less of the symptoms already described as due to loss of conductivity in the fibres—viz. paralysis of motion, and anæsthesia. Sometimes the impairment of conductivity in the sensitive fibres shows itself by an appreciable time required for the reception of impressions transmitted through them, giving rise to the remarkable phenomenon of delayed sensation. Degeneration of the nerve peripherally from the point of lesion, and consequently of the muscles, will likewise take place in a greater or less degree, according to the amount of the injury and the subsequent morbid changes, and give rise to the degenerative reaction which has been already described. We will not, however, always encounter the degenerative reaction in the typical form which presents itself after the complete division of nerves. Many variations from it have been observed; as, for instance, Erb's middle form of degenerative reaction, in which the nerve does not lose the power of replying to the faradic or galvanic current, but the muscles show both the loss of the faradic with increased galvanic excitability, with also the qualitative change in regard to the poles of the galvanic current. Such irregularities may be explained by the supposition of an unequal condition of degeneration in the nerve and the muscles. A rare modification has been recorded which has once come under the writer's observation, in which the muscles reply with the sluggish contraction characteristic of the degenerative reaction to the application of the faradic current.
A highly important class of symptoms arise later in injuries of nerves, due not so much to a loss as to an exaggeration or perversion of their functions: they are the result of molecular changes in the nerves, giving rise to the condition called irritation. Irritation of motor nerves shows itself in muscular spasm, or contractions of a tonic or clonic character, or in tremor. If the sensitive fibres are irritated by an injury or the subsequent changes in the nerve resulting from it, we may have hyperæsthesia of the skin, in which, although the sense of touch may be blunted, the common sensation is exaggerated, it may be, to such a degree that the slightest contact with the affected part gives rise to pain or to an indescribable sensation of uneasiness almost emotional in its character—something of the nature of the sensation of the teeth being on edge. There may be hyperæsthesia of the muscles, shown by a sensitiveness upon deep pressure, in which the skin has no part. Pain, spontaneous in its character, is a very constant result of nerve-irritation, whether caused by gross mechanical interference or by the subtler processes of inflammation in the nerve-tissue. It is generally felt in the distribution of the branches of the nerve peripheral to the point of lesion, although it is occasionally located at the seat of the injury. Neuralgias are a common result of the irritation of nerves from injuries.
[p. 1187]Causalgia, a burning pain, differing from neuralgia, and sometimes of extreme severity, is very frequent after injuries of nerves, especially in parts where the skin has undergone certain trophic changes (glossy skin). A number of abnormal sensations (paræsthesiæ) result from the irritation of sensitive fibres, and are common after nerve injuries. Among these we may mention a sensation of heat (not the burning pain of causalgia) in the region of the distribution of the nerve, which does not coincide with the actual temperature of the part; it occurs not unfrequently after injury to a nerve-trunk, and may be of value in diagnosis.
The effect of irritative lesions of mixed nerves upon nutrition is very marked, and sometimes gives rise to grave complications and disastrous results. Any or all of the tissues of the part to which the injured nerve is distributed may be the seat of morbid nutritive changes.
In the skin we may have herpetic or eczematous eruptions or ulcerations. It may become atrophied, thin, shining, and, as it were, stretched tightly over the parts it covers, its low nutrition showing itself in the readiness with which it ulcerates from trifling injuries. This condition, called glossy skin, usually appears about the hands or feet, and is very frequently associated with causalgia. The hair may drop off, or, as has been occasionally seen, be increased in amount and coarsened, and the nails become thickened, crumpled, and distorted.
The subcutaneous cellulo-adipose tissue sometimes becomes œdematous, sometimes atrophies, and rarely has been known to become hypertrophied. The bones and joints, finally, may, under the influence of nerve-irritation, undergo nutritive changes, terminating in various deformities.
With regard to the trophic changes, as well as to the pain and paræsthesiæ resulting from nerve-injury, we must bear in mind that they may be attributed not only to the direct irritation of trophic and sensitive fibres in the injured nerve, but also, in part, to influences reflected from abnormally excited nutritive centres in the spinal cord, and to the spread of the sensitive irritation conveyed to the brain by the injured fibres to neighboring sensitive centres, thus multiplying and exaggerating the effect, causing, as it were, sensitive echoes and reverberations. Indeed, the variety of the symptoms resulting from apparently similar nerve lesions would seem to point to the introduction of other factors in their causation than the simple injuries of the nerve-fibres themselves.
DIAGNOSIS OF NERVE INJURIES.—Although in the great majority of cases the circumstances attending nerve injuries render their diagnosis a matter of little difficulty, it is yet important to keep in mind those symptoms which distinguish them from lesions or diseases of the brain and spinal cord, inasmuch as in cases of multiple lesion, injuries to the spinal column, or where the history of the case is imperfect, it may be difficult to determine to which part of the nervous system, peripheral or central, some of the gravest resulting troubles are due. Paralysis, spasm, anæsthesia, atrophy, etc. may be of central or spinal as well as peripheral origin, and an intelligent prognosis and rational treatment alike demand that we should distinguish between them. Moreover, many diseased conditions of the peripheral nerves of whose pathology we are ignorant, and in which localizing symptoms—i.e. those indicating the exact point at which the nerve is implicated—are wanting, can only be distinguished as peripheral affections by the occurrence of symptoms which we [p. 1188] recognize as identical with those arising from injuries of nerves, in which definite histological changes are known to occur. Indeed, cases of disease of the nervous system are not infrequent in which a careful study of their symptomatology leads to a difference of opinion in the minds of the best observers as to whether their seat is central or peripheral. We will notice here some of the prominent symptoms resulting from nerve injuries which may be useful in distinguishing peripheral from central lesions, although in many cases it is only by the careful consideration of all symptoms and the impartial weighing of all attending circumstances that a probable conclusion can be arrived at.
The rapid loss of muscular tone and the early atrophy of the muscles is a mark of paralysis from nerve-injury which distinguishes it from cerebral paralysis, even when the latter occupies circumscribed areas, as is sometimes the case in cortical brain lesion. In spinal paralysis also the muscles retain their tone and volume (the latter being slightly diminished by disuse), except in extensive destruction of gray matter, when all tonicity is lost, and in lesions of the anterior horns of gray matter (poliomyelitis), when there is loss of muscular tone and marked atrophy. The first of these spinal affections may be distinguished by the profound anæsthesia and by the paralysis being bilateral—by the implication of bladder and rectum and the tendency to the formation of bed-sores; such symptoms being only possible from nerve-injury when the cauda equina is involved. In poliomyelitis the complete integrity of sensation—which is almost always interfered with at some period after nerve-injury—and the history of previous constitutional disturbance will aid us in recognizing the diseased condition. While the reflexes are wanting in peripheral, they are, as a rule, retained, and often exaggerated, in cerebral and spinal paralysis; the exceptions being in the two lesions of the cord above mentioned, in which the reflex arc is of course destroyed by the implication of the gray matter. Loss or alteration of sensation, where it occurs from nerve-injury, generally shows itself in the distribution of the nerve, while the sensitive disturbances from disease or injury of the brain or spinal cord are less strictly confined to special nerve territories. The trophic disturbances arising from nerve-irritation are distinctively characteristic of nerve-injury.
But it is in the behavior of the nerves and muscles to electricity that we find some of the strongest points on which to base a diagnosis of nerve-injury, and, although not always conclusive as to the seat of lesion, it enables us to reduce within very narrow limits the field for discrimination. The degenerative reaction which we have seen takes place in muscles the continuity of whose nerves have been destroyed, or in which degenerative changes have taken place in consequence of injury to their nerves, is never found in muscles paralyzed from the brain. In spinal paralysis resulting from transverse myelitis the electrical excitability of the nerves and muscles may be increased or diminished, but there is no degenerative reaction. In progressive muscular atrophy a careful electrical examination may discover the degenerative reaction in the affected muscles; but it is too obscure, and there are besides too many characteristic symptoms in that disease, to allow of a practical difficulty in diagnosis from its presence. In poliomyelitis anterior (infantile paralysis and the kindred affection in the adult) we have, it is true, the quantitative, [p. 1189] qualitative changes of degenerative reaction, such as are seen after nerve-injury, and in such cases its presence is not conclusive of peripheral lesion. Here we may be assisted by remembering that while in poliomyelitis sensation is intact, in nerve-injury it is almost always affected in a greater or less degree, although it may have been recognizable but for a short time. In lead paralysis we also have the degenerative reaction, but whether the seat of lesion in that affection is central or peripheral is an undecided question.
TREATMENT OF NERVE-INJURIES.—The therapeutics of nerve-injuries belong largely to surgery. When there is complete division of a nerve the ends should be united by suture at the time of injury. When this has not been done, and after the lapse of time no return of function is observed, the ends of the nerve should be sought for, refreshed with the knife, and brought together by suture. There is the more hope that such a procedure will be successful as we know that after a time the fibres of the peripheral portion of the nerve may be regenerated, even when there has been no reunion, and thus be in a condition to render the operation successful. It is a matter for consideration whether in injuries in which a certain portion of the nerve, not too great in extent, has been crushed or otherwise obviously destroyed, it would not be best to excise the destroyed portion and bring the ends together. Whether the use of electricity, the galvanic current, hastens the regeneration and restitution of the injured nerves cannot be affirmed with certainty, although in practice this has seemed to us to be the case, and the known catalytic action of the current gives us a possible explanation of such beneficial effects. But, however this may be, it is certain that with the first symptoms of returning function in the nerves and muscles the use of electricity obviously accelerates the improvement. And, again, in the treatment of the results of nerve-injury, such as paralysis, anæsthesia, pain, it is in the careful and very patient use of the electric currents, both faradic and galvanic, that most confidence is to be placed; the galvanic being generally most applicable and giving the better results. The symptoms of nerve-irritation are amongst those most difficult to treat successfully. Counter-irritation, heat, cold, electricity, may all be tried in vain, and as a last resource against pain, ulceration, and perverted nutrition we may be obliged to resort to nerve-stretching, or neurotomy. Under the head of Neuritis much must be said of treatment applicable to the inflammation, acute and chronic, resulting from nerve-injuries.
Although inflammation of the nerves has been for a long time a recognized disease, its frequency and the extent and importance of its results have been appreciated only within a comparatively short time. The observations upon neuritis were formerly almost exclusively confined [p. 1190] to acute cases, the results of traumatic lesions or the invasion of neighboring disease, while the more obscure forms occurring from cold, toxic substances in the circulation, constitutional disease, etc., or those apparently of spontaneous origin, escaped attention, or were classed according to their symptoms simply as neurosis, functional disease of the nerves, or affections of the spinal cord. Hence the classic picture of neuritis is made to resemble exclusively the acute inflammation of other tissues, and tends to blind as to the subtler but not less important morbid processes in the nerves which at present we must classify as inflammation, though wanting, it may be, in some of the striking features seen in connection with inflammatory processes elsewhere. In short, we must not look for heat, redness, pain, and swelling as absolutely necessary to a neuritis.
Entering into the structure of the peripheral nerves we have the true nervous constituent, the fibres, and the non-nervous constituent, the peri- and endoneurium, in which are found the blood-vessels and lymph-channels. Though intimately combined, these tissues, absolutely distinct structurally and functionally, may be separately invaded by disease; and although it may not be practicable nor essential in every case to decide if we have to do with a parenchymatous or interstitial (peri-) neuritis, it is necessary to keep in mind how much the picture of disease may be modified according as one or the other of the constituents of the nerve are separately or predominantly involved. Thus, a different group of symptoms will be seen when the vascular peri- and endoneurium is the seat of inflammation from that which appears when the non-vascular nerve-fibres are themselves primarily attacked and succumb to the inflammatory process with simple degeneration of their tissue. Furthermore, it is not too speculative to consider that the different kinds of nerve-fibres may be liable separately or in different degrees to morbid conditions, so that when mixed nerves are the seat of neuritis, motor, sensitive, or trophic symptoms may have a different prominence in different cases in proportion as one or other kind of fibres is most affected.
ETIOLOGY.—Traumatic and mechanical injuries of nerves are the most common and best understood causes of neuritis. Not only may it be occasioned by wounds, blows, compression, and other insults to the nerves themselves, but jolting and concussion of the body, and even sudden and severe muscular exertion, have been recorded as giving rise to it. We readily understand how neuritis is caused by the nerves becoming involved in an inflammation extending to them from adjacent parts, although the nerves in many instances show a remarkable resistance to surrounding disease. Less easily understood but undoubted causes of neuritis are to be found in the influence of cold, especially when the body is subjected to it after violent exertion. Although the causal connection is unexplained, we find neuritis a frequent sequel of acute diseases, as typhoid fever, diphtheria, smallpox, etc. In the course of many chronic constitutional affections, as syphilis, gout, elephantiasis græcorum, we encounter neuritis so frequently as to make us look for its cause in these diseases. Finally, neuritis may develop apparently spontaneously in one or many nerves.
MORBID ANATOMY.—The macroscopic appearance of nerves affected by neuritis is very varied, according as the disease is more interstitial or parenchymatous, acute or chronic. Sometimes the nerve is swollen, red, [p. 1191] or livid, the blood-vessels distended, with here and there points of hemorrhage, the glistening white of the fibres being changed to a dull gray. Sometimes the nerves are reduced to gray shrunken cords. When the perineurium has been the principal seat of the inflammation we may have swellings at intervals along the course of the nerve (neuritis nodosa, perineuritis nodosa acuta) or, as in chronic neuritis, the trunk of the nerve may be hard and thickened from proliferation of the connective tissue, sclerosis of the nerve. The nerve does not always present the appearance of continuous inflammation, but the evidence of neuritis may be seen at points along its course which are separated by sound tissue. These points of predilection are usually exposed positions of the nerve or near joints. Often the nerve appears to the naked eye normal, and the characteristic changes of neuritis are only revealed by the microscope. The microscopical changes in neuritis may extend to all of the constituents of the nerve, and present the ordinary picture of acute inflammation, hyperæmia, exudation, accumulation of white corpuscles in the tissues, and even the formation of pus, the nerve-fibres exhibiting in various degrees the destruction of the white substance of Schwann and the axis-cylinder. Or, as in chronic neuritis, the alterations may consist in the more gradual proliferation of the peri- and endoneurium, which, contracting, renders the nerve dense and hard and destroys the nerve-fibres by compression. In acute as well as in chronic neuritis the perineurium may be exclusively affected, the fibres remaining normal (Curschman and Eisenlohr). The nerve-fibres themselves may be the primary and almost exclusive seat of the neuritis, exhibiting more or less complete destruction of all their constituent parts, except the sheath of Schwann, without hyperæmia and with little or no alteration of the interstitial tissue. Sometimes the fibres are affected at intervals, the degeneration occupying a segment between two of Ranvier's nodes, leaving the fibre above and below normal (nèvrite segmentaire peri-axile, Gombault). All of these lesions of the nerve-fibres may be recovered from by a process of regeneration, the fibres showing a remarkable tendency to recover their normal structure and function.
SYMPTOMS OF NEURITIS.—When a mixed nerve is the seat of an acute neuritis, with hyperæmia of its blood-vessels, it becomes swollen by inflammatory exudation, and can be felt as a hard cord amongst the surrounding tissues. It is not only highly sensitive to direct pressure, but muscular exertion, or even passive movement of the part, excites pain. Spontaneous pain is one of the most prominent symptoms, and is sometimes so severe and continuous as to destroy the self-control of the patient, and demand the employment of every agent we possess for benumbing sensibility and quieting the excited system. At first there may be hyperæsthesia of the skin in the region of the distribution of the nerve, but a much more constant and significant symptom is cutaneous anæsthesia, which generally makes its appearance early in the course of the disease. The degree and extent of the anæsthesia varies very much in different cases, but is seldom total, except over small areas, even when the inflammation has seriously damaged the nerve-fibres. This is explained by the sensibility supplied to the part by neighboring nerves, as already described in treating of traumatic nerve-injuries. Very characteristic of acute neuritis are various abnormal sensations (paræsthesiæ) which are [p. 1192] developed in a greater or less degree during the progress of the disease, and are described by the patients as numbness, tingling, pins and needles, burning, etc. In a case of acute neuritis of the ulnar nerve seen by the writer the patient was much annoyed by a persistent sensation of coldness in the little and ring fingers, which caused him to keep them heavily wrapped up even in the warm weather of summer. When motor symptoms make their appearance they begin with paresis of the muscles, which may increase rapidly to paralysis. As this is the result of destructive changes, more or less complete, in the motor nerve-fibres, we will have, as would be expected, accompanying the paralysis the symptoms already detailed in the consideration of nerve-injuries with destruction of continuity—namely, absence of muscular tone, loss of skin and tendon reflexes, increased mechanical excitability, atrophy of muscles, and the different forms of degenerative reaction, with loss of faradic contractility. When spasm or tremor has been observed in acute neuritis of mixed nerves, it is a matter of doubt whether it is not to be explained by reflex action of the cord excited by irritated centripetal fibres. Various trophic symptoms may show themselves, as herpes zoster or acute œdema. Erythematous streaks and patches are sometimes observed upon the skin along the course of the inflamed nerve-trunks. In chronic neuritis, into which acute neuritis generally subsides or which arises spontaneously, the symptoms above described are very much modified; indeed, cases occur which exist for a long time almost without symptoms. While the affected nerve may be hard and thickened by proliferation of its connective tissue, pain, spontaneous or elicited by pressure, is not of the aggravated character present in acute neuritis, and may be quite a subordinate symptom. It has more of a rheumatic character, is less distinctly localized, more paroxysmal, and has a greater tendency to radiate to other nerves. It is probable that many ill-defined, so-called rheumatic pains which are so frequently complained of are the result of obscure chronic neuritis. Anæsthesia and various paræsthesiæ are often more prominent symptoms than pain. Sometimes there is a hyperæsthesic condition of the skin, in which touching or stroking the affected part causes a peculiarly disagreeable nervous thrill, from which the patient shrinks, but which, however, is not described as pain.
The motor symptoms in chronic neuritis of mixed nerves often remain for a remarkably long time in abeyance or may be altogether wanting. They may appear as tremor, spasm, or contraction, these, however, being probably reflex phenomena. Most commonly there is paresis, which may deepen into paralysis with atrophy of muscles and degenerative reaction. The trophic changes dependent on chronic neuritis are frequently very prominent and important. The skin sometimes becomes rough and scaly, sometimes atrophied, smooth, and shining (glossy skin). Œdema of the subcutaneous cellular tissue is often seen, for example, on the dorsum of the hand, where it may be very marked. The hair of the affected part shows sometimes increased growth, sometimes it falls off. The nails may become thickened, ridged, and distorted. Deformity of joints with enlargement of the ends of the bones is not infrequently met with as the result of chronic neuritis. In short, we may meet with all of those trophic changes which have been described as arising from nerve-irritation, and which occur in chronic neuritis as the result of compression of [p. 1193] nerve-fibres by the contraction of the proliferated connective tissue in the nerve-trunk.
The symptom-complex varies greatly in neuritis, so that there is hardly a symptom which may not be greatly modified or even wanting in some cases—a fact, which, as we have already said, may be explained by the morbid process fixing itself exclusively or in different degrees upon one or other of the component parts of the nerve-trunk, or, it may be, upon fibres of different functional endowment. Thus pain, usually one of the most prominent symptoms of neuritis, may be quite subordinate, or even absent, in cases of neuritis acute in invasion and progress. In a case of neuritis of the ulnar nerve seen by the writer, beginning suddenly with numbness and paresis, and rapidly developing paralysis, atrophy of muscles, loss of faradic contractility, with degenerative reaction, there was no pain during the disease, which ended in recovery.7 On the other hand, in mixed nerves the sensitive fibres may be long affected, giving rise to pain and various paræsthesiæ before the motor fibres are implicated, or these last may escape altogether.
7 “Two Cases of Neuritis of the Ulnar Nerve,” Maryland Medical Journal, Sept., 1881.
The swollen condition of the nerve, so characteristic in many cases of neuritis where the perineurium is the seat of a hyperæmia, is wanting in cases where the stress of the attack is upon the nerve-fibres themselves. Again, the trophic changes induced in the tissues by a neuritis may predominate greatly over the sensitive or motor alterations. Thus, in the majority of cases in which herpes zoster occurs it is without pain or paræsthesia. Indeed, in chronic neuritis the symptoms show such variations in different cases that it is difficult to give a general picture of the disease sufficiently comprehensive and at the same time distinctive. The prognosis in acute neuritis is generally favorable, although it must depend in a great measure upon the persistence of the cause producing it. Thus, if it has been excited by the inflammation of neighboring organs it cannot be expected to disappear while these continue in their diseased condition. In other cases the symptoms may subside with comparative rapidity; and so great is the capacity of the nerve-fibres for regeneration that recovery may be complete and nothing remain to indicate the previous inflammation. The nerve, however, that has once suffered from neuritis shows for a long time a tendency to take on an inflammatory action from slight exciting causes. If there has resulted an atrophy of muscles, we must expect some time to elapse before they recover their functional activity and normal electric reaction.
Acute neuritis most frequently passes into the chronic form, and it may then drag on indefinitely, stubbornly resisting treatment and giving rise to permanent derangement of sensibility, loss of muscular power, or perverted nutrition. Neuritis shows a tendency to spread along the affected nerve centripetally, sometimes reaching the spinal cord, and, as it has appeared in some cases, even the brain, causing tetanus or epilepsy.
Reflex paralyses, which at one time were believed to be the not infrequent result of nerve-irritation and inflammation, affecting from a distance the functions of the spinal cord, have been shown to be the effect of an extension of the lesion of the inflamed nerve to the cord, causing organic disease. Instances of the extension of a neuritis to distant nerves, as those of an opposite extremity, without the implication of the spinal [p. 1194] cord (neuritis sympathica), are most probably cases of multiple neuritis, to be considered farther on.
The DIAGNOSIS of cases of traumatic neuritis can scarcely present a difficulty. Acute neuritis with spontaneous pain, swelling, and tenderness of the nerve, presents distinctive features hardly to be confounded with any other affection, although thrombosis of certain veins, as the saphenous, may present some of its symptoms. To distinguish chronic neuritis or the cases wanting those obvious symptoms just indicated (many cases of sciatica) from neuralgia is a more difficult task. The following distinctive points may be noted: In neuritis the persistent and continuous character of the pain helps us to distinguish it from the more paroxysmal exacerbations of neuralgia, and its tendency, often seen, to spread centripetally spontaneously or when pressure is made on the nerve, may be also considered as characteristic of neuritis. Cutaneous anæsthesia, paresis, and atrophy of muscles are distinctive in any case of a neuritis rather than a neuralgia. Herpes zoster and other trophic changes speak strongly for a neuritis.
In the TREATMENT of neuritis the first indication is to get rid, as far as possible, of such conditions as may cause or keep up the inflammation, as, for instance, the proper treatment of wounds, the removal of foreign bodies, the adjustment of fractures, the reduction of dislocations, the extirpation of tumors, etc. Absolute repose of the affected part in the position of greatest relaxation and rest is to be scrupulously enforced. In acute neuritis local abstraction of blood by leeches and cups in the beginning of the affection is of the greatest advantage and should be freely employed. The application of heat along the course of the inflamed nerve has appeared to us preferable to the use of ice, although this also may be employed with excellent effect. The agonizing pain must be relieved by narcotics, and the hypodermic injection of morphia is the most efficient mode of exhibition. Salicylic acid or salicylate of sodium in large doses contributes to control the pain. Iodide of potassium in large doses appears to act beneficially, even in cases with no syphilitic complications. In subacute or chronic neuritis local bloodletting is not as imperatively demanded as in the acute form, although it is sometimes useful. Here counter-irritation in its various forms and degrees, even to the actual cautery, is to be recommended. An excellent counter-irritation is produced by the application of the faradic current with the metallic brush. It appears from general experience that the counter-irritation has the best effect when applied at a little distance from the inflamed nerve, and not directly over its course. In the galvanic current we possess one of the very best means not only for relieving the symptoms of chronic neuritis, but for modifying the morbid processes in the nerve and bringing about a restoration to the healthy condition. Its application is best made by placing the anode or positive pole as near as possible to the seat of the disease, while the cathode or negative pole is fixed upon an indifferent spot at a convenient distance. The positive pole may be held stationary or slowly stroked along the nerve. Finally, in protracted cases nerve-stretching may be resorted to with great benefit. It probably owes its good effects to the breaking up of minute adhesions which have formed between the sheath of the nerve and the surrounding tissues, and which act as sources of irritation.
Cases of this important form of neuritis have been observed and recorded since 1864, but the resemblance of its symptoms to those of certain diseases of the central nervous system (poliomyelitis, Landry's paralysis, etc.) has prevented its general recognition, and it is only within the last few years that its distinctive pathological lesions have been demonstrated and its diagnosis made with considerable certainty. We can hardly overrate the importance of this in view of the great difference in gravity of prognosis between it and other diseases with which it may be confounded.
Multiple neuritis consists in a simultaneous or more or less rapidly succeeding inflammation of several or many usually bilaterally situated nerves, with a greatly preponderating, almost exclusive, lesion of the motor fibres. Commonly the disease attacks the lower extremities and progresses upward, although occasionally it has been seen to begin in the arms. It does not confine itself to the nerves of the extremities and trunk, but often involves the phrenics, causing paralysis of the diaphragm, and frequently invades one or more of the cranial nerves, notably the vagus, thus giving rise to the rapid heart-beat so often seen in the disease. In the cases of multiple neuritis observed the muscles of deglutition have never been paralyzed. The sphincter ani and bladder have likewise escaped. All degrees of acuteness are observed in the course it runs, from the cases terminating rapidly in death to those in which the disease extends over months, slowly involving nerve after nerve, until nearly all of the muscles of the body are paralyzed, when death may result or a more or less complete recovery take place. The invasion of the disease is in most cases sudden, even when its subsequent course is chronic, and is often marked by decided constitutional disturbance, as rigors, fever, delirium, albuminuria, etc. Disturbances of sensation are prominent among the initial symptoms, and are of great importance for the diagnosis of the disease. Severe, spontaneous, paroxysmal pain of a shooting, tearing character has ushered in most of the cases on record, remitting, however, during their progress. Pain is not always present, nevertheless, and cases not infrequently occur which run a painless course. In some cases which have come under the writer's notice spontaneous pain did not occur until some days after the disease was fully declared by other symptoms. More constantly present, and more characteristic of multiple neuritis, are the disturbances of sensation which show themselves in subjective feelings of numbness, tingling, pins and needles, coldness, burning, and other paræsthesiæ, which appear at its outset and continue to be present more or less during its course. Anæsthesia, not of a high degree nor at all coextensive with the paralysis of the muscles—sometimes, indeed, confined to very circumscribed areas—may be said to exist always in multiple neuritis—a fact of great diagnostic value. Hyperæsthesia of the skin is frequently seen. Hyperalgesia and analgesia are sometimes observed. Hyperæsthesia of the muscles is a very marked symptom in almost every case, and shows itself not only upon direct pressure being made, but also in the pain elicited by passive movements of the parts affected. Pressure upon nerve-trunks does not cause pain as [p. 1196] invariably as might have been expected from the location of the disease. Delayed sensation has been frequently observed.
Paresis of muscles, often commencing suddenly, is early seen in multiple neuritis, and increases until there is more or less complete paralysis, the most important feature of the disease. The paralyzed muscles present the flabby condition characteristic of muscles deprived of the tonic influence of the spinal cord. Atrophy, which is not commensurate, however, with the paralysis, soon begins, and may go on to an extreme degree. As the paralysis develops the tendon reflexes are lost, and there may be diminution or loss of the skin reflexes also. The paralyzed muscles lose their faradic contractility, and exhibit diminution of electric excitability to the galvanic current, and, finally, the various forms of degenerative reaction. It is remarkable that neither the impairment of sensation nor the paralysis is, as a rule, strictly confined to the areas of distribution of particular nerves, but is diffused over regions of the body. Thus in the limbs the motor and sensory symptoms are most marked at their extremities, gradually diminishing toward the trunk. In some cases multiple neuritis appears to have occasioned the inco-ordinate movements of locomotor ataxy. In the progress of the disease a rigidity and contracted condition of muscles may be developed, occasioning a fixed flexion of some of the joints. Profuse sweating, œdema of the hands and feet, trophic changes in the skin, mark at times the implication of trophic and vaso-motor nerves. Bed-sores do not occur.
The pathological changes in pure cases of multiple neuritis are found in the nerve-trunks, mainly toward their peripheral terminations, and in their muscular branches, the evidences of disease diminishing toward the larger trunks, the nerve-roots being unaffected and the spinal cord showing no lesions. Sometimes the affected nerves present, even to the naked eye, unmistakable proof of acute inflammation. They are reddened by hyperæmia, swollen by exudation, and small extravasations of blood may be seen among their fibres. The microscope shows congestion of the blood-vessels, exudation of the white corpuscles, even to the formation of pus, alteration of the endo- and perineurium; in short, all the evidence of an interstitial inflammation, the nerve-fibres being comparatively little altered, and suffering, as it were, at second hand. In most of the cases, however, the nerves macroscopically present little or nothing giving indication of disease. The microscopic changes, however, are extensive, and pertain almost exclusively to the nerve-fibres themselves. These are altered and degenerated, giving an appearance almost precisely the same as already described in treating of the changes occurring in nerves separated by injury from the centres—Wallerian degeneration.8 There is no hyperæmia, thickening, or change in the endoneurium. So great are these differences in the microscopic appearance of the nerves in different cases of multiple neuritis that objection has been raised to classing the two varieties together, and it has been argued that we cannot with right designate the cases in which hyperæmia and other evidence of [p. 1197] a general inflammation are absent as neuritis. It has been, however, argued—apparently, to the writer, with better reason—that the same morbid influence which at one time affects the blood-vessels, causing their congestion and the passage through their walls of the white corpuscles and the exudation of inflammation, may at another time, by a direct and isolated influence upon the nerve-fibres, cause their degeneration; in other words, that there may be a parenchymatous neuritis, which shall affect only the nerve-fibres. The vastly disproportionate implication of the motor fibres would point to the fact of a selective infection in multiple neuritis of certain fibres, as there is a selective infection in poliomyelitis of the motor cells of the anterior horns of the spinal gray matter.
8 Gombault's observations (Arch. de Névrologie, 1880) would seem to show that there is a difference in the lesion of the fibres in neuritis from that in simple Wallerian degeneration, inasmuch as that in the former the first alteration is seen about the nodes of Ranvier, and occurs at points separated from each other by healthy fibre, and also in the more tardy destruction of the axis-cylinder.
ETIOLOGY.—Much in the symptomatology of multiple neuritis, especially of its invasion, strongly urges us to the conclusion that it is a constitutional disease caused by an unknown morbid influence, the stress of which falls upon the nervous system. This view receives strong support from the history of the Japanese kak-ke or Indian beriberi, a disease at times epidemic in those countries, and which has the undoubted symptoms and the characteristic pathological alterations of multiple neuritis. After many acute infectious diseases neuritis of individual nerves is not uncommon, but the distinctive characteristics of multiple neuritis have, so far, been observed almost exclusively after diphtheria, to which it is not infrequently a sequel. It has been observed as the result at least occurring in intimate connection with polyarthritis, and the frequency with which it has occurred in the phthisical is remarkable. There have been not a few cases of multiple neuritis recorded as having been produced by chronic alcohol-poisoning. A well-marked case has come under the writer's observation in which the immediate cause was acute poisoning by arsenious acid, a very large amount having been taken at one dose by mistake. The poison of syphilis has been regarded as standing in a causal relation to multiple neuritis. For the rest, the exciting causes (probably acting in connection with a peculiar condition of the system) have appeared to be exposure to cold, great muscular exertion, direct mechanical injury to the nerves, as the rough jolting of a wagon, or the inflammation of a nerve which has in some unknown way extended to others.
The DIAGNOSIS of multiple neuritis in certain cases presents great difficulty, from the close resemblance of its symptoms to those of poliomyelitis. The prominent symptoms in the muscular system—viz. paralysis, atrophy, the degenerative reaction—are the same in both. It may be remarked, however, that in multiple neuritis the paralysis is more generally diffused over the muscles of the affected limbs, while in poliomyelitis it is more confined to the areas of distribution of particular nerve-branches. Pain is common to the beginning of both diseases, but it generally passes off more quickly and completely in poliomyelitis. The persistent hyperæsthesia of the muscles is wanting in poliomyelitis. But it is in the diminution and alteration of sensation that we have the surest means of distinguishing between the two affections. This symptom seldom or never fails to show itself in multiple neuritis, although its area may be circumscribed and it may be slight in degree, while it certainly makes no part of the symptomatology [p. 1198] of poliomyelitis. It has been asserted that the implication of the cranial nerves so often seen in multiple neuritis never occurs in poliomyelitis. When we consider the intimate connection of the anterior horns of the spinal gray matter with the motor nerve-fibres, it appears highly probable that the same morbid influence may invade both simultaneously or in quick succession, thus producing a complex of symptoms rendering a diagnosis very difficult, and probably giving rise to some confusion in the recorded symptoms of multiple neuritis. From Landry's paralysis multiple neuritis is to be distinguished by the impairment of sensibility, the loss of faradic contractility, and absence of the tendon reflex; from progressive muscular atrophy, by the loss of sensibility and the much more obvious degenerative reaction.
The PROGNOSIS of multiple neuritis is in the great majority of cases not grave, so far as life is concerned, even when there is extensive paralysis. Death may occur early in the acute form of the disease or it may take place at the end of chronic cases. When the disease proves fatal, it is from paralysis of the diaphragm and the other muscles of respiration. Where the paralysis and atrophy have been great, showing profound alteration of the nerves, a long time is required for recovery, and more or less paralysis, contracture, or defective sensibility may permanently remain.
The TREATMENT consists, at the outset, in rest and position, the local abstraction of blood (in cases where the nerve-trunk is swollen and tender), and the administration of such drugs as we suppose act favorably upon the inflammation of the nerves. Salicylic acid or salicylate of sodium seem to act beneficially in relieving the severe pains in the outset of the disease. Iodide of potassium, gradually increased until large doses are taken, has, in the experience of the writer, seemed to beneficially modify the course of multiple neuritis. The necessary relief of pain is best obtained by hypodermic injections of morphia, supplemented by heat applied to the affected nerves. To these means may be added rubbing with chloroform and applying to the painful parts cloths dipped in a 5 per cent. solution of carbolic acid. After the acute stage has been passed and in chronic cases, just as soon as we have reason to suppose that the degenerative process in the nerves has come to a standstill, we possess in the use of electricity the means of hastening the regeneration of the nerve-fibres, strengthening the paralyzed muscles, and restoring the sensation. The galvanic current is to be preferred, and it is to be applied to the crippled nerves and muscles—sometimes stable for its electrolytic action, sometimes interrupted to obtain its exciting and stimulating effect. The excitement to nerves and muscles by the use of the faradic current has also its uses in hastening recovery. Protracted treatment and much patience are required to overcome contractions and restore the nerves and muscles, and the effects of the disease may be seen for a long time in the weakness and diminished electric reaction of the muscles.
A prominent and important symptom of the lesion of peripheral nerves is the diminution and loss of cutaneous sensibility. Besides the [p. 1199] anæsthesia caused by the affections of the fibres themselves, which has been touched upon in the preceding pages, it may be produced by morbid states of the peripheral end-organs or cutaneous terminations of the nerves. Cold applied to a nerve-trunk may produce alterations which for days after cause numbness and paræsthesia in the surface to which it is distributed, and the application of cold to the surface of the body, as we know from common observation, causes blunting of the cutaneous sensations, especially that of touch. In this way, from exposure to the atmosphere at low temperatures, to cold winds, or by the immersion of the body in cold water, the end-organs of the nerves in the skin are morbidly affected, and anæsthesia results, the so-called rheumatic anæsthesia. Many substances, as acids, notably carbolic acid, alkalies, narcotics, etc., act upon the cutaneous end-organs in a way to destroy their capacity for receiving or transmitting impressions and produce a more or less persistent anæsthesia of the skin. In the anæsthesia so often observed in the hands and forearms of washerwomen we have an example of the action probably of several of these causes, as the frequent plunging of the hands into cold water and the action upon the skin of alkalies and alkaline soaps. The diminution or interruption of the circulation through the skin, as in ischæmia from spasm of the minute arteries due to an affection of the vaso-motor nerves, is also a cause of cutaneous anæsthesia. In lepra anæsthetica (Spedalskhed) the cutaneous anæsthesia is dependent upon a neuritis of the minute branches in the skin. The local anæsthesia met with so often in syphilis, though its pathology is doubtful, is not improbably sometimes caused by an affection of the peripheral nerves (neuritis?) and their end-organs. After many acute diseases, diphtheria, typhoid fever, etc., we have cutaneous anæsthesia in connection with muscular paralysis, the cause of both being a neuritis. The patient is made aware of the loss of sensation by some interference with his usual sensations and movements. If he puts a glass to his lips, the sensation is as if a bit were broken out of the rim; his accustomed manipulations are awkward, because of the want of distinct appreciation of the objects he holds; he fumbles in buttoning his clothes or he stumbles unless looking to his steps. An examination, nevertheless, almost always reveals that the anæsthesia is greater than would have been supposed from the subjective feelings of the patient; indeed, cases occur in which he is not aware of an existing defect of sensation. But a careful examination is not only required to determine the extent, but by it alone can we arrive at a knowledge of the quality of the anæsthesia—viz. whether there is a loss of all of the different kinds of sensation, whether they are affected in an unequal degree, or whether some have entirely escaped. Thus we must test for the acuteness of the simple sense of touch by comparing the sensations elicited by the contact of small surfaces of unequal size, as the point and head of a pin or pencil, observing the appreciation by touch of the patient for different substances, as woollen, silk, linen, cloth, or comparing the sensation of the anæsthesic part with the same part on the opposite healthy side of the body. The sense of locality and space may be examined by placing at the same instant upon the skin of the patient, his eyes being closed, two points (the anæsthesiometer or the points of a compass), and observing his capacity for appreciating the impression as double. As there is an enormous difference of acuteness of the [p. 1200] space-sense in the skin of different parts of the body (see textbooks of physiology)—ranging from the tip of the tongue, where the touch of two points separated 1.2 mm. gives a double sensation, to the thigh, where the points must be separated 77 mm. to be felt as two—we must be careful to consider in making the examination the normal space-perception of the region. Care must be taken not to repeat the test too often, as a rapid education of the surface to a more delicate appreciation of the impressions is the result. In certain abnormal conditions from spinal disease we have a condition of polyæsthesia in which the impression of one point is felt as two or more. The sense by which we appreciate the pressure of objects must be tested by placing upon the surface to be examined, in succession, objects of different weight, care being taken to have the area which touches the skin and the temperature the same in each. The parts to be tested must be firmly supported, and all muscular contraction on the part of the patient prevented. The temperature sense is examined by the application of hot and cold water or bodies of different temperature. We sometimes meet with a perversion of this sense in which the application of a cold surface to the skin gives the sensation of warmth, and the contrary. In testing the sense of temperature and the sense of pressure it is not the absolute capacity of appreciating on the part of the patient that we investigate, but the power of discriminating between different degrees of temperature or pressure. The sense of pain must likewise be tested, since morbid conditions occur in which it may be caused more readily than is normal by exciting the cutaneous nerves, and that, too, in parts which have in a great measure or quite lost the sense of touch; or, on the other hand, touch may be retained, while irritation of the skin can excite no feeling of pain (analgesia). We have in the faradic current an excellent means of testing the cutaneous sensibility, inasmuch as it excites the skin over the various parts of the body about equally, and it can be employed in very gradually increasing or decreasing strength. Its effects on the affected part must be compared with those produced on the healthy surface of other parts of the patient's body or on healthy individuals.
Frequently accompanying cutaneous anæsthesia, but constituting no part of it, are various paræsthesiæ, as formication, pins and needles, burning, etc. Pain, sometimes of great intensity, is not infrequently connected with it (anæsthesia dolorosa). The paræsthesiæ and pain are the result of irritation in some portion of the conducting tracts, and, together with the trophic changes so often seen in connection with nerve-injuries, they have been already considered under that head.
It is a very important point to make the diagnosis between central and peripheral anæsthesia, but it is often a matter of great difficulty, and sometimes not to be made at all. The history of the case must be carefully considered, and an examination made for symptoms of brain or spinal disease, the existence of nerve lesions, or if there is a history of toxic influences, etc. In peripheral anæsthesia the reflexes which may be normally excited from the affected surface are wanting, in contradistinction to anæsthesia of central origin, in which they are most generally retained or even increased. Concomitant trophic changes speak strongly for a peripheral origin, as do also paralysis and atrophy of muscles. [p. 1201] Loss of some of the forms of sensation, with retention of others—i.e. partial paralysis of sensation—indicate a central origin.
The TREATMENT of peripheral anæsthesia must look, in the first place, to removal, if possible, of its cause, and the treatment of diseased conditions, if any exist, of the nerve-trunks, as neuritis, mechanical injuries, etc. Local applications of a stimulating character may be advantageously used upon the anæsthesic parts. By far the most effective stimulant to the diseased nerves is the faradic or galvanic current, and it should be used in the way that will produce the greatest amount of excitation in the cutaneous end-organs. This is best done by applying the faradic current to the dry skin with the metallic brush, or by allowing the cathode of the galvanic current to rest upon it for some time.
The PROGNOSIS in peripheral anæsthesia is in the main favorable, but it must, of course, depend much on the gravity of the lesion causing it, as mechanical injury, pressure, neuritis, cold, etc. Rheumatic anæsthesia, the result of exposure to cold, is in general readily recovered from. Vaso-motor anæsthesia yields in most cases without difficulty to treatment. Washerwoman's anæsthesia and allied cases are intractable, and often resist the patient and well-conducted application of remedies.
As a concrete picture of peripheral anæsthesia we will give a description of anæsthesia of the fifth nerve—the rather that in its consideration we meet with some of the most interesting and important complications occurring in connection with paralysis of sensitive nerves. The fifth nerve may have either of its three branches separately affected, giving rise to anæsthesia limited to the distribution of that branch, or all of its fibres may be simultaneously involved, giving rise to complete anæsthesia of the nerve. In the latter case the lesion of the nerve in all likelihood exists at some point of its course between the apparent origin from the pons and the ganglion of Gasser, which rests upon the apex of the petrous portion of the temporal bone. Beyond this point the nerve divides into its three branches. Amongst the causes of trigeminal anæsthesia are injuries, tumors, syphilitic thickening of the dura mater, neuritis, etc., affecting the nerve within the cranial cavity. In complete anæsthesia of the fifth nerve the parts implicated are the skin of the forehead to the vertex, the nose, the lips, and chin up to the median line, the cheek and temporal region, including the anterior portion of the ear, the conjunctiva, the mucous membrane of the nose, the mucous membrane of the mouth, and partly of the fauces of the same side. The tongue is deprived not only of common sensation on the affected side in its anterior two-thirds, but the sense of taste is also lost over the same region, by reason that the fibres of the chorda tympani, the nerve of taste for this region of the tongue, are derived from the fifth nerve. If the whole thickness of the nerve-trunk is involved, including the small motor root, there is, in connection with the anæsthesia, paralysis of the muscles of mastication on the side affected, which may be distinguished by the want of hardening of the masseter when the jaws are forcibly brought together, and by the thrusting of the chin over to the paralyzed side when the mouth is widely opened, caused by the want of action of the external pterygoid muscle, which allows the condyle on the paralyzed side to remain in the glenoid fossa, while the condyle of the opposite side is pulled forward upon the articular eminence by the sound [p. 1202] pterygoid. The face is of a dusky or livid color, and cooler than natural. Ulcers of a stubborn character in the mucous membrane of the cheek may be caused by the patient unconsciously biting the insensitive parts. An inflammation of the conjunctiva is frequently set up, which may extend to the cornea, causing ulceration, perforation, panophthalmitis, and destruction of the eye (ophthalmia neuro-paralytica). This has been regarded by some as caused by trophic changes in the tissues, the direct result of irritation or destruction of trophic fibres connected with the ganglion of Gasser. Experiments made upon animals, however, seem to show that the inflammation of the eye depends upon the irritation caused by the intrusion of foreign bodies, which, owing to the loss of sensation, are not appreciated, and which from loss of reflex action are not removed by winking nor washed away by an increased lachrymal secretion, as in the healthy eye. It may be that although the latter is the true explanation of the origin of the inflammation, nevertheless the tissues may have lost their normal power of resistance to its invasion by reason of nutritive changes consequent upon the lesion of trophic fibres running in the trunk of the nerve. The reflexes ordinarily induced by irritation of the parts in their normal state are lost. Irritation of the conjunctiva causes no winking of the lids nor secretion of tears, and titillation of the nostrils no movements of the muscles of the face nor mucous or lachrymal secretion. The movements of the face are less lively on the affected side, not on account of paralysis of the muscles, but from the loss of that constant play of reflex activity in them which takes place in the normal condition. The loss of the reflexes distinguishes peripheral trigeminal anæsthesia from that of cerebral origin, in which they may still be excited by irritating the anæsthesic surfaces. In trigeminal anæsthesia, which sometimes occurs from the effect of cold upon the surface of the face, the mucous surfaces are not affected.
The SYMPTOMS and DIAGNOSIS of peripheral paralysis having been already given under the heads of Injuries of Nerves and Neuritis, a consideration of the distribution of any motor nerve will enable us to anticipate the distinguishing features of the paralysis dependent upon it. With each the picture will be modified according to the position of the muscles paralyzed and the motor functions destroyed. It now remains to give the symptoms, diagnosis, and treatment of the paralysis of an individual motor nerve, which may serve as an example and paradigm, in the consideration of which points of interest and instruction may be touched upon applicable to all other cases.
Of all the peripheral paralyses, probably that of the seventh is the one we are most frequently called upon to treat and the symptoms of which are the most complex and interesting. The frequency of its paralysis is due to the length and peculiarity of its course, enclosed as it is in a bony canal which permits no increase of its volume without compression, the run of its terminal branches through parts liable to inflammation and disease (parotid gland), and their final distribution to parts exposed to all vicissitudes of heat and cold and in constant danger of mechanical injury. [p. 1203] The complexity and interest of the symptoms of its paralysis depend in a great measure upon the intimate connections it forms at different points of its course with the fibres of other nerves of entirely different functions (acoustic and fifth).
The seventh nerve is liable not only to intercranial compression from tumors, inflammation of the meninges, syphilitic processes, etc., but its long course through the petrous portion of the temporal bone renders it liable to injury from fracture or caries, and its close proximity to the middle ear causes it often to suffer from the diseased conditions of the bony walls or mucous lining membrane of that chamber, its paralysis being not infrequently the result of simple aural catarrh. After the exit of the nerve from the stylo-mastoid foramen it is imbedded in the parotid gland, and sometimes suffers from compression produced by an inflammation or abscess in that organ or by enlarged lymphatic glands in the neighborhood. Surgical operations, so often demanded for disease of the bones or soft parts of the face, may necessitate the lesion of its trunk or branches. The exposed position of this nerve is sometimes the occasion of its injury at the very outset of the life of the individual, when the application of the forceps to the head has been resorted to in delivery. But the most frequent cause of facial paralysis appears to be the exposure of one side of the face directly to cold—as sleeping in a draught of air, sitting at the open window of a railroad coach, etc. Here the causal connection appears evident from the rapidity with which the paralysis usually follows, although cases occur in which an interval of hours or days elapses after the exposure before the paralysis declares itself. Although this is usually designated rheumatic paralysis, there is nothing to connect it with that disease, nor are rheumatics more liable to it than others. Under such circumstances the paralysis is probably brought about by the occurrence of a neuritis of the nerve-trunk, which is compressed by the hyperæmia, and it may be by an inflammatory exudation against the bony walls surrounding it, until not only does it lose the power of conduction, but its fibres undergo the degenerative process. In some cases the neuritis thus excited by exposure to cold attacks the nerve after it has issued from the bony canal, and then the resulting injury to the fibres is much less grave. Although in some cases there are prodromal symptoms, as stiffness or pain in the face, generally the paralysis occurs suddenly, very often being first observed upon awaking. The patient may be first made aware of the paralysis by an inability to drink without the fluid dribbling from the affected side of the mouth or by the overflow of tears from the eye of the same side. When the paralysis is recent and the face in complete repose, there may be little or no deformity to mark the condition of the muscles. When, however, the patient speaks or the slightest emotional or reflex movements of the face are excited, as laughing, frowning, etc., it becomes obvious from the bizarre grimace caused by a one-sided contraction. After the paralysis has existed for some time the contrast of the two sides of the face is marked. The paralyzed side is characterized by a vacancy of expression to which the staring, unwinking eye contributes. From loss of the tonicity of the muscles the angle of the mouth droops, and the expressive furrows and lines about the brow, below the eye, and beside the nose are smoothed out and obliterated. Speech is affected, inasmuch as the paralysis of the [p. 1204] lip interferes with the pronunciation of the labials, and all attempts to purse up the mouth, as in whistling, is abortive. The eye not only remains open, the lids motionless, but there is partial eversion of the lower lid (lagophthalmos), and the tears, no longer directed to the punctum (paralysis of Horner's muscle), flow over the cheek. The natural impulse to reflex winking caused by evaporation from the conjunctiva or by the contact of particles of dust is answered by a rolling of the eyeball upward to wipe the cornea beneath the momentarily relaxed and drooping upper lid. Excited respiration causes no movement of the ala of the nose on the affected side, but in deep inspiration, in contrast to the normal elevation of the ala, it is flattened down by the suction of the inrushing current of air. In masticating, the cheek bulges out from want of power in the paralyzed buccinator to press the food inward against the opposing movements of the tongue. In persons who have the rather unusual power of voluntarily moving the ear we may detect the paralysis of the muscles concerned in those movements—a useful point in diagnosis. Moreover, on the sound side of the face the features have not entirely the natural appearance. The angle of the mouth is drawn upward and the naso-labial line more deeply impressed than natural. This results not from excessive contraction, but from the muscles remaining in the position they have taken during contraction, the antagonistic tonic traction from the opposite side, which would have restored them to their normal position, being wanting. This may be in a measure remedied by mechanical appliances which will keep up an elastic pull from the paralyzed side, or by restoring the muscles after contraction to position with the hand. The tongue rests symmetrically in the floor of the mouth, and is thrust out straight, although in appearance it is pushed toward the side paralyzed—a deceptive appearance produced by the asymmetrical position of the mouth. In some cases there is partial paralysis of the velum palati, the half arch on the affected side hanging lowest, and if we cause the patient to make the sound of ah the opposite side of the palate is alone drawn upward. The uvula may also participate in the paralysis, but the explanation of its position, sometimes directed away from, sometimes toward, the side of the paralysis, cannot be given. In proportion to the amount of the paralysis of the soft palate will be the prominence of the symptoms caused by it, such as difficulty in deglutition, a nasal tone in speaking, and the escape of fluids through the nostril in swallowing. The sense of hearing is often affected coincidently with facial paralysis. Thus by reason of their close juxtaposition the same cause may in common affect the acoustic and the facial, causing imperfect hearing, subjective noises, etc. The hearing is frequently affected by diseased conditions of the middle ear, which also cause a facial paralysis. Still another defect of hearing, however, is caused by the paralysis of the facial nerve itself. The stapedius muscle, supplied by a branch of the facial, is the antagonist of the tensor tympani, and when it is paralyzed the over-tense tympanic membrane vibrates more readily to sound-waves, and a condition of uncomfortably exaggerated sensitiveness to sounds is the result (hyperacuisis). The rarely-occurring symptom of dryness of the mouth on the side of the paralysis receives its explanation in the well-known fact of the presence of secretory fibres for the salivary gland in the chorda tympani, which are derived from the facial. We observe sometimes, in connection with facial paralysis, that the patient [p. 1205] complains of certain subjective sensations of taste, as sour or metallic, and an examination will in some cases reveal that the sense of taste is lost on the anterior two-thirds of the tongue on the side of the paralysis. The fibres which convey the sense of taste pass centripetally from the tongue in the chorda tympani nerve, join the facial just within the stylo-mastoid foramen, and continue united with it to the geniculate ganglion of the facial, at which point they leave it to pass in the great superficial petrosal to the spheno-palatine ganglion, and thence to the trunk of the fifth nerve. Loss of sensation over the face only occurs in cases where the fifth nerve has been simultaneously affected with the facial, which may occur from exposure to cold.
It is obviously of importance in cases of facial paralysis to determine if they are of central or peripheral origin. The most prominent symptoms which mark a peripheral paralysis are the implication of all the branches of the nerve, the loss of the reflexes, the development of the degenerative reaction, and atrophy of the muscles. In facial paralysis of cerebral origin the frontal and orbital branches are not at all or but slightly affected, leaving the eye with its natural appearance, in contrast to the lagophthalmos, and the open eye which does not close even in sleep. In cerebral paralysis the reflexes are normal and the muscles retain their natural electric reaction. Accompanying brain symptoms assure the diagnosis. In facial paralysis of bulbar origin the electric reactions are diminished, and we have a complex of symptoms made up in a great measure by the implication of neighboring nerves. After the diagnosis of a peripheral facial paralysis has been made, by a careful consideration of the symptoms we may with more or less accuracy determine at which point of the nerve the lesion is situated. If there is paralysis of all the muscles of the face, without alteration of taste or hearing, the electric reaction of nerve and muscles normal, the nerve is affected outside of the stylo-mastoid foramen. This is usually the form of slight rheumatic paralysis. If we discover that the muscles of the external ear are paralyzed, it shows that the point of lesion is just within the stylo-mastoid foramen, where the posterior auricular branch is given off from the facial. If with paralysis of the face there is alteration of the sense of taste, with dryness of the mouth, without interference with hearing, the trunk of the nerve is affected within the Fallopian canal, involving the chorda tympani fibres below the point where the stapedius nerve is given off. If to the above symptoms there is added over-sensitiveness to sounds, hyperacuisis, and there is no paralysis of the palate, we have the nerve affected still higher up, but below the geniculate ganglion. If the geniculate ganglion is involved, there is, in addition to the foregoing, symptoms of paralysis of the palate. If, now, the lesion is above the geniculate ganglion, we will have eliminated the symptom due to implication of the chorda tympani, which leaves the trunk of the facial at the geniculate ganglion, and the sense of taste is unaffected, while there remains paralysis of the face, dryness of the mouth (the secretory fibres run in the trunk of the seventh), hyperacuisis, and paralysis of the palate.
It was in facial paralysis that the first observations upon the degenerative reaction in muscles were made, and it is in that affection that these electric phenomena have been best studied, and give us the clearest [p. 1206] indications for prognosis and treatment in peripheral paralysis generally. In rheumatic facial paralysis, the most common form of peripheral facial paralysis, the electric reactions of the paralyzed muscles enable us to classify the cases into three groups, the prognosis and duration of which vary very much. In the first group are the slight forms of facial paralysis. Here the faradic or galvanic current, applied to nerve or muscles, causes an ordinary contraction; the electric reactions are normal. These cases scarcely require treatment, and recover in two or three weeks. In a second group are those cases in which within a short time after the invasion of the paralysis (two weeks) complete degenerative reaction is observed. This degenerative reaction, with the accompanying anatomical changes in nerve and muscle, has already been treated of in this article, and it is sufficient here to say that it is marked by total loss of electric excitability, both faradic and galvanic, in the nerve, loss of faradic and increased galvanic excitability in the paralyzed muscles, with a reversal of the normal reply of the muscles to the different poles of the galvanic battery. These cases constitute the severe form of rheumatic facial paralysis, and the prognosis is grave, recovery takes place only after months, and even after the lapse of years traces of the disease remain in the imperfect action of the muscles. A third group of cases are of a gravity intermediate between these two. In them is present the milder form of degenerative reaction; that is, there is a diminution, but not a total loss, of electric excitability in the nerve for both the galvanic and faradic currents; but in the muscles there is a marked increase of galvanic excitability, with qualitative change—i.e. greater contraction upon application to them of the positive than of the negative pole. These cases may be expected to recover in from four to eight weeks, the muscles still exhibiting the degenerative reaction after voluntary motion has returned. Among the symptoms to be particularly noticed in the progress of the severe forms of facial paralysis are spasmodic twitchings or spasms of the muscles on the affected side of the face, about the angle of the mouth, and around the eye, occurring spontaneously or when voluntary movements are made. Also a state of tonic contraction and rigidity may develop in some of the muscles, causing a permanent elevation of the angle of the mouth, a narrowing of the opening of the eye, or a rigidity of the cheek. These symptoms have been erroneously attributed to the use of electricity in the treatment, but they occur as frequently in cases in which it has not been employed. Traumatic facial paralysis, as from wounds, surgical operations, use of the forceps in delivery, or paralysis from compression of the nerve, as from tumors, syphilitic thickening of the dura mater, etc., do not require a detailed mention here, as such cases come under the head of nerve-injuries, already discussed. Paralysis of both facials (diplegia facialis), in so far as it is caused by peripheral nerve lesion, is an accidental occurrence, and need not be considered as a separate form of facial paralysis. It is often the result of central disease.
The TREATMENT of peripheral facial paralysis must begin with the effort to remove its cause. If syphilis is suspected, mercury and iodide of potassium must be freely used. If the cause is an affection of the middle ear, this must be treated. Wounds or traumatic injuries must receive the necessary surgical attention. In addition, in such cases electricity [p. 1207] must be employed in the manner presently to be described. In cases of rheumatic facial paralysis the treatment will vary with their gravity. In the lighter form in which the nerve is affected outside of the Fallopian canal, recovery takes place in a comparatively short time, even without treatment, but is hastened by the use of the faradic or galvanic current daily along the branches of the nerve. In the severe form we must open the treatment by an attempt to combat the condition of inflammation—of inflammatory exudation—which we suppose exists within the Fallopian canal. Local blood-letting by leeching upon the mastoid process may be appropriately used in the very first outset of the paralysis. Iodide of potassium, given persistently in large doses during the earlier period of the disease, appears to act beneficially independently of any syphilitic taint. Electricity is the remedy, however, on which most reliance is to be placed in the treatment of rheumatic facial paralysis, and the manner of its application may be taken as a model of how it should be employed in all cases of peripheral paralysis. The galvanic current, on account of its power of penetrating to the deeper parts and its catalytic action, is to be preferred for the direct electrical treatment of the nerve which should be instituted in recent cases. Its action is best obtained by placing the positive pole behind the ear on the affected side, the cathode behind the opposite ear, and passing a moderate current across the base of the skull (the affected nerve being thus in the course of the current) for one or two minutes. Occasionally the position of the poles may be reversed. Besides this direct application of galvanism to the point of lesion, it is necessary to make a peripheral application of electricity to the branches of the nerve and to the paralyzed muscles. For this we use both the faradic and galvanic currents. The galvanic current is used by applying the positive pole stationary behind the ear, while the negative pole, with an electrode of suitable size, is stroked over each branch of the nerve and applied to each muscle, a current being used sufficiently strong to produce decided contractions. This peripheral application should be made once daily, the time of application being from two to five minutes. The application of the faradic current is made by simply placing one electrode upon an indifferent spot, and moving the other over the face, with a current strong enough to cause contractions if the muscles still respond to it, or if they do not of such strength as the patient can bear without discomfort. Without doubt, one of the beneficial effects of peripheral electrization is the reflex excitement of the facial above the point of lesion through the irritation of the terminations of the fifth nerve in the skin. A certain advantage derived from it is that it maintains the tone of the paralyzed muscles, which in the case of the orbicularis palpebrarum is of great importance in preventing the eversion of the lower lid and the overflow of the tears. As it is impossible during the first days succeeding the paralysis to distinguish severe cases from those of the middle form, it is best to begin the treatment of all cases in the manner above described. The use of strychnia in rheumatic facial paralysis, both internally and by hypodermic injection, may be mentioned on account of the widespread preposession in its favor, and to point out distinctly its utter futility.
Mechanical appliances and manipulation are used with advantage in the treatment of facial paralysis to prevent the paralyzed muscles about [p. 1208] the mouth and cheek from being drawn out of place and over-stretched by the action of the sound ones of the opposite side, thus having their tonicity and nutrition impaired.
Contractions and rigidity of muscles receive little benefit from the use of electricity, and must be treated by mechanical procedures, such as stretching, massage, etc.
The term neuromata was applied to all tumors involving the nerve-trunks at a time when their histological differences had not been studied and they were all supposed to be composed of nerve-tissue; and even yet the name is conveniently retained, because, although differing widely histologically, tumors situated upon the nerves have a very similar clinical history.
Neuromas must be divided into true and false, the true consisting of nerve-tissue, the false, or pseudo-neuromas, being composed of many varieties, having this only in common, that they are seated upon the nerves.
The true neuromas are again subdivided into those in which the nerve-tissue composing them resembles exactly the fibres of the peripheral nerves, showing with the microscope the double-contoured white substance of Schwann surrounding an axis-cylinder, and those in which the tumor is made up of fibres which Virchow has shown to be non-medullated nerve-fibres—i.e. the axis-cylinder without the white substance of Schwann. These two forms have been distinguished by the names myelinic and non-myelinic. The true neuromas are non-malignant, although showing the tendency to recur after extirpation, are of slow growth, and as a rule do not increase to a very great size. The best type of the myelinic neuromas is found in the spherical or spindle-shaped enlargements at the cut ends of nerves, particularly in the stumps of amputated limbs, where they are found oftenest intimately connected with the cicatricial tissue, though sometimes lying free. They consist of true medullated fibres mixed with some fibrous tissue. The fibres composing them are derived partly from splitting up and proliferation of the fibres of the nerve itself, partly are of new formation, the appearances strongly recalling the process of regeneration in nerves. Myelinic neuromas consist of fibres and nuclei so closely resembling in microscopic appearance the fibromas that they have hitherto been confounded with them; and there is a difference among the highest authorities as to the certainty of their diagnosis, and, in consequence, of the frequency of their occurrence. The true neuromas may include in their structure all of the fibres of the nerve-trunk or only a portion of them (partial neuroma)—a fact of importance in their symptomatology. Of the false neuromas, the fibromas are by far the most frequently met with. They appear as knots, more or less hard, upon the course of the nerve-trunk, which they may involve completely or partially. They are often excessively painful to the touch or spontaneously, most of the so-called tubercula dolorosa belonging to the fibro-neuromas. Fibromas sometimes occur along the trunk and branches of a nerve, forming a plexus of knotted cords (plexiform neuroma). Fibro-sarcomas are not an infrequent form of neuroma.
[p. 1209]Myxomas often occur upon the peripheral nerves, and are frequently multiple, their points of predilection being the larger trunks, as the sciatic, ulnar, etc. They show their characteristic soft structure, and are usually spindle-shape, assuming a rounder form as they attain a large size. The various forms of sarcoma occasionally form tumors upon the nerves, attacking generally the large trunks. Carcinomatous tumors beginning upon the nerves sometimes occur, but as a rule these growths involve the nerve by extension to it from adjacent parts.
Syphilitic gummata have been found almost exclusively upon the intracranial portion of the cranial nerves.
Gliomas appear to affect only the optic and acoustic nerves. Lepra nervorum (lepra anæsthetica) produces usually a spindle-form thickening upon the nerve-trunks, but sometimes there are more distinct knots, which may be felt beneath the skin, bead-like, along the course of the nerves of the extremities.
Like the true neuromas, the false neuromas, developing from the neurilemma and perineurium, may involve the whole or only a part of the fibres of a nerve, or the nerve-fibres may run at the side of the tumor—different conditions, which may alter materially the effects produced upon the nerve.
Neuromas, both false and true, may occur not only singly, but often in large numbers, many hundreds having been counted upon an individual. Sometimes they are numerous upon a single nerve-trunk and its branches, and again they may appear scattered over nearly all of the nerves of the body, even to the cauda equina and roots of the nerves. According to Erb,9 isolated neuromas are more frequent in females, while multiple neuromas are found almost exclusively in men. Neuromas vary greatly in size, as we might expect from the very great difference of their nature and structure; sometimes no larger than a pea, they may attain the size of a child's head.
9 Ziemssen's Handbuch.
ETIOLOGY.—In cases of multiple neuromata it would seem as if there was a constitutional condition or diathesis as the foundation of the affection. This we may the more readily believe as there appears good evidence to show that the tendency to the formation of these nerve-tumors is sometimes hereditary, and some of them are congenital.
Idiots and cretins have been observed to suffer in undue proportion with multiple neuromas. We find a direct exciting cause of neuromas in mechanical injuries of nerves, wounds, blows, pressure, etc. Thus, as has been already seen, true neuromas occur in the divided ends of the nerves after amputations or otherwise where a nerve-trunk has been divided (cicatricial neuroma). As such neuromas are in some degree the result of inflammation, it is probable that they may sometimes be caused by chronic neuritis.
For a large number of neuromas no cause can be assigned, and we must at present consider them as originating spontaneously.
SYMPTOMS.—The position and connections of neuromas being so different, sometimes simply in contact with the nerve; sometimes situated in the thickness of the nerve-trunk, the fibres being pressed aside and spread out upon the surface of the tumor; sometimes involving in their tissue a part or the whole of the nerve-fibres,—we cannot but expect a [p. 1210] very marked difference in their clinical history. Not a few cases occur in which the presence of neuromas, even in large numbers, gives rise to no symptoms during life, and their existence has been revealed only upon a post-mortem examination.
The symptom most common to neuromas, and one to be expected from their mechanical interference with the nerves, is neuralgic pain—sometimes extreme, local or shooting along the course of the nerves, stubborn, and hardly to be alleviated by remedies. It is paroxysmal, notwithstanding the unvarying character of its cause, in consonance with the tendency to periodical activity which prevails in the nervous system. Sometimes the pain is increased notably by atmospheric changes. The pain may sometimes be arrested by firm pressure upon the nerve above the seat of the tumor. In some cases pressure upon the neuroma, or even handling it, causes great pain. The intensity of the pain does not depend upon the size of the tumor, some of the smallest having earned the appropriate name of tubercula dolorosa. The continued irritation of a neuroma sometimes produces a condition of general nervous excitability, which shows itself in hysterical and even in true epileptic convulsions. Occasionally there are abnormal sensations (paræsthesiæ), formication, numbness, etc., in the distribution of the nerve affected, and when from pressure or histological changes the fibres are destroyed anæsthesia results.
The interference with the conductivity of the motor fibres, which occurs less frequently than alterations of sensation, shows itself in cramps, tumors, paresis, and paralysis, according to its degree.
Neuromas may destroy life by the continued excessive pain, which wears down the strength and depresses the vitality. Death may be caused by their peculiar situation; as, for instance, upon the cauda equina, where they produce paraplegia, paralysis of the sphincter and bladder, and trophic changes.
The DIAGNOSIS of neuromas can only be made when they are sufficiently superficial to be recognized by the touch, and along with the symptoms above detailed the tumor is situated upon the known course of a nerve, to which, moreover, its attachment allows a lateral movement.
The only TREATMENT available for neuromas is extirpation, which must be conducted with a view to sparing any fibres of the nerve not involved in the tumor. Where it is necessary to divide the nerve in the removal of the tumor, as small a portion as possible must be excised, with the hope of a regeneration and reuniting of the cut ends. The success of extirpation depends largely upon the nature of the neuroma. The true neuromas, while they often show a strong tendency to recur after removal, are benign and show no metastasis. For the false neuromas the prognosis will be in accordance with their benign or malignant character.
DEFINITION.—It is customary to describe as neuralgic those pains for which no adequate cause can be assigned in any irritation of the sensory nerves from outside, which recur paroxysmally, are unattended by fever, and are distributed along the course of one or more nerves or nerve-branches.
The general use of the term neuralgia further implies the common belief that there is a disease or neurosis, not covered by any other designation, of which these pains are the characteristic symptom. Of the pathological anatomy of such a disease, however, nothing is known; and if it could be shown for any given group of cases that the symptoms which they present could be explained by referring them to pathological conditions with which we are already familiar, these cases would no longer properly be classified under the head of neuralgia.
The attempt has frequently been made, and on good grounds, in obedience to this reasoning, to cut down the list of the neuralgias, strictly so called, and to account for many of the groups of symptoms usually classified under that head by referring them to anæmia or congestion of the sensory nerves, to neuritis, etc.
One of the best and most recent statements of this view is that of Hallopeau,1 who, although he does not wholly deny the existence of a neurosis which may manifest itself as neuralgia, goes so far as to maintain that the gradual onset and decline and more or less protracted course so common in the superficial neuralgias, such as sciatica, suggest rather the phases of an inflammatory process than the transitions of a functional neurotic outbreak, and that, in general terms, a number of distinct affections are often included under the name of neuralgia which are really of different origin, one from the other, and resemble each other only superficially. This subject will be discussed in the section on Pathology, and until then we shall, for convenience' sake, treat of the various neuralgic attacks as if they were modifications of one and the same disease.
1 Nouveau Dict. de Méd. et de Chir. pratiques, art. “Névalgies.”
GENERAL SYMPTOMATOLOGY.—The neuralgias may be conveniently divided into—1, external or superficial; 2, visceral; 3, migraine and the migrainoid headaches.
The most prominent symptom of a neuralgic attack of the superficial [p. 1212] nerves is of course the pain, and sometimes, from first to last, no other sign of disease is present. In an acute attack the pain is usually ushered in by a sense of discomfort, which the patient vainly tries to shake off, or by a feeling of weight and pressure or of numbness and prickling, or of itching. Sometimes, though far less often than in the case of migraine, there are prodromal signs of a more general character, such as a feeling of thirst2 or of mental depression or drowsiness.
2 Spoken of by Mitchell's patient with neuralgia of the stump (see below).
A dart of pain may then be felt, which soon disappears, but again returns, covering this time a wider area or occupying a new spot as well as the old. The intensity, extension, and frequency of the paroxysms then increase with greater or less rapidity, but, as a rule, certain spots remain as foci of pain, which radiates from them in various directions, principally up or down in the track of the nerve-trunk mainly implicated. The pain rarely or never occupies the whole course and region of distribution of a large nerve or plexus, but only certain portions, which may be nearly isolated from one another.
In an acute attack the affected parts may at first look pale and feel chilly, and later they frequently become congested and throb. Mucous surfaces or glandular organs in the neighborhood often secrete profusely, sometimes after passing through a preliminary stage of dryness.
The skin often becomes acutely sensitive to the touch, even though firm, deep pressure may relieve the suffering. Movement of the painful parts, whether active or passive, is apt to increase the pain. When the attack is at its height, the pain is apt to be felt over a larger area than at an earlier or a later period, and may involve other nerves than those first attacked. Thus, a brachial becomes a cervico-brachial neuralgia or involves also the mammary or intercostal nerves. A peculiarly close relationship exists between the neuralgias of the trigeminal and of the occipital nerves. It is said that when the attack is severe the corresponding nerves of the opposite side may become the seat of pain. This is perhaps remotely analogous to the complete transference of the pain from one side to the other which is so characteristic of periodical neuralgic headaches, especially if they last more than one day.
Some cutaneous neuralgias pass away after a few hours' or a night's rest, after the manner of a migraine or a headache, and patients in whom this takes place are, as a rule, constitutionally subject to neuralgia or other neuroses. Toward the end of such an attack there is often a copious secretion of pale, limpid urine. In a large class of cases, on the other hand, the attack is of several days' or weeks', or even months' or years', duration, with remissions or intermissions and exacerbations, which may be either periodical or irregular.
The most marked periodicity of recurrence is seen with the neuralgias of malarial origin, which may take on any one of the typical forms of that disease.
These malarial neuralgias affect pre-eminently, though not exclusively, the supraorbital branch of the fifth nerve; but it should not be forgotten that there is also a typically periodical supraorbital neuralgia of non-malarial origin, of which the writer has seen several pronounced examples, the pain usually recurring regularly every morning at eight or nine o'clock and passing away early in the afternoon. The same periodicity [p. 1213] is seen, though less often, in other neuralgias. Thus, Trousseau3 speaks of neuralgic attacks from cancer of the uterus in a young woman, which recurred daily at exactly the same hour. Some of the traumatic neuralgias show the same peculiarity to a marked degree.
3 Clin. Méd.
In many neuralgias, on the other hand, the exacerbations are worse at night, like the pains of neuritis. In the intervals between the attacks the pain may be wholly absent, or may persist, usually as a dull aching.
After a neuralgia has lasted a few days—sometimes, indeed, from the outset if the attack is severe—it is usually found that definite spots of tenderness have made their appearance at certain limited points on the course of the nerve. These are the famous points douloureux which Valleix described with such minute accuracy, believing them to be invariably present in true neuralgias. This is certainly not strictly the case, though they are very common. They are not necessarily coincident with the foci of spontaneous pain, as Valleix supposed, but do correspond in general to the points at which the affected nerve emerges from its bony canal or from deep muscles and fascia, and to portions of its area of distribution in the skin. The spinous process corresponding to an affected spinal nerve may also become tender, but this is probably to be looked on, like the same symptom in so-called spinal irritation, not as a sign of local disease, but as due to a general reaction on the part of the nervous system, and as a fact of a different order from the tenderness along the nerve.
The termination of an acute neuralgic attack is usually gradual, like its onset, although in some cases of headache, and in other neuralgias to a less degree, there comes a moment when the patient suddenly declares that he is free from pain.
Neuralgic attacks are usually characterized, besides the pain, by a highly-interesting series of symptoms, which are in part transitory and functional, and in part due to structural changes in the tissues.4
4 See Notta, Arch. gén. de Méd., 1854; Anstie, Neuralgia and its Counterfeits.
The spasm and subsequent dilatation of blood-vessels in the affected area have already been alluded to. A disturbance of secreting organs in the neighborhood of the painful region, the lachrymal gland, the skin, the mucous membranes, the salivary glands, is of equally common occurrence, and is probably in great measure due to direct irritation of the glandular nerves, since the increased secretion is said to occur sometimes unattended by congestion.
The hair may become dry and brittle and inclined to fall out, or may lose its color rapidly, regaining it after the attack has passed.
The increased secretion of urine already alluded to attends not only renal neuralgias, but those of the fifth pair, intercostal, and other nerves. There may be unilateral furring of the tongue (Anstie).
The muscles supplied by the branches of the affected nerve or of related nerves may be the seat of spasm, or, on the other hand, may become paretic; and this is true even of the large muscles of the extremities.
Vision may be temporarily obscured or lost in the eye of the affected side in neuralgia of the fifth pair, and hearing, taste, and smell are likewise deranged, though more rarely. I am not aware that distinct [p. 1214] hemianopsia is observed except in cases of true migraine, where it forms an important prodromal symptom.
In connection with these disorders of the special senses the occasional occurrence of typical anæsthesia of the skin of one-half of the body should be noted, which several observers have found in connection with sciatica. The writer has seen a cutaneous hyperæsthesia of one entire half of the body in a case of cervico-occipital neuralgia of long standing. These symptoms are probably analogous to the hemianæsthesia which comes on after epileptic or other acute nervous seizures, or after concussion accidents, as has lately been observed both in this country and in Europe, and it is perhaps distantly related to the hemianæsthesia of hysteria. Local disorders of the sensibility in the neuralgic area are far more common than this, and, in fact, are usually present in some degree. The skin is at first hyperæsthetic, but becomes after a time anæsthetic; and this anæsthesia offers several interesting peculiarities. When this loss of sensibility is well marked, areas within which the anæsthesia is found are apt to be sharply defined, but they may be either of large size or so small as only to be discovered by careful searching (Hubert-Valleroux). The sensibility within these areas may be almost wanting, but in spite of this fact it can often be restored by cutaneous faradization around their margins, and the functional or neurosal origin of the anæsthesia is thus made apparent. Where the anæsthesia is due, as sometimes happens, to the neuritis with which the neuralgia is so often complicated, it is more lasting, but usually less profound and less sharply defined.
These changes may be transient, or, if a neuralgia is long continued and severe, they may pass into a series of more lasting and deeper affections of the nutrition.
The skin and subjacent tissues, including the periosteum, from being simply swelled or œdematous may become thickened and hypertrophied. The writer has known a case of supraorbital neuralgia, at first typically intermittent, to lead to a thickening of the periosteum or bone over the orbit, which even at the end of several years had not wholly disappeared.
Neuralgias of the fifth pair, which are as remarkable in their outward results as they are in their severity and their relation to other neuroses, are said to give rise to clouding and ulceration of the cornea, to iritis, and even to glaucoma.
Herpetic eruptions on the skin sometimes occur, of which herpes zoster is the most familiar instance.
Muscular atrophy is very common, especially in sciatica, and in some cases this occurs early and goes on rapidly, while in others it may be only slight and proportioned to the disease and relaxation of the muscles, even where the neuralgia has lasted for weeks or months.
Neuritis of the affected nerve is a common result or attendant of neuralgia, and may remain behind for an indefinite period after the acute pain has gone, manifesting itself by subjective and objective disorders of sensibility, by occasional eruptions on the skin, or by muscular atrophy.
It is plain that in this list of symptoms a variety of conditions have been described which would never all be met with in the same case, and which, as will be shown in the section on Pathology, are probably due to different pathological causes.
These neuralgias are less definitely localized by the sensations of the patient than those of the superficial nerves, and it is not definitely known what set of nerves are at fault.
They are deep-seated and are referred to the general neighborhood of the larynx, œsophagus, heart, or one of the abdominal or genital organs, as the case may be.
The pain is usually of an intense, boring character, and does not dart like the pain of superficial neuralgia, but is either constant or comes in waves, which swell steadily to a maximum and then die away, often leaving the patient in a state of profound temporary prostration.
Deep pressure often brings relief. A patient of the writer, who is subject to attacks of this kind in the right hypochondrium, will bear with her whole weight on some hard object as each paroxysm comes on, or insist that some one shall press with his fists into the painful neighborhood with such force that the skin is often found bruised and discolored.
The functions and secretions of the visceral organs are apt to be greatly disordered during a neuralgic attack, and it is often difficult or impossible to tell with certainty which of these conditions was the parent of the other. Undoubtedly, either sequence may occur, but the pain excited by disorder of function, or even organic disease of any organ, is not necessarily felt in that immediate neighborhood. Thus I have known the inflammation around an appendix cæci, of which the patient shortly afterward died, to cause so intense a pain near the edge of the ribs that the passage of gall-stones or renal calculus was at first suspected.
There seems to be as much variation as to modes of onset and duration among the visceralgias as among the superficial neuralgias, but the tendency to short typical attacks of frequent recurrence seems to be greater with the former.
The visceral neuralgias are quite closely enough related to certain of the superficial neuralgias to show that they belong in the same general category. The two affections are often seen in the same person, and not infrequently at the same time or in immediate succession. Thus in the case of the patient just alluded to above, the attacks of deep-seated neuralgia in the neighborhood of the right flank are at times immediately preceded by severe neuralgia of the face or head. Similarly, intercostal neuralgia may occur in immediate connection with neuralgias of the cardiac or gastric nerves.
The phenomenon of tender points is not entirely wanting in the visceralgias, though less constant and definite than in the superficial neuralgias.
The liver and the uterus especially become the seat of more or less localized tenderness, and possibly the tenderness in the ovarian region which is so common, and so often unattended by real inflammation, is, in part, of this order.
The secondary results of the visceralgias are not easy to study. Besides the disorders of secretion and function above alluded to, swelling of the liver with jaundice and paresis of the muscular walls of the hollow viscera may be mentioned as having been ascribed to neuralgia.
It is not known to what degree neuritis occurs as a cause or [p. 1216] complication of these neuralgias, and this is a question which is greatly in need of further study.
This is often classified as an affection of a different order from the neuralgias, but there seem to be no real grounds for this distinction.
The superficial neuralgias themselves are probably not one, but a group of affections, with the common bond of severe and paroxysmal pain.
Neither is what is called migraine always one and the same disease.
Although in its most typical form it presents very striking characteristics, such as a marked preliminary stage, with peculiar visual and sensory auras, sometimes occupying one entire half of the body, a short and regular course and periodical return, deep-seated pain without tender points, and prominent unilateral vascular disorders, yet these symptoms shade off by imperceptible degrees into those of neuralgia of the fifth pair, or more often into one or another form of unilateral neuralgic headache which stands midway between the two.
The vascular phenomena of migraine are believed by various observers, as is well known, to constitute the primary and essential pathological feature of the disease, and to be the cause of the pain. But this is a pure hypothesis, and as a matter of fact the cases are abundant in which no greater vascular changes are present than in other neuralgias of equal severity.
Migraine seems to occupy an intermediate position between the grave neuroses, especially epilepsy, and the neuralgias of neurosal origin.
The symptomatology will be described at greater length below.
GENERAL ETIOLOGY.—The causes of neuralgia may be divided into predisposing and exciting causes.
The most important of the first group are—
1. Hereditary tendencies;
2. The influences associated with the different critical periods of life;
3. The influences attached to sex;
4. The action of constitutional diseases, such as phthisis, anæmia, gout, syphilis, diabetes, nephritis, malarial poisoning, metallic poisoning.
The most important of the second group of causes are—
1. Atmospheric influences and the local action of heat and cold;
2. Injuries and irritation of nerves;
3. Irritation of related nerves (so-called reflex and sympathetic neuralgias);
4. Acute febrile diseases.
In most cases more than one cause is to blame, and each should be separately sought for.
PREDISPOSING CAUSES.—1. Hereditary Tendencies.—It is generally admitted as beyond question that neuralgias are most common in families in which other signs of the neuropathic taint are prominent. Such affections as hysteria, neurasthenia, epilepsy, asthma, chorea, dipsomania, and even gout and phthisis as it would seem, are akin to the neuralgic tendency.
[p. 1217]The neuropathic family is thought to contain, in fact, a much larger number of members than this,5 but there is danger of exaggerating the importance of an influence of which we know as yet so little.
5 Féré, Arch. de Névrologie, 1884, Nos. 19 and 20, “La famille névropathique.”
It should be remembered, moreover, that even where an inherited taint is present its influence may be but slight as compared with that of some special exciting cause.
Some neuralgias are more closely associated with the inherited neuropathic diathesis than others. The connection is especially close in the case of migraine;6 then follow other forms of periodical headache and the visceral neuralgias. Even the superficial neuralgias7 are more or less subject to this influence. This is thought to be especially true of the facial neuralgias.
6 There is a witty French saying (quoted by Liveing), “La migraine est le mal des beaux esprits;” which might be rendered, “The disease of nervous temperaments.”
7 For tables of illustrative cases see Anstie, Neuralgia and its Counterfeits, and J. G. Kerr, Pacific Med. and Surg. Journ., May, 1885.
Reasons will be offered later for suspecting that many cases usually classed as neuralgia, and characterized by gradual onset and protracted course, are essentially cases of neuritis; and there is need of further inquiry as to how far hereditary influences are concerned in producing them, and whether such influences act by increasing the liability of the peripheral nerves to become inflamed, or only by increasing the excitability of the sensory nervous centres.
2. Age.—Neuralgia is oftenest seen in middle life and at the epochs marked by the development and the decline of the sexual functions. The affection, when once established, may run over into advanced age, but cases beginning at this period are relatively rare and very intractable (Anstie).
Childhood is commonly said to be almost exempt from neuralgia, but, in fact, there seems no sufficient reason for withholding this term from the so-called growing pains of young children8 so long as it is accorded to the almost equally irregular neuralgias of anæmia in the adult. The same remark applies to the attacks of abdominal pain in children, which often seem to be entirely disconnected from digestive disorders.
8 Probably due to anæmia or imperfect nutrition (see Jacobi, “Anæmia of Infancy and Childhood,” Archives of Med., 1881, vol. v.).
Adolescents and children also suffer from periodical headaches, both of the migrainoid and of the neuralgic type. These are obstinate and important affections.9 Migraine especially, coming on in early life, points to a neuropathic constitution, and will be likely to recur at intervals through life, or possibly to give place to graver neuroses.
9 Blache, Revue mensuelle de l'enfance, Mar., 1883, and Keller, Arch. de Névroloqie. 1883.
3. Sex.—Women show a stronger predisposition than men to certain forms of neuralgia, as to the other neuroses, but it is generally conceded that whereas neuralgias of the fifth and occipital and of the intercostal nerves are met with oftenest among them, the brachial, crural, and sciatic neuralgias are commoner among men. This probably indicates that the neurosal element is of greater weight in the former group, the neuritic element in the latter.
4. Constitutional Diseases.—The blood-impoverishment of phthisis and anæmia, the poison of malaria, syphilis, and gout, and the obscurer [p. 1218] forms of disordered metamorphosis of tissue, undoubtedly predispose to neuralgia and the other neuroses, as well as to neuritis and others of the direct causes of neuralgic attacks.
Anstie regards the influence of phthisis as so important as to place it fairly among the neuroses. Gout is likewise reckoned by some observers among the neuroses,10 but we tread here upon uncertain ground. Anstie does not regard gout as a common cause of neuralgia, but most writers rate it as more important, and gouty persons are certainly liable to exhibit and to transmit an impaired nervous constitution, of which neuralgia may be one of the symptoms. The neuralgias of gout are shifting, irregular in their course, and sometimes bilateral.
10 Dyce-Duckworth, Brain, vol. iii., 1880.
Syphilitic patients are liable to suffer, not only from osteocopic pains and pains due to the pressure of new growths, but also from attacks of truly neuralgic character. These may occur either in the early or the later stages of the disease. They may take the form of typical neuralgias, as sciatica or neuralgia of the supraorbital nerve (Fournier11), or they may be shifting, and liable to recur in frequent attacks of short duration, like the pains from which many persons suffer under changes of weather, anæmia, or fatigue.
11 Cited by Erb in Ziemssen's Encyclopædia.
There are other obscure disorders of the nutrition, as yet vaguely defined, in connection with which neuralgia of irregular types is often found. Some of these are classed together under the name of lithæmia, and are believed to be due to imperfect oxidation of albuminoid products.12
12 See DaCosta, Am. Journ. of Med. Sciences, Oct., 1881, and W. H. Draper, New York Med. Record, Feb. 24, 1883.
Diabetes seems also to be an occasional cause of neuralgia, especially sciatica, and Berger,13 who has recently described them, says that they are characterized by limitation of the pain to single branches of the sacral nerves, by a tendency to occur at once on both sides of the body, by the prominence of vaso-motor symptoms, and, finally, by their long duration and obstinacy. There may not, at the moment, be any of the characteristic symptoms of diabetes present.
13 Neurologisches Centralblatt, 1882, cited in the Centralbl. für Nervenheilk., etc., 1882, p. 455.
Chronic nephritis also causes neuralgia, either directly or indirectly; and severe neuralgic attacks may accompany the condition, which is as yet but imperfectly known, characterized pathologically by a general arterio-fibrosis and by increased tension of the arterial system.
True rheumatism does not appear to be a predisposing cause of neuralgia.
Anæmia, both acute and chronic, is a frequent cause of neuralgia, both through the imperfect nutrition of the nervous tissues, to which it leads, and, it is thought, because the relatively greater carbonization of the blood increases the irritability of the ganglionic centres.
Even a degree of anæmia which might otherwise be unimportant becomes of significance in the case of a patient who is otherwise predisposed to neuralgia; for such persons need to have their health kept at its fullest flood by what would ordinarily seem a surplus of nourishment and care.
Under the same general heading comes the debility from acute and [p. 1219] chronic diseases, and the enfeeblement of the nervous system from moral causes, such as anxiety, disappointment, fright, overwork and over-excitement, and especially sexual over-excitement, whether gratified or suppressed (Anstie), or, on the other hand, too great monotony of life; also from the abuse of tea, coffee, and tobacco.
Lead, arsenic, antimony, and mercury may seriously impair the nutrition of all the nervous tissues, and in that way prepare the way for neuralgia.
IMMEDIATE CAUSES.—1. Atmospheric and Thermic Influences.—Neuralgia is very common in cold and damp seasons of the year, in cold and damp localities, and in persons whose work entails frequent and sudden changes of temperature. Exposures of this sort may at once excite twinges of pain here and there over the body, and may eventually provoke severe and prolonged attacks of neuralgia.
The action of damp cold upon the body is complicated, and it exerts a depressing influence on the nervous centres in general which is not readily to be explained. One important factor, however, is the cooling of the superficial layers of the blood, which occurs the more easily when the stimulus of the chilly air is not sufficiently sharp and sudden to cause a firm contraction of the cutaneous vessels, while the moisture rapidly absorbs the heat of the blood. From this result, indirectly, various disorders of nutrition of the deeper-lying tissues or distant organs; and, among these, congestion and neuritis of the sensitive nerves.
Neuralgia often coincides with the presence or advent of storms. A noteworthy and systematic study of this relationship was carried on through many years under the direction of S. Weir Mitchell14 by a patient of his, an officer who suffered intensely from neuralgia of the stump after amputation of the leg. The attacks of pain were found to accompany falling of the barometer, yet were not necessarily proportionate to the rapidity or amount of the fall. Saturation of the air with moisture seemed to have a certain effect, but the attacks often occurred when the centre of the storm was so remote that there was no local rainfall. It was impossible to study the electrical disturbances of the air with accuracy, but a certain relationship was observed between the outbreak of the attacks and the appearance of aurora borealis.
14 Am. Journ. of Med. Sci., April, 1877, and Philada. Med. News, July 14, 1883.
This patient's neuralgic attacks were almost certainly of neuritic origin, and it is possible that the exacerbations were due to changes of blood-tension in and around the nerve-sheaths. It is also possible that they were the result of circulatory changes and disordered nutrition of the nervous centres, already in a damaged condition from the irritation to which they had been exposed.
2. Injuries and Irritation of Nerves.—Wounds and injuries of nerves15 and the irritation from the pressure of scars, new growths, and aneurisms are prolific causes of neuralgic pain, partly by direct irritation, partly by way of the neuritis which they set up. Neuralgias are likewise common during the period of the healing of wounds, as Verneuil long since pointed out. The pain may be near the wound itself or in some distant part of the body.
15 See S. Weir Mitchell, Injuries of Nerves.
Neuralgia due to the pressure and irritation of tumors, new growths, [p. 1220] or aneurisms requires a special word. The pain is apt to be intensely severe, but what is of especial importance is that the symptoms may not present anything which is really characteristic of their origin, except their long continuance; and this should always excite grave suspicion of organic disease.
These attacks of pain may be distinctly periodical; and this is true whether they are felt in the distribution of the affected nerve or of distant nerves.
Not only are direct injuries of nerves a cause of neuralgia, but sudden concussion or jar may have a like effect—whether by setting up neuritis or in some other way is not clear. Ollivier16 reports a case where a blow beneath the breast caused a neuralgia which eventually involved a large portion of the cervico-brachial plexus; and the writer has seen a like result from a blow between the shoulders.
16 Cited by Axenfeld and Huchard, p. 116.
Peripheral irritations, such as caries of the teeth (see below, under Facial Neuralgia) and affections involving other important plexuses, such as those of the uterine nerves, are a frequent cause of neuralgia, and should always be sought for. They act in part by setting up neuritis, and in part evidently in some more indirect manner, since the neuralgia which they excite may be referred to more or less distant regions, forming the so-called—
3. Reflex and Sympathetic Neuralgias.—The term reflex, as here used, is ill chosen, and the term sympathetic only covers our ignorance of the real processes involved, and which we should seek for in detail. Thus, disease of the uterus or ovaries may cause facial, mammary, intercostal, or gastric neuralgia.
Hallopeau17 suggests that some of these results may be brought about by the pressure of enlarged lymphatic glands attached to the affected organ.
17 Loc. cit., p. 766.
Another important centre of nervous irritation is the eye. Slight errors of refraction, or weakness of the muscles of fixation, especially the internal recti, are a source of frontal headaches and other nervous symptoms, and even of typical migraine,18 to a degree which is not usually appreciated. It is improbable that in the latter case the irritation acts as more than an exciting cause, but it may nevertheless be a conditio sine quâ non of the attack.
18 St. Barthol. Hosp. Repts., vol. xix.
Acute and chronic inflammations of the mucous membrane of the frontal sinuses, perhaps even of the nasal membrane, are likewise important; and although it is probable that the opinions sometimes expressed as to the significance of these causes are exaggerated, it is equally true that obstinate and, as it were, illogical persistence in their removal will sometimes be richly rewarded.
It is especially worthy of note that there need be no local sign whatever to call the attention of the patient to the presence of the peripheral irritation.
Nothnagel19 has described neuralgias which come on in the first week of typhoid, and are to be distinguished from the general hyperæsthesia of later stages. He describes an occipital neuralgia of this sort which finally disappeared under the use of a blister. Other acute diseases may have a like effect. The writer has seen a severe facial neuralgia in the [p. 1221] first week of an insidious attack of pneumonia in a person who was not of neuralgic habit, and before the fever or inflammation had become at all severe.
19 Virch. Arch., vol. liv., 1872, p. 123.
PATHOLOGY AND DIAGNOSIS.—In surveying the clinical history of the neuralgias and the circumstances under which they occur, we have grouped together a large number of symptoms of very different character from each other, and we have now to inquire to what extent these symptoms are really united by a pathological bond.
Two opposite opinions have been held concerning the pathology of neuralgic affections. According to one opinion, every neuralgic attack, no matter how it is excited, is the manifestation of a neurosis—that is, of a functional affection of the nervous centres—to which the term neuralgia may properly be applied. This view is based on the resemblance between the different forms of neuralgia, or the apparent absence, in many cases, of any adequate irritation from without, and the fact that the persons in whom neuralgias occur usually show other signs of a neuropathic constitution.
According to the other opinion, the various forms of neuralgia are so many different affections, agreeing only in their principal symptom, and are due sometimes to congestion or anæmia of the nerves or the nerve-centres; sometimes to neuritis, the pressure of tumors, or the irritation of distant nerves; sometimes, finally, to a functional disorder of the nervous centres. The arguments in favor of this opinion are that the difference between the symptoms of the different neuralgias as regards their mode of onset and decline, their duration, the persistence of the pain, and the degree to which the attacks are accompanied by organic changes of nutrition in the tissues and in the nerve itself, are so great as to make it appear improbable that we are dealing in every case simply with one or another modification of a single affection.
This is a valid reasoning, and it is certainly proper to exhaust the possibilities of explaining the symptoms that we find in a particular case by referring them to morbid processes which we can see or of which we can fairly infer the presence, before we invoke an influence of the nature of which we understand so little as we do that of the functional neuroses. At the same time, it must be distinctly borne in mind that the symptoms of certain neuralgias, and the relation which the neuralgias in general bear to other neuroses, can only be accounted for on the neurosal theory, and that in a given case we can never be sure that this neurosal tendency is not present and is not acting as at least a predisposing cause. It is especially important to bear this possible influence in mind in deciding upon prognosis and treatment.
We may now review briefly the signs which should lead us to diagnosticate or suspect the presence of the various special causes of neuralgic symptoms.
Neuritis is indicated by the presence of organic disorders of nutrition affecting the skin, hair, or nails, or of well-marked muscular wasting; by pain, not only occurring in paroxysms, but felt also in the intermissions between the paroxysms, or continuous sensations of prickling and numbness, even without pain; by tenderness along the course of the nerve; by anæsthesia, showing itself within the first few days of the outbreak of a neuralgia; by persistent paralysis or paresis of muscles.
[p. 1222]Neuritis may be suspected, even if one or all of these signs are absent, in the prolonged neuralgias which follow wounds or strains of nerves or exposure to damp cold, or which occur in nerves which are in the immediate neighborhood of diseased organs; also where the pain is relieved by compression of the nerve above the painful part, or, on the other hand, where pressure on the nerve excites a pain which runs upward along the course of the nerve.
It may also be suspected in the large class of superficial neuralgias which follow a regular and protracted course with gradual onset and decline, and where the pain is felt not only in the region of distribution of a nerve, but also along its course—that is, in the nerve-fibres (either the recurrent nerves or the nervi nervorum) which are distributed in the sheath of the main trunk or the adjoining tissues.20
20 See Cartaz, Des Névralgics envisagés au point de vue de la sensibilité récurrente, Paris, 1875.
It must be remembered that the study of neuritis, and especially of chronic neuritis, is still in its infancy, and that we are by no means in possession of its complete clinical history.21
21 See Pitres and Vaillard, Arch. de Névrologie, 1883.
The presence of congestion of the sensory nerves or nerve-centres may be inferred with some degree of probability where neuralgic attacks of relatively sudden onset and short duration occur in parts which have been exposed to heat or cold, or in connection with suppression of the menstruation, or, it is said, as a result of intermittent fever. The exacerbations of pain which take place in cases of chronic neuritis under changes of weather and after fatigue are very likely due to this cause; and the same may be true of some of the fleeting pains which occur in chlorotic and neuropathic persons who are subject to fluctuations of the circulation of vaso-motor origin.
The same vaso-motor influences which cause congestion may also cause the correlative state of anæmia, which becomes thus a cause of transient and shifting though often severe attacks, which may be irregular in their distribution. General anæmia is also a predisposing cause of severe typical seizures, as has been pointed out above.
The pressure of new growths or of aneurisms is to be suspected when neuralgic attacks are unusually severe and prolonged, recur always in the same place, and occur in persons who are not predisposed to neuralgias. The pains from this cause are apt to be relatively continuous, but they may, on the other hand, be distinctly paroxysmal, and may occupy a part of the body far removed from the irritating cause.
Bilateral pains should also excite suspicion of organic disease, though they may be due to other causes, such as gout, diabetes, and metallic poisoning.
Neuralgic attacks may be supposed to be of neurosal origin when they are of sudden onset and short duration, or when they occur in persons of neuropathic constitution, and, by exclusion, when no other cause is found. These conditions are best fulfilled in the case of migraine and the visceral neuralgias. It must, however, be borne in mind that the neuropathic predisposition is sometimes well marked even in the case of the superficial neuralgias, especially the epileptiform neuralgia of the face.
GENERAL TREATMENT.—To treat neuralgia with satisfaction it is [p. 1223] necessary to look beyond the relief of the particular attack and search out the causes by which it was provoked. As has already been remarked, these are usually multiple, and among them will be found, in the great majority of cases, some vice of nutrition or faulty manner of life.
It is safe to say that any dyscrasia occurring simultaneously with neuralgia, whether gout, phthisis, malaria, or diabetes, should receive its appropriate treatment, whatever theory we may hold as to the real connection between the two conditions.
In protracted neuralgias it is always proper to assume that neuritis may be present—i.e. to treat the nerve itself by galvanism and local applications. Local irritations, such as diseases of the eye, ear, teeth, nose, or uterus, should be sought out and removed; and attention may here be called again to the fact that a neuralgia may be due to some local condition which does not of itself attract the patient's attention.
Patients who are subject to pain at changes of weather or on exposure should be suitably protected by clothing, and should have their cutaneous regulatory apparatus strengthened by baths and friction. The best protection, however, is incapable of entirely warding off the effect of atmospheric changes upon the nervous centres. Vaso-motor changes of neurotic origin can be, in a measure, prevented by removing the patient from the influence of irregularity of life and emotional excitement and through an improved nutrition.
If the patient has been subjected to chronic fatigue or nervous strain, not only must these be avoided, but their action should be counteracted by the requisite rest and tonic treatment.
Long hours of sleep at night may often be supplemented to advantage by rest during certain hours of the daytime. If the patient cannot take active exercise, massage is indicated, and in some cases of anæmia this may advantageously be combined with the wet pack, in the manner described by Mary Putnam Jacobi.22
22 Massage and Wet Pack in the Treatment of Anæmia.
Where these measures cannot be carried out, the writer has found it of much service in these, as in a large class of debilitated conditions, to let the patient rub himself toward the end of the forenoon in a warm room with a towel wet in cold or warm water, and then lie down for an hour or so or until the next meal. If acceptable, the same operation may be repeated in the afternoon.
Neuralgic patients are apt to be underfed, and even where this is not distinctly the case, a systematic course of over-feeding,23 with nourishing and digestible food, such as milk, gruel, and eggs, given at short intervals, is often of great service if thoroughly carried out. The full benefit of this treatment cannot always be secured unless the patient is removed from home, and, if need be, put to bed and cared for by a competent nurse.
23 See S. Weir Mitchell, Fat and Blood; and Nervous Diseases, especially of Women.
A change of climate, and especially the substitution of a dry and warm for a moist and cold climate, will sometimes break up the neuralgic habit, for the time at least. In making choice of climate or locality, however, the physician should keep distinctly in view the end that he desires to gain. Thus, the debility or anæmia which is the essential condition of many neuralgias may often be relieved by surroundings which [p. 1224] would not be thought favorable to the neuralgic tendency as such. Oftentimes the sedative influence of quiet country life is all that is required.
Of the tonic drugs, cod-liver oil, iron, arsenic, and quinine are by far the most important, and it is often well to give them simultaneously. Iron may be used in large doses if well borne, for a short time at least. Quinine may be given in small doses as a tonic, or in larger doses to combat the neuralgic condition of the nervous system. This remedy has long been found to be of great value in the periodical neuralgias of the supraorbital branch of the fifth pair, but its usefulness is not limited to these cases. It may be of service in periodical neuralgias of every sort, and often even in non-periodical neuralgia.
When the attacks recur at stated intervals care should be taken to anticipate them with the quinine by about four hours, even if the patient has to be waked in the early morning for the purpose. Single doses of fifteen, twenty, or even thirty grains may check the attacks where smaller doses have failed. Such doses cannot, however, be long continued, and are not to be classed as tonic.
Of other remedies which directly influence the neuralgic condition, the following are the most important: opium, aconite, gelsemium, phosphorus, belladonna, chloride of ammonium, cannabis Indica, croton-chloral, electricity, hydropathy, massage, counter-irritation, subcutaneous injections of water, chloroform, osmic acid, etc.; surgical operations.
Opium is usually employed only for the momentary relief of pain, but it has also been claimed that in small and repeated doses it may exert a really curative action. This should not, however, be too much counted on. Opium should never be used continuously for the simple relief of pain unless under exceptional circumstances, the danger of inducing the opium habit is so much to be dreaded. Moreover, both patient and physician are less likely to seek more permanent means of cure if this temporary remedy can always be appealed to. It is best given by subcutaneous injections of the various salts of morphine. The dose should always be small at first (gr. 1/12 and upward), unless the idiosyncrasy of the patient is already known; and there is probably no advantage in making the injections at the seat of pain or in the immediate neighborhood of the nerve supplying the affected part, except such as might attend the injection of any fluid (see below).
Belladonna (atropia), which is so often given with morphine to diminish its unpleasant effects, seems at times, even when given alone, to have an effect on neuralgia out of proportion to its anæsthetizing action, which is very slight. It is considered to be especially useful in the visceralgias.
Aconite, given, if necessary, in doses large enough and repeated often enough to cause numbness and tingling of the lips and the extremities for some days, will sometimes break up an attack, especially of trigeminal neuralgia,24 better than any other means; but its use is liable to depress the heart, and it is a dangerous remedy if not carefully watched. Some patients complain that it causes a marked sense of depression or faintness, and a feeling of coldness; and indeed its full therapeutic effect is sometimes not obtained until such symptoms as these are induced to some degree. The use of the crystallized alkaloid, aconitia, has the advantage of ensuring certainty of dose.
24 See Seguin, Arch. of Med., vol. i., 1879; vol. vi., 1881.[p. 1225]
The susceptibility of different persons to this drug is so different that the dose should first be as small as 1/400 gr., but this may be repeated every three hours, and gradually increased to 1/100 gr., or until its physiological effects are felt. Patients must sometimes be kept under its influence for weeks together.25 It is, however, a remarkable fact that occasionally a few full doses will secure an immunity from pain for a long period. Although most useful in facial neuralgias, the writer has known it to be effective in brachial and mammillary neuralgia. Aconitia can now be had in granules of 1/400 gr., or can be given in alcoholic solution.
25 See Seguin, Arch. of Med., vol. vi., 1881.
Gelsemium is also occasionally very useful in facial and even in intercostal neuralgia, and is said to be of special service in the neuralgia due to carious teeth. The commencing dose of the fluid extract is five minims, which may be gradually increased to twenty, or until a slight degree of muscular prostration, ptosis, or dilatation of the pupil is induced.
The use of phosphorus has been revived of late years, chiefly through the efforts of J. Ashburton Thompson, and it is at least occasionally of service. Success is said to be best obtained by full doses (about 1/20 gr. every three or four hours, up to 1/5 or 1/4 gr. daily for some days), watch being kept for signs of gastric irritation. The best preparation is an alcoholic solution (Thompson's), such as the following:
| Rx. | Phosphorus, | gr. j; |
| Abs. alcohol, | fluidrachm vi. | |
| Dissolve with heat. | ||
| Glycerin, | fluidounce iss; | |
| Alcohol, | fluidrachm ij; | |
| Spts. peppermint, | minim v. | |
| One teaspoonful represents gr. 1/20. | ||
Electricity, if properly used, is capable of temporarily, and even radically, relieving the neuralgic state. The forms most often employed are faradic and galvanic electricity, though frictional electricity has also been coming into use of late, mainly as a substitute for faradism. The galvanic current is by far the most efficacious of all. This probably acts mainly by directly inducing better nutritive and better functional conditions in the nerves and nerve-centres, but the fact that it is often of use in cases of undoubted neuritis seems to indicate that it may also influence the grosser structural changes in the affected parts, if such are present. It is impossible to explain its action more exactly, and the teachings of physiological experiments do not lend us much aid.
It is probably not of much consequence which pole is used in the neighborhood of the affected nerve. It should be remembered that the peripheral nerve-trunks are so deeply buried that the electrodes cannot be directly applied to them, as they are to the exposed nerve of a frog in the laboratory, and, further, that instead of being isolated they are surrounded with tissues of good conducting power, into which the current must rapidly flow off. For these reasons the nerve near which either electrode is applied is virtually exposed to the action of both poles in almost equal degree; and although it is more customary to use the positive pole in the neighborhood of parts which are considered to be in a state of irritation, yet clinical experience has not justified the conversion of this custom into a rule. Neither is the direction of the current of material consequence.
[p. 1226]It is, however, very important in acute cases to take care that the current-strength should not be rapidly changed; and for this reason the electrode should be drawn slowly to a distance from the nerve before it is removed, or left in situ while the current is gradually diminished by a suitable rheostat. As a rule, the former method is the more practicable.
In the treatment of acute cases moderate currents and short applications, frequently repeated, are the best. On the other hand, in cases of long standing, especially cases of sciatica, strong currents are sometimes more effective, and even interruptions and reversals of the current may be in place.
The choice of a battery is not a matter of indifference. Any stationary battery of high interior resistance will answer the purpose, but most of the portable (zinc-carbon) batteries in common use are objectionable,26 for the reason that their interior resistance is so low in proportion to that of the body that it may almost be counted out as a factor in determining the strength of the current. The latter is liable to rise, therefore, quite suddenly as the resistance of the body—i.e. the vascularity of the skin—becomes modified. This objection is obviated if a large, constant resistance (water or graphite rheostat) is attached to the battery and kept always in the main circuit.
26 Archives of Medicine, April, 1884.
Faradism probably owes its efficiency to the indirect effects of stimulation of the sensitive nerves of the skin. This may be produced either by the wire brush, which causes a sharp irritation and reddening, and is to be compared with the counter-irritants, or by the milder application of a moist or dry electrode or the hand of the operator. The latter procedure may be compared to the superficial manipulation which is sometimes so grateful, especially in nervous headaches.
The value of electricity as a general tonic should be remembered in this connection.
Hydropathy.—Douches and baths of various kinds have doubtless proved of much value in the treatment of neuralgia. The majority of them, however, are difficult of application for the general practitioner, and we confine ourselves to mentioning the tonic and soothing action of the wet pack and of the prolonged warm bath, which should be followed by sponging with cool water, and used under every possible precaution against exposure.
Long-continued local applications of gentle heat (bags of sand or salt, or hot water) are often temporarily grateful, and in the treatment of chronic cases the daily application of hot water or ice-bags to the spine is said to have a good effect. In acute and subacute neuritis, and in those forms of neuralgia in which neuritis plays a large part, such as sciatica, the persistent application of ice-bags along the course of the affected nerve, even for days together, is sometimes of great service. Even where we cannot be sure that neuritis is present, long-continued applications of ice may be of use, but alternations of cold and heat, on the other hand, are usually to be carefully avoided. This treatment is safer in chronic than in acute cases, though it may be useful in either.
Counter-irritation.—A spray of ether may be substituted for ice when only a temporary chilling is desired, for its counter-irritant effect. This [p. 1227] has even been used on the face, the eye being protected by some suitable covering, and a good deal of benefit is to be hoped for both from this and from the similar use of chloride of methyl.
Debove27 has found the chloride of methyl, used in this manner, singularly effective in the treatment of sciatica. A considerable and long-continued counter-irritation is thus made over a large surface and without great pain. The neuralgia is said to be greatly relieved and a rapid cure sometimes affected.
27 Bulletin générale de Thérap., cited in the Boston Med. and Surg. Journ., vol. cxii. p. 210.
Counter-irritation is also practised by making applications of cutaneous irritants, such as blisters, mustard, turpentine, chloroform, or of the actual cautery carried in light superficial stripes over the skin, and repeated if necessary at short intervals. As a rule, the counter-irritation is more effective the larger the surface which is covered.
The use of the cautery and of blisters is in place in almost every form of neuralgia where the temporary disfigurement is of no consequence.
Of other cutaneous applications, aconite and chloroform liniments, menthol in substance or in alcoholic solution (drachm j or drachm ij to fluidounce j), aconite and veratrine ointments, are the most useful. A strong aconitine ointment, made with Duquesnet's aconitia and lard (drachm j to ounce j), has been recommended by Webber28 to be used in portions of the size of half a split pea, but, though effective, it needs to be employed with great caution.
28 Nervous Diseases, Boston, 1885.
These applications act in part as irritants, by keeping up a play of sensitive impressions in virtue of the lodgment which they effect in the skin, but also, no doubt, by reducing the sensitiveness of the cutaneous nerve-fibres, and thus removing one source of excitation of the diseased nervous centres. The remarkable temporary benefit sometimes obtained from the instillation of cocaine into the eye in cases of neuralgia of the ophthalmic division of the fifth nerve bears testimony in favor of this explanation.
Surgical operations for neuralgia are of three kinds—section (neurotomy), removal of a piece of nerve (neurectomy), and nerve-stretching. The two former operations are of course rarely practised, except upon the purely-sensitive fifth pair of nerves, the latter upon mixed nerves also.
Neurectomy is now almost always substituted for simple neurotomy, and sometimes still more effective means are taken to prevent the reunion of the nerve, such as doubling over the cut end, destroying the nerve throughout the length of the bony canal in which it lies, and even plugging the canal with cement.29
29 Heustis (Med. News, Dec. 8, 1883) found that the infraorbital nerve could be readily drilled out with a piece of piano wire.
The inconvenience following nerve-section is as nothing compared to the pain of a severe and intractable neuralgia. It has rarely happened that the disease has been increased by the operation, and under proper antiseptic precautions the surgical risks are not great. There is some chance of permanent cure, and a much greater chance of securing an immunity from pain for a long period.
It is important to remember that when the neuralgia occupies the distribution of several branches of the fifth nerve, an operation on the one primarily or most severely affected may relieve the pain in all. On the [p. 1228] other hand, the converse may be true,30 inasmuch as the same district is supplied by recurrent fibres from several different sources. Before any operation is decided on it should be remembered that even in apparently desperate cases of trigeminal neuralgia the persistent and thorough use of tonic and other remedies may in the end be crowned with success, perhaps at the moment when it is least expected.
30 Cartaz, Des névralgies envisagés au point de vue de la sensibilité récurrente.
During the past few years the operation of nerve-section has been to some degree superseded by that of nerve-stretching, as being less serious in its immediate (though not necessarily in its remote) consequences, and sometimes more efficacious. Hildebrandt, indeed, raises the question whether the traction which is apt to be exerted when a nerve is cut is not an important element in bringing about the result. On the other hand, cases are reported where neuralgia which had not been relieved by stretching was cured by resection.31
31 Nocht, Ueber die Gefolge der Nerven-dehnung.
The best showing for the operation is in the treatment of sciatica, but most of the other superficial nerves, including the intercostals, have been successfully treated in the same manner.
On the other hand, this treatment is not without its dangers. Apart from the risks of the operation itself, cases have been reported in which the spinal cord has been injured, so that chronic myelitis has been set up, and a greater or less degree of paralysis—rarely permanent, it is true—may be induced by the direct injury to the nerve.
This means of treatment is therefore certainly to be thought of in serious and obstinate cases, but not lightly decided on.
A substitute operation for sciatica is the so-called bloodless stretching, in which, the patient having been etherized, the thigh is forcibly flexed on the pelvis, and then the leg extended on the thigh and the foot on the leg (dorsal flexion), and held for a short time in this position. A very material degree of stretching of the sciatic nerve is doubtless possible in this way, and a number of cures have been thus effected. But, though less dangerous than the stretching of the exposed nerve, this operation is not a trifling one.
In one case of sciatica the writer has seen a neuritis of some severity lighted up by this operation, perhaps because the disease was in too active a state, although it had lasted some months. The operation is probably most indicated in chronic cases.
The anatomical effects of nerve-stretching are manifold. Nerve-fibres are usually destroyed in greater or smaller number, and the conducting power of the nerve correspondingly impaired. Small blood-vessels are broken and the circulation and nutrition of the nerve-trunks altered, and it is probable that adhesions in and around the nerve-sheaths, where such exist, are severed. The nerve-fibres ramifying in the inflamed sheaths of the large trunks may also be ruptured, and it may be that the displacement of the fluid contents of the nerve brings about better nutritive conditions.32 It is also probable that the operation either directly or indirectly affects the nutrition of the nerve-centres,33 and although this is not without its dangers, the chances are in favor of a beneficial result.
32 See “Die Rückenmarks-dehnung,” Hegar, Samml. klin. Vorträge, 239.
33 Hegar, loc. cit.[p. 1229]
Another means of directly acting on neuralgic nerves is by subcutaneous injections of water, chloroform, ether, osmic acid, nitrate of silver, and other substances. The deep injection of water over the affected nerve is attended with but little danger, and is occasionally successful. The similar use of chloroform, in doses of 15 to 30 minims, is much more often effective, but sometimes causes great pain, and even abscess. It has been mainly used in sciatica, also in other neuralgias, even those of the fifth pair. In this case the injection is best made through the buccal mucous membrane. This treatment is not without danger of causing collapse, or even death, probably due to the wounding of a small vein. In one case of sciatica treated by the writer the chloroform probably entered the nerve itself to some extent, as the injection was followed by very severe pain lasting for several hours, and eventually by some degree of muscular wasting. The neuralgic pain, which had continued obstinately for a long period, was, however, cured, and had not returned at the end of some days, when the patient was lost sight of.
Osmic acid has been used recently in the same way, and the reports show about an equal number of successes and failures. The dose is about 8 minims of a 1 per cent. solution, and the injection may be repeated at intervals of a few days. It has been used successfully in various parts of the body, including the face and the fingers. The injection causes no great pain, but occasionally, though rarely, excites abscess.
Under the general heading of massage a number of manipulations may be grouped which are of value in the treatment of neuralgia, even of long-standing cases of sciatica and the like.34 When, as often happens in the case of sciatica, the nerve is the seat of congestion and exudation, strong and deep kneading along its course, with vigorous stroking upward in the direction of the lymph-vessels, is the important part of the treatment. Besides this, however, the prolonged and gentle manipulation of the painful region may greatly relieve the patient for a time, apparently by acting on the sensitive nerves and exerting a sort of inhibitory action, in which it is not at all impossible that an influence upon the attention analogous to that of Braidism plays a part.
34 See Reibmayr, Die Massage, etc., Wien, 1883.
A striking instance of the effect of this treatment is seen in the case of nervous headaches, which are often very greatly relieved by a series of gentle, monotonous movements of the finger-tips, as well as by the domestic remedy of gently and persistently combing or brushing the patient's hair. A still more efficient application of a similar kind is the regular vibration communicated by a large magnet or by the instrument devised by Mortimer Granville. A thoroughly satisfactory explanation of the action of this treatment is yet to be furnished.
There is no doubt that in the treatment of neuralgia a persistent and thorough use of the remedies suggested is usually the key to success. Nevertheless, special cases are sometimes reached by special means of treatment, and the following are appended as occasionally useful: Ammonio-sulphate of copper (grs. ij-vj, taken in divided doses in the course of the day); salicylate of soda, in full doses; caffeine; tonka (fluidrachm j of the fluid extract at repeated intervals of a few hours); oil of turpentine; muriate of ammonia.
35 Consult, in connection with this subject, the sections on Symptomatology and Treatment.
MIGRAINE AND PERIODICAL HEADACHE.—In many of the recent treatises upon nervous disease migraine and headache are removed from the category of the neuralgias and placed in that of the functional affections of the sympathetic vaso-motor system of nerves. This classification is based upon the fact that in many of these cases marked vascular changes—congestion or anæmia, as the case may be—are observed in the external tissues of the affected parts, while the sensations of the patient often lead us to infer the presence of similar conditions within the cranium. The pain and the other symptoms of the outbreak, it is thought, are due to the changes in blood-tension in the cortex cerebri or in the region of expansion of sensitive nerves, or, in part, to the spasm of the muscular walls of the vessels themselves. This theory is seductive from its appearance of pathological simplicity and exactness, but the writer believes, with Anstie, Latham, Allbutt, and other observers, that it is not borne out by clinical experience, and that its adoption tends to cloak the wider relationship that exists between the sensory neuroses.
Migraine, nervous headache, and the superficial and the visceral neuralgias hardly differ more fundamentally from each other than individual cases of either affection differ among themselves. It is not improbable, as we have seen, that all the phenomena of some neuralgic attacks are wholly or in part the expression of irritation of the sensory nervous system from without; but in many cases, on the other hand, the signs of the neurosal tendency are clearly marked, and there is hardly one of the symptoms of a typical migraine of which the analogue may not be found, though perhaps faintly pronounced, in one or another form of superficial neuralgia, while the relation of both to the whole family of the neuroses is still more clearly evident.
Migraine is a disease of youth and middle life, characterized, in its most typical form, by attacks of severe headache of a few or many hours' duration, of gradual onset and decline, ushered in by well-marked auras involving one or more of the cerebral functions, and terminating in nausea or vomiting or profuse secretion of pale urine, or in some other critical nervous outbreak. The pain is usually, but not invariably, deep-seated. It may be confined to one side of the head, most often the left, or may involve both sides, either from the outset or in the course of the attack. The forehead or temple is usually the first part to become painful, but in severe or prolonged seizures the parietal and occipital regions are prone to be affected likewise.
The auras are manifold and important. On the day before an attack the patient may feel remarkably well, or may complain only of such sensations as thirst or giddiness. The attack itself is apt to be ushered in by visual hallucinations of dazzling and vibrating points or serrated images, sometimes with prismatic outlines, accompanied by a loss or obscuration of vision over one-half or some other portion of the field, which lasts half an hour or more, and sometimes clearing up in one part while it advances in another. Simultaneously or immediately after this there may be [p. 1231] tingling and a sense of numbness of the tongue, lips, hand, or one-half of the body, sometimes followed by partial hemiparesis, and, if the right side be affected, by more or less aphasia or mental confusion. Occasionally the other special senses are affected. Sometimes the aura may constitute the whole of the seizure.
The writer has observed a case in which migraine was represented throughout boyhood by repeated attacks of subjective numbness and tingling of the entire right side of the face, the right arm, and the right half of the body, with aphasia and hemianopsia, followed during many years by trifling headache or none at all; later in life by severe pain. Here migraine as well as neuralgia in other forms was a well-marked family disease.
These auras are especially worthy of notice, because they occasionally point to epilepsy, an affection with which migraine is allied.
The pain may begin on the same side with these prodromal symptoms or on the opposite side. Sometimes drowsiness is a marked symptom throughout the attack, and this differs in significance from the sound, refreshing sleep with which the paroxysm often comes to an end. Sometimes the arteries of the affected side seem strongly contracted, as shown by pallor and coldness of the face and dilatation of the pupil (angio-tonic form); sometimes, on the other hand, they are dilated and pulsate strongly, or the latter condition may follow the former (angio-paralytic form). The radial pulse may show corresponding modifications. These vascular phenomena are often, however, entirely wanting.
Migraine appears to be slightly more common in women than in men. The liability to the attacks often shows itself in extreme youth, usually increases at puberty, and generally ceases at the age of forty or fifty. The attacks sometimes recur at regular intervals of a week, a month, etc., but, on the other hand, they may remain absent for years unless brought on by some exciting cause.
ETIOLOGY AND CLINICAL RELATIONS.—Migraine is a directly inheritable disease, and one which stands in a close relationship to the other grave neuroses, as well as to the neuropathic temperament. Cases are occasionally seen in which the migraine of youth gives place to epilepsy in later years. It is often met with also in families and individuals of neuralgic tendency, and in fact it shades off into neuralgia of the fifth and occipital nerves on the one hand and into periodic nervous headaches on the other. It frequently occurs in gouty persons, and is thought to be related to the brow ague of malaria. The attacks may be brought on by any of the causes which depress the vitality of the nervous system, and by various special irritations, among which errors of refraction are prominent.
The PROGNOSIS is unfavorable in well-marked cases, in which the habit of regular recurrence is established, and where the neuropathic predisposition is pronounced and no special exciting cause can be found. On the other hand, there are many cases where the tendency is less deeply rooted, and where with the removal of the exciting cause or causes the outbreaks cease.
Finally, there is great probability that the disease will cease of itself with advancing years, not always, however, without having left its mark on the patient's mental and bodily vitality.
[p. 1232]The TREATMENT should be directed first to the detection and removal of special sources of irritation, whether in the eye, stomach, uterus, or elsewhere. Causes of anxiety and mental strain should be as far as possible avoided, and great caution enjoined in the use of stimulants and narcotics. The nutrition should be maintained at its highest level by tonics, and, if need be, by electricity, massage, and hydropathy. Sometimes, besides this a special diet is advisable, for it seems beyond question that some patients have fewer headaches if they abandon all animal food, while others—whether because of a gouty tendency is not clear—do best on a nitrogenous diet with exclusion of sugar and starch.
Of the drugs used to control the liability to the attacks, the most important is cannabis Indica, given in doses of about half a grain of a good preparation of the extract several times daily for weeks or months together. Valerianate of zinc and the iodide and bromide of potassium in full doses are also recommended, but are less efficacious.
In the treatment of the attack itself, besides absolute rest and quiet, large and repeated doses of guarana or caffeine, either alone or combined with drachm doses of bromide of potassium, are sometimes of use if given at the very outset.
It is thought by some observers that ergot or ergotin is of value if the vessels are dilated, and conversely nitrite of amyl or glonoine if they are contracted. It must not be forgotten, however, in case of doubt, that the throbbing due to the latter drugs may increase the pain.
The writer has known a strong faradic current applied with the moistened hand to the back of the neck to relieve an attack, and prolonged but gentle manipulation of the painful area with the finger-tips may have a like effect if the pain is not too severe; as, for example, toward the end of a paroxysm.
Three varieties of these neuralgias may conveniently be distinguished:
1. Ordinary facial neuralgia, analogous to the neuralgias of the other superficial nerves;
2. Intermittent supraorbital neuralgia, sometimes called brow ague, though by no means always of malarial origin;
3. Epileptiform neuralgia (tic douloureux).
These varieties are of course closely allied, and have many features and causes in common.
THE ORDINARY FACIAL NEURALGIA is a painful and obstinate malady, although not so serious as the typical tic douloureux. The pain may remain fixed in one position or it may shift from one part of the face to another; and the latter is especially common in those forms which occur in anæmic or ill-nourished persons. It associates itself readily with occipital neuralgia, and sometimes also with neuralgia of the pharynx and other parts. It occurs most often in persons of neurotic tendencies or impaired nutrition, and may be provoked by disorders of the ears, teeth, and even distant organs. The possibility of aneurisms of the internal carotid or of cerebral tumor should also be borne in mind, and signs of herpes zoster and locomotor ataxia carefully sought for.
[p. 1233]The relation of caries of the teeth to neuralgia of the fifth pair forms a very important chapter, which is admirably treated by J. Ferrier.36 Opinions on this subject are conflicting and unsatisfactory, and the fact that many patients have had nearly all their teeth drawn in the vain attempt to get cured of one of the severe forms of facial neuralgia often creates an impatience of further investigation in the matter. Ferrier points out that as a rule it is not the severest cases of epileptiform tic douloureux that arise in this way, but, on the other hand, that it is a mistake to conclude, because a neuralgia is benefited by medical treatment and made worse by fatigue, exposure, etc., and because it occurs in a person of neurotic temperament, that it is not likely to be due to this form of irritation. The teeth need not themselves be the seat of pain, and the disease in them may be detected only after diligent search.
36 Les Névralgies reflexes d'Origine dentaires, Paris, 1884.
The most important lesions are said to be caries, exostosis, and other affections involving the pulp-cavity, exposure of the sensitive dentine, ulcerations of the gums, injuries caused in extraction, and other diseases of the alveolar process. The wisdom tooth, by its pressure on other roots and on the gums, is not infrequently the one at fault.
Chronic inflammation of the mucous membrane of the nose or pharynx is said to be an occasional cause of neuralgia of the face, as well as of the upper portions of the body.
THE INTERMITTENT NEURALGIA OF THE SUPRAORBITAL is an interesting affection to which too little attention has been paid. One variety seems to bear a certain relationship to migraine, inasmuch as it occurs under similar circumstances—i.e. in distinctly neuropathic individuals and families, and in attacks of about the same duration and periodicity of recurrence.
Another variety approaches the other neuralgias in the longer duration of the attacks, but is characterized by a daily seizure which recurs with absolute regularity, coming on usually at about nine in the morning and increasing in severity for an hour or so, then persisting unchanged until midday or later, when it gradually diminishes, finally disappearing in the course of the afternoon. As a rule, it is brought on by catarrh of the frontal sinuses, often following an acute attack of coryza. A certain amount of neurosal predisposition is often found in this form, and the first attacks may show themselves in early youth, rarely in the decline of life. The writer has seen one family in which a number of members in at least two generations have been attacked in this way, the seizures having been brought on by exhaustion or coryza, or both combined.
This form of neuralgia is often greatly controlled by quinine if given in sufficiently large doses (15 to 20 or 25, or even 30, grains) and as long as four hours before the attack.
Lange37 thinks the action of galvanism is remarkably successful, but the writer's experience does not fully bear this out.
37 Cited in the Centralbl. für Nervenheilkunde, etc., 1881, p. 10.
Seeligmüller38 speaks very highly of the effect of the nasal douche, used for the sake of curing the catarrh of the frontal sinuses, and potassic iodide may be useful by rendering the secretions more fluid.
38 Centralbl. für Nervenheilkunde, etc., June 1, 1880.
THE EPILEPTIFORM FACIAL NEURALGIA, OR TIC DOULOUREUX, [p. 1234] is a chronic affliction, characterized by the suddenness of onset and the severity of its paroxysms of pain, which may recur every few minutes with lightning-like rapidity, either spontaneously or brought on by motion of the jaw or the taking of food, and disappear again as quickly. After a group of such paroxysms as this there may be an intermission of some hours or days. During the attack the patient is apt to rub the seat of pain with great violence. The path pursued by the darts of pain may be either in the direction of the nerve-trunks or in an irregularly inverse direction.
In spite of their sufferings, these patients may present an appearance of health. In its worst forms, and especially in advanced life, this variety of neuralgia may be incurable, and at the best it is sure to tax the care and skill of the physician. Anstie thinks that it is apt to be associated with a taint of insanity.
The best TREATMENT consists in the most painstaking attention to hygiene, in the persistent use of galvanism, arsenic, cod-liver oil, quinine, aconite (see under General Treatment), and phosphorus. Croton chloral is occasionally of service.
As a last resort, surgical measures (see above) may be appealed to, but it should be borne in mind that even when the prospect seems most hopeless the relief under medicinal and hygienic treatment may really be near at hand. Where section of nerves is without result, the operation of tying the larger vessels, the carotid or vertebral, on the affected side may be tried, and offers some chance of success.
OCCIPITAL AND CERVICO-OCCIPITAL NEURALGIAS are second only to trigeminal neuralgia in severity, though, fortunately, less common, and either is liable by extension to give rise to the other.
Neuralgic pains in the occipital region may attend Potts's disease of the cervical vertebræ; and this is especially important to bear in mind because the osseous deformity is often wanting for a long time.
The writer has known a persistent pain in this region to be due to intracranial syphilitic disease, and to cease suddenly with the advent of more serious cerebral symptoms.
CERVICO-BRACHIAL AND BRACHIAL NEURALGIAS are less often indicative of the neuropathic taint than the facial neuralgias; and, on the other hand, they are, like sciatica, relatively often due to neuritis set up by injury, amputation, strains, enlarged cervical glands, periarthritis of the shoulder,39 etc., or associated with herpes zoster. When not due to an unremovable cause the prognosis is favorable. The treatment needs no special description.
39 See J. J. Putnam, “A Form of Painful Periarthritis of the Shoulder,” Boston Med. and Surg. Journ., 1882.
INTERCOSTAL NEURALGIA is a very important form, both on account of its frequency and obstinacy, and because it is often associated both with anæmia and chlorosis and with affections of the visceral organs, especially the uterus. The distressing cardiac palpitation of neurasthenic patients often associates itself with pain in the left side, and there is an intimate connection between neuralgia of the cardiac plexus (angina pectoris; see below) and neuralgia of the intercostal and brachial nerves.
Pain in this region, often due to neuritis, may accompany acute and chronic thoracic disorders, and may be the precursor of herpes zoster. [p. 1235] Caries of the vertebræ and meningitis should be thought of, and cancer if the neuralgia is very persistent, even if it is paroxysmal in character.
TREATMENT.—Besides the general indications for treatment referred to above, it is worthy of special note that nerve-stretching has been successfully tried for intercostal neuralgia. In one interesting case seven nerves were stretched at one operation.40 The reporter discusses the surgical aspects of the operation, and points out that the nerves should be sought for, not directly beneath the rib, but behind and beneath it, and thinks that the failure to bear this fact in mind might lead to puncturing the pleura.
40 Lesser, Deutsch. Med. Wochenschr., Sto. 20, 1884.
MAMMILLARY NEURALGIA (irritable breast of Astley Cooper), though often met with in company with intercostal neuralgia, may occur entirely independently. It is sometimes bilateral, and is apt to be associated with irregularity of the uterine functions. Cutaneous hyperæsthesia is often present to a distressing degree, and small tumors of either temporary or permanent duration may make their appearance (A. Cooper), which, however, do not affect the prognosis.
There is no especially effective TREATMENT beyond what has been spoken of. Surgical interference is not especially to be recommended, though it has occasionally been useful.
LUMBO-ABDOMINAL NEURALGIA, or neuralgia of that part of the lumbar plexus which supplies the flank and abdomen and the external genital region. These neuralgias are apt to accompany those of the intercostal nerves and share in their significance.
The most important facts with regard to them are that they are intimately associated, in relation both of cause and of effect, with affections of the abdominal and the pelvic organs and of the testis. Neuralgias of the terminal branches of the lumbar plexus, the obturator and anterior crural nerves, though well recognized, are comparatively rare.
One of the chief respects in which they are important is in calling attention to the possible presence of disease of the hip-joint or of periarthritis of the hip, as well as of tumors or inflammation within the pelvis.
NEURALGIA OF THE SCIATIC NERVE is one of the most severe and common forms. While sharing in the common etiology and history of the other neuralgias, it is peculiarly prone to be due to peripheral causes, which give rise to thickening of interstitial and investing connective tissue of the nerve. The distribution of the pain may be coextensive with the whole distribution of the great and little sciatic nerve, but far oftener the patient indicates certain regions as the seat of his severest suffering; and these are especially the sacral region of one side, the neighborhood of the sciatic notch, the popliteal space, the calf, and the outer side of the foot and ankle. Not infrequently the whole course of the sciatic nerve is traced out by the darts of pain; and in this case it is the nerves which supply the sheath of the sciatic itself which are supposed to be the seat of the neuralgic process.
Sciatica is usually unilateral, but exceptionally bilateral, or attacks the two sides alternately. The tender points most often met with are at the sacro-iliac synchondrosis, the posterior border of the great trochanter, just beneath the head of the peroneal bone, below and behind the [p. 1236] external malleolus, but numerous others are likewise noted by Valleix. Sometimes no tender points can be found. Sometimes, also, it is one or more of the collateral branches of the sciatic plexus that are the seat of the neuralgia, and the distribution of the pain and of the tender points varies accordingly.
It is in sciatica pre-eminently—in part, no doubt, because of the frequency of neuritis—that disorders of sensibility of the skin are noticed, as well as muscular paresis or spasm. This anæsthesia has been studied with great care by Hubert-Valleroux and others, and it has been shown that it is often confined to limited spots, a centimeter or so in diameter, within which the loss of sensibility may be nearly absolute. Nevertheless, their functional origin is proved by the fact that under faradization they may rapidly disappear.
The duration of an attack of sciatica varies from a week or two to months or even years, and it shows a marked liability to recur, especially with changes of weather. First attacks occur pre-eminently, though not exclusively, in middle life, and oftener in men than in women, evidently because they are oftener exposed to mechanical injury and, through their occupations, to sudden changes of temperature and the like.
The occasional causes are numerous, and include sudden wrenches and jars, even if not very severe, interpelvic pressure from tumors or impacted feces, etc. Gout, syphilis, and diabetes may act as predisposing and even exciting causes, and, it is said, gonorrhœa likewise. Periarthritic inflammations of the hip-joint and varicose veins frequently excite pains in the various sciatic nerve-branches which simulate true sciatica.
As has been indicated, although sciatica may be a pure neuralgia (see under Pathology), running its course without leading to any appreciable change in the nerve, yet subacute and chronic neuritis is very common, either as a primary condition or a complication, and its presence puts a graver aspect upon the case. The pain of neuritis, when severe, is relatively constant, remittent instead of intermittent, dull rather than lancinating, increased by motion and pressure; whereas the purely neuralgic pains are sometimes relieved by movement. It is, however, doubtful whether an accurate differential diagnosis is possible (see above). It is to this neuritis that the muscular atrophy is due which is often so marked, and it may likewise give rise to various cutaneous lesions of herpetic character. The severe pain that accompanies typical herpes zoster of this region is well known.
The TREATMENT of sciatica must vary with the probable cause of the disease and its stage of progress. Diathetic taints are to be met if present, and the greatest measure of physical health secured that the circumstances possibly admit. It is a good precaution in all cases to secure free evacuation of the bowels and to guard against hemorrhoidal congestions.
As against the neuralgia itself, the proper means vary with the acuteness of the attack and the presence or absence of neuritis. For the acute stage absolute rest is almost always desirable as a prime condition. Quinine, belladonna, aconite, and turpentine in full doses should be thoroughly tried, and special reference had to the periodicity of the seizures.
Frequent and extensive but superficial counter-irritation (actual [p. 1237] cautery, blistering, ether, or chloride of methyl) is in place in this stage, and galvanism (constant current) is often of great service. It is probable that for the acute stage the prolonged use of mild currents is the best, whereas in more chronic cases the stronger, even very strong, currents, brought to bear as accurately as possible upon the nerve itself, are sometimes more useful.
Hydropathic treatment is in great repute both for acute and chronic cases, but as success in this way demands care and knowledge, the reader is referred to the special treatises.
In cases of long standing the continued application of ice-bags along the length of the limb for days together is often of excellent service, but this method of treatment is not without its dangers and needs to be carefully watched.
In chronic cases deep injections are of service, and nerve-stretching (see above) is in place.
THE VISCERAL NEURALGIAS have not received the attention which is due them both on account of their intrinsic importance and their constitutional significance. Not only are they found in common with the superficial neuralgias in the overtired and the underfed, but they point more strongly than the latter to the neuropathic diathesis, alternating with such symptoms as migraine, asthma, nervous dyspepsia, and insomnia. They occur also in the gouty and among the neuropathic descendants of the gouty, and as a result of functional and organic disorders of the viscera.
The pain of these neuralgias, though usually described as vague, ill-defined, dull, etc., yet often stirs the nervous system to its depths, causing nausea, faintness, sweating, prostration, reflex disorders of the secretions, and like symptoms.
ANGINA PECTORIS is a neuralgia probably of the pneumogastric and sympathetic nervous apparatus of the heart. The pain, which is usually of a heavy, dull, oppressive, or tearing character, and capable of rising to intense agony, is usually deep-seated, and felt to the left of the sternum and beneath the breast, often involving the left arm and side, and occasionally the left side of the face and neck, and even the leg of the same side or the right arm. It may also, as the writer has seen, be confined to the sternal region. In the case referred to this pain recurred every afternoon and evening with great regularity. Sometimes instead of pain the arm may be the seat of a tingling numb sensation only.
During the attacks the action of the heart may continue unchanged, or it may become slow and feeble or intermittent, yet without necessarily being the seat of organic disease. The onset of anginic attacks is usually, but by no means always, sudden, and their duration is commonly short. All the features of the attack, however, are subject to considerable variation, and nervous symptoms of a variety of kinds, which it is not necessary to detail, may precede or attend the seizure. In severe attacks the patient's anguish and prostration are extreme; the face and extremities become pale and cold, and a cold sweat breaks out.
In a large proportion of cases, especially the severest ones, these neuralgic attacks are associated with organic disease of the heart or blood-vessels.
A variety of causes have been suggested to account for the seizures, [p. 1238] prominent among which is a widespread contraction of the arterioles, bringing a sudden strain upon the left ventricle of the heart. This theory is especially noteworthy because of the success which has attended the treatment by nitrite of amyl, which brings on a rapid vascular relaxation. In other cases spasm of this kind is manifestly absent. Fraenkel41 has recently defended the view that a momentary paralysis and over-distension of the left ventricle is the exciting cause. In other cases all sign of arterial or cardiac disease is and remains absent.
41 Zeitschr. für klin. Med., 1882.
In this latter group the tendency to the attacks may cease under appropriate hygienic treatment. Thus, in an instance known to the writer a lady of usually good health suffered for several months from slight attacks of præcordial pain, with pain or a sense of numbness in the left arm, and often a feeling of breathlessness on very slight exertion. This condition had manifestly been brought about by prolonged physical and mental strain, and disappeared completely after a period of rest. Other such cases are described by Anstie, Allbutt,42 and others.
42 London Lancet, 1884, i.
In judging of the significance of anginic attacks in a given case the signs of circulatory disease should first be studiously sought, and especially, as more likely to escape notice, indications of cardiac enlargement or weakness, or of increased vascular tension, or of chronic nephritis.
Dull pains in the intervals of the attacks are also regarded as important, as indicating the presence of neuritis of the cardiac nerves, which without doubt often exists. On the other hand, as pointing rather to a neurotic origin of the symptoms, a tendency, individual or inherited, to neuralgias of other forms, to asthma, migraine, and the other neuroses, is to be looked for.
Heredity plays a certain part in the etiology, and among the special causes of the non-organic form abuse of tobacco is said to be important.
The TREATMENT would be likely, of course, to be widely different according to the nature of the case, being on the one hand addressed to the circulatory apparatus, on the other to the health of the nervous system, in both cases following well-known lines.
In the treatment of the individual attacks the diffusible stimulants and the narcotics are of value when there is time to employ them. With regard to nitrite of amyl and the longer-acting nitro-glycerin, which have given so much relief in some cases, it would be premature to confine their use to the cases of demonstrable vascular spasm or even organic disease, and they are fair agents for trial in the apparently non-organic cases as well.
A patient of Romberg's used to get great relief from swallowing pieces of ice.
When the attacks are long continued or frequent, electricity, either as galvanism or by the wire brush, is applicable, and also counter-irritation over the chest, even by vesication.
GASTRALGIA (syns. gastrodynia, cardialgia, gastric colic, cramp of the stomach, etc.) may be associated with organic disease of the stomach or may occur as an independent neurosis. It is met with in individuals and families in which asthma, migraine, gout, etc. are found. In general it is common in persons of nervous, mobile temperament, and is moreover apt to point to temporary exhaustion from some cause, though this is by no [p. 1239] means always true. The writer has seen several sensory disorders of this class at the period of life of which the menopause is the chief feature. The pains of apparently hypochondriacal patients doubtless belong sometimes in this group.
The pain of gastralgia is felt primarily at the epigastrium, whence it may radiate upward and backward along the œsophagus and through into the back, as well as laterally in various directions. Allbutt says that it is sometimes associated with anginiform attacks.
Other associated symptoms are dyspnœa, prostration, faintness, coldness of the extremities, or reflex changes in the action of the heart, which may beat feebly, rapidly, and irregularly, or more slowly than normal.
Apropos of the relation of gastralgia to organic disease, it is important to recall the fact that some of the organic diseases of the stomach, notably chronic ulcer and cancer, may fail to reveal their presence by any physical sign. In a case seen by the writer a cancerous growth had invaded the entire stomach, causing an enormous thickening of its walls, yet no tumor was to be felt, and the most marked symptoms were gastralgia and exhaustion.
The relations of gastralgia to the other purely functional disorders of the stomach are interesting and peculiar. It is beyond a question that every variety of digestive disorder, from simply delayed and painful digestion to pyrosis, the formation of gas, and constant vomiting, is much more often of purely neurotic origin than has been supposed.
The DIAGNOSIS of catarrhal gastritis as distinguished from nervous dyspepsia is indeed often difficult or even impossible. Leube has recently recorded a case where the matter vomited during life contained fungoid growths, such as are usually considered pathognomonic of gastritis, and yet at the autopsy the mucous membrane appeared perfectly healthy.
With these nervous disorders of digestion, which are by no means confined to hysterical patients, gastralgia may be variously associated, or it may occur independently of them all, or vice versâ. On the other hand, digestion may be attended with a sense of discomfort, often amounting to severe pain, yet without regular outbreaks.43 This symptom is classified by Allbutt as a hyperæsthesia of the stomach rather than as a neuralgia, but from this to true gastralgia there is only a sliding scale of difference. Sometimes a persistent neuralgic habit is set up by a local disorder which itself passes away entirely.
43 Allbutt, loc. cit.
TREATMENT.—In acute attacks the aim is simply to relieve pain by whichever of the well-known methods promises the best. The real field for thought and care is in the treatment of the underlying states—first, those which, like gout, anæmia, syphilis, or nervous debility, predispose to the attacks; second, the local or special conditions which act as exciting causes. Sometimes it will be found that such patients have special idiosyncrasies with regard to the nature of food or time of meals.
In that condition of the system which is indicated by frequent or paroxysmal excess of uric acid in the urine a long-continued use of Vichy water or lithia is sometimes of service. If it be finally concluded that the stomach is in an hyperæsthetic, not in an inflamed, condition, it may not be advisable to diminish the amount of food, but, on the contrary, by one means or another, to increase it.
[p. 1240]NEURALGIA OF THE UTERUS AND OVARIES.—Attention has repeatedly been called to the fact that affections of these organs may excite neuralgias in distant parts of the body or in the lumbo-abdominal nerves; but besides these the uterine and ovarian nerves themselves sometimes are the seat of neuralgia, and it is claimed that menorrhagia and metrorrhagia may occur as a consequence.
The other abdominal organs and the testis are occasionally the seat of neuralgic pains, and attacks which involve the liver may be followed by swelling of the liver and by jaundice.
It is not always easy to assert with confidence whether an attack of abdominal neuralgia affects the external or the visceral nerves.
NEURALGIA OF THE ANUS AND RECTUM is a well-marked and painful affection, and the tendency to it may be hereditary. The seizures themselves may come on spontaneously, especially after fatigue, or may be excited by slight irritations, such as the passage of hardened feces, or may follow seminal emissions. The pain may be accompanied by quick, clonic spasm of the perineal muscles.
The rapid injection of hot water into the rectum often at once relieves the attack.
We have not space to discuss at length the neuralgiform affections of the joints and muscles and those due to the metallic poisons and other causes which do not follow the course and distribution of special nerves.
In accordance with the belief which we have expressed, that neuralgic attacks are not always of the same nature, but are the manifestations of many different conditions, we should be inclined to include many of these irregular affections under the neuralgias instead of classifying them apart, as Anstie and most writers have done. Thus, a patient of the writer, a gentleman of middle life, who has had migraine since childhood and belongs to a neuropathic family, suffers on the slightest exertion from violent pain in both thighs, which comes on very gradually, beginning at the knees and spreading upward, eventually passing away after a night's rest. One might diagnosticate this as myalgia if he confined himself to topographical considerations, but the history of the patient and the regular march of the attacks point to a different conclusion.
DEFINITION.—In the term vaso-motor and trophic neuroses it is intended to include a number of forms of disturbance of circulation and nutrition which are caused by disorders of the nervous system. Such disturbances may occur in any part of the body. They are not to be regarded as distinct diseases, but rather as symptoms of lesions in the peripheral or central nervous system. They may present themselves in various forms, as hyperæmia or anæmia or instability of vascular tone, as atrophy or hypertrophy or disintegration of normal tissue. Their consideration cannot, however, be assigned to any previous department of this volume nor relegated to various divisions of it; partly because in some cases they are to be traced to lesions of the sympathetic system, not elsewhere considered; partly because of our ignorance as to the exact location in many cases of the lesion of which they are manifestations.
It is probable that at a future time this chapter will disappear from a system of medicine, as the chapter on ascites has disappeared, and that the symptoms under consideration will be distributed among various departments as symptoms of ascertained lesions in various organs. For the present, however, they demand a separate discussion.
It is not possible to distinguish accurately in all cases between the vaso-motor and the trophic neuroses, for while in many features they are distinct, in a large proportion of cases they occur together. But it is not possible to ascribe all trophic changes to vascular disturbance, nor all vaso-motor changes to a defect or excess of trophic action. Hence a separate consideration of these allied subjects must be given. It is always to be remembered, however, that each may give rise to the other, and that in their pathology they are closely connected. Vaso-motor disturbances manifest themselves (1) by a dilatation of the vessels, producing redness, heat, and rapid metabolism in the part affected; or (2) by a contraction of the vessels, causing pallor, coldness, and malnutrition; or (3) by an alternation of these conditions and consequent temporary disturbance of function. Trophic disturbances may occur in consequence of such increase or decrease of blood-supply, or independently of any vascular change, causing (1) an abnormal production of tissue in an organ, or (2) a decrease in the size and number of its constituent cells, or (3) an actual degeneration of the elements which make it up, after which their place may be taken by another kind of tissue. Under all these circumstances the function of the part affected will be disturbed, and symptoms will be produced which will vary with the tissue or organ involved. Hence a [p. 1242] general consideration of these symptoms must be given. Before proceeding to a detailed consideration of these neuroses it is necessary to review the physiology of the vaso-motor and trophic systems, in order to make clear the manner in which they perform their functions. And inasmuch as the pathology of these affections is best understood by comparison with experimental lesions made by physiologists in investigating their function, it will be treated together with their physiology.
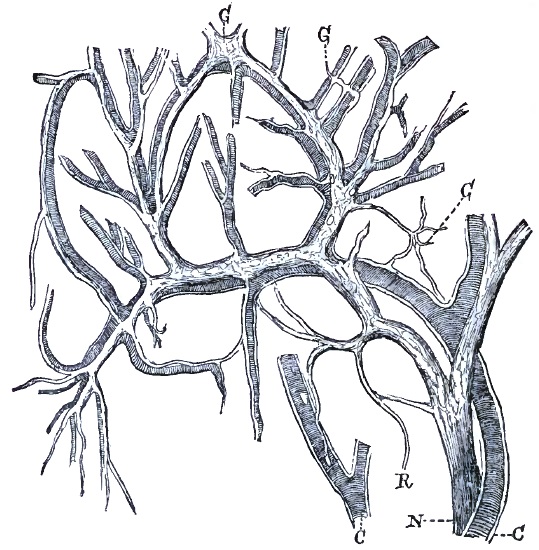
PHYSIOLOGY.—Local Vascular Tone.—Since changes in the force and frequency of the heart's action, and variations in the total amount of blood in the body, affect the body as a whole, the state of circulation in any one organ or part must be dependent upon the degree of contraction or dilatation of its own vessels. This is known as the local vascular tone. It is under the control of a system of nerve-ganglia with their subservient fibres which are found in the middle coat of all arterioles (Fig. 56). The energy expended by these ganglia is manifested by a constant moderate contraction of the circular muscular coat of the artery—a contraction which is as constantly opposed by the dilating force of the blood-pressure within the vessel. An exact equipoise between these two forces never occurs, since each varies constantly, but in a state of health one never becomes permanently excessive. Considerable variations, however, in the local [p. 1243] vascular tone are frequently observed. Thus each organ is influenced to a certain degree by every other, since an increase of blood in one part must involve a decrease in all other parts, the total amount of blood in the vessels being constant. Alteration in the heart's action is felt more quickly in some organs than in others, and thus the general blood-pressure by its variations may cause secondarily a disturbance of local vascular tone. The variations now under consideration, however, are not of this kind. They are such as are produced by influences acting directly upon the ganglia in the vessel-walls.
Local irritation is such an influence, and it may excite the ganglia to increased activity, so producing a contraction of the vessel and consequent pallor; or it may suspend the action of the ganglia, so producing a dilatation of the vessel and consequent flushing.
Another influence is irritation acting from a distance and conveyed to the local ganglia by nerve-fibres. These nerve-fibres can be distinguished from all others by their structure, being non-medullated, and by the fact that they have an indirect course, passing from the central nervous system to the sympathetic ganglia, and from these to the local ganglia in the vessels. The impulses sent along these nerves may affect the local ganglia in one of two ways, and either cause contraction by exciting the ganglia, or dilatation by inhibiting the action of the ganglia. The result produced has determined the names given to the impulse, to the fibre transmitting it, and to the centre whence the impulse proceeds, and hence vaso-constrictors and vaso-dilators are distinguished from one another.
The history of the development of the sympathetic nervous system,1 as well as its gross anatomy, affords distinct proof that it is not an independent system, as Bichat supposed, but is closely connected in its physiological action with the spinal cord and brain. Impulses which reach the sympathetic ganglia from a distance along the vaso-constrictor or vaso-dilator fibres originate in the central nervous system. The nervous mechanism which controls the local vascular tone is therefore a complex one, consisting not only of the set of local ganglia connected with larger sympathetic ganglia, but also of centres in the spinal cord connected with higher centres in the brain. The brain-centres in turn are complex, consisting of an automatic mechanism in the medulla regulating the action of all the subordinate parts below it, and of a series of cortical centres whose function it is to stimulate or inhibit the medullary mechanism. It therefore becomes evident that local vascular tone may be modified by local causes acting on the ganglia in the vessels—e.g. cold or heat; by changes in the sympathetic ganglia—e.g. the hyperæmia of the face in lesions of the cervical ganglia; by reflex action through the spinal cord—e.g. pallor produced by pain; by reflex action through the medulla oblongata—e.g. glycosuria following sciatica; or by conscious or unconscious impulses coming from the cortex—e.g. the blush of shame, the vaso-motor paralysis of hemiplegia.
1 W. R. Birdsall, “Embryogeny of the Sympathetic System,” Arch. of Med., vol. i. where a bibliography of the subject is to be found.
Vaso-constrictors.—Such a mechanism, however complex in structure, would be easily comprehended if the constant manifestation of energy in the maintenance of arterial tone had its only source in the action of the local ganglia in the vessels, and was affected only occasionally by impulses [p. 1244] from a distance, as has been thus far supposed. This, however, is not the case, as has been demonstrated by a series of experiments beginning with the brilliant researches of Claude Bernard. The classical experiments of the French physiologist were made upon the sympathetic cord in the neck of a rabbit. Division of this was found to produce a dilatation of the vessels of the ear. Irritation of the peripheral end of the divided cord produced a contraction of the vessels. Division of the spinal nerves connected with the cervical sympathetic and of their anterior roots, or irritation of the cut ends, produced effects similar in character to those caused by division or irritation of the cervical sympathetic. Destruction of the spinal cord in the lower cervical region, or division of the cord at any higher level up to the medulla, was followed by dilatation of the vessels. If the segment of the divided cord just below the section was irritated the vessels contracted. Destruction of the medulla at the calamus scriptorius and above it for three centimeters produced a general dilatation of all the vessels in the body, but division above this level had no effect. The initial congestion produced by these various experiments was accompanied by a rise of temperature in the part. It was followed after a time by a partial recovery of vascular tone, which was more complete the farther the division from the local ganglia. These facts warranted the conclusion that the energy expended by the local ganglia in holding the vessels in a state of constant moderate contraction is derived from the central nervous system, primarily from the automatic centre in the medulla, which in turn is reinforced by each of the secondary centres in the spinal cord and sympathetic ganglia; and also that while the medullary centres control the entire body, the cord and sympathetic centres control only those parts with which they are especially related. In order, therefore, to the maintenance of normal vascular tone the local ganglia must be intact, and they must be in connection with the sympathetic ganglia; these must be active, and must be connected with the spinal cord; the cord must be normal, and its tracts from the medulla must be capable of conduction; the medullary centre must be active, and not hindered or spurred by cortical impulses of a conscious or unconscious nature. Any injury to one or more of these parts will produce a vascular dilatation by interfering with the transmission of vaso-constrictor impulses from within outward, and any irritation of one or more of these parts may cause a contraction of the vessels by increasing the normal stimulus sent to the local ganglia by the vaso-constrictors.
Vaso-dilators.—The action thus far considered has been wholly of a vaso-constrictor kind, and the dilatation which has been mentioned has been due to cessation of the constrictor energy normally passing outward. This may be termed a passive dilatation. It is the kind produced by division of any one of the sympathetic ganglia or cords. But further experiments have shown that another kind of dilatation may be produced, traceable not to a mere cessation of constrictor impulses, but to an impulse of a positive kind sent to the local ganglia and resulting in a sudden suspension of their activity. Such an impulse is really an inhibitory impulse arresting the action of the ganglia in spite of the continued stimulus sent to them from the central nervous system. Its result is a dilatation of the arteries, produced by the blood-pressure within them, which may be termed an active dilatation. Thus, Bernard [p. 1245] found that irritation of the chorda tympani caused an immediate flow of blood to the submaxillary gland because of the dilatation of its vessels. And Dastre and Morat2 have demonstrated a similar effect in the head and extremities after irritation of portions of the cervical sympathetic and of the peripheral nerves.
2 See Archives de Physiologie, “Vaso-dilateurs,” 1879, 1880, 1882; Comptes rendus de l'Academie des Sciences, 1880, pp. 393 and 441.
Much confusion has arisen from the use of the term active dilatation, and many explanations of its mechanism have been offered. At first it was supposed that a system of longitudinal fibres in the vessel-wall acted as opponents to the circular constrictor fibres. This theory, originating with Stilling and Duchenne,3 has been lately revived by Anrep and Cybulski.4 They hold that since a vessel elongates as well as dilates with every heart-beat, its total distension is the result of two factors—viz. transverse and horizontal distension. If one of these is neutralized, they claim that the other will be increased. Longitudinal fibres in the wall by preventing elongation may thus allow the entire force of the heart to be expended in dilating the vessel. This theory has not, however, been accepted, and with that of Schiff, that contractile elements of the connective tissue surrounding the vessel-walls could pull outward the walls and thus dilate the vessel, has lapsed, because of lack of demonstration of the necessary anatomical structure in all arterioles. Another theoretical explanation, that dilatation of the arteries is caused by contraction of the veins damming back the blood, is disproved by the fact proven by Dastre and Morat, that blood-pressure increases instead of diminishing in the veins during vaso-dilator action. Legros5 and Onimus,6 noticing the normal occurrence of a peristaltic motion of centrifugal direction in the arteries of the retina, which if increased produced a certain degree of hyperæmia, attempted to explain the phenomena of dilatation by supposing a sudden increase of peristalsis. But Vulpian has proved that the peristalsis is both too slight and too slow in its effects to account for the rapid action of the vaso-dilators, and Dastre and Morat have shown that the peristalsis, not being synchronous with the heart-beat, really impedes the flow of blood. The last theory to be mentioned has a chemical basis, and is known as the theory of attraction (Brown-Séquard, Severini.) According to this, the organs, when active, manifest increased metabolism, to maintain which the blood is drawn toward them by the chemical changes in progress. This theory was based on the fact that irritation of the chorda tympani causes an increased secretion of saliva as well as a congestion of the submaxillary gland. It is now known, however, that these two acts are independent of each other, as either can be suspended while the other continues. Hence this theory too has lapsed.
3 Von Recklinghausen, Handbuch der Pathologie des Kreislaufs und der Ernahrung, 1883, where a full bibliography is to be found.
4 St. Petersburg Med. Wochenschrift, 1884, i. 215.
5 Des Nerfs vaso-moteurs, Thèse de Concours, Paris, 1873.
6 Des Congestions actives, Paris, 1874.
The view already stated, that vaso-dilators act by inhibiting local ganglia which cause contraction, is now accepted, especially since it is found that such inhibitory activity is constantly displayed by other parts of the nervous system, and is competent to explain the facts. The active dilatation produced by the inhibition of the action of the local ganglia is [p. 1246] therefore to be clearly distinguished from the passive dilatation caused by the cessation of normal tonic impulses sent to them from higher centres. The former is a positive active vaso-dilator phenomenon. The latter is a negative paralytic vaso-constrictor phenomenon. The former is more effective, the dilatation being greater in degree and more permanent than the latter, and resembles exactly the dilatation produced experimentally by exhaustion of the activity of the local ganglia by over-stimulation of the constrictors.7
7 Goltz, Arch. f. d. gesammt. Physiol., xi. 92.
An important point of contrast which has been established between vaso-constrictor and vaso-dilator impulses is that while the former are constant the latter are intermittent. Hence they cannot be regarded as opponents of one another. In a normal quiescent state vaso-constrictor energy is always being supplied to counteract the continued intravascular pressure ever renewed with the cardiac systole. The vaso-dilators are inactive. In an organ thrown into functional activity an increased flow of blood at once takes place, proportionate to the work being done by the organ. Such a functional hyperæmia might be produced either by a cessation of constrictor impulses or by an inhibition of their effects. It is by the latter means and through the vaso-dilators that it is produced, and it is probably the chief function of the vaso-dilator nerves to regulate the blood-supply in accordance with the need of a part. For this reason these nerves have been supposed to pass with the motor nerves to the muscles. As few organs exist without a possible use, it is probable that vaso-dilators pass to all parts of the body, as Vulpian asserts, though they have not been demonstrated in every organ or every part.
Like the vaso-constrictors, the vaso-dilators can be traced to the spinal cord, and their centres there are governed by a general centre in the medulla, which in turn may be affected by impulses from the cortex. A destructive lesion in any part of the vaso-dilator system does not produce as marked effects as one involving the vaso-constrictor system, since the symptoms of such a lesion will only appear when the vaso-dilators are called into play. When the vaso-dilator nerve to the submaxillary gland is cut, no change is observed until by some sapid substance put in the mouth its function should be excited, when the gland is no longer found to flush with blood as in the normal state. It is by means of the vaso-dilators that erectile organs become engorged with blood. Eckhard has shown the nervi erigentes of the penis to be vaso-dilator nerves. If they are destroyed, the organs will not respond to the wonted stimulus—a symptom which, however, would only be noticed at intervals. An irritative lesion of the vaso-dilator system may produce permanent congestion of an organ or part, but this seems to be rather more rare than a congestion from paralysis of the constrictors. It is seen in injuries of the peripheral nerves.
Origin of the Vaso-motor Nerves.—The exact course of the vaso-constrictor and vaso-dilator nerves has been traced from various parts into the central nervous system by the careful experiments of Dastre and Morat,8 and more recently by Gaskell.9 It is now established that they [p. 1247] exist as separate nerves, although they often run together, and that they usually enter the spinal cord at different levels.
8 See Comptes rendus Soc. de Biologie, and Arch. de Physiol., 1879-84.
9 W. H. Gaskell, “On the Structure and Function of the Nerves which Innervate the Vascular System,” Journ. of Physiol., Jan., 1886.
If the various spinal nerves be cut singly from above downward, and the effects noted, and if the peripheral ends be irritated and the effects noted, and if with proper care the results be analyzed and compared, it will be found that the anatomical connections of the segments of the spinal cord with the sympathetic ganglia, which are so evident at each level, are not the ones by which physiological impulses pass out at that level. The vaso-constrictors of the head, which can be traced to the superior cervical ganglion, do not come from the upper cervical region of the cord, as might be supposed from the connections of that ganglion, but from the first three dorsal nerves. They reach the ganglion through the sympathetic cord in the neck, having traversed the inferior cervical ganglion on the way. There are vaso-constrictors in the cranial cavity which accompany the third, fifth, seventh, and twelfth nerves to the eye, face, and mouth. It is still undecided whether they originate in the cord and medulla, issue in the spinal accessory nerve, and with it enter the cranium (Gaskell), or reach those nerves by way of the carotid and vertebral plexus from the inferior cervical ganglion (Dastre and Morat). The vaso-constrictors of the arm, which can be traced to the inferior cervical and upper thoracic ganglia and to the thoracic sympathetic cord, are derived from the seven upper dorsal nerves. It is true that division of the roots of the brachial plexus causes a slight dilatation of the vessels of the arm, but this is so much increased when the dorsal nerve-roots are divided that it is evident that it is through them that the constrictor fibres chiefly pass. The vaso-constrictors of the leg, which can be traced into the second and third lumbar ganglia and lumbar sympathetic cord, are derived from the five lower dorsal and first lumbar nerves, and only join the crural and sciatic nerves after passing through the abdominal sympathetic. The thoracic viscera are probably supplied partly through the branches of the inferior cervical and thoracic ganglia, and partly through the pneumogastric, the latter statement being disputed by Gaskell. The abdominal viscera are supplied partly through the splanchnic nerves, which are made up of fibres issuing from the cord in the fifth to the twelfth dorsal nerves inclusive, and partly through the pneumogastric. Thus the dorsal region of the cord is the origin of the majority of vaso-constrictor fibres in the body.
The origin of the vaso-dilators is also to be traced to the dorsal cord. The vaso-dilators of the bucco-facial region come from the second to the fifth dorsal nerves, whence they pass to the first thoracic ganglion, and thence by the annulus of Vieussens into the cervical sympathetic cord. Those of the eye, head, and ear come from the same ganglion, but have their spinal origin in the eighth cervical and first dorsal nerves. Those of the arm are traced into the upper thoracic sympathetic cord, which they reach from the five upper dorsal and last cervical nerves. Those of the leg are traced to the first and second lumbar ganglia and the lumbar sympathetic cord, which they reach from all the dorsal nerves from the sixth downward. Gaskell holds, however, that the vaso-dilators of the extremities pass out of the cord in the cervical and lumbar plexuses and accompany the cerebro-spinal nerves. The vaso-dilators of the thorax and [p. 1248] abdomen are supposed to pass in the pulmonary plexus and splanchnic nerves, but this is not yet fully determined.
Gaskell10 believes that vaso-motor nerves can be distinguished from motor and sensory nerves in the spinal nerve-roots by the smallness of their calibre. He finds such fine fibres only in the spinal nerve-roots between the second dorsal and second lumbar segments of the cord (in the dog), and in the three upper roots of the spinal accessory nerve. According to his account, the vaso-constrictors issue from the spinal cord in both anterior and posterior nerve-roots as medullated fibres, and pass to the sympathetic ganglia lying on the vertebræ (proximal or lateral ganglia); there they lose their medullary sheath, and either end in cells whence new fibres issue, or more probably pass directly onward as non-medullated fibres, having a connection with the unipolar cells of the ganglia only for purposes of nutrition. The number of fibres issuing from any one ganglion is much greater than the number entering it from the cord; hence it is supposed that each medullated fibre splits up into a group of non-medullated fibres; which is possible, as the researches of Ranvier have shown that each axis-cylinder is made up of numerous fibrils. Leaving these ganglia, the nerves pass either to the second series of ganglia (distal or collateral ganglia), whence they issue in plexuses to enter the vessels, or to the vessels directly, where they divide in plexuses. It is in the meshes of the plexus that the local ganglia of the vessel-walls are found. The vaso-dilators are thought to differ from the vaso-constrictors in passing directly to the distal ganglia as medullated fibres, not being connected in any way with the proximal ganglia. Gaskell makes no statement regarding their limits of origin from the cord, except to state that the nervi erigentes issue with the sacral nerves. He agrees with the view that the vaso-dilators act as inhibitory nerves upon the local ganglia.
10 Journal of Physiology, Jan., 1886.
Vaso-motor Reflexes.—Thus far, reference has been made only to fibres whose direction of transmission is centrifugal, and whose exit from the spinal cord is by the anterior nerve-roots. There are other fibres, however, through which centripetal impulses pass, and these enter the spinal cord with the posterior nerve-roots. The function of these fibres is to transmit sensory impulses inward to reflex centres, and thus set in action motor mechanisms of a vaso-constrictor or dilator kind whose effects are produced at the periphery. There are, therefore, vaso-motor reflexes, as well as skin and tendon reflexes, whose centres are in the spinal cord. These reflex acts may be excited by impulses reaching the centre not only through the vaso-motor centripetal nerves, but also through the sensory nerves of the cerebro-spinal system. The effect of changes of temperature on the circulation in the skin (if the right hand be plunged in cold water there is a fall of temperature in the left hand), the effect of pain upon the color of the face and the size of the pupil, the red cheek on the affected side in pneumonia, the occurrence of glycosuria during sciatica,—are all instances of such reflex acts. Many vaso-motor affections are produced by irritation causing reflex effects at a distance from the seat of irritation—a fact always to be kept in mind. The utility of counter-irritation to the surface in diseases of the internal organs is explained by supposing that vascular changes are produced in those [p. 1249] organs through reflex mechanisms set in action by the local irritation. While some of these reflexes may have their central mechanism in the local ganglia, it is probable that the majority are to be traced to the spinal cord. It is believed that the sympathetic ganglia are not the seat of reflex centres.
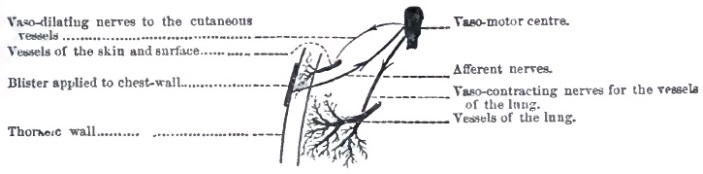
Since the vaso-motor nerves are connected almost exclusively with the dorsal portion of the spinal cord, it is very natural to conclude that the vaso-motor reflex centres are situated in this region; and the hypothesis has been advanced by Jacubovitch, and strongly urged by Gaskell,11 that the cells of the vesicular columns of Clarke, which are peculiar to this region, are the seat of these reflex mechanisms. This hypothesis gains some support from the pathology of syringo-myelia. In this disease the gray matter surrounding the central canal and the vesicular columns are destroyed. The characteristic symptoms are vaso-motor and trophic disturbances, consisting of changes in the vascular tone, changes of local temperature, and various eruptions, in some cases going on to ulceration in the skin and mucous membranes. It is, however, undecided whether the vaso-motor centres of the cord are limited to the columns of Clarke, or are situated in the gray matter surrounding the central canal, since both these parts are destroyed in this disease.12 That they are not located in the anterior or posterior gray cornua is determined by the fact that diseases limited exclusively to these areas do not cause vaso-motor disturbances. The situation of the various reflex centres for the various parts of the body is at different levels of the cord, as has been determined by the experiments already cited to establish the level of origin of the vaso-motor nerves. The exact location of the vaso-constrictor and vaso-dilator reflex centres for definite parts is yet to be ascertained.
11 Loc. cit.
12 See Fürstner, Arch. für Psych., xiv. 422.
Vaso-motor Tracts.—These reflex centres are connected with the medulla by tracts which lie in the lateral columns of the spinal cord,13 although it is not determined in which part of these columns. It is not possible as yet to separate the constrictors from the dilators in this tract, nor to determine whether it transmits impulses in both directions or only from above downward. Nor is the course of associating fibres between reflex centres at different levels known. In cases of transverse myelitis the control of the medulla is removed from the vascular centres below the lesion, and the lack of vascular tone seen in the paralyzed limbs, together with the susceptibility to local irritation, is the result of this division of the vaso-motor tracts.
13 “Owsjanikow and Tschirijew,” Bull. de l'Acad. de St. Petersbourg, xviii. 18.[p. 1250]
Medullary Centres.—It has been stated already that a general vaso-motor centre with both constrictor and dilator powers is situated in the medulla. This lies in two divisions on each side of the middle line, in or just beneath the floor of the fourth ventricle, from the calamus scriptorius up to the level of the sixth nerve-nucleus. Each division governs the vascular tone of its own side of the body,14 and lesions in its region in man produce unilateral vaso-motor symptoms.15 This centre can be excited to reflex action by strong irritation locally or through the blood, in which case a general constriction or dilatation of the vessels of the entire body will ensue. It seems probable, however, that the general centre in the medulla is made up of a number of special centres, each of which governs a definite set of organs. The vascular tone of the thoracic and abdominal viscera is certainly regulated by a series of such centres. Brown-Séquard and Schiff have produced hemorrhages in the lungs, pleura, stomach, intestines, and kidneys at different times by destructive lesions of the medulla, and the well-known experiments of Bernard, in which by puncture of the medulla local hyperæmia of the liver or kidneys was caused, producing glycosuria or polyuria, confirm this view. Lesions of these parts in man produce similar effects. Charcot has shown that in cerebral hemorrhage ecchymoses may be found in the stomach, pleura, and endocardium, and that pneumonia is especially frequent upon the paralyzed side. De Jonge16 has been able to collect thirteen cases of diabetes mellitus in which a lesion of the medulla (hemorrhage or tumor) was found after death; and Flatten17 has proven the existence of similar lesions in diabetes insipidus. The connection of these centres with the liver and kidneys has been traced elsewhere.18 The medulla contains a special centre for the vaso-motor nerves of the abdomen, which are in the domain of the splanchnic nerves. This centre is excited reflexly by impulses reaching it through the depressor nerve of Cyon from the heart; so that when that organ is overburdened it may be relieved by a fall of arterial pressure produced by dilatation of the abdominal vessels. Whether the connection of the medulla with the centres in the semilunar ganglion which preside directly over these vessels is made by way of the spinal cord or by way of the pneumogastric nerve is still undetermined, though the researches of Gaskell favor the former view. Gastric and intestinal disturbances are certainly produced by nervous lesions in the medulla, but whether they are due to vascular changes is uncertain. The vomiting of mucus and blood, and the large watery evacuations which accompany mental shock or anxiety, as well as the polyuria associated with mental effort, have been ascribed to irritation of local centres in the medulla governing the gastro-intestinal and urinary organs by impulses received from the cortex above. The spleen is under the control of vaso-motor centres, since section of the splenic branches of the semilunar ganglia will produce a great enlargement of the organ, and irritation of the cut end of these branches will produce [p. 1251] contraction.19 The medulla also contains a vaso-dilator centre for the erectile tissues of the genital organs, irritation of which by mental action or local disease causes impulses to pass to the nervi erigentes by way of the spinal cord, resulting in a flow of blood to the parts. Although a centre has been thought to exist controlling the circulation in the lungs, whose paralysis has been supposed to explain the occurrence of sudden pulmonary œdema without other known cause, no definite facts regarding it are known. That the action of the heart is under the control of the medulla is a fact too well known to require more than a mention. The physiology of the nervous control of the heart cannot be discussed here.
14 Owsjanikow, Arbeiten aus d. Physiol. Instit. zu Leipzig, 1871.
15 M. A. Starr, “Sensory Tract in Central Nervous System,” Journ. Nerv. and Ment. Dis., July, 1884, pp. 396-398.
16 Arch. f. Psych., xiii.
17 Ibid.
18 See Tyson, “Diabetes Mellitus,” Pepper's System of Medicine, Vol. I. p. 195; Edes, “Diabetes Insipidus,” ibid., Vol. IV. p. 30.
19 Tarchanoff, Pflüger's Arch., viii. p. 97; Ross, Diseases of the Nervous System, vol. i. p. 225.
While these medullary centres are certainly influenced by impulses reaching them from the cerebral hemispheres, as is evident from the vaso-motor symptoms produced by mental action—e.g. pallor from fright, blushing, etc.—it is impossible to state in what portion of the hemispheres in man the higher vaso-motor centres lie. Eulenburg and Landois locate them in the motor area in animals.20 They are certainly beyond control of the will, and are wholly reflex in their action, a purely mental act in this case being the excitant of a purely physical result.21
20 Arch. f. Path. Anat., Bd. lxviii. p. 245.
21 In addition to the articles already cited the reader is referred to Landois's Physiology, to Duval's article, “Vaso-moteurs,” in the Dictionnaire de Médecine et de Chirurgie, vol. xxxviii. (1885), for a summary of vaso-motor physiology, and to Gerhardt's “Ueber Angio-neurosen,” Volkmann's Sammlung klin. Vorträge, No. 209. Gaskell's researches, published in the Journal of Physiology, are the most recent and satisfactory.
PATHOGENESIS.—From this review of the physiology of the vaso-motor system it becomes evident that disturbances of vascular tone may be produced by many different causes acting upon many various parts. They may be due to local affections of the part in which the symptoms are present, as in the case of erythema22 after burns or frost-bite, or congestion of any organ after injury. They may be due to affections of the vaso-motor nerves passing to the part affected, as in the case of vascular changes due to peripheral nerve lesions.23 They may be due to affections of the sympathetic ganglia connected with the part affected, as in the case of migraine,24 sudden flushing of one ear, certain cases of polyuria,25 and Basedow's disease.26 They may be due to lesions in the spinal cord affecting the vaso-motor centres27 or compressing the nerve-roots on their way to and from the sympathetic ganglia,28 as is the case in the various forms of myelitis and in Raynaud's disease or symmetrical gangrene, and in meningitis, tumors of the cord, or Pott's disease. They may also be caused by such conditions in the cord as cut off the vaso-motor centres from the medullary centres, such as transverse myelitis from compression or traumatism.29 They may be due to lesions of the medulla oblongata,30 as is seen in some cases of polyuria and glycosuria,31 and in cases of universal erythema32 following acute fevers. They may be due to diseases of the cerebral hemispheres, as is evident from the vaso-motor symptoms occurring in hemiplegia and hysteria. Finally, they may be of a reflex [p. 1252] origin, dependent upon some obscure source of irritation in a part quite distant from the region in which the symptoms appear.33
22 Vol. IV. p. 511.
23 Vol. V., “Neuritis.”
24 Vol. V., “Migraine.”
25 Vol. IV., “Polyuria.”
26 Vol. III. p. 761.
27 Vol. V., “Syringo-myelitis.”
28 Vol. V., “Meningitis Spinalis.”
29 Vol. V., “Transverse Myelitis.”
30 Vol. V., “Medulla.”
31 Vol. I., “Diabetes Mellitus.”
32 Vol. IV. p. 512.
33 Vol. V. p. 205.
The DIAGNOSIS of the seat of the lesion in many cases of vaso-motor neurosis may be made if the organ or the exact limitation of the area affected be ascertained, and the history of the case, together with the concurrent symptoms of other kinds, be considered. In some cases no organic cause can be found, and in these a reflex cause should be diligently searched for.
SYMPTOMS.—A vaso-motor affection may manifest itself either by a spasm or a paralysis of the vessels. In angiospasm the part affected becomes pale, and irritation no longer causes a vaso-motor reflex. It looks shrunken, and if the skin over it is loose it may be thrown into folds or shrivelled, presenting the appearance seen in the hands after long immersion in hot water. The lack of blood in the part arrests the processes of metabolism which are normally constant, and if the condition continues this may result in such a disturbance of nutrition that ulceration, or even gangrene, may ensue. The local anæmia, combined with the cessation of metabolism, produces a fall of temperature in the affected part, which is then more easily affected by the temperature of the air than in a normal state, so that exposure to cold is very liable to cause freezing. These conditions necessarily produce an impairment of function, so that if the affection is located in the extremities, as the fingers, they are soon rendered useless. The term digiti mortui has been applied to this state. In the surface of the body angiospasm causes cutis anserina, pallor, numbness, tingling, slight anæsthesia, and analgesia. If it occurs in a limb, the finer motions are imperfectly performed, and in time the nutrition of the muscles may be so impaired as to produce atrophy and paresis. It may even lead to gangrene. Nothnagel has recorded34 five cases of sciatica in which the pain produced a reflex spasm of the vessels of the leg, which, persisting, resulted in partial paralysis, atrophy, lowering of temperature, pallor, and sensory disturbances. Ross mentions35 the sudden appearance of circumscribed patches on the hands and forearms of washerwomen, in which there is a pallor, coldness, and partial anæsthesia. These may be limited to the distribution of a single nerve, and may be accompanied by trophic affections.
34 Arch. f. Psych., v.
35 Vol. I. p. 221.
Spasm of the veins may occur as well as of the arteries,36 or independently of them. In the latter case the blood will not pass out of the capillaries. The part will then be blue, swollen, œdematous, and painful; the temperature will be lowered by increased radiation of heat, and all the sensations and functions be impaired in greater or less degree. If this continues, nutrition may suffer, and in the end gangrene develop, which will take its course and lead to the throwing off of the part. Grainger Stewart has described such a condition occurring in both hands and feet.37 It may be likened to a severe form of Raynaud's disease.
36 Weiss, “Symmetrische Gangrän,” Wiener Klinik, 1882.
37 Grainger Stewart, An Introduction to the Study of Nervous Diseases, p. 138.
Angio-paralysis is more frequent than angiospasm, and may be due either to paralysis of the vaso-constrictors or to excitement of the vaso-dilators. It shows itself by a bright-red or mottled appearance of the skin, and increase of local temperature, and more rapid processes of [p. 1253] nutrition, together with an increase of secretion if the part is a gland or a mucous membrane, and an increase of sweat if it is the skin. In the latter case an increased sensitiveness to changes of temperature, a subjective sensation of heat, and hyperæsthesia and hyperalgesia may occur. The hyperæsthesia on the paralyzed side which is present in hemiparaplegia spinalis is ascribed to the vaso-motor paralysis. But these symptoms soon give place to others. The dilatation of the vessels, which at first caused an increased flow of blood to the part, produces a slowing of the blood-current in the part, just as a river runs less rapidly where it becomes wider. The slowing of the current in the skin allows of a more complete cooling of the part as the radiation of heat and the evaporation of moisture are increased, and the slowness of the renewal of blood impairs the processes of nutrition, so that to the first stage of redness, heat, and increased metabolism there ensues a stage of blueness, cold, and defective nutrition, and the function of the part may be impaired. In this stage it usually presents a mottled appearance, and may be slightly swollen and œdematous, and the continued increase of perspiration gives it a clammy coldness to the touch. In all of these conditions severe pain, sometimes of a burning character, is a very distressing symptom (causalgia). These conditions are seen in peripheral nerve-lesions, and give rise to the appearances which have been so admirably described by Weir Mitchell.38
38 Injuries of Nerves.
A peculiar combination of symptoms may be mentioned here, to which Weir Mitchell has given the name of erythromelalgia.39 This disease begins with tenderness and pain in the soles of the feet, which are soon followed by a marked distension of the capillary vessels. The congestion is attended by a sensation of burning pain similar to that produced by a blister. The surface is at first of a dull dusky-red color; later it appears purple. The redness is not uniformly distributed over the sole, but occurs in patches of irregular shape, being especially frequent over prominent parts exposed to pressure and friction, and the attacks seem to be brought on by long standing or walking. At first there is a rise of temperature in the affected surface, the arteries pulsate visibly, the veins are swollen, and there may be some œdema. Later, the foot is cold and pale. Sensations of touch and temperature are normal, but the part is so extremely tender that walking is impossible. There is no paralysis. One or both feet may be affected, but the patches of redness are rarely symmetrical. The hands are occasionally affected. The condition may occur in paroxysms or may remain for some time. It resists all known methods of treatment, although applications of cold relieve the burning pain to some extent and the tenderness enforces rest.
39 Amer. Journ. of the Med. Sci., July, 1878.
With angio-paralysis may be classed the taches cérébrales of Trousseau no longer considered diagnostic of meningitis, but denoting a weakened condition of vaso-constrictor action in the local ganglia of the vessel-wall which may occur upon local irritation of the skin in any severe disease affecting the nutrition of the general nervous system.
Actual rupture of the capillaries in the course of vaso-motor diseases is rarely observed, although the stigmata appearing in hysterical and cataleptic patients may be ascribed to this cause. In this connection tabetic ecchymoses may be mentioned, which appear suddenly without local injury, [p. 1254] and resemble an ordinary bruise, running a similar course. They occur only in the course of locomotor ataxia.40
40 Straus, Arch. de Neurologie, tome i. p. 536.
In addition to these forms of vaso-motor affections there is a condition of instability of vascular tone which manifests itself by sudden transient changes in the circulation of various organs. This is a functional affection, usually due to malnutrition. It is seen in many cases of neurasthenia and hysteria, and manifests itself by sudden flushes or pallor, alternations of heat and cold, local sweating, attacks of mental confusion, and inability to use any organ continuously from disturbance of the power of the vaso-dilators to maintain a condition of functional hyperæmia.41 Little is actually known about the causes of this state of the vascular system, although much has been written about it. (For a fuller description the article on Neurasthenia may be consulted.)
41 Anjel, Arch. für Psychiatrie, xv. 618.
Many functional derangements of the internal viscera have been ascribed to such vaso-motor instability with more or less probability,42 but hypothesis of this kind, however plausible, is evidently beyond confirmation. It is especially in affections of this kind that causes of reflex irritation are to be carefully sought. Cutaneous angio-neuroses, such as have just been described, may affect any part of the body. They usually appear suddenly, producing much discomfort and an impairment of function in the part if it is an extremity. They disappear as rapidly as they come. The duration of such attacks varies from a few minutes to several days. They are very liable to recur. If it is the vessels under the control of the cervical sympathetic which are affected, the symptoms will be those of migraine or of lesion of the ganglia.43 If it is the vessels in the extremities which are involved, the condition of digiti mortui or erythromelalgia or symmetrical gangrene44 may be produced.
42 Fox, The Influence of the Sympathetic System in Disease, London, 1885.
43 See p. 1263.
44 See p. 1257.
A singular epidemic occurred in France in 1828 and 1830 which was termed acrodynia. Many persons were suddenly seized with vomiting and purging, and soon after the onset the extremities became red or mottled in blotches, swollen and œdematous, and hot, painful, and tender. The attacks lasted from a few days to two months, and during this time the skin became thick and hard, the muscles weak and subject to spasms, and the general health was impaired. Relapses occurred in many cases, but all finally recovered, and hence the exact nature of the disease was not ascertained.
COURSE.—In any case of vaso-motor neurosis the course of the disease and its termination will depend chiefly upon its cause. If the cause is some permanent lesion of the nervous system, the condition will remain, and in this case the termination will depend upon the severity of the symptoms. Angiospasm may be so severe as to lead to gangrene ana the separation of the part affected, or may be so slight as to cause only subjective discomfort and a little pallor. Angio-paralysis may lead to an extreme degree of congestion, which is attended by heat and pain at first, later by paræsthesia and coolness, with increased liability of the part to be affected by changes in the surrounding air. This stage is succeeded by one of less marked dilatation of the vessels and a spontaneous partial [p. 1255] recovery, although the more moderate symptoms may continue indefinitely and seriously impair the function of the part. If the cause is a temporary derangement of function in the vascular mechanism, is reflex irritation which can be removed, or is a curable organic disease, the symptoms will subside rapidly or gradually and perfect recovery may follow. If the condition is one of irritability in the vaso-motor centres, producing alternations of flashing or pallor, such as is observed in nervous exhaustion, it may recur irregularly for a considerable length of time until the causative condition can be removed.
PROGNOSIS.—The prognosis must be determined in each case by a consideration of the cause of the affection, of the nature of the symptoms, of the severity of the disease, and of the possibility of success in both symptomatic and causative treatment. In the angio-paralytic cases an eventual spontaneous relief from much of the discomfort may be promised, although the duration of the symptoms cannot be predicted.
TREATMENT.—Treatment must be directed primarily to removing or diminishing the severity of the cause. A review of the section on Pathogenesis will indicate how wide a field this may include, and the reader must be referred to the special articles which are alluded to in that place for therapeutic measures. Special diligence is to be shown in searching for a source of reflex irritation. When the cause cannot be reached, and when the symptoms are of such severity as to demand immediate attention, treatment may be directed to them.
In all conditions of vaso-motor disease it is important to shield the part from external injury; for if the vessels are dilated they are liable to rupture, and any abrasion of the surface may produce serious inflammation and ulceration; and if the vessels are contracted any injury will be repaired slowly and imperfectly on account of the anæmia, and may even hasten the approach of gangrene.
Perfect rest, bandaging with cotton, and even the application of a light splint to the extremities will be advisable in cases of angiospasm. It is desirable to retain the animal heat, inasmuch as its supply is deficient. In angio-paralysis rest in a somewhat elevated position and applications of mild evaporating lotions are indicated in the early stage; later, the limb may be bandaged. It is not advisable to attempt by tight bandaging to counteract the effect of the vascular paralysis, for the nutrition of the limb is liable to suffer and gangrene may be induced.
Massage of a part affected with vaso-motor symptoms is of great service, since the circulation can be increased in the veins, and thus indirectly in the capillaries, and the nutrition of the part can thus be favored. It is more efficacious in angio-paralysis than in angiospasm. Too rough rubbing is of course to be avoided, lest the skin be injured. All counter-irritation is to be strictly forbidden.
Electricity has been used with varying results. According to Erb,45 moderate faradic applications contract the vessels; strong faradic applications, especially with the brush, dilate the vessels. The galvanic current at first contracts the vessels, but this is followed by a secondary dilatation, which will be greater and occur more rapidly the stronger the current used.46 Cathodal closures contract the vessels; the anodal [p. 1256] continuous current dilates them widely. Stabile continuous currents through a nerve dilate the vessels which the nerve supplies. Inasmuch as vaso-constrictors and vaso-dilators pass together in many nerves, and are found together in all parts, it is impossible to apply electricity to either alone. In those cases, therefore, in which it has been ascertained which set of vaso-motors is affected, it is not always possible to produce a direct effect upon that set by electrical treatment. Erb recommends, in conditions of vaso-motor spasm a trial of the galvanic current, the cathode on an indifferent point, the anode being applied over the vaso-motor centres governing the part, and also over the area of the body which is affected, and held there while a moderate continuous current is passing, interruptions being avoided; or, the cathode being placed on the neck, the anode may be applied to the nerves passing to the affected part; or a strong continuous current may be sent through the nerve, its direction being changed several times during a moderately long application. Finally, the faradic brush applied to the part or a strong faradic current sent through its nerve may relax the spasm. In any case, all these methods should be tried before electrical treatment is abandoned.
45 Electrothérapie, 562.
46 To this statement Lauder Brunton assents—Pharmacology, p. 250.
In vaso-motor paralysis other methods are used. The cathode is placed on the part congested, and a weak galvanic current is employed with frequent interruptions or even with changes of the pole; or the cathode may be moved about upon the reddened skin while a mild continuous current is passing. A very weak faradic current with wet electrodes, or even a weak faradic current applied with a brush, may be of service. Here, again, various methods may be tried.
If the extremities are affected, it may be well to immerse them in a basin of water which is connected with one pole of the battery, and the current directed in the manner just described, according to the case. It must be confessed that no definite results can be predicted from the use of electricity in these cases, and much more experience is needed before definite rules can be laid down. The records show that in apparently similar cases opposite methods of application have produced favorable effects, while in other cases all methods have failed. Too much reliance should not be placed in electrical treatment. Erythromelalgia is an obstinate affection, and symptomatic treatment, directed chiefly to quieting the pain by opium and allaying the sensation of burning by cool baths, must be resorted to.
Internal remedies may be tried appropriate to the condition present. In angiospasm nitrite of amyl inhaled, or nitro-glycerin 1/100 gr. t. i. d., may give considerable relief, although both of these drugs are to be used with caution. Chloral hydrate is also of some service, and where the patient is in pain and suffers from insomnia this may fulfil several indications. In angio-paralysis ergot has been used with advantage. Oxygen inhalations are of service. Chloride of potassium may also be tried. It is evident, however, that such remedies, acting as they do upon the general arterial system, are not to be depended upon in the treatment of local conditions, since they have no selective action upon the affected part. The majority of the drugs known as sedatives and antispasmodics have been used in these conditions, but the records of individual cases show that they are not of much avail. Theoretical therapeutic measures based upon [p. 1257] experimentation on animals have been fully discussed by Lauder Brunton,47 but practical experience has not yet been sufficiently extensive to warrant any further statements.
47 Pharmacology, Therapeutics, and Materia Medica, pp. 229-360. Lea Bros., 1886.
SYNONYMS.—Local asphyxia, Asphyxie locale, Raynaud's disease; Symmetrische Gangrän.
DEFINITION.—Symmetrical gangrene is an affection of the nervous system characterized by arterial or venous spasm appearing in symmetrical parts of the body, especially in the phalanges of all the extremities, which may result in trophic changes or in gangrene. There are various stages in the disease, which have given rise to the various names by which it is known. The stage of local syncope, in which there occurs a moderate contraction of the arterioles and consequent pallor of the part, may be followed by a stage of local asphyxia, in which the complete contraction of the arterioles cuts off entirely the supply of arterial blood, and the regurgitation of venous blood produces cyanosis of the part; and this, if continued, may result in the gangrene of the part, which is then thrown off. Instead of a condition of local asphyxia, there may be a spasm of the smaller veins, resulting in a local erythema, which may go on to capillary stasis and then to gangrene. The spasm of the vessels may cease at any stage as suddenly as it began; and if this occurs in the first or second stage, no gangrene results.
HISTORY.—While isolated cases of this affection had been recorded as curiosities during the past two centuries,48 the disease was first studied with care by Raynaud in his Thèse de Paris in 1862. He collected twenty-eight cases which had been described with accuracy or had been personally observed in the hospitals of Paris, and after a thorough analysis of the symptoms defined the disease as “a neurosis characterized by an exaggeration of the excito-motor power of the cord presiding over the vaso-motor nerves.” He called particular attention to the condition of spasm in the vessels, and proposed the name asphyxie locale to designate the peculiar appearance of the parts affected. He also noticed the resulting gangrene as a new variety of gangrene, not dependent upon embolism or upon changes of an atheromatous nature in the coats of the vessels.
48 Schrader, 1629; Hertius, 1685; Bouquet, 1808; Moulin, 1830; Racle, 1859—cited in full by Weiss, “Symmetrische Gangrän,” Wiener Klinik, 1882.
The condition was at once recognized by others, and several cases had been reported prior to 1873, when Raynaud published a more complete article on the subject in the Dictionnaire de Médecine et de Chirurgie under the title gangrene symmétrique; in 1874 he recorded five new cases in the Archives générales de Médecine, vol. i. pp. 5 and 189.
The disease, having been thus established as a definite nervous affection, began to be noticed in other countries than France; and Billroth in Vienna,49 Weir Mitchell,50 Mills,51 A. McL. Hamilton,52 and J. C. Warren53 [p. 1258] in this country, and many other careful observers, published cases, together with more or less complete articles upon the disease. In 1882, Weiss produced a monograph54 upon the subject containing references to all the cases which had appeared; and this is still the most complete article to be found, although the essay of R. Lauer55 and the discussion of the disease by the Berlin Medical Society,56 as well as the short articles of Schulz57 and Lutz,58 deserve mention, for they contain additional observations of cases and numerous facts not to be found elsewhere.
49 Wiener Med. Wochensch., 1878, No. 23.
50 Amer. Journ. of the Med. Sci., 1878, July.
51 Ibid., 1878, Oct.
52 N. Y. Med. Journ., 1874, Oct.
53 Boston Surg. and Med. Journ., 1879, No. 3.
54 Weiss, Wiener Klinik, 1882, “Symmetrische Gangrän;” also Zeitschrift für Prac. Heilkunde, 1882.
55 Inaug. Dissert., Strasburg, 1884.
56 Zeitschrift für klin. Med., vi. p. 277, 1883.
57 Deut. Arch. f. klin. Med., xxxv. 183, 1884.
58 Bäyr. ärzt Intell. Blatt, 1884, xxxi. 24.
SYMPTOMS.—The disease begins suddenly in all cases, and the constitutional symptoms are less prominent than the local ones. In some cases there are noticed a certain degree of mental disturbance, a condition of depression with a tendency to sigh and cry without cause, disturbed sleep with unpleasant dreams, irritability, and headache. A loss of appetite and disorders of digestion may follow, and then the local symptoms appear. In other cases, which seem to be the majority, the local condition develops without any such premonitory disturbances of the nervous and digestive systems, although these may ensue. The local symptoms first noticed may be paræsthesiæ or pain in all the extremities, usually limited to the tips of the fingers and the toes. These are continuous and severe, and are immediately followed (and occasionally preceded) by an appearance of ischæmia or of cyanosis or of erythema, in the order of frequency named.
(1) The fingers may look pale and dead, presenting the appearance of the so-called digiti mortui, and may be cold, painful, and anæsthetic. If this condition is moderate in degree, a certain amount of blood will continue to flow through the contracted arterioles, and then it corresponds to the description given by Raynaud of syncope locale. If it is extreme, the part may be wholly deprived of arterial blood, and then a true local asphyxia is present. In this stage the patients usually suffer considerably, although some do not complain of pain until the next stage. The ischæmia is attended with an impairment of sensation to touch, temperature, and pain, and finer motions become clumsy on account of the subjective numbness and actual anæsthesia. At the same time, the fingers look shrunken, the skin being thrown into folds, as if the hand had been soaked in hot water, or they may appear as if frozen, the skin being hard and immovable.59 The secretion of perspiration may be increased, and the fingers feel damp as well as cold, or it may be suspended. The local temperature is lowered. If the part is cut, little or no blood will flow. At this stage the arterial spasm may suddenly relax and the part return gradually to its normal condition, the cessation of the constriction of the arteries and the return of blood being usually accompanied by burning pain, which may last for some hours. The duration of such an attack may vary from a few moments to several days. If it continues longer, this stage is usually succeeded by the second stage, of cyanosis.
59 Finlayson, Medical Chronicle, 1885, No. 4.
(2) The stage of cyanosis results from one of two conditions: either the arterial spasm is so complete that no blood passes into the part, in [p. 1259] which case venous blood from lack of vis a tergo or in response to gravitation regurgitates into the capillaries, distending them and producing a state of blueness; or a venous spasm occurs, preventing the exit of blood from the part, which then becomes actively congested, and the blood in the capillaries, from want of renewal, soon becomes venous and produces the cyanotic appearance. The stage of ischæmia may be so short that it is hardly noticed, so that the patient's attention is first attracted by the swollen, blue, and extremely painful condition. The skin may be stretched, the tissue infiltrated with products of exudation, which can be pressed out, as can also the venous blood, and the surface may itch as well as be painful. Anæsthesia is rarely present in this stage, and there may even be hyperæsthesia. The part is cool from the increased radiation of heat and cessation of the processes of metabolism, the local temperature being lowered. The small vessels on the surface will be visibly injected, and capillary ecchymoses may rarely be seen. There is less liability to difficulty in movement in this stage than in the former one, as the sensations of the part are not benumbed, but if present it is due to the swelling. This condition, like that in the former stage, may cease suddenly, the recovery of the normal appearance being, as a rule, slower than after a simple ischæmia. The duration of this stage has varied from a few seconds to several days. It is usually followed by gangrene.
(3) The condition of local erythema is described here because it may lead to gangrene, and has therefore been considered by Weiss as one of the early stages of the disease. As a rule, however, it is not followed by the death of the part, and the affection in these cases is probably one of erythromelalgia rather than of symmetrical gangrene. Like the stage of ischæmia, the stage of erythema may appear suddenly. The part presents a bright-red or a mottled appearance—is hot and swollen, and painful. The vessels are visibly injected, the local temperature is raised, the secretion of sweat may or may not be increased, and the patient feels a burning sensation rather than pain. Hyperæsthesia to touch and temperature and pain is usually present, or the sensations are normal. The blood can be pressed out, but returns immediately. In this condition of hyperæmia slight injuries lead frequently to an inflammatory process, ulcers may form in the pulps of the fingers or around the nails, and the eschars may appear dark and even gangrenous; or an actual condition of gangrene may appear in the tips of the fingers, the exact method of its occurrence being a matter of dispute. The erythematous condition is much more likely to be permanent than are the other stages of the disease—another fact which has led to some hesitation in considering it a true stage. This condition of erythema may be due to a paralysis of the vaso-constrictors, the converse of the spasm occurring in ischæmia. It has also been ascribed to an irritation of the vaso-dilators; and this appears to be the more probable hypothesis.
(4) The stage of gangrene is always preceded by that of cyanosis, and the death of the tissue is due to the arrest of nutrition consequent upon a stasis of the blood. It is not necessary to invoke the injury of trophic nerves to explain its appearance. In the tips of the cyanotic fingers, on their palmar surface, beneath the epidermis, a small blister appears, filled with a dark serous fluid or with pus or blood. This soon ruptures, and a dark dry scab forms, beneath which an ulceration may go on destroying [p. 1260] the corium, but not penetrating deeper. In the majority of cases the gangrene is limited to a small area of the pulps of the fingers, and only involves the superficial layers of the corium. The gangrenous spot is surrounded by a purple margin. When the sphacelus has separated a scar remains which is frequently insensitive. In other cases when the sphacelus is thrown off it leaves a deep ulcer, which may look as if the lost tissue had been cut out with a punch, and this gradually granulates and heals. In still other cases the entire skin of the terminal phalanx may become black and dry, presenting a true gangrenous appearance. Then a line of demarcation is formed, usually at the junction of the terminal with the middle phalanx; separation of the gangrenous part occurs, and a stump is left covered with thin, glossy skin. This extensive gangrene, involving an entire phalanx, is the exception rather than the rule.
While the gangrenous process is in progress in the tip of the finger the nails cease to grow, and may become bulbous and rigid; the epidermis elsewhere may become dry and desquamate, and ulceration around the root of the nail may take place. With the completion of the stage of gangrene, which may last from one to five weeks according to its extent, the local symptoms terminate.
It is the symmetrical distribution of the local symptoms just enumerated which is the peculiar characteristic of the disease. The fingers of both hands, the toes of both feet, symmetrically situated spots upon the back, trunk, thighs, legs, forearms, and arms (in the order of frequency named), are affected either singly or in combination. In the majority of cases fingers and toes are affected together, and a few spots are seen on the trunk. In many cases the toes escape. In a large number of cases the face has been affected, spots of cyanosis appearing on the nose or ears or lips. As a rule, the stage of gangrene only ensues in the tips of the extremities, but a few cases are recorded in which little areas of skin elsewhere have passed through all the stages of the disease. Pigmentation occurs in spots upon the body when the process does not go on to gangrene.
Among the rare symptoms which have occurred in some cases are great impairment of temperature, pain, and electric sensations in the affected extremities; swelling, pain, redness about, and effusion into, the joints; considerable loss of motion in the muscles of the hands and feet, with diminution of electric excitability, but no qualitative change; and oculo-pupillary changes ascribed to an irritation of the cervical sympathetic fibres at their origin in the spinal cord.
In addition to the constitutional symptoms mentioned, which may usher in the disease and may continue during its course, there have been observed temporary albuminuria, glycosuria, and hæmaturia. Fever never occurs as a symptom of the disease, and if present must be ascribed to some other condition. The special senses have been affected in a few cases. In one case a spastic contraction of the retinal arteries alternated with attacks of ischæmia in the extremities.60 The intellect is usually unaffected, but Weiss observed a case in which transient aphasia occurred, which he attributes to local spasm in the arteries of the cortex. The patient could find words only after long thought, and spoke slowly and with difficulty.
60 Raynaud, Arch. gén. de méd., 1874, p. 11; Galezowski examined the discs.[p. 1261]
COURSE AND DURATION.—The onset of the disease is sudden. The symptoms in the first two stages may last only for a few minutes and pass off, or the disease may pass through all the stages and terminate in gangrene. It is usual for the first stage of ischæmia to last several days, varying in severity; for the second stage to last several days; and for the stage of gangrene to occupy about three weeks. The shortest duration of a single attack has been ten days, the longest five months. If the gangrene begins simultaneously in all the fingers, the duration will be shorter than if it proceeds to one after another. In one-third of the cases a recurrence of the disease within a year of the first attack has been observed, and it is probable that the proportion would have been larger had all the patients been kept under observation. In some cases three and four attacks have succeeded each other with some rapidity, some of the attacks being much less severe and shorter than others. In some cases the condition of gangrene has developed only in one out of three attacks. When the condition is one of local erythema the duration may be indefinite, the state becoming chronic and lasting for several years.
NATURE.—The nature of the disease is a matter of deduction from the study of the symptoms, no autopsies having as yet been made. As already stated, the symptoms are explained on the theory of a vaso-constrictor irritation in the stages of ischæmia and cyanosis—of a vaso-dilator irritation in the stage of erythema. Whether this irritation is the direct result of abnormal processes going on in the vaso-motor centres in the spinal cord, or is the reflex result of irritation arising elsewhere, is undetermined. Raynaud held that it must be of central origin, since in his cases galvanization of the spinal cord modified the arterial spasm. The latter observation has not been confirmed by other observers. Weiss believes that the condition may occur in response to irritation arising in the skin, in the viscera, or in the brain, and thus prefers the theory of reflex origin. This theory is adopted by several observers, who find a source for such irritation in the female genital organs in their cases.
ETIOLOGY.—The disease occurs in adult life, only two cases having been observed in persons fifty years old. It is most frequent between the ages of fifteen and thirty, although children and adults beyond the age of thirty are about equally liable. Females are more liable to it than males, four-fifths of the recorded cases having been in women. It occurs more frequently in the winter months, exposure to cold being a common exciting cause. Other exciting causes are nervous exhaustion, especially occurring in those who are predisposed to nervous diseases by heredity; general weakness from anæmia, malnutrition, or the occurrence of acute fever or exhausting disease; and mental agitation, a fright having preceded the attack in several cases. In women menstrual disorders and uterine disease have been considered as etiological factors. Occupation has something to do with its occurrence, since washerwomen, waitresses, and chambermaids are the class most often affected. In many cases, however, no cause of local irritation can be found.
DIAGNOSIS.—The diagnosis rests upon the development of vaso-motor symptoms in the extremities, situated symmetrically, going on to gangrene, in a person not afflicted with cardiac disease or with endarteritis of any kind, and not having been exposed to frost-bite or ergot-poisoning. The age of the patient, the symmetrical position of the symptoms, the [p. 1262] persistence of the pulse in the main arteries, and the limitation of the gangrene to the tips of the extremities distinguish it readily from senile gangrene. The history of the case, the absence of itching, and the presence of pain during the arterial spasm which passes off when the spasm ceases, serve to separate it clearly from chilblains. Congenital cyanosis is produced by cardiac anomalies, and the entire body is affected. Ergot-poisoning can be ascertained by the history.
PROGNOSIS.—Life is not endangered by this disease, no fatal cases having been recorded. Recovery from an attack is certain, but the duration cannot be stated, as it will depend in any case on the character, the extent, and the severity of the symptoms. The possibility of a recurrence of the attack should be stated to the patient.
TREATMENT.—The methods of treatment have varied, and none are wholly satisfactory. If the causes can be met—e.g. anæmia, nervous exhaustion—they should be treated. If not, the disease itself may be attacked by means of electricity. Or the symptoms may be treated as they demand it. Electricity has been used by almost all observers. The faradic current produces an aggravation of all the symptoms except in the stage of erythema, and has been discarded. The galvanic current may be employed in several ways. Two methods are in use. In the first the positive pole is applied over the cervical region, and the negative pole over the lumbar region, a descending current being thus sent through the spinal cord. The current should be of moderate strength, not above twenty-five milliamperes, few patients being able to endure the strength implied in Raynaud's statement that he used sixty-four cells of a Daniel battery. The duration of the application should be ten minutes, and the electricity may be applied once daily. In the second method the anode is applied over the brachial or lumbar plexus, as the case may be, and the cathode passed over the affected extremity, the current being constant and care being taken not to break it suddenly. The strength, duration, and frequency should be the same as in the first method. From these two methods, separately or combined, Raynaud claimed to have seen favorable results. His assertions have not been confirmed by other observers who have followed his directions closely, and hence considerable doubt at present prevails as to the efficacy of the electric current. The so-called electrical application to the cervical sympathetic is certainly useless. In the stage of erythema a very weak faradic current applied to the hands in a bath may be of service.
Many observers have found that the progress of the case to recovery was quite rapid if the limb were put at rest in an elevated position, were kept warm by cotton batting or similar bandaging, and were kept clean with antiseptic lotions when the stage of gangrene set in. Massage is to be used in all cases, the limbs or affected parts being gently rubbed with the dry hand or with aromatic liniments or oils. All local injury, however, and especially counter-irritation, are to be carefully avoided. General tonic treatment, especially iron and cod-liver oil, is to be used in all cases.
The pain occurring in the early stages is often so severe as to require the use of opium or other narcotics. And when the nervous symptoms are especially aggravated, and irritability and insomnia give the patient discomfort, bromide and chloral may be employed.
ETIOLOGY.—Diseases of the cervical sympathetic ganglia or cord may be of two kinds—either irritative or destructive.61 They are produced by pressure upon the cervical ganglia or upon the sympathetic cord between these ganglia, by tumors, especially aneurisms, and enlarged glands; by abscesses; and by cicatrices of old wounds in the neck. They are also due to extension of inflammation from a thickened pleura in phthisis and chronic pleuritis of the apex. They may be caused by injuries, such as stab-wounds, gunshot wounds, etc. Any disease which produces marked irritation of peripheral branches of the sympathetic in the neck, or of the cerebro-spinal cervical nerves, may cause reflex phenomena resembling the symptoms of actual disease. From such phenomena it is not justifiable to conclude that the sympathetic cord and ganglia are the seat of lesions, and the only cases which will be considered here are those in which actual disease was proven to be present by an autopsy.
61 Ogle, Medico-Chirurgical Transactions, xli. 397-440, 1858, 27 cases; Poiteau, “Le Nerf sympathetique,” Thèse de Paris, 1869, 19 cases; Eulenburg and Guttmann, Die Pathologie der Sympathicus, 1873; Nicati, Le Paralysie du Nerf sympathique-cervicale, 1873, 25 cases; Seeligmüller, Inaug. Dissertation, 1876; Mitchell, Injuries of Nerves; Mobius, “Pathologie der Sympathicus,” Berlin. klin. Woch., 1884, Nos. 15-19.
Inasmuch as the cervical sympathetic is in close anatomical connection with the spinal cord, especially with the eighth cervical to the second dorsal segments (the so-called cilio-spinal centre of Budge), and as the functions of the sympathetic are dependent upon the integrity of the spinal cord, it is evident that any lesion of the nerves uniting it with the cord, or any lesion in the cord itself at the levels mentioned, may produce symptoms which resemble closely those of disease of the sympathetic. Thus, cervical pachymeningitis, myelitis (especially from injury of the cord, or hæmato-myelia), and diseases of the cervical vertebræ which produce either or both conditions, may cause a train of symptoms somewhat similar to those to be described.62 A careful distinction must be made between primary and secondary disease of the sympathetic, between reflex and direct symptoms, between lesions in its substance and lesions in its governing centres in the spinal cord. The symptoms produced by affections of a reflex or central nature are rarely as numerous as those of disease of the sympathetic itself. An example of such a secondary affection is the combination of sympathetic symptoms occurring in progressive muscular atrophy. And, finally, since mental action of an emotional nature may cause flushing or pallor of the face, with profuse sweating and variations in the size of the pupil and prominence of the eyeballs, as well as palpitation or arrest of the heart, there is reason to believe that symptoms of sympathetic disease may be produced by cerebral lesions.
62 Ross, Diseases of the Nervous System, 2d ed., i. 686-688.
PATHOLOGY.—The pathological anatomy of the cervical sympathetic is obscure. This is probably owing to the fact that the ganglia are rarely examined, and pathologists have not been familiar with their histology. Lesions of the cervical sympathetic have been described in almost every imaginable form of disease, and at one time, when many obscure conditions were blindly termed sympathetic, the records were filled with descriptions of fatty degeneration or interstitial inflammation or pigment deposit in the ganglia. As no actual symptoms of disease of the cervical [p. 1264] sympathetic, as now understood, were present in such cases, it is impossible to believe that the lesion was other than hypothetical.
The conditions which have been observed in a few carefully-studied cases of primary disease have been—(1) A parenchymatous inflammation of the cells of the ganglia, attended by swelling, loss of nuclei, granular and fatty degeneration, and by atrophy, together with a degeneration of the fibres issuing from the cells. (2) A sclerotic process in the connective tissue in and about the ganglia and in the nerves, resulting in such an increase in the interstitial tissue as to compress and injure the cells and axis-cylinders. These may be observed together in the later stages of the disease. (3) In a number of cases the capillaries within and about the ganglia have been found dilated, tortuous, and varicose, and hemorrhages from them are not rare.
SYMPTOMS.—The symptoms of irritation of the cervical sympathetic are dilatation of the pupil, widening of the palpebral fissure, protrusion of the eyeball, pallor of the entire side of the face and head, with slight fall of local temperature and possibly an increased secretion of perspiration, and an increased frequency of the heart. It is rarely that these are all observed in any case, dilatation of the pupil with slight pallor and rapid pulse being the only signs of irritation as a rule. Such irritation is a less common occurrence than might be supposed, many lesions which produce pressure even of a slight degree on the sympathetic having caused symptoms of a suspension of its function rather than of an increased activity. This is doubtless due to the non-medullated structure of the fibres, which thus lack protection from injury.
The symptoms of destructive disease of the cervical sympathetic are the converse of those just mentioned, and they are all present when the part is seriously involved. The patient will then have a marked contraction of the pupil, which no longer responds to light or to irritation of the skin of the neck, but may change slightly in the act of accommodation. It resists the action of mydriatics. The vessels of the choroid and retina may be dilated, as well as those of the iris, in which case the patient will feel a sense of weariness on any long-continued attempt to use the eyes. There is no actual disturbance of vision, and the cornea is not usually flattened, as was formerly supposed. There is a noticeable narrowing of the palpebral fissure, the upper lid falling slightly as in a mild state of ptosis, and the lower lid being slightly elevated. This is due to the paralysis of the muscles of Müller in the eyelids, which are controlled by the sympathetic. It is present in 90 per cent. of the recorded cases, and in many the apparent size of the eye is reduced a half. Retraction of the eyeball is a less constant symptom, and one which develops only after the disease has existed some time. It is due partly to the paralysis of the orbital muscle of Müller, and partly to the decrease in the amount of fat in the orbit behind the eye. A marked symptom, and one which is constant, is a dilatation of the vessels of the face, conjunctiva, nasal mucous membrane, ear, and scalp. This is attended by redness, a subjective sense of heat, and an actual rise of local temperature, which may exceed that of the other side by 1.5° F., measured in the auditory meatus or nose. This vascular congestion has persisted in some cases for three years. In others it has been followed much earlier (in nine months) by a partial or complete return to the normal condition, and [p. 1265] even when the local temperature remains higher on the affected side, the visible congestion and the sensation of heat may have disappeared. The dilatation, succeeded by the contraction (normal tone), of the vessels has led to a division of the disease into two stages, and in a few cases the affected side has become paler than the other in the second stage. In both stages the part affected is less sensitive to changes in the external temperature.
An increased secretion of tears and of perspiration has been supposed to accompany dilatation of the vessels of the skin of the head inevitably. This is not a constant symptom, as the recent cases have demonstrated. And no definite statement of the effect of disease of the cervical sympathetic on the occurrence of dryness or dampness of the face can be made, both conditions having been observed. A difference between the degree of moisture on the two sides of the face on exposure to heat is usually present. Palpitation of the heart has been an annoying symptom to the patient in many cases, and is usually associated with a marked slowing of the pulse. This was reduced from 74 to 66 in Möbius' case,63 and remained slow for some weeks. The frequency of the heart may, however, be increased after the first period of slowing, but never reaches a very high rate (88 in the case cited). A slight atrophy of the affected side of the face has been observed in several cases, appearing after the disease has existed for some time. The muscles of the cheek feel flabby and are slightly sunken; but the condition does not approach in severity true facial hemiatrophy, nor is it sufficiently rapid to be considered due to a trophic disturbance. Changes in the secretion of saliva, dryness of the nasal mucous membrane, and symptoms referable to paralysis of the intracranial vessels, such as might be expected from the result of physiological division of the sympathetic, have only been occasionally observed. Glycosuria has been noted in a few cases.64
63 Berlin. klin. Woch., 1884, No. 16.
64 Gerhardt, Volkmann's Sammlung klin. Vorträge, No. 209, “Ueber Angioneurosen,” p. 11.
COURSE.—The course of the disease has been divided into two stages, as already mentioned, the majority of the symptoms remaining permanently from the onset. The second stage is characterized by the cessation of the dilatation of the vessels, by the appearance of retraction of the eyeball, and by the development of slight facial atrophy. In the cases where the sympathetic is extensively destroyed by the lesion no recovery is possible. When it is simply divided by a wound there has been a considerable degree of recovery, probably due to a spontaneous union of the divided ends and re-establishment of the function. From these facts the prognosis can be deduced.
DIAGNOSIS.—The symptoms are so characteristic that there is no difficulty in reaching a diagnosis. The most important point in any case is to determine the cause, care being taken to consider all the possibilities already mentioned in discussing the causation. The symptoms of lesion are always unilateral.
TREATMENT.—If the cause can be removed, an indication for treatment is afforded. Sources of reflex irritation are to be eliminated. If the sympathetic has been divided by a wound, it may be well to unite the cut ends, as in suture of other nerves, although this has not yet been attempted; otherwise there is little hope from any method of treatment. [p. 1266] Electricity has been applied in vain, and galvanization of the sympathetic in the neck is now regarded by all good authorities as useless.
Diseases of the thoracic and abdominal sympathetic ganglia and cords have been suspected, but nothing definite is known of their symptoms or pathology; the statements which have recently been made regarding visceral neurosis not being based upon any cases in which post-mortem lesions were found.
TROPHIC NERVES AND NERVOUS CENTRES.—The nutrition of the body depends upon the nutrition of the individual cells of which it is made up. Each cell has the power of appropriating from the blood such substances as will preserve its existence, enable it to perform its functions, and produce a successor. Whether this power is inherent in the cell or is controlled by the nervous system is a question upon which authorities are divided. Those who hold the first position deny the existence of trophic nervous centres and of trophic nerves from those centres to the organs and elements of the body, claiming that this hypothetical trophic system has not been demonstrated anatomically, and that the facts urged in its support are capable of another interpretation. Those who believe in the existence of a trophic system have been able to demonstrate the existence of fine peripheral nerve-fibres passing to and ending in individual cells of the skin, glands, and other organs,65 and have brought forward a large collection of facts which merit a careful examination.66 They are as follows:
65 Bericht der Section für Dermatologie, Versammlung Deutscher aerzte, Strasburg, 1885; Vierteljahrschrift für Dermatologie und Syphilis, 1885, 4 Heft, S. 683.
66 “Tropho-neurosen,” Real Cyclopædie f. d. gesammt. Medicin, vol. xiv., 1883; Erb, Ziemssen's Cyclopædia, xi. pp. 408-423.
ATROPHY.—When a nerve is cut certain changes occur in it which are known as Wallerian degeneration.67 This affects the peripheral end of a severed nerve, the peripheral end of a severed anterior nerve-root, and the central end of a posterior nerve-root. To maintain its integrity a motor nerve must be in direct continuity with a normal cell of the anterior cornu of the spinal cord; a sensory nerve must be in connection with the intervertebral spinal ganglion on the posterior nerve-root. Nerves which pass between two such ganglia do not degenerate when cut. The degeneration consists68 in a coagulation of the myelin in the medullary sheath, a fatty degeneration of the coagulum, and a gradual absorption of the débris. The axis-cylinder is compressed, and finally disintegrated, by a mass of protoplasm which develops about the nuclei of the interannular segments, and after undergoing fatty degeneration its débris becomes mingled with that of the myelin, and is also absorbed. The sheath of Schwann, whose nuclei have in the mean time increased by a process of subdivision, is partly filled by the protoplasm (from which the new axis-cylinder develops if regeneration occurs), remaining as a fine [p. 1267] thread of connective tissue when all other traces of the nerve-fibre have disappeared. There may be a proliferation of cells of the endo- and perineurium at the same time which aids in the transformation of the nerve into a connective-tissue strand. This process of degeneration involves the terminal plates by which the nerves join the muscles, but the terminations of the sensory nerves—i.e. tactile corpuscles—do not appear to be affected. The central end of the cut nerve may display a similar change for a distance not greater than one centimeter; it usually develops a bulbous swelling of connective tissue, and retains its conducting power indefinitely.
67 Waller, Philosoph. Transactions, 1850, ii. p. 423; Comptes rendus de l'Acad. de Sci., 1852-55.
68 Ranvier, Leçons sur l'Histologie de Système nerveux, Paris, 1878; Von Recklinghausen, Pathologie der Ernahrung, 1883.
Degeneration in the tracts of the spinal cord occurs after various forms of lesion,69 and is similar in its processes to degeneration in the peripheral nerves. The increase in the connective-tissue elements is more noticeable in contrast with the parts unaffected, and from the density of the tract involved the result has been called sclerosis. The recent researches of Homen70 have shown that the process of degeneration begins in the entire length of the affected tract, and does not proceed from the point of lesion onward, as was formerly supposed.
69 See Vol. V., “Myelitis—The Secondary Scleroses,” p. 892; Schültze, Arch. für Psych., xiv. 2.
70 Fortschritte der Medicin, 1885, No. 9.
When a muscle is separated from its connection with the central nervous system, either by a division of the nerve passing to it or by a destruction of the cells in the anterior cornu of the spinal cord from which that nerve arises, it undergoes an atrophy which is peculiar in being immediate and rapidly progressive, thus contrasting strongly with the gradual and slighter atrophy from disuse in cases of cerebral paralysis where the cells mentioned and the nerve-fibres are intact. There is at first a simple diminution in the number of the fibrillæ of which the muscular fibre is made up, together with an increase in the interstitial connective tissue nuclei. Then an albuminoid and fatty degeneration of the muscular elements occurs, with a proliferation of muscle-corpuscles or nuclei, and a gradual absorption of the débris. The interstitial connective tissue then increases rapidly, forming fibrous bands through the degenerated muscle which compress the few muscular fibres remaining, until as a result the muscle is transformed into a mere ribbon of connective tissue without any power of contractility.71 As these changes go on the electrical reactions change, the three degrees of reaction of degeneration corresponding to the three stages of atrophy described.72 These phenomena of nerve- and muscle-degeneration are observed in traumatic or idiopathic neuritis, in acute and chronic poliomyelitis anterior, in general myelitis involving the anterior cornua, and in bulbar paralysis.
71 Hayem, G., Recherches sur l'Anatomie pathologique des Atrophies musculaires, Paris, 1873; Ross, Diseases of the Nervous System, vol. i. p. 238.
72 See Vol. V., “Electric Reactions.”
The influence of the nervous system on the nutrition of the bones has also been ascertained. When a bone is developing, a lesion of the nerve to it, or of the deeper portion of the anterior cornua of the spinal cord from which these nerves arise, will modify and partly arrest its growth. This is often seen in anterior poliomyelitis and in hemiatrophy of the face occurring in children. In the adult a no less marked effect is produced, although the results are less noticeable. A condition known as [p. 1268] osteoporosis is caused, consisting of an enlargement of the Haversian canals and an infiltration of fatty matter into them and an actual decrease in all the inorganic constituents of the bone, which loses in weight, becomes thinner and more fragile, so that spontaneous fractures may occur.73 This condition has been noticed more frequently in diseases of the spinal cord than in neuritis; it is said to occur in locomotor ataxia. It has been found in a few cases of long-standing hemiplegia and also in dementia paralytica, no explanation of its pathogeny in these instances, however, being offered. In a case of ataxia with a lesion in the medulla which involved the nuclei of the fifth, ninth, tenth, and eleventh nerves on one side, all the teeth of the upper jaw on that side fell out within a few weeks, those in the lower jaw remaining.74 Changes in the nutrition of the bones have also been recorded in cases of progressive muscular atrophy in the paralyzed limbs.75
73 Weir Mitchell, Amer. Journ. of the Med. Sci., 1873, p. 113; Charcot, Arch. de Phys., 1874, p. 166.
74 Demange, Rev. de Médecine, 1882, p. 247.
75 Friedreich, Progressive Muskelatrophie, p. 347, 1873.
The condition of the skin and its appendages is influenced decidedly by changes in the nervous system, either in the nerves, in the spinal ganglia, or in the central gray matter. Here it is the sensory nerves which convey the trophic influence, not the motor nerves, as in the cases hitherto considered; and when the lesion producing trophic changes in the skin is central, it is situated in the posterior cornua of the spinal cord or in the gray matter near the central canal. The glossy skin seen on the fingers after injuries to the nerves is a type of such atrophy from disturbance of trophic impulses. Glossy fingers present a smooth, shining appearance, are dry from the diminution in the secretion of sweat, feel soft and satin-like to the touch from the marked thinning of the skin, and frequently show a defective or irregular growth of the nails, which may be ridged, curved, or deformed.76 They are red and mottled from accompanying vaso-motor paralysis, and are usually hot and painful. Changes in the pigmentation of the skin and hair are recorded as a not infrequent accompaniment of severe neuralgia and as a result of great mental anxiety. Thus in several cases of supraorbital neuralgia the eyebrow on the affected side has turned white; in infraorbital neuralgia the beard has become gray; and in both the hair has been observed to fall out.77 The sudden turning white of the hair is ascribed to a swelling of the hair by air within it.78 In one case, frequently cited, the hair and nails fell out after a stroke of lightning.
76 Weir Mitchell, Injuries of Nerves. See also Vol. IV. p. 683.
77 Seeligmüller, Lehrbuch der Krankheiten d. Peripheren Nerven, p. 157, 1882.
78 Arch. f. Path. Anat., xxxv. 5, 575, Landois.
When a gland is cut off from its nervous connection with the cord or cerebral axis by section of its nerves, its function is impaired and its nutrition suffers, so that after a time it loses weight and undergoes a progressive total atrophy. This has been proven experimentally in animals in the submaxillary gland. It has been observed in the testicle in man after division of the spermatic nerve (Nélaton) and after destruction of the spinal cord by traumatic and idiopathic myelitis (Klebs, Föster).79 The sweat-glands are known to be under the control of a central [p. 1269] nervous mechanism, as cases of hyperidrosis, anidrosis, and chromiodrosis prove;80 and an atrophy of them and of the sebaceous glands has been observed81 after nervous lesions.
79 Cited by Samuel, Realcyclop., loc. cit. See also Obolensky, Centralblatt für med. Wissen., 1867, 5, 497.
80 See Vol. IV. pp. 583-586.
81 See Vol. IV. pp. 683 et seq.
Progressive hemiatrophy of the face is treated elsewhere. The following case of progressive hemiatrophy of the entire body may be mentioned here: A boy, aged fourteen, dislocated his ankle, which in a few days became swollen, red, hot, and painful. The inflammation extended up the leg, but did not involve the knee, and soon subsided. After a short time the foot began to atrophy. The atrophy extended up the leg, and involved the thigh; it then progressed to the trunk and the arm, and lastly to the face on the affected side, until in the course of two years there had developed a unilateral atrophy of the entire body. Muscles, fat, and bones were all affected, but no difference in the skin or hair of the two sides was noticed. Fibrillary tremors were present in the muscles. The electric reactions were not altered, but were gradually lost. There was a hypersensitiveness to touch and to cold, but no other sensory disturbance. The boy was alive and fairly well when the case was reported.82 It is unique.
82 Heuschen, Schmidt's Jahrbuch., vol. cxcviii. p. 130.
These various instances of atrophy cannot be ascribed to simple disuse, since they differ markedly in their pathological changes and in the rapidity of their progress from such atrophy. Nor are they to be referred to vaso-motor disturbances, since in many cases no vascular changes are evident. Their distribution in the body often corresponds exactly with that of peripheral nerves, and they accompany nerve lesions too frequently to be explained on any theory of coincidence. There are many authorities, however, who refuse to ascribe them to a lesion of trophic nerves.83 In regard to the degeneration of nerves it is said that each nerve axis-cylinder is a part of the nerve-cell from which it arises, and hence destruction of the cell or division of the cylinder, by disturbing the unity of existence, results in the death of the part. The fibre shares all the changes of nutrition which the nerve-cell undergoes, and if separated from it necessarily perishes. To this it is replied that trophic paths and motor paths are distinct at some points in their course, at least in the central nervous system, since each can be affected alone. Erb, who has studied this subject carefully,84 believes that trophic are distinct from motor centres in the spinal cord, but that both impulses may be conveyed by the same axis-cylinder in the peripheral nerves—a middle ground which is widely accepted. It is now known that each axis-cylinder is made up of several fibrils, so that this theory gains probability. This would also explain the occurrence of atrophy in the muscles, the trophic centres being affected when the muscle atrophies, and unaffected when it is paralyzed without atrophy. Mayer, however, denies this explanation of the muscular atrophy, holding that the motor system, cell, nerve, and muscle-fibre, forms a nutritive as well as functional unit, and that the simple suspension of function, by interfering with the special [p. 1270] conditions of nutrition attendant upon physiological excitement, is competent to cause a pathological change. To this it is replied that the parts of the motor system are not interdependent, since disease of the muscle does not produce degeneration of the nerve and of the cell, and the fact of a degeneration in a peripheral direction alone is evidence of central trophic influence. The attempt to ascribe trophic changes in the skin, nails, and hair to vaso-motor disturbance has been equally unsuccessful in covering all the observed cases.
83 See Handfield Jones, St. George's Hospital Reports, 1868, vol. iii. pp. 89-110; Sigmund Meyer, Hermann's Handbuch d. Physiol., ii. Th. 2, “Trophische Nerven,” 1879; Gowers, Diseases of the Brain, 1885, p. 4.
84 Arch. f. Psych., v. S. 445, 1875; also Ziemssen's Cyclo., vol. xiii. p. 117 (Amer. trans.); also Deut. Arch. f. klin. Med., v. S. 54.
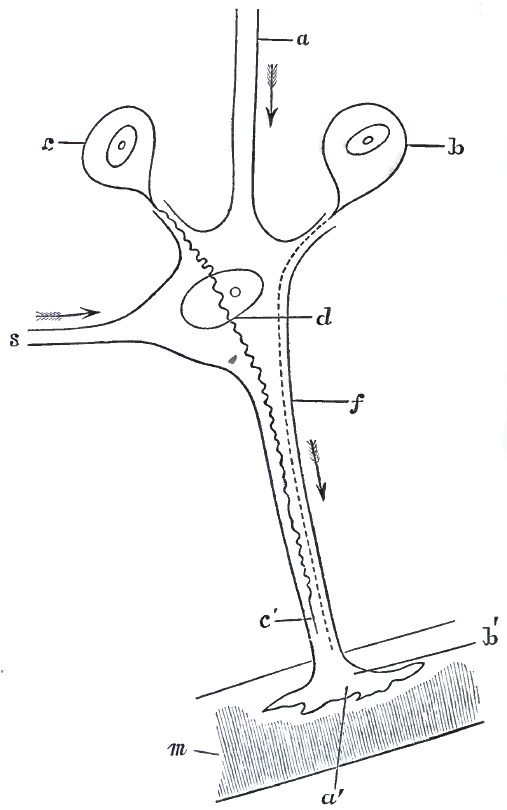
HYPERTROPHY.—Trophic changes are not limited to the process of atrophy. There are conditions of hypertrophy of supposed nervous origin. Samuel considers the hypertrophy of one testicle which attends atrophy of the other from section of its nerve as an example of this. It has been ascertained that one kidney hypertrophies when the other is atrophied or extirpated. When the spleen is removed the lymphatic glands increase in size. But these facts are capable of another explanation—viz. that increased demand upon the organ leads to its increased growth. Hypertrophy of the skin and of the tongue is seen in cretins in contrast with the deformity of the body and atrophy of the limbs. A hemihypertrophy of the face has been noticed in several cases, the counterpart of hemiatrophy; and in one case a unilateral hypertrophy of the entire body was observed.85 The local thickening of the skin known as ichthyosis hystrix, and other hypertrophies of the skin, certain deposits of pigment, and vitiligo, have been ascribed to nervous causes. Mitchell has recorded cases of abnormal growth of the nails and hair after injuries to the nerves, and similar phenomena have followed central lesions. He has also described a thickening of the skin of the first three fingers and of the back of the hand following a wound of the brachial plexus. These conditions of the skin and its appendages indicate an abnormal activity in the cells of the affected part, a rapid metabolism and reproduction, resulting in an undue production of tissue, apparently dependent on nervous impulses reaching the cells from a distance. The insane ear may be mentioned in this connection as a trophic disturbance due to central lesion.
85 Ziel, Virchow's Archiv, xci., S. 92.
MYXŒDEMA (cachexie pachydermique) is a disturbance of nutritive processes characterized by a production of mucin, which is deposited in all the tissues of the body, but especially in the subdermal connective tissue.86 It is considered by the majority of authors a trophic neurosis, and is therefore considered here.
86 Sir William W. Gull, “On a Cretinoid State supervening in Adult Life,” Trans. Clin. Soc. London, 1874, vol. vii. p. 170; Ord, “On Myxœdema,” Med.-Chir. Trans., 1878, vol. lxi. p. 57; Mahomed, Lancet, 1881, ii. No. 26; Hadden, Brain, 1882; W. A. Hammond, Neurological Contributions, 1881, i. p. 36; Ballet, Archives de Neurologie, 1881, vol. iii. p. 30; Schmidt's Jahrbucher, vol. clxxxix. p. 30, and cxcviii. 264; “The Brown Lectures,” Victor Horseley, Lancet, Jan., 1886.
PATHOLOGY.—In the few autopsies which have been made an increase in the connective tissue of all the organs has been found, in the meshes of which a thick, transparent, slimy substance (called animal gum), consisting of mucin, is present. This may compress and destroy the parenchyma of the organs involved. There is also found a thickening of the coats (adventitia and media) of the vessels. An atrophy of the thyroid gland has occurred in every case, and experimental extirpation of the thyroid in animals produces symptoms so nearly identical with those of myxœdema that this is considered the chief pathological feature of the disease. Whether this atrophy is due to a compression by the mucin deposited, or is due to a disease of the trophic centres of the thyroid in the medulla, or is a primary affection of the gland, remains to be determined.
ETIOLOGY.—The actual causation is unknown. Cold and mental shock have been considered exciting causes in some cases. Women are much more liable to the disease than men, and it develops after the age of forty in the majority of cases. It may occur in childhood and result in a [p. 1272] cretinoid state. Syphilis and tuberculosis do not appear to be etiological factors.
SYMPTOMS.—The disease begins gradually, and the nervous symptoms or the local œdema may appear together or in succession. The patient notices a thickening of the skin, which becomes dry, rough, and scaly. The thickening is uniform and involves the entire body. It is most marked where the subdermal connective tissue is loose, as in the cheeks, lips, eyelids, and in all parts where the skin is thrown into folds. The hands and feet do not escape. The thickened skin is hard, and does not pit on pressure, thus differing from ordinary œdematous swelling. It appears of a waxy color, and is free from perspiration, the sweat-glands becoming atrophied from pressure. The hair may fall out or become woolly and brittle, and may change its color. In a few cases spots of pigment have appeared on various regions.87 The nails are brittle. The teeth are carious. The mucous membranes show similar changes, and the mouth and tongue, rectum and vagina, may be so swollen as to impair their respective functions. Digestive disturbances, constipation alternating with diarrhœa, and uterine hemorrhages, which occur, are ascribed to this cause. Albumen is occasionally found in the urine, but is not a constant symptom. The nervous symptoms are constant. The patients complain of paræsthesiæ and anæsthesia of the extremities or over the entire body, and the special senses may be impaired, as well as the tactile sense. They are very liable to severe attacks of neuralgia. They suffer from subjective sensations of cold, and are easily affected by changes of temperature. Motion is interfered with; tremors occur early; movements become slow and awkward; the gait is unsteady; the voice is rough and nasal; but no true paralysis or muscular atrophy has been observed. The patella-tendon reflex is occasionally lost, but not in all cases.
87 Allan McLane Hamilton, Journ. Nerv. and Ment. Dis., 1885, April, p. 180.
These symptoms have been ascribed to the pressure of the mucin upon the terminal filaments of the nerves, and also to changes in the central nervous system. That the latter theory is probably correct is shown by the occurrence of mental symptoms in the majority of cases. The patients become apathetic and all mental action is slowly performed. Indifference to surroundings, loss of memory, and inability to concentrate the attention may be succeeded by transient delirium, hallucinations, and occasionally by delusions of persecution, and the patient finally lapses into a state of imbecility. If the disease develops in early life, education is impossible, and the patient remains in an infantile condition.
Whether the changes in the nervous system are due to pressure by deposit of mucin (Hadden), or are due to an altered nutrition of the most delicate tissues of the body consequent upon the general metabolic derangement (Horseley), is undetermined. In experimental myxœdema the degenerative processes have been found in the nerve-cells.
There are no symptoms referable to the heart or lungs, and if cirrhosis of the kidney and liver develop, their symptoms supervene upon and are secondary to those of myxœdema. High arterial tension has been noticed in the majority of the cases.
The COURSE of the disease is a chronic one, and is progressive. There are, however, intermissions in the severity of the symptoms in some cases. Recovery does not occur.
[p. 1273]DIAGNOSIS.—The diagnosis from the accumulation of fat is made by observing the thickening of the nose, lips, fingers, and tongue, and the changes in the skin and its appendages. Scleroderma is not universal like myxœdema. In scleroderma the skin is harder and more adherent to subjacent parts, is not transparent and waxy, and the nervous symptoms are wanting. Cretinism seems to be closely allied to myxœdema, but is only observed before the age of seven and is accompanied by hypertrophy of the thyroid gland.
TREATMENT.—The treatment is only palliative. Simple nutritious diet, especially milk diet, with the use of such tonics as iron and quinine, has been found useful. The progress of the disease is hastened by exposure to cold, and in a very warm climate the symptoms may remain stationary for several years. Jaborandi or pilocarpine has been used in some cases with a moderate degree of success. Nitro-glycerin, gr. 1/100, has also been of benefit. For the paræsthesiæ and anæsthesia of the early stage the faradic brush has been applied, and for the motor weakness the faradic current, with the effect of relieving but not curing these symptoms. During the attacks of neuralgia morphine may be employed.
Inflammation.—The most important trophic disturbances are those which consist of an actual disintegration of tissue. These are very numerous. Herpes zoster, certain forms of eczema and pemphigus, lepra anæsthetica, scleroderma, acute ulceration of the fingers, perforating ulcer of the foot, acute bed-sores, keratitis with anæsthesia of the cornea, sympathetic ophthalmia, and various forms of joint disease, are examples of such trophic diseases.88 For the discussion of the skin and eye diseases mentioned the reader is referred to special articles on those subjects. In regard to lepra anæsthetica, it may be mentioned that in this disease lesions have been found both in the sensory nerves and in the posterior cornua of the spinal cord.89
88 Leloir, “Tropho-neuroses,” Nouveau Dictionnaire de Médecine et Chirurgie practiques, 1885.
89 Virchow, “Nerven Lepra,” Geschwülste, ii. 521; Tschirijew, Travaux du Laboratoire de Vulpian, 1879.
I have reported90 a case of acute ulceration of the ends of the fingers and toes occurring in an anæmic girl aged twelve, and persisting for more than a year, associated with cyanosis of the hands and feet, and with a tendency to rapid ulceration of any part of the body which happened to be exposed to pressure. The hair of the eyebrows, eyelids, and to a less extent that of the scalp, fell out during the disease. There was no local asphyxia and no appearance of gangrene; hence the case was not one of Raynaud's disease. Its symmetrical distribution, the lack of any constitutional organic disease or of any local cause for the production of the ulceration, and the anæmic and nervous condition present, all pointed to a disturbance of the central nervous system. It did not yield to treatment, either local or general or electrical. Mills has seen a similar case.91
90 Journal Nerv. and Ment. Disease, Feb., 1886, clinical cases.
91 Mills, Amer. Journ. Med. Sci., Oct., 1878.
Perforating ulcer of the foot begins on the sole, beneath any of the metatarso-phalangeal articulations, preferably the first or the fifth, or under the heel, as a small pustule under the epidermis. This ruptures, and the ulcer which results begins to extend in a direction vertical to the surface, involving the deeper tissues or even opening into the joint and destroying the bone. It appears rather like a sinus than an ulcer, and is [p. 1274] remarkable from the fact that it is not painful and is insensitive to touch, although it may prevent the patient from walking on account of extreme tenderness. The epidermis around the sinus is thickened and insensitive, and there may be anæsthesia of the entire sole of the foot, and even of the leg, although this is due to the neuritis present, which is also the cause of the ulcer, rather than to the ulceration. The circulation is sluggish in the affected extremity; it becomes cyanotic on exposure to cold, and seems peculiarly liable to become œdematous. The œdema may go on to suppuration, and involve the articulations, and ankylosis of the smaller joints may follow. This, too, is to be traced to the neuritis. The skin of the foot becomes pigmented, and may be dry or covered with offensive sweat. As the patient cannot walk while the ulcer remains, the condition demands treatment. Rest, moist warm applications, antiseptic lotions, scraping out the sinus, and other surgical means appropriate to the treatment of ulcers and sinuses do not often prove of benefit, and in obstinate cases recourse has been had to amputation of the foot. Electrical treatment has been tried in vain.
Such perforating ulcers may occur symmetrically on both feet, and may be numerous. They also occur rarely on the hands. They have been observed not infrequently in locomotor ataxia, occurring either early or late in the disease,92 and have appeared in patients suffering from dementia paralytica. The only constant lesion found is a degeneration of the peripheral nerve supplying the affected part.
92 For bibliography see Ross, Diseases of Nervous System, 2d ed., i. p. 256, and Blum, Berliner klin. Wochen., 1875, Nos. 13-15.
Acute bed-sores (decubitus) develop in many cases of spinal and cerebral disease, but not in all. It is argued that anæsthesia of a part or simple pressure upon a part or irritation of an anæsthetic part will not explain their occurrence, and that they must be traced to a destruction of trophic centres in the cord or brain. No amount of attention to the position and cleanliness of the patient is thought to be sufficient to prevent them in some cases, and their progress is often so rapid as to remove them from the category of simple ulceration. Their most frequent seat is upon the buttocks, over the sacrum, on the heels, and over the scapulæ; but it is believed that in the conditions in which they appear in these places pressure on any part may cause one. They begin within a few hours after the occurrence of the lesion as irregular mottled patches of redness, in which there soon appear small or large vesicles filled with dark serum. These rupture, leaving little areas of ulcerated surface, which soon unite to form a large ulcer with softened, infiltrated, and bloody base and ragged edges. The tissues around and within the ulcer have a tendency to slough and to become gangrenous, and the process goes on rapidly until a considerable area of the surface is completely destroyed, together with the deeper structures, fat, muscles, and fasciæ, down to the bone, which may become necrosed. Acute cystitis is so frequently associated with acute bed-sore that it is traced to the same nervous cause, though here, again, another explanation is possible. The constitutional disturbance produced by these two affections may be increased by a true septicæmia, to which the patient succumbs; or metastatic abscesses may be formed, and pyæmia cause death; or, lastly, the ulcer on the back may lay bare the vertebræ and erode their ligaments, thus opening a way for the extension of suppuration to [p. 1275] the meninges of the spinal cord. The duration may be from a few days to two weeks, and the prognosis is very grave.
Chronic bed-sores develop in a similar manner, although all the processes described occur more slowly and are much less severe. They do not show the tendency to extend so widely or so deeply, nor to become gangrenous. They remain stationary after attaining a certain size, and the tissues seem to lack all tendency to reproduction and repair. When the central lesion which they follow begins to pass away they heal; sometimes local treatment is successful; but in many cases they persist for years, always threatening the life of the patient from the possibility of their sudden aggravation or from the occurrence of the complications already mentioned in connection with the acute process.
Since neither form of decubitus occurs after lesion of the anterior cornua of the spinal cord, nor in sclerosis of the posterior or lateral columns, nor in those cases of locomotor ataxia in which extensive invasion of the posterior cornua is present, while they are particularly frequent as a complication of general myelitis, hemorrhage in the cord, and syringo-myelitis, it is argued that the trophic centres whose destruction is the cause of these bed-sores lie in the central gray matter of the cord, near to the central canal. In unilateral lesion of the cord the bed-sore occurs on the anæsthetic side of the body—i.e. on the side opposite to the seat of the lesion—a fact which may indicate a decussation of the trophic nerve-fibres in the cord,93 but which has also been urged in proof of the theory that the sore is always due to irritation of an insensitive surface.
93 Recklinghausen believes that these cases of disturbance of nutrition can be explained by injury of anæsthetic parts in which vaso-motor disturbances of central origin exist (Handbuch d. Path. d. Ernahrung, pp. 236, 237).
The treatment of bed-sores belongs to the domain of surgery, the same methods being pursued as in the case of any large ulcer. The application of electricity to the sore has been tried, but the results are not sufficiently encouraging to warrant its recommendation.
Joint affections of neurotic origin are discussed in the articles upon Locomotor Ataxia, Hemiplegia, and Hysteria.
It is evident from this review that the nervous centres have some influence upon the activity of the cells of which the body is made up, and that they control the processes of growth, function, repair, and reproduction. The facts are too numerous, too varied, and too positive to admit of any other explanation. Trophic disturbances must therefore be considered as a set of symptoms referable to various lesions of the nervous system. It is evident from the preceding discussion that they may be produced by disease of the peripheral nerves; by disease of the ganglionic cells, which nourish those nerves; by disease of the spinal cord, especially in the region of the central gray matter; and, finally, by disease of the brain. Whether in the last condition the effect is a direct one, or is produced secondarily by an irritation of the spinal centres, cannot yet be determined. There are no trophic centres as yet localized in the cerebrum, but the pathological facts already mentioned warrant the conclusion that such centres will not long elude search. Certain facts observed in cases of infantile hemiplegia point to the motor area of the cortex as the seat of trophic centres for the motor mechanisms; since it is found that when the motor cortex is destroyed in early life the bones and muscles [p. 1276] which it controls fail to develop properly. Trophic centres for sensory mechanisms are not yet discovered. Certain investigations of Luciani recently published94 point to the cerebellum as the part of the brain which governs the general nutrition of the body, but these need confirmation.
94 Alienist and Neurologist, July, 1885.
CONCLUSION.—While an attempt has been made here to consider vaso-motor and trophic neuroses separately, it must be admitted that in very many conditions the two are coincident. This follows inevitably from what has been stated regarding the localization of the vaso-motor and trophic centres in the spinal cord, and regarding the course of the vaso-motor and trophic nerves from the spinal centres to the periphery. These two classes of centres and nerves lie side by side in the central and peripheral organs, and it is less surprising that they should be jointly affected than that one should ever be involved alone. In any case of lesion of the peripheral nerves or of the central nervous system they may be expected. In all cases they are to be regarded as symptoms of such lesions rather than as distinct diseases.